With your host…Ms. Turner! Cancer & Biotechnology Test Review.
Upload
apple-cherry-deziplesCategory
view
217download
0
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 1/31
Bladder Cancer
Description
1. Bladder cancer is papillomatous growth in the bladder urothelium that undergo malignant change
and that may infiltrate the bladder wall.
2. Predisposing factors include cigarette smoking, exposure to industrial chemicals and exposure to
radiation.3. Common signs of metastasis include the liver, bones and lungs
4. As the tumor progresses can extend to the rectum, vagina and retro- peritoneal structures.
Assessment
Painless hematuria
Dysuria
Gross hematuria
Obstruction of urine flow
Development of fistula ( urine from the vagina, fecal material in the urine)
Diagnostic Evaluation
Biopsies of the tumor and adjacent mucosa are definitive, but the following procedures are also used:
Cystoscopy, biopsy of tumor and adjacent mucosa
Excretory urography
Computed CT Scan
Ultrasonography
Bimanual examination by anesthesia
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 2/31
Cytologic evaluation of fresh urine and saline bladder washings
Molecular assays, bladder tumor antigens, adhesion molecules and others are being studied.
Primary Nursing Diagnosis
Risk for altered urinary elimination related to the obstruction of urinary flow
Medical Management
Radiation
1. Most bladder cancer are poorly radio sensitive and require high doses of radiation
2. Radiation therapy is more acceptable for advance disease that cannot be eradicated by surgery.
3. Palliative radiation maybe used to relieve pain and bowel obstruction and control potential
hemorrhage and leg edema cause by venous or lymphatic obstruction.4. Intracavitary radiation maybe prescribed which protect adjacent tissues.
5. External radiation combined with chemotherapy or surgery maybe prescribed because the externaradiation alone may be ineffective.
6. Complications of radiations:
a. A bacterial cystitis
b. Proctitis
c. Fistula formation
d. Ileitis or colitise. Bladder ulceration and hemorrhage
Chemotherapy
1. Intravesical instillation
An alkylating chemotherapeutic agent is instilled into the bladder
This method provides an concentrated topical treatment with little systemic absorption
Chemotherapeutic agents used may include thiotepa, mitomycin (Mutamycin), doxorubicin(Adriamycin), cyclophosphamide (Cytoxan), and bacille Calmette-Guerin.
The medication is injected into a urethral catheter and retain for two hours.
Following instillation, the clients position is rotated every 15 to 30 minutes, starting in the supine
position to avoid lying on full bladder. After 2 hours, the client voids in a sitting position and is instructed to increase fluids to flash the
bladder.
Treat the urine as biohazard and send to radioisotope laboratory for monitoring.
For 6 hours following intravesical therapy, disinfect the toilet with household bleach after the
client has voided.

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 3/31
2. Systemic chemotherapy
Systemic chemotherapy is used to treat inoperable or late tumors.
Agents used may include, cysplatin (Platinol), doxorubicin (Adremycin), cyclophospamide(Cytosan), methotrexate (Folex) and Pyridoxine
3. Complications of chemotherapy
Bladder irritation
Hemorrhagic cystitis
Surgical Interventions
1. Transurethral resection of the bladder
Local resection and fulguration ( destruction of tissue by electrical current through electrodes
place in direct contact with the tissue) Perform for early tumor for cure or for inoperable tumors for palliation.
2. Partial Cystectomy
Partial cystectomy is the removal of up to half of the bladder
The procedure is done for early tumors and for clients who cannot tolerate radical cystectomy.
During the initial postoperative period bladder capacity is reduced greatly to about 60 mL;however, as the bladder tissue expand, the capacity increases to 200 -400 mL.
Maintenance of a continuous output of urine following surgery is critical to prevent bladder
distention and stress on the suture line.
A urethral catheter and a suprapubic catheter maybe in place, in the suprapubic catheter maybeleft in place for 2 weeks until healing occurs.
3. Cystectomy and urinary diversion
The procedure involves removal of the bladder and urethra in the women, and the bladder, theurethra, and usually the prostrate and seminal vesicles in men.
When the bladder and urethra are remove, permanent urinary diversion is required.
The surgery may be performed into stages if the tumor is expensive, with the creation of the
urinary diversion first and the cystectomy several weeks later.
If a radical cystectomy is performed lower extremity lymphedema may occur as a result of lymp
node dissection, and impotence may occur in the client.
4. Ileal conduit
The ileal conduit also is called ureteroileostomy or Bricker’s procedure.
Ureters are implanted into a segment of the ileum, with the formation of an abdominal stoma.
The urine flows into the conduit and is propelled continually out through the stoma by peristalsis
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 4/31
The client is required to wear an appliance over the stoma to collect the urine.
Complications include obstruction, pyelonephritis, leakage at the anastomosis site, stenosis,
hydronephrosis, calculuses, skin irritation and ulceration, and stomal defects.
5. Kock pouch
The Koch pouch is a continent internal ileal reservoir created from a segment of the ileum and
ascendingcolon.
The ureters are implanted into the side of the reservoir, and a special nipple valve is constructed t
attach the reservoir to the skin.
Postoperatively, the client will have a 24 to 26 Foley catheter in place to drain urine continuously
until the pouch has healed.
The catheter is irrigated gently with NS to prevent obstruction from mucus or clots.
Following removal of the catheter, the client is instructed in how to self-catheterize and to drainthe reservoir at 4 to 6 hour intervals.
6. Indiana pouch
A continent reservoir is created from the ascending colon and terminal ileum, making a pouchlarger than the Koch pouch.
Postoperatively, the client will have a 24 to 26 Foley catheter in place to drain urine continuously
until the pouch has healed.
The Foley catheter is irrigated gently with NS to prevent obstruction from mucus or clots.
Following removal of the Foley catheter, the client is instructed in how to self-catheterize and to
drain the reservoir at 4 to 6 hour intervals.
7. Creation of a neobladder
Creation of a neobladder is similar to the creation of an internal reservoir, with the differencebeing that instead of emptying through an abdominal stoma, the bladder empties through a pelvic
outlet into the urethra.
The client empties the neobladder by relaxing the external sphincter and creating abdominalpressure or by intermittent self- catheterization.
8. Percutaneous nephrostomy or pyelostomy
These procedures are used when the cancer is inoperable to prevent obstruction.
The procedures involve a percutaneous or surgical insertion of a nephrostomy tube into the kidne
for drainage. Nursing interventions involves stabilizing the tube to prevent dislodgement and monitoring
output.

