Morbidities in Non-Transfusion-Dependent ... - Thalassemia Cappellini Morbidities in...
46
Morbidities in Non-Transfusion-Dependent Thalassemias (NTDT) Ali T. Taher, MD, PhD, FRCP Professor of Medicine, Hematology & Oncology American University of Beirut Medical Center Beirut – Lebanon Professor of Hematology & Medical Oncology (Adj.) Emory School of Medicine Atlanta – USA Thalassemia Intermedia: is disease morbidity as we know it today less severe than Thalassemia Major ?
Transcript of Morbidities in Non-Transfusion-Dependent ... - Thalassemia Cappellini Morbidities in...

Morbidities in Non-Transfusion-Dependent Thalassemias (NTDT)
Ali T. Taher, MD, PhD, FRCPProfessor of Medicine, Hematology & OncologyAmerican University of Beirut Medical Center
Beirut – Lebanon
Professor of Hematology & Medical Oncology (Adj.)Emory School of Medicine
Atlanta – USA
Thalassemia Intermedia: is disease morbidity as we know it today less
severe than Thalassemia Major ?

Non-transfusion-dependent thalassemia (NTDT)
Morbidity in NTDT
– Clinical complications profile
– Ineffective erythropoiesis and anemia
– Iron overload and target organ damage
– Hypercoagulability and vascular disease
Agenda

Non-transfusion-dependent thalassemia (NTDT)
Morbidity in NTDT
– Clinical complications profile
– Ineffective erythropoiesis and anemia
– Iron overload and target organ damage
– Hypercoagulability and vascular disease
Agenda

HbE, haemoglobin E; HbH, haemoglobin H.
1. Taher AT, et al. Br J Haematol. 2011;152:512-23. 2. Galanello R, Origa R. Orphanet J Rare Dis. 2010;5:11.3. Vichinsky E. Hematology Am Soc Hematol Educ Program. 2007;79-83. 44. Muncie HL Jr, Campbell J. Am Fam Physician. 2009;80:339-44. 5. Figure adapted from Musallam KM, et al. Haematologica. 2013;98:833-44.
Occasional transfusions required (e.g. surgery, pregnancy, infection)
Intermittent transfusions required (e.g. poor growth and development,
specific morbidities)
Regular, lifelong transfusions required
for survival
Transfusions seldom required
Transfusions not required α-thalassaemia trait β-thalassaemia minor
Non transfusion dependent thalassaemia (NTDT) β-thalassaemia intermedia Mild/moderate HbE/β-thalassaemia HbH disease (α-thalassaemia) HbS β-thalassaemia HbC thalassaemia
Transfusion dependent thalassaemia (TDT) β-thalassaemia major Severe HbE/β-thalassaemia Hb Barts hydrops (α-thalassaemia major)
NTDT patients do not require regular transfusions, although they may require occasional transfusions for growth failure, pregnancy, infections, and other specific situations1–4
NTDT: a designation based on transfusion requirement

1Weatherall DJ. Blood Rev 2012;26 Suppl 1:S3–S6;2Available from: http://emedicine.medscape.com/article/959122-overview#a0156;3Harteveld CL and Higgs DR. Orphanet J Rare Dis 2010;5:13; 4Weatherall DJ. Blood 2010;115:4331–4336.
3
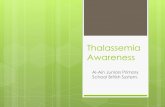
Prevalence of Hb H disease in Europe and North America
increasing due to migration3
β thalassemia intermedia –
most common in Africa, Mediterranean, India and
East Europe1,2
Hb H – most common in Southeast Asia, Middle East and
Mediterranean3
Approx. 9500 annual births4
Hb E/β thalassemia – most common in East India, Bangladesh and Southeast Asia1 Approx.
19,000 annual births4
The increased migration flow expands the reach of these diseases
World distribution of hemoglobinopathies3
The prevalence of NTDT is increasing worldwide due to migration

Non-transfusion-dependent thalassemia (NTDT)
Morbidity in NTDT
– Clinical complications profile
– Ineffective erythropoiesis and anemia
– Iron overload and target organ damage
– Hypercoagulability and vascular disease
Agenda

