monoclonal antibodies in therapeutics
59
Monoclonal Antibodies in Therapeautics DR. SARJU R. ZILATE
-
Upload
sarju-zilate -
Category
Health & Medicine
-
view
216 -
download
2
Transcript of monoclonal antibodies in therapeutics

Monoclonal Antibodies in Therapeautics
DR. SARJU R. ZILATE

Monoclonal Antibodies
Monoclonal antibodies (MAb) are antibodies that are
identical because they are produced by one type of immune
cell; all are clones of a single parent cell.
Monoclonal antibodies (MAbs) are an integral part of
targeted therapy approach for various diseases which
result in decrease in adverse effects and increase in
efficacy.
They target various receptors or various growth factors on
the cell surface and modulate their vital functions and
cause cell death by various mechanisms.


The Structure of an Antibody

Antibody FunctionAntibodies have two major functions:
•Recognize and bind antigen
•Induce immune responses after binding
The variable region mediates binding
•Affinity for a given antigen
•confers absolute specificity for an antigen
The constant region mediates immune response afterbinding
•Different classes of constant regions generatedifferent isotypes
•Different isotypes of antibody have differingproperties

Production of monoclonal antibodies
• Since 1975, when Keller and Milstein developed
hybridoma technology,
• technological strides towards the production of antibodies
have been made.
• The first success in generating human mAbs (hmAbs)
with predefined specificity was conducted in 1980
through
• the fusion of human spleen cells from patients with
human myelomas.

• Since then, several major methods have been
established to generate hmAbs, including
• 1) immortalization of antigen-specific human B cells;
• 2) acquisition of antigen-specific human B cells via
phage display technology;
• 3) the production of hmAbs from transgenic mice;
• 4) single human B cell cloning techniques to directly
clone and express immunoglobulin (Ig) genes in vitro
from antigen-specific B cells.


Conventional hybridoma technology
• Step 1: Immunization of mice
• Mice are immunized with an antigen (attached to
adjuvant).
• The antigen can be whole cells, membrane fragment, or
complex molecules.
• Mice serum’s are screened using various techniques such
as ELISA.
• When sufficient titre is reached the mice are euthanized
and spleen is removed as a source of cells for cell fusion.

• Step 2: Preparation of Myeloma Cells
• Myeloma cells are immortalized cells that are capable of
dividing indefinitely.
• These cells are treated with 8-azaguanine to ensure
sensitivity to HAT

• Step 3: Fusion of myeloma cells with Spleen cells:
• spleen cells harvested from mice are fused with myeloma
cells. ,through co-centrifuging in polyethylene glycol.
• Cells are plated in selection medium
• Hypoxanthine-aminipterin-thymidine (HAT) selection
medium –blocks nucleotide synthesis.
• Only fused cells with grow on HAT. Cells are distributed on
feeder cells (murine bone-marrow) to promote growth of
the hybridomal cells.

• Step 4: Cloning of Hybridoma cells .
• A mouse is inoculated with the cell and thereby becomes a
factory for producing the MAbs.
• Ascites fluid collected from the mouse
• Step 5: Antibody is screened and purified:
• Antibodies are screened using specific Ag binding.
Advantage of in vivo
• Step 6: Desired antibodies are cloned:
• This is done in vitro on culture bottle

Immortalization of antigen-specific humanB cell and hybridoma technology
• Hybridoma technology has contributed to virtually all
areas of biology and medicine
• and has been greatly refined since its introduction in 1975.
• human antibody-secreting cells can be immortalized by
fusion of antibody-producing human B lymphocytes with
either mouse or human myeloma or lymphoblastoid cells
by infection with the EBV.

Phage display(1985)
• successfully used
• to select antigen-specific variable region genes and
• to express functional antibody fragments with unique
specificity.
• the library of diverse human immunoglobulin-heavy
chain variable (VH) gene and light chain variable (VL)
gene segments are prepared by reverse transcription of
mRNA from B cells and PCR amplification.

• The gene encoding single chain variable fragment (scFv)
can be created by randomly combining VH and VL gene
segments using PCR.
• After bio-panning the phages bound to a range of antigens
or haptens, antigen-specific antibody fragments with good
affinities can be identified.
• One phage display-derived mAb has been approved by the
FDA and at least 35 human mAbs generated by phage
display technology have entered into clinical development.
Phage display(1985)

Transgenic mice
• Genetically engineered mice expressing humanantibody repertoires were first reported forgenerating hmAbs using the hybridoma technology in1994.
• disruption of endogenous mouse
Ig-heavy chain and
Igκ-light chain loci together
• with the introduction of
human Ig-heavy chain and
Igκ-light chain genes.

