
Moving and Handling (MH1)
57
MH1 – Moving and Handling Policy 1 of 69 Version 1 (Feb 2015) Moving and Handling (MH1)
Transcript of Moving and Handling (MH1)

MH1 – Moving and Handling Policy
1 of 69 Version 1 (Feb 2015)
Moving and Handling (MH1)

MH1 – Moving and Handling Policy
2 of 69 Version 1 (Feb 2015)
Document Information This is a controlled document. It should not be altered in any way without the express permission of the author or their representative. On receipt of a new version, please destroy all previous versions.
Date of Issue: Feb 2015 Next Review Date: Feb 2017
Version: V1 Last Review Date: Not Applicable
Author: Moving and Handling Team
Director(s) Responsible: Estates and Facilities Management
Approval /Consultation Route: Health and Safety Committee
Approved By: Date Approved:
Health and Safety Committee Feb 2015
Amendment History
Version Status Date Reason for Change Authorised

MH1 – Moving and Handling Policy
3 of 69 Version 1 (Feb 2015)
Contents
1 Policy Statement 4
2 Introduction 4
3 Equality Impact Assessment 5
4. Roles and Responsibilities 5
5 Principles of moving and handling 8
6 Risk Assessment Process 9
7 Manual Handling equipment 10
8 Moving and Handling training 10
9 Provisions of training for trainers 11
10 Communication and Implementation of policy 12
11 Monitoring, Review and Evaluation of this policy 12
12 References 14
13 Appendix 1 -Moving & Handling Team Structure 15
14 Appendix 2 - Risk Assessment Process 16
15 Appendix 3 -Guidelines for lifting inert loads 17
16 Appendix 4- Risk Assessment form Inanimate loads 18
17 Appendix 5 - Risk Assessment form Pushing/Pulling 24
18 Appendix 6 - SS10A Handling Assessment Community 31
19 Appendix 7 - Handling Assessment child/young patient 32
20 Appendix 8 - Patient Handling Falls & Bed rail assessment - acute 38
21 Appendix 9 - Guide to Therapeutic handling in therapy treatment 42
22 Appendix 10-Hoist & Sling provision 54
22 Appendix 11 - Procedure for post fall of patient - acute 56
23 Appendix 11- Post fall flow chart -in patient community 58
24 Appendix 12 - Reba Assessment tool 59
25 Appendix 12A- RULA assessment tool 59
26 Appendix 13 - Practical Training Record- Induction 60
27 Appendix 14 - Practical Training Record- Refresher 65
28 Appendix 15 - Training Non Attendance letter 67
29 Appendix 16 - Training Persistent Non Attendance Letter 68
30 Appendix 17 - Non Attendance Process 69
If you require a copy of this policy in an alternative format (for example large print, easy read) or would like any assistance in relation to the content of this policy, please contact the Equality and Diversity team on 01803 656680.

MH1 – Moving and Handling Policy
4 of 69 Version 1 (Feb 2015)
1. Policy Statement
1.1 The aim of this policy is to contribute to providing an effective service by reducing
injuries and ill health; improving patient care and patient experience, and where possible reducing unnecessary loss and liabilities. The objectives of the policy are:
Reduce the number of injuries year on year resulting from moving and handling activities to staff within the organisation;
Minimise the risks to staff and patients when loads including patients/service users are moved by bodily force;
Create a safer working environment for all staff, and anybody else, who may be affected or involved with moving and handling activities;
Clarify the procedure of performing a moving and handling risk assessment in order to deal with hazardous moving and handling operations;
Ensure that managers assess and control risks arising from moving and handling activities within their department/unit and are responsible for them;
Ensure that handling equipment is used when reasonably practicable to do so;
Provide information training and instruction to employees to ensure safe working;
Ensure the effectiveness of moving and handling training.
To monitor quality assurance, the implementation and delivery of this policy. 2 Introduction 2.1 South Devon Healthcare NHS Foundation Trust & Torbay and Southern Devon Health
and Care NHS Trust (hereafter known as the Trusts) are committed to protecting staff and providing the highest standards of quality of care to our patients.
2.2 Moving and handling is a key part of the working day for most employees; from moving
of equipment, laundry, catering, supplies or waste to assisting patients/clients in moving.
2.3 “Moving and Handling” means ‘any transporting or supporting of a load (including
lifting, putting down, pushing, pulling, carrying or moving) by hand or bodily force (such as the shoulder)’. The force applied is human, not mechanical. Clearly in a healthcare environment, it is useful to distinguish between patient and non-patient handling.
2.4 Poor moving and handling practice can lead to:
back pain and musculoskeletal disorders, which can lead to inability to work
moving and handling accidents – which can injure both the person being moved and the employee
discomfort and a lack of dignity for the person being moved 2.5 This policy details the robust and effective arrangements that the Trusts have in place
to support staff in moving and manual handling. 2.6 This policy applies to all staff in the Trusts, including permanent, temporary, bank
workers and contractors.

MH1 – Moving and Handling Policy
5 of 69 Version 1 (Feb 2015)
3 Equality Impact Assessment
3.1 The Trusts are committed to preventing discrimination, valuing diversity and
achieving equality of opportunity. No employee will receive less favourable treatment on the grounds of age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex or sexual orientation, or on the grounds of trade union membership.
4 Roles and Responsibilities 4.1 The Chief Executive is accountable for the health and safety of staff within their
organisations. 4.2 The Trust Boards are responsible for ensuring the effective implementation,
communication and delivery of the Moving and Handling Policy. 4.3 The Health and Safety Committee are accountable to the Chief Executive of the trusts.
4.4 The Moving and Handling Team are accountable to the Health and Safety Committee. The diagram in Appendix 1 details the structure of the moving and handling team.
4.5 The Trusts recognise that the objectives set out above cannot be achieved without the full co-operation of all staff.
4.6 All Managers are responsible for ensuring that:
This policy is is implemented at a local level and communicated to and read by all staff;
All staff comply with this policy;
All staff receive Moving and Handling training, in accordance with the training needs analysis. This includes taking appropriate action when a member of staff fails to complete their mandatory training;
Moving and Handling tasks are eliminated where possible, and where they cannot be eliminated that a suitable risk assessment is performed and recorded;
The risks associated with moving and handling operations are reduced to the lowest level practicable, and that where appropriate, risks are recorded on the risk register. Any risks that cannot be managed locally are escalated in accordance with the Risk Management Policy;
Adequate arrangements and equipment are in place following all moving and handling risk assessments;
Employees adhere to safe systems of work and are adequately trained to correctly use any equipment provided;
All moving and handling incidents are reported following the Trusts incident reporting procedure and are investigated appropriately;
Occupational Health are contacted if an employee is injured as a result of moving and handling, and liaison with the employee to ensure that any rehabilitation plan to assist the individual in a return to normal working duties is achieved;
Managers need to be aware of the moving and handling practices within their areas and highlight if staff are posing any risk to themselves or patients.
They follow the New and Expectant Mothers Risk Assessment Procedure.

MH1 – Moving and Handling Policy
6 of 69 Version 1 (Feb 2015)
4.7 Moving and Manual Handling Advisors are qualified staff who are specialists in moving
and handling. All advisors have regular training and have undergone the required “train the trainer” through the University of Plymouth, or an equivalent qualification, as well as experience of front line working. In addition to this all advisors are members of the National Back Exchange, and share working practices across Devon and Nationally with other advisors.
Advisors have responsibility for;
Providing training on moving and handling techniques to staff, with the assistance of Moving and Handling Key Trainers where appropriate;
Providing training and advice to Moving and Handling Key Trainers as well as on-going annual assessment of their competence;
Providing specialist advice to managers regarding moving and handling;
Providing training and advice to Moving and Handling Trained Risk Assessors in the assessment and control of moving and handling risks;
Liaising with the Health and Safety Manager to ensure that serious moving and handling incidents and RIDDORS are investigated, and that appropriate follow up action is taken;
Monitoring the effectiveness of this policy through reviewing incidents reported, equipment provision and training provision.
Attending the Health and Safety Committee groups, and providing a quarterly report on moving and manual handling.
All of the advisors are based at Horizons Centre on the Torbay Hospital site, but are willing to travel across the Trusts to advise on Moving and Handling issues.
4.8 Accredited Trainers are qualified staff in front line positions who are responsible for:
Delivering training to staff
Supervising moving and handling practice in the workplace
Perform moving and handling risk assessments when required.
Complete an annual training update.
Monitoring compliance to policy and risk assessment process. Reporting any concerns to the moving and handling advisors.
Please contact the Moving and Handling Team for the names of a Trainer or Risk Assessor in your area.
4.9 In the Acute Trust Manual Handling Ward Coaches are appointed for each area. These
coaches have an additional interest in moving and handling and receive additional training in Patient Handling activities. They do not have an accredited training certificate.
Their duties include iintroducing new staff to:
Departments general Moving and Handling tasks
Ward MH File, guidance notes and risk assessments
Instruction and guidance on specific equipment usedReporting system and policy access online – Contact / Icare

MH1 – Moving and Handling Policy
7 of 69 Version 1 (Feb 2015)
They also assist the manager;
With workplace assessments ( hazardous manual handling activities)
Monitor practice to reduce risk of injury
Monitor completion of moving & handling documentation (traffic light form etc.)
Monitor team competency; refer to training or competency sheet Coaches will act as a link person between the workplace and moving & handling
advisors. They are committed to:
Attend meetings as planned (twice Yearly) to keep in the loop.
Feed into and feedback to quarterly newsletters.
Disseminate information to colleagues.
Share good practice.
4.10 In Community, Risk Assessors are based in community hospitals and the wider community teams. They are responsible for:
Performing patient and non-patient manual handling risk assessments in their area;
Performing complex service users/ patient handling risk assessments;
Keeping records of risk assessments and escalating any issues;
Ensuring any action plans are followed up;
The person responsible for the risk assessment is responsible for monitoring of the action plan immediately after the risk assessment has been set up. Thereafter this should be audited periodically.
Encouraging good practice in moving and handling of loads;
Assist Trainers to deliver practical training sessions as required;
Attend an annual Risk Assessor update 4.10.1 To gain further advice and assistance with complex needs contact the moving and
handling team at the Horizons Centre.
4.11 The Human Resources directorate are responsible for:
Ensuring all new staff attend induction sessions according to the Training Needs Analysis (either patient or non-patient moving and handling);
Maintaining a database to evidence which staff have received induction and mandatory training;
Informing managers of staff who are due or overdue mandatory training;
Reporting attendance at training sessions on a monthly basis to the Moving and Manual Handling Advisor.
4.12 Occupational Health will:
Accept management referrals for employees suffering adverse health effects because of moving and handling and provide advice and support, where appropriate, and as necessary;
4.13 The following organisations are commissioned to provide services in Patients/Clients
own homes following assessment by an authorised prescriber;
Community Equipment Services
PLUSS in Exeter serves the Torbay and Southern Devon Health & Care Trust.
NRS in Torbay serves the Torbay area.

