Morphological and immunohistochemical analysis in ovaries and fallopian tubes of tamoxifen,...
7
1 3 Arch Gynecol Obstet DOI 10.1007/s00404-014-3234-4 GYNECOLOGIC ONCOLOGY Morphological and immunohistochemical analysis in ovaries and fallopian tubes of tamoxifen, letrozole and clomiphene‑treated rats Suzanne Lima · Alix Clemenson · Beatrice Trombert · Romain Lecointre · Claude‑Regis Lacoste · Michel Peoc’h · Gautier Chene Received: 12 October 2013 / Accepted: 24 March 2014 © Springer-Verlag Berlin Heidelberg 2014 Results Histopathological lesions were found in both ova- ries and tubes. The mean ovarian dysplasia score was sig- nificantly higher in the tamoxifen group whatever the dos- age (p = 0.006 and 0.0002) and in the letrozole group with 0.5 mg/kg/day (p = 0.0002) compared with the control group. The mean tubal dysplasia score was significantly higher in all groups that received drug treatment compared with the control group, whatever the dosage used. The proliferation index (Ki67) was significantly higher in the tamoxifen and letrozole groups while no significant differ- ence was found for apoptosis marker p53. Conclusions Ovulation induction may induce histopatho- logical abnormalities in ovaries and tubes with a different immunohistochemical profile in comparison with salpingo- oophorectomies for genetic risk. Keywords Ovulation stimulation · Ovarian dysplasia · Ki67 expression · p53 expression · Clomid · Tamoxifen Introduction Hereditary predisposition is one of the most important risk factors for breast and ovarian cancers, and concerns between 5 and 10 % of all ovarian cancers [1, 2]. Micro- scopic analysis of materials from oophorectomies for genetic risk may reveal histopathological abnormalities termed “ovarian epithelial dysplasia”, by analogy with other precancerous lesions of the genital tract [3–5]. The hypothesis of a tubal origin in the genesis of ovarian cancer was recently suggested, following the discovery of tubal lesions (serous tubal intraepithelial lesions or STIL, tubal dysplasia and serous tubal intraepithelial carcinoma or STIC) in women carrying a BRCA mutation [6–8]. Tubal ligation leads directly to a risk reduction of ovarian cancer. Abstract Purpose Ovarian and tubal dysplasia may be precursors to ovarian cancer. The goal of this study was to check whether these histopathological lesions would be found after ovulation induction using tamoxifen, clomiphene citrate and letrozole. Methods Seventy-two rats were divided into four groups. In the first group, 24 rats received normal saline. The sec- ond group (16 rats) received clomiphene citrate for six cycles. The third group, divided into two sub-groups of eight rats each, were stimulated with tamoxifen for six cycles, with a dosage, respectively, of 0.4 and 0.8 mg/kg/ day. In the last group, eight rats received letrozole 0.1 mg/ kg/day and eight other rats received letrozole 0.5 mg/kg/ day, for six cycles. Once the six cycles had been completed the rats were killed in order to remove ovaries and tubes for histopathological analysis (morphological, p53 and Ki67 immunohistochemical assessment). S. Lima · C.-R. Lacoste · G. Chene Department of Obstetric, Gynecology and Reproductive Medicine, CHU Nord, 42000 St Etienne, France A. Clemenson · M. Peoc’h Department of Histopathology, CHU Nord, 42000 St Etienne, France B. Trombert Department of Medical Information, CHU Nord, 42000 St Etienne, France R. Lecointre Department of Pharmacy of Clinical Oncology, Lyon Sud Hospital, 69000 Lyon, France G. Chene (*) Department of Gynecology, HFME, Hospices Civils de Lyon, 69000 Lyon, France e-mail: [email protected]
Transcript of Morphological and immunohistochemical analysis in ovaries and fallopian tubes of tamoxifen,...

