
MSc Biomedical Basis of Disease. Pain Theory for...
46
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015 1 Pain Theory for Therapists Introducing the Biopsychosocial Model by Alan P Smith BSc(Hons) MSc DO 2 Alan Smith • Osteopath since obtaining DO in 1994. • MSc Biomedical Basis of Disease. Sheffield Hallam University, 1999. • BSc(Hons) in Physical Science. Leicester University Contact Details [email protected] www.ebmseminars.co.uk 38 Barroon, Castle Donington, Derby DE74 2PE. Tel: 01332 853777 Objectives • To Better Understand Pain Mechanisms • To “Introduce” the Biopsyhcosocial Model • To Learn New Clinical Skills in Treating Patients’ Pain Relevance of Understanding Pain • Most patients will have pain • Pain generates the anxiety that motivates the patient seek help • The better we understand pain the more efficiently we can identify & treat the cause What Is Pain? IASP Definition Pain is "an unpleasant sensory and emotional experience associated with actual or potential tissue damage , or described in terms of such damage.“ Pain motivates us to withdraw from potentially damaging situations, protect a damaged body part while it heals, and avoid those situations in the future. International Association for the Study of Pain 1979 Pain is a Multidimensional Experience Sensory-Discriminitive Intensity, Location, Quality Affective-Motivational Unpleasantness, Suffering, Urge to Escape Cognitive-Evaluative Appraisal, Threat – past experiences, conditioning
Transcript of MSc Biomedical Basis of Disease. Pain Theory for...
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
1
Pain Theory for Therapists Introducing the Biopsychosocial Model
by Alan P Smith BSc(Hons) MSc DO
2
Alan Smith bull Osteopath since obtaining DO in 1994
bull MSc Biomedical Basis of Disease
Sheffield Hallam University 1999
bull BSc(Hons) in Physical Science
Leicester University
Contact Details
alan_smith_ostyahoocouk
wwwebmseminarscouk
38 Barroon Castle Donington Derby DE74 2PE Tel 01332 853777
Objectives
bull To Better Understand Pain Mechanisms
bull To ldquoIntroducerdquo the Biopsyhcosocial Model
bull To Learn New Clinical Skills in Treating Patientsrsquo Pain
bull To Earn More Money
Relevance of Understanding Pain
bull Most patients will have pain
bull Pain generates the anxiety that
motivates the patient seek help
bull The better we understand pain the more efficiently we can identify amp treat the cause
What Is Pain IASP Definition
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue
damage or described in terms of such damageldquo
Pain motivates us to withdraw from potentially damaging situations protect a damaged body part while it heals and
avoid those situations in the future
International Association for the Study of Pain 1979
Pain is a Multidimensional Experience
Sensory-Discriminitive Intensity Location Quality
Affective-Motivational Unpleasantness Suffering Urge to Escape
Cognitive-Evaluative Appraisal Threat ndash past experiences conditioning
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
2
Pain intensity (the sensory discriminative dimension) and unpleasantness (the affective-motivational dimension) are not simply
determined by the magnitude of the painful stimulus but higher cognitive activities can influence perceived intensity and
unpleasantness
Pain can be treated not only by trying to cut down the sensory input but also by influencing the motivational-affective and
cognitive factors as well
Pain is a Multidimensional Experience
Cognitive activities may affect both sensory and affective experience or they may modify primarily the affective-motivational
dimension
Pain in the Absence of Physical Injury is sometimes referred to as
ldquoPhysiological Painrdquo
It Stops as soon as you Withdraw or ldquoEscaperdquo from the Stimulus
Pain in the Presence of Physical Injury (Pathology) is sometimes referred to as
ldquoPathophysiological Painrdquo
Here the stimulus will have a component from the products of Inflammation and Pain Impulses will Bombard the CNS for some
Considerable Time
Physiological amp Pathophysiological Pain
How Do We Treat PatientsrsquoPain
Find the Tissue Lesion
Treat the Lesioned Tissue - to assist healing
Resolution
This is the Traditional Physical Therapy Approach
Understanding amp Treating Pain
Tissue Injury
Nociceptor Firing
CNS
PAIN
Tissue Injury
Nociceptor Firing
CNS
PAIN
Gate
Anxiety Worry
Uncertainty lsquoThreatrsquo
THERAPY Belief Trust
Reassurance (Distraction)
Rubbing Shaking TENS
PathoanatomicalBiomedical Model (Bottom-up) Biopsychosocial Model (Bottom-up and Top-Down)
Professor Eyal Lederman DO PhD is the director of the Centre for Professional Development in Osteopathy and Manual Therapy London
2010
ldquoThe effectiveness of most medical interventions is derived partially from contextual or nonspecific factors commonly referred to as placebo effects These
effects have demonstrated remarkable potency for the alleviation of pain and under certain circumstances placebos have produced effect sizes
indistinguishable from established medications surgeries and other analgesic treatmentsrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
3
ldquoAlthough the effects of manual therapy are classically explained within a biomechanical paradigm research now points to the important role of
neurophysiological processes at both spinal and supraspinal levels in the modulation of nociceptive informationrdquo hellip ldquoin clinical practice manual therapy
articular mobilizations andor manipulations are seldom being used as an isolated interventionrdquohellip ldquocombining various strategies imparts a synergistic
effect on the brain-orchestrated analgesic systemrdquo
2015 Understanding amp Treating Pain
Tissue Injury
Nociceptor Firing
CNS
PAIN
Gate
Anxiety Worry
Uncertainty lsquoThreatrsquo
THERAPY Belief Trust
Reassurance (Distraction)
Rubbing Shaking TENS
Biopsychosocial Model (Bottom-up and Top-Down)
Targets for Treating Pain
1) Tissues Traditional Modalities 2) Gate Non-specific (lsquoplaceborsquo) 3) Consciousness Distraction
ldquoCognitive distraction could be mediated mainly by direct frontal-corticol somatosensory interactions without the engagement of brainstem pain-
control systemsrdquo ldquoPlacebo analgesia does not depend on active redirection of attention and that expectancy and distraction can be combined to maximize
pain reliefrdquo
2012
C Stimulus
Pain is Generated in the Brain
Reneacute Descartes
(1596-1650)
Descartes wrote ldquoThe flame particle jumps from the fire
touches the toe moves up the spinal cord until a little bell goes off in the brain and says lsquoouch It
hurtrsquordquo
Treatise of Man 1662
It is a disturbance which passes along nerve fibres to the brain
Reneacute Descartes ndash Pain is a disturbance that passes along nerve fibres to the brain
The Cartesian Legacy
bull Pain is a Direct Measure of Tissue Damage
bull Brain amp CNS Play a Passive Role
bull No Reason to Look Beyond the Painful Tissues bull In Chronic Pain Tissues are Not Healing and Damage is Ongoing
bull Stopping the Stimulus is the Way to Stop Pain ndash Or Cutting the Wire
bull lsquoMind-Body splitrsquo Pain is Either Physical Or Psychological (Mental Illness)
Pain Management Main CJ et al 2nd Edition 2008 Churchill Livingstone
ldquoIn the past decade scientific evidence has shown that the biomedical model falls short in the treatment of patients with musculoskeletal pain To understand musculoskeletal pain and a patients health behavior and beliefs physical therapists should assess the illness perceptions of their patientsrdquo ldquoThe overall impression was that the assessments of the physical therapists were still bio-medically oriented in these patients with chronic musculoskeletal painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
4
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
ldquoTrust your patient they are telling you the truth it is up to you to find out why If your patient tells you they have widespread pain they do even if
you cannot understand itrdquo
2014
Answers from Neuroscience A Pain Theory Revolution Was Happening
On returning to university (SHU) in 1996 faculty of Biomedical Science I found
bull Pain theory was a hot topic
bull Biomedical model was being overthrown by the lsquoBiopsychosocialrsquo bull A number of landmark discoveries had been made in the 80rsquos
bull Knowledge was largely contained within the academic world of neuroscience
Louis Gifford M App Sc BSc MCSP
httpwwwachesandpainsonlinecomaboutusphp
It is not an exaggeration to say that this book marks a milestone not only for an understanding of pain but also for the maturation of physiotherapy Professor Patrick Wall (1925 ndash 2001) Review 1998
Subsequently adopted as core reading for post graduate and undergraduate training programmes in the UK and abroad
Research Physiotherapist international lecturer Author of the Yearbooks of the Physiotherapy Pain Association (1994) for Chartered Physiotherapists
David Butler M App Sc (NOI)
Physiotherapist international freelance educator senior lecturer at the University of South Australia and a director of the NOI
httpwwwactuariesasnauACS2011ProgramPlenarySpeakersaspx
ldquoI believe the ideal approach in the clinic should be one that encompasses three things the best skills from current therapy the best information from science and the best therapeutic relationship
with a particular patientrdquo
Integrating pain awareness into physiotherapy-wise action for the future In Gifford Topical Issues in Pain 1 1998
Sensory Receptor Afferent Nerve (Axon) C
Mechanoreceptors Touch
Thermoreceptors Cold Warm
Photoreceptors Colour Light
Audioreceptors Sound
Chemoreceptors Taste Smell
Proprioreceptors Position etc body parts
Interoreceptors eg Baroreceptors Osmoreceptors
Nociceptors (Mechano ndash Chemo) Pain
Exteroreceptors enable us to make sense of the External Physical World
Sensation amp Perception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
5
Everything we See Hear Taste and Smell and feel as Touch or Pain Exists in our brains
ldquoWe acknowledge that all the individual features of the world are experienced through our sense organs The information that reaches us through those organs is converted into electrical signals and the individual parts of our brain analyze and process these signals After this interpreting process takes place inside our brain we will for example see a book taste a strawberry smell a flower feel the texture of a silk fabric or hear leaves shaking in the windrdquo
httpwwwsecretbeyondmattercomourbrainstheworldinourbrainshtml
Stimulus Electrical Signal
Meaning
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Nociception
To brain
Zone of Lissauer
Substantia gelatinosa
Dorsal root
DRG
Ventral root
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Pain Cannot Exist Outside of Consciousness
Nociception
Nociception Can Occur Without the Brain
When we Stub Our Toe it Hurts But only because Our Brain Says so
INJURY
PAIN
bull Damage has Occurred bull It has been Inflicted on the Toe bull Something Needs to be Done
(raise foot hobble utter expletive)
The Brain Decides
httpwwwwellcomeacukenpainmicrositescience2html
httparchivesciencewatchcomdrfmf201111mayf
mf11mayfmfCrai
AD (Bud) Craig Principal InvestigatorDirector Atkinson Pain Research Laboratory Barrow Neurological Institute Phoenix
When we Stub Our Toe it Hurts But only because Our Brain Says so
INJURY
PAIN
ldquoIt may feel as if our toe is throbbing but the experience is all contained within a mental projection of the
condition of our toe within our brainrdquo
httpwwwwellcomeacukenpainmicrositescience2html
httparchivesciencewatchcomdrfmf201111mayf
mf11mayfmfCrai
AD (Bud) Craig Principal InvestigatorDirector Atkinson Pain Research Laboratory Barrow Neurological Institute Phoenix
httpgoldsmithsacademiaeduMaxVelmansPapers980457Physical_psychological_and_virtual_realities
Neural Activity (In The Brain) Can Result In Spatially Located
Extended Experiences
ldquoPerceptual processing in the brain can result in experiences that have a subjective location and extension beyond the brain In
Velmans (1990) I have called this phenomenon perceptual projection How spatial encodings and other encodings in the
brain are translated into such spatial phenomenology are matters for scientific researchrdquo Max Velmans
Max Velmans is an Emeritus Professor of Psychology at Goldsmiths University of London
httpwwwspracukexpcmsindexphpsection=87
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
6
ldquoThe localisation of pain (and other tactile sensation) is a projection from the brain into 3-dimensional space To facilitate
this the brain makes use of a map of the body surface and lsquoperipersonal spacersquo ldquo
2012
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Perceived Pain in the Tissues is an Illusion Created by the Brain
Somatotopy Somatotopy The correspondence between the position of a receptor in part of
the body and the corresponding area of the cerebral cortex that is activated by it
httpneurocriticblogspotcouk2009_08_01_archivehtml
Penfieldrsquos Somatosensory Homunculus
httpwwwmadscientistblogcamad-scientist-5-
paracelsus-pt-2-paracelsus-homunculus
httpmvameeducationalbrain_areashtml
Neurosurgeon Wilder Penfield (1891ndash1976)mapped the body onto the brain by electrically stimulating the cortex of over 400 conscious epileptic patients and
noting their responses
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
ldquoMicro-electrode stimulation of the somatosensory cortex produces feelings of numbness and tingling which are
subjectively located in different regions of the body not in the brainmdashanother clear case of perceptual projectionrdquo
Max Velmans
2013
Sudden Pain-Related Signals need to be rapidly transformed into External Spatial Coordinates to facilitate defensive reactions and prevent tissue
damage Pain localisation appears to take place in S1 co-localised with touch and in the Insular Cortex where there is more lsquocoarsersquo somatotopic
representation of pain
Insular Cortex
S1 M1
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
7
The Posterior Parietal Cortex houses lsquoExternal Spatial Representationrsquo It Remaps touch from a Somatatopic to a lsquoSpatiotopicrsquo external spatial frame of
reference by integrating touch with proprioceptive information about body posture This area about the body is called lsquoPeripersonal Spacersquo
2010 S1 M1 Important Points ndash Pain Perception
bull Percieved pain is an illusion lsquoprojectedrsquo by the brain
bull Nociception arises in the tissues
bull Nociception can exist without pain
bull Pain can exist without nociception
bull Pain is generated in the brain
bull To the patient the whole pain experience is contained within the tissues
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors High Threshold Gated Ion Channels on Free Nerve Endings
Location
Externally Skin
Cornea Mucosa
Internally Muscles
Joints Bladder Gut etc
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors amp LT Mechanoreceptors
TOUCH
PAIN
Pain amp Touch information travel to the brain in different Tracts ndash Dorsal Columns and Spinothalamic Tracts respectively
Schematic of ion channels in nociceptor function
Mechanical Noxious Cold ndash (lt5C) Protons (Acid-sensing-ion channel) Noxious Heat ndash (gt42C) Serotonin ATP Nerve Growth Factor Chemicals (G-protein-coupled receptors) eg histamine bradykinin prostaglandins
Capsaicin found in ldquoHotrdquo Peppers such as Red Chillies and Jalapenos is able to selectively activate the Trpv1 receptor and thus provides a
means of inducing pain experimentally without tissue damage
C
Stimulators of Nociception
Nociceptor Nociception (Axon)
Brain
Nociceptor Activators Mechanical pressure Thermal stimuli (gt42C lt5C) Chemical (inflammatory mediators or products of damaged cells) Potassium ions ATP Protons (acidity hypoxia) Histamine Serotonin Bradykinin
Nociceptor Sensitisers Chemical (released from damaged tissue or axon reflex) Prostaglandins Cytokines Substance P CGRP
Transduction Pain Conduction
Neuropeptides
CGRP = Calcitonin Gene Related Peptide
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
8
Axon Reflex ndash Neurogenic Inflammation Neuropeptides (eg Substance P CGRP) and Inflammation
Action potentials in branches of an afferent nociceptor can move
peripherallyThis is called the axon reflex The release of substance P and CGRP (sensitises) increases inflammation by causing histamine
release and dilation of blood vessels
httpcourseswashingtoneduconjsensorypainhtm
Mechanisms Associated with Peripheral Sensitisation to Pain
After an injury occurs there is a time-dependent expansion in the area of sensitivity as tissue that is not damaged becomes increasingly sensitive to any sort of stimulus that is applied This is called HYPERALGESIA
wwwpagesdrexeledu~mab337Pain20Lectureppt
C Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Peripheral Sensitisation (Hyperalgesia)
If there is tissue injury diffusion of the lsquoinflammatory souprsquo activates adjacent nociceptors causing the painful tender area to
expand The barrage of nociception is then the source of pathophysiological pain
Injury
A Critical Number of Open Sensors will Start the Response
Acute_Pain_Normal
httptriactionpotentialblogspotcom
Movie Clip ndash Key Points
Injury
Inflammatory Reaction
Electrical Signal - Fast Ad and Slow C Fibre Nociceptors
Dorsal Horn
Spinothalamic Tract
Thalamus
Cortex Frontal Lobe Limbic System
PERCEPTION - Texture amp Intensity Emotional Impact Link to Memory Meaning
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
9
Fast Ad Fibre Pain bull Sharp and well localised bull Nociceptive impulses synapse in the dorsal horn initiate withdrawal reflexes and travel to the sensory cortex via the thalamus
Slow C Fibre Pain bull Diffuse more burning and unpleasant ndash lingers bull Nociceptive impulses synapse with interneurons in the dorsal horn then travel to
1) Sensory cortex and insular cortex 2) Limbic System ndash memory and emotion 3) Hypothalamus (ANS) and brain stem
Only C fibres respond to Chemical stimulation
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Can be Referred to as Projection Neurons
Dorsal Horn Neurons 2nd Order Neurons
httpwwwrnceuscomagesnociceptivehtm
They arise from Lamina 1 as Nociception
Specific (NS) neurons and Lamina V as Wide Dynamic
Ranging (WDR) neurons
NS
WDR
How Mechanoreceptor Activity Can Decrease Nociceptive Processing
(Why Movement and Rubbing Decreases The Perception of Pain)
Melzack and Wallrsquos Pain Gate Theory was the first real challenge to the Pathoanatomical model It postulated that nociception could be lsquomodulatedrsquo at the dorsal horn
and that some lsquointegrationrsquo of nociceptive and other sensory
information could occur
httppublicationsmcgillcaheadwaymagazine
the-king-of-understanding-pain-qa-with-ronald-melzack
naturecom
Ronald Melzack Patrick Wall
1965
R Melzack PD Wall Pain mechanisms a new theory Science 1965150971ndash979
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Many interneurons and interconnections within
the dorsal horn allow integration of different sensory channels Eg Inhibitory interneurons
can be activated by touch and propriceptive input to deep laminae to lsquogatersquo NS
output from lamina 1
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
As Wall himself wrote evaluating the gate theory in the light of further experiments lsquolsquoThe least and perhaps the best that can be said for the 1965
paper is that it provoked discussion and experimentrsquorsquo
2014
Free Access httpwwwsciencedirectcomscience
articlepiiS0306452214007830
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
10
Neurons That Conduct Nociception (Pain Impulses) to the Brain
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
NS neurons are more associated with the emotional suffering
dimension of pain Also autonomic motivational
amp homeostatic responses
WDR neurons are mainly associated with the
sensory discriminative dimension of pain ndash location amp intensity
Spinal Polysynaptic Interneurons (PSINs) (Eg Flexor amp Crossed Extensor Reflex)
httpalexandriahealthlibrarycadocumentsnotesbomunit_6lec2025_moo_spinreflexxml
Withdrawal reflexes are mainly initiated by Ad fibres and involve
interneurons that cross the midline
Other cord level responses effected by nociceptors and interneurons include altered muscle tone and sympathetic effects (sweating vasoconstrictiondilation) via links to the preganglionic cell bodies in the lateral horn
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Experiment to Demonstate Secondary Hyperalgesia with Capsaicin induced Nociception
Nerve Block (local anaesthetic)
Nerve Block
Capsaicin
Amplification
R L R L
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Amplifier
Injury
Discovery of the dorsal horn amplifier proved that the pain circuitry exhibits lsquoactivity-dependent-synaptic-plasticityrsquo It is not
hard-wired
Clifford Woolf Discovered central sensitization whilst researching at University College London alongside Patrick Wall and published his findings in 1983 (Woolf CJ Evidence for a central component of post-injury pain hypersensitivity Nature 1983 306686-8)
ldquo pain does not simply reflect the presence intensity or duration of specific lsquopainrsquo stimuli in the periphery but also changes in the
function of the central nervous systemrdquo
Woolf CJ Central sensitization ndashuncovering the relation between pain and plasticity Anesthesiology 2007106864-7
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
11
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
C
C
C C
C C
C
C
C C
C C C
C
C C C
C
Peripheral amp Central Sensitisation Stimulus
Injury + Inflammation
Dorsal Horn Amplification
Amplification In The Brain
PNS CNS
C
C
C
C C C
C Peripheral amp Central Sensitisation
As Inflammation Resolves Peripheral Sensitisation dies down but Central Sensitisation
sometimes persists to be the cause of Chronic pain
lsquoNormallyrsquo ndash Pain goes
lsquoPathologicalrsquo ndash Pain becomes Chronic Brain continues to generate pain Cortical Reorganisation
Dorsal Horn Amplifier stays on High Gain
PAIN
Important Points ndash Pain Sensitisation
bull Peripheral sensitisation drives central sensitisation
bull Secondary hyperalgesia (central sensitisation) gives additional warning of the need to protect the injured anatomy whilst it is inflamed thus assisting healing
bull Perceived worsening pain and an often massive spread of tenderness into multiple tissues is mainly on account of central sensitisation These tissues are not all injured
bull Pain circuitry is not hard-wired
bull Spreading pain is lsquobeyond dermatomesrsquo
Glutamate amp NMDA Receptors Main Neurotransmitter Released by C Fibres
During prolonged excitation the sum of EPSPs lowers the membrane potential sufficiently for the NMDA channels to expel their magnesium molecule allowing an influx of Ca2+ This triggers the release of retrograde messengers that stimulate the
release of more glutamate from the pre-synaptic membrane This all leads to a greater response from the secondary nerve
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Glutamate normally opens only AMPA channels because NMDA channels are blocked by a magnesium molecule
Substance P Sensitising Neuropeptides Also Released by C Fibres
Subtance P and CGRP sensitise the secondary nerve to glutamate Within the dorsal horn these can diffuse around several levels of the spinal cord sensitising
other secondary nerves (dorsal horn neurons) in the process
What was previously an innocuous stimulus may now be perceived as pain and pain may be perceived at a seemingly unrelated anatomical site
Substance P
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
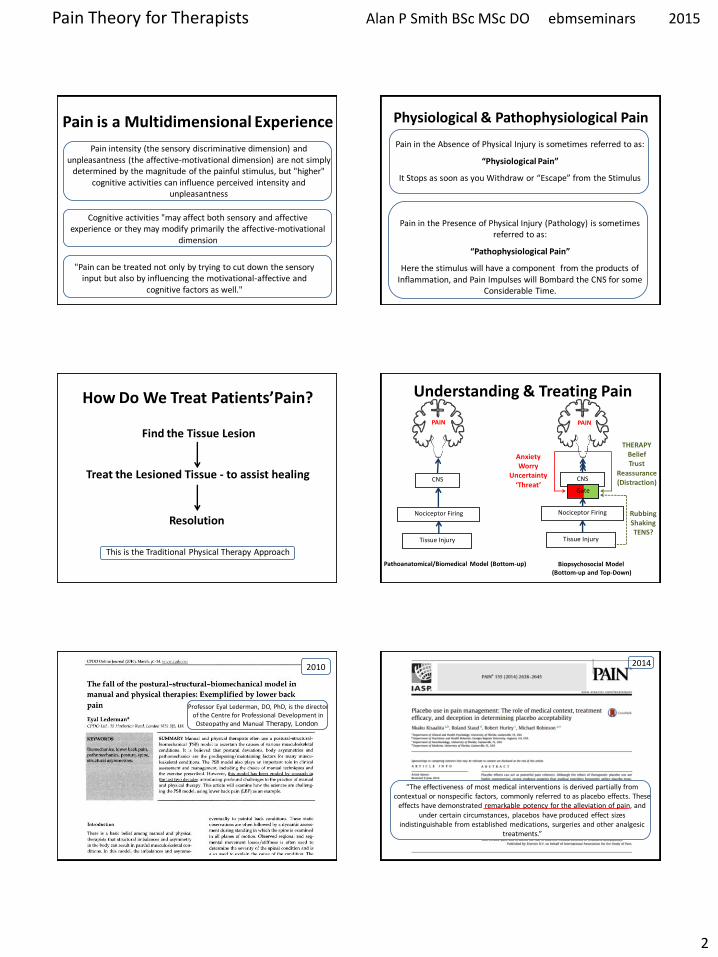
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
2
Pain intensity (the sensory discriminative dimension) and unpleasantness (the affective-motivational dimension) are not simply
determined by the magnitude of the painful stimulus but higher cognitive activities can influence perceived intensity and
unpleasantness
Pain can be treated not only by trying to cut down the sensory input but also by influencing the motivational-affective and
cognitive factors as well
Pain is a Multidimensional Experience
Cognitive activities may affect both sensory and affective experience or they may modify primarily the affective-motivational
dimension
Pain in the Absence of Physical Injury is sometimes referred to as
ldquoPhysiological Painrdquo
It Stops as soon as you Withdraw or ldquoEscaperdquo from the Stimulus
Pain in the Presence of Physical Injury (Pathology) is sometimes referred to as
ldquoPathophysiological Painrdquo
Here the stimulus will have a component from the products of Inflammation and Pain Impulses will Bombard the CNS for some
Considerable Time
Physiological amp Pathophysiological Pain
How Do We Treat PatientsrsquoPain
Find the Tissue Lesion
Treat the Lesioned Tissue - to assist healing
Resolution
This is the Traditional Physical Therapy Approach
Understanding amp Treating Pain
Tissue Injury
Nociceptor Firing
CNS
PAIN
Tissue Injury
Nociceptor Firing
CNS
PAIN
Gate
Anxiety Worry
Uncertainty lsquoThreatrsquo
THERAPY Belief Trust
Reassurance (Distraction)
Rubbing Shaking TENS
PathoanatomicalBiomedical Model (Bottom-up) Biopsychosocial Model (Bottom-up and Top-Down)
Professor Eyal Lederman DO PhD is the director of the Centre for Professional Development in Osteopathy and Manual Therapy London
2010
ldquoThe effectiveness of most medical interventions is derived partially from contextual or nonspecific factors commonly referred to as placebo effects These
effects have demonstrated remarkable potency for the alleviation of pain and under certain circumstances placebos have produced effect sizes
indistinguishable from established medications surgeries and other analgesic treatmentsrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
3
ldquoAlthough the effects of manual therapy are classically explained within a biomechanical paradigm research now points to the important role of
neurophysiological processes at both spinal and supraspinal levels in the modulation of nociceptive informationrdquo hellip ldquoin clinical practice manual therapy
articular mobilizations andor manipulations are seldom being used as an isolated interventionrdquohellip ldquocombining various strategies imparts a synergistic
effect on the brain-orchestrated analgesic systemrdquo
2015 Understanding amp Treating Pain
Tissue Injury
Nociceptor Firing
CNS
PAIN
Gate
Anxiety Worry
Uncertainty lsquoThreatrsquo
THERAPY Belief Trust
Reassurance (Distraction)
Rubbing Shaking TENS
Biopsychosocial Model (Bottom-up and Top-Down)
Targets for Treating Pain
1) Tissues Traditional Modalities 2) Gate Non-specific (lsquoplaceborsquo) 3) Consciousness Distraction
ldquoCognitive distraction could be mediated mainly by direct frontal-corticol somatosensory interactions without the engagement of brainstem pain-
control systemsrdquo ldquoPlacebo analgesia does not depend on active redirection of attention and that expectancy and distraction can be combined to maximize
pain reliefrdquo
2012
C Stimulus
Pain is Generated in the Brain
Reneacute Descartes
(1596-1650)
Descartes wrote ldquoThe flame particle jumps from the fire
touches the toe moves up the spinal cord until a little bell goes off in the brain and says lsquoouch It
hurtrsquordquo
Treatise of Man 1662
It is a disturbance which passes along nerve fibres to the brain
Reneacute Descartes ndash Pain is a disturbance that passes along nerve fibres to the brain
