
Movement is Improvement: The Therapeutic Effects of ...
26
ORIGINAL RESEARCH Movement is Improvement: The Therapeutic Effects of Exercise and General Physical Activity on Glycemic Control in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials Sayed Z. A. Shah . Jawad A. Karam . Alam Zeb . Rafi Ullah . Arif Shah . Ijaz Ul Haq . Iftikhar Ali . Haider Darain . Hong Chen Received: November 10, 2020 / Accepted: January 15, 2021 / Published online: February 5, 2021 Ó The Author(s) 2021 ABSTRACT Introduction: Exercise is considered a corner- stone in achieving an optimized blood glucose level and reducing body weight, body mass index (BMI), and waist circumference. This study aimed to investigate and quantitatively summarize the literature regarding the thera- peutic effects of exercise and general physical activity on glycemic control. Methods: A systematic review and meta-analy- sis of the literature on the therapeutic effects of exercise on glycemic control in patients with type 2 diabetes mellitus (type 2 DM) were con- ducted using electronic databases. Studies with an exercise intervention lasting more than 8 weeks were included. Both qualitative and quantitative analyses were performed. Qualita- tive data were presented narratively in table form. Quantitative analysis was performed using a random-effects model with a 95% con- fidence interval and a significance level of 0.05. The Physiotherapy Evidence Database (PEDro) scale and the Cochrane Risk of Bias 2 (RoB2) tool were used to assess the quality of evidence and the risk of bias. Results: A total of 21,559 articles were identi- fied through different databases. Out of 21559 studies, only 32 randomized controlled trials were deemed eligible for inclusion in this study. The average exercise session was 45.15 min, while the average follow-up duration was 21.94 weeks. The mean exercise frequency according to our findings was 3.25 days/week. Almost all the studies reported decreases in glycated hemoglobin (HbA1c; P \ 0.0001), fasting blood glucose (P = 0.03), BMI (P = 0.04), and waist circumference (P = 0.007) after the exercise intervention. S. Z. A. Shah Á H. Chen (&) Department of Rehabilitation Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China e-mail: [email protected]; [email protected] J. A. Karam Department of applied exercise science, Concordia University Chicago, 7400 Augusta St., River Forest, IL 60305, United States A. Zeb School of Health Sciences, Peshawar, Pakistan R. Ullah Á A. Shah Á I. U. Haq Á I. Ali Paraplegic Centre, Phase#4, Hayatabad, Peshawar, Pakistan H. Darain Institute of Physical Medicine and Rehabilitation Sciences, Khyber Medical University, Hayatabad, Peshawar, Pakistan H. Chen WHO Collaborating Center for Training and Research in Rehabilitation, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China Diabetes Ther (2021) 12:707–732 https://doi.org/10.1007/s13300-021-01005-1
Transcript of Movement is Improvement: The Therapeutic Effects of ...

ORIGINAL RESEARCH
Movement is Improvement: The Therapeutic Effectsof Exercise and General Physical Activity on GlycemicControl in Patients with Type 2 Diabetes Mellitus:A Systematic Review and Meta-Analysisof Randomized Controlled Trials
Sayed Z. A. Shah . Jawad A. Karam . Alam Zeb . Rafi Ullah .
Arif Shah . Ijaz Ul Haq . Iftikhar Ali . Haider Darain . Hong Chen
Received: November 10, 2020 /Accepted: January 15, 2021 / Published online: February 5, 2021� The Author(s) 2021
ABSTRACT
Introduction: Exercise is considered a corner-stone in achieving an optimized blood glucoselevel and reducing body weight, body massindex (BMI), and waist circumference. Thisstudy aimed to investigate and quantitatively
summarize the literature regarding the thera-peutic effects of exercise and general physicalactivity on glycemic control.Methods: A systematic review and meta-analy-sis of the literature on the therapeutic effects ofexercise on glycemic control in patients withtype 2 diabetes mellitus (type 2 DM) were con-ducted using electronic databases. Studies withan exercise intervention lasting more than8 weeks were included. Both qualitative andquantitative analyses were performed. Qualita-tive data were presented narratively intable form. Quantitative analysis was performedusing a random-effects model with a 95% con-fidence interval and a significance level of 0.05.The Physiotherapy Evidence Database (PEDro)scale and the Cochrane Risk of Bias 2 (RoB2)tool were used to assess the quality of evidenceand the risk of bias.Results: A total of 21,559 articles were identi-fied through different databases. Out of 21559studies, only 32 randomized controlled trialswere deemed eligible for inclusion in this study.The average exercise session was 45.15 min,while the average follow-up duration was21.94 weeks. The mean exercise frequencyaccording to our findings was 3.25 days/week.Almost all the studies reported decreases inglycated hemoglobin (HbA1c; P\ 0.0001),fasting blood glucose (P = 0.03), BMI (P = 0.04),and waist circumference (P = 0.007) after theexercise intervention.
S. Z. A. Shah � H. Chen (&)Department of Rehabilitation Medicine, TongjiHospital, Tongji Medical College, HuazhongUniversity of Science and Technology, Wuhan,People’s Republic of Chinae-mail: [email protected];[email protected]
J. A. KaramDepartment of applied exercise science, ConcordiaUniversity Chicago, 7400 Augusta St., River Forest,IL 60305, United States
A. ZebSchool of Health Sciences, Peshawar, Pakistan
R. Ullah � A. Shah � I. U. Haq � I. AliParaplegic Centre, Phase#4, Hayatabad, Peshawar,Pakistan
H. DarainInstitute of Physical Medicine and RehabilitationSciences, Khyber Medical University, Hayatabad,Peshawar, Pakistan
H. ChenWHO Collaborating Center for Training andResearch in Rehabilitation, Tongji Hospital, TongjiMedical College, Huazhong University of Scienceand Technology, Wuhan, People’s Republic ofChina
Diabetes Ther (2021) 12:707–732
https://doi.org/10.1007/s13300-021-01005-1

Conclusion: Exercise plays an important role inoptimizing glycemic control and improvingquality of life (QoL), BMI, and waist circumfer-ence in type 2 DM patients. Exercise could be asafe adjunct therapy to medical treatments inthese patients.Registration: PROSPERO: CRD42020210816
Keywords: Diabetes mellitus, type 2; Exercise;Fasting blood glucose; Glycated hemoglobin;Meta-analysis; Physical activity; Systematicreview
Key Summary Points
Why carry out this study?
Exercise is considered a cornerstone in type 2DM management, but diabetes patients areincreasingly likely to lead a sedentarylifestyle.
This study investigated the effects ofdifferent exercise regimens on glycemiccontrol, anthropometric parameters, andquality of life for type 2 DM patients.
What was learned from the study?
Exercise significantly affects glycemiccontrol, induces beneficial anthropometricchanges, and enhances quality of life.
General physical activity and walking areconsidered low-impact activities, but theycan still benefit type 2 DM patients.
DIGITAL FEATURES
This article is published with digital features,including a summary slide, to facilitate under-standing of the article. To view digital featuresfor this article go to https://doi.org/10.6084/m9.figshare.13574684.
INTRODUCTION
Diabetes mellitus (DM), a very common medi-cal condition, is associated with decreased
production of insulin or an inability of the bodyto utilize it properly (types 1 and 2 DM,respectively) [1]. Type 2 DM is the most preva-lent form of diabetes, accounting for nearly90% of all cases of diabetes [2, 3]. According tostatistics from the International Diabetes Fed-eration (IDF), the estimated combined globalprevalence of type 1 and type 2 DM, bothdiagnosed and undiagnosed, was 463.0 millionadults aged 20–79 years in 2019. Based on this2019 estimation, a prevalence of 578.4 millionis projected by the year 2030, and if the presenttrend continues, 700.2 million adults aged20–79 years will be diabetic by 2045 [4]. Thereason behind this escalation of the prevalenceof diabetes could be sedentary lifestyles,increasing levels of obesity, aging populations,and diets that are high in calories and fat [5].
Body mass index (BMI) and waist hip ratio(WHR) are independent risk factors for type 2DM [6]. In developed countries, diabetes mostlyoccurs in the elderly, while in developingcountries, diabetes mostly affects people aged34–65 years [7]. It is often reported that a highproportion of patients with diabetes performonly a small amount of physical activity,including structured exercises [3]. Type 2 DM isa major cause of premature morbidity andmortality associated with cardiovascular disor-ders, kidney diseases, neuropathies, retinopa-thy, and amputation [5]. Along with othercomplications, diabetic patients may also sufferfrom depression, anxiety, denial, worries, andfrustration [1]. Poor health management ser-vices and a lack of awareness of diabetes canincrease diabetes-related mortality [8]. Diabetesmellitus has increased the socioeconomic bur-den on developing countries [9], and is consid-ered to be a prime reason for increasinghealthcare costs worldwide [10]. Diabetes drugsare expensive, and most patients fail to gethigh-quality treatment due to the expensivenature of the treatment, the poor allocation offunds for healthcare, and the lack of medicalreimbursement in developing countries [11].
Studies have shown that regular exercise candelay diabetes and associated complications,but it has been observed that most diabeticpatients are inactive. Generally speaking, dia-betic patients can attain a controlled level of
708 Diabetes Ther (2021) 12:707–732