1 3
Arch Gynecol ObstetDOI 10.1007/s00404-014-3234-4
GynecOlOGIc OncOlOGy
Morphological and immunohistochemical analysis in ovaries and fallopian tubes of tamoxifen, letrozole and clomiphene‑treated rats
Suzanne Lima · Alix Clemenson · Beatrice Trombert · Romain Lecointre · Claude‑Regis Lacoste · Michel Peoc’h · Gautier Chene
Received: 12 October 2013 / Accepted: 24 March 2014 © Springer-Verlag Berlin Heidelberg 2014
Results Histopathological lesions were found in both ova-ries and tubes. The mean ovarian dysplasia score was sig-nificantly higher in the tamoxifen group whatever the dos-age (p = 0.006 and 0.0002) and in the letrozole group with 0.5 mg/kg/day (p = 0.0002) compared with the control group. The mean tubal dysplasia score was significantly higher in all groups that received drug treatment compared with the control group, whatever the dosage used. The proliferation index (Ki67) was significantly higher in the tamoxifen and letrozole groups while no significant differ-ence was found for apoptosis marker p53.Conclusions Ovulation induction may induce histopatho-logical abnormalities in ovaries and tubes with a different immunohistochemical profile in comparison with salpingo-oophorectomies for genetic risk.
Keywords Ovulation stimulation · Ovarian dysplasia · Ki67 expression · p53 expression · clomid · Tamoxifen
Introduction
Hereditary predisposition is one of the most important risk factors for breast and ovarian cancers, and concerns between 5 and 10 % of all ovarian cancers [1, 2]. Micro-scopic analysis of materials from oophorectomies for genetic risk may reveal histopathological abnormalities termed “ovarian epithelial dysplasia”, by analogy with other precancerous lesions of the genital tract [3–5]. The hypothesis of a tubal origin in the genesis of ovarian cancer was recently suggested, following the discovery of tubal lesions (serous tubal intraepithelial lesions or STIl, tubal dysplasia and serous tubal intraepithelial carcinoma or STIc) in women carrying a BRcA mutation [6–8]. Tubal ligation leads directly to a risk reduction of ovarian cancer.
Abstract Purpose Ovarian and tubal dysplasia may be precursors to ovarian cancer. The goal of this study was to check whether these histopathological lesions would be found after ovulation induction using tamoxifen, clomiphene citrate and letrozole.Methods Seventy-two rats were divided into four groups. In the first group, 24 rats received normal saline. The sec-ond group (16 rats) received clomiphene citrate for six cycles. The third group, divided into two sub-groups of eight rats each, were stimulated with tamoxifen for six cycles, with a dosage, respectively, of 0.4 and 0.8 mg/kg/day. In the last group, eight rats received letrozole 0.1 mg/kg/day and eight other rats received letrozole 0.5 mg/kg/day, for six cycles. Once the six cycles had been completed the rats were killed in order to remove ovaries and tubes for histopathological analysis (morphological, p53 and Ki67 immunohistochemical assessment).
S. lima · c.-R. lacoste · G. chene Department of Obstetric, Gynecology and Reproductive Medicine, cHU nord, 42000 St etienne, France
A. clemenson · M. Peoc’h Department of Histopathology, cHU nord, 42000 St etienne, France
B. Trombert Department of Medical Information, cHU nord, 42000 St etienne, France
R. lecointre Department of Pharmacy of clinical Oncology, lyon Sud Hospital, 69000 lyon, France
G. chene (*) Department of Gynecology, HFMe, Hospices civils de lyon, 69000 lyon, Francee-mail: [email protected]

Arch Gynecol Obstet
1 3
A recent meta-analysis of tubal ligation and ovarian cancer found a 34 % reduction in risk, essentially for endometrioid (RR = 0.4) and serous (RR = 0.73) cancers [9], suggesting that surgical strategy (i.e., prophylactic bilateral salpingec-tomy) could have significant implications.
More recently, other works have reported that ovarian dysplastic lesions have been found in oophorectomy speci-mens after ovarian hyperstimulation in a context of in vitro fertilization (IVF) protocols [10, 11]. The possibility that tubal dysplasia might exist in women who have undergone induced ovulation was also raised [12, 13].
little is known about the association between dysplas-tic lesions and the use of tamoxifen or letrozole to induce ovulation. These two drugs are frequently used as adjuvant treatment for breast cancer, despite the fact they have a clo-mid-like effect. They are also used instead of clomiphene citrate to treat infertility by some teams [14, 15].
