Molecular Pathogenesis and Targeted Therapies for...
11
Review Molecular Pathogenesis and Targeted Therapies for Intrahepatic Cholangiocarcinoma Agrin Moeini 1,2 , Daniela Sia 1,2,3 , Nabeel Bardeesy 4 , Vincenzo Mazzaferro 3 , and Josep M. Llovet 1,2,5 Abstract Intrahepatic cholangiocarcinoma (iCCA) is a molecularly heterogeneous hepatobiliary neoplasm with poor prognosis and limited therapeutic options. The incidence of this neoplasm is growing globally. One third of iCCA tumors are amenable to surgical resection, but most cases are diagnosed at advanced stages with chemotherapy as the only established standard of practice. No molecular therapies are currently available for the treatment of this neoplasm. The poor understanding of the biology of iCCA and the lack of known oncogenic addiction loops has hindered the development of effective targeted therapies. Studies with sophisticated animal models defined IDH mutation as the first gatekeeper in the carcinogenic process and led to the discovery of striking alternative cellular origins. RNA- and exome-sequencing technologies revealed the presence of recurrent novel fusion events (FGFR2 and ROS1 fusions) and somatic mutations in metabolic (IDH1/2) and chromatin- remodeling genes (ARID1A, BAP1). These latest advancements along with known mutations in KRAS/BRAF/EGFR and 11q13 high-level amplification have contributed to a better under- standing of the landscape of molecular alterations in iCCA. More than 100 clinical trials testing molecular therapies alone or in combination with chemotherapy including iCCA patients have not reported conclusive clinical benefits. Recent discover- ies have shown that up to 70% of iCCA patients harbor potential actionable alterations that are amenable to therapeu- tic targeting in early clinical trials. Thus, the first biomarker- driven trials are currently underway. Clin Cancer Res; 22(2); 291–300. Ó2015 AACR. Introduction Intrahepatic cholangiocarcinoma (iCCA) is the second most common liver cancer following hepatocellular carcinoma (HCC), accounting for 5% to 10% of all primary liver malignancies with an annual incidence of 2 cases per 100,000 in Western countries (1, 2). At present, it is widely accepted that iCCA arises from the malignant transformation of the intrahepatic cholangiocytes and is anatomically distinguished from the extrahepatic biliary tract cancers (eCCA), which are known as perihilar (pCCA) and distal (dCCA), with the second-order bile ducts acting as the separation point (3). During the past decade a growing interest has been expressed in iCCA due to a marked increase in both incidence and mortality rates (1, 4). Currently, surgical resection represents the sole curative treatment option in 30% to 40% of patients with 5-year survival of 20% to 40% (1, 5). The majority of iCCA patients have no underlying liver disease or known risk factors, which further hinders the development of screening strategies for early detec- tion. In patients with advanced disease, the combination of gemcitabine and cisplatin has been shown to confer a survival advantage over gemcitabine alone and is currently proposed as the standard of practice (6). As opposed to HCC, to date there is no approved targeted molecular therapy for iCCA, and the identifi- cation of a first-line conclusive treatment remains an unmet need. Recently, the use of next-generation sequencing technologies has enabled the identification of recurrent actionable molecular alterations that hold the promise of improving the management of advanced iCCA patients. Herein, we provide an overview of the recent discoveries of new molecular targets that should ultimately lead to the development of more personalized therapeutic approaches. Epidemiology and Risk Factors iCCA is a devastating disease with poor prognosis. Several studies have reported global trends of increasing incidence and mortality for iCCA in contrast with decreasing rates for eCCA (7– 10). iCCA presents more commonly at older age with a slight predominance in men (male to female ratio 1.2–1.5:1; ref. 1). There is a considerable geographic and demographic variation in the epidemiology of iCCA, which likely reflects distinct environ- mental and genetic predispositions. The incidence of iCCA is the highest in Southeast Asia and more specifically in Thailand (>80 1 Liver Cancer Translational Research Laboratory, Liver Unit, Institut d'Investigacions Biom ediques August Pi i Sunyer (IDIBAPS), Hospi- tal Clínic, CIBERehd, Universitat de Barcelona, Barcelona, Catalonia, Spain. 2 Liver Cancer Program, Division of Liver Diseases, Depart- ment of Medicine, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, New York. 3 Gastrointestinal Surgery and Liver Transplantation Unit, Department of Surgery, National Cancer Insti- tute IRCCS Foundation, Milan, Italy. 4 Cancer Center, Center for Regenerative Medicine, and Department of Molecular Biology, Mas- sachusetts General Hospital, Harvard University, Boston, Massachu- setts. 5 Instituci o Catalana de Recerca i Estudis Avan¸ cats, Barcelona, Catalonia, Spain. Note: V. Mazzaferro and J.M. Llovet share senior authorship. Corresponding Author: Josep M. Llovet, BCLC Group, Liver Unit, IDIBAPS, CIBERehd, Hospital Clínic, University of Barcelona, Rosell o 149, Barcelona 08036, Catalonia, Spain. Phone: 349-3227-9156; Fax: 349-3227-5792; E-mail: [email protected] doi: 10.1158/1078-0432.CCR-14-3296 Ó2015 American Association for Cancer Research. Clinical Cancer Research www.aacrjournals.org 291 on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296
Transcript of Molecular Pathogenesis and Targeted Therapies for...

Review
Molecular Pathogenesis and Targeted Therapiesfor Intrahepatic CholangiocarcinomaAgrin Moeini1,2, Daniela Sia1,2,3, Nabeel Bardeesy4, Vincenzo Mazzaferro3, andJosep M. Llovet1,2,5
Abstract
Intrahepatic cholangiocarcinoma (iCCA) is a molecularlyheterogeneous hepatobiliary neoplasm with poor prognosisand limited therapeutic options. The incidence of this neoplasmis growing globally. One third of iCCA tumors are amenable tosurgical resection, but most cases are diagnosed at advancedstages with chemotherapy as the only established standard ofpractice. No molecular therapies are currently available for thetreatment of this neoplasm. The poor understanding of thebiology of iCCA and the lack of known oncogenic addictionloops has hindered the development of effective targetedtherapies. Studies with sophisticated animal models definedIDHmutation as the first gatekeeper in the carcinogenic processand led to the discovery of striking alternative cellular origins.RNA- and exome-sequencing technologies revealed the presence
of recurrent novel fusion events (FGFR2 and ROS1 fusions)and somatic mutations in metabolic (IDH1/2) and chromatin-remodeling genes (ARID1A, BAP1). These latest advancementsalong with known mutations in KRAS/BRAF/EGFR and 11q13high-level amplification have contributed to a better under-standing of the landscape of molecular alterations in iCCA.More than 100 clinical trials testing molecular therapies aloneor in combination with chemotherapy including iCCA patientshave not reported conclusive clinical benefits. Recent discover-ies have shown that up to 70% of iCCA patients harborpotential actionable alterations that are amenable to therapeu-tic targeting in early clinical trials. Thus, the first biomarker-driven trials are currently underway. Clin Cancer Res; 22(2);291–300. �2015 AACR.
IntroductionIntrahepatic cholangiocarcinoma (iCCA) is the second most
common liver cancer following hepatocellular carcinoma (HCC),accounting for 5% to 10% of all primary liver malignancies withan annual incidence of 2 cases per 100,000 in Western countries(1, 2). At present, it is widely accepted that iCCA arises from themalignant transformation of the intrahepatic cholangiocytes andis anatomically distinguished from the extrahepatic biliary tractcancers (eCCA), which are known as perihilar (pCCA) and distal(dCCA), with the second-order bile ducts acting as the separationpoint (3).
