Morbidity & Mortality - SUNY Downstate Medical Center · Adrenal Gland • The adrenal cortex and...
71
Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005
Transcript of Morbidity & Mortality - SUNY Downstate Medical Center · Adrenal Gland • The adrenal cortex and...
Morbidity & Mortality
Mark H. Tseng MDSUNY Downstate Medical Center
Lutheran Medical CenterDecember 16, 2005
Case presentation
• Pt is a xx year old Asian woman who present to the ED with cc of epigastricpain and tenderness for the past 2 days. Pt denies any previous history of abdominal pain, nausea/vomiting, nor radiation to back. Pt denies any weight loss, headaches, palpitations, and diaphoresis. Surgery was consult after CT scan was performed.
Case presentation
• PMH: none• PSH: none• Shx: denies etoh, smoking, ivdu• Fhx: none• Allergy: nkda
Case presentation
Vital Signs• T: 98.6• BP: 110/70• HR: 80• RR:18
Case presentation
Physical Exam• A x O x 3, calm, age appropriate,
average wt for height• Abdomen: soft, right flank
tenderness, negative murphy’s sign, no mass appreciated, normal bowel sounds
Case presentation
LabWbc 4.2 H/H 12/36 Plt 209Na 141 K 4.0 Glucose 95LFT within normal limitsCortisol 13.3 (nl)VMA 3.3 (nl <6)metanephrine 199 (nl 95 to 475)
Case presentation
Lab:Wbc: 4.2 H/H: 12/36 Plt: 209Na: 141K: 4.0 Glucose: 95LFT: within normal limits
Lab:Cortisol: 13.3 (nl)VMA: 3.3 (nl <6)metanephrine: 199 (nl 95 to 475)
Case presentation
• CXR: unremarkable
• Sono: large mass in RUQ
Case presentation
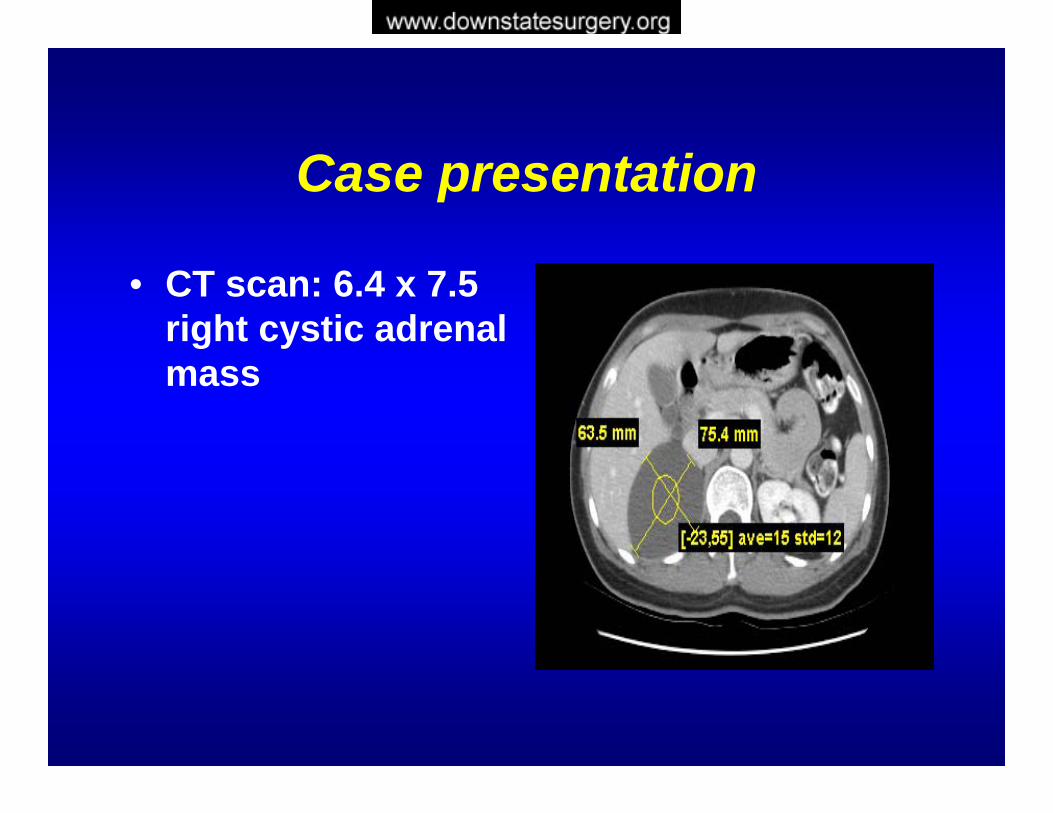
• CT scan: 6.4 x 7.5 right cystic adrenal mass
Case presentation
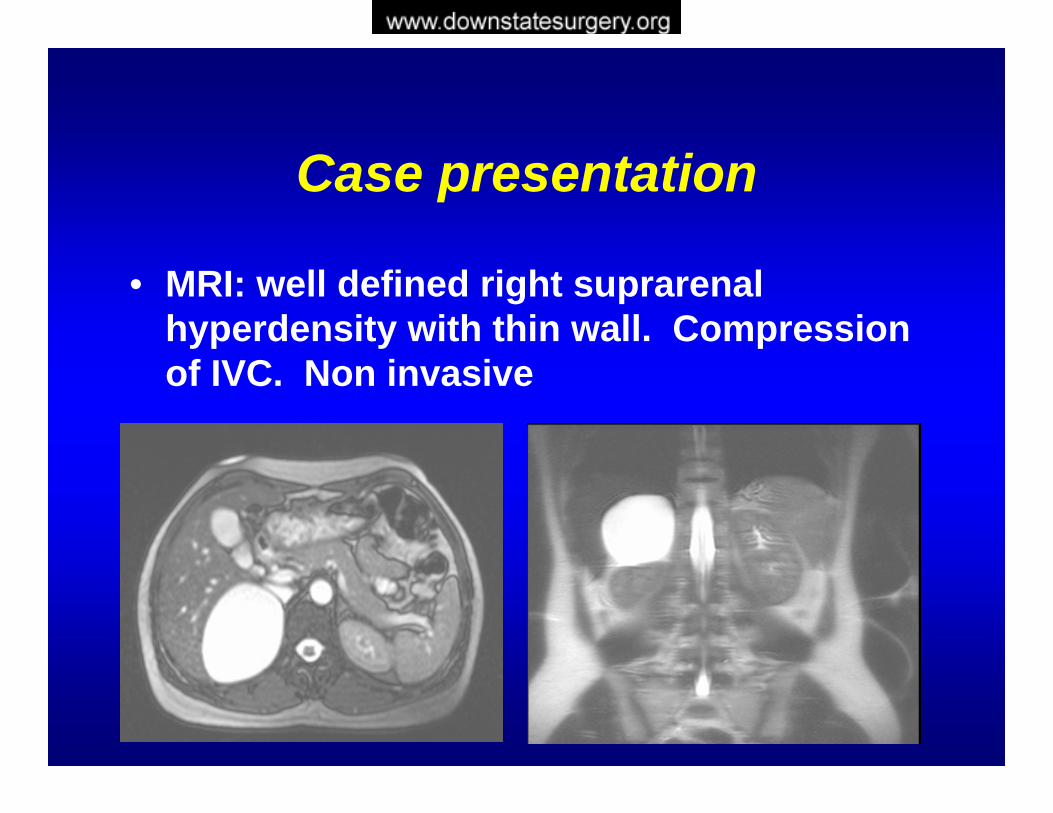
• MRI: well defined right suprarenal hyperdensity with thin wall. Compression of IVC. Non invasive
Case presentation
• Pt was taken to OR• Right adrenalectomy was performed
via a right flank incision• Fluid fill cyst was identified and
resected• Pt tolerated the procedure well
Case presentation
• POD #1 start on clears• POD #2 pain management• POD #3 discharge planning• POD #4 discharged home
Case presentation
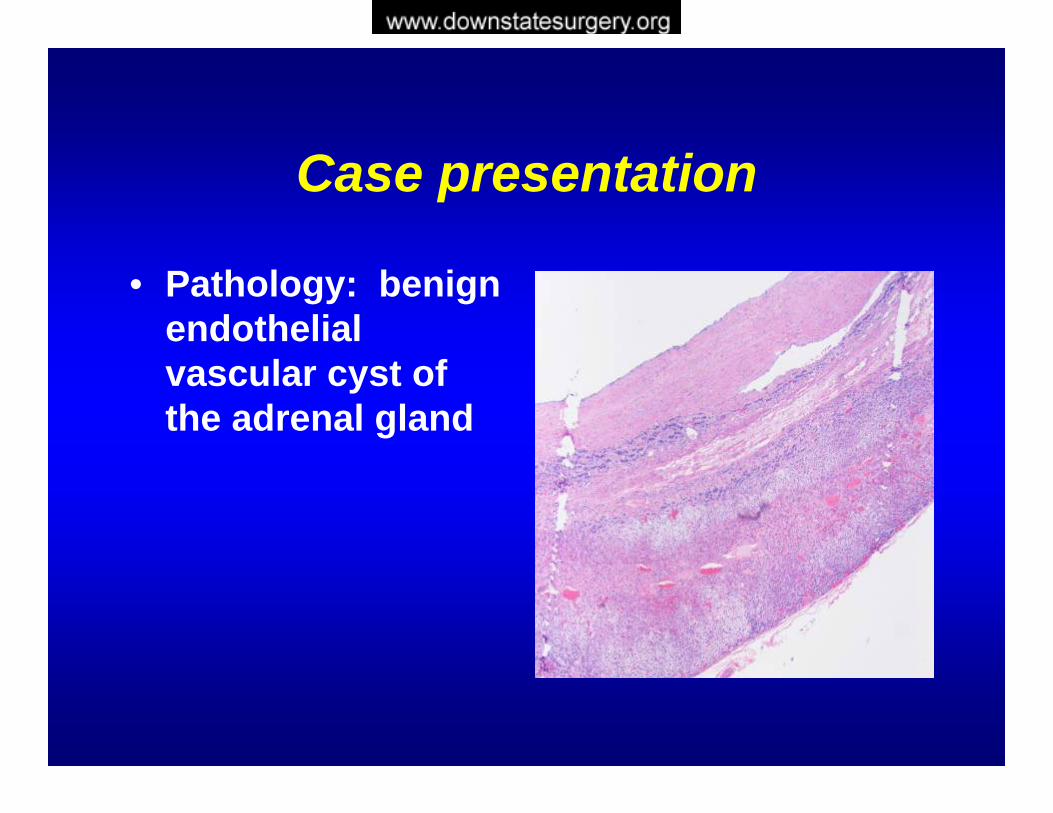