blood sugar by adopting a healthy nutritionalplan, exercising regularly, and reducing bodyweight, although some may need to useexogenous insulin [12].
According to Gabriel and Zierath [13], theacute effects of exercise include enhanced glu-cose metabolism and improved insulin sensi-tivity. Blood glucose was found to be animportant substrate in the skeletal muscle oxi-dation process during strenuous exercise, andexercising increases glucose utilization withoutaffecting blood insulin levels. Exercise alsoincreases certain protein levels that are impor-tant for glucose homeostasis. The increase inthe level of glucose transporter type 4 protein(GLUT4) induced by exercise training enhancesskeletal muscle glucose uptake. This strategycould regulate blood glucose levels in the case ofinsulin resistance. Gabriel and Zierath alsonoted that performing exercise training forlonger increases the aerobic threshold and theconcentration of mitochondria in skeletalmuscles [13]. Exercise has long been consideredthe cornerstone of diabetes mellitus manage-ment, along with diet adjustment and drugtreatment. Aerobic exercise, which consists ofexercising large groups of muscles in a rhyth-mic, repeated, and continuous manner for atleast 10 min, is used in diabetes management.In strenuous short-duration exercise, musclesmainly use energy from the glycogen stores, butthe muscle glycogen stores are gradually deple-ted during long-duration exercise, so energy ismainly provided by glucose and free fatty acidsfrom adipose tissues [13, 14]. High-intensityexercise consumes glucose at a higher rate thanit is produced by the liver, so the blood sugarlevel drops [14]. It has been proven that exerciseincreases the sensitivity of muscle cells toinsulin and increases the activity of oxidativeenzymes [5]. Moreover, the overall effects ofexercise on carbohydrate metabolism are asso-ciated with improved insulin sensitivity [15].
The results of a randomized controlled trialof adults with type 2 diabetes that explored thebenefits of aerobic or resistance training aloneor combined indicated that both types of exer-cise training alone improved glycemic control,but the improvement was greatest with com-bined resistance and aerobic training [16].
The increase in glucose uptake by skeletalmuscles, enhanced insulin sensitivity, andimproved oxidative enzyme activity during exer-cise are the rationale for incorporating exercise asa therapeutic adjunct into the management oftype 2 DM. The purpose of this systematic reviewand meta-analysis was to investigate and quanti-tatively summarize the literature regarding thetherapeutic effects of exercise and general physi-cal activity on glycemic control, exercise-associ-ated anthropometric changes, and the quality oflife of type 2 DM patients.
METHODS
A systematic review and meta-analysis of ran-domized controlled trials was conductedaccording to the Preferred Reporting Items forSystematic Reviews and Meta-Analyses(PRISMA) 2009 guidelines [17]. This study wasregistered with PROSPERO (registration ID:CRD42020210816).
Study Objective
To explore and quantitatively summarize theliterature regarding the therapeutic effects ofexercise and general physical activity on gly-cemic control, exercise-associated anthropo-metric changes, and quality of life of type 2 DMpatients.
Study Question
Do exercise and general physical activity havebeneficial therapeutic effects on the glycemiccontrol, anthropometric parameters, and qual-ity of life of type 2 DM patients?
PICO
P (Population): Type 2 DM patientsI (Intervention): Exercise and general physical
activity or combinations of exercise with othertherapies
C (Comparison): Nonexercise/standard treat-ment/placebo, or different exercise regimengroups of type 2 DM patients
Diabetes Ther (2021) 12:707–732 709

O (Outcomes): HbA1c, fasting blood glucose(FBG), quality of life (QOL), BMI, weight, waistcircumference.
Search Strategy
The electronic databases AMED, Embase, HMIC,BNI, MEDLINE, PsycInfo, CINAHL, HEALTHBUSINESS, PubMed, Web of Science (WoS), andEBSCO were used to conduct a systematic liter-ature search. The limits applied were publica-tion year (2011–2020), English language studies,and human studies. Another method of identi-fying relevant studies was to screen the refer-ence lists of studies retrieved from thedatabases. We included studies up to the year2000 identified through screening the referencelists of the studies retrieved from the databases.A search alert was created for Web of Scienceand EBSCO to retrieve recently published stud-ies. The following keywords and MeSH termswere identified for every database individuallyand used during the searches: ‘‘physical activ-ity,’’ ‘‘exercise,’’ ‘‘diabetes mellitus,’’ ‘‘type 2.’’Another method of identifying relevant studieswas to screen the reference lists of the studiesretrieved from the databases.
Study Selection
Inclusion and Exclusion CriteriaThe study inclusion criteria were as follows: (1)randomized controlled trials (RCTs) that stud-ied the effects of exercise on glycemic control inpatients with type 2 DM and had a follow-upperiod of C 8 weeks; (2) participants of any ageand gender; and (3) quantitative measurementof glycemic control or anthropometric changes.The following studies were excluded: studieswith a diabetes mellitus type 1 population,single-arm studies, animal studies, ex vivo/in vitro studies, review studies, retrospectivestudies, and case studies.
Types of InterventionExercise, walking, or general physical activitycompared with the nonexercise control groupor the use of other treatments or exerciseinterventions. Studies combining other
therapies with exercise, walking, or physicalactivity were also included.
Types of ParticipantsStudies with type 2 DM patients were included;studies where all subjects were only at risk ofdiabetes were excluded.
Types of Outcome MeasuresThe primary study variable was HbA1c, andsecondary outcomes were FBG, QOL, BMI,bodyweight, and waist circumference.
Study Selection Process
The study selection process comprised threescreening phases: study title screening, abstractscreening, and, finally, full-text screening.There were two independent reviewers at eachscreening phase. The corresponding authorresolved any conflicts or disagreements betweenthe two reviewers. The search results wereuploaded to Rayyan QCRI (https://www.rayyan.qcri.org: Data Analytics, Qatar ComputingResearch Institute) for citation screening by twoindependent reviewers [18]. After screening thetitles, the abstracts of the selected titles werescreened. Finally, the full texts of the selectedstudies were screened in detail for relevancy.
Study Quality and Risk of Bias Assessment
Data extracted for external validity and report-ing quality assessment included study ID (firstauthor’s name along with the year and refer-ence), study design characteristics (data regard-ing experimental design and study groups,number of participants per group), participantdetails, intervention (types of exercise, inten-sity, frequency, and follow-up), control (controltype and control intervention details), primaryand secondary outcome measures, and infor-mation regarding adverse events.
The Physiotherapy Evidence Database(PEDro) scale was used for study quality assess-ment [19]. Two independent reviewers per-formed the study quality evaluation; anyconflicts/disagreements were resolved by com-paring the recorded data and through
710 Diabetes Ther (2021) 12:707–732

discussion with the corresponding author. ThePEDro scale has 11 quality assessment items (yesor no), of which 10 are used to calculate thefinal PEDro score (0–10). Sackett’s levels of evi-dence were used to simplify the study qualitylevels, and a study was considered to be level 1(higher quality) if it scored C 6 on the PEDroscale and level 2 if it scored\6 [20].
The risk of study bias was assessed by twoindependent reviewers using the Cochrane riskof bias (RoB 2) tool [21]. Every study was ratedwith the RoB 2 tool for selection bias, detectionbias, performance bias, outcome assessment,incomplete data, outcome reporting, and otherthreats to study validity identified by tworeviewers. The risk of bias was categorized aseither a low risk of bias (the domain was con-sidered adequate), a high risk of bias (thedomain was considered inadequate), or anunclear risk of bias (not enough information tomake a judgment about the bias). The RoB 2Excel tool was filled for individual studies, andthe results were entered into Cochrane ReviewManager 5.3 [22].
Data Extraction
For the study of primary and secondary vari-ables, postintervention means and standarddeviations (SD) as well as sample size detailswere retrieved by two independent reviewers.Any conflicts/disagreements were resolvedthrough discussion with the correspondingauthor and by comparing the recorded data.The Microsoft data extraction form includedthe following details of the included studies:study design, population details, target vari-ables, interventional procedures (study groups,exercise type, volume, and intensities), andstudy findings. The authors prepiloted the dataextraction form in some studies. Data wereextracted from the texts, tables, and figures ofthe included studies.
Data Synthesis
We performed both qualitative and quantitativeanalyses. The data extracted were summarizedin table form to effectively present the
characteristics and results of the included stud-ies. To study the primary and secondary vari-ables, a meta-analysis was performed using arandom-effects model.
Meta-Analysis
Quantitative analysis was performed for thestudy’s primary outcome measure (HbA1c) andthe secondary outcome measures (FBGs, BMI,weight, and waist circumference). The meansand standard deviations of outcomes from theexercise and control groups were comparedusing mean differences and a random-effectsmodel with a 95% confidence interval. The timepoints for data extraction regarding the primaryand secondary variables were not specified, butwe preferred time points of 8 weeks and above.For some studies where the standard deviations(SD) were not provided, we calculated SDs withan online calculator using the formula providedby Hozo et al. [23].
Effect sizes of 0.2, 0.5, and 0.8 were consid-ered small, moderate, and large, respectively[24]. I2 and the chi-square test were used toevaluate heterogeneity among the studies. Weconsidered an I2 value of 25% to indicate lowheterogeneity, 50% to represent moderateheterogeneity, and 75% to indicate highheterogeneity [25]. All the analyses were per-formed in Cochrane Review Manager 5.3 [22],and p\0.05 was taken to indicate statisticalsignificance.
Compliance with Ethics Guidelines
This study is based on previous studies; theauthors did not perform any clinical or pre-clinical experiment involving humans oranimals.
RESULTS
Study Selection
The research databases AMED, Embase, HMIC,BNI, MEDLINE, PsycInfo, CINAHL, HEALTHBUSINESS, PubMed, Web of Science (WoS), and
Diabetes Ther (2021) 12:707–732 711

