Motivations Underlying the Adoption of ERP Systems in ...
12
Cahier de recherche CR-2012-01 Motivations Underlying the Adoption of ERP Systems in Healthcare Organizations: An Analysis from “Success Stories” Placide Poba-Nzaou Louis Raymond Sylvestre Uwizeyemungu Guy Paré Février 2012 Institut de recherche sur les PME
Transcript of Motivations Underlying the Adoption of ERP Systems in ...

Cahier de recherche
CR-2012-01
Motivations Underlying the Adoption of ERP Systems in Healthcare
Organizations: An Analysis from “Success Stories”
Placide Poba-Nzaou
Louis Raymond Sylvestre Uwizeyemungu
Guy Paré
Février 2012
Institut de recherche sur les PME

2
Proceedings of the 45th Hawaii International
Conference on System Sciences

3
Motivations Underlying the Adoption of ERP Systems in Healthcare
Organizations: An Analysis from “Success Stories”
Placide Poba-Nzaou Université
du Québec à Montréal poba-
Louis Raymond
Université du Québec à Trois-Rivières
Sylvestre Uwizeyemungu Université du Québec à Trois-Rivières
Guy Paré HEC-
Montréal
Abstract
In order to deal with continuous drastic increases in
healthcare spending and major demographic
changes, governments in industrialised countries are
initiating major reforms aimed at improving the
efficiency and the quality of care services provided to
their citizens. These reforms along with increasing
requirements for accountability tend to
“corporatize” these institutions by exposing them to
market-like pressures. To face their changing
environment, healthcare institutions have invested in
ERP systems as their basic technological
infrastructure, highlighting a phenomenon that
recalls the earlier popularity of the ERP movement
with private companies. Based on the analysis of 180
public “success stories,” the main objective of this
study is to identify and characterize the sets of
motivations that lead to the adoption of ERP systems
in healthcare organizations. Our findings indicate
that these motivations can be classified into six
categories, namely technological, managerial
operational, managerial strategic, clinical
operational, clinical strategic, and financial. Three
clusters of healthcare organizations were identified
with regard to these motivations, and labelled as a
Business View, a Clinical View, and an Institutional
View of ERP systems.
1. Introduction
Despite governments’ enormous financial efforts, the
gap between the demand for healthcare services from
an increasingly well-informed and expectant public,
and the capacity of healthcare organizations to meet
this demand increases regularly [1]. It is in this
context that many, if not most, governments are
initiating major reforms aimed at improving the
efficiency and the quality of care services provided to
their citizens [2]. These reforms along with
increasing autonomy and accountability tend to
“corporatize” healthcare organizations by exposing
them to market-like pressures. Consequently, these
organizations are facing the same challenges than
other modern organizations [3] and thus seek
flexibility, rapidity, integration, and innovation [4].
In order to deal with these challenges, most
scholars and experts recommended intensive use of
information technology (IT) [5]. Following these
recommendations, healthcare organizations have
increased their capital investments in IT, although
they still lag behind organizations operating in other
information intensive industries such as the financial
industry, the telecommunications industry, and the
airline sector [6]. Following Pollock and Cornford
[7], it might be argued that since the healthcare sector
shares common problems with a wide range of
sectors or industries, IT innovations such as
enterprise resource planning (ERP) systems
implemented in contemporary business corporations
would also apply in healthcare institutions. Indeed,
ERP systems were arguably the most popular IT
innovation in the 1990s [8] and even at the beginning
of the 21st
century [9, 10], so much so that the large
enterprise market for these systems became saturated,
forcing ERP vendors to look for other market
segments, particularly in the service and small
business sectors [11]. One could thus assume that
there is a convergence of interests between healthcare
organizations and ERP system vendors. On the one
hand, the former would be attracted by the benefits
purportedly obtained from ERP adoption in the
private sector, benefits such as the integration of
business processes and the greater quality of
information available for decision-making [12]. On
the other hand, ERP vendors recognize the healthcare

4
Type of motivation Specific examples of motivations References
Technological
"The majority of administrative systems are 10-25 year old [...]
While many of these systems have had major modifications to adapt
to changing requirements, the original design and intent of the
systems remain a barrier for users"
"The current Student System is unable to support core University
functions (such as the management of student information) and must
be replaced as a priority"
[19]
[19]
Operational
"In this industry, we make very fast decisions. Our old systems just
didn't have the flexibility to react to the market that quickly."
"These current systems, built originally to support an organizational
view, should be systematically replaced with systems supporting a
process view"
[32]
[33]
Strategic
"Enhance the view that the university is an information
technologically advanced and open institution"
"increased student support and enhanced teaching activities"
[33]
[33]
Financial
"To deal with the projected decline in state funding support and to
reduce the pressure to increase tuition, costs need to be contained or
reduced. Of particular importance is the need to focus on personnel
costs, which are the largest component of the expenditure base, and
the need to streamline processes and procedures which add to
administrative costs."
"We needs to increase the use of electronic documents internally and
the exchange of information electronically with external
organizations through the use of industry standards [...] will simplify
business processing, reduce costs"
[19]
[19]
sector to have the greatest potential for growth in the
ERP systems market [13]. Indeed, the global
healthcare systems market is estimated to be worth
$53.8 billion by 2014, growing at an annual rate of
16% [14].
As more and more healthcare organizations are
adopting ERP systems, analyzing the motivations for
which they undertake an ERP system project has
become important for at least three reasons. Firstly,
these motivations affect the project’s scope, design
and implementation [15, 16]. It has also been
confirmed empirically that the influence of
motivations to adopt a health information system
influence the project’s implementation outcome [17,
18]. Secondly, most studies on motivations to
adopting ERP systems have been conducted in the
context of large, private sector [19-21] and public
sector organizations [22-24]. Thirdly, ERP system
adoption in the healthcare industry is a relatively
recent phenomenon, less than 20 percent of hospitals
having implemented an ERP by the year 2006 [6].