• Pathology: benign endothelial vascular cyst of the adrenal gland
Adrenal IncidentalomaMark H. Tseng MD
SUNY Downstate Medical CenterLutheran Medical Center
December 16, 2005
Overview
• Embryology• Anatomy and Physiology• Epidemiology• Incidentaloma• Conclusion• References
Adrenal Gland
• The adrenal cortex and medulla are anatomically and functionally distinct endocrine units that are contained in a single capsule
1563 – Eustachius describes the anatomy of the adrenal gland1855 – Addison correlates clinical features of adrenal disease with pathology found in autopsies1886 – Frankel describes pheochromocytoma1912 – Cushing presents clinical features of hypercortisolism1955 – Conn describes hyperaldosteronism
Embryology
• Cortex is mesodermal in origin– Week 4 to 6 – begin development from
coelomic mesoderm adjacent to urogenitalridge
– Week 8 – differentiates into thin outer definitive cortex and thick inner fetal cortex
– Fetal cortex produces fetal steroids during gestation then involutes at birth
– Definitive cortex develops into functional adrenal cortex
• Zona glomerlulosa and fasiculata present at birth• Zona reticularis develops during the first year of life
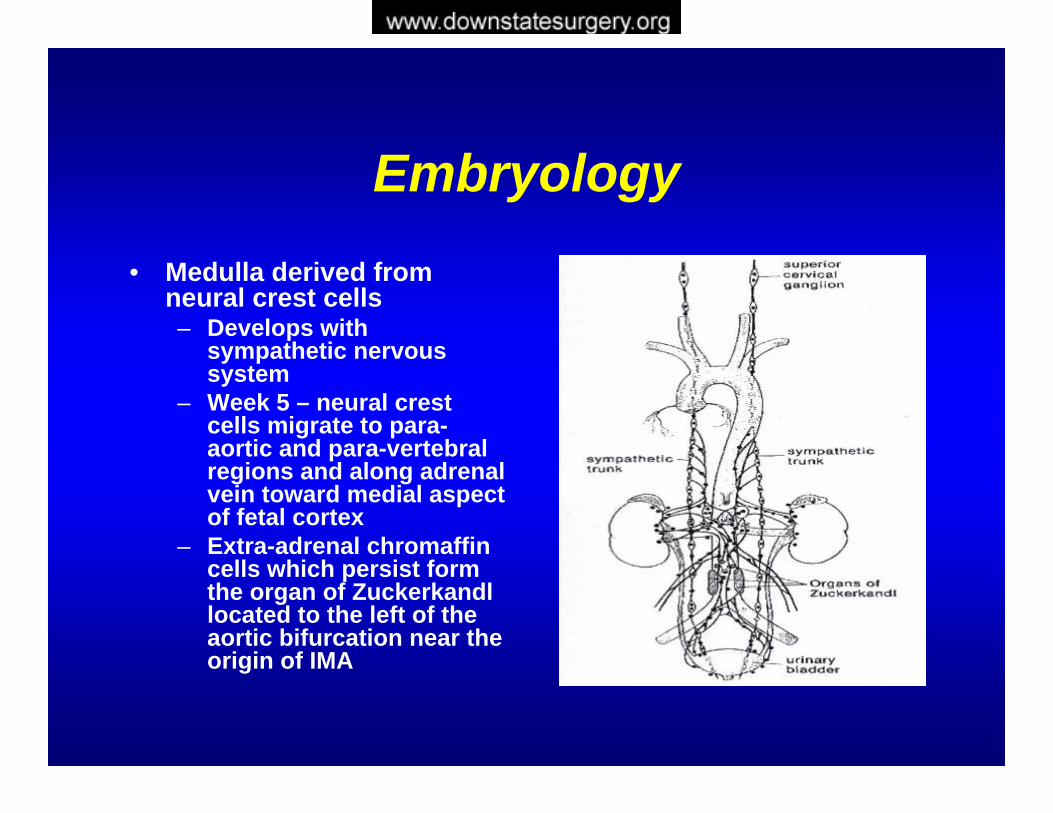
Embryology• Medulla derived from
neural crest cells– Develops with
sympathetic nervous system
– Week 5 – neural crest cells migrate to para-aortic and para-vertebral regions and along adrenal vein toward medial aspect of fetal cortex
– Extra-adrenal chromaffincells which persist form the organ of Zuckerkandllocated to the left of the aortic bifurcation near the origin of IMA
Anatomy
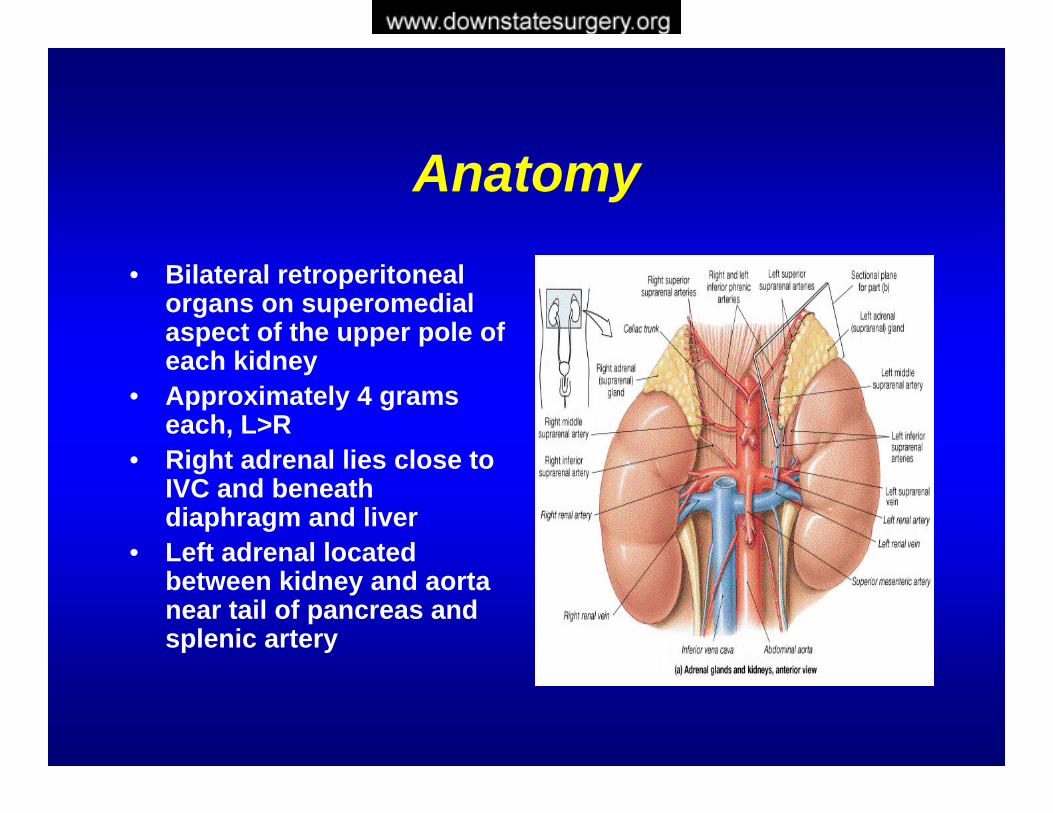
• Bilateral retroperitoneal organs on superomedialaspect of the upper pole of each kidney
• Approximately 4 grams each, L>R
• Right adrenal lies close to IVC and beneath diaphragm and liver
• Left adrenal located between kidney and aorta near tail of pancreas and splenic artery
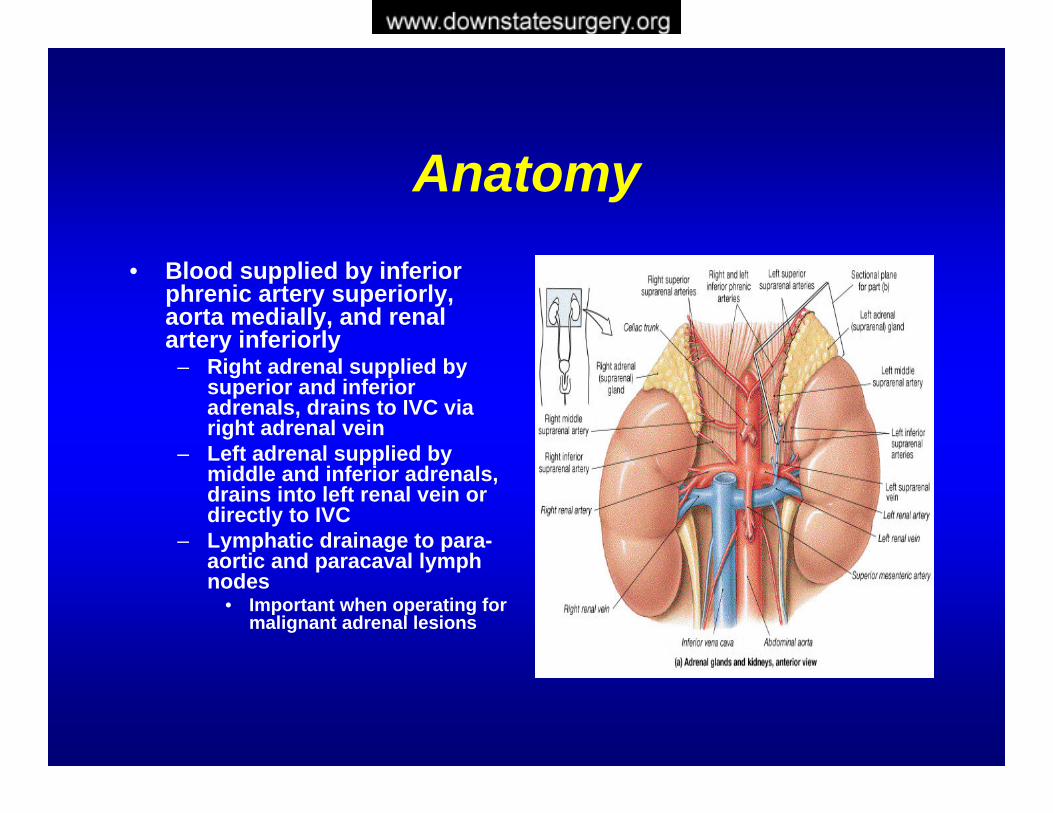
Anatomy• Blood supplied by inferior
phrenic artery superiorly, aorta medially, and renal artery inferiorly