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 5/31
9. Ureterostomy
Ureterostomy may be performed as a palliative procedure if the ureters are obstructed by the
tumor.
The ureters are attached to the surface of the abdomen, where the urine flows directly into a
drainage appliance without a conduit. Potential problems include infection, skin irritation,and obstruction to urinary flow as a result of
strictures at the opening.
10. Vesicostomy
The bladder is sutured to the abdomen, and a stoma is created in the bladder wall.
The bladder empties through the stoma.
Pharmacologic Intervention
Chemotheraphy with a combination of methotrexate, 5-fluorouracil (5-FU), vinblastine,doxorubicin (Adriamycin), and cisplatin (M-VAC) and new agents gemcitabine and taxane,
possibly by topical chemotheraphy applied directly to the bladder wall
Intravesical BCG (effective with superficial transitional cell carcinoma)
Cytotoxic agent infusions through the arterial supply of the involved organ
Formalin, phenol, or silver nitrate instillations to achieve relief of hematuria and strangury (slow
and painful discharge of urine) in some patients
Nursing Intervention
For patients who require radical cystectomy with urinary diversion, offer support and reinforcement of
the information. Be sure what to expect. Involve another family member in the preoperative education. If
it is needed, arrange a preoperative visit by someone who has adjusted well to a similar diversion.
If any type of stoma is to be created, arrange for a preoperative visit from the enterostomal therapist. The
enterostomal therapist can assist in the selection and marking of the stoma site (although the stoma site i
somewhat contingent upon the type of urinary diversion to be performed) and can introduce the patient tothe external urine collection pouch and related care.
Preoperative interventions
1. Administer bowel preparation as prescribed, which may include a clear liquid diet, laxatives and
enemas, and antibiotics to lower the bacterial count in the bowel.
2. Assist the surgeon and the enterostomal nurse in selecting an appropriate skin site for creation of the abdominal stoma.
3. Encourage the client to talk about his or her feelings related to the stoma creation.
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 6/31
Postoperative interventions
1. Monitor Vital signs.
2. Assess incision site.3. Assess stoma (should be red and moist) every hour for the first 24 hours.
4. Monitor for edema in the stoma, which may be present in the immediate postoperative period.5. If the stoma appears dark and dusky, notify the physician immediately because this indicates
necrosis
6. Monitor for prolapse or retraction of the stoma.
7. Assess for return of bowel function; monitor for peristalsis, which will return in 3 to 4 days.
8. Maintain NPO status as prescribed until bowel sounds return.9. Monitor urine flow, which is continuous (30 to 60 mL per hour) following surgery.
10. Notify the physician if the urine output is less than 30 mL an hour or if no urine output occurs for
more than 15 minutes.
11. Ureteral stents or catheters may be in place for 2 to 3 weeks or until healing occurs; maintainstability with catheters to prevent dislodgment.
12. Monitor urinary output closely and irrigate catheter (if present ) gently to prevent obstruction, asprescribed, with 60 mL of NS.
13. Monitor for hematuria.
14. Monitor for signs of peritonitis.
15. Monitor for bladder distention following a partial cystectomy.16. Monitor for shock, hemorrhage, thrombophlebitis, and lower extremity lymphedema following a
radical cystectomy.
17. Monitor the urinary drainage pouch for leaks, and check skin integrity.
18. Monitor the pH of the urine (do not place the dipstick in the stoma) because strong alkali urinecan cause skin irritation and facilitate crystal formation.
19. Instruct the client regarding the potential for urinary tract infection or the development of the
calculuses.20. Instruct the client to assess the skin for irritation and to monitor the urinary drainage pouch for
any leakage.
21. Encourage the client to express feelings about changes in body image, embarrassment, and sexualdysfunction.
Documentation Guidelines
Description of all dressings, wounds, and drainage-collection devices
Physical findings related to the pulmonary assessment, abdominal assessment, presence of edema
condition of extremities, bowel and bladder patterns of voiding Response to and side effects experienced related to intravesical instillations of chemotherapy or
BCG; systemic chemotherapy
Teaching performed, the patient’s understanding of the content, the patient’s ability to performprocedures demonstrated
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 7/31
Discharge and Home Healthcare Guidelines
PATIENT TEACHING
Following creation of an ileal conduit, teach the patient and significant others the care of the
stoma and urinary drainage system. If needed, arrange for follow-up home nursing care or visitswith an enterostomal therapist.
Teach the patient the specific procedure to catheterize the continent cutaneous pouch or reservoir
A simple stoma covering made from a feminine hygiene pad can be worn between
catheterizations.
Stress the need for the patient to wear a medical ID bracelet.
Following orthotopic bladder replacement, teach the patient how to irrigate the Foley catheter.
Suggest the use of a leg bag during the day and a Foley drainage bag at night. Once the pouch has
healed and the Foley catheter, ureteral stents, and pelvic drain have been removed, teach the
patient to ―push‖ or ―bear down‖ with each voiding.
Instruct the patient on methods for performing Kegel exercises during and between voidings to
minimize incontinence. Suggest wearing incontinence pads until full control is achieved. Also instruct the patient on self-catheterization techniques in case the patient is unable to void.
Instruct patients where to obtain ostomy pouches, catheters, and other supplies. Teach the patient
how to clean and store catheters between used following the clean technique.
CARE OF SKIN IN EXTERNAL RADIATION FIELD
Encourage the patient to verbalize concerns about radiation therapy, and reassure the patient that
she or he is not ―radioactive.‖ Instruct the patient to wash skin gently with mild soap, rinse withwarm water, and pat the skin dry each day but not to wash off the ink marking that outlines the
radiation field.
Encourage the patient to avoid applying any lotions, perfumes, deodorants, or powder to thetreatment area.
Encourage the patient to wear nonrestrictive soft cotton clothing directly over the treatment areaand to protect the skin from sunlight and extreme cold.
Stress the need to maintain the schedule for follow-up visits and disease surveillance as
recommended by the physician.

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 8/31
Breast Cancer
Figure 1 Lump changes in breast cancer
Description
1. Is the leading type of cancer in women.Most breast cancer begins in the lining of the milk ducts,sometimes the lobule.
2. The cancer grows through the wall of the duct and into the fatty tissue.
3. Breast cancer metastasizes most commonly to auxiliary nodes, lung, bone, liver, and the brain.
4. The most significant risk factors for breast cancer are gender (being a woman) and age (growingolder).
5. Other probable factors include nulliparity, first child after age 30, late menopause, early
menarche, long term estrogen replacement therapy, and benign breast disease.
6. Controversial risk factors include oral contraceptive use, alcohol use, obesity, and increased
dietary fat intake.7. About 90% of breast cancers are due not to heredity, but to genetic abnormalities that happen as a
result of the aging process and life in general.8. A woman’s risk of breast cancer approximately doubles if she has a first-degree relative (mother,
sister, daughter) who has been diagnosed with breast cancer. About 20-30% of women diagnosed
with breast cancer have a family history of breast cancer.