Generation of mAbs from single human B cells by Ig gene cloning and expression in vitro
This approach requires the
• isolation of individual B cells from mouse
spleen or human PBMCs using magnetic
microbeads conjugated with B-cell-selective
markers
•The light-chain and heavy-chain genes
• coding for variable fragments of antibody
• in each cell
•are separately amplified by RT-PCR
•and then combined with the sequences by anoverlapping PCR technique.
•For each cell,
• Ig heavy- and corresponding Ig light-chain gene
transcripts are amplified by nested RT-PCR and
• cloned into mammalian expression vectors to
produce hmAb with defined specificity in vitro.

Types of mAbs
19
Purple denotes human component orange murine component

EVOLUTION OF MONOCLONAL ANTIBODY
1. TRANSGENIC
2. LIBRARIES
a.BACTERIOPHAGE
b. mRNA
c. Cell Surface
Ist
generation
mab
2nd generation mab
daclizumab

Types of monoclonal antibodies
1. Murine source MAbs: rodent MAbs with excellentaffinities and specificities generated usingconventional hybridoma technology.
2. Chimeric MAbs: chimers combine the humanconstant regions with the intact rodent variableregions. Affinity and specificity unchanged.
3. Humanized MAbs: contained only the CDRs of therodent variable region grafted onto human variableregion framework
4. Recombinant DNA engineered MAbs

Murine
Derived from mice
Patients treated with murine mAbs develop a human
antimouse antibody (HAMA) response
Rapid clearance of the mAb
Poor tumour penetration
Hypersensitivity reactions
90Y-ibritumomab
131I -Tositumomab
22
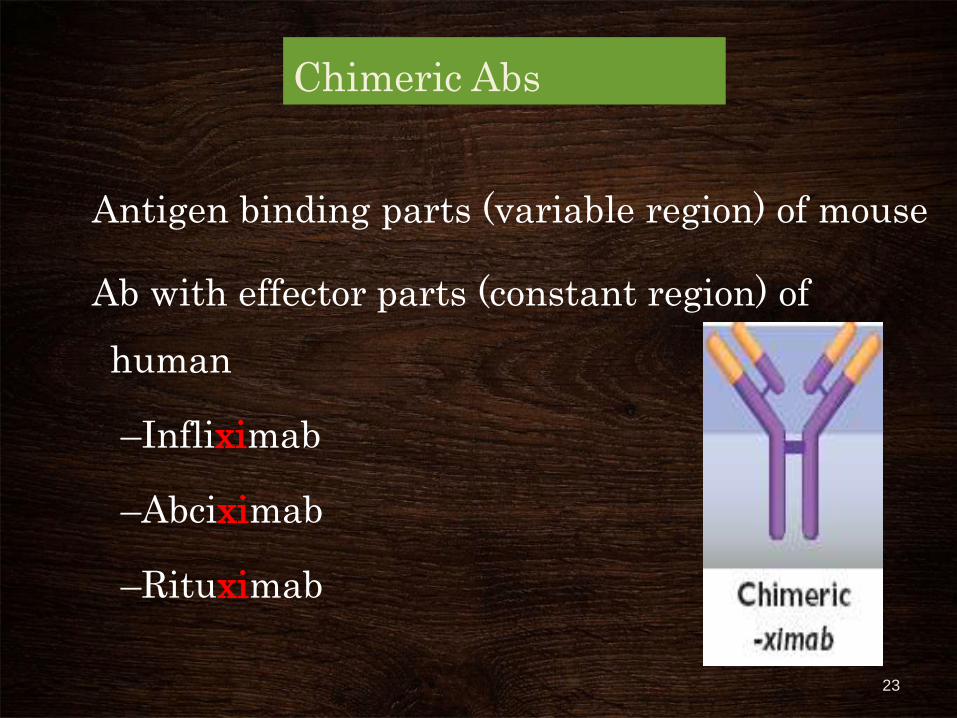
Chimeric Abs
Antigen binding parts (variable region) of mouse
Ab with effector parts (constant region) of
human
–Infliximab
–Abciximab
–Rituximab
23
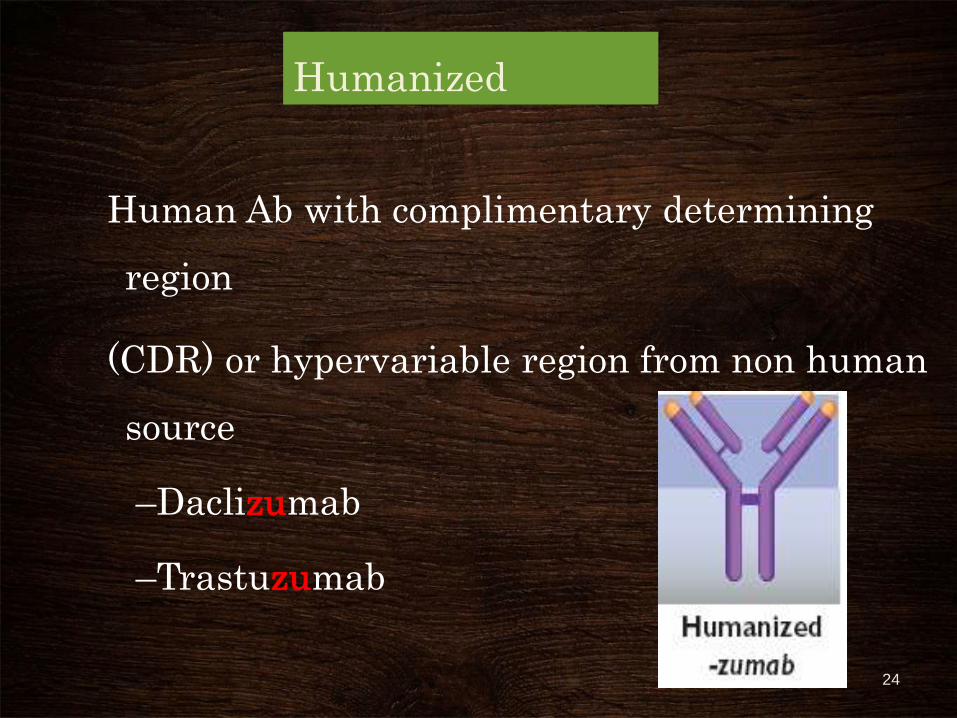
Humanized
Human Ab with complimentary determining
region
(CDR) or hypervariable region from non human
source
–Daclizumab
–Trastuzumab
24