We propose a morphological and immunohistochemical study of ovaries and tubes exposed to ovulation stimulation protocol using tamoxifen, letrozole and clomiphene citrate in the rat.
Materials and methods
This study was carried out between September and Octo-ber 2010 in the Jacques lisfranc Faculté de Médecine Animal experiment center (PleXAn) in Saint etienne. Institutional Review Board (IRB) approval was previ-ously obtained from the Auvergne Animal experiment ethics committee (ceMeA Auvergne) in accordance with european regulations applicable to animal experi-ments (Official Journal of the european community dated 12-18-1986).
experimental protocol
Seventy-two female Wistar Han rats (age 70 days, weight between 220 and 240 g and with regular oestrus cycles) were used in this study. The rats were housed in the Jacques lisfranc Faculty of Medicine Animal centre in Saint etienne. Two rats were kept in each cage under controlled light and temperature conditions. They had free access to food and water.
The animals were subjected to cycles of ovarian stimu-lation using different ovulation inducers and were divided into four groups:
• control group: this group received normal saline and a dosage of 2.5 ml/kg/day: 24 rats.
• clomid group: group stimulated using clomiphene cit-rate (clomid®; Sanofi-Aventis): 1 mg/kg/day for the first 2 days of the cycle (D1 and D2) and HcG (Preg-
nil®; Schering-Plough): 100 UI/kg on the third day of the cycle (D3): 16 rats.
• Tam group: group stimulated using tamoxifen (nolva-dex®; AstraZeneca): 16 rats split into two sub-groups of 8 rats each: Tam 0.4 (nolvadex®: 0.4 mg/kg/day) and 0.8 (nolvadex®: 0.8 mg/kg/day).
• let group: group stimulated using letrozole (Femara®; novartis Pharma SA): 16 rats split into two sub-groups of eight rats each: let 0.1 (Femara®: 0.1 mg/kg/day) and 0.5 (Femara®: 0.5 mg/kg/day).
The oestrus cycle lasted 4 days on average. Various drugs were administered on the first 3 days of the cycle (D1, D2 and D3) with a therapeutic interruption on the fourth day, corresponding to the last day of the cycle (D4). The same ovulation induction programme was used for six cycles. each day the clomiphene citrate, tamoxifen and letrozole were diluted in normal saline and administered by intraperitoneal injection. normal saline was also adminis-tered by intraperitoneal injection in the control group. At the end of the six ovulation induction cycles the rats were anaesthetised by intraperitoneal administration of ketamine (2 ml/kg).
each animal was installed on its back and careful asep-sis of the abdominal region was carried out using normal saline; then a vertical midline incision was made to give access to the pelvic organs. The salpingo-oophorectomies were carried out according to a standard procedure in all the groups on the same day. Rats were then killed using a lethal injection of pentobarbital.
Histopathological analysis
The tubes and ovaries resected were placed immediately in a 10 % formol solution and then embedded in paraf-fin. Sections 4–5 μm thick were made using a microtome, placed on slides and then coloured using standard H and e (hematoxylin–eosin) staining. The histology slides were examined by two expert gynaecological pathologists (Ac and MP) using an optical microscope.
A specific scale for epithelial ovarian dysplasia and tubal dysplasia previously described in the literature was used for histopathological ovarian and tubal analysis [13, 16–18].
The ovarian score was based on the 11 following items:
• epithelial multilayering• epithelial proliferation• surface papillomatosis• nuclear chromatin irregularity• nuclear contour irregularity• cellular pleomorphism• nuclear size enlargement• epithelial inclusion cysts

Arch Gynecol Obstet
1 3
• cortical invaginations• psammoma• stromal hyperplasia
The tubal score was based on the seven following items:
• epithelial multilayering• tufting• increased nuclear density• nuclear atypia• loss of nuclear polarity• nuclear size enlargement• loss of ciliation
In each case, the most representative area was given a score between 0 and 2 (0 = normal, 1 = moderately abnor-mal, 2 = severely abnormal).