Taher A, et al. Blood Cells Mol Dis. 2006;37:12-20.
How it all started: realizing morbidity is highly prevalent and different from TDT in our clinics
Complication (% of patients affected)
β-TI β-TM
Lebanon(n = 37)
Italy(n = 63)
Lebanon(n = 40)
Italy(n = 60)
Splenectomy 90 67 95 83
Cholecystectomy 85 68 15 7
Gallstones 55 63 10 23
Extramedullary haemopoiesis 20 24 0 0
Leg ulcers 20 33 0 0
Thrombotic events 28 22 0 0
Cardiopathya 3 5 10 25
PHTb 50 17 10 11
Abnormal liver enzymes 20 22 55 68
HCV infection 7 33 7 98
Hypogonadism 5 3 80 93
Diabetes mellitus 3 2 12.5 10
Hypothyroidism 3 2 15 11
a Fractional shortening < 35%. bDefined as pulmonary artery systolic pressure > 30 mmHg; a well-enveloped tricuspid regurgitant jet velocity could be detected in only 20 patients, so frequency was assessed in these patients only.

Musallam KM et al. Haematologica. 2013;98:833–844.
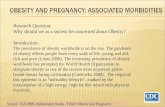
Non-Transfusion-Dependent Thalassemias (NTDT)
β-Thalassemia Major(Regularly transfused)
Silent cerebral ischemia
Pulmonary hypertensionRight-sided heart failure
Cardiac siderosisLeft-sided heart failure
Splenomegaly
Gall stones
Hepatic fibrosis, cirrhosis and cancer
Hepatic failureViral hepatitis
Diabetes mellitus
Hypogonadism
Facies Bone deformity(Hair on end)
Extramedullary hematopoietic psuedotumors
Venous thrombosis
Osteoporosis
HypothyroidismHypoparathyroidism
Osteoporosis
Leg ulcers
Musallam KM, et al. Haematologica. 2013;98:833-4.
Observations were similar in reported literature

Better understanding of the morbidity profile and associated risk factors was thus warranted and motivated a large research program to revisit morbidity in NTDT patients

Cross-sectional study of 584 patients with β-TI from 6 comprehensive care centres in the Middle East and Italy
β-TI, β-thalassaemia intermedia. Taher AT, et al. Blood. 2010;115:1886-92.
The OPTIMAL CARE studyOverview on Practices in β-Thalassaemia Intermedia Management
Aiming for Lowering Complication rates Across a Region of Endemicity:
n = 12S. Daar
n = 127A.T. TaherK.M. Musallam
n = 200M. Karimi
n = 51A. El-Beshlawy
n = 153M.D. Cappellini
n = 41K. BelhoulM. Saned

Taher AT, et al. Blood. 2010;115:1886-92.
High morbidity rates were confirmed
ParameterFrequency
n (%)
Age (years)
< 18 172 (29.5 )
18–35 288 (49.3)
> 35 124 (21.2)
Male:female 291 (49.8) : 293 (50.2)
Splenectomized 325 (55.7)
Serum ferritin (µg/L)
< 1,000 376 (64.4)
1,000–2,500 179 (30.6)
> 2,500 29 (5)
Complications
Osteoporosis
EMH
Hypogonadism
Cholelithiasis
Thrombosis
Pulmonary hypertension
Abnormal liver function
Leg ulcers
Hypothyroidism
Heart failure
Diabetes mellitus
134 (22.9)
124 (21.2)
101 (17.3)
100 (17.1)
82 (14)
64 (11)
57 (9.8)
46 (7.9)
33 (5.7)
25 (4.3)
10 (1.7)
TreatmentFrequency
n (%)Hydroxyurea 202 (34.6)Transfusion
NeverOccasionalRegular
139 (23.8)143 (24.5)302 (51.7)
Iron chelationNoneDeferoxamineDeferiproneDeferiprone + deferoxamineDeferasirox
248 (42.5)300 (51.4)
12 (2.1)3 (0.5)
21 (3.6)