Human Abs
Recombinant DNA technology:
Genes for variable Fab portion of human Abs is
inserted in genome of bacteriophages & replicated
Mixed with Ag & complementary Ab producing
phages selected
e.g. Adalimumab
25
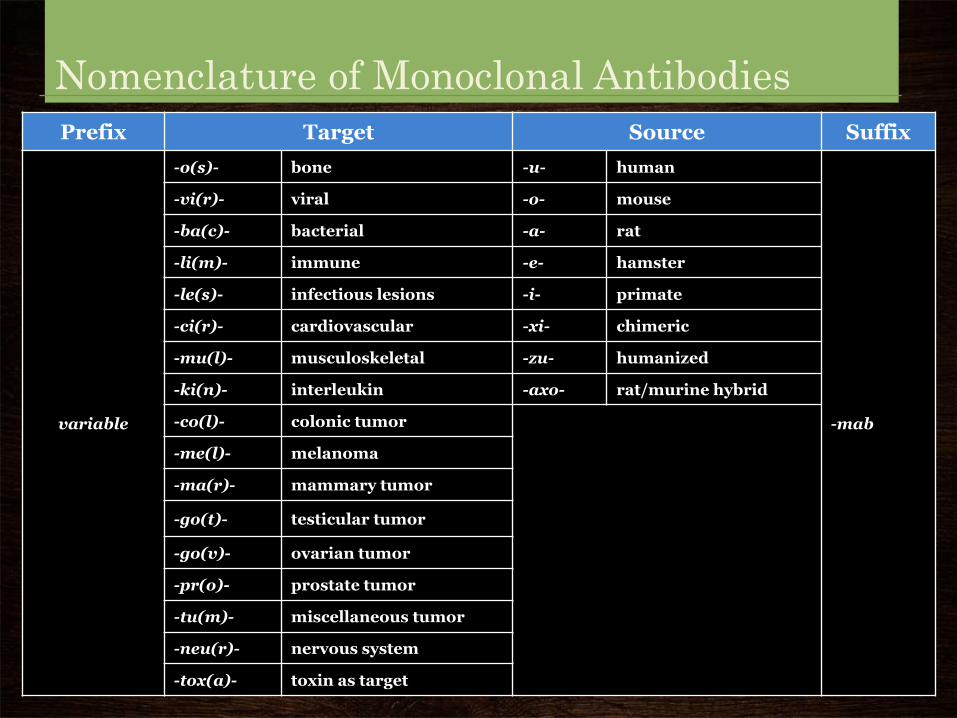
Nomenclature of Monoclonal Antibodies
Prefix Target Source Suffix
variable
-o(s)- bone -u- human
-mab
-vi(r)- viral -o- mouse
-ba(c)- bacterial -a- rat
-li(m)- immune -e- hamster
-le(s)- infectious lesions -i- primate
-ci(r)- cardiovascular -xi- chimeric
-mu(l)- musculoskeletal -zu- humanized
-ki(n)- interleukin -axo- rat/murine hybrid
-co(l)- colonic tumor
-me(l)- melanoma
-ma(r)- mammary tumor
-go(t)- testicular tumor
-go(v)- ovarian tumor
-pr(o)- prostate tumor
-tu(m)- miscellaneous tumor
-neu(r)- nervous system
-tox(a)- toxin as target