During the past decade a growing interest has been expressed iniCCA due to a marked increase in both incidence and mortalityrates (1, 4). Currently, surgical resection represents the solecurative treatment option in 30% to 40% of patients with 5-yearsurvival of 20% to 40% (1, 5). Themajority of iCCA patients haveno underlying liver disease or known risk factors, which furtherhinders the development of screening strategies for early detec-tion. In patients with advanced disease, the combination ofgemcitabine and cisplatin has been shown to confer a survivaladvantage over gemcitabine alone and is currently proposed asthe standardof practice (6). Asopposed toHCC, todate there is noapproved targeted molecular therapy for iCCA, and the identifi-cation of a first-line conclusive treatment remains an unmet need.Recently, the use of next-generation sequencing technologies hasenabled the identification of recurrent actionable molecularalterations that hold the promise of improving the managementof advanced iCCA patients. Herein, we provide an overview of therecent discoveries of newmolecular targets that should ultimatelylead to the development of more personalized therapeuticapproaches.
Epidemiology and Risk FactorsiCCA is a devastating disease with poor prognosis. Several
studies have reported global trends of increasing incidence andmortality for iCCA in contrast with decreasing rates for eCCA (7–10). iCCA presents more commonly at older age with a slightpredominance in men (male to female ratio 1.2–1.5:1; ref. 1).There is a considerable geographic and demographic variation inthe epidemiology of iCCA, which likely reflects distinct environ-mental and genetic predispositions. The incidence of iCCA is thehighest in Southeast Asia and more specifically in Thailand (>80
1Liver Cancer Translational Research Laboratory, Liver Unit, Institutd'Investigacions Biom�ediques August Pi i Sunyer (IDIBAPS), Hospi-tal Clínic, CIBERehd, Universitat de Barcelona, Barcelona, Catalonia,Spain. 2Liver Cancer Program, Division of Liver Diseases, Depart-ment of Medicine,Tisch Cancer Institute, Icahn School of Medicine atMount Sinai, NewYork, NewYork. 3Gastrointestinal Surgeryand LiverTransplantation Unit, Department of Surgery, National Cancer Insti-tute IRCCS Foundation, Milan, Italy. 4Cancer Center, Center forRegenerative Medicine, and Department of Molecular Biology, Mas-sachusetts General Hospital, Harvard University, Boston, Massachu-setts. 5Instituci�o Catalana de Recerca i Estudis Avancats, Barcelona,Catalonia, Spain.
Note: V. Mazzaferro and J.M. Llovet share senior authorship.
Corresponding Author: Josep M. Llovet, BCLC Group, Liver Unit, IDIBAPS,CIBERehd, Hospital Clínic, University of Barcelona, Rosell�o 149, Barcelona08036, Catalonia, Spain. Phone: 349-3227-9156; Fax: 349-3227-5792; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-14-3296
�2015 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 291
on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296

cases per 100,000) and can be as low as 0.2 per 100,000 in someWestern countries (1, 11). Even though the vast majority ofiCCAs are sporadic, several risk factors have been identified.Historically, most of these risk factors have been establishedfor CCAwithout distinguishing between iCCA and eCCA, despitethe fact that increasing evidence supports the hypothesis thatthey represent distinct entities with marked differences in theirgenomic features and epidemiology (Table 1; refs. 3, 12–15). Themost prevalent risk factors for HCC have also been significantlyassociated with iCCA but not with eCCA (Table 1), includingcirrhosis and chronic hepatitis B and C infections (1, 11, 16–23).Other risk factors for iCCA include primary sclerosing cholangitis(PSC), biliary duct cysts, hepatolithiasis, and hepatobiliary flukes.Hepatolithiasis has been defined as a well-known risk factor foriCCA (up to 20%) in Asian countries but not inWestern countries(11). Less-established risk factors with modest associationsinclude inflammatory bowel disease, obesity, diabetes, and alco-hol abuse (1, 11).
Cells of OriginiCCA includes a group of histologically heterogeneous tumors
with diverse cellular phenotypes and cell markers, which suggeststhe possible existence ofmultiple cells of origin (Fig. 1; ref. 24). Inaddition, the existence of mixed hepatocellular cholangiocarci-noma (HCC-iCCA) tumors (25), a subtypewith predominance ofstem cell features, points out the presence of a possible common
cell of origin. Thus, iCCA is currently believed to derive frombiliary epithelial cells (cholangiocytes) of the intrahepatic biliarytract, hepatic progenitor cells (HPC), or evenmature hepatocytes.
All liver cells share a common embryonic origin, arising frombipotential progenitors known as hepatoblasts (26). However,in the adult liver, normal tissue turnover is mainly sustained bydifferentiated hepatocytes and cholangiocytes. Nevertheless,upon major injury, there is an expansion of cells in the regionof the canals of Hering that have been proposed to be bipotentHPCs capable of differentiating into hepatocyte or cholangio-cyte lineages (Fig. 1; ref. 27). Alternatively, hepatocytes candedifferentiate into progenitor-like cells in response to acuteinjury (28, 29).
With this backdrop, the hypothesis that iCCA and HCC mayshare a commonancestor such as theHPCs has been an importantsubject of discussion during the past decade. Notably, emergingdata point to an overlapping molecular profile between specificsubclasses of iCCA and HCC tumors. Two independent studies(30, 31) have demonstrated that a subset of iCCA tumors areenriched with liver-specific stem cell gene signatures (30, 32, 33)and molecular subclasses of poor prognosis and aggressive phe-notype of HCC (proliferation; ref. 34; and S2 subclass; ref. 35).Reciprocally, a subset of HCC samples expressing biliary cellmarkers (i.e., CK19 and CK7; ref. 36) or enriched by iCCA-likegene expression signatures (37) showoverall survival rates similarto those for iCCA patients. In addition, cholangiolocellular car-cinoma (CLC), a stem cell featured mixed HCC-iCCA tumor,
Table 1. Main epidemiologic and molecular differences between iCCA and extrahepatic subtypes (pCCA-dCCA)
Gene or molecule iCCA pCCA-dCAA References
Proportion of CCA cases 5%–20% pCCA (50%–70%), dCCA (15%–20%) (12–15)
Incidence rate Increasing Stable or slightly decreasing (7–10)
Anatomic location Intrahepatic biliary tract Extrahepatic biliary tract (3)pCCA (near origin of cystic duct)dCCA (lower half of large duct)
Differenctial risk factors (n ¼ positive cases/total, % casesa)Biliary lithiasisb 377/1,539 (24%) 289/549 (52%) (17, 18, 20–23)Cirrhosis 161/1,622 (10%) 23/712 (3%) (17–23)HCV 61/1,522 (4%) 11/712 (1.5%) (17–21, 23)HBV 129/1,411 (9%) 4/712 (0.6%) (17–22)Alcoholc 158/1,524 (10%) 37/712 (5%) (17–22)
Molecular alterations (n ¼ positive cases/total, % casesa)Somatic mutationsTP53 99/606 (16%) 36/137 (26%) (50–53, 56–62)KRAS 165/885 (19%) 29/152 (19%) (50–53, 56–62)IDH1/2 143/951 (15%) 3/164 (2%) (51–54, 56–62)ARID1A 50/390 (13%) 20/137 (14%) (51–54, 56–57, 59, 61–62)BAP1 45/443 (11%) 3/164 (2%) (51–54, 56–57, 59, 61–62)BRAF 28/574 (5%) 0/137 (0%) (50–51, 53–54, 55–59, 61)EGFR 14/545 (3%) 3/151 (2%) (50–51, 53–54, 55–59, 61)
Fusion proteinsFGFR2 fusions 71/307 (23%) 0/36 (0%) (51, 56, 57, 72, 73, 75)
Chromosomal abberations (ampifications)d
17q11 (ERBB2) 0/170 (0%) 10/55 (18%) (31, 66)11q13 (FGF19, CCDN1, ORAOV1) 5/128 (4%) NA (31)
NOTE: Frequencies in iCCA have been calculated only in non–liver fluke cases.Abbreviations: dCCA, distal cholangiocarcinoma; HBV, hepatitis B virus infection; HCV, hepatitis C virus infection; iCCA, intrahepatic cholangiocarcinoma; NA, notapplicable; pCCA, perihilar cholangiocarcinoma.aThe percentage of cases has been calculated by considering the number of samples presenting themolecular alteration over the total number of samples analyzed inall cohorts (discovery and validation set of samples).bBiliary lithiasis includes patients with hepatolithiasis, cholelithiasis, and choledocholithiasis.cPatients with heavy alcohol consumption or alcoholic liver disease.dGenomic amplifications evaluated by FISH assay or copy number alteration by SNP array.