MH1 – Moving and Handling Policy
8 of 69 Version 1 (Feb 2015)
PLUSS/NRS maintain a database of all moving and handling equipment in the Trust and arranges for the inspection and maintenance of the equipment in accordance with the Lifting Operations and Lifting Equipment Regulations 1998. The following individuals/ groups/ organisations are responsible for making sure that they comply with these regulations:
Medical Electronics- Acute Hospital maintenance
Individual (Privately owned)- These individuals are responsible for their own maintenance.
Residential and Nursing Homes- All Homes are responsible for their own maintenance.
4.14 All Staff must:
Read, understand and follow this policy, and should raise any queries with their line manager;
Make full and proper use of any system of work put in place following risk assessment to reduce the risk of injury during moving and handling;
Ensure they attend moving and handling training and updates and that they undertake moving and handling tasks in accordance with the training provided;
Ensure that they have received adequate training before undertaking new moving and handling tasks or using new handling aids, etc;
Inspect any lifting equipment before it is used and report any defects via the Trust’s incident reporting procedure. Defective items must be withdrawn from service until their safety can be guaranteed;
Report every injury or near miss from moving and handling via the Trust’s incident reporting procedure.
5 Principles of Moving and Manual Handling 5.1 This policy is based on the Moving and Handling Operations Regulations 1992
(amended 2002), which impose the following duties on the Trust:
To avoid so far as is reasonably practicable the need for employees to carry out those moving and handling operations which involve a risk of injury;
Where moving and handling cannot be eliminated, to make and keep up to date a suitable and sufficient risk assessment of moving and handling tasks, considering the factors and questions specified in the Schedule to the Regulations.
To take appropriate steps to reduce the risk of injury to employees arising from moving and handling operations to the lowest level reasonably practicable.
To take appropriate steps to provide employees who are carrying our moving and handling operations with general indications and, where reasonably practicable to do so, precise information on the wright of each load at the heaviest side of any load whose centre of gravity is not centrally positioned.
5.2 These duties must be carried out as far as is reasonably practicable. This involves
balancing risk with cost and practicality.
6 Risk Assessment Process 6.1 The Management of Health & Safety at Work Regulations 1999 require suitable and
sufficient risk assessments to be undertaken. Where this general risk assessment identifies a risk of injury from any hazardous manual handling that cannot be avoided,

MH1 – Moving and Handling Policy
9 of 69 Version 1 (Feb 2015)
a risk assessment must be carried out (See Appendix 2). The risk is then reduced as far as is reasonably practicable.
6.2 All ‘loads’ should be continually re-assessed to ensure that the risk continues to be
eliminated/ reduced.
6.3 If the identified risk control measures cannot be fully implemented, which may include lack of appropriate equipment, then the risk must be recorded in the zone/ department risk register and escalated to the directorate and/ or the Health and Safety Manager.
6.4 Inanimate Manual Handling Assessment – For inanimate Manual Handling of loads please see the guidelines set out in Appendix 3 and complete the Manual Handling of Loads Checklist, Appendix 4. Appendix 5 is a specific Pulling and Pushing checklist.
6.5 Client Handling Assessments - A Handling Assessment and Summary Plan (Appendix 6,7 or 8) must be completed for every client who requires manual handling assistance from Trust staff. The assessment must be kept in the clients’ notes and reviewed regularly. Immediately prior to each handling task staff must assess the risk and where necessary change the care plan accordingly. It is our responsibility to handover this risk assessment and moving and handling advice to the appropriate organisation or care agency on discharge
6.6 Therapeutic Handling - For additional Information on Therapeutic Handling please
refer to Appendix 9.
6.7 Bariatric Care – The Trusts are committed to treating people with a BMI of 35 and above plus associated co morbidities, safely and with dignity whilst ensuring the health and safety of staff involved in their care.
For further information and Bariatric equipment provision please refer to the Management of Bariatric Procedure (This is available on Trust intranet)
6.8 Children and Young People – See Appendix 7
6.9 Unplanned Events – In the event of employees encountering a collapsed or fallen client a clinical assessment should be undertaken and the appropriate action taken. See appendix 11.
6.10 The Falling Patient - At all times DO NOT RESIST or STOP a Patient from falling if you are at risk of injuring yourself. Allow the patient to go to the floor as safely as possible for both parties. See Appendix 11
7 Manual Handling Equipment 7.1 In hospitals Manual handling equipment will be provided in each working area relevant
to the identified handling task and based on completed risk assessments. If the equipment identified is not available, this should be reported to the Line Manager for action.
7.2 Where lifting equipment is provided, managers must ensure compliance with the
Lifting Operations and Lifting Equipment Regulations 1998.

MH1 – Moving and Handling Policy
10 of 69 Version 1 (Feb 2015)
7.3 Any moving and handling equipment that is found to be defective must be labelled as unsafe and reported in accordance with the Trusts procedures
7.4 In patients own homes staff visiting (OT, Physio or Nursing staff) should offer advice and risk assessment.
8 Moving and Manual Handling Training 8.1 To ensure compliance with the Moving and Handling Regulations, the Trust endorses
a cascade training system for the provision of information, instruction and practical training. Training sessions will include:
Back Care
Legislative information
Basic equipment available within the Trust
Principles of good handling
Practical training in moving and handling activities required by the individual.
Training needs to be undertaken on induction for all staff and yearly for all staff who are required to move patients as part of their role. For non-patient handlers, moving and handling training is required two yearly. Please see Core Training Policy (T1) for methods of delivery. All Occupational Therapists and Physiotherapists and (with exception of Musculoskeletal MSK physios) are required to undertake an initial 2 day risk assessor course and annually update.
8.2 Trainers are not experts, but individuals who have undergone additional training and
are able to pass on necessary skills. 8.3 Persons other than the Moving and Handling Trainer or designated qualified persons
will not deliver training. Risk assessors will demonstrate methods and techniques for individual patients.
8.4 All staff who attend a Manual Handling course will be inputted onto their individual Electronic Staff Record. (ESR) The manual handling team will also have a record of attendees for to enable them to monitor compliance..
8.5 Training needs analysis of mandatory and other training is undertaken annually by line managers. Line managers will receive staff attendance reports and it is their responsibility to ensure that their staff are adequately trained.
8.6 Manual handling training attendance reports are provided to the moving and handling team who will report on attendance of the training to the Health and Safety Committee on a quarterly basis.
8.7 See Appendix 15 for the letter of non-attendance that will be sent to delegates who do
not attend a training session. The letter will highlight the next available training dates and who to contact.
8.8 See Appendix 16 for persistent non attendee’s a letter will be sent to the individual at
their home address and their line manager will receive the letter as an email attachment internally.

MH1 – Moving and Handling Policy
11 of 69 Version 1 (Feb 2015)
8.9 See Appendix 17 for the Non Attendee process
9. Provision of training for Advisors/Trainers 9.1 The Trusts will send nominated persons on an initial 5 day training course. During this
course students will be instructed in:
Relevant Legislation
Moving and handling risk assessment
Basic ergonomics
Normal body movement
Moving loads
Moving and handling people
Teamwork
Teaching skills
Record keeping
Managing change
Basic anatomy and physiology of the spine Following successful completion of this course the trainer will be competent in moving
and handling risk assessment, and will be responsible for the delivery of moving and handling training within the trusts.
9.2 All Trust moving and handling trainers are required to attend an annual update to
maintain their training role. Attendance is required to ensure they remain on the moving and handling trainer register.
9.3 Appendices 12 and 12 A REBA and RULA templates are useful for trainers to assist in the risk assessment process.
9.4 Templates to record and evidence training induction Appendix 13 and Refresher
training Appendix 14.
10 Communication and Implementation of policy 10.1 All staff must read and understand the Moving and Handling Policy. 10.2 The policy will be published on iCare and Contact as well as the external Website.
The publication of this document will be highlighted on the news section on iCare, in the staff bulleting and via management meetings.
10.3 It is the responsibility of the Health and Safety Manager to ensure this policy is published in the final version with a completed ratification document. It is also the responsibility of the Health and Safety Manager to ensure that the publication of this document is communicated to all line managers.
10.4 It is the responsibility of each line manager to ensure that their staff read and understand the information contained within this policy.