EBSCO were used to conduct a systematic liter-ature search. The search retrieved 21,559 arti-cles. A total of 32 articles were also identifiedfrom the reference lists of other studies. 1448duplicates were identified using Rayyan QCRIand EndNote. Title and abstract screening bytwo independent reviewers resulted in theexclusion of a further 20,063 studies. Eightyarticles were deemed eligible for full-textscreening, while 48 were excluded for particularreasons. Finally, 32 articles were eligible forinclusion in the systematic review, and 26 inthe meta-analysis (see the PRISMA flow diagramin Fig. 1).
Study Characteristics
The average age calculated from 26 studies was57.36 years. Two studies recruited participantsin the age ranges 30–80 years [26] and 40–65years [27], respectively; another recruitedelderly patients above 50 years [28]. The averageexercise session was 45.15 min, while the aver-age follow-up duration was 21.94 weeks. Themean exercise frequency according to our find-ings was 3.25 days/week.
For all studies, the study population com-prised type 2 DM patients. Depending on thestudy, the participants were also obese [29],hypertensive [30], adults with coronary artery
Fig. 1 PRISMA flow diagram depicting the study selection process
712 Diabetes Ther (2021) 12:707–732

disease (CAD) [31], or newly diagnosed type 2DM patients [32], had received their diagnosis5–8 months earlier [26] or\5 years earlier [33],or were female participants only [34], sedentarypatients with 5 years of diagnosis [35], elderlypatients with peripheral neuropathy [28], oroverweight, dysregulated, and sedentarypatients [36]. Most of the studies recruited par-ticipants with HbA1c levels of 6.4–7.0[26, 30, 32, 37–44], followed by levels of C 6.5[27, 45, 46], 7.0–10.0 [34], 7.2–9.0 [28, 31,33, 47], 10.0–11.0 [48, 49], or 7.0–11.0 [36].
A variety of exercise interventions were uti-lized in the studies, but aerobic training (12studies) [27, 28, 30, 32, 39, 41, 44, 45, 49–52]and resistance training (RT) (14 studies)[27, 31, 36, 39–41, 44, 45, 47, 48, 52–55] werethe most common. More specifically, the exer-cises used in the studies were as follows: aerobicexercises: moderate-intensity continuous (MIC)training [30, 32], supervised structured aerobicexercise training (SSAET) [51]; anaerobic train-ing: 5 studies [32, 37, 55–57], high-intensityinterval training (HIIT) [30, 32, 37, 56], sprintinterval training (SIT) [32]; resistance training(RT): biodensity resistance exercise [40], pro-gressive resistance training (PRT) [53, 54];endurance training: 1 study [37]; combinedexercise training: combined exercise regimen[38, 44, 45, 47]; walking: [29, 31, 39, 43, 45, 46];general physical activity: [26, 31, 33, 42, 44];nonlocomotive physical activity [42]; yoga:[34, 43]; and nonspecific exercises [35].
The common outcome measures used bymost of the studies were as follows: HbA1c (allstudies), FBG (20 studies) [26–29, 32, 35–37,40, 42–44, 47, 48, 50–52, 56–58], BMI (17studies) [27, 29, 30, 34–38, 44, 45, 48, 50,51, 54–57], bodyweight (13 studies)[26, 27, 31, 33, 35, 36, 42, 44, 45, 48, 54, 56, 57],waist circumference (11 studies) [26, 29, 33,35, 41, 44, 45, 47, 48, 53, 54, 56], and QoL (5studies) [33, 36, 43, 48, 54].
The durations of interventions reported bythe included studies were as follows: 8–12 weeks[27, 28, 30, 35, 37, 38, 42, 43, 48, 55–57], 16–-25 weeks [36, 37, 44, 50, 51, 53], and 6 months
to 1 year [26, 29, 31, 39–41, 46, 52]. Three daysper week (3d/wk) [30, 32, 35–38, 41, 45–48,51, 53–55, 57] was the most common exercisefrequency, followed by 5d/wk, [39, 50, 56], 1d/wk [59], and 2d/wk [31, 34, 43], daily [29], 7visits/3 month [44], and 1d/5 weeks [44]. Mostof the studies were consistent in the duration ofan exercise session: 5–10 min [40], 20–45 min[30, 32, 35, 37, 38, 44, 47, 49, 50], 45–60 min[27, 31, 34, 36, 39, 43, 51, 55, 56], 270 min/wk[41], or 150 min/wk [33, 45, 52].
Progression and increasing intensity ofexercise were reported by 12 studies as follows:based on an increasing number of steps at eachvisit [29]; based on monitoring body weight andmaximum oxygen uptake (VO2 max) everythree months, progression from 70% to 80%HRR was observed [47]; based on increasedexercise intensity with every session [32]; basedon increasing the mean treadmill grade andMETs progressively [41]; based on a progressiveincrease in resistance [53, 56]; based on anindividualized elevation of exercise intensity(14–16 on the Borg scale) at week 12 [48]; basedon a 30-min increase in each phase of a five-phase program [51]; based on increasing non-locomotive physical activity [42]; based onprogression in the completion of 12 repetitionsduring the final set of exercises in two consec-utive sessions [45]; and based on the progres-sion of low-volume HIIT to high-volume HIITover 6–12 weeks [55]. A detailed description ofthe study characteristics is available in Table 1.
Study Quality and Risk of Bias
The selection, performance, and detection bia-ses were similar for most of the studies (Fig. 2,3). The quality and level of evidence of eachstudy are summarized in Table 2. The majority(26) of the studies were of high quality (level 1),but 6 studies were of lower quality (level 2)[33, 39, 42, 44, 45, 57].
Diabetes Ther (2021) 12:707–732 713

Table
1Characteristics
ofthestudiesincluded
inthisreview
Stud
y
no.
Reference
Participant
inform
ation
Group
sExercise
frequency/du
ration
/
volume/intensity/mod
e
Progression
Adverse
events
Pvaluea
Con
clusion
1Abdelbasset
etal.(2020)
[30]
Samplesize
=48
G1n=16,G
2n=16,
G3n=16
Sex:M
=27,F
=21
Age
=40–6
0years
G1.
MIC
G2.
HIIT
G3.
Control
40min
exercise
3times/
weekfor8weeks
Not
reported
Not
reported
\0.05
BothMIC
andHIIT
groups
show
eda
significant
decrease
in
BMI,IH
TG,visceral
lipids,ALT,H
bA1c,
andlipid
profile
2Brinkmann
etal.(2019)
[38]
Samplesize
=30
G1n=15,G
2n=15
Sex:M
=19,F
=11
Age
=60
±8years
G1.
Trainingin
the
overnight-fasted
state
G2.
Trainingin
thefed
state
30min
combined
endurance/strength
training
program
3
times/w
eekfor
8weeks
Not
reported
Not
reported
0.001
Exercisingin
either
the
fasted
orfedstate
resultedin
improvem
entsin
the
subjects’p
hysical
fitness,b
ody
composition,glucose,
andfastingtriglyceride
values
3Dasguptaet
al.
(2017)
[29]
Samplesize
=347
G1n=174,G2n
=173
Sex:M
=157,
F=190
Age
=60
±11
years
G1.3000
steps/dayover
a
year
G2.30–6
0min
ofactivity
daily
3000
steps/dayover
1year,3
0–60
min
of
activity
daily
Num
berof
steps
increased
witheach
visit
Not
reported
\0.05
HBA1c
andinsulin
sensitivitysignificantly
improved
4Magalhaesetal.
(2019)
[47]
Samplesize
=80
G1n=28,G
2n=25,
G3n=27
Sex:M
=38,F
=42
Age
=58.5
±7.7years
G1.
MCT
withRT
G2.
HIITwithRT
G3.
Control
group
5.0±
7.1min
MCT
group,33.1
±6.4min
HIITgroup3times/
wk
Exercisesessions
were
upgraded
every
3monthsfor
VO2max
Not
reported
[0.05
Nosignificant
effectson
glycem
iccontrolwere
reported,b
utthe
combination
ofMCT
withRTim
proved
body
composition
and
CRF
714 Diabetes Ther (2021) 12:707–732