The Cartesian Legacy
bull Pain is a Direct Measure of Tissue Damage
bull Brain amp CNS Play a Passive Role
bull No Reason to Look Beyond the Painful Tissues bull In Chronic Pain Tissues are Not Healing and Damage is Ongoing
bull Stopping the Stimulus is the Way to Stop Pain ndash Or Cutting the Wire
bull lsquoMind-Body splitrsquo Pain is Either Physical Or Psychological (Mental Illness)
Pain Management Main CJ et al 2nd Edition 2008 Churchill Livingstone
ldquoIn the past decade scientific evidence has shown that the biomedical model falls short in the treatment of patients with musculoskeletal pain To understand musculoskeletal pain and a patients health behavior and beliefs physical therapists should assess the illness perceptions of their patientsrdquo ldquoThe overall impression was that the assessments of the physical therapists were still bio-medically oriented in these patients with chronic musculoskeletal painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
4
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
ldquoTrust your patient they are telling you the truth it is up to you to find out why If your patient tells you they have widespread pain they do even if
you cannot understand itrdquo
2014
Answers from Neuroscience A Pain Theory Revolution Was Happening
On returning to university (SHU) in 1996 faculty of Biomedical Science I found
bull Pain theory was a hot topic
bull Biomedical model was being overthrown by the lsquoBiopsychosocialrsquo bull A number of landmark discoveries had been made in the 80rsquos
bull Knowledge was largely contained within the academic world of neuroscience
Louis Gifford M App Sc BSc MCSP
httpwwwachesandpainsonlinecomaboutusphp
It is not an exaggeration to say that this book marks a milestone not only for an understanding of pain but also for the maturation of physiotherapy Professor Patrick Wall (1925 ndash 2001) Review 1998
Subsequently adopted as core reading for post graduate and undergraduate training programmes in the UK and abroad
Research Physiotherapist international lecturer Author of the Yearbooks of the Physiotherapy Pain Association (1994) for Chartered Physiotherapists
David Butler M App Sc (NOI)
Physiotherapist international freelance educator senior lecturer at the University of South Australia and a director of the NOI
httpwwwactuariesasnauACS2011ProgramPlenarySpeakersaspx
ldquoI believe the ideal approach in the clinic should be one that encompasses three things the best skills from current therapy the best information from science and the best therapeutic relationship
with a particular patientrdquo
Integrating pain awareness into physiotherapy-wise action for the future In Gifford Topical Issues in Pain 1 1998
Sensory Receptor Afferent Nerve (Axon) C
Mechanoreceptors Touch
Thermoreceptors Cold Warm
Photoreceptors Colour Light
Audioreceptors Sound
Chemoreceptors Taste Smell
Proprioreceptors Position etc body parts
Interoreceptors eg Baroreceptors Osmoreceptors
Nociceptors (Mechano ndash Chemo) Pain
Exteroreceptors enable us to make sense of the External Physical World
Sensation amp Perception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
5
Everything we See Hear Taste and Smell and feel as Touch or Pain Exists in our brains
ldquoWe acknowledge that all the individual features of the world are experienced through our sense organs The information that reaches us through those organs is converted into electrical signals and the individual parts of our brain analyze and process these signals After this interpreting process takes place inside our brain we will for example see a book taste a strawberry smell a flower feel the texture of a silk fabric or hear leaves shaking in the windrdquo
httpwwwsecretbeyondmattercomourbrainstheworldinourbrainshtml
Stimulus Electrical Signal
Meaning
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Nociception
To brain
Zone of Lissauer
Substantia gelatinosa
Dorsal root
DRG
Ventral root
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Pain Cannot Exist Outside of Consciousness
Nociception
Nociception Can Occur Without the Brain
When we Stub Our Toe it Hurts But only because Our Brain Says so
INJURY
PAIN
bull Damage has Occurred bull It has been Inflicted on the Toe bull Something Needs to be Done
(raise foot hobble utter expletive)
The Brain Decides
httpwwwwellcomeacukenpainmicrositescience2html
httparchivesciencewatchcomdrfmf201111mayf
mf11mayfmfCrai
AD (Bud) Craig Principal InvestigatorDirector Atkinson Pain Research Laboratory Barrow Neurological Institute Phoenix
When we Stub Our Toe it Hurts But only because Our Brain Says so
INJURY
PAIN
ldquoIt may feel as if our toe is throbbing but the experience is all contained within a mental projection of the
condition of our toe within our brainrdquo
httpwwwwellcomeacukenpainmicrositescience2html
httparchivesciencewatchcomdrfmf201111mayf
mf11mayfmfCrai
AD (Bud) Craig Principal InvestigatorDirector Atkinson Pain Research Laboratory Barrow Neurological Institute Phoenix
httpgoldsmithsacademiaeduMaxVelmansPapers980457Physical_psychological_and_virtual_realities
Neural Activity (In The Brain) Can Result In Spatially Located
Extended Experiences
ldquoPerceptual processing in the brain can result in experiences that have a subjective location and extension beyond the brain In
Velmans (1990) I have called this phenomenon perceptual projection How spatial encodings and other encodings in the
brain are translated into such spatial phenomenology are matters for scientific researchrdquo Max Velmans
Max Velmans is an Emeritus Professor of Psychology at Goldsmiths University of London
httpwwwspracukexpcmsindexphpsection=87
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
6
ldquoThe localisation of pain (and other tactile sensation) is a projection from the brain into 3-dimensional space To facilitate
this the brain makes use of a map of the body surface and lsquoperipersonal spacersquo ldquo
2012
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Perceived Pain in the Tissues is an Illusion Created by the Brain
Somatotopy Somatotopy The correspondence between the position of a receptor in part of
the body and the corresponding area of the cerebral cortex that is activated by it
httpneurocriticblogspotcouk2009_08_01_archivehtml
Penfieldrsquos Somatosensory Homunculus
httpwwwmadscientistblogcamad-scientist-5-
paracelsus-pt-2-paracelsus-homunculus
httpmvameeducationalbrain_areashtml
Neurosurgeon Wilder Penfield (1891ndash1976)mapped the body onto the brain by electrically stimulating the cortex of over 400 conscious epileptic patients and
noting their responses
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
ldquoMicro-electrode stimulation of the somatosensory cortex produces feelings of numbness and tingling which are
subjectively located in different regions of the body not in the brainmdashanother clear case of perceptual projectionrdquo
Max Velmans
2013
Sudden Pain-Related Signals need to be rapidly transformed into External Spatial Coordinates to facilitate defensive reactions and prevent tissue
damage Pain localisation appears to take place in S1 co-localised with touch and in the Insular Cortex where there is more lsquocoarsersquo somatotopic
representation of pain
Insular Cortex
S1 M1
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
7
The Posterior Parietal Cortex houses lsquoExternal Spatial Representationrsquo It Remaps touch from a Somatatopic to a lsquoSpatiotopicrsquo external spatial frame of
reference by integrating touch with proprioceptive information about body posture This area about the body is called lsquoPeripersonal Spacersquo
2010 S1 M1 Important Points ndash Pain Perception
bull Percieved pain is an illusion lsquoprojectedrsquo by the brain
bull Nociception arises in the tissues
bull Nociception can exist without pain
bull Pain can exist without nociception
bull Pain is generated in the brain
bull To the patient the whole pain experience is contained within the tissues
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors High Threshold Gated Ion Channels on Free Nerve Endings
Location
Externally Skin
Cornea Mucosa
Internally Muscles
Joints Bladder Gut etc
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors amp LT Mechanoreceptors
TOUCH
PAIN
Pain amp Touch information travel to the brain in different Tracts ndash Dorsal Columns and Spinothalamic Tracts respectively
Schematic of ion channels in nociceptor function
Mechanical Noxious Cold ndash (lt5C) Protons (Acid-sensing-ion channel) Noxious Heat ndash (gt42C) Serotonin ATP Nerve Growth Factor Chemicals (G-protein-coupled receptors) eg histamine bradykinin prostaglandins
Capsaicin found in ldquoHotrdquo Peppers such as Red Chillies and Jalapenos is able to selectively activate the Trpv1 receptor and thus provides a
means of inducing pain experimentally without tissue damage
C
Stimulators of Nociception
Nociceptor Nociception (Axon)
Brain
Nociceptor Activators Mechanical pressure Thermal stimuli (gt42C lt5C) Chemical (inflammatory mediators or products of damaged cells) Potassium ions ATP Protons (acidity hypoxia) Histamine Serotonin Bradykinin
Nociceptor Sensitisers Chemical (released from damaged tissue or axon reflex) Prostaglandins Cytokines Substance P CGRP
Transduction Pain Conduction
Neuropeptides
CGRP = Calcitonin Gene Related Peptide
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
8
Axon Reflex ndash Neurogenic Inflammation Neuropeptides (eg Substance P CGRP) and Inflammation
Action potentials in branches of an afferent nociceptor can move
peripherallyThis is called the axon reflex The release of substance P and CGRP (sensitises) increases inflammation by causing histamine
release and dilation of blood vessels
httpcourseswashingtoneduconjsensorypainhtm
Mechanisms Associated with Peripheral Sensitisation to Pain
After an injury occurs there is a time-dependent expansion in the area of sensitivity as tissue that is not damaged becomes increasingly sensitive to any sort of stimulus that is applied This is called HYPERALGESIA
wwwpagesdrexeledu~mab337Pain20Lectureppt
C Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Peripheral Sensitisation (Hyperalgesia)
If there is tissue injury diffusion of the lsquoinflammatory souprsquo activates adjacent nociceptors causing the painful tender area to
expand The barrage of nociception is then the source of pathophysiological pain
Injury
A Critical Number of Open Sensors will Start the Response
Acute_Pain_Normal
httptriactionpotentialblogspotcom
Movie Clip ndash Key Points
Injury
Inflammatory Reaction
Electrical Signal - Fast Ad and Slow C Fibre Nociceptors
Dorsal Horn
Spinothalamic Tract
Thalamus
Cortex Frontal Lobe Limbic System
PERCEPTION - Texture amp Intensity Emotional Impact Link to Memory Meaning
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
9
Fast Ad Fibre Pain bull Sharp and well localised bull Nociceptive impulses synapse in the dorsal horn initiate withdrawal reflexes and travel to the sensory cortex via the thalamus
Slow C Fibre Pain bull Diffuse more burning and unpleasant ndash lingers bull Nociceptive impulses synapse with interneurons in the dorsal horn then travel to
1) Sensory cortex and insular cortex 2) Limbic System ndash memory and emotion 3) Hypothalamus (ANS) and brain stem
Only C fibres respond to Chemical stimulation
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Can be Referred to as Projection Neurons
Dorsal Horn Neurons 2nd Order Neurons
httpwwwrnceuscomagesnociceptivehtm
They arise from Lamina 1 as Nociception
Specific (NS) neurons and Lamina V as Wide Dynamic
Ranging (WDR) neurons
NS
WDR
How Mechanoreceptor Activity Can Decrease Nociceptive Processing
(Why Movement and Rubbing Decreases The Perception of Pain)
Melzack and Wallrsquos Pain Gate Theory was the first real challenge to the Pathoanatomical model It postulated that nociception could be lsquomodulatedrsquo at the dorsal horn
and that some lsquointegrationrsquo of nociceptive and other sensory
information could occur
httppublicationsmcgillcaheadwaymagazine
the-king-of-understanding-pain-qa-with-ronald-melzack
naturecom
Ronald Melzack Patrick Wall
1965
R Melzack PD Wall Pain mechanisms a new theory Science 1965150971ndash979
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Many interneurons and interconnections within
the dorsal horn allow integration of different sensory channels Eg Inhibitory interneurons
can be activated by touch and propriceptive input to deep laminae to lsquogatersquo NS
output from lamina 1
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
As Wall himself wrote evaluating the gate theory in the light of further experiments lsquolsquoThe least and perhaps the best that can be said for the 1965
paper is that it provoked discussion and experimentrsquorsquo
2014
Free Access httpwwwsciencedirectcomscience
articlepiiS0306452214007830
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
10
Neurons That Conduct Nociception (Pain Impulses) to the Brain
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
NS neurons are more associated with the emotional suffering
dimension of pain Also autonomic motivational
amp homeostatic responses
WDR neurons are mainly associated with the
sensory discriminative dimension of pain ndash location amp intensity
Spinal Polysynaptic Interneurons (PSINs) (Eg Flexor amp Crossed Extensor Reflex)
httpalexandriahealthlibrarycadocumentsnotesbomunit_6lec2025_moo_spinreflexxml
Withdrawal reflexes are mainly initiated by Ad fibres and involve
interneurons that cross the midline
Other cord level responses effected by nociceptors and interneurons include altered muscle tone and sympathetic effects (sweating vasoconstrictiondilation) via links to the preganglionic cell bodies in the lateral horn
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Experiment to Demonstate Secondary Hyperalgesia with Capsaicin induced Nociception
Nerve Block (local anaesthetic)
Nerve Block
Capsaicin
Amplification
R L R L
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Amplifier
Injury
Discovery of the dorsal horn amplifier proved that the pain circuitry exhibits lsquoactivity-dependent-synaptic-plasticityrsquo It is not
hard-wired
Clifford Woolf Discovered central sensitization whilst researching at University College London alongside Patrick Wall and published his findings in 1983 (Woolf CJ Evidence for a central component of post-injury pain hypersensitivity Nature 1983 306686-8)
ldquo pain does not simply reflect the presence intensity or duration of specific lsquopainrsquo stimuli in the periphery but also changes in the
function of the central nervous systemrdquo
Woolf CJ Central sensitization ndashuncovering the relation between pain and plasticity Anesthesiology 2007106864-7
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
11
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
C
C
C C
C C
C
C
C C
C C C
C
C C C
C
Peripheral amp Central Sensitisation Stimulus
Injury + Inflammation
Dorsal Horn Amplification
Amplification In The Brain
PNS CNS
C
C
C
C C C
C Peripheral amp Central Sensitisation
As Inflammation Resolves Peripheral Sensitisation dies down but Central Sensitisation
sometimes persists to be the cause of Chronic pain
lsquoNormallyrsquo ndash Pain goes
lsquoPathologicalrsquo ndash Pain becomes Chronic Brain continues to generate pain Cortical Reorganisation
Dorsal Horn Amplifier stays on High Gain
PAIN
Important Points ndash Pain Sensitisation
bull Peripheral sensitisation drives central sensitisation
bull Secondary hyperalgesia (central sensitisation) gives additional warning of the need to protect the injured anatomy whilst it is inflamed thus assisting healing
bull Perceived worsening pain and an often massive spread of tenderness into multiple tissues is mainly on account of central sensitisation These tissues are not all injured
bull Pain circuitry is not hard-wired
bull Spreading pain is lsquobeyond dermatomesrsquo
Glutamate amp NMDA Receptors Main Neurotransmitter Released by C Fibres
During prolonged excitation the sum of EPSPs lowers the membrane potential sufficiently for the NMDA channels to expel their magnesium molecule allowing an influx of Ca2+ This triggers the release of retrograde messengers that stimulate the
release of more glutamate from the pre-synaptic membrane This all leads to a greater response from the secondary nerve
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Glutamate normally opens only AMPA channels because NMDA channels are blocked by a magnesium molecule
Substance P Sensitising Neuropeptides Also Released by C Fibres
Subtance P and CGRP sensitise the secondary nerve to glutamate Within the dorsal horn these can diffuse around several levels of the spinal cord sensitising
other secondary nerves (dorsal horn neurons) in the process
What was previously an innocuous stimulus may now be perceived as pain and pain may be perceived at a seemingly unrelated anatomical site
Substance P
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
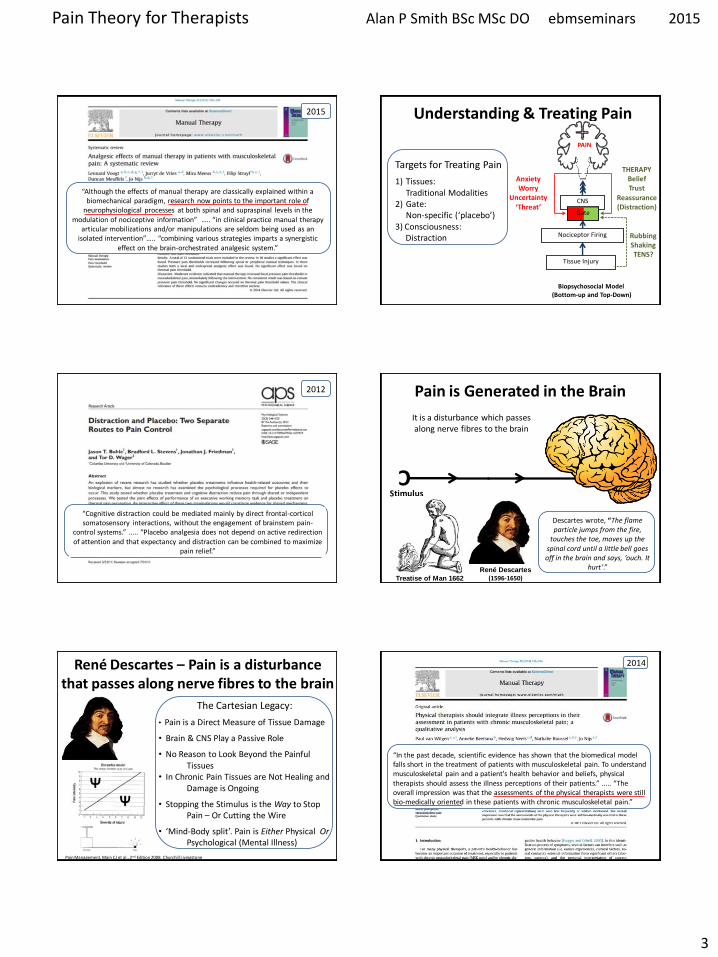
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
3
ldquoAlthough the effects of manual therapy are classically explained within a biomechanical paradigm research now points to the important role of
neurophysiological processes at both spinal and supraspinal levels in the modulation of nociceptive informationrdquo hellip ldquoin clinical practice manual therapy
articular mobilizations andor manipulations are seldom being used as an isolated interventionrdquohellip ldquocombining various strategies imparts a synergistic
effect on the brain-orchestrated analgesic systemrdquo
2015 Understanding amp Treating Pain
Tissue Injury
Nociceptor Firing
CNS
PAIN
Gate
Anxiety Worry
Uncertainty lsquoThreatrsquo
THERAPY Belief Trust
Reassurance (Distraction)
Rubbing Shaking TENS
Biopsychosocial Model (Bottom-up and Top-Down)
Targets for Treating Pain
1) Tissues Traditional Modalities 2) Gate Non-specific (lsquoplaceborsquo) 3) Consciousness Distraction
ldquoCognitive distraction could be mediated mainly by direct frontal-corticol somatosensory interactions without the engagement of brainstem pain-
control systemsrdquo ldquoPlacebo analgesia does not depend on active redirection of attention and that expectancy and distraction can be combined to maximize
pain reliefrdquo
2012
C Stimulus
Pain is Generated in the Brain
Reneacute Descartes
(1596-1650)
Descartes wrote ldquoThe flame particle jumps from the fire
touches the toe moves up the spinal cord until a little bell goes off in the brain and says lsquoouch It
hurtrsquordquo
Treatise of Man 1662
It is a disturbance which passes along nerve fibres to the brain
Reneacute Descartes ndash Pain is a disturbance that passes along nerve fibres to the brain
The Cartesian Legacy
bull Pain is a Direct Measure of Tissue Damage
bull Brain amp CNS Play a Passive Role
bull No Reason to Look Beyond the Painful Tissues bull In Chronic Pain Tissues are Not Healing and Damage is Ongoing
bull Stopping the Stimulus is the Way to Stop Pain ndash Or Cutting the Wire
bull lsquoMind-Body splitrsquo Pain is Either Physical Or Psychological (Mental Illness)
Pain Management Main CJ et al 2nd Edition 2008 Churchill Livingstone
ldquoIn the past decade scientific evidence has shown that the biomedical model falls short in the treatment of patients with musculoskeletal pain To understand musculoskeletal pain and a patients health behavior and beliefs physical therapists should assess the illness perceptions of their patientsrdquo ldquoThe overall impression was that the assessments of the physical therapists were still bio-medically oriented in these patients with chronic musculoskeletal painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
4
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
ldquoTrust your patient they are telling you the truth it is up to you to find out why If your patient tells you they have widespread pain they do even if
you cannot understand itrdquo
2014
Answers from Neuroscience A Pain Theory Revolution Was Happening
On returning to university (SHU) in 1996 faculty of Biomedical Science I found
bull Pain theory was a hot topic
bull Biomedical model was being overthrown by the lsquoBiopsychosocialrsquo bull A number of landmark discoveries had been made in the 80rsquos
bull Knowledge was largely contained within the academic world of neuroscience
Louis Gifford M App Sc BSc MCSP
httpwwwachesandpainsonlinecomaboutusphp
It is not an exaggeration to say that this book marks a milestone not only for an understanding of pain but also for the maturation of physiotherapy Professor Patrick Wall (1925 ndash 2001) Review 1998
Subsequently adopted as core reading for post graduate and undergraduate training programmes in the UK and abroad
Research Physiotherapist international lecturer Author of the Yearbooks of the Physiotherapy Pain Association (1994) for Chartered Physiotherapists
David Butler M App Sc (NOI)
Physiotherapist international freelance educator senior lecturer at the University of South Australia and a director of the NOI
httpwwwactuariesasnauACS2011ProgramPlenarySpeakersaspx
ldquoI believe the ideal approach in the clinic should be one that encompasses three things the best skills from current therapy the best information from science and the best therapeutic relationship
with a particular patientrdquo
Integrating pain awareness into physiotherapy-wise action for the future In Gifford Topical Issues in Pain 1 1998
Sensory Receptor Afferent Nerve (Axon) C
Mechanoreceptors Touch
Thermoreceptors Cold Warm
Photoreceptors Colour Light
Audioreceptors Sound
Chemoreceptors Taste Smell
Proprioreceptors Position etc body parts
Interoreceptors eg Baroreceptors Osmoreceptors
Nociceptors (Mechano ndash Chemo) Pain
Exteroreceptors enable us to make sense of the External Physical World
Sensation amp Perception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
5
Everything we See Hear Taste and Smell and feel as Touch or Pain Exists in our brains
ldquoWe acknowledge that all the individual features of the world are experienced through our sense organs The information that reaches us through those organs is converted into electrical signals and the individual parts of our brain analyze and process these signals After this interpreting process takes place inside our brain we will for example see a book taste a strawberry smell a flower feel the texture of a silk fabric or hear leaves shaking in the windrdquo
httpwwwsecretbeyondmattercomourbrainstheworldinourbrainshtml
Stimulus Electrical Signal
Meaning
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Nociception
To brain
Zone of Lissauer
Substantia gelatinosa
Dorsal root
DRG
Ventral root
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Pain Cannot Exist Outside of Consciousness
Nociception
Nociception Can Occur Without the Brain
When we Stub Our Toe it Hurts But only because Our Brain Says so
INJURY
PAIN
bull Damage has Occurred bull It has been Inflicted on the Toe bull Something Needs to be Done
(raise foot hobble utter expletive)
The Brain Decides
httpwwwwellcomeacukenpainmicrositescience2html
httparchivesciencewatchcomdrfmf201111mayf
mf11mayfmfCrai
AD (Bud) Craig Principal InvestigatorDirector Atkinson Pain Research Laboratory Barrow Neurological Institute Phoenix
When we Stub Our Toe it Hurts But only because Our Brain Says so
INJURY
PAIN
ldquoIt may feel as if our toe is throbbing but the experience is all contained within a mental projection of the
condition of our toe within our brainrdquo
httpwwwwellcomeacukenpainmicrositescience2html
httparchivesciencewatchcomdrfmf201111mayf
mf11mayfmfCrai
AD (Bud) Craig Principal InvestigatorDirector Atkinson Pain Research Laboratory Barrow Neurological Institute Phoenix
httpgoldsmithsacademiaeduMaxVelmansPapers980457Physical_psychological_and_virtual_realities
Neural Activity (In The Brain) Can Result In Spatially Located
Extended Experiences
ldquoPerceptual processing in the brain can result in experiences that have a subjective location and extension beyond the brain In
Velmans (1990) I have called this phenomenon perceptual projection How spatial encodings and other encodings in the
brain are translated into such spatial phenomenology are matters for scientific researchrdquo Max Velmans
Max Velmans is an Emeritus Professor of Psychology at Goldsmiths University of London
httpwwwspracukexpcmsindexphpsection=87
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
6
ldquoThe localisation of pain (and other tactile sensation) is a projection from the brain into 3-dimensional space To facilitate
this the brain makes use of a map of the body surface and lsquoperipersonal spacersquo ldquo
2012
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Perceived Pain in the Tissues is an Illusion Created by the Brain
Somatotopy Somatotopy The correspondence between the position of a receptor in part of
the body and the corresponding area of the cerebral cortex that is activated by it
httpneurocriticblogspotcouk2009_08_01_archivehtml
Penfieldrsquos Somatosensory Homunculus
httpwwwmadscientistblogcamad-scientist-5-
paracelsus-pt-2-paracelsus-homunculus
httpmvameeducationalbrain_areashtml
Neurosurgeon Wilder Penfield (1891ndash1976)mapped the body onto the brain by electrically stimulating the cortex of over 400 conscious epileptic patients and
noting their responses
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
ldquoMicro-electrode stimulation of the somatosensory cortex produces feelings of numbness and tingling which are
subjectively located in different regions of the body not in the brainmdashanother clear case of perceptual projectionrdquo
Max Velmans
2013
Sudden Pain-Related Signals need to be rapidly transformed into External Spatial Coordinates to facilitate defensive reactions and prevent tissue
damage Pain localisation appears to take place in S1 co-localised with touch and in the Insular Cortex where there is more lsquocoarsersquo somatotopic
representation of pain
Insular Cortex
S1 M1
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
7
The Posterior Parietal Cortex houses lsquoExternal Spatial Representationrsquo It Remaps touch from a Somatatopic to a lsquoSpatiotopicrsquo external spatial frame of
reference by integrating touch with proprioceptive information about body posture This area about the body is called lsquoPeripersonal Spacersquo
2010 S1 M1 Important Points ndash Pain Perception
bull Percieved pain is an illusion lsquoprojectedrsquo by the brain
bull Nociception arises in the tissues
bull Nociception can exist without pain
bull Pain can exist without nociception
bull Pain is generated in the brain
bull To the patient the whole pain experience is contained within the tissues
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors High Threshold Gated Ion Channels on Free Nerve Endings
Location
Externally Skin
Cornea Mucosa
Internally Muscles
Joints Bladder Gut etc
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors amp LT Mechanoreceptors
TOUCH
PAIN
Pain amp Touch information travel to the brain in different Tracts ndash Dorsal Columns and Spinothalamic Tracts respectively
Schematic of ion channels in nociceptor function
Mechanical Noxious Cold ndash (lt5C) Protons (Acid-sensing-ion channel) Noxious Heat ndash (gt42C) Serotonin ATP Nerve Growth Factor Chemicals (G-protein-coupled receptors) eg histamine bradykinin prostaglandins
Capsaicin found in ldquoHotrdquo Peppers such as Red Chillies and Jalapenos is able to selectively activate the Trpv1 receptor and thus provides a
means of inducing pain experimentally without tissue damage
C
Stimulators of Nociception
Nociceptor Nociception (Axon)