To our knowledge, no prior research has
examined the motivations for adopting ERP systems
in the healthcare sector. This paper attempts to fill
this gap by first aiming to identify and characterize
the actual motivations that lead to the adoption of
these systems by healthcare organizations. Another research objective is to characterize these
organizations with regard to ERP by uncovering
typical profiles or patterns of motivations among
them. And following previous work done in public
sector institutions [25], our final aim is to ascertain
whether these motivations are influenced by certain
aspects of the organizational context.
2. Conceptual and Empirical Background
What can motivate an organization to adopt an ERP
system, knowing the high cost and high risk
associated with such an undertaking? In prior
research, the motivations underlying an
organization’s decision to adopt an ERP system have
been examined mostly in an incidental manner [e.g.
16, 26-28], whereas few empirical studies have
focused on these motivations per se.
In the private sector, Oliver and Romm [19]
found that there are three categories of motivations
that lead an organization to search for an ERP
solution: 1) the need to improve the performance of
current operations, 2) the need to integrate data and
systems, and 3) the need to prevent a competitive
disadvantage or a business risk from becoming
critical. In the same setting, Ross and Vitale [20]
identified six reasons generally cited by enterprises,
classifying them into three categories (infrastructure,
capacity, and performance). These authors underlined
the sequential character of these categories as the
firm’s new common systems platform (infrastructure)
makes it possible to develop new capabilities
(process improvement, data visibility), which in turn
are meant to improve organizational performance
(cost reduction, strategic decision making, customer
responsiveness). Essentially the same three types of
motivations can also be found in Parr and Shanks
[15], under different names, that is, technological
(common platform, obsolescence of legacy systems),
operational (process improvement, data visibility,
operating cost reductions), and strategic motivations
(Y2K compliance, multi-site standardization,
customer responsiveness, decision-making
improvement, need for efficiencies and integration,
business restructuring).
In the public sector, the only empirical study on
ERP motivations that could be found was that of
Raymond et al. [22]. Based on their analysis of data
from 46 stories of public organizations, these authors
found that the motivations that lead public sector
organizations to adopt an ERP system are related to
four types of performance, namely, technological,
operational, strategic, and financial performance. In
the healthcare sector, while four ERP implementation
studies could be found [29-32], none focused on the
motivations that underlie the adoption of these
systems. Hence to our knowledge, no prior research
has specifically examined such ERP adoption
motivations in healthcare organizations.
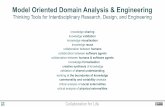
As shown in Table 1, for the purpose of the
present study, an initial taxonomy of ERP adoption
motivations was elaborated by integrating the
previously cited categorizations.
Table 1. Taxonomic framework

5
This produced the following four generic categories:
1) technological performance, 2) operational
performance, 3) strategic performance, and 4)
financial performance motivations. Technological
performance motivations have mainly to do with the
IT infrastructure. Operational performance
motivations concern the improvement of processes.
Strategic performance motivations are related to a
change in orientation, in the design or delivery of
services, or in the image of the organization.
Financial performance motivations apply to
profitability, cost reduction, and revenue growth.
This classification initially appears to have sufficient
face validity and discriminating power for the
purposes of this research.
3. Methodology
3.1 Selection and description of the cases
In identifying success stories of ERP system
adoption and implementation in the healthcare sector,
we followed Shang and Seddon’s [32] approach in
using case studies published by ERP vendors on their
websites. The main reasons for using such data were
that they provide a broad view of the ERP adoption
and implementation experience, they contain
verifiable facts, including the disclosure of the
adopting organization’s identity as well as that of the
main project actors, and they are reported from the
perspective of the adopting organization. All stories
are considered successful from the adopting
organization’s and vendor’s perspective.
Now, stories related by vendors evidently tend to
oversell their products and services and the business
benefits they provide. Our study’s main purpose
however was not to evaluate the degree of attainment
of these benefits but rather to identify and analyze the
primary motivations that led healthcare organizations
to adopt ERP systems. Hence the main data
collection task was centered on the various
experiences described in each story rather than on the
conclusions of their authors [34].
As an initial step, we consulted the websites of
SAP, Oracle, and Microsoft which together represent
more than 50% of the ERP world market. We then
consulted the websites of McKesson, Cerner, and
HLTH who represent the leaders of the health IT
sector with 30% of the market. Thereafter, we
performed general web searches with the following keywords: “ERP,” “healthcare,” and “hospital.” The
web sites were accessed between November 15, 2010
and January 20, 2011. Altogether, we identified 225
“success stories” qualified as healthcare sector
implementations by ERP vendors.
We disqualified 45 of these stories for different
reasons. After preliminary analysis, some stories did
not pertain at all to the healthcare sector even though
they were presented as such on the ERP vendors’
websites. We also disqualified other stories after
concluding that the system implemented could not be
truly considered as an ERP product. Other stories
were written in languages other than English or
French, the two languages spoken and understood by
the researchers. Last, other stories were eliminated
because not enough explicit or implicit information
about the ERP adoption motivations could be found.
As shown in Table 2, altogether, 180 stories from
a variety of healthcare ERP vendors were recorded:
100 from Oracle, 38 from SAP, 37 from Cerner and 5
from other vendors such as McKesson, Siemens and
Compiere. These stories emanate from 31 different
countries on five continents, the majority being North
American (92) and European (68), including the
United States with 89, and the United Kingdom, Germany and The Netherlands with 17, 15 and 8
stories, respectively. One may note here that while
Oracle’s and SAP’s success stories are equally found
in North America and Europe, Cerner’s stories are
almost exclusively found in North America.
