Multi-Center Pediatric CRRT Registry
26
pCRRT Multi-Center Registry Data Effective April 1, 2002 Multi-Center Pediatric CRRT Registry Stuart L. Goldstein, MD Assistant Professor of Pediatrics Baylor College of Medicine
-
Upload
xenos-guerra -
Category
Documents
-
view
28 -
download
2
description
Multi-Center Pediatric CRRT Registry. Stuart L. Goldstein, MD Assistant Professor of Pediatrics Baylor College of Medicine. Overview. Registry study phases Study design Study aims Current participating centers Institutional practice protocol variation Current data analysis. - PowerPoint PPT Presentation
Transcript of Multi-Center Pediatric CRRT Registry

pCRRT Multi-Center Registry Data Effective April 1, 2002
Multi-Center Pediatric CRRT Registry
Stuart L. Goldstein, MDAssistant Professor of Pediatrics
Baylor College of Medicine

pCRRT Multi-Center Registry Data Effective April 1, 2002
Overview
• Registry study phases– Study design
– Study aims
• Current participating centers– Institutional practice protocol variation
• Current data analysis

pCRRT Multi-Center Registry Data Effective April 1, 2002
pCRRT Registry: Phase 1 Design
• Collect prospective data from 5 to 10 pediatric centers treating 15 to 20 patients annually (200-300 patients over 3 years)
• Each center follows own institutional practice– Patient selection
– Initiation and termination
– Anti-coagulation protocols
– Convection versus diffusion versus hemodiafiltration
– Fluid composition
• Cytokine clearance study

pCRRT Multi-Center Registry Data Effective April 1, 2002
pCRRT Registry: Phase 1 Aims
• Assess for potential associations between various practices and pediatric patient outcomes
• Assess for potential associations between varying practices and CRRT machine functioning
• Determine CRRT clearance rates of various SIRS and CARS cytokines in children with sepsis

pCRRT Multi-Center Registry Data Effective April 1, 2002
Current Registry Centers and PI
• Texas Children’s Hospital (January 2001)• Boston Children’s Hospital (March 2001)• Seattle Children’s Hospital (July 2001)• Univ of Alabama Children’s (July 2001)• Univ of Michigan (December 2002)
• Stuart Goldstein, MD• Michael Somers, MD• Jordan Symons, MD• Timothy Bunchman, MD• Patrick Brophy, MD Melissa
Gregory, MD

pCRRT Multi-Center Registry Data Effective April 1, 2002
Pre-CRRT Registry Data
• Demographics– Primary disease, co-morbid illness, age, gender, days in PICU
• CRRT specifics– Treatment or prevention of fluid overload and/or electrolyte
imbalance
– Access size and site
• Renal failure indices– GFR (Schwartz)
– Percent fluid overload (%FO)
– Urine output in previous 24 hours

pCRRT Multi-Center Registry Data Effective April 1, 2002
Registry PICU Data
• PRISM 2 at ICU admission and CRRT initiation• CRRT initiation
– CVP
– MAP
– Pressor number and specific drugs
– Diuretic use
• CRRT course– Maximum pressor number
– MAP change
– Pressors weaned?

pCRRT Multi-Center Registry Data Effective April 1, 2002
pCRRT Registry Circuit Data
• Separate data page for each circuit
• Machine brand
• Extracorporeal volume
• Priming fluid– NS
– albumin
– blood mixed with • FFP, albumin, or bicarbonate
• Dialysis or replacement fluid composition– Normocarb™ (Dialysis Solutions, Inc)
– Baxter hemofiltration fluid™
– Saline, Ringer’s lactate, peritoneal dialysis fluid

pCRRT Multi-Center Registry Data Effective April 1, 2002
pCRRT Registry Circuit Data
• Anticoagulation– Citrate
– Heparin rate• ACT measured per hour
• Mean ACT
• # ACT < 180 seconds
• Clearance prescription– CVVH versus CVVHD versus CVVHDF
– ml/1.73m2/hour
• Nutrition prescription– Kcal/kg/day
– Grams protein/kg/day

pCRRT Multi-Center Registry Data Effective April 1, 2002
pCRRT Registry Patient Data: Outcome
• Survival versus death (discharge from PICU)• Attainment of target dry weight• Reason to discontinue CRRT
– Death
– Regained renal function
– Underlying illness resolved
– Tolerates intermittent hemodialysis

pCRRT Multi-Center Registry Data Effective April 1, 2002
pCRRT Registry Circuit Data: Outcome
• Filter life-span (hours)• Reason for circuit change
– clotting
– access malfunction
– machine malfunction
– unrelated patient indication (e.g., needs CT scan)
– CRRT discontinued

pCRRT Multi-Center Registry Data Effective April 1, 2002
pCRRT Registry: Results (4/1/2002)
• 42 patients entered into study• 36 with complete data• 128 circuits• 4905 cumulative treatment hours
– Mean 41.2 + 28.9 hours
– Range 1 to 118 hours

pCRRT Multi-Center Registry Data Effective April 1, 2002
Baseline Demographics
Age 8.2 + 7.3 years
Weight 33.8 + 28.4 kg
GFR 35.3 + 25.3 ml/min/1.73m2

pCRRT Multi-Center Registry Data Effective April 1, 2002
Registry Center Census
Center
Pa
tien
ts
0
2
4
6
8
10
12
14
16
18
20
Houston Boston UAB Seattle

