Monitoring of Aflatoxins in Human Body Fluids and...
8
[CANCER RESEARCH 45, 922-928, February 1985] Meeting Report Monitoring of Aflatoxins in Human Body Fluids and Application to Field Studies1 The objective of this workshop was 2-fold: (a) to review critically the current methodologies for detecting AFB!2 and its metabolic by-products in biological materials in order to assess human exposure to this carcinogen; and (o) to identify field studies planned or in progress which might be suitable for the examination of the interaction between persistent HBV infection, AF exposures, and/or other factors in the etiopathogenesis of PHC. Epidemiological studies (3,32,35) have strongly implicated HBV infection as a major risk factor in the induction of PHC. However, a number of other studies also indicate a multifactorial origin for this type of cancer. Recent studies (16, 26, 47) have shown that the differences in hepatitis B surface antigen carrier rates in urban and rural populations could not account for the difference in incidence of PHC in these 2 groups. At present, there is no clear evidence that HBV as such has neoplastic transforming activity in cultured cells or in experimental animals, although viruses similar to HBV have been found to cause PHC under natural conditions in woodchucks. Integration of HBV DMA in both normal and neoplastic liver cells has been demonstrated (32, 43). Additional risk factors, including mycotoxins (16, 22, 23, 30) and alcohol consumption (4), must, however, continue to be considered of etiological importance. The considerable evidence implicating AF as a carcinogen in animals and the correlation studies demonstrating geographic concordance between populations with high AF exposure rates and a high incidence of PHC suggest that AF may be an important human carcinogen (23, 50). However, only longitudinal studies of individuals at high risk of PHC will conclusively establish AF as a human carcinogen. To date, the lack of tests suitable for measuring short- and long-term individual exposure to AF has impeded these longitudinal studies. Although there is limited systematic survey in some countries, AF has been demonstrated in many commonly consumed food- 1This meeting was organized by the International Agency for Research on Cancer (IARC, Lyon, France) and was held in Lyon, on April 26 to 27,1984. The participants were H. Autrup, Miljo og Kraett Laboratories Copenhagen, Denmark; H. Bartsch, IARC; F. X. Bosch, IARC; F. S. Chu, Department of Food Microbiology and Toxicology, Food Research Institute, University of Wisconsin, Madison, Wl; N. Day, IARC; M. Friesen, IARC; C. Gamer (Recorder), Cancer Research Unit, Heslington, York, United Kingdom; C. Harris, NIH, Laboratory of Human Carcinogenesis, Bethesda, MD; R. Montesano (Secretary), IARC; N. Mu ñoz,IARC; G. E. Neal, Toxicology Unit, Medical Research Council, Carshalton, Surrey, United Kingdom; K. Randerath, Department of Pharmacology, Baylor College of Medicine, Texas Medical Center, Houston, TX; R. Ryder (Recorder), Tufts University School of Medicine, New England Medical Center Hospital, Boston, MA; P. Sizaret, Biologicals Unit, World Health Organization, Geneva, Switzerland; L. Tomatis (Director), IARC; T. Sun, Department of Immunology, Cancer Institute, Chinese Academy of Medical Sciences, Beijing, People's Republic of China; D. Umbenhauer, IARC; H. P. van Egmond, National Institute of Public Health, Bil- thoven, Netherlands; G. N. Wogan (Chairman), Department of Nutrition and Food Science, Massachusetts Institute of Technology, Cambridge, MA. This document has been published as an IARC Internal Technical Report 1984/ 03. 2 The abbreviations used are: AFBi, aflatoxin B,; AF, aflatoxin; ELISA, enzyme- linked immunoabsorbent assay; HBV, hepatitis B virus; HPLC, high-pressure liquid chromatography; PHC, primary hepatocellular carcinoma; RIA, radioimmunoassay; HB, hepatitis B. Received October 1, 1984; accepted November 13,1984. stuffs. The occurrence of AF in foods is not only due to poor storage but also attributed to its presence in raw materials in which the toxins are produced in the fields due to fungal infes tation (1, 5, 36, 55). However, epidemiological studies seeking to establish AF as a human hepatocarcinogen have not been able to establish whether the important risk factor for PHC is the degree of individual exposure to AF over a prolonged period of time or if it is the presence of a unique metabolic pathway. Particularly carcinogenic AF metabolites may be produced in certain high-risk individuals; alternatively, AF exposure may be particularly important in patients with persistent HBV infection. The clarification of these various possibilities may result in more effective measures of primary prevention of PHC. Various vaccination projects against HBV are planned or are under way in regions of the world where HB infection is endemic and where the long-term outcome may be expected to reduce the incidence of PHC. Given the relatively extensive knowledge of the activity of AF in human cell systems, its routes of metab olism, the availability of markers for metabolic by-products and cellular damage, and the evidence that not all cases of PHC can be attributed solely to HBV, it would seem that, in large-scale intervention trials with HBV vaccine, concurrent efforts should be devoted to better defining the possibly associated role of AF as a human hepatocarcinogen by monitoring human AF expo sure. The recent development of immunological techniques (24, 33, 40) that use antibodies with a high degree of sensitivity and specificity against certain carcinogens, including AFBi (see Table 1), opens the possibility of determining individual exposure in a relatively large human population. Particular attention at the Workshop was given to the development and use in field studies of immunoassays for the detection of AFBi and its metabolites in body fluids. Methodological Aspects of AF Analysis Common methods of AF analysis include either thin-layer chromatography or HPLC of extracted samples with confirmation of identity by physicochemical methods such as fluorescence photon counting or mass spectrometry with selective ion moni toring. The methodology for measuring AF levels in food by thin- layer chromatography or HPLC is well established, and there have been many reports on the use of these 2 methods in collaborative studies. However, the methods can be time con suming and costly, require technical skill, and have not been widely applied to measurements of metabolites in human body fluids. Table 2 lists the various publications in which AF or metabolites have been measured in human body fluids by physicochemical or antibody techniques. The development of immunoassays for the detection of AFB, and its metabolites appears much more promising in this respect (7-9). The Working Group reviewed the CANCER RESEARCH VOL. 45 FEBRUARY 1985 922 on July 5, 2018. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Transcript of Monitoring of Aflatoxins in Human Body Fluids and...