MH1 – Moving and Handling Policy
12 of 69 Version 1 (Feb 2015)
11 Monitoring, Review and Evaluation of this policy 11.1 The Moving and Handling team will provide a quarterly report on moving and handling
issues and attendance of courses to the Health and Safety Committee. 11.2 Mandatory training attendance will be monitored and managed in accordance with the
Core Training Policy (T1) 11.3 The Health and Safety Team will provide quarterly staff incident reports encompassing
moving and handling issues to all directorates for discussion and monitoring.
11.4 This policy and associated documents will be reviewed on an annual basis (or sooner in the event of major organisational change), by the Moving and handling team, to ensure that it is relevant and effective.
11.5 The Induction and Mandatory Training Lead will monitor compliance with the policy by
reviewing individual ward/units compliance figures and meeting with workplace leads.
11.6 Statistical information regarding attendances at mandatory training will be produced by workforce and sent to managers on a quarterly basis. This information will be monitored by Workstream 4.
11.7 Feedback from all staff regarding this policy is encouraged and should be sent to the
Moving and handling team.
12 Key references
Health & Safety Executive - www.hse.gov.uk
Health and Safety in Human Health and Social Care in Great Britain, 2013
NHS UK – www.nhs.uk/backinwork
British Association/ College of Occupational Therapists – www.cot.co.uk
Chartered Society of Physiotherapy – www.csp.org.uk
The Royal College of Midwives – www.rcm.org.uk
The Royal College of Nursing – www.rcn.org.uk
Royal College of Radiologists – www.rcr.ac.uk
HSE Guidance on Regulations – Moving and Handling Operations Regulations 1192
(as amended 2004)
The Guide to the Handling of people 6th edition - Backcare
Rapid Entire Body Assessment (REBA), Sue Hignett and Lynn McAtamney 2000
A Rapid Upper Limb Assessment Tool (RULA), Nigel Corlett and Lynn McAtamney
1993
Moving and Handling of Plus Size People- an illustrated guide. National Back
Exchange 2013
Manual Handling of Children. National Back Exchange 2011

MH1 – Moving and Handling Policy
13 of 69 Version 1 (Feb 2015)
Appendix 1 – Moving and Handling Team Structure
INDUCTION AND
MANDATORY TRAINING
LEAD
COMMUNITY
2 LEARNING AND DEVELOPMENT
ADVISORS
ALL ACCREDITED TRAINERS
COMMUNITY
RISK ASSESSORS
BASED WITHIN
ZONES AND TEAMS
ACUTE
WARD BASED
COACHES
ACUTE
2 MOVING AND HANDLING ADVISORS
1 MOVING AND HANDLING TRAINER
ALL ACCREDITED TRAINERS

MH1 – Moving and Handling Policy
14 of 69 Version 1 (Feb 2015)
Appendix 2 - Risk Assessment Process Where a moving and handling operation is seen as a significant risk, and cannot be avoided, an assessment will be made having regard to the following factors
i) The task iii) The working environment ii) The load iv) The individual capability
How to follow the Moving and Handling Operations Regulations 1992: No Yes No
Yes /possibly No Yes No Yes No Yes/Possibly Yes No
Do the Regulations apply – i.e. does the work involve a moving and handling operation?
Is there a risk of injury?
Is it reasonably practicable to avoid moving the load?
Does some risk of manual handling injury remain?
Carry out assessment
Determine measures to reduce risk of injury to the lowest level reasonably practicable
Implement the measures
Is risk of injury sufficiently reduced?
Written record End of initial exercise
Review if conditions change
Is it reasonably practicable to auto-mate or mechanise the operation?

MH1 – Moving and Handling Policy
15 of 69 Version 1 (Feb 2015)
Appendix 3 - Guidelines for the Lifting of Inert Loads
Think before handling/lifting.
Plan the lift / handling activity.
Where is the load going to be placed?
Use appropriate handling aids where possible.
Will help be needed with the load?
Remove obstructions, such as discarded wrapping materials.
For long lifts, such as from floor to shoulder height, consider resting the load mid-way on a table or bench to change grip.
Keep the load close to the waist.
Keep the load close to the waist for as long as possible while lifting.
The distance of the load from the spine at waist height is an important factor in the overall load on the spine and back muscles.
Keep the heaviest side of the load next to the body.
If a close approach to the load is not possible, try to slide it towards the body before attempting to lift it.
Adopt a stable position.
The feet should be shoulder width apart with one leg slightly forward to maintain balance (alongside the load if it is on the ground).
Be prepared to move your feet during the lift to maintain a stable posture.
Wearing over-tight clothing or unsuitable footwear may make this difficult.
Ensure a good hold on the load. Where possible hug the load as close as
possible to the body. This may be better than gripping it tightly only with the hands.

MH1 – Moving and Handling Policy
16 of 69 Version 1 (Feb 2015)
Moderate flexion (slight bending) of the back, hips and knees at the start of the lift is preferable to either fully flexing the back (stooping) or fully flexing the hips and knees (full/deep squatting). Don't flex the back any further while lifting.
This can happen if the legs begin to straighten before starting to raise the load.
Avoid twisting the back or leaning sideways especially while the back is bent.
Keep shoulders level and facing in the same direction as the hips.
Turning by moving the feet is better than twisting and lifting at the same time.
Keep the head up when handling.
Look ahead, not down at the load once it is held securely.
Move smoothly.
Do not jerk or snatch the load as this can make it harder to keep control and can increase the risk of injury.
Don't lift or handle more than can be easily managed.
There is a difference between what people can lift and what they can safely lift. If in doubt, seek advice or get help.
Put down, then adjust. If precise positioning of the load is necessary, put it down first and then slide it into the desired position.

MH1 – Moving and Handling Policy
17 of 69 Version 1 (Feb 2015)
Appendix 4 - Risk Assessment Form
To be used for inanimate loads and complex patient/equipment handling
Example of Moving and Handling of Loads:
Assessment Checklist

Appendix 5 - Risk Assessment Form
Example of Manual Handling of loads: Pushing and Pulling Checklist

19 of 69 Version 1 (Feb 2015)
Appendix 6- SS10A – community hospital and community setting only
HANDLING ASSESSMENT SUMMARY AND PLAN REMEMBER! Frequency (approx.) X severity = risk
The purpose of this handling plan is to describe the assessed handling needs of the patient/service user named below and to specify how these should be met to reduce the risks of injury to both carers
and service user (refer to Risk Assessment and Manual Handling Policies).
Patient/Service User Detail
Name: …………………………………………………………………………. Ward/Location: ………………………………………………………. Address: Patient Number: ………………………………………………………. CareFirst Number: ……………………………………………………. ……………………………………………………………………….. / / Date of Birth: ……………………………………………………………….. Initially Assessed by: …………………………………………………. / / GP: …………………………………………………………………………… Initial Assessment Date: ……………………………………………… Disability/ Height: ………………….. Weakness: …………………………………………………………………… Weight: …………………… BMI: …………………..
Initial assessment Yes No Equipment
Can they co-operate/communicate effectively?
Can they weight bear/stand?
Have they got standing balance?
Can they walk?
Can they maintain sitting balance?
Can they get into/out of bed?
Can they sit up in bed?
Can they move up in bed?
Do they have any attachments (e.g. catheter?)
Are they receiving medication which may affect movement?
Do they have a history of falling/ Refer to falls team
Do they use any mobility aids?
If you need to add any further details, please use the Additional Information section on Page 3.
Service User Risk Level Date: / / / /
Patient unable to assist in any way, due to unconsciousness, likely to behave unpredictably, may be heavy, or have high level of disability
RED High/Significant Risk
Able to co-operate and can move with assistance and/or requires the use of small moving aids.
YELLOW Medium Risk
Needs minimal assistance, supervision, or guidance GREEN Low Risk
Data Protection Act: Details you have provided have been used to inform this handling plan and identify any agreed actions. This information may be stored on computer and will be shared with other agencies working with us to meet the agreed needs within your Care Needs Summary and Care Plan.
These recommendations have been agreed by the patient/service user or representative: Patient/Service User Signature: ……………………………………………………………. Initial Assessor Signature: …………………………………………………………………… Date: ……../……./…………. Designation: ……………………………………………………………………………………
20 of 69 Version 1 (Feb 2015)
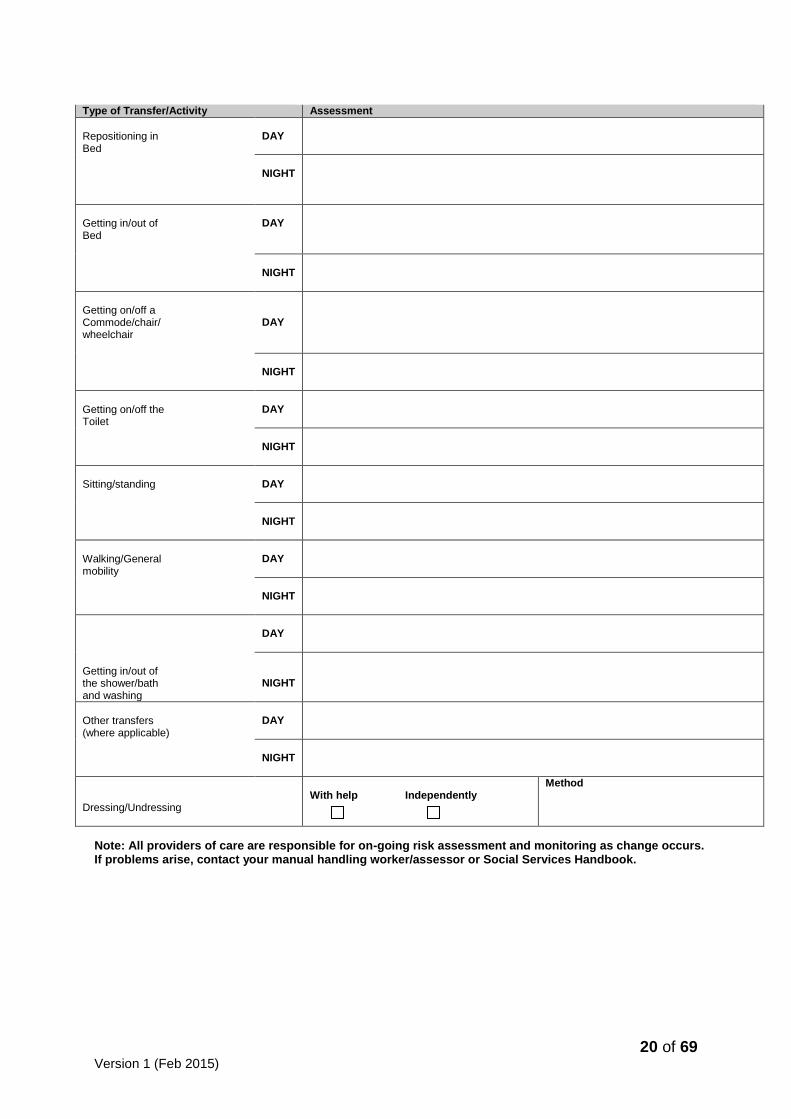
Type of Transfer/Activity Assessment
Repositioning in Bed
DAY
NIGHT
Getting in/out of Bed
DAY
NIGHT
Getting on/off a Commode/chair/ wheelchair
DAY
NIGHT
Getting on/off the Toilet
DAY
NIGHT
Sitting/standing
DAY
NIGHT
Walking/General mobility
DAY
NIGHT
DAY
Getting in/out of the shower/bath and washing
NIGHT
Other transfers (where applicable)
DAY
NIGHT
Dressing/Undressing
With help Independently
Method
Note: All providers of care are responsible for on-going risk assessment and monitoring as change occurs. If problems arise, contact your manual handling worker/assessor or Social Services Handbook.