Moeini et al.
Clin Cancer Res; 22(2) January 15, 2016 Clinical Cancer Research292
on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296

shares similar histopathologic features with iCCA and CK19-positive HCC (12, 38). These data suggest HPC as a possiblecommon ancestor for a subset of primary liver cancers. Alterna-tively, the mutations associated with these tumors may "repro-gram" differentiated liver cells toward a progenitor-like state.
Recently, several studies using genetically engineered mousemodels (GEMM) and primary progenitor cell models have shedlight on the link between cell differentiation and iCCA path-
ogenesis. The expression of gain-of-function IDH mutations,commonly reported in iCCA, led to the inhibition of hepato-cyte differentiation both in vitro and in vivo and caused theexpansion of HPCs (39). In turn, combined IDH and KRASmutations in GEMMs showed pronounced oncogenic cooper-ation, leading to the development of premalignant biliarylesions and subsequent progression to iCCA. These data impli-cate mutant IDH in the subversion of liver differentiation states
© 2015 American Association for Cancer Research
HepatocyteHepatic
progenitorcells
Portal triad
Artery
Injury and/oroncogenic hit
ALB+/AFP+
EpCAM+
NCAM+
CK7+/CK19+
CD133+
ALB–/AFP–
EpCAM+
NCAM+
CK7+/CK19+
ALB–/AFP–
EpCAM+
NCAM–
CK7+/CK19+NOTCH signaling
activation
Cholangiocyte-committedprecursor
Maturehepatocyte
Hepatocyte-committedprecursor
EpCAM+
NCAM+
CK7+/CK19+
Maturecholangiocyte
EpCAM+
CK7+/CK19+
Hep-markers+/–
EpCAM+
NCAM+/–
CK7+/CK19+
CD133+
ALB+/AFP+
EpCAM+
NCAM–
CK7+/CK19+
ALB+/AFP+
EpCAM+
CK19+
ALB+/AFP+
ALB+/AFP+
EpCAM–
NCAM–
CK7–/CK19–
CoH Ductule BD
Renewal
WNT and NOTCH signaling activationIDH1/2 mutations
HPCs
?
Renewal
Vein
Cholangiocyte
HCC
MixedHCC–iCCA
iCCA
CLCProgenitor–like HCC
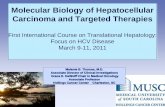
Figure 1.Schematic representation of multiple cells of origin in primary liver cancers. Hepatic progenitor cells (HPC) are located at canals of Hering (CoH) near the portaltriads and are thought to have the potential to differentiate into hepatocytes and cholangiocytes. There is evidence that the differentiated hepatocytes cangive rise to such cells. HCC and iCCA can develop from the neoplastic transformation of mature hepatocytes and cholangiocytes, respectively. In addition,HPC and its intermediate states are thought to be the common cell of origin for hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma (iCCA), andmixed HCC-iCCA tumors [i.e., cholangiolocellular carcinoma (CLC)]. Furthermore, recent evidence supports the hypothesis that mature hepatocytes cantransdifferentiate to cholangiocytes, leading to the development of iCCA.
Pathogenesis and Targeted Therapies in iCCA
www.aacrjournals.org Clin Cancer Res; 22(2) January 15, 2016 293
on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296

and in the persistence of HPCs that are susceptible to theaccumulation of additional oncogenic hits (Fig. 1). While thesestudies did not directly determine the origin of HPCs, they didpoint to expansion of progenitor-like cells as a key mechanismcontributing to liver carcinogenesis. Similarly, mice with genet-ic alterations in Hippo pathway components in the liver (i.e.,YAP, SAV1, MST1/2) show expansion of progenitor-like cells,followed by the development of both HCC and iCCA (40–42).In parallel, two independent studies demonstrated that differ-entiated hepatocytes have the potential to give rise to iCCAthrough the activation of NOTCH signaling (43, 44). Aberrantactivation of NOTCH signaling has been described in bothiCCA (60%) and HCC (30%) tumors (45, 46). Interestingly, ina GEMM with constitutive overexpression of NOTCH1, a subsetof the HCC tumors presented progenitor-like cell features witha mixed biliary and hepatocytic phenotype (45). In contrast, arecent study revealed that iCCA originates from the transfor-mation of biliary epithelial cells in the context of chronic injuryand p53 inactivation (47). Collectively, it appears that iCCAcan emerge from different liver cell types depending on theinitial triggering mutation and/or environmental insult. Futurestudies are needed to fully define these routes to iCCA, and tounderstand their molecular underpinnings as well their rele-vance to different iCCA subtypes.
Molecular PathogenesisOver the past 15 years,major scientific breakthroughs that have
significantly changed the management of human cancers havebeen driven by the discovery and successful therapeutic targetingof the so-called "oncogenic addiction loops." The term "oncogeneaddiction" is used to define the dependency status of cancer cellson the activation or loss of specific genes. Several examples exist of
the striking survival benefits obtained in BRAF-mutated melano-mas treated with vemurafenib (48) or in lung cancer harboringALK rearrangements and treated with crizotinib (49). Unfortu-nately, to date, no oncogene addiction loop has been reported iniCCA.
The molecular pathogenesis of iCCA is a complex processinvolving multiple genomic alterations and signaling pathwayderegulations. Before the implementation of next-generationsequencing technologies, our knowledge of the role of muta-tions in iCCA was limited, encompassing recurrent activatingmutations in KRAS (19%), low frequency mutations in BRAF(5%), and EGFR (3%), and widely varying reports of loss-of-function mutations in the tumor suppressor TP53 (16%, range1%–38%; Tables 1 and 2; refs. 31, 50–64). While KRAS andTP53mutations are relatively common in all CCA, mutations inIDH1/2 and BRAF are considerably more prevalent in iCCA(Table 1). Epigenetic alterations through promoter hyper-methylation have also been described, and the most recurrent(>25%) affects p16INK4A/CDKN2, p14ARF, RASSF1A, APC,GSTP, and SOCS-3 (58). Inflammation-related signaling path-ways, such as JAK–STAT3, and proliferation-related pathways,such as EGFR and HGF–MET signaling, show profound dereg-ulation in iCCA (58). In addition, recent studies have proposedemerging roles for NOTCH and WNT signaling in iCCA path-ogenesis. Furthermore, two independent whole-transcriptomeanalyses discerned the existence of two distinct molecularsubclasses of iCCA (31, 50). Both studies identified a prolifer-ation molecular subclass that defines tumors with activation ofoncogenic signaling pathways, including RAS–MAPK, MET, andEGFR, and poor prognosis. In addition, approximately 40% ofpatients belong to the Inflammation subclass, characterized byenrichment of cytokine related pathways, constitutive activa-tion of STAT3, and better prognosis (31).