[CANCER RESEARCH 45, 922-928, February 1985]
Meeting Report
Monitoring of Aflatoxins in Human Body Fluids and Application to FieldStudies1
The objective of this workshop was 2-fold: (a) to reviewcritically the current methodologies for detecting AFB!2 and its
metabolic by-products in biological materials in order to assess
human exposure to this carcinogen; and (o) to identify fieldstudies planned or in progress which might be suitable for theexamination of the interaction between persistent HBV infection,AF exposures, and/or other factors in the etiopathogenesis ofPHC. Epidemiological studies (3,32,35) have strongly implicatedHBV infection as a major risk factor in the induction of PHC.However, a number of other studies also indicate a multifactorialorigin for this type of cancer. Recent studies (16, 26, 47) haveshown that the differences in hepatitis B surface antigen carrierrates in urban and rural populations could not account for thedifference in incidence of PHC in these 2 groups. At present,there is no clear evidence that HBV as such has neoplastictransforming activity in cultured cells or in experimental animals,although viruses similar to HBV have been found to cause PHCunder natural conditions in woodchucks. Integration of HBV DMAin both normal and neoplastic liver cells has been demonstrated(32, 43). Additional risk factors, including mycotoxins (16, 22,23, 30) and alcohol consumption (4), must, however, continue tobe considered of etiological importance.
The considerable evidence implicating AF as a carcinogen inanimals and the correlation studies demonstrating geographicconcordance between populations with high AF exposure ratesand a high incidence of PHC suggest that AF may be an importanthuman carcinogen (23, 50). However, only longitudinal studiesof individuals at high risk of PHC will conclusively establish AFas a human carcinogen. To date, the lack of tests suitable formeasuring short- and long-term individual exposure to AF has
impeded these longitudinal studies.Although there is limited systematic survey in some countries,
AF has been demonstrated in many commonly consumed food-
1This meeting was organized by the International Agency for Research on
Cancer (IARC, Lyon, France) and was held in Lyon, on April 26 to 27,1984.The participants were H. Autrup, Miljo og Kraett Laboratories Copenhagen,
Denmark; H. Bartsch, IARC; F. X. Bosch, IARC; F. S. Chu, Department of FoodMicrobiology and Toxicology, Food Research Institute, University of Wisconsin,Madison, Wl; N. Day, IARC; M. Friesen, IARC; C. Gamer (Recorder), CancerResearch Unit, Heslington, York, United Kingdom; C. Harris, NIH, Laboratory ofHuman Carcinogenesis, Bethesda, MD; R. Montesano (Secretary), IARC; N. Muñoz,IARC; G. E. Neal, Toxicology Unit, Medical Research Council, Carshalton,Surrey, United Kingdom; K. Randerath, Department of Pharmacology, BaylorCollege of Medicine, Texas Medical Center, Houston, TX; R. Ryder (Recorder),Tufts University School of Medicine, New England Medical Center Hospital, Boston,MA; P. Sizaret, Biologicals Unit, World Health Organization, Geneva, Switzerland;L. Tomatis (Director), IARC; T. Sun, Department of Immunology, Cancer Institute,Chinese Academy of Medical Sciences, Beijing, People's Republic of China; D.
Umbenhauer, IARC; H. P. van Egmond, National Institute of Public Health, Bil-thoven, Netherlands; G. N. Wogan (Chairman), Department of Nutrition and FoodScience, Massachusetts Institute of Technology, Cambridge, MA.
This document has been published as an IARC Internal Technical Report 1984/03.
2The abbreviations used are: AFBi, aflatoxin B,; AF, aflatoxin; ELISA, enzyme-
linked immunoabsorbent assay; HBV, hepatitis B virus; HPLC, high-pressure liquidchromatography; PHC, primary hepatocellular carcinoma; RIA, radioimmunoassay;HB, hepatitis B.
Received October 1, 1984; accepted November 13,1984.
stuffs. The occurrence of AF in foods is not only due to poorstorage but also attributed to its presence in raw materials inwhich the toxins are produced in the fields due to fungal infestation (1, 5, 36, 55). However, epidemiological studies seekingto establish AF as a human hepatocarcinogen have not beenable to establish whether the important risk factor for PHC is thedegree of individual exposure to AF over a prolonged period oftime or if it is the presence of a unique metabolic pathway.Particularly carcinogenic AF metabolites may be produced incertain high-risk individuals; alternatively, AF exposure may be
particularly important in patients with persistent HBV infection.The clarification of these various possibilities may result in moreeffective measures of primary prevention of PHC.
Various vaccination projects against HBV are planned or areunder way in regions of the world where HB infection is endemicand where the long-term outcome may be expected to reduce
the incidence of PHC. Given the relatively extensive knowledgeof the activity of AF in human cell systems, its routes of metabolism, the availability of markers for metabolic by-products andcellular damage, and the evidence that not all cases of PHC canbe attributed solely to HBV, it would seem that, in large-scaleintervention trials with HBV vaccine, concurrent efforts shouldbe devoted to better defining the possibly associated role of AFas a human hepatocarcinogen by monitoring human AF exposure.
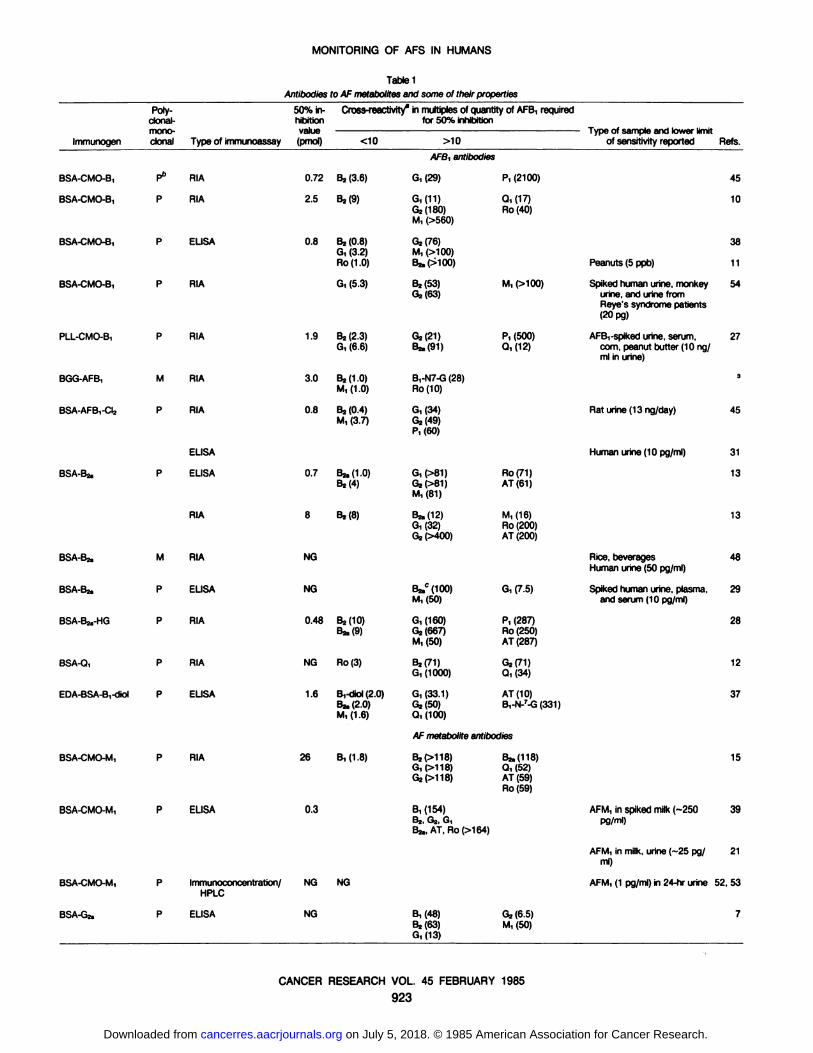
The recent development of immunological techniques (24, 33,40) that use antibodies with a high degree of sensitivity andspecificity against certain carcinogens, including AFBi (see Table1), opens the possibility of determining individual exposure in arelatively large human population. Particular attention at theWorkshop was given to the development and use in field studiesof immunoassays for the detection of AFBi and its metabolitesin body fluids.