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 9/31
Stages of Breast Cancer
STAGE DEFINITION
Stage 0 Cancer cells remain inside the breast duct, without invasion intonormal adjacent breast tissue.
Stage I Cancer is 2 centimeters or less and is confined to the breast (lymph
nodes are clear).
Stage IIA No tumor can be found in the breast, but cancer cells are found in
the axillary lymph nodes (the lymph nodes under the arm)
OR
the tumor measures 2 centimeters or smaller and has spread to the
axillary lymph nodes
OR
the tumor is larger than 2 but no larger than 5 centimeters and has not
spread to the axillary lymph nodes.
Stage IIB The tumor is larger than 2 but no larger than 5 centimeters and has spread
to the axillary lymph nodes
OR
the tumor is larger than 5 centimeters but has not spread to the axillary
lymph nodes.Stage IIIA No tumor is found in the breast. Cancer is found in axillary lymph
nodes that are sticking together or to other structures, or cancer may be
found in lymph nodes near the breastbone
OR
the tumor is any size. Cancer has spread to the axillary lymphnodes, which are sticking together or to other structures, or cancer may
be found in lymph nodes near the breastbone.
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 10/31
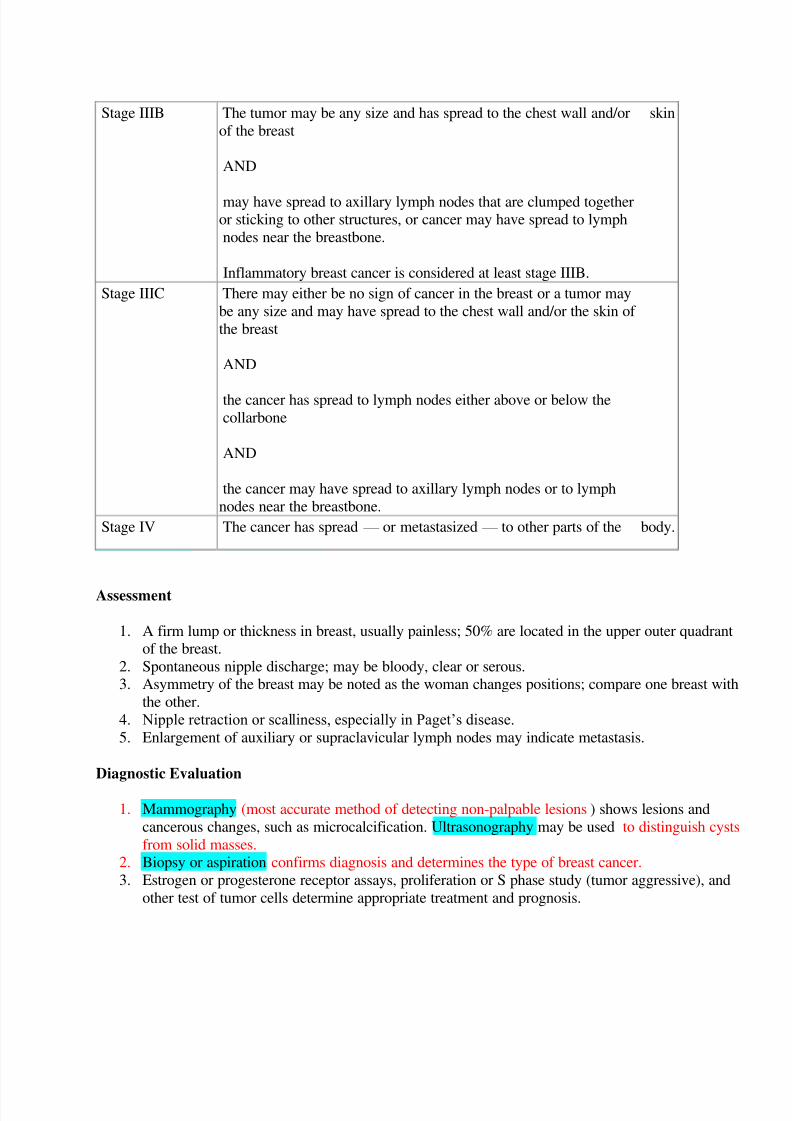
Stage IIIB The tumor may be any size and has spread to the chest wall and/or skin
of the breast
AND
may have spread to axillary lymph nodes that are clumped togetheror sticking to other structures, or cancer may have spread to lymph
nodes near the breastbone.
Inflammatory breast cancer is considered at least stage IIIB.
Stage IIIC There may either be no sign of cancer in the breast or a tumor may
be any size and may have spread to the chest wall and/or the skin of
the breast
AND
the cancer has spread to lymph nodes either above or below the
collarbone
AND
the cancer may have spread to axillary lymph nodes or to lymph
nodes near the breastbone.
Stage IV The cancer has spread — or metastasized — to other parts of the body.
Assessment
1. A firm lump or thickness in breast, usually painless; 50% are located in the upper outer quadrantof the breast.
2. Spontaneous nipple discharge; may be bloody, clear or serous.3. Asymmetry of the breast may be noted as the woman changes positions; compare one breast with
the other.
4. Nipple retraction or scalliness, especially in Paget’s disease.
5. Enlargement of auxiliary or supraclavicular lymph nodes may indicate metastasis.
Diagnostic Evaluation
1. Mammography (most accurate method of detecting non-palpable lesions) shows lesions and
cancerous changes, such as microcalcification. Ultrasonography may be used to distinguish cysts
from solid masses.2. Biopsy or aspiration confirms diagnosis and determines the type of breast cancer.
3. Estrogen or progesterone receptor assays, proliferation or S phase study (tumor aggressive), and
other test of tumor cells determine appropriate treatment and prognosis.
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 11/31
4. Blood testing detects metastasis; this includes liver function tests to detect liver metastasis andcalcium and alkaline phosphatase levels to detect bony metastasis.
5. Chest x-rays, bone scans, or possible brain and chest CT scans detect metastasis.
Primary Nursing Diagnosis
Body image disturbance related to significance of loss of part or all of the breast
Pharmacological Intervention
1. Chemotherapy is the primary used as adjuvant treatment postoperatively; usually begins 4 weeksafter surgery (very stressful for a patient who just finished major surgery).
o Treatments are given every 3 to 4 weeks for 6 to 9 months. Because the drugs differ in
their mechanisms of action, various combinations are used to treat cancer.
o Principal breast cancer drugs include cyclosphosphamide, methotrexate, fluorouracil,doxorubicin, and paclitaxel.
o Additional agents for advanced breast cancer include docetaxel, vinorelbine, mitoxantronand fluorouracil.
o Herceptin is a monoclonal antibody directed against Her-2/neu oncogene; may be effectiv
for patients who express this gene
2. Indications for chemotherapy include large tumors, positive lymph nodes, premenopausal womenand poor prognostic factors.
3. Chemotheraphy is also used as primary treatment in inflammatory breast cancer and as palliative
treatment in metastatic disease or recurrence.4. Anti-estrogens, such as tamoxifen, are used as adjuvant systemic therapy after surgery.
5. Hormonal agents may be used in advanced disease to induce remissions that last for months toseveral years.
Surgical Interventions
1. Surgeries include lumpectomy (breast-preventing procedure), mastectomy (breast removal), andmammoplasty (reconstructive surgery).
2. Endocrine related surgeries to reduce endogenous estrogen as a palliative measure.
3. Bone marrow transplantation may be combined with chemotherapy.

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 12/31
Figure 2: Lumpectomy
Figure 3: Mammoplasty

