MULTI-CASUALTY INCIDENT POLICY I. PURPOSE · 2020-01-03 · MULTI-CASUALTY INCIDENT POLICY I....
116
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY Policy Reference No.: 8000 Effective Date: XXXX 2010 Review Date: XXXX Supersedes: February 1, 2005 MULTI-CASUALTY INCIDENT POLICY I. PURPOSE This policy supports the San Francisco Emergency Medical Services Multi-Incident Casualty (MCI) Plan. The MCI Plan identifies and delineates the structure and processes for the provision of emergency medical care by local EMS system participants during a MCI event of any size or magnitude. The overall objective of the MCI Plan is to minimize the morbidity and mortality associated with large scale emergency patient care incidents occurring in San Francisco by ensuring the provision of rapid and appropriate emergency medical care to the most possible patients through a coordinated response system based on incident management principles. II. AUTHORITY A. Statutory authorities for the MCI plan include: California Health and Safety Code, Sections 1797.103; 1797.150-153; 1797.204; and 1797.220 California Code of Regulations, Title 19, Division 2, Chapter 1 California Code of Regulations, Title 22, Section 100167 (b) (2 - 3); 100168 (b) (4); and 100169 (a) California Code of Regulations, Title 22, Division 9, Section 100255 California Government Code, Article 9, Section 8605 California Master Mutual Aid Agreement California Emergency Services Act B. The MCI Plan complies with the following standards or has reference the following partner plans: National Incident Management System (NIMS) City and County Emergency Response Plan, April 2008 San Francisco Bay Area Regional Coordination Plan – Medical and Health Subsidiary Plan, March 2008 Firescope Field Operations Guide, ICS 420-1, July 2007 California Standardized Emergency Management System (SEMS) California Disaster Medical Operations Manual from California Emergency Medical Services Authority (draft version 09/09/08) California Disaster Health Operations Manual (Interim version, October 2009) Page 1
Transcript of MULTI-CASUALTY INCIDENT POLICY I. PURPOSE · 2020-01-03 · MULTI-CASUALTY INCIDENT POLICY I....

SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY
Policy Reference No.: 8000 Effective Date: XXXX 2010
Review Date: XXXXSupersedes: February 1, 2005
MULTI-CASUALTY INCIDENT POLICY
I. PURPOSE
This policy supports the San Francisco Emergency Medical Services Multi-Incident Casualty (MCI) Plan. The MCI Plan identifies and delineates the structure and processes for the provision of emergency medical care by local EMS system participants during a MCI event of any size or magnitude.
The overall objective of the MCI Plan is to minimize the morbidity and mortality associated with large scale emergency patient care incidents occurring in San Francisco by ensuring the provision of rapid and appropriate emergency medical care to the most possible patients through a coordinated response system based on incident management principles.
II. AUTHORITY
A. Statutory authorities for the MCI plan include: California Health and Safety Code, Sections 1797.103; 1797.150-153; 1797.204; and 1797.220 California Code of Regulations, Title 19, Division 2, Chapter 1 California Code of Regulations, Title 22, Section 100167 (b) (2 - 3); 100168 (b) (4); and 100169 (a) California Code of Regulations, Title 22, Division 9, Section 100255 California Government Code, Article 9, Section 8605 California Master Mutual Aid Agreement California Emergency Services Act
B. The MCI Plan complies with the following standards or has reference the
following partner plans: National Incident Management System (NIMS) City and County Emergency Response Plan, April 2008 San Francisco Bay Area Regional Coordination Plan – Medical and Health Subsidiary Plan, March 2008 Firescope Field Operations Guide, ICS 420-1, July 2007 California Standardized Emergency Management System (SEMS) California Disaster Medical Operations Manual from California Emergency Medical Services Authority (draft version 09/09/08) California Disaster Health Operations Manual (Interim version, October 2009)
Page 1

Policy Reference No.: 8000 Effective Date: XXXX 2010
III. POLICY
A. The San Francisco Emergency Medical Services MCI Plan is an approved policy and procedure of the Department of Emergency Management - EMS Agency. EMS provider organizations shall comply with the operational roles and standards as defined in the MCI Plan. This includes all San Francisco ambulance providers, dispatch centers, hospitals and relevant Emergency Operations Center or departmental operations center command staff.
B. All San Francisco ambulance providers, dispatch centers, and hospitals shall
develop, maintain and train staff on Emergency Response Plans for their organizations, and maintain disaster supplies and equipment that will allow for a minimum of 72-hours of self-sufficient operations.
IV. TRAINING and EXERCISES
A. All EMS provider organizations shall provide annual training and updates on the San Francisco Emergency Medical Services MCI Plan and participate in regular exercises of that plan with other EMS system participants.
B. EMS provider organizations shall provide training to relevant staff to ensure
proficiency in the following:
1. First Receiver (Hospitals Only) a) Simple Triage and Rapid Treatment (START) and JUMPSTART b) Hospital Incident Command System c) Hospital Incident Command System Hazardous Materials Awareness d) Incident Command System (up to ICS 200 level) e) National Incident Management System (NIMS) IS-700 and IS-800 f) Working knowledge of San Francisco EMS Agency Policies and
Procedures g) EMS related communication tools (radios, EMSystem, etc.) as required in
EMS policy.
2. All Field First Responders a) Simple Triage and Rapid Treatment (START) and JUMPSTART b) California Standardized Emergency Management System (SEMS) c) Incident Command System (up to ICS 200 level) d) National Incident Management System (NIMS) IS-700 and IS-800 e) Hazardous Materials First Responder Awareness f) Working knowledge of San Francisco EMS Agency Policies and
Procedures g) EMS related communication tools (radios, EMSystem, etc.) as required in
EMS policy.
3. Ambulance Strike Team Leader a) Incident Command System (up to ICS 300 level)
Page 2

Policy Reference No.: 8000 Effective Date: XXXX 2010
Page 3
b) Ambulance Strike Team Leader Training (State EMS Authority course) c) Ambulance Strike Team Provider Training (State EMS Authority course) d) EMS related communication tools (radios, EMSystem, etc.) as required in
EMS policy.
4. On-Scene Command Staff a) Incident Command System (up to ICS 400 level) b) EMS related communication tools (radios, EMSystem, etc.) as required in
EMS policy. c) EMS related communication tools (radios, EMSystem, etc.) as required in
EMS policy.
5. Assigned EOC or DOC Command Staff a) City and County Emergency Response Plan b) City Departmental Emergency Response Plans (any city DOC staff) c) Provider Emergency Operations Plan (any private provider DOC staff) d) MGT 313 (or equivalent) – Incident Management / Unified Command e) EMS related communication tools (radios, EMSystem, etc.) as required in
EMS policy.
V. MCI PLAN UPDATES
The EMS Agency is responsible for updates of the San Francisco Emergency Medical Services MCI Plan through its regular policy and protocol public comment process. This policy will be updated as appropriate to support the MCI Plan.
VI. QUALITY IMPROVEMENT
A. The Medical Group Supervisor for a MCI will submit the MCI Post Event Report Form (see Policy 8000 Attachment) along with a written MCI Summary to the EMS Agency within 24 hours of the incident.
B. DEC will submit a MCI Post Event Report Form to the EMS Agency within 24
hours of the incident.
C. EMS provider organizations shall submit other incident or patient-related information as requested for the EMS Agency. Any submitted patient information must NOT contain specific patient identifiers in compliance with all applicable federal or state confidentiality requirements.
D. The DEM-EMS Agency will review all MCI Post Event Report Forms and MCI
Summary Reports within 24 hours of receiving the documentation as part of our on-going Quality Improvement process. The EMS Agency will coordinate an inter-agency debriefing for significant MCIs within four weeks of an incident and summarize its findings in an After Action Report / Plan of Correction. At a minimum, a representative from each department or agency with an active role in the MCI incident will attend the debriefing.

STATUS
Veteran
Calif
Red Yellow Green Total
RedCross
TIME
Green Treatment:
Morgue:
Rehab:
DISPATCH
Transport:
MGS:
EMSA Policy 8000: v. xx/xx/10
Page ____ of _____ MCI Date / Time:CAD Incident Number:
Fax Copy to DEM ‐ EMS Agency (552‐0194) Report Completed By:within 24 hr of MCI
MCI POST EVENT REPORT FORM V. 05/12/10
SCENE INFORMATION UNIT STATUS HOSP
UNIT ALS / DISPATC SPORTED HOSCall Sign: H STATUS TRAN P # AVAIL # TYPESTATUS HOSP Location: # R # Y # G # R # Y # GBLS TIME HOSP / CAN STATUS BEDS / CAN
Incident Type: CalPac
Hazards: Dav
Staging: KaiSF
Access: St Fran
St LukesEgress:
St Mary
COMMAND STAFF SFGH
IC: UCSF
MGS: Veteran
Triage: Chinese
Treatment:
Staging:
ESTIMATED NUMBER OF PATIENTS
LOCATION OF OTHER UNITS
ICP: Transport: TYPE # PTS
Triage: Staging: Bus
Treatment: Supply: Helicop

PART 3 MCI PLAN:
TABLE OF CONTENTS I. MCI RESPONSE CHARTS
II. MCI MEDICAL OPERATIONS: CORE RESPONSE
III. BACKGROUND
IV. APPENDICES:
A. SAN FRANCISCO HEALTH AND MEDICAL CONTACTS (NOTE: THIS IS LISTS ALL EMS PROVIDERS ADDRESSES AND PHONE NUMBERS AND IS NOT INCLUDED IN
TODAY’S MEETING DISCUSSION) B. FIELD POSITION DESCRIPTIONS AND FIELD LAYOUT DIAGRAM C. PATIENT DISTRIBUTION GROUP POSITION DESCRIPTIONS D. MCI FIELD BOARDS E. ABBREVIATIONS, ACRONYMS AND GLOSSARY F. MAP OF CALIFORNIA MUTUAL AID REGIONS

PART 1: MCI RESPONSE CHARTS
LEVEL ZERO – MEDICAL 911 SERVICE DISRUPTION ALERT Description Actions
Activation Criteria 1. Extreme demand for EMS resources resulting in either an ambulance shortages and/or saturation of all hospitals (ambulance shortage must exceed 30 minutes).
2. Physical plant disruption at one or more hospitals that affects their ability to participate in the medical 911 system.
Example(s) • Extreme hot weather generates hundreds of medical 911 calls resulting in ambulance shortages. • Flu season has filled the hospitals. All Emergency Departments are full and cannot accept 911 ambulances. • Catastrophic power failure at SFGH disrupts the San Francisco trauma system. • Wide‐spread power failure in a city sector closes several neighboring hospital emergency departments.
Summary Concept of Operations
Level Zero is a notification and assessment‐based alert. EMS providers will be notified of the specific service disruption and requested to assess their resources. Subsequent actions will be on based the assessment and determined by the DEM Duty Officer in consultation with the EMS Agency Medical Director, the Director of Health, the SFFD Chief and the leadership of the affected EMS providers.
Activation Authority DEC Deck Officer or DEM Duty Officer
Notifications Actions DEC (911 Dispatch) 1. DEM Agency Duty Officer.
2. Level Zero alert on EMSystem. Note cause for alert (ambulance shortage, hospital saturation, hospital disruption) with polling: a. Hospitals for available ED Bed Status. b. ALS and BLS Ambulance Providers for available ambulance units.
Dispatch / Communications
Actions
DEC Early recognition and notification to DEM Duty Officer about medical 911 service disruption.
1

Private Amb Dispatch
1. Respond to EMSystem query.2. Place available ambulances on DEC AVL System if there is an ambulance shortage.
Ambulance / Field Actions All Providers 1. Monitor EMSystem for hospital diversion / closures.
2. DEM Duty Officer will provide instructions about any modifications to the EMS Response. 3. Respond to other DEM Duty Officer requests for information.
Receiving Facilities Actions Hospitals 1. Notify DEC of any service disruption and whether the Emergency Department can continue to receive 911 ambulances.
2. Improve ambulance turnaround time at hospitals through more rapid transfer of care between field crews and ED staff. 3. Respond to EMSystem poll for available ED beds. 4. Respond to other DEM Duty Officer requests for information.
Patient Distribution
Actions
Patient Distribution Group DEM Duty Officer will determine need and provide further instruction about activating Patient Distribution Group.
DEM Actions DEM DUTY OFFICER 1. Assess cause and impact on medical 911 system capability through:
a. EMSystem polling b. First Watch ‐ Quantify call volume / type and number of standard deviations above norm. c. Consultation with:
• DEC Deck Officer. • Ambulance company and / or hospital supervisory staff.
d. Consultation as appropriate with: • DEM Administrator on Call • DPH Communicable Disease Control Duty Officer or Environmental Health Duty Officer • DEM command staff • Other city, regional, state or federal agency as warranted. • MHOAC to notify RDHMC and state EMS Authority, if warranted.
. 2. Develop Action Plan in consultation with EMS Medical Director, DPH Director of Health, SFFD Chief and the leadership of affected EMS Providers that will include a determination of the need to escalate the system alert level to a same response actions used during a Level 1,2, or 3 MCI Alert.
2

Coordination / Mutual Aid
Actions
MHOAC DEM Duty Officer will consult with DEM AOC who will determine need for additional notifications or activations. DPH DOC
Fire DOC City EOC RDMHC State EMSA
Alert Upgrade or Termination
Actions
DEC 1. May be upgraded or terminated by DEM Duty Officer.2. DEC Deck Officer announces alert upgrade or termination on EMSystem and paging system.
3
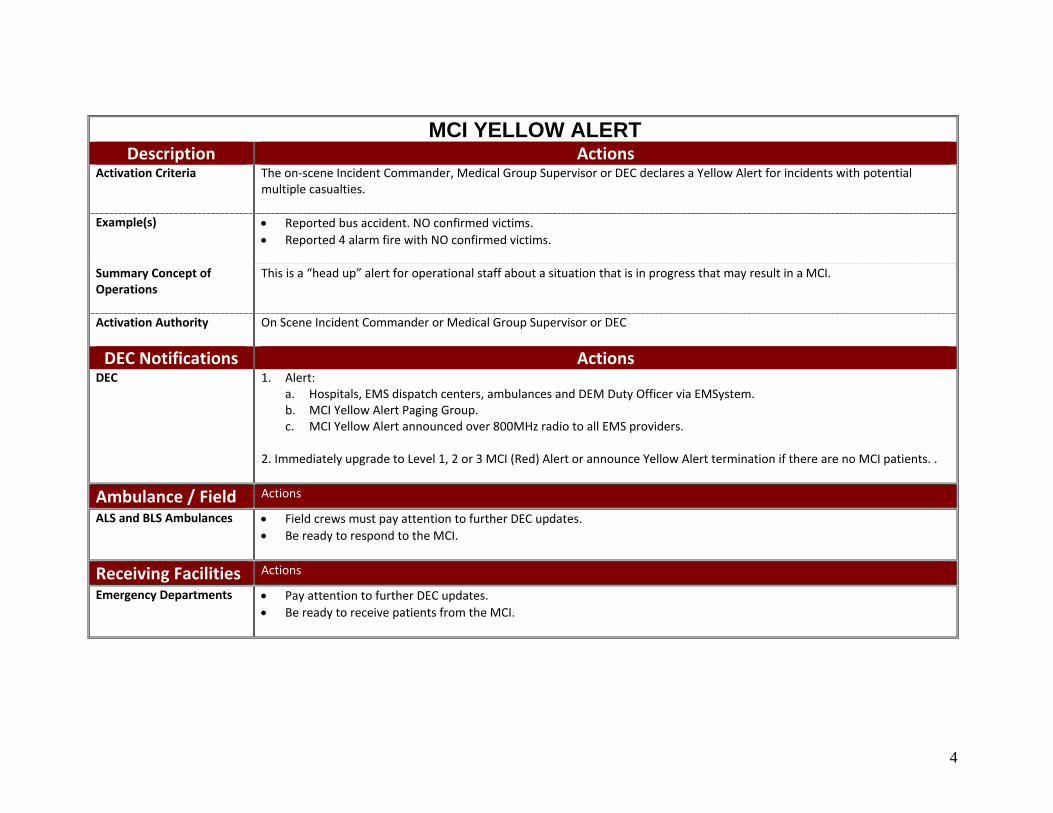
MCI YELLOW ALERT Description Actions
Activation Criteria The on‐scene Incident Commander, Medical Group Supervisor or DEC declares a Yellow Alert for incidents with potential multiple casualties.
Example(s) • Reported bus accident. NO confirmed victims.
• Reported 4 alarm fire with NO confirmed victims.
Summary Concept of Operations
This is a “head up” alert for operational staff about a situation that is in progress that may result in a MCI.
Activation Authority On Scene Incident Commander or Medical Group Supervisor or DEC
DEC Notifications Actions DEC 1. Alert:
a. Hospitals, EMS dispatch centers, ambulances and DEM Duty Officer via EMSystem. b. MCI Yellow Alert Paging Group. c. MCI Yellow Alert announced over 800MHz radio to all EMS providers.
2. Immediately upgrade to Level 1, 2 or 3 MCI (Red) Alert or announce Yellow Alert termination if there are no MCI patients. .
Ambulance / Field Actions
ALS and BLS Ambulances • Field crews must pay attention to further DEC updates. • Be ready to respond to the MCI.
Receiving Facilities Actions
Emergency Departments • Pay attention to further DEC updates. • Be ready to receive patients from the MCI.
4

LEVEL 1 MCI (RED) ALERT Description Actions
Activation Criteria MCI with 6 or greater of Immediate category victims or 10 ‐ 50 victims of any triage level. EMS resources available during usual daily operations can contain and manage the situation.
Example(s) Bus accident with 15 patients all triaged as YELLOW.
Summary Concept of Operations
• EMS resources available during daily operations can contain and manage situation. • Alert results in notifications to hospitals, EMS dispatch centers, ambulances and DEM Duty Officer.
Activation Authority On Scene Incident Commander or Medical Group Supervisor
DEC Notifications Actions DEC 1.Alert:
• Hospitals, EMS dispatch centers, ambulances and DEM Duty Officer via EMSystem. • Level 1 MCI Alert Paging Group. • Level 1 MCI Alert announced over 800MHz radio to all EMS providers.
2. Provide updates on EMSystem screen every 15 minutes.
Dispatch / Communications
Actions
DEC 1. Assigns field units and tactical channels.2. EMSystem polling every 15 minutes w/ updates:
a. Hospitals for available ED Bed Status. b. ALS and BLS Ambulance Providers for available ambulance units.
3. Assign command and tactical channel to responding units. 4. Ambulance diversion is automatically suspended ONLY for MCI patients.
Private Amb Dispatch
1. Respond to EMSystem poll for available ambulances. 2. Place available ambulances on DEC AVL System. 3. Inform responding units about DEC assigned tactical radio channel. 4. Ambulance diversion is automatically suspended ONLY for MCI patients.
5

Ambulance / Field Actions SFFD 1. Medical Group activated.
2. EMS Response Time Standards are still in effect. 3. Ambulance diversion is automatically suspended ONLY for MCI patients. 4. Crews do NOT provide radio notifications to hospitals about in‐coming MCI patients.
ALS Ambulance 1. EMS Response Time Standards are still in effect. 2. Ambulance diversion is automatically suspended ONLY for MCI patients. 3. Crews do NOT provide radio notifications to hospitals about in‐coming MCI patients.
BLS Ambulance 1. Routine operations.
Field Documentation 1. Triage Tags and Patient Care Records used for MCI patients.
Receiving Facilities Actions Hospitals 1. Respond to EMSystem bed poll. Provides the number of MCI patients ED can accept in ADDITION to the minimum in the
pre‐assigned distribution plan. 2. Ambulance crews do NOT provide radio notifications to hospitals about in‐coming MCI patients. 3. Ambulance diversion is automatically suspended ONLY for MCI patients.
Patient Distribution
Actions
Patient Distribution Group 1. Follow Pre‐Assigned Distribution Scheme. 2. DEC Deck Officer activates the DEC‐based Patient Distribution Group.
DEM Actions DEM Duty Officer
1. Monitor for:a. Alert upgrade or termination and provider response to DEC polling. b. EMS System overload.
2. Ambulance diversion is automatically suspended ONLY for MCI patients. Duty Officer may suspend diversion for all 911
ambulances if necessary. 3. Contact DEM Administrator on Call to determine need for additional notifications or alerting to region or state.
6
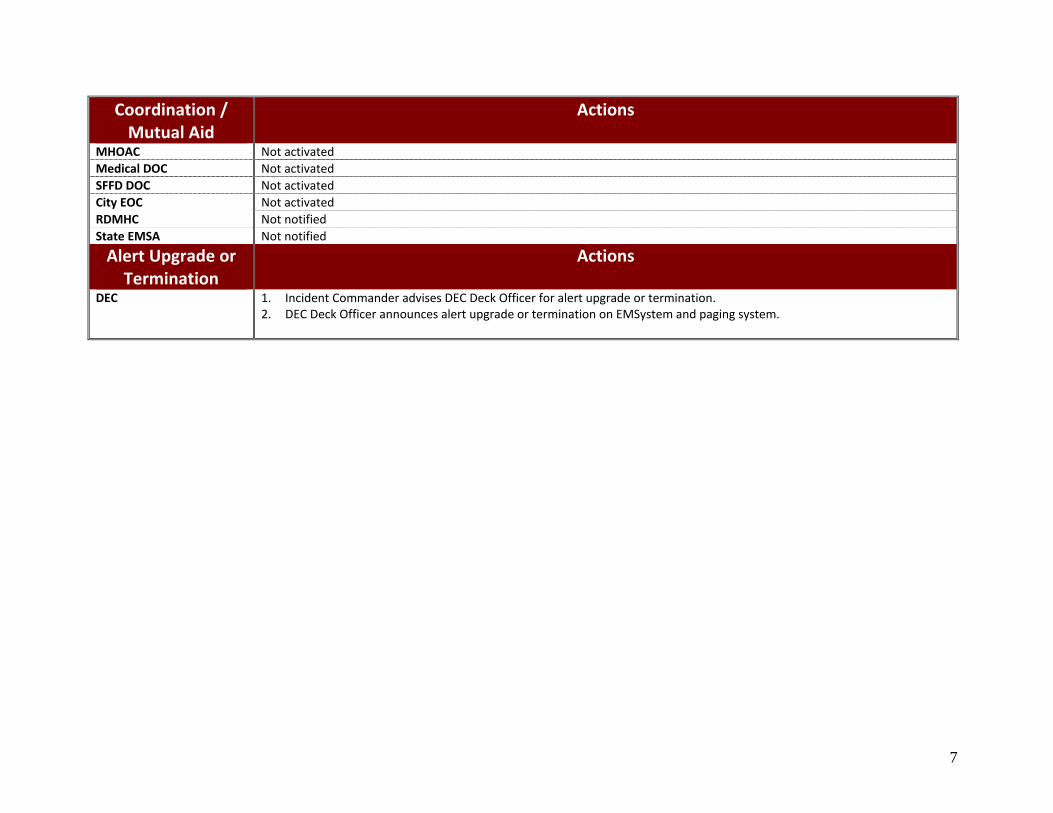
Coordination / Mutual Aid
Actions
MHOAC Not activatedMedical DOC Not activatedSFFD DOC Not activatedCity EOC Not activatedRDMHC Not notified State EMSA Not notified
Alert Upgrade or Termination
Actions
DEC 1. Incident Commander advises DEC Deck Officer for alert upgrade or termination. 2. DEC Deck Officer announces alert upgrade or termination on EMSystem and paging system.
7