Table 2. Number of ERP adoption stories
North
America Europe Asia South
America Oceania Total
Oracle 40 44 10 3 3 100 SAP 16 18 2 2 0 38 Cerner 35 2 0 0 0 37 Other 1 4 0 0 0 5 Total 92 68 12 5 3 180
As ERP vendors structure their offer in a modular
fashion, the various modules described in the stories
include the following functions: administrative
systems (145 stories), clinical information systems
(38 stories), clinical support systems (36 stories), and
patient management systems (22 stories). Table 3
presents the breakdown by vendor of the ERP
modules implemented. One may note here Cerner’s
under-representation in the “administrative systems”
category, and conversely its over-representation in
the other three categories versus Oracle and SAP.
3.2 Coding and analysis
To collect the story data, we elaborated an initial
coding sheet with two main categories of data: case
attributes and ERP adoption motivations. The case
attributes refer to institutional attributes and ERP
system attributes. The institutional attributes

6
Rank Technological performance Managerial -
operational Clinical - operational Managerial -
strategic Clinical - strategic Financial
performance
1
Search for IT integration
(51)
Improve
effectiveness of
administrative processes
(88)
Improve
effectiveness and efficiency of patient care
(44)
Improve
administrative performance
management capabilities
(30)
Strengthen
clinical strategic
positioning (8)
Monitor cost
trends (40)
2
Improve IT
infrastructure
capabilities (44)
Improve administrative
data availability
and accessibility
(29)
Improve
effectiveness
of clinical processes (29)
Enhance compliance
with laws and regulations
(30)
Transform care delivery and respond to
changing needs
(5)
Increase profitability or return on investment
(17)
3
Modernize IT systems (43)
Improve HR management
performance (19)
Facilitate access to
clinical information
(21)
Support organizational
growth and expansion (26)
Improve clinical
performance management
capabilities (4)
Improve financial
transparency (5)
4
Improve IT productivity
(20)
Improve administrative data accuracy and relevance
(15)
Improve
patient safety (21)
Facilitate connectivity with majors stakeholders
(19)
Implement a patient safety
culture (3)
Monitor asset value (1)
5
Build a knowledge
management infrastructure
(2)
Search for business
process integration
(14)
Enhance the preservation of patients’
privacy (16)
Improve decision- making
processes (14)
considered here include tax status (for-profit vs not-
for-profit), organization status (hospital or clinic vs
other type of organization), location (urban vs rural),
organizational size (number of employees and
number of beds when applicable), network affiliation
(yes or no), and university affiliation (yes or no). For
their part, the ERP system attributes considered here
refer to ERP vendor, functional coverage of the ERP
system, and modules implemented.
Table 3. Breakdown of healthcare ERP modules and stories by ERP vendor
Oracle
freq. (%) SAP freq. (%) Cerner
freq. (%) Other freq. (%) χ
2 Administrative systems (145) 94 (65) 36 (25) 10 (7) 5 (3) 85.3*** Clinical information systems (38) 9 (24) 3 (8) 26 (68) 0 (0) 67.8*** Clinical support systems (36) 3 (8) 5 (14) 28 (78) 0 (0) 92.1*** Patient management systems (22) 1 (5) 6 (27) 15 (68) 0 (0) 40.5*** Total number of ERP stories 100 (56) 38 (21) 37 (20) 5 (3) *** p < 0.001
Administrative modules: accounting, HR, disease costing, material management, etc.
Clinical modules: emergency room system, operating room system, nursing system, CPOE, etc.
Clinical support modules: pharmacy information system, LIS, RIS, etc.
Patient management modules: patient admission, transfer and discharge system
As for ERP motivations, four main categories
were created based on the initial research framework:
technological, operational, strategic, and financial
performance (see Table 1). In the coding process,
however, two of these categories were refined. As
cases were analyzed to identify actual motivations
leading to ERP adoption, a further breakdown of the
operational and strategic categories into both a
“managerial” and a “clinical” category was deemed
necessary. The success stories retrieved from the
ERP vendors’ websites were loaded as source
documents in the NVivo 9 software.
3.3 Methodological rigor
This study used public secondary data, noting that
this method has proven to be a valid source of
insights in previous information systems research
[e.g. 22, 32, 35]. Being publicly available and
accessible, these data are deemed to provide
confirmability to qualitative research [36, 37].
Although the study cannot claim to be a case survey,
our approach was guided by basic techniques of this
method, namely, selecting relevant cases from
inclusion criteria, developing a coding scheme to
convert qualitative case description into quantified
variables, and using multiple coders and assessing
inter-rater reliability [34].
The coding process was performed by two of the
four researchers. The cases recorded were randomly
subdivided into two equivalent parts, and each part
were independently analyzed and coded by one
coder. Certain measures were taken to ensure the
relative concordance of the coding process between
the two coders. First of all, the two coders used the
same previously described coding scheme. Second, a
pre-coding test was conducted by randomly selecting
ten stories. These were analyzed and coded
independently by the two coders, who then compared
and discussed their coding. This step allowed them to
harmonize their understanding of the different codes.
Third, at the end of the process, the two coders
worked together to harmonize the phrasing of
different codes and to group similar codes. Fourth, to
ascertain the validity of the coding process, each of
the two other researchers not involved in the
preceding steps independently coded 50 transcript
segments from the cases. Cohen’s kappa inter-coder
reliability coefficient was equal to 0.61 in the first
case and 0.74 in the second case, indicating
substantial agreement [38].