– Right adrenal supplied by superior and inferior adrenals, drains to IVC via right adrenal vein
– Left adrenal supplied by middle and inferior adrenals, drains into left renal vein or directly to IVC
– Lymphatic drainage to para-aortic and paracaval lymph nodes
• Important when operating for malignant adrenal lesions
Anatomy
• The location of the adrenal gland deep in the retroperitonium has in the past made them relatively inaccessible
• Understanding the anatomical relationships and appreciate their relationship to the arterial supply and venous drainage are important and have significant surgical ramifications
Histology
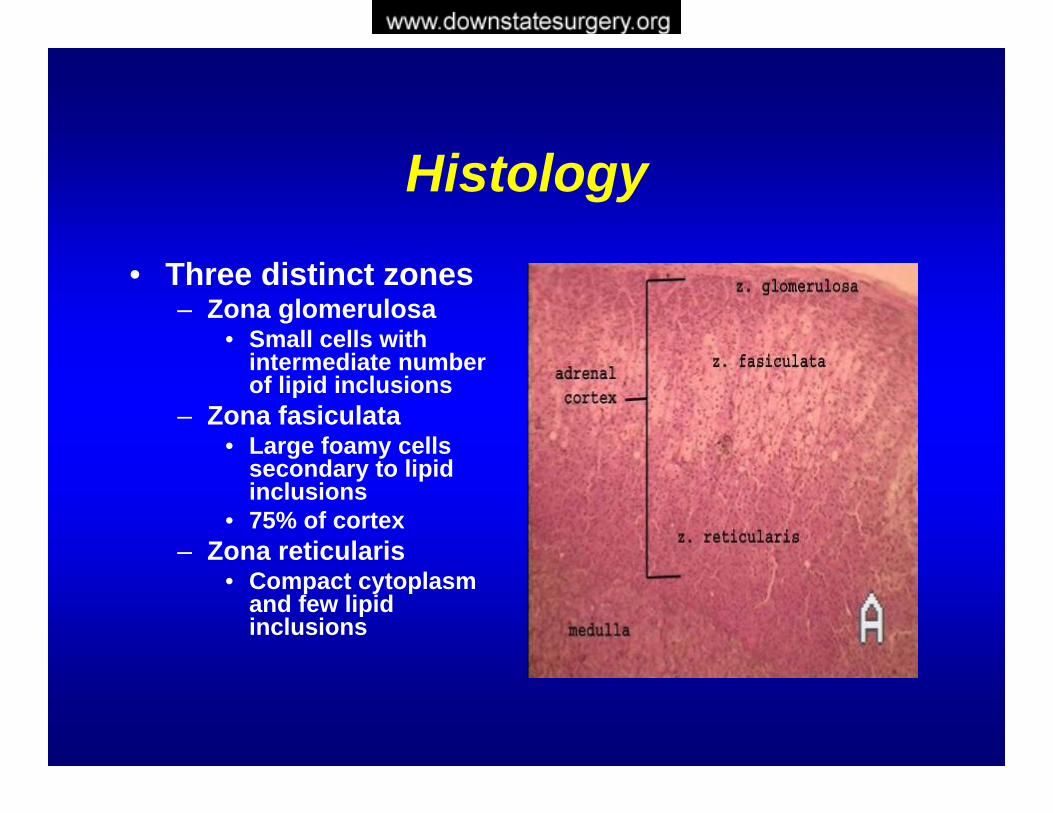
• Three distinct zones– Zona glomerulosa
• Small cells with intermediate number of lipid inclusions
– Zona fasiculata• Large foamy cells
secondary to lipid inclusions
• 75% of cortex– Zona reticularis
• Compact cytoplasm and few lipid inclusions
Physiology
• Composed of two distinct organs– Adrenal cortex and adrenal medulla
• Three major biosynthetic pathways produce *glucocorticoids, mineralocorticoids, and adrenal androgens– Zona glomerulosa synthesizes
mineralocorticoids– Zona fasiculata synthesizes glucocorticoids *– Zona reticularis synthesizes adrenal
androgens
* Absolutely required for life
Epidemiology
Figures Vary From O.4-6% Of CT Scans
6.5-8.7% Of Autopsy Series
Incidence Increases With Age; 7% After 70
Seen More Commonly In Women
NATIONAL INSTITUTES OF HEALTHManagement of the Clinically Inapparent Adrenal Mass (Incidentaloma). Final Statement. July 16, 2002
Adrenal Incidentaloma• The evaluation and decision
paradigm for an incidentalomahinges on three issues:
IS IT MALIGNANT? IS IT METASTATIC?IS IT FUNCTIONAL?
Major Causes
Benign Adenoma 50%Cyst 10%Myelolipoma 10%Pheochromocytoma 10%Metastases 6-30%Adrenal Cancer 0.01%
The incidental adrenal mass. Am J Med 1996
Is It Malignant?
• An important and unresolved issue in the management if incidentalomasis the determination of what size of adrenal tumor has malignant potential and requires surgical resection.
Is It Malignant?