Brain
Nociceptor Activators Mechanical pressure Thermal stimuli (gt42C lt5C) Chemical (inflammatory mediators or products of damaged cells) Potassium ions ATP Protons (acidity hypoxia) Histamine Serotonin Bradykinin
Nociceptor Sensitisers Chemical (released from damaged tissue or axon reflex) Prostaglandins Cytokines Substance P CGRP
Transduction Pain Conduction
Neuropeptides
CGRP = Calcitonin Gene Related Peptide
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
8
Axon Reflex ndash Neurogenic Inflammation Neuropeptides (eg Substance P CGRP) and Inflammation
Action potentials in branches of an afferent nociceptor can move
peripherallyThis is called the axon reflex The release of substance P and CGRP (sensitises) increases inflammation by causing histamine
release and dilation of blood vessels
httpcourseswashingtoneduconjsensorypainhtm
Mechanisms Associated with Peripheral Sensitisation to Pain
After an injury occurs there is a time-dependent expansion in the area of sensitivity as tissue that is not damaged becomes increasingly sensitive to any sort of stimulus that is applied This is called HYPERALGESIA
wwwpagesdrexeledu~mab337Pain20Lectureppt
C Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Peripheral Sensitisation (Hyperalgesia)
If there is tissue injury diffusion of the lsquoinflammatory souprsquo activates adjacent nociceptors causing the painful tender area to
expand The barrage of nociception is then the source of pathophysiological pain
Injury
A Critical Number of Open Sensors will Start the Response
Acute_Pain_Normal
httptriactionpotentialblogspotcom
Movie Clip ndash Key Points
Injury
Inflammatory Reaction
Electrical Signal - Fast Ad and Slow C Fibre Nociceptors
Dorsal Horn
Spinothalamic Tract
Thalamus
Cortex Frontal Lobe Limbic System
PERCEPTION - Texture amp Intensity Emotional Impact Link to Memory Meaning
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
9
Fast Ad Fibre Pain bull Sharp and well localised bull Nociceptive impulses synapse in the dorsal horn initiate withdrawal reflexes and travel to the sensory cortex via the thalamus
Slow C Fibre Pain bull Diffuse more burning and unpleasant ndash lingers bull Nociceptive impulses synapse with interneurons in the dorsal horn then travel to
1) Sensory cortex and insular cortex 2) Limbic System ndash memory and emotion 3) Hypothalamus (ANS) and brain stem
Only C fibres respond to Chemical stimulation
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Can be Referred to as Projection Neurons
Dorsal Horn Neurons 2nd Order Neurons
httpwwwrnceuscomagesnociceptivehtm
They arise from Lamina 1 as Nociception
Specific (NS) neurons and Lamina V as Wide Dynamic
Ranging (WDR) neurons
NS
WDR
How Mechanoreceptor Activity Can Decrease Nociceptive Processing
(Why Movement and Rubbing Decreases The Perception of Pain)
Melzack and Wallrsquos Pain Gate Theory was the first real challenge to the Pathoanatomical model It postulated that nociception could be lsquomodulatedrsquo at the dorsal horn
and that some lsquointegrationrsquo of nociceptive and other sensory
information could occur
httppublicationsmcgillcaheadwaymagazine
the-king-of-understanding-pain-qa-with-ronald-melzack
naturecom
Ronald Melzack Patrick Wall
1965
R Melzack PD Wall Pain mechanisms a new theory Science 1965150971ndash979
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Many interneurons and interconnections within
the dorsal horn allow integration of different sensory channels Eg Inhibitory interneurons
can be activated by touch and propriceptive input to deep laminae to lsquogatersquo NS
output from lamina 1
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
As Wall himself wrote evaluating the gate theory in the light of further experiments lsquolsquoThe least and perhaps the best that can be said for the 1965
paper is that it provoked discussion and experimentrsquorsquo
2014
Free Access httpwwwsciencedirectcomscience
articlepiiS0306452214007830
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
10
Neurons That Conduct Nociception (Pain Impulses) to the Brain
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
NS neurons are more associated with the emotional suffering
dimension of pain Also autonomic motivational
amp homeostatic responses
WDR neurons are mainly associated with the
sensory discriminative dimension of pain ndash location amp intensity
Spinal Polysynaptic Interneurons (PSINs) (Eg Flexor amp Crossed Extensor Reflex)
httpalexandriahealthlibrarycadocumentsnotesbomunit_6lec2025_moo_spinreflexxml
Withdrawal reflexes are mainly initiated by Ad fibres and involve
interneurons that cross the midline
Other cord level responses effected by nociceptors and interneurons include altered muscle tone and sympathetic effects (sweating vasoconstrictiondilation) via links to the preganglionic cell bodies in the lateral horn
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Experiment to Demonstate Secondary Hyperalgesia with Capsaicin induced Nociception
Nerve Block (local anaesthetic)
Nerve Block
Capsaicin
Amplification
R L R L
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Amplifier
Injury
Discovery of the dorsal horn amplifier proved that the pain circuitry exhibits lsquoactivity-dependent-synaptic-plasticityrsquo It is not
hard-wired
Clifford Woolf Discovered central sensitization whilst researching at University College London alongside Patrick Wall and published his findings in 1983 (Woolf CJ Evidence for a central component of post-injury pain hypersensitivity Nature 1983 306686-8)
ldquo pain does not simply reflect the presence intensity or duration of specific lsquopainrsquo stimuli in the periphery but also changes in the
function of the central nervous systemrdquo
Woolf CJ Central sensitization ndashuncovering the relation between pain and plasticity Anesthesiology 2007106864-7
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
11
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
C
C
C C
C C
C
C
C C
C C C
C
C C C
C
Peripheral amp Central Sensitisation Stimulus
Injury + Inflammation
Dorsal Horn Amplification
Amplification In The Brain
PNS CNS
C
C
C
C C C
C Peripheral amp Central Sensitisation
As Inflammation Resolves Peripheral Sensitisation dies down but Central Sensitisation
sometimes persists to be the cause of Chronic pain
lsquoNormallyrsquo ndash Pain goes
lsquoPathologicalrsquo ndash Pain becomes Chronic Brain continues to generate pain Cortical Reorganisation
Dorsal Horn Amplifier stays on High Gain
PAIN
Important Points ndash Pain Sensitisation
bull Peripheral sensitisation drives central sensitisation
bull Secondary hyperalgesia (central sensitisation) gives additional warning of the need to protect the injured anatomy whilst it is inflamed thus assisting healing
bull Perceived worsening pain and an often massive spread of tenderness into multiple tissues is mainly on account of central sensitisation These tissues are not all injured
bull Pain circuitry is not hard-wired
bull Spreading pain is lsquobeyond dermatomesrsquo
Glutamate amp NMDA Receptors Main Neurotransmitter Released by C Fibres
During prolonged excitation the sum of EPSPs lowers the membrane potential sufficiently for the NMDA channels to expel their magnesium molecule allowing an influx of Ca2+ This triggers the release of retrograde messengers that stimulate the
release of more glutamate from the pre-synaptic membrane This all leads to a greater response from the secondary nerve
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Glutamate normally opens only AMPA channels because NMDA channels are blocked by a magnesium molecule
Substance P Sensitising Neuropeptides Also Released by C Fibres
Subtance P and CGRP sensitise the secondary nerve to glutamate Within the dorsal horn these can diffuse around several levels of the spinal cord sensitising
other secondary nerves (dorsal horn neurons) in the process
What was previously an innocuous stimulus may now be perceived as pain and pain may be perceived at a seemingly unrelated anatomical site
Substance P
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
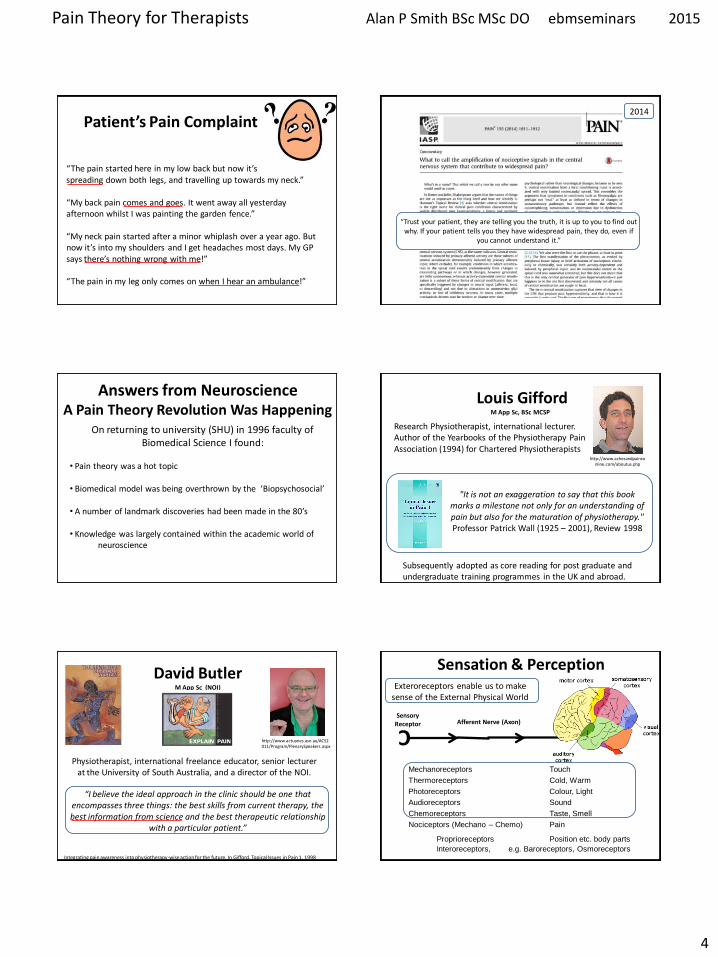
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
4
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
ldquoTrust your patient they are telling you the truth it is up to you to find out why If your patient tells you they have widespread pain they do even if
you cannot understand itrdquo
2014
Answers from Neuroscience A Pain Theory Revolution Was Happening
On returning to university (SHU) in 1996 faculty of Biomedical Science I found
bull Pain theory was a hot topic
bull Biomedical model was being overthrown by the lsquoBiopsychosocialrsquo bull A number of landmark discoveries had been made in the 80rsquos
bull Knowledge was largely contained within the academic world of neuroscience
Louis Gifford M App Sc BSc MCSP
httpwwwachesandpainsonlinecomaboutusphp
It is not an exaggeration to say that this book marks a milestone not only for an understanding of pain but also for the maturation of physiotherapy Professor Patrick Wall (1925 ndash 2001) Review 1998
Subsequently adopted as core reading for post graduate and undergraduate training programmes in the UK and abroad
Research Physiotherapist international lecturer Author of the Yearbooks of the Physiotherapy Pain Association (1994) for Chartered Physiotherapists
David Butler M App Sc (NOI)
Physiotherapist international freelance educator senior lecturer at the University of South Australia and a director of the NOI
httpwwwactuariesasnauACS2011ProgramPlenarySpeakersaspx
ldquoI believe the ideal approach in the clinic should be one that encompasses three things the best skills from current therapy the best information from science and the best therapeutic relationship
with a particular patientrdquo
Integrating pain awareness into physiotherapy-wise action for the future In Gifford Topical Issues in Pain 1 1998
Sensory Receptor Afferent Nerve (Axon) C
Mechanoreceptors Touch
Thermoreceptors Cold Warm
Photoreceptors Colour Light
Audioreceptors Sound
Chemoreceptors Taste Smell
Proprioreceptors Position etc body parts
Interoreceptors eg Baroreceptors Osmoreceptors
Nociceptors (Mechano ndash Chemo) Pain
Exteroreceptors enable us to make sense of the External Physical World
Sensation amp Perception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
5
Everything we See Hear Taste and Smell and feel as Touch or Pain Exists in our brains
ldquoWe acknowledge that all the individual features of the world are experienced through our sense organs The information that reaches us through those organs is converted into electrical signals and the individual parts of our brain analyze and process these signals After this interpreting process takes place inside our brain we will for example see a book taste a strawberry smell a flower feel the texture of a silk fabric or hear leaves shaking in the windrdquo
httpwwwsecretbeyondmattercomourbrainstheworldinourbrainshtml
Stimulus Electrical Signal
Meaning
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Nociception
To brain
Zone of Lissauer
Substantia gelatinosa
Dorsal root
DRG
Ventral root
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Pain Cannot Exist Outside of Consciousness
Nociception
Nociception Can Occur Without the Brain
When we Stub Our Toe it Hurts But only because Our Brain Says so
INJURY
PAIN
bull Damage has Occurred bull It has been Inflicted on the Toe bull Something Needs to be Done
(raise foot hobble utter expletive)
The Brain Decides
httpwwwwellcomeacukenpainmicrositescience2html
httparchivesciencewatchcomdrfmf201111mayf
mf11mayfmfCrai
AD (Bud) Craig Principal InvestigatorDirector Atkinson Pain Research Laboratory Barrow Neurological Institute Phoenix
When we Stub Our Toe it Hurts But only because Our Brain Says so
INJURY
PAIN
ldquoIt may feel as if our toe is throbbing but the experience is all contained within a mental projection of the
condition of our toe within our brainrdquo
httpwwwwellcomeacukenpainmicrositescience2html
httparchivesciencewatchcomdrfmf201111mayf
mf11mayfmfCrai
AD (Bud) Craig Principal InvestigatorDirector Atkinson Pain Research Laboratory Barrow Neurological Institute Phoenix
httpgoldsmithsacademiaeduMaxVelmansPapers980457Physical_psychological_and_virtual_realities
Neural Activity (In The Brain) Can Result In Spatially Located
Extended Experiences
ldquoPerceptual processing in the brain can result in experiences that have a subjective location and extension beyond the brain In
Velmans (1990) I have called this phenomenon perceptual projection How spatial encodings and other encodings in the
brain are translated into such spatial phenomenology are matters for scientific researchrdquo Max Velmans
Max Velmans is an Emeritus Professor of Psychology at Goldsmiths University of London
httpwwwspracukexpcmsindexphpsection=87
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
6
ldquoThe localisation of pain (and other tactile sensation) is a projection from the brain into 3-dimensional space To facilitate
this the brain makes use of a map of the body surface and lsquoperipersonal spacersquo ldquo
2012
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Perceived Pain in the Tissues is an Illusion Created by the Brain
Somatotopy Somatotopy The correspondence between the position of a receptor in part of
the body and the corresponding area of the cerebral cortex that is activated by it
httpneurocriticblogspotcouk2009_08_01_archivehtml
Penfieldrsquos Somatosensory Homunculus
httpwwwmadscientistblogcamad-scientist-5-
paracelsus-pt-2-paracelsus-homunculus
httpmvameeducationalbrain_areashtml
Neurosurgeon Wilder Penfield (1891ndash1976)mapped the body onto the brain by electrically stimulating the cortex of over 400 conscious epileptic patients and
noting their responses
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
ldquoMicro-electrode stimulation of the somatosensory cortex produces feelings of numbness and tingling which are
subjectively located in different regions of the body not in the brainmdashanother clear case of perceptual projectionrdquo
Max Velmans
2013
Sudden Pain-Related Signals need to be rapidly transformed into External Spatial Coordinates to facilitate defensive reactions and prevent tissue
damage Pain localisation appears to take place in S1 co-localised with touch and in the Insular Cortex where there is more lsquocoarsersquo somatotopic
representation of pain
Insular Cortex
S1 M1
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
7
The Posterior Parietal Cortex houses lsquoExternal Spatial Representationrsquo It Remaps touch from a Somatatopic to a lsquoSpatiotopicrsquo external spatial frame of
reference by integrating touch with proprioceptive information about body posture This area about the body is called lsquoPeripersonal Spacersquo
2010 S1 M1 Important Points ndash Pain Perception
bull Percieved pain is an illusion lsquoprojectedrsquo by the brain
bull Nociception arises in the tissues
bull Nociception can exist without pain
bull Pain can exist without nociception
bull Pain is generated in the brain
bull To the patient the whole pain experience is contained within the tissues
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors High Threshold Gated Ion Channels on Free Nerve Endings
Location
Externally Skin
Cornea Mucosa
Internally Muscles
Joints Bladder Gut etc
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors amp LT Mechanoreceptors
TOUCH
PAIN
Pain amp Touch information travel to the brain in different Tracts ndash Dorsal Columns and Spinothalamic Tracts respectively
Schematic of ion channels in nociceptor function
Mechanical Noxious Cold ndash (lt5C) Protons (Acid-sensing-ion channel) Noxious Heat ndash (gt42C) Serotonin ATP Nerve Growth Factor Chemicals (G-protein-coupled receptors) eg histamine bradykinin prostaglandins
Capsaicin found in ldquoHotrdquo Peppers such as Red Chillies and Jalapenos is able to selectively activate the Trpv1 receptor and thus provides a
means of inducing pain experimentally without tissue damage
C
Stimulators of Nociception
Nociceptor Nociception (Axon)
Brain
Nociceptor Activators Mechanical pressure Thermal stimuli (gt42C lt5C) Chemical (inflammatory mediators or products of damaged cells) Potassium ions ATP Protons (acidity hypoxia) Histamine Serotonin Bradykinin
Nociceptor Sensitisers Chemical (released from damaged tissue or axon reflex) Prostaglandins Cytokines Substance P CGRP
Transduction Pain Conduction
Neuropeptides
CGRP = Calcitonin Gene Related Peptide
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
8
Axon Reflex ndash Neurogenic Inflammation Neuropeptides (eg Substance P CGRP) and Inflammation
Action potentials in branches of an afferent nociceptor can move
peripherallyThis is called the axon reflex The release of substance P and CGRP (sensitises) increases inflammation by causing histamine
release and dilation of blood vessels
httpcourseswashingtoneduconjsensorypainhtm
Mechanisms Associated with Peripheral Sensitisation to Pain
After an injury occurs there is a time-dependent expansion in the area of sensitivity as tissue that is not damaged becomes increasingly sensitive to any sort of stimulus that is applied This is called HYPERALGESIA
wwwpagesdrexeledu~mab337Pain20Lectureppt
C Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Peripheral Sensitisation (Hyperalgesia)
If there is tissue injury diffusion of the lsquoinflammatory souprsquo activates adjacent nociceptors causing the painful tender area to
expand The barrage of nociception is then the source of pathophysiological pain
Injury
A Critical Number of Open Sensors will Start the Response
Acute_Pain_Normal
httptriactionpotentialblogspotcom
Movie Clip ndash Key Points
Injury
Inflammatory Reaction
Electrical Signal - Fast Ad and Slow C Fibre Nociceptors
Dorsal Horn
Spinothalamic Tract
Thalamus
Cortex Frontal Lobe Limbic System
PERCEPTION - Texture amp Intensity Emotional Impact Link to Memory Meaning
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
9
Fast Ad Fibre Pain bull Sharp and well localised bull Nociceptive impulses synapse in the dorsal horn initiate withdrawal reflexes and travel to the sensory cortex via the thalamus
Slow C Fibre Pain bull Diffuse more burning and unpleasant ndash lingers bull Nociceptive impulses synapse with interneurons in the dorsal horn then travel to
1) Sensory cortex and insular cortex 2) Limbic System ndash memory and emotion 3) Hypothalamus (ANS) and brain stem
Only C fibres respond to Chemical stimulation
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Can be Referred to as Projection Neurons
Dorsal Horn Neurons 2nd Order Neurons
httpwwwrnceuscomagesnociceptivehtm
They arise from Lamina 1 as Nociception
Specific (NS) neurons and Lamina V as Wide Dynamic
Ranging (WDR) neurons
NS
WDR
How Mechanoreceptor Activity Can Decrease Nociceptive Processing
(Why Movement and Rubbing Decreases The Perception of Pain)
Melzack and Wallrsquos Pain Gate Theory was the first real challenge to the Pathoanatomical model It postulated that nociception could be lsquomodulatedrsquo at the dorsal horn
and that some lsquointegrationrsquo of nociceptive and other sensory
information could occur
httppublicationsmcgillcaheadwaymagazine
the-king-of-understanding-pain-qa-with-ronald-melzack
naturecom
Ronald Melzack Patrick Wall
1965
R Melzack PD Wall Pain mechanisms a new theory Science 1965150971ndash979
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Many interneurons and interconnections within
the dorsal horn allow integration of different sensory channels Eg Inhibitory interneurons
can be activated by touch and propriceptive input to deep laminae to lsquogatersquo NS
output from lamina 1
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
As Wall himself wrote evaluating the gate theory in the light of further experiments lsquolsquoThe least and perhaps the best that can be said for the 1965
paper is that it provoked discussion and experimentrsquorsquo
2014
Free Access httpwwwsciencedirectcomscience
articlepiiS0306452214007830
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
10
Neurons That Conduct Nociception (Pain Impulses) to the Brain
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
NS neurons are more associated with the emotional suffering
dimension of pain Also autonomic motivational
amp homeostatic responses
WDR neurons are mainly associated with the
sensory discriminative dimension of pain ndash location amp intensity
Spinal Polysynaptic Interneurons (PSINs) (Eg Flexor amp Crossed Extensor Reflex)
httpalexandriahealthlibrarycadocumentsnotesbomunit_6lec2025_moo_spinreflexxml
Withdrawal reflexes are mainly initiated by Ad fibres and involve
interneurons that cross the midline
Other cord level responses effected by nociceptors and interneurons include altered muscle tone and sympathetic effects (sweating vasoconstrictiondilation) via links to the preganglionic cell bodies in the lateral horn
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Experiment to Demonstate Secondary Hyperalgesia with Capsaicin induced Nociception
Nerve Block (local anaesthetic)
Nerve Block
Capsaicin
Amplification
R L R L
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Amplifier
Injury
Discovery of the dorsal horn amplifier proved that the pain circuitry exhibits lsquoactivity-dependent-synaptic-plasticityrsquo It is not
hard-wired
Clifford Woolf Discovered central sensitization whilst researching at University College London alongside Patrick Wall and published his findings in 1983 (Woolf CJ Evidence for a central component of post-injury pain hypersensitivity Nature 1983 306686-8)
ldquo pain does not simply reflect the presence intensity or duration of specific lsquopainrsquo stimuli in the periphery but also changes in the
function of the central nervous systemrdquo
Woolf CJ Central sensitization ndashuncovering the relation between pain and plasticity Anesthesiology 2007106864-7
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
11
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
C
C
C C
C C
C
C
C C
C C C
C
C C C
C
Peripheral amp Central Sensitisation Stimulus
Injury + Inflammation
Dorsal Horn Amplification
Amplification In The Brain
PNS CNS
C
C
C
C C C
C Peripheral amp Central Sensitisation
As Inflammation Resolves Peripheral Sensitisation dies down but Central Sensitisation
sometimes persists to be the cause of Chronic pain
lsquoNormallyrsquo ndash Pain goes
lsquoPathologicalrsquo ndash Pain becomes Chronic Brain continues to generate pain Cortical Reorganisation
Dorsal Horn Amplifier stays on High Gain
PAIN
Important Points ndash Pain Sensitisation
bull Peripheral sensitisation drives central sensitisation
bull Secondary hyperalgesia (central sensitisation) gives additional warning of the need to protect the injured anatomy whilst it is inflamed thus assisting healing
bull Perceived worsening pain and an often massive spread of tenderness into multiple tissues is mainly on account of central sensitisation These tissues are not all injured
bull Pain circuitry is not hard-wired
bull Spreading pain is lsquobeyond dermatomesrsquo
Glutamate amp NMDA Receptors Main Neurotransmitter Released by C Fibres
During prolonged excitation the sum of EPSPs lowers the membrane potential sufficiently for the NMDA channels to expel their magnesium molecule allowing an influx of Ca2+ This triggers the release of retrograde messengers that stimulate the
release of more glutamate from the pre-synaptic membrane This all leads to a greater response from the secondary nerve
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Glutamate normally opens only AMPA channels because NMDA channels are blocked by a magnesium molecule
Substance P Sensitising Neuropeptides Also Released by C Fibres
Subtance P and CGRP sensitise the secondary nerve to glutamate Within the dorsal horn these can diffuse around several levels of the spinal cord sensitising
other secondary nerves (dorsal horn neurons) in the process
What was previously an innocuous stimulus may now be perceived as pain and pain may be perceived at a seemingly unrelated anatomical site
Substance P
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
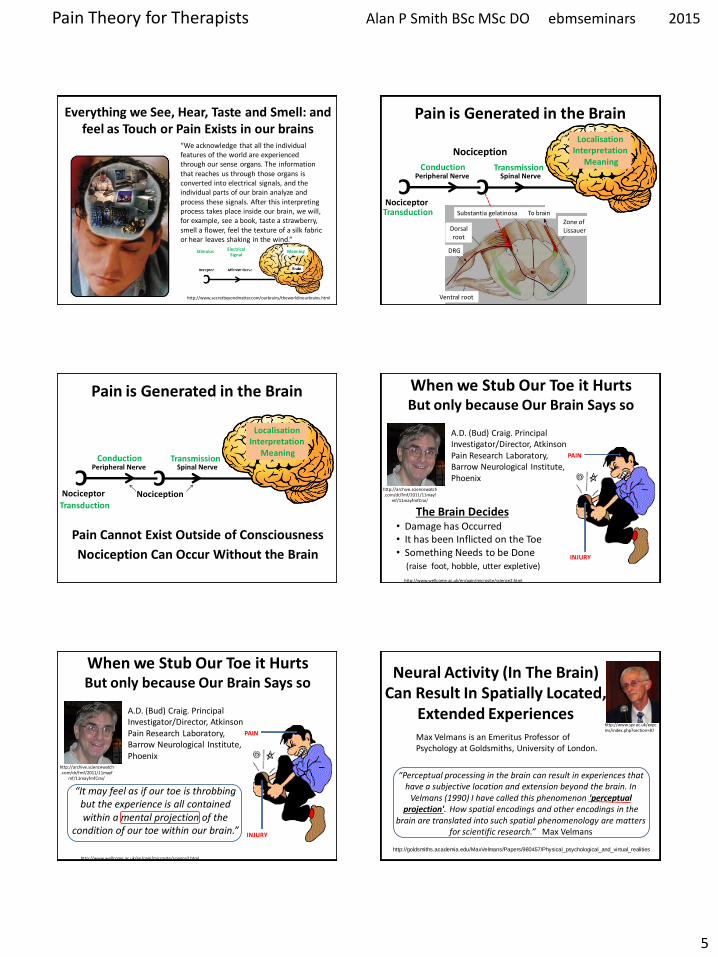
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
5
Everything we See Hear Taste and Smell and feel as Touch or Pain Exists in our brains
ldquoWe acknowledge that all the individual features of the world are experienced through our sense organs The information that reaches us through those organs is converted into electrical signals and the individual parts of our brain analyze and process these signals After this interpreting process takes place inside our brain we will for example see a book taste a strawberry smell a flower feel the texture of a silk fabric or hear leaves shaking in the windrdquo
httpwwwsecretbeyondmattercomourbrainstheworldinourbrainshtml
Stimulus Electrical Signal
Meaning
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Nociception
To brain
Zone of Lissauer
Substantia gelatinosa
Dorsal root
DRG
Ventral root
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Pain Cannot Exist Outside of Consciousness
Nociception
Nociception Can Occur Without the Brain
When we Stub Our Toe it Hurts But only because Our Brain Says so
INJURY
PAIN
bull Damage has Occurred bull It has been Inflicted on the Toe bull Something Needs to be Done
(raise foot hobble utter expletive)
The Brain Decides
httpwwwwellcomeacukenpainmicrositescience2html
httparchivesciencewatchcomdrfmf201111mayf
mf11mayfmfCrai
AD (Bud) Craig Principal InvestigatorDirector Atkinson Pain Research Laboratory Barrow Neurological Institute Phoenix
When we Stub Our Toe it Hurts But only because Our Brain Says so
INJURY
PAIN
ldquoIt may feel as if our toe is throbbing but the experience is all contained within a mental projection of the
condition of our toe within our brainrdquo
httpwwwwellcomeacukenpainmicrositescience2html
httparchivesciencewatchcomdrfmf201111mayf
mf11mayfmfCrai
AD (Bud) Craig Principal InvestigatorDirector Atkinson Pain Research Laboratory Barrow Neurological Institute Phoenix
httpgoldsmithsacademiaeduMaxVelmansPapers980457Physical_psychological_and_virtual_realities
Neural Activity (In The Brain) Can Result In Spatially Located
Extended Experiences
ldquoPerceptual processing in the brain can result in experiences that have a subjective location and extension beyond the brain In
Velmans (1990) I have called this phenomenon perceptual projection How spatial encodings and other encodings in the
brain are translated into such spatial phenomenology are matters for scientific researchrdquo Max Velmans
Max Velmans is an Emeritus Professor of Psychology at Goldsmiths University of London
httpwwwspracukexpcmsindexphpsection=87
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
6
ldquoThe localisation of pain (and other tactile sensation) is a projection from the brain into 3-dimensional space To facilitate
this the brain makes use of a map of the body surface and lsquoperipersonal spacersquo ldquo
2012
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Perceived Pain in the Tissues is an Illusion Created by the Brain
Somatotopy Somatotopy The correspondence between the position of a receptor in part of
the body and the corresponding area of the cerebral cortex that is activated by it
httpneurocriticblogspotcouk2009_08_01_archivehtml
Penfieldrsquos Somatosensory Homunculus
httpwwwmadscientistblogcamad-scientist-5-
paracelsus-pt-2-paracelsus-homunculus
httpmvameeducationalbrain_areashtml
Neurosurgeon Wilder Penfield (1891ndash1976)mapped the body onto the brain by electrically stimulating the cortex of over 400 conscious epileptic patients and