Nomenclature
Suffix
–Human: -umab
–Humanized: -zumab
–Murine: -momab
–Chimeric: -ximab
27

Examples
•ab- + -ci- + -xi- + -mab: chimeric monoclonal antibody used on the cardiovascular system.
•tras- + -tu- + -zu- + -mab: humanized monoclonal antibody used against a tumor.
• Pali- + -vi- + -zu- + -mab
humanized mab used against a virus (RSV)

Pharmacokinetics: mAbs
• Routes of administration:
Subcutaneously (Rituximab, Trastuzumab, Adalimumab)
Intramuscularly (Palivizumab)
Intravenously
• IV route: preferred because of 100% bioavailability
• Route for elimination of antibodies
Via uptake & catabolism by reticuloendothelial system & target tissue.
29

P/K: mAbs
•Half-life
Chimeric : 4 –15 days
Humanized: 3 - 24 days
Recombinant human: 11– 24 days
•Human antimouse antibody (HAMA) response develops 7–10 days following exposure to murine antibody
30

MOA
• 1.Make the cell more visible to the immune system:
• The immune system attacks foreign invaders in your body, but it doesn't always recognize cancer cells as enemies. A monoclonal antibody can be directed to attach to certain parts of a cancer cell. In this way, the antibody marks the cancer cell and makes it easier for the immune system to find.
• 2. Block growth signals- cetuximab
• 3.Deliver radiation to cells: By combining a radioactive particle with a monoclonal antibody, doctors can deliver radiation directly to the cancer cells.

Therapeutic uses
• Immunosuppression
•Autoimmune diseases
•Malignancies
•Antiplatelet therapy
• Infectious diseases
•Asthma
• Osteoporosis32

Monoclonal antibodies in therapeutic use:
• ANTI CD3:
• CD 3 is a co receptor which plays an important role inT cell receptor signaling.
• MUROMUMAB (OKT3) is a drug which blocks thisreceptor. It blocks killing by cytotoxic T cells and manyother T cell functions. It kills cells by blocking vitalfunctions of CD3, approved for treatment of renalallograft rejection crisis.
• TEPLIZUMAB is a newer anti CD3 drug. It isused for
• protecting remaining beta cells in newly diagnosedtype I DM. It is currently in phase III clinical trials.

• ANTI CD20:
• RITUXIMAB:
• Its mechanisms of action in killing cancer cells are-
ADCC ,CDC and direct induction of apoptosis with
proven efficacy against wide range of NHL B-cell
malignancies.
• Dose: 375mg/m2 IV infusion weekly for 4 weeks.
• Side effects are fever with rash, dyspnoea and late onset
neutropenia.

• OCRELIZUMAB is a newer CD20 drug .
• It targets mature B lymphocytes and thus is an
immunosuppressive drug.
• It is currently in Phase III.
• It is used in RA, SLE, MS and lymphomas.
• OFATUMUMAB
• is also a newer CD20 drug.
• It inhibits early B lymphocyte activation.
• It targets different epitope of that by rituximab.
• It was approved in February 2010 for refractory CLL.