4. Results
As determinants of ERP adoption, motivations refer
to the initial reasons that led to the ERP adoption
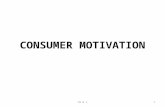
decision. Table 4 presents the most frequent
motivations found in the stories analyzed. Given the
limited richness of the information provided in the
stories by the ERP vendors, the various motivations
for the adoption of ERP systems identified within
each story were coded as 46 binary variables (1:
present, 0: absent). These include 7 technological
motivations, 9 managerial-operational, 12 managerial
-strategic, 10 clinical-operational, 4 clinical-strategic,
and 4 financial.
Table 4. Most Frequent Motivations (number of stories)
The hierarchy of the motivation categories stems
from the logic found in many of the stories, that is,
from the way ERP adoption motivations were
formulated. Consider the following transcripts from
case #29:
“We believed that rationalizing technology and
standardizing processes would enforce the
sharing of best practices across all therapy areas
and enable [our organization] to reduce

7
Number of ERP motivations
Business View
(n= 54) Clinical
View (n=34)
Institutional View
(n=92) F Technological motivations
Managerial operational motivations
Managerial strategic motivations
Clinical operational motivations
Clinical strategic motivations
Financial motivations
1.0
1.4
1.4
0.7
0.0
1.0
0.4
0.6
0.9
2.5
0.6
0.3
0.5
0.8
0.7
0.3
0.0
0.0
5.4**
8.9***
11.4***
62.6***
82.5***
115.2***
Total number of motivations 5.5 5.3 2.3 41.3***
operating costs through automation and shared
service centers.”
“We also wanted to build a scalable, flexible IT
environment that would allow [our organization]
to leverage its market-leading position and
continue generating strong cash flow and
profitable growth.”
It appears from these two transcripts that
technological motivations such as “rationalizing
technology” and “building a scalable, flexible IT
environment” were not the ultimate trigger of the
organization’s decision, but were deemed a necessary
condition for managerial performance (“automation
and shared service centers,” “leverage market-leading
position”), clinical performance (“sharing of best
practices across all therapy areas”), and financial
performance (“reduce operating costs,” “continue
generating strong cash flow and profitable growth”).
Another notable result lies in the frequency with
which certain types of ERP motivations are present in
the 180 stories examined. The most frequently
mentioned motivations pertain to managerial-
operational performance (in 84% of the cases). For
instance, “improving the effectiveness of managerial
processes” and “leveraging the ERP system to
improve performance management capabilities,”
mentioned in 88 and 30 cases respectively, are the
most frequently mentioned individual motivations in
this regard. Next in order of appearance are
motivations that pertain to clinical performance (in
44% of the cases) and to technological performance
(in 41%). Here, one finds “improving the
effectiveness and efficiency of the care provided to
patients” (in 44 cases) and “searching for IT
integration” (in 51 cases) as being the motivations
most often cited. The least frequent motivations are
the ones that pertain to financial performance (in
29% of the cases). Being present in 44 cases,
“monitoring cost trends” is the most prevalent
motivation of this last category.
To obtain further descriptive insights from the
stories, cluster analysis was used to group the
healthcare organizations on the basis of their
motivations for adopting ERP systems. This approach
aims to group organizations into clusters such that
each cluster’s membership is highly homogeneous
with respect to certain characteristics. A second aim
is that each group differs from other groups with
respect to these same characteristics. The number of
motivations of each type present in a story was
chosen here as clustering variables. The SPSS
TwoStep algorithm was used to identify clusters as it
can handle a large number of cases and has the ability
to determine the optimal number of clusters [39]. A
three-cluster solution was found to be optimal in
identifying groups of stories that could be clearly
distinguished from one another, based on an
interpretable and meaningful pattern of relationships
among the clustering variables.
As shown in Table 5, the three clusters of
healthcare organizations were labelled as having a
Business View (30% of the stories), a Clinical View
(19%), and an Institutional View of ERP systems
(51%). Significant differences between cluster means
for all clustering variables and for the organization’s
total number of motivations demonstrate the unique
character of each cluster.
Table 5. Cluster analysis of healthcare ERP stories by type of motivations
**: p < 0.01 ***: p < 0.001
The first group is comprised of healthcare
organizations whose motivations pertain more
significantly to managerial-operational as well as
managerial-strategic performance, technological
performance and financial performance than the other
two groups. As such, they are seen as taking a purely
“business” view of ERP system, i.e. the dominant
view propounded by the large ERP system vendors
such as Oracle, SAP and Microsoft, and adopted by
most firms in the manufacturing sector from which
ERP originated and where its market penetration is
the greatest. In contrast, the second group is made up
of organizations that look at ERP system offerings
from a more “clinical” perspective, that is, whose
motivations to adopt such a system pertain
significantly more to their core business, i.e. clinical
processes than the other two groups.
For its part, the third group stands as the one with
the least number of ERP adoption motivations,
whatever the type. For these healthcare organizations,
there is no specific type of motivations that seems to
play a central role in the ERP adoption decision.
These organizations are seen as following an
“institutional” perspective, referring to neo- institutional theory for which technology adoption is
a result of external or environmental pressures rather
than internal rational decisions or cognizant choices
by the organization’s management [40]. An
organization’s institutional context determines to
some extent the pressures it will undergo to align
itself either to common practices, often referred to as
“best practices” (a frequent argument for justifying

8
ERP adoption), or to legal and regulatory
requirements. This context will also force the
organization to adapt itself to the power shifts within
the various stakeholder groups in its immediate
environment.
A further characterization of the three groups of
healthcare organizations can be obtained by looking
at the different modules implemented within their
ERP system. Looking at Table 6, one may note that
organizations whose view of ERP is “clinical” tend to
implement clinical IS and clinical support modules in
greater proportion than the other two groups, as
expected. Conversely, the organizations with the least
motivations, that is, those whose view is labelled as
“institutional”, tend to implement patient
management system modules in lesser proportion.