Table
1continued
Stud
y
no.
Reference
Participant
inform
ation
Group
sExercise
frequency/du
ration
/
volume/intensity/mod
e
Progression
Adverse
events
Pvaluea
Con
clusion
5Vanroyet
al.
(2017)
[39]
Samplesize
=48,
G1n
=27,G
2n
=21
Sex:M
=27,F
=21
Age
=59.4
±8.2years
G1.
IC
G2.
CC
60min
walking,aerobic
andstrength
training
for8weeks
Not
reported
Not
reported
\0.05
HbA
1clevelsdecreased
significantly
6Winding
etal.
(2018)
[37]
Samplesize
=32
G1n=12,G
2n=13,
G3n=7
Sex:M
=19,F
=13
Age
=58
±8years
G1.
END
G2.
HIIT
G3.
Control
group
40min
END
or20
min
HIIT,3
days/w
k
Not
reported
Not
reported
\0.05
Fastingglucose,HbA
1c
levels,
andglycem
ic
variability
werereduced
intheHIITgroup
7Halvariet
al.
(2017)
[31]
Samplesize
=108
G1n=57,G
2n=51
Sex:M
=88,F
=20
Age
=63.1
±7.9years
G1.
Physicalactivity
G2.
Non-physicalactivity
60min
walking,
swim
ming,bicycling,
resistance
training
for
2days/w
k
Not
reported
Not
reported
0.001
Physicalactivity
intervention
was
effectivein
decreasing
glucoselevelsrelative
to
anon-PA
controlgroup
8Hangpinget
al.
(2019)
[40]
Samplesize
=300
G1n=200,
G2n=100
Sex:M
=122,
F=178
Age
=50–7
0Years
G1.
BioDensity
resistance
exercise
G2.
Control
group
5-10
min
for1day/wk
Not
reported
Not
reported
\0.05
BioDensity
resistance
training
device
lowered
fastingplasmaglucose
andHbA
1c
9Heiskanen
etal.(2017)
[32]
Samplesize
=26
G1n=13,G
2n=13
Sex:M
=16,F
=10
Age
=40–5
5Years
G1.
SIT
G2.
MIC
T
6sessions
in2weeks,
SIT:4–
69
30sof
all-o
utcycling,MIC
T:
40–6
0min
atthe
intensityof
60%
of
peak
workload
Boutsand
duration
were
increased
witheach
session
Not
reported
0.002
Fastingglucose,insulin
,
and2hglucose
remainedun
altered,but
HbA
1cdecreasedafter
training
Diabetes Ther (2021) 12:707–732 715
Table
1continued
Stud
y
no.
Reference
Participant
inform
ation
Group
sExercise
frequency/du
ration
/
volume/intensity/mod
e
Progression
Adverse
events
Pvaluea
Con
clusion
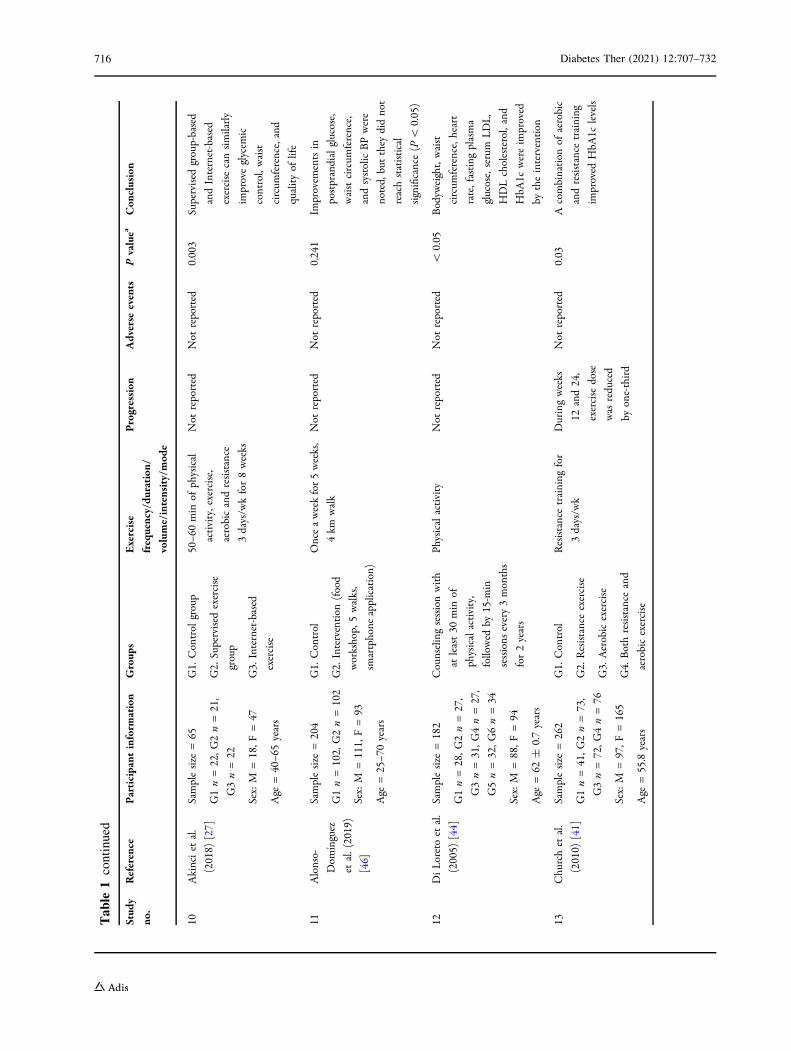
10Akinciet
al.
(2018)
[27]
Samplesize
=65
G1n=22,G
2n=21,
G3n=22
Sex:M
=18,F
=47
Age
=40–6
5years
G1.
Control
group
G2.
Supervised
exercise
group
G3.
Internet-based
exercise
50–6
0min
ofphysical
activity,exercise,
aerobicandresistance
3days/w
kfor8weeks
Not
reported
Not
reported
0.003
Supervised
group-based
andInternet-based
exercise
cansimilarly
improveglycem
ic
control,waist
circum
ference,and
qualityof
life
11Alonso-
Dom
ınguez
etal.(2019)
[46]
Samplesize
=204
G1n=102,
G2n=102
Sex:M
=111,
F=93
Age
=25–7
0years
G1.
Control
G2.
Intervention
(food
workshop,
5walks,
smartphone
application)
Onceaweekfor5weeks,
4km
walk
Not
reported
Not
reported
0.241
Improvem
entsin
postprandialglucose,
waistcircum
ference,
andsystolicBPwere
noted,
butthey
didnot
reachstatistical
significance(P
\0.05)
12DiLoretoet
al.
(2005)
[44]
Samplesize
=182
G1n=28,G
2n=27,
G3n=31,G
4n=27,
G5n=32,G
6n=34
Sex:M
=88,F
=94
Age
=62
±0.7years
Counselingsessionwith
atleast30
min
of
physicalactivity,
followed
by15-m
in
sessions
every3months
for2years
Physicalactivity
Not
reported
Not
reported
\0.05
Bodyw
eight,waist
circum
ference,heart
rate,fasting
plasma
glucose,serum
LDL,
HDLcholesterol,and
HbA
1cwereim
proved
bytheintervention
13Churchet
al.
(2010)
[ 41]
Samplesize
=262
G1n=41,G
2n=73,
G3n=72,G
4n=76
Sex:M
=97,F
=165
Age
=55.8
years
G1.
Control
G2.
Resistanceexercise
G3.
Aerobicexercise
G4.
Bothresistance
and
aerobicexercise
Resistancetraining
for
3days/w
k
Duringweeks
12and24,
exercise
dose
was
reduced
byone-third
Not
reported
0.03
Acombination
ofaerobic
andresistance
training
improved
HbA
1clevels
716 Diabetes Ther (2021) 12:707–732

Table
1continued
Stud
y
no.
Reference
Participant
inform
ation
Group
sExercise
frequency/du
ration
/
volume/intensity/mod
e
Progression
Adverse
events
Pvaluea
Con
clusion
14Balducciet
al.
(2012)
[52]
Samplesize
=606
G1n=303,
G2n=303
Sex:M
=351,
F=254
Age
=58.8years
G1. Exercise?
coun
selling
group
G2.
Counsellin
galone
Exercise150min/w
kin
2sessions
ofmixed
aerobicandresistance
Not
reported
Not
reported
0.002
Physicalactivity
improved
HbA
1c,B
MI,andwaist
circum
ferencein
subjectswithtype
2
diabetes
15Castaneda
etal.
(2002)
[53]
Samplesize
=62
G1n=31,G
2n
=31
Sex:M
=22,F
=40
Age
=66
±8years
G1.
PRT(progressive
resistance
training)
G2.
Control
group
45min
sessionfor
3days/w
k
Not
reported
3incidentsof
chestpain
in
subjectswith
CAD
\0.05
PRTwas
effectiveat
improvingglycem
ic
controland
someof
the
abnorm
alitiesassociated
withmetabolic
synd
romein
type
2
diabetes
adults
16Earnestet
al.
(2014)
[45]
Samplesize
=262
G1n=41,G
2n=72,
G3n=73,G
4n=76
Sex:M
=97,F
=165
Age
=30–7
5years
G1.Control
G2.
Aerobic
G3.
Resistancetraining
G4.
Aerobic?
resistance
training
Treadmill
for3–
5days/
wk,
10–1
2repetitions;
AER?
RES=2
sessions
ofRES/wk,
10–1
2repetitions
Not
reported
Not
reported
\0.02
Aerobicandaerobicplus
resistance
training
significantlyim
proved
metabolicsynd
rome
scores
inpatientswith
T2D
M
17And
rewset
al.
(2011)
[26]
Samplesize
=593
G1n=99,G
2n=248,
G3n=246
Sex:M
=385,
F=208
Age
=30–8
0years
G1.
Control
G2.
Intensivedietary
support
G3.
Intensivedietary
supportandactivity
30min
briskwalk
5days/w
k
Increasedover
5weeks
then
maintained
Not
reported
0�013
Anintensivediet
intervention
soon
after
diagnosisim
proved
glyaem
iccontrol;the
addition
ofan
activity
intervention
conferred
noadditionalbenefit
18Cox
etal.
(2016)
[33]
Samplesize
=47
G1n=21,G
2n=18
Sex:M
=18,F
=21
Age
=24–8
0years
G1.
Routine
care
G2.
GEM
intervention
Routine
activitiesof
daily
livingandfood
choices
Not
reported
Not
reported
0.01
GEM
intervention
ledto
significant
improvem
entsin
HbA
1c
Diabetes Ther (2021) 12:707–732 717

Table
1continued
Stud
y
no.
Reference
Participant
inform
ation
Group
sExercise
frequency/du
ration
/
volume/intensity/mod
e
Progression
Adverse
events
Pvaluea
Con
clusion
19Hem
mati
(2017)
[60]
Samplesize
=90
G1n=30,G
2n=30,
G3n
=30
Sex:M
=51,F
=39
Age
=50.6
years
G1.
FTF
G2.
TEG
G3.
CTG
30min
ofmoderate-to-
vigorous
intensity
aerobicexercise
Initially
twice/month
then
once/m
onth
for2months
Not
reported
0.21
Improvem
entsin
BMI,
HbA
1c,F
BS,
cholesterol,and
triglyceride
werenoted,
butwerenot
statistically
significant
20Hsieh
etal.
(2018)
[48]
Samplesize
=30
G1n=15,G
2n=15
Sex:M
=11,F
=19
Age
=35–6
5years
G1.
RTA
G2.
CG
RT
2times/w
k,walking
orcycling(60–
80%
aerobiccapacity)5
times/w
k
Not
reported
Not
reported
0.407
Supervised
RTexercises
improved
waist
circum
ference,fasting
glucoselevels,
andpeak
diastolic
bloodpressure;
nosignificant
changes
inoverallQoL
21Miyam
otoetal.
(2017)
[42]
Samplesize
=32
G1n=10,G
2n=12,
G3n=10
Age
=60.0
±3.1years
G1.
LPA
G2.
NLPA
G3.
Control
group
Weartriaxial
accelerometer
and
increaseLPA
byverbal
instructionfrom
PT
for12
weeks
Not
reported
Not
reported
0.684
There
weremarked
improvem
entsin
both
HbA
1candinsulin
sensitivity
22Mensberget
al.
(2016)
[36]
Samplesize
=34
G1n=18,G
2n=16
Sex:F=10,M
=24
Age
=56.5
years
G1.
GLP-1R
A
G2.
Placebogroup(PG)
Supervisespinning
and
resistance
exercises1h
3times/w
kfor16
weeks
Not
reported
Not
reported
\0.001
Acombination
of
supervised
exercise
training
andliraglutide
inducedmajor
improvem
entsin
glycem
iccontrol
718 Diabetes Ther (2021) 12:707–732