noting their responses
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
ldquoMicro-electrode stimulation of the somatosensory cortex produces feelings of numbness and tingling which are
subjectively located in different regions of the body not in the brainmdashanother clear case of perceptual projectionrdquo
Max Velmans
2013
Sudden Pain-Related Signals need to be rapidly transformed into External Spatial Coordinates to facilitate defensive reactions and prevent tissue
damage Pain localisation appears to take place in S1 co-localised with touch and in the Insular Cortex where there is more lsquocoarsersquo somatotopic
representation of pain
Insular Cortex
S1 M1
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
7
The Posterior Parietal Cortex houses lsquoExternal Spatial Representationrsquo It Remaps touch from a Somatatopic to a lsquoSpatiotopicrsquo external spatial frame of
reference by integrating touch with proprioceptive information about body posture This area about the body is called lsquoPeripersonal Spacersquo
2010 S1 M1 Important Points ndash Pain Perception
bull Percieved pain is an illusion lsquoprojectedrsquo by the brain
bull Nociception arises in the tissues
bull Nociception can exist without pain
bull Pain can exist without nociception
bull Pain is generated in the brain
bull To the patient the whole pain experience is contained within the tissues
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors High Threshold Gated Ion Channels on Free Nerve Endings
Location
Externally Skin
Cornea Mucosa
Internally Muscles
Joints Bladder Gut etc
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors amp LT Mechanoreceptors
TOUCH
PAIN
Pain amp Touch information travel to the brain in different Tracts ndash Dorsal Columns and Spinothalamic Tracts respectively
Schematic of ion channels in nociceptor function
Mechanical Noxious Cold ndash (lt5C) Protons (Acid-sensing-ion channel) Noxious Heat ndash (gt42C) Serotonin ATP Nerve Growth Factor Chemicals (G-protein-coupled receptors) eg histamine bradykinin prostaglandins
Capsaicin found in ldquoHotrdquo Peppers such as Red Chillies and Jalapenos is able to selectively activate the Trpv1 receptor and thus provides a
means of inducing pain experimentally without tissue damage
C
Stimulators of Nociception
Nociceptor Nociception (Axon)
Brain
Nociceptor Activators Mechanical pressure Thermal stimuli (gt42C lt5C) Chemical (inflammatory mediators or products of damaged cells) Potassium ions ATP Protons (acidity hypoxia) Histamine Serotonin Bradykinin
Nociceptor Sensitisers Chemical (released from damaged tissue or axon reflex) Prostaglandins Cytokines Substance P CGRP
Transduction Pain Conduction
Neuropeptides
CGRP = Calcitonin Gene Related Peptide
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
8
Axon Reflex ndash Neurogenic Inflammation Neuropeptides (eg Substance P CGRP) and Inflammation
Action potentials in branches of an afferent nociceptor can move
peripherallyThis is called the axon reflex The release of substance P and CGRP (sensitises) increases inflammation by causing histamine
release and dilation of blood vessels
httpcourseswashingtoneduconjsensorypainhtm
Mechanisms Associated with Peripheral Sensitisation to Pain
After an injury occurs there is a time-dependent expansion in the area of sensitivity as tissue that is not damaged becomes increasingly sensitive to any sort of stimulus that is applied This is called HYPERALGESIA
wwwpagesdrexeledu~mab337Pain20Lectureppt
C Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Peripheral Sensitisation (Hyperalgesia)
If there is tissue injury diffusion of the lsquoinflammatory souprsquo activates adjacent nociceptors causing the painful tender area to
expand The barrage of nociception is then the source of pathophysiological pain
Injury
A Critical Number of Open Sensors will Start the Response
Acute_Pain_Normal
httptriactionpotentialblogspotcom
Movie Clip ndash Key Points
Injury
Inflammatory Reaction
Electrical Signal - Fast Ad and Slow C Fibre Nociceptors
Dorsal Horn
Spinothalamic Tract
Thalamus
Cortex Frontal Lobe Limbic System
PERCEPTION - Texture amp Intensity Emotional Impact Link to Memory Meaning
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
9
Fast Ad Fibre Pain bull Sharp and well localised bull Nociceptive impulses synapse in the dorsal horn initiate withdrawal reflexes and travel to the sensory cortex via the thalamus
Slow C Fibre Pain bull Diffuse more burning and unpleasant ndash lingers bull Nociceptive impulses synapse with interneurons in the dorsal horn then travel to
1) Sensory cortex and insular cortex 2) Limbic System ndash memory and emotion 3) Hypothalamus (ANS) and brain stem
Only C fibres respond to Chemical stimulation
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Can be Referred to as Projection Neurons
Dorsal Horn Neurons 2nd Order Neurons
httpwwwrnceuscomagesnociceptivehtm
They arise from Lamina 1 as Nociception
Specific (NS) neurons and Lamina V as Wide Dynamic
Ranging (WDR) neurons
NS
WDR
How Mechanoreceptor Activity Can Decrease Nociceptive Processing
(Why Movement and Rubbing Decreases The Perception of Pain)
Melzack and Wallrsquos Pain Gate Theory was the first real challenge to the Pathoanatomical model It postulated that nociception could be lsquomodulatedrsquo at the dorsal horn
and that some lsquointegrationrsquo of nociceptive and other sensory
information could occur
httppublicationsmcgillcaheadwaymagazine
the-king-of-understanding-pain-qa-with-ronald-melzack
naturecom
Ronald Melzack Patrick Wall
1965
R Melzack PD Wall Pain mechanisms a new theory Science 1965150971ndash979
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Many interneurons and interconnections within
the dorsal horn allow integration of different sensory channels Eg Inhibitory interneurons
can be activated by touch and propriceptive input to deep laminae to lsquogatersquo NS
output from lamina 1
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
As Wall himself wrote evaluating the gate theory in the light of further experiments lsquolsquoThe least and perhaps the best that can be said for the 1965
paper is that it provoked discussion and experimentrsquorsquo
2014
Free Access httpwwwsciencedirectcomscience
articlepiiS0306452214007830
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
10
Neurons That Conduct Nociception (Pain Impulses) to the Brain
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
NS neurons are more associated with the emotional suffering
dimension of pain Also autonomic motivational
amp homeostatic responses
WDR neurons are mainly associated with the
sensory discriminative dimension of pain ndash location amp intensity
Spinal Polysynaptic Interneurons (PSINs) (Eg Flexor amp Crossed Extensor Reflex)
httpalexandriahealthlibrarycadocumentsnotesbomunit_6lec2025_moo_spinreflexxml
Withdrawal reflexes are mainly initiated by Ad fibres and involve
interneurons that cross the midline
Other cord level responses effected by nociceptors and interneurons include altered muscle tone and sympathetic effects (sweating vasoconstrictiondilation) via links to the preganglionic cell bodies in the lateral horn
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Experiment to Demonstate Secondary Hyperalgesia with Capsaicin induced Nociception
Nerve Block (local anaesthetic)
Nerve Block
Capsaicin
Amplification
R L R L
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Amplifier
Injury
Discovery of the dorsal horn amplifier proved that the pain circuitry exhibits lsquoactivity-dependent-synaptic-plasticityrsquo It is not
hard-wired
Clifford Woolf Discovered central sensitization whilst researching at University College London alongside Patrick Wall and published his findings in 1983 (Woolf CJ Evidence for a central component of post-injury pain hypersensitivity Nature 1983 306686-8)
ldquo pain does not simply reflect the presence intensity or duration of specific lsquopainrsquo stimuli in the periphery but also changes in the
function of the central nervous systemrdquo
Woolf CJ Central sensitization ndashuncovering the relation between pain and plasticity Anesthesiology 2007106864-7
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
11
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
C
C
C C
C C
C
C
C C
C C C
C
C C C
C
Peripheral amp Central Sensitisation Stimulus
Injury + Inflammation
Dorsal Horn Amplification
Amplification In The Brain
PNS CNS
C
C
C
C C C
C Peripheral amp Central Sensitisation
As Inflammation Resolves Peripheral Sensitisation dies down but Central Sensitisation
sometimes persists to be the cause of Chronic pain
lsquoNormallyrsquo ndash Pain goes
lsquoPathologicalrsquo ndash Pain becomes Chronic Brain continues to generate pain Cortical Reorganisation
Dorsal Horn Amplifier stays on High Gain
PAIN
Important Points ndash Pain Sensitisation
bull Peripheral sensitisation drives central sensitisation
bull Secondary hyperalgesia (central sensitisation) gives additional warning of the need to protect the injured anatomy whilst it is inflamed thus assisting healing
bull Perceived worsening pain and an often massive spread of tenderness into multiple tissues is mainly on account of central sensitisation These tissues are not all injured
bull Pain circuitry is not hard-wired
bull Spreading pain is lsquobeyond dermatomesrsquo
Glutamate amp NMDA Receptors Main Neurotransmitter Released by C Fibres
During prolonged excitation the sum of EPSPs lowers the membrane potential sufficiently for the NMDA channels to expel their magnesium molecule allowing an influx of Ca2+ This triggers the release of retrograde messengers that stimulate the
release of more glutamate from the pre-synaptic membrane This all leads to a greater response from the secondary nerve
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Glutamate normally opens only AMPA channels because NMDA channels are blocked by a magnesium molecule
Substance P Sensitising Neuropeptides Also Released by C Fibres
Subtance P and CGRP sensitise the secondary nerve to glutamate Within the dorsal horn these can diffuse around several levels of the spinal cord sensitising
other secondary nerves (dorsal horn neurons) in the process
What was previously an innocuous stimulus may now be perceived as pain and pain may be perceived at a seemingly unrelated anatomical site
Substance P
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
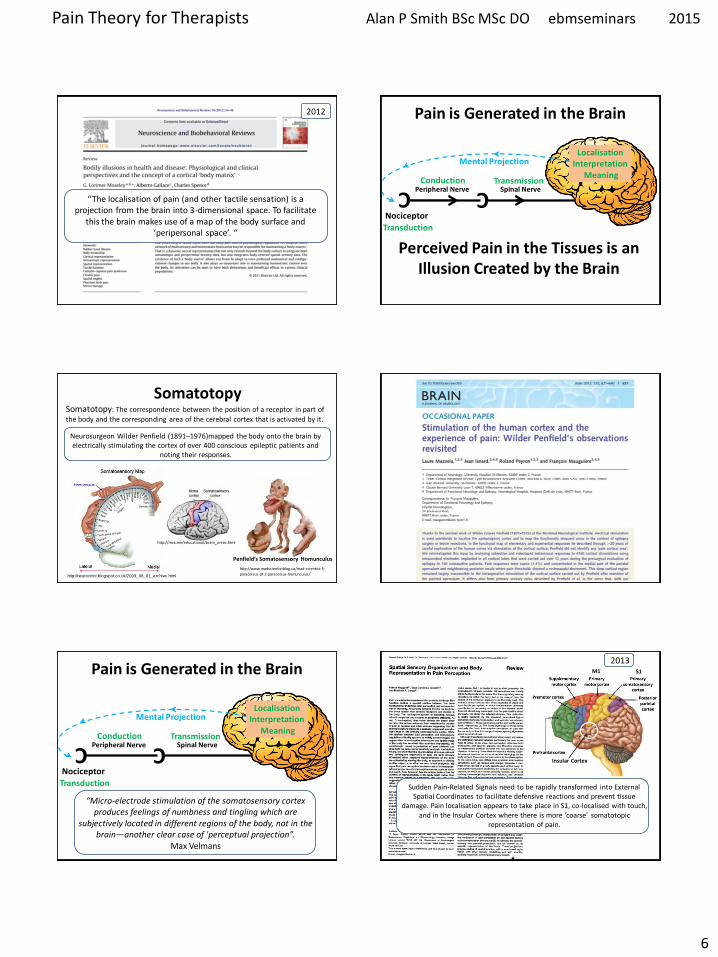
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
6
ldquoThe localisation of pain (and other tactile sensation) is a projection from the brain into 3-dimensional space To facilitate
this the brain makes use of a map of the body surface and lsquoperipersonal spacersquo ldquo
2012
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Perceived Pain in the Tissues is an Illusion Created by the Brain
Somatotopy Somatotopy The correspondence between the position of a receptor in part of
the body and the corresponding area of the cerebral cortex that is activated by it
httpneurocriticblogspotcouk2009_08_01_archivehtml
Penfieldrsquos Somatosensory Homunculus
httpwwwmadscientistblogcamad-scientist-5-
paracelsus-pt-2-paracelsus-homunculus
httpmvameeducationalbrain_areashtml
Neurosurgeon Wilder Penfield (1891ndash1976)mapped the body onto the brain by electrically stimulating the cortex of over 400 conscious epileptic patients and
noting their responses
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
ldquoMicro-electrode stimulation of the somatosensory cortex produces feelings of numbness and tingling which are
subjectively located in different regions of the body not in the brainmdashanother clear case of perceptual projectionrdquo
Max Velmans
2013
Sudden Pain-Related Signals need to be rapidly transformed into External Spatial Coordinates to facilitate defensive reactions and prevent tissue
damage Pain localisation appears to take place in S1 co-localised with touch and in the Insular Cortex where there is more lsquocoarsersquo somatotopic
representation of pain
Insular Cortex
S1 M1
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
7
The Posterior Parietal Cortex houses lsquoExternal Spatial Representationrsquo It Remaps touch from a Somatatopic to a lsquoSpatiotopicrsquo external spatial frame of
reference by integrating touch with proprioceptive information about body posture This area about the body is called lsquoPeripersonal Spacersquo
2010 S1 M1 Important Points ndash Pain Perception
bull Percieved pain is an illusion lsquoprojectedrsquo by the brain
bull Nociception arises in the tissues
bull Nociception can exist without pain
bull Pain can exist without nociception
bull Pain is generated in the brain
bull To the patient the whole pain experience is contained within the tissues
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors High Threshold Gated Ion Channels on Free Nerve Endings
Location
Externally Skin
Cornea Mucosa
Internally Muscles
Joints Bladder Gut etc
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors amp LT Mechanoreceptors
TOUCH
PAIN
Pain amp Touch information travel to the brain in different Tracts ndash Dorsal Columns and Spinothalamic Tracts respectively
Schematic of ion channels in nociceptor function
Mechanical Noxious Cold ndash (lt5C) Protons (Acid-sensing-ion channel) Noxious Heat ndash (gt42C) Serotonin ATP Nerve Growth Factor Chemicals (G-protein-coupled receptors) eg histamine bradykinin prostaglandins
Capsaicin found in ldquoHotrdquo Peppers such as Red Chillies and Jalapenos is able to selectively activate the Trpv1 receptor and thus provides a
means of inducing pain experimentally without tissue damage
C
Stimulators of Nociception
Nociceptor Nociception (Axon)
Brain
Nociceptor Activators Mechanical pressure Thermal stimuli (gt42C lt5C) Chemical (inflammatory mediators or products of damaged cells) Potassium ions ATP Protons (acidity hypoxia) Histamine Serotonin Bradykinin
Nociceptor Sensitisers Chemical (released from damaged tissue or axon reflex) Prostaglandins Cytokines Substance P CGRP
Transduction Pain Conduction
Neuropeptides
CGRP = Calcitonin Gene Related Peptide
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
8
Axon Reflex ndash Neurogenic Inflammation Neuropeptides (eg Substance P CGRP) and Inflammation
Action potentials in branches of an afferent nociceptor can move
peripherallyThis is called the axon reflex The release of substance P and CGRP (sensitises) increases inflammation by causing histamine
release and dilation of blood vessels
httpcourseswashingtoneduconjsensorypainhtm
Mechanisms Associated with Peripheral Sensitisation to Pain
After an injury occurs there is a time-dependent expansion in the area of sensitivity as tissue that is not damaged becomes increasingly sensitive to any sort of stimulus that is applied This is called HYPERALGESIA
wwwpagesdrexeledu~mab337Pain20Lectureppt
C Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Peripheral Sensitisation (Hyperalgesia)
If there is tissue injury diffusion of the lsquoinflammatory souprsquo activates adjacent nociceptors causing the painful tender area to
expand The barrage of nociception is then the source of pathophysiological pain
Injury
A Critical Number of Open Sensors will Start the Response
Acute_Pain_Normal
httptriactionpotentialblogspotcom
Movie Clip ndash Key Points
Injury
Inflammatory Reaction
Electrical Signal - Fast Ad and Slow C Fibre Nociceptors
Dorsal Horn
Spinothalamic Tract
Thalamus
Cortex Frontal Lobe Limbic System
PERCEPTION - Texture amp Intensity Emotional Impact Link to Memory Meaning
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
9
Fast Ad Fibre Pain bull Sharp and well localised bull Nociceptive impulses synapse in the dorsal horn initiate withdrawal reflexes and travel to the sensory cortex via the thalamus
Slow C Fibre Pain bull Diffuse more burning and unpleasant ndash lingers bull Nociceptive impulses synapse with interneurons in the dorsal horn then travel to
1) Sensory cortex and insular cortex 2) Limbic System ndash memory and emotion 3) Hypothalamus (ANS) and brain stem
Only C fibres respond to Chemical stimulation
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Can be Referred to as Projection Neurons
Dorsal Horn Neurons 2nd Order Neurons
httpwwwrnceuscomagesnociceptivehtm
They arise from Lamina 1 as Nociception
Specific (NS) neurons and Lamina V as Wide Dynamic
Ranging (WDR) neurons
NS
WDR
How Mechanoreceptor Activity Can Decrease Nociceptive Processing
(Why Movement and Rubbing Decreases The Perception of Pain)
Melzack and Wallrsquos Pain Gate Theory was the first real challenge to the Pathoanatomical model It postulated that nociception could be lsquomodulatedrsquo at the dorsal horn
and that some lsquointegrationrsquo of nociceptive and other sensory
information could occur
httppublicationsmcgillcaheadwaymagazine
the-king-of-understanding-pain-qa-with-ronald-melzack
naturecom
Ronald Melzack Patrick Wall
1965
R Melzack PD Wall Pain mechanisms a new theory Science 1965150971ndash979
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Many interneurons and interconnections within
the dorsal horn allow integration of different sensory channels Eg Inhibitory interneurons
can be activated by touch and propriceptive input to deep laminae to lsquogatersquo NS
output from lamina 1
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
As Wall himself wrote evaluating the gate theory in the light of further experiments lsquolsquoThe least and perhaps the best that can be said for the 1965
paper is that it provoked discussion and experimentrsquorsquo
2014
Free Access httpwwwsciencedirectcomscience
articlepiiS0306452214007830
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
10
Neurons That Conduct Nociception (Pain Impulses) to the Brain
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
NS neurons are more associated with the emotional suffering
dimension of pain Also autonomic motivational
amp homeostatic responses
WDR neurons are mainly associated with the
sensory discriminative dimension of pain ndash location amp intensity
Spinal Polysynaptic Interneurons (PSINs) (Eg Flexor amp Crossed Extensor Reflex)
httpalexandriahealthlibrarycadocumentsnotesbomunit_6lec2025_moo_spinreflexxml
Withdrawal reflexes are mainly initiated by Ad fibres and involve
interneurons that cross the midline
Other cord level responses effected by nociceptors and interneurons include altered muscle tone and sympathetic effects (sweating vasoconstrictiondilation) via links to the preganglionic cell bodies in the lateral horn
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Experiment to Demonstate Secondary Hyperalgesia with Capsaicin induced Nociception
Nerve Block (local anaesthetic)
Nerve Block
Capsaicin
Amplification
R L R L
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Amplifier
Injury
Discovery of the dorsal horn amplifier proved that the pain circuitry exhibits lsquoactivity-dependent-synaptic-plasticityrsquo It is not
hard-wired
Clifford Woolf Discovered central sensitization whilst researching at University College London alongside Patrick Wall and published his findings in 1983 (Woolf CJ Evidence for a central component of post-injury pain hypersensitivity Nature 1983 306686-8)
ldquo pain does not simply reflect the presence intensity or duration of specific lsquopainrsquo stimuli in the periphery but also changes in the
function of the central nervous systemrdquo
Woolf CJ Central sensitization ndashuncovering the relation between pain and plasticity Anesthesiology 2007106864-7
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
11
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
C
C
C C
C C
C
C
C C
C C C
C
C C C
C
Peripheral amp Central Sensitisation Stimulus
Injury + Inflammation
Dorsal Horn Amplification
Amplification In The Brain
PNS CNS
C
C
C
C C C
C Peripheral amp Central Sensitisation
As Inflammation Resolves Peripheral Sensitisation dies down but Central Sensitisation
sometimes persists to be the cause of Chronic pain
lsquoNormallyrsquo ndash Pain goes
lsquoPathologicalrsquo ndash Pain becomes Chronic Brain continues to generate pain Cortical Reorganisation
Dorsal Horn Amplifier stays on High Gain
PAIN
Important Points ndash Pain Sensitisation
bull Peripheral sensitisation drives central sensitisation
bull Secondary hyperalgesia (central sensitisation) gives additional warning of the need to protect the injured anatomy whilst it is inflamed thus assisting healing
bull Perceived worsening pain and an often massive spread of tenderness into multiple tissues is mainly on account of central sensitisation These tissues are not all injured
bull Pain circuitry is not hard-wired
bull Spreading pain is lsquobeyond dermatomesrsquo
Glutamate amp NMDA Receptors Main Neurotransmitter Released by C Fibres
During prolonged excitation the sum of EPSPs lowers the membrane potential sufficiently for the NMDA channels to expel their magnesium molecule allowing an influx of Ca2+ This triggers the release of retrograde messengers that stimulate the
release of more glutamate from the pre-synaptic membrane This all leads to a greater response from the secondary nerve
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Glutamate normally opens only AMPA channels because NMDA channels are blocked by a magnesium molecule
Substance P Sensitising Neuropeptides Also Released by C Fibres
Subtance P and CGRP sensitise the secondary nerve to glutamate Within the dorsal horn these can diffuse around several levels of the spinal cord sensitising
other secondary nerves (dorsal horn neurons) in the process
What was previously an innocuous stimulus may now be perceived as pain and pain may be perceived at a seemingly unrelated anatomical site
Substance P
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
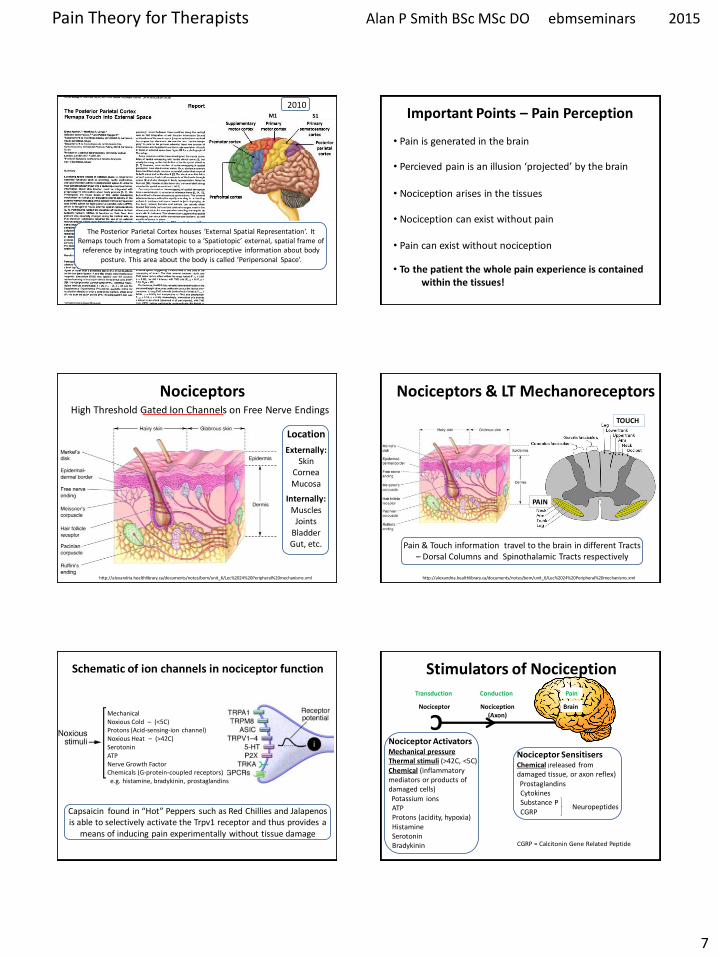
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
7
The Posterior Parietal Cortex houses lsquoExternal Spatial Representationrsquo It Remaps touch from a Somatatopic to a lsquoSpatiotopicrsquo external spatial frame of
reference by integrating touch with proprioceptive information about body posture This area about the body is called lsquoPeripersonal Spacersquo
2010 S1 M1 Important Points ndash Pain Perception
bull Percieved pain is an illusion lsquoprojectedrsquo by the brain
bull Nociception arises in the tissues
bull Nociception can exist without pain
bull Pain can exist without nociception
bull Pain is generated in the brain
bull To the patient the whole pain experience is contained within the tissues
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors High Threshold Gated Ion Channels on Free Nerve Endings
Location
Externally Skin
Cornea Mucosa
Internally Muscles
Joints Bladder Gut etc
httpalexandriahealthlibrarycadocumentsnotesbomunit_6Lec202420Peripheral20mechanismsxml
Nociceptors amp LT Mechanoreceptors
TOUCH
PAIN
Pain amp Touch information travel to the brain in different Tracts ndash Dorsal Columns and Spinothalamic Tracts respectively
Schematic of ion channels in nociceptor function
Mechanical Noxious Cold ndash (lt5C) Protons (Acid-sensing-ion channel) Noxious Heat ndash (gt42C) Serotonin ATP Nerve Growth Factor Chemicals (G-protein-coupled receptors) eg histamine bradykinin prostaglandins
Capsaicin found in ldquoHotrdquo Peppers such as Red Chillies and Jalapenos is able to selectively activate the Trpv1 receptor and thus provides a
means of inducing pain experimentally without tissue damage
C
Stimulators of Nociception
Nociceptor Nociception (Axon)
Brain
Nociceptor Activators Mechanical pressure Thermal stimuli (gt42C lt5C) Chemical (inflammatory mediators or products of damaged cells) Potassium ions ATP Protons (acidity hypoxia) Histamine Serotonin Bradykinin
Nociceptor Sensitisers Chemical (released from damaged tissue or axon reflex) Prostaglandins Cytokines Substance P CGRP
Transduction Pain Conduction
Neuropeptides
CGRP = Calcitonin Gene Related Peptide
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
8
Axon Reflex ndash Neurogenic Inflammation Neuropeptides (eg Substance P CGRP) and Inflammation
Action potentials in branches of an afferent nociceptor can move
peripherallyThis is called the axon reflex The release of substance P and CGRP (sensitises) increases inflammation by causing histamine
release and dilation of blood vessels
httpcourseswashingtoneduconjsensorypainhtm
Mechanisms Associated with Peripheral Sensitisation to Pain
After an injury occurs there is a time-dependent expansion in the area of sensitivity as tissue that is not damaged becomes increasingly sensitive to any sort of stimulus that is applied This is called HYPERALGESIA
wwwpagesdrexeledu~mab337Pain20Lectureppt
C Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Peripheral Sensitisation (Hyperalgesia)
If there is tissue injury diffusion of the lsquoinflammatory souprsquo activates adjacent nociceptors causing the painful tender area to
expand The barrage of nociception is then the source of pathophysiological pain
Injury
A Critical Number of Open Sensors will Start the Response
Acute_Pain_Normal
httptriactionpotentialblogspotcom
Movie Clip ndash Key Points
Injury
Inflammatory Reaction
Electrical Signal - Fast Ad and Slow C Fibre Nociceptors
Dorsal Horn
Spinothalamic Tract
Thalamus
Cortex Frontal Lobe Limbic System
PERCEPTION - Texture amp Intensity Emotional Impact Link to Memory Meaning
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
9
Fast Ad Fibre Pain bull Sharp and well localised bull Nociceptive impulses synapse in the dorsal horn initiate withdrawal reflexes and travel to the sensory cortex via the thalamus
Slow C Fibre Pain bull Diffuse more burning and unpleasant ndash lingers bull Nociceptive impulses synapse with interneurons in the dorsal horn then travel to
1) Sensory cortex and insular cortex 2) Limbic System ndash memory and emotion 3) Hypothalamus (ANS) and brain stem
Only C fibres respond to Chemical stimulation
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Can be Referred to as Projection Neurons
Dorsal Horn Neurons 2nd Order Neurons
httpwwwrnceuscomagesnociceptivehtm
They arise from Lamina 1 as Nociception
Specific (NS) neurons and Lamina V as Wide Dynamic
Ranging (WDR) neurons
NS
WDR
How Mechanoreceptor Activity Can Decrease Nociceptive Processing
(Why Movement and Rubbing Decreases The Perception of Pain)
Melzack and Wallrsquos Pain Gate Theory was the first real challenge to the Pathoanatomical model It postulated that nociception could be lsquomodulatedrsquo at the dorsal horn
and that some lsquointegrationrsquo of nociceptive and other sensory
information could occur
httppublicationsmcgillcaheadwaymagazine
the-king-of-understanding-pain-qa-with-ronald-melzack
naturecom
Ronald Melzack Patrick Wall
1965
R Melzack PD Wall Pain mechanisms a new theory Science 1965150971ndash979
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Many interneurons and interconnections within
the dorsal horn allow integration of different sensory channels Eg Inhibitory interneurons
can be activated by touch and propriceptive input to deep laminae to lsquogatersquo NS
output from lamina 1
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
As Wall himself wrote evaluating the gate theory in the light of further experiments lsquolsquoThe least and perhaps the best that can be said for the 1965
paper is that it provoked discussion and experimentrsquorsquo
2014
Free Access httpwwwsciencedirectcomscience
articlepiiS0306452214007830
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
10
Neurons That Conduct Nociception (Pain Impulses) to the Brain
