MoveS - Pediatric Rheumatology Society · The antbody reacton occurs in the vascular uvea. Although...
11
MoveS President Dr. Raju Khubchandani Mumbai General Secretary Dr. Priyankar Pal Kolkata Treasurer Dr. Santanu Bhakta Kolkata Immediate Past President Dr. Sujata Sawhney, New Delhi Zonal coordinators North: Dr. Sujata Sawhney New Delhi South: Dr. Nutan Kamath Mangalore West: Dr. Nandini Bhabulkar Nagpur East: Dr. Tapas Sabui Siliguri Towards beer pediatric rheumatology care ...... Editor’s Message April, 2011 Address for correspondence: Dr. Priyankar Pal 2 G, Dilkusha Street, Kolkata-700017 West Bengal email: [email protected] Bulletn of Pediatric Rheumatology Chapter, IAP Message from the Editorial team Dear friends Greetngs from the editorial team We have a packed e newsleer, albeit somewhat delayed. This issue of the newsleer has the following features • Message from the President of the chapter • Secretary’s message • The theme this quarter is “ Uveits and the Paediatric rheumatologist” • Please also find details about the upcoming annual paediatric rheumatology chapter meetng at SGPGI , being conducted by Dr. Amita Agarwal Happy Reading! Dr. Sujata Sawhney and Dr. Rashna Dass April 2011 Contents: 1. Message from President 2. Message from Secretary 3. Uveitis and the Pediatric Rheumatologist Layout & Designed by: David Nongrum, Meghalaya, Shillong: 08794256812
Transcript of MoveS - Pediatric Rheumatology Society · The antbody reacton occurs in the vascular uvea. Although...

MoveS President
Dr. Raju Khubchandani Mumbai
General SecretaryDr. Priyankar Pal
Kolkata
TreasurerDr. Santanu Bhakta
Kolkata
Immediate Past PresidentDr. Sujata Sawhney,
New Delhi
Zonal coordinatorsNorth:
Dr. Sujata SawhneyNew Delhi
South: Dr. Nutan Kamath
Mangalore
West:Dr. Nandini Bhabulkar
Nagpur
East:Dr. Tapas Sabui
Siliguri
Towards better pediatric rheumatology care ......
Editor’s MessageApril, 2011
Address for correspondence:
Dr. Priyankar Pal2 G, Dilkusha Street,
Kolkata-700017West Bengal
email: [email protected]
Bullet n of Pediatric Rheumatology Chapter, IAP
Message from the Editorial team
Dear friends
Greetngs from the editorial team
We have a packed e newsletter, albeit somewhat delayed.This issue of the newsletter has the following features• Message from the President of the chapter• Secretary’s message• The theme this quarter is “ Uveits and the Paediatric rheumatologist”• Please also find details about the upcoming annual paediatric rheumatology chapter meetng at SGPGI , being conducted by Dr. Amita AgarwalHappy Reading!
Dr. Sujata Sawhney and Dr. Rashna DassApril 2011
Contents:
1. Message from President
2. Message from Secretary
3. Uveitis and the Pediatric
Rheumatologist
Layout & Designed by: David Nongrum, Meghalaya, Shillong: 08794256812