Methodological Aspects of AF Analysis
Common methods of AF analysis include either thin-layerchromatography or HPLC of extracted samples with confirmationof identity by physicochemical methods such as fluorescencephoton counting or mass spectrometry with selective ion monitoring. The methodology for measuring AF levels in food by thin-layer chromatography or HPLC is well established, and therehave been many reports on the use of these 2 methods incollaborative studies. However, the methods can be time consuming and costly, require technical skill, and have not beenwidely applied to measurements of metabolites in human bodyfluids.
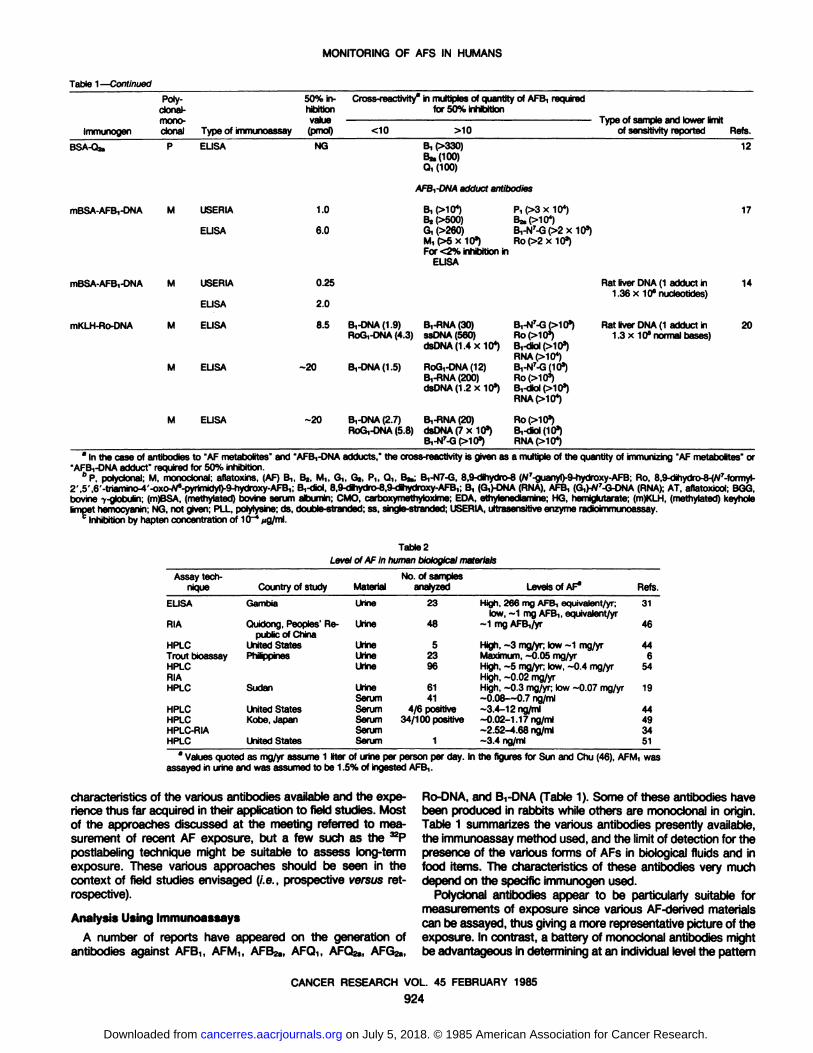
Table 2 lists the various publications in which AF or metaboliteshave been measured in human body fluids by physicochemicalor antibody techniques. The development of immunoassays forthe detection of AFB, and its metabolites appears much morepromising in this respect (7-9). The Working Group reviewed the
CANCER RESEARCH VOL. 45 FEBRUARY 1985
922
on July 5, 2018. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
MONITORING OF AFS IN HUMANS
Table 1Antibodies to AF metabolitesand some ot their properties
ImmunogenBSA-CMO-B,BSA-CMO-B,BSA-CMO-B,BSA-CMO-B,PLL-CMO-B,BGG-AFB,BSA-AFB,-CI2BSA-Bu.BSA-B2.BSA-BZ.BSA-BJ.-HGBSA-Q,EDA-BSA-B,-diolPoly-
50% ¡n-clonal- hibitionmono- valueclonal Type of immunoassay(pmol)P6
RIA0.72P
RIA2.5P
ELISA0.8P
RIAP
RIA1.9M
RIA3.0P
RIA0.8ELISAP
ELISA0.7RIA
8M
RIANGP
ELISANGP
RIA0.48P
RIANGP
ELISA 1.6Cross-reactivity3
in multiples of quantity of AFB, required
for 50%inhibition<1082(3.6)B,(9)B2
(0.8)G, (3.2)Ro (1.0)G,
(5.3)B2
(2.3)G,(6.6)82(1.0)
M,(1.0)B2
(0.4)M,(3.7)Bz.(1.0)
B2<4)82(8)B2(10)
B2.(9)Ro(3)B,-diol
(2.0)B* (2.0)M, (1.6)>10AFB,
antibodiesG,(29)8,
(11)G2(180)
M,(>560)G2(76)
M, (>100)BafXlOO)82
(53)02(63)G2(21)
Bj.P1)B,-N7-G
(28)Ro(10)G,(34)
G2<49)P,(60)G,
(>81)G2(>81)M,(81)82.