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
NS neurons are more associated with the emotional suffering
dimension of pain Also autonomic motivational
amp homeostatic responses
WDR neurons are mainly associated with the
sensory discriminative dimension of pain ndash location amp intensity
Spinal Polysynaptic Interneurons (PSINs) (Eg Flexor amp Crossed Extensor Reflex)
httpalexandriahealthlibrarycadocumentsnotesbomunit_6lec2025_moo_spinreflexxml
Withdrawal reflexes are mainly initiated by Ad fibres and involve
interneurons that cross the midline
Other cord level responses effected by nociceptors and interneurons include altered muscle tone and sympathetic effects (sweating vasoconstrictiondilation) via links to the preganglionic cell bodies in the lateral horn
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Experiment to Demonstate Secondary Hyperalgesia with Capsaicin induced Nociception
Nerve Block (local anaesthetic)
Nerve Block
Capsaicin
Amplification
R L R L
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Amplifier
Injury
Discovery of the dorsal horn amplifier proved that the pain circuitry exhibits lsquoactivity-dependent-synaptic-plasticityrsquo It is not
hard-wired
Clifford Woolf Discovered central sensitization whilst researching at University College London alongside Patrick Wall and published his findings in 1983 (Woolf CJ Evidence for a central component of post-injury pain hypersensitivity Nature 1983 306686-8)
ldquo pain does not simply reflect the presence intensity or duration of specific lsquopainrsquo stimuli in the periphery but also changes in the
function of the central nervous systemrdquo
Woolf CJ Central sensitization ndashuncovering the relation between pain and plasticity Anesthesiology 2007106864-7
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
11
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
C
C
C C
C C
C
C
C C
C C C
C
C C C
C
Peripheral amp Central Sensitisation Stimulus
Injury + Inflammation
Dorsal Horn Amplification
Amplification In The Brain
PNS CNS
C
C
C
C C C
C Peripheral amp Central Sensitisation
As Inflammation Resolves Peripheral Sensitisation dies down but Central Sensitisation
sometimes persists to be the cause of Chronic pain
lsquoNormallyrsquo ndash Pain goes
lsquoPathologicalrsquo ndash Pain becomes Chronic Brain continues to generate pain Cortical Reorganisation
Dorsal Horn Amplifier stays on High Gain
PAIN
Important Points ndash Pain Sensitisation
bull Peripheral sensitisation drives central sensitisation
bull Secondary hyperalgesia (central sensitisation) gives additional warning of the need to protect the injured anatomy whilst it is inflamed thus assisting healing
bull Perceived worsening pain and an often massive spread of tenderness into multiple tissues is mainly on account of central sensitisation These tissues are not all injured
bull Pain circuitry is not hard-wired
bull Spreading pain is lsquobeyond dermatomesrsquo
Glutamate amp NMDA Receptors Main Neurotransmitter Released by C Fibres
During prolonged excitation the sum of EPSPs lowers the membrane potential sufficiently for the NMDA channels to expel their magnesium molecule allowing an influx of Ca2+ This triggers the release of retrograde messengers that stimulate the
release of more glutamate from the pre-synaptic membrane This all leads to a greater response from the secondary nerve
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Glutamate normally opens only AMPA channels because NMDA channels are blocked by a magnesium molecule
Substance P Sensitising Neuropeptides Also Released by C Fibres
Subtance P and CGRP sensitise the secondary nerve to glutamate Within the dorsal horn these can diffuse around several levels of the spinal cord sensitising
other secondary nerves (dorsal horn neurons) in the process
What was previously an innocuous stimulus may now be perceived as pain and pain may be perceived at a seemingly unrelated anatomical site
Substance P
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
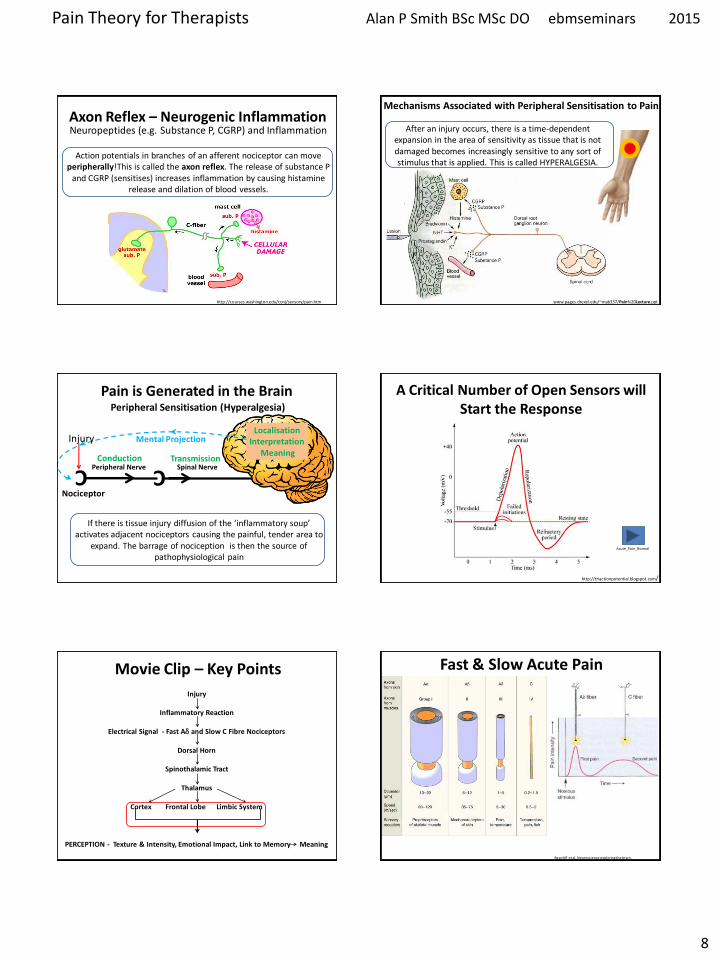
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
8
Axon Reflex ndash Neurogenic Inflammation Neuropeptides (eg Substance P CGRP) and Inflammation
Action potentials in branches of an afferent nociceptor can move
peripherallyThis is called the axon reflex The release of substance P and CGRP (sensitises) increases inflammation by causing histamine
release and dilation of blood vessels
httpcourseswashingtoneduconjsensorypainhtm
Mechanisms Associated with Peripheral Sensitisation to Pain
After an injury occurs there is a time-dependent expansion in the area of sensitivity as tissue that is not damaged becomes increasingly sensitive to any sort of stimulus that is applied This is called HYPERALGESIA
wwwpagesdrexeledu~mab337Pain20Lectureppt
C Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Peripheral Sensitisation (Hyperalgesia)
If there is tissue injury diffusion of the lsquoinflammatory souprsquo activates adjacent nociceptors causing the painful tender area to
expand The barrage of nociception is then the source of pathophysiological pain
Injury
A Critical Number of Open Sensors will Start the Response
Acute_Pain_Normal
httptriactionpotentialblogspotcom
Movie Clip ndash Key Points
Injury
Inflammatory Reaction
Electrical Signal - Fast Ad and Slow C Fibre Nociceptors
Dorsal Horn
Spinothalamic Tract
Thalamus
Cortex Frontal Lobe Limbic System
PERCEPTION - Texture amp Intensity Emotional Impact Link to Memory Meaning
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
9
Fast Ad Fibre Pain bull Sharp and well localised bull Nociceptive impulses synapse in the dorsal horn initiate withdrawal reflexes and travel to the sensory cortex via the thalamus
Slow C Fibre Pain bull Diffuse more burning and unpleasant ndash lingers bull Nociceptive impulses synapse with interneurons in the dorsal horn then travel to
1) Sensory cortex and insular cortex 2) Limbic System ndash memory and emotion 3) Hypothalamus (ANS) and brain stem
Only C fibres respond to Chemical stimulation
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Can be Referred to as Projection Neurons
Dorsal Horn Neurons 2nd Order Neurons
httpwwwrnceuscomagesnociceptivehtm
They arise from Lamina 1 as Nociception
Specific (NS) neurons and Lamina V as Wide Dynamic
Ranging (WDR) neurons
NS
WDR
How Mechanoreceptor Activity Can Decrease Nociceptive Processing
(Why Movement and Rubbing Decreases The Perception of Pain)
Melzack and Wallrsquos Pain Gate Theory was the first real challenge to the Pathoanatomical model It postulated that nociception could be lsquomodulatedrsquo at the dorsal horn
and that some lsquointegrationrsquo of nociceptive and other sensory
information could occur
httppublicationsmcgillcaheadwaymagazine
the-king-of-understanding-pain-qa-with-ronald-melzack
naturecom
Ronald Melzack Patrick Wall
1965
R Melzack PD Wall Pain mechanisms a new theory Science 1965150971ndash979
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Many interneurons and interconnections within
the dorsal horn allow integration of different sensory channels Eg Inhibitory interneurons
can be activated by touch and propriceptive input to deep laminae to lsquogatersquo NS
output from lamina 1
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
As Wall himself wrote evaluating the gate theory in the light of further experiments lsquolsquoThe least and perhaps the best that can be said for the 1965
paper is that it provoked discussion and experimentrsquorsquo
2014
Free Access httpwwwsciencedirectcomscience
articlepiiS0306452214007830
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
10
Neurons That Conduct Nociception (Pain Impulses) to the Brain
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
NS neurons are more associated with the emotional suffering
dimension of pain Also autonomic motivational
amp homeostatic responses
WDR neurons are mainly associated with the
sensory discriminative dimension of pain ndash location amp intensity
Spinal Polysynaptic Interneurons (PSINs) (Eg Flexor amp Crossed Extensor Reflex)
httpalexandriahealthlibrarycadocumentsnotesbomunit_6lec2025_moo_spinreflexxml
Withdrawal reflexes are mainly initiated by Ad fibres and involve
interneurons that cross the midline
Other cord level responses effected by nociceptors and interneurons include altered muscle tone and sympathetic effects (sweating vasoconstrictiondilation) via links to the preganglionic cell bodies in the lateral horn
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Experiment to Demonstate Secondary Hyperalgesia with Capsaicin induced Nociception
Nerve Block (local anaesthetic)
Nerve Block
Capsaicin
Amplification
R L R L
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Amplifier
Injury
Discovery of the dorsal horn amplifier proved that the pain circuitry exhibits lsquoactivity-dependent-synaptic-plasticityrsquo It is not
hard-wired
Clifford Woolf Discovered central sensitization whilst researching at University College London alongside Patrick Wall and published his findings in 1983 (Woolf CJ Evidence for a central component of post-injury pain hypersensitivity Nature 1983 306686-8)
ldquo pain does not simply reflect the presence intensity or duration of specific lsquopainrsquo stimuli in the periphery but also changes in the
function of the central nervous systemrdquo
Woolf CJ Central sensitization ndashuncovering the relation between pain and plasticity Anesthesiology 2007106864-7
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
11
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
C
C
C C
C C
C
C
C C
C C C
C
C C C
C
Peripheral amp Central Sensitisation Stimulus
Injury + Inflammation
Dorsal Horn Amplification
Amplification In The Brain
PNS CNS
C
C
C
C C C
C Peripheral amp Central Sensitisation
As Inflammation Resolves Peripheral Sensitisation dies down but Central Sensitisation
sometimes persists to be the cause of Chronic pain
lsquoNormallyrsquo ndash Pain goes
lsquoPathologicalrsquo ndash Pain becomes Chronic Brain continues to generate pain Cortical Reorganisation
Dorsal Horn Amplifier stays on High Gain
PAIN
Important Points ndash Pain Sensitisation
bull Peripheral sensitisation drives central sensitisation
bull Secondary hyperalgesia (central sensitisation) gives additional warning of the need to protect the injured anatomy whilst it is inflamed thus assisting healing
bull Perceived worsening pain and an often massive spread of tenderness into multiple tissues is mainly on account of central sensitisation These tissues are not all injured
bull Pain circuitry is not hard-wired
bull Spreading pain is lsquobeyond dermatomesrsquo
Glutamate amp NMDA Receptors Main Neurotransmitter Released by C Fibres
During prolonged excitation the sum of EPSPs lowers the membrane potential sufficiently for the NMDA channels to expel their magnesium molecule allowing an influx of Ca2+ This triggers the release of retrograde messengers that stimulate the
release of more glutamate from the pre-synaptic membrane This all leads to a greater response from the secondary nerve
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Glutamate normally opens only AMPA channels because NMDA channels are blocked by a magnesium molecule
Substance P Sensitising Neuropeptides Also Released by C Fibres
Subtance P and CGRP sensitise the secondary nerve to glutamate Within the dorsal horn these can diffuse around several levels of the spinal cord sensitising
other secondary nerves (dorsal horn neurons) in the process
What was previously an innocuous stimulus may now be perceived as pain and pain may be perceived at a seemingly unrelated anatomical site
Substance P
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
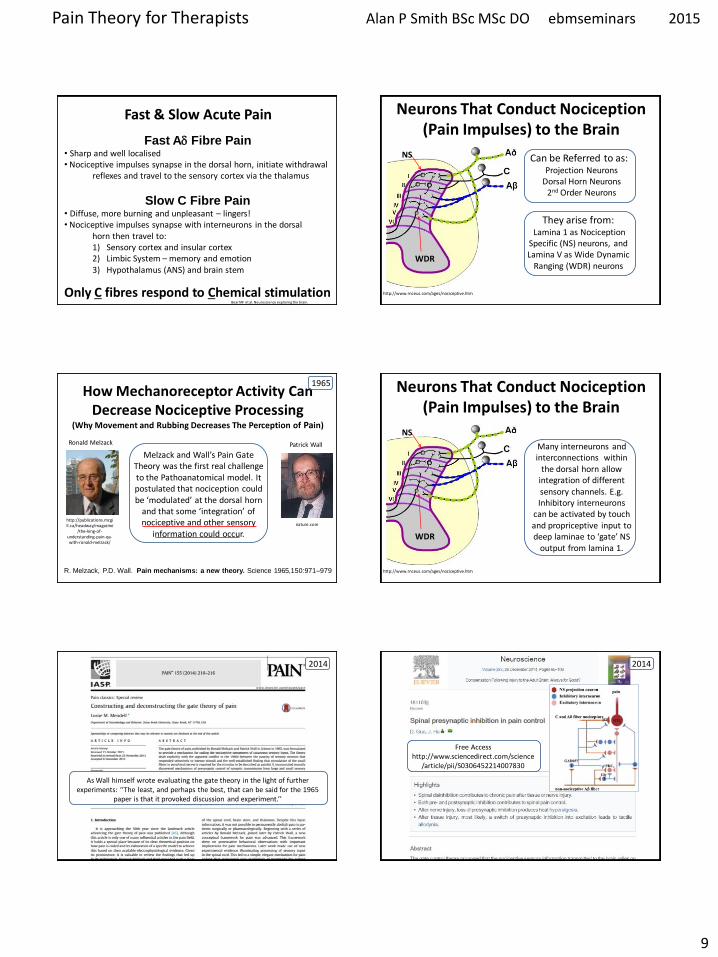
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
9
Fast Ad Fibre Pain bull Sharp and well localised bull Nociceptive impulses synapse in the dorsal horn initiate withdrawal reflexes and travel to the sensory cortex via the thalamus
Slow C Fibre Pain bull Diffuse more burning and unpleasant ndash lingers bull Nociceptive impulses synapse with interneurons in the dorsal horn then travel to
1) Sensory cortex and insular cortex 2) Limbic System ndash memory and emotion 3) Hypothalamus (ANS) and brain stem
Only C fibres respond to Chemical stimulation
Fast amp Slow Acute Pain
Bear MF et al Neuroscience exploring the brain
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Can be Referred to as Projection Neurons
Dorsal Horn Neurons 2nd Order Neurons
httpwwwrnceuscomagesnociceptivehtm
They arise from Lamina 1 as Nociception
Specific (NS) neurons and Lamina V as Wide Dynamic
Ranging (WDR) neurons
NS
WDR
How Mechanoreceptor Activity Can Decrease Nociceptive Processing
(Why Movement and Rubbing Decreases The Perception of Pain)
Melzack and Wallrsquos Pain Gate Theory was the first real challenge to the Pathoanatomical model It postulated that nociception could be lsquomodulatedrsquo at the dorsal horn
and that some lsquointegrationrsquo of nociceptive and other sensory
information could occur
httppublicationsmcgillcaheadwaymagazine
the-king-of-understanding-pain-qa-with-ronald-melzack
naturecom
Ronald Melzack Patrick Wall
1965
R Melzack PD Wall Pain mechanisms a new theory Science 1965150971ndash979
Neurons That Conduct Nociception (Pain Impulses) to the Brain
Many interneurons and interconnections within
the dorsal horn allow integration of different sensory channels Eg Inhibitory interneurons
can be activated by touch and propriceptive input to deep laminae to lsquogatersquo NS
output from lamina 1
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
As Wall himself wrote evaluating the gate theory in the light of further experiments lsquolsquoThe least and perhaps the best that can be said for the 1965
paper is that it provoked discussion and experimentrsquorsquo
2014
Free Access httpwwwsciencedirectcomscience
articlepiiS0306452214007830
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
10
Neurons That Conduct Nociception (Pain Impulses) to the Brain
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
NS neurons are more associated with the emotional suffering
dimension of pain Also autonomic motivational
amp homeostatic responses
WDR neurons are mainly associated with the
sensory discriminative dimension of pain ndash location amp intensity
Spinal Polysynaptic Interneurons (PSINs) (Eg Flexor amp Crossed Extensor Reflex)
httpalexandriahealthlibrarycadocumentsnotesbomunit_6lec2025_moo_spinreflexxml
Withdrawal reflexes are mainly initiated by Ad fibres and involve
interneurons that cross the midline
Other cord level responses effected by nociceptors and interneurons include altered muscle tone and sympathetic effects (sweating vasoconstrictiondilation) via links to the preganglionic cell bodies in the lateral horn
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Experiment to Demonstate Secondary Hyperalgesia with Capsaicin induced Nociception
Nerve Block (local anaesthetic)
Nerve Block
Capsaicin
Amplification
R L R L
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Amplifier
Injury
Discovery of the dorsal horn amplifier proved that the pain circuitry exhibits lsquoactivity-dependent-synaptic-plasticityrsquo It is not
hard-wired
Clifford Woolf Discovered central sensitization whilst researching at University College London alongside Patrick Wall and published his findings in 1983 (Woolf CJ Evidence for a central component of post-injury pain hypersensitivity Nature 1983 306686-8)
ldquo pain does not simply reflect the presence intensity or duration of specific lsquopainrsquo stimuli in the periphery but also changes in the
function of the central nervous systemrdquo
Woolf CJ Central sensitization ndashuncovering the relation between pain and plasticity Anesthesiology 2007106864-7
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
11
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
C
C
C C
C C
C
C
C C
C C C
C
C C C
C
Peripheral amp Central Sensitisation Stimulus
Injury + Inflammation
Dorsal Horn Amplification
Amplification In The Brain
PNS CNS
C
C
C
C C C
C Peripheral amp Central Sensitisation
As Inflammation Resolves Peripheral Sensitisation dies down but Central Sensitisation
sometimes persists to be the cause of Chronic pain
lsquoNormallyrsquo ndash Pain goes
lsquoPathologicalrsquo ndash Pain becomes Chronic Brain continues to generate pain Cortical Reorganisation
Dorsal Horn Amplifier stays on High Gain
PAIN
Important Points ndash Pain Sensitisation
bull Peripheral sensitisation drives central sensitisation
bull Secondary hyperalgesia (central sensitisation) gives additional warning of the need to protect the injured anatomy whilst it is inflamed thus assisting healing
bull Perceived worsening pain and an often massive spread of tenderness into multiple tissues is mainly on account of central sensitisation These tissues are not all injured
bull Pain circuitry is not hard-wired
bull Spreading pain is lsquobeyond dermatomesrsquo
Glutamate amp NMDA Receptors Main Neurotransmitter Released by C Fibres
During prolonged excitation the sum of EPSPs lowers the membrane potential sufficiently for the NMDA channels to expel their magnesium molecule allowing an influx of Ca2+ This triggers the release of retrograde messengers that stimulate the
release of more glutamate from the pre-synaptic membrane This all leads to a greater response from the secondary nerve
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Glutamate normally opens only AMPA channels because NMDA channels are blocked by a magnesium molecule
Substance P Sensitising Neuropeptides Also Released by C Fibres
Subtance P and CGRP sensitise the secondary nerve to glutamate Within the dorsal horn these can diffuse around several levels of the spinal cord sensitising
other secondary nerves (dorsal horn neurons) in the process
What was previously an innocuous stimulus may now be perceived as pain and pain may be perceived at a seemingly unrelated anatomical site
Substance P
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
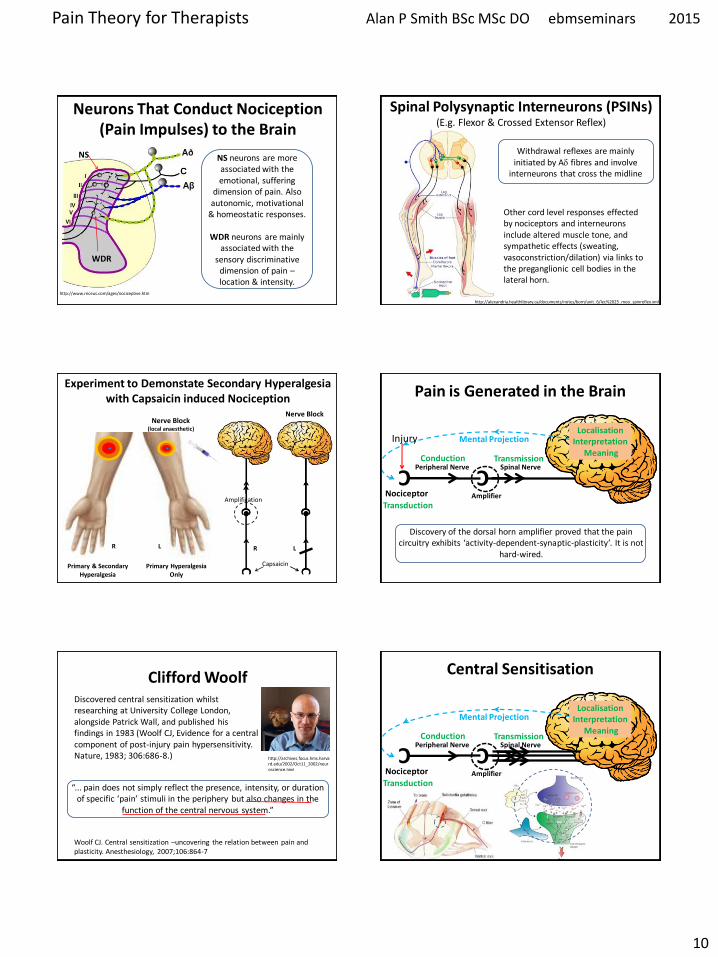
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
10
Neurons That Conduct Nociception (Pain Impulses) to the Brain
httpwwwrnceuscomagesnociceptivehtm
NS
WDR
NS neurons are more associated with the emotional suffering
dimension of pain Also autonomic motivational
amp homeostatic responses
WDR neurons are mainly associated with the
sensory discriminative dimension of pain ndash location amp intensity
Spinal Polysynaptic Interneurons (PSINs) (Eg Flexor amp Crossed Extensor Reflex)
httpalexandriahealthlibrarycadocumentsnotesbomunit_6lec2025_moo_spinreflexxml
Withdrawal reflexes are mainly initiated by Ad fibres and involve
interneurons that cross the midline
Other cord level responses effected by nociceptors and interneurons include altered muscle tone and sympathetic effects (sweating vasoconstrictiondilation) via links to the preganglionic cell bodies in the lateral horn
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Experiment to Demonstate Secondary Hyperalgesia with Capsaicin induced Nociception
Nerve Block (local anaesthetic)
Nerve Block
Capsaicin
Amplification
R L R L
C Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Mental Projection
Amplifier
Injury
Discovery of the dorsal horn amplifier proved that the pain circuitry exhibits lsquoactivity-dependent-synaptic-plasticityrsquo It is not
hard-wired
Clifford Woolf Discovered central sensitization whilst researching at University College London alongside Patrick Wall and published his findings in 1983 (Woolf CJ Evidence for a central component of post-injury pain hypersensitivity Nature 1983 306686-8)
ldquo pain does not simply reflect the presence intensity or duration of specific lsquopainrsquo stimuli in the periphery but also changes in the
function of the central nervous systemrdquo
Woolf CJ Central sensitization ndashuncovering the relation between pain and plasticity Anesthesiology 2007106864-7
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
11
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
C
C
C C
C C
C
C
C C
C C C
C
C C C
C
Peripheral amp Central Sensitisation Stimulus
Injury + Inflammation
Dorsal Horn Amplification
Amplification In The Brain
PNS CNS
C
C
C
C C C
C Peripheral amp Central Sensitisation
As Inflammation Resolves Peripheral Sensitisation dies down but Central Sensitisation
sometimes persists to be the cause of Chronic pain
lsquoNormallyrsquo ndash Pain goes
lsquoPathologicalrsquo ndash Pain becomes Chronic Brain continues to generate pain Cortical Reorganisation
Dorsal Horn Amplifier stays on High Gain
PAIN
Important Points ndash Pain Sensitisation
bull Peripheral sensitisation drives central sensitisation
bull Secondary hyperalgesia (central sensitisation) gives additional warning of the need to protect the injured anatomy whilst it is inflamed thus assisting healing
bull Perceived worsening pain and an often massive spread of tenderness into multiple tissues is mainly on account of central sensitisation These tissues are not all injured
bull Pain circuitry is not hard-wired
bull Spreading pain is lsquobeyond dermatomesrsquo
Glutamate amp NMDA Receptors Main Neurotransmitter Released by C Fibres
During prolonged excitation the sum of EPSPs lowers the membrane potential sufficiently for the NMDA channels to expel their magnesium molecule allowing an influx of Ca2+ This triggers the release of retrograde messengers that stimulate the
release of more glutamate from the pre-synaptic membrane This all leads to a greater response from the secondary nerve
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Glutamate normally opens only AMPA channels because NMDA channels are blocked by a magnesium molecule
Substance P Sensitising Neuropeptides Also Released by C Fibres
Subtance P and CGRP sensitise the secondary nerve to glutamate Within the dorsal horn these can diffuse around several levels of the spinal cord sensitising
other secondary nerves (dorsal horn neurons) in the process
What was previously an innocuous stimulus may now be perceived as pain and pain may be perceived at a seemingly unrelated anatomical site
Substance P
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
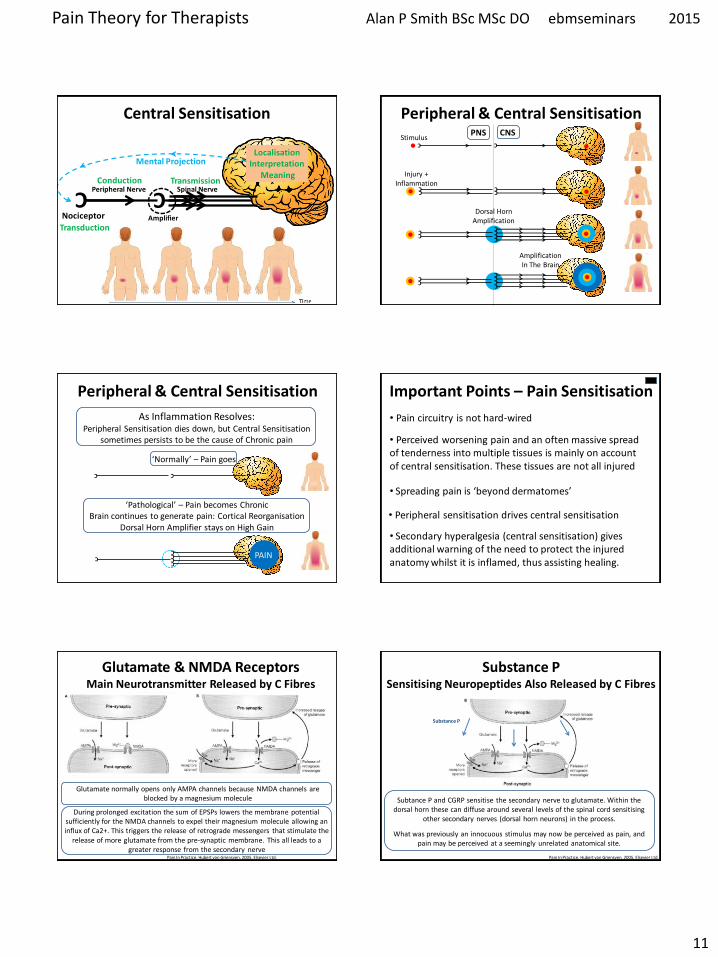
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
11
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Central Sensitisation
Mental Projection
Amplifier
Transduction
C
C
C C
C C
C
C
C C
C C C
C
C C C
C
Peripheral amp Central Sensitisation Stimulus
Injury + Inflammation
Dorsal Horn Amplification
Amplification In The Brain
PNS CNS
C
C
C
C C C
C Peripheral amp Central Sensitisation
As Inflammation Resolves Peripheral Sensitisation dies down but Central Sensitisation
sometimes persists to be the cause of Chronic pain
lsquoNormallyrsquo ndash Pain goes
lsquoPathologicalrsquo ndash Pain becomes Chronic Brain continues to generate pain Cortical Reorganisation
Dorsal Horn Amplifier stays on High Gain
PAIN
Important Points ndash Pain Sensitisation
bull Peripheral sensitisation drives central sensitisation
bull Secondary hyperalgesia (central sensitisation) gives additional warning of the need to protect the injured anatomy whilst it is inflamed thus assisting healing
bull Perceived worsening pain and an often massive spread of tenderness into multiple tissues is mainly on account of central sensitisation These tissues are not all injured
bull Pain circuitry is not hard-wired
bull Spreading pain is lsquobeyond dermatomesrsquo
Glutamate amp NMDA Receptors Main Neurotransmitter Released by C Fibres
During prolonged excitation the sum of EPSPs lowers the membrane potential sufficiently for the NMDA channels to expel their magnesium molecule allowing an influx of Ca2+ This triggers the release of retrograde messengers that stimulate the
release of more glutamate from the pre-synaptic membrane This all leads to a greater response from the secondary nerve
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Glutamate normally opens only AMPA channels because NMDA channels are blocked by a magnesium molecule
Substance P Sensitising Neuropeptides Also Released by C Fibres
Subtance P and CGRP sensitise the secondary nerve to glutamate Within the dorsal horn these can diffuse around several levels of the spinal cord sensitising
other secondary nerves (dorsal horn neurons) in the process
What was previously an innocuous stimulus may now be perceived as pain and pain may be perceived at a seemingly unrelated anatomical site
Substance P
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
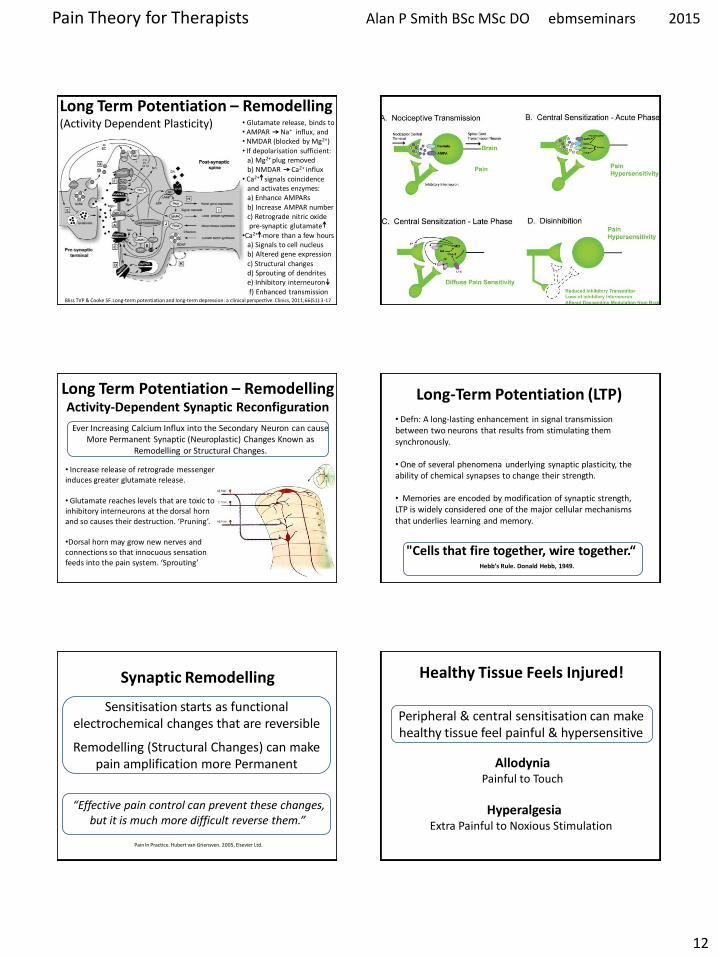
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
12
Long Term Potentiation ndash Remodelling (Activity Dependent Plasticity)
Bliss TVP amp Cooke SF Long-term potentiation and long-term depression a clinical perspective Clinics 201166(S1)3-17
bull Glutamate release binds to bull AMPAR Na+ influx and bull NMDAR (blocked by Mg2+) bull If depolarisation sufficient a) Mg2+ plug removed b) NMDAR Ca2+ influx bull Ca2+ signals coincidence and activates enzymes a) Enhance AMPARs b) Increase AMPAR number c) Retrograde nitric oxide pre-synaptic glutamate bullCa2+ -more than a few hours a) Signals to cell nucleus b) Altered gene expression c) Structural changes d) Sprouting of dendrites e) Inhibitory interneuron f) Enhanced transmission
Long Term Potentiation ndash Remodelling Activity-Dependent Synaptic Reconfiguration
Ever Increasing Calcium Influx into the Secondary Neuron can cause More Permanent Synaptic (Neuroplastic) Changes Known as
Remodelling or Structural Changes
bull Increase release of retrograde messenger induces greater glutamate release bull Glutamate reaches levels that are toxic to inhibitory interneurons at the dorsal horn and so causes their destruction lsquoPruningrsquo bullDorsal horn may grow new nerves and connections so that innocuous sensation feeds into the pain system lsquoSproutingrsquo
Long-Term Potentiation (LTP) bull Defn A long-lasting enhancement in signal transmission
between two neurons that results from stimulating them synchronously bull One of several phenomena underlying synaptic plasticity the ability of chemical synapses to change their strength bull Memories are encoded by modification of synaptic strength LTP is widely considered one of the major cellular mechanisms that underlies learning and memory
Cells that fire together wire togetherldquo Hebbrsquos Rule Donald Hebb 1949
Synaptic Remodelling
Sensitisation starts as functional electrochemical changes that are reversible
Remodelling (Structural Changes) can make pain amplification more Permanent
ldquoEffective pain control can prevent these changes but it is much more difficult reverse themrdquo
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Healthy Tissue Feels Injured
Peripheral amp central sensitisation can make healthy tissue feel painful amp hypersensitive
Allodynia Painful to Touch
Hyperalgesia Extra Painful to Noxious Stimulation
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
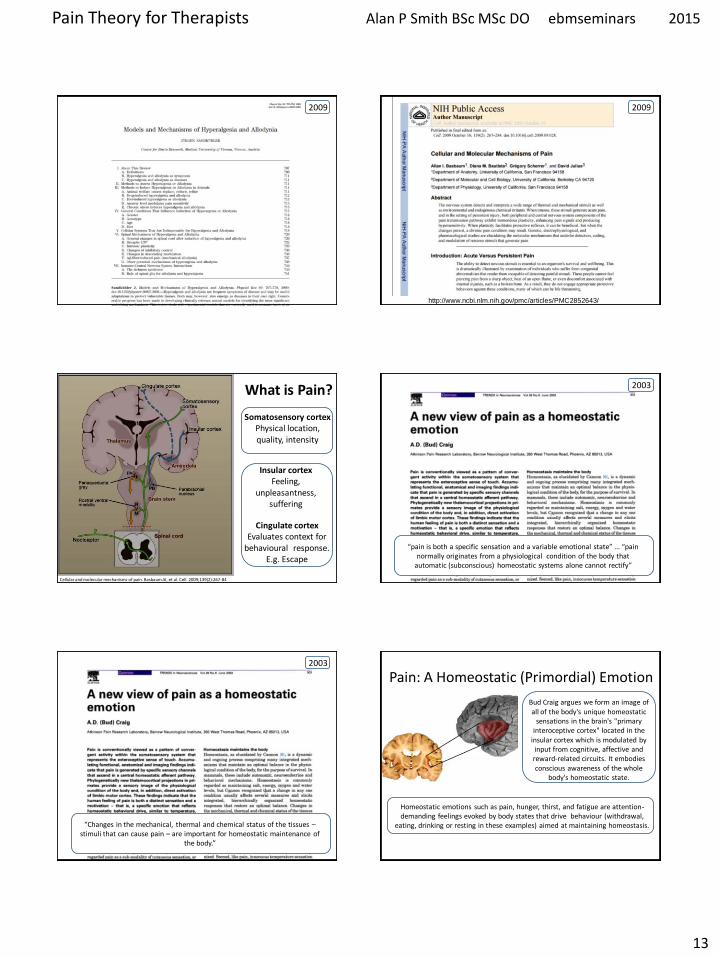
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
13
2009
httpwwwncbinlmnihgovpmcarticlesPMC2852643
2009
Cellular and molecular mechanisms of pain Basbaum AI et al Cell 2009139(2)267-84
Somatosensory cortex Physical location quality intensity
Insular cortex Feeling
unpleasantness suffering
Cingulate cortex Evaluates context for
behavioural response Eg Escape
What is Pain
ldquopain is both a specific sensation and a variable emotional staterdquo ldquopain normally originates from a physiological condition of the body that
