Multi drug resistant
31
MULTI-DRUG RESISTANT TUBERCULOSIS &EXTENSIVE D, RESISTANT MDR&XDR DR/HESHAM BEN ISSA GP,ABUSITTA HOSPITAL
-
Upload
hiba-ashibany -
Category
Health & Medicine
-
view
32 -
download
1
Transcript of Multi drug resistant

MULTI-DRUG RESISTANTTUBERCULOSIS
&EXTENSIVE D, RESISTANTMDR&XDR
DR/HESHAM BEN ISSA GP,ABUSITTA HOSPITAL

Presentation OutlineDEFINITION
CAUSES EPIDEMIOLOGYPRESENTATIONMANAGEMENT
MONITORINGPREVENTION
CONCLUSION
Drug-Resistant TB: Definitions
DEFINITIONS OF DRUG RESISTANCEMono-resistant: Resistance to a single
drug (e.g INH Only).Poly-resistant(non-MDR): Resistance to more
than one drug, but not the combination of isoniazid and rifampicin.
Multidrug-resistant (MDR): Resistance to at least isoniazid and rifampicin.
Extensively drug-resistant (XDR): MDR plus resistance to fluoroquinolones and at least 1 of the 3 injectable drugs (amikacin, kanamycin, capreomycin).
REPORTING PURPOSES
Primary drug-resistance: “New Cases”Drug resistance in a patient who has never been treated for tuberculosis or received less than one month of therapy
Secondary (acquired) drug-resistance:“Previously Treated Cases”
Drug resistance in a patient who has received at least one month of anti-TB therapy

Causes of DR&/MDR
EPIDEMIOLOGY

Estimated absolute numbers of reported cases with MDR-TB*Notified cases of MDR-TB
Cases of MDR-TB
0–99
100–999
1000–9999
≥10 000
NA

Distribution of MDR-TB among new TB cases, 1994-2010.
0-<3
3-<6
6-<12
12-<18
>18
No data available
Subnational data only

Distribution of MDR-TB among previously treated TB cases, 1994-2010
0-<6
6-<12
12-<30
30-<50
>50
No data available
Subnational data only

Epidemiology
Some of the highest statistics of HIV and multi-drug resistant tuberculosis co-infection are seen in sub-Saharan Africa where HIV/AIDS
prevalence is so high .Currently, world wide MDR-TB mortality rates are at about “40-60% depending on the country of residence and access to immediate care”. These rates are consistent with the rates of untreated tuberculosis

Notifications of MDR-TB increasing
•Notified cases of MDR-TB
•MDR-TB cases treated and estimated numbers
not treated for MDR-TB, among notified TB
patients, 2010
0
10
20
30
40
50
60
2005 2006 2007 2008 2009 2010
Nu
mb
er
of
pa
tie
nts
(th
ou
sa
nd
s)
0
50
100
150
200
250
300
SE Asi
a
W. P
acifi
c
Europe
Africa
EMR
Americ
as
World
Not on treatment
Treated

Why INH and Rifampin
Most potent and bacteriocidalTb can be treated effectively with INH+Rif aloneMono-resistance to one of them can be treated effectively with a regimen containing the other agent with very low failure rate (2.5-5%)Failure rate when INH+Rif resistant is 44% in non-HIV and 70% in HIV patientsDuration required for cure doubles to triples.

PresentationSneezingcoughing
deep cough with bloody sputumchest pain
Chillsunintended weight loss
slight fevernight sweats
loss of appetitepain with breathing

MANAGEMENT

DiagnosisHistory is IMPORTANT
Mantoux tuberculin skin test (TST) chest radiograph
QuantiFERON-TB Gold test (QFT-G)The presence of acid-fast bacilli on a sputum
smear may aid in the diagnosis of tuberculosis, but it is not 100% diagnostic .
The definitive diagnosis is made with a culture of the smear .
susceptibility testing by culture and sensitivity

Predictors of Drug-resistant TB
Assess drug resistance in any patient being started on treatment for tuberculosis
Non-adherence, defaultHistory of prior treatment
Exposure to possible drug-resistant source caseCommunity prevalence of drug resistance
If drug resistance is suspected based on any of the above factors, culture and susceptibility testing should be performed for at least INH and rifampicin