(12)G, (32)G2(>400)82.°
(100)
M,(50)G,
(160)G2 (667)M,(50)82(71)
G,(1000)G,
(33.1)G2(50)Q, (100)P,
(2100)Q,(17)
Ro(40)M,
(>100)P,
(500)0,(12)Ro(71)
AT(61)M,
(16)Ro (200)AT(200)G,
(7.5)Pi
(287)Ro (250)AT(287)G2<71)
0,(34)AT
(10)B,-N-7-G(331)-
Type of sample and lower limit
of sensitivityreportedPeanuts
(5ppb)Spiked
human urine, monkeyurine, and urine fromReye's syndrome patients
(20pg)AFB,
-spiked urine, serum,com, peanut butter (10 ng/ml inurine)Rat
urine (13ng/day)Human
urine(10pg/ml)Rice,
beveragesHumanurine (50pg/ml)Spiked
human urine, plasma,and serum (10 pg/ml)Refs.451038
1154273453113134829281237AF
metaboliteantibodiesBSA-CMO-M,BSA-CMO-M,BSA-CMO-M,BSA-Gj.P
RIA26P
ELISA0.3P
Immunoconcentratton/ NGHPLCP
ELISA NGB,(1.8)NGB2(>118)
G, (>118)G2(>118)B,
(154)B2, G2, G,Bj., AT,Ro(>164)B,
(48)82(68)G, (13)82,
(118)Q, (52)AT (59)Ro(59)62(6.6)
M, (50)AFM,
in spiked milk (-250pg/ml)AFM,
in milk, urine (-25 pg/ml)AFM,
(1 pg/ml) in 24-hr urine15392152,537
CANCER RESEARCH VOL. 45 FEBRUARY 1985
923
on July 5, 2018. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
MONITORING OF AFS IN HUMANS
Table 1—Continued
ImmunogenBSA-O.2.Poly-
clonal-mono-clonal Type ofimmunoassayP
ELISA50%
in- Cross-reactivity* in multiples of quantity of AFB, required
hibition for 50%inhibition(pmol)
<NG10 >10B,
(>330)
Q, (100)of
sensitivity reported Refs.12
AFBi-DNA adduci antibodies
mBSA-AFB,-DNA M USERIA
ELISA
mBSA-AFB,-DNA
mKLH-Ro-DNA
M
M
M
USERIA
ELISA
ELISA
ELISA
ELISA
1.0
6.0
0.25
2.0
8.5
B, (ì.104)Bj (>500)G, (>260)M, (>5x 103)For <2% inhibition in
ELISA
P,(>3x 104)
B,-N7-G(>2x 103)Ro(>2x 103)
B,-DNA(1.9) B,-RNA(30)RoG,-DNA (4.3) ssDNA (560)
dsDNAO^xlO4)Ro(>10a)
Rat liver DNA (1 adduct in1.36 x 10* nucleotides)
Rat liver DNA (1 adduct in1.3x 10* normal bases)
17
14
20
-20 B,-DNA(1.5) RoG,-DNA(12)B,-RNA(200)dsDNA(1.2x 103)
RNA(>10*)B,-N7-G(10")
RNAIXIO4)
-20 B,-DNA(2.7) B,-RNA(20)RoG,-DNA (5.8) dsDNA (7 x 103) B,-<Jiol(103)
B,-N7-G(>103) RNA (>104)
* In the case of antibodies to "AF metabolites" and "AFB,-DNA adducts," the cross-reactivity is given as a multiple of the quantity of immunizing "AF metabolites" or"AFB,-DNA adduct" required for 50% inhibition.
°P,polyclonal; M, monoclonal; aflatoxins, (AF) Bi, 82, M,, Gì,Gz, Pi, Qi, B»;B,-N7-G, 8,9-dihydro-8 (W7-guanyl)-9-hydroxy-AFB;Ro, 8.9-dihydro-8-(W7-formyl-2',5',6'-triamino-4'-oxo-Ws-pyrimidyl)-9-hydroxy-AFB1; B,-diol, 8,9-dihydro-8,9-dihydroxy-AFB,; B, (G,)-DNA (RNA),AFB, (G,)-N7-G-DNA(RNA);AT, aflatoxicol; BGG,bovine -y-globulin;(m)BSA, (methylated) bovine serum albumin; CMO, carboxymethytoxime; EDA, ethytenediamine;HG, hemiglutarate; (m)KLH, (methylated) keyholelimpet hemocyanin;NG, not given; PLL, polylysme;ds, double-stranded;ss, single-stranded;USERIA,ultrasensitiveenzyme radioimmunoassay.
0 Inhibition by hapten concentration of 10~*»ig/ml.
Table 2Level ot AF in humanbiologicalmaterialsAssay
techniqueELISARIAHPLCTrout
bioassayHPLCRIAHPLCHPLCHPLCHPLC-RIAHPLCCountry
ofstudyGambiaQuidong,
Peoples' Re
public ofChinaUnitedStatesPhilippinesSudanUnited
StatesKobe,JapanUnited
StatesMaterialUrineUrineUrineUrineUrineUrineSerumSerumSerumSerumSerumNo.
ofsamplesanalyzed23485239861414/6
positive34/100 positive1Levels
ofAF"High,
266 mg AFB,equivalent/yr;low,-1 mg AFBi,equivalent/yr-1
mgAFB,/yrHigh,
-3 mg/yr; tow -1mg/yrMaximum,-0.05mg/yrHigh,
-5 mg/yr; tow, -0.4mg/yrHigh,-0.02mg/yrHigh,-0.3 mg/yr; low -0.07mg/yr-0.08—0.7ng/ml~3.4-12ng/ml-0.02-1.
17ng/ml-2.52-4.68ng/ml-3.4
ng/mlRefs.3146446541944493451
8 Values quoted as mg/yr assume 1 liter of urine per person per day. In the figures for Sun and Chu (46), AFM, was
assayed in urine and was assumed to be 1.5% of ingested AFB,.
characteristics of the various antibodies available and the experience thus far acquired in their application to field studies. Mostof the approaches discussed at the meeting referred to measurement of recent AF exposure, but a few such as the ^Ppostlabeling technique might be suitable to assess long-term
exposure. These various approaches should be seen in thecontext of field studies envisaged (i.e., prospective versus retrospective).
Analysis Using Immunoassays
A number of reports have appeared on the generation ofantibodies against AFBt, AFMi, AFB2a, AFQ,, AFQ2a, AFG2a,
Ro-DNA, and Bi-DNA (Table 1). Some of these antibodies havebeen produced in rabbits while others are monoclonal in origin.Table 1 summarizes the various antibodies presently available,the immunoassay method used, and the limit of detection for thepresence of the various forms of AFs in biological fluids and infood items. The characteristics of these antibodies very muchdepend on the specific immunogen used.