Table 2. Potential molecular alterations amenable for targeted therapies in iCCA
Gene or molecule Type of alterationNo. of positive/totalsamples (frequency)a References
Somatic mutationsMetabolic enzymesIDH1/2 Activating mutations 143/951 (15%) (51–54, 56–62)
Tyrosine kinase signalingKRAS Activating mutations 165/885 (19%) (50–53, 56–62)BRAF Activating mutations 28/574 (5%) (50–51, 53–54, 55–59, 61)EGFR Activating mutations 14/545 (3%) (50–51, 53–54, 55–59, 61)
Chromatin-remodeling genesARID1A Inactivating mutations 50/390 (13%) (51–54, 56–57, 59, 61–62)BAP1 Inactivating mutations 45/443 (11%) (51–54, 56–57, 59, 61–62)PBRM1 Inactivating mutations 34/443 (8%) (51–54, 56–57, 59, 61)
Tyrosine kinase (TK) fusion proteinsFGFR2 fusionsFGFR2–BICC1 TK fusion protein 46/211 (22%) (51, 56, 57, 72, 73, 75)FGFR2–PPHLN1 TK fusion protein 17/153 (11%) (51, 56, 57, 72, 73, 75)FGFR2–AHCYL1 TK fusion protein 7/111 (6%) (51, 56, 57, 72, 73, 75)FGFR2–MGEA5 TK fusion protein 1/53 (2%) (51, 56, 57, 72, 73, 75)FGFR2–TACC3 TK fusion protein 2/53 (4%) (51, 56, 57, 72, 73, 75)FGFR2–KIAA1598 TK fusion protein 1/53 (2%) (51, 56, 57, 72, 73, 75)
ROS fusionsROS1 fusions TK fusion protein 2/23 (9%) (77)
Chromosomal aberrations11q13 (FGF19, CCND1, ORAOV1) High-level amplification 5/128 (4%) (32)
aThe frequency in iCCAhas been calculated by considering the number of samples presenting themolecular alteration over the total number of samples for which thespecific alteration has been evaluated (discovery and validation set of samples) in different studies. Frequencies in iCCA have been calculated only in non–liver flukecases.
Moeini et al.
Clin Cancer Res; 22(2) January 15, 2016 Clinical Cancer Research294
on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296

Emerging signaling pathwaysNOTCH signaling. The NOTCH signaling pathway is known toplay an important role during embryonic development and isessential for a proper maturation of the liver architecture. Recent-ly, NOTCH pathway deregulation has been implicated in induc-tion of inflammation (65) and the development and progressionof iCCA (66, 67). In human CCAs, upregulation ofNOTCH1 andNOTCH4 has been reported in 82.9% and 56.1%, respectively,(46). In preclinical studies, liver-induced expression of NOTCH1intracellular domain in mice resulted in the formation of iCCAs(67). Considering that a number of NOTCH inhibitors are cur-rently under development, the NOTCH pathway may represent anovel amenable target in iCCA (Fig. 2). However, a recent studyreported different effects of targeting NOTCH receptors in amouse model of primary liver cancer driven by v-akt viral onco-gene homolog (AKT) and neuroblastoma RAS viral oncogenehomolog (NRAS; ref. 68). Interestingly, while the inhibition ofNOTCH2 reduced tumor burden,NOTCH1 inhibition altered therelative proportion of tumor types, reducingHCC-like tumors butdramatically increasing CCA-like tumors (68). Thus, further stud-ies are needed to understand the complex role of NOTCH sig-naling in primary liver cancer.
WNT signaling. TheWNTpathway is highly activated in the tumorepithelium of human CCAs and is often characterized by over-expression of the ligandsWNT7B andWNT10A alongwith severaltarget genes (69, 70). It has been demonstrated that inflammatorymacrophages in the stroma surrounding the tumor are requiredfor the maintenance of this highly activated WNT signaling status(69, 71). As recently demonstrated in two rodent models mim-icking human iCCA, the WNT pathway was progressively activat-ed during the course of iCCA development, and treatment in vitroand in vivo with WNT inhibitors (ICG001 and C59) successfullyinhibited tumor growth (69). Considering the recent develop-ment of several pharmacologicWNT inhibitors and the absence ofAPC and CTNNB1 mutations in iCCA, the WNT pathway mayrepresent another important clinical opportunity (Fig. 2).
Identification of Novel DriversRecent technological advancements have led to a better under-
standing of the genetic and molecular forces that drive humancancers. Significant progress has been made also in iCCA, wheredeep-sequencing studies have unveiled novel mutations (i.e.,IDH1/2, ARID1A) and oncogenic fusion genes (ROS1 and FGFR2fusions). In the following section, we highlight the most prom-ising discoveries, with particular emphasis on those potentiallyamenable to targeted therapies (Table 2; Fig. 2).
Tyrosine kinase fusion genesFGFR2 is a tyrosine kinase (TK) protein that acts as cell-surface
receptor for fibroblast growth factors and plays an essential rolein the regulation of cell proliferation, differentiation, migration,and apoptosis. Recently, several FGFR2 chromosomal fusionswith multiple genomic partners have been identified in severalcancers, including iCCA (Table 2; refs. 51, 56, 57, 72–75). Allof these fusions contain the same portion of the FGFR2 recep-tor (exons 1–19) and are fused to different partners throughgenomic breakpoints within the same intronic region (e.g.,BICC1, PPHLN1, CCDC6, MGEA5, TACC3). The oncogenic acti-vation of these FGFR2 fusion proteins relies on the activation
of the TK included in the rearrangement and involves enforceddimerization, subsequent transautophosphorylation, and acti-vation of downstream signaling pathways (57, 72, 73). Trans-forming and oncogenic potential of FGFR2 fusions (FGFR2–BICC1, FGFR2–PPHLN1, FGFR2–AHCYL1, FGFR2–TACC3) hasbeen proven in vitro (57, 72, 73, 76) and in vivo (72). Furthermore,the presence of FGFR2 fusions seems to predict higher sensitivityto selective FGFR2 inhibitors (57, 72, 73, 76). However, therelative oncogenic potential of the different FGFR2 fusions ortheir sensitivity to specific FGFR2 inhibitors remains unknownand should be extensively investigated in future studies.Screening of FGFR2 fusions in multiple studies by massiveparallel sequencing technologies or FISH-based assay hasrevealed striking differences in the incidence of the FGFR2fusion events with a range between 3% and 50% of iCCApatients (51, 56, 57, 72, 73, 75). FGFR2 fusions were found tobe rare in mixed HCC-iCCA and mostly absent in HCC andeCCA (Table 1; refs. 57, 72). Thus, FGFR2 fusions are a novelhallmark of iCCA.
A significant association has been observed between the pres-ence of FGFR2 fusions (FGFR2–PPHLN1, FGFR2–BICC1) andKRAS mutations and signaling pathway activation, suggesting apossible cooperative role in driving iCCApathogenesis (57). Eventhough no clear association between presence of FGFR2 fusionsand clinicopathologic parameters (e.g., gender, age, stage, andprognosis) has been identified across themultiple datasets, a largestudy conducted in Japan has suggested a significant associationwith viral hepatitis (72), and a female predominance wasobserved in a North American cohort (75). Larger epidemiologicstudies need to be conducted to clarify such discrepancies.
Besides FGFR2 fusions, ROS1 kinase fusion proteins have beenidentified in 8.7% (2/23) of CCAs (77). Expression of FIG–ROS1in NIH3T3 cells conferred transforming ability both in vitro and invivo, which could be inhibited by specific targeting (77). Further-more, the oncogenic potential of FIG–ROS has been recentlyvalidated in an orthotopic allograftmouse iCCAmodel harboringKRAS and TP53 mutations (78). FIG–ROS alone was also able topromote tumorigenesis, although with reduced penetrance andlonger latency. Notably, preliminary data support the efficacy oftherapeutic targeting of ROS1 kinase in vitro and in vivowith smallATP-competitive inhibitors (e.g., foretinib, crizotinib). Furtherinvestigation will be required to establish the frequency of ROSfusions across different iCCA patient populations and to evaluatethe potential benefit of such therapies for patients with thesetranslocated alleles.