ALF, abnormal liver function; DM, diabetes mellitus; HF, heart failure. Taher AT, et al. Br J Haematol. 2010;150:486-9.
Morbidities seemed to increase with advancing age
Fre
qu
en
cy (
%)
≤ 10 years 11–20 years 21–32 years > 32 years
0
5
10
15
20
25
30
35
40
45
0
*Statistically significant trend.
6.7
13.3
16.7
40.0
26.7
3.3
6.7
16.7
26.7
3.3
13.3
20.0 20.0
3.3
6.7
10.0 10.0
3.3
6.7
33.3
13.3
10.0
20.0
13.3
3.3
6.7
10.0
13.3
0 0
3.3
16.7
0
3.3
10.0
30.0
6.7
16.7
23.3
20.0
0
16.7
23.3
*
* *
**
*
120 treatment-naive patients

• Leg ulcers• Thrombotic events• Pulmonary hypertension
• Bone deformities• Osteoporosis
Impaired α:βglobin ratio
• Diabetes mellitus• Growth deficiency• Hypothyroidism• Hypoparathyroidism• Hypogonadism• Hepatic cancer• Renal disease
Ineffective erythropoiesis haemolysis
Anaemia
Tissue oxygenation
Iron overload
• Gall stones
Hypercoagulable state
Red cell pathology
Musallam KM, et al. Haematologica. 2013;98:833-4.
Erythroid marrow expansion
• Hepatosplenomegaly• Extramedullary
haematopoieticpseudotumors
The pathophysiology and risk factors were predicted … but not yet evaluated

Non-transfusion-dependent thalassemia (NTDT)
Morbidity in NTDT
– Clinical complications profile
– Ineffective erythropoiesis and anemia
– Iron overload and target organ damage
– Hypercoagulability and vascular disease
Agenda

As the primary source of disease process, the question was how can ineffective erythropoiesis and anemia lead to such a diverse complication profile?

Musallam KM, et al. Blood Cells Mol Dis. 2011;47:232-4.
10
100
1000
10000
100000
1000000
- - --
-- -
-
HV
SS
Thal
-tra
it
α-T
hal
β-T
hal
CD
A I
RA
RS
PK
D
β-T
I
GD
F15
(p
g/m
l) -
Ineffective erythropoiesis in untreated patients with β-thalassemia intermedia

Musallam KM, et al. Curr Opin Hematol. 2013; 20:187-92.
Ineffective erythropoiesis
Chronic anemia/hypoxia
↓ Hepcidin↑ Erythropoietin
↓ Ferroportin
↑ Intestinal iron absorption↑ Release of recycled iron
from reticuloendothelial system
Iron overload
?GDF-15
TWGF-1
HIFs
Tmprss6
Transfusions
Minor role
Ineffective erythropoiesis leads to iron overload in NTDT

0
200
400
600
800
1000
1200
1400
1600
1800
2000
0 5 10 15
Seru
m f
err
itin
(n
g/m
L)
Hemoglobin level (g/dL)
Pearson's r=−0.5951, p b 0.001
A hemoglobin of <7 g/dL was the level below which all patients developed a morbidity while a
hemoglobin of >10 g/dLwas the level after which none of the
patients had a morbidity (area under the curve = 0.84, 95% CI:
0.70 to 0.97, p b 0.001)
Taher AT, et al. Blood Cell Mol Dis. 2015;55:108-9.
Chronic anemia is also independently associated with clinical morbidity and iron
overload in NTDT

Thoracic and lumbar regions are most commonly involved
Symptoms develop as a result of pressure on surrounding structures
Spinal cord compression and possible irreversible neurological damage is most significant and debilitating
Haidar R et al. Eur Spine J 2010;19:871–878; Castelli R et al. Am J Med Sci 2004;328:299–303; Chehal A et al. Spine 2003;28:E245–E249; Borgna-Pignatti C. Br J Haematol 2007;138:291–304.
Extramedullary hematopoietic psuedotumorsin NTDT as a result of ineffective
erythropoiesis and anemia/hypoxia
Defective Hb F unloading
Increased bone marrow hematopoietic activity and expansion
Formation of erythropoietic tissue masses
+
Chronic anemia Hypoxia
EXTRAMEDULLARYhematopoiesis
Liver
Glands SpleenPleura
Spine