LEVEL 2 MCI (RED) ALERT Description Actions
Activation Criteria MCI with 51 ‐ 100 victims of any triage level OR response requires resources from or distribution of casualties to other counties within our California mutual aid region.
Example(s) • Building collapse with 30 victims triaged RED and all meet trauma triage criteria for trauma center care. Patients must distribute patients to SFGH and other Bay Area trauma hospitals.
• BART train accident with 95 victims. • Multiple simultaneous incident(s) that overwhelm local EMS resources.
Summary Concept of Operations
Situation requires response resources from and the distribution of patients to outside the Operational Area. Alert results in notifications to EMS system, city disaster command staff and Regional Medical Mutual Aid System.
Activation Authority • Medical Group Supervisor or Field Incident Commander • DEM Duty Officer • MHOAC (if DOC / EOC is not activated) • Director or Operations Section Chief in DOC (if activated and EOC is not activated). • Director or Operations Section Chief in EOC (if activated).
DEC Notifications Actions DEC Alert to:
1. Hospitals, EMS dispatch centers, ambulances and DEM Duty Officer via EMSystem. 2. DEM Duty Officer. 3. Level 2 MCI Alert Paging Group. 4. Level 2 MCI Alert over 800MHz radio to all EMS providers.
Dispatch / Communications
Actions
DEC 1. Assigns field units and tactical channels.2. EMSystem polling every 15 minutes w/ updates:
• Hospitals for available ED Bed Status. • ALS and BLS Ambulance Providers for available ambulance units.
3. Assign command and tactical channel to responding units. 4. Diversion is automatically suspended for ALL ambulance patients during a Level 2 MCI Alert. DEM Duty Officer will
8

determine when reinstate. 5. DEM Duty Officer may provide instructions about modifying EMS Response patterns. 6. Consider activating internal Emergency Response Plan.
Private Amb Dispatch
1. Respond to EMSystem poll for available ambulances. 2. Place available ambulances on DEC AVL System. 3. Inform responding units about DEC assigned tactical radio channel. 4. Diversion is automatically suspended for ALL ambulance patients during a Level 2 MCI Alert. DEM Duty Officer will
determine when reinstate. 5. DEM Duty Officer may provide instructions about modifying EMS Response patterns. 7. Consider activating internal Emergency Response Plan.
Ambulance / Field Actions SFFD and ALS Ambulances 1. Medical Group activated.
2. EMS Response Time Standards are suspended during Modified EMS Responses. 3. Diversion is automatically suspended for ALL ambulance patients during a Level 2 MCI Alert. DEM Duty Officer will
determine when reinstate. 4. Crews do NOT provide radio notifications to hospitals about in‐coming MCI patients. 5. Request field supplements as needed:
• Mobile Multi‐Casualty Unit (request through SFFD) • MMTF (through SFFD) • Mutual Aid Ambulance Strike Team(s) (request through DEM Duty Officer) • MCI Trailers (through DEM Duty Officer)
6. Consider activating internal Emergency Response Plan to surge available resources. 7. DEM Duty Officer may provide instructions about modifying EMS Response patterns.
BLS Ambulance 1. DEM Duty Officer may request BLS ambulances to supplementing response.2. Consider activating internal Emergency Response Plan to surge available resources.
Field Mutual Aid Resources
Mutual aid ambulances from other Bay counties may be used.
Field Documentation Triage Tags used for MCI patients.
Alternate Transport Alternate transport vehicles (e.g. Muni buses, etc.) may be used to transport walking wounded (Green) patients.
9

Receiving Facilities Actions Hospitals 1. Respond to EMSystem bed poll. Provides the number of MCI patients ED can accept in ADDITION to the minimum in the
pre‐assigned distribution plan. 2. Ambulance crews do NOT provide radio notifications to hospitals about in‐coming MCI patients. 3. Diversion is automatically suspended for ALL ambulance patients during a Level 2 MCI Alert. DEM Duty Officer will
determine when reinstate. 4. Consider activating internal Emergency Response Plan.
Alternate Treatment Sites
May be used at incident site by First Responders holding patients awaiting transport.
Patient Distribution
Actions
Patient Distribution Group 1. Follow Pre‐Assigned Distribution Scheme. 2. DEC Deck Officer activates the DEC‐based Patient Distribution Group. 3. DEC may contact Regional Disaster Medical‐Health Coordinator for out‐of‐county beds if DEM Duty Officer or MHOAC are not available. 3. May transition Patient Distribution Group to Medical DOC.
DEM Actions DEM Duty Officer
1. Diversion is automatically suspended for ALL ambulance patients during a Level 2 MCI Alert. DEM Duty Officer will determine when reinstate.
2. DEM Duty Officer may support DEC with Patient Distribution as needed. 3. Assess medical 911 system capability through:
a. EMSystem polling b. First Watch ‐ Quantify call volume / type and number of standard deviations above norm. c. CAD d. Consultation with:
• DEC Deck Officer. • Ambulance company and / or hospital supervisory staff.
e. Consultation as appropriate with: • DEM Administrator on Call • DPH Communicable Disease Control Duty Officer • DPH Environmental Health Duty Officer • DEM command staff
10

• Other city, regional, state or federal agency as warranted. 4. DEM Administrator on Call to determine:
a. Need for additional alerts through Alert SF/CCSF or nee need to escalate the system alert level to a same response actions used during a Level 3 MCI Alert.
b. Incident entry into LEO system (DEM staff use only). c. EOC activation d. Notification of Regional Medical‐Health Disaster Coordinator, CAlEMA Warning Center.
5. Contact EMS Medical Director who may determine whether to do the following:
a. Suspension of Medical Priority Dispatch pre‐arrival instructions for 911 calls. b. Suspension of inter‐facility transports. c. Modify EMS response standards. Modifications of the standard responses will be authorized by the EMS Agency
Medical Director or EMS Duty Officer in his/her absence, in consultation with the Director of Health, the SFFD Chief and the leadership of the affected EMS providers.
Coordination / Mutual Aid
Actions
MHOAC Monitor health and medical situation and resources and coordinate all medical mutual aid requests including ambulance strike teams.
Medical DOC May be activated.
SFFD DOC May be activated.
City EOC May be activated.
RDMHC Notified by DEM Duty Officer or MHOAC.
In or Out medical mutual aid requested by MHOAC will be coordinated through the Region 2 RDMHC.
State EMSA Notified by DEM Duty Officer, MHOAC or RDMHC.
Alert Upgrade or Termination
Actions
DEC 1. Level 2 MCI Alert may be upgraded or terminated by Incident Command or DEM AOC.2. Deck Officer at DEC announces alert upgrade or termination on EMSystem and paging system.
11

LEVEL 3 MCI (RED) ALERT Description Actions
Activation Criteria MCI with 101 or more victims of any triage level OR requires resources from or distribution of casualties to outside our California mutual aid region using state or federal systems and resources.
Example(s) • High magnitude earthquake with numerous buildings collapsed and hundreds of casualties. • Isolated, large scale incident such as the World Trade Towers collapse.
Summary Concept of Operations
• Assumes infrastructure is essentially intact and partial disruptions may or may not be present. EMS and citywide resources need significant support and coordination above the field level and operational area command.
• Patients must be distributed to hospitals in other California OES regions and / or other parts of the U.S. using State and/or Federal systems and resources.
Activation Authority • County Health Officer
• EOC Director • DEM AOC • Disaster declarations from Mayor’s Office
DEC Notifications Actions DEC 1. Alert to:
a. Hospitals, EMS dispatch centers, ambulances and DEM Duty Officer via EMSystem. b. DEM Duty Officer. c. Level 3 MCI Alert Paging Group. d. Level 3 MCI Alert over 800MHz radio to all EMS providers.
2. Poll hospitals via EMSystem to determine if communications intact and facility is open. The 800 MHz radio or Hearnet
radio are backup communications.
Dispatch / Communications
Actions
DEC 1. Assign field units and tactical channels. 2. Activate Emergency Response Plan. 3. Diversion is automatically suspended for ALL ambulance patients for the duration of the Level 3 MCI Alert. DEM Duty
Officer will determine when to reinstate.
12

4. Report operational status to Medical Transport Group at Medical DOC. 5. Provide designated staging area(s) information to mutual aid ambulances. 6. DEM Duty Officer will provide instructions about modifications to the standard medical 911Response.
Private Amb Dispatch
1. Activate Emergency Response Plan.2. Respond to EMSystem ambulance poll. 3. Place available ambulances on DEC AVL System. 4. Diversion is automatically suspended for ALL ambulance patients for the duration of the Level 3 MCI Alert. DEM Duty
Officer will determine when to reinstate. 5. Report operational status to Medical Transport Group at Medical DOC. 6. DEM Duty Officer will provide instructions about modifications to the standard medical 911Response.
Ambulance / Field Actions SFFD 1. Activate Emergency Response Plan to surge available resources.
2. Medical Group activated. 3. Diversion is automatically suspended for ALL ambulance patients for the duration of the Level 3 MCI Alert. DEM Duty
Officer will determine when to reinstate. 4. Crews do not radio notifications to hospitals about in‐coming MCI patients. 5. Request Field Supplements as needed:
a. Mobile Multi‐Casualty Unit b. MMTF c. Mutual Aid Ambulance Strike Team(s) (request through SFFD DOC to DEM Duty Officer/Medical DOC) d. MCI Trailers (request through SFFD DOC to DEM Duty Officer/Medical DOC)
6. Set up designated staging areas for Mutual Aid Ambulances. 7. Use alternate treatment sites (casualty collection points) at incident scene as needed. 7. Report operational status to SFFD DOC. 8. DEM Duty Officer will provide instructions about modifications to the standard medical 911Response. EMS Response Time
Standards are suspended during Modified EMS Responses.
ALS Ambulance 1. Activate Emergency Response Plan to surge available resources. 2. Medical Group activated. 3. Diversion is automatically suspended for ALL ambulance patients for the duration of the Level 3 MCI Alert. DEM Duty
Officer will determine when to reinstate. 4. Crews do not radio notifications to hospitals about in‐coming MCI patients. 5. Request Field Supplements as needed through Medical Group Supervisor:
a. Mobile Multi‐Casualty Unit b. MMTF
13
c. Ambulance Strike Team(s)d. MCI Trailers
6. Use alternate treatment sites (casualty collection points) at incident scene as needed. 7. Report operational status to Medical Transport Group at Medical DOC. 9. DEM Duty Officer will provide instructions about modifications to the standard medical 911Response. EMS Response Time
Standards are suspended during Modified EMS Responses.
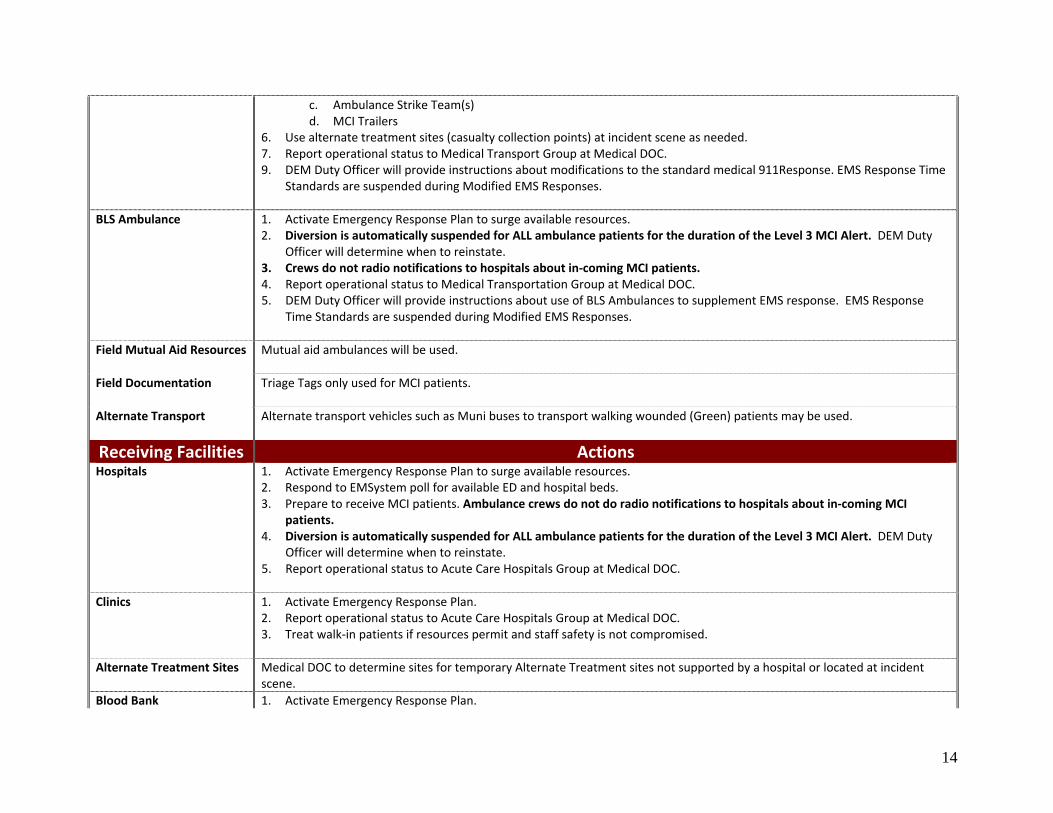
BLS Ambulance 1. Activate Emergency Response Plan to surge available resources. 2. Diversion is automatically suspended for ALL ambulance patients for the duration of the Level 3 MCI Alert. DEM Duty
Officer will determine when to reinstate. 3. Crews do not radio notifications to hospitals about in‐coming MCI patients. 4. Report operational status to Medical Transportation Group at Medical DOC. 5. DEM Duty Officer will provide instructions about use of BLS Ambulances to supplement EMS response. EMS Response
Time Standards are suspended during Modified EMS Responses.
Field Mutual Aid Resources
Mutual aid ambulances will be used.
Field Documentation Triage Tags only used for MCI patients.
Alternate Transport Alternate transport vehicles such as Muni buses to transport walking wounded (Green) patients may be used.
Receiving Facilities Actions Hospitals 1. Activate Emergency Response Plan to surge available resources.
2. Respond to EMSystem poll for available ED and hospital beds. 3. Prepare to receive MCI patients. Ambulance crews do not do radio notifications to hospitals about in‐coming MCI
patients. 4. Diversion is automatically suspended for ALL ambulance patients for the duration of the Level 3 MCI Alert. DEM Duty
Officer will determine when to reinstate. 5. Report operational status to Acute Care Hospitals Group at Medical DOC.
Clinics 1. Activate Emergency Response Plan. 2. Report operational status to Acute Care Hospitals Group at Medical DOC. 3. Treat walk‐in patients if resources permit and staff safety is not compromised.
Alternate Treatment Sites Medical DOC to determine sites for temporary Alternate Treatment sites not supported by a hospital or located at incident
scene. Blood Bank 1. Activate Emergency Response Plan.
14
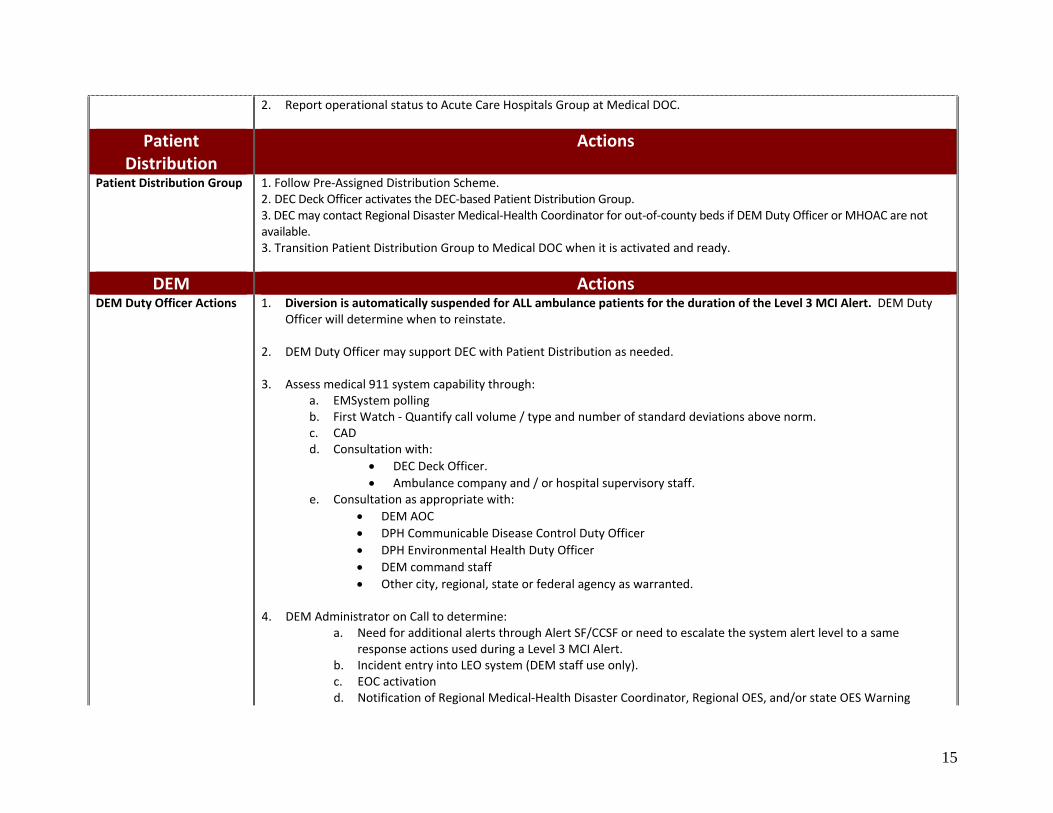
2. Report operational status to Acute Care Hospitals Group at Medical DOC.
Patient Distribution
Actions
Patient Distribution Group 1. Follow Pre‐Assigned Distribution Scheme. 2. DEC Deck Officer activates the DEC‐based Patient Distribution Group. 3. DEC may contact Regional Disaster Medical‐Health Coordinator for out‐of‐county beds if DEM Duty Officer or MHOAC are not available. 3. Transition Patient Distribution Group to Medical DOC when it is activated and ready.
DEM Actions DEM Duty Officer Actions
1. Diversion is automatically suspended for ALL ambulance patients for the duration of the Level 3 MCI Alert. DEM Duty Officer will determine when to reinstate.
2. DEM Duty Officer may support DEC with Patient Distribution as needed.
3. Assess medical 911 system capability through: a. EMSystem polling b. First Watch ‐ Quantify call volume / type and number of standard deviations above norm. c. CAD d. Consultation with:
• DEC Deck Officer. • Ambulance company and / or hospital supervisory staff.
e. Consultation as appropriate with: • DEM AOC • DPH Communicable Disease Control Duty Officer • DPH Environmental Health Duty Officer • DEM command staff • Other city, regional, state or federal agency as warranted.
4. DEM Administrator on Call to determine:
a. Need for additional alerts through Alert SF/CCSF or need to escalate the system alert level to a same response actions used during a Level 3 MCI Alert.
b. Incident entry into LEO system (DEM staff use only). c. EOC activation d. Notification of Regional Medical‐Health Disaster Coordinator, Regional OES, and/or state OES Warning
15

Center. 5. Contact EMS Medical Director who may determine whether to do the following:
a. Suspension of Medical Priority Dispatch pre‐arrival instructions for 911 calls. b. Suspension of inter‐facility transports. c. Modify medical 911 response standards. Modifications of the standard responses will be authorized by the EMS
Agency Medical Director or EMS Duty Officer in his/her absence, in consultation with the Director of Health, the SFFD Chief and the leadership of the affected EMS providers.
Coordination / Mutual Aid
Actions
MHOAC 1. Activated and reports to EOC: Operations Section – Human Services Branch.2. Verifies RDMHC and State EMSA notified about incident and activation and provide regular updates. 3. Monitor health and medical situation and resources and coordinate all medical mutual aid requests. 4. Austere medical care for pre‐hospital providers only is authorized by the County Health Officer or, in his/her absence,
the Deputy Health Officer.
Medical DOC 1. Activated. 2. Assesses medical facility resources for maintaining medical operations for San Francisco. 3. Establish contact with SFFD DOC EMS staff to coordinate casualty counts from the field and request ambulance strike
teams. 4. Coordinate medical mutual aide requests through MHOAC. 5. Assume Patient Distribution Group role from DEC. 6. Medical DOC to determine sites for temporary Alternate Treatment sites not supported by a hospital or located at incident
scene. 5. Austere medical care for pre‐hospital providers only is authorized by the County Health Officer or, in his/her absence,
the Deputy Health Officer.
SFFD DOC 1. Activated. 2. Establish contact with Medical Transport Group at Medical DOC to report field casualty counts and request ambulance
strike teams. 3. Request field supplements as needed:
a. Mobile Multi‐Casualty Unit b. MMTF c. Mutual Aid Ambulance Strike Team(s) (request through SFFD DOC to DEM Duty Officer/Medical DOC) d. MCI Trailers (request through SFFD DOC to DEM Duty Officer/Medical DOC)
4. Set up designated staging areas for Mutual Aid Ambulances.
16

5. Use alternate treatment sites (casualty collection points) at incident scene as needed.
City EOC 1. EOC Activated. 2. Coordinate support of MCI and citywide operations.
RDMHC Notified by DEM Duty Officer or MHOAC. The MHOAC coordinates In or out medical mutual aid requested through the Region 2 RDMHC.
State EMSA Notified by MHOAC or Region 2 RDMHC.
Alert Upgrade or Termination
Actions
DEC Alert may be terminated by Director of DEM or the Mayor’s Office.
17

LEVEL 4 MCI (RED) ALERT Description Actions
Activation Criteria Catastrophic disaster with unknown number of casualties and deaths. City response and communications infrastructure aredisrupted.
Example(s) San Francisco 1906 earthquake and fire.
Summary Concept of Operations
Assumes complete disruption of the City response and communications infrastructure. The Emergency District Coordination Centers (EDCCs) decentralized command structure is invoked. State and federal assistance required to restore services and / or city infrastructure. Recovery outlook is long‐term.
Activation Authority San Francisco Fire Department Battalion Chief
DEC Notifications Actions DEC None due to 911 service interruption. (NOTE: For the planning purposes, it is assumed that DEC has a complete service
disruption and is not operational during a catastrophic Level 4 MCI)
SFFD
Actions
SFFD • Emergency District Coordination Centers (EDCCs) are a decentralized command structure that may be invoked by SFFD when central dispatch is interrupted. There are 10 emergency districts in San Francisco that correspond to the 10 fire battalion stations.
• Each battalion station is the designated EDCC and each Battalion Chief controls all of the assets in his/her emergency
district. When Fire Battalion Stations are used to house the EDCC, primary coordination and communication will be with the Fire DOC utilizing all available communication systems.
• Other city department representatives at the EDCC will communicate and coordinate their departmental resources with the relevant DOC when it becomes operational. Unified Command is used at the EDCC when there are other city department representatives present.
• EDCC will determine resource allocation priorities within its district. Resource requests will be communicated to the EOC through the Community Branch when it is activated.
18

19
Dispatch / Communications
Actions
DEC and Private Amb Dispatch
Activate Emergency Response Plan. Restore communication services.
Ambulance / Field Actions All Ambulance Units Ambulance response units will be organized through the Emergency District Coordination Centers until the dispatch
communications infrastructure and central command are restored. This includes mutual aid ambulances.
Receiving Facilities Actions All Receiving Facilities • Activate Emergency Response Plan. Restore services.
• Support to all hospitals will be organized through the Emergency District Coordination Centers until the communications infrastructure and central command are restored.
Patient Distribution
Actions
Patient Distribution Group The ability for a formal patient distribution system to be organized will be determined at the time of the incident based upon the presenting circumstances. The Medical DOC will manage the Patient Distribution Group whenever it is staffed and ready.
DEM Actions DEM Duty Officer Actions
Full EOC activation if building site is safe and staff available. Full Emergency Response Plan activation including Community Disaster Response Hubs used to bring resources to neighborhoods to meet basic human service needs for: medical/mental health support, shelter, food and water distribution, vulnerable persons support and information dissemination to residents.
Coordination / Mutual Aid
Actions
City EOC • City EOC and all departmental DOCs are activated if building sites are safe and staff available to operate. • All emergency declarations are invoked and fire, law and health mutual aid requested from the region, state and federal
government.
Alert Termination Actions SFFD has the authority to activate/deactivate an Emergency District Coordination Centers (EDCCs) decentralized command structure.

20
REVISED ERD MAP IS PENDING Ten Emergency response districts in San Francisco include ten within San Francisco City and County jurisdiction and one under federal jurisdiction: 1) Chinatown ‐ No. Beach ‐ Financial District, 2) Civic Center – Tenderloin – Inner Mission, 3) SOMA – Southern Waterfront – Treasure Island, 4) Pacific Heights – Marina, 6) Mission – Noe Valley – Diamond Heights – Glen Park, 7) Richmond ‐ Western Addition, 8) Sunset, 9) Outer Mission – Ingleside – Ocean View – Visitation Valley, 10) Potrero Hill – Bayview ‐ Hunters Point, and 11) Presidio (federal jurisdiction). NOTE: ERD #5 has been disbanded and its districts have been reorganized into the other ERDs. However, the system still retains the old numbering system ERD 1‐4, and 6‐ 10.