automatic (subconscious) homeostatic systems alone cannot rectifyrdquo
2003
ldquoChanges in the mechanical thermal and chemical status of the tissues ndash stimuli that can cause pain ndash are important for homeostatic maintenance of
the bodyrdquo
2003
Bud Craig argues we form an image of all of the bodys unique homeostatic
sensations in the brains primary interoceptive cortex located in the
insular cortex which is modulated by input from cognitive affective and reward-related circuits It embodies conscious awareness of the whole
bodys homeostatic state
Pain A Homeostatic (Primordial) Emotion
Homeostatic emotions such as pain hunger thirst and fatigue are attention-demanding feelings evoked by body states that drive behaviour (withdrawal
eating drinking or resting in these examples) aimed at maintaining homeostasis
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
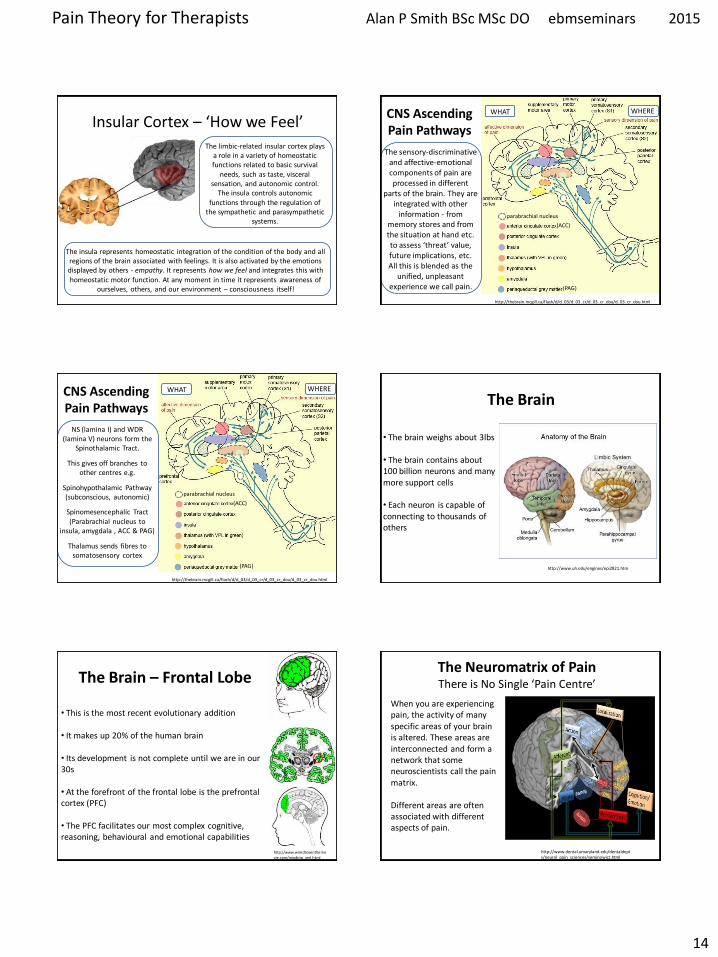
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
14
Insular Cortex ndash lsquoHow we Feelrsquo The limbic-related insular cortex plays
a role in a variety of homeostatic functions related to basic survival
needs such as taste visceral sensation and autonomic control
The insula controls autonomic functions through the regulation of
the sympathetic and parasympathetic systems
The insula represents homeostatic integration of the condition of the body and all regions of the brain associated with feelings It is also activated by the emotions displayed by others - empathy It represents how we feel and integrates this with homeostatic motor function At any moment in time it represents awareness of
ourselves others and our environment ndash consciousness itself
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
(ACC)
(PAG)
WHERE WHAT
The sensory-discriminative and affective-emotional components of pain are processed in different
parts of the brain They are integrated with other
information - from memory stores and from the situation at hand etc to assess lsquothreatrsquo value future implications etc All this is blended as the
unified unpleasant experience we call pain
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
CNS Ascending Pain Pathways
parabrachial nucleus
NS (lamina I) and WDR (lamina V) neurons form the
Spinothalamic Tract
This gives off branches to other centres eg
Spinohypothalamic Pathway (subconscious autonomic)
Spinomesencephalic Tract (Parabrachial nucleus to
insula amygdala ACC amp PAG)
Thalamus sends fibres to somatosensory cortex
(ACC)
(PAG)
WHERE WHAT
The Brain
bull The brain weighs about 3lbs
bull The brain contains about 100 billion neurons and many more support cells
bull Each neuron is capable of connecting to thousands of others
httpwwwuheduenginesepi2821htm
The Brain ndash Frontal Lobe
bull This is the most recent evolutionary addition
bull It makes up 20 of the human brain
bull Its development is not complete until we are in our 30s
bull At the forefront of the frontal lobe is the prefrontal cortex (PFC)
bull The PFC facilitates our most complex cognitive reasoning behavioural and emotional capabilities
httpwwwwiredtowinthemoviecommindtrip_xmlhtml
The Neuromatrix of Pain There is No Single lsquoPain Centrersquo
When you are experiencing pain the activity of many specific areas of your brain is altered These areas are interconnected and form a network that some neuroscientists call the pain matrix Different areas are often associated with different aspects of pain
httpwwwdentalumarylandedudentaldeptsneural_pain_sciencesseminowiczhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
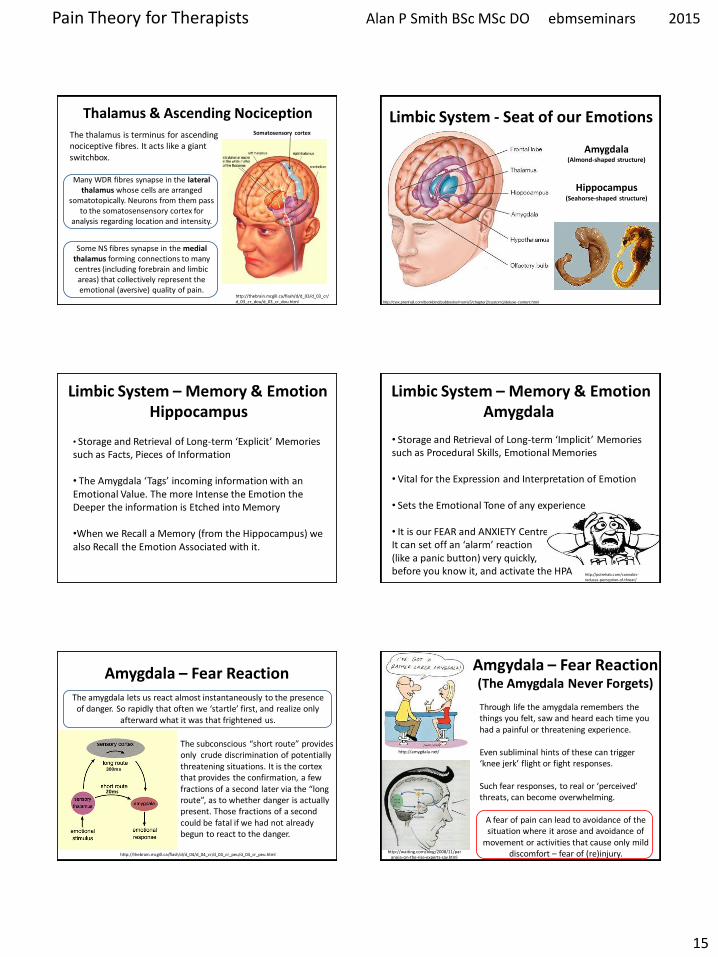
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
15
Thalamus amp Ascending Nociception
The thalamus is terminus for ascending nociceptive fibres It acts like a giant switchbox
Somatosensory cortex
httpthebrainmcgillcaflashdd_03d_03_crd_03_cr_doud_03_cr_douhtml
Many WDR fibres synapse in the lateral thalamus whose cells are arranged
somatotopically Neurons from them pass to the somatosensensory cortex for
analysis regarding location and intensity
Some NS fibres synapse in the medial thalamus forming connections to many centres (including forebrain and limbic areas) that collectively represent the emotional (aversive) quality of pain
Limbic System - Seat of our Emotions
httpcwxprenhallcombookbindpubbooksmorris5chapter2custom1deluxe-contenthtml
Amygdala (Almond-shaped structure)
Hippocampus (Seahorse-shaped structure)
Limbic System ndash Memory amp Emotion Hippocampus
bull Storage and Retrieval of Long-term lsquoExplicitrsquo Memories such as Facts Pieces of Information bull The Amygdala lsquoTagsrsquo incoming information with an Emotional Value The more Intense the Emotion the Deeper the information is Etched into Memory bullWhen we Recall a Memory (from the Hippocampus) we also Recall the Emotion Associated with it
Limbic System ndash Memory amp Emotion Amygdala
bull Storage and Retrieval of Long-term lsquoImplicitrsquo Memories such as Procedural Skills Emotional Memories
bull Vital for the Expression and Interpretation of Emotion
bull Sets the Emotional Tone of any experience
bull It is our FEAR and ANXIETY Centre It can set off an lsquoalarmrsquo reaction (like a panic button) very quickly before you know it and activate the HPA
httppotrehabcomcannabis-reduces-perception-of-threat
The amygdala lets us react almost instantaneously to the presence of danger So rapidly that often we lsquostartlersquo first and realize only
afterward what it was that frightened us
The subconscious ldquoshort routerdquo provides only crude discrimination of potentially threatening situations It is the cortex that provides the confirmation a few fractions of a second later via the ldquolong routerdquo as to whether danger is actually present Those fractions of a second could be fatal if we had not already begun to react to the danger
httpthebrainmcgillcaflashdd_04d_04_crd_04_cr_peud_04_cr_peuhtml
Amygdala ndash Fear Reaction
300ms
20ms
Amgydala ndash Fear Reaction (The Amygdala Never Forgets)
httpwaitingcomblog200811paranoia-on-the-rise-experts-sayhtml
httpamygdalanet
Through life the amygdala remembers the things you felt saw and heard each time you had a painful or threatening experience Even subliminal hints of these can trigger lsquoknee jerkrsquo flight or fight responses Such fear responses to real or lsquoperceivedrsquo threats can become overwhelming
A fear of pain can lead to avoidance of the situation where it arose and avoidance of
movement or activities that cause only mild discomfort ndash fear of (re)injury
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
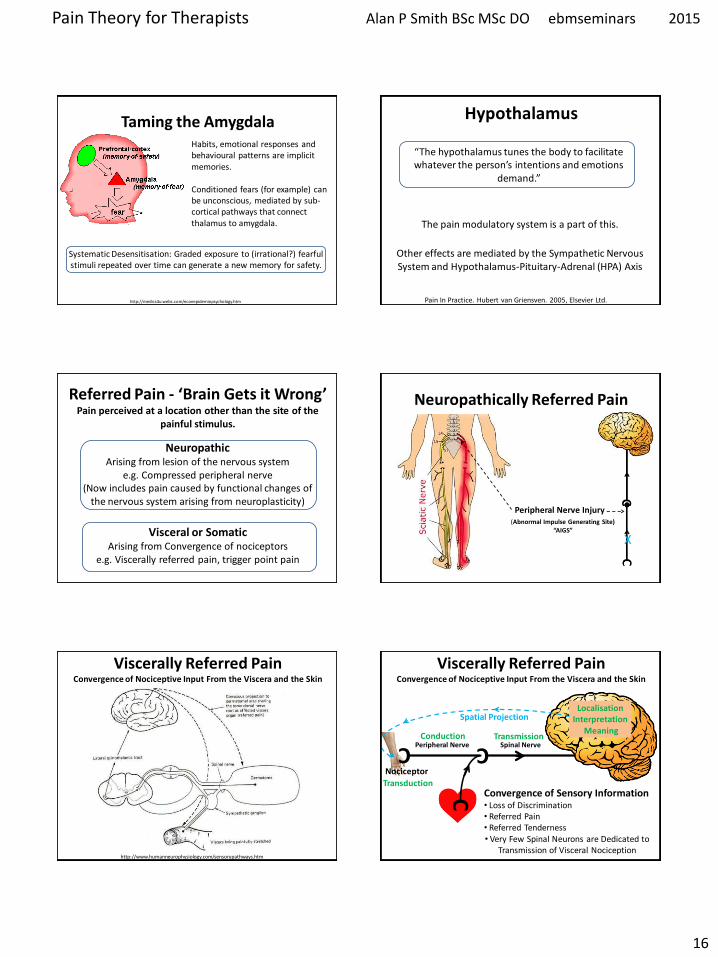
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
16
httpmedics4uwebscomeconepidemiopsychologyhtm
Taming the Amygdala Habits emotional responses and behavioural patterns are implicit memories Conditioned fears (for example) can be unconscious mediated by sub-cortical pathways that connect thalamus to amygdala
Systematic Desensitisation Graded exposure to (irrational) fearful stimuli repeated over time can generate a new memory for safety
Hypothalamus
ldquoThe hypothalamus tunes the body to facilitate whatever the personrsquos intentions and emotions
demandrdquo
The pain modulatory system is a part of this
Other effects are mediated by the Sympathetic Nervous System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Referred Pain - lsquoBrain Gets it Wrongrsquo Pain perceived at a location other than the site of the
painful stimulus
Neuropathic Arising from lesion of the nervous system
eg Compressed peripheral nerve (Now includes pain caused by functional changes of
the nervous system arising from neuroplasticity)
Visceral or Somatic Arising from Convergence of nociceptors
eg Viscerally referred pain trigger point pain
Neuropathically Referred Pain
Peripheral Nerve Injury
X
(Abnormal Impulse Generating Site) ldquoAIGSrdquo
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
httpwwwhumanneurophysiologycomsensorypathwayshtm
C
Nociceptor
Peripheral Nerve
Transduction
Conduction Spinal Nerve
Transmission C
Localisation Interpretation
Meaning
C
Spatial Projection
Convergence of Sensory Information bull Loss of Discrimination bull Referred Pain bull Referred Tenderness bull Very Few Spinal Neurons are Dedicated to
Transmission of Visceral Nociception
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
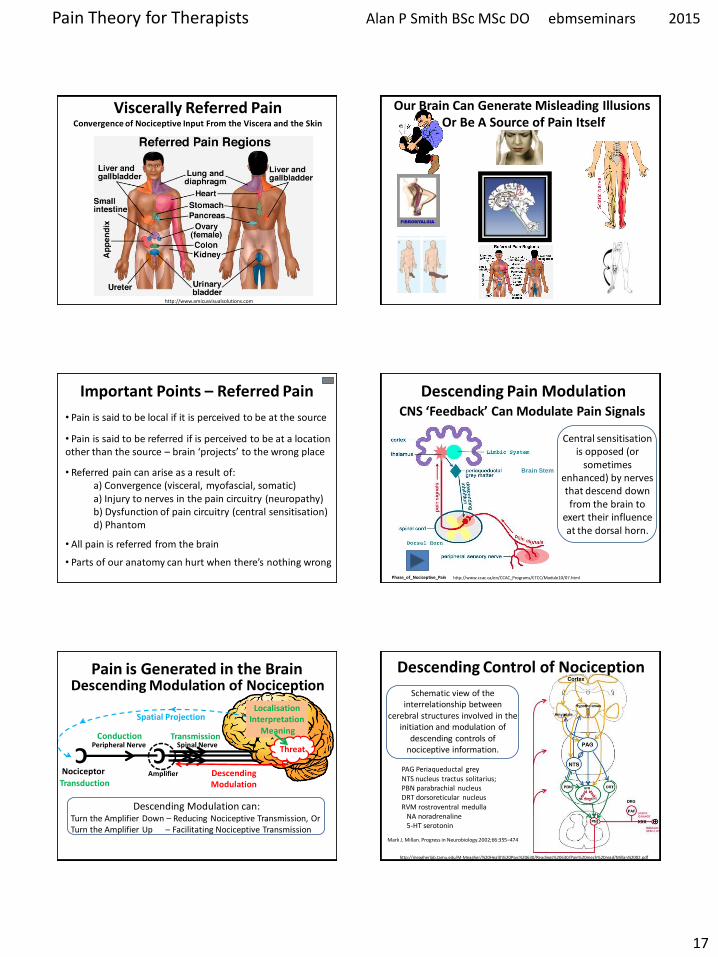
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
17
httpwwwamicusvisualsolutionscom
Viscerally Referred Pain Convergence of Nociceptive Input From the Viscera and the Skin
Our Brain Can Generate Misleading Illusions Or Be A Source of Pain Itself
Important Points ndash Referred Pain
bull Pain is said to be referred if is perceived to be at a location other than the source ndash brain lsquoprojectsrsquo to the wrong place
bull Referred pain can arise as a result of a) Convergence (visceral myofascial somatic) a) Injury to nerves in the pain circuitry (neuropathy) b) Dysfunction of pain circuitry (central sensitisation) d) Phantom
bull All pain is referred from the brain
bull Pain is said to be local if it is perceived to be at the source
bull Parts of our anatomy can hurt when therersquos nothing wrong
CNS lsquoFeedbackrsquo Can Modulate Pain Signals
Descending Pain Modulation
httpwwwccaccaenCCAC_ProgramsETCCModule1007html Phase_of_Nociceptive_Pain
Brain Stem
Central sensitisation is opposed (or
sometimes enhanced) by nerves that descend down from the brain to
exert their influence at the dorsal horn
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Descending Modulation can Turn the Amplifier Down ndash Reducing Nociceptive Transmission Or Turn the Amplifier Up ndash Facilitating Nociceptive Transmission
Descending Modulation of Nociception Schematic view of the
interrelationship between cerebral structures involved in the
initiation and modulation of descending controls of
nociceptive information
PAG Periaqueductal grey NTS nucleus tractus solitarius PBN parabrachial nucleus DRT dorsoreticular nucleus RVM rostroventral medulla NA noradrenaline 5-HT serotonin
httpmeagherlabtamueduM-Meagher20Health20Psyc20630Readings20630Pain20mech20readMillan2002pdf
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
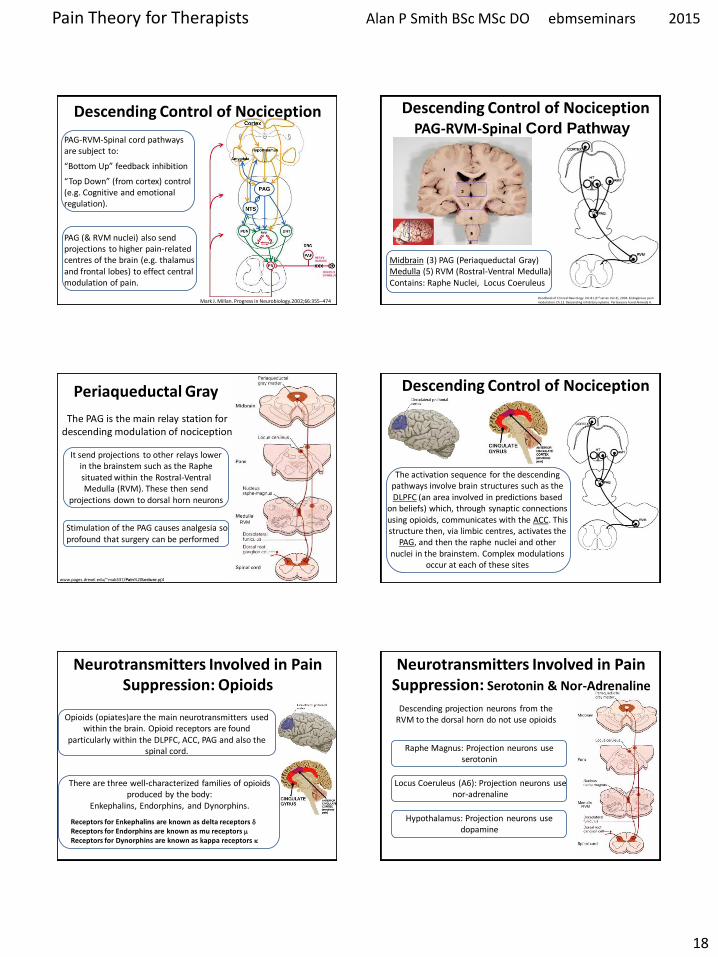
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
18
Mark J Millan Progress in Neurobiology200266355ndash474
Descending Control of Nociception
PAG-RVM-Spinal cord pathways are subject to
ldquoBottom Uprdquo feedback inhibition
ldquoTop Downrdquo (from cortex) control (eg Cognitive and emotional regulation) PAG (amp RVM nuclei) also send projections to higher pain-related centres of the brain (eg thalamus and frontal lobes) to effect central modulation of pain
PAG-RVM-Spinal Cord Pathway
Handbook of Clinical Neurology Vol81 (3rd series Vol3) 2006 Endogenous pain modulation Ch13 Descending inhibitory systems Pertovaara A and Almeida A
Midbrain (3) PAG (Periaqueductal Gray) Medulla (5) RVM (Rostral-Ventral Medulla) Contains Raphe Nuclei Locus Coeruleus
Descending Control of Nociception
Stimulation of the PAG causes analgesia so profound that surgery can be performed
wwwpagesdrexeledu~mab337Pain20Lectureppt
RVM
Periaqueductal Gray
The PAG is the main relay station for descending modulation of nociception
It send projections to other relays lower in the brainstem such as the Raphe situated within the Rostral-Ventral Medulla (RVM) These then send
projections down to dorsal horn neurons
The activation sequence for the descending pathways involve brain structures such as the DLPFC (an area involved in predictions based
on beliefs) which through synaptic connections using opioids communicates with the ACC This structure then via limbic centres activates the
PAG and then the raphe nuclei and other nuclei in the brainstem Complex modulations
occur at each of these sites
Descending Control of Nociception
Opioids (opiates)are the main neurotransmitters used within the brain Opioid receptors are found
particularly within the DLPFC ACC PAG and also the spinal cord
Receptors for Enkephalins are known as delta receptors d
Receptors for Endorphins are known as mu receptors m
Receptors for Dynorphins are known as kappa receptors k
There are three well-characterized families of opioids produced by the body
Enkephalins Endorphins and Dynorphins
Neurotransmitters Involved in Pain Suppression Opioids
Hypothalamus Projection neurons use dopamine
RVM
Neurotransmitters Involved in Pain Suppression Serotonin amp Nor-Adrenaline
Descending projection neurons from the RVM to the dorsal horn do not use opioids
Raphe Magnus Projection neurons use serotonin
Locus Coeruleus (A6) Projection neurons use nor-adrenaline
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
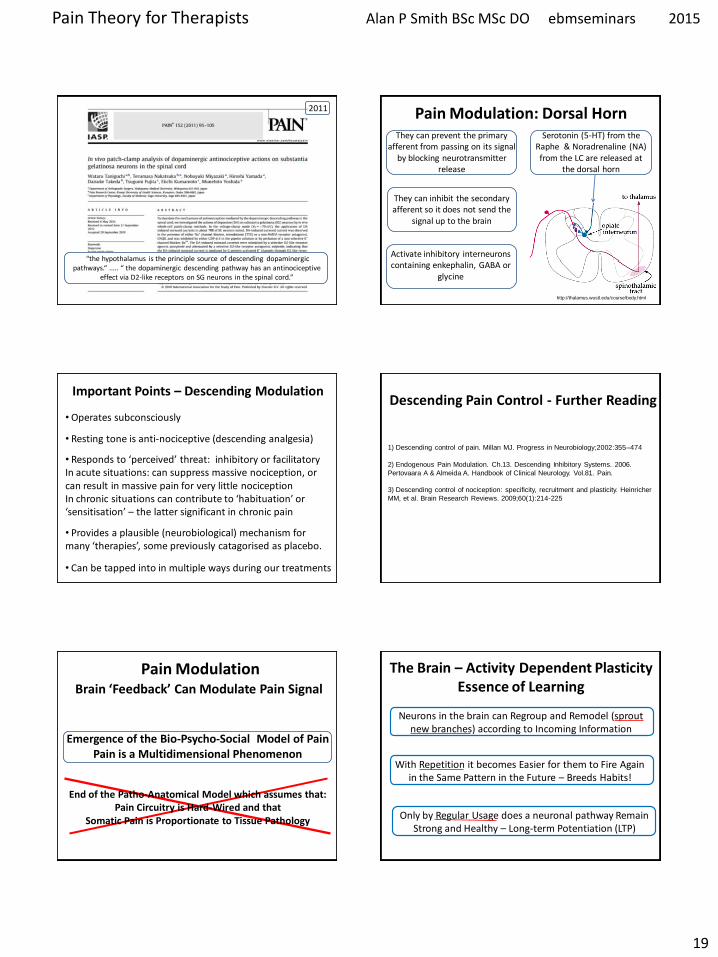
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
19
ldquothe hypothalamus is the principle source of descending dopaminergic pathwaysldquo ldquo the dopaminergic descending pathway has an antinociceptive
effect via D2-like receptors on SG neurons in the spinal cordrdquo
2011
httpthalamuswustleducoursebodyhtml
Pain Modulation Dorsal Horn Serotonin (5-HT) from the
Raphe amp Noradrenaline (NA) from the LC are released at
the dorsal horn
They can prevent the primary afferent from passing on its signal
by blocking neurotransmitter release
They can inhibit the secondary afferent so it does not send the
signal up to the brain
Activate inhibitory interneurons containing enkephalin GABA or
glycine
Important Points ndash Descending Modulation
bull Resting tone is anti-nociceptive (descending analgesia)
bull Responds to lsquoperceivedrsquo threat inhibitory or facilitatory In acute situations can suppress massive nociception or can result in massive pain for very little nociception In chronic situations can contribute to lsquohabituationrsquo or lsquosensitisationrsquo ndash the latter significant in chronic pain bull Provides a plausible (neurobiological) mechanism for many lsquotherapiesrsquo some previously catagorised as placebo
bull Operates subconsciously
bull Can be tapped into in multiple ways during our treatments
Descending Pain Control - Further Reading
1) Descending control of pain Millan MJ Progress in Neurobiology2002355ndash474
2) Endogenous Pain Modulation Ch13 Descending Inhibitory Systems 2006
Pertovaara A amp Almeida A Handbook of Clinical Neurology Vol81 Pain
3) Descending control of nociception specificity recruitment and plasticity Heinricher
MM et al Brain Research Reviews 200960(1)214-225
Brain lsquoFeedbackrsquo Can Modulate Pain Signal
Pain Modulation
Emergence of the Bio-Psycho-Social Model of Pain Pain is a Multidimensional Phenomenon
End of the Patho-Anatomical Model which assumes that
Pain Circuitry is Hard-Wired and that Somatic Pain is Proportionate to Tissue Pathology
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons in the brain can Regroup and Remodel (sprout new branches) according to Incoming Information
With Repetition it becomes Easier for them to Fire Again in the Same Pattern in the Future ndash Breeds Habits
Only by Regular Usage does a neuronal pathway Remain Strong and Healthy ndash Long-term Potentiation (LTP)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
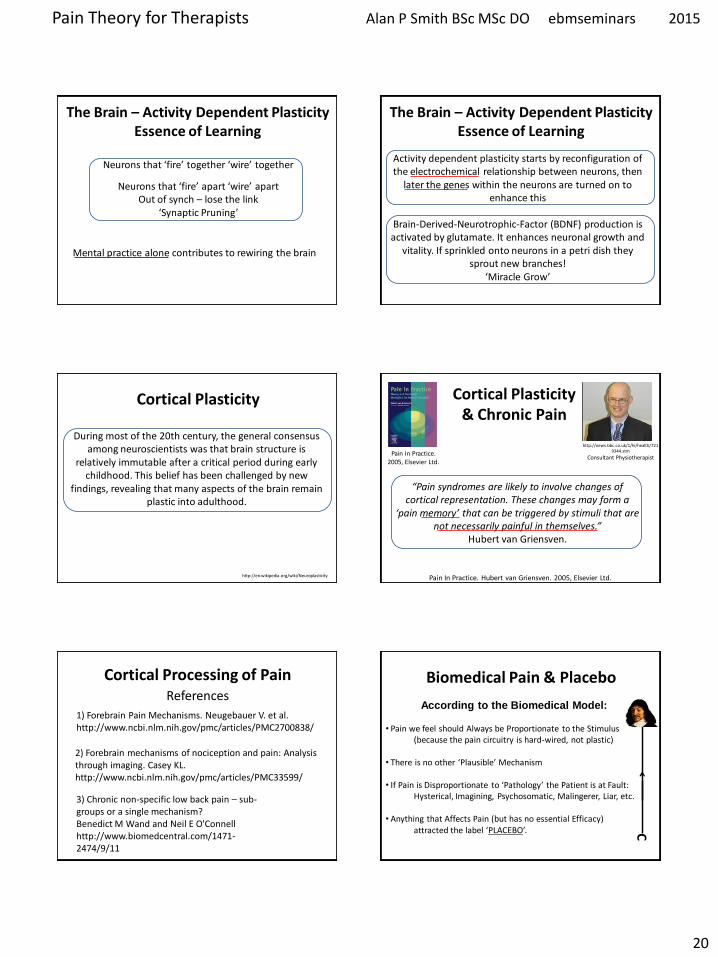
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
20
The Brain ndash Activity Dependent Plasticity Essence of Learning
Neurons that lsquofirersquo together lsquowirersquo together
Neurons that lsquofirersquo apart lsquowirersquo apart Out of synch ndash lose the link
lsquoSynaptic Pruningrsquo
Mental practice alone contributes to rewiring the brain
The Brain ndash Activity Dependent Plasticity Essence of Learning
Activity dependent plasticity starts by reconfiguration of the electrochemical relationship between neurons then
later the genes within the neurons are turned on to enhance this
Brain-Derived-Neurotrophic-Factor (BDNF) production is activated by glutamate It enhances neuronal growth and
vitality If sprinkled onto neurons in a petri dish they sprout new branches
lsquoMiracle Growrsquo
Cortical Plasticity
During most of the 20th century the general consensus among neuroscientists was that brain structure is
relatively immutable after a critical period during early childhood This belief has been challenged by new
findings revealing that many aspects of the brain remain plastic into adulthood
httpenwikipediaorgwikiNeuroplasticity
Cortical Plasticity amp Chronic Pain
ldquoPain syndromes are likely to involve changes of cortical representation These changes may form a
lsquopain memoryrsquo that can be triggered by stimuli that are not necessarily painful in themselvesrdquo
Hubert van Griensven
Pain In Practice 2005 Elsevier Ltd
httpnewsbbccouk1hihealth7219344stm
Consultant Physiotherapist
Pain In Practice Hubert van Griensven 2005 Elsevier Ltd
Cortical Processing of Pain
1) Forebrain Pain Mechanisms Neugebauer V et al httpwwwncbinlmnihgovpmcarticlesPMC2700838
2) Forebrain mechanisms of nociception and pain Analysis through imaging Casey KL httpwwwncbinlmnihgovpmcarticlesPMC33599
References
3) Chronic non-specific low back pain ndash sub-groups or a single mechanism Benedict M Wand and Neil E OConnell httpwwwbiomedcentralcom1471-2474911
Biomedical Pain amp Placebo
According to the Biomedical Model bull Pain we feel should Always be Proportionate to the Stimulus (because the pain circuitry is hard-wired not plastic) bull There is no other lsquoPlausiblersquo Mechanism
bull If Pain is Disproportionate to lsquoPathologyrsquo the Patient is at Fault Hysterical Imagining Psychosomatic Malingerer Liar etc
bull Anything that Affects Pain (but has no essential Efficacy) attracted the label lsquoPLACEBOrsquo C
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
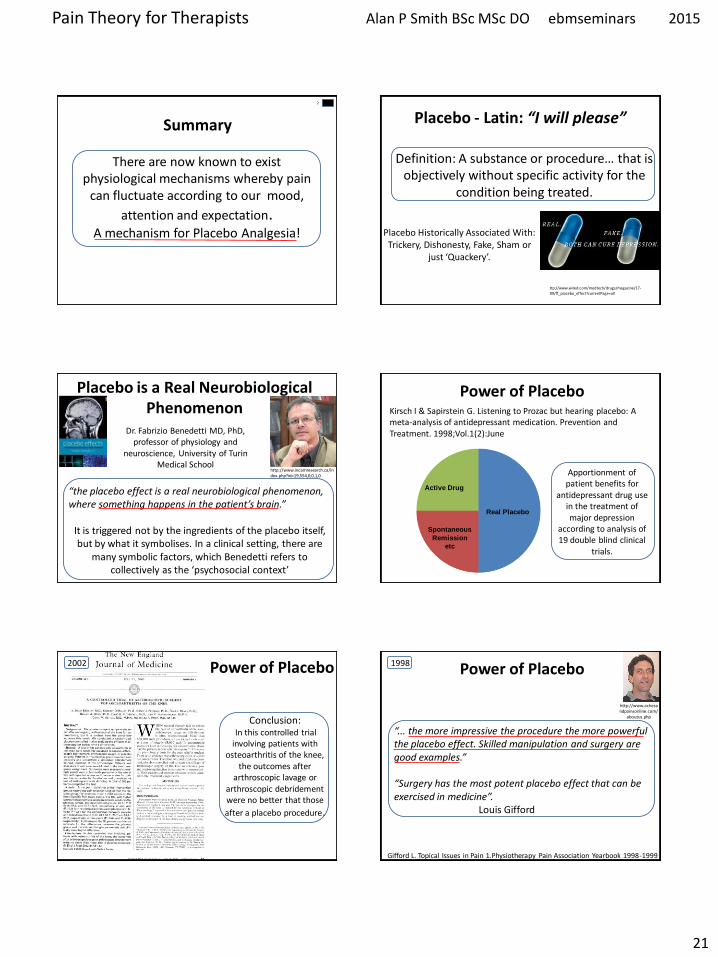
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
21
There are now known to exist physiological mechanisms whereby pain
can fluctuate according to our mood
attention and expectation A mechanism for Placebo Analgesia
Summary
Placebo - Latin ldquoI will pleaserdquo
Placebo Historically Associated With Trickery Dishonesty Fake Sham or
just lsquoQuackeryrsquo
Definition A substance or procedurehellip that is objectively without specific activity for the
condition being treated
ttpwwwwiredcommedtechdrugsmagazine17-
09ff_placebo_effectcurrentPage=all
Placebo is a Real Neurobiological Phenomenon
Dr Fabrizio Benedetti MD PhD professor of physiology and
neuroscience University of Turin Medical School
ldquothe placebo effect is a real neurobiological phenomenon where something happens in the patientrsquos brainrdquo
It is triggered not by the ingredients of the placebo itself but by what it symbolises In a clinical setting there are
many symbolic factors which Benedetti refers to collectively as the lsquopsychosocial contextrsquo
httpwwwincamresearchcaindexphpid=195540010
Power of Placebo
Real Placebo
Active Drug
Spontaneous
Remission
etc
Apportionment of patient benefits for
antidepressant drug use in the treatment of major depression
according to analysis of 19 double blind clinical
trials
Kirsch I amp Sapirstein G Listening to Prozac but hearing placebo A meta-analysis of antidepressant medication Prevention and Treatment 1998Vol1(2)June
Conclusion In this controlled trial involving patients with
osteoarthritis of the knee the outcomes after
arthroscopic lavage or arthroscopic debridement were no better that those
after a placebo procedure
Power of Placebo 2002 Power of Placebo
ldquo the more impressive the procedure the more powerful the placebo effect Skilled manipulation and surgery are good examplesrdquo ldquoSurgery has the most potent placebo effect that can be exercised in medicinerdquo Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
1998
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
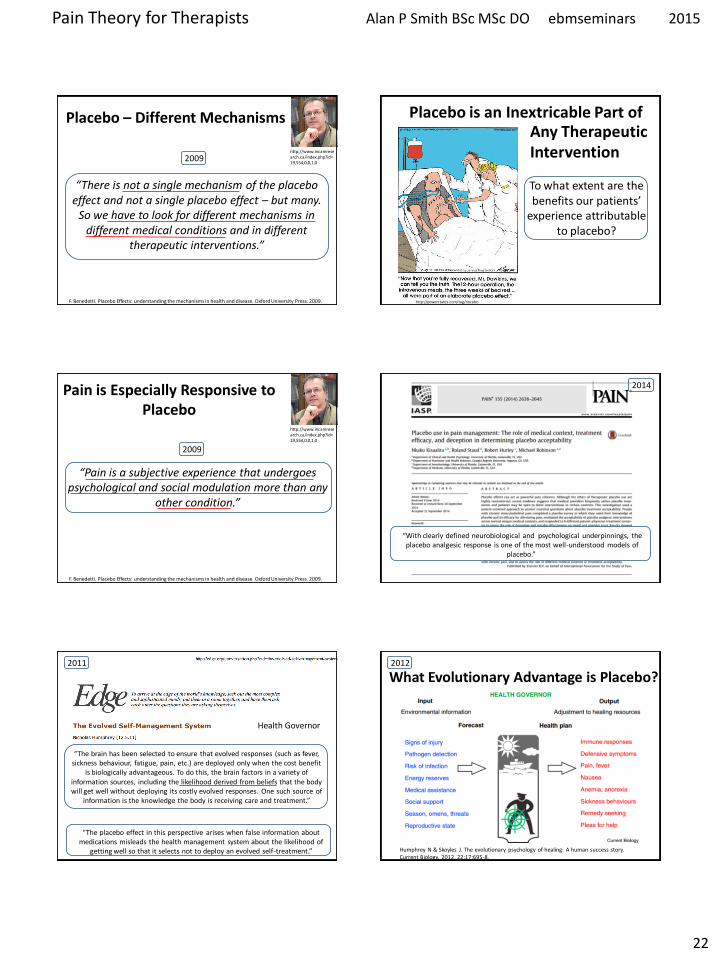
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
22
Placebo ndash Different Mechanisms
ldquoThere is not a single mechanism of the placebo effect and not a single placebo effect ndash but many
So we have to look for different mechanisms in different medical conditions and in different
therapeutic interventionsrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
Placebo is an Inextricable Part of
httppowerstatescomtagnocebo
To what extent are the benefits our patientsrsquo
experience attributable to placebo
Any Therapeutic Intervention
Pain is Especially Responsive to Placebo
ldquoPain is a subjective experience that undergoes
psychological and social modulation more than any other conditionrdquo
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
httpwwwincamresearchcaindexphpid=195540010
2009
ldquoWith clearly defined neurobiological and psychological underpinnings the placebo analgesic response is one of the most well-understood models of
placebordquo
2014
ldquoThe brain has been selected to ensure that evolved responses (such as fever sickness behaviour fatigue pain etc) are deployed only when the cost benefit
is biologically advantageous To do this the brain factors in a variety of information sources including the likelihood derived from beliefs that the body will get well without deploying its costly evolved responses One such source of
information is the knowledge the body is receiving care and treatmentrdquo
The placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of getting well so that it
selects not to deploy an evolved self-treatment[101
ldquoThe placebo effect in this perspective arises when false information about medications misleads the health management system about the likelihood of
getting well so that it selects not to deploy an evolved self-treatmentrdquo
2011
Health Governor
What Evolutionary Advantage is Placebo
Humphrey N amp Skoyles J The evolutionary psychology of healing A human success story Current Biology 2012 2217695-8
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
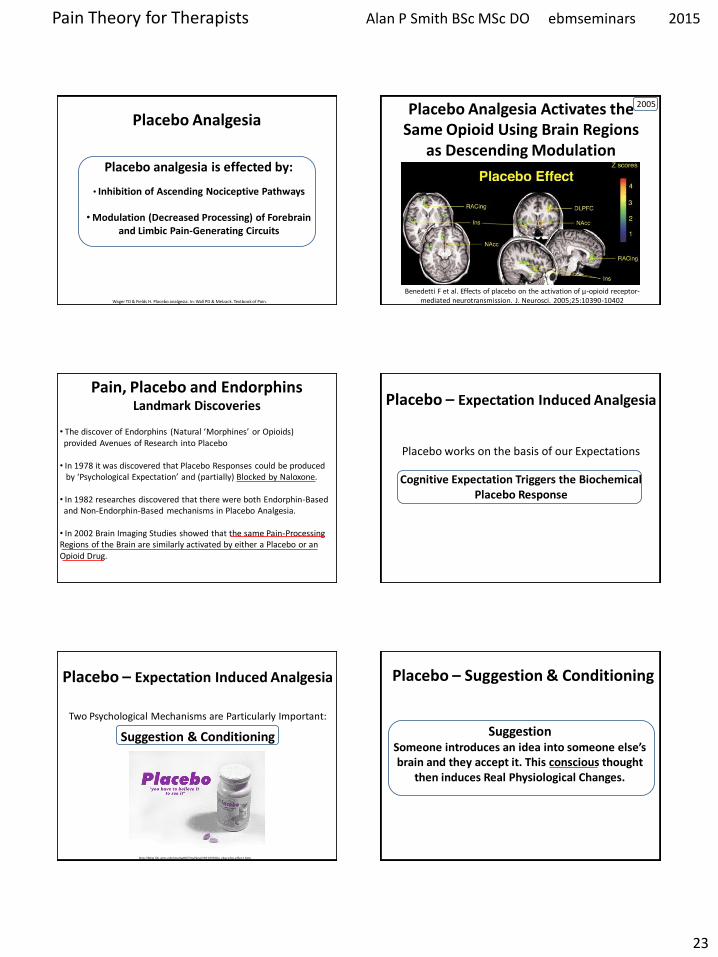
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
23
Placebo Analgesia
Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
Placebo analgesia is effected by
bull Inhibition of Ascending Nociceptive Pathways
bull Modulation (Decreased Processing) of Forebrain and Limbic Pain-Generating Circuits
Benedetti F et al Effects of placebo on the activation of μ-opioid receptor-mediated neurotransmission J Neurosci 20052510390-10402
Placebo Analgesia Activates the Same Opioid Using Brain Regions
as Descending Modulation
2005
Pain Placebo and Endorphins Landmark Discoveries
bull The discover of Endorphins (Natural lsquoMorphinesrsquo or Opioids) provided Avenues of Research into Placebo
bull In 1978 it was discovered that Placebo Responses could be produced by lsquoPsychological Expectationrsquo and (partially) Blocked by Naloxone
bull In 1982 researches discovered that there were both Endorphin-Based and Non-Endorphin-Based mechanisms in Placebo Analgesia bull In 2002 Brain Imaging Studies showed that the same Pain-Processing Regions of the Brain are similarly activated by either a Placebo or an Opioid Drug
Placebo ndash Expectation Induced Analgesia
Placebo works on the basis of our Expectations
Cognitive Expectation Triggers the Biochemical Placebo Response
Placebo ndash Expectation Induced Analgesia
Two Psychological Mechanisms are Particularly Important
Suggestion amp Conditioning
httpbloglibumnedumeriw007myblog201202the-placebo-effecthtm
Placebo ndash Suggestion amp Conditioning
Suggestion Someone introduces an idea into someone elsersquos brain and they accept it This conscious thought
then induces Real Physiological Changes
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
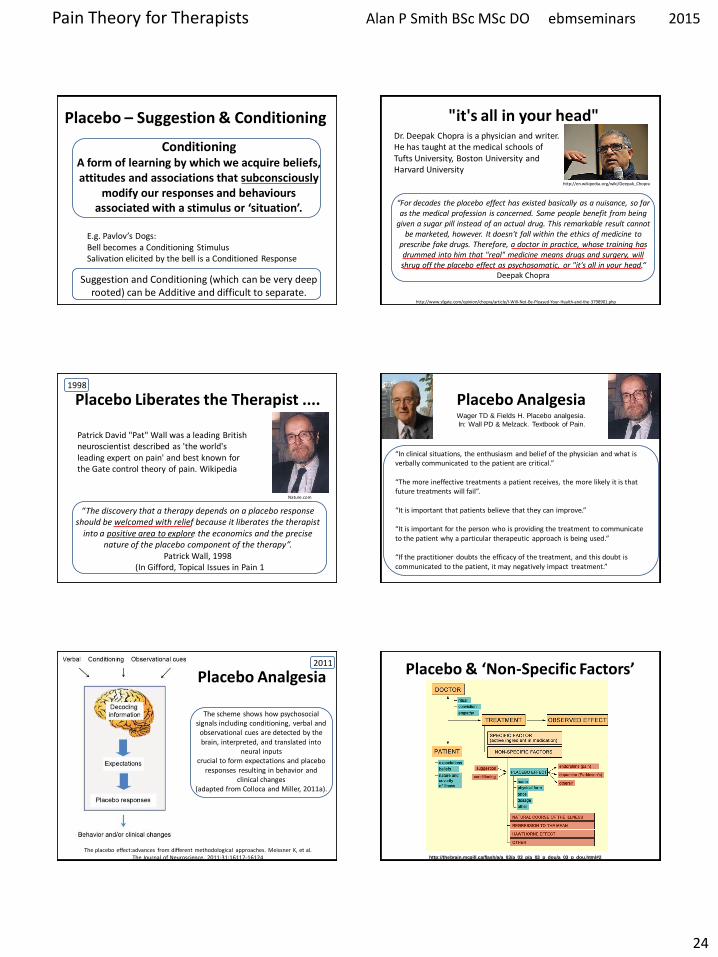
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
24
Placebo ndash Suggestion amp Conditioning
Conditioning A form of learning by which we acquire beliefs attitudes and associations that subconsciously
modify our responses and behaviours associated with a stimulus or lsquosituationrsquo
Eg Pavlovrsquos Dogs Bell becomes a Conditioning Stimulus Salivation elicited by the bell is a Conditioned Response
Suggestion and Conditioning (which can be very deep rooted) can be Additive and difficult to separate
its all in your head
ldquoFor decades the placebo effect has existed basically as a nuisance so far as the medical profession is concerned Some people benefit from being
given a sugar pill instead of an actual drug This remarkable result cannot be marketed however It doesnt fall within the ethics of medicine to
prescribe fake drugs Therefore a doctor in practice whose training has drummed into him that real medicine means drugs and surgery will shrug off the placebo effect as psychosomatic or its all in your headldquo
Deepak Chopra
httpwwwsfgatecomopinionchopraarticleI-Will-Not-Be-Pleased-Your-Health-and-the-3798901php
httpenwikipediaorgwikiDeepak_Chopra
Dr Deepak Chopra is a physician and writer He has taught at the medical schools of Tufts University Boston University and Harvard University
Placebo Liberates the Therapist
ldquoThe discovery that a therapy depends on a placebo response should be welcomed with relief because it liberates the therapist
into a positive area to explore the economics and the precise nature of the placebo component of the therapyrdquo
Patrick Wall 1998 (In Gifford Topical Issues in Pain 1
Patrick David Pat Wall was a leading British neuroscientist described as the worlds leading expert on pain and best known for the Gate control theory of pain Wikipedia
Naturecom
1998
Placebo Analgesia Wager TD amp Fields H Placebo analgesia
In Wall PD amp Melzack Textbook of Pain
ldquoIn clinical situations the enthusiasm and belief of the physician and what is verbally communicated to the patient are criticalrdquo ldquoThe more ineffective treatments a patient receives the more likely it is that future treatments will failrdquo ldquoIt is important that patients believe that they can improverdquo ldquoIt is important for the person who is providing the treatment to communicate to the patient why a particular therapeutic approach is being usedrdquo ldquoIf the practitioner doubts the efficacy of the treatment and this doubt is communicated to the patient it may negatively impact treatmentrdquo
Placebo Analgesia
The scheme shows how psychosocial signals including conditioning verbal and
observational cues are detected by the brain interpreted and translated into
neural inputs crucial to form expectations and placebo
responses resulting in behavior and clinical changes
(adapted from Colloca and Miller 2011a)
The placebo effectadvances from different methodological approaches Meissner K et al The Journal of Neuroscience 20113116117-16124
2011 Placebo amp lsquoNon-Specific Factorsrsquo
httpthebrainmcgillcaflashaa_03a_03_pa_03_p_doua_03_p_douhtml2
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
25
Expectation of analgesia can be directed via attentional mechanisms to different spatial loci of the body
Somatotopic organization of the PAG
Somatotopic Activation of Opioid Systems by Target-Directed Expectations of Analgesia
Four body parts simultaneously injected with capsaicin Specific expectations of analgesia were induced by applying a placebo cream on one of these body parts and by telling the subjects that it was a powerful local anaesthetic A placebo analgesic response occurred only on the treated part whereas no variation in pain sensitivity was found on the untreated parts
Benedetti F et al Somatotopic activation of opioid systems by target-directed expectations of analgesia The Journal of Neuroscience 1999193639-48
1999
Nocebo - Latin ldquoI will harmrdquo