Message from the President, RCIAP 2011-2012
In my second innings as President, I inherit a stronger, sturdier, more expanded structure on a firm
base. With the annual conference and CME firmly in place and with an “e” newsletter of high qual-
ity being brought out by the previous team, all the elements are in order.
Fortunately Sujata volunteered to contnue bringing out the e Newsletter easing my tme to plan
other actvites.
There are three principal areas that I wish to focus on in 2011 – 2012. First, an administratve issue- In
2005 the central IAP had written to all its consttuent chapters and branches to apply for and get recognized
as individual enttes (societes) and obtain their own PAN numbers. Though we have been chugging along
without this having happened so far, I believe it is tme to set our house in order. We have set the wheels in
moton and will keep you informed about the developments though this is likely to be a long and arduous
governmental process. As and when we do achieve it, the legitmacy, opening and transferring of bank ac-
counts etc, acceptng money from sponsors etc will all be a breeze. Any of you having questons suggestons
etc about this process please feel free to write in. All democratc principles will be followed.
Secondly, the Pediatric Rheumatology European Society had heard about our Reach and Teach Pro-
gram. They approached me to hold an advanced course on similar lines for pediatric rheumatologists of the
Asia Pacific and have agreed to sponsor the event to the tune of about 50 % of the costs. Tentatvely sched-
uled for Dec 2012, this program would be the anchor event of my tenure.
Thirdly, I am considering putting together a day long training module as an orientaton to rheumatol-
ogy for the general Pediatrician. The main aim of this program would be to give a crash course in fundamen-
tals of Pediatric Rheumatology in the form of a standardized power point presentaton. This module would
be run at various centers on request with several of you serving as trainers. At the moment I am only dream-
ing of this and am in talks with the central IAP to recognize this program and find at least a shoe string budget
for our “orphan” subspeciality.
Please do write in with comments, suggestons etc at [email protected]
Best Wishes
Dr. Raju KhubchandaniPresident, Rheumatology Chapter, IAP
~~~~~~~~~~***~~~~~~~~~~
~i~

Message from the Secretary, RCIAP 2011-2012
Over the years awareness about Pediatric Rheumatology has increased in India. We now have 219
registered members in the chapter. This number is a reflecton of Paediatricians with an interest
in this area.
During my tenure as secretary of the chapter I will focus on three areas:
1. The first priority is to increase the numeric strength of the chapter. I urge you all to motvate your
younger colleagues to join this vibrant and actve chapter where disseminaton of knowledge and
educaton are key priority areas. The life tme membership fees is Rs 2000/- only and this will bring
with it an e newsletter, and informaton about educaton and courses in our field. For details please
contact me at: [email protected]
2. Spread the simple message : “Early diagnosis and appropriate care is the key to best outcome for kids
with rheumatologic problems”
3. The final priority is to get a PAN card for the chapter. This is a must and will be helpful for all future
actvites of the chapter.
It is great that the newsletter of our chapter has gone green, thanks to the team effort of Dr. Sujata
and Dr. Rashna. So please....... if you want to stay connected send me your email Id.
We have a veritable academic feast planned for the year ahead, stay tuned in for regular updates.
Please find in this newsletter informaton about our annual Paediatric Rheumatology conference: Dr. Amita
Agarwal has put together a superb programme. See you in Lucknow, September 2011!
Signing off for now.Best wishes
Dr. Priyankar PalGeneral Secretary, Rheumatology Chapter, IAP
~~~~~~~~~~***~~~~~~~~~~
~ii~

Uveitis and the Paediatric Rheumatologist
~1~
INTRODUCTION As pediatric rheumatologists (PR) you may be called upon to review a child with uveits. The child with uveits is often seen in concert with an ophthalmologist and here the PR has several responsibilites which are: 1. To ensure prompt detecton of uveits 2. To evaluate the child for possible etologic factors 3. To define the associated extra-ocular disease 4. Consider indicatons for introducing advanced immunomodulatory therapies 5. Monitor the efficacy and safety of such treatments.
I will address this topic in the form of simple questons and answers as follows:
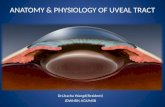
WHY IS UVEAL TRACT INFLAMMATION ASSOCIATED WITH SEVERAL DISEASES? Autoimmune reactons need an antgen –antbody reacton, usually the antgen is unknown but its persistence in the local area is important. Antgens persist in the vitreous as there is relatve stagnaton of the vitreous. In additon the antgens are able to form stable complexes with hyaluronic acid and collagen. This depot effect causes augmentaton and prolongaton of the immune response to antgens deposited in the vitreous. The antbody reacton occurs in the vascular uvea. Although the antgen is processed extraocularly, primed immune cells return to the eye. Antbody producton, in response to intraocular antgens, occurs in the eye, especially in the vascularized uvea. Thus, the producton of antbody occurs locally and memory lymphocytes remain in the uveal tract.
Fig 1: Anatomy of the eye
Dr. Sujata Sawhney. Consultant Pediatric and Adolescent Rheumatologist. M.D.(Pediatrics), M.R.C.P.(U.K.), C.C.S.T (U.K.); GradCertPRheum (Australia)Pediatric Rheumatology Divison, Institute for Child Health, Sir Ganga Ram Hospital, New Delhi - 110060E mail: [email protected]
Dr. Rashna Dass, Assoc. Professor & HeadDeptt. of Pediatric Disciplines, Faculty Room (Rn. 218)North Eastern Indira Gandhi Regional Institute of Health and Medical SciencesPO: Mawdiangdiang, Shillong - 793018Email: [email protected]