Table
1continued
Stud
y
no.
Reference
Participant
inform
ation
Group
sExercise
frequency/du
ration
/
volume/intensity/mod
e
Progression
Adverse
events
Pvaluea
Con
clusion
23Jibril(2017)
[35]
Samplesize
=60
G1n=30,G
2n=30
Sex:M
=28,F
=32
Age
=65.3
±8years
G1.
RE
G2.
CG
REfor12
weeks
of
20min
REthrice
or
threetimes/w
k
Not
reported
Not
reported
[0.05
The
PAintervention
asa
wholedidnotproduce
theexpected
effectsin
patientswithT2D
M,
buttimeeffectssuggest
that
certainaspectsare
effective
24Shakil-ur-
Rehman
etal.(2018)
[51]
Samplesize
=102
G1n=51
G2n=51
Sex:M
=55,F
=47
Age
=58
±8years
G1.
SSAET
G2.
CG
25weeks
ofSSAET
exercises,routine
medication,
and
dietaryplan
Not
reported
Not
reported
P\
0.05
SSAETwas
equally
effective,irrespective
of
gend
er,ascomparedto
thenonexercisecontrol
groupin
T2D
M
patients
25Sreedeviet
al.
(2017)
[34]
Samplesize
=124
G1n=41,G
2n=42,
G3n=41
Age
=30–6
5years
G1.
YG
G2.
PIG
G3.
CG
Yogafor60
min
2days/
wk,peer
mentorship
of13–1
4T2D
M
patientswith45-to
60-m
ineducational
classon
diabetes/w
k
Not
reported
Not
reported
0.5
Alonger
follow-upis
needed
toobservethe
effectsof
yoga
andpeer
mentorshipon
glycem
ic
control
26Cassidy
etal.
(2019)
[57]
Samplesize
=22
G1n=11,G
2n=11
Sex:M
=17,F
=5
Age
=60
±2years
G1.
HIIT
G2.
Control
group
36cyclesessions
over
12weeks,3
sessions/
wk
High-intensity
intervals
increasedby
10seach
week
Not
reported
0.03
HIITim
proved
glycem
ic
control
27Dixitet
al.
(2017)
[28]
Samplesize
=87
G1n=47,G
2n=40
Sex:M
=53,F
=34
Age
=50
years
G1.
Moderate-intensity
aerobicexercise
G2.
Control
group
Moderate-intensity
aerobicexercise
for8
weeks
Not
reported
Not
reported
\0.001
Moderate-intensity
aerobicexercise
enhanced
glycem
ic
control
Diabetes Ther (2021) 12:707–732 719

Table
1continued
Stud
y
no.
Reference
Participant
inform
ation
Group
sExercise
frequency/du
ration
/
volume/intensity/mod
e
Progression
Adverse
events
Pvaluea
Con
clusion
28Fayh et
al.(2018)
[49]
Samplesize
=30
G1n=15,G
2n=15
Sex:M
=12,F
=18
Age
=50.57±
6.38
years
G1.
Placeboplus
exercise
G2.
n-3PU
FAcapsules
plus
exercise
High-intensityexercise,
30min,twosessions
during
thestudy
Exerciseun
til
exhaustion
Not
reported
0.752
PUFA
n-3
supplementation
reducedtriglyceride
as
wellas
TRAPlevels
afterexercise,b
utits
effectson
HbA
1c,
inflammatory,and
oxidativestressmarkers
werenotsignificant
29Francoiset
al.
(2018)
[55]
Samplesize
=53
G1n=18,G
2n=16,
G3n=19
Sex:M
=19,F
=34
Age
=56
±9years
G1.
Milk
?HIIT
G2.
Macronu
trient
control?
HIIT
G3.
Placebo?
HIIT
12weeks
ofcardio
and
resistance-based
HIIT
thrice
weekly
Not
reported
Not
reported
\0.01
HIIT
stronglyim
proved
HBA1c
and
cardiovascular
risk
factors,so
thereis
potentialforreduced
cardiovascular
mortality
andmorbidity
30Bocket
al.
(2019)
[43]
Samplesize
=48
G1n=24,G
2n=24
Sex:M
=18,F
=30
Age
=32–7
4years
G1.
Lyengar
yoga
G2.
Program
ofstandard
exercise
Two60-m
insessions
weeklyfor12
weeks,
moderate-intensity
exercise
Not
reported
Musculoskeletal
pain
observed
\0.05
Yogaintervention
produced
improvem
entsin
blood
glucoseand
psychosocialmeasures
ofdiabetes
managem
ent
31Wycherley
etal.
(2014)
[54]
Samplesize
=84
G1n=33,G
2n=51
Sex:M
=49,F
=35
Age
=55.6
G1.Calorie-restricteddiet
CRD
G2.
CRD
?exercise
Moderateenergy-
restricted
diet
for16
weeks,8
weeks
resistance
exercise
3days/w
k
Not
reported
Not
reported
0.04
Lifestylemodification
and
participationin
structured
weight-loss
programswere
beneficialforthe
managem
entof
type
2
diabetes
720 Diabetes Ther (2021) 12:707–732

Table
1continued
Stud
y
no.
Reference
Participant
inform
ation
Group
sExercise
frequency/du
ration
/
volume/intensity/mod
e
Progression
Adverse
events
Pvaluea
Con
clusion
32Zhang
etal.
(2017)
[56]
Samplesize
=32
G1n=17,G
2n=15
Sex:M
=15,F
=17
G1.
Exercisegroup
G2.
CG
60-m
inaerobicbicycle
training
5times/w
k
for12
weeks
Not
reported
Not
reported
0.099
Aerobicexercise
significantlydecreased
serum
fetuin-A
levelsin
type
2diabetesmellitus.
There
was
no
significant
difference
in
fastingglucose,OGTT
2-hglucose,HbA
1c,
fastinginsulin
,and
HOMA-IRlevels
betweentheexercise
andcontrolgroups
Tableshow
sthecharacteristicsof
thestudiesincluded
inthissystem
aticandmeta-analysisreview
T2D
Mtype
2diabetes
mellitus,HIIT
high-in
tensityinterval
training,RT
resistance
training,MCT
continuous
moderate-intensitytraining,END
endurance,
MIC
moderate-intensity
continuous,SIT
sprint
intervaltraining,M
ICTmoderate-intensitycontinuous
training,w
kweek,M
male,Ffemale,nsamplesize,F
TFface-to-face
group,TEGtelephoniceducationgroup,
CTG
controlgroup,RTG
resistance
training
group,GLP-1R
Aglucagon-like
peptide-1receptor
agonist,REreboun
dexercise,SSA
Esupervised
structured
aerobicexercise
training,Y
Gyoga
group,PIGpeerintervention
group,CRDcalorie-restricted
diet,PAphysicalactivity,L
PAlocomotivephysicalactivity,N
PLAnonlocom
otivephysicalactivity,T
RAPtotalreactiveantioxidant
potential
aPvalues
areonlyforglycem
iccontrolvariables(H
bA1c)
Diabetes Ther (2021) 12:707–732 721

META-ANALYSIS
Outcomes
Effects of Exercise Intervention on GlycemicControlPostexercise Improvements in Glycated Hemo-globin (HbA1c) A total of 26 studies wereanalyzed in this segment. There were significantdifferences between the exercise and controlgroups regarding HbA1c improvement afterexercise intervention (Fig. 4a, P\0.0001,z = 4.28, I2 = 81%) [26–34, 37–42, 44, 46–49,51, 53, 54, 56, 57, 60]. Similarly, when the fourstudies [29, 32, 38, 49] with no nonexercisegroups were excluded, significant improve-ments in HbA1c were observed after exerciseintervention (Fig. 4b, P\ 0.0001, z = 3.81,I2 = 83%).
Postexercise Improvements in Fasting BloodGlucose (FBG) Fasting blood glucose wasreported by 13 studies. Analysis of FBG showeda significant difference between the exerciseand nonexercise groups (Fig. 4c, P = 0.03,
z = 2.21, I2 = 99%) [26, 27, 34, 35, 37, 42, 44,47, 48, 51, 56, 57].
Anthropometric ChangesEffect of Exercise Intervention on Body MassIndex (BMI) A comparison of 13 studies thatreported BMI changes after exercise interven-tion showed that BMI improved significantlywith exercise (Fig. 5a, P = 0.04, z = 2.04,I2 = 91%) [26, 29, 30, 34, 35, 41, 44, 47, 51, 54,56, 57, 60].
Effect of Exercise Intervention on BodyWeight A total of 11 studies were analyzed toassess the weight reduction after exercise inter-vention. No significant improvement in weightreduction was achieved following exerciseintervention, according to random-effectsmodels (Fig. 5b, P = 0.11, z = 1.60, I2 = 78%),but significant improvement was seen with afixed-effects model (P = 0.02) [26, 29, 31, 33,35, 42, 44, 48, 54, 56, 57].
Effect of Exercise Intervention on Waist Cir-cumference Ten studies reported waist cir-cumference changes following exercise
Fig. 2 Risk of bias graph. The review authors’ judgments about each risk of bias item are presented as percentages across allincluded studies
722 Diabetes Ther (2021) 12:707–732

