Magnetic Resonance Imaging of Intracranial Tumors in Children and ...

Introduction
The pathogenesis of germ cell tumors (GCTs) is unknown.These tumors have been classified as germinoma, tera-toma, choriocarcinoma, endodermal sinus tumor, embryo-nal carcinoma, and mixed GCT [7, 12]. The outcome ofintracranial germinoma has been dramatically improved[11], but malignant intracranial GCTs, such as immatureteratoma, choriocarcinoma, endodermal sinus tumor, andembryonal carcinoma, still have a poor prognosis [7, 15].The study of multiple primary neoplasms may yield someinsight into the pathogenesis of such tumors [3]. There havebeen few reports of multicentric intracranial GCTs otherthan synchronous lesions in the pineal and suprasellar re-gions (GCTSPS) [7, 13]. We describe a rare case of mul-tiple intracranial GCTs with sequential occurrence.
Case report
First admission
An 8-year-old boy was initially admitted in November 1988 with leftleg numbness. Neurologic examination revealed slight left motorweakness. Computed tomography (CT) demonstrated a cystic masswith calcification and slight contrast enhancement in the right basalganglia (Fig. 1 upper left). There was an abnormal serum level of α-fetoprotein (AFP) (36 ng/ml). Histologic examination of the spec-imens from stereotactic biopsy revealed only reactive gliosis. AnOmmaya reservoir was inserted into the cystic cavity. Without his-tologic verification, on the grounds of the characteristic of the tumoras indicated by CT, the age of the patient, the tumor location, and theabnormal serum level of AFP, this tumor was clinically diagnosedas a GCT mixed with nongerminomatous GCTs, such as endodermalsinus tumor or embryonal carcinoma with teratomatous elements. Atotal dose of 50 Gy in daily fractions of 2 Gy over 5 weeks was de-livered to the local brain field by parallel opposed ports. The tumordisappeared completely, leaving only calcification (Fig. 1 upperright). The patient was followed up with CT or magnetic resonanceimaging (MRI) performed every 6–12 months. There was no recur-rence according to MRI in December 1993.
Child’s Nerv Syst (1997) 13:178–181© Springer-Verlag 1997 CASE REPORT
Multiple intracranial mixed germ cell tumorsToshihiro KumabeTeiji TominagaTakashi YoshimotoTakamasa Kayama
Abstract A case of sequential oc-currence of multiple intracranialmixed germ cell tumors is presented.An 8-year-old boy with a cystic cal-cified tumor in the basal ganglia andan increased serum α-fetoproteinconcentration was initially treatedwith radiotherapy. Six years later, atumor composed of embryonal carci-noma and immature teratoma arosefrom the right temporo-parietal lobe.This tumor was treated successfullywith surgery and radiochemotherapy.The possibility of multicentricity or
intra-axial metastasis distant fromthe original site during the long-termcourse should be considered in treat-ment for intracranial germ cell tumors.
Key words Embryonal carcinoma ·Immature teratoma · Brain neoplasm ·Mixed germ cell tumor · Multiplicity
Received: 6 November 1995Revised: 17 July 1996
T. Kumabe (½) · T. TominagaT. YoshimotoDepartment of Neurosurgery, Tohoku University School of Medicine, 1-1 Seiryo-machi, Aoba-ku, Sendai, 980-77 JapanTel.: (81) 22-274-1111,ext. 2333 or 273-9295Fax: (81) 22-272-9539
T. KayamaDepartment of Neurosurgery, Yamagata University School of Medicine,Yamagata, Japan

179
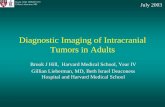
Fig. 1 Sequential neuroimages. Upper left axial contrast-enhancedCT on first admission, demonstrating a cystic tumor with some cal-cification in the right basal ganglia. Upper right axial contrast-enhanced CT after local radiation, demonstrating complete dis-appearance of the tumor, leaving only calcification. An Ommaya reservoir was inserted into the cystic cavity (arrowhead). Lower leftaxial gadolinium-enhanced T1-weighted MRI on second admission,demonstrating a large tumor with heterogeneous enhancement in the right temporo-parietal lobe. The basal ganglia was unchanged.Lower right axial gadolinium-enhanced T1-weighted MRI after sur-gical resection, showing no residual tumor and no continuity withthe initial lesion in the right basal ganglion
Second admission
The patient complained of headache and nausea in August 1994. InNovember, he complained of gait disturbance and deteriorated pro-gressively, requiring readmission. Neurologic examination revealeda bilateral abducent nerve palsy, left homonymous hemianopsia, andleft hemiparesis. The right pupil was larger than the left and reactedsluggishly to light. Bilateral papilledema was present. MRI demon-strated a large tumor in the right temporo-parietal lobe with hetero-geneous enhancement (Fig. 1, lower left). The right basal gangliawas unchanged. The right posterior temporal artery and angular ar-tery appeared to supply the tumor. His serum AFP level had increasedto 84 ng/ml.