WHAT IS THE CLINCIAL APPROACH TO A CHILD WITH UVEITIS? When considering the etology of uveits in a child one has to keep several features of uveits in mind:
1. Intraocular locaton of the inflammatory process :This in turn can be of three types a) Anterior uveits b) Intermediate uveits c) Posterior uveits
2. Course of the disease: this can be acute, chronic or recurrent 3. The characteristcs of the immune process: e.g. the type and distributon of inflammatory cells e.g.
mutton fat Kerattc Precipitates.4. Demographic characteristcs of the patent: The age, sex, extra-ocular features of systemic disease
help guide the PR towards specific aetologies.5. Results of microbiologic studies: separate out the Infectous vs. non infectous causes of uveits.
HOW DO CHILDREN PRESENT?5 to 10% of all uveits occurs in the pediatric populaton. The classic teaching for various presentatons are: 1. Anterior uveits: presents with redness, pain, photophobia.2. Posterior uveits: the predominant complaints are blurring of vision, scotomas and floaters. In children the commonest cause of uveits is Juvenile Idiopathic arthrits. The uveits in JIA is “White eyed disease, no symptoms”
Fig 2: Sites of involvement in Uveitis
WHAT ARE THE COMMON CAUSES OF UVEITIS?The common etologies of pediatric uveits are listed in Fig 3. It is important to remember that the following conditons can masquerade as uveits and are usually detected by the astute ophthalmologist. The masquer-ade syndromes in children are1. Retnoblastoma2. Leukemia3. Lymphoma4. Foreign body5. Juvenile Xanthogranuloma
Site of UveitisAnterior Uveitis:• Irits• Anterior cyclits• Iridocyclits
Refers to inflammaton of the iris and / or pars plicata (anterior ciliary body)
Intermediate Uveitis:• Pars planits• Posterior cyclits• Basal retnochoroidits
Refers to inflammaton of the pars plana (posterior ciliary body) and / or adjacent peripheral retna
Posterior Uveitis:• Focal, multfocal, diffuse choroidits• Chorioretnits• Neuroretnits
Refers to inflammaton involving the cho-roid and / or retna
~2~

Fig 3: Etiologies of uveitis in children
WHAT ARE SIGNS OF UVEITIS? The signs of anterior and posterior uveits are different on eye examinaton. Anterior uveits presents with kerattc precipitates which may be both small and large, cells in the anterior chamber (AC) and flare in the AC. The presence of posterior synechiae suggests past anterior uveits.Posterior uveits on the hand presents as Snowball and Snowbank, Vitrits, Choroidits, Optc Nerve edema and Cystoid macular edema.
HOW SHOULD A CHILD WITH UVEITIS BE INVESTIGATED? No panel can or indeed should be ordered. One has to take into consideraton all the details listed above to decide what tests to run. Some of the commonly ordered tests are
• CBC/ESR/LFT/CALCIUM• ANA• HLA B 27• X-Ray Chest PA• Montoux test• ACE levels• TORCH• VDRL• HIV
Of the several causes of uveits listed in Fig 3, two important ones will be discussed.• JIA• TB
UVEITIS ASSOCIATED WITH JIAIntroductionThough JIA is as common as juvenile diabetes, it is often missed, wrongly labeled as rheumatc fever/TB. Thus many children with JIA who present with monoarthrits will be labeled to have TB of the joint and it is
Common etiologies of Pediatric UveitisAnterior: 44 - 52% Intermediate Posterior• JIA: 50 - 80%• Syphilis• Tubulointersttal nephrits and
uveits syndrome (TINU)• Sarcoidosis
• Idiopathic pars planits: 25%• Tuberculosis• Lyme disease• Sarcoidosis
• Toxocariasis• Toxoplasmosis
P a n u v e i t i s
Remember: The signs of uveitis are detected on slit lamp examination by a skilled ophthalmologist and this may even mean an EUA (examination under anesthesia) if needed
~3~