Leg ulcers2Leg ulcers are more common in older than in younger patients with β-TI
The skin at the extremities of elderly β-TI patients can be thin due to reduced tissue oxygenation; this makes the subcutaneous tissue fragile and increases the risk of lesions
Ulcers are very painful and difficult to cure1
Risk factors: severe anaemia, ineffective erythropoiesis, splenectomy, and hypercoagulability levels3–5
A role for local IOL is suggested; IOL may play a role in the pathophysiology of leg ulcers by causing oxidative stress and not just by local accumulation6 1. Taher AT, et al. Blood Cells Mol Dis. 2006;37:12-20.
2. Levin C, Koren A. Isr Med Assoc J. 2011;13:316-8.
3. Taher AT, et al. Blood. 2010;115:1886-92.
4. Musallam KM, et al. Blood Cells Mol Dis. 2011;47:232-4.
5. Musallam KM, et al. Cold Spring Harb Perspect Med. 2012;a013482.
6. Matta BN, et al. J Eur Acad Dermatol Venereol. 2014;28(9):1245-50.
Leg ulcers in NTDT can develop in the context of anemia and tissue hypoxia

Non-transfusion-dependent thalassemia (NTDT)
Morbidity in NTDT
– Clinical complications profile
– Ineffective erythropoiesis and anemia
– Iron overload and target organ damage
– Hypercoagulability and vascular disease
Agenda

Since it was apparent that NTDT patients develop iron overload in the absence of transfusions, the question was should we be concerned with this iron overload?

● Cumulative process
• Positive correlations between iron overload indices and advancing age1-5
● Slower than transfusionalsiderosis
• 3-4 mg/day or as much as 1,000 mg/year6
• Annual increase in liver iron concentration of 0.38 ± 0.49 mg Fe/g dry7
1. Taher A, et al. Br J Haematol. 2009;146:569-72.2. Taher AT, et al. Br J Haematol. 2010;150:486-9.3. Taher A, et al. Haematologica. 2008;93:1584-6.4. Lal A, et al. N Engl J Med. 2011;364:710-8.5. Chen, FE et al. N Eng J Med. 2000;343:544-50.6. Musallam KM, et al. Blood Rev. 2012;26:16-9.7. Taher AT, et al. Blood. 2012;120:970-7.
0
500
1000
1500
2000
2500
3000
0 20 40 60
Seru
m f
err
itin
(µ
g/L
)
Age (years)
Iron overload in NTDT
β-thalassemia intermedia2
Hemoglobin H disease5
r=0.65P<0.001

0
100
200
300
400
500
600
700
800
900
1000
1100
1200
1300
1400
1500
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Me
an
se
rum
fe
rrit
inle
ve
l a
nd
95
% C
I (n
g/m
l)
p<0.001
Musallam KM, et al. Haematologica 2014;99:e218-21.
SF levels increased over 11 years in 52 non-chelated β-TI patients: The ORIENT study

20
25
30
35
40
45
50
55
60
65
0 500 1000 1500 2000 2500 3000 3500
Serum ferritin (ng/mL)
Car
dia
c T2
* (
ms)
Normal LIC (< 3 mg Fe/g dry wt)
Mild LIC (3–7 mg Fe/g dry wt)
Moderate LIC (7–15 mg Fe/g dry wt)
Severe LIC (> 15 mg Fe/g dry wt)
Normal cardiac R2*
0
5
10
15
20
25
30
0 20 40 60 80 100
LIC
(m
g Fe
/g d
ry w
t)
Cardiac R2* (Hz)
1. Origa R, et al. Haematologica. 2008;93:1095-6.2. Roghi A, et al. Ann Hematol. 2010;89:585-9.3. Taher AT, et al. Am J Hematol. 2010;85:288-90.4. Mavrogeni S, et al. Int J Cardiovasc Imaging. 2008;24:849-54.
n=20 n=49
No evidence of cardiac siderosis even in NTDT patients with considerable iron overload1-4
Iron overload and the heart