intervention. A significant difference wasobserved among the studies regardingimprovement in waist circumference afterexercise intervention (Fig. 5c, P = 0.007,
z = 2.71, I2 = 91%) [26, 29, 33, 35, 41, 44,47, 48, 53, 56].
DISCUSSION
This systematic review and meta-analysis aimedto quantitatively examine the evidence regard-ing the therapeutic effects of exercise and gen-eral physical activity on glycemic control,exercise-associated anthropometric changes,and QoL in type 2 DM patients. Thirty-twostudies with 2140 participants who underwent awide variety of exercise interventions wereincluded in this systematic review and meta-analysis. The main findings of this study arethat various types of exercise can improve gly-cemic control and quality of life and can inducesignificant anthropometric changes in type 2DM patients.
Glycemic Control
Our meta-analysis of 26 studies [26–31, 33, 34,38–42, 44, 46–49, 51, 53, 54, 56, 57, 60] thatreported patient HbA1c levels revealed thatexercise intervention significantly improvedpatient HbA1c levels. However, these findingscould be limited by variation in the HbA1c levelset as an enrollment criterion in the includedstudies. This enrollment criterion was eitherHbA1c C 6.5 [27, 43–45], HbA1c 7–10 [34],HbA1c 6.4–7 [26, 30, 32, 37–44], HbA1c 7.2–9[28, 31, 33, 47], HbA1c 10–11 [36, 48, 49], orHbA1c 6.5–11 [27, 36, 45]. We can assume thatthere is a greater chance of a decrease in HbA1cin a population with higher HbA1c levels thanin a population with lower HbA1c levels. Simi-larly, a significant reduction in FBG wasobserved in this study, further verifying thetherapeutic efficacy of exercise.
Anthropometric Changes
In this study, significant improvements in BMI[26, 29, 30, 34, 35, 41, 44, 47, 50, 51, 54, 56, 57]and waist circumference [26, 29, 33, 35, 41, 44,47, 48, 53, 56] were observed with exerciseintervention. These anthropometric changes
Fig. 3 Risk of bias summary table that presents theauthors’ judgments about each risk of bias item for eachincluded study
Diabetes Ther (2021) 12:707–732 723
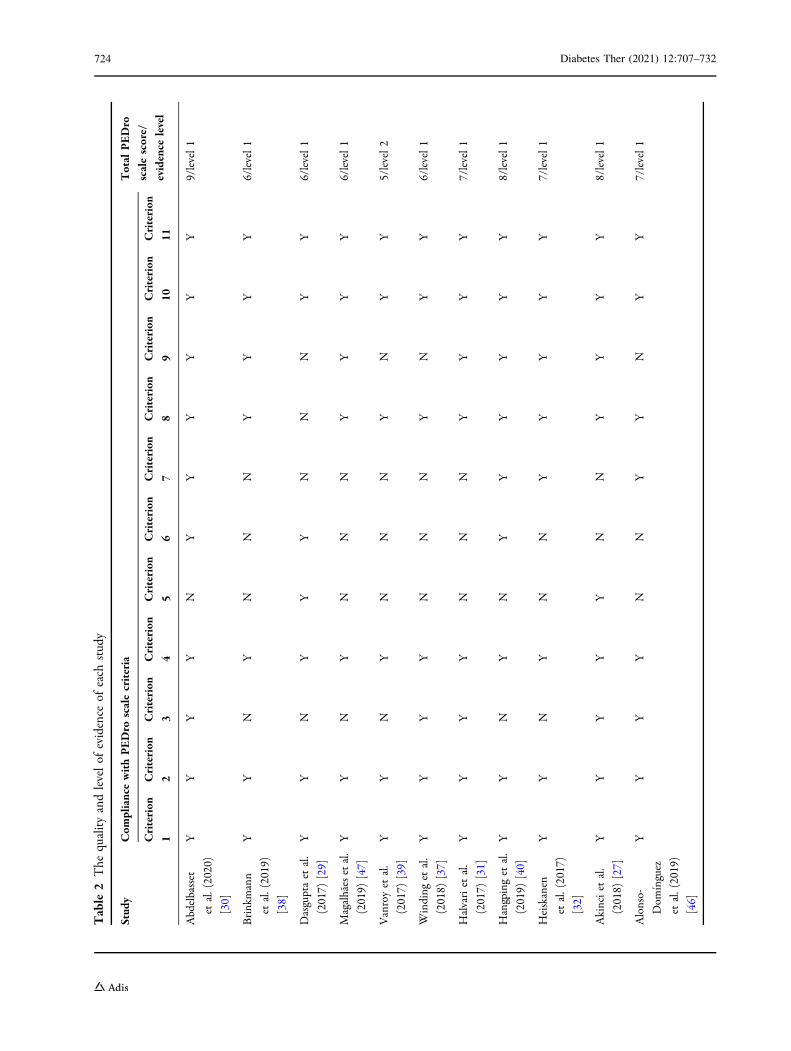
Table
2The
qualityandlevelof
evidence
ofeach
study
Stud
yCom
pliancewithPEDro
scalecriteria
Total
PEDro
scalescore/
evidence
level
Criterion
1
Criterion
2
Criterion
3
Criterion
4
Criterion
5
Criterion
6
Criterion
7
Criterion
8
Criterion
9
Criterion
10
Criterion
11
Abdelbasset
etal.(2020)
[30]
YY
YY
NY
YY
YY
Y9/level1
Brinkmann
etal.(2019)
[38]
YY
NY
NN
NY
YY
Y6/level1
Dasguptaet
al.
(2017)
[29]
YY
NY
YY
NN
NY
Y6/level1
Magalhaesetal.
(2019)
[47]
YY
NY
NN
NY
YY
Y6/level1
Vanroyet
al.
(2017)
[39]
YY
NY
NN
NY
NY
Y5/level2
Winding
etal.
(2018)
[37]
YY
YY
NN
NY
NY
Y6/level1
Halvariet
al.
(2017)
[31]
YY
YY
NN
NY
YY
Y7/level1
Hangpinget
al.
(2019)
[40]
YY
NY
NY
YY
YY
Y8/level1
Heiskanen
etal.(2017)
[32]
YY
NY
NN
YY
YY
Y7/level1
Akinciet
al.
(2018)
[27]
YY
YY
YN
NY
YY
Y8/level1
Alonso-
Dom
ınguez
etal.(2019)
[46]
YY
YY
NN
YY
NY
Y7/level1
724 Diabetes Ther (2021) 12:707–732

Table
2continued
Stud
yCom
pliancewithPEDro
scalecriteria
Total
PEDro
scalescore/
evidence
level
Criterion
1
Criterion
2
Criterion
3
Criterion
4
Criterion
5
Criterion
6
Criterion
7
Criterion
8
Criterion
9
Criterion
10
Criterion
11
DiLoretoet
al.
(2005)
[44]
YY
NY
NN
NY
NY
Y5/level2
Churchet
al.
(2010)
[41]
YY
NY
NN
NY
YY
Y6/level1
Balducciet
al.
(2012)
[52]
YY
NY
NN
YY
NY
Y6/level1
Castaneda
etal.
(2002)
[53]
YY
NY
NN
NY
YY
Y6/level1
Earnestet
al.
(2014)
[45]
YY
NY
NN
NY
NY
Y5/level2
The
tableshow
swhich
ofthe11
criteriaof
thePE
Dro
scaleweremet(Y)or
notm
et(N
)by
each
study;thetotalP
EDro
scalescorecorrespond
stothetotalnum
berof
thecriteriathat
weremet
bythestudy(notethat
criterion1was
excluded
from
thescoring,so
themaxim
umpossiblescorewas
10)
Diabetes Ther (2021) 12:707–732 725

726 Diabetes Ther (2021) 12:707–732

could maximize the wellbeing of diabetespatients and reduce the likelihood of obesity- orweight-gain-associated complications. Most ofthe studies reported a decrease in body weightafter the intervention; however, the findings ofthe meta-analysis were nonsignificant. We
hypothesize that weight reduction needs vig-orous exercises and long-term follow-up.
Quality of Life
Exercise improves wellbeing and enhances thequality of life. Two studies showed that exerciseled to improved psychological functioning [33],significant improvements in overall QoL, sexu-ality, mobility, anxiety and worry, diabetescontrol, and severity, and no significant change
bFig. 4 Glycemic control. a HbA1c exercise vs controlgroups. b HbA1c exercise vs nonexercise control groups.c Fasting blood glucose (FBG) exercise vs control groups
Fig. 5 Anthropometric changes due to exercise intervention. a Improvements in BMI (body mass index). b Improvementsin body weight. c Reduction in waist circumference
Diabetes Ther (2021) 12:707–732 727

in the social burden domain (D-39) [54]. A studyreported similar increases in QoL in two groups,one receiving liraglutide and exercise interven-tion and the other receiving placebo and exer-cise intervention. Despite some liraglutidetreatment-associated side effects, the QoL in theexercise plus liraglutide group was not inferior.These findings indicate the importance ofexercise in improving QoL [36]. Another studyreported that yoga led to a greater increase inQoL than standard exercise, but there was nosignificant between-group difference in QoL[43]. One study reported that the change in QoLfollowing exercise intervention was nonsignifi-cant; it was argued that this result was obtainedbecause the QoL questionnaire—the Audit ofDiabetes Dependent Quality of Life(ADDQoL)—may not have been appropriate forthe population studied [48]. However, onlythree of the studies that reported QoL had anonexercise group. When the study only com-pares exercise groups, all of the participantsmay undergo similar improvements in QoL. Acomparison between nonexercise and exercisegroups could offer greater insight into theeffects of exercise on QoL [33, 48, 54].
Different Exercise Regimens and TheirEffects on Blood Sugar and BodyComposition
Nutrition Plus ExerciseInterestingly, it was observed that nutritionalstatus (fasted overnight or fed) is not animportant factor in exercise interventions toimprove glycemic control in type 2 DM patients[38]. Diet plus exercise leads to a significantweight reduction [54]; moreover, glucose levelscan be strongly controlled by following anintensive diet plan after being diagnosed withtype 2 DM, such that the addition of physicalactivity (PA) may produce no additional bene-fits [26]. The GEM (glycemic load, exercise, andmonitoring blood glucose) program is uniqueand effective at modifying lifestyle and con-trolling HbA1c in diabetic patients [33].
Anaerobic TrainingEvidence has shown that HIIT significantlyimproves glycemic control (HbA1c) [30, 55, 57]and BMI [30]. Unsupervised HIIT [57] and HIITeven in lower training volume than enduranceexercise, has better effects than enduranceexercise on fitness and glycemic control [37].However, one study reported that SIT may beless beneficial for a diabetic heart than MICT,but MICT may reduce the HbA1c level morethan SIT [32]. Another study added that HIITwith RT did not affect glycemic control; how-ever, a year of combined MCIT and RT inter-vention improved body composition [47].
Aerobic TrainingAerobic exercise plays a key role in optimizingblood glucose and inducing anthropometricchanges. Different types of aerobic traininghave been shown to be effective in type 2 DMpatients. MICT significantly improves HbA1c[28, 30, 56], BMI [30], and body composition[47], and assists with weight loss [56]. Super-vised structured aerobic exercise training(SSAET) is effective at reducing BMI, FBG, andHbA1c [51]. Additionally, a study reported thatthe full benefits of aerobic exercise could beachieved with an energy expenditure of morethan 20 METs/hr/week [44].
Resistance TrainingResistance exercises are of paramount impor-tance to weight loss and glycemic control.Studies included in this review revealed signifi-cant glycemic control and anthropometricchanges [48] with resistance training (RT)interventions such as bioDensity resistancetraining [59], progressive resistance training(PRT) [53], and supervised and structured RT[48].
Combined Exercise TrainingCombining different exercise regimens couldresult in additional benefits. A combined aero-bic and RT approach was found to be better forHbA1c control than aerobic or resistance train-ing alone [41]. Moreover, aerobic and resistancetraining with exercise counseling significantlyimproved fitness, HbA1c, and weight loss [52].
728 Diabetes Ther (2021) 12:707–732