pCRRT Multi-Center Registry Data Effective April 1, 2002
Primary Disease
Primary Disease
Pa
tien
ts
0
1
2
3
4
5
6
7
8
9
10
Se
psi
s
Ca
rdio
myo
pa
thy
RV
T
BM
T
AT
N
CV
Sh
ock
Tu
mo
r Ly
sis
AM
L
Bo
we
l Pe
rf
Me
tab
x
FO
MO
SF
Ne
ph
rtx
Me
tab
olic
AR
F
HU
S
pCRRT Multi-Center Registry Data Effective April 1, 2002
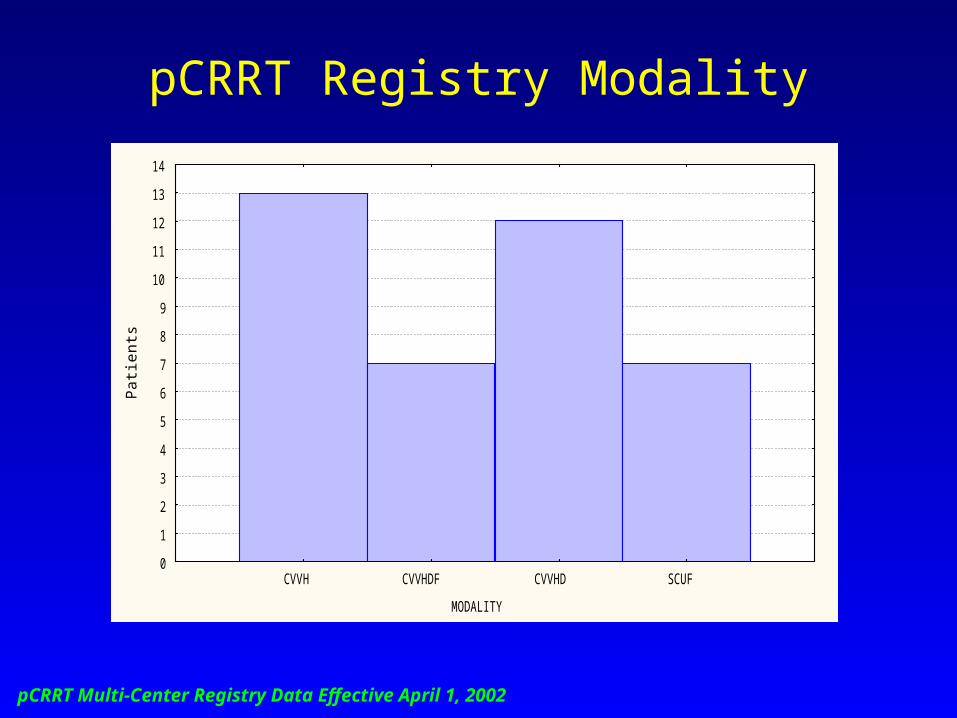
pCRRT Registry Modality
MODALITY
Pa
tien
ts
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
CVVH CVVHDF CVVHD SCUF

pCRRT Multi-Center Registry Data Effective April 1, 2002
Reason to Start CRRT
Reason to Start CRRT
Pa
tien
t N
um
be
r
35.9% 35.9%
12.8%
7.7% 7.7%
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
FO Only FO and EI EI Only Other Prevention of FO

pCRRT Multi-Center Registry Data Effective April 1, 2002
Outcome
OUTCOME
Pa
tien
ts
38.9%
61.1%
0
2
4
6
8
10
12
14
16
18
20
22
24
Death Survival

pCRRT Multi-Center Registry Data Effective April 1, 2002
Clinical Variables and Outcome
• Survival not associated with– GFR
– Pressor number
– MAP
– PRISM at ICU admission
– Age
– Weight
• Survival associated with– PRISM at CRRT initiation
– % Fluid overload at CRRT initiation

pCRRT Multi-Center Registry Data Effective April 1, 2002
PRISM at CRRT Initiation and Outcome
±Std. Dev.
±Std. Err.
Mean
OUTCOME
PR
ISM
AT
CR
RT
In
itia
tion
2
6
10
14
18
22
26
30
Death Survival
P < 0.0005

pCRRT Multi-Center Registry Data Effective April 1, 2002
Fluid Overload and Outcome
±Std. Dev.
±Std. Err.
Mean
OUTCOME
Pe
rce
nt
Flu
id O
verl
oa
d a
t C
RR
T I
niti
atio
n
-5
0
5
10
15
20
25
30
35
40
Death Survival
P < 0.05

pCRRT Multi-Center Registry Data Effective April 1, 2002
Fluid Overload and Outcome:Renal Failure Only
±Std. Dev.
±Std. Err.
Mean
OUTCOME
Pe
rce
nt
Flu
id O
verl
oa
d a
t C
RR
T I
niti
atio
n
-5
0
5
10
15
20
25
30
35
40
Death Survival
P < 0.05

pCRRT Multi-Center Registry Data Effective April 1, 2002
Fluid Overload, Severity of Illness and Outcome
• Greater degrees of fluid overload associated with death, even when controlled for severity of illness by PRISM score (multiple regression analysis; p<0.03)

pCRRT Multi-Center Registry Data Effective April 1, 2002
Circuit Change Reason
Reason to Change Circuit
Cir
cuit
Nu
mb
er
0
3
6
9
12
15
18
21
24
27
30
33
36
Scheduled ChangeClotted
OtherAccess Malfunction
Patient Test

pCRRT Multi-Center Registry Data Effective April 1, 2002
Anticoagulation Method and Circuit Life
±Std. Dev.
±Std. Err.
Mean
Anticoagulation
Cir
cuit
Life
(H
ou
rs)
-10
10
30
50
70
90
Heparin Citrate
P < 0.003
N=69
N=38

pCRRT Multi-Center Registry Data Effective April 1, 2002
pCRRT Registry Future Phases
• Assess association between nutrition and outcome
• Assess cytokine levels and clearance
• Test new products devices safely and efficiently
• Prospective randomized trials– Dose
– Fluid options
– Selective cytokine removal
– Time to intervention
– Disease-specific protocol and outcome
• Web-based for easy access and query