PART 2MCI OPERATIONS:
CORE RESPONSE
SECTION 2.0 ‐ INTRODUCTION
The Department of Emergency Management ‐ Emergency Medical Services (EMS) Agency Multi Casualty Incident (MCI) Plan (herein referred to as the “Plan” or “MCI Plan”) identifies and delineates the structure and processes for the provision of emergency medical care by local Emergency Medical Services (EMS) system participants during a MCI event of any size or magnitude This MCI Plan is organized into three primary sections:
1. Plan 2. Annexes 3. Appendices
The Plan describes core emergency medical response operations during a multi‐casualty incident (MCI). The Plan is subdivided into three parts:
• Part 1 ‐ Response Charts • Part 2 ‐ Core Response • Part 3 ‐ Background
The Part 1 ‐ Response Charts provide easy and rapid access to the required actions for front‐line responders. Part 2 ‐ Core Response is the operational “playbook” that prescribes in detail the activities that all EMS participants must follow during a general response to a MCI. Part 3 ‐ Background provides the relevant background information to the reader with the “how” and “why” for the selected structure and processes of the response operations.
SECTION 2.1 – ALERTING, NOTIFICATIONS & ACTIVATION The classification of an incident level determines the corresponding alert and activation level that the Department of Emergency Management – Division of Emergency Communication (DEC) sends to EMS provider organizations. The alert levels correspond to Standardized EMS System Orders which are defined as pre‐determined EMS system participant actions in response to a MCI. Standardized EMS System Orders are similar to Job Action Sheets or Position Descriptions that individual field personnel or EOC / DOC command staff follow during a
1

disaster response. The difference though is that Standardized EMS System Orders apply to the response actions of an entire EMS provider organization (e.g. a hospital or an ambulance provider company). The purpose of the alert levels and corresponding Standardized EMS System Orders is to improve the speed, efficiency and overall coordination of the initial operational response to a MCI. An alert initiates the start of a Standardized EMS System Order that is followed in the first hour(s) to days of a MCI response until an Incident Command is organized and able to create and distributes an Incident Action Plan with response objectives that are specific to the incident. The Standardized EMS System Orders for each alert level are listed in Part 1 – Response Charts of this plan.
SECTION 2.2 – INTERAGENCY FIELD RESPONSE
2.2.1 Dispatch Sends Alerts
DEC sends out an alert when a MCI is first reported. Field Incident Commander determines the appropriate alert level based on the number of victims and if outside resources is needed to manage the incident. The lowest alert level to adequately meet the situational demands should be used. A single alert level is issued for every incident. The alert level may be upgraded or downgraded at any time during the incident based on the direction of Field Incident Commander. It is important to note that the cut off points for the number of victims needed to call a either a Level 1, 2 or 3 MCI alert is flexible. For example, 30 pediatric trauma victims may require sending some of the victims to out‐of‐county destinations – a Level 2 MCI alert. In a situation with more than one incident in progress, the incident that has the higher level of need will determine the alert issued. For example, Incident #1 is a Level 1 MCI Alert and Incident #2 is a Level 2 MCI Alert. DEC will send out a Level 2 MCI Alert – the higher level of the two possible alerts. 2.2.2 Scene Communications DEC is the lead dispatch agency for all San Francisco MCI Operations except for those occurring within the National Parks. DEC assigns the command and 1st assigned tactical radio channel to the responding units. The Incident Commander will determine the assignment of additional radio channels. On large incidents, the Incident Commander may delegate this to the Communications Unit Leader. Responding EMS units will switch to and coordinate their response through the DEC assigned channel. If the assigned channel does not provide coverage in given area, then Responding
2

Units will coordinate their activities through their respective communications centers on their primary radio channels and talkgroups. During a MCI, only the Incident Commander and the Medical Group Supervisor should converse with DEC about patient related information. The Incident Commander may delegate this task to Transport Area Unit Leader.
All Responding Units and dispatch centers should always state their agency name as well as their radio identifier when communicating, i.e. “Presidio Medic‐52,”or “SFFD Medic 31.” Radio users must only use clear text language when communicating on the radio. 2.2.3 Scene Management Assessment First‐in units will do the initial scene size‐up (“windshield assessment”) to establish:
• Confirmation of 911 reports of an actual MCI. • Type of incident (trauma, medical, Hazmat or combination). • Exact location and boundaries. • Incident magnitude. • Estimated number of potential or actual number of victims (if known), and • Additional response resources (type and number) if needed.
All information will be reported to the DEC who will relay the scene assessment information to the EMS providers through EMSystem. If EMSystem is not operable, DEC will communicate to EMS providers via the 800 MHz radios, or telephone.
Command
The highest‐ranking official of the first on‐scene agency initially establishes Command until relieved by a higher ranking, more qualified personnel. The Incident Commander (IC) is responsible for overall management of the incident. It is his/her responsibility to prepare the Incident Objectives that are broad, measurable and follow an ordered sequence of events. The IC will also determine:
• The assigned name for the incident based on its location and type (e.g. Shotwell Street Fire Incident; California Street Building Collapse Incident),
• Whether to do a more detailed Incident assessment, • Appropriate alert level, • ICS structure, • Whether additional response resources (number and type) are needed, and • Requests for Dept Parking Transport or SFPD (or other law enforcement) to secure
scene and perimeter.
3

All MCIs / disasters will be managed using SEMS and ICS. A Unified Command Post with Fire/EMS, Police, Public Health or other agency may be utilized for multi‐agency responses or at jurisdictional borders. If the scene is spread out over a large area, the IC will determine whether it is more appropriately managed as two separate incidents or as a single incident and its appropriate command structure.
EMS MCI Field Operations are the responsibility of the Operations Section. For a small single‐site incident, one Operations Section Medical Group will be established. For larger incidents or multi‐site incidents with more than one Operations Section Medical Group, a Medical Branch with several Medical Groups may be established.
The First‐In EMS unit will function as the Medical Group Supervisor until an EMS Officer arrives for assignment as the Medical Group Supervisor to manage the Medical Group. Overall command of EMS field operations in a full Branch response is delegated to the Multi‐Casualty Branch Director. The Medical Group Supervisor or Multi‐ Casualty Branch Director will report to the IC or the Operations Chief if an Operations Section is activated.
Initial Duties for First‐In, Second‐In and Subsequent EMS Units
First‐In EMS units (Rescue Captains, Field Supervisors, paramedics and EMTs) will report to the Incident Commander or Medical Group if already established. The First‐In EMS Unit will do a medical survey of the scene to assess the number of casualties and recommend Triage, Treatment, Transportation and Ambulance Staging Areas to Incident Commander. The First‐In EMS Unit will ask the IC to request specialized resources from DEC as appropriate (i.e. Multi‐Casualty Unit, Metropolitan Medical Task Force, MUNI buses, additional ground or air ambulances and EMS Field Supervisory personnel).
After the medical survey is completed, the First‐In EMS unit will function as the Medical Group Supervisor (MGS) until an EMS Officer arrives for assignment as the Medical Group Supervisor to run medical group. The First‐In Unit’s Paramedic (or EMT) #1 will be the Medical Group Supervisor and Paramedic (or EMT) # 2 will be the Triage Unit Leader until relieved.
Second‐In EMS units will report to Incident Commander or MGS as directed. The Second‐In Unit Paramedic (or EMT) #1 will be the Treatment Unit Leader and Paramedic (or EMT) # 2 will be the Transport Unit Leader until relieved.
Subsequent Ambulances will report to the Medical Group Supervisor who will direct the crews to the Treatment Area for staffing the Immediate, Delayed and Minor Treatment Areas. When an Ambulance Staging Area is established, DEC will announce to all in‐coming ambulance crews its location. In‐coming crews will park in the Ambulance Staging Area and report to the Ambulance Staging Manager who will give them their assignments. If NO Ambulance Staging Manager is designated, crews will report into the Transport Unit Leader (or Medical Group Supervisor, if necessary). Crews will stay with their vehicles in the Ambulance Staging Area while awaiting assignment.
4

At Greater Alarm Fires and MCIs, only the first ambulance unit to arrive should go “on‐scene” with the radio. Subsequent arriving ambulances shall go “on‐scene” via their mobile data terminals. Radio channel assignment for MCI communications are found in the Appendices.
Medical Group Set Up
EMS Field Supervisory staff (SFFD Paramedic Rescue Captains and private ALS Ambulance Field Supervisors) will assume roles in the Medical Group and / or Incident Command Post as assigned by the Incident Commander. Set up of the Medical Group or Branch will start with the first on scene EMS Field Supervisory Staff:
First EMS Field Supervisory Staff On‐Scene
• Report to Incident Commander. • Receive Situation Report (Sit Rep) from Incident Commander and interim
paramedic MGS. • Assume the role of MGS. On large incidents, designate the paramedic or EMT
who served as interim MGS as an “Assistant. Medical Group Supervisor” who will assist with radios and management of incident.
• Repeat the medical assessment of incident and work with Incident Commander to request additional resources and personnel if needed for triage and litter teams or patient transport.
• Usual work site is at the Command Post with the IC. • The MGS monitors/utilizes the Tactical Channel to talk to IC and Medical Group
Channel to talk to Medical officers. • If delegated by IC, MGS will assume task of giving updates and requesting
additional medical resources through the DEC.
Second EMS Field Supervisory Staff On‐Scene
• Report to MGS and receive Situation Report from MGS. • 2nd EMS Field Supervisory Staff will normally be assigned critical role of Transport
Leader. • Utilize secondary Medical Channel (or cell phone) to talk to DEC to distribute
patients to hospitals throughout City. • The IC / MGS can special call additional EMS Field Supervisory Staff to the scene,
if required.
Third EMS Field Supervisory Staff On‐Scene
• Report to MGS and receive Situation Report from MGS. Determine if a Medical Branch with several Medical Groups will be established. Consult with IC who will make the final determination on the organization of the field medical response.
• 3rd EMS Field Supervisory Staff may serve as Medical Branch director, if established, or as an additional MGS, or support MGS or Triage, Treatment or
5

Transport Officers as directed by the MGS. Medical Branch Director or MGS should be staffed with an experienced supervisor.
Scene Organization
Locations of designated medical areas shall be approved by the Incident Commander or his/her designee. The determination of all locations will factor in the following considerations:
• Safe distance from the scene and hazards. • Upwind from any noxious fumes. • Adequate space for patient care, personnel, and in‐coming / out‐going vehicles. • Environmental controls, if possible (out of wind, rain or extreme heat/cold).
Once the locations have been approved, the Medical Group Supervisor or his/her designee will oversee the set up of specific medical areas until delegated to the Unit Leaders below:
1) Triage Area Victims are usually be triaged where they lie. A separate Triage Area may be created if there is a hazard or if the physical location is not conducive for patient triage. Patients are triaged and tagged in the triage area before walking or being moved by litter bearers (if non‐ambulatory) to the Treatment Area. The decease or “expectant” are also triaged and tagged. Deceased are left where they lie or if adequate resources are available to set up a morgue, moved to a separate morgue area along with their personal effects. If the MCI is a crime scene, decedents are not moved without prior approval of the Medical Examiner or SFPD. 2) Treatment Area In a small incident, one Treatment Area may be set up with patients grouped together according to triage levels (Immediate, Delayed and Minor). For larger incidents, separate Immediate, Delayed and Minor Treatment Areas are established. 3) Patient Transport Area This area is for loading patients into transporting vehicles. Ideally, the loading area should be adjacent to the treatment area(s) and in‐line with the one way traffic from the Ambulance Staging Area. When a one‐way traffic pattern is not possible to due the topography or building density, scene personnel should improvise (e.g. create a patient gurney shuttle using firefighters, etc.). 4) Ambulance Staging Area In a small incident, the Ambulance Staging Area may be combined with the incident Staging Area for other response vehicles and personnel. In larger incidents, it may be a
6

separate location. This area will be the gathering point for EMS personnel and equipment. Supervision of this area may be assigned to the first unit which arrives in the Staging Area. Transport vehicles will be maintained in a one way traffic pattern towards the loading area, if possible. Law enforcement assistance may be used to establish traffic patterns to optimize the flow of patients out of the incident. 5) Morgue Area In most cases the deceased are left where they lie. A Morgue Area may be established when adequate resources are available and/or if it becomes necessary to remove deceased patients from the impacted site. This area should be located away from the treatment area(s) and is the responsibility of the Medical Examiner. EMS personnel assistance may be required in the establishment of the field morgue.
Medical Group Roles & Responsibilities
Firescope defines 15 positions for the Medical Group. Below briefly describes the roles and responsibilities for each position. Position descriptions for all Medical Group personnel are found in the Appendices.
1. Medical Branch Director – Has overall command of EMS field Operations in a full branch response. Responsible for the implementation of the Incident Action Plan within the Medical Branch. Reports to Operations Chief. Supervises Medical Group Supervisor(s) and Transportation function (Unit or Group). Reports out casualty information to the Operations Chief.
2. Medical Group Supervisor (MGS) ‐ In charge of EMS Field Operations in an initial and
reinforced level of response. Reports to the Medical Branch Director. Supervises Triage, Treatment and Transport Unit Leaders and Medical Supply Coordinator. Reports out casualty information to the Medical Branch Director.
3. Triage Unit Leader ‐ Coordinates the triage of all patients. Reports to MGS. Supervises
Triage Personnel / Litter Bearers and Morgue Manager.
4. Triage Personnel – Responsible for triaging patients and assigning them to appropriate Treatment Areas. Reports to Triage Unit Leader.
5. Morgue Manager ‐ Responsible for Morgue Area functions. Reports to Triage Unit
Leader.
6. Treatment Unit Leader ‐ Coordinates on scene emergency medical treatment of all victims. Reports to MGS. Supervises Treatment Dispatch Manager, Immediate Treatment Manager, Delayed Treatment Manager and Minor Treatment Manager.
7
7. Immediate Treatment Area Manager – Responsible for treatment and re‐triage of patients assigned to the Immediate Treatment Area.
8. Delayed Treatment Area Manager – Responsible for treatment and re‐triage of
patients assigned to the Delayed Treatment Area. 9. Minor Treatment Area Manager ‐ Responsible for treatment and re‐triage of patients
assigned to the Minor Treatment Area. 10. Treatment Dispatch Manager – Coordinates movement of patients from Treatment
Area to Transport Area. Reports to Treatment Unit Leader. 11. Patient Transportation Unit Leader (or Group Supervisor) ‐ Oversees the coordination
of patient transport vehicles and hospital destinations. Supervises Ground Ambulance Coordinator, Air Ambulance Coordinator and Medical Communications Coordinator. At his / her discretion, may add additional positions in Patient Transportation Unit to coordinate transportation to out‐of‐county destinations.
12. Ground Ambulance Coordinator ‐ Coordinates ground ambulances. Reports to
Transportation Unit Leader. 13. Air Ambulance Coordinator ‐ Establishes and coordinates helispots and air medical
operations with the Air Operations Group. Reports to Transportation Unit Leader.
14. Medical Communications Coordinator ‐ Maintains medical communications with the Patient Distribution Group and selects the mode of transport and patient destination based upon patient need using patient condition information provided by the Treatment Dispatch Manager. Reports to Transportation Unit Leader.
15. Medical Supply Coordinator – Coordinates medical supply requests and maintains stock. Reports to MGS.
2.2.4 Medical Group Operations Below describes the general operations for a MCI response. Refer to the Annexes in this plan for special emergency medical response operations for scenario specific situations (e.g. bombings, contaminated scenes, etc.).
Medical Group Supervisor
The Medical Group Supervisor(s) ensures command and control of all activities within the Medical Group and the integration of those activities with the overall operational response. This includes assuring that adequate personnel and resources are available to the Medical Group to accomplish its assigned objectives.
8
Triage Area / Triage Team
The Triage Team shall rapidly triage and tag all patients. Emergency medical care during the triage process is generally limited to establishing an airway and controlling hemorrhage. All patients are triaged and tagged prior to leaving the Triage Area. The Triage Team Leader shall set up a physical “triage funnel” with tape, sawhorses, etc. through which all patients are routed. The Triage Funnel should be in close proximity to Treatment Area.
The Triage Team Leader is responsible for tallying and reporting the total number of victims and classifying the MCI type as trauma, medical, Hazmat or combination. Results of the tally are reported as total number of patients and their triage categories (e.g. “Total of 10 trauma patients: 2 Immediate Heads, 4 Delayed, and 4 Minors. No decontamination needed.”). The Triage Team Leader reports this information to the Medical Group Supervisor.
Once all patients have been triaged, “Immediate” patients must be transported as soon as possible. Immediate patients are be moved to the Treatment Area only if there is a delay in transport due to a lack of transportation units or a high number of victims. Treatment Area The Treatment Areas will be set up with equipment from the first –in ambulances with the SFFD MCU vehicles supplementing equipment as needed. EMT and paramedic personnel will staff all Treatment Areas. Walk‐up volunteer medical personnel must be cleared through the incident Logistics Section before patient contact. The Treatment Unit Leader will check through the chain of command where to send walk‐up volunteer medical staff for clearance checks. Once a patient is in the Treatment Area, treatment will consist of:
• Re‐triaging patients. • Checking and recording vital signs and chief complaint on the triage tag. • Establishing and maintaining an airway and controlling hemorrhage. • First aid, BLS and ALS level care depending on provider training, availability of
personnel and resources, and only if the situation safely allows for it. • Preparing patients for transport.
Patient Transport Area / Patient Distribution The Patient Transport Area matches patients needing transportation with vehicles and assigned destinations. The Treatment Dispatch Manager (located in the Treatment Area) will provide to the Medical Communications Coordinator (located in the Transport Area) which Immediate, Delayed and Minor patients are prioritized for transport. The Medical Communications Coordinator will
9

communicate with the Patient Distribution Group to identify available hospital beds when there are more patients than can be handled through the pre‐assigned distribution scheme (see Section 2.3 for additional details). The Patient Distribution Group will match the field patient with an available bed at a facility, and communicate the selected destination to the Medical Communications Officer. The Medical Communications Coordinator will then chose an appropriate mode of transportation for the patient. Possible patient transportation options include:
• Ground Ambulance • Air Ambulance • At the discretion of the Transport Unit Leader, other vehicles (e.g. buses,
wheelchair vans) may be substituted for ambulances as appropriate for the patients’ condition.
The Medical Communications Coordinator will request medical transport vehicles through the Ground Ambulance Coordinator or Air Medical Coordinators. All requests for transportation will include specific details such as number and description of transport units, e.g., "2 ALS ground ambulances, 1 BLS ground ambulance, and 1 ALS air ambulance. Patients will be moved from the Treatment Area to the Patient Transport Area only when:
• The patient is “packaged” and ready to go, • A hospital bed destination is identified, and • The transport vehicle is ready to go.
The Ground Ambulance Coordinator and the Air Medical Coordinator are responsible for securing requested transport vehicle(s) and for maintaining a “Patient Log” for patients leaving the scene via ground or air that includes:
1. Triage tag number 2. Triage Level 3. Patient name (if known) 4. Patient Age and Gender 5. Chief complaint 6. Type of transport unit 7. Name of transport unit provider 8. Transport unit provider unit number 9. Destination 10. Date / Time of departure
Medical Supply The Medical Supply Coordinator requests, receives, distributes, tracks and maintains stock for medical supplies and equipment assigned to the Medical Group. The Medical Supply Coordinator reports to the MGS. If the Logistics Section is established, the Medical Supply Coordinator will
10
coordinate request through the Logistics Section Chief or the Supply Unit Leader. Otherwise, requests are funneled through the MGS to the Incident Commander. Resource requests are done by resource type and number when possible. MCI resource requests may consist of the following:
Transportation
• Ground Ambulances • Air Ambulances • Buses • Strike Teams or Task Forces
Personnel
• ALS Personnel • BLS Personnel • Litter Bearers • Strike Teams or Task Forces • Californian Medical Assistance Teams (Cal‐MAT – state) • Disaster Medical Assistance Teams (DMAT ‐ federal)
Supplies and Equipment
• Medical Supplies Caches and Equipment Trailers • Rescue Equipment • Specialized Equipment
2.2.5 MCI Status Updates and Termination Only the IC and Transport Officer may communicate with the DEC to provide updates and request medical resources. The IC may elect to delegate this task to the Medical Group Supervisor. The IC will make the determination when the MCI response is completed and communicate the termination notice to DEC to relevant participants.
2.2.6 Modified 911 EMS Responses during a MCI Minor and / or major modifications of the standard EMS responses may be necessary to maintain the sound operations of the entire EMS system during a sizeable MCI event. An example of a minor modification includes suspending advance notification to hospitals about in‐coming patients. Below lists examples of major modifications to EMS practices and response that may be invoked during a MCI.
Possible Modified Responses during a Level 2 MCI Alert
• ALS ambulances dispatched only to Code 3 (Delta and Echo) calls. • BLS ambulances dispatched to Code 2 (Alpha, Bravo, and Charlie) calls.
11

• First Responder dispatched to Code 2 ((Alpha, Bravo, and Charlie) calls.
Possible Modified Responses during a Level 3 MCI Alert • BLS Ambulance dispatched to only Code 3 (Delta and Charlie) calls. • First Responder dispatched to only Code 2 ((Alpha, Bravo, and Charlie) calls. • No response to Code 2 (Alpha, Bravo, and Charlie) calls.
Any decision to do a major modification of the standard 911 medical responses must be authorized by the EMS Agency Medical Director in consultation with the Director of Health, the SFFD Chief and the leadership of the affected EMS providers. The Part 1 Response Charts list all modifications to the EMS practices and responses.
SECTION 2.3 PATIENT DISTRIBUTION SYSTEM Patient distribution refers to the allocation of MCI patients to receiving hospitals. The overall goal of patient distribution operations are to deliver MCI patients to appropriate and available treatment beds to meet their medical needs without overwhelming any one hospital with too many patients. San Francisco utilizes a Patient Distribution System that simultaneously expands overall system capacity while rapidly distributing patients to hospital destinations. The Patient Distribution System consists of a combine approach using 1) Standardized EMS System Orders, 2) pre‐assigned distribution plan, and 3) Patient Distribution Group. Standardized EMS System Orders are defined as pre‐determined EMS system participant actions in response to a MCI. Standardized EMS System Orders are described in Section 3.3 and found in Part 1 – Response Charts. These orders include instructions to individual EMS participants to initiate activities for managing a surge of patients. The cumulative result of these coordinated activities is that the entire EMS system flexes its capacity to accommodate an influx of MCI patients. During MCI field operations, patients will be distributed to receiving facilities through the combined use of a pre‐assigned distribution plan and a Patient Distribution Group described below. 2.3.1 Pre‐Assigned Distribution Plan The pre‐assigned distribution plan pre‐assigns a fixed, minimum number of patients to each hospital. San Francisco hospitals MUST accept their assigned minimum allocation of patients. Hospitals can indicate their ability to accept ADDITIONAL patients above their required minimum number on EMSystem. The pre‐assigned distribution plan for MCI patients to San Francisco hospitals is found in Section 2.4.2 The Patient Transport Unit at the incident scene will distribute to each San Francisco EMS Receiving Hospital the minimum allocation of MCI patients as defined in the pre‐assigned
12

distribution plan. If the total number of patients from an incident exceeds the total number of pre‐assigned slots, then the Patient Distribution Group will determine the hospital assignment for those patients. To summarize:
Medical Group – Patient Transport Unit Handles “automatic” distribution of patients using pre‐assigned distribution plan
Patient Distribution Group Handles the assembly of a distribution plan for patients when their numbers exceed the total number of pre‐assigned slots
2.3.2 Patient Distribution Group Organization, Set Up and Activation
The Patient Distribution Group identifies available hospital beds when there are more patients than can be handled through the pre‐assigned distribution scheme. It also determines patient destinations in instances when there is no pre‐assigned distribution plan for field patients, such as when free‐standing field disaster clinics have been set up. At the start of the MCI, the DEC Deck Officer activates a Patient Distribution Group. Patient Distribution Group activation means that some or all of the group positions will be active during the management of the MCI response. The DEM Duty Officer may augment the Patient Distribution Group functions when requested by DEC. As the incident expands or moves into multiple operational periods, the Patient Distribution Group function will be transferred from DEC to the Dept of Emergency Management – Medical DOC once it is activated and ready for operations. Patient Distribution Group Roles & Responsibilities
The following briefly describes the roles and responsibilities for each position in the Patient Distribution Group. Detailed position descriptions for the Patient Distribution Group are found in the Appendices.
1) Patient Distribution Branch Director – Has overall command of Patient Distribution Group
operations in a full branch response. Responsible for the implementation of the Incident Action Plan within the Patient Distribution Branch. Reports to Operations Chief. Supervises Patient Distribution Group Supervisor(s). Reports patient distribution information to the Operations Chief.
2) Patient Distribution Group Supervisor – Supervisory role for the Patient Distribution Group
operations. Reports through the usual chain‐of‐command. Oversee the activities of the Patient Distribution Officer and Receiving Facility Status Officer. Liaison to all external parties and agencies except field responders and receiving facilities.
13