Several case reports and case series suggest an association between iron overload and HCC in hepatitis C-negative patients with NTDT
Borgna-Pignatti C et al. Br J Haematol 2004;124:114–117;Maakaron JE et al. Ann Hepatol 2013;12:142–146;Maakaron JE et al. Br J Haematol 2013;161:1;Mancuso A. World J Hepatol 2010;2:171–174;Restivo Pantalone G et al. Br J Haematol 2010;150:245–247.
HCC is one of the most clinically severe complications of NTDT & may be related to iron
overload
Plus iron
HCV
• Possible reasons for increased risk of HCC
in NTDT
– Iron overload is undiagnosed
(serum ferritin underestimates iron
burden compared with TDT)
– Chelation is started late or not at all
– NTDT patients survive longer than
TDT, often an older population
– Hepatocellular > macrophage
distribution

Case reports and case series in the literature reviewed for consistency between patient characteristics
HCC observed in patients with non-viral (hepatitis), non-cirrhotic livers– Of 36 cases, 22 were β TI patients, of whom six were negative for hepatitis B or C
Survey for HCC using an abdominal ultrasound every 6 months is recommended in at-risk patients
*At diagnosisAb, antibody; AFP, alpha-fetoprotein; HBV, hepatitis B virus; HBsAg, hepatitis B surface antigen Maakaron JE et al. Ann Hepatol 2013;12:142–146.
HCC found in non-viral, non-cirrhotic livers, highlighting the potential severity of iron overload and its
complications
HCC is a serious yet often overlooked complication in NTDT with appropriate screening, early detection and adequate iron chelation, complications can be minimized
Sex Age* SurvivalHCV Ab
HCV RNA
HBV AbHBs Ag
AFP (kU/L)
Serum ferritin
(ng/mL)
Serum ferritin peak (ng/mL)
LIC
M 48 Alive at 26 months – – – – 2851 1520 5250 NA
F 61 5 months + – – – 132 369 6000 NA
F 59 25 months + – NA NA NA 990 NA NA
M 73 7 months – – NA NA NA 574 NA NA
M 54 1 months – – – – 17.8 1291 2490 12.3
M 51 4 years – – Vaccinated – 3.8 5602 7138 23.9

Musallam KM, et al. Blood Cells Mol Dis. 2012;49:136-9.
● ∆ TE in non-chelated patients:
4.4 to 5.7 kPa, P<0.001
● ∆ TE in chelated patients:
7.0 to 4.7 kPa, P=0.005
● ∆ TE/yr non-chelated vs. chelated:
+0.3 vs. -0.9 kPa/year, P<0.001
S <3 (n=11)
S 3 (n=1)
S 4 (n=1)
S 5 (n=1)
S <3 (n=11)
S 3 (n=3)
S <3 (n=28) S <3 (n=26)
S 3 (n=2)
First measurement
Lastmeasurement
Chelated
Non-chelated
Transient elastography values corresponding to fibrosis stages are: ≤7.9 kPa for S<3; >7.9 to 10.3 for S 3; >10.3 to 12.0 for S 4; and >12.0 for S 5.
Patients with iron overload had higher fibrosis values on Fibroscan
Iron overload and liver fibrosis

Morbidity absent
Morbidity present
LIC
(m
g Fe
/g d
ry w
t)
p = 0.027p = 0.490 p = 0.245 p = 0.682p = 0.002 p < 0.001 p < 0.001 p = 0.040 p < 0.001 p < 0.001
0
3
6
9
12
15
18
21168 non-chelated
β-TI
On multivariate analysis, a 1 mg Fe/g dw increase in LIC was significantly associated with higher odds of thrombosis, pulmonary
hypertension, hypothyroidism, osteoporosis, and hypogonadism
Adjusted for age, gender, splenectomy status, transfusion history, total hemoglobin level, fetal hemoglobin level, platelet count, NRBC count, and serum ferritin level
Musallam KM, et al. Haematologica. 2011;96:1605-12.
Iron overload and other morbidities