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 13/31
Figure 4 Modified radical mastectomy
Nursing Interventions
1. Monitor for adverse effects of radiation therapy such as fatigue, sore throat, dry cough, nausea,
anorexia.2. Monitor for adverse effects of chemotherapy; bone marrow suppression, nausea and vomiting,
alopecia, weight gain or loss, fatigue, stomatitis, anxiety, and depression.
3. Realize that a diagnosis of breast cancer is a devastating emotional shock to the woman. Provide
psychological support to the patient throughout the diagnostic and treatment process.4. Involve the patient in planning and treatment.
5. Describe surgical procedures to alleviate fear.
6. Prepare the patient for the effects of chemotherapy, and plan ahead for alopecia, fatigue.
7. Administer antiemetics prophylactically, as directed, for patients receiving chemotherapy.8. Administer I.V. fluids and hyperalimentation as indicated.
9. Help patient identify and use support persons or family or community.
10. Suggest to the patient the psychological interventions may be necessary for anxiety, depression, osexual problems.
11. Teach all women the recommended cancer-screening procedures.
Documentation Guidelines
Response to surgical interventions: Condition of dressing and wound, stability of vital signs,
recovery from anesthesia Presence of complications: Pain, edema, infection, seroma, limited ROM
Knowledge of and intent to comply with adjuvant therapies
Reaction to cancer and body changes
Knowledge of and intent to comply with incision care, postoperative exercises, arm precautions,
follow-up care, and early detection methods for recurrence
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 14/31
Discharge and Home Healthcare Guidelines
PATIENT TEACHING
The patient can expect to return home with dressings and wound drains. Instruct the patient to do
the following: empty the drainage receptacle twice a day, record the amount on a flow sheet, andtake this information along when keeping a doctor’s appointment; report symptoms of infection oexcess drainage on the dressing or the drainage device; sponge bathe until the sutures and drains
are removed; continue with daily lower arm ROM exercises until the surgeon orders more
strenuous exercises; avoid caffeinated foods and drinks, nicotine, and secondary smoke for 3
weeks postoperatively. Review pain medication instructions for frequency and precautions.
Teach precautions to prevent lymphedema after node dissection (written directions or pamphlet
from American Cancer Society [ACS] is desirable for lifetime referral):
Request no blood pressure or blood samples from affected arm.
Do not carry packages, handbags, or luggage with the affected arm; avoid elastic cuffs.
Protect the hand and arm from burns, ticks, and cuts by wearing gloves to do gardening and
housework, using a thimble to sew, applying sunscreen and insect repellent when out-of-doors.Report swelling, pain, or heat in the affected arm immediately. Put the arm above the head andpump the fist frequently throughout the day.
FOLLOW-UP
Prepare the patient and family for a variety of encounters with healthcare providers (radiologist,oncologist, and phlebotomist). Try to provide a continuity between the providers (yourself,
clinical nurse specialist, or nurse consultant system, if available) as a resource for the patient or
family to call with questions.
Provide lists and information of local community resources and support groups for emotional
support: Reach to Recovery, Y-ME, Wellness Center, Can Surmount, I Can Cope; a list of businesses that specialize in breast prostheses; phone numbers for ACS and Cancer Information
System

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 15/31
Colorectal Cancer
Description
Adenocarcinoma is the most common type of colon cancer and may spread by direct extension
through the walls of the intestine or through the lymphatic or circulatory system. Metastasis ismost often to the liver.
Duke’s Classification of Colorectal Cancer
Stage A: confined to bowel mucosa, 80-90 % 5 years survival rate
Stage B: invading muscle wall
Stage C; Lymph node involvement
Stage D: Metastases or locally unresectable tumor, less than 5% , 5 years survival rate.
Causes/ Risk Factors
Modifiable
Diet: Whether diet plays a role in developing colon cancer remains under debate. The belief that a
high-fiber, low-fat diet could help prevent colon cancer has been questioned. Studies do indicate
that exercise and a diet rich in fruits and vegetables can help prevent colon cancer. Obesity: Obesity has been identified as a risk factor for colon cancer. Smoking: Cigarette smoking has been definitely linked to a higher risk for colon cancer. Drug effects: Recent studies have suggested that estrogen replacement therapy and nonsteroidal
anti-inflammatory drugs such as aspirin may reduce colorectal cancer risk.
Non-Modifiable
Most colorectal cancers arise from adenomatous polyps-clusters of abnormal cells in the glandscovering the inner wall of the colon. Over time, these abnormal growths enlarge and ultimatelydegenerate to become adenocarcinomas.
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 16/31
People with any of several conditions known as adenomatous polyposis syndromes have a greater-than-normal risk of colorectal cancer.
In these conditions, numerous adenomatous polyps develop in the colon, ultimately leading to
colon cancer. The cancer usually occurs before age 40 years. Adenomatous polyposis syndromes tend to run in families. Such cases are referred to as familial
adenomatous polyposis (FAP). Celecoxib (Celebrex) has been FDA approved for FAP. After 6months, celecoxib reduced the mean number of rectal and colon polyps by 28% compared toplacebo (sugar pill) 5%.
Another group of colon cancer syndromes, termed hereditary nonpolyposis colorectal cancer (HNPCC
syndromes, also run in families. In these syndromes, colon cancer develops without the precursor polyps
HNPCC syndromes are associated with a genetic abnormality. This abnormality has been
identified, and a test is available. People at risk can be identified through genetic screening. Once identified as carriers of the abnormal gene, these people require counseling and regular
screening to detect precancerous and cancerous tumors. HNPCC syndromes are sometimes linked to tumors in other parts of the body.
Also at high risk for developing colon cancers are people with any of the following:
Ulcerative colitis or Crohn colitis (Crohn disease) Breast, uterine, or ovarian cancer now or in the past A family history of colon cancer
The risk of colon cancer increases 2-3 times for people with a first-degree relative (parent or
sibling) with colon cancer. The risk increases more if you have more than one affected familymember, especially if the cancer was diagnosed at a young age.
Assessment
Ascending (Right) Colon Cancer
Occult blood blood in stool
Anemia
Anorexia and weight loss
Abdominal pain above umbilicus Palpable mass

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 17/31
Distal Colon/ Rectal Cancer
Rectal bleeding
Change bowel habits
Constipation or diarrhea Pencil or ribbon shaped stool
Tenesmus
Sensation of incomplete
Diagnostic Evaluation
Fecal occult blood test (FOBT) - checks for hidden blood in the stool. Sometimes cancers orpolyps can bleed and this test is used to pick up small amounts of bleeding. Have this test every
year.
Flexible sigmoidoscopy - an exam where a health care provider looks at the rectum and the lowerpart of the colon using a sigmoidoscope, a tube with a light on the end. Have this test every 5
years.
Colonoscopy - an exam when a health care provider looks at the rectum and the entire colon usinga colonoscope, an instrument with a light on the end. If polyps are found, they can be removed.
Have this test every 5 to 10 years.
Double contrast barium enema (DCBE) - a series of x-rays of the colon and rectum. You are firstgiven an enema with barium in it, which outlines the colon and rectum on the x-rays. Have this
test every 5 to 10 years (only if not having a colonoscopy every 10 years).
Digital rectal exam - a health care provider inserts a lubricated, gloved finger into the rectum to
feel for any problem areas. Have this test every 5 to 10 years at the time of other screening tests
(flexible sigmoidoscopy, colonoscopy, or DCBE).
Primary Nursing Diagnosis
Pain related to tissue injury from tumor invasion and the surgical incision
Therapeutic Intervention / Medical Management
Treatment of cancer depends on stage of disease and related complications. Obstruction is treated with
intravenous fluids and nasogastric suction and with blood therapy if bleeding is significant. Supportivetherapy and adjuvant therapy (e.g., chemotherapy, radiation therapy, immuno therapy) are included.
Surgical Management
Surgery is the primary treatment for most colon and rectal cancers; the type of surgery depends on
the location and size of tumor, and it may be curative or palliative.