3) Receiving Unit Leader – Alert hospitals. Coordinates beds and patient assignments with all receiving facilities. Communicates the availability of beds to the Patient Unit Leader. Reports to the Patient Distribution Group Supervisor.
4) Patient Unit Leader – Coordinates the receiving destination for field patients with the Medical Communication Coordinator located at the Field Patient Transport Area. Reports to Patient Distribution Group Supervisor.
2.3.3 Scene Communications to the Patient Distribution Group The Medical Group Supervisor will designate the Medical Communications Coordinator to be the single point‐of‐contact for the Patient Distribution Group at the MCI scene. At no time, should more than one field person from an incident communicate with the Patient Distribution Center about the distribution of MCI patients to receiving facilities. If more than 1 incident is in progress, designated field contacts from each incident will clearly identify and distinguish their assigned incident by using the assigned name (e.g. “This is the Medical Communications Coordinator for the California Street Building Collapse Incident”). 2.3.4 Hospital or Other Receiving Facility Communications to the Patient Distribution Group Each receiving facility will designate a Receiving Point‐of‐Contact (POC) for all MCI Alerts. The Receiving POC is responsible for being the hospital’s designated single point‐of‐contact to the Patient Distribution Group. The Receiving POC may be the Emergency Department Charge Nurse or designee. This designation may be transferred to Hospital Command Center staff during large incidents or ones extending into multiple operational periods. For other facilities (alternate care sites, etc.) a Receiving Facility Point of Contact will be designated by the facility commander. At no time should more than one receiving facility staff person communicate with the Patient Distribution Group about the receipt of MCI patients. Hospitals will communicate to the Patient Distribution Group through EMSystem. If EMSystem is not functioning, the Patient Distribution Group will direct hospitals communications to the 800 MHz radio for a bed availability roll call. Landline telephones may provide backup communications in the event the 800 MHz radio is not functional. Satellite phones may also be considered for backup. The use of radio, phones or other communications for alternate care sites will be determined by their command. 2.3.5 Patient Distribution Group Operations See Section 2.2.4 for a description of patient distribution operations in the Medical Group – Transportation Unit. Below describes general operations for patient distribution in a MCI. The DEC Deck Officer activates a Patient Distribution Group at the start of a MCI by designating a Patient Distribution Group Supervisor. The Patient Distribution Group Supervisor will designate a Receiving Unit Leader and a Patient Unit Leader and start operations.
14

The Receiving Unit Leader does the following:
1. Polls hospitals at regular intervals to determine the number of available beds and provides that information to the Patient Unit Leader.
2. Has on‐going communications with the Receiving Hospital Point‐of‐Contact available beds, in‐coming patients and the status of the overall MCI response.
The Patient Unit Leader does the following:
1. Communicates with the Patient Transport Area ‐ Medical Communications Coordinator about the number of patients on scene.
2. Obtains from the Receiving Unit Leader, the number of available hospital beds. 3. Matches available hospital beds with the MCI patients remaining on scene. 4. Advises the Medical Communications Coordinator about the hospital bed
assignment. 2.3.6 Operational Control vs. Medical Control of Patient Distribution Operations The Patient Distribution Group Supervisor is responsible for all operations of the Patient Distribution Group including resolving questions or issues about patient bed assignments except for those involving clinical decisions. On‐scene personnel are responsible for the clinical determination of a patient destination. The Medical Communications Coordinator located at the Field Patient Transport Area must directly contact the Base Hospital for any clinically‐related questions about patient bed assignments. The Base Hospital at San Francisco General Hospital makes the final determination for a patient destination in the event of clinical questions or clinical disagreements over which receiving facility is the most appropriate to meet the medical needs of a MCI patient. The Medical Health Operations Coordinator (MHOAC) at the Emergency Operations Center may only advise the Patient Distribution Group Supervisor and the Base Hospital on operational or clinical issues. The MHOAC is not to provide field medical direction in a MCI. This applies in all Level 1, 2 or 3 MCIs as may be reasonably executed given the circumstances of the situation.
2.3.7 Patient Distribution Group Back Up
The field Medical Communications Officer at the Patient Transportation Area will take over the function of the Patient Distribution Group in the event of a technical communications failure that disrupts communications.
15

SECTION 2.4 PATIENT DISTRIBUTIONS ‐ LEVEL 1 MCI (RED) ALERT For a Level 1 MCI, EMS providers distribute triaged patients to receiving hospitals through the combined use of a pre‐assigned distribution plan and a Patient Distribution Group. 2.4.1 Triage
A. Medical Patients Triaged as Immediate (RED) or Delayed (YELLOW): Immediate medical patients will be distributed to hospitals beginning with those furthest away from the incident. Delayed medical patients will be distributed in the same manner after all Immediate medical patients have been transported.
B. Trauma Patients Triaged as Immediate (RED) or Delayed (YELLOW): Trauma patients
will be re‐triaged in the Treatment or Transport Area using the Trauma Triage Criteria when possible to identify critical patients requiring trauma center care criteria:
1) Meets physiologic or anatomic criteria: • The 1st four trauma patients shall be transported to San Francisco General
Hospital (SFGH). SFGH will indicate their ability to take additional critical trauma patients on EMSystems or via radio.
• When SFGH is at capacity, remaining patients shall be transported to regional trauma centers via either ground ambulance or air medical services – which ever has the shortest total travel time. Air medical transports are done in accordance with EMS Policy #4020 for EMS Aircraft Utilization.
• Patients may be transported to community hospitals only if SFGH and regional trauma centers capacity are at capacity OR if it is determined that a patient is likely to not survive travel time to an out‐of‐county trauma center.
2) Meets mechanism criteria: • May be transported to community hospitals.
C. Trauma Patients Triaged as Minor (Green): Minor (Green) patients shall be
transported to community (Non‐trauma center) hospitals.
D. Pediatric Trauma / Trauma with Burns / Microsurgical Needs: Transport Officer will make every effort distribute specialty need patients (pediatric trauma, burns with trauma, microsurgical needs) to appropriate Specialty Care Facilities.
E. Patients Triaged as Deceased (Black): Medical Examiner's Office is responsible for the management of this category.
16

2.4.2 Pre‐Assigned Distribution Plan The Transport Unit Leader will distribute to each San Francisco EMS Receiving Hospital the minimum allocation of MCI patients according to the Pre‐Assigned Distribution Plan on the following page. NOTE: The numbering for the hospitals is provided to indicate “at a glance” the number of available hospitals. It does NOT imply that patients must be sent to the hospitals according to a specific sequence.
17

Pre‐Assigned Distribution Plan for MCI Patients to San Francisco Hospitals
Hospital Trauma Incidents Medical Incidents 1 SFGH Trauma Center 1st 4 major trauma 2 patients2 CPMC Pacific Campus 2 patients 2 patients3 CPMC Davies 2 patients 2 patients4 CPMC St Lukes 2 patients 2 patients5 CPMC California St Campus 2 patients 2 patients6 St Francis Memorial 2 patients 2 patients7 Kaiser 2 patients 2 patients8 St Mary’s Medical Center 2 patients 2 patients9 UCSF 2 patients 2 patients
10 Seton – Daly City 2 patients 2 patients11 Chinese Hospital (ONLY DELAYED + MINOR ) 2 patients 2 patients12 VA Medical Center (ONLY DELAYED + MINOR) 2 patients 2 patients
TOTAL: 26 patients 24 patientsAll hospitals are required to accept the above minimum number of MCI patients. Hospitals must indicate if they are able to accept ADDITIONAL patients above the minimum on EMSystem.
The Transport Unit Leader may distribute critical trauma to the Regional Trauma Centers according to the Pre‐Assigned Distribution Plan below:
Pre‐Assigned Distribution Plan for Critical Trauma MCI Patients to
Regional Trauma Centers Hospital Patients Helipad
1 Oakland Children’s _ Oakland (Level II pediatric)
2 patients Yes
2 Eden Hospital – Castro Valley (Level II)
2 patients Yes
3 John Muir Hospital – Walnut Creek (Level II)
2 patients Yes
4 Stanford Medical Center – Palo Alto (Level I adult & Level I pediatric)
2 patients Yes
5 Regional Medical Center – San Jose (Level II adult)
2 patients Yes
6 Santa Clara Valley Medical Center ‐ San Jose (Level I)
2 patients Yes
7 Santa Rosa Memorial‐ Santa Rosa (Level II)
2 patients Yes
8 UC Davis – Sacramento (Level I adult & pediatric)
2 patients Yes
9 Highland Hospital ‐ Oakland 2 patients NO
10 Marin General ‐ Greenbrae 2 patients NO
TOTAL: 20 patients
18

SECTION 2.4.3 Patient Distribution Group The Patient Distribution Group identifies available hospital beds when there are more patients than can be handled through the pre‐assigned distribution scheme through polling hospitals about the number of available and matching on‐scene MCI patients with those beds. Critical patients receive first priority for bed assignments.
SECTION 2.5 PATIENT DISTRIBUTIONS – LEVEL 2 MCI (RED) ALERT Field operations and the Patient Distribution Group operations during a Level 2 MCI will follow the SAME procedures as outlined for a Level 1 MCI as may be reasonably executed given the circumstances of the situation. A Level 2 MCI may be upgraded to a Level 3 MCI at any time when significant resource shortages develop (e.g. all San Francisco and Bay area hospitals at or above capacity). Patient distributions to San Francisco hospitals will continue until there are no patients remaining at the scene or hospitals are at capacity. When San Francisco hospitals reach capacity, patients will be distributed to Bay Area hospitals through the Medical Mutual Aid process facilitated by the MHOAC. Additional roles and responsibilities for the Patient Distribution Group during a Level 2 MCI Alert include:
1. The Patient Distribution Group monitors and advises the Medical Health Operations
Coordinator (MHOAC) about hospital saturation.
2. The Patient Distribution Group assists the MHOAC as needed in patient distribution to out‐of‐county sites.
3. The Medical DOC may take over operation of the Patient Distribution Group if the MCI is large and / or runs over several operations periods.
2.5.1 MHOAC and RDMHC Role in Patient Distributions during a Level 2 MCI Alert During a Level 2 MCI, the MHOAC will notify Region 2 RDMHC through the Mutual Aid process as described in Section 2.12. The RDMHC will identify available beds in Bay Area hospitals.
1. The RDMHC will provide direction on patient distributions to hospitals beyond the Bay
Area if the incident is large or there are incidents simultaneously occurring in other counties that require sending patients to more distant areas within Region 2.
2. The MHOAC will request ambulance strike teams to either do the patient transports to
Bay Area hospitals or backfill San Francisco 911 ambulances.
19

3. If San Francisco AND Bay Area hospitals are near or at capacity, the MHOAC will advise DEC to upgrade the San Francisco incident alert to a Level 3 MCI.
4. The city EOC will provide as needed support and coordination.
2.5.2 Field Treatment Sites Role in Patient Distributions during a Level 2 MCI Alert Patient distribution to San Francisco and Bay Area county hospitals will continue until there are no patients remaining at the scene or the hospitals are at capacity. For larger incidents, Delayed (Yellow) and Minor (Green) patients may be delayed or held at the treatment area indefinitely or treated and released from there. If patients are held at the treatment site for several hours to days, it will be designated with as a formal Field Treatment Site and adjust its operations accordingly with additional supplies, personnel and shelter provided through field cache and alternate care supplies. All decisions to hold patients at the scene or establish Field Treatment Sites will be relayed through the Medical Group Supervisor to the Incident Commander for approval. The Medical Examiner's Office shall be responsible for the management of patients classified as Deceased (Black). For incidents with large fatality counts, a temporary morgue may be set up at the site or at a nearby location. 2.5.3 Hospitals Role in Patient Distributions during a Level 2 MCI Alert
All San Francisco hospitals will surge their internal capacity through their pre‐planned activities to accommodate the additional patients. Hospitals will update the Patient Distribution Group when additional beds are made available.
SECTION 2.6 PATIENT DISTRIBUTIONS ‐ LEVEL 3 MCI (RED) ALERTS This section assumes that overall city infrastructure is essentially intact, although it has numerous disruptions. The Medical DOC will assume Patient Distribution Group function once it is activated, operational and ready. Patient distribution will be supported by the MHOAC /RDMHC and mutual aid assets with additional local coordination and support through the city EOC
2.6.1 MHOAC and RDMHC Role in Patient Distributions during a Level 3 MCI Alert The MHOAC will work with the Region 2 RDMHC to locate out‐of‐county receiving facility beds. If there are no available beds within our region, the RDMHC will work with the California Dept of Public Health/State EMS Authority Joint Emergency Operations Center (JEOC) to identify the next appropriate region(s) within California to identify available beds. If there are no beds
20

within California, the California Dept of Public Health/State EMS Authority JEOC will contact the federal National Disaster Medical System to identify beds in other states.
The MHOAC, RDMHC, and California Dept of Public Health/State EMS Authority JEOC do all initial contacts, briefings and coordination between the local, region, state and federal levels of government responsible for the movement of patients in a disaster. The MHOAC, San Francisco EOC, RDMHC, and State EMS Authority will jointly work together to secure and coordinate as needed medical transportation arrangements and / or other logistical needs for patient movement out‐of‐county.
2.6.2 Field Patient Distribution and Operations during a Level 3 MCI Alert Field operations and the Patient Distribution Group operations during a Level 3 MCI will follow the SAME procedures as outlined for a Level 1 MCI as may be reasonably executed given the circumstances of the situation and available resources. Patient distributions to San Francisco hospitals will continue until there are no patients remaining at the scene or hospitals are at capacity. Free‐standing or hospital‐based alternate care sites may also be used during the Level 3 MCI response. Modified field operations may be invoked and include: 1. Field Triage is limited to START or JUMP START Triage only. 2. Field patients may be sent to hospital‐based or free‐standing alternative care sites.
3. Field Treatment Sites will be formally designated to hold patients at the treatment area
indefinitely or treated and released from there. Field cache and alternate care supplies will supply the Field Treatment Sites until out‐of‐county mutual aid destination or resources are received.
4. The Medical Examiner's Office shall be responsible for the management of patients triaged as Deceased (Black). Temporary morgue(s) will be set up on site or nearby locations.
2.6.3 Hospitals and Alternate Care Sites in a Level 3 MCI 1. Hospitals will surge their internal capacity by setting up alternate care areas.
2. The Department of Public Health may set up free‐standing alternative care sites. The
MHOAC and Department of Public Health ‐ Health Officer will determine the role of free‐standing alternative care sites in supporting the medical system and / or field operations and what outside support is needed (e.g. state or federal Disaster Medical Assistance Teams).
21

SECTION 2.7 PATIENT DISTRIBUTIONS ‐ LEVEL 4 MCI (RED) ALERTS A Level 4 MCI is a citywide catastrophic event. For planning purposes, it is assumed that there is a complete disruption of the City response and communications infrastructure. The ability for a formal patient distribution system to be organized will be determined at the time of the incident based upon the presenting circumstances. A decentralized command structure using Emergency District Coordination Centers may be invoked by SFFD when central dispatch is interrupted. Ambulance response units may be organized through the Emergency District Coordination Centers until the dispatch communications infrastructure and central command are restored. Patient distributions may be directed through the Emergency District Coordination Center with the overall goal of executing mass medical evacuations.
SECTION 2.8 MASS MEDICAL EVACUATIONS 2.8.1 Procedures Mass medical evacuations may be undertaken when all in‐county and Bay Area medical and health facilities are at capacity, or compromised due to damage to their infrastructure. Due to the resource intensive nature of medical care, mass medical evacuations may also be done when there is significant damage to non‐medical infrastructures or utilities (e.g. water, etc.) that interferes with the ability to provide critical support services to medical facilities. The MHOAC, in consultation with the Health Officer, city leadership and the medical facilities will determine whether to undertake mass medical evacuations after weighing its benefits versus risks. The MHOAC with support from the Medical DOC‐based Patient Distribution Group will work through the RDMHC and California Dept of Public Health/State EMS Authority JEOC to secure transportation and out‐of‐county destinations. Possible transportation options include:
I. Mobile Ground Vehicles A. Private vehicles B. Buses C. Wheel Chair Vans / Gurney Vans D. Ambulances ‐ BLS, ALS, Critical Care Transport Units, Specialty Units (Neonatal
transports, Bariatric Ambulances) II. Air Medical Services
A. Rotary B. Fixed Wing
III. Large Military Transport or Federalized Medical Aircraft For mobile ground medical vehicles, field operations will follow the same mutual aid procedures used for the Ambulance Strike Teams. EMS Policy #4020 EMS Aircraft Utilization will be followed for air medical transport categorized as:
22

• Air Ambulance • ALS Rescue Aircraft • BLS Rescue Aircraft • Auxiliary Rescue Aircraft
San Francisco International Airport (SFO) will be used as a landing and coordinating facility if large numbers of air ambulances are used to move patients. The Patient Distribution Group will work through the San Francisco EOC to coordinate with SFO. The Patient Distribution Group will check with the sending agency about its aircraft’s patient capacity and landing zone requirements. 2.8.2 Mass Medical Evacuations Requiring Large Military Transport or Federalized Aircraft The MHOAC and Medical DOC‐based Patient Distribution Group will work through the Region 2 RDMHC to contact state or federal agencies to secure large capacity military transport or federalized aircraft if thousands of patients must be moved. Federal transportation resources will likely be coordinated through the U.S. Dept of Defense Aero medical Evacuation System. Potential landing sites for large medical aircraft are SFO, Moffett Airfield or Travis Air Force Base. The 129th Rescue Wing of the Air National Guard, based at Moffett Airfield, has large transport helicopters that may land in San Francisco. The MHOAC/Patient Distribution Group will work through the San Francisco EOC to coordinate with SFO, Moffett Airfield or Travis Air Force Base to secure landing sites and patient transport areas. The MHOAC/Patient Distribution Group will check with the sending agency about its transport craft’s patient capacity and landing zone requirements. 2.8.3 Patient Destination and Distribution When Large Military Transport or Federalized Aircraft Are Used The National Disaster Medical System (NDMS) will identify and distribute patients to out‐of‐state destinations through the Federal Coordination Centers if they are not done through the CalEMA Region 2 RDMHC to in‐state locations. The RDMHC contact NDMS through the State Operations Centers for the MHOAC/Patient Distribution Group. All large military transport or federalized aircraft landing sites must have an established on‐site temporary medical facility that includes a sheltering structure, medical personnel and supplies. These temporary facilities are used to stage and provide care to patients while they await long‐range evacuation by air. The temporary sites are called Casualty Distribution Points. The MHOAC will determine whether San Francisco can assemble the resources or whether it will be staffed by California Medical Assistance Teams (CAL‐MATs) or federal Disaster Medical Assistance Teams (DMATs). The MHOAC/Patient Distribution Group will confer with the ICS Operations Chief and Incident Commander to determine if a separate Air Operations Branch will be established in the ICS
23

structure to manage and support the Casualty Distribution Point at the landing site for the aircraft. The Firescope ICS 420‐1 Manual Air Operations Branch organizational chart and position descriptions may be adapted for organizing air medical evacuations.
SECTION 2.9 MASS MEDICAL EVACUATIONS PATIENT TRACKING Patient information will be tracked on both the sending and receiving side of MCI operations. The Patient Transportation Coordinator in the field Transport Area and the Patient Unit Leader in the Patient Distribution Group both maintain Patient Logs that include:
1. Incident Name / Incident Type 2. Patient name (if known) 3. Patient Age and Gender 4. Triage tag number 5. Triage Level 6. Chief complaint 7. Name of transport provider and unit number 8. Destination 9. Date/Time of departure 10. City/State of Origin (for out‐of‐county destinations)
Below is a sample completed triage tag for out‐of‐county destinations: City, State of Origin: San Francisco, California Date / Time of departure: 2/14/2010 1400 hrs Type of transport unit: Air medical Transport provider/ unit : Air National Guard Unit #30 Destination / Contact Person: Univ of Washington Hospital, Seattle, WA Kermit The Frog, Univ of Washington Hospital, Seattle, WA
Incident Name / Incident Type: 10 California Street building collapse Triage tag number: 100010010 Triage Level: Delayed (Yellow) Patient name: Bird, Big Age / Gender: 37 yrs, male Chief complaint: Left leg crush injury + fracture
SECTION 2.10 SAN FRANCISCO RECEIPT OF OUT‐OF‐COUNTY MCI PATIENT
2.10.1 Procedures for Accepting Out‐of‐County Patients
The Medical‐Health Operations Coordinator (MHOAC) in consultation with the San Francisco Health Officer and city leadership are the only authorized individuals to make the final determination of whether or not to accept mutual aid patients from out‐of‐county. City departmental Duty Officers or staff in other city departments, who receive requests to receive
24

patients from out‐of‐county medical facilities, must refer those requests to the MHOAC or San Francisco Department of Public Health ‐ Health Officer.
The Region 2 RDMHC will first contact the San Francisco MHOAC to brief him/her on the number and types of out‐of‐county patients needing care. The MHOAC will work with the DEC or, if activated, the Medical DOC‐based Patient Distribution Group, to determine the number and types available beds. Every effort will be made to accommodate the request. However, the MHOAC and Health Officer will weigh the supply of available beds against the current local demands for those resources and only accept out‐of‐county patients if San Francisco medical facilities can reasonably accommodate additional patients while continuing to meet local demands for medical resources.
2.10.2 Organization for Receipt of Out‐of‐County Patients
The number and types of incoming patients will determine the local organizational structure for accepting and managing their distribution:
1. For a small number of patients, the MHOAC may request that the sending facility directly contact the local receiving facility.
2. For larger numbers of patients, the MHOAC may request a limited activation of the Medical DOC‐based Patient Distribution Group to serve as the single‐point‐of‐contact for the RDMHC. The MHOAC may also request a limited citywide EOC activation to support the receipt of out‐of‐county patients.
3. For significant events in other counties that necessitate sending large numbers of patients to San Francisco, the MHOAC in consultation with the Dept of Emergency Management will fully activate:
• Emergency Operations Center
• Medical DOC and other relevant departmental DOCs
• Hospital Command centers
During situations when San Francisco is receiving out‐of‐county patients, the Patient Distribution Group functions in the same manner as they would for distributing patients from a local incident. The only difference thought is that the Patient Distribution Group will work with a designated Regional Patient Distribution Group to match available local beds with out‐of‐county patients.
If large numbers of patients are being airlifted into San Francisco, the MHOAC will follow the same procedures for mass medical evacuations to out‐of‐county destinations identified in Sections 2.8 ‐ 2.9 to receive the patients. When receiving patients evacuated by air, the medical facility at the landing site is called the Casualty Receiving Point. The MHOAC will also work with local ambulance providers to secure transportation to in‐county hospital destinations from the landing site.
25

SECTION 2.11 – MEDICAL COMMAND 2.11.1 Organization The Medical‐Health Operations Area Coordinator (MHOAC) in the EOC Human Services Branch along with the Medical DOC coordinates medical services and resources within the Operational Area (County) in the event of a disaster or major incident. The MHOAC is the designated single‐point of contact between the Operational Area and the Region 2 Regional Disaster Medical Health Medical Coordinator (RDMHC) when medical mutual aid is required.
2.11.2 Medical Incident and Resource Assessment in a MCI
The overall goal for Medical Command in a disaster operation is to match the demand for medical resources with the supply of medical resources. This is done through initial and on‐going assessments of the incident and medical resources to provide direction for the response and management strategies. Assessments may include:
• Situation (Incident)Assessments
• Medical Resource Assessments
• Resource Mobilization, Allocation and Tracking
• Demobilization
The MHOAC and Medical DOC are responsible for doing initial and on‐going citywide medical resource assessments. Medical‐health information assessments include, but are not limited to the following:
MCI Medical‐Health Assessment Assessment Source Data Points Impact of MCI on the medical 911 system
DEC Dispatch
Number of EMS calls, queue times, call types, number of ambulances available
Hospitals Medical DOC Number and types of beds available (HAVbed format) and Hospital Facility Status Reports Incident Response:
Number of Immediate, Delayed, and Minor patients received. Number of patient deaths related to the incident.
SFFD Ambulances
SFFD DOC reports to Medical DOC
Available Ambulances: Number available now and in 24‐hours. Adequacy of resources (supplies, personnel, etc.). Incident Response:
Number of Immediate, delayed, and minor patients transported from the incident. Number of patient deaths related to the incident. Whether resource surge efforts are underway.
26