However these organizations are the ones that have
most implemented administrative system modules,
that is, modules that are the most “generic” by ERP
standards and the least specifically related to the
healthcare sector.
Table 6. Breakdown of ERP modules by cluster
Cluster
Variable
Business
view (n= 54)
freq. (%)
Clinical
View (n=34)
freq. (%)
Institutional view (n=92) freq. (%)
χ2
ERP module
Administrative systems
Patient management systems
Clinical support systems
Clinical information systems
43 (30)
10 (46)
8 (22)
10 (26)
20 (14)
8 (36)
15 (42)
18 (48)
82 (56)
4 (18)
13 (36)
10 (26)
14.6***
11.4**
15.2***
26.7*** ***: p < 0.001
The three groups of healthcare organizations can
also be characterized by the vendor selected to
provide their ERP system. Here, as indicated in Table
7, one may note that healthcare organizations whose
view of ERP is “clinical” tend to select an ERP
provided by Cerner rather than the other two groups,
again a result that was to be expected.
Table 7. Breakdown of ERP vendors by cluster
Cluster
ERP vendor
Business
View (n= 54)
freq. (%)
Clinical
View (n=34)
freq. (%)
Institutional
View (n=92) freq. (%)
χ
2
Oracle
SAP
Cerner
Other
33 (33)
13 (34)
7 (19)
1 (20)
10 (10)
4 (11)
20 (54)
0 (0)
57 (57)
21 (55)
10 (27)
4 (80)
38.8***
***: p < 0.001
Now, one may also ascertain whether the
organizational context influences the motivations for
which healthcare ERP is adopted. Initial evidence
presented in Table 8 to this effect indicates that it is
with regard to technological and clinical performance
motivations that such influence occurs.
Specifically, it was initially found that the smaller
the size of the hospital or clinic (number of beds), the
more ERP is adopted for clinical reasons. Also,
healthcare organizations located in the United States
(49% of the cases) show less technological
motivations but more clinical motivations than those
located in other countries. The majority of American
stories relate the experience of hospitals who have
implemented an ERP provided by Cerner and meant
to support clinical processes primarily.
Table 8. Influence of organizational context on ERP adoption motivations
T M/O M/S C/O C/S F
Number of employees .03
-.06
.02
-.15
-.03
.10
Number of beds .05
.10
-.04
-.29**
-.15
.00
Country (1: USA, 0: other)
-.19*
.03
-.04
.18*
.14
-.04
Location (1: rural, 0: urban)
-.09
-.02
.08
-.08
-.02
.02
Tax status
(1: for profit, 0: other)
.21*
-.05
.03
-.15
-.14
-.14 Network affiliation
(1: yes, 0: no)
-.09
.07
-.04
.08
.12
.01 University affiliation (1: yes, 0: no)
-.22*
-.00
.03
.16
.02
.13
Type of organization
(1: hospital or clinic, 0: other)
-.25***
.00
-.05
-.24***
.14
.00
*** p < 0.001; ** p < 0.01; ; * p < 0.05
T=technological; M/O=managerial operational; M/S=managerial strategic; C/O=clinical operational; C/S=clinical strategic; F=financial
In terms of tax status and affiliation, not-for-profit
and university-affiliated health organizations show
less technological motivations than for-profit and
non-affiliated ones. As to the type of organization,
hospitals or clinics (66% of the cases) also show less
technological motivations but more clinical
motivations than other types of organizations.
5. Discussion
The results presented above indicate that the
performance motivations that underlie the adoption
of ERP systems in healthcare organizations are
technological, managerial-operational, managerial-
strategic, clinical-operational, clinical-strategic, and
financial in nature. These organizations differ
however as to whether the managerial or the clinical
benefits of ERP is the one that is privileged. Scholars
have previously stressed the importance of contextual
factors in order to fully understand technology
adoption processes [e.g. 41, 42]. Therefore, it is not
surprising that motivations related to clinical
performance emerge from our analysis at both the
operational and strategic levels, clinical activities
representing the “core business” of this industry.
Furthermore, it is worth noting that it is only in
the 1990s that healthcare organizations started to use
information systems for clinical purposes to improve
care services [43]. Consistent with this trend, our
results show a clear domination of motivations
related to managerial performance over clinical
performance. Indeed, at the operational level, one
may recall that the most frequent motivation is to
“improve administrative process effectiveness”
(expressed in 88% of the stories), as compared to
“improve the effectiveness and efficiency of care

9
provided to patients” (44%). The second-most
frequently mentioned motivation is related to
technological performance, that is, the “search for IT
integration” (51%). On this matter, it is worth
reminding that integration of business operations and
processes is one benefit of ERP that is highly-valued
by all types of organizations [44]. It is also worth
noting that frequently mentioned motivations such as
“monitor cost trends” (40%), “leverage the ERP
system to improve administrative performance
management capabilities” (30%), and “leverage the
ERP system to enhance compliance with applicable
laws and regulations” (30%) denote the influence of
the environmental context of healthcare
organizations. In fact, the healthcare industry is
characterized by a high level of regulatory and legal
requirements that can both accelerate and inhibit IT
adoption [45]. In addition, due to increasing level of
governmental as well as competitive pressures,
healthcare organizations are becoming more aware of
their need to improve overall performance and to
develop their performance management capabilities
[46, 47].
The preceding results concur with Caldas and
Wood’s [48] findings in that most motivations
reported by the sampled healthcare organizations are
“substantive” in nature, i.e. based on a “rational”
organizational expression of requirements and
problems for which ERP systems appear to be an
adequate solution. These authors note however that
substantive motivations are not the only ones that
come into play. Less evident (or less acceptable)
motivations of the institutional or the political type
may also be present. The former type refers to
external pressures that may be coercive, normative or
mimetic in nature, whereas the latter refer to power
and conflict within the organization. Given that such
motivations could not be detected with the data
collection method employed here, further research
should do well to look into the institutional and
political factors that may underlie the ERP adoption
in healthcare organizations.
