Monday Case presentation Beyond CDC recommendations Presented by Nabil Khoury, MD.
20
Monday Case presentation Beyond CDC recommendations Presented by Nabil Khoury, MD
-
Upload
lisa-robertson -
Category
Documents
-
view
216 -
download
1
Transcript of Monday Case presentation Beyond CDC recommendations Presented by Nabil Khoury, MD.
Monday Case presentation
Beyond CDC recommendations
Presented by Nabil Khoury, MD
Disclosures
None
History
A 55 year AA male with DMI, who has just came back from Nigeria 10 days prior, presents to the ER for: Fever Headaches Myalgias Vomiting Abdominal pain
Malaria smear: positive ID fellow paged at 1:00 AM for rec
Work-up
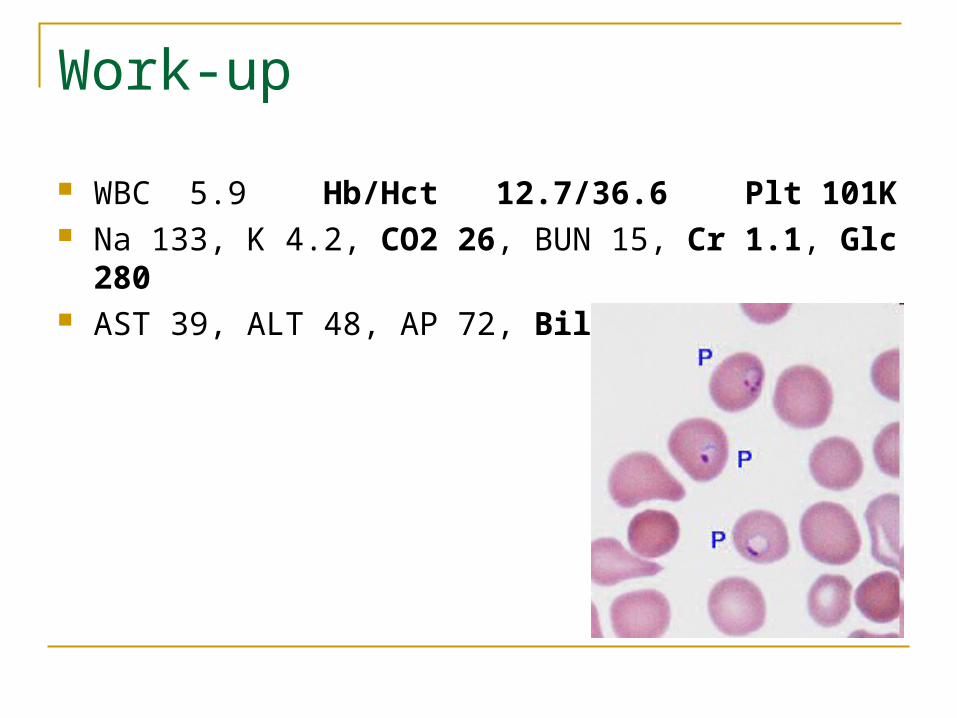
WBC 5.9 Hb/Hct 12.7/36.6 Plt 101K Na 133, K 4.2, CO2 26, BUN 15, Cr 1.1, Glc 280 AST 39, ALT 48, AP 72, Bil T 2.4 (I 1.8)
Now what?
What if you were told the smear is negative? What questions should you ask the ER
attending? What drug should you recommend?

Complicated or Uncomplicated? Remember pathophysiology! RBC lysis and adherence Review of systems: negative besides HPI, Diabetic
No confusion - No dyspnea Physical: including Vitals BP, HR, Pox, RR stable Labs and Chest X-ray:
No severe anemia No severe thrombocytopenia No acidosis No renal failure No hypoglycemia No severe hyperbilirubinemia
Did not take any prophylaxis I told Dr Bell, it seems uncomplicated case of Malaria!!
Parasetemia? Type of Malaria? Parasitemia > 5% makes the case
complicated ! When parasitemia is > 2 %: frequently it is
Plasmodium Falciparum In this case, it was a Saturday! In our case Parasitemia 3.8%, P. Falciparum Now, you got all the info, what is next?
Type of Malaria
P. Falciparum: no liver hypnozoite P. ovale and vivax: need to treat liver
hypnozoite with primaquine
Uncomplicated gets a little bit complicated Chloroquine sensitive v/s resistant areas When in doubt consider it Chloroquine
resistant CDC website: Malaria Map application
CDC guidelines Uncomplicated P. falciparumA. Atovaquone-proguanil(Malarone) x 3d
B. Artemether-lumefantrine(Coartem) x 3d
C. Quinine sulfate + doxy (or clinda) Quinine x 3 days Doxy or Clinda x 7 days
D. Mefloquine: less recommended because of severe neuropsychiatric side effects
A-B-C equally recommended
Atovaquone-proguanil (Malarone) Effectiveness: highly effective even in multi-drug
resistant areas 87-100% for P. Falciparum Side effects: overall well tolerated
Abd pain 13-31% Diarrhea 6 – 8 % Nausea 12% Vomiting 1-19% ↑ LFTs 17-27% Headache 10% Cough 10%
Contraindicated if Cr Cl < 30 To be avoided if patient was on Malarone prophylaxis
Artemether-lumefantrine (Coartem) Effectiveness >95% Rapid clearance : 1st choice WHO Side effects: well tolerated
Palpitations: 18% Potential for QT prolongation Abdominal pain 17% Diarrhea 7% Loss of appetite 40% Nausea 26% Vomiting 17% Arthralgias/Myalgias 34% / 32% Asthenia 38% Dizziness 39% Headache 56% Fever 25%
Quinine based regimens
Efficacy > 90% except SE Asia Side effects:
May trigger hypoglycemia! Cinchonism: frequent
Tinnitus: reversible Hearing loss: reversible Headache Nausea
Narrow therapeutic window that may lead to: rarely Cardiotoxicity Blindness Deafness
Complicated is easy!
IV quinidine in ICU setting that may cause Ventricular arrhythmia Hypotension Prolongation of QT c Hypoglycemia! Monitor EKG for QT, QRS
v/s IV artesunate from the CDC (IND?) Consider exchange transfusion
Next day on Sunday
His Fever was down and mildly symptomatic Cr 1.1 Same Hb dropped from 12.710.4 Plt dropped from 10164 Total Bil increased 2.45.6 ALT increased from 4865 AST increased from 3952 What happened? Hospitalist concerned about G6PD deficiency! Family asking for Coartem!

Anemia in Malaria
He kept dropping progressively his Hb until it stabilized at Hb of 9 (4%30%)
Most of the hemolysis affects non-infected RBC! Up to 90% of lyzed RBCs are not infected Multiple mechanisms of hemolysis:
Oxidative stress Bone marrow suppression Increase phagocytic activity Auto-immune anemia
Assessment of therapeutic response Parasite clearance times Fever clearance times
WHO definitions of early treatment failure: Danger signs or severe malaria days 1-3 (+ parasitemia) Parasitemia on day 2 > day 0 Parasitemia on day 3 with Temp>37.5 C(99.5F) Parasitemia on day 3 of > 25% of day 0
G6PD Deficiency
X-linked recessive disorder : Common in AA Frequency: 10-15% Type A in AA Hemolysis is triggered by the malaria
infection itself and drugs: quinine/Primaquine Hemolysis triggered by quinine is self-limited
even with continuous use of the drug
Coartem
Family asking for Coartem Accusing us of giving him an ineffective drug
to cut cost! Coartem is very cheap! Watch drug-drug interactions when switching