New somatic alterationsThe application of exome-sequencing technologies has led to
the discovery of novel somatic mutations in the protein-codingregion of several genes and has defined amutational landscape ofthe disease. Interestingly, emerging data supports a differentgenetic profile between liver fluke–related and non–liver flukerelated CCAs in terms of gene expression (79) and mutationprofiles (80). Exome sequencing of 8 cases of liver fluke-relatedCCAs identified 10 novel mutated genes involved in histonemodification, genomic instability, and G protein signaling(e.g., KMT2C, ROBO2, PEG3, and GNAS) and confirmed muta-tions in already known genes (TP53 and KRAS; ref. 80). A follow-up study was later conducted by the same group and profiled209 CCAs collected from Asia and Europe, associated withOpisthorchis viverrini (n ¼ 108) and non–O. viverrini–related
Pathogenesis and Targeted Therapies in iCCA
www.aacrjournals.org Clin Cancer Res; 22(2) January 15, 2016 295
on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296

© 2015 American Association for Cancer Research
CetuximabPanitumumab Bevacizumab Antiligand mAbs
(e.g., OMP-21M18)JAG1–2DLL1–4
NOTCH1–4
Antireceptor mAbs(e.g., OMP-52M51,
OMP-59R5)
WNT inhibitors(e.g., XAV-939, ICG-001,
IWP-2, IWR-1-endo)
WNTFZD
Tumorcell
DVL
GSK3
APCUb
UbUb
PPP
P PP P
P P P P P P
GSK3 inhibitors(e.g., CHIR-99021,
TWS119, tideglusib)
γ-secretase
α-KG
Degradation
γ-secretaseinhibitors
(e.g., RO4929097,MK0752)
BICC1PPHLN1MGEA5TACC3KIAA1598
Cellmembrane
Nucleus
LapatinibErlotinib
Vandetanib
ERBB
2 PDG
FR
FGFR
2
FGFR
2
PDG
FR
EGFR
EGFR
VEG
FR
VEG
FR
ERBB
2
TKTK TK
TK TK TK TK TK TK
TK
CediranibSunitinib
RefametinibSelumetinibTrametinib
HDAC inhibitors(e.g., vorinostat,panabinostat)
SorafenibRegorafenib
PTEN
ARID1A
BAP1
TET1/2
TCF/LEF
Target geneexpression
Histonedemethylation
Everolimus
AG-221
TCAcycle
RAS–MAPKpathway
PIK3–AKTpathway
MTOR
AKT
PIK3
IDH1
Mitochondria
AG-120
Isocitrate
Citrate
WNT/β-catenin inhibitors(e.g., XAV-939, ICG-001,
IWP-2, IWR-1-endo)
β-catenin
β-catenin
β-catenin β-catenin β-catenin
NC
ID
NC
ID
2-HGα-KG
IDH2Isocitrate
Citrate
2-HG
IDH1mut
IDH2mut
ERK
MEK
BRAF
KRAS
BGJ398AZD4547
LY2874455Ponatinib
AXIN
AXIN
FGFR2 fusionsEGF VEGF
Moeini et al.
Clin Cancer Res; 22(2) January 15, 2016 Clinical Cancer Research296
on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296

etiologies (n¼ 101; ref. 52). In summary, these studies reveal that(i) TP53, SMAD4, KMT2C, and GNAS are more commonlymutated in O. viverrini–infected CCA cases; (ii) IDH1/IDH2mutations are almost exclusive for non–O. viverrini–related iCCA;and (iii) fluke-related CCAs present a mean of 26 somatic muta-tions per tumor, compared with a mean of 16 mutations pertumor in CCA with other etiologies. In addition, whole-exomesequencing (WES) studies have led to the identificationof somaticmutations in chromatin-remodeling genes, BAP1, ARID1A, andPBRM1—in iCCA (52, 54). Functional studies have revealedtumor-suppressive activity of BAP1 and ARID1A, further support-ing the potential role of chromatin modulators in iCCA devel-opment (52). In particular, ARID1A encodes an accessory subunitof the SWI/SNF chromatin-remodeling complex andmutations inthis gene have recently been identified in awide variety of cancers.Silencing of ARID1A in CCA cell lines (including non–O. viver-rini–associated and O. viverrini–associated) resulted in a signifi-cant increase of cell proliferation. Conversely, overexpression ofwild-typeARID1A led to retarded cell proliferation confirming thetumor-suppressive role of this gene (52). Thepossibility that iCCApatients harboring mutations in these genes may benefit fromtreatment with histone deacetylase (HDAC) inhibitors, such asvorinostat or panobinostat, remains unclear and needs to befurther explored.
IDH1 and IDH2mutations havebeen reported in approximately14% of iCCAs (Table 2). In a large cohort of iCCA cases (n¼ 326),IDH1/2mutationswere associatedwithbetter overall survival (60).In contrast, in a recent WES-based study, patients with IDH1 orIDH2mutations had shorter survival compared with patients withwild-type IDH genes (3-year survival of 33% in IDH mutants vs.81% in IDHwild-type; ref. 54). IDH1 and IDH2mutations in iCCAand other cancer types cluster at the hotspots codons 132 and 172,respectively. IDH1 and IDH2 encode metabolic enzymes whosenormal function is to interconvert the metabolic intermediateisocitrate to a-ketoglutarate (a-KG) in conjunction with the gen-eration of NADPH. Mutations in IDH1 and IDH2 are alwayspresent in a heterozygous state with the wild-type allele and theyresult in the acquisition of an abnormal enzymatic activity, thereduction of a-KG to 2-hydroxyglutarate (2-HG). 2-HG has beendesignated as an "oncometabolite" that contributes to cancerformation by inhibiting multiple dioxygenase enzymes thatrequire a-KG for their activity, resulting in altered cell differenti-ation, survival, and extracellularmatrixmaturation (Fig. 2). Abnor-mal DNA methylation and increased protein levels of TP53 arecommon features of tumors with IDH1 and IDH2mutations (60).Furthermore, using in vitro stem cell systems and GEMMs, it hasbeen demonstrated that mutant IDH mutations are able to pro-mote iCCA formation by blocking hepatocyte differentiation andinducing proliferation of hepatic progenitors (39).
Management and Molecular TargetedTherapies
At present, the treatment of choice for iCCA when feasible issurgical resection (1), whereas liver transplantation remains con-troversial. Upon resection, the median overall survival is ofaround 3 years and recurrence occurs in up to 60% of patients,depending on several prognostic factors, among which tumorburden and lymphonodal status appear to be the most relevant(1, 16). The prognosis for patients diagnosed with unresectabledisease is even more dismal, with a life expectancy around 1 yearand actuarial probability of survival of 5% at 5 years (1, 58).
The lack of clinical trials conducted specifically in iCCA pati-ents as opposed to all biliary tract cancers (BTC) and the limitednumber of patients studied are among the challenges that precludeclinical practice guidelines in establishing a standard of care forpatients with advanced iCCA (1). Among the 112 clinical trialsreported in advanced BTCs testing systemic therapies (81), themajority are single-arm phase II studies with low statistical powerand unclear impact on overall survival. The current standard ofpractice for advanced-stage iCCA is represented by systemic che-motherapy with gemcitabine and cisplatin (6). Survival benefitsfavoring the combination arm as opposed to gemcitabine alone(11.7 vs. 8 months; ref. 6) were demonstrated in a subgroupanalysis of patients with iCCA (n ¼ 80) included in a largerandomized phase III trial (n ¼ 410, ABC-02) of patients withadvanced and metastatic BTCs.