Polyclonal antibodies appear to be particularly suitable formeasurements of exposure since various AF-derived materials
can be assayed, thus giving a more representative picture of theexposure. In contrast, a battery of monoclonal antibodies mightbe advantageous in determining at an individual level the pattern
CANCER RESEARCH VOL. 45 FEBRUARY 1985
924
on July 5, 2018. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

MONITORING OF AFS IN HUMANS
of AF metabolites present in the urine.The 2 procedures of ELISA and RIA have both been used to
assay AFs. RIA requires radiolabeled substrates, access toscintillation counters, and skilled personnel. On the other hand,ELISA requires no radioactivity, expensive analytical equipment,or highly trained technical personnel, and ELISA procedures areat least as sensitive as if not more sensitive than RIA. It shouldbe possible to construct simple ELISA kits to estimate AFs infield laboratories in Third World countries. It was generally agreedthat ELISA methods should be concentrated on for routinemonitoring work. Furthermore, immunoassay procedures werethought to be equal to Chromatographie techniques in sensitivity(limits of sensitivity: 0.005 to 0.1 ¿tg/üterfor HPLC; 0.01 to 0.25itg/liter for immunoassay) while being simpler to perform. Goodcorrelations have been shown between AF estimated by ELISAand AF estimated by HPLC (9).
Collection and Storage of Sample
It was generally agreed that if a cause-effect relationship
between AF exposure and PHC incidence were to be established, it was essential that AF exposure be monitored at anindividual level with a time component. The Working Groupgenerally agreed that for field studies urine is the easiest materialto collect. Some research groups who had carried out preliminaryfield studies had collected urine at a single voiding (time of daynot stated) while others had collected urine over a 24-hr period.
No data were available to indicate which was the preferredmethod. The group that had measured total AF content in urinevoided at a single time had not corrected for individual differencesin volume voided by estimating creatinine concentration. Thisshould be done for any single time point measurements in orderto compare AF concentration differences.
The metabolism of AF in animals has been explored, and avariety of metabolites have been identified; these have tendedto be those readily obtained by chloroform extraction. In humanurine, AFM! and AFPt have been identified (5), but water-solublemetabolites which would include AFBi-diol, AFB^mercapturic
acid, and AFB^cysteine have not been positively identified inhuman urine but are likely to be present. It was generally agreedthat urine samples should be stored cold if possible after voidingand protected from light. Failing this, it was thought that additionof sodium azide and buffering to neutrality would be adequatefor transportation of samples. A Sep-Pak C18 reversed-phase
cartridge had been used by one group to concentrate AF metabolites from urine and to transport specimens (21). This procedurewould be useful only in those circumstances in which the metab-
olite(s) of interest would be retained on the cartridge, i.e., nothighly polar metabolites.
A novel procedure was presented at the meeting in whichurine was concentrated by immunoabsorption. An immunoab-
sorbant column was prepared by binding polyclonal or monoclonal antibody against AFs to Sepharose. Urine suspected ofbeing contaminated by AF was passed through the column, andany bound material was removed by eluting with methanol. Itwas possible using this technique to concentrate as much as1500 ml urine and to remove quite specifically AF or relatedmaterials (48, 52, 53).3 Other concentration procedures that can
3J. D. Groopman, L. J. Trudel, P. R. Donahue, A. Marshak-Rothstein, and G.
N. Wogan. High affinity monoclonal antibodies for aflatoxins and their applicationto solid phase immunoassays, submitted for publication.
be used include freeze-drying, solvent extraction, or use of Sep-
Pak CÃacartridges as described above.The Working Group was aware that these methodologies
permit the determination only of relatively recent exposure. Thismethodological limitation stresses the necessity to develop methods that may permit estimates of long-term exposure.
Other AF Monitoring Methods
The use of the 32Ppostlabeling technique (41) was described
at the meeting. The method is nonspecific but can detect levelsof carcinogen reaction with DMA down to 1 base/107 to 10s
nucleotides. While the procedure appears to be promising for anumber of compounds including polycyclic aromatic hydrocarbons, present results suggest that AFBi-DNA is not a good
substrate for this procedure. Were this problem to be overcome,then this method might be used to examine DNA isolated fromblood cells or from liver biopsy samples. Another approachmentioned might be the determination of hemoglobin adduci,which could be potentially of interest due to the relatively longhalf-life of this protein.
Relevant Field Studies of Human Risk Associated with Exposure to AF
Although not specifically reviewed at the Workshop, the limitation of published reports demonstrating a concordance between geographical regions with high AF exposure levels andregions with high rates of PHC was recognized. The inability ofthese population-based studies to clearly incriminate AF as a
human carcinogen emphasizes the importance of focusing futurework on individuals exposed to AF who are at known high riskof developing PHC.
During the workshop, preliminary studies from Kenya (2) thatused a fluorescence assay for the detection of AFB^uanine inthe urine of subjects living in a region with high exposure ratesto AF and with elevated incidence of PHC were reported. Inseveral persons, AFB^guanine was found in urine collected upto 72 hr after the ingestion of AF-contaminated foods. The
adaptability of this method for use in the field warrants furtherinvestigation.
Collaborative studies (31) between investigators at the YorkCancer Research Unit, International Agency for Research onCancer, and the MRC Laboratories in The Gambia were reportedin which a polyclonal rabbit antibody preparation against AFB,(which had been adapted for use in an ELISA system) demonstrated detectable AF levels in urine samples collected fromindividuals with PHC, their immediate family contacts, and controls. In a limited number of analyzed urine samples, there wereno significant differences between AF levels in PHC cases andtheir family contacts when compared with those in controls.Using the 24-hr dietary recall method, these studies were ex
tended to investigate a possible correlation between the foodsthat patients and matched controls had eaten in the previous 24hr and the AFB! level found in a urine sample obtained thefollowing day. Because of the limited availability of food in TheGambia at the time this study was carried out, these investigatorsfound that cases and controls were very likely to be consumingsimilar foods in nearly the same amounts throughout the year.Urinary AF levels did not correlate with the quantity of particular
CANCER RESEARCH VOL. 45 FEBRUARY 1985
925
on July 5, 2018. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
MONITORING OF AFS IN HUMANS
foods eaten.A recent report (18) of an excess of cancer deaths among
workers at a Dutch oil-pressing facility in which exposure to AF
primarily occurred via the respiratory route highlights the use ofoccupational mortality studies as a potential way of collectingdata which may help bridge the gap between the known rolewhich AF plays as a carcinogen in animals and its potential rolein humans.
A recent case-control investigation from the Philippines (4) has
emphasized the potential role of alcohol in an interactive rolewith persistent HBV infection and/or exposure to AF in promotingPHC. A study of cases of PHC coming from rural and urbanareas in South Africa (26) demonstrated an increased incidenceof PHC in rural areas and a lower mean age of onset in ruralPHC cases. These differences are not explained by differentialrates of exposure to a persistent infection with hepatitis B virus.Thus, differential rates of exposure to AF may possibly accountfor these marked differences.