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 18/31
Cancers limited to one site can be removed to a colonoscope
Laparoscopy colostomy with polypectomy.
Neodymium-yttrium-aluminum-garnet (Nd:YAG) laser is effective in some lesions
Bowel resection with anastomosis and possible temporary or permanent colostomy or illeostomy
less than 1/3 of patients) or coloanal resevoir (colonic J pouch).
Pharmacologic Intervention
Narcotic analgesic is often administered as patient-controlled anesthesia to manages surgical painor pain from metastasis
Nursing Intervention
Administer chemotherapy agents as ordered; provide care for the client receiving chemotherapy.
Provide care for the client receiving radiation therapy.
Provide care for the client with bowel surgery.
Documentation Guidelines
Response to diagnosis of colorectal cancer, diagnostic tests, and treatment regimen
Description of all dressings, wounds, and drainage collection devices: Location of drains; color
and amount of drainage; appearance of the incision; color of the ostomy stoma; presence, amount
and consistency of ostomy effluent
Discharge and Home Healthcare Guidelines
PATIENT TEACHING
Teach the patient the care related to the abdominal incision and any perineal wounds. Giveinstructions about when to notify the physician (if the wound separates or if any redness, bleeding
purulent drainage, unusual odor, or excessive pain is present).
Advise the patient not to perform any heavy lifting (10 lbs), pushing, or pulling for 6 weeks after
surgery.
If the patient has a perineal incision, instruct her or him not to sit for long periods of time and to
use a soft or ―waffle‖ pillow rather than a rubber ring whenever in the sitting position.
Teach the patient colostomy care and colostomy irrigation.
Give the following instructions for care of skin in the external radiation field: Tell the patient to
wash the skin gently with mild soap, rinse with warm water, and pat the skin dry each day; not towash off the dark ink marking that outlines the radiation field; to avoid applying any lotions,
perfumes, deodorants, and powder to the treatment area; to wear nonrestrictive soft cottonclothing directly over the treatment area; and to protect skin from sunlight and extreme cold.
Explain the purpose, action, dosage, and side effects of all medications prescribed by thephysician.
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 19/31
FOLLOW-UP
Stress the need to maintain a schedule for follow-up visits recommended by the physician
Encourage patients with early-stage disease and complete healing of the bowel to eat a dieconsisting of a low-fat and high-fiber content with cruciferous vegetables (Brussels sprout
cauliflower, broccoli, cabbage). Most colorectal tumors grow undetected as symptoms slowldevelop. Survival rates are best when the disease is discovered in the early stages and when thpatient is asymptomatic. Unfortunately, 50% of patients have positive lymph node involvement a
the time of diagnosis. Participation in procedures for the early detection of colorectal cancer need
to be encouraged. Suggest follow-up involvement with community resources such as the Unite
Ostomy Association and the American Cancer Society.
Gastric Cancer
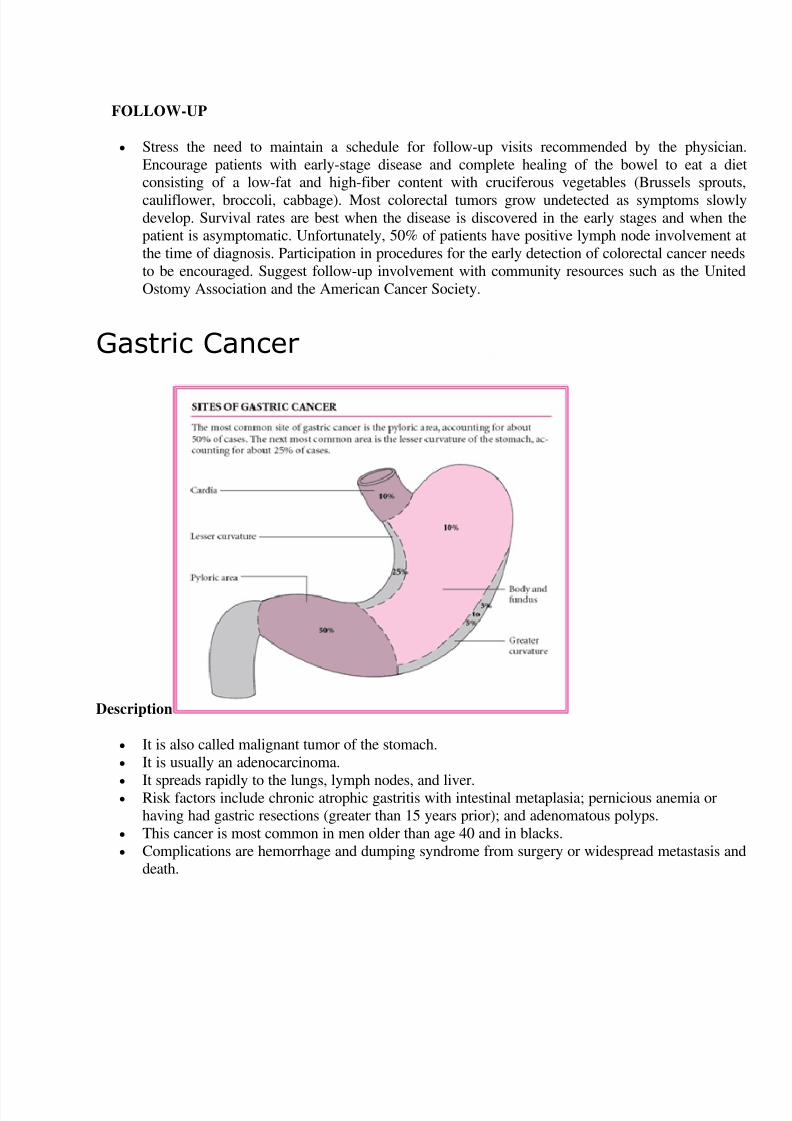
Description
It is also called malignant tumor of the stomach.
It is usually an adenocarcinoma.
It spreads rapidly to the lungs, lymph nodes, and liver.
Risk factors include chronic atrophic gastritis with intestinal metaplasia; pernicious anemia orhaving had gastric resections (greater than 15 years prior); and adenomatous polyps.
This cancer is most common in men older than age 40 and in blacks.
Complications are hemorrhage and dumping syndrome from surgery or widespread metastasis andeath.

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 20/31
Causes/ Risk Factors
No one knows why some people develop stomach cancer and others don't. The number of people affected
varies widely between different countries. For example, stomach cancer is far more common in Japan
than in the UK. There is also evidence that people from poorer backgrounds are at increased risk.
There are a many other factors that increase the risk of developing stomach cancer.
Age. Stomach cancer is most common around the age of 60. It's rare under the age of 40.
Gender . Men are around twice as likely to develop stomach cancer as women.
Helicobacter pylori infection. These bacteria live in the stomach lining of many people, and don'tusually cause any symptoms. However, the infection sometimes causes inflammation of the
stomach lining (gastritis), indigestion and stomach ulcers. It is known to increase the risk of
stomach cancer.
Diet . A diet high in salt and foods that are smoked or cured may increase the risk of stomachcancer. In particular, certain food preservative chemicals known as nitrosamines, which are found
cured meats such as bacon and ham, may increase your chance of developing stomach cancer. Family history. Some people inherit an increased risk of developing stomach cancer.
Type A blood group. Some research indicates that people who have type A blood are at higher ris
of developing stomach cancer.
Smoking. When you smoke, you swallow small amounts of tobacco smoke, which increases yourrisk of getting stomach cancer.
Atrophic gastritis. This condition causes the lining of the stomach to waste away. It has also been
linked with an increased risk of stomach cancer.
Pernicious anaemia. This is type of anaemia raises your risk of stomach cancer.
Assessment
1. Most often, the patient presents with the same symptoms as gastric ulcer. Later, evaluation showsthe lesion to be malignant.
2. Gastric fullness (early satiety), dyspepsia lasting more than 4 weeks, progressive loss of appetite
are initial symptoms.
3. Stool samples are positive for occult blood.4. Vomiting may occur and may have coffee-ground appearance.
5. Later manifestations include pain in black or epigastric area (often induced by eating, relieved by
antacids or vomiting); weight loss; hemorrhage; gastric obstruction.
Diagnostic Evaluation
1. Upper GI X-ray with contrast media may initially show suspicious ulceration that requires furtherevaluation.
2. Endoscopy with biopsy and cytology confirms malignant disease.
3. Imaging studies (bone scan, liver scan, CT scan) helps determining metastasis.