On the other hand, so far no molecular targeted therapy hasbeen proven effective for iCCA or other biliary tract cancers.The results of few trials with targeted therapies as monotherapy(i.e., selumitinib) or in combination with chemotherapy (i.e.,sorafenib plus gemcitabine, cetuximab plus gemcitabine–oxali-platin) have been discouraging with limited effects on overallsurvival (1). In this sense, patient stratification based on molec-ular biomarkers (Table 2) may be essential for clinical success intreating iCCA patients. Toward this direction, the first clinicaltrials driven by biomarkers (e.g., FGFR2 aberrations and IDH1/2mutations) in BTCs, including iCCA, are currently ongoing andtheir results are anxiously awaited (Fig. 2, Table 3). BGJ398, aselective FGFR inhibitor, has shown efficacy in vitro by blockingthe neoplastic transformation and growth of cell lines expressingFGFR2 fusions (57). Clinical efficacy of BGJ398 is currently beinginvestigated in a phase II multicenter single-arm study in adultpatients with advanced or metastatic CCA harboring FGFR2 genefusions or other FGFR genetic alterations who have failed che-motherapy (NCT02150967). Furthermore, promising prelimi-nary data have been reported following treatmentwith ponatinib,a multikinase inhibitor, in 2 iCCA patients harboring FGFR2fusions (FGFR2–TACC3, FGFR2–MGEA5), resulting in tumor size
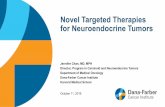
Figure 2.Current and potential targeted therapies in intrahepatic cholangiocarcinoma. Tyrosine kinase receptor signaling: several growth factor signaling pathways(i.e., EGF/EGFR) have been reported to be aberrantly activated in iCCA. The specify binding of growth factors results in oligomerization and autophosphorylationof their receptors, followed by signaling through the RAS–MAPK and PI3K–AKT effector cascades. FGFR2 fusions: The presence of fusion partners in thecytoplasmic domain of FGFR2 results in constitutively active receptors that induce signaling through downstream signaling pathways. NOTCH signaling: Bindingof ligands on the surface of neighboring cells to the extracellular domain of NOTCH receptors (NOTCH-R) induces proteolytic cleavage of the receptor,releasing its intracellular domain (NICD), which then translocates to the nucleus and regulates expression of target genes. WNT/b-catenin signaling: activation offrizzled (FZD) receptors by WNT ligands triggers the displacement of the regulatory APC/Axin/GSK3-complex, accumulation of b-catenin and induction oftarget genes. IDH signaling: Mutated IDH enzymes acquire the capacity to synthesize 2-hydroxygluterate (2-HG) from a-ketoglutarate (a-KG). 2-HG alters theactivity of a-KG–dependent dioxygenase enzymes involved in multiple cellular processes, including cell differentiation, survival, and DNA methylation.Molecular targeted therapies havealsobeenhighlighted; drugs currently assessed in phase II clinical trials (red) and thoseevaluated in early clinical trials or preclinicalstudies (brown) are shown.
Pathogenesis and Targeted Therapies in iCCA
www.aacrjournals.org Clin Cancer Res; 22(2) January 15, 2016 297
on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296

reduction (51). Currently, a pilot studywith ponatinib is ongoingin BTC patients with FGFR2 fusions (NCT02265341). At the sametime, based on demonstrated efficacy in preclinical studies, spe-cific inhibitors for IDH1 (AG-120) and IDH2 (AG-221) arecurrently being investigated inphase I (NCT02073994) andphaseI/II (NCT02273739) clinical trials, respectively (Table 3). Inparallel, considering the emerging roles of NOTCH and WNTpathway activation in the pathogenesis of iCCA, the first clinicaltrials targeting these pathways using available specific inhibitorsare expected to move forward (Fig. 2).
Future PerspectivesThe application of new technologies has led to a more accurate
mapping of the genomic landscape of iCCA, a devastating diseasewith limited treatment options. Among the newly discoveredmolecular alterations, FGFR2 fusions and IDH1/2mutations hold
great promise for improving the future management and treat-ment of iCCA patients through the first biomarker-driven clinicalstudies currently ongoing. Whether FGFR2 aberrations may rep-resent a novel oncogene addiction loop in iCCA still remains anunanswered question. Nevertheless, FGFR2 fusions have thepotential to represent a new avenue of research for basic inves-tigators and clinicians. Finally, the intriguing possibility of mul-tiple cells of origin in iCCA deserves further investigation as ameans to understand the mechanisms underlying the carcino-genesis process and to determine whether this can be of relevancein clinical application.
Disclosure of Potential Conflicts of InterestV. Mazzaferro reports receiving speakers bureau honoraria from Bayer and
BTG. J.M. Llovet reports receiving commercial research grants from Bayer,Blueprint Medicines, and Boehringer Ingelheim; other commercial researchsupport from Bayer, Boehringer Ingelheim, and Bristol-Myers Squibb; and is
Table 3. Ongoing clinical trials using targeted therapiesa
Treatment Targets Clinical trial phase Number of trials
Biomarker drivenBGJ398 FGFR, ABL, FYN, KIT, LCK, LYN, YES II 1Ponatinib hydrocloride BCR-ABL, VEGFR, PDGFR, FGFR, EPH, SRC, KIT, RET, TIE2, FLT3 II 1AG-221 Mutated IDH2 I/II 1AG-120 Mutated IDH1 I 1
MonotherapyCabozantinib (XL-184) MET, VEGFR2, RET, c-KIT, FLT1/3/4, TIE2 II 1Everolimus mTOR II 2Sunitinib VEGFR, PDGFR, KIT, FLT3, RET II 1Regorafenib RET, RAF-1, VEGFR, KIT, BRAF (V600E), PDGFRB, FGFR1, TIE2 II 2Celecoxib COX IV 1c
Trastuzumab HER2-neu II 1LY2801653 c-MET, MST1R, FLT3, AXL, MERTK, TEK, ROS1, DDR1/2 I 1BKM120 VPS34/mTOR/DNAPK/PI4Kb II 1Lapatinib ErbB2-4/EGFR/SRC II 2Selumetinib MEK1/2 II 1MK2206 AKT1-3 II 1RAV12 RAAG12 I 1PLX8394 BRAF I/II 1
CombinationSelumetinib þ MK-2206 MEK1 þ AKT1-3 II 1Bosutinib þ capecitabine ABL/SRC/c-KIT I 1AZD2171 þ AZD0530 VEGFR/PDGFR/FGFR1/c-KIT þ SRC/ABL/LCK/YES/EGFR/LYN I 1Pazopanib þ GSK1120212 VEGFR/PDGFR/FGFR/KIT þ MEK1/2 I 1Cetuximab þ erlotinib EGFR I/II 2c
Trastuzumab þ tipifarnib HER2-neu þ FTI I 1Erlotinib þ bevacizumab EGFR þ VEGFA II 2
Combination with chemotherapyRadiotherapy þ bevacizumab VEGFA I 1Chemotherapyb þ veliparib PARP1/2 I 1Chemotherapy þ bevacizumab VEGFA II 2c
Chemotherapy � panitumumab EGFR II 5c
Chemotherapy � vandetanib (ZD6474) VEGFR, EGFR I, II 2c
Chemotherapy þ cediranib VEGFR II 1Chemotherpy � sorafenib BRAF, VEGFR, PDGFR I/II 2Chemotherapyb � cetuximab EGFR II 2c
Chemotherpyb þ selumetinib MEK1/2 I/II 1Chemotherpy � trametinib MEK1/2 II 1Chemotherapyb þ sirolimus mTOR I 1Chemotherapy þ pazopanib VEGFR/PDGFR/FGFR/KIT II 1Chemotherapy þ AZD2171 VEGFR/PDGFR/FGFR1/c-KIT II 1Chemotherapyb � CX-4945 CX2 I/II 1c
Chemotherapy þ erlotinib EGFR I/II 3
Abbreviations: FGFR, fibroblast growth factor; KIT, c-kit proto-oncogene receptor tyrosine kinase; PDGFR, platelet-derived growth factor receptor.aInformation acquired from clinicaltrials.gov.bChemotherapy (standard of practice: gemcitabine and cisplatin).cRandomized controlled clinical trials.
Moeini et al.
Clin Cancer Res; 22(2) January 15, 2016 Clinical Cancer Research298
on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296

a consultant/advisory board member for Bayer, Biocompatibles, BlueprintMedicines, Boehringer Ingelheim, Bristol-Myers Squibb, Celsion, Eli Lilly,GlaxoSmithKline, andNovartis. No potential conflicts of interest were disclosedby the other authors.
Grant SupportA. Moeini is supported by a fellowship from Spanish National Health
Institute (FPI program, BES-2011-046915). D. Sia is supported by theILCA-Bayer Fellowship. N. Bardeesy holds the Gallagher Endowed Chairin Gastrointestinal Cancer Research at Massachusetts General Hospital andis supported by a V Foundation Translational Award, the TargetCancer Foun-
dation, and the NIH under award numbers R01CA136567-02 andP50CA1270003. V. Mazzaferro is partially supported by the AIRC (ItalianAssociation for Cancer Research) and a 5�1000 Milan-INT institutional grantin hepato-oncology. J.MLlovet is supported by grants from the SamuelWaxmanCancer Research Foundation, Asociaci�on Espa~nola Contra el C�ancer, SpanishNational Health Institute (SAF-2013-41027), and a European CommissionHEP-CAR grant (667273-2).