In China, recent studies (46) have demonstrated marked geographical differences in the incidence of PHC. The areas with thehighest incidence of PHC are largely rural. Serological surveysconducted in high- and low-PHC incidence areas have failed to
demonstrate proportional differences in the prevalence of HBVcarrier rates between these regions. However, marked differences in the level of dietary exposure to AF have been noted,with rural areas having higher rates of exposure to AF. Usingpolyclonal antibodies against AFMi and other AF derivatives forimmunoconcentration, it was found that 100 ng AFIvl! could bepresent in 24-hr urine in high-risk areas, while levels mostlybelow 2 ng were present in low-risk areas. Chinese investigators
have interpreted these findings to suggest that the regionaldifferences in PHC incidence may be partly accounted for byregional differences in exposure to AF on the background ofHBV infection. An intervention study to reduce AF exposure iscurrently under way in Quidong County of China, an area with ahigh incidence of PHC. The incidence rates of PHC over time willbe observed to determine if dietary intervention might be instrumental in decreasing the incidence of PHC among people at veryhigh risk. An interesting and possibly relevant study completedin China involved the feeding of AF-contaminated food to domestic ducks known to be frequently infected with "duck hepatitis virus" and at high risk of developing PHC. The ducks
receiving the special, AF-free food did not develop PHC, unlike
their domestically fed counterparts (46).
Potential Future Studies
One of the first studies which ought to be carried out wouldbe to provide interested laboratories with aliquots of urine containing known amounts of AFB, and AFB,-guanine. These labo
ratories would assay the aliquots following a standard protocoland make interlaboratory comparisons. The reasons for theapparently 1000-fold differences in AF exposure which were
reported to occur between China and Africa (AF exposure levelsbeing much greater in Africa) must be pursued. While the mostobvious explanation for this difference is methodological it needsto be satisfactorily addressed and some of the methodologicalproblems which have impeded research in this area should beemphasized.
A second helpful preliminary study would be careful measure
ment of intake levels of AF in subjects known to consume AF-contaminated food frequently. Urinary output of AFMi and AFB!-guanine and total AF activity could then be measured in urinescollected over the following days. The adequacy of a morningpostconsumption urine sample versus spot urine collections overthe ensuing 48 hr, versus 24-hr urine collections could then be
assessed. These data would be helpful in deciding what sampleof urine collection and what pattern of urinary AF metaboliteswould be most likely to provide meaningful data on previousdietary AF exposure.
In addition to the importance of the variation in dietary AFexposure as a PHC risk factor, the importance of varying metabolic breakdown pathways, given a standard AF exposure, wasemphasized by several participants. The use of "predictor drugs"
which might indicate individual differences in metabolic capacitywas mentioned. As yet, little information using this approach isavailable (42).
Potential field studies in Swaziland and the Philippines werealso discussed. In Swaziland, marked regional variations in exposure to AF have been observed. Since some preliminary fieldwork has been carried out in that country concerning exposureto AF and HBV in relation to PHC, a field study to measureindividual dietary exposure to AF and subsequent urinary outputof various AF metabolites could be undertaken in that country.
In the Philippines, PHC mortality rates also show markedgeographical variation in the country. One potential study wouldinvolve cohorts of men from the high- and low-PHC-incidenceregions. The prevalence of various HBV markers and AF metabolites in these groups could be compared. A second projectwould be a case-control study of chronic liver disease (chronicactive hepatitis, cirrhosis, and PHC) in the high-PHC-incidence
region to explore the role of several risk factors such as HBV,AF, alcohol, and smoking. Individual exposure to AF and alcoholcould be determined in this case-control investigation.
In Singapore, AF monitoring could be carried out in a group ofhepatitis B surface antigen carriers (symptomatic and asymptomatic) and a group of noncarriers. The risk of developing PHCwould be determined by linking the cohorts to the cancer registry.
A group of Chinese investigators has shown that a subpopulation of hepatitis carriers has both raised transaminases andfluctuating serum a-fetoprotein patterns, a fact that reflects
persistent liver cell damage and hyperplasia. These subjects areat increased risk of developing PHC (47). This observation needsto be confirmed in further studies.
Two potential studies in The Gambia were mentioned. Thefirst would be a longitudinal cohort study of adult men withpersistent HBV infection. Their levels of exposure to AF basedon dietary monitoring and periodic measurement of AF metabolites in carefully collected urine samples would be measured. Thesecond study would be a proportionate cancer mortality studyof workers at the groundnut mill in the country. These workersare known to inhale dust which intermittently contains high levelsof AF.
In general, the meeting believed that retrospective assessmentof AF intake by questionnaire or other available techniques, asrequired in a case-control study, was unlikely to be informative.
Future work should concentrate on individual assessment of AFexposure, in order to link in a prospective manner AF intake andmetabolism to liver cancer risk. Such studies should includeevaluation of the individual HBV status in order to give informa-
CANCER RESEARCH VOL. 45 FEBRUARY 1985
926
on July 5, 2018. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
MONITORING OF AFS IN HUMANS
tion on HBV-AF interaction. Concentration on high-risk groups,
such as those with chronic active hepatitis, would reduce thesize of the study population which would be required.
Conclusions
The several currently available methodologies to detect andquantify short-term exposure to AF and measure the degree of
resultant cellular damage suggest that future effects should bedirected at standardizing these analytical methods. This standardization would be particularly helpful in large-scale studies aiming
at relating individual exposure to AF to the subsequent risk ofPHC. Efforts to identify biochemical markers which accuratelyindicate dietary exposure to AF over a prolonged period alsoneed to be pursued. Finally, the currently planned PHC prevention trials in which wide-scale controlled distribution of HBVvaccine will be carried out would be strengthened if AF-monitor-
ing studies are included concurrently to determine possiblechanges in AF exposure that may influence the overall incidenceof PHC in the target population of these expensive trials. Severemethodological limitations may have restricted efforts to incriminate AF conclusively as the human carcinogen with the broadestpublic health implications for global primary cancer prevention.Nevertheless, the Working Group, in ending the meeting, acknowledged that the data which currently exist on AF provide astrong basis for continued targeted research on AF.
Acknowledgments
The help of C. Wild in the preparation of this report is greatly appreciated.
Colin GarnerCancer Research UnitHeslington, York, United Kingdom
Robin RyderTufts University School of MedicineNew England Medical Center HospitalBoston, Massachusetts 02111
Ruggero Montesano*
International Agency for Research on Cancer150 Cours Albert Thomas69372 Lyon Cedex, France
References
1. Anderson, H. W., Nehring, E. W., and Wichser, W. R. Aflatoxin contaminationof corn in the field. J. Agrie. Food Chem., 23: 775-782, 1975.