Radiolabelled Anti CD20
• Radiolabelling the monoclonal antibodies increases
their efficacy.
• They can also be used for various imaging purposes.
• Yttrium 90-ibritumomab (Y90),
• Indium 111- ibritumomab (In111),
• Iodine 131- tositumomab (I131 sub) are the 3
commonly radiolabelled anti CD20 MAbs.

• They show increase in efficacy than their naked
counterparts.
• Effective in relapsed /refractory/advanced cases
of follicular B-cell lymphoma and NHL in the
doses of 0.4 ci/kg IV.
• Its side effects are myelodysplasia and
hematological toxicities

ANTI CD 22:
• CD22 is a co receptor important for B cell receptor
signaling.
• EPRATUZUMAB is a drug which blocks CD22
signaling.
• It is currently in phase III clinical trials.
• It is active against malignant B cells and used in SLE.
• It produces cell death by ADCC

ANTI CD52:
• CD52 is present on thymocytes, macrophages,lymphocytes and monocytes.
• ALEMTUZUMAB, is a drug which blocks the CD52
• signaling.
• It kills tumor cells by ADCC, CDC and apoptosis.
• It is Administered IV 30mg/day thrice weekly.
• Premedication with diphenhydramine andacetaminophen should precede this drug sincehypersensitivity reactions are common.
• It used in B cell and T cell lymphomas and MS.
• Its side effects are T cell depletion andimmunosuppression.
ANTI CD33:
• CD33 is a co receptor found on myeloid cell surface.
• GEMTUZUMAB OZOGAMICIN (MAb linked to a
toxin). Humanized MAb covalently linked to a
semisynthetic derivative of calicheamicin .
• It causes DS DNA breaks and cell death.
• Its dose is 2 doses of 9mg/m2 IV separated by 14 days.
• It is used in AML.
• Its side effects are hematopoietic suppression and vaso
occlusive disorders.

• LINTUZUMAB
• is a newer anti CD33 MAb.
• It is currently in phase III for AML.

ANTI CD 11a:
• CD 11a is a co receptor found on B cells and important
in cell to cell adhesion and co-stimulation.
• EFALIZUMAB is a drug that blocks CD11a signaling.
• It is approved for the treatment of adult patients with
severe psoriasis.
• It administered by SC injections.

ANTI HUMAN EPIDERMAL GROWTH FACTOR RECEPTOR 2/ NEU:
• Human epidermal growth factor receptor is a factor which
plays an important role in growth of many breast cancers.
• TRASTUZUMAB
• is a drug which blocks this receptor.
• it causes cell death by inhibition of HER2 signaling with
G1 arrest and also by ADCC and apoptosis .
• Its dose is loading dose of 4mg/kg IV followed by 2 mg/kg
weekly.

• It is used in HER2-positive metastatic breast
cancers.
• Its side effects are cardiomyapathy and flu like
syndrome.
• PERTUZUMAB is a newer HER2 blocking MAb.
• It is currently in clinical trials

ANTI EPIDERMAL GROUTH FACTOR RECEPTOR (EGFR)
• Epidermal growth factor receptor plays a vital role in
growth of many cancers.
• CETUXIMAB is a drug which blocks EGFR signaling and
causes cell death by ADCC.
• Its dose is loading dose of 400mg/kg infusion followed by
250mg/kg weekly.
• It is used in metastatic colorectal and head and neck
cancers.
• ITS SIDE effects are infusion related toxicity and skin rash.

• PANITUMUMAB –
• It is an another EGFR receptor blocking MAb..
• Produces cell death by similar mechanism as
cetuximab.
• It was approved in September 2006.
• It is used in metastatic colorectal and head and neck
cancers.
• Its adverse effects are skin rash and fatigue.
• First MAb approved by FDA developed from transgenic
mice.

• MATUZUMAB and NIMOTUZUMAB
• are the other EGFR blocking MAbs
• which are in phases III of clinical trials.

ANTI VASCULAR ENDOTHELIAL GROUTH FACTOR (VEGF)
• Vascular endothelial growth factor plays an important role
in angiogenesis and neo vascularization of various tumors.
• BEVACIZUMAB is a drug which blocks VEGF.
• It inhibits angiogenesis and neovascularization
• in the dose of 5mg/kg IV every 14 days until disease
progression stops.
• It is used in colorectal and head and neck cancers.
• Its side effects are hypertension, pulmonary hemorrhages,
GI perorations and CCF.

• RANIBIZUMAB is a newer VEGF blocking drug.
• It is used in neovascular macular degeneration.
• It is injected directly into vitreous cavity.