Received June 5, 2015; revised August 6, 2015; accepted August 6, 2015;published OnlineFirst September 24, 2015.
References1. Bridgewater J, Galle PR, Khan SA, Llovet JM, Park JW, Patel T, et al.
Guidelines for the diagnosis and management of intrahepatic cholangio-carcinoma. J Hepatol 2014;60:1268–89.
2. Yang JD, Kim B, Sanderson SO, Sauver JS, Yawn BP, Larson JJ, et al. Biliarytract cancers in Olmsted County, Minnesota, 1976–2008. Am J Gastro-enterol 2012;107:1256–62.
3. Rizvi S, Gores GJ. Pathogenesis, diagnosis, and management of cholan-giocarcinoma. Gastroenterology 2013;145:1215–29.
4. Njei B. Changing pattern of epidemiology in intrahepatic cholangiocarci-noma. Hepatology 2014;60:1107–8.
5. de JongMC, Nathan H, Sotiropoulos GC, Paul A, Alexandrescu S, MarquesH, et al. Intrahepatic cholangiocarcinoma: an international multi-institu-tional analysis of prognostic factors and lymph node assessment. J ClinOncol 2011;29:3140–5.
6. Valle J, Wasan H, Palmer DH, Cunningham D, Anthoney A, Maraveyas A,et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer.N Engl J Med 2010;362:1273–81.
7. Khan SA, Toledano MB, Taylor-Robinson SD. Epidemiology, risk factors,and pathogenesis of cholangiocarcinoma. HPB 2008;10:77–82.
8. Patel T. Increasing incidence and mortality of primary intrahepatic cho-langiocarcinoma in the United States. Hepatology 2001;33:1353–7.
9. Patel T. Worldwide trends in mortality from biliary tract malignancies.BMC Cancer 2002;2:10.
10. Taylor-Robinson SD, Toledano MB, Arora S, Keegan TJ, Hargreaves S, BeckA, et al. Increase inmortality rates from intrahepatic cholangiocarcinoma inEngland and Wales 1968–1998. Gut 2001;48:816–20.
11. Tyson GL, El-Serag HB. Risk factors for cholangiocarcinoma. Hepatology2011;54:173–84.
12. Blechacz B, Komuta M, Roskams T, Gores GJ. Clinical diagnosis andstaging of cholangiocarcinoma. Nat Rev Gastroenterol Hepatol 2011;8:512–22.
13. DeOliveira ML, Cunningham SC, Cameron JL, Kamangar F, Winter JM,Lillemoe KD, et al. Cholangiocarcinoma: thirty-one-year experience with564 patients at a single institution. Ann Surg 2007;245:755–62.
14. Khan SA, Davidson BR, Goldin RD, Heaton N, Karani J, Pereira SP, et al.Guidelines for the diagnosis and treatment of cholangiocarcinoma: anupdate. Gut 2012;61:1657–69.
15. Khan SA, Emadossadaty S, Ladep NG, Thomas HC, Elliott P, Taylor-Robinson SD, et al. Rising trends in cholangiocarcinoma: is the ICDclassification system misleading us? J Hepatol 2012;56:848–54.
16. RazumilavaN,GoresGJ. Cholangiocarcinoma. Lancet 2014;383:2168–79.17. Donato F, Gelatti U, Tagger A, Favret M, Ribero ML, Callea F, et al.
Intrahepatic cholangiocarcinoma and hepatitis C and B virus infection,alcohol intake, and hepatolithiasis: a case-control study in Italy. CancerCauses Control 2001;12:959–64.
18. Lee TY, Lee SS, Jung SW, Jeon SH, Yun SC, Oh HC, et al. Hepatitis B virusinfection and intrahepatic cholangiocarcinoma in Korea: a case-controlstudy. Am J Gastroenterol 2008;103:1716–20.
19. Shaib YH, El-Serag HB, Nooka AK, Thomas M, Brown TD, Patt YZ,et al. Risk factors for intrahepatic and extrahepatic cholangiocarci-noma: a hospital-based case-control study. Am J Gastroenterol 2007;102:1016–21.
20. Welzel TM,Graubard BI, El-SeragHB, Shaib YH,Hsing AW,Davila JA, et al.Risk factors for intrahepatic and extrahepatic cholangiocarcinoma in theUnited States: a population-based case-control study. Clin GastroenterolHepatol 2007;5:1221–8.
21. Yamamoto S, Kubo S, Hai S, Uenishi T, Yamamoto T, Shuto T, et al.Hepatitis C virus infection as a likely etiology of intrahepatic cholangio-carcinoma. Cancer Sci 2004;95:592–5.
22. Peng NF, Li LQ, Qin X, Guo Y, Peng T, Xiao KY, et al. Evaluation of riskfactors and clinicopathologic features for intrahepatic cholangiocarcinomain Southern China: a possible role of hepatitis B virus. Ann Surg Oncol2011;18:1258–66.
23. Welzel TM, Graubard BI, Zeuzem S, El-Serag HB, Davila JA, McGlynn KA.Metabolic syndrome increases the risk of primary liver cancer in the UnitedStates: a study in the SEER-Medicare database. Hepatology 2011;54:463–71.
24. Roskams T, Katoonizadeh A, Komuta M. Hepatic progenitor cells: anupdate. Clin Liver Dis 2010;14:705–18.
25. Akiba J, Nakashima O, Hattori S, Tanikawa K, Takenaka M, Nakayama M,et al. Clinicopathologic analysis of combined hepatocellular-cholangio-carcinoma according to the latest WHO classification. Am J Surg Pathol2013;37:496–505.
26. Si-Tayeb K, Lemaigre FP, Duncan SA. Organogenesis and development ofthe liver. Dev Cell 2010;18:175–89.
27. Kordes C, Haussinger D. Hepatic stem cell niches. J Clin Invest 2013;123:1874–80.
28. TarlowBD, Pelz C,NauglerWE,Wakefield L,Wilson EM, FinegoldMJ, et al.Bipotential adult liver progenitors are derived from chronically injuredmature hepatocytes. Cell Stem Cell 2014;15:605–18.
29. Yanger K, Zong Y, Maggs LR, Shapira SN, Maddipati R, Aiello NM, et al.Robust cellular reprogramming occurs spontaneously during liver regen-eration. Genes Dev 2013;27:719–24.
30. Oishi N, Kumar MR, Roessler S, Ji J, Forgues M, Budhu A, et al. Transcrip-tomic profiling reveals hepatic stem-like gene signatures and interplay ofmiR-200c and epithelial-mesenchymal transition in intrahepatic cholan-giocarcinoma. Hepatology 2012;56:1792–803.
31. SiaD,Hoshida Y, Villanueva A, Roayaie S, Ferrer J, Tabak B, et al. Integrativemolecular analysis of intrahepatic cholangiocarcinoma reveals 2 classesthat have different outcomes. Gastroenterology 2013;144:829–40.
32. Lee JS, Heo J, Libbrecht L, Chu IS, Kaposi-Novak P, Calvisi DF, et al. A novelprognostic subtype of human hepatocellular carcinoma derived fromhepatic progenitor cells. Nat Med 2006;12:410–6.
33. Yamashita T, Ji J, Budhu A, Forgues M, Yang W, Wang HY, et al. EpCAM-positive hepatocellular carcinoma cells are tumor-initiating cells withstem/progenitor cell features. Gastroenterology 2009;136:1012–24.
34. Chiang DY, Villanueva A, Hoshida Y, Peix J, Newell P, Minguez B, et al.Focal gains of VEGFA and molecular classification of hepatocellularcarcinoma. Cancer Res 2008;68:6779–88.