21 of 69 Version 1 (Feb 2015)
Information/equipment required for service user 1. Hoist: Specify type Sling: detail size, type and loops used
2. Small handling aids
3. Toilet and/commode
4. Bed and Chair: specify types/heights/mattress
5. Equipment usage demonstrated to carer:
6. Additional information:
Assessor’ s Signature: ……………………………………………………. Date: ……/……/………………………… Designation: ……………………………………………………… Review Date: ……/…../………………………….
Copies sent to:
Adult & Community Services Patient/service user Carer(s) Service Provider(s) Health worker(s) File Other (please specify)
……………………………………………………………………………………… Sent by: ………………………………………………………………… Date sent: ………./……./………..

22 of 69 Version 1 (Feb 2015)
Appendix 7: HANDLING ASSESSMENT SUMMARY AND PLAN REMEMBER Frequency (approx) X severity = risk The purpose of this handling plan is to describe the assessed handling needs of the Child/Young Person named below and to specify how these should be met to reduce the risks of injury to both carers and Child/Young Person (refer to risk Assessment and Manual Handling Policies). Within Torbay Council and Torbay & Southern Devon Care Trust
Child / Young Person User Detail
Name: __________________________ Ward/Location:____________________________ Address: NHS Number: _____________________________ ___________________________ Paris Number: _____________________________ Date of Birth: / / ___ Initially Assessed by: ________________________ GP: _____________________________ Initial Assessment Date: / / Disability/ Height: ______________ Weakness: _______________________________ Weight: _____________ BMI: ___________
Service User Ability Yes No Details Can they co-operate/communicate effectively?
Can they weight bear/stand?
Have they got standing balance?
Can they walk?
Can they maintain sitting balance?
Can they get into/out of bed?
Can they sit up in bed?
Can they move up the bed?
Do they have any attachments (e.g. catheter pegs)?
Are they receiving medication which may affect movement?
Do they have a history of falling? Refer to falls team.
Do they use any mobility aids?
If you need to add any further details, please use the Additional Information section on Page 3
Service User Risk Level Date / / / /
Patient unable to assist in any way, due to unconsciousness, likely to behave unpredictably, may be heavy, or have high level of disability
RED High/significant
Risk
Able to co-operate and can move with assistance and/or requires the use of small moving aids
YELLOW Medium Risk
Needs minimal assistance, supervision, or guidance
GREEN Low Risk

23 of 69 Version 1 (Feb 2015)
Data Protection Act: Details you have provided have been used to inform this handling plan and identify any agreed actions. This information may be stored on computer and will be shared with other agencies working with us to meet the agreed needs within your Care Needs Summary and Care Plan.
These recommendations have been agreed by the patient/service user or a representative: Child/Young Person or Parent/Carer with parental responsibility Signature __________________________________________ Initial Assessor Signature _____________________________________ Date: _________/_______/___________ Designation ____________________________________________
Type of Transfer/Activity
Assessment
Repositioning in bed/cot
Day
Night
Getting in/out of bed/cot
Day
Night
Getting on/off a commode /chair /wheelchair /buggy
Day
Night
Getting on/off the toilet/ potty
Day
Night
Sitting/standing
Day
Night
Walking/general mobility
Day
Night
Getting in/out of the shower/bath and washing
Day
Night
Other transfers (where applicable)
Day
Night
Getting in/out of the car/car seat
Day
Night
Dressing/Undressing
With Help Independently
Method
Note: All providers of care are responsible for on-going risk assessment and monitoring as change occurs. If problems arise, contact your manual handling worker/assessor or Social Services Handbook.

24 of 69 Version 1 (Feb 2015)
Information/equipment required for service user
1. Hoist: Specify type Sling: detail size, type and loops used
2. Small handling aids
3. Toilet and / or Commode
4. Bed and Chair: Specify types/heights/mattress
5. Equipment usage demonstrated to carer:
6. Additional information:
Assessor’s Signature: ______________________________ Date _____/____/____ Designation: _____________________________ Review Date ______/_____/___
25 of 69 Version 1 (Feb 2015)
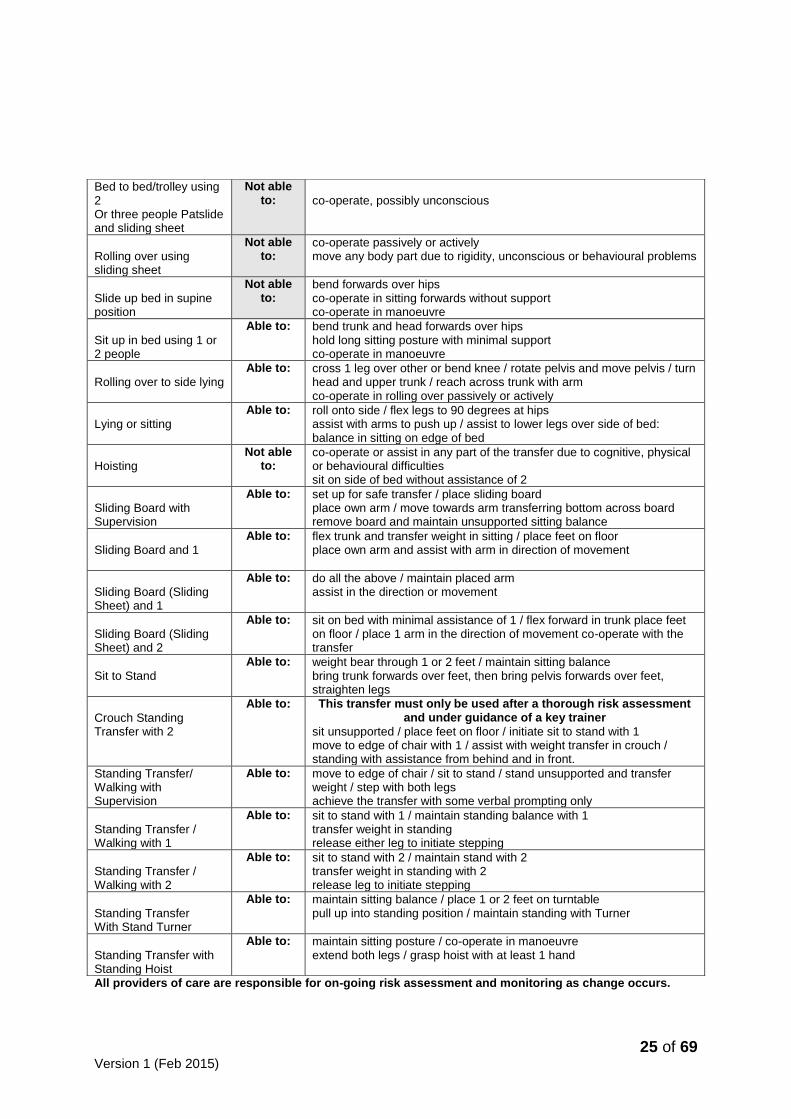
All providers of care are responsible for on-going risk assessment and monitoring as change occurs.
Bed to bed/trolley using 2 Or three people Patslide and sliding sheet
Not able to:
co-operate, possibly unconscious
Rolling over using sliding sheet
Not able to:
co-operate passively or actively move any body part due to rigidity, unconscious or behavioural problems
Slide up bed in supine position
Not able to:
bend forwards over hips co-operate in sitting forwards without support co-operate in manoeuvre
Sit up in bed using 1 or 2 people
Able to: bend trunk and head forwards over hips hold long sitting posture with minimal support co-operate in manoeuvre
Rolling over to side lying
Able to: cross 1 leg over other or bend knee / rotate pelvis and move pelvis / turn head and upper trunk / reach across trunk with arm co-operate in rolling over passively or actively
Lying or sitting
Able to: roll onto side / flex legs to 90 degrees at hips assist with arms to push up / assist to lower legs over side of bed: balance in sitting on edge of bed
Hoisting
Not able to:
co-operate or assist in any part of the transfer due to cognitive, physical or behavioural difficulties sit on side of bed without assistance of 2
Sliding Board with Supervision
Able to: set up for safe transfer / place sliding board place own arm / move towards arm transferring bottom across board remove board and maintain unsupported sitting balance
Sliding Board and 1
Able to: flex trunk and transfer weight in sitting / place feet on floor place own arm and assist with arm in direction of movement
Sliding Board (Sliding Sheet) and 1
Able to: do all the above / maintain placed arm assist in the direction or movement
Sliding Board (Sliding Sheet) and 2
Able to: sit on bed with minimal assistance of 1 / flex forward in trunk place feet on floor / place 1 arm in the direction of movement co-operate with the transfer
Sit to Stand
Able to: weight bear through 1 or 2 feet / maintain sitting balance bring trunk forwards over feet, then bring pelvis forwards over feet, straighten legs
Crouch Standing Transfer with 2
Able to: This transfer must only be used after a thorough risk assessment and under guidance of a key trainer
sit unsupported / place feet on floor / initiate sit to stand with 1 move to edge of chair with 1 / assist with weight transfer in crouch / standing with assistance from behind and in front.
Standing Transfer/ Walking with Supervision
Able to: move to edge of chair / sit to stand / stand unsupported and transfer weight / step with both legs achieve the transfer with some verbal prompting only
Standing Transfer / Walking with 1
Able to: sit to stand with 1 / maintain standing balance with 1 transfer weight in standing release either leg to initiate stepping
Standing Transfer / Walking with 2
Able to: sit to stand with 2 / maintain stand with 2 transfer weight in standing with 2 release leg to initiate stepping
Standing Transfer With Stand Turner
Able to: maintain sitting balance / place 1 or 2 feet on turntable pull up into standing position / maintain standing with Turner
Standing Transfer with Standing Hoist
Able to: maintain sitting posture / co-operate in manoeuvre extend both legs / grasp hoist with at least 1 hand