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 21/31
4. Complete blood count (CBC) may indicate anemia from blood loss.
Primary Nursing Diagnosis
Pain (acute) related to gastric erosion
Therapeutic Intervention / Medical Management
The only successful treatment of gastric cancer is gastric resection, surgical removal of part of the
stomach with involved lymph nodes; postoperative staging is done and further treatment may be
necessary.
Surgical options include proximal or distal subtotal gastric resection; total gastrectomy (includes
adjacent organs such as tail of pancreas, portion of liver, duodenum); or palliative surgery such as
subtotal gastrectomy with gastroenterostomy to maintain continuity of the GI tract.
Surgery may be combined with chemotherapy to provide palliation and prolong life.
Pharmacologic Intervention
Chemotherapeutic agents used as adjuvant (in addition to) or neoadjuvant (before surgery) oftenin combination: fluorouracil, doxorubicin, methyl-CCNU, cisplatin, methotrexate, etoposide to
treat cancer that has metastasized to organs beyond stomach; shrink tumors before surgery.
B vitamin complex tablet Combat vitamin B12deficiency and megaloblastic anemia from lack of intrinsic factor
Narcotic analgesics manage pain, side effects of treatment drugs such as morphine, meperidine
which increase patient comfort during end-stage disease Other Medications: Antiemetics may be used to control nausea, which increases as the tumor
enlarges. In the advanced stages, the physician may prescribe sedatives, narcotics, and
tranquilizers to increase the patient’s comfort. Antispasmodics and antacids may also help relieve
GI discomfort.
Nursing Intervention
1. Monitor nutritional intake and weigh patient regularly.
2. Monitor CBC and serum vitamin B12 levels to detect anemia, and monitor albumin and
prealbumin levels to determine if protein supplementation is needed.3. Provide comfort measures and administer analgesics as ordered.
4. Frequently turn the patient and encourage deep breathing to prevent pulmonary complications, toprotect skin, and to promote comfort.
5. Maintain nasogastric suction to remove fluids and gas in the stomach and prevent painfuldistention.
6. Provide oral care to prevent dryness and ulceration.
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 22/31
7. Keep the patient nothing by mouth as directed to promote gastric wound healing. Administerparenteral nutrition, if ordered.
8. When nasogastric drainage has decreased and bowel sounds have returned, begin oral fluids and
progress slowly.
9. Avoid giving the patient high-carbohydrate foods and fluids with meals, which may trigger
dumping syndrome because of excessively rapid emptying of gastric contents.10. Administer protein and vitamin supplements to foster wound repair and tissue building.
11. Eat small, frequent meals rather than three large meals.12. Reduce fluids with meals, but take them between meals.
13. Stress the importance of long term vitamin B12 injections after gastrectomy to prevent surgically
induced pernicious anemia.14. Encourage follow-up visits with the health care provider and routine blood studies and other
testing to detect complications or recurrence.
Documentation Guidelines
Physical findings related to gastric cancer:Epigastric discomfort,dyspepsia,anorexia,nausea, sense
of fullness, gas pains, unusual tiredness, abdominal pains, constipation, weight loss,
vomiting,hematemesis,blood in the stool,dysphagia,jaundice,ascites,bone pain
GI decompression data: Irrigation and patency of tube, assessment of bowel sounds and passage
of gas,complaints of nausea,amount and description of gastric fluid output
Presence of postoperative complications: Hemorrhage, obstruction, anastomotic leaks,
infection,peritonitis
Presence of postoperative dumping syndrome and associated patient symptoms
Discharge and Home Healthcare Guidelines
Teach the patient the importance of compliance with palliative and follow-up care. Be sure thepatient understands all medications, including the dosage, route, action, and adverse effects.
Teach the patient the signs and symptoms of infection and how to care for the incision. Instruct
the patient to notify the physician if signs of infection occur.
Encourage the patient to seek psychosocial support through local support groups (e.g.,I Can
Cope),clergy,or counseling services. If appropriate,suggest hospice services.
Teach the patient methods to enhance nutritional intake to maintain ideal body weight. Several
small meals a day may be tolerated better than three meals a day. Take liquid supplements andvitamins as prescribed. Refer the patient to the dietitian for a consultation. Teach family member
and friends prevention strategies. Strategies include increasing the intake of fresh fruits andvegetables that are high in vitamin C; maintaining adequate protein intake; and decreasing intakeof salty, starchy, smoked, and nitrite- preserved foods.
Lung Cancer
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 23/31
Description
Also called bronchogenic cancer. It is a malignant tumor of the lung arising within the bronchial wall or epithelium.
Bronchogenic cancer is classified according to cell type: epidermoid (squamous cell – most
common), adenocarcinoma, small cell (oat cell) carcinoma, and large cell (undifferentiated)carcinoma.
The lung is also a common site of metastasis from cancer elsewhere in the body through venous
circulation or lymphatic spread.
The primary predisposing factor in lung cancer is cigarette smoking.
Lung cancer risk is also high in people occupationally exposed to asbestos, arsenic, chromium,
nickel, iron, radioactive substances, isopropyl oil, coal tar products, and petroleum oil mists.
Complications include superior vena cava syndrome, hypercalcemia (from bone metastasis),
syndrome of inappropriate antidiuretic hormone (SIADH), pleural effusion, pneumonia, brainmetastasis, and spinal cord compression.
Risk Factors
Modifiable
Approximately 80% of lung cancers are related to cigarette smoking. Lung cancer is 10 timesmore common in smokers than in nonsmokers. In particular,squamous cell and small cell
carcinoma are associated with smoking
Other risk factors include exposure to carcinogenic industrial and air pollutants — such asasbestos,coal dust,radon,and arsenic
Non-modifiable
Family history

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 24/31
Assessment
New or changing cough, dyspnea, wheezing, excessive sputum production, hemoptysis, chest pai(aching, poorly localized), malaise, fever, weight loss, fatigue, or anorexia.
Decreased breath sounds, wheezing, and possible pleural friction rub (with pleural effusion) onexamination.
Diagnostic Evaluation
Chest X-ray may be suspicious for mass; CT or position emission tomography scan will be bettervisualize tumor.
Sputum and pleural fluid samples for cytologic examination may show malignant cells.
Fiberoptic bronchoscopy determines the location and extent of the tumor and may be used to
obtain a biopsy specimen.
Lymph node biopsy and mediastinoscopy may be ordered to establish lymphatic spread and helpplan treatment.
Pulmonary function test, which may be combined with a split-function perfusion scan, determine
if the patient will have adequate pulmonary reserve to withstand surgical procedure.
Primary Nursing Diagnosis
Ineffective airway clearance related to obstruction caused by secretions or tumor
Medical Management
Oxygen through nasal cannula based on level of dyspnea.
Enteral or total parenteral nutrition for malnourished patient who is unable or unwilling to eat.
Removal of the pleural fluid (by thoracentesis or tube thoracostomy) and instillation of sclerosing
agent to obliterate pleural space and fluid recurrence.
Radiation therapy in combination with other methods.
Surgical Intervention
Resection of tumor, lobe, or lung.
Pharmacologic Intervention
Expectorants and antimicrobial agents to relieve dyspnea and infection.
Analgesics given regularly to maintain pain at tolerable level. Titrate dosages to achieve pain
control.