For each rat, an ovarian score was obtained by summing the scores of the 11 ovary items (0–22) and a tubal score was calculated by summing the scores for the 7 tube items (0–14). All the slides were evaluated in a blinded order (Figs. 1, 2).
For the immunohistochemical analysis (Figs. 3 and 4), the 4 to 5 mm sections were processed automatically (Benchmark XT Ventana® automated slide preparation sys-tem) after elimination of paraffin at 75 °c. The standard preliminary treatment for antigen unmasking was applied for 60 min at 95 °c. The monoclonal antibodies used were anti-rat Ki67/MIB5 antibodies (Dako®, France, 1:20 dilu-tion), antibody anti-p53 (Dako®, France, 1:80 dilution). Incubation took place at 37 °c for 48 min. After rinsing, the ultraView universal DAB (Ventana Medical Systems®) revelation system was used.
The slides were read under the same conditions as described above for the morphological analysis.
To assess the Ki67 immunohistochemical staining, we proposed a scale suitable for preliminary screening of all the slides. For the follicles, marking was assessed according
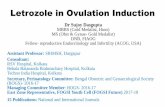
Fig. 1 Surface papillomatosis, H and e ×5
Fig. 2 epithelial multilayering, H and e ×20
Fig. 3 High Ki67 immunohistochemical expression

Arch Gynecol Obstet
1 3
to the number of follicles marked for each ovary (1, 2 or 3). For the stroma and ovarian surface layer, the intensity of marking was assessed on the basis of the number of nuclei marked per field: none (0), up to 5 nuclei (1+), 6–10 nuclei (2+), 11 or more nuclei (3+). concerning the proliferation sectors on the ovarian surface identified during morpholog-ical examination, marking was binary (0 no marking, 1+ presence of nuclear marking).
For the tubes, the score applied was the following: no marking (0), 1–9 nuclei per field (1+), 10–30 nuclei (2+), more than 30 nuclei (3+).
In addition, p53 staining was assessed on the follicles, stroma, ovarian surface epithelium together with the prolif-eration areas identified by simple morphological analysis, and the tube. The same score was used for all these sites: 0, 1, 2 or 3 crosses according to the intensity of staining (none, slight, intense, very intense).
Statistical analysis
The mean ovarian and tubal scores represent the main measurements made in this study, the assumption being that ovaries and tubes of rats exposed to ovulation stimu-lating treatment would be associated with higher dysplasia scores than in of the control group.
each treated group was compared to the control group and then the treated groups were also compared to each other. Mean values were compared using Student’s para-metric test. The level of statistical significance was set at 5 %.
Statistical measurements were made using SAS (version 9.2) software, by the staff in the Public Health and Medical
Information Department of Saint etienne University Hospi-tal centre.
Results
The mean surface of the ovaries of the rats in each group is shown in Table 2. This was significantly greater for the clomid, let 0.1 and 0.5 groups compared with the control group. However, the ovarian surface area of the tamoxifen group did not differ from that of the control group.
no cancer was observed in our seriesA mean ovarian score was calculated for each group.
The mean scores are shown in Table 1. The mean ovarian scores were significantly higher in the tamoxifen group and in the letrozole group in comparison with the control group. There was no difference between the Tam 0.4 and 0.8 groups. The ovarian score in let 0.5 was statistically higher than in let 0.1 group (p = 0.025).
Analysis of the histopathological abnormalities revealed more pronounced modifications in the stimulated groups. All the data are in Table 2.
A mean tubal score was calculated for each group. The mean tubal score was significantly higher in all the treated groups compared with the control group, whatever the dos-age. There was not any statistical difference between Tam 0.4 and 0.8 and, on the other hand, between let 0.1 and 0.5. Data are shown in Table 3.
close analysis of the histopathological abnormalities revealed more pronounced modifications in the stimulated groups. Histopathological abnormalities were extremely rare in the control rats, except for epithelial multilayering which was found in 66.6 % of cases. All the data are in Table 4.
cells expressing Ki67 were found in the ovarian epithe-lium, follicles, stroma and tubes. Follicular cells in devel-oping follicles presented significantly higher immunoreac-tivity in all stimulated groups compared with the control group (p < 0.05).
