Multi-Indication Pricing: Pros, Cons and Applicability to the UK
18
Jorge Mestre-Ferrandiz*, Adrian Towse*, Renato Dellamano** and Michele Pistollato***; *Office of Health Economics; ** MME Europe and ValueVector; *** formerly OHE Multi-Indication Pricing: Pros, Cons and Applicability to the UK
-
Upload
kerry-sheppard -
Category
Presentations & Public Speaking
-
view
41 -
download
0
Transcript of Multi-Indication Pricing: Pros, Cons and Applicability to the UK

Jorge Mestre-Ferrandiz*, Adrian Towse*, Renato Dellamano** and Michele Pistollato***; *Office of Health Economics; ** MME Europe
and ValueVector; *** formerly OHE
Multi-Indication Pricing: Pros, Cons and Applicability to the UK

AES 2016
Agenda• Context• Aims• Methodology• Results• Discussion• Conclusion

AES 2016
What is MIP, and why do we care?
• Multi-indication pricing (MIP) involves setting a different price for each indication approved for the medicine
• Many medicines currently available, and many more in pharmaceutical industry pipelines, are likely to be effective in multiple indications – oncology prime example
• Assessment of value for oncology products more complex• Prices paid for branded medicines should aim to reflect
their value – thus, for multi-indication medicines, prices should be different across indications to reflect their different values
• Yet current pricing and reimbursement systems are not equipped to handle this

AES 2016
The case for …a single, uniform, price across indications has negative consequences
• There tends to be one single (uniform) price across all indications => price and clinical value will rarely match up across multiple indications
• Single price based on higher-valued indications• higher than optimal for one or more lower-value uses/indications,
leading to restricted access• Single price based on lower value indications
• discourage development of further potentially higher-value indications• Both consequences are sub-optimal from society’s point of view• Multiple indication (or patient sub-group) pricing increases the
numbers of patients receiving treatment• Some current pricing models do allow for what is termed as
“blended” pricing – mostly volume driven

AES 2016
We can illustrate the challenge of differential value by indication or patient sub-group ….
Source: Hebborn A. Value-based pricing across indications: A company perspective. ISPOR Montreal, 3 June 2014, used in Pearson S, Dreitlein B, Henshall C (2016)

AES 2016
Previous literature (1)

AES 2016
Previous literature (2)

AES 2016
Aims
1. Can MIP be a flexible pricing scheme that delivers a sustainable solution?
2. If it does, can MIP be implemented in the UK, and how?

AES 2016
Methodology
OHE BRIEFING
UK WORKSHOP
DESK RESEARCHConceptual Analysis International Examples
Explore the pros and cons of multi-indication pricing (MIP), its barriers and facilitators

AES 2016
Summary on international case studies• Based on a relatively limited set of examples, MIP seems
practically applicable, in certain countries and conditions
• Especially in the case of drugs approved as different medicinal products in different disease areas, extreme price differences seem to be achievable

AES 2016
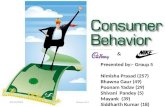
Aflibercept (Eylea in ophthalmology & Zaltrap in oncology)– Comparison of per mg Prices (Official/Visible Ex-factory Price Level)
EU5 + Switzerland averageZaltrap= £2.95
EU5 + Switzerland averageEylea= £176.66
France Germany Italy Spain UK Switzerland £-
£20
£40
£60
£80
£100
£120
£140
£160
£180
£200
£155.87
£195.23
£171.10
£162.77
£198.33
£182.04
£2.48 £3.23 £3.32 £3.16 £2.59 £2.94
Exchange Rates: 90 days average Sep-Dec 2014 (rates in appendix)
Sources: MME analysis of country drug compendia and institutional websites
Ex-
Fact
ory
Pric
e
Separation is helped by dosage form. Oncology use is an infusion; ophthalmology use is pre-filled syringes

AES 2016
Summary on international case studies• In the case of multiple indications approved for the
same medicinal product• MIP seems to be achievable in some countries, in
particular, in Italy and (potentially) in the UK• Other countries, in particular, France, prefer a “blended”
pricing approach, with across the board price cuts when the composite value proposition of the medicinal product changes over time as a consequence of the availability of new clinical evidence

AES 2016
Results (1)Framework to outline possible MIP schemes for medicines with
multiple indications

AES 2016
Results (2): Using the Systematic Anti-cancer Therapy (SACT) dataset

AES 2016
Results (3)Is MIP possible in the UK? Two operational challenges:
1. Whether the NHS can handle MIP schemes involving variable net selling prices by indication, requiring monitoring of volume usage per patient per indication, and undertake any financial reconciliation ex post to ensure that the correct funds flow across the necessary stakeholders, be it at national or local level
2. Data availability: are there data sets which allow such monitoring of volume usage per patient per indication, and is the necessary data being generated routinely or requiring ad hoc intervention?
• Separate branding by indication can work but significant costs attached to this, and still potential for arbitrage

AES 2016
Discussion• Intrigued by potential use of MIP
• Support value reflective pricing• There is a need to ensure collaboration across all
stakeholders (NHS, industry, patients, doctors, nurses and other health care professionals) if the NHS were to benefit from any future pricing scheme(s) that allow different prices across indications.
• If MIP were pursued, there was interest in using either (i) “blended” pricing (at list level) or (ii) schemes that might generate variable “net” selling prices.
• NHS’s Systemic Anti-cancer Therapy (SACT) data can in principle support the implementation of MIP, albeit with challenges. The current UK collaboration will help us understand whether the SACT dataset could in practice underpin such pricing systems

AES 2016
Conclusion• Handling multiple indications within the same disease
area – including different potential lines of treatment and/or combination regimens – is a challenge
• Innovative pricing schemes require potential to track the specific utilisation of the drug in its different indications, regimens and patient sub-populations
• The (limited) international experience shows that certain health systems have already accumulated significant experience in the form of indication-specific net selling-price arrangements, both at the national and at the sub-national levels
• There is also a need to consider the dynamic-pricing case, given the interest in adaptive pathways

AES 2016
To enquire about additional information and analyses, please contact Dr. Jorge Mestre-Ferrandiz at [email protected] To keep up with the latest news and research, subscribe to our blog, OHE NewsFollow us on Twitter @OHENews, LinkedIn and SlideShare
Office of Health Economics (OHE) Southside, 7th Floor105 Victoria StreetLondon SW1E 6QT United Kingdom+44 20 7747 8850 www.ohe.org
OHE’s publications may be downloaded free of charge for registered users of its website.