Private Ambulances
Medical DOC Available Ambulances: Number available now and in 24‐hours. Companiesoperating in multiple counties must count only ambulances physically based within San Francisco to avoid double counting with other counties. Adequacy of resources (supplies, personnel, etc.). Incident Response:
Number of Immediate, delayed, and minor patients transported from the incident. Number of patient deaths. Whether resource surge efforts are underway.
2.11.3 Status Reporting to Medical Command
The Medical DOC reports to MHOAC at EOC Operations Section, Human Services Branch the following summary information:
1. Medical assessment results for all San Francisco hospitals and private ambulances noting the data points described above.
2. Pertinent information related to health threats and status of medical‐health containment efforts.
3. Total hospital and field casualty and fatality counts for the incident. 4. Requests for medical resources.
SFFD DOC reports to Fire EMS at EOC Operations Section, Fire and Rescue Branch the following information:
1. Pertinent incident scene information such as threatened structures, and status of fire containment or rescue efforts.
2. Requests for EMS resources that cannot be fulfilled through SFFD resources. 3. Field casualty and fatality counts are reported to Medical DOC. The Medical DOC is
responsible for the reporting of field counts with the overall healthcare facility counts to the MHOAC at EOC Operations Section, Human Services Branch.
2.11.4 Situation Status Reporting To Region and State
The MHOAC, DEM Duty Officer or Medical DOC (if activated) provides written medical Situation Status (SitStat) reports on Level 2 and 3 MCI alerts and activities to the Coastal Region ‐ Regional‐Health Disaster Medical Coordinator (RDMHC) using the procedures and format outlined in the California Disaster Health Operations Manual. The MHOAC is also responsible for providing on‐going medical Sit Stat briefings to the RDMHC. A copy of the California Disaster Health Operations Manual SitStat report is found in the Appendices.
SECTION 2.12 – MEDICAL MUTUAL AID
This section covers general medical mutual aid concepts and use. Refer to Section 2.14 for Ambulance Strike Team requests.
27

2.12.1 Medical Mutual Aid Use
Medical mutual aid is driven by the medical needs of the patients. Therefore, medical mutual aid may be used in more situations that non‐medical mutual aid. These situations may include:
• When the surging of medical resources within San Francisco has been exhausted due to overwhelming patient demand.
• For medical resources that have a limited supply in San Francisco. For example, limited supplies of trauma center beds for critical trauma patients or burn care beds for severely burned patients may necessitate sending patients to out of county facilities even though the total number of patients resulting from a particular incident is low.
• When it is determined that patients may receive treatment faster if they are sent to out‐of‐county facilities using the Mutual Aid process rather than “surging” in‐county assets. For example, San Francisco has disaster medical field care clinics that may take several hours to set up, supply and staff whereas sending patients to out‐of‐county facilities may take less than one hour.
Many medical assets are available within San Francisco and should be accessed first before activating Mutual Aid, unless it has been determine by direct patient care providers (field or hospital) that out‐of‐county assets may provide a better patient outcome.
2.12.2 Initiating a Request for Medical Mutual Aid into San Francisco The Incident Commander (IC), the DEC, any hospital or medical facility, DPH or other city agency may initiate a medical mutual aid resource request by notifying the following:
• DEM Duty Officer if the EOC and Medical DOC are not activated. The DEM Duty Officer may be contacted 24/7 through the DEC. The DEM Duty Officer will contact the MHOAC.
• Medical DOC if activated. The Medical DOC will contact the MHOAC.
2.12.3 Medical Mutual Aid into San Francisco
All requests for Health and Medical mutual aid resources into the San Francisco Operational Area shall be authorized and coordinated through the MHOAC or his/her designee. The MHOAC, DEM Duty Officer or Medical DOC (if activated) shall complete the mutual aid resource request using the California Disaster Health Operations Manual process and templates. The California Emergency Management Agency (CalEMA) will assign a Mission Number once the request is entered into the Regional Information Management System (RIMS). The MHOAC or designee may also request EOC or DOC activations to assist in supporting the receipt of out‐of‐county mutual aid assets. The MHOAC and / or DEM Duty Officer will advise DEM and city leadership about any medical mutual requests.
28

2.12.4 Medical Mutual Aid from San Francisco
Requests originating through the regional/state Health and Medical mutual aid system for San Francisco medical resources shall be authorized and coordinated through the MHOAC or his/her designee. The Region 2 RDMHC will contact the MHOAC directly if the citywide EOC is activated or the DEM Duty Officer through the DEC if the EOC is not activated. The DEM Duty Officer will then contact the MHOAC.
The MHOAC or designee will take the mutual aid request information and contact the appropriate city agency or medical‐health facility to fulfill the request. The MHOAC may elect to coordinate the sending of mutual aid assets to the out‐of‐county destinations, or delegate that task to the agency fulfilling the request or request EOC and/or DOC activations to supporting the sending of San Francisco mutual aid assets to out‐of‐county destinations.
Requests originating through the Fire Mutual Aid system for SFFD ambulances will be coordinated through SFFD. See Section 2.14 on ambulance strike teams.
Resource Request Tracking and Fulfillment
The RDMHC and the MHOAC will advise each other when a resource request(s) has been fulfilled, whether any changes in quantity or substitutions were necessary, its projected delivery time, or if the request was cancelled. The MHOAC may task the EOC or Medical DOC Logistic Section with tracking the status of the resource request.
SECTION 2.13 – MEDICAL MUTUAL AID RESOURCES Many medical assets are available within San Francisco and should be accessed first before activating the Medical Mutual Aid System, unless it has been determine by direct patient care providers (field or hospital) that an out‐of‐county asset may provide a better patient outcome or if it is determined that local resources are exhausted/overwhelmed.
“Ready‐to‐Go” options for medical mutual aid resources or responses within include:
Patient Transportation • Ground – Ambulances; alternative transport (Muni buses for green patients able to
tolerate sitting upright) • Air Ambulances • Strike Teams or Task Forces
Supplies and Equipment • Medical Supplies Caches and Equipment Trailers • Specialized Equipment
Treatment Areas • Portable or Mobile Facilities • Medical Equipment and Supplies • Pharmaceuticals
Personnel
29

• ALS or BLS Personnel • Californian Medical Assistance Teams (Cal‐MAT – state) • Disaster Medical Assistance Teams (DMAT ‐ federal) • Medical and Nursing Personnel affiliated with Medical Volunteer Registries • Mission Support Teams provide administrative, logistical, and liaison support.
The MHOAC maintains a guide of Medical & Health Special Resources that may be available during a MCI. The San Francisco Department of Public Health Emergency Operations Manual also contains a list of other available medical and health resources. The DPH list does not include equipment and supplies that may be available from individual medical providers within San Francisco such as private hospitals. Other available options for in‐county resources include the caches that each medical‐health provider maintains. This may be an available option if your resource need is very limited or if there are medical specialty items that may only be immediately available through another medical provider (e.g. special surgical instruments, etc.). Requests for to access provider caches must go through an individual provider’s leadership or, if activated, their disaster command center. Other non‐medical supplies lists maybe found through the citywide EOC Logistics Section.
SECTION 2.14 – MUTUAL AID REQUESTS FOR AMBULANCE STRIKE TEAMS In California, the standard Ambulance Strike Team consist of five ambulances (ambulance with two personnel) with common communications and a leader and are typed according to FEMA typing for medical and health resources. Each may include a Disaster Medical Support Unit or comparable local support unit to serve as an operational command, control, and communications center. 2.14.1 Ambulance Strike Teams Standard Configurations
ALS Ambulance Strike Team: • 5 ambulances with 2 ALS personnel, or 1 ALS and 1 BLS personnel, both trained in
ICS 100 plus 1 Strike Team Leader trained in ICS 100, 200 & 300, and Strike Team Leader Training.
BLS Ambulance Strike Team:
• 5 ambulances with BLS personnel trained in ICS 100 plus 1 Strike Team Leader trained in ICS 100, 200 & 300, and Strike Team Leader Training.
30

2.14.2 Requesting Ambulance Strike Teams into San Francisco The Incident Commander (IC) or Medical Group Supervisor, cleared through the Incident Commander, may initiate an Ambulance Strike Team request by notifying the following:
• DEM Duty Officer if the EOC and Medical DOC are NOT activated. The DEM Duty Officer may be contacted 24/7 through the DEC. The DEM Duty Officer will contact the MHOAC.
• Medical DOC if activated. The Medical DOC will contact the MHOAC.
2.14.3 Receipt of Requests for Ambulance Strike Teams from San Francisco The MHOAC shall authorized and coordinate requests originating through the regional/state Medical Mutual Aid system for San Francisco ambulances. However, requests originating through the Fire Mutual Aid system for SFFD ambulances will be approved through SFFD in consultation with the MHOAC. The MHOAC will contact local ambulance providers, including SFFD, to ascertain their availability of ambulances and staff for a Strike Team. The RDMHC and the MHOAC will advise each other of the following when an ambulance Strike Team request(s) has been fulfilled:
• Provider company or agency name, unit number, unit type (ALS or BLS), and estimated time of arrival (ETA) for each ambulance dispatched.
• Contact number in the event of for cancellation while the Strike Team is en route.
• Location of ambulance staging area(s).
The San Francisco MHOAC is also responsible for coordinating the receipt of out‐of‐county ambulance strike teams with the OES Region 2 RDMHC, but may delegate that to the field Incident Command. 2.14.4 Mutual Aid Medical Treatment Protocols EMS Personnel operating in another county during a mutual aid response will follow all applicable San Francisco EMS Agency Policies and Medical Protocols with the exception of EMS Agency #5000 Destination Policy. The Incident Commander, Medical Group Supervisor or Transport Unit Leader for the incident will assign local receiving facility destinations for the mutual aid response.
SECTION 2.15 EMERGENCY DECLARATIONS – AUSTERE MEDICAL CARE 2.15.1 Defined
Austere Medical Care is a modified standard of care provided during situations of duress when medical resources, supplies and / or medical personnel are limited or unavailable. The
31

32
modified standard is toward providing a more basic, less time and resource intensive level of medical care. The intent of austere medical care is to “do the most good for the greatest number of people” during a disaster. By modifying the standard of care to a more basic (austere) level, fewer medical resources are provided to an individual person, but, overall, are distributed to a greater number of individuals in a given population.
2.15.2 Authorization and Limitations
In San Francisco, austere care only applies to field care. It does not affect in‐patient hospital services.
Austere medical care is only used in situations of extreme duress resulting from a catastrophic event. Field personnel should consider requests for authorization of Austere Medical Care Standards when the situation is completely overwhelming local resources and the possibility of mutual aid are remote. Requests for authorization of Austere Medical Care Standards must be routed through the chain of command. Austere medical care in the pre‐hospital environment is authorized only by the County Health Officer or, in his/her absence, the Deputy Health Officer. Authorization of the use of austere medical care will be communicated through the Incident Command System.
2.15.3 How to Perform Austere Care
The San Francisco EMS Agency P‐100 Austere Care Protocol is the approved guideline for austere care in the pre‐hospital environment. Refer to that protocol for further details. EMS Agency P‐100 Austere Care Protocol does NOT apply to in‐hospital care.
SECTION 2.16 DEMOBILIZATION
Demobilization will not be covered in this plan. For incidents in San Francisco, demobilization plans will be developed and disseminated through the EOC or delegated to the relevant DOC.
San Francisco EMS responders deployed in mutual aid response will be released from their assignment through that incident’s demobilization process. Units that are released will advise their respective provider agency. A supervisor from the provider agency will contact the MHOAC to advise them that the San Francisco mutual units are released and that their mission is complete.

1
PART 3BACKGROUND
SECTION 3.0‐ INTRODUCTION 3.0.1 Plan Objectives The Department of Emergency Management ‐ Emergency Medical Services (EMS) Agency Multi Casualty Incident (MCI) Plan (herein referred to as the “Plan” or “MCI Plan”) identifies and delineates the structure and processes for the provision of emergency medical care by local EMS system participants during a MCI event of any size or magnitude. The intent is to ensure the provision of rapid and appropriate emergency medical care to the most possible patients through a coordinated response system based on incident management principles. The overall objective of the plan is to minimize the morbidity and mortality associated with large scale emergency patient care incidents occurring in San Francisco. This plan is compliant with the State of California Firescope, the California Standardized Emergency Management System (SEMS), the federal National Incident Management System (NIMS), as well as local planning, policies and procedures related to MCI activities. 3.0.2 Plan Organization
This MCI Plan is organized into three primary sections:
1. Plan 2. Annexes 3. Appendices
The Plan describes core emergency medical response operations during a multi‐casualty incident (MCI). The Plan is subdivided into three parts:
• Part 1 ‐ Response Charts • Part 2 ‐ Core Response • Part 3 ‐ Background
The Part 1 ‐ Response Charts provide easy and rapid access to the required actions for front‐line responders. Part 2 ‐ Core Response is the operational “playbook” that prescribes in detail the activities that all EMS participants must follow during a general response to a MCI. Part 3 ‐ Background provides the relevant background information to the reader with the “how” and “why” for the selected structure and processes of the response operations.

2
The Core plan is further subdivided into sections based on the various components and phases of a MCI response. The use of discrete sections provides responders with the information they need in user‐friendly format that does not require reading the entire plan. The intent of this format is to provide quick, clear information on specific response operations. It also fulfills the requirement for scalability since only portions of the plan may be required for a particular incident response operation
The Annexes describe special emergency medical response operations for scenario specific situations (e.g. bombings, contaminated scenes, etc.). The Annexes supplement the Core Plan and are intended to be used tandem with the general response information in the Core Plan.
The Appendices provide reference information relevant to supporting a successful response operation. It includes guides to the various EMS resources, Field Incident Command System Position Descriptions, maps, glossary and etc.
3.0.3 Authorities, Standards and Guidelines The following authorities, standards and guidelines provide compliance for the development and implementation of this Plan: Local
• The San Francisco Emergency Medical Services MCI Plan is an approved policy and procedure of the Department of Emergency Management ‐ EMS Agency
• City and County Emergency Response Plan, April 2008 Region
• San Francisco Bay Area Regional Coordination Plan – Medical and Health Subsidiary Plan, March 2008
State
• Firescope Field Operations Guide, ICS 420‐1, July 2007 • California Standardized Emergency Management System (SEMS) • California Health and Safety Code, Sections 1797.103; 1797.150‐153; 1797.204; and
1797.220 • California Code of Regulations, Title 19, Division 2, Chapter 1 • California Code of Regulations, Title 22, Section 100167 (b) (2 ‐ 3); 100168 (b) (4);
and 100169 (a) • California Code of Regulations, Title 22, Division 9, Section 100255 • California Government Code, Article 9, Section 8605 • California Disaster Medical Operations Manual from California Emergency Medical
Services Authority (draft version 09/09/08) • California Disaster Health Operations Manual (Interim version, October 2009) • California Master Mutual Aid Agreement

3
• California Emergency Services Act • California Emergency Medical Services Authority Publication #215 Ambulance Strike
Teams / Medical Taskforce Guidelines (2003). Federal
• National Incident Management System (NIMS) 3.0.4 Personnel Training and Competency Levels All EMS providers should check with their respective training providers for the most current training requirements specific to their roles during a MCI response. At a minimum, this plan assumes that users of this plan will be familiar with and proficient in the following:
First Receiver (Hospitals Only) • Simple Triage and Rapid Treatment (START) and JUMPSTART • Hospital Incident Command System • Hospital Incident Command System Hazardous Materials Awareness • Incident Command System (up to ICS 200 level) • National Incident Management System (NIMS) IS‐700 and IS‐800 • Working knowledge of San Francisco EMS Agency Policies and Procedures
All Field First Responders
• Simple Triage and Rapid Treatment (START) and JUMPSTART • California Standardized Emergency Management System (SEMS) • Incident Command System (up to ICS 200 level) • National Incident Management System (NIMS) IS‐700 and IS‐800 • Hazardous Materials First Responder Awareness • Working knowledge of San Francisco EMS Agency Policies and Procedures
Ambulance Strike Team Leader
• Incident Command System (up to ICS 300 level) • Ambulance Strike Team Leader Training (State EMS Authority course) • Ambulance Strike Team Provider Training (State EMS Authority course)
On‐Scene Command Staff
• Incident Command System (up to ICS 400 level)
Assigned EOC or DOC Command Staff • City and County Emergency Response Plan • City Departmental Emergency Response Plans (any city DOC staff) • Provider Emergency Operations Plan (any private provider DOC staff) • (Recommended) MGT 313 – Incident Management / Unified Command

4
SECTION 3.1 PATIENTS 3.1.1 Triage
Triage is a French word meaning “to sort.” It is used to identify patients that have the most immediate need for medical care vs. those that may wait. Triage is the primary tool used in determining the most appropriate allocation of available medical care resources in a large multi‐casualty incident.
Field treatment and the eventual distribution of patients to receiving facilities are determined by the systematic triage of patients at the scene. The flow of the entire emergency medical MCI response is driven by both the total number patients and their assigned triage levels. It is therefore crucial that First Responders do appropriate patient triage at the onset of every MCI – no matter how large or small the incident.
3.1.2 Required Triage Standard – START Triage and Jump START
The EMS Agency requires that First Responders do START Triage during a MCI on all adult patients and JUMP START on all pediatric patients. Both systems are physiological assessment methods based on a simple mnemonic “RPM” (Respirations, Perfusion, Mentation). START is an acronym for Simple Triage and Rapid Treatment. Once the START triage evaluation is complete, the victims are labeled with one of four color‐coded triage level categories:
Minor = walking wounded / can delay care for up to three hours
Delayed = serious non‐life‐threatening injury / can delay care for 1 hour
Immediate = life‐threatening injury / requires immediate care
Deceased / Expectant = pulseless / non‐breathing or imminent demise
Triage categories are an indication of the desired time to receive treatment. In a large scale incident, actual time to treatment may vary based on the availability of resources.
JumpSTART is based on the START physiologic triage system used for adults. However, JumpSTART system recognizes the key differences between adult and pediatric physiology and substitutes appropriate pediatric physiologic parameters at triage decision points. JUMP START is used for the following:
1. Children ages newborn to 8 years or, 2. When the patient appears to be a child or, 3. Whenever you can use a length‐based (Broselow) resuscitation tape.

5
Both START Triage and JumpSTART Triage are designed for use in only disaster and multi‐casualty situations, not for daily EMS or hospital triage. Refer to Figure 1 and Figure 2 for the START and JUMP START Flow Charts.
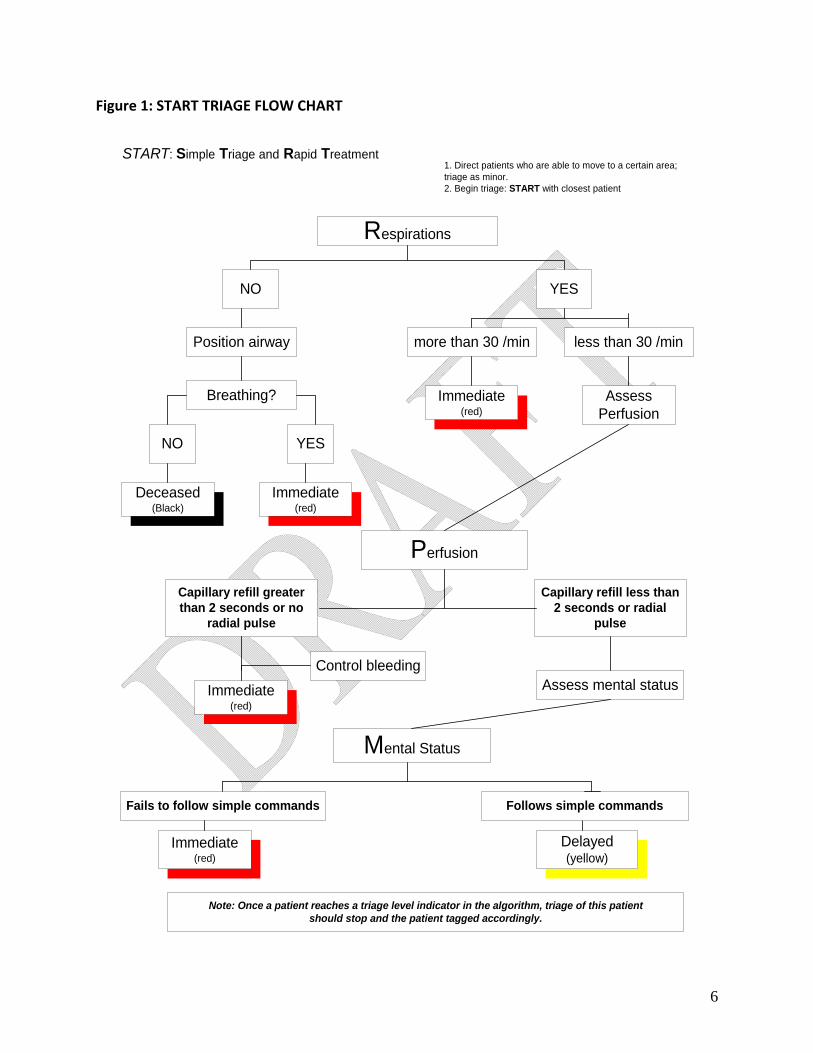
6
Figure 1: START TRIAGE FLOW CHART
Respirations
NO YES
Position airway
Breathing?
NO YES
Deceased(Black)
more than 30 /min
Perfusion
Capillary refill greaterthan 2 seconds or no
radial pulse
Control bleedingAssess mental status
Mental Status
Fails to follow simple commands
Delayed(yellow)
Note: Once a patient reaches a triage level indicator in the algorithm, triage of this patientshould stop and the patient tagged accordingly.
Immediate(red)
less than 30 /min
Immediate(red)
AssessPerfusion
Capillary refill less than2 seconds or radial
pulse
Immediate(red)
Immediate(red)
to a certain area;
tient
1. Direct patients who are able to movetriage as minor.2. Begin triage: START with closest pa
START: Simple Triage and Rapid Treatment
Follows simple commands

7
START TRIAGE STEPS
Use the mnemonic “RPM” (Respirations, Perfusion, Mental Status) for the START Triage assessment sequence
1. MOVE WALKING WOUNDED
• Direct patients who are able to walk to another area. Tag GREEN.
2. RESPIRATIONS • If respiratory rate is 30/minute or less go to PERFUSION assessment.
• If respiratory rate is over 30/ minute, tag RED.
• If victim is not breathing, open the airway, remove any visible obstructions and re‐position head to open
airway. Re‐assess respiratory rate.
• If victim is still not breathing, tag BLACK.
3. PERFUSION • Palpate radial pulse or assess capillary refill (CR) time.
• If radial pulse is present or CR is 2 seconds or less, go to MENTAL STATUS assessment.
• No radial pulse or CR is greater than 2 seconds, tag RED.
• Control any major external bleeding at this point.
4. MENTAL STATUS • Assess ability to follow simple commands and orientation to time, place and person.
• If the victim does not follow commands, is unconscious, or is disoriented, tag RED.
• If the victim follows simple commands tag YELLOW.
SPECIAL CONSIDERATIONS.
• Stop further any point in the RPM assessment when a RED triage level is identified.
• Tag YELLOW obvious significant injuries (e.g. burns, fractures).
• Correct only life‐threatening issues (e.g. airway obstruction, severe hemorrhage) during initial triage.