26 of 69 Version 1 (Feb 2015)
Appendix 8 – Acute Setting Only
Patient Handling, Falls & Bed Rail Assessment To be completed WITHIN 6 hours of admission, if patient’s condition deteriorates, on transfer or post fall
Surname........................................................................ (Attach name label)
Forename…………………………………………………………..…………..
Hospital No.…………………………………………….…………..….……….
Date of Birth....................................................Age.....................................
Ward/Area…...............................................................................................
Weight........................................kg
scale weight estimate
Height........................................cm
BMI...............................................
Width at waist…………………. cm
Patient History – tick appropriate column Yes No Details
Is the patient uncooperative/have inadequate comprehension?
Is the patient receiving medication which affects movement?
Is the patient’s centre of gravity altered, e.g. stroke?
Does the patient have fixed/swollen/flaccid limbs?
Does the patient have attachments e.g. catheters/IV?
Falls History – tick appropriate column Yes No Details
Is the patient confused/disorientated? Yes? Intentionally round
Is the patient unsteady of his/her feet? Yes? Intentionally round
Is there a history of falls one year prior to this admission? Yes? Intentionally round
Has the patient fallen since admission? Yes? Intentionally round
Record of falls since admission: please circle. 1 2 3 4 5 More (No)
Patient ability – tick the appropriate column No Yes Assistance reqd
Can the patient turn over in bed?
Can the patient sit up in bed?
Can the patient move back up the bed?
Is the patient able to maintain a sitting balance?
Can the patient get into/out of bed?
Is the patient able to weight bear/stand?
Is the patient able to walk?
Does the patient use mobility aids and require assistance?
Overall Assessment based upon answers & clinical judgement – review if any changes
Initial ass
t
Date 1
Review Date 2
Review Date 3
Follow Falls & Patient Manual Handling Assessment Plan
HIGH RISK
Follow Low Risk Strategies & Basic Falls Advice & Patient Manual Handling Assessment Plan
LOW RISK
Low Risk Strategies & Basic Falls Advice Tick
Introduce patient to ward environment, washing & toilet facilities
Remind patient to request assistance as required
Check environment for slip/trip hazards & other obstacles
Ensure hearing aids are working & spectacles clean & within reach
Teach patient to use bed controls and call bell (leave within reach)
Check patient has supportive, well fitted footwear with a non-slip sole
If no one is available to bring in footwear use ‘top-up’ slippers
Ensure walking aids are kept within patient’s reach
Assessor……………………………………………………….Sign…………………………………………………..
Designation…………………………………………………….Date/Time…………………………………………….
High Risk Strategies & Interventions Complete Manual Handling Plan & Falls Assessment
Yes
No
Comments

27 of 69 Version 1 (Feb 2015)
N.B. Ensure that patient is included in safety brief/handover as high falls risk
Is Patient being observed? (Tick as appropriate)
Intentional Rounding □ Cohorting □ 1 to 1 nursing □
Should patient be moved to observable area? N.B. High priority for patients with evidence of confusion
Is Yellow Falls Symbol above bed & on Nurse Information Board?
Is night lighting required for patient?
ECG required?
Is patient on >4 medications, anti-hypertensive, sedatives or anti-psychotics? N.B. If Yes, arrange review by Medical staff or Pharmacist.
If evidence of /risk of fragility fracture, refer to medics/FLS for calcium, vitamin D and/or bisphosphonate consideration
If evidence of /risk of fragility fracture, refer to medics/FLS for calcium, vitamin D and/or bisphosphonate consideration
Has a lying/standing BP been recorded? Postural Hypotension Leaflet □ N.B. If Systolic differential is >20 mm Hg arrange review by Medical staff.
Consider use of bed/chair sensor pads & Hi-Lo bed
Leaflets given to patient (Tick as appropriate)
In-patient falls □ “Staying Steady” □
Is patient incontinent? (If yes consider referring to Continence Advisory Service) If patient is symptomatic, take urinalysis to exclude UTI?
Manual Handling Plan Complete relevant activities ONLY - AVOID UNDERARM LIFTING - Review any changes
Activity Assessment No
& Date N
o of
staff Equipment required Additional information
Moving in
bed/movement up bed
1
2
3
Sit up on side of
bed
1
2
3
Sit to stand
1
2
3
Assessor………………………………………………………….Sign………………………………………………… Designation………………………………………………………Date/Time…………………………………………
Manual Handling Plan Complete relevant activities ONLY - AVOID UNDERARM LIFTING - Review any changes
Activity Assessment No
& Date N
o of
staff Equipment required Additional information
Walking
1

28 of 69 Version 1 (Feb 2015)
2
3
Transfers
(Bed to Chair Chair to chair)
1
2
3
Other transfers
(Detail)
1
2
3
Lateral Transfer
1
2
3
Hoisting
Detail hoist used
Sling size/type
1
2
3
1
2
3
Bariatric Equipment Required
Bed Chair Commode Hoist & Sling (size) Walking aid Other
Assessor………………………………………………………….Sign……..…………………………………………… Designation………………………………………………………Date/Time…………...……………………………….
Bed Rail Assessment
Mobility
Patient is very immobile (bedfast or hoist dependent)
Patient is neither independent nor immobile
Patient can mobilise without help from staff
1 2 3
Mental state
Patient is confused & disorientated
A Use bed rails with care Bed rails not recommended
Bed rails not recommended
Patient is drowsy B
Bed rails recommended Use bed rails with care
Bed rails not recommended
Patient is alert & orientated
C Bed rails recommended Bed rails recommended
Bed rails not recommended

29 of 69 Version 1 (Feb 2015)
Patient is unconscious D Bed rails recommended N/A N/A
Please use the risk matrix above in conjunction with nursing judgement, remembering:-
To assess, consider Mental State score in combination with Mobility score, e.g. A1, C3, etc.
Patients with capacity can make their own decisions about bed rail use.
Patients with visual impairment may be more vulnerable to falling from bed.
Patients with involuntary movements (e.g. spasm) may be more vulnerable to falling from bed, and if bed rails are
used, may need additional support systems or protection.
Assessment Score & Date Additional Information
1
2
3
Physio/OT/S</Dietitian referral reqd
Yes / No Details
Dementia Awareness Yes / No Details
Further information
Data Protection Act: Details that you have provided have been used to inform this assessment and identify any agreed actions.
This information will be shared with other agencies working with us to meet these agreed needs within your Care Needs Summary and Care Plan.
These recommendations have been agreed by the patient or their representative:
Patient
signature………………………………………………………………………Date/Time…………………….…..............................
Assessor…………………………………………………………..Sign……………………………………………..…… Designation……………………………………………………….Date/Time……………………………………………..