only when they do not improve after a long trial of ant- tubercular treatment that the penny drops: Incor-rect diagnosis! If such a child had uveits at disease onset, surely after a year of no therapy he would be in big trouble. As per the ILAR classificaton the subcategories of JIA are:
• Oligoarthrits o Persistent o Extended
• Systemic arthrits• Polyarthrits o RF negatve o RF positve
• Enthesits related arthrits (ERA)• Psoriatc arthrits• Other arthrits
The associaton of JIA and uveits is stll not understood properly. It is thought to be related to higher frequency of immunity to retnal S antgen and also to a higher frequency of immunity to low molecular weight iris antgen.
What are the types of uveitis that can occur in a child with JIA?Uveits in JIA is of two types
• Chronic anterior: This occurs most frequently in an ANA positive, young preschool female patent with oligoartcular disease.
• Acute anterior uveits: Classically occurs in an adolescent male, with enthesits, arthrits, inflamma-tory low back pain: ERA. These children are often HLA B 27 positive.
How often should children with uveitis be screened? This depends on the risk stratficaton of a patent with JIA i.e. the chance that the child will develop uveits. For this children with JIA are divided into three groups: low, medium and high risk. The screening recommendatons are listed in Table 1.
Table 1: Monitoring guidelines for identifying new-onset uveitis in juvenile idiopathic arthritis
RISK TYPE ANA AGE AT ONSET DURATION OF DISEASE
HIGH Oligo or poly + ≤ 7 years ≤ 4 years
MODERATE Oligo or polyOligo or poly
+-
any any
> 4 years≤ 4 years
LOWSystemic
Oligo or polyOligo or poly
--
+ or -
any≤ 7 years> years
any> 7 years> 4 years
High RiskModerate RiskLow Risk
Ophthalmologic exam every 3 - 4 monthsOphthalmologic exam every 6 monthsOphthalmologic exam every 12 months
Recommendations for low risk follow-up continue into adulthood
~4~

Can one predict the course /prognosticate about uveitis in a child with JIA?This is an imprecise science. However as a general rule:
• The young onset age, (preschooler) female patent with oligoarthrits and antnuclear antbody posi-tvity is at highest risk of developing uveits.
• The child who has a short duraton between the onset of arthrits and uveits or has uveits onset prior to arthrits onset has a poorer prognosis. In additon severity of uveits at first detecton of ocular disease can also predict disease outcome. Serologically, antbodies to retnal S-antgen and an elevated alpha-2 globulin have a relatvely adverse prognosis.
• Acute uveits in ERA patents that presents with a painful red photophobic eye is usually unilateral, recurrent; however there is usually no ocular residue. Twenty percent ( 20%) adults with AS get this complicaton. Upto 30-35% of children with ERA develop acute uveits.
What are the morphologic features of chronic anterior uveitis in JIA? The chronic anterior uveits in JIA is a non-granulomatous uveits. The choroid (posterior uvea) is rarely affected. It is uncommon for unilateral uveits to become bilateral after one year. The uveits is bilateral in 70%, severity is symmetrical.
Is it is a uniphasic / short duration illness in children? Not usually. In 10% mild disease persists <12 months, 15% have one attack. Up to 50% have moder-ate to severe disease for >4 months. Twenty five percent (25%) have very severe disease and a poor visual outcome.
How are the children usually treated? This depends on the severity of the eye disease with the first line of therapy being topical steroid eye drops (Prednisone acetate 1%, has the ability to cross intact corneal epithelium) and mydriatcs. The therapy is quickly stepped up if the child has persistent actve disease. The various therapies that can be used se-quentally or together are:
• Oral NSAIDs• Oral steroids• IV pulsed solumedrol• Weekly methotrexate• Oral cyclosporine• Ant TNF agents
What are the goals of treatment?The goals of treatment are to
• Prevent phthisis• Prevent surgical complicatons• Prevent complicatons of treatment• Halt inflammaton
Always Remember: The Eye and the joint do not get involved in parallel.
~5~