Figure 2: JUMP START TRIAGE FLOWCHART*
*See www.jumpstarttriage.com for additional information.
8

3.1.3 Other Considerations for Patient Triage
START Triage and JUMP START are the first triage systems used in the designated MCI Triage Area, followed by Trauma Triage Criteria in the designated Treatment and / or Transport Area(s). Other clinical considerations should be factored into the determination of an appropriate triage level and destination for patients depending on the provider training, availability of personnel, and if the situation safely allows for it. Below is list of other injury scoring systems and clinical considerations that may be applicable during the MCI triage process:
• Glasgow Coma Scale • Burn Rule of Nines • Significant Medical Complaints • Special Populations:
Age Extremes Pregnant Medically Fragile
3.1.4 Required Triage Tags and Patient Records
First Responders must use a triage tag to label triaged patients by the severity of their injury. Triage tape is permitted in the Triage Area, but should be replaced by a tag in the Treatment or Transport Area(s). The required standard triage tag is the bar coded Disaster Management Systems' All Risk® Triage (Military Version (DMS‐05006M) Tag from Disaster Management Systems available on‐line at www.TriageTags.com
Patient identifying information, vital signs, treatment, and destination should be written on the triage tags when the time and situation permit it. EMS patient care records may be used if adequate personnel resources are available and the patient is held at the scene for an extended period of time. 3.1.5 Deceased Care
Deceased patients must be labeled as Deceased with the triage tag. Deceased patients require no further care and may be left in place while responders attend to other viable patients. Responders should notify the San Francisco Medical Examiner to assume responsibility for the disposition of deceased patients.
Efforts should be made to treat deceased patients with respect, and to cover or move them as resources and the situation permits. If the incident is a crime scene, the Medical Examiner or SFPD must approve moving deceased patients. When moving a body, Responders should do the following:
9

1. Fill out information on identifying information on the triage tag or attach a morgue tag or other label directly to the body. Include:
• Date, time and location body found, • Name/address of decedent, if known, • If identified, how and when, • Name/phone of person making identity or filling out tag, and • Note any contamination
2. The personal effects must remain with the body at all times. If personal effects are found and
thought to belong to a body, place them in a separate container and tag. Do not assume any loose effects belong to a body.
3. Place the body in a disaster body bag or in plastic sheeting and securely tie to prevent
unwrapping. Attach a second exterior tag to the sheeting or pouch. 4. Move the properly tagged body with their personal effects to a separate, safeguarded location,
preferably with refrigerated storage.
SECTION 3.2 INCIDENTS 3.2.1 Disaster Classification Schemes vs. Multi‐Casualty Incident Classification Schemes
Disaster classification schemes do not always address the unique nature of large‐scale patient care incidents. A small number of victims requiring a limited supply of a particular medical resource may constitute a local disaster. For example, 20 pediatric trauma victims may easily overwhelm the limited capacity of local pediatric trauma care services. Therefore, an effective MCI classification scheme must be factor in the level of unmet need for medical resources to effectively mitigate the incident rather than classifying the incident solely on the number of victims.
3.2.2 California’s Disaster Medical System Multi‐Casualty Incident Classification Scheme The California’s Disaster Medical System uses an incident scale and required medical resource classification scheme to classify MCI levels:
1. LEVEL 1 Multi‐Casualty Incident – Requires response resources from and the distribution of casualties within the Operational Area only.
2. LEVEL 2 Multi‐Casualty Incident – Requires response resources from or distribution of casualties to other Operational Areas within the mutual aid region of the impacted Operational Area(s).
10

3. LEVEL 3 Multi‐Casualty Incident – Requires State or Federal response resources or distribution of patients beyond the mutual aid region using state or federal systems and resources.
SECTION 3.3 SAN FRANCISCO INCIDENT CLASSIFICATIONS AND ALERT LEVELS
San Francisco uses a classification scheme for MCI Levels that is similar to the one used by the California’s Disaster Medical System. The progressive MCI Levels for San Francisco are important because they determine an alert level that is communicated to all EMS participants that corresponds to a specific set of actions they should take to respond to the MCI incident. It is important to note that the cut off points for the number of victims needed to call a either a Level 1, 2 or 3 MCI alert is flexible. Section 2.2.1 of this Plan describes the operation use of the MCI alert levels. LEVEL ZERO MEDICAL 911 SERVICE DISRUPTION ALERT = Disruption of the medical 911 services due to
1) Overwhelming demand for EMS resources due to factors affecting the overall city population (e.g. extreme weather, wildfire smoke or flu) results in ambulance and / or hospitals supply shortages. 2) Physical plant disruption at one or more hospitals that disrupts their participation in the medical 911 system.
Level Zero is a notification and assessment‐based alert. EMS providers will be notified of the specific service disruption and requested to assess their resources. Subsequent actions will be on based the assessment and determined by the DEM Duty Officer in consultation with the EMS Agency Medical Director, the Director of Health, the SFFD Chief and the leadership of the affected EMS providers. MCI YELLOW ALERT = Declared for incidents with a potential for multiple casualties so as to give a “head up” to operational staff.
LEVEL 1 MCI (RED) ALERT = MCI with 6 or greater of Immediate category victims or 10 ‐ 50 victims of any triage level. EMS resources available during usual daily operations can contain and manage the situation.
LEVEL 2 MCI (RED) ALERT = MCI with 51 ‐ 100 victims of any triage level OR response requires resources from or distribution of casualties to other counties within our California mutual aid region. LEVEL 3 MCI (RED) ALERT = MCI with 101 or more victims of any triage level OR response requires significant resources from or distribution of casualties outside our California mutual aid region using state or federal systems and resources.
11
LEVEL 4 (RED) MCI = Catastrophic event with complete disruption of the City response and communications infrastructure. The infrastructure disruption precludes the use of a centralized command structure. Recovery outlook is long‐term.
The chart on the next page describes the San Francisco incident levels and their corresponding alert levels followed by examples of incidents that would trigger the alerts.
12

ALERT LEVEL EXAMPLES
Definition
Examples Level Zero Medical
911 Service Disruption
Disruption of the medical 911 services due to:1) Extreme service demand usually that results in an ambulances shortage and/or saturation of all hospitals, 2) Physical plant disruption at one or more hospitals that disrupts the medical 911 system’s ability to provide patient services.
• Extreme hot weather generates hundreds of medical 911 calls resulting in an ambulance shortage and/ or saturation of hospital emergency departments.
• Catastrophic power failure at SFGH disrupts the
San Francisco trauma system.
MCI Yellow Alert
On‐Scent Incident Commander or DEC declares a Yellow Alert for incidents with potential multiple casualties.
Large residential building is on fire, but no casualties yet identified.
Level 1 (Red) MCI Alert
MCI with 6 or greater of Immediate category victims or 10 ‐ 50 victims of any triage level. EMS resources available during usual daily operations can contain and manage the situation.
• Bus accident with 15 patients. All 15 patients triaged as YELLOW.
• Muni train collision with 20 green, 10 yellow and 1 red.
Level 2 (Red) MCI Alert
MCI with 51 ‐ 100 victims of any triage level OR response requires resources from or distribution of casualties to other counties within our California mutual aid region. Situation requires response resources from and the distribution of patients to outside the Operational Area.
• Building collapse with 30 victims triaged RED that all meet trauma triage criteria for trauma center care. Must distribute patients to SFGH and other Bay Area trauma centers.
• BART train accident with 95 victims. • Multiple simultaneous incident(s) that
overwhelm local EMS resources.
Level 3 (Red) MCI Alert
MCI with 101 or more victims of any triage level OR requires resources from or distribution of casualties to outside our California mutual aid region using state or federal systems and resources. Assumes infrastructure is essentially intact, although it has numerous disruptions. EMS and citywide resources need significant support and coordination above the field level and operational area command.
High magnitude earthquake with numerous buildings collapsed and hundreds of casualties. Assumes infrastructure is essentially intact, but has numerous disruptions. The 1989 Loma Prieta Earthquake is an example.
Level 4 (Red) MCI
Catastrophic event with complete disruption of the City response and communications infrastructure. Recovery outlook is long‐term
High magnitude earthquake with numerous buildings collapsed and hundreds of casualties and widespread disruption of infrastructure. The 1906 San Francisco Earthquake is an example.
13
SECTION 3.4 ALERT LEVELS AND STANDARDIZED EMS SYSTEM ORDERS The alert levels correspond to Standardized EMS System Orders which are defined as pre‐determined EMS system participant actions in response to a MCI. Standardized EMS System Orders are similar to Job Action Sheets or Position Descriptions that individual field personnel or EOC / DOC command staff follow during a disaster response. The difference though is that Standardized EMS System Orders apply to the response actions of an entire EMS provider organization (e.g. a hospital or an ambulance provider company). The purpose of the alert levels and corresponding Standardized EMS System Orders is to improve the speed, efficiency and overall coordination of the initial operational response to a MCI. An alert initiates the start of a Standardized EMS System Order that is followed in the first hour(s) to days of a MCI response until an Incident Command is organized and able to create and distributes an Incident Action Plan with response objectives that are specific to the incident. Standardized EMS System Orders are found in Part 1 – Response Charts.
SECTION 3.5 EMS PROVIDER MCI ROLES AND RESPONSIBILITIES
3.5.1 Primary EMS Providers San Francisco Fire Department SFFP provides fire suppression services, and ALS ambulances and BLS First Responder in the San Francisco EMS System. The SFFD field role in a MCI is to provide emergency medical care at the scene, transport victims to receiving facilities and to fill any position within the field ICS structure, especially positions within the medical branch. SFFD operates mobile Multi‐Casualty Units that can quickly bring additional emergency medical supplies to a scene. SFFD staffs the San Francisco Metropolitan Medical Task Force (MMTF) that provides special responses for Chemical, Radiological, and Radiological Incidents. The SFFD Departmental Operations Center provides command, coordination and support for their suppression and EMS units during a MCI. ALS Ambulance Providers Advanced Life Support (ALS) Ambulance Providers (e.g. American Medical Response, King American Ambulance, and Presidio Fire Department) provide emergency ALS level ambulance services and ALS inter‐facility transport services. ALS Ambulance Providers’ role in a MCI is to provide emergency medical care at the scene, transport victims to hospital or other alternate treatment sites (if in use and authorized) and to fill any position within the field ICS structure, especially positions within the medical branch.
14

BLS Ambulance Providers Private Basic Life Support (BLS) Ambulance Providers (e.g. Bayshore Ambulance, St. Joseph’s Ambulance, and ProTransport‐1) provide BLS inter‐facility transport services in the San Francisco EMS system. BLS Ambulances Providers’ may have a direct role in a MCI field response by providing emergency medical care at the scene, transporting victims to hospital or other alternate treatment sites (if in use and authorized) and filling any position within the field ICS structure, especially positions within the medical branch. BLS may also provide back‐ up ambulance “surge capacity” to the day‐to‐day EMS System if an incident(s) requires all available ALS resources. Alternative uses of the BLS providers during a large MCI are only authorized by the EMS Medical Director in consultation with the Director of Health/Health Officer and management at each BLS provider company. Air Medical Service Providers Air Medical Services Providers offer on scene emergency medical care and air evacuation of patients. REACH, Stanford Lifeflight and CalSTAR provide services for San Francisco EMS and throughout most of Northern California. During an MCI, air medical services are primarily used to transport the most critically injured patients to out‐of‐county trauma centers. General Acute Care Hospitals Hospitals provide emergency medical care and definitive medical treatment to patients. Their role is the same during MCI event within the limits of their capacity to “surge” their staff and internal resources. Hospitals may “stabilize and transfer” if the patient’s medical needs require specialty services not available at that hospital or if they are at capacity and cannot offer an available bed or staffed treatment space. Department of Emergency Management DEM provides various emergency management functions and consists of two divisions: Division of Emergency Communications (911) and the Division of Emergency Services (DES).
• Division of Emergency Communications (DEC) DEC is responsible for receiving 911 calls and dispatching police, fire, and EMS services. The primary role of DEC during a MCI is to notify and alert of key response personnel, and to dispatch and track field response resources including mutual aid resources and initially staff the Patient Distribution Group.
• Division of Emergency Services (DES) DES is responsible for developing citywide emergency plans, activating the City’s Emergency Operations Center (EOC) and preparing citizens for all‐hazards events (i.e. earthquakes, terrorism, and tsunamis). During an MCI, DES may activate the City’s EOC to support overall MCI operations and request emergency declarations from the Mayor.
• EMS Agency
15
The San Francisco EMS Agency is in under DES. The EMS Agency is responsible for planning, coordinating, and evaluating emergency medical services for San Francisco. During a MCI or medical disaster, the EMS Agency fulfils diverse roles, including serving as the Medical Health Operational Area Coordinator, modifying or creating EMS policy or protocols to meet changing situational needs, activating or staffing the Medical Department Operations Center, or the City Emergency Operations Center.
3.5.2 Supporting Providers and Participants In addition to the primary EMS System participants, there are other organizations that may work closely with the EMS System during a MCI or Mass Casualty Event. San Francisco Police Department SFPD provides law enforcement to most of the San Francisco. They serve as the law enforcement element of the San Francisco Metropolitan Medical Task Force. They also can provide SWAT, Explosive Ordinance Disposal, and other specialized law enforcement services. During an MCI, they may provide force protection, security for critical assets, and create cordons. San Francisco Sheriff’s Department San Francisco Sheriff’s Department provides protective and security service for City and County facilities and buildings, including San Francisco General Hospital, and the Department of Public Health Department buildings. They also can provide aerial surveillance or recognizance using their air units. During an MCI, they may provide force protection, security for critical assets, and create cordons. California Highway Patrol California Highway Patrol provides law enforcement to the State and Federal highways within San Francisco and provides protection and security for state facilities and buildings. During an MCI, they may provide force protection, provide security for critical assets, and create cordons. Auxiliary Communication Service Auxiliary Communication Service (ACS), coordinated by the Dept of Emergency Management’s Division of Emergency Services, provides amateur radio operators with equipment for disaster response and large special events. In a MCI, ACS may provide amateur radio operators to field, hospital, and emergency operations centers or be used to replace or to augment communication capabilities. Department of Public Health
• Communicable Disease Control and Prevention Section CDCP provides community monitoring for communicable diseases, conducts epidemiological investigations, and provides communicable disease control and prevention information to medical professionals and the community that may include:
16

infection control protective measures, prophylaxis or treatment, identification of the type and source of an outbreak, and if necessary, issue isolation or quarantine orders.
• Environmental Health Section EHS is assures the safety of the food and water supplies. They also provide technical and scientific advice to the SFFD on the detection, identification, and handling of hazardous materials and management of hazardous situation. They are also responsible for approving the location and safety of all mass shelters.
• Behavioral Health Services BHS provides mental and substance abuse services. During a large MCI, they will provide crisis intervention services for health providers, and may be available for public, first responder and first receiver crisis intervention.
• Clinics and San Francisco Community Clinics DPH Clinics and the Community Clinics provide varying levels of general clinical or specialized clinical care at the clinic level. During larger MCIs, when general acute care hospitals are overwhelmed, clinics may be and option for use as an alternate treatment site.
San Francisco Office of the Medical Examiner The Medical Examiner investigates, and determines cause and manner of death for cases under the Office's legal jurisdiction. During a large MCI, the Medical Examiner’s Office is responsible for identifying and handling corpses and body parts, and responsible for the decedent’s personal effects.
SECTION 3.6 INTERAGENCIES COORDINATION 3.6.1 Scene Organization NIMS and SEMS are based on the Incident Command System (ICS) and are used to provide the basic organizational structure for all incident operations including MCI field operations. ICS is designed to coordinate the efforts of all involved agencies at the scene of a large, complex, emergency situation, as well as the small day‐to‐day situation. The organizational structure of ICS may be expanded in a modular fashion based upon the changing conditions and/or size/scope of the incident. ICS has been summarized as a "first‐on‐scene" structure, where the first responder to arrive on a scene assumes command until the incident is resolved or there is a formal transfer of command to a more‐qualified individual arriving later. The essential elements of ICS are:
• Command: Overall management and setting of objectives for the response. • Operations: Direct control of tactical operations and the implementation of response
objectives.
17

• Planning: Development of a plan for response operations. • Logistics: Coordinates acquisition and distribution of resources. • Finance: Purchases resources. Records what resources were involved in the response for
purposes of reimbursement. 3.6.2 Field Command‐ Single vs. Unified The Incident Commander is responsible for the overall management and setting of objectives for the incident response. Depending on the size and duration of the MCI, the Incident Commander may directly supervise operations or delegate this responsibility to an Operations Section Chief. EMS Multi‐Casualty Field Operations are within the responsibility of the Operations Section. Single Command Most incidents involve a single Incident Commander. In these incidents, a single person commands the incident response and is the final authority for decision‐making. A single incident commander is chosen when a single agency has responsibility for an incident. The Incident Commander is usually the individual first on scene representing the public safety agency having primary investigative authority. There may be exceptions to this rule, based the characteristics of the incident. In San Francisco, the following are examples for when a single command may be implemented. Any of these scenarios may evolve from a Single Command into a Unified Command.
• San Francisco Fire Department – All fires and rescues. The fire department is usually in charge of incident site EMS and rescue functions, even during incidents where other agencies are the incident commander because of their investigative responsibility.
• San Francisco Police Department – All crime related incidents, civil disorders, and most
mass gatherings and pre‐identified events. • San Francisco Department of Public Health – Contagious diseases and other public
health emergencies.
• California Highway Patrol – Accidents or incidents on all freeways, including right of way.
• US Military/Department of Defense ‐ National Defense Area; a military reservation or an
area with "military reservation status" that is temporarily under military control, e.g., military aircraft crash site.
• FBI – Terrorist incidents. FBI is in charge of investigation and may direct response
operations. However, most consequence management functions will continue to be managed by local agencies, such as police and fire.
18

• US Secret Service/US Department of Homeland Security – Designated National Special
Security Events Unified Command Unified Command is used for larger incidents usually when multiple agencies are involved. A Unified Command functions as a single entity. Unified Command typically includes a command representative from the involved agencies with one person from that group designated to act as the group spokesperson, and not as an Incident Commander. Unified Command is used anytime an incident crosses jurisdictional boundaries or exceeds the responsibility of a single agency. Unified Command allows all agencies with responsibility for an incident to establish a common set of incident objectives, strategies, plans, and priorities to jointly execute the incident operations and maximize the use of assigned resources. Most significant incidents in San Francisco will involve unified command, with San Francisco Fire, San Francisco Police, and San Francisco Dept of Public Health fulfilling lead roles. However, any of the above agencies may be involved in Unified Command.
3.6.3 Field Command ‐ Single Site Incidents and Multi‐Site Incidents In Single Site Incidents, all MCI field operations are at one location usually under a single ICS command structure. Multi‐Site Incidents are two or more related or unrelated MCIs regardless of type, occurring simultaneously within a single Operational Area. The size and configuration of the ICS structure and command for a single site or multi‐site incidents depends on various factors such as jurisdictional complexity, size of involved geographic area, span of control, logistical needs and potential for growth. Incident Complexes or Area Command are ICS structures and command for major incidents. An Incident Complex is two or more individual incidents located in the same general proximity assigned to a single Incident Commander or Unified Command to facilitate management. These incidents are typically limited in scope and complexity and can be managed by a single entity. Area Command is NOT used in the San Francisco Emergency Management structure. EMS MCI Field Operations are under the responsibility of the Operations Section. For single‐site incidents that are small, one Operations Section Medical Group will be established. For larger incidents or multi‐site incidents with more than one Operations Section Medical Group, a Medical Branch with several Medical Groups will be established. The Medical Branch structure will provide the IC with a basic expandable system to manage large number of patients during an incident.
19

SECTION 3.7 – INTRACOUNTY DISASTER MEDICAL MANAGEMENT 3.7.1 Departmental Operation Centers and Emergency Operations Centers For large or multi‐site incidents, higher‐level support facilities above the field level may be activated. These facilities provide logistical and administrative support or in some instances, set response priorities and objectives to ensure efficient use of resources. Activated facilities may include either Departmental Operations Centers (DOC) or Emergency Operations Center (EOC) or both. In San Francisco, a DOC is an operational/logistical entity that is designed to serve as departmental or functional coordinating body in direct support of incident management. The role of the DOC encompasses two broad functions: to maintain internal departmental operations (continuity of operations) and, when necessary, to contribute to citywide response through communications and coordination with the EOC. Any of the city department DOCs may be involved in supporting a MCI response, especially in a large‐scale event that covers several operational periods. However, Departments that are most relevant to an initial MCI response are:
• San Francisco Fire Department (SFFD) – Fire DOC • Department of Emergency Management (DEM) ‐ Medical DOC • Department of Public Health Department (DPH) ‐ Public Health DOC
The Emergency Operations Center (EOC) is activated when citywide multi‐agency coordination is needed for an MCI event. The EOC provides:
• A central coordination point for multi‐agency emergency management of the MCI through coordination provided by the Human Services Branch in the Operations Section of the EOC.
• A common location to collect and disseminate information to create a common operating picture of San Francisco’s citywide response activities, and
• Facilitate actions necessary to protect residents and property of San Francisco during a citywide event.
The EOC exchanges information with city DOCs and other governmental and non‐governmental agencies in order to maintain a comprehensive situational analysis. It also serves as San Francisco’s Multi‐Agency Coordination Center (MACC), as described in NIMS, thereby ensuring that all response systems are interconnected and complementary rather than duplicative. The EOC provides space and facilities for the centralized coordination of emergency functions (e.g., emergency operations, communications, damage assessment, public information). It is staffed with specially trained personnel and is equipped with a variety of systems and tools that aid in data collection and sharing, resource allocation, and other critical functions.
20

3.7.2 SFFD and DEM DOCs vs. EOC Human Services Branch Roles during a MCI The SFFD DOC and DEM Medical DOC, and the EOC Human Services Branch play significant roles in the MCI emergency medical response. SFFD DOC:
• (Suppression duties are not addressed in this plan.) • Field support for:
- SFFD paramedic and EMT personnel plus command staff. - Provision of emergency medical care at the scene in addition to rescue and fire
suppression. - Transport of victims to hospitals or other alternate treatment sites.
• Establishment of field response priorities for large, complex or multi‐site MCIs. • Optimize deployment and use of SFFD resources and specialty teams and equipment
including: - Ambulances - Mobile Mass Casualty Unit. - SFFD Hazmat Team. - SFFD Heavy and light rescue Teams. - San Francisco Metropolitan Medical Task Force (MMTF).
• Coordination of in‐coming / out‐going EMS mutual aid with Medical‐Health Operational Area Coordinator at the EOC.
• Tracking and compiling field patient distribution to receiving facilities. • Collection and reporting of field situational and response information to the EOC Fire
Branch.
• Providing initial and regular updating of field casualty count information to the DEM Medical DOC. The DEM Medical DOC is responsible for adding field casualty counts to hospital and other health provider casualty counts to determine the total casualty count for the overall incident. Only the DEM Medical DOC may report the total casualty count for the overall incident to the Medical‐Health Coordinator at the EOC.
DEM Medical DOC:
• Establishment of citywide medical response priorities for large, complex or multi‐site MCIs.
• May assume Patient Distribution Group operations. • Authorization of alternate treatment sites. • Supporting disaster medical operations for all San Francisco hospitals and medical
providers. • Coordinate public health and medical protective measures with DPH. • Receive, track and fulfill requests for medical resources.
21

• Collect and report situational and response information to the EOC Human Services Branch.
• Coordinating in‐coming / out‐going requests for medical mutual aid with Medical‐Health Operational Area Coordinator at the EOC.
• Identifies and resolves competing priorities for medical resources with Medical‐Health Operational Area Coordinator at the EOC in consultation with the Director of Health.
• Obtains initial and regular updates of field casualty count information from the SFFD DOC. DEM Medical DOC is responsible for compiling field casualty counts, hospital and other medical provider casualty counts to determine the total casualty count for the overall incident. Only the DEM Medical DOC may report the TOTAL casualty count for the overall incident to the Medical‐Health Coordinator at the EOC Operations Branch ‐ Human Services Branch.
3.7.3 EOC Operations Section ‐ Human Services Branch Roles during a MCI
• Provides coordination among all mass care, housing, human services, public health, medical services, animal response, and mass fatality departments responding to an event and supports the following during a MCI:
• Provides overall system planning and support and establishment of medical response priorities / objectives for large, complex or multi‐site MCIs (if multiple DOCs are activated).
• Provides operational and logistical support through other City Agencies or mutual aid requests for out‐of‐county resources.
• Collates and reports situational and response information from all activated DOCs for reporting to other local, regional, state and federal government and non‐governmental agencies.
• Approves Medical‐health related public information for the EOC Joint Information Center.
• Collates incident casualty counts from all activated DOCs for reporting to other local, regional, state and federal government and non‐governmental agencies.
3.7.4 DOC AND EOC ACTIVATIONS DURING A MCI
When a MCI is reported, DEC (911) automatically invokes an alert that initiates the start of a Standardized EMS System Order. The number of victims and the necessary resources to manage the incident determines the incident classification and alert level that the DEC sends to EMS providers. The Standardized System Orders lists the necessary notifications and activations.
A Level 1 MCI is handled using only resources internal to San Francisco. A Level 1 MCI Incident is usually handled through a field command, but may require the San Francisco Fire DOC or DEM Medical DOC activation for additional resource coordination. The Citywide EOC would rarely be activated during a Level 1 MCI. DOC activations may be initiated by departmental
22

leadership or at the request of the DEM Director or Deputy Director or DEM Duty Officer if neither is available.
For MCI’s requiring multi‐city agency responses or significant out‐of‐county resources, the EOC will be activated. Any decision to activate the EOC is done in consultation with the DEM Deputy Director or DEM Duty Officer. The City and County of San Francisco Emergency Response Plan describes in further detail the organization and command of the citywide response to large or complex disaster incidents. The same plan is followed for citywide organization and command of large or complex multi‐casualty incidents.
SECTION 3.8 – INTERCOUNTY DISASTER MEDICAL MANAGEMENT: MEDICAL MUTUAL AID Mutual Aid is defined as the voluntary provision of services and facilities by other agencies or organizations to assist each other when existing resources are inadequate or depleted. In California, mutual aid generally refers to aid that comes from outside the Operational Area. Medical Mutual Aid is specific to supplementing / augmenting medical and health resources. Medical mutual aid is defined as the voluntary provision of medical services/equipment and medical facilities by other agencies or organizations to assist each other when existing medical resources are inadequate or depleted. All medical mutual aid requests follow the SEMS and NIMS systems. Medical mutual aid is initiated when the surging of medical resources within San Francisco has been exhausted. It also may be used in medical incidents when it is determined that it may be faster to supplement or augment San Francisco resources from assets from outside the county. For example, San Francisco has several disaster medical field care clinics that may take several hours to set up, supply and staff. Patients would get to medical treatment in less time if they are sent to out‐of‐county medical facilities using the Medical Mutual Aid process. In California, counties are grouped into six Mutual Aid regions by the state California Emergency Management Agency (CalEMA). The Medical‐Health Mutual Aid system uses the same county groupings for its six Mutual Aid regions. San Francisco is in Region 2. Within a region, resources are distributed from the unaffected Operational Area to the affected one. There are three personnel roles that are unique to the Medical Mutual Aid system in California:
Medical Health Operational Area Coordinator (MHOAC) – An individual appointed by a county Department of Health Director / local Health Officer who is responsible for coordinating medical‐health services and resources within the Operational Area (County) in the event of a disaster or major incident where medical mutual aid is required.
23