30 of 69 Version 1 (Feb 2015)
Appendix 9 Guidelines to Therapeutic Handling in Therapy Treatment
These Guidelines are designed to assist therapists to use informed clinical reasoning behind using therapeutic activities that may increase the risk of injury to the therapist. These guidelines must be used in conjunction with the Therapeutic Risk Assessment form and the patient-handling plan. All therapy staff must work within their own level of competence and ability; Refer to (CSP Rules of Professional Conduct and Standards, CSP Guidance in Manual Handling for Chartered Physiotherapists (CSP 2008), Guidance on Manual Handling in Treatment, (ACPIN MH Working Party 2001), Trust Moving and Handling Policy. All handling tasks must be explained to the patient and informed consent given prior to any moving and handling activity. Patient Specific Assessment Protocol
1. Assess the patient clinically 2. Consider realistic clinical goals and functional outcomes if possible in discussion with
the patient 3. Does the proposed treatment/therapeutic handling involve hazardous manual
handling? 4. Can the hazardous manual handling be avoided while still meeting the patient’s
clinical and functional goals by using aids or equipment? 5. If the hazardous manual handling cannot be avoided then a full risk assessment
using the TILE process must be carried out. 6. Reduce the hazardous manual handling activity by adapting the technique,
assistance of appropriate trained colleagues or use of equipment. 7. Record risk assessment and risk management protocols or 8. Re-evaluate and consider competence to proceed. Reconsider the goals.
IF THE THERAPIST FEELS THAT A PARTICULAR TECHNIQUE IS THE ONLY ONE POSSIBLE AND THAT HE/SHE CAN EXECUTE THIS TECHNIQUE SAFELY, THE CLINICAL REASONING BEHIND THE DECISION NEEDS TO BE DOCUMENTED. THE THERAPIST MUST MINIMISE, AS FAR AS IS REASONABLY PRACTICABLE, THE RISK OF DAMAGE TO THEMSELVES, STAFF AND PATIENTS WHILE STILL ENABLING THE PATIENT’S PROMPT PROGRESS TOWARDS FUNCTION. MOVING AND HANDLING CSP 1998

31 of 69 Version 1 (Feb 2015)
Rolling over Clinical Reasoning
Experiencing movement with a low centre of gravity
Facilitate rotation in the trunk
Facilitate trunk and head righting and equilibrium reactions
To achieve a functional goal Patient Criteria Patient is medically stable Patient can co-operate in rolling supine to side lying Patient has no pathology that would negate rolling, e.g. hip replacement, acute back injury. Patient can be facilitated to:
Place left leg in flexion
Facilitate left arm across the trunk
Turn head in direction of rolling
Facilitated from pelvis and shoulder girdles to roll from supine to right side lying
Possible Hazards
Patient fearful of moving.
Surface the patient is rolling on is unstable or soft and low to the ground
Therapists have to work in poor postures
Temptation to pull the patient over into side lying rather than facilitate, this is usually due to the therapist not using their own dynamic movement to facilitate the patient activity.
Lying to Sitting Therapist will use guidelines to roll patient over to side lying. Single therapist facilitation Therapist in front of patient in side lying With other hand flex knees to 90º and tip feet over edge of bed Places hand on pelvis Therapist moves laterally pressing down on pelvis and stabilising shoulder girdle, facilitates patient into a sitting position Double therapist facilitation If 2 assistants are needed the therapist behind the patient kneels on the bed close to patient One hand on lower shoulder girdle, one hand on rib cage Therapist in front has one hand on top of pelvis and one hand supporting lower limbs Front therapist pushes down through pelvis, back therapist facilitates trunk up over pelvis into a sitting position

32 of 69 Version 1 (Feb 2015)
Modifications
Head of bed could be raised to bring patient into more of a sitting position
Number of assistants needed may vary depending on the head control and tone of patient, level of postural control, number of attachments etc.
Patients arm position may vary depending on ability to assist
If bed height can vary it may be more beneficial to start with bed high and then lower when patient in a sitting position to put their feet on the floor
Hazards
Change in medical status
Co-operation of patient may change during manoeuvre
Tonal changes
Low plinth/bed
Soft/Air mattresses
Potentially poor postures
Cluttered environments
Maintain Sitting Clinical Reasoning
Facilitate righting and equilibrium reactions
Accept base of support with hips and lower limbs
Experience mid line orientation
Free upper limbs for reaching and placing
To achieve a functional goal Patient Criteria Patient is medically stable Able to be placed up against gravity Able to facilitate trunk into extension over pelvis Able to place one or both upper limbs at 90º Patient co-operative both physically and cognitively Therapist behind kneels on supporting surface or stands behind supporting surface Therapists place patient on a stable supportive surface Therapist behind stabilises upper trunk The pelvis is placed so that equal weight bearing is experienced through the hips The hips and knees are at 90º with the feet on the floor under the knees The thighs are in contact with base of support and placed parallel to each other The trunk is facilitated into extension over the pelvis The shoulder girdles are aligned over the hips Reaching with the upper limbs across midline while keeping the body’s centre of gravity with in the base of support may assist to create midline orientation The second therapist may sit or kneel in front of patient and facilitate from the pelvis and align lower limbs

33 of 69 Version 1 (Feb 2015)
Hazards
Patient can become medically unstable
Patient may push into extension
Tonal changes in response to gravity
Base of support is not sufficiently stable for the patient and therapist i.e.; use of unstable
pressure mattress or soft mattress
Therapists adopt sustained/ poor posture
Modifications
Use a side supported sitting position on more active side
Use of low back upright chair
Therapist behind can sit on a ball that supports patients trunk in preparation for mobilisation
Sit to Stand Clinical Reasoning
Experience movement into extension over feet
Access righting reactions
As preparation for walking and transfers
Building a background of extensor postural tone Patient Criteria
Weight bear through 1 or 2 feet
Maintain sitting balance
Move trunk forwards over feet
Tilt pelvis forwards over feet
Straighten legs Patient facilitated to move forwards in chair Patient can maintain unsupported sitting using their hands or facilitation from proximal key points Patient’s feet can be placed on floor with more than 90º at ankle Patient can be facilitated to move trunk over feet Patient can be facilitated to move pelvis forwards over feet Patient can maintain standing with centre of gravity over base of support

34 of 69 Version 1 (Feb 2015)
Modifications
Use of equipment
Patient stands down from high plinth
More than one person needed to facilitate patient
Use of patient’s upper limbs
Hazards
Tonal changes patient may thrust backwards, pull into flexion, or lose feet off floor
Patients behaviour/co operation
Attachments to patient e.g. drips, tracheostomy
Medical status
Staff level of skill and competence
Height relationship of therapists to each other and the patient
Crouch Transfer This is a high risk activity and must be thoroughly risk assessed as the only option to use therapeutically and documented Clinical Reasoning
To be actively involved in transfer
To weight bear through all four limbs
Increase awareness of affected side
To access lateral weight transfer through rotation
To achieve a functional goal
Patient Criteria
To be able to place feet on floor
To be able to maintain sitting balance
To be able to place hands
To be able to initiate sit to stand
To be able to transfer weight laterally through hips
Patient facilitated from proximal key points to move forward in the chair Patient’s hand is placed on transfer surface that they are moving to Patient’s other hand is placed on supporting surface Patient’s feet are placed on floor in direction of transfer Patient is facilitated from proximal key points to bring weight over feet Patient is facilitated to transfer pelvis laterally to new supporting surface Patient’s pelvis and trunk are aligned on new seating surface

35 of 69 Version 1 (Feb 2015)
Modifications
Number of facilitators required
Use of sliding board and handling belt
Stand aids Hazards
Therapists’ in poor posture
Therapists’ unbalanced
Therapists’ skill and competence
Level of co-operation and ability of patient
Tonal changes
Attachments to patient
Heights of transfer surfaces
Changing types of base of support
Standing Transfer through 90degrees
Clinical Reasoning
Access righting and equilibrium reactions
Experience displacement through gravity using rotation through midline
Initiate stepping
Preparation for walking
To achieve a functional goal Patient Criteria
Able to sit unsupported
Able to place feet
Able to sit to stand
Able to maintain Standing Balance
Able to achieve single leg stance
Able to step with either leg sideways, forwards, and backwards
Patient can be facilitated sit to stand from proximal key points Patient can be facilitated to transfer weight to one leg Patient can release non standing leg Patient can be facilitated to step through rotation with non-standing leg Patient can be facilitated to transfer weight diagonally over stepping leg Patient can be facilitated to step backwards with non-weight bearing leg Patient can be facilitated to stand to sit Modifications
Use of equipment
Number of facilitators required
Facilitation from different key points
Assistance for correct foot placing
Patient’s use of Upper Limbs

36 of 69 Version 1 (Feb 2015)
Hazards
Changing medical status of patient
Therapist’s freedom of movement and balance
Therapist’s level of skill and competence
Change in Patient’s co-operation and behaviour
Tonal changes during transfer
Patient attachments; e.g. drips etc.
Functional Walking Clinical Reasoning
Access Righting and Equilibrium Reactions
Access stepping reactions
Experience displacement through gravity
Improve balance mechanisms
To achieve a functional goal Patient Criteria
Able to sit to stand
Able to maintain standing
Able to transfer weight to left and right
Able to orientate to midline
Able to initiate stepping forwards, backwards, and sideways Patient medically stable Patient can co-operate physically and mentally Patient can maintain standing with assistance Patient can be: Facilitated sit to stand from the pelvis and shoulder girdle Facilitated to transfer weight to right and left Facilitated to step with alternate leg forwards, backwards, and sideways Modifications
Number of facilitators required
Use of equipment
Assistance to correct foot placing
Patients use of upper limbs Hazards
Changing medical status of patient
Therapist’s freedom of movement and balance
Therapist’s level of skill and competence
Change in Patient’s co-operation and behaviour
Tonal changes during transfer
Patient attachments e.g.drips etc.