At stromal level, Ki67 expression was significantly higher for ovaries after stimulation than in the controls.
Fig. 4 p53 immunohistochemical expression
Table 1 Mean ovarian dysplasia score
Group Mean score comparison with the control group
control 1.2
clomid 1.6 nS
Tam 0.4 3.38 p = 0.006
Tam 0.8 4 p = 0.0002
let 0.1 1.88 nS
let 0.5 3.88 p = 0.0002

Arch Gynecol Obstet
1 3
The epithelial surface of the ovary presented signifi-cantly moderate expression in all stimulated groups com-pared with the control group (p < 0.05).
Ki67 expression remained comparable with that in the control group, whatever the number of stimulation cycles.
concerning the tubes, the difference between the stimu-lated groups and controls was significant for stimulated groups.
p53 appeared to be low expressed in all the stimulated groups.
Discussion
In 1971, Fathalla [19] developed the theory of inces-sant ovulation: ovulation could be involved in neoplas-tic transformation due to repeated trauma at the epithe-lial surface. During the scarring process, inclusion cysts could be formed from epithelial invaginations and then it could appear as malignant transformation under the influ-ence of cellular growth and hormonal factors (stromal microenvironment).
even more recently, different studies enabled the exist-ence of dysplastic ovarian lesions to be revealed in patients
who underwent stimulation treatment compared with a control group [10, 11]. The severity of ovarian dysplasia increased with the number of stimulation cycles (dose–effect) [11]. Animal experimental studies seem to confirm these results [20–22]. celik et al. [20] compared the rates of ovarian dysplasia in three groups of rats receiving stimu-lation using gonadotropins for, respectively, one, three and six cycles, and observed a concordance between the sever-ity of the dysplasia and the number of ovulation cycles. Dysplastic lesions were also found in significant fashion on rat ovaries in the studies by corakci et al. [21] and Ozcan et al. [22] after treatment with gonadotropins and clomi-phene citrate or gonadotropins, respectively. Our results support the idea that ovulation inducing agents could give rise to morphological abnormalities in the ovary as we have already demonstrated in a previous animal study [23]. The ovarian dysplasia score is significantly higher for the ova-ries of rats stimulated using tamoxifen and letrozole at a dosage of 0.5 mg/kg/day. Although there is not any dose–effect with tamoxifen, with letrozole the lesions were more severe as the dosage increases (p = 0.025). However, in our series there is no statistically significant difference between the mean dysplasia score of the group treated with clomi-phene citrate and that of the control group. This may be due to an insufficient number of stimulation cycles to reveal distinct morphological changes.
It is accepted that tamoxifen results in ovarian cysts in pre-menopausal women [24, 25]. However, the associa-tion often suggested in the literature between tamoxifen (used as an anti-cancer treatment) and an increased risk of ovarian cancer remains the subject of debate in the litera-ture [25–27]. Spicer et al. [27] showed in pre-menopausal women that the use of tamoxifen was associated with an increase in the risk of ovarian neoplasia. In opposition, Swerdlow et al. [25] concluded that the risk of malignant ovarian tumour was not affected when this drug was used
Table 2 comparison of respective frequencies of the 11 histopathologic abnormalities in the ovarian dysplasia scoring system
Histopathological abnormalities control group (n = 24) (%)
clomid group (n = 16) (%)
Tam 0.4 (n = 8) (%)
Tam 0.8 (n = 8) (%)
let 0.1 (n = 8) (%)
let 0.5 (n = 8) (%)
epithelial multilayering 0 18.7 25 50 0 12.5
epithelial proliferation 35.4 25 50 75 37.5 87.5
Surface papillomatosis 0 0 25 0 0 25
nuclear chromatin irregularity 0 0 0 12.5 0 0
nuclear contour irregularity 2.1 12.5 37.5 50 25 75
cellular pleomorphism 0 0 0 0 0 0
nuclear size enlargement 21.1 12.5 50 75 25 62.5
epithelial inclusion cysts 0 6.2 0 0 0 0
cortical invaginations 58.3 81.3 87.5 87.5 75 87.5
Psammoma 0 0 0 0 0 0
Stromal hyperplasia 0 0 0 12.5 0 12.5
Table 3 Mean tubal dysplasia score
Group Mean score comparison with the control group
control 0.67
clomid 1.42 p = 0.02
Tam 0.4 1.38 p = 0.027
Tam 0.8 1.25 p = 0.032
let 0.1 1.37 p = 0.011
let 0.5 2 p = 0.0001

Arch Gynecol Obstet
1 3
in pre- or peri-menopausal women. In an animal model, one team found dysplastic ovarian lesions after adminis-tration of tamoxifen [28]. However, this study concerned a series of cancerous ovaries and there could be actually a bias, given that the ovaries were already affected.
