Movement disorders: A complication of chronic Hyperglycemia? A case report
5
Movement disorders: A complication of chronic Hyperglycemia? A case report
-
Upload
apollo-hospitals -
Category
Health & Medicine
-
view
201 -
download
1
description
The association of chorea with a specific lesion on brain imaging is described as an atypical manifestation of chronic hyperglycemia. This is a rare syndrome, affecting more elderly, presenting a diabetes poorly controlled. There is hyperglycemia without ketosis and moderate hyperosmolarity.
Transcript of Movement disorders: A complication of chronic Hyperglycemia? A case report

Movement disorders: A complication of chronic Hyperglycemia? A case report

Case Report
Movement disorders: A complication of chronichyperglycemia? A case report
R. Ben Othman a,*, A. Ben Mahmoud b, A. Mankai a, N. Trabelsi a,F. Hentati b, F. Ben Mami a
aDepartment (C) of Diabetology, Nutrition and Metabolic Diseases, The National Institute of Nutrition,
Avenue Jbel Lakhdhar, 1007 Tunis, TunisiabDepartment of Neurology, National Institute Mongi Ben Hmida of Neurology, Tunis, Tunisia
a r t i c l e i n f o
Article history:
Received 29 March 2013
Accepted 9 October 2013
Available online xxx
Keywords:
Diabetes mellitus
Chorea
Dyskinesia
Hyperglycemia
Nonketotic hyperglycemia
a b s t r a c t
Introduction: The association of chorea with a specific lesion on brain imaging is described
as an atypical manifestation of chronic hyperglycemia.
Case report: Patient of 77 years, hospitalized for bilateral choreic movements predominant
on the right with dystonic movements, appeared a month ago.
At admission: Hyperglycemia at 2.4 g/L, without ketosis, a type 2 diabetes (HbA1c 17.3%) on
oral antidiabetic agents. CT scan shows hyperdensity of putamen and lenticular nucleus
that eliminates an ischemic attack. Evolution after glycemic reequilibration and treatment
by haloperidol is favorable, with regression of chorea.
Discussion: This is a rare syndrome, affecting more elderly, presenting a diabetes poorly
controlled. There is hyperglycemia without ketosis and moderate hyperosmolarity. The
symptomsusually regress after glycemic control andneuroleptic treatment (recurrence in 13%
of cases). The appearance of this syndrome seems to be related to the achievement of the
control system GABAergic of the basal ganglia leading to an excitation of the cerebral cortex,
causing involuntary movements. The etiopathogenic hypotheses advanced are multiple:
impairedstriatalneurotransmissionassociatedwithmetabolicdisturbancesofhyperglycemia,
dysfunctionof thehematoencephalicbarrier andabnormalitiesof the cerebralvascularization.
Conclusion: Chorea secondary to nonketotic hyperglycemia is a rare complication and little
known of type 2 diabetes. Transitional neuroleptic treatment and glycemic control make
the symptoms regress in most cases with the disappearance of the lesion imaging.
Copyright ª 2013, Indraprastha Medical Corporation Ltd. All rights reserved.
1. Introduction
The uncontrolled diabetes can be responsible for different
neurological symptoms such as epileptic seizures and disor-
ders of consciousness. Transient chorea or ballism provoked
by an episode of nonketotic hyperglycemia has been reported
by numerous authors over the past couple of decades.1,2 In
this case, the choreiform movements have resolved within
days after normalization of blood glucose. In the vast majority
of cases, the chorea/ballism triggered by hyperglycemia has
* Corresponding author. Tel.: þ216 97291139.E-mail address: [email protected] (R. Ben Othman).
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.elsevier .com/locate/apme
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e3
Please cite this article in press as: Ben Othman R, et al., Movement disorders: A complication of chronic hyperglycemia? A casereport, Apollo Medicine (2014), http://dx.doi.org/10.1016/j.apme.2013.10.006
0976-0016/$ e see front matter Copyright ª 2013, Indraprastha Medical Corporation Ltd. All rights reserved.http://dx.doi.org/10.1016/j.apme.2013.10.006