Side effects of monoclonal antibody
• In general, the more common side effects caused by
monoclonal antibody drugs include:
• Allergic reactions, such as hives or itching
• Flu-like symptoms, including chills, fatigue, fever, and
muscle aches and pains
• Nausea
• Diarrhea
• Skin rashes

Rare, but more serious side effects of monoclonal antibody therapy may include:
• Infusion reactions. Severe allergy-like reactions can occur
and in very few cases lead to death.
• Dangerously low blood cell counts. Low levels of red blood
cells, white blood cells and platelets may lead to serious
complications.
• Skin problems
• Bleeding. Some of the monoclonal antibody drugs are
designed to stop cancer from forming new blood vessels.
There have been reports that these medications can cause
bleeding.

Agent Target(s) FDA-approved
indication(s)
Ado-trastuzumab emtansine
(Kadcyla)
HER2 (ERBB2/neu) Breast cancer
(HER2+)
HER2 (ERBB2/neu) exon 21
substitution
(L858R) mutations)
Aldesleukin (Proleukin) Renal cell carcinoma
Melanoma
Alemtuzumab (Campath) CD52 B-cell chronic
lymphocytic
leukemia
Brentuximab vedotin (Adcetris) CD30 Hodgkin lymphoma
Anaplastic large cell
lymphoma
Belimumab (Benlysta) BAFF Lupus
erythematosus
Belinostat (Beleodaq) HDAC Peripheral T-cell
lymphoma

Bevacizumab (Avastin) VEGF ligand Cervical cancer
Colorectal cancer
Fallopian tube
cancer
Glioblastoma
Non-small cell
lung cancer
Ovarian cancer
Peritoneal cancer
Renal cell
carcinoma
Canakinumab (Ilaris) IL-1β Juvenile idiopathic
arthritis Cryopyrin-
associated periodic
syndromes
Cetuximab (Erbitux) EGFR (HER1/ERBB1) Colorectal cancer
(KRAS wild type)
Squamous cell
cancer of the head
and neck

Denosumab (Xgeva) RANKL Giant cell tumor of
the boneIbritumomab tiuxetan (Zevalin) CD20 Non-Hodgkin's
lymphoma
Ipilimumab (Yervoy) CTLA-4 Melanoma
Nivolumab (Opdivo) PD-1 Melanoma
Obinutuzumab (Gazyva) CD20 Chronic lymphocytic
leukemia
Ofatumumab (Arzerra, HuMax-
CD20)
CD20 Chronic lymphocytic
leukemia
Panitumumab (Vectibix) EGFR (HER1/ERBB1) Colorectal cancer
(KRAS wild type)
Pembrolizumab (Keytruda) PD-1 Melanoma

Pertuzumab (Perjeta) HER2 (ERBB2/neu) Breast cancer (HER2+)
Ramucirumab (Cyramza) VEGFR2 Gastric cancer or
Gastroesophageal
junction (GEJ)
adenocarcinoma Non-
small cell lung cancer
Rituximab (Rituxan, Mabthera) CD20 Non-Hodgkin’s lymphoma
Chronic lymphocytic
leukemia Rheumatoid
arthritis Granulomatosis
with polyangiitis
Siltuximab (Sylvant) IL-6 Multicentric Castleman's
disease
Tocilizumab (Actemra) IL-6R Rheumatoid arthritis
Juvenile idiopathic
arthritis

Tositumomab (Bexxar) CD20 Non-Hodgkin's
lymphoma
Trastuzumab (Herceptin) HER2 (ERBB2/neu) Breast cancer
(HER2+) Gastric
cancer (HER2+)

TO SUMMARISE :
MAbs are highly specific Abs produced by a clone of
single hybrid cells formed by fusion of B cell with the
tumor cell.
The hybridoma formed yields higher amount of
MAbs.
MAbs can be produced in vitro and in vivo .
Animals are utilized to produce MAbs, but these
antibodies are associated with immunogenicity and
ethical problems.

Recombinant DNA technology, genetic
engineering and transgenic animals are used to
produce humanized MAbs or pure human MAbs,
with fewer ADRs
Used for treatment of cancer, autoimmune
disorders, graft rejections, infections, asthma etc.

•THANKS









![Monoclonal Antibodies - Copy [Autosaved]](https://static.fdocuments.in/doc/165x107/577c7e6a1a28abe054a109e9/monoclonal-antibodies-copy-autosaved.jpg)