37 of 69 Version 1 (Feb 2015)
Patient Facilitated off the floor Clinical Reasoning
Access righting and equilibrium reactions
Reduce fear of falling
Re-educate independence to get down to and up from floor
Improve upper and lower limb functional movement Patient Criteria
Be able to maintain sitting balance
Able to flex hips and knees to 90º
Able to weight bear through all four limbs
Able to kneel with or without support
Able to co-operate with instructions Facilitate patient into side lying Facilitate patient into side sit Facilitate the patient into 4 point kneeling Facilitate the patient to kneel Facilitate the patient to weight transfer onto one knee Bring other foot onto floor into ½ kneeling Facilitate patient into standing Modifications
Stool/chair in front patient facilitate to crouch stand and turn pelvis to place in chair
Patient facilitated to crawl to piece of furniture in preparation to sit
When patient is in ½ kneel put small stool under the right angle hip, allow patient to sit
back onto stool
A pillow is placed under knees in 4 point kneeling to relieve pressure/pain
Equipment e.g. Air cushion, hoist Hazards
Patient co-operation
Tonal changes
Weakness in lower limbs
Painful joints
Stairs Clinical reasoning
To increase ability to transfer weight
To strengthen anti-gravity muscles
To improve exercise tolerance
To increase confidence in balance
To achieve a functional goal
38 of 69 Version 1 (Feb 2015)
Stairs with 2 Patient Criteria
Able to sit to stand with assistance of 1
Able to stand with assistance of 1
Able to step up and over a block with assistance of 1 (with or without arm support)
Able to walk with assistance of 1 +/- walking aid
Able to control knees to maintain extension during weight bearing Going Upstairs Patient is positioned in standing at edge of stairs with appropriate arm support One therapist is positioned behind the patient and one in front of the patient The therapist in front faces the patient and is the lead. They can gain eye contact, and communicate with the patient and watch their facial expression. They can also make sure the hands are placed on any appropriate support and shoulders stay forward The therapist behind the patient stands on the step below the patient, and is responsible for placing the patient’s foot on the step and facilitating the pelvis if necessary. Going down stairs One therapist stands behind the patient and one therapist in front of the patient about 2 steps below them facing the patient. The therapist behind is responsible for keeping the patient’s shoulders and back in extension. While the patient places their hand appropriately on the stair rail. The front therapist guides the patient’s foot onto the lower step and stabilises hip when necessary.
Stairs with 1 Patient Criteria
Able to sit to stand with supervision
Able to stand with supervision of 1
Able to follow commands
Able to step up and over a block with supervision of 1 (with or without arm support)
Able to walk with close supervision of 1 +/- walking aid
The patient has good trunk control, and can use own upper limb for support if needed.
Going upstairs therapist takes the position and function of the therapist behind the patient (Stairs with 2). Going downstairs the therapist takes up the position and function of the therapist in front of the patient (Stairs with 2)
Stairs with supervision Patient Criteria
Able to step up and over a block with or without arm support
Able to walk with or without aid
May require verbal prompts to achieve any of the above but physically independent

39 of 69 Version 1 (Feb 2015)
Modifications
Patient’s use of upper limbs
Number of stair rails used
May need to facilitate from different key points and therefore vary hand position as outlined above
Therapist’s position in front may vary
Consideration of whether patient should be in suitable footwear or bare feet
Stair technique may vary
Hazards
Change in patient’s co-operation and behaviour during activity
Therapist may have an unstable base of support
Therapist may adopt a flexed posture
Tonal changes in patient during activity
Therapist walking backwards down the stairs

40 of 69 Version 1 (Feb 2015)
Appendix 9: Therapeutic Handling Assessment
Name DOB
Address Height: Weight:
Area seen:
Name of Therapists:
Named Task and Clinical Reasoning
Date/Time Signature
Individuals assisting
Job title/grade persons assisting
where relevant
Client Details Relevant to risk Clients ability
criteria
Environment Record details relevant to risk not just location
of task
Risk Reducing Measures
Date and reason no
longer applicable

41 of 69 Version 1 (Feb 2015)
Named Task and Clinical Reasoning
Date/Time Signature
Individuals assisting
Job title/grade, person/s assisting
where relevant
Client Details Relevant to risk Clients ability
criteria
Environment Record details relevant
to risk
Risk reducing measures
Date and reason no
longer applicable

42 of 69 Version 1 (Feb 2015)
Appendix 10
Hoist and Sling Provision
Prescribing Hoists
The several of hoists; hydraulic(these are rare today but you may come across one) mobile hoists, electric mobile hoists, gantry and track hoists. From a moving and handling perspective the track hoists are the favoured in the community, as they reduce the risks to care assistants by avoiding the need to push a heavy load possibly on carpet (See HSE guidelines Moving and handling Operations Regulations revised 2004). However, these can be restrictive and so the mobile hoist may be more appropriate in a given situation as they are more flexible.
There are a variety of sizes of each type of hoist, when prescribing the size the smallest and lightest possible should be prescribed after taking into account: weight of service user and heights of lifting surfaces.
Larger hoists will require more space to manoeuvre (Always a problem in the community) and will make the load heavier.
Where space is limited a number of pushing and pulling manoeuvres need to take place to avoid twisting.
The start of any pushing or pulling manoeuvre requires more effort to overcome inertia than the continuation. (Newton’s first law of motion) (The guide to the Handling of People, Chapter 6, Page 57, P Leggett)
Twisting is particularly stressful on the back. The HSE have given guidelines that suggest where the spine is twisted it takes 10 -20% less force to injure it. (HSE MHOR Guidance on Regulations 2004)
Where possible an overhead hoist should be prescribed to avoid the need for pushing and pulling the hoist plus service user and so reducing the risk of injury as described above.
The Hydraulic hoist increases the risk of neck and shoulder injury to the care assistant. This is due to the repetitive movements, under load, of the upper arm required to pump up a hydraulic hoist and the difficulty of maintaining a safe posture while doing so (Wilson 2002).
The heavier the service user, the more pressure required to pump the hydraulic lever.
If there is only one care assistant involved, it is very difficult to lower the service user into a sitting position, and position them correctly at the same time, while maintaining a good posture. This activity can take several seconds to complete with the care assistant maintaining a poor posture, often stooping and twistinThis static posture combined with twisting and stooping increase the risk of a back injury considerably.
With an electric hoist the service user can sometimes take control of the lifting and lowering so that the care assistant can move around to care for the service user’s positioning. Or the care assistants can control the lifting and lowering and care for the service user in more appropriate postures.
The mechanism of a hydraulic hoist uses the repeated pumping of a lever to lift the boom of the hoist and its load. If this is only done once or twice a day by a fit person, and he/she is aware of the dangers and so minimizes them by being in a good position, the risks are low. However, domiciliary care staff may well be going from one moving and handling task to another with little rest between and could well end up being at high risk of injury if they have several service users with hydraulic hoists.
Employers of care staff have a responsibility to ensure that staff are not put at risk in this way.
If there are problems with recharging the batteries reliably on an electric hoist, a hydraulic one may be the more appropriate. This should be documented in the risk assessment.
It is therefore recommended that only in exceptional circumstances should a hydraulic hoist be prescribed instead of an electric one.
Once a need for a hoist has been identified; if there are no electric hoists available, but there are hydraulic ones, then it would reduce the risk to the care assistant to use the hydraulic hoist rather than attempt to lift the service user. This should be a short term measure until an electric one can be delivered.

43 of 69 Version 1 (Feb 2015)
It is important to do a thorough risk assessment when providing a hoist and make sure control measures are in place to reduce the risks of using the equipment. The carers or care assistants must be trained and able to use the equipment safely.
Slings There have been some falls nationally from hoists due to poor compatibility of slings and hoists, inappropriate laundering of slings, inadequate type of sling for service user, and inadequate maintenance. Action There should be a thorough risk assessment before prescribing a sling and hoist. This should ensure:
The sling is compatible with the hoist, i.e. it should have the correct attachments.
The appropriate sling for the service user’s needs
Transfers that will be carried out with it.
For advise on types and use of slings please contact:- o Moving and Handling Team at Horizons 01803 656600 Moving and Handling o CES/PLUSS/NRS o Independent Living Centre – Newton Abbot o Disabled Living Foundation o Individual Company Representatives
All hoists and slings are visually inspected before use and removed from service if defects are found.
Slings should be laundered according to manufacturer’s instructions.
Please note single use slings should not be laundered.
All hoists and slings are used and maintained according to manufacturer’s instructions and inspected by a competent person every six months as outlined in the Lifting Operations and Lifting Equipment Regulations (LOLER).
Summary
Hoists and slings should only be prescribed after careful risk assessment. Slings and hoists should be compatible with each other and appropriate to the service user and transfer they will be used for.

44 of 69 Version 1 (Feb 2015)
Appendix 11 Procedure for getting a fallen patient off the floor. Acute
Patient Falls
Assess using post fall checklist in falls care plan.
Hip Injury Suspected Spinal Injury Suspected
No sign of fracture or other injury If patient able – “talk up from floor” If unable, access scoop stretcher or consider hoisting if patient consents
Assess for hip and
spinal injury (see
guidance)
Do not hoist Immobilise
Contact PORTERS to bring Scoop Stretcher OR
Hoverjack
Do not Hoist Access Spinal Board
Immobilise

45 of 69 Version 1 (Feb 2015)

46 of 69 Version 1 (Feb 2015)
Appendix 12
Use Table C Score A Score B
Score C
REBA: Scoring Use Table A Use Table B
Group A
L
L
L
Lower arms
Upper arms
Wrists
R
R
R + +
Load/Force Coupling
Trunk
Neck
Legs
Group B
+
Activity Score
REBA Score
Source: Hignett, S., McAtamney, L. (2000) Applied Ergonomics, 31, 201-5. ©Professor Alan Hedge, Cornell University, September 2001.

47 of 69 Version 1 (Feb 2015)
Appendix 12A

48 of 69 Version 1 (Feb 2015)
Appendix 13: Moving and Handling Practical Training Record – Induction
Risk Assessors Course …………………….. Location……………………… Assisted Transfers Topic Discussed Principles of normal movement Principles of safe patient handling Unsafe practises
Activities Discussed Demo Practiced Date/Signature
Move patient forward in chair one/two carers
Move patient back in chair with one/ two carers
Sit to stand from chair with one/ two carers
Sit to stand from bed with one/ two carers
Stand to sit to chair with one/ two carers
Stand to sit to bed with one/ two carers
Assisted walking with one/ two carers
Rolling over in bed/floor
Lying to sit edge of bed
Lying to sit in bed
Assist patient to move up bed with one carer
Assist fallen patient from floor
Trainee’s Name……………………. Trainee’s Signature…………………. Trainer’s Name………………….. Trainer’s Signature……………………..