A right temporo-parieto-occipital craniotomy was performed inNovember 1994. The cortex overlying the tumor was normal. Thewell-demarcated tumor was resected completely. The tumor had anirregular, lobulated surface. The cut surface revealed its teratoma-tous nature by the presence of cartilage.
Histologic examination
Histologic examination revealed foci of embryonal carcinoma ad-mixed with immature teratoma (Fig. 2). The immature teratomatouslesion was composed of immature elements derived from all threegerm layers, that is, mesenchymal, neuroectodemal, and epithelialtissues with embryonic features. A dense proliferation of large po-lygonal tumor cells with foamy cytoplasm and irregularly roundedpale nuclei forming an epithelial arrangement were seen alongsideimmature teratomatous elements. There were globular intra- and ex-tracellular eosinophilic masses, which were positive for PAS andAFP. These malignant epithelial cells were identified as embryonalcarcinoma.
The patient recovered except for slight left motor weakness andleft homonymous hemianopsia. MRI after resection showed no re-sidual tumor (Fig. 1, lower right). He received 50 Gy of radiothera-py locally to the temporo-occipital region, followed by adjuvantchemotherapy with cisplatin (CDDP) and etoposide. The serum AFPlevel returned to the normal range.
Discussion
As far as the intracranial examples are concerned, the terms‘embryonal carcinoma’ and ‘endodermal sinus tumor’have often been used interchangeably [12]. For the diag-nosis of endodermal sinus tumor, Bjornsson et al. [2] re-quired the presence of endodermal sinuses (Schiller-Du-val bodies) and extracellular or intracellular PAS-positiveand diastase-resistant globules immunoreactive for AFP.In our case, the presence of Schiller-Duval bodies was notconfirmed. Thus, the malignant epithelial cells in the tu-mor arose from right temporo-parietal lobe, and the tumorwas diagnosed as embryonal carcinoma.
Intracranial GCTs disseminate by infiltration into adja-cent brain, or via ventricle and subarachnoid pathways [7].To our knowledge, there are no reports describing intra-axial remote metastasis from primary intracranial GCT. Inour case, the second tumor in the right temporo-parietallobe was not continuous with the initial tumor, as indicatedby both radiological and histologic findings. There wereno tumor cells in the cortex overlying the tumor on histo-logic study. Thus, it is less likely that the second tumor wasdue to direct infiltration or dissemination via the cerebro-spinal fluid pathway. Further, the blood supply of the sec-ond tumor derived from the cortical branches of the mid-dle cerebral artery, but not from the perforating arteries andchoroidal arteries that supplied the initial tumor. There-fore, it seems more likely that these GCTs were multicen-tric in origin, rather than the results of metastatic dissem-ination.
Swischuk and Byran [14] have reported four patientswith intracranial GCT presenting with synchronous lesionsin the pineal and suprasellar regions (GCTSPS). They described this presentation as “double midline atypical teratoma.” After the introduction of MRI, a higher fre-quency of GCTSPS was found than before. In Europe andNorth America, GCTSPS accounts for approximately 6%

180
of intracranial GCTs [7]. In Japan, GCTSPS accounts formore than 10% of all intracranial GCT [13]. It is unclearwhether GCTSPS is of multicentric origin or representsmetastatic spread. There are few reports of multicentricintracranial GCT other than GCTSPS. Miyamachi et al.[10] have described a case of multiple mature teratomaslocated in the suprasellar region and the septum pellu-cidum. Aoyama et al. [1] reported the same lesions in the pineal region and the IV ventricle. Bilateral testicularGCT occurs in 2–5% of all patients with testicular GCT.Mostly these are sequential and not synchronous [8], as inour case.
While GCT may arise because of neoplastic changesduring embryonic development, the pathogenesis of intra-cranial GCT is still uncertain. It may be due to germinalmalmigration, embryonic “cell rests” or a localized hamar-tomatous or dysplastic process [4, 7]. Kratzik et al. [8] sug-gested that genetic factors might be important in the de-velopment of sequential bilateral testicular GCT. Theremight be some genetic aberrations in our case. Geneticanalysis with advanced molecular techniques seems topromise progress in clarifying the pathogenesis of intra-cranial GCT [9].