A review of the literature found no study on letrozole and ovarian dysplasia. This is despite the fact that this drug has a “clomid-like” effect and does cause ovarian cysts. When used as a treatment for cancer, this drug is known to give rise to fewer gynaecological side effects. In our study, tamoxifen and letrozole are both associated with higher ovarian dysplasia scores than in the control group. In addition, in rats stimulated with tamoxifen, the dysplas-tic lesions appeared to be significantly more severe than in those stimulated with letrozole. However, we do not know how these lesions would evolve.
Finally, the abnormalities found most frequently in our study are epithelial multilayering and proliferation, sur-face papillomatosis, irregular nuclear contour, increased nuclear size and deep epithelial invaginations. This agrees with the profile of ovarian dysplasia described for human stimulated ovaries. Dauplat et al. [16] showed that stimu-lated ovaries presented pseudostratified epithelium, sur-face papillomatosis, increased nuclear size and cellular pleomorphism more often, while psammoma bodies and stromal hyperplasia appeared less frequently. On the con-trary, ovaries with genetic risk were for the great majority found to have inclusion cysts, psammoma bodies and stro-mal hyperplasia [5].
Given that the hypothesis of dysplastic ovarian lesions in women having undergone ovarian stimulation arose from the discovery of particular ovarian lesions in women with a BRcA mutation, we felt that a study of tubal dys-plasia after ovulation induction was logical and justified in order to confirm the existence of such lesions and establish whether they are a continuation of ovarian dysplasia, or a separate and independent phenomenon. Our results show some dysplastic lesions in the tubes of rats given clomi-phene citrate, tamoxifen and letrozole suggesting that these drugs can interact with the tube [29, 30]. Moreover, unlike
for the ovary, there is no difference within the groups administered tamoxifen or letrozole. The lesions appear to be independent of any dose–effect.
In the newly described serous carcinogenic sequence, tubal dysplasia has been described by an overexpression of p53 and a moderate-to-high proliferation index. Ovarian dysplasia from ovariectomies for genetic risk has also the same pattern [6–8, 31].
In contrast, we have found a low expression of p53 and a high Ki67 expression in stimulated ovaries and tubes. There is only one animal study on the same topic and the authors have evaluated cell proliferation and apoptosis with Ki67, cD95 and PTen in ovaries stimu-lated by tamoxifen: the apoptosis index of ovarian epi-thelium, follicles, corpus luteum and stroma was low whereas proliferative index was significantly higher [32]. There is likely a balance between proliferation and apop-tosis-related factors in favour of proliferation (without any compensation by apoptosis) that may predispose to the development of ovarian cysts and tubo-ovarian dys-plasia [20, 27].
Mahdavi et al. [33] critically reviewed the literature about the relationship between induction of ovulation and ovarian cancer. They found a stronger association between fertility drugs and borderline ovarian tumors. Therefore we postulate that the different profiles of dysplasia observed in genetic risk (BRcA mutation) and in stimulated ovaries could have a different evolution: towards invasive cancer for patients with genetic risk and an unknown evolution for ovaries with ovulation induction (possibly towards border-line tumors) [20, 33].