Useful in determining malignant potential:
• Size of the mass
• Radiological Findings
The Mayo Clinic Study
• 342 Patients With Adrenal IncidentalomaRetrospectively Evaluated
• Tumor Diameter Averaged 2.5 cm.• Most Malignant Tumors Measured > 5 cm. • Removing All Tumors > 4 cm Would Have
Removed Eight Benign Tumors For Every Carcinoma
Incidentally discovered adrenal tumors: an institutional perspective. Herrera MF; Grant CS; van Heerden JA; Sheedy PF; Ilstrup DM. Surgery 1991 Dec;110(6):1014-21
Mass
• Masses > 6 cm Usually Are Treated Surgically
• Masses < 4 cm Are Generally Monitored
• Masses Between 4 And 6 cm:Criteria Other Than Size Should Be Considered In Making The Decision To Monitor Or Proceed To Surgery
• Experienced investigators now recommend excision of all tumors >4 cmNational Institutes Of HealthManagement Of The Clinically Inapparent Adrenal Mass (Incidentaloma) 2002
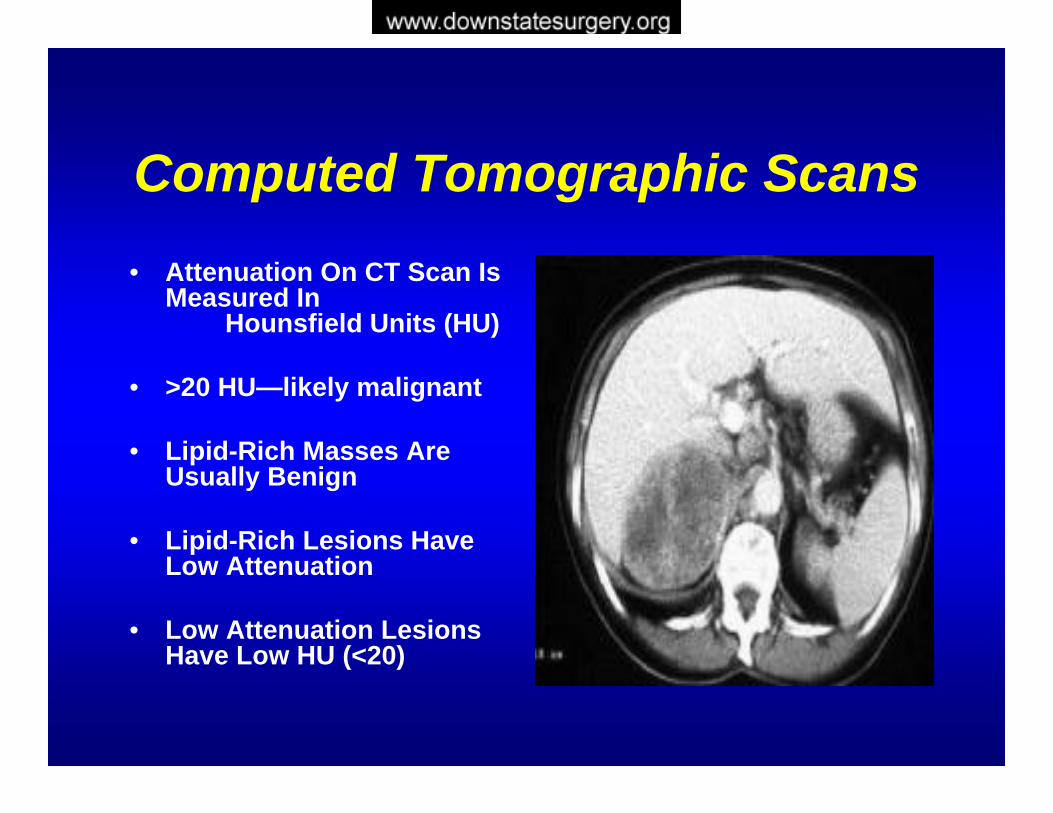
Computed Tomographic Scans• Attenuation On CT Scan Is
Measured In Hounsfield Units (HU)
• >20 HU—likely malignant
• Lipid-Rich Masses Are Usually Benign
• Lipid-Rich Lesions Have Low Attenuation
• Low Attenuation Lesions Have Low HU (<20)
Computed Tomographic Scans
• Unenhanced CT:Adenomas: < 10 HUMalignancies: > 20 HU Sensitivity: 73% Specificity: 96%
• Delayed Enhanced CT:Adenomas: < 30 HU Malignancies: > 30 HU Sensitivity 95% And Specificity: 100%
MRI
• Equally Effective As CT
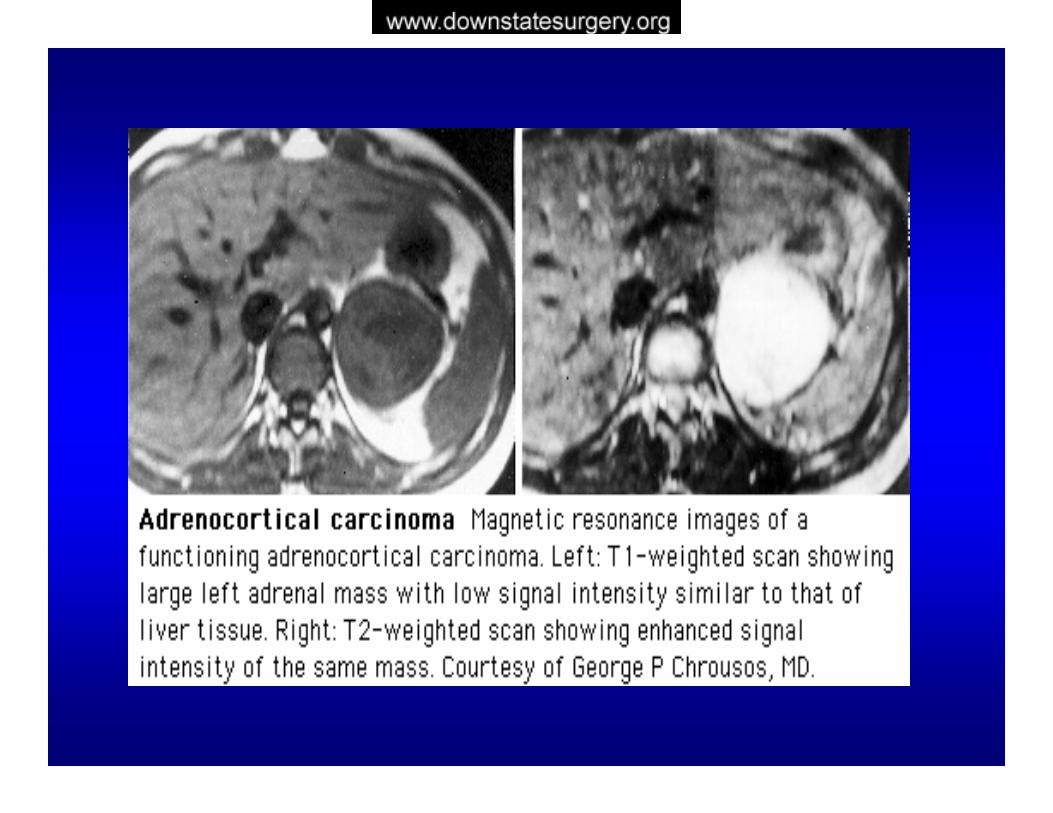
• Adenomas Are Iso-Intense With The Liver On T2-weighted Images
• Carcinomas Have A Hyper-Intense Signal Compared With The Liver
Fine-Needle Aspiration Biopsy
CANNOT Distinguish A Benign Adrenal Mass From Adrenal
Carcinoma
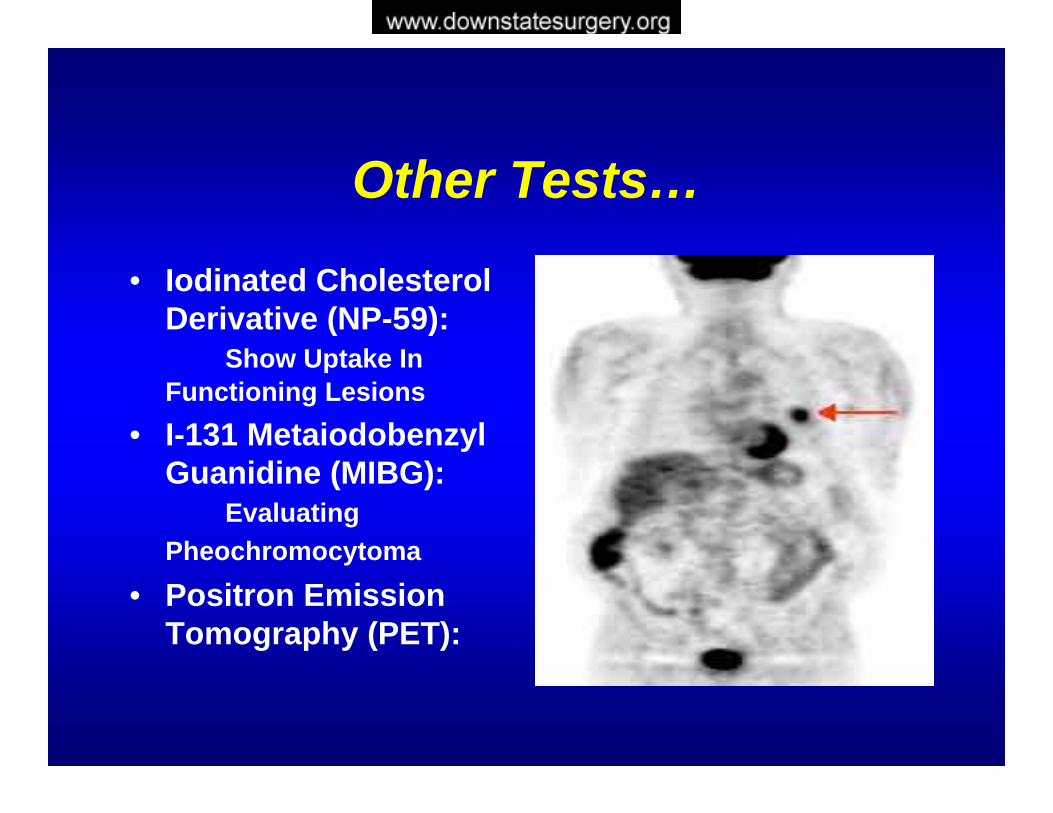
Other Tests…
• Iodinated Cholesterol Derivative (NP-59):
Show Uptake In Functioning Lesions
• I-131 MetaiodobenzylGuanidine (MIBG):
Evaluating Pheochromocytoma
• Positron Emission Tomography (PET):
Is It Metastatic?