2. Autrup, H., Bradley, K. A., Shamsuddin, A. K. M., Wakhisi, J., and Wasunna,A. Detection of putative adduci with fluorescence characteristics identical to2,3-dihydro-2-<7'-guanyl)-3-hydroxyaflatoxin B, in human urine collected inMurang'a district, Kenya. Carcinogenesis (Lond.), 4: 1193-1195,1983.
3. Beasley, R. P. Hepatitis B virus as the etologie agent in hepatocellularcarcinoma. Epidemiological considerations. Hepatology, 2: 21S-26S, 1982.
4. Bulatao-Jayme, J., Aimera, E. M., Castro, C. A., Jardeleza, T. H., and Salamat,L. A. A case-control dietary study of primary liver cancer risk from aflatoxinexposure. Int. J. Epidemici., 11:112-119, 1982.
5. Campbell, T. C., Caedo, J. P., Bulato-Jayme, J., Salamat, L, and Engel, R. W.Aflatoxin M, in human urine. Nature (Lond.), 227: 403-404, 1970.
6. Campbell, C. T., Sinnhuber, R. 0., Lee, D. J., Wales, J. H., and Salamat, L.Hepatocarcinogenic material in urine specimens from humans consumingaflatoxin. J. Nati. Cancer Inst., 52: 1647-1649, 1974.
4To whom requests for reprints should be addressed.
7. Chu, F. S. Immunochemical methods for mycotoxin analysis. In: Naguib ef al.(eds.), Proceedings of the International Symposium on Mycotoxins, Cairo,Egypt, pp. 177-194.
8. Chu, F. S. Immunoassays for analysis of mycotoxins. J. Food Prot 47 562-569,1984.
9. Chu, F. S. Immunochemical studies on mycotoxins. In: H. Kurata and Y. Ueno(eds.), Toxigenic Fungi—Their Toxins and Health Hazard, p. 234. Amsterdam:Elsevier/North-Holland BiomédicalPress, Inc., 1984.
10. Chu, F. S., and Ueno, I. Production of antibody against aflatoxin B,. Appi.Environ. Microbiol., 33: 1125-1128,1977.
11. EI-Nakib, 0., Pestka, J. J., and Chu, F. S. Analysis of aflatoxin B, in corn,wheat, and peanut butter by an enzyme-linked immunosorbent assay and asolid-phase radioimmunoassay. J. Assoc. Off. Anal. Chem., 64: 1077-1082,1981.
12. Fan, T. S., Zhang, G. S., and Chu, F. S. Production and characterization ofantibody against aflatoxin Q,. Appi. Environ. Microbiol., 47: 526-532, 1984.
13. Gaur, P. K., Lau, P., Pestka, J. J., and Chu, F. S. Production and characterization of aflatoxin Bz. antiserum. Appi. Environ. Microbiol., 41: 478-482,1981.
14. Groopman, J. D., Haugen, A., Goodrich, G. R., Wogan, G. N., and Harris, C.C. Quantitäten of aflatoxin B! modified DMA using monoclonal antibodies.Cancer Res., 42: 3120-3124,1982.
15. Harder, W. 0., and Chu, F. S. Production and characterization of antibodyagainst aflatoxin fvV Experientia (Basel), 35: 1104-1107, 1979.
16. Hams, C. C., and Sun, T. Multifactoral etiology of human liver cancer. Carcinogenesis (Lond.), 5: 697-701, 1984.
17. Haugen, A., Groopman, J. D., Hsu, I.-C., Goodrich, G. R., Wogan, G. N., andHarris, C. C. Monoclonal antibody to aflatoxin B,-modified DNA detected byenzyme immunoassay. Proc. Nati. Acad. Sci. USA, 78: 4124-4127, 1981.
18. Hayes, R. B., van Nieuwenhuize, J. P., Raatgever, J. W., et al. Aflatoxinexposures in the industrial setting: an epidemiological study of mortality. FordChem. Toxic., 22: 39-43,1984.
19. Hendricks, R. G., Coulter, J. B. S., Lamplugh, S. M., Macfartane, S. B. J.,Williams, T. E., Omer, M. I. A., and Suliman, G. I. Aflatoxins and kwashiorkor:a study in Sudanese children. Br. Med. J., 285: 843-846,1982.
20. Hertzog, P. J., Lindsay Smith, J. R., and Gamer, R. C. Production of monoclonalantibodies to guanine iminazole ring-opened aflatoxin B, DNA, the persistentDNA adduct/r? vivo. Carcinogenesis (Lond.), 3: 825-828, 1982.
21. Hu, H. J., Hoychich, N., and Chu, F. S. ELISA of picogram quantities ofaflatoxin M, in urine and milk. J. Food Prat., 47:126-127, 1983.
22. IARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals toHumans, Vol. 10. Lyon: International Agency for Research on Cancer, 1976.
23. IARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals toHumans, Supplement No. 4. IARC Monographs, Vols. 1 to 29. Lyon: International Agency for Research on Cancer, 1982.
24. IARC/IPCS. Development and Possible Use of Immunological Techniques toDetect Individual Exposure to Carcinogens, Joint IARC/IPCS Working GroupReport, IARC Internal Technical Report No. 82/001, 1982.
25. Kam, W., Rail, L. B., Smuckler, E. A., Schmid, R., and Rutter, W. J. HepatitisB viral DNA in liver and serum of asymptomatic carriers. Proc. Nati. Acad. Sci.USA, 79: 7522-7526, 1982.
26. Kew, M. C., Rossouw, E., Hodkinson, J., Paterson, A., Dusheiko, G. M., andWhitcutt, J. M. Hepatitis B virus status of Southern African blacks withhepatocellular carcinoma: comparison between rural and urban patients.Hepatology, 3: 65-68, 1983.
27. Langone, J. J., and van Vunakis, H. Aflatoxin B,: specific antibodies and theiruse in radioimmunoassay. J. Nati. Cancer Inst., 56: 591-595, 1976.
28. Lau, H. P., Gaur, P. K., and Chu, F. S. Preparation and characterization ofaflatoxin B^-hemiglutarate and its use for the production of antibody againstaflatoxin B1. J. Food Safety, 3: 1-13, 1981.
29. Lawellin, D. W., Grant, D. W., and Yoyce, B. K. Enzyme-linkedimmunoasorbentanalysis of aflatoxin B,. Appi. Environ. Microbiol., 34: 94-96. 1977.