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 25/31
Chemotherapy using cisplatin in combination with a variety of other agents and immunotherapytreatments may be indicated.
Nursing Intervention
Elevate the head of the bed to ease the work of breathing and to prevent fluid collection in upperbody (from superior vena cava syndrome).
Teach breathing retraining exercises to increase diaphragmatic excursion and reduce work of
breathing.
Augment the patient’s ability to cough effectively by splinting the patient’s chest manually.
Instruct the patient to inspire fully and cough two to three times in one breath.
Provide humidifier or vaporizer to provide moisture to loosen secretions.
Teach relaxation techniques to reduce anxiety associated with dyspnea. Allow the severelydyspneic patient to sleep in reclining chair.
Encourage the patient to conserve energy by decreasing activities.
Ensure adequate protein intake such as milk, eggs, oral nutritional supplements; and chicken,fowl, and fish if other treatments are not tolerated – to promote healing and prevent edema.
Advise the patient to eat small amounts of high-calorie and high-protein foods frequently, rather
than three daily meals.
Suggest eating the major meal in the morning if rapid satiety is the problem.
Change the diet consistency to soft or liquid if patient has esophagitis from radiation therapy.
Consider alternative pain control methods, such as biofeedback and relaxation methods, to
increase the patient’s sense of control.
Teach the patient to use prescribed medications as needed for pain without being overlyconcerned about addiction.
Documentation Guidelines
Physical findings:Adequacy of airway and breathing; vital signs; heart and lung sounds; pain

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 26/31
(nature, location,duration,and intensity); intake and output
Complications:Pneumonia,hypoxia,infection,dehydration, poor wound healing
Response to interventions:Response to pain medication
Response to treatment:Chest tube drainage; wound healing; condition of skin following radiation
side effects from chemotherapy
Discharge and Home Healthcare Guidelines
Teach the patient to recognize the signs and symptoms of infection at the incision site, including redness,
warmth, swelling, and drainage. Explain the need to contact the physician immediately. Be sure thepatient understands any medication prescribed, including dosage, route,action,and side effects. Provide
the patient with the names,addresses,and phone numbers of support groups, such as the American Cance
Society, the National Cancer Institute, the local hospice, the Alliance for Lung Cancer Advocacy, Suppo
& Education (ALCASE), and the Visiting Nurses Association. Teach the patient how to maximize her orhis respiratory effort.
Liver Cirrhosis
Description
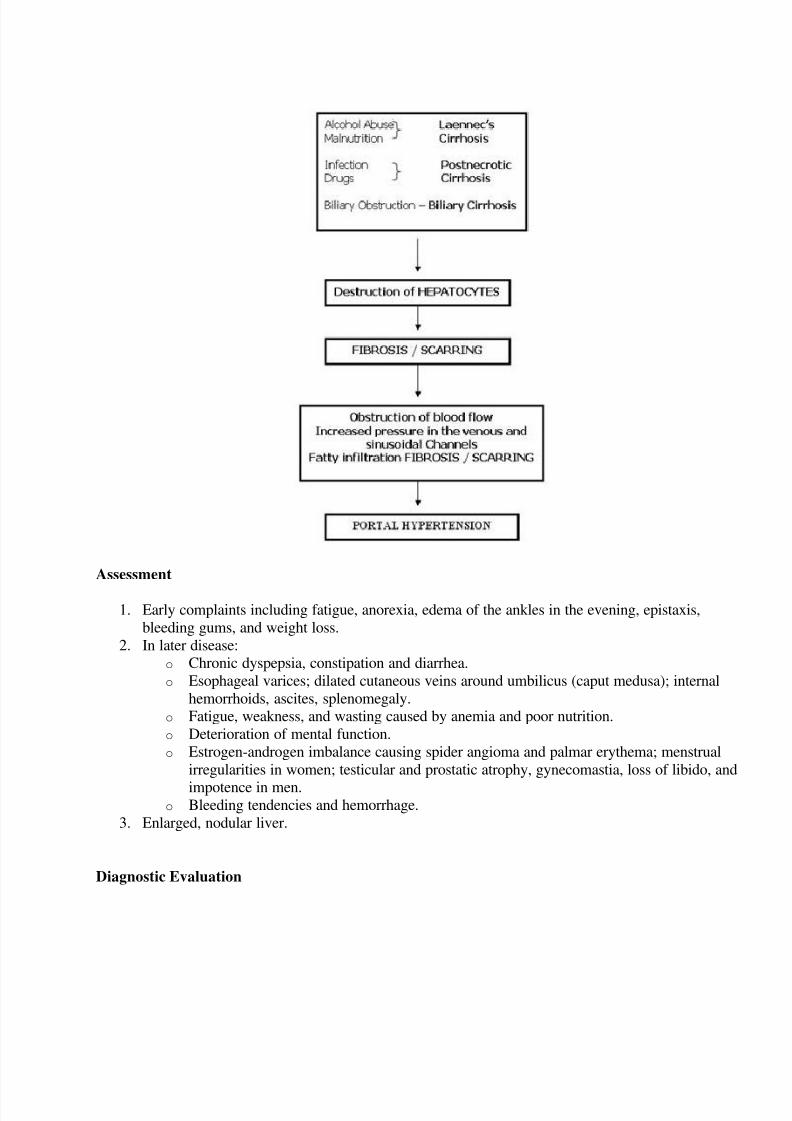
Is a chronic disease that causes cell destruction and fibrosis (scarring) of hepatic tissue.
Fibrosis alters normal liver structure and vasculature, impairing blood and lymph flow and
resulting in hepatic insufficiency and hypertension in the portal vein.
Complications include hyponatremia, water retention, bleeding esophageal varices, coagulopathy
spontaneous bacterial peritonitis, and hepatic encephalopathy.
Three major forms:
1. Laennec’s (alcohol induced) Cirrhosis o Fibrosis occurs mainly around central veins and portal areas.
o This is the most common form of cirrhosis and results from chronic alcoholism and