35. Hoshida Y, Nijman SM, KobayashiM, Chan JA, Brunet JP, ChiangDY, et al.Integrative transcriptome analysis reveals commonmolecular subclasses ofhuman hepatocellular carcinoma. Cancer Res 2009;69:7385–92.
36. Roskams T. Liver stem cells and their implication in hepatocellular andcholangiocarcinoma. Oncogene 2006;25:3818–22.
37. WooHG, Lee JH, Yoon JH, KimCY, Lee HS, Jang JJ, et al. Identification of acholangiocarcinoma-like gene expression trait in hepatocellular carcino-ma. Cancer Res 2010;70:3034–41.
38. Komuta M, Spee B, Vander Borght S, De Vos R, Verslype C, Aerts R, et al.Clinicopathological study on cholangiolocellular carcinoma suggestinghepatic progenitor cell origin. Hepatology 2008;47:1544–56.
39. Saha SK, Parachoniak CA,Ghanta KS, Fitamant J, Ross KN,NajemMS, et al.Mutant IDH inhibits HNF-4alpha to block hepatocyte differentiation andpromote biliary cancer. Nature 2014;513:110–4.
www.aacrjournals.org Clin Cancer Res; 22(2) January 15, 2016 299
Pathogenesis and Targeted Therapies in iCCA
on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296

40. Fitamant J, Kottakis F, Benhamouche S, Tian HS, Chuvin N, ParachoniakCA, et al. YAP inhibition restores hepatocyte differentiation in advancedHCC, leading to tumor regression. Cell Rep 2015;10:1692–707.
41. Lee KP, Lee JH, Kim TS, Kim TH, Park HD, Byun JS, et al. The Hippo-Salvador pathway restrains hepatic oval cell proliferation, liver size, andliver tumorigenesis. Proc Natl Acad Sci U S A 2010;107:8248–53.
42. Lu L, Li Y, Kim SM, Bossuyt W, Liu P, Qiu Q, et al. Hippo signaling is apotent in vivo growth and tumor suppressor pathway in the mammalianliver. Proc Natl Acad Sci U S A 2010;107:1437–42.
43. Fan B, Malato Y, Calvisi DF, Naqvi S, Razumilava N, Ribback S, et al.Cholangiocarcinomas can originate fromhepatocytes inmice. J Clin Invest2012;122:2911–5.
44. Sekiya S, Suzuki A. Intrahepatic cholangiocarcinoma can arise fromNotch-mediated conversion of hepatocytes. J Clin Invest 2012;122:3914–8.
45. Villanueva A, Alsinet C, Yanger K, Hoshida Y, Zong Y, Toffanin S, et al.Notch signaling is activated in human hepatocellular carcinoma andinduces tumor formation in mice. Gastroenterology 2012;143:1660–9.
46. WuWR, Shi XD, Zhang R, ZhuMS, Xu LB, Yu XH, et al. Clinicopathologicalsignificance of aberrant Notch receptors in intrahepatic cholangiocarci-noma. Int J Clin Exp Pathol 2014;7:3272–9.
47. Guest RV, Boulter L, Kendall TJ, Minnis-Lyons SE, Walker R, Wigmore SJ,et al. Cell lineage tracing reveals a biliary origin of intrahepatic cholangio-carcinoma. Cancer Res 2014;74:1005–10.
48. Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J, et al.Improved survival with vemurafenib in melanoma with BRAF V600Emutation. N Engl J Med 2011;364:2507–16.
49. Shaw AT, Kim DW, Nakagawa K, Seto T, Crino L, Ahn MJ, et al. Crizotinibversus chemotherapy in advanced ALK-positive lung cancer. N Engl J Med2013;368:2385–94.
50. Andersen JB, Spee B, Blechacz BR, Avital I, Komuta M, Barbour A, et al.Genomic and genetic characterization of cholangiocarcinoma identifiestherapeutic targets for tyrosine kinase inhibitors. Gastroenterology 2012;142:1021–31.
51. Borad MJ, Champion MD, Egan JB, Liang WS, Fonseca R, Bryce AH, et al.Integrated genomic characterization reveals novel, therapeutically relevantdrug targets in FGFR and EGFR pathways in sporadic intrahepatic cho-langiocarcinoma. PLoS Genet 2014;10:e1004135.
52. Chan-On W, Nairismagi ML, Ong CK, Lim WK, Dima S, Pairojkul C, et al.Exome sequencing identifies distinctmutational patterns in liver fluke-relatedand non-infection-related bile duct cancers. Nat Genet 2013;45:1474–8.
53. ChuriCR, Shroff R,WangY, RashidA, KangHC,Weatherly J, et al.Mutationprofiling in cholangiocarcinoma: prognostic and therapeutic implications.PLoS ONE 2014;9:e115383.
54. Jiao Y, Pawlik TM, Anders RA, Selaru FM, Streppel MM, Lucas DJ, et al.Exome sequencing identifies frequent inactivating mutations in BAP1,ARID1A and PBRM1 in intrahepatic cholangiocarcinomas. Nat Genet2013;45:1470–3.
55. Leone F, Cavalloni G, Pignochino Y, Sarotto I, Ferraris R, PiacibelloW, et al.Somatic mutations of epidermal growth factor receptor in bile duct andgallbladder carcinoma. Clin Cancer Res 2006;12:1680–5.
56. Ross JS, Wang K, Gay L, Al-Rohil R, Rand JV, Jones DM, et al. New routes totargeted therapy of intrahepatic cholangiocarcinomas revealed by next-generation sequencing. Oncologist 2014;19:235–42.
57. Sia D, Losic B, Moeini A, Cabellos L, Hao K, Revill K, et al. Massive parallelsequencing uncovers actionable FGFR2–PPHLN1 fusion and ARAF muta-tions in intrahepatic cholangiocarcinoma. Nat Commun 2015;6:6087.
58. SiaD,TovarV,MoeiniA, Llovet JM. Intrahepatic cholangiocarcinoma: patho-genesis and rationale for molecular therapies. Oncogene 2013;32:4861–70.
59. SimboloM, FassanM, Ruzzenente A,Mafficini A,Wood LD, Corbo V, et al.Multigene mutational profiling of cholangiocarcinomas identifies action-able molecular subgroups. Oncotarget 2014;5:2839–52.
60. Wang P, Dong Q, Zhang C, Kuan PF, Liu Y, Jeck WR, et al. Mutations inisocitrate dehydrogenase 1 and 2 occur frequently in intrahepatic cholan-giocarcinomas and share hypermethylation targets with glioblastomas.Oncogene 2013;32:3091–100.
61. Zou S, Li J, Zhou H, Frech C, Jiang X, Chu JS, et al. Mutational landscape ofintrahepatic cholangiocarcinoma. Nat Commun 2014;5:5696.
62. Fujimoto A, Furuta M, Shiraishi Y, Gotoh K, Kawakami Y, Arihiro K, et al.Whole-genome mutational landscape of liver cancers displaying biliaryphenotype reveals hepatitis impact andmolecular diversity. Nat Commun2015;6:6120.
63. Kim HJ, Yoo TW, Park DI, Park JH, Cho YK, Sohn CI, et al. Geneamplification and protein overexpression of HER-2/neu in human extra-hepatic cholangiocarcinoma as detected by chromogenic in situ hybrid-ization and immunohistochemistry: its prognostic implication in node-positive patients. Ann Oncol 2007;18:892–7.
64. Zhu AX, Borger DR, Kim Y, Cosgrove D, Ejaz A, Alexandrescu S, et al.Genomic profiling of intrahepatic cholangiocarcinoma: refining prog-nosis and identifying therapeutic targets. Ann Surg Oncol 2014;21:3827–34.
65. Ishimura N, Bronk SF, Gores GJ. Inducible nitric oxide synthase up-regulates Notch-1 in mouse cholangiocytes: implications for carcinogen-esis. Gastroenterology 2005;128:1354–68.
66. El KhatibM, Bozko P, Palagani V,MalekNP,Wilkens L