• The adrenal gland, although relatively small, has the highest blood flow of any endocine organ on a gram per flow basis.
• It is therefore not surprising that metastatic diseases, particularly from lung, esophageal, and breast cancer, occurs in the adrenal gland.
• Majority has history of malignant diseases and metastases to multiple additional sites.
Is It Metastatic?
• Patients with bilateral adrenal metastases are at some risk for adrenal insufficiency.
• Patients with isolated adrenal metastases pose a diagnostic dilemma.
• Tissue diagnosis may affect subsequent care or an adrenalectomy might be indicated.
• FNA is controversial• The only situation where FNA appears indicated
is when metastatic disease is not only likely, but its detection would alter patient management.
IS IT HYPERSECRETORY?
Cortisol
Catecholamines
Mineralcorticoids
Androgens
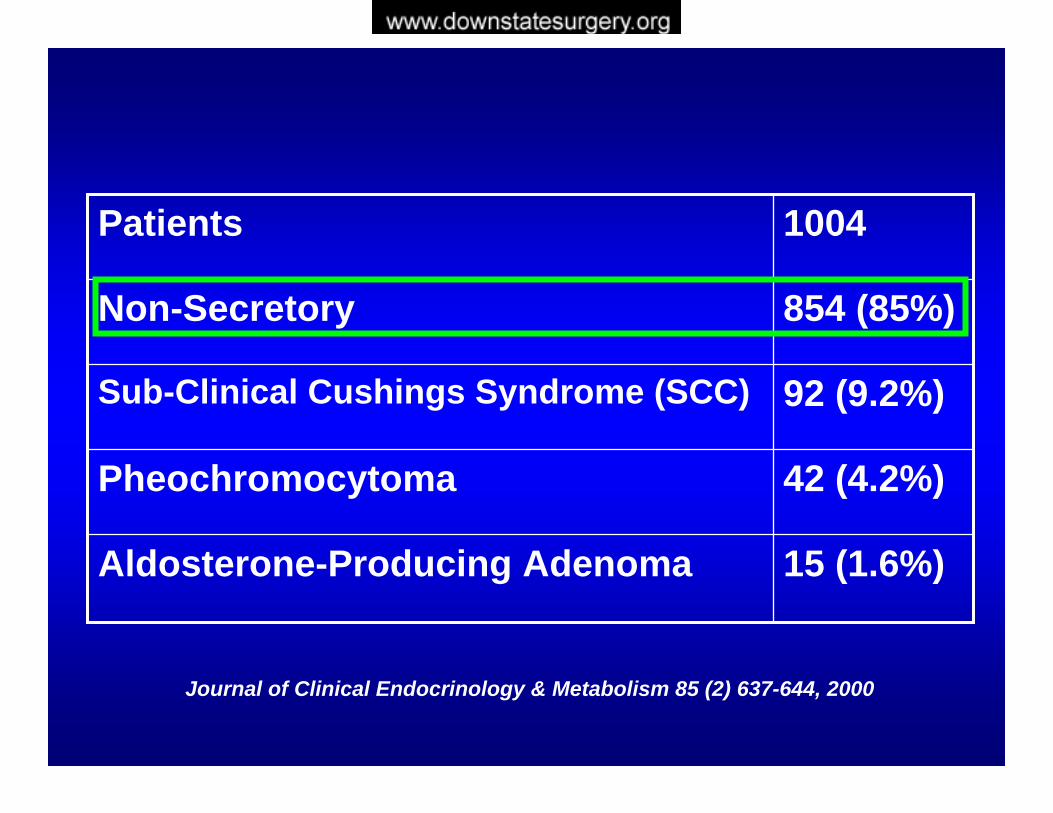
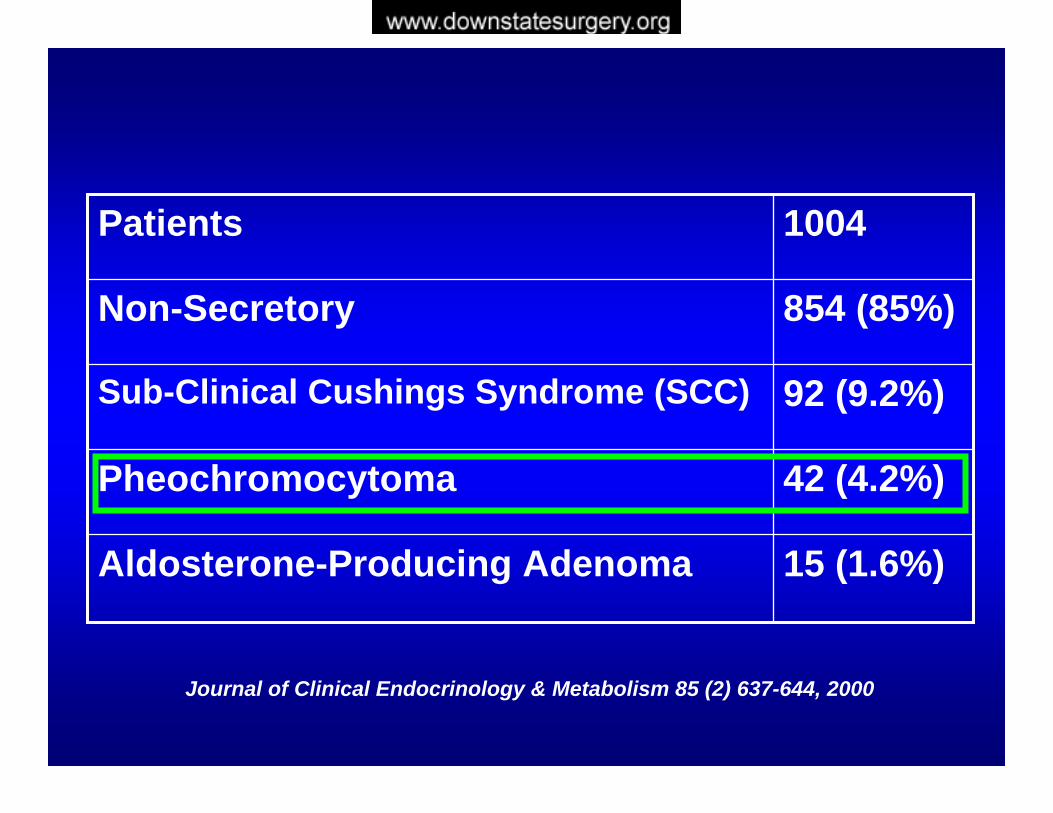
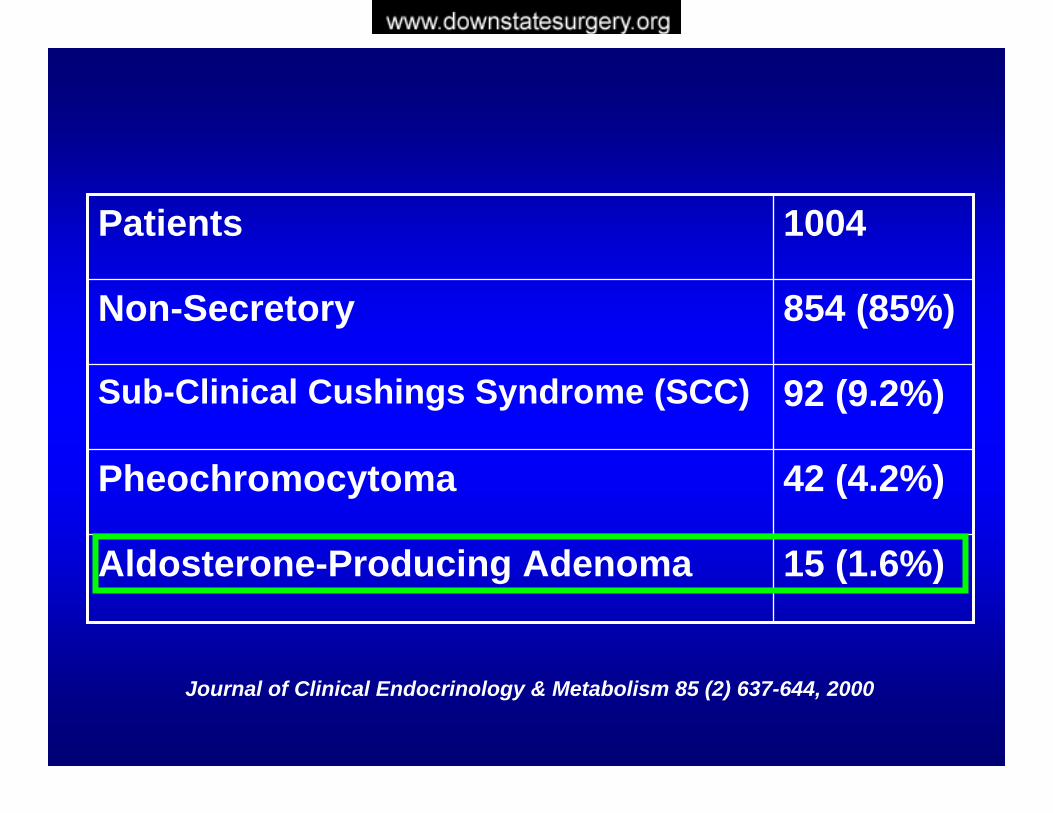
15 (1.6%)Aldosterone-Producing Adenoma
42 (4.2%)Pheochromocytoma
92 (9.2%)Sub-Clinical Cushings Syndrome (SCC)
854 (85%)Non-Secretory
1004Patients
Journal of Clinical Endocrinology & Metabolism 85 (2) 637-644, 2000
Non-Secretory
• All evaluations begin with a detailed history and physical examination.
• If there are signs and symptoms suggesting a functional adrenal neoplasm, in addition to routine screening evaluation, specific hormone studies are indicated
• Most patients are asymptomatic, CT findings can be pathognomonic
• Hormone screening studies are therefore not required.
Ross NS. Hormonal evaluation of the patient with an incidentally discovered adreanl mass. NEJM 1990:323:1401-1405
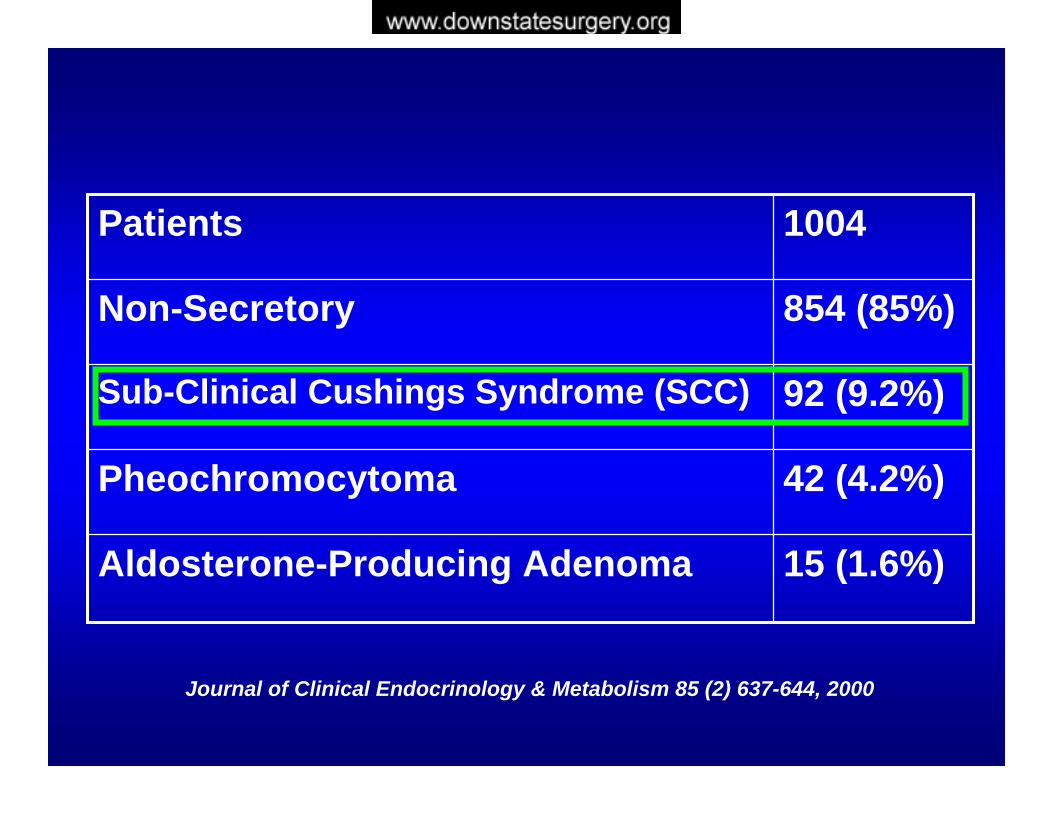
15 (1.6%)Aldosterone-Producing Adenoma
42 (4.2%)Pheochromocytoma
92 (9.2%)Sub-Clinical Cushings Syndrome (SCC)
