MRSA Outbreak Management March 25, 2008. Citywide Program Medical Director, Manager, Educator + 12...
36
MRSA Outbreak Management March 25, 2008
-
Upload
colby-robotham -
Category
Documents
-
view
213 -
download
0
Transcript of MRSA Outbreak Management March 25, 2008. Citywide Program Medical Director, Manager, Educator + 12...

MRSA Outbreak Management
March 25, 2008


Citywide Program Medical Director, Manager, Educator + 12 FTE Infection
Control Practitioners, 1 program secretary 8 hospital sites Approx 2,363 beds - 1,118 acute care beds (cardiac,
transplant, neuro, ortho surgery, burns, trauma, obstetric, pediatric)
- 130 ICU beds- Ambulatory/Short stay- LTC, Complex Care, Palliative, Rehab,
Regional Psychiatric, Dialysis, Cancer Care

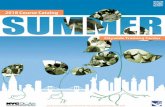
MRSA: A growing problem First outbreaks in late 1995 2002-2003 increases began again Increasing rates each year since CNISP data QMPLS data

Canadian Nosocomial Infection Surveillance Data – 1995-2006
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
5500
6000
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Num
ber o
f MRS
A ca
ses
0.0
2.0
4.0
6.0
8.0
10.0
12.0
Rate
per
1,0
00 a
dmiss
ions

Ontario QMPLS Report – July 2007

QMPLS Reported Number of Bacteremias – July 2007

Complicating Factors Restructuring Nursing shortages Multiple organizational priorities SARS Infrastructure challenges Changes in the care delivery model Non adoption of Routine Practices

What’s being done to stem this tide? Provincial recommendations CPSI CCHSA Organizational Scorecard reporting

Making a Change HappenD x V x F > R
D- Discomfort (or dissatisfaction with the status quo)
V- Vision (of the preferred future)F- First steps (clarity of the plan for how to move
forward)R- Resistance factors
“The product of the discomfort, vision, and first steps must be greater than the resistance or the change will fail
Dannemiller & Jacobs (1992)