TB AND THE EYE
Introduction: Tuberculosis of the eye can occur as a hypersensitvity phenomenon or as part of a hematogenous spread from a distant site. It rarely occurs as isolated disease. If the ocular features are suspicious the child should be investgated for TB.
How should the Montoux test be interpreted? The Montoux test also called the tubercular skin test (TST) is a useful guide. A TST of > 20mm / ulcer-atve is usually tubercular disease. If the TST is 10-20 mm: look for systemic disease, if < 10mm, negatve . As TB patents may not be picked up by the TST, the IGRA tests e.g the Quantferon Gold test for TB may be used as an additonal screening tool.
What are the signs of tubercular eye disease? A study of 92 published case reports showed that the most common presentng manifestatons were as shown in Table 2. Most commonly, tuberculous uveits presents as a posterior uveits.
Table 2: Eye manifestations in tuberculosis
Lal and Gupta (1985) studied clinical signs associated with tuberculous uveits and found four signs to be very specific as shown in Table 3.
Common manifestations of tubercular eye disease
Choroidal mass with or withour inflammatory signs 34%
Choroidits / chorioretnits 27%
Vitrits 24%
Iridocyclits / anterior reacton 13%
Panuveits 11%
~6~

Table 3: Specific eye findings in tuberculosis
How are the patients with tubercular uveitis treated? Ant tubercular therapy with topical /oral steroids is the mainstay of treatment.
IN CONCLUSION
JIA associated chronic anterior uveits is the commonest cause of uveits in children. Tuberculous ocular involvement is commonly posterior uveits. Investgatons should be patent appropriate with early aggressive treatment and a low threshold for DMARDS.Team approach is what offers the best outcome for the child.
~~~~~~~~~~***~~~~~~~~~~
Specific signs of tubercular eye disease (Lal & Gupta Afro - Asian J of Ophthalmol, 1985)
Broad - based posterior synechiae 93%
Retnal vasculits without choroidits 97%
Retnal vasculits with choroidits 99%
Serpiginous - like choroidits 98%
~7~

Life Membership Form of “Rheumatology chapter of IAP”(Only for Life Members of Central IAP)
1. Membership No. of central IAP……………...……………………….............................................……………………………..
2. Name:…………………………………………..............................................................…………………………………………………
3. Corresponding Address:………………………………………………………………………………………….....................................
.......................................................................................................................................................................
4. Permanent Address:………………………………........................................…………………………….................................
……………………………………………………..................................................................……………………………………………
5. Phone No (s):……………………..........................…………. Mobile (s):……….........................…………………………………
6. Email (essental):………………………………………….………....................................................…………………………........
7. Professional Attachment:………………………………...................................................…………………………………………
8. Academic Qualificatons:………………………...............................................…….……………………………………….........
9. Date of Birth:………………………………….…..........................................................……………………………………………...
Date: Signature:
Present fees of Life Membership is Rs. 2000/-. To be paid in DD in favour of “IAP Rheumatology Chapter”,
Payable at Kolkata.
Please send it to:Dr. Priyankar Pal, 2 G, Dilkusha Street, Kolkata-700017, West Bengal
The Department of Clinical Immunology, Sanjay Gandhi Postgraduate institute will be organizing the NCPR 2011 from September 3-4, 2011. The session would include CPC, debate, state of the art lecture, interesting case vi-
gnettes etc. The conference will have poster and oral presentation of original research work also. Two workshops are proposed on the pre-conference day: Primer to musculoskeltal ultrasound and Autoantibodies: How to do and
what do they contribute. If you would like anything else to be included please send your suggestions.
For details contact:Dr Amita Aggarwal, Department of Clinical Immunology
Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow [email protected]; [email protected]