In our case, the second tumor occurred just outside theradiation field. We might have prevented the second tumorwith whole brain radiation. However, myelosuppression,mental and physical deterioration, and endocrinologic dysfunction are serious problems after such radiotherapy[11]. Chemotherapy may minimize the radiation dose andfield [11, 15]. CDDP-based combination chemotherapyhas been reported to be effective in intracranial GCT [5, 6, 15].
For any cases of intracranial GCT, long-term follow-upby neuroimaging and serial determinations of the serumlevels of AFP and β-HCG (β-human chorionic gonadotro-pin) should be done to look for recurrence of the initial tu-mor and the sequential occurrence of multiple GCT.
Fig. 2 A–C Photomicrographs of the various portions of immatureteratoma. A Magnified view of neuroepithelial rosette. B Large areas of rhabdomyoblastic differentiation. C Ductal cells. D Photo-micrograph of the tumor, showing a dense proliferation of large polygonal tumor cells with foamy cytoplasm and irregularly rounded pale nuclei, forming an epithelial arrangement. These pre-sented globular intra- and extracellular eosinophilic masses whichwere positive for periodic acid–Schiff (PAS) and AFP (arrowhead).The presence of endodermal sinuses (Schiller-Duval bodies) was notconfirmed in our case. Thus, these malignant epithelial cells wereidentified as embryonal carcinoma. (H&E, original magnification A ×400, B,C ×100, D ×200

181
1. Aoyama I, Makita Y, Nabeshima S,Motomochi M (1982) Intracranial double teratomas. Surg Neurol17:383–387
2. Bjornsson J, Scheithauser BW, Oka-zaki H, Leech RW (1985) Intracranialgerm cell tumors: pathological and im-munohistochemical aspects of 70 cases.J Neuropathol Exp Neurol 44:32–46
3. Dieckmann K-P, Wegner HEH, Krain J(1994) Multiple primary neoplasms inpatients with testicular germ cell tumor. Oncology 51:450–458
4. Horowitz MB, Hall WA (1991) Centralnervous system germinomas. ArchNeurol 48:652–657
5. Itoyama Y, Kochi M, Yamamoto H,Kuratsu J, Uemura S, Ushio Y (1990)Clinical study of intracranial nonger-minomatous germ cell tumors produc-ing α-fetoprotein. Neurosurgery27:454–460
6. Itoyama Y, Kochi M, Kuratsu J, Taka-mura S, Kitano I, Marubayashi T, Uemura S, Ushio Y (1995) Treatmentof intracranial nongerminomatous malignant germ cell tumors producingα-fetoprotein. Neurosurgery36:459–466
7. Jennings MT, Gelman R, Hochberg F(1985) Intracranial germ-cell tumors:natural history and pathogenesis. J Neurosurg 63:155–167
8. Kratzik C, Aiginger P, Kuber W, Ric-cabona M, Kuhrer I, Joos H, Frick J,Amann G, Mayr W (1991) Risk factorsfor bilateral testicular germ cell tumors. Cancer 68:916–921
9. Leon SP, Zhu J, Black PM (1994) Genetic aberrations in human brain tumors. Neurosurgery 34:708–722
10. Miyamachi T, Abe H, Tashiro T, AidaT (1986) A case of multiple teratomascombined with embryonal carcinoma.Neurol Surg 14:1161–1165
11. Ono N, Kakegawa T, Zama A, Naka-mura M, Inoue HK, Tamura M, WakaoT, Uki J, Takeda F, Kurihara H, Shimi-zu T, Handa I (1994) Factors affectingfunctional prognosis in survivors ofprimary central nervous system germi-nal tumors. Surg Neurol 41:9–15
12. Russel DS, Rubinstein LJ (1989) Pathology of tumors of the central ner-vous system, 5th edn. Arnold, London
13. Sugiyama K, Uozumi T, Kiya K, Mu-kada K, Arita K, Kurisu K, Hotta T,Ogasawara H, Sumida M (1992) Intra-cranial germ-cell tumor with synchro-nous lesions in the pineal and suprasel-lar regions: report of six cases and re-view of the literature. Surg Neurol38:114–120
14. Swischuk LE, Bryan RN (1974) Double midline intracranial atypicalteratomas. AJR Am J Roentgenol122:517–524
15. Yoshida J, Sugita K, Kobayashi T,Takakura K, Shitara N, Matsutani M,Tanaka R, Nagai H, Yamada H, Yama-shita J, Oda Y, Hayakawa T, Ushio Y(1993) Prognosis of intracranial germcell tumours: effectiveness of chemo-therapy with cisplatin and etoposide (CDDP and VP-16). Acta Neurochir(Wien) 120:111–117
References