Supervised RT with HIIT exercise training andliraglutide induced major improvements inglycemic control along with robust weight loss[36]. Another study showed that a year of MCTwith RT improved body composition [47].
YogaA limited number of studies used yoga as anintervention for type 2 DM. Findings regardingthe effects of yoga on glycemic control are notconclusive due to the limited number of studiesthat included yoga. In one of the studies, yogasignificantly improved HbA1c as compared tostandard exercise [43], while it had incrementaleffects on glycemic control in another study[34]. Long-term studies of the benefit of yoga intype 2 DM are warranted.
Walking and Physical Activity (PA)General physical activity is generally consideredto be of less value than exercise interventionwhen it comes to weight loss and glycemiccontrol in type 2 DM patients. However, thefindings of the studies in the present review inrelation to general physical activity are inter-esting, with most of them showing that suchactivity improved glycemic control [29, 31, 39].Miyamoto et al. reported that nonlocomotivephysical activity (N-LPA) did not affect glucoseand fat levels [42].
A study reported that rebound exercise couldbe beneficial in type 2 DM [35]. Moreover, asupervised group-based or Internet-based exer-cise is more beneficial than simple counselingfor achieving glycemic control, reducing thewaist circumference, and improving quality oflife [27].
Limitations
A limitation of this study is the inability togroup the findings of different studies accordingto the exercise regimes used, such as resistancetraining, aerobic training, high-intensity inter-val training, and moderate-intensity continu-ous training. An ability to group the findings inthis manner would provide readers with a betterunderstating of the effects of a variety of exer-cise regimens. However, we have partly
mitigated this limitation by discussing eachexercise regimen separately.
CONCLUSIONS
Exercise is the cornerstone to good Glycemiccontrol in type 2 DM patients. Exercise trainingcan lead to significant anthropometric changesand enhance the quality of life. An exercise planinvolving 40- to 60-min sessions 3–5 days perweek or 150 min of exercise per week can sig-nificantly improve glycemic control, BMI, andwaist circumference. However, according to ourfindings, structured exercise performed as rarelyas 1–2 days per week can also reduce bloodglucose. Although considered to be less intenseactivities, general physical activity and walkingcould still help to reduce blood glucose.
ACKNOWLEDGEMENTS
Funding. No funding or sponsorship wasreceived for this study or the publication of thisarticle. The Rapid Service Fee was funded by theauthors.
Authorship. All named authors meet theInternational Committee of Medical JournalEditors (ICMJE) criteria for authorship for thisarticle, take responsibility for the integrity ofthe work as a whole, and have given theirapproval for this version to be published.
Disclosures. Sayed Zulfiqar Ali Shah, JawadAlam Karam, Alam Zeb, Rafi Ullah, Arif Shah,Ijaz Ul Haq, Iftikhar Ali, Haider Darain, andHong Chen declare that they have no conflict ofinterest.
Compliance with Ethics Guidelines. Thisarticle is based on previously conducted studiesand does not contain any studies with humanparticipants or animals performed by any of theauthors.
Data Availability. All data for this articleare presented in this manuscript.
Diabetes Ther (2021) 12:707–732 729
Open Access. This article is licensed under aCreative Commons Attribution-Non-Commercial 4.0 International License, whichpermits any non-commercial use, sharing,adaptation, distribution and reproduction inany medium or format, as long as you giveappropriate credit to the original author(s) andthe source, provide a link to the CreativeCommons licence, and indicate if changes weremade. The images or other third party materialin this article are included in the article’sCreative Commons licence, unless indicatedotherwise in a credit line to the material. Ifmaterial is not included in the article’s CreativeCommons licence and your intended use is notpermitted by statutory regulation or exceeds thepermitted use, you will need to obtain permis-sion directly from the copyright holder. To viewa copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
REFERENCES
1. Ijaz S, Ajmal M. Experiencing type II diabetes inPakistan. Pak J Social Clin Psychol. 2011;9(1).
2. Sazlina S-G, Browning CJ, Yasin S. Promotingphysical activity in sedentary elderly Malays withtype 2 diabetes: a protocol for randomised con-trolled trial. BMJ Open. 2012;2(6):e002119.
3. Taylor JD, Fletcher JP, Tiarks J. Impact of physicaltherapist-directed exercise counseling combinedwith fitness center-based exercise training on mus-cular strength and exercise capacity in people withtype 2 diabetes: a randomized clinical trial. PhysTher. 2009;89(9):884–92.
4. International Diabetes Federation. IDF diabetesatlas, 9th edn. Brussels: IDF; 2019. https://www.diabetesatlas.org
5. Short KR, Vittone JL, Bigelow ML, et al. Impact ofaerobic exercise training on age-related changes ininsulin sensitivity and muscle oxidative capacity.Diabetes. 2003;52(8):1888–96.
6. Khan I, King H. Pakistan National Diabetes Surveyprevalence of glucose intolerance and associatedfactors in North West Frontier Province (NVVFP) ofPakistan. JPMA. 1999;49:206.
7. Rosenbloom AL, Joe JR, Young RS, Winter WE.Emerging epidemic of type 2 diabetes in youth.Diabetes Care. 1999;22(2):345–54.
8. Iqbal T, Rashid F, Saleem SA, Shah SA, Khalid GH,Ishtiaq O. Awareness about diabetes mellitusamongst diabetics. JRMC. 2013;17(2):294–6.
9. Qidwai W, Ashfaq T. Imminent epidemic of dia-betes mellitus in Pakistan: issues and challenges forhealth care providers. JLUMHS. 2010;9(3):112–3.
10. Akhter J. The burden of diabetes in Pakistan: theNational Diabetes Survey. JPMA. 1999;49(9):205.
11. Hakeem R, Fawwad A. Diabetes in Pakistan: epi-demiology, determinants and prevention. J Dia-betol. 2010;1(3):3.
12. Anderson RM, Funnell MM, Arnold MS, Barr PA,Edwards GJ, Fitzgerald JT. Assessing the culturalrelevance of an education program for urban Afri-can Americans with diabetes. Diabetes Educ.2000;26(2):280–9.
13. Gabriel BM, Zierath JR. The limits of exercisephysiology: from performance to health. CellMetab. 2017;25(5):1000–11.
14. Sigal RJ, Kenny GP, Wasserman DH, Castaneda-Sceppa C, White RD. Physical activity/exercise andtype 2 diabetes a consensus statement from theAmerican Diabetes Association. Diabetes Care.2006;29(6):1433–8.
15. Sigal RJ, Kenny GP, Wasserman DH, Castaneda-Sceppa C. Physical activity/exercise and type 2diabetes. Diabetes Care. 2004;27(10):2518–39.
16. Sigal RJ, Kenny GP, Boule NG, et al. Effects of aer-obic training, resistance training, or both on gly-cemic control in type 2 diabetes: a randomized trial.Ann Intern Med. 2007;147(6):357–69.
17. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMAGroup. Preferred reporting items for systematicreviews and meta-analyses: the PRISMA statement.PLoS Med. 2009;6(7):e1000097
18. Ouzzani M, Hammady H, Fedorowicz Z, Elma-garmid A. Rayyan—a web and mobile app for sys-tematic reviews. Syst Rev. 2016;5(1):210.
19. Maher CG, Sherrington C, Herbert RD, MoseleyAM, Elkins M. Reliability of the PEDro scale forrating quality of randomized controlled trials. PhyTher. 2003;83:713–21.
20. Eng J, Teasell R, Miller W, et al. Spinal cord injuryrehabilitation evidence: method of the SCIRE sys-tematic review. Top Spinal Cord Inj Rehabil.2007;13:1–10.
730 Diabetes Ther (2021) 12:707–732
21. Higgins JPT, Altman DG. Assessing risk of bias inincluded studies. In: Higgins JPT, Green S, editors.Cochrane handbook for systematic reviews ofinterventions. Chichester: Wiley; 2008. p. 187–241.
22. Cochrane Collaboration. Review Manager, version5.3. Copenhagen: Cochrane Collaboration; 2014.
23. Hozo SP, Djulbegovic B, Hozo I. Estimating themean and variance from the median, range, and thesize of a sample. BMC Med Res Methodol.2005;5(1):13.
24. Leppink J, O’Sullivan P, Winston K. Effect size—large, medium, and small. Perspectives Med Educ.2016;5(6):347–9.
25. Lipsey MW, Wilson DB. Practical meta-analysis.Thousand Oaks: SAGE; 2001.
26. Andrews R, Cooper A, Montgomery A, et al. Diet ordiet plus physical activity versus usual care inpatients with newly diagnosed type 2 diabetes: theEarly ACTID randomised controlled trial. The Lan-cet. 2011;378(9786):129–39.
27. Akinci B, Yeldan I, Satman I, Dirican A, OzdinclerAR. The effects of Internet-based exercise comparedwith supervised group exercise in people with type2 diabetes: a randomized controlled study. ClinRehabil. 2018;32(6):799–810. PubMed PMID:29417832. eng.
28. Dixit S, Maiya A, Shastry B. Effect of moderate-in-tensity aerobic exercise on glycosylated haemoglo-bin among elderly patients with type 2 diabetes &peripheral neuropathy. Indian J Med Res.2017;145(1):129.
29. Dasgupta K, Rosenberg E, Joseph L, et al. Physicianstep prescription and monitoring to improveARTERial health (SMARTER): A randomized con-trolled trial in patients with type 2 diabetes andhypertension. Diabetes Obes Metab. 2017;19(5):695–704. PubMed PMID: 28074635.
30. Abdelbasset WK, Tantawy SA, Kamel DM, et al.Effects of high-intensity interval and moderate-in-tensity continuous aerobic exercise on diabeticobese patients with nonalcoholic fatty liver disease:a comparative randomized controlled trial. Medi-cine. 2020;99(10):e19471. PubMed PMID:32150108.
31. Halvari H, Healey J, Olafsen AH, et al. Physicalactivity and motivational predictors of changes inhealth behavior and health among DM2 and CADpatients. Scand J Med Sci Sports. 2017;27(11):1454–69. PubMed PMID: 27688002.
32. Heiskanen MA, Sjoros TJ, Heinonen IH, et al. Sprintinterval training decreases left-ventricular glucose
uptake compared to moderate-intensity continuoustraining in subjects with type 2 diabetes or predia-betes. Sci Rep. 2017;7(1):1–11.
33. Cox DJ, Taylor AG, Singh H, et al. Glycemic load,exercise, and monitoring blood glucose (GEM): aparadigm shift in the treatment of type 2 diabetesmellitus. Diabetes Res Clin Pract. 2016;111:28–35.
34. Sreedevi A, Gopalakrishnan UA, Ramaiyer SK,Kamalamma L. A randomized controlled trial of theeffect of yoga and peer support on glycaemic out-comes in women with type 2 diabetes mellitus: afeasibility study. BMC Complement Altern Med.2017;17(1):100.
35. Nuhu JM, Maharaj SS. Influence of a mini-trampo-line rebound exercise program on insulin resis-tance, lipid profile and central obesity inindividuals with type 2 diabetes. J Sports Med PhysFitness. 2017;58(4):503–9. PubMed PMID:28249384.
36. Mensberg P, Nyby S, Jørgensen PG, et al. Near-normalization of glycaemic control with glucagon-like peptide-1 receptor agonist treatment combinedwith exercise in patients with type 2 diabetes. Dia-betes Obes Metab. 2016;19(2):172–80. PubMedPMID: 27717126.
37. Winding KM, Munch GW, Iepsen UW, Van Hall G,Pedersen BK, Mortensen SP. The effect on glycaemiccontrol of low-volume high-intensity intervaltraining versus endurance training in individualswith type 2 diabetes. Diabetes Obes Metab.2018;20(5):1131–9. PubMed PMID: 29272072.
38. Brinkmann C, Weh-Gray O, Brixius K, Bloch W,Predel HG, Kreutz T. Effects of exercising beforebreakfast on the health of T2DM patients—a ran-domized controlled trial. Scand J Med Sci Sports.2019;29(12):1930–6. PubMed PMID: 31442336.
39. Vanroy J, Seghers J, Bogaerts A, Devloo K, De CockS, Boen F. Short- and long-term effects of a need-supportive physical activity intervention amongpatients with type 2 diabetes mellitus: a random-ized controlled pilot trial. PLoS One. 2017;12(4):e0174805. PubMed PMID: 28384237.
40. Hangping Z, Xiaona Q, Qi Z, et al. The impact onglycemic control through progressive resistancetraining with bioDensityTM in Chinese elderlypatients with type 2 diabetes: the PReTTy2 (Pro-gressive Resistance Training in Type 2 Diabetes)trial. Diabetes Res Clin Pract. 2019;150:64–71.
41. Church TS, Blair SN, Cocreham S, et al. Effects ofaerobic and resistance training on hemoglobin A1clevels in patients with type 2 diabetes: a random-ized controlled trial. JAMA. 2010;304(20):2253–62.
Diabetes Ther (2021) 12:707–732 731