MRSA REDUCTION Logic Model 2007- 2012
Core Competencies Education and
Increased Awareness of
AROs
Environmental and Infection Control
Supports
Active Surveillance
Cultures
Planning, Research, Evaluation & Monitoring
o Annual Core Competency e- learning with emphasis on routine practices and contact precautions
o Review of hand hygiene practices, focus on opportunities, healthy hands
o Review of correct glove and gown use, discuss inappropriate usage
o Educational Presentations o Development of MRSA
educational toolkit for leaders to share with staff
o Display boards and posters with unit specific rates along with facility, citywide, and provincial benchmarks
o Q & A’s and Case Studies o Tools for Clinical Educators o Dissemination of rates to
leadership q 6 mths
o Audit and monitor environmental cleaning practices
o Assess usage of hand cleansing products
o Reduce room stocking of supplies to reduce waste and transmission opportunities
o Implementation of cohorting o Algorithm for patient
management o Establishment of MRSA
outbreak management policy
o Establish a process that adequately captures patients at risk for MRSA
o Ensure responsibility is assigned to one person on each unit for screening accountability
o Audit compliance with ARO screening directive q 6 mths and report to unit and senior leaders
o EPR support of screening o Ensure screening is in line with
PIDAC recommendations
o Research best practice documents, and published literature for direction on practice changes
o Establish a multi level working group to identify ways to reduce transmission and support necessary change
o Complete reports on incidence and nosocomial transmission rates and share throughout the organization every? 6 months? every month
o Identify successful interventions and utilize these to make organization wide improvements
o Collect data on nosocomial ARO rates on an ongoing basis to measure HH impact
o Monitor Patient Satisfaction Survey Results
o Review program plan annually and revise as needed
Healthcare Workers Patients Visitors
Physicians Nursing and other professional staff Housekeeping & Dietary Support Staff Clinical Educators Patients & Families
Senior leaders, Unit managers, Housekeeping, PSAs, TSAs Nursing, Pharmacy
Nursing Senior leadership Unit managers Admitting , Preadmit and other Patient entry assessment areas
Working group Infection Prevention & Control Team Infection Prevention and Control Site and Citywide Committees LHSC & SJHC health care workers
1. To establish factors that support lasting behaviour change in routine precautions through a variety of interventions aimed at patients & staff 2. Where possible demonstrate the link between MRSA reduction/transmission and routine practices
1. To have IP&C practices in place that prevent transmission 2. To have a resource and facility wide plan to prevent and manage outbreaks 3. Engage Pharmacy and Therapeutics in monitoring antibiotic usage
1. To improve screening compliance in order to capture patients that are at increased risk of colonization/infection
1. To identify practices that contribute to reduced transmission.
2. To monitor MRSA rates and summarize biannually.
3. To engage leaders and HCW across the organization in committing to MRSA transmission reduction
To have improved compliance with IP&C practices at London Health Sciences Center and St Josephs Health Care that are reflected in reduced MRSA rates.
To reduce MRSA transmission through improved infection prevention and control practices at London Health Sciences Center and St Josephs Health Care.
Activities
Target Groups
Activity Objectives
Long Term Objective
Goal
Short Term Objectives
1. To increase education and awareness of the seriousness of MRSA transmission and the infection prevention and control measures necessary to reduce transmission. 2. To determine interventions that are successful in interrupting transmission of MRSA 3. To engage leaders and HCW in shared accountability for reducing transmission of MRSA 4. To improve HCW compliance with routine practices, hand hygiene, MRSA screening as well as contact precautions throughout the organization 5. To reduce nosocomial ARO rates by 25% each year of the project.
1. To provide a variety of educational opportunities to raise awareness of MRSA
2. To develop alternative self directed learning tools for staff
3. Teaching on the importance of colonized patients as reservoirs for transmission
Strategies
Antibiotic Utilization
1. Ensure systems are in place to promote optimal treatment of infections and appropriate antimicrobial use
o P & T committee o Senior Leadership o Pharmacy o MAC
o Ensure that a multi-disciplinary group reviews utilization and susceptibility patterns
o Ensure computer system capable of providing clinician with appropriate treatment choices
o Perform audits of antibiotic usage
MRSA Reduction, Logic Model 2007-2012

ARO Reduction Plan, 2007-2012 LHSC/SJHC
↑ training for HCWs ↑feedback of rates to leaders and front line staff ↑screening Develop city-wide hand hygiene committee Install point of care ABHR Compliance audits (hand hygiene, infection control
precautions, multi-disciplinary clinical walk-abouts, screening practices with feedback)
Establish unit specific workgroups ARO specific Infection Control team meetings


Step 1
Process Flow Map, MRSA
Screening
Step 2
Control Plan, MRSA Screening
and Containment
Step 3
Failure Modes and Effects Analysis
(FMEA)

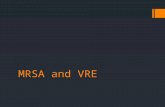
Leader ReportsQuarterly Report Infection Control Indicators
Service Unit
MRSA HAIRate/1,000 ptdays
25% Reduction Target
Screening Compliance Target
CoreCompetency Completion
6 Mth Target
Hand HygieneCompliance Target
Medicine A5 0.8 0.6 75% 100% 25% 50% 48% 100%
A6 0.5 0.37 68% 100% 42% 50% 39% 100%
4IP 0.62 0.46 85% 100% 30% 50% 45% 100%
Surgery D6 0.7 0.52 78% 100% 60% 50% 42% 100%
B8 0.68 0.51 82% 100% 75% 50% 68% 100%
Neurology 7A 0.58 0.43 98% 100% 58% 50% 52% 100%

Be Prepared For an Outbreak! Well established surveillance program Relationships, team work Flagging system
Discuss issues and problem solve scenarios beforehand Suppression therapy, cohorting, bed closures, staff
screening Policies & procedures
Isolation, indications for patient screening, admission, contact, prevalence

What is an Outbreak?
New cases (incidence) in a given population, during a given
time period, at a rate that substantially exceeds what is
"expected.”
How do you know you are having an outbreak?