been unilateral. Several recent reports have documented
characteristic brain imaging findings consisting of high den-
sity on computed tomography (CT) scans. We describe a case
of chorea developing subacutely during an episode of revers-
ible nonketotic hyperglycemia.
2. Observation
A patient, aged 77 years, followed for type II diabetes on oral
antidiabetic agents for three months and for hypertension
since two years, presents to the emergency for abnormal
movements of the upper limbs, the head and neck. These
movements are type of flexion-extension and rotation. They
are abrupt, irregular and of large amplitude, exaggerating to
emotion and disappearing during sleep.
There is no remarkable family history or a prior history of
dopamine antagonist or estrogen medication use and no his-
tory of rheumatic fever/Sydenham’s chorea.
At admission, the patient was conscious, afebrile and well
oriented in time and space. Neurological examination objec-
tify chorea in both upper limbs, the head and neck predomi-
nant at right without oral or lingual abnormal movements. In
addition, the review found hypotonia in all four limbs.
The remainder of the examination shows no motor or
sensory deficit, nor parkinsonism nor cerebellar nor cranial
disorder. A specialized neuropsychological examination did
not show significant cognitive disorders (mini-mental
state ¼ 28/30) except an alteration of executive functions
(frontal score ¼ 8/18). In addition, a psychomotor instability
was noted as well as irritability.
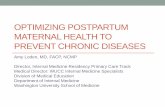
A cerebral CT scan was performed in emergency, which
objectified a spontaneous hyperdensity of putamen and
lenticular nuclei (Fig. 1a et b). Our patient did not benefit of
brain MRI. Urinalysis was strongly positive for glucose and
negative for ketones. The following laboratory data were
notable: fasting blood glucose 13.2 mmol/l (240 mg/dl), glyco-
sylated hemoglobin A1c 17.3%, creatinine 140 mmol/l, clear-
ance 37 ml/min.
The patient was put on insulin and small doses of halo-
peridol (3 mg/day in three divided doses). A significant
reduction in abnormal movements was noted, these dis-
appeared within four days, which motivated progressive
stopping of haloperidol .The patient was admitted in dia-
betology for initiation of insulin 6UI at morning due to
contraindication for the use of oral antidiabetic .The patient is
still asymptomatic after six months. Control brain CT scan
was not performed.
3. Discussions
Chorea and ballism are hyperkinetic movement disorders
which are characterized by the occurrence of uncontrollable,
sudden, irregular, high amplitude and short duration move-
ments of all or a part of the body.3,4 Chorea and/or ballismhave
been reported for thefirst time, as a complication ofnonketotic
hyperglycemia by Bedwell in 1960.5 These abnormal move-
mentsare rarely revealingofdiabetes.2 The symptomatology is
made from hemichorea and/or hemiballismus in most cases
correlated to unilateral scannographic images.6 For our case
thedamage is bilateral predominantly to the right in relation to
imagery and in accordancewith somesimilar cases reported in
the literature where the lesion is bilateral.7
Physiopathology subtending the development of these
movements during hyperglycemia without ketosis is still un-
clear.3 Several hypotheses have been evoked.
Brain structures implicated in the genesis of chorea are
represented by the basal ganglia, mainly the subthalamic
nucleus, theway pallido-subthalamic, striatum and to a lesser
degree the cerebral cortex and the thalamus.8 These cores are
susceptible to ATP and cellular energy depletion which prob-
ably explain the predilection of lesions at their level.8
Indeed, during hyperglycemia, there is an alteration of the
bloodebrain barrier (BBB) leading to, on one hand, the reduc-
tion of regional cerebral blood flow and on the other hand, the
passage of the cerebral metabolism to anaerobic, resulting in
an inhibition of the tricarboxylic acid cycle (Krebs).9,10
Fig. 1 e (a and b) A CT scan showing a spontaneous hyperdensity in the putamen and the lenticular nucleus.
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e32
Please cite this article in press as: Ben Othman R, et al., Movement disorders: A complication of chronic hyperglycemia? A casereport, Apollo Medicine (2014), http://dx.doi.org/10.1016/j.apme.2013.10.006