42. Miyamoto T, Fukuda K, Oshima Y, Moritani T. Non-locomotive physical activity intervention using atri-axial accelerometer reduces sedentary time intype 2 diabetes. Phys Sportsmed. 2017;45(3):245–51. PubMed PMID: 28664755.
43. Bock BC, Thind H, Fava JL, et al. Feasibility of yogaas a complementary therapy for patients with type2 diabetes: the Healthy Active and in Control(HA1C) study. Complement Ther Med. 2019.42:125–31. PubMed PMID: 30670230.
44. Di Loreto C, Fanelli C, Lucidi P, et al. Make yourdiabetic patients walk: long-term impact of differ-ent amounts of physical activity on type 2 diabetes.Diabetes Care. 2005;28(6):1295–302.
45. Earnest CP, Johannsen NM, Swift DL, et al. Aerobicand strength training in concomitant metabolicsyndrome and type 2 diabetes. Med Sci SportsExerc. 2014;46(7):1293.
46. Alonso-Domınguez R, Garcıa-Ortiz L, Patino-Alonso MC, et al. Effectiveness of a multifactorialintervention in increasing adherence to theMediterranean diet among patients with diabetesmellitus type 2: a controlled and randomized study(EMID study). Nutrients. 2019;11(1):162.
47. Magalhaes JP, Judice PB, Ribeiro R, et al. Effective-ness of high-intensity interval training combinedwith resistance training versus continuous moder-ate-intensity training combined with resistancetraining in patients with type 2 diabetes: a one-yearrandomized controlled trial. Diabetes Obes Metab.2019;21(3):550–9. PubMed PMID: 30284352.
48. Hsieh P-L, Tseng C-H, Tseng YJ, Yang W-S. Resis-tance training improves muscle function and car-diometabolic risks but not quality of life in olderpeople with type 2 diabetes mellitus: a randomizedcontrolled trial. J Geriatr Phys Ther. 2018;41(2):65–76.
49. Fayh APT, Borges K, Cunha GS, et al. Effects of n-3fatty acids and exercise on oxidative stress param-eters in type 2 diabetic: a randomized clinical trial.J Int Soc Sports Nutr. 2018;15:18. PubMed PMID:29713249.
50. Hemmati Maslakpak M, Razmara S, Niazkhani Z.Effects of face-to-face and telephone-based family-oriented education on self-care behavior andpatient outcomes in type 2 diabetes: a randomizedcontrolled trial. J Diabetes Res. 2017;2017:8404328.PubMed PMID: 29359166.
51. Shakil-Ur-Rehman S, Karimi H, Gillani SA, Amjad I,Ahmad S, Yaseen A. Response to a supervisedstructured aerobic exercise training program inpatients with type 2 diabetes mellitus—does gendermake a difference? A randomized controlled
clinical trial. J Natl Med Assoc. 2018;110(5):431–9.PubMed PMID: 30129517.
52. Balducci S, Zanuso S, Cardelli P, et al. Changes inphysical fitness predict improvements in modifiablecardiovascular risk factors independently of bodyweight loss in subjects with type 2 diabetes partic-ipating in the Italian Diabetes and Exercise Study(IDES). Diabetes Care. 2012;35(6):1347–54.
53. Castaneda C, Layne JE, Munoz-Orians L, et al. Arandomized controlled trial of resistance exercisetraining to improve glycemic control in older adultswith type 2 diabetes. Diabetes Care. 2002;25(12):2335–41.
54. Wycherley TP, Clifton PM, Noakes M, BrinkworthGD. Weight loss on a structured hypocaloric dietwith or without exercise improves emotional dis-tress and quality of life in overweight and obesepatients with type 2 diabetes. J Diabetes Investig.2014;5(1):94–8.
55. Francois ME, Pistawka KJ, Halperin FA, Little JP.Cardiovascular benefits of combined intervaltraining and post-exercise nutrition in type 2 dia-betes. J Diabetes Complications. 2018;32(2):226–33. PubMed PMID: 29198993.
56. Zhang L-Y, Liu T, Teng Y-Q, et al. Effect of a12-week aerobic exercise training on serum fetuin-Aand adipocytokine levels in type 2 diabetes. ExpClin Endocrinol Diabetes. 2018;126(08):487–92.
57. Cassidy S, Vaidya V, Houghton D, et al. Unsuper-vised high-intensity interval training improvesglycaemic control but not cardiovascular auto-nomic function in type 2 diabetes patients: a ran-domised controlled trial. Diab Vasc Dis Res.2019;16(1):69–76.
58. Savikj M, Gabriel BM, Alm PS, et al. Afternoonexercise is more efficacious than morning exerciseat improving blood glucose levels in individualswith type 2 diabetes: a randomised crossover trial.Diabetologia. 2019;62(2):233–7. PubMed PMID:30426166.
59. Hangping Z, Xiaona Q, Qi Z, et al. The impact onglycemic control through progressive resistancetraining with bioDensity(TM) in Chinese elderlypatients with type 2 diabetes: The PReTTy2 (Pro-gressive Resistance Training in Type 2 Diabetes)trial. Diabetes Res Clin Pract. 2019;150:64–71.PubMed PMID: 30779971.
60. Hemmati Maslakpak M, Razmara S, Niazkhani Z.Effects of face-to-face and telephone-based family-oriented education on self-care behavior andpatient outcomes in type 2 diabetes: a randomizedcontrolled trial. J Diabetes Res. 2017:8404328.
732 Diabetes Ther (2021) 12:707–732


