We believe that our results may suggest a clinical impli-cation and may justify an interventional attitude in women with clinical or ultrasound ovarian abnormalities (espe-cially an ovarian cyst) several years after ovarian stimu-lation [20, 34]. Further complementary studies are still needed to know what long-term effects remain on both tubes and ovaries after stopping stimulation.
Conflict of interest We declare that we have no conflict of interest.
Table 4 comparison of respective frequencies of the 11 histopathologic abnormalities in the tubal dysplasia scoring system
Histopathological abnormalities control group (n = 24) (%)
clomid group (n = 16) (%)
Tam 0,4 (n = 8) (%)
Tam 0.8 (n = 8) (%)
let 0.1 (n = 8) (%)
let 0.5 (n = 8) (%)
epithelial multilayering 66.6 87.5 87.5 100 100 100
Tufting 0 0 0 0 0 0
Increased nuclear density 0 0 0 0 0 0
nuclear atypia 0 18.75 25 0 12.5 50
loss of nuclear polarity 0 6.25 0 0 0 0
nuclear size enlargement 8.33 18.75 12.5 0 0 37.5
loss of ciliation 0 12.5 12.5 25 25 12.5

Arch Gynecol Obstet
1 3
References
1. chene G, Dauplat J, Robin n, caure A, Penault-llorca F (2013) Tu-be or tu-be: that is the question… About serous ovarian car-cinogenesis. crit Rev Oncol/Hematol 88:134–143
2. Auersperg n (2010) The origin of ovarian carcinomas: a unifying hypothesis. Int J Gynecol Pathol 30:12–21
3. Deligdisch l, Gil J (1989) characterization of ovarian dysplasia by interactive morphometry. cancer 63:748–755
4. Deligdisch l, Miranda c, Barba J (1993) Ovarian dysplasia: nuclear texture analysis. cancer 72:3253–3257
5. chene G, Penault-llorca F, le Bouedec G et al (2009) Ovarian epithelial dysplasia and prophylactic oophorectomy for genetic risk. Int J Gynecol cancer 19:65–72
6. Medeiros F, Muto MG, lee y et al (2006) The tubal fimbria is a preferred site for early adenocarcinoma in women with familial ovarian cancer syndrome. Am J Surg Pathol 30:230–236
7. Folkins AK, Jarboe eA, Saleemuddin A et al (2008) A candidate precursor to pelvic serous cancer (p53 signature) and its preva-lence in ovaries and fallopian tubes from women with BRcA mutations. Gynecol Oncol 109:168–173
8. crum cP, Drapkin R, Kindelberger D, Medeiros F, Miron A, lee y (2007) lessons from BRcA: the tubal fimbria emerges as an origin for pelvic serous cancer. clin Med Res 5:35–44
9. cibula D, Widschwendter M, Majek O, Dusek l (2011) Tubal ligation and the risk of ovarian cancer: review and meta-analysis. Human Reprod update 17:55–67
10. nieto JJ, crow J, Sundaresan M et al (2001) Ovarian epithe-lial dysplasia in relation to ovulation induction and nulliparity. Gynecol Oncol 82:344–349
11. chene G, Penault-llorca F, le Bouedec G et al (2009) Ovar-ian epithelial dysplasia after ovulation induction: time and dose effect. Human Reprod 24:132–138
12. chene G, Penault-llorca F, Tardieu A et al (2012) Is there a relationship between ovarian epithelial dysplasia and infertility? Obstet Gynecol Int 2012:429085
13. chene G, Raoelfils I, Dauplat J et al (2012) Don’t forget Fallo-pian tubes: a morphologic and immunohistochemical study about Fallopian tubes with genetic risk (BRcA mutation). Gynecol Obstet Fertil 40:14–18
14. Brown J, Farquhar c, Beck J, Boothroyd c, Hugues e (2009) clomiphene and anti-oestrogens for ovulation induction in PcOS. cochrane Database Syst Rev 4:cD002249