854 (85%)Non-Secretory
1004Patients
Journal of Clinical Endocrinology & Metabolism 85 (2) 637-644, 2000
Subclinical Hypercortisolism
• Cushing’s syndrome is important to consider in all patients with adrenal tumors
• Some patients has obvious signs and symptoms and are not difficult to diagnose
• However, some patients presents with subtle stigmata of Cushing’s syndrome or “subclinical”and require additional testing.
• Approximately 15% of patients with incidentalomas have subclinical features.
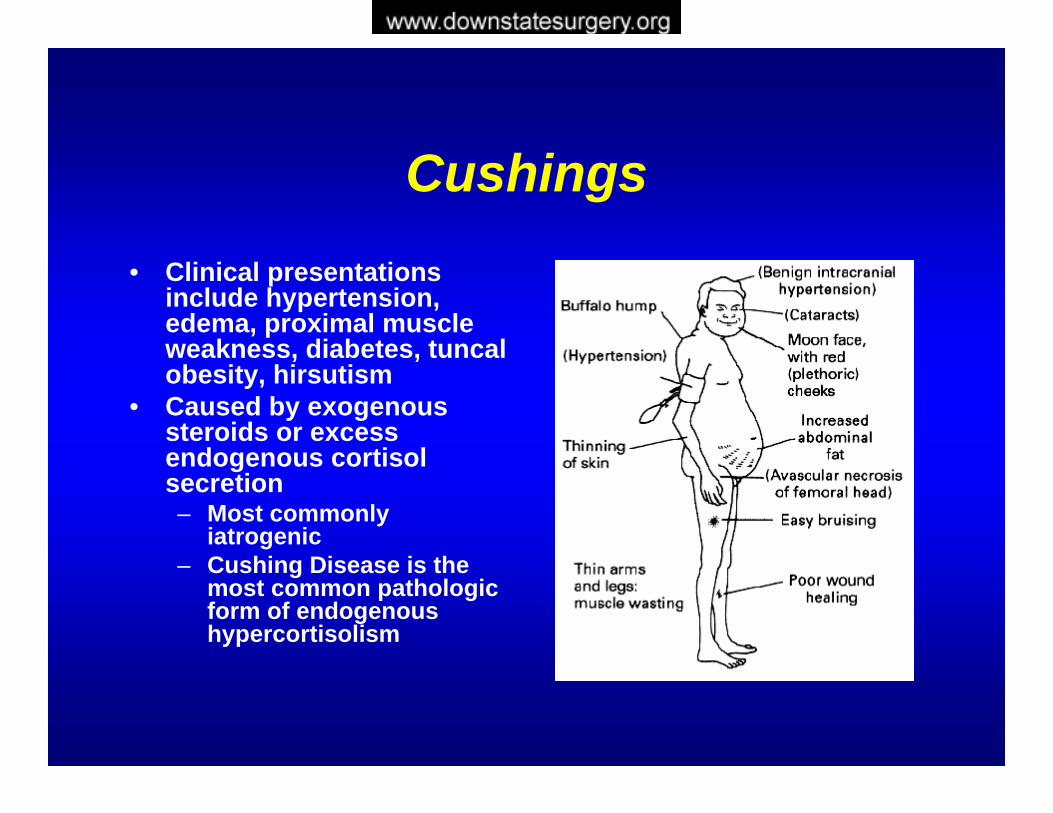
Cushings• Clinical presentations
include hypertension, edema, proximal muscle weakness, diabetes, tuncalobesity, hirsutism
• Caused by exogenous steroids or excess endogenous cortisolsecretion– Most commonly
iatrogenic– Cushing Disease is the
most common pathologic form of endogenous hypercortisolism
Subclinical Hypercortisolism
Defined By Any Two Of The Following:Defined By Any Two Of The Following:
Increased Urinary Free Cortisol (UFC) Unsuppressed Serum Cortisol Levels
After 1-mg Overnight DexamethasoneLow ACTH Levels No Clinical Signs Of Cushing Syndrome
Mantero F, Masini AM, Opocher G, Giovagnetti M, Arnaldi G. Horm Res47:284–289, 1997
Subclinical Hypercortisolism
• It is important to rule out subclinicalCushing’s syndrome for two reasons:
• 1) if one elects not to peform an adrenalectomy, then the endocrinopathywill continue and deleterious effects will occur
• 2) if one does perform an adrenalectomy, the contralateral adrenal will be suppressed and if perioperativeglucocorticoids are not administered, the patient will be at risk for Addisonian crisis
Hypercortisolism24 Hour Urinary Free Cortisol
Positive: More Than 3-4 Times The Upper Limit Of Normal Range
Mildly Elevated Levels Can Be Seen In Anxiety, Depression, Alcoholism
When the 24 hr UFC Is Not Conclusive……..