49 of 69 Version 1 (Feb 2015)
Lateral Transfers
Topic Discussed Principles of Safe Patient Handling Unsafe practise
Activities Discussed Demo Practised Date/ Signature
Lateral transfer from bed /chair to chair/commode with minimal assistance
Lateral transfer from bed /chair to chair /commode with one person
Lateral transfer from bed/ chair to chair/ commode with two people
Lateral transfer from bed/ chair to chair/ commode with frame
Lateral transfer from bed/ chair to chair/ commode with stand- turner
Lateral transfer from bed to chair/ commode with stand hoist
Lateral transfer from bed /chair to chair /commode using ceiling track hoist
Lateral transfer from bed / chair to chair/ commode using transfer board
Trainee’s Name ………………… Trainee’s Signature…………………….. Trainer’s Name…………………… Trainer’s Signature …………………….

50 of 69 Version 1 (Feb 2015)
Hoisting
Topics Discussed Principles of Hoist use and types of hoist available. Type, selection and use of slings. Main points of LOLER 1998. Unsafe practise.
Activities Discussed Demo Practised Date and signature
Fitting hoist sling with patient in bed
Fitting hoist sling in bed using slide sheets
Fitting a sling with patient in chair
Fitting sling in chair with sliding sheets
Hoisting from bed / chair to chair/ commode
Hoisting fallen patient from floor
Trainee’s Name ………………….. Trainee’s Signature……………………… Trainer’s Name…………………… Trainer’s Signature……………………….

51 of 69 Version 1 (Feb 2015)
Sliding sheets
Topic Discussed Principles of using sliding sheets Main points of PUWER 1998 Unsafe practise
Activity Discussed Demo Practised Date / Signature
Introduce slide sheets under supine patient
Slide patient. up bed in supine
Slide patient .into side lying from supine
Slide patient from bed to trolley with patslide in supine
Slide patient out of confine space on floor
Remove slide sheets from under patient.
Instruct patient to slide in sitting up the bed
Slide patient from chair to floor(emergency)
Trainee’s Name ………………….. Trainee’s Signature…………………. Trainer’s Name…………………… Trainer’s Signature …………………

52 of 69 Version 1 (Feb 2015)
Inanimate Load Handling& Practical Application of Ergonomics
Topic Discussed
Principle of safer handling of inanimate loads Safer handling inanimate load risk assessment Principle of handling large and awkward loads Awareness of good posture and application of ergonomic principles in the workplace and when driving
Practical Skills
Manoeuvre Discussed Demo Practised Date & Signature
Pushing & Pulling
Lifting & Lowering from floor to waist
level Insert technique used a) b) c)
Carrying object with two people
(State task used)
Appropriate set up of seating at work station
Trainee’s Name ………………….. Trainee’s Signature…………………. Trainer’s Name…………………… Trainer’s Signature …………………

53 of 69 Version 1 (Feb 2015)
Appendix 14
Manual Handling Training Session Patient Handling Refresher Date: Division: Trainer:
N.B. Manual Handling training is a practical subject. During this session you may be asked to participate in
certain practical tasks. If you have any condition that may be aggravated by physical activity, or which may
affect your ability to carry out these tasks safely, please let the instructor know, at the start of the session. If
at any time during the session you are unhappy about a particular task or are unsure of exactly how to carry it
out, please say so before attempting it.
Aims and Objectives
On completion of the course the candidate should be able to:
State the employer/employee’s responsibilities under relevant legislation, Trust policies and procedures
and departmental guidelines.
State the principles of risk assessment and how to apply to the workplace.
State the principles of safer manual handling, correct working posture and how best practice can reduce
risk.
Name Job Title Workplace Signature

54 of 69 Version 1 (Feb 2015)
Equipment Discuss Demo Practice Moving patients Discuss Demo Practice
LINET electric profiling bed Patient mobility assessment
Sliding sheets: Fabric Principles of normal movement
Disposable Sit to stand: assist with 1
Hoists: Passive/hammock assist with 2
Active/raising aid Turn in bed
Small aids: Handling belts Move flat up bed
Sit out of bed
Rotastand Lateral transfer
ARJO Stedy Hoisting: from bed
PatSlide from chair
Scoop stretcher from floor
Bariatric equipment
- location & access -
Falling & fallen patient
‘Talk patient’ up from floor
Other (specify) Transfer collapsed patient to floor
Other (specify)
Comments:
Trainer………………………………………………………………………………………………………
Signature………………………………………………………………………………………………......

55 of 69 Version 1 (Feb 2015)
Appendix 15 South Devon Health Services
Horizon Centre Torbay Hospital
Lawes Bridge Torquay
TQ2 7AA Date as postmark Dear , Ref: Non-Attendance at XXXX It has come to our attention that you are due to attend the above training. Trust policy states that all staff must their mandatory training so we therefore ask that you attend the next possible session for which dates are listed below.
COURSE NAME
**LIST DATES HERE** To book onto one of the above dates please phone the Horizon Centre on 01803 656600, or, alternatively, send an email to [email protected]. We look forward to hearing from you. With best wishes Education & Development Horizon Centre Torbay Hospital Tel: 01803 656600
56 of 69 Version 1 (Feb 2015)
Appendix 16 South Devon Health Services Horizon centre
Torbay Hospital Lawes Bridge
Torquay TQ2 7AA
Date as postmark «AddressBlock» «GreetingLine» Ref: Persistent Non-Attendance at XXXXX. Further to recent correspondence highlighting your non-attendance on the above training, it has been noted that you are yet to book onto an appropriate course. Trust policy states that all staff must attend mandatory training. Consequently, non-attendance is being taken very seriously and may result in a formal course of action or you being prohibited from working any further shifts until the training has been completed. It is your personal responsibility to book and complete the training that your role requires therefore please find available course dates below and book onto the training as a matter of urgency.
TRAINING
***LIST DATES & VENUES*** To book onto one of the above dates please phone the Horizon Centre on 01803 656600, or, alternatively, send an email to [email protected]. With best wishes Education & Development Horizon Centre Torbay Hospital Tel: 01803 656600 Cc: «Budget_Holder» Human Resources
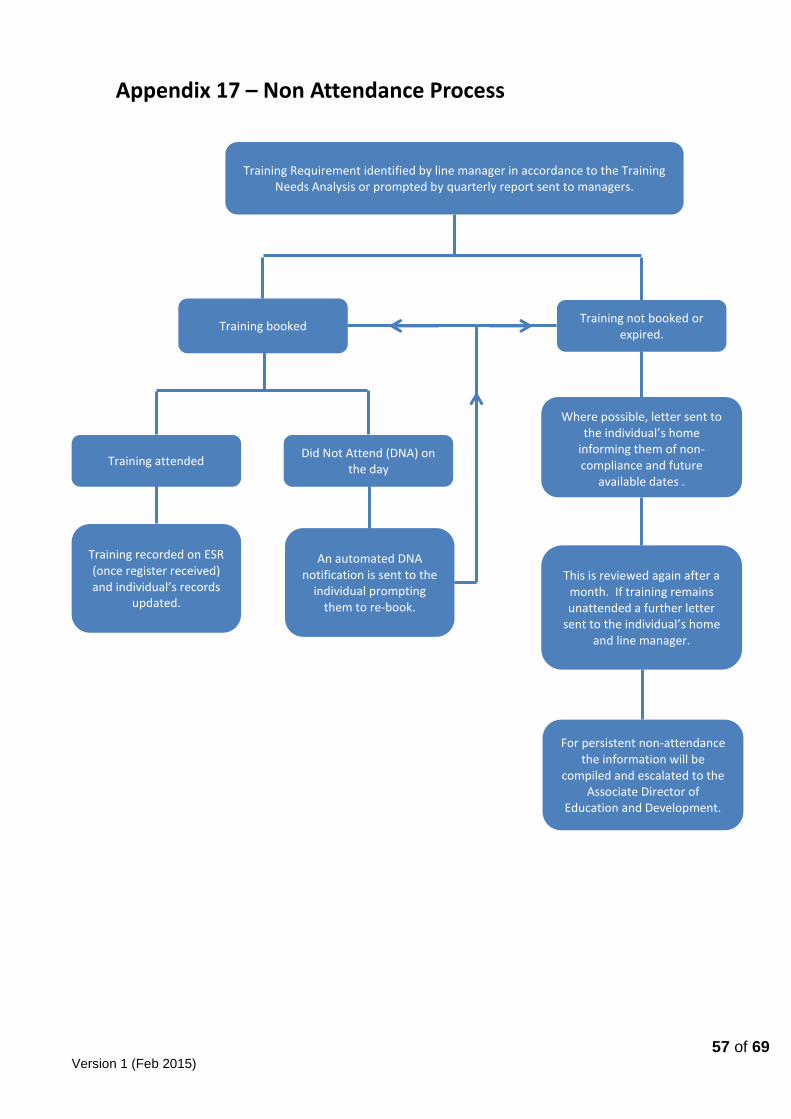
57 of 69 Version 1 (Feb 2015)
Training Requirement identified by line manager in accordance to the Training Needs Analysis or prompted by quarterly report sent to managers.
Training booked Training not booked or
expired.
Where possible, letter sent to the individual’s home
informing them of non-compliance and future
available dates .
This is reviewed again after a month. If training remains unattended a further letter
sent to the individual’s home and line manager.
For persistent non-attendance the information will be
compiled and escalated to the Associate Director of
Education and Development.
Training attended Did Not Attend (DNA) on
the day
An automated DNA notification is sent to the
individual prompting them to re-book.
Training recorded on ESR (once register received) and individual’s records
updated.
Appendix 17 – Non Attendance Process


