Regional Disaster Medical Health Coordinator (RDMHC) – The RDMHC is responsible for the coordination of medical and health mutual aid among the operational areas within a California mutual aid region during a disaster or other major event.
Regional Disaster Medical Health Specialist (RDMHS) – The RDMHS is staff to the RDMHC and provides assistance for the coordination of medical and health mutual aid among the operational areas within a California mutual aid region.
During Level 2 or 3 Incident, the Medical‐Health Operational Area Coordinator (MHOAC) coordinates all out‐of‐area medical mutual aid resource requests – whether they are in‐coming or out‐going. The MHOAC is responsible for coordinating disaster medical resources and communicating with the Region 2 ‐ Regional Disaster Medical Health Medical Coordinator (RDMHC) all requests for medical supplies, personnel, and equipment. All requests that have no pre‐agreement go through the MHOAC to the RDMHC. In San Francisco, the MHOAC is the DEM EMS Agency Medical Director, with a DEM EMS Agency physician and a Department of Public Health’s Communicable Disease physician as designated back‐ups. The MHOAC is in the Operations Section – Human Services Branch during activation of the citywide EOC. The Regional Disaster Medical Health Coordinator is based at the Contra Costa County EMS Agency.
The RDMHC will handle resource requests if they are available within their assigned region. If the medical resource needs exceed the response capabilities of the impacted Operational Area and its region, the RDMHC communicates with the state to obtain resources from either non‐adjacent regions or the federal government. State agencies handle communications with federal disaster response organizations. In some instances, State and/or Federal government response agencies may automatically begin forward deployment of resources or provide them through their own supplies channels if there is advance notice of a major event (e.g. hurricanes). Details about state and federal entities involved in a disaster response are found in the California Disaster Medical Operations Manual from the California EMS Authority and the California Disaster Health Operations Manual from the California Department of Public Health. Operational details about the Medical Mutual Aid process are further described in Section 2.12 of this Plan.
24

Annexes (TO BE DEVELOPED)
TRAUMA Bombings and Explosive Incidents Contaminated Scenes
CHEMICAL (HAZMAT) RADIOLOGICAL Treatment protocols for treatment in hot and warm zone Standards for transport of decontaminated victims
Crime Scene Operations
Interaction with Law Enforcement Evidence Control
ENVIRONMENTAL
EXTREME WEATHER BIOLOGICAL
SPECIAL RESPONSES
CASUALTY COLLECTION POINTS FIELD TREATMENT SITES (CALIFORNIA EMS AUTHORITY DEVELOPING GUIDELINES) ALTERNATE CARE SITES (CALIFORNIA DEPT OF PUBLIC HEALTH DEVELOPING GUIDELINES)
25

26

27
Appendices

APPENDIX B: FIELD MEDICAL BRANCH - POSITION DESCRIPTIONS
1. Common Responsibilities for All Field Personnel
2. Medical Branch Director 3. Medical Group Supervisor (MGS) 4. Triage Area:
a. Triage Area Unit Leader b. Triage Personnel c. Morgue Manager
5. Treatment Area:
a. Treatment Area Unit Leader b. Immediate Treatment Area Manager c. Delayed Treatment Area Manager d. Minor Treatment Area Manager e. Treatment Dispatch Manager
6. Transportation Area:
a. Transport Area Unit Leader b. Air Ambulance Coordinator c. Ground Ambulance Coordinator d. Medical Communications Coordinator
7. Medical Supply Coordinator
1

COMMON RESPONSIBILITIES: All Field Personnel
Listed below are the common responsibilities for all field personnel and supervisory staff. ALL personnel must immediately complete these actions upon arrival at the scene. Field Personnel – Immediate Actions
Report for duty and receive assignment position from Incident Commander (IC), Medical Branch Director or Medical Group Supervisor if used.
Don color‐coded MCI Position Vests. Use flashcards, command boards and triage tags to manage incident work and treat patients.
Acquire any necessary work materials. Know your assigned radio frequency and ensure that radios are available and functioning.
Use clear text and ICS terminology in all communications. Maintain activity log (ICS form 214). Respond to orders to escalate response and response actions. Response to order to demobilize or scale back efforts.
Field Supervisory Personnel – Immediate Actions
Complete all immediate actions listed for field personnel above. Assign, organize and brief subordinates. Maintain accountability of assigned personnel as to Assignment Location, personal safety and welfare.
Assure rotation of personnel from high stress or high risk areas. Monitor personnel for signs of stress or fatigue. Request additional resources as needed.
2

Medical Branch Director Reports to: Operations Section Chief or Incident Commander Supervises: Medical Group Supervisor(s) and Transportation function (Unit or Group). Assignment Location: Command Post Talk Group: _________ Radio call sign: Medical Branch Director Skills needed: ALS level EMS professional with management and command experience and knowledge of SEMS, ICS and MCI management policies.
Mission: To implement the Incident Action Plan within the Medical Branch, including the direction and execution of branch planning for the assignment of resources.
Immediate Actions:
Assist the IC in setting strategic goals, establish objectives, setting priorities and assigning specific objective to units or groups.
Act as liaison between the Medical Groups and the Operations Chief and/or Incident Commander
Supervise personnel in the Medical Groups Coordinate activities and response efforts between Medical Groups Reports out casualty information to the Operations Chief.
Ongoing Actions:
Maintain a written record of activities using the Standardized MCI Forms. Monitor conditions within the medical incident for safe practices Coordinate re‐supply efforts with Logistics Coordinate special staffing procedures including call backs and hold over of employees Updates casualty information for the Operations Chief.
3

Medical Group Supervisor Reports to: Incident Commander or Operations Section Chief (may report to Medical Branch Director in larger events) Supervises: Triage, Treatment and Transport Unit Leaders and Medical Supply Coordinator Assignment Location: Command Post Talk Group: _________ Radio call sign: MGS Skills needed: ALS level EMS professional with management and command experience and knowledge of SEMS, ICS and MCI management policies. Mission: To supervise the Unit Leaders and establish command and control of the activities within the Medical Group for effective delivery of emergency medical care during the MCI.
Immediate Actions:
Designate areas for MCI management to include triage and treatment areas, temporary morgue, and medical equipment resources area.
Maintain a written record of al MCI activities using ICS form IC 214 and assist the IC with preparation of IC 201.
Assures that other members of the group have been supplies with the appropriate ICS forms and job actions sheets for their positions.
Monitors conditions with the medical incident for hazards and unsafe practices. Notifies Safety Officer of unsafe or hazardous conditions.
Requests additional resources through the Incident Commander Acts as the liaison between MCI Branch and the Operations Section Chief or IC and gives updates as needed.
Reports out casualty information to the Medical Branch Director.
Ongoing Actions:
Maintain a written record of activities using the Standardized MCI Forms. Monitor conditions within the medical incident for safe practices Coordinate re‐supply efforts with Logistics Coordinate special staffing procedures including call backs and hold over of employees Updates casualty information to the Medical Branch Director. Ensures that there are enough personnel to assist in Medical Group / Branch activities.
4

Triage Area Unit Leader Reports to: Medical Group Supervisor Supervises: Triage Personnel, Litter Bearers and Morgue Manager Assignment Location: Triage Area or base of Triage route Talk Group: _________ Radio call sign: Triage Area Leader Skills needed: EMS professional with experience and training in principles of START and JUMP START triage.
Mission: Supervise and coordinate triage personnel to rapidly identify and triage all MCI patients and assign them to appropriate Treatment Areas.
Immediate Actions:
Designate triage teams. Do systematic sweep through scene to locate and triage casualties. Organize Litter Teams – Comprised or four persons on flat terrain and 6 persons on broken terrain or uneven terrain. Used to evacuate patient or move them between the Medical Group Areas.
Establish route with barrier tape through which casualties are moved. Coordinate patient triage using the START (adults) and JUMP START (pediatric) triage systems.
Maintain written records for patients using triage tags. In a Level 1 MCI, PCRs will be completed on all patients.
Ensure safe practices within the Triage Area including monitoring of adequate decontamination in the event a hazardous materials incident.
Periodically scan the scene for new or overlooked patients. Reassign triage teams to treatment Areas after al victims have been evaluated. Notify Medical Group Supervisor, Treatment Unit Leader when all patients have received initial and secondary triage.
Ongoing Actions:
Monitor patient flow. Provide medical Supply Manger with list of supplies to be replenished Participate in incident planning meetings as directed.
5

Triage Personnel Reports to: Triage Unit Leader Assignment Location: Triage Area Talk Group: _________ Radio call sign: Triage Skills needed: First responders, EMT‐1s, and paramedics with experience in START triage, JUMP START triage and trauma triage criteria. Mission: Triage patients and assign them to appropriate Treatment Areas.
Immediate Actions:
Report to designated on scene triage Assignment Location(s). Using the principles of START and JUMP START, triage and tag injured patients with triage tags affixed to upper extremities.
Classify patients while noting injuries and vital signs taken. Direct movement of patients to appropriate Treatment Areas. Carry non‐ambulatory patients to Treatment Areas. Assist with secondary triage of patients in treatment Areas using Trauma Center triage criteria.
Provide appropriate medical treatment to patients prior to movement as incident conditions allow.
6

Morgue Manager Reports to: Triage Unit Leader Assignment Location: Morgue Area Talk Group: _________ Radio call sign: Morgue Manager Skills needed: First responders or Medical Examiner’s Office Staff. Mission: Responsible for all Morgue Area operations.
Immediate and On‐Going Actions:
Tracks, records and reports out the number of deceased and their names (if known) to Triage Unit Leader.
Assess resource/supply needs and order as needed. Keep area off limits to all but authorized personnel. Coordinate with law enforcement and assist the Coroner or Medical Examiner representative.
Evidence preservation for crime scenes.
7

Treatment Area Unit Leader Reports to: Medical Group Supervisor Supervises: Immediate Treatment Manager, Delayed Treatment Manager, Minor Treatment Manager and Treatment Dispatch Manager Assignment Location: Treatment Area or between Red and Yellow Treatment Areas Talk Group: _________ Radio call sign: Treatment Area Leader Skills needed: EMTs and paramedics with experience in BLS and ALS as appropriate. Mission: Supervise and coordinate Treatment Area Managers to rapidly perform on‐scene medical treatment of victims and preparation / coordination for their transport.
Immediate Actions:
Supervise personnel in the Treatment Area Coordinate all patient care in the Treatment Area Oversee preparations for patient transport Provides supplies for Red, Yellow and Green Treatment Areas. Coordinate the rapid movement of patients from Triage Areas to Treatment Areas. Ensures ongoing triage and reclassification of all patients in Treatment Areas. Redirects Treatment Area Managers to perform secondary triage of patients using the Trauma Triage categories.
Ensures patients are “packaged” for transport. Coordinates the movement of patients to Transportation Area. Maintain written records of patients using triage tags and Treatment Areas Status Boards.
Ongoing Actions:
Requests additional staffing and resources through the Medical Group Supervisor.
8

Immediate Treatment Manager Reports to: Treatment Unit Leader Assignment Location: Immediate Treatment Area Talk Group: _________ Radio call sign: as assigned Skills needed: EMTs and paramedics with experience in BLS and ALS as appropriate. Mission: Supervises treatment and re‐triage of patients assigned to Immediate Treatment Area.
Immediate Actions:
Establish medical teams as necessary; request personnel from Treatment Unit Leader Assign treatment personnel to patients received in the Immediate Treatment Area Perform secondary triage of patients. Ensure that patients are prioritized for transportation. Ensures patients are “packaged” for transport. Coordinate transportation of patients with the Transport Unit Leader Notify Treatment Unit Leader of patient readiness and priority for transport. Assure that treatment is documented and patient information is recorded on triage tags and patient status boards.
Ongoing Actions:
Request additional resources and personnel as needed.
9

Delayed Treatment Manager Reports to: Treatment Unit Leader Assignment Location: Delayed Treatment Area Talk Group: _________ Radio call sign: as assigned Skills needed: EMTs and paramedics with experience in BLS and ALS as appropriate. Mission: Supervises treatment and re‐triage of patients assigned to Delayed Treatment Area.
Immediate Actions:
Establish medical teams as necessary; request personnel from Treatment Unit Leader. Assign treatment personnel to patients received in the Delayed Treatment Area Perform secondary triage of patients. Ensure that patients are prioritized for transportation. Ensures patients are “packaged” for transport. Coordinate transportation of patients with the Transport Unit Leader. Notify Treatment Unit Leader of patient readiness and priority for transport. Assure that treatment is documented and patient information is recorded on triage tags and patient status boards.
Ongoing Actions:
Request additional resources and personnel as needed.
10

Minor Treatment Manager Reports to: Treatment Unit Leader Assignment Location: Treatment Area Talk Group: _________ Radio call sign: as assigned Skills needed: EMTs and paramedics with experience in BLS and ALS as appropriate. Mission: Supervises treatment and re‐triage of patients assigned to Minor Treatment Area.
Immediate Actions:
Establish medical teams as necessary; request personnel from Treatment Unit Leader Assign treatment personnel to patients received in the Minor Treatment Area Perform secondary triage of patients. Ensure that patients are prioritized for transportation Coordinate transportation of patients with the Transport Unit Leader Ensures patients are “packaged” for transport. Notify Treatment Unit Leader of patient readiness and priority for transport. Assure that treatment is documented and patient information is recorded on triage tags and patient status boards.
Ongoing Actions:
Request additional resources and personnel as needed
11

Treatment Dispatch Manager Reports to: Treatment Unit Leader Assignment Location: Treatment Area or between Immediate, Delayed and Minor Treatment Areas Talk Group: _________ Radio call sign: Treatment Dispatch Manger Skills needed: EMTs and paramedics with experience in BLS and ALS as appropriate. Mission: Coordinates movement of patients from Treatment Area to Transport Area with Patient Transportation Unit Leader usually through their Medical Communications Coordinator.
Immediate Actions:
Establish communications with the Immediate, Delayed, and Minor Treatment Managers. Establish communications with the Patient Transportation Unit Leader. Verify that patients are prioritized for transportation. Verify that patients are “packaged” and ready for transport. Advise Medical Communications Coordinator (located in Patient Transport Unit) of patient readiness and priority for transport.
Coordinate transportation of patients with Medical Communications Coordinator (located in Patient Transport Unit).
Assure that appropriate patient tracking information is recorded. Coordinate ambulance loading with the Treatment Managers and ambulance personnel. Maintain Unit/Activity Log (ICS Form 214)
12

Patient Transportation Area Unit Leader Reports to: Medical Group Supervisor Supervises: Ground Ambulance Coordinator, Air Ambulance Coordinator and Medical Communications Coordinator Assignment Location: Transport Corridor Talk Group: _________ Radio call sign: Patient Transport Area Leader Skills needed: EMTs and paramedics with experience in BLS and ALS as appropriate. Knowledge of hospital destination criteria. Mission: Oversees the coordination of patient transport vehicles and hospital destinations.
Immediate Actions:
Determine and maintain access and egress routes for patients and transporting units Coordinate movement of patients to transportation Area with Treatment Unit Leader Coordinate ambulance flow through Transport Area. Oversee assignment of sufficient personnel to bear litters. Utilize destination schematics for patient movement. Review available trauma center and hospital resources. Determine need for transport to regional trauma centers; notify MGS if indicated.
Ensure that trauma triage criteria are utilized in determining patient movement to trauma center(s).
Coordinate destination decisions with the Patient Distribution Group. Ensure that patients in different triage categories are not mixed together in transport vehicles (ex: do not mix red and green patients in same ambulance).
On‐Going Actions:
Maintain Unit/Activity Log (ICS Form 214) Request additional resources through Patient Transport Area Unit Leader or Medical Supply Coordinator if used.
At his / her discretion, may add additional positions in Patient Transportation Unit to coordinate transportation to out‐of‐county destinations.
13

Ground AmbulanceCoordinator Reports to: Patient Transportation Unit Leader Assignment Location: Transport Corridor Talk Group: _________ Radio call sign: Ground Ambulance Coordinator Skills needed: Knowledge of hospital Assignment Locations and destination criteria. Mission: Coordinates ground ambulances or other ground‐based patient transportation vehicles. Manages the Ambulance Staging Area(s). Dispatches ambulances as requested.
Immediate Actions:
Establishes access and egress routes for ground ambulances. Establish appropriate staging area(s) for ambulances. Establish and maintain communications with the Medical Communications Coordinator and Treatment Dispatch Manager.
Establish and maintain check‐in procedures for new arrivals. Provide ambulances upon request from the Medical Communications Coordinator. Request additional transportation resources as appropriate.
On‐Going Actions:
Maintain Transport Worksheet of patient transports that includes: 1. Triage tag number 2. Triage Level 3. Patient name (if known) 4. Patient Age and Gender 5. Type of transport unit 6. Name of transport unit provider 7. Transport unit provider unit number 8. Destination 9. Time of departure 10. ETA
Assure that necessary equipment is available for patient needs during transportation. Request additional resources through Patient Transport Area Unit Leader or Medical Supply Coordinator if used.
14

Air Ambulance Coordinator Reports to: Patient Transportation Unit Leader Assignment Location: Transport Corridor Talk Group: _________ Radio call sign: Ambulance Coordinator Skills needed: Knowledge of hospital Assignment Locations and destination criteria. Mission: Establishes and coordinates helispots and air medical operations with the Air Operations Group.
Immediate Actions:
Establish appropriate helispots for air ambulances. Establish routes of travel for air ambulances for incident operations. Establish and maintain communications with the Air Operations Branch Director regarding Air Ambulance Transportation Assignments.
Establish and maintain communications with the Medical Communications Coordinator and Treatment Dispatch Manager.
Establish and maintain check‐in procedures for new arrivals. Provide air ambulances upon request from the Medical Communications Coordinator. Coordinate ground ambulance transport of patients to helispots.
On‐Going Actions:
Maintain Transport Worksheet of patient transports that includes: 1. Triage tag number 2. Triage Level 3. Patient name (if known) 4. Patient Age and Gender 5. Type of transport unit 6. Name of transport unit provider 7. Transport unit provider unit number 8. Destination 9. Time of departure 10. ETA
Assure that necessary equipment is available for patient needs during transportation. Request additional resources through Patient Transport Area Unit Leader or Medical Supply Coordinator if used.
15

Medical Communications Coordinator Reports to: Patient Transportation Unit Leader Assignment Location: Transport Corridor Talk Group: _________ Radio call sign: Medical Communications Coordinator Skills needed: EMTs and paramedics with experience in BLS and ALS as appropriate. Knowledge of hospital destination criteria. Mission: Maintains medical communications with the Patient Distribution Group for assignment of hospital destinations for MCI patients. Selects the mode of medical transport based upon patient need using patient condition information provided by the Treatment Dispatch Manager.
Immediate Actions:
Receives basic patient information and condition from Treatment Dispatch Manager. Contacts the Patient Distribution Group to obtain the name and contact information for the Patient Distribution Unit Leader.
Reports to the Patient Distribution Unit Leader, the number of MCI patients, their triage levels and triage tag numbers.
Obtains from the Patient Distribution Unit Leader, the assigned receiving facility for each patient.
Confirms assigned facilities, (“This is Medical Communications Coordinator at Transport Area – I copy to take 2 Green patients with Triage Tag numbers 6293 and 6456 to Kaiser Hospital. Is the correct?”).
Advises the Patient Distribution Unit Leader of any remaining field MCI patients awaiting disposition.
Communicates ground transportation requests to Ground Ambulance Coordinators. Communicates air ambulance requests to the Air Operations Branch Director or Air Ambulance Coordinator.
16
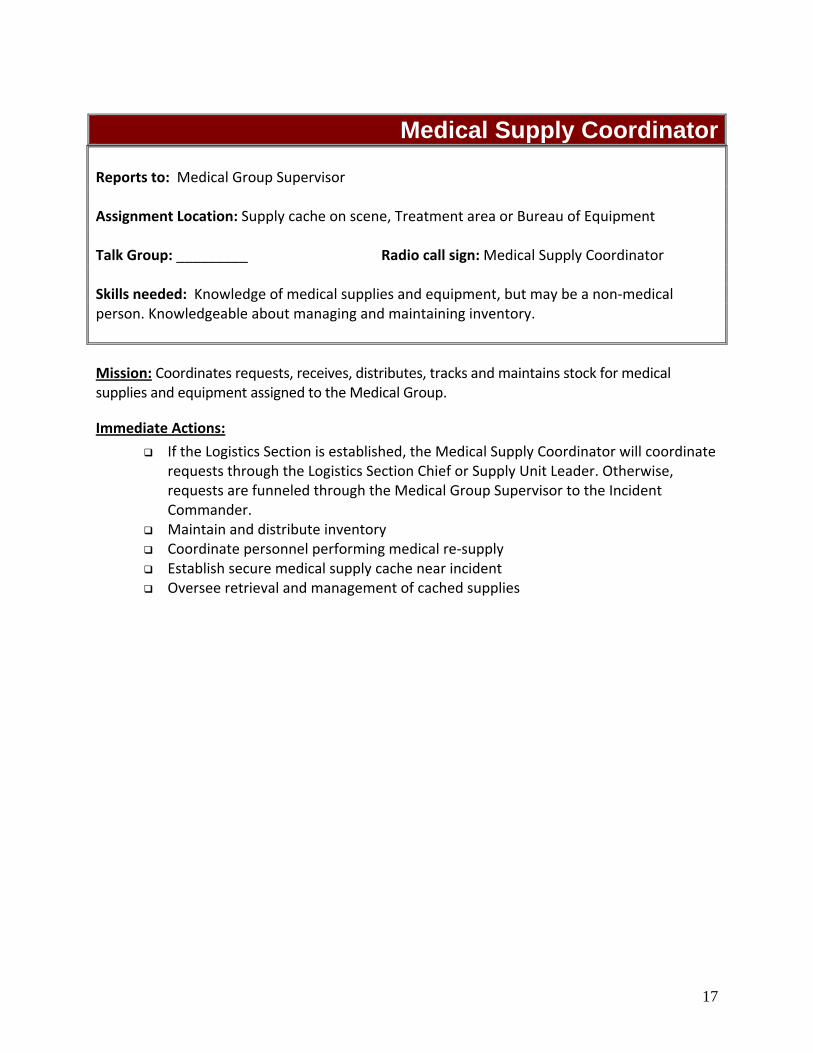
17
Medical Supply Coordinator Reports to: Medical Group Supervisor Assignment Location: Supply cache on scene, Treatment area or Bureau of Equipment Talk Group: _________ Radio call sign: Medical Supply Coordinator Skills needed: Knowledge of medical supplies and equipment, but may be a non‐medical person. Knowledgeable about managing and maintaining inventory. Mission: Coordinates requests, receives, distributes, tracks and maintains stock for medical supplies and equipment assigned to the Medical Group.
Immediate Actions:
If the Logistics Section is established, the Medical Supply Coordinator will coordinate requests through the Logistics Section Chief or Supply Unit Leader. Otherwise, requests are funneled through the Medical Group Supervisor to the Incident Commander.
Maintain and distribute inventory Coordinate personnel performing medical re‐supply Establish secure medical supply cache near incident Oversee retrieval and management of cached supplies

18

APPENDIX C: PATIENT DISTRIBUTION GROUP -
POSITION DESCRIPTIONS
1. Patient Distribution Group Branch Director
2. Patient Distribution Group Supervisor
3. Receiving Unit Leader
4. Patient Unit Leader
19

Patient Distribution Group Branch Director Report to: Operations Section Chief or Incident Commander Supervise: Patient Distribution Group Supervisor(s) Assignment Location: DEC or Medical DOC Talk Group: _________ Radio call sign: Patient Distribution Group Branch Director Skills needed: Knowledge of local EMS system, supervisory experience and knowledge of SEMS, ICS and MCI management policies
Mission: Has overall command of Patient Distribution Group operations in a full branch response. Reports patient distribution information to the Operations Section Chief.
Immediate Actions:
Assist the IC in setting strategic goals, establish objectives, setting priorities and assigning specific objective to units or groups.
Act as liaison between the Patient Distribution Groups and the Operations Chief and/or Incident Commander
Supervise personnel in the Patient Distribution Groups Coordinate activities and response efforts between Patient Distribution Groups Reports patient distribution information to the Operations Chief.
Ongoing Actions:
Maintain a written record of activities using the Standardized MCI Forms. Monitor conditions within the medical incident for safe practices Coordinate re‐supply efforts with Logistics Coordinate special staffing procedures including call backs and hold over of employees Updates patient distribution information for the Operations Chief.
20