GFR, glomerular filtration rate.
Adapted from Mallat NS, et al. J Nephrol 2013;26:821-8.Adapted from Musallam KM, Taher AT. J Am Soc Nephrol. 2012;23:1299-302.
Renal dysfunction in thalassemia is generally caused by persistent hypoxia, anemia, and
severe IOL
Glomerular dysfunction− vascular resistance results in − GFR
Tubulointerstitial dysfunction– epithelial – mesenchymal transdifferentiation– accumulation of extracellular matrix– activation of fibroblasts– diffusion capacity of oxygen
Tubulointerstitial dysfunction– direct iron cytotoxicity on tubules and
glomerular permeability causes enzymuria + proteinuria
– moderate tubular atrophy and interstitial fibrosis
Tubular dysfunction– vacuolization of proximal tubular epithelium– apoptosis of tubule cell– tubular absorption of solutes
Anemia
Iron overload
Hypoxia
Iron chelation
Glomerular dysfunction– mild to moderate glomerulosclerosis– GFR
Glomerular dysfunction– reversible haemodynamic changes

Renal dysfunction in β-TI is associated with iron overload
• 48% had evidence of glomerular hyperfiltration
• 14% patients had proteinuria* patients had elevated LIC>7 mg Fe/g dw, NTBI and nucleated RBC counts
A considerable proportion of patients showed evidence of abnormally elevated
eGFR, with a declining trend towards advancing age
Occurrence of proteinuria associated with anemia, hemolysis and iron toxicity
*UPr/UCr ratio >500 mg/g Ziyadeh FN, et al. Nephron Clin Prac. 2012;121:c136-c43.
rs=0.357P=0.011
rs=0.444P=0.001
N=50

• 127 TI patients were observed for 10 years
• 6 (4.7%) developed ESRD that required regular haemodialysis– 4 showed no abnormality in
urine sediment or proteinuria
– 2 showed glomerular-range proteinuria
• 1 reached nephrotic range (biopsy showed FSGS)
ESRD, end-stage renal disease; FSGS, focal segmental glomerulosclerosis. Mallat NS, et al. Blood Cells Mol Dis. 2013;51:146-8.
Long-term follow-up of NTDT patients is crucial to identify TI patients at risk of end-
stage renal disease
Tubular atrophy and interstitial fibrosis
Segmental sclerosis in a glomerulus
Iron deposits (Prussian blue stain)

Non-transfusion-dependent thalassemia (NTDT)
Morbidity in NTDT
– Clinical complications profile
– Ineffective erythropoiesis and anemia
– Iron overload and target organ damage
– Hypercoagulability and vascular disease
Agenda

Surely, iron overload is not the only risk factor for morbidity, so the question was what other key players are involved?

Transfusion
↓ Antithrombin III↓ Protein C↓ Protein S
Iron overload
Endocrine & hepaticdysfunction
Endothelial injury Expression of adhesion molecules and tissue factor
Splenectomy
Platelet abnormalities Thrombocytosis Chronic activation
↑ Adhesion and aggregation
Pathologic RBCs ↑ Thrombin generation
(phosphatidyl serine exposure) ↑ Rigidity, deformability, and
aggregation
↑ Circulating microparticles
?↑ Atherosclerosis
THROMBOSIS
↓↑ ↑ ↑
↑
Musallam KM, et al. Haematologica. 2013;98:833-4.
Hypercoagulability and vascular disease in NTDT

Musallam KM, et al. Thromb Res. 2012;130:695-702.
Hemoglobin
Denaturation Degradation
Excess α-chains
Hemichromes
Inclusion bodies
Band 3 clustering
Oxidation
ROS
Fe++
Spectrin & Band 3 abnormalities
PS exposure
PS
PS
ThrombinFVa, FXa, FII
↓ Protein C & S
↑ RBC adhesion & aggregation
↑ Platelet activation& adhesion
↑ WBC activation
Fibrin
Endothelial damage/activation
Tissue factor, ELAM-1, ICAM-1, VCAM-1, VWF
Thrombus formation
RBC