In comparing our results with those of similar
studies conducted in other contexts, one must keep in
mind the limitation of such an exercise due to
difference in data collection methods. That being
said, healthcare organizations globally appear to be
driven by the same substantive motivations as
organizations in the private sector [15, 19, 20] and in
the public sector [23]. However, clinical performance
motivations at both the operational and the strategic
level are specific to organizations in the healthcare
sector. In addition, healthcare sector-specific
characteristics (e.g. financing systems, legislation,
regulatory requirements) imply that certain
motivations will have a greater impact than others,
when compared with the private or the public sector.
For example, the need to comply with legislation or
regulatory requirements is of paramount importance
in this industry.
The need for greater transparency and
accountability could also have more weigh in both
the healthcare and the public sectors when compared
to private enterprises. In line with Raymond et al.’s
[23] findings, one could assert that, contrary to
healthcare or governmental organizations, private
firms can be motivated to adopt an ERP system in
part by the need to reduce a competitive disadvantage
or to prevent a business risk from becoming critical
[19]. Conversely, private sector organizations would
most often not be motivated by pressures to join with
other organizations in an ERP implementation
project, as can be the case for healthcare and public
sector organizations.
As found above, three organizational profiles
were identified with regard to ERP adoption
motivations, that is, healthcare institutions were seen
as having a Business View, a Clinical View, or an
Institutional View of ERP systems. The first two
views are consistent with a rational perspective of
innovation adoption [49]. The emergence of the third
profile is rather surprising however, as it represents
about a half of the sampled organizations. While the
rational perspective of innovation adoption does not
apply to this group, another line of reasoning may be
of interest to these organizations. Contrary to
DiMaggio and Powell [50] for whom the “first
adopters” of an innovation are the ones motivated by
a desire to improve their performance, it stems from
our results that healthcare organizations in the third
group may have adopted an ERP system as a result of
environmental pressures, be them coercive or
normative, or by imitation, possibly following a
management “fashion wave” [51].
With regard to our third research aim, our results
indicate that five characteristics of the organizational
context (hospital or clinic size, country, tax status,
university affiliation and type of organization) play a
significant role in motivating the adoption of ERP
systems in the healthcare sector. First, organizational
size is one of the most widely investigated
antecedents of IT adoption in hospitals [52]. Our
results indicate that smaller organizations are
motivated more by improving their clinical
performance. While in contradiction with two
previous studies [e.g. 53, 54], this result may be
explained by an argument analogous to the one used
to characterize the greater “proximity” of small and
medium-sized enterprises to their clients [55]. Thus,
in the case of small and medium-sized hospitals, this

10
proximity would be achieved through improvements
in patient care enabled by an ERP system.
Another result worth discussing is the greater
emphasis on technological performance and the
lesser emphasis on clinical performance of the for-
profit healthcare organizations, as opposed to the not-
for-profit ones. Here, one clearly sees the former’s
“business” orientation of ERP as opposed to the
latter’s “clinical” orientation, wherein the adoption
behaviour of for-profit healthcare institutions would
more resemble that of other business corporations in
initially seeking the IT integration and improved IT
capabilities brought by implementing an ERP system.
In a similar fashion, university-affiliated
institutions tend to adopt more of a “clinical” rather
than a “business” orientation of ERP, that is, they are
more motivated by clinical performance, and less
motivated by technological performance than non-
affiliated institutions. Given the primary mission of
teaching hospitals, this last result is not surprising.
The same can be said of hospitals and clinics versus
other types of healthcare organizations as the latter
are mostly for-profit organizations. Overall, these
results confirm the importance of the organizational
context in determining why, in the healthcare sector,
organizations differ in their motivations to adopt an
ERP system.
In concluding this discussion, an obvious
limitation must be acknowledged in relation to this
study’s use of secondary data, that is, data initially
compiled for a different purpose than that of the
research. In using “success stories” published by ERP
vendors, one may be concerned with the inherent bias
in the selection and presentation of these stories for
publicity reasons. For instance, more space is given
to the benefits derived from the system and to the
reasons for choosing the vendor and the proposed
solution. Motivations for adoption are treated
incidentally, and difficulties or problems encountered
in adopting ERP are rarely mentioned. Hence, it
could reasonably be assumed that motivations in the
selected stories are less susceptible to distortion.
Finally, the terminology used in the stories varies
substantially from vendor to vendor, rendering
comparison more difficult.
6. Conclusion
In the present article, we have explored the key
motivations that underlie the adoption of ERP
systems in healthcare organizations. The research
contributions lie in a better understanding of the
reasons why healthcare organizations decide to
implement these systems. A thorough analysis of the
motivations of healthcare organizations would help
avoid what Markus and Tanis [56] called the
“bandwagon effect”, that is, adopting ERP systems
simply because other comparable organizations have
done so. Such analysis would also allow ERP
vendors to better define their strategies in order to
meet the expectations of healthcare organizations.
The popularity of ERP systems in private sector
combined with optimistic growth forecasts in the
healthcare segment within the IT market, lead one to
believe that the adoption of these systems in
healthcare organizations will continue to increase. As
the pressure from governments continues with regard
to efficiency and effectiveness, integrated systems
will be required in order to enable and better manage
processes in healthcare organizations, both upstream
and downstream, and without loss in the quality of
care provided to citizens. Alike other information
systems, ERP systems can provide benefits to
healthcare organizations; it has also shown that
realizing these benefits is not automatic and that the
risk of partial or total failure is still very high. Thus,
ERP adoption issues must be better understood in
light of fundamental differences in the various
organizational contexts that frame these issues, be
they represent differences between public and private
organizations, small and large organizations, or
service and manufacturing organizations.
7. References [1] Grimson, J., “Delivering the electronic healthcare
record for the 21st Century”, International Journal of Medical Informatics, 64, 2001, pp. 111–127.
[2] Paré, G. and Sicotte, C., “Information technology
sophistication in healthcare: an instrument validation study
among Canadian hospitals”, International Journal of
Medical Informatics, 63, 2001, pp. 205–223.
[3] World Bank, “Understanding organizational reforms:
The corporatization of public hospitals”, HNP discussion
paper, 2000. [4] Ashkenas, R., Ulrich, D., Jick, T. and Kerr, S., The
Boundaryless Organization, Jossey-Bass, San Francisco,
1995.
[5] Medicare Payment Advisory Council, Report to the
Congress: Medicare payment policy, 2006, http://www.
medpac.gov/documents/Mar06_EntireReport.pdf
[6] HIMSS, Annual Report of the US Hospital IT Market,
2005, http://www.himss.org/DorenfestInstitute/docs/
HIMSS AnalyticsAnnualReport.pdf (last accessed June 14, 2011).

11
[7] Pollock, N and Cornford, J., “Customizing industry
standard computer systems for universities: ERP systems
and the university as an ‘unique’ organisation”, Information
Technology & People, 17 (1), 2004, pp. 31-52.
[8] Davenport, T., “Putting the enterprise into the enterprise
system”, Harvard Business Review, 76 (4), 1998, pp. 121-
132.
[9] Dorobek, C.J., “ERP: It's not dead yet”, Federal
Computer Week, June 11, 2001, http://www.
fcw.com/fcw/articles/2001/0611/tec-erp06-11-01.asp.
[10] Wagner, E. L and Newell, S., “Repairing ERP:
Producing social order to create a working information
system”, Journal of Applied Behavioral Science, 42 (1),
2006, pp. 40-57.
[11] Kumar, V. and van Hillegersberg, J., “ERP
experiences and evolution”, Communications of the ACM,
43 (4), 2000, pp. 23-26.
[12] Marbert, V.A., Soni, A. and Venkataramanan, M.A., “
Enterprise resource planning survey of U.S. manufacturing
firms”, Production and Inventory Management Journal, 41
(2), 2000, pp. 52-58.
[13] Scavo, F. “The Enterprise System Spectator: ERP
Market on the Rebound”, http://fscavo.blogspot.com/2004/ 05/erp-market-on-rebound.html (last accessed on June 14,
2011).
[14] MarketsandMarkets, “Healthcare Information
Technology Systems market to be worth $53.8 billion by
2014”, 2009, http://www.marketsandmarkets.com/ PressReleases/healthcare-information-technology-systems-
market-worth-53.8-billion-by-2014.asp
[15] Parr, A.N. and Shanks, G., “A taxonomy of ERP
implementation approaches”, Proceedings of the 33rd
Hawaii International Conference on System Sciences,
2000.
[16] Akkermans, H. and van Helden, K., “Vicious and
virtuous cycles in ERP implementation: a case study of
interrelations between critical success factors”, European
Journal of Information Systems, 11, 2002, pp. 35–46.
[17] Trudel, M.C., Paré, G. and Laflamme, J., “Health
information technology success and the art of being
mindful: Preliminary insights from a comparative case
study analysis”, Health Care Management Review, 2011,
(forthcoming).
[18] Swanson, E.B. and Ramiller, N.C., “Innovating
mindfully with information technology”, MIS Quarterly, 28
(4), 2004, pp. 553-583.
[19] Oliver, D. and Romm, C., “Enterprise Resources
Planning: The route to adoption”, Proceedings of the 6th
Americas Conference on Information Systems, Long Beach,
California, 2000.
[20] Ross, J.W. and Vitale, M.R., “The ERP revolution:
Surviving vs. thriving”, Information Systems Frontiers, 2 (2), 2000, pp. 233-241.
[21] Blick, G., Gulledge, T. and Sommer, R., “Defining
business process requirements for large scale public sector
ERP implementations: A case study”, Proceedings of the
European Conference on Information Systems, Wirtschafts
Universität, Wien, 2000.
[22] Brown, M.M. and Brudney, J.L., “Public sector
information technology initiatives: Implications for
programs of public administration”, Administration &
Society, 30 (4), 1998, pp. 421-442.
[23] Raymond, L., Uwizeyemungu, S. and Bergeron, F.,
“Motivations to implement ERP in e-government: An
analysis from success stories”, Electronic Government, 3
(3), 2006, pp. 225-240.
[24] Allen, D., Kern, T. and Havenhand, M., “ERP critical
success factors: An exploration of the contextual factors in public sector institutions”, Proceedings of the 35th Hawaii
International Conference on System Sciences, 2002.
[25] Chang, S.I., Gable, G., Smythe, E. and Timbrell, G.
“A Delphi examination of public sector ERP
implementation issues”, Proceedings of the Twenty First
International Conference on Information Systems,
Brisbane, Queensland, Australia, 2000, pp. 494-500.
[26] Heintze, T. and Bretschneider, S., “Information
technology and restructuring in public organizations: Does
adoption of information technology affect organizational
structures, communications, and decision making?”,
Journal of Public Administration Research and Theory, 10
(4), 2000, pp. 801-830.
[27] Uwizeyemungu, S. and Raymond, L., “Exploring an
alternative method of evaluating the effects of ERP: a
multiple case study”, Journal of Information Technology,
24 (3), pp. 251-268.
[28] Boonstra, A. and Govers, M., “Understanding ERP
system implementation in a hospital by analysing
stakeholders”, New Technology, Work and Employment, 24
(2), 2009, pp. 177-193.
[29] Huq, Z. and Martin, T.N., “The recovery of BPR
implementation through an ERP approach: A hospital case
study”, Business Process Management Journal, 12 (5),
2006, pp. 576 – 587.
[30] McGinnis, S.K., Pumphrey, L.D., Trimmer, K.J. and
Wiggins, C., “A case study in IT innovation in a small,
rural community hospital”, Research in Healthcare
Financial Management, 9 (10), 2004, pp. 9-21.

12
[31] Stefanou, C.J. and Revanoglou, A., “ERP integration
in a healthcare environment: A case study”, Journal of
Enterprise Information Management, 19 (1), 2006, pp. 115-
130.
[32] Shang, S. and Seddon, P.B., “A comprehensive framework for classifying the benefits of ERP systems”,
Proceedings of the 6th Americas Conference on Information Systems, Long Beach, California, 2000.
[33] Oliver, D. and Romm, C., “Justifying enterprise
resource planning adoption”, Journal of Information
Technology, 17, 2002, pp. 199-213.
[34] Yin, R.K. and Heald, K.A., “Using the case survey
method to analyze policy studies”, Administrative Science
Quarterly, 20 (3), 1975, pp. 371-381.
[35] Seddon, P. B., Calvert, C. and Yang, S., “A multi-
project model of key factors affecting organizational
benefits from enterprise systems”, MIS Quarterly, 34 (2),
2010, pp. 305-328.
[36] Cousins, K. C. and Robey, D., “The social shaping of electronic metals: An institutional theory perspective”,
Information Technology & People, 18 (3), 2005, pp. 212- 229.
[37] Miles, M.B. and Huberman, A.M., Qualitative Data
Analysis, 2nd edition, Sage Publications, Thousand Oaks,
California, 1994.
[38] Menold, N., “How to use information technology for cooperative work: Development of shared technological
frames”, Computer Supported Cooperative Work, 18 (1), 2008, pp. 47–81.
[39] Zhang, T., Ramakrishnon, R., and Livny, M.,
“BIRCH: An efficient data clustering method for very large
databases”, Proceedings of the ACM SIGMOD Conference
on Management of Data., Montreal, 1996, pp. 103-114.
[40] Tsikriktsis, N., Lanzolla, G. and Frohlich, M.,
“Adoption of e-processes by service firms: An empirical
study of antecedents”, Production and Operations
Management, 13 (3), 2004, pp. 216-229.
[41] Rogers, E. M., Diffusion of Innovations, 5th edition,
Free Press, New York, 2003.
[42] Tornatsky, L. and Fleischer, M., The Processes of
Technological Innovation, Lexington Books, New York,
1990.
[43] Anderson, J.G. “Clearing the Way for Physicians’ Use
of Clinical Information Systems”, Communications of the
ACM, 40 (8), 1997, pp.83-90.
[44] Marbert, V.A., Soni, A. and Venkataramanan, M.A.,
“Enterprise resource planning: Measuring value”,
Production and Inventory Management Journal, 42
(3/4), 2001, pp. 46-51.
[45] Robert Wood Johnson Foundation. Health Information
Technology in the United States: The Information Base for Progress, 2006, http://www.rwjf.org/files/publications/
other/HER Report0609.pdf (last accessed June 14, 2011).
[46] Information Base for Progress, Health Information
Technology in the United States, 2006,
http://www.rwjf.org/files/publications/other/EHRReport06
09.pdf.
[47] Raju, P.S. and Lonial, S.C. (2002), “The impact of
service quality and marketing on financial performance in
the hospital industry: an empirical examination”, Journal of
Retailing and Consumer Services, 9 (6), 2002, pp. 335-348.
[48] Caldas, M.P. and Wood Jr. T., “How consultants can
help organizations survive the ERP frenzy”, Academy of
Management Annual Meeting, Chicago, August 6-11, 1999,
http://www.gv.br/prof_alunos/ thomaz/ingles/paper6.tm.
[49] Birkinshaw, J.M., Hamel, G. and Mol, M.,.
“Management innovation”, Academy of Management
Review, 33 (4): 2008, pp. 825-845.
[50] DiMaggio, P.J. and Powell, W.W., “The iron cage
revisited: Institutional isomorphism and collective
rationality in organizational fields”, American Sociological Review, 48, 1983, pp. 147-160.
[51] Baskerville, R.L. and Myers, M.D., “Fashion waves in
information systems research and practice”, MIS Quarterly, 33 (4), 2009, pp. 647-662.
[52] McCullough J.S. “The Adoption of Hospital
Information Systems”, Health Economics, 17, 2008, pp.
649–664.
[53] Hikmet, N., Bhattacherjee, A., Menachemi, N.,
Kayhan, V.O. and Brooks, R. G., “The role of
organizational factors in the adoption of healthcare
information technologies in hospitals,” Healthcare
Management Science, 11 (1), 2008, pp. 1-9.
[54] Paré G, Jaana M. and Sicotte C., “Exploring health
information technology innovativeness and its antecedents
in Canadian hospitals”, Methods of Information in
Medicine, 49 (1), 2010, pp. 28-36.
[55] Ramsey, E., Ibbotson, P. and McCole, P., “Factors that
impact technology innovation adoption among Irish
professional service sector SMEs”, International Journal of
Innovation Management, 12 (14), 2008, pp. 1-26.
[56] Markus, L.M. and Tanis, C., “The enterprise system
experience: from adoption to success”, in Framing the
domain of IT management: Projecting the future…through
the past, Zmud, R.W. (ed.), Pinnaflex Education Resources,
Cincinnati, Ohio, 2000, pp. 173-207.