15. Badawy A, Gibreal A (2011) clomiphene citrate versus tamox-ifen for ovulation induction in women with PcOS: a prospective randomized trial. eur J Obstet Gynecol Reprod Biol 159:151–154
16. Dauplat J, chene G, Pomel c et al (2009) comparison of dyspla-sia profiles in stimulated ovaries and in those with a genetic risk for ovarian cancer. eur J cancer 45:2977–2983
17. Schloosshauer PW, cohen cJ, Penault-lllorca F, Miranda cR, Bignon yJ, Dauplat J, Deligdisch l (2003) Prophylactic oopho-rectomy. cancer 98:2599–2606
18. carcangiu Ml, Radice P, Manoukian S et al (2003) Atypical epi-thelial proliferation in Fallopian tubes in prophylactic salpingo-oophorectomy specimens from BRcA 1 and BRcA 2 germline mutation carriers. Int J Gynecol Pathol 23:35–40
19. Fathalla M (1971) Incessant ovulation: a factor in ovarian neopla-sia? lancet 2:163
20. celik c, Gezginç K, Aktan M et al (2004) effects of ovulation induction on ovarian morphology: an animal study. Int J Gynecol cancer 14:600–606
21. corakci A, Filiz S, caliskan e, Dalcik c, Ozeren S, Dalcik H (2005) The effect of ovulation induction on ovarian epithelium dysplasia score and Ki67 expression: an experimental study on rats. Int J Gynecol cancer 15:866–871
22. Ozcan Z, celik H, Gurates B et al (2009) effects of ovulation induction agents on ovarian surface epithelium in rats. RBM online 19:314–318
23. lacoste cR, clemenson A, lima S, lecointre R, Peoc’h M, chene G (2013) Tubo-ovarian dysplasia in relationship with ovu-lation induction in rats. Fertil Steril 99:1768–1773
24. Vicus D, Rosen B, lubinski J et al (2009) Tamoxifen and the risk of ovarian cancer in BRcA1 mutation carriers. Gynecol Oncol 115:135–137
25. Swerdlow AJ, Jones Me (2007) Ovarian cancer risk in premeno-pausal and perimenopausal women treated with tamoxifen: a case-control study. Br J cancer 96:850–855
26. cohen I, Beyth y, Tepper R et al (1996) Ovarian tumors in postmenopausal breast cancer patients treated with tamoxifen. Gynecol Oncol 60:54–58
27. Spicer DV, Pike Mc, Henderson Be (1991) Ovarian cancer and long-term tamoxifen in premenopausal women. lancet 337:1414
28. Ting Ay, Kimler BF, Fabian cJ, Petroff BK (2008) Tamoxifen prevents premalignant changes of breast, but not ovarian cancer in rats at high risk for both diseases. cancer Prev Res 1:546–553
29. Pickel H, Reich O, Tamussino K (1999) Bilateral atypical hyper-plasia of the fallopian tube associated with tamoxifen: a report of two cases. Int J Gynecol Pathol 17:284–285
30. Diwan BA, Anderson lM, Ward JM (1997) Proliferative lesions of oviduct and uterus in cD-1 mice exposed prenatally to tamox-ifen. carcinogenesis 18:2009–2014
31. Piek JM, van Diest PJ, Zweemer RP (2001) Dysplastic changes in prophylactic removed fallopian tubes of women predisposed to developing ovarian cancer. J Pathol 195:451–456
32. cirpan T, Terek Mc, Ulukus M, Ulukus ec, Akman l, Kanit l (2008) Immunohistochemical evaluation of cell proliferation and apoptosis markers in ovaries and uterus of tamoxifen-treated rats. Int J Gynecol cancer 18:141–145
33. Mahdavi A, Pejovic T, nezhat F (2006) Induction of ovulation and ovarian cancer: a critical review of the literature. Fertil Steril 85:819–826
34. chene G, Rahimi K, Mes Masson AM, Provencher D (2013) Surgical implications of the potential new tubal pathway for the ovarian carcinogenesis. J Minim Invasive Gynecol 20:153–159