• Patients (N = 8,860)
– 6,670 with β-TM
– 2,190 with β-TI
• 146 (1.65%) thrombotic events
– 61 (0.9%) with β-TM
– 85 (3.9%) with β-TI
• Risk factors for developing thrombosis in β-TI were
– age (> 20 years)
– previous thromboembolic event
– family history
– splenectomy
Thromboembolic events in a large cohort of β-TI patients
Taher A, et al. Thromb Haemost. 2006;96:488-91.DVT = deep vein thrombosisPVT = portal vein thrombosis; STP = superficial thrombophlebitis
Thromboembolic events (%)
Typ
e o
f ev
en
t12
8
19
12
39
9
66
30
0
11
8
23
28
48
0 20 40 60 80
Others
STP
PVT
PE
DVT
Stroke
Venous
TM (n = 61)
TI (n = 85)

Parameter Group OR 95% CI p value
NRBC count ≥ 300 x 106/L Group III 1.00 Referent
< 0.001Group II 5.35 2.31–12.35
Group I 11.11 3.85–32.26
Platelet count ≥ 500 x 109/L Group III 1.00 Referent
< 0.001Group II 8.70 3.14–23.81
Group I 76.92 22.22–250.00
PHT Group III 1.00 Referent
0.020Group II 4.00 0.99–16.13
Group I 7.30 1.60–33.33
Transfusion naivety Group III 1.00 Referent
0.001Group II 1.67 0.82–3.38
Group I 3.64 1.82–7.30
OPTIMAL CARE study: multivariate analysis on risk factors for thrombosis in
splenectomised patients
Group I patients had significantly higher NRBC, platelets, and PHT occurrence, and were
mostly non-transfused
NRBC = nucleated red blood cell; PHT = pulmonary hypertension; OR = adjusted odds ratio; CI = confidence interval.
Taher AT, et al. J Thromb Haemost. 2010;8:2152-8.

Study Number of
patients
Age (years) MRI technique Definition of infarction Prevalence of SCI
(95% CI)
Manfre et al. 1999 16 Mean: 29
Range: 9-48
0.5 Tesla
T2- spin-echo
weighted
imaging
Abnormally high signal
intensity on long TR-
weighted images
Two blinded
neuroradiologists
37.5% (18.4-61.7)
Taher et al. 2010 30 Mean: 32.1
Range: 18-54
3.0 Tesla
T1-, T2-gradient-
echo-, FLAIR-,
diffusion-
weighted
imaging
Abnormally high signal
intensity on the T2- and
FLAIR-weighted imagesa
Two blinded
neuroradiologists
60.0% (42.2-75.5)
Karimi et al. 2010 30 Mean: 24.3
Range: 18-34
1.5 Tesla
T1-, T2-, FLAIR-
weighted
imaging
Abnormally high signal
intensity on the T2- and
FLAIR- weighted images
One neuroradiologist
26.7% (14.2-44.6)
Teli et. al 2012 24 Mean: 12
Range: 4.5-20
N/A N/A 0%
Musallam KM, et al. Thromb Res. 2012;130:695-702.
aOther diagnoses were ruled out based on the radiological appearance of lesions (e.g. viral encephalopathy or multiple sclerosis) or absence of associated risk factors and clinical symptoms (e.g. vasculitis or Binswanger’s disease).FLAIR, fluid attenuation inversion recovery; N/A, data not available; CI, confidence interval.
Silent cerebral infarction in splenectomized patients

Increasing age and transfusion naivety are associated with a higher incidence and multiplicity of white matter lesions
Pro
bab
ility
of
abn
orm
alit
y
Age (years)
10 15 20 25 30 35 40 45 50 55 600.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1.1
Pat
ien
ts (n
)
No. of abnormalities
0
12
3
4
5
6
≤ 30 30–40 40–50 > 50
Non-transfused
Occasionally transfused
0
12
3
4
5
6
Age (years)
0 > 11
Taher AT, et al. J Thrombosis Haemost. 2010;8:54-9.
Risk factors for silent cerebral infarction

Large vessel stenosis on MRA1
– Association with anemia and high NTBI
Decreased neuronal function on PET-CT2
– Association with elevated LIC
Other cerebrovascular complications in splenectomized β-TI patients
1. Musallam KM, et al. Eur J Haematol. 2011;87:539-462. Musallam KM, et al. Ann Hematol. 2012;91:235-41.