Dexamethasone Suppression Test
1 mg Dexamethasone At 11 pm Measure Cortisol At 8 am
Normal: Cortisol < 5 ug/dl
Specificity Is Reduced In Acute Or Chronic Illness
Subclinical cushings syndrome?
Increased Incidence Of:HTNObesity DMIGT Increased CV Risk Bone Disease
15 (1.6%)Aldosterone-Producing Adenoma
42 (4.2%)Pheochromocytoma
92 (9.2%)Sub-Clinical Cushings Syndrome (SCC)
854 (85%)Non-Secretory
1004Patients
Journal of Clinical Endocrinology & Metabolism 85 (2) 637-644, 2000
PheochromocytomaRareArise From Neuroectodermally Derived Chromaffin CellsSecretion of Norepinephrine—Most Common19-76% Of Pheochromocytomas Not Diagnosed Until After Death80% Of Patients With Unsuspected PheochromocytomasWho Underwent Surgery Or Anesthesia DiedNot Possible To Determine Which Will Present With CrisisNot Possible To Determine The Malignant
Potential Of Pheochromocytoma
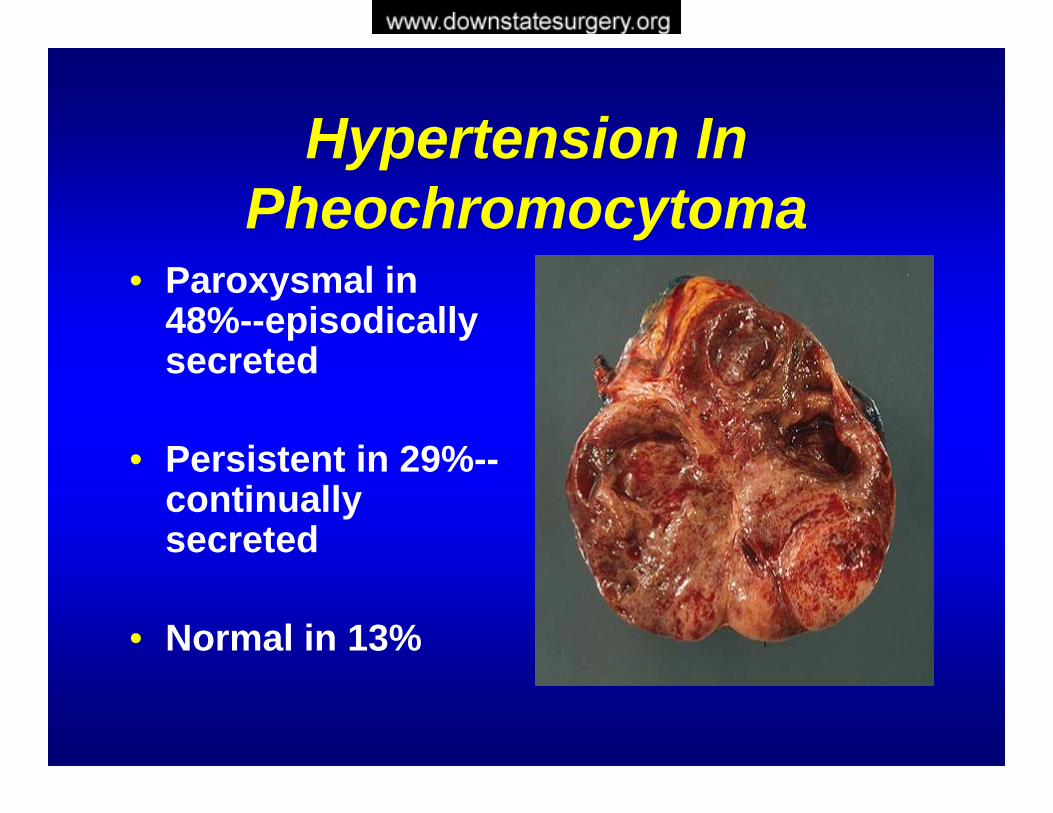
Hypertension In Pheochromocytoma
• Paroxysmal in 48%--episodically secreted
• Persistent in 29%--continually secreted
• Normal in 13%

Clinical Presentation
• Attacks of Headaches (80%) • Palpitations (64%)• Diaphoresis (57%)
Symptomatic Triad Of Headache, Sweating, And Tachycardia In A Hypertensive Patient
Sensitivity 90.9% And Specificity 93.8%
How To Screen…• Because the risk of complications associated with an
occult pheochromocytoma is significant, all incidentalomashould be screened for pheochromocytoma
• Urine Collection Of Catecholamines and Metabolites
• Plasma Collection Of Catecholamines And Metabolites
• Collections are analyzed for metanephrines, vanillylmandelic acid (VMA), and fractional catecholamines.
Which Is Better?
Catecholamine-Secreting Tumors Histologically Proven In 31 of 340
Patients:
Sensitivity Of Plasma Free Metanephrine 97% Specificity 98%
Sensitivity Of Urinary Total MetanephrineAnd Catecholamines 90%; Specificity 85%
Sawka et al. JCEM 88(2): 553-558. 2003.