httpboingboingnet20120814nocebo-now-available-withouthtml
Opposite of the Placebo Effect Worsening of symptoms
because of Negative Expectations
httpbloglibumneduvanm0049psy1001section09spring2012201203the-nocebo-effecthtml
Nocebo-Effect Noncompliance When Telling The Patient Enough May Be Too Much
httpalignmapcom20081126clinicians-can-choose-how-not-if-they-influence-patient-compliance
Nocebo Effects
What we do know suggests the impact of nocebo is far-reaching Voodoo death if it exists may represent an extreme form of the nocebo phenomenon says anthropologist Robert Hahn of the US Centers for Disease Control and Prevention in Atlanta Georgia who has studied the nocebo effect
httpcurrentcomshowsupstream90045865_the-science-of-voodoo-the-nocebo-effecthtm
Can Nocebo Kill
Nocebo Hyperalgesia is Mediated by Cholecystokinin (CCK)
Nocebo Hyperalgesia only occurs as a result of Anxiety due to
Anticipation of Pain Attention is Focussed on the Impending Pain
Other extreme Anxiety Producing Situations induce Analgesia Here Attention is Focussed Not on Pain but on some
Environmental Stressor
CCK has Pronociceptive and Anti-Opioid actions that are effected particularly via the PAG and RVM CCK causes tolerance to opioid drugs CCK receptors can be Blocked by the drug Proglumide
ldquoCholecystokinin (CCK) has been suggested to be both pro-nociceptive and anti-opioid by actions on pain-modulatory cells within the rostral ventromedial
medulla (RVM) ldquo ldquoProstaglandins such as PGE2 are known to function as important mediators in the development of central sensitization and when
applied to the spinal cord produce an allodynic and hyperalgesic staterdquo
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
26
Within the RVM two distinct cell types modulate spinal nociceptive signalsmdash on cells and off cells Tonic activation of off cells is thought to inhibit
nociceptive signals in the dorsal horn whereas activation of on cells supports hyperalgesic states
2013
Nocebo induces anxiety which in turn activates two different and independent biochemical pathways bull A CCK-ergic facilitation of pain and bull The Hypothalamic-Pituitary-
Adrenal (HPA) axis raising plasma ACTH and cortisol
The anti-anxiety drug diazepam prevents both hyperalgesia and HPA activation
The CCK antagonist proglumide inhibits hyperalgesia but not HPA activity
Nocebo Hyperalgesia
F Benedetti Placebo Effects understanding the mechanisms in health and disease Oxford University Press 2009
Placebo amp lsquoNon-Specific Factorsrsquo ldquoWhilst some clinicians are natural walking placebos others
may have to work hard at patientrelationship issues There is a placebonocebo component or percentage in all we do as
cliniciansrdquo Louis Gifford
Listen to the Patient Show Caring
Understanding Empathy
Placebo ndash Further Reading 1) Benedetti F et al Neurobiological mechanisms of the placebo effect The Journal of
Neuroscience 20052510390-10402
2) Scott DJ et al Placebo and nocebo effects are defined by opposite opioid and
dopaminergic responses Archives of General Psychiatry 200865220-231
3) Benedetti F et al How placebos change the patientrsquos brain
Neuropsychopharmacology 201136339-354
4) Wager TD amp Fields H Placebo analgesia In Wall PD amp Melzack Textbook of Pain
httpwagerlabcoloradoedufilespapersWager_Fields_Textbookofpain_tosharepdf
5) Schweinhardt P et al The anatomy of the mesolimbic reward system a link between
personality and the placebo analgesic response The Journal of Neuroscience
2009294882-4887
6) Lidstone SC et al The placebo response as a reward mechanism Seminars in pain
medicine 2005337-42
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain may persist because the original inciting stimulus is still present andor because changes to the nervous system have occurred
making it more sensitive to painrdquo
Lee YC et al Arthritis Research amp Therapy 2011 13211
2011
Chronic Pain
Traditional Definition
Pain Persisting for at least 3 ndash 6 months
ldquoChronic pain has been a mystery because we were just looking at the tissues and joints
while ignoring the nervous system and the brain But It is in the brain and the nervous
system that the action happensrdquo
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time

Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
27
ldquoArising from these data is the striking argument that chronic pain is a disease of the nervous system which distinguishes this phenomena from acute pain that is
frequently a symptom alerting the organism to injury rdquo
2015 In Clinical Practice What Does Pain Tell Us
ldquoSensitisation of Ad and C fibre nerve endings rarely outlast the primary cause for pain ndash thus peripheral sensitisation may be considered as always adaptiverdquo
ldquoIn contrast central changes in the processing of nociceptive information may potentially outlast their
trigger events for days months or even years ndash and may spread to sites remote from the primary cause of painrdquo
Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
In Clinical Practice What Does Pain Tell Us
ldquoWhen the location the duration or the magnitude of pain hyperalgesia and allodynia has become maladaptive rather than protective then the pain is no longer a meaningful homeostatic factor or symptom of a disease but rather a disease in its own rightrdquo Clifford J Woolf
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Central Sensitisation
Definition Enhanced Responsiveness of Nociceptive Neurons in the CNS to their Normal Afferent Input IASP
(Umbrella Term for All Changes in the CNS which Enhance Pain Perception)
Includes
Wind-up and Long Term Potentiation of Dorsal Horn Neurons
Malfunction of Descending Anti-Nociceptive Mechanisms
Altered Sensory Processing in the Brain ndash Cortical Plasticity
Jo Nijs holds a PhD in rehabilitation science and physiotherapy He is a
researcher and assistant professor at the Vrije Universiteit Brussel (Brussels
Belgium) and the Artesis University College Antwerp (Belgium) and he is a
physiotherapist at the University Hospital Brussels His research and clinical interests are patients with chronic painfatigue He has (co-)
authored more than 100 peer reviewed publications and served over
40 times as an invited speaker at national and international meetings
httpbodyinmindorgprimary-care-physical-therapy-treatment-of-fibromyalgia
Dr Jo Nijs
Practice Guidelines by Jo Nijs for the treatment of chronic musculoskeletal pain are being adopted
worldwide within Physical Therapy and
Manual Therapy
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
28
lsquoPathologicalrsquo Central Sensitisation
Frequently Present in Chronic Musculoskeletal Pain Disorders
ldquo implies an increased complexity of the clinical picture (ie an increase in unrelated symptoms and hence a more difficult clinical reasoning process) as
well as decreased odds for a favourable rehabilitation outcomerdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010 Central Sensitisation amp Acute Traumatic Injury
Nociception arising from traumatic injury that has a high lsquoPhysical Threatrsquo andor lsquoPsychological Distressrsquo value is particularly potent at inducing central sensitisation Whiplash injury is a classic example A high percentage of victims who suffer minor whiplash injury (Grade 1 or 2) lapse into chronic pain syndromes or even fibromyalgia This is virtually unknown in those who sustain similar injury on fairground rides
The speed of onset and lsquocontextrsquo of injury is pivotal
httpwwwaddonheadrestcomneckpainhtml
Pain Memories
ldquoA reasoned understanding of pain mechanisms validates the reality of ongoing unrelenting and often
untreatable chronic post-whiplash painrdquo
ldquoAdequate management in the acute stages that recognises the biopsychosocial and hence
neurobiological impact of injuries like whiplash is probably the best hope at this timerdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Volume 384 Issue 9938 12ndash18 July 2014 Pages 109ndash111
ldquoCentral sensitisation in patients with chronic whiplash-associated disorders warrants
treatment of cognitive emotional factors like pain catastrophising hypervigilance and maladaptive beliefs
about illnessrdquo
2014
Chronic whiplash-associated disorders to exercise or not NijsJ and Ickmans K
Soft Tissue Injury
Soft Tissue Healing Review Tim Watson (2009)
(Tissue Healing)
2 Days
3 to 4 Weeks
Soft Tissue Healing Phases amp Timescales
ldquoAn important and ongoing source of pain is required before the process of peripheral sensitisation can establish central
sensitisationrdquo ldquoPain due to damage or inflammation of peripheral tissues is clearly capable of causing chronic widespread painrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Chronic Pain
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
29
Butler D Moseley GL Explain Pain Adelaide NOI Group Publishing 2003
Chronic Pain
ldquo appropriate and effective manual therapy in those with (sub)acute musculoskeletal disorders is important to prevent
evolvement from an acute localised problem to more complex clinical cases characterised by chronic widespread pain rdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Memories
ldquoMemories are hard to get rid of and if ongoing pain has a large memory component it may be beyond any tooltherapy we
presently haverdquo Louis Gifford
ldquo many probably all ongoing pains have a major component of their pain source within the central nervous system in the form of
a somatosensory memory or imprintrdquo ldquothe roots are in the biology of memory and synaptic efficacyrdquo
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
1998
Pain Memories
ldquoMemories can be put into subconsciousness but dragged back up if given the right cues Some memories and experiences may if
given great significance stay continuously in our consciousness rather like an annoying tune or nagging worry tends tordquo
ldquothere has been a gross error in reasoning in the past with the insistence that all pain should have a tissue sourcerdquo
Louis Gifford
httpwwwachesandpainsonlinecom
aboutusphp
Louis Gifford (Topical Issues in Pain 1) 1998
Pain_Chronic
1998 Important Questions for Patients with Acute Musculoskeletal Pain
Have you had pain like this before
Was the original injury emotionally charged
Their present pain experience may be largely on account of reawakening of a pain memory Any
present physical injury may be much less than the perceived level of pain suggests
Pathological Central Sensitisation
ldquoThere is now enough evidence available indicating that chronic pain syndromes such as low back pain whiplash and fibromyalgia share the same pathogenesis namely sensitization of pain modulating systems in the central
nervous system ldquo
van Wilgen CP amp Keizer D The sensitization model to explain how chronic pain exists without tissue damage Pain Management Nursing 201213(1)60-5
2012
Pathological Central Sensitisation
ldquoWhy some of these chronic pain disorders remain localized to few body areas whereas others become
widespread is unclear at this time Genetic environmental and psychosocial factors likely play an
important rolerdquo
Staud R Evidence for shared pain mechanisms in osteoarthritis low back pain and fibromyalgia Current Rheumatology Reports 201113(6)513-20
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time

Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
30
Fibromyalgia ndash Pain Processing Disease
httpdardipaincliniccomfibromyalgiaphp
Location of the 18 tender points that make
up the criteria for identifying fibromyalgia
Patient must feel pain in
at least 11 of these points when a pressure of 4Kgcm2 is applied
Patient must also have
had pain in all 4 quadrants of the body for at least 3 months
Fibromyalgia amp Central Sensitisation
ldquoThe precise etiology and pathogenesis of fibromyalgia syndrome remains undefined and there is no definite curerdquo ldquoFMS is
characterised by sensitisation of the central nervous system which explains the majority of if not all symptomsrdquo Central sensitisation is ldquothe sole feature of FMS pathophysiology that is no longer in debaterdquo
Jo Nijs et al
Nijs J et al Primary care physical therapy in people with fibromyalgia opportunities and boundaries within a monodisciplinary setting Physical Therapy 2010901815-22
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
httpwwwfmcfsmecomresearchers_spotlightphp
ScienceDaily (June 25 2007) mdash Fibromyalgia a chronic widespread pain in muscles and soft tissues accompanied by fatigue is a fairly
common condition that does not manifest any structural damage in an organ Twenty-five years ago Muhammad B Yunus MD and
colleagues published the first controlled study of the clinical characteristics of fibromyalgia syndrome
Further Legitimization Of Fibromyalgia As A True Medical Condition
Yunus MB Fibromyalgia and overlapping disorders the unifying concept of central sensitivity syndromes Seminars in Arthritis and Rheumatism 200736(6)339ndash356
Fibromyalgia 2007
Without question Muhammad Yunus is the father of our modern view of fibromyalgiardquo
John B Winfield MD (accompanying editorial)
ldquoThere is now significant evidence that fibromyalgia is part of a much larger continuum that has been called many things including functional somatic
syndromes medically unexplained symptoms chronic multisymptom illnesses somatoform disorders and perhaps most appropriately central pain or central
sensitivity syndromes ldquo
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
Together these advances have led to an emerging recognition that chronic central
pain itself is a ldquodiseaserdquo and that many of the underlying mechanisms operative in these
heretofore ldquoidiopathicrdquo or ldquofunctionalrdquo pain syndromes may be similar no matter
whether the pain is present throughout the body (eg in FM) or localized to the low
back the bowel or the bladder httpwwwsciencedailycomreleases200706070625095756htm
2011
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia
The notion that fibromyalgia and related syndromes might represent biological amplification of all sensory stimuli has
significant support from functional imaging studies that suggest that the insula is the most consistently hyperactive region This
region has been noted to play a critical role in sensory integration fibromyalgia patients also display a low noxious
threshold to auditory tones httpwwwsciencedailycomreleases200706070625095756htm
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
31
Fibromyalgia
ldquo in FM the stress response system notabably the HPA axis and the sympathetic
nervous system is deregulatedrdquo this can ldquofoster pathological immune activation with
release of pro-inflammatory cytokines provoking a so-called lsquosickness responsersquo
(lethargy and malaise social withdrawal flu-like symptoms concentration difficulties) and generalised pain hypersensitivity)rdquo
httpwwwsciencedailycomreleases200706070625095756htm
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201125141-154
Fibromyalgia amp ldquoFibromyalgia-nessrdquo
httpwwwsciencedailycomreleases200706070625095756htm
many patients with chronic pain disorders have variable degrees of
ldquofibromyalgia-nessrdquo When this occurs we need to treat both the peripheral and
central elements of pain along with other somatic symptoms The era of
evidence-based individualized analgesia in chronic pain is upon us
2011
Fibromyalgia Treatment Considerations
ldquoManual therapists unaware of or ignoring the processes involved in the development and maintenance of chronic
widespread painFM may cause more harm than benefit to the patient by triggering or sustaining central sensitisationrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice Manual Therapy 2009143-12
ldquoFor some therapists central sensitisation remains a theoretical concept that is unlikely to occur in the patients they are treatingrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
httpbestfibromyalgiatreatmentnetpage_id=4
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoClinicians should be aware of the consequences of central sensitisation (ie marked reduced sensory threshold) and adapt their hands-on techniques and exercise programs accordingly
Any therapeutic interventions triggering more pain will serve as a new source of nociceptive barragerdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httplakescenterchirocomchiropractic-carefibromyalgia
ldquoSoft-tissue mobilisation is required to free up restrictions and restore local blood flow However it is important not to increase pain during treatment Starting superficially with well-tolerated
strokes along the length of the muscle fibres and progressing towards deeper strokes that go perpendicular to the soft-tissue
fibres is recommendedrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Fibromyalgia Treatment Considerations
httpbestfibromyalgiatreatmentnetpage_id=4
ldquoAggressive ways of treating trigger points (eg by using ischaemic pressure) are not usually well tolerated and therefore
not recommendedrdquo ldquoSensitised muscle nociceptors are more easily activated and may respond to normally innocuous and weak stimuli such as light pressure and muscle movementrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
32
Fibromyalgia Treatment Considerations
Exercise
ldquoPain thresholds increase during physical activity in healthy individuals and can stay augmented for up to 30 min post-
exercise This is the result of endogenous opioid release and related activation of several (supra)spinal anti-nociceptive
mechanisms such as adrenergic and serotinergic pathwaysrdquo ldquoA constant or decreased pain threshold during and following
exercise suggests malfunctioning of anti-nociceptive mechanisms and hence central sensitisationrdquo
Nijs J et al Recognition of central sensitisation in patients with musculoskeletal pain application of pain neurophysiology in manual therapy practice
Manual Therapy 201015135-141
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2010
Exercise-induced Analgesia
In Healthy Individuals Exercise Stimulates Brain Release of Opioids Pituitary Release of Peripherally Acting Opioids (b-endorphins) Hypothalamus Release of Centrally Acting Opioids (b-endorphins) Eg Via projections to PAG
Also Peripherally Increased Ab fibre input to dorsal horn (Gate Control) and DNIC from muscle ischaemia and lactate accumulation
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Brain centres involved in pain modulation are believed to be stimulated by arterial baroreceptors in response to increasing blood pressure
2012
Fibromyalgia Treatment Considerations
Exercise
Suitable exercises and activities are low-intensity (aqua)aerobics gentle stretching relaxation sessions etc Any post-exertional pain soreness or malaise should be responded
to by cutting back Else very gradual pacing-up may be beneficial in improving exercise and activity tolerance
httpwwwlivestrongcomarticle324688-relaxation-exercises-for-
fibromyalgia
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Central Sensitisation amp Chronic Inflammatory States
Research studies of pain patients with RhA and OA (traditionally considered as peripheral or
nociceptive pain states) indicate that the pain has an important central component
The evidence comes from mechanistic studies (ie experimental pain testing functional neuroimaging and genetic studies) and
therapeutic trials
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
OA like nearly all other chronic pain states is likely a ldquomixed pain staterdquo with individual variability in the relative balance of peripheral (ie nociceptive) and
central elements of pain
httpwwwbuzzlecomarticlesarthritic-fingershtml
Central Sensitisation amp Chronic Inflammatory States
2012
ldquoAs a consequence of their training and education the majority of musculoskeletal therapists are educated in the biomedical model of pain This
traditional model of pain assumes that there is a direct link between the amount of local tissue damage (ie structural joint degeneration) and the pain
experienced by the patient ldquoHowever chronic OA-related pain does not always adhere to this biomedical model of pain It is common to observe a
discordance between the degree of structural joint damage and the amount of symptoms experienced by the patientrdquo
2015
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
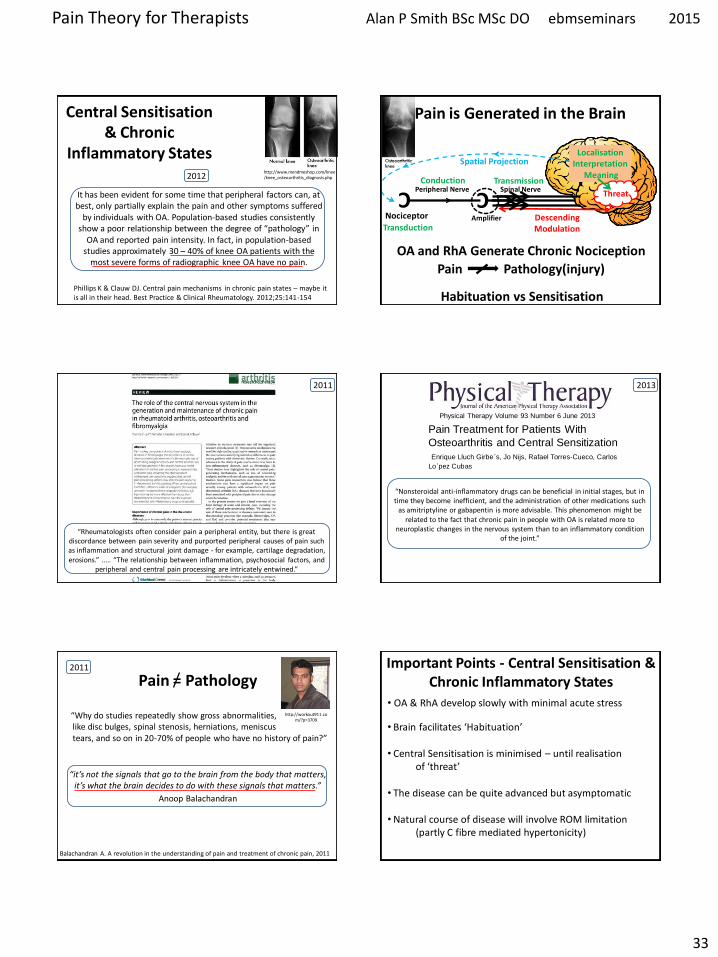
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
33
Phillips K amp Clauw DJ Central pain mechanisms in chronic pain states ndash maybe it is all in their head Best Practice amp Clinical Rheumatology 201225141-154
Central Sensitisation amp Chronic
Inflammatory States
It has been evident for some time that peripheral factors can at
best only partially explain the pain and other symptoms suffered by individuals with OA Population-based studies consistently
show a poor relationship between the degree of ldquopathologyrdquo in OA and reported pain intensity In fact in population-based
studies approximately 30 ndash 40 of knee OA patients with the most severe forms of radiographic knee OA have no pain
httpwwwmendmeshopcomkneeknee_osteoarthritis_diagnosisphp 2012
C
Nociceptor
Peripheral Nerve Conduction
Spinal Nerve Transmission C
Localisation Interpretation
Meaning
Pain is Generated in the Brain
Spatial Projection
Amplifier
Transduction Descending Modulation
Threat
Pain Pathology(injury)
OA and RhA Generate Chronic Nociception
Habituation vs Sensitisation
2011
ldquoRheumatologists often consider pain a peripheral entity but there is great discordance between pain severity and purported peripheral causes of pain such as inflammation and structural joint damage - for example cartilage degradation erosionsrdquo ldquoThe relationship between inflammation psychosocial factors and
peripheral and central pain processing are intricately entwinedrdquo
Pain Treatment for Patients With
Osteoarthritis and Central Sensitization
Enrique Lluch Girbeacutes Jo Nijs Rafael Torres-Cueco Carlos
Loacutepez Cubas
Physical Therapy Volume 93 Number 6 June 2013
ldquoNonsteroidal anti-inflammatory drugs can be beneficial in initial stages but in time they become inefficient and the administration of other medications such
as amitriptyline or gabapentin is more advisable This phenomenon might be related to the fact that chronic pain in people with OA is related more to
neuroplastic changes in the nervous system than to an inflammatory condition of the jointrdquo
2013
ldquoWhy do studies repeatedly show gross abnormalities like disc bulges spinal stenosis herniations meniscus tears and so on in 20-70 of people who have no history of painrdquo
ldquoitrsquos not the signals that go to the brain from the body that matters itrsquos what the brain decides to do with these signals that mattersrdquo
Anoop Balachandran
Pain = Pathology
Balachandran A A revolution in the understanding of pain and treatment of chronic pain 2011
httpworkout911comp=3709
2011 Important Points - Central Sensitisation amp Chronic Inflammatory States
bull OA amp RhA develop slowly with minimal acute stress
bull Brain facilitates lsquoHabituationrsquo
bull Central Sensitisation is minimised ndash until realisation of lsquothreatrsquo
bull The disease can be quite advanced but asymptomatic
bull Natural course of disease will involve ROM limitation (partly C fibre mediated hypertonicity)
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
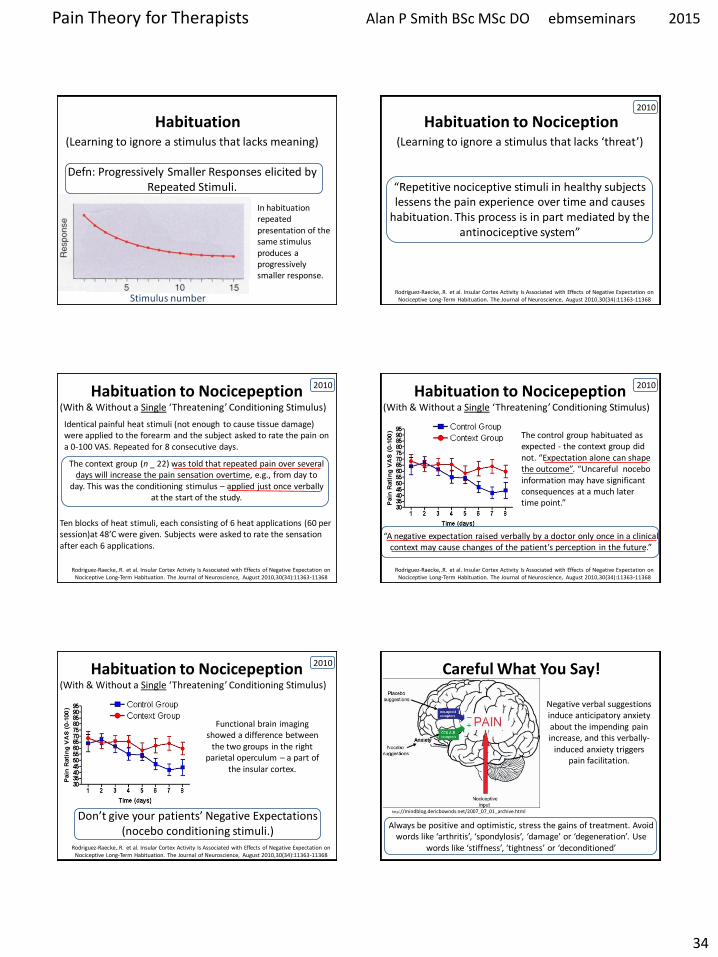
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
34
Habituation (Learning to ignore a stimulus that lacks meaning)
Defn Progressively Smaller Responses elicited by
Repeated Stimuli
In habituation repeated presentation of the same stimulus produces a progressively smaller response
Stimulus number
Habituation to Nociception (Learning to ignore a stimulus that lacks lsquothreatrsquo)
ldquoRepetitive nociceptive stimuli in healthy subjects lessens the pain experience over time and causes
habituation This process is in part mediated by the antinociceptive systemrdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The context group (n _ 22) was told that repeated pain over several days will increase the pain sensation overtime eg from day to
day This was the conditioning stimulus ndash applied just once verbally at the start of the study
Identical painful heat stimuli (not enough to cause tissue damage) were applied to the forearm and the subject asked to rate the pain on a 0-100 VAS Repeated for 8 consecutive days
Ten blocks of heat stimuli each consisting of 6 heat applications (60 per session)at 48rsquoC were given Subjects were asked to rate the sensation after each 6 applications
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
The control group habituated as expected - the context group did not ldquoExpectation alone can shape the outcomerdquo ldquoUncareful nocebo information may have significant consequences at a much later time pointrdquo
ldquoA negative expectation raised verbally by a doctor only once in a clinical context may cause changes of the patientrsquos perception in the futurerdquo
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010
Habituation to Nocicepeption (With amp Without a Single lsquoThreateningrsquo Conditioning Stimulus)
Donrsquot give your patientsrsquo Negative Expectations (nocebo conditioning stimuli)
Functional brain imaging showed a difference between
the two groups in the right parietal operculum ndash a part of
the insular cortex
Rodriguez-RaeckeR et al Insular Cortex Activity Is Associated with Effects of Negative Expectation on Nociceptive Long-Term Habituation The Journal of Neuroscience August 201030(34)11363-11368
2010 Careful What You Say
Negative verbal suggestions induce anticipatory anxiety about the impending pain increase and this verbally-
induced anxiety triggers pain facilitation
httpmindblogdericbowndsnet2007_07_01_archivehtml
Always be positive and optimistic stress the gains of treatment Avoid words like lsquoarthritisrsquo lsquospondylosisrsquo lsquodamagersquo or lsquodegenerationrsquo Use
words like lsquostiffnessrsquo lsquotightnessrsquo or lsquodeconditionedrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
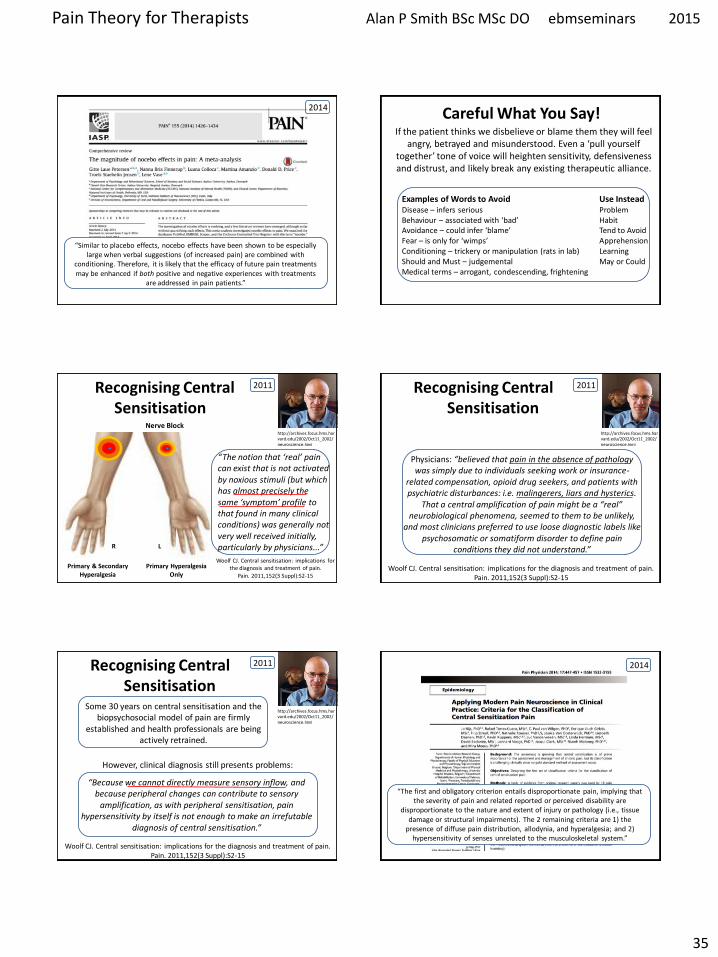
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
35
ldquoSimilar to placebo effects nocebo effects have been shown to be especially large when verbal suggestions (of increased pain) are combined with
conditioning Therefore it is likely that the efficacy of future pain treatments may be enhanced if both positive and negative experiences with treatments
are addressed in pain patientsrdquo
2014 Careful What You Say If the patient thinks we disbelieve or blame them they will feel
angry betrayed and misunderstood Even a lsquopull yourself togetherrsquo tone of voice will heighten sensitivity defensiveness and distrust and likely break any existing therapeutic alliance
Examples of Words to Avoid Use Instead Disease ndash infers serious Problem Behaviour ndash associated with lsquobadrsquo Habit Avoidance ndash could infer lsquoblamersquo Tend to Avoid Fear ndash is only for lsquowimpsrsquo Apprehension Conditioning ndash trickery or manipulation (rats in lab) Learning Should and Must ndash judgemental May or Could Medical terms ndash arrogant condescending frightening
Primary amp Secondary Hyperalgesia
Primary Hyperalgesia Only
Nerve Block
R L
Recognising Central Sensitisation