30. Linsell, C. A. Environmental chemical carcinogens and liver cancer. J. Toxicol.Environ. Health, 5: 183-191, 1979.
31. Martin, C. N., Gamer, R. C., Tursi, F., Gamer, J. V., Whittle, H. C., Ryder, R.W., Sizaret, P., and Montesano, R. An ELISA procedure for assaying aflatoxinB,. In: A. Berlin, M. Draper, K. Hemminki, and H. Vainio (eds.), MonitoringHuman Exposure to Carcinogenic and Mutagenic Agents. IARC ScientificPublications No. 59. Lyon: International Agency for Research on Cancer, inpress, 1985.
32. Mason, W. S., Halpern, M. S., and Thomas, W. Hepatitis B viruses, liverdisease and hepatocellular carcinoma. Cancer Surv., 3: 1, 1984.
33. Müller,R., Adamkiewicz, J., and Rajewsky, M. F. Immunological detectionsand quantification of carcinogen-modified DNA components. In: H. Bartsch
and B. Armstrong (eds.). Host Factors in Human Carcinogenesis, IARC Scientific Publication No. 39. pp. 463-479. Lyon: International Agency for Research on Cancer, 1982.
34. Nelson, D. B., Kimbrough, R., Landrigan, P. S., Hayes. A. W., Yang, G. C.,and Benanides, J. Aflatoxin and Reye's syndrome: a case control study.
Pediatrics, 66: 865-869,1980.
35. Okuda, K., and Mackay, I. (eds). Hepatocellular Carcinoma, A Series ofWorkshops on the Biology of Human Cancer, Report No. 17, UICC TechnicalReport Series, Vol. 74. Geneva: UnióInternational Contra Cancrum, 1982.
CANCER RESEARCH VOL. 45 FEBRUARY 1985
927
on July 5, 2018. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

MONITORING OF AFS IN HUMANS
36. Peers,F.G., and Linsell,C. A. Dietaryaflatoxins and livercancer—apopulationbased study in Kenya. Br. J. Cancer, 27: 473-483,1973.
37. Pestka, J. J., and Chu, F. S. Aflatoxin B, dihydrodiol antibody: production andspecificity. Appi. Environ. Mirobiol., 47: 472-477, 1984.
38. Pestka, J. J., Gaur, P. K., and Chu, F. S. Quantitätenof aflatoxin B, andaflatoxin B, antibody by an enzyme-linked immunosorbent microassay. Appi.Environ. Microbiol., 40: 1027-1031, 1980.
39. Pestka, J. J., Li, Y., Harder, W. O., and Chu, F. S. Comparison of radioimmu-noassay and enzyme-linked immunosorbent assay for determining aflatoxinM, in milk. J. Assoc. Off. Anal. Chem., 64: 294-301, 1981.
40. Poirier,M. C. Antibodies to carcinogen-DNAadducts. J. Nati. Cancer Inst., 67:515-519,1981.
41. Randerath,K., Reddy, M. V., and Gupta, R.^P-Labeling test for DMAdamage.Proc. Nati. Acad. Sci. USA, 78: 6126-6129, 1981.
42. Ritchie, J. D., and Idle, J. R. Population studies of polymorphism in drugoxidation and its relevance to carcinogenesis. IARC Scientific PublicationNo.39, pp. 381-394. Lyon: InternationalAgency for Researchon Cancer, 1982.
43. Shafritz, D. A., Shouval, D., Sherman, H. I., Hadziyannis,S. J., and Kew, M.C. Integrationof hepatitis B virus DMAinto the genome of liver cells in chronicliver diseaseand hepatocellularcarcinoma. N. Engl. J. Med., 305:1067-1073,1981.
44. Siraj, M. Y., Hayes, A. W., Unger, P. D., Hogan, G. R., Ryan, N. J., and Wray,B. B. Analysis of aflatoxin B, in human tissues with high-pressure liquidchromatography. Toxicol. Appi. Pharmacol.,58: 422-430, 1981.
45. Sizaret, P., Malaveille. C., Montesano, R., and Frayssinet, C. Detection ofaflatoxins and related metabolites by R.I.A. J. Nati. Cancer Inst., 69: 1375-
1380.1980.46. Sun, T., and Chu, Y. Carcinogenesisand prevention strategy of liver cancer in
areas in prevalence.J. Cell. Physiol.,Suppl. 3, 39-44, 1984.47. Sun, T., and Wang, N. Studies on human liver carcinogenesis.In: C. C. Harris
and H. N. Autrup (eds.), Human Carcinogenesis, pp. 757-780. New York:Academic Press, Inc., 1983.
48. Sun, T., Wu, Y., and Wu, S. Monoclonal antibody against aflatoxin B! and itspotential applications. Chin. J. Oncol., 5: 401-405,1983.
49. Tsuboi, S., Nakagawa, T., Tornita, M., Seo, T., Ono, H., Kawamura, K., andIwamura, N. Detection of aflatoxin B, in serum samples of male Japanesesubjects by radioimmunoassayand high performance liquid chromatography.Cancer Res., 44:1231-1234,1984.
50. Wogan, G. N. Aflatoxins and their relationship to hepatocellularcarcinoma.In:K. Okuda and R. L. Peters (eds.), HepatocellularCarcinoma,pp. 25-42. NewYork: John Wiley and Sons, Inc., 1976.
51. Wray, B. B., and Hayes, A. W. Aflatoxin B, in the serum of a patient withprimary hepatic carcinoma. Environ. Res., 22: 400-403, 1980.
52. Wu, S., Wei, Y., Ku, G., Lo, G., Wu, Y., and Sun, T. Study on urinaryexcretionof AFM, in Beijing and Qidong people. Chin. J. Oncol., 6: 163-167, 1984.
53. Wu, S., Yang, G., and Sun, T. Studies on immuno-concentrationand immune-assay of aflatoxins. Chin. J. Oncol., 5: 81-84, 1983.
54. Yang, G., Nesheim,S., Benavides,J., Veno, I., Campbell,A. D., and Pohland,A. Radioimmunoassaydetection of aflatoxin B, in monkey and human urine.In: Preusser (ed.), Medical Mycology, Zentralblatt Bukt Suppl. 8. Stuttgart:Gustaf Fischer Verlag, 1980.
55. Yea, F. S., Yan, R. C., Mor, C. C., üv,Y. K., and Yang K. C. In: Proceedingsof the 13th InternationalCancerCongress,p. 340,1982.
CANCER RESEARCH VOL. 45 FEBRUARY 1985
928
on July 5, 2018. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
1985;45:922-928. Cancer Res Colin Garner, Robin Ryder and Ruggero Montesano to Field StudiesMonitoring of Aflatoxins in Human Body Fluids and Application
Updated version
http://cancerres.aacrjournals.org/content/45/2/922.citation
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/45/2/922.citationTo request permission to re-use all or part of this article, use this link
on July 5, 2018. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from