Verify Existence of Outbreak Evidence that transmission has occurred Consistent definition of hospital acquired Epidemiologic review
Person, place, time History- access to health care in the previous
12 months Retrospective analysis of current stay
Previous rooms, units, contacts, staff
Molecular typing may be helpful

Control Measures
Contact precautions Cohort patients Epidemiologic
investigation Multi-disciplinary team Case Finding Communicate &
educate Feedback
Audit Environment Isolation Practice Compliance
Cohort staff Suppression therapy? Staff screening? Restrict admissions?

Suppression Therapy
Insufficient evidence to support the use of topical or systemic antimicrobial treatment for eradicating MRSA.
Loeb. M., Main, C., Walker-Dilks, C., Eady, A.(2003). Antimicrobial drugs for treating MRSA colonization. Cochrane Database Systematic Review 4 CD003340.
Value in outbreak? (decrease reservoir) Nasal mupirocin Mupirocin plus systemic Mupirocin +/- CHG CHG alone

Common Challenges, Acute and Non-acute Care
Cohorting patients & staff Patient mobility Staff screening Communication Patient supplies & cleaning Non-compliance Insufficient ABHR

…………Challenges ContinuedAcute Care
Shortage of nurses High acuity Bed closures Students Competing priorities
Non-acute Care
Physical limitations Insufficient supplies Frequent staff
turnover Non-regulated HCW Poor lab access

Non-Acute Care Literature
Lack of studies on measures to prevent transmission
Studies show nursing home is risk factor Studies show prevalence is increasing Screening high risk admissions? Train key staff Hand hygiene adherence, environmental
cleaning
Hughes, C., Smith, M., Tunney, M.(2008). Infection control strategies for preventing the transmission of MRSA in nursing homes for older people. Cochrane Database Systematic Review 1. CD006354.

Are Control Measures Generalizable to all Settings?
No…………Why?Settings may be very different; Acute care vs non-acute care Tertiary teaching facility vs community
hospital Intensive care vs general medical unit Baseline epidemiology on unit
Is MRSA epidemic or endemic?

Our Conclusions
Observation must be constant Team work pays off MRSA management is resource consuming Nosocomial acquisition can be reduced
through intervention Multiple unit specific interventions are
required

Screening patients for MRSA

Screening Issues
Turn around timeSensitivityCost

Screening
Focused screening Screen only high risk patients
Universal screening Screen all patients being admitted
Universal + focused Screen all patients in areas where there is a
problem Screen high risk patients elsewhere

Focused Screening
Choose patients for screening based on risk factors Previous hospitalization major risk factor
In Ontario based an admission or >12 hour stay in any healthcare facility in previous 12 months

Focused Screening
Advantages: Cheaper May be all you need
Disadvantages: Need to identify patients who need screening Poor compliance with screening May miss patients with other risk factors

Universal Screening
Advantages: No need to “flag” patients Compliance may be better More sensitive for identification of carriers
Disadvantages: More costly

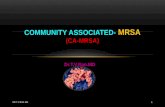
Old Screening algorithm New Screening algorithm
MRSA Screen Swabs (nasal + rectal)
Oxacillin Salt Mannitol Agar (X2) Chromogenic Agar (MRSA Select)
Pick Yellow Colonies Presumptive Reporting to Ward 4X daily
Confirm as MRSA by PCR Confirm as MRSA by PCR if no previous isolate identified from patient
24-48 hrs 24 hours
Innoculate Separate plates Both swabs single plate
4X/day
Report to Ward once daily

Time to reporting MRSA positive patients to the ward
Time to Reporting*
Mannitol Oxacillin Salt plate 58.0 +/- 17.9 hours
MRSAselect plate 34.0 +/- 12.3 hours
*Statistically significant difference, p<0.0001

Number of contacts of index case
Average number of contacts*
Mannitol Oxacillin Salt plate 2.88 +/- 2.03
MRSA select plate 2.30 +/- 1.43
*Statistically significant difference, p<0.05

Number of contacts who become MRSA positive
2005 2007
287 MRSA cases 475 cases
37 contacts (12.89%) 28 contacts (5.89%)