Pheochromocytoma
Plasma-Free Metanephrines Are Recommended As The Test Of Choice For Excluding Or
Confirming The Diagnosis Of Pheochromocytoma
NATIONAL INSTITUTES OF HEALTHManagement of the Clinically Inapparent Adrenal Mass (Incidentaloma). Final Statement. July 16, 2002
Pre-operative Treatment
• Because of chronic hypersecretion of catecholamines, pt with pheochromocytomas are often severely volume contracted and severely hemodynamically unstable after general anesthesia
• selective Alpha 1 adrenergic receptor blocker• Phenoxybenamine-increase dosage until pt experience
orthostatic hypotension • Given 1-4 weeks before surgery• Beta blocker- for breakthrough tachycardia• Alpha blocker before beta blocker• Fear of unapposed alpha recepter would induced malignant
hypertension
Cleveland Clinic study
• 63 pts with pheochromocytoma can undergo successful surgical treatment without preoperative preparation with alpha adrenergic blockade
15 (1.6%)Aldosterone-Producing Adenoma
42 (4.2%)Pheochromocytoma
92 (9.2%)Sub-Clinical Cushings Syndrome (SCC)
854 (85%)Non-Secretory
1004Patients
Journal of Clinical Endocrinology & Metabolism 85 (2) 637-644, 2000
Aldosterone Producing Adenoma
• Rare• Most Common Cause of
Hyperaldosteronism• Twice as Common in Women• Mean Age 30-50 Years Old• Conn in 1955—First Curative Treatment of
APA by Unilateral Adrenalectomy• Mostly Unilateral• Mostly < 2 cm in size
Hypertension HeadacheWeakness/ FatigueParesthesiasMuscle CrampsPolyuria/ PolydipsiaArrhythmias
HypokalemiaNo Other Cause For Hypertension Or HypokalemiaMetabolic AlkalosisHyperaldosteronismHyporeninemia
Signs, Symptoms, and Laboratory Datain Primary Hyperaldosteronism

Aldosterone-Producing Adenoma
Serum Potassium And Aldosterone /Plasma Renin Activity Ratio Should Be Determined To Evaluate For Primary Aldosteronism
Less Affected by Physiological or Pharmacological Variables
NATIONAL INSTITUTES OF HEALTHManagement of the Clinically Inapparent Adrenal Mass (Incidentaloma). Final Statement. July 16, 2002
Aldosterone/PRA Ratio• Normals < 20
• Primary Aldosteronism > 30
• > 90% Sensitivity And Specificity
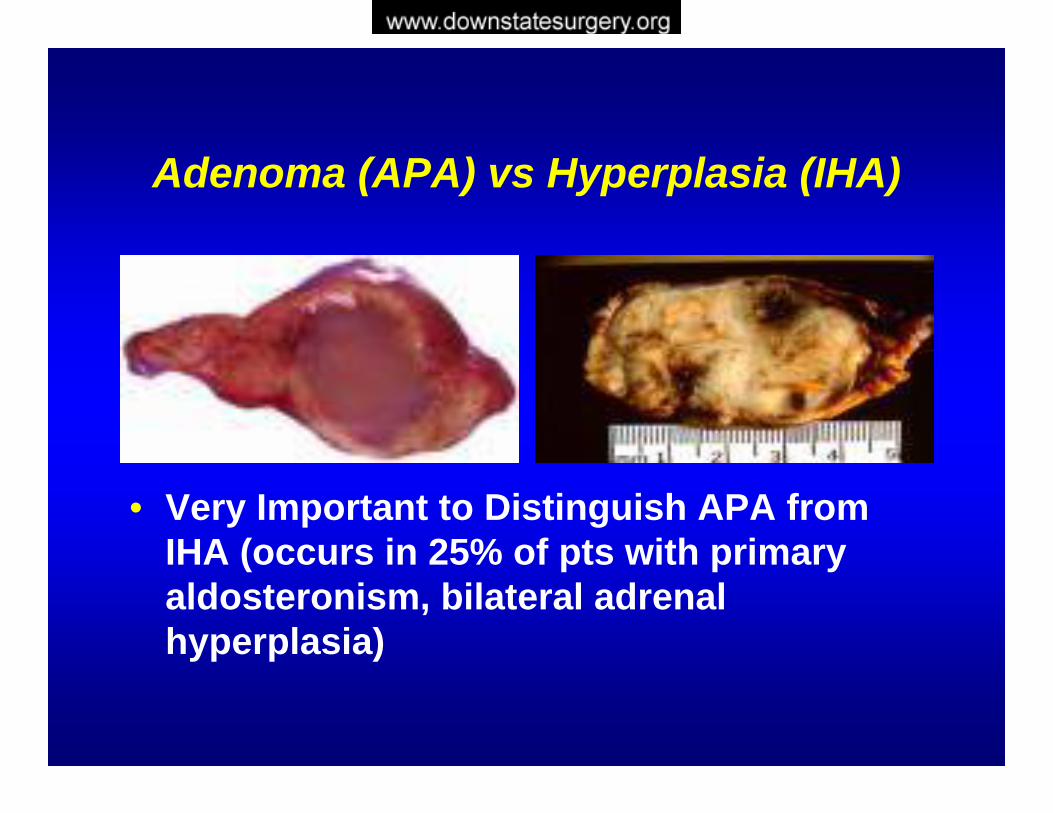
Adenoma (APA) vs Hyperplasia (IHA)
• Very Important to Distinguish APA from IHA (occurs in 25% of pts with primary aldosteronism, bilateral adrenal hyperplasia)
Adenoma (APA) vs Hyperplasia (IHA)
• Very High aldosterone/Plasma ReninActivity Adenoma – Surgical resection of unilateral
adenoma is curative• Increased 18-OH-Corticosterone
Adenoma if >100 mg/dl and hyperplasia if <50 ng/dl– Treatment is with spironolactone
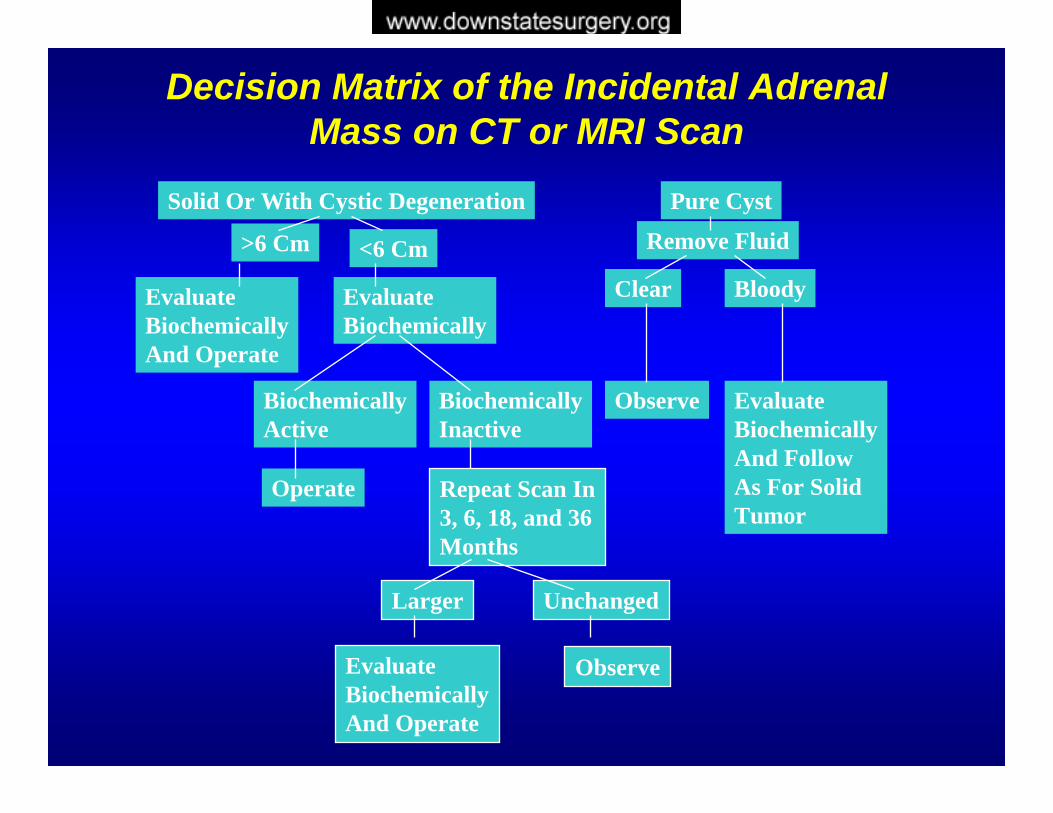
Solid Or With Cystic Degeneration
>6 Cm <6 Cm
EvaluateBiochemicallyAnd Operate
EvaluateBiochemically
BiochemicallyActive
Operate
BiochemicallyInactive
Repeat Scan In3, 6, 18, and 36Months
Larger
EvaluateBiochemicallyAnd Operate
Unchanged
Observe
Pure Cyst
Remove Fluid
Clear Bloody
Observe EvaluateBiochemicallyAnd FollowAs For SolidTumor
Decision Matrix of the Incidental Adrenal Mass on CT or MRI Scan
If the Decision is to Observe?
• Will The Mass Become Malignant?
• Will The Mass Become Hypersecretory?
National Institutes Of Health: Management Of The Clinically InapparentAdrenal Mass (Incidentaloma). Final Statement. July 16, 2002
Incidental Adrenal MassRisk of Progression
Adrenal Hyperfunction: Unlikely If Lesion < 3 cmCortisol Hypersecretion Most Likely Disorder 4% After 1 Year9.5% Within 3 YearsThe Risk Of Tumor Hyperfunction Appears To Plateau After 3 Years
Mass Enlargement:8% After 1 Year18% After 5 YearsMost Enlargement Occurred Within 3 Years
Take Home Points…
Incidental Adrenal MassGood history and physical examSize and HU units Important>4 cm Surgical Removal after workupExclude Hypersecretion:24 Urine Free CortisolPlasma Free MetanephrinesPotassium and Aldo/Renin
![Adrenal Imaging - University of Floridaxray.ufl.edu/files/2010/02/Adrenal-Imaging.pdfadrenal glands [3], and a metastasis might ... CT, adrenal imaging, adrenal lymphoma imaging, adrenal](https://static.fdocuments.in/doc/165x107/5b26814c7f8b9a8c0f8b4820/adrenal-imaging-university-of-glands-3-and-a-metastasis-might-ct-adrenal.jpg)