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 27/31
malnutrition.
2. Postnecrotic (micronodular) Cirrhosis o Consist of broad bands of scar tissue and results from previous acute viral hepatitis or
drug-induced massive hepatic necrosis.
3. Biliary Cirrhosis o Consist of Scarring of bile ducts and lobes of the liver and results from chronic biliary
obstruction and infection (cholangitis), and is much rarer than the preceding forms.
Causes/ Risk Factors
Cirrhosis of the liver is a chronic disease that causes cell destruction and fibrosis (scarring) of
hepatic tissues. Fibrosis alters normal liver structure and vasculature, impairing blood and lymph
flow and resulting in hepatic insufficiency and hypertension in the portal vein. Complicationsinclude hyponatremia, water retention, bleeding esophageal varices, coagulopathy, spontaneous
bacterial peritonitis, and hepatic encephalopathy.
Cirrhosis is known in three major forms. In Laennec’s (alcohol-induced) cirrhosis, fibrosisoccurs mainly around central veins and portal areas. This is the most common form of cirrhosis
and results from chronic alcoholism and malnutrition. Postnecrotic (micronodular) cirrhosis
consist of broad bands of scar tissue and results from previous acute viral hepatitis or drug-induced massive hepatic necrosis. Biliary cirrhosis consists of scarring of bile ducts and lobes of
the liver and results from chronic biliary obstruction and infection (cholangitis), and is much rare
than the preceding forms.
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 28/31
Assessment
1. Early complaints including fatigue, anorexia, edema of the ankles in the evening, epistaxis,
bleeding gums, and weight loss.
2. In later disease:
o Chronic dyspepsia, constipation and diarrhea.
o Esophageal varices; dilated cutaneous veins around umbilicus (caput medusa); internal
hemorrhoids, ascites, splenomegaly.
o Fatigue, weakness, and wasting caused by anemia and poor nutrition.
o Deterioration of mental function.
o Estrogen-androgen imbalance causing spider angioma and palmar erythema; menstrual
irregularities in women; testicular and prostatic atrophy, gynecomastia, loss of libido, and
impotence in men.o Bleeding tendencies and hemorrhage.
3. Enlarged, nodular liver.
Diagnostic Evaluation
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 29/31
1. Elevated serum liver enzyme levels, reduced serum albumin.2. Liver biopsy detects cell destruction and fibrosis of hepatic disease.
3. Liver scan shows abnormal thickening and a liver mass.4. CT scan determines the size of the liver and its irregular nodular surface.
5. Esophagoscopy determines the presence of esophageal varices.6. Percutaneous transhepatic cholangiography differentiates extrahepatic from intrahepatic
obstructive jaundice.
7. Paracentesis examines ascitic fluid for cell, protein, and bacteria counts.
Primary Nursing Diagnosis
Fluid volume excess related to retention
Therapeutic Intervention / Medical Management
Medical management is based on presenting symptoms.
Treatment includes antacids, vitamins, balanced diet, and nutritional supplements; potassium-
sparing diuretics (for ascites); avoidance of alcohol.
Colchicine may increase the length of survval in patients with mild to moderate cirrhosis.
Surgical Intervention
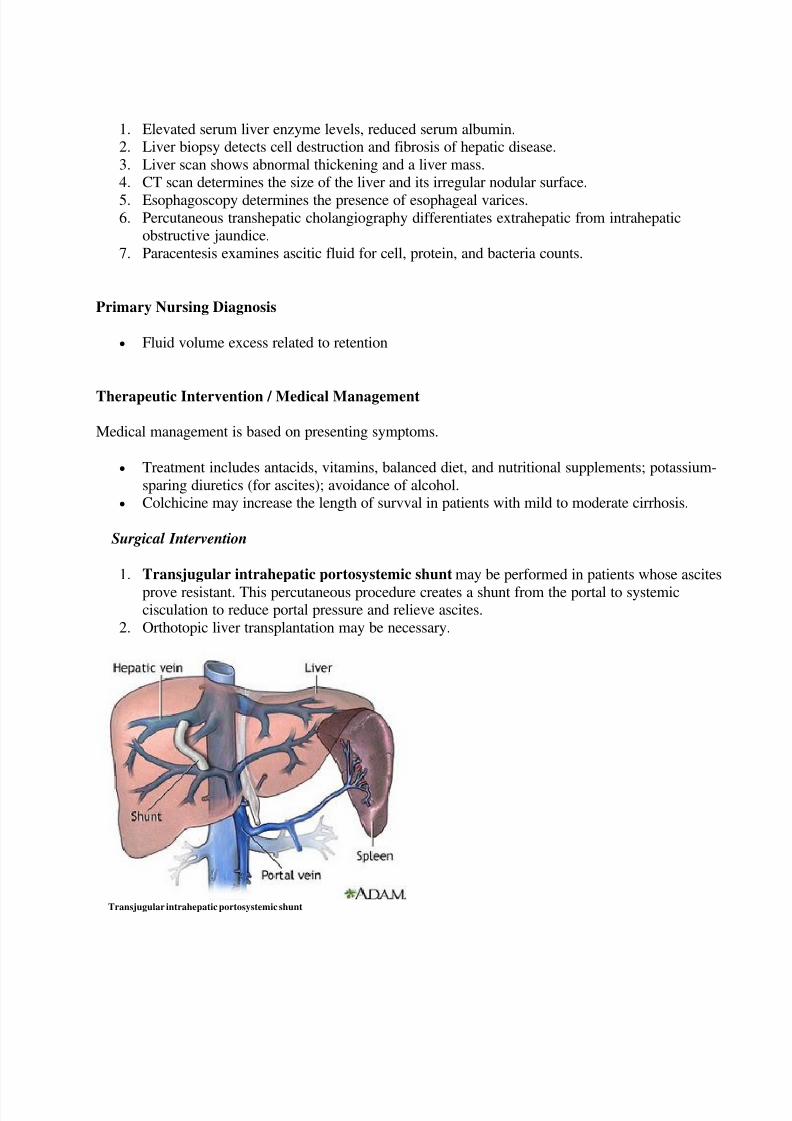
1. Transjugular intrahepatic portosystemic shunt may be performed in patients whose ascites
prove resistant. This percutaneous procedure creates a shunt from the portal to systemiccisculation to reduce portal pressure and relieve ascites.
2. Orthotopic liver transplantation may be necessary.
Transjugular intrahepatic portosystemic shunt
8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 30/31
Pharmacologic Intervention
Provide asymptomatic relief measures such as pain medications and antiemetics.
Diuretic therapy, frequently with spironolactone, a potassium-sparing diuretic that inhibits theaction of aldosteroe on the kidneys.
I.V albumin to maintain osmotic pressure and reduce ascites.
Administration of lactulose or neomycin through a nasogastric tube or retention enema to reduce
ammonia levels during periods of hepatic encephalopathy.
Nursing Intervention
Observe stools and emesis for color, consistency, and amount, and test each one for occult blood.
Monitor fluid intake and output and serum electrolyte levels to prevent dehydration and
hypokalemia, which may precipitate hepatic encephalopathy. Maintain some periods of rest with legs elevated to mobilize edema and ascites. Alternate rest
periods with ambulation.
Encourage and assist with gradually increasing periods of exercise.
Encourage the patient to eat high-calorie, moderate protein meals and supplementary feedings.
Suggest small, frequent feedings.
Encourage oral hygiene before meals.
Administer or teach self-administration of medications for nausea, vomiting, diarrhea or
constipation.
Encourage frequent skin care, bathing with soap, and massage with emollient lotions.
Keep the patient’s finger nails short to prevent scratching from pruritus.
Keep the patient quiet and limit activity if signs of bleeding are evident. Encourage the patient to eat foods high vitamin C content.
Use small gauge needles for injections and maintain pressure over injection site until bleedingstops.
Protect from sepsis through good handwashing and prompt recognition and management of
infection.
Pad side rails and provide careful nursing surveillance to ensure the patient’s safety.
Stress the importance of giving up alcohol completely.
Involve the person closest to the patient, because recovery usually is not easy and relapses are
common.
Documentation Guidelines
Physical findings:Bleeding,abdominal enlargement,weight gain or loss,fluid intake andoutput,easy respirations,breath sounds,heart sounds,level of consciousness,gastrointestinal status(nausea,vomiting,anorexia, diarrhea),color of skin and sclera
Laboratory results:White blood cell count, hemoglobin and hematocrit, albumin, serum

8/3/2019 MS-cancer
http://slidepdf.com/reader/full/ms-cancer 31/31
electrolytes,ALT,AST
Nutrition:Tolerance of diet,appetite,ability to maintain body weight
Response to treatment:Medications,surgery,pericentesis
Discharge and Home Healthcare Guidelines
ALCOHOL ABUSE TREATMENT. Emphasize to the patient with alcoholic liver cirrhosis tha
continued alcohol use exacerbates the disease. Stress that alcoholic liver disease in its early stage
is reversible when the patient abstains from alcohol. Encourage family involvement in alcoholabuse treatment. Assist the patient in obtaining counseling or support for her or his alcoholism.
FOLLOW-UP. Encourage the patient to seek frequent medical follow-up. Visits from a
community health nurse to monitor the patient’s progress and to help with any questions or
problems at home are also helpful.
SUPPORT GROUPS. Refer the patient to an alcohol support group or liver transplant support
group.