* p < 0.001 for all parameters for patients with PHT versus those without PHTAOR = adjusted odds ratio
β-TI patients (N = 64)
Parameters PHT+* PHT−
Splenectomized%AOR (95% CI)
84.44.9 (1.9–8.5)
46.9
History of thromboembolic events%AOR (95% CI)
40.63.69 (2.38–7.05)
7.8
Nucleated RBC countMean (SD; x 106/L)AOR (95% CI)
354.2 (199.2)2.59 (1.69–6.05)
214.7 (94.5)
Transfusion naivety%AOR (95% CI)
56.23.5 (2.1–6.25)
78.1
Iron chelation naivety%AOR (95% CI)
37.52.3 (1.2–4.25)
62.5
Hydroxyurea naivety%AOR (95% CI)
17.22.6 (1.1–5.25)
34.4
Karimi M, et al. Eur J Intern Med. 2011;22:607-10.
Risk factors for PHT: OPTIMAL CARE

PASP, pulmonary artery systolic pressure; TCG, tricuspid gradient.
Derchi G, et al. Circulation. 2014;129:338-45. Isma’eel H, et al. Am J Cardiol. 2008;102:363-7.
Risk of Pulmonary Hypertension in NTDT increases with high LIC, advancing age, and splenectomy
PHT (defined as PASP ≥ 30 mmHg) present in 38.5%
Significantly correlated with LIC
Not correlated with age, Hb level, and SF level
LIC
(m
g Fe
/g d
ry w
t)
Tricuspid gradient (mmHg)
40
30
20
10
0
SF (µg/L)
r = 0.514p = 0.01
r = 0.097p = 0.513
20 40 60 80
5,000
4,000
3,000
2,000
1,000
0
SFLICTCG and SFTCG and LIC
0
10
20
30
40
50
60
70
80
90
100
18 28 38 48 58 68 78P
rob
abili
ty o
f P
HT
(%)
Age (years)
All patientsNon-splenectomisedSplenectomised
PHT prevalence in thalassaemia was 2.1%
(TI 4.8%, TM 1.1%)

With all this morbidity it was not surprising that β-TI patients had poor HR-QoL
***
*P < 0.05
0102030405060708090
100
β-TIβ-TM
Mea
n s
cale
sco
re
Musallam KM, et al. Eur J Haematol. 2011;87:73-9.

Takeaways• There is a high prevalence of morbidities in NTDT patients and their
prevalence increases with age, starting at the age of 10 years.
• Morbidities in NTDT stem from the interaction of multiple pathophysiological factors: ineffective erythropoiesis, iron overload (IOL), and hypercoagulability
• Ineffective erythropoiesis and hemolysis are also associated with a hypercoagulable state, ultimately leading to a high incidence of thromboembolic and cerebrovascular events, as well as pulmonary hypertension
• Ineffective erythropoiesis is associated with low hepcidin levels, which subsequently lead to IOL.

Takeaways• IOL in NTDT patients is a cumulative process that can lead to several iron-
related morbidities in the liver (liver fibrosis), endocrine glands (endocrinopathies), and vascular system (vascular disease)
• There exists an association between IOL and hepatocellular carcinoma (HCC) in hepatitis C-negative patients with NTDT, suggesting that HCC is a newly emerging adverse complication as a consequence of the prolonged survival of thalassemia patients.
• Renal dysfunction in NTDT has also been described and is caused by persistent hypoxia, anemia, and severe IOL