Thebrain thenuses thegamma-aminobutyricacid (GABA) as
an alternative source of energy. In patients without ketosis,9e12
the amount of GABA and acetate is rapidly depleted.11,13
Because of this deficiency of acetate, acetylcholine synthesis
may also be decreased. The depletion of these two principal
neurotransmitters (GABAandacetylcholine) in thebasalganglia,
in combinationwith loss of energy andmetabolic acidosis is the
cause of the appearance of movement disorders.11,13,14
Hyperglycemia has also a role in the extravasation of red
blood cells that is the cause of hemorrhagic suffusions found
in cerebral imaging of the majority of these patients.8
Other indirect factorshavebeen incriminated in thegenesis
of chorea, in fact most cases of chorea during nonketotic hy-
perglycemia have been reported in elderly patients with hy-
pertension associated with diabetes.14,15 Indeed, these two
vascular risk factors are often responsible for cerebral vascular
lesions especially lacunar mainly at the basal ganglia.16 These
lesions are usually not visible on standard neuroimagery, but
responsible for clinical manifestations such as chorea.14,17
Finally, the acanthocytosis as a predictor of the onset of
chorea during diabetes has been reported.12 Several hypotheses
have suggested that erythrocyte membrane proteins can un-
dergo, secondary to a particular metabolic state (diabetes),
functional and morphological changes, with acanthocytes for-
mation.18 So hyperviscosity induced by hyperglycemia may
cause a transientmalfunction in striatal neurons inpredisposed
individuals. This hypothesis is in agreement with the concept
that hyperglycemia worsens the evolution of stroke. For our
patient, the search for acanthocytes came back negative.
Chorea in the context of hyperglycemia without ketosis is
generally good prognosis. Most patients improve when
normalization of blood glucose, sometimes without the use of
neuroleptics or with very low doses.10,14 Radiological abnor-
malities may persist longer and disappear for days or weeks
after normalization of glycemia.12
Neuroleptics is the treatment of choice. Benzodiazepines
can also be used.
4. Conclusion
Chorea during uncontrolled diabetes is an unusual compli-
cation, however it remains favorable prognosis in most cases,
which makes necessary the knowledge of this association
since therapeutic implications arising.
Conflicts of interest
All authors have none to declare.
r e f e r e n c e s
1. Chang CV, Felicio AC, Godeiro-Junior CO, et al. Chorea-ballism as a manifestation of decompensated type 2 diabetesmellitus. Am J Med Sci. 2007;333:175e177.
2. Lai PH, Tien RD, Chang MH, et al. Chorea-ballismus withnonketotic hyperglycemia in primary diabetes mellitus. Am JNeuroradiol. 1996;17:1057e1064.
3. Mihai CM, Catrinoiu D, Stoicescu RM. Atypical onset ofdiabetes in a teenage girl: a case report. Cases J. 2008;1:425.
4. Vingerhoets F, Russmann H, Carruzzo A, et al. Mouvementsanormaux (dystonie, athetose, choree, ballisme). EMC. 2004,17:007-B-10.
5. Bedwell SF. Some observations on hemiballismus. Neurology.1960;10:619e622.
6. Rafai MA, Gynerane M, et al. Hemichoree-hemiballisme ethyperglycemie non cetonique. NPG. 2010;10:229e232.
7. Nakagawa T, Mitani K, et al. Chorea-ballism associated withnonketotic hyperglycemia and presenting with bilateralhyperintensity of the putamen on MR T1-weighted imageseacase report. Rinsho Shinkeigaku. 1994;34(1):52e55.
8. Felicio AC, Chang CV, Godeiro-Junior C, et al. Hemichorea-hemiballism as the first presentation of type 2 diabetesmellitus. Arq Neuropsiquiatr. 2008;66(2-A):249e250.
9. Low PA, Ward K, Schmelzer JD, et al. Ischemic conductionfailure and energy metabolism in experimental diabeticneuropathy. Am J Physiol. 1985;248:E457eE462.
10. Oerlemans WGH, Moll LC. Non ketotic hyperglycemia in ayoung woman presenting as hemiballism-hemichorea. ActaNeurol Scand. 1999;100:411e414.
11. Guisado R, Arieff AI. Neurological manifestations of diabeticcomas: correlation with biochemical alterations in the brain.Metabolism. 1975;24:665e679.
12. Pisani A, Diomedi M, Rum A. Acanthocytosis as apredisposing factor for non-ketotic hyperglycaemia inducedchorea-ballism. J Neurol Neurosurg Psychiatry.2005;76:1717e1719.
13. Rector WG Jr., Herlong HF, Moses H 3rd. Nonketotichyperglycemia appearing as choreoathetosis or ballism. ArchIntern Med. 1982;142:154e155.
14. Lin JJ, Chang MK. Hemiballism-hemichorea and nonketotic hyperglycemia. J Neurol Neurosurg Psychiatry.1994;57:748e750.
15. Nagai C, Kato T, Katagiri T, et al. Hyperintense putamen onT1-weighted images in a case of chorea with hyperglycemia.Am J Neuroradiol. 1995;16:1243e1246.
16. Weisberg LA. Diagnostic classification of stroke, especiallylacunes. Stroke. 1988;19:1071e1073.
17. Cherian A, Thomas B, Baheti NN, et al. Concepts andcontroversies in nonketotic hyperglycemia-inducedhemichorea: further evidence from susceptibility-weightedMR imaging. J Magn Reson Imaging. 2009;29(3):699e703.
18. Rampoldi L, Danek A, Monaco AP. Clinical features andmolecular bases of neuroacanthocytosis. J Mol Med.2002;80:475e491.
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e3 3
Please cite this article in press as: Ben Othman R, et al., Movement disorders: A complication of chronic hyperglycemia? A casereport, Apollo Medicine (2014), http://dx.doi.org/10.1016/j.apme.2013.10.006

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/