ldquoThe notion that lsquorealrsquo pain can exist that is not activated by noxious stimuli (but which has almost precisely the same lsquosymptomrsquo profile to that found in many clinical conditions) was generally not very well received initially particularly by physiciansrdquo
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain
Pain 2011152(3 Suppl)S2-15
2011
Physicians ldquobelieved that pain in the absence of pathology was simply due to individuals seeking work or insurance-
related compensation opioid drug seekers and patients with psychiatric disturbances ie malingerers liars and hysterics
That a central amplification of pain might be a ldquorealrdquo neurobiological phenomena seemed to them to be unlikely
and most clinicians preferred to use loose diagnostic labels like psychosomatic or somatiform disorder to define pain
conditions they did not understandrdquo
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
2011
Woolf CJ Central sensitisation implications for the diagnosis and treatment of pain Pain 2011152(3 Suppl)S2-15
httparchivesfocushmsharvardedu2002Oct11_2002neurosciencehtml
Recognising Central Sensitisation
ldquoBecause we cannot directly measure sensory inflow and because peripheral changes can contribute to sensory
amplification as with peripheral sensitisation pain hypersensitivity by itself is not enough to make an irrefutable
diagnosis of central sensitisationrdquo
Some 30 years on central sensitisation and the biopsychosocial model of pain are firmly
established and health professionals are being actively retrained
However clinical diagnosis still presents problems
2011
ldquoThe first and obligatory criterion entails disproportionate pain implying that the severity of pain and related reported or perceived disability are
disproportionate to the nature and extent of injury or pathology (ie tissue damage or structural impairments) The 2 remaining criteria are 1) the
presence of diffuse pain distribution allodynia and hyperalgesia and 2) hypersensitivity of senses unrelated to the musculoskeletal systemrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
36
Recognising (lsquoDysregulatedrsquo) Central Sensitisation
bull Pain persisting beyond expected healing times bull Widespread diffuse pain bull Widespread tissue tenderness to palpation bull Bizarre symptoms disproportionate unpredictable bull Excessive post-treatment soreness bull Exercise exacerbates pain bull Previous similar pain episodes or past traumatic associations bull Anxietyworryangerdepression negative emotions bull Unhelpful beliefs or expectations bull History of failed (manual) treatments ndash or made worse by bull Hypersensitivity to bright light noise highlow temperatures bull Presence of trigger points bull Poor response to analgesics such as NSAIDs respond to TCAs
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
lsquoCognitive-emotional sensitisationrsquo activates forebrain areas that exert powerful influences on various
brainstem nuclei including those identified as the origin of descending pain facilitatory pathways This in
turn sustains the process of central sensitisation
Psychosocial Prevention amp Treatment of lsquoDysregulatedrsquo Central Sensitisation
Introducing CBT
Cognitive-behavioral therapy is an action-oriented form of psychosocial therapy that assumes that maladaptive or faulty thinking patterns cause maladaptive behavior and negative emotions (Maladaptive behavior is behavior that is counter-productive or interferes with everyday living) The treatment
focuses on changing an individuals thoughts (cognitive patterns) in order to change his or her behavior and emotional state
FreeOn-LineDictionary
Cognitive-Behavioural Therapy Should we be giving psychological treatment
ldquoDespite the fact that physiotherapists do not receive CBT training they still may apply some of its principles within their treatmentrdquo
ldquoThis does not suggest that physiotherapists should become
amateur psychologists but be much more aware that psychological factors are involved and that physiotherapists are in a position to influence those factors related to physical fitness and functionrdquo
Louis Gifford
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoThus we demonstrate that central sensitization can be modified volitionally by altering pain-related thoughtsrdquo
2014 Cognitive-Behavioural Therapy
In practice a patient with musculoskeletal type pain symptoms will consult a lsquophysical therapistrsquo If the physical therapist lacks
biopsychosocial understanding of pain he will try to rationalise and treat the problem according to the old Pathoanatomical Model -
and miss important psychosocial barriers to recovery
httpwwwachesandpainsonlinecom
aboutusphp
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
37
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising
2) Fear-Avoidance Syndrome
3) Disuse or Deconditioning Syndrome
4) Hypervigilance
Worried or Anxious thinking generated within the Human Cortex (from Real or Perceived Threat) can Persist over Long Periods
Common Clinical Findings
Cognite-Behavioural Therapy
For patients with low back pain studies have shown that ldquocatastrophising has been found to be seven times more
powerful than any other predictor in predicting the transition from acute to chronic painrdquo ldquofear also appears
to play a rolerdquo
Dr Sean Mackey Associate Professor amp Chief of the Pain Management Division at Stanford University 2011
httpnewsstanfordedunews2006january11med-rein-011106html
Dr Sean Mackey
State of Mind Can Turn Acute Pain to Chronic
2011
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
1) Catastrophising The injury is worse (or worse consequences) than it is
I canrsquot work because of the pain therefore
bull I canrsquot earn any money bull I canrsquot pay the mortgage bull I will lose my house bull My family will leave me bull I have nothing to live for bull There is no point in trying
Therapists Role Be on the lookout for this type of thinking Question as to its origin Offer appropriate explanation and reassurance
httpchipurcom20110801catastrophizing-finding-a-sense-of-peace
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
2) Fear-Avoidance Syndrome Fear of pain and consequent withdrawal from activity in the
belief that even a small amount will cause injury or re-injury
bull Limits activities bull Limits treatment compliance bull Becomes self-perpetuating bull Lessening activity promotes deconditioning amp disability
Therpists Role This usually starts soon after the injury and should be easy to recognise Common in cases of recurring injury Need to
identify movements or activities that are being avoided and confront them with lsquopacedrsquo exercise
httpgoalisticscom201106chronic-pain-management-fear-avoidance-disability
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
3) Disuse or Deconditioning Syndrome Result of Inactivity
bull Tissue weakness Pain increased fatigue decreased function bull Altered patterns of movement and muscle function bull Learned responses and protective habits bull Leads to accelerated degenerative changes
Therpists Role Similar approach as in fear-avoidance Need to identify movements or activities that are being avoided and
confront them with lsquopacedrsquo exercise
httpwwwmerlinochiropracticclinic
comnew-chronic-painhtml
Cognitive-Behavioural Therapy Psychosocial Barriers to Recovery
4) Hypervigilance
bull Excessive preoccupation with their problem bull Excessive attention to bodily sensations bull Obssessional search for a lsquocurersquo (therapists tests) bull Always lsquoat the doctorsrsquo
Therapists Role Need to show empathy and give reassurances Prescribe exercises or encourage activities as a distraction
httpwwwanxietytreatment2com
hypervigilance-and-anxietyhtml
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time

Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
38
Cognitive-Behavioural Therapy Pain - Fear it or Confront it
Vlaeyen amp Geert Fear amp Pain Pain Clinical UpdatesXV6
httpwwwsportsphysionorthsydneycomauchronic_low_back_painphp
Cognitive-Behavioural Therapy
Gifford L Topical Issues in Pain 1Physiotherapy Pain Association Yearbook 1998-1999
httpwwwachesandpainsonlinecom
aboutusphp
ldquoSuccessful cognitive behavioural approaches to pain management stear patients away from a focus on pain
and pain related behaviour and towards positive functional achievementsrdquo
Louis Gifford
CBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT
changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to increased access to executive regions for
reappraisal of pain
ldquoCBT led to increased activations in the ventrolateral prefrontallateral orbitofrontal cortex regions associated with executive cognitive control We suggest that CBT changes the brainrsquos processing of pain through an altered cerebral loop between pain signals emotions and cognitions leading to
increased access to executive regions for reappraisal of painrdquo
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
Pathoanatomical beliefs about pain ie that it must have some lsquoproportionatersquo cause in the tissues may
constitute a psychological barrier to recovery
ldquoPlacebo effects in pain treatment can be enhanced by informing the patients about placebo mechanisms and by explaining their effects to them Such an
educational informative approach ought to explain the placebo effect based on the models of classical conditioning and expectancy but also its neurobiological
bases without overstraining the patientrdquo
2014
ldquoThe course of CBT led to significant improvements in clinical measures of pain and self-efficacy for coping with chronic painrdquo ldquoCBT is a valuable
treatment option for chronic painrdquo
2014
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
39
When to Use CBT Introducing lsquoPain Physiology Educationrsquo
ldquoPain Physiology Education is indicated when
1) The clinical picture is characterised and dominated by central sensitisation
2) Maladaptive pain cognitions illness perceptions or coping strategies are present
Both indications are prerequisites for commencing pain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
2011 When to Use CBT
Introducing lsquoPain Physiology Educationrsquo
ldquoIt is important for clinicians to recognise that pain cognitions such as fear of movement and
catastrophizing are not only of importance to chronic pain patients but may even be crucial at
the stage of acutesubacute musculoskeletal disordersrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2009
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011 When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
Examples of Maladaptive pain cognitions illness perceptions or coping strategies
1) Moderate hip OA Cartilage is eroding away any exercise will accelerate 2) Chronic whiplash Convinced of severe damage lsquoinvisiblersquo to scans 3) Fibromyalgia patient Convinced she has an undetectable lsquonewrsquo virus
Initiating a treatment such as paced exercise is unlikely to be successful in these patients
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
When to Use CBT Introducing lsquoPain Physiology
Educationrsquo
ldquoIt is crucial to change the patientrsquos maladaptive illness perceptions and maladaptive pain
cognitions and to reconceptualise pain before initiating the treatment This can be accomplished
by patient education about central sensitisation and its role in chronic pain a strategy frequently
referred to as lsquopain physiology educationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
Pain Physiology Education
ldquoDetailed pain physiology education is required to reconceptualise pain and to convince the patient that hypersensitivity of the central nervous system
rather than local tissue damage is the cause of their presenting symptomsrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
40
Pain Physiology Education
ldquoPhysiotherapists or other health care professionals are required to provide tailored education to
address individual needsrdquo ldquoface-to-face sessions of pain physiology education in conjunction with
written educational material are effectiverdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
ldquoThe education is presented verbally (explanations by the therapist) and visually (summaries
pictures and diagrams on computer and paper) During the sessions patients are encouraged to ask questions and their input should be used to
individualise the informationrdquo
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Pain Physiology Education
Nijs J et al How to explain central sensitization to patients with lsquounexplainedrsquo chronic musculoskeletal pain Practice guidelines
Manual Therapy 201115413-418
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquoPain physiology education is typically followed by various components of a biopsychosocial-orientated rehabilitation
program like stress management graded activity and exercise therapy It is important for clinicians to introduce
these treatment components during the educational sessions and to explain why and how the various treatment
components are likely to contribute to decreasing the hypersensitivity of the central nervous systemrdquo
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2011
Use of Exercise Motor Control Training
httpwwwricorgaboutusmediacenterpress2010painmedicinenews2010
ldquo manual therapy aimed at improving motor control in symptomatic regionsjoints is likely to have its place in the
prevention of chronicityrdquo Indeed a sustained mismatch between motor activity and sensory feedback is able to
serve as an ongoing source of nociception inside the CNSrdquo ldquoIn case of inaccurate execution of movements due to
deconditioning or joint tissue damage (and consequently altered proprioception) an incongruence is likelyrdquo
Nijs J amp Houdenhove BJ From acute musculoskeletal pain to chronic widespread pain and fibromyalgia application of pain neurophysiology in manual therapy practice
Manual Therapy 2009143-12
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html 2009
ldquoIn acute musculoskeletal pain the main focus for treatment is to reduce the nociceptive trigger Such a focus on peripheral pain generators is often effective
for treatment of (sub)acute musculoskeletal pain In patients with chronic musculoskeletal pain ongoing nociception rarely dominates the clinical
picturerdquo hellip ldquoThe goal of cognition-targeted exercise therapy is systematic desensitization or graded repeated exposure to generate a new memory of
safety in the brain replacing or bypassing the old and maladaptive movement-related pain memoriesrdquo
2015 Use of Exercise
Prescribing of home exercises is extremely useful where there is fear-avoidance deconditioning movement or postural lsquofaultsrsquo
hypervigilance etc to improve function and to serve as a distraction from pain Attention to pain will expand itrsquos cortical representation
Exercise should always be lsquopacedrsquo ie intensity and duration
increased gradually (eg 10 per week) starting from a lsquobasersquo level that is initially comfortably attainable by the patient Warn about the
possibility of lsquoflare-upsrsquo especially if pacing is exceeded but not to worry about it if it happens
If patient says they lsquocanrsquotrsquo do something gently explain that there
are always degrees of lsquocanrsquo
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
41
Use of Exercise in Chronic Pain Patients
Guidelines by Jo Nijs
Exercise is good for all chronic pain sufferers But fibromyalgia and CFS (and also chronic whiplash) are particularly associated with dysfunctional endogenous analgesia in response to aerobic and
local muscle exercise LBP OA and RhA sufferers are more tolerant For more details see paper below
Nijs J et al Dysfunctional endogenous analgesia during exercise in patients with chronic pain to exercise or not to exercise Pain Physician 201215ES203-ES213
httpwwwmeresearchorgukinformationpublicationsconferencesnewhorizons2008html
2012
httpphysical-therapyadvancewebcomArchivesArticle-ArchivesPassion-and-Purposeaspx
dailymailcouk
Use of Exercise
Goals of Pain Therapy
Acute Pain1
bull Provide rapid and effective Analgesia bull Treat the Cause
Chronic Pain2
bull Reduce Pain bull Address Functional Impairment and Depression bull Address Psychosocial Issues 1 Fields HL et al InHarrisonrsquos Principles of Internal Medicine 199853-58 2 Marcus DA Postgraduate Medicine 200311349-66
httpwwwmedscapeorgviewarticle487064
Chronic Pain Induced Cortical Remodelling
Evidence from Brain Imaging Studies
Cortex amp Pain
httpenwikipediaorgwikiPain
Recent advances in brain imaging
technology have vastly increased our
ability to see how the brain processes
pain
Cortical Plasticity
Real time brain scanning (eg fMRI PET) has revealed that
people with chronic pain syndromes show greater
activity in areas of the brain that generate pain and lesser activity in areas that suppress pain than do healthy controls
when subjected to experimental pain
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
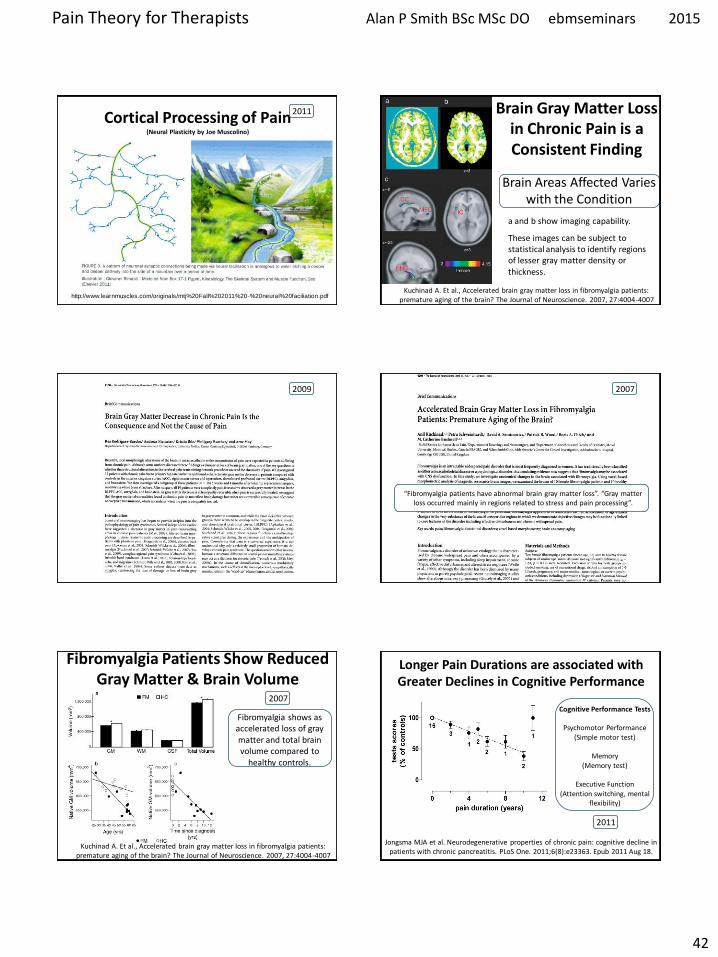
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
42
Cortical Processing of Pain (Neural Plasticity by Joe Muscolino)
httpwwwlearnmusclescomoriginalsmtj20Fall20201120-20neural20faciliationpdf
2011 Brain Gray Matter Loss in Chronic Pain is a Consistent Finding
Brain Areas Affected Varies with the Condition
a and b show imaging capability
These images can be subject to statistical analysis to identify regions of lesser gray matter density or thickness
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2009
ldquoFibromyalgia patients have abnormal brain gray matter lossrdquo ldquoGray matter loss occurred mainly in regions related to stress and pain processingrdquo
2007
Fibromyalgia Patients Show Reduced Gray Matter amp Brain Volume
Fibromyalgia shows as accelerated loss of gray matter and total brain volume compared to
healthy controls
Kuchinad A Et al Accelerated brain gray matter loss in fibromyalgia patients premature aging of the brain The Journal of Neuroscience 2007 274004-4007
2007
Cognitive Performance Tests
Psychomotor Performance (Simple motor test)
Memory
(Memory test)
Executive Function (Attention switching mental
flexibility)
Jongsma MJA et al Neurodegenerative properties of chronic pain cognitive decline in patients with chronic pancreatitis PLoS One 20116(8)e23363 Epub 2011 Aug 18
Longer Pain Durations are associated with Greater Declines in Cognitive Performance
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
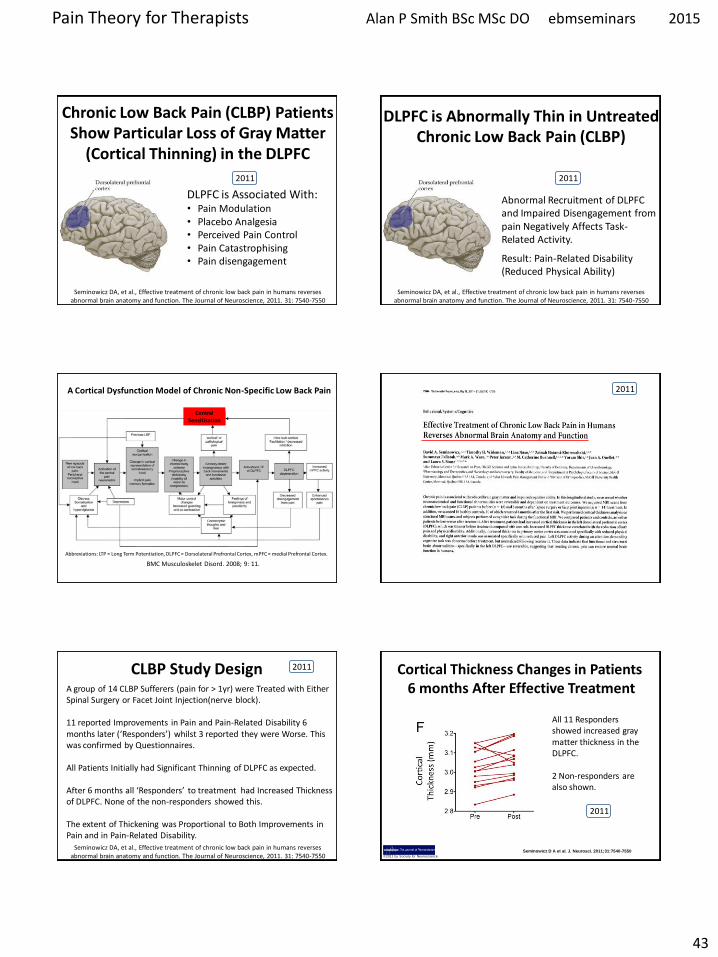
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
43
Chronic Low Back Pain (CLBP) Patients Show Particular Loss of Gray Matter
(Cortical Thinning) in the DLPFC
DLPFC is Associated With bull Pain Modulation bull Placebo Analgesia bull Perceived Pain Control bull Pain Catastrophising bull Pain disengagement
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
DLPFC is Abnormally Thin in Untreated Chronic Low Back Pain (CLBP)
Abnormal Recruitment of DLPFC and Impaired Disengagement from pain Negatively Affects Task-Related Activity
Result Pain-Related Disability (Reduced Physical Ability)
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011
A Cortical Dysfunction Model of Chronic Non-Specific Low Back Pain
BMC Musculoskelet Disord 2008 9 11
Abbreviations LTP = Long Term Potentiation DLPFC = Dorsolateral Prefrontal Cortex mPFC = medial Prefrontal Cortex
Central Sensitisation
2011
CLBP Study Design A group of 14 CLBP Sufferers (pain for gt 1yr) were Treated with Either Spinal Surgery or Facet Joint Injection(nerve block) 11 reported Improvements in Pain and Pain-Related Disability 6 months later (lsquoRespondersrsquo) whilst 3 reported they were Worse This was confirmed by Questionnaires All Patients Initially had Significant Thinning of DLPFC as expected After 6 months all lsquoRespondersrsquo to treatment had Increased Thickness of DLPFC None of the non-responders showed this The extent of Thickening was Proportional to Both Improvements in Pain and in Pain-Related Disability
Seminowicz DA et al Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function The Journal of Neuroscience 2011 31 7540-7550
2011 Cortical Thickness Changes in Patients 6 months After Effective Treatment
Seminowicz D A et al J Neurosci 2011317540-7550 copy2011 by Society for Neuroscience
All 11 Responders showed increased gray matter thickness in the DLPFC 2 Non-responders are also shown
2011
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
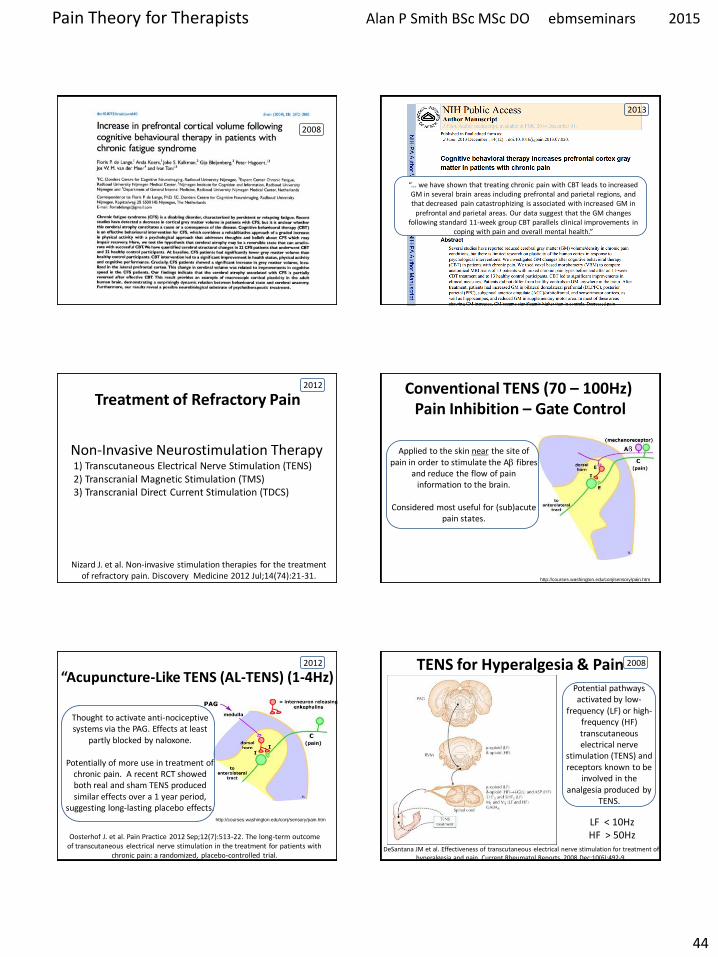
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
44
2008
ldquo we have shown that treating chronic pain with CBT leads to increased GM in several brain areas including prefrontal and parietal regions and that decreased pain catastrophizing is associated with increased GM in
prefrontal and parietal areas Our data suggest that the GM changes following standard 11-week group CBT parallels clinical improvements in
coping with pain and overall mental healthrdquo
2013
Treatment of Refractory Pain
Non-Invasive Neurostimulation Therapy 1) Transcutaneous Electrical Nerve Stimulation (TENS) 2) Transcranial Magnetic Stimulation (TMS) 3) Transcranial Direct Current Stimulation (TDCS)
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory pain Discovery Medicine 2012 Jul14(74)21-31
2012
httpcourseswashingtoneduconjsensorypainhtm
Conventional TENS (70 ndash 100Hz) Pain Inhibition ndash Gate Control
Applied to the skin near the site of pain in order to stimulate the Ab fibres
and reduce the flow of pain information to the brain
Considered most useful for (sub)acute
pain states
ldquoAcupuncture-Like TENS (AL-TENS) (1-4Hz)
httpcourseswashingtoneduconjsensorypainhtm
Thought to activate anti-nociceptive systems via the PAG Effects at least
partly blocked by naloxone
Potentially of more use in treatment of chronic pain A recent RCT showed both real and sham TENS produced similar effects over a 1 year period
suggesting long-lasting placebo effects
Oosterhof J et al Pain Practice 2012 Sep12(7)513-22 The long-term outcome of transcutaneous electrical nerve stimulation in the treatment for patients with
chronic pain a randomized placebo-controlled trial
2012
Potential pathways activated by low-
frequency (LF) or high-frequency (HF) transcutaneous electrical nerve
stimulation (TENS) and receptors known to be
involved in the analgesia produced by
TENS
TENS for Hyperalgesia amp Pain
DeSantana JM et al Effectiveness of transcutaneous electrical nerve stimulation for treatment of hyperalgesia and pain Current Rheumatol Reports 2008 Dec10(6)492-9
LF lt 10Hz HF gt 50Hz
2008
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
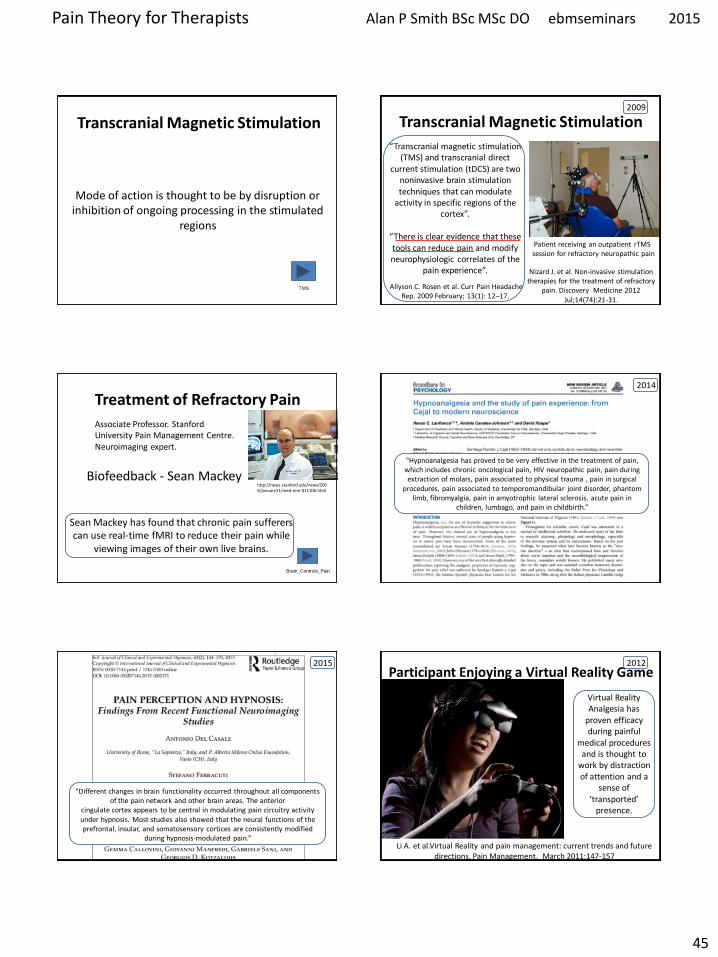
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
45
Transcranial Magnetic Stimulation
Mode of action is thought to be by disruption or
inhibition of ongoing processing in the stimulated regions
TMS
Transcranial Magnetic Stimulation
ldquoTranscranial magnetic stimulation (TMS) and transcranial direct
current stimulation (tDCS) are two noninvasive brain stimulation techniques that can modulate
activity in specific regions of the cortexrdquo
ldquoThere is clear evidence that these tools can reduce pain and modify neurophysiologic correlates of the
pain experiencerdquo
Allyson C Rosen et al Curr Pain Headache Rep 2009 February 13(1) 12ndash17
Patient receiving an outpatient rTMS session for refractory neuropathic pain
Nizard J et al Non-invasive stimulation therapies for the treatment of refractory
pain Discovery Medicine 2012 Jul14(74)21-31
2009
Treatment of Refractory Pain
Biofeedback - Sean Mackey
Brain_Controls_Pain
httpnewsstanfordedunews2006january11med-rein-011106html
Associate Professor Stanford University Pain Management Centre Neuroimaging expert
Sean Mackey has found that chronic pain sufferers can use real-time fMRI to reduce their pain while
viewing images of their own live brains
ldquoHypnoanalgesia has proved to be very effective in the treatment of pain which includes chronic oncological pain HIV neuropathic pain pain during extraction of molars pain associated to physical trauma pain in surgical
procedures pain associated to temporomandibular joint disorder phantom limb fibromyalgia pain in amyotrophic lateral sclerosis acute pain in
children lumbago and pain in childbirthrdquo
2014
ldquoDifferent changes in brain functionality occurred throughout all components of the pain network and other brain areas The anterior
cingulate cortex appears to be central in modulating pain circuitry activity under hypnosis Most studies also showed that the neural functions of the prefrontal insular and somatosensory cortices are consistently modified
during hypnosis-modulated painrdquo
2015 Participant Enjoying a Virtual Reality Game
Li A et alVirtual Reality and pain management current trends and future directions Pain Management March 2011147-157
Virtual Reality Analgesia has
proven efficacy during painful
medical procedures and is thought to
work by distraction of attention and a
sense of lsquotransportedrsquo
presence
2012
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time
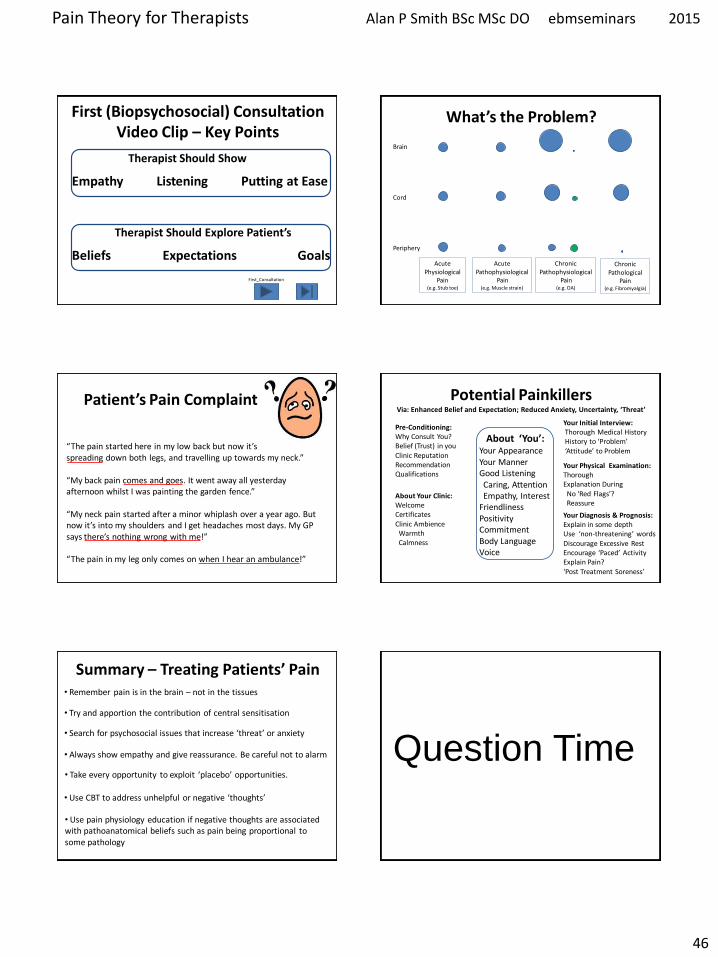
Pain Theory for Therapists Alan P Smith BSc MSc DO ebmseminars 2015
46
First (Biopsychosocial) Consultation Video Clip ndash Key Points
Therapist Should Show
Empathy Listening Putting at Ease
Therapist Should Explore Patientrsquos
Beliefs Expectations Goals
First_Consultation
Whatrsquos the Problem
Brain Cord Periphery
Acute Physiological
Pain (eg Stub toe)
Acute Pathophysiological
Pain (eg Muscle strain)
Chronic Pathophysiological
Pain (eg OA)
Chronic Pathological
Pain (eg Fibromyalgia)
Patientrsquos Pain Complaint
ldquoThe pain started here in my low back but now itrsquos spreading down both legs and travelling up towards my neckrdquo ldquoMy back pain comes and goes It went away all yesterday afternoon whilst I was painting the garden fencerdquo ldquoMy neck pain started after a minor whiplash over a year ago But now itrsquos into my shoulders and I get headaches most days My GP says therersquos nothing wrong with merdquo ldquoThe pain in my leg only comes on when I hear an ambulancerdquo
Potential Painkillers Via Enhanced Belief and Expectation Reduced Anxiety Uncertainty lsquoThreatrsquo
Pre-Conditioning Why Consult You Belief (Trust) in you Clinic Reputation Recommendation Qualifications
About lsquoYoursquo Your Appearance Your Manner Good Listening Caring Attention Empathy Interest Friendliness Positivity Commitment Body Language Voice
Your Initial Interview Thorough Medical History History to lsquoProblemrsquo lsquoAttitudersquo to Problem
Your Diagnosis amp Prognosis Explain in some depth Use lsquonon-threateningrsquo words Discourage Excessive Rest Encourage lsquoPacedrsquo Activity Explain Pain lsquoPost Treatment Sorenessrsquo
About Your Clinic Welcome Certificates Clinic Ambience Warmth Calmness
Your Physical Examination Thorough Explanation During No lsquoRed Flagsrsquo Reassure
Summary ndash Treating Patientsrsquo Pain bull Remember pain is in the brain ndash not in the tissues
bull Try and apportion the contribution of central sensitisation
bull Search for psychosocial issues that increase lsquothreatrsquo or anxiety
bull Always show empathy and give reassurance Be careful not to alarm
bull Take every opportunity to exploit lsquoplaceborsquo opportunities
bull Use CBT to address unhelpful or negative lsquothoughtsrsquo
bull Use pain physiology education if negative thoughts are associated with pathoanatomical beliefs such as pain being proportional to some pathology
Question Time


