Categories of Anti-TB MDR Drugs: WHO
Group 1 – First-line drugs: Isoniazid , rifampicin , ethambutol , pyrazinamide
Group 2 - Injectable agents: Kanamycin, amikacin, capreomycin, streptomycin
Group 3 - Fluoroquinolones: Levofloxacin, moxifloxacin, ofloxacin
Group 4 - Oral bacteriostatic agents: Ethionamide, cycloserine, para-aminosalicylic acid (PAS), prothionamide, terizadone
Group 5 – Unclear role: Clofazamine, linezolid, amoxicillin/clavulanate, Imipenem/cilastatin, thioacetazone, high-dose isoniazid, clarithromycin
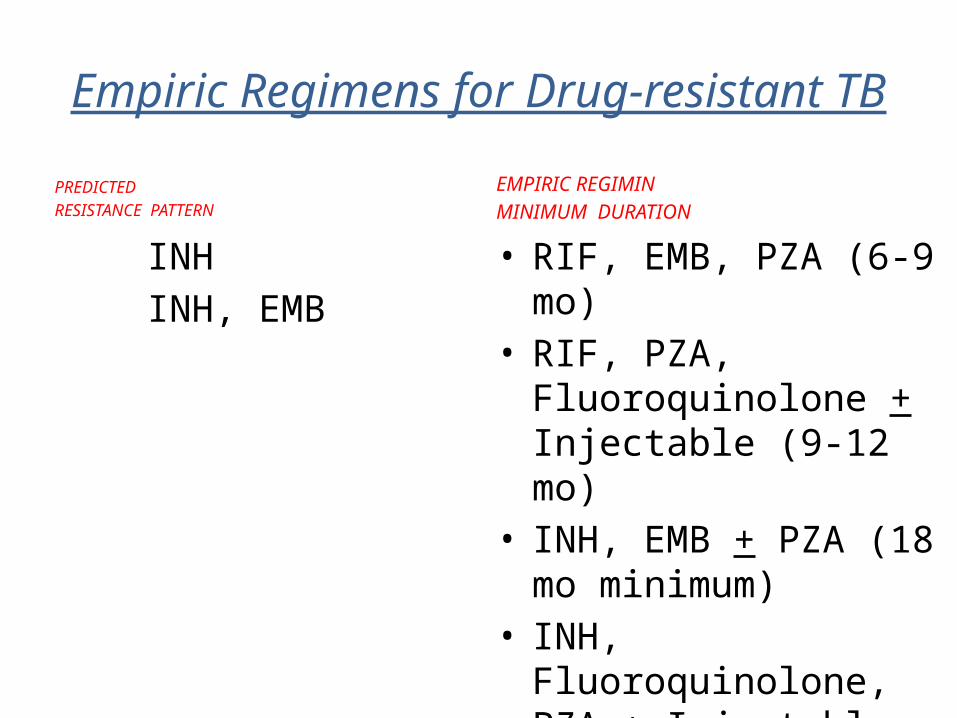
Empiric Regimens for Drug-resistant TBPredicted
Resistance Pattern
PREDICTEDRESISTANCE PATTERN
INH INH, EMB
RIF
RIF, EMB
Empiric Regimen
(minimum duration)
EMPIRIC REGIMINMINIMUM DURATION
• RIF, EMB, PZA (6-9 mo)• RIF, PZA, Fluoroquinolone +
Injectable (9-12 mo)• INH, EMB + PZA (18 mo
minimum)• INH, Fluoroquinolone,
PZA + Injectable (18-month minimum)

“I have been treated several times over the past five years and I’m still coughing and can’t gain weight”!

Empiric Regimens for MDR-TBPREDICTED RESISTANCE PATTERN
INH, RIF INH, RIF, EMB
INH, RIF, PZA
INH, RIF, PZA, EMB
EMPIRIC REGIMIN
• Fluoroquinolone, PZA, EMB, Injectable Fluoroquinolone, PZA, Injectable, CS, + PAS or ETH
• Fluoroquinolone, EMB, Injectable, CS, + PAS or ETH
• Fluoroquinolone, Injectable, CS, PAS or ETH, + one more drug

Common Adverse Effects• G.I. complaints
• Hepatotoxicity(early symptoms are anorexia and
malaise, then abdominal pain, vomiting, jaundice)
• Ethionamide CycloserinePAS Fluoroquinolones Clofazimine Rifabutin
• INH Rifampicin/rifabutin Ethionamide PZA PAS Fluoroquinolones

Common Adverse Effects
PERIPHERAL NEUROPDATHY
RASH
HEADACHE
SEIZURES
• INH • Ethionamide • Cycloserine • Linezolid• Ethambutol• All• Fluoroquinolones • Isoniazid • Cycloserine • Ethionamide • Ethambutol• Cycloserine

Common Adverse Effects
• HypothyroidismHEARING LOSS&VESTIBULAR TOXICITY
BEHAVIORAL CHANGES
VISUAL CHANGES
RENAL F• HYPOKALEMIA
• Ethionamide, PAS• Aminoglycosides,
Capreomycin• Cycloserine,
Ethionamide, Isoniazid, Fluoroquinolones
• Ethambutol, Rifabutin, Isoniazid, Linezolid
• Aminoglycosides, Capreomycin

MDR/XDR-TB: MonitoringCLINICALLY
SIGNS OF TREATMENT FAILUREPERSISTANT OR NEW WT LOSS
PERSISTANT OR DEVELOPING NEW TB SYM ASFEVER ,COUGH,
PERSISTANT SPUTUM POSITIVE RESULT OR POS CULTURE SMEAR.

MDR/XDR-TB: MonitoringLAB
CBC UREA,E,C
LFT AST,ALT,BILIRUBINPREGNANCY TEST FOR WOMEN
TSH AT SECOND MONTH FOR EARLY DETECTION OF HYPOTHYRODISM

How is MDRTB prevented?MDRTB is a condition that can be prevented by following the international TB control strategy called DOTS, which stands for Directly Observed Treatment, Short-course.
Health care providers should always adhere to the National Tuberculosis Program Guidelines and use only the recommended anti-TB treatment regiments, drug combinations and drug dosages.Anti-TB drugs, preferably Fixed Dose Combinations of high quality should be
available in regular and sufficient quantities .
Adherence to anti-TB treatment must be ensured with support, encouragement and monitoring of adherence by a relative, community volunteer, or a clinic nurse.

XDR-TB

CAUSES OF DEATH AMONG MDR &XDR
RESPIRATORY ARRESTADVERSE DRUG REACTIONSSEPTIC SHOCKPROGRESSION OF HIV DISEASEMASSIVE HAEMOPTYSISARF

Conclusion
MDR-TB is a problem!As PAs we must follow our appropriate procedures for diagnosing, reporting, and treatingWe can be effective globally with our time, education, supporting research for vaccines, etc.

THANKS