Patient Distribution Group Supervisor Report to: Branch Director or Operations Section Chief or Incident Commander Supervise: Patient Distribution Unit Leader, Receiving Unit Leader and support staff (if used). Assignment Location: DEC or Medical DOC Talk Group: _________ Radio call sign: none Skills needed: Knowledge of local EMS system, supervisory experience and knowledge of SEMS, ICS and MCI management policies Mission: Supervisory role for the Patient Distribution Group operations. Oversee activities of the Patient Distribution Unit Leader and Receiving Unit Leader. Liaison to other ICS sections or groups and to all external parties and agencies except field responders and receiving facilities.
Immediate Actions:
Assigns Patient Distribution Unit Leader and Receiving Unit Leader roles. Supports or assigns additional staff as needed to assist Patient Distribution Unit Leader and Receiving Unit Leader.
Notifies DEM Duty Officer and Medical‐Health Operations Coordinator (MHOAC) about MCI incident. May notify the Region 2 Regional Medical‐Health Operations Coordinator (RDMHC) about MCI incident if the DEM Duty Officer or MHOAC are not available.
Request Mutual Aid through the Medical‐Health Operations Coordinator (MHOAC) at the EOC when Receiving Unit Leader identifies that all San Francisco hospitals are near or at capacity.
Works with MHOAC during Mutual Aid situations to match patients with available beds either in San Francisco or out‐of‐county.
Resolves questions or issues about patient bed assignments except for those involving clinical decisions. (Clinical questions about patient bed assignments are resolved between the Medical Communications Coordinator located at the Field Patient Transport Area and the Base Hospital located at San Francisco General Hospital.)
Ongoing Actions:
Maintains a written log of activities. Monitors workload conditions for safe practices. Coordinates on‐going staffing including call backs and hold over of employees as needed.
Completes final summary of Patient Distribution Group activities.
21

Receiving Unit Leader Report to: Patient Distribution Group Supervisor Supervise: Any assigned support staff (if used). Assignment Location: DEC or Medical DOC Talk Group: _________ Radio call sign: Receiving Unit Leader Skills needed: Knowledge of local EMS system and knowledge of SEMS, ICS and MCI management policies. Proficient in the use of EM System, 800 MHz Radio and Hearnet Radio. Mission: Coordinates beds and patient assignments with all receiving facilities.
Immediate Actions:
Creates MCI event in EMSystems to alert and poll all EMS providers. Polls hospitals to determine the number of available hospital beds. Tabulates the results of the hospital bed polls, prioritizes the first receiving facilities and provides that information to the Patient Unit Leader.
Notifies hospitals about their assigned patients (e.g. “Kaiser ‐ you will receive 2 green patients with triage tag numbers 6293 and 6456”).
Re‐polls hospitals every 15 minutes or as needed until all MCI patients receive a disposition.
Notifies the Patient Distribution Supervisor and Patient Unit Leader when hospitals are near or at capacity.
Works with Patient Distribution Group Supervisor and MHOAC during Mutual Aid situations to match patients with available beds out‐of‐county beds or in‐county beds if receiving patients.
Ongoing Actions:
Documents available hospital bed types. Request back‐up assistance for workload as needed. Provides regular status updates about the MCI to receiving facilities.
22

Patient Distribution Unit Leader Report to: Patient Distribution Group Supervisor Supervise: Any assigned support staff (if used). Assignment Location: DEC or Medical DOC Talk Group: _________ Radio call sign: Patient Distribution Unit Leader Skills needed: Knowledge of local EMS system and knowledge of SEMS, ICS and MCI management policies
Mission: Coordinates hospital assignments for MCI patients with the Patient Transport Area Unit Leader or Medical Communications Coordinator located at the Field Patient Transport Area.
Immediate Actions:
Establishes and maintains contact with Patient Transport Area Unit Leader or Medical Communications Coordinator about MCI patients needing a hospital disposition.
Obtains from the Receiving Unit Leader, the tabulated available hospital beds. Matches available hospital beds with the MCI patients remaining on scene.
Notifies the field Medical Communications Coordinator about the bed assignment (e.g. “Medical Communications Coordinator at Transport Area – take 2 Green patients with Triage Tag numbers 6293 and 6456 to Kaiser Hospital”).
Advises the Medical Communications Coordinator to hold patients at scene to hold patients at scene when hospitals are at capacity until out‐of‐county Mutual Aid beds are identified.
Ongoing Actions:
Documents patient assignments. Request back‐up assistance for workload as needed. Clinical questions about patient bed assignments will be resolved between the Medical Communications Coordinator located at the Field Patient Transport Area and the Base Hospital located at San Francisco General Hospital.
Other questions or issues about patient bed assignments will be resolved by the Distribution Center Supervisor.
23
APPENDIX D: MCI FIELD BOARDS
Not Included for June EMSAC meeting
24
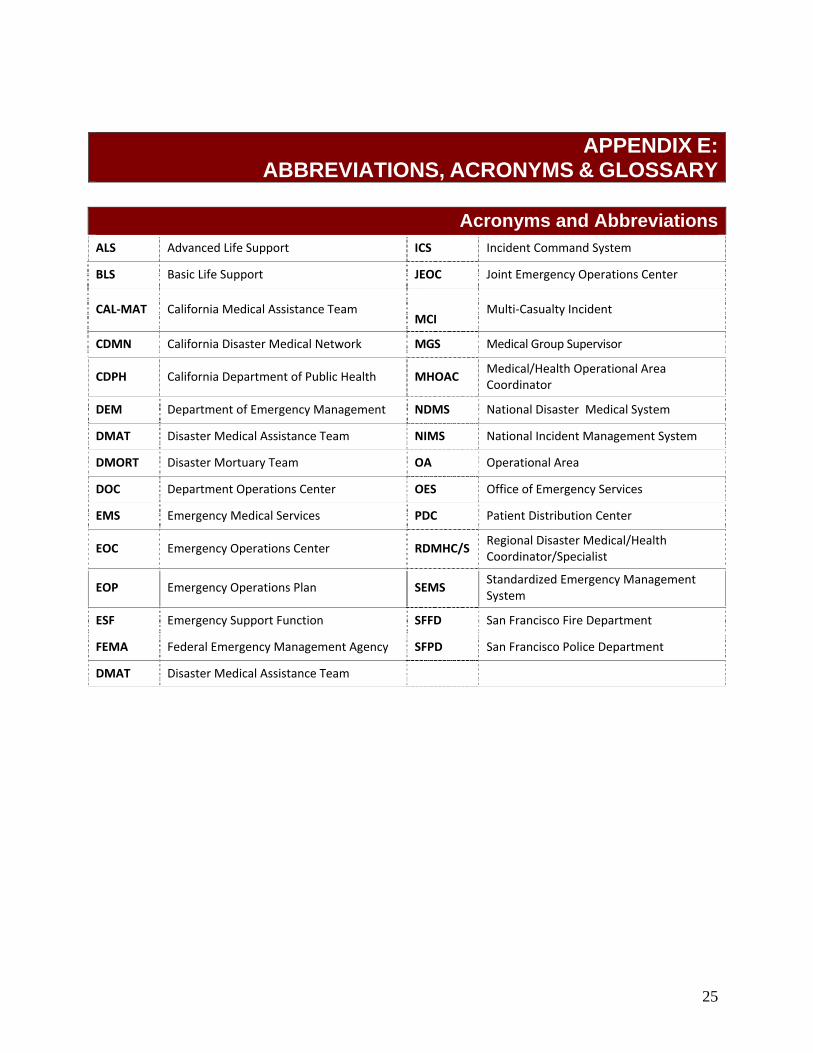
25
APPENDIX E: ABBREVIATIONS, ACRONYMS & GLOSSARY
Acronyms and Abbreviations
ALS Advanced Life Support ICS Incident Command System
BLS Basic Life Support JEOC Joint Emergency Operations Center
CAL‐MAT California Medical Assistance Team MCI
Multi‐Casualty Incident
CDMN California Disaster Medical Network MGS Medical Group Supervisor
CDPH California Department of Public Health MHOAC Medical/Health Operational Area Coordinator
DEM Department of Emergency Management NDMS National Disaster Medical System
DMAT Disaster Medical Assistance Team NIMS National Incident Management System
DMORT Disaster Mortuary Team OA Operational Area
DOC Department Operations Center OES Office of Emergency Services
EMS Emergency Medical Services PDC Patient Distribution Center
EOC Emergency Operations Center RDMHC/S Regional Disaster Medical/Health Coordinator/Specialist
EOP Emergency Operations Plan SEMS Standardized Emergency Management System
ESF Emergency Support Function SFFD San Francisco Fire Department
FEMA Federal Emergency Management Agency SFPD San Francisco Police Department
DMAT Disaster Medical Assistance Team
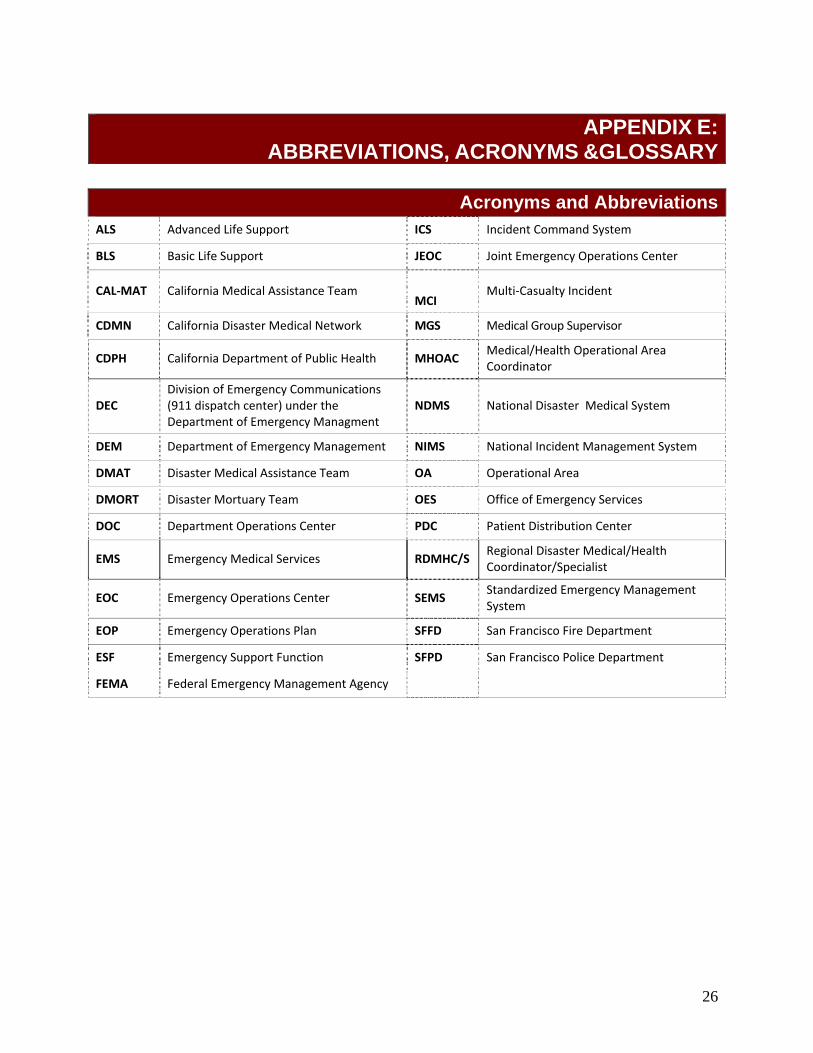
APPENDIX E:
ABBREVIATIONS, ACRONYMS &GLOSSARY
Acronyms and AbbreviationsALS Advanced Life Support ICS Incident Command System
BLS Basic Life Support JEOC Joint Emergency Operations Center
CAL‐MAT California Medical Assistance Team MCI
Multi‐Casualty Incident
CDMN California Disaster Medical Network MGS Medical Group Supervisor
CDPH California Department of Public Health MHOAC Medical/Health Operational Area Coordinator
DEC Division of Emergency Communications (911 dispatch center) under the Department of Emergency Managment
NDMS National Disaster Medical System
DEM Department of Emergency Management NIMS National Incident Management System
DMAT Disaster Medical Assistance Team OA Operational Area
DMORT Disaster Mortuary Team OES Office of Emergency Services
DOC Department Operations Center PDC Patient Distribution Center
EMS Emergency Medical Services RDMHC/S Regional Disaster Medical/Health Coordinator/Specialist
EOC Emergency Operations Center SEMS Standardized Emergency Management System
EOP Emergency Operations Plan SFFD San Francisco Fire Department
ESF Emergency Support Function SFPD San Francisco Police Department
FEMA Federal Emergency Management Agency
26

Glossary Advisory Informational bulletin with no immediate action required.
ALS (Advanced Life Support) Skills and knowledge that a practitioner possesses for performing advanced procedures and skills on a patient involving invasive and non‐invasive procedures. These include:
• AHA Advanced Cardiac Life Support (ACLS) protocols • AHA Pediatric Advanced Life Support (PALS) protocols • Pre‐Hospital Trauma Life Support (PHTLS) protocols
ALS Responder Licensed and locally accredited Paramedic.
Alert Informational bulletin that requires immediate action.
Ambulance Strike Team
A team of five properly staffed and equipped medical transport vehicles of the same capabilities with like communications equipment and one team leader with vehicle and like communications equipment. In California’s, Ambulance Strike Teams consist of five ambulances (an approved vehicle with two personnel) with common communications and a leader and are typed according to FEMA typing for medical and health resources. Each may include a Disaster Medical Support Unit or comparable local support unit to serve as an operational command, control, and communications center. A Mission Support Teams will provide administrative, logistical, and liaison support to dispatched Ambulance Strike Teams.
Alternate Care Sites Used by public health departments or hospitals for as a temporary patient overflow area when healthcare facilities are overwhelmed. ACS are appropriate only for low acuity or end‐of‐life patients. May be used to cohort infectious disease patients.
Area Command (Unified Area Command)
An ICS organization established (1) to oversee the management of multiple incidents when each is being handled by a separate ICS command or (2) to oversee the management of large or multiple incidents to which several Incident Management Teams have been assigned.
Austere Medical Care Refers to an authorized, reduced intensity of care delivered to a patient during a disaster or other situation of duress.
Auxiliary Communications System
Amateur Radio System used in the event that local EMS radio system, and telephone systems are unavailable.
27

BLS (Basic Life Support) Basic non‐invasive first‐aid procedures and techniques utilized by paramedics, EMTs and First Responder personnel to stabilize critically sick and injured patient(s).
BLS Responder Certified EMT‐I or First Responder.
California Disaster Medical Network
A web‐based network for developing and regularly updating situation status reports; requesting, mobilizing, and tracking the status of medical resources; and distributing patients during moderate, major, and catastrophic Incidents. The California Emergency Medical Services Authority is developing this network.
Casualty Distribution Points
Sites established at airports near impacted Operational Areas to gather and stage victims for long‐range evacuation by air to unaffected areas. These sites may be staffed by CAL‐MATs or DMATs.
Casualty Receiving Points
Sites established at airports in unaffected areas to receive victims evacuated by air and distribute them to local hospitals.
Delayed Treatment Patients with injuries are not immediately life threatening who can wait up to several hours for definitive medical care or surgical intervention.
Department of Emergency Management (DEM)
DEM provides various emergency management functions and consists of two divisions: Division of Emergency Communications (DEC) and the Division of Emergency Services (DES). DEC is the 911 dispatch center. DES is responsible for citywide disaster planning and response. The Emergency Medical Services Agency is under DES.
EMT I (Emergency Medical Technician)
An individual trained in Basic Life Support according to the standards prescribed by the Health and Safety Code and who has a current and valid EMT‐I certificate in the State of California issued pursuant to the Health and Safety Code.
EMT II (Emergency Medical Technician II)
An individual with additional training in limited Advanced Life Support according to the standards prescribed by the Health and Safety Code and who has a current and valid certificate issued pursuant to the Health and Safety Code.
Emergency Operations Center (EOC)
The physical location at which civil jurisdictions coordinate information and resources to support incident management (on‐scene operations). An EOC may be a temporary facility or permanently established in a fixed facility.
28

Field Treatment Site Used by EMS for the congregation, triage temporary care, holding and evacuation of injured patients in a multiple or mass casualty situation. A Field Treatment site operates for brief periods of time (e.g. 48 hours) or until new patients no longer arrives at the site.
First Responder Personnel who have responsibility to initially respond to emergencies such as firefighters, police officers, California Highway Patrol Officers, lifeguards, forestry personnel, ambulance attendants and other public service personnel. California law requires such persons to have completed a first‐aid course and to be trained in cardiopulmonary resuscitation.
Immediate Treatment Patients with life threatening injuries that require immediate definitive medical or surgical intervention.
Incident Command System (ICS)
Standardized, on‐scene, all‐hazard incident management concept designed to allow diverse emergency management agencies to work together by providing a flexible, and scalable response organization framework.
Mass Casualty Incident A disaster that results in a large number of casualties that overwhelm available emergency medical services, facilities, and resources.
Medical Health Operational Area Coordinator (MHOAC)
An individual designated by the local Health Officer and EMS Agency Administrator who implements the Operational Area’s disaster medical/health response plan, coordinates the Medical/Health Branch of the Operational Area EOC, coordinates developing mutual aid requests for external resources and the response to external requests, and facilitates the establishment of priorities.
Minor Treatment Ambulatory patients with injuries that only require first‐aid treatment.
Multi‐Casualty Incident (MCI) A medical incident that results in multiple casualties. (A smaller incident than a Mass Casualty Event.)
29
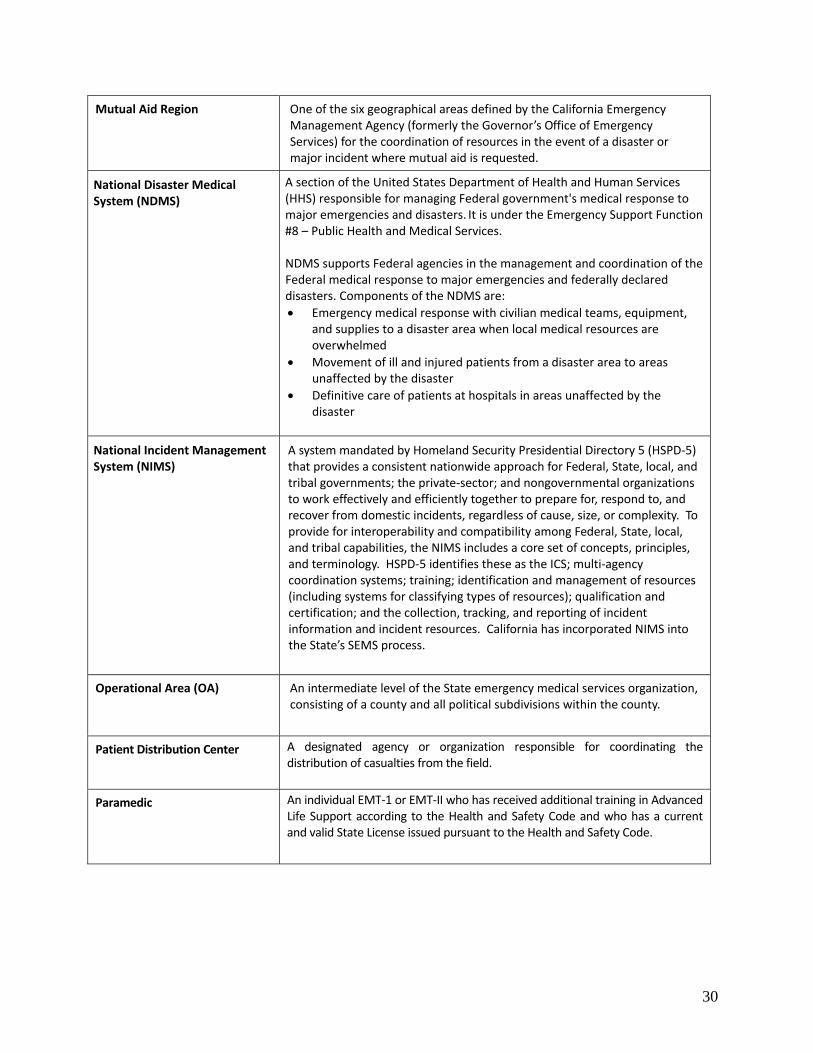
Mutual Aid Region One of the six geographical areas defined by the California Emergency Management Agency (formerly the Governor’s Office of Emergency Services) for the coordination of resources in the event of a disaster or major incident where mutual aid is requested.
National Disaster Medical System (NDMS)
A section of the United States Department of Health and Human Services(HHS) responsible for managing Federal government's medical response to major emergencies and disasters. It is under the Emergency Support Function #8 – Public Health and Medical Services. NDMS supports Federal agencies in the management and coordination of the Federal medical response to major emergencies and federally declared disasters. Components of the NDMS are:
• Emergency medical response with civilian medical teams, equipment, and supplies to a disaster area when local medical resources are overwhelmed
• Movement of ill and injured patients from a disaster area to areas unaffected by the disaster
• Definitive care of patients at hospitals in areas unaffected by the disaster
National Incident Management System (NIMS)
A system mandated by Homeland Security Presidential Directory 5 (HSPD‐5) that provides a consistent nationwide approach for Federal, State, local, and tribal governments; the private‐sector; and nongovernmental organizations to work effectively and efficiently together to prepare for, respond to, and recover from domestic incidents, regardless of cause, size, or complexity. To provide for interoperability and compatibility among Federal, State, local, and tribal capabilities, the NIMS includes a core set of concepts, principles, and terminology. HSPD‐5 identifies these as the ICS; multi‐agency coordination systems; training; identification and management of resources (including systems for classifying types of resources); qualification and certification; and the collection, tracking, and reporting of incident information and incident resources. California has incorporated NIMS into the State’s SEMS process.
Operational Area (OA) An intermediate level of the State emergency medical services organization, consisting of a county and all political subdivisions within the county.
Patient Distribution Center A designated agency or organization responsible for coordinating the distribution of casualties from the field.
Paramedic An individual EMT‐1 or EMT‐II who has received additional training in Advanced Life Support according to the Health and Safety Code and who has a current and valid State License issued pursuant to the Health and Safety Code.
30

Regional Disaster Medical and Health Coordinator (RDMHC)
At the regional level, EMS Authority and CDPH jointly appoint the Regional Disaster Medical Health Coordinator (RDMHC) whose responsibilities include supporting the mutual aid requests of MHOACs for disaster response within the region and providing mutual aid support to other areas of the state in support of the state medical response system. The RDMHC also serves as an information source to the state medical and health response system.
Regional Disaster Medical Health Specialist (RDMHS)
The RDMHS provides the day‐to‐day planning and coordination of medical and health disaster response in the six mutual aid regions. During disaster response, the RDMHS may be designated by the RDMHC as the key contact for OAs to request and/or to provide medical and health resources.
Regional Emergency Operations Center (REOC)
The first level facility of the Governor’s Office of Emergency Services to manage a disaster. The REOC provides an emergency support staff operating from a fixed facility, which are responsive to the needs of the Operational Areas and coordinates with the State Operational Center.
Simple Triage And Rapid Treatment
Usually called START. Initial triage system that has been adopted for use by the California Fire Chiefs' Association.
Strategic National Stockpile Push Packages (SNS)
Push packages are an asset of the CDC’s Strategic National Stockpile program. While their locations are not publicized, the system is designed to deliver part or all of a package to any location in the U.S. within 12 hours of an approved request. Push packages include large quantities of pharmaceuticals, IV solutions, medical supplies, equipment and other assets to treat mass casualties from a wide variety of incidents.
Standardized Emergency Management System (SEMS)
The emergency management system identified in the California Government Code 8607, for managing emergency response to multi‐agency or multi‐jurisdictional operations. SEMS is based on the ICS and is intended to standardize response to emergencies in the State.
Triage The screening and classification of sick, wounded, or injured persons to determine priority needs in order to ensure the efficient use of medical manpower, equipment, and facilities.
E:
31

VIATIONS, ACRONARY APPENDIX E: ABBREVIATIONS, ACRONYMS &
Appendix F: Map of California Mutual Aid Regions
GLOSSARY
32