Motivation in Addiction Medicine Practice Psychotherapy in Small Doses James Finch, MD Governor’s...
54
Motivation in Addiction Medicine Practice Psychotherapy in Small Doses James Finch, MD Governor’s Institute on Substance Abuse Changes By Choice, Durham, NC
-
Upload
diana-johnston -
Category
Documents
-
view
216 -
download
0
Transcript of Motivation in Addiction Medicine Practice Psychotherapy in Small Doses James Finch, MD Governor’s...

Motivation in Addiction Medicine Practice
Psychotherapy in Small Doses
James Finch, MD
Governor’s Institute on Substance Abuse
Changes By Choice, Durham, NC
Objectives
Define a time efficient, motivational approach to the Addiction Medicine encounter.
Define a reasonable “standard of care” for brief MAT follow-up visits.
Outline basic elements of “psychotherapy” as they apply to this time-limited but longitudinal setting.
Describe what we can learn and apply from Cognitive Behavioral and Motivational approaches.

“Two-year experience with buprenorphine-naloxone for maintenance treatment of opioid-dependence within a private practice setting”
• Office based setting • Mid-size urban community sample in North Carolina• Mixed prescription opioid and illicit opioid dependent patients• Minimal staff resources (solo practice)• Standard visits: 45-60 min initial, 15-20 min follow-up• Used standard community referral resources
Finch JW, Kamien KB, Amass L, J of Addiction Medicine, 2007.
Clinical Sample (n=71)
Patient Characteristics: Age: 16-62 (mean 32) Gender: 69% male Employed: 70%
Opioid dependence history: Heroin: 51% Prescription analgesics: 49% Years of dependence: 1-18 (mean 4.3)
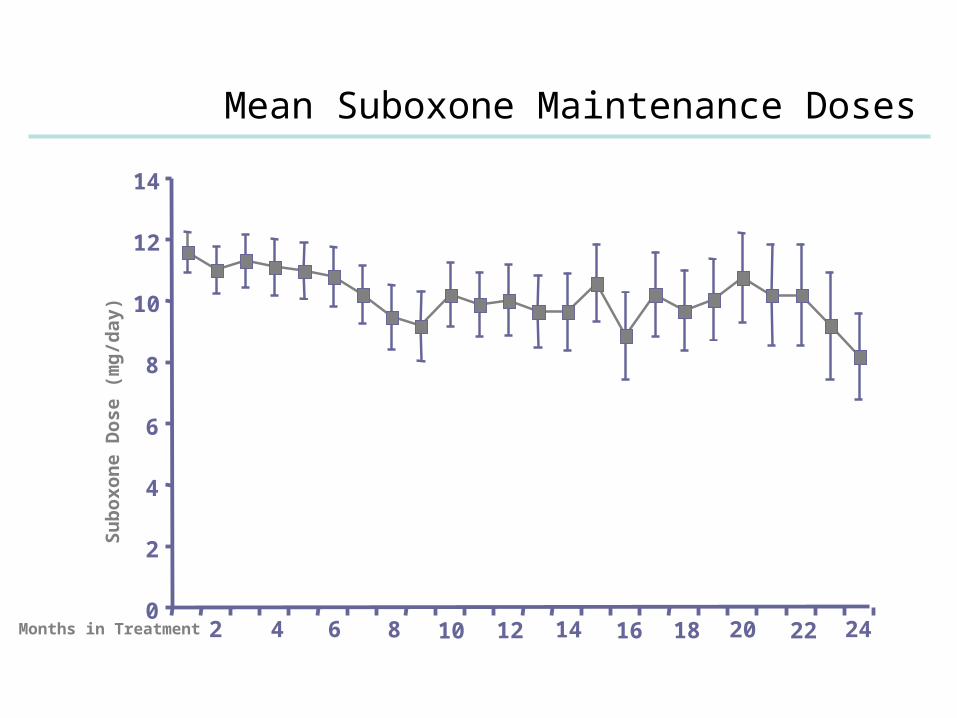
Mean Suboxone Maintenance Doses
Months in Treatment0
2
4
6
8
10
12
14
2 4 6 8 10 12 14 16 18 20 22 24
Su
boxon
e D
ose (
mg
/day)

Rates of Opioid Abstinence
0%
20%
40%
% N
eg
ati
ve
0%
20%
40%
60%
80%
100%
1 2 3 4 6 8 10 12 14 16 18 20 22 24Treatment Month
% N
eg
ati
ve 2 tests/month
Pre

Participation in counseling
Overall rate of involvement in supportive psychosocial therapy: 58%
Kinds of supportive counseling:
Individual or group: 68% Psychiatric follow-up/med mgmt: 29% Drug treatment program: 7% Peer support/12 Step: 2%
The “COMBINE” Study
Combined Pharmacotherapies and Behavioral Interventions for Alcohol Dependence: A Randomized Controlled Trial
Anton, RF, O’Malley, SS, et al. JAMA, May 2006
Groups randomized to med management with naltrexone, acamprosate, both and/or both placebos, with or without a combined behavioral intervention (CBI). One group with CBI only.
Evaluated for up to one year after treatment.

The Combine Study: Outcomes
Patients receiving medical management with naltrexone, CBI or both fared better on drinking outcomes.
No combination produced better efficacy than naltrexone or CBI alone in the presence of medical management.
Placebo pills and meeting with a health care professional had a positive effect above that of CBI alone during treatment.
Medical Management (MD, RN, PA): Initial 45 min visit, followed by 20 min visits, on week 1 and 2 and then every 2 to 4 weeks.

Medication Assisted Treatment for Primary Addiction Treatment
Demonstrated efficacy and FDA approval: Alcohol:
disulfiram, naltrexone, acamprosate Nicotine:
nicotine replacement, buproprion, varenicline Opioids:
agonist: methadone, buprenorphine/naloxone antagonist: naltrexone
Investigational but preliminary findings of efficacy: Cannabinoids Cocaine and other stimulants

Routine Elements of Medication Assissted Treatment (MAT) Follow-up
Assess response to med: Efficacy/Side-Effects
Assess abstinence (primary and other drugs)
Assess overall stability (bio/psycho/social)
Reinforce participation in counseling/peer-support
Problem solve/provide advice/support recovery

Roles of the Addiction Medicine Physician in Relation to Counseling
Apply knowledge of therapeutic alternatives available for referral
Understand and support the elements of cognitive behavioral therapy and peer-support
Apply counseling skills within the setting of the medical encounter

Psychosocial Therapeutic Support Alternatives
Mutual peer-support groups Faith-based support groups Individual and/or group therapy Cognitive Behavioral Therapy (CBT) Motivational Enhancement Therapy Incentive Based Therapy Coping Skills Development (DBT) Trauma Processing Therapies (EMDR) Anger Management Therapies Relaxation/Meditation
Common Elements of CBT for Substance Abuse
1. Drug Refusal Skills Training 2. Managing Negative Thinking 3. Managing Thoughts About Using 4. Managing Negative Moods and Depression 5. Effective Problem Solving 7. Seemingly “Irrelevant” Decisions 8. Alcohol and Other Drug Use 9.Coping with Anger 10.Progressive Muscle Relaxation/Meditation11.Managing Insomnia12.Giving and Receiving Criticism 13.Sharing Feelings 14.Vocational Counseling 15.Financial Management 16.Time Management 17.Relationship Counseling18.Taking Responsibility for Choices

Potential counseling roles for the medical clinician
Psychotherapist Counselor Coach Guide
Do we want to take on a counseling role? Do we want to stay in a traditional medical role?

Types of Power for Behavior Change Inherent in the Clinical Encounter
Reward: ability to give people what they want or need
Coercive: disapproval, denying requests, not seeing
Referent: the “admired other”, role-model
Legitimate: validated authority
Expert: access to knowledge, training, information

5 Basic Elements of Psychotherapy
Expectation of receiving help Therapeutic relationship Obtaining external perspective Encouraging corrective experiences Opportunity to test reality

“Psychotherapy means a form of treatment of mental illness or emotional disorders which is based primarily on verbal interaction with the client.”
NC Dept MH/DD/SAS
“the efficacy of psychotherapeutic methods lies in the shared belief of the participants that these methods will work.”
JD Frank

Core Elements of CBT: Recognize/Avoid/Cope
Recognize: triggers/cues (external/internal)
Anticipate/Avoid: (situations/people/places)
“People/Places/Things”
“Playmates/Playgrounds/Playthings”
“Play the tape to the end.”
“It is easier to avoid temptation,
than to resist temptation”.

Core Elements of CBT:Recognize/Avoid/Cope
Cope: develop or reinforce skills:
Explore other ways to relax/deal with stress/problem solve
Re-expand dormant behavioral options to socialize/have fun
Connect/re-connect with sources of reward
and “hedonic tone”
“Who needs life when you’ve got heroin.” (Trainspotting)
Rebuild/Reward

“How come if alcohol kills millions of brain cells, it never killed the ones that made
me want to drink?”
Anonymous

Editing the Patient’s “Story”
The language of the story: generalizations/delitions/distortions
Therapeutic interventions:
Challenging “learned helplessness”
Reinforcing the power of “yet”
Supporting “self-efficacy”


MotivationaI Interviewing (MI) aims to help the client…
Enhance intrinsic motivation for change (mobilize client’s own change resources)
Recognize the need to do something about the current or potential problem
Resolve ambivalence and reach a decision for change
Build commitment to change

Nn
Transtheoretical Model
Determination
Relapse
Pre-contemplation
Contemplation
Maintenance
Action
Termination
SynonymsDetermination = Preparation
Termination = ExitProchaska and DiClemente
Continuum of Communication Styles
Directing Guiding
Following
Directing
PrescribeTellShow the wayLeadManagePoint towardConduct SteerDetermine
Take commandPresideRuleTake chargeAuthorizeGovernTake the reinsPushAdminister

Following
ListenAttendUnderstandObserveTake inBe responsiveTrustGo along
Be withShadowPermitAllowSupportHave faith in

Guiding
EnlightenEncourageMotivateAwakenLay beforeCollaborateInvolve
Take alongLook afterAccompanyElicitEvokeOffer optionsInvite
In practice and in management…
There is an appropriate role for directingThere is an appropriate role for followingBut when your goal is behavior change, the optimal style
is usually guiding
William Miller
A Guiding Style…
Reduces resistance (relative to a directing style)Improves working allianceEnhances openness to consider changeFacilitates behavior changeIncreases self-regulation and internalization of
change
“More like dancing than wrestling.” William Miller
Two Stages of Motivational Interviewing
Phase 1: Building Motivation for Change
Phase 2: Strengthening Commitment to Change

Four Basic Principles
Express Empathy Focus on understanding the person’s dilemma
Roll with Resistance Don’t be the one arguing for change
Develop Discrepancy Evoke the person’s own arguments for change

Support Self-Efficacy Encourage belief that change is possible

Change Talk
Change talk is any client speech that favors movement in the direction of change
Previously called “self-motivational statements”
Change talk is by definition linked to a particular behavior change target

Preparatory Change Talk
DESIRE to change (want, like, wish . . ) ABILITY to change (can, could . . ) REASONS to change (if . . then) NEED to change (need, have to, got to)

Sustain Talk
The other side of ambivalence.
I really like alcohol/oxy/weed I don’t see how I could give it up I need to use to be social I intend to keep using/no one can stop me I don’t think I have to quit I can drink/use once in a while

Implementing Change Talk
Reflects resolution of ambivalence.
COMMITMENT (intention, decision, readiness)
ACTIVATION (willing, trying, preparing) TAKING STEPS










Resources
Motivational Interviewing by William Miller CSAT TIP 35: Enhancing Motivation for Change in
Substance Abuse Treatment The 15 Minute Hour by Stuart and Lieberman Treating Alcohol Dependence: A Coping Skills
Training Guide by Monti, et al. www.SA4Docs website ASAM trainings and involvement
“…alcoholics recover not because we treat them but because they heal
themselves.”
George Vaillant
The Natural History of Alcoholism, 1983

You can’t always get what you want…
But if you try sometimes…
You get what you need.
Mick Jagger, The Rolling Stones, 1969
JWF: The Vintage Image Gallery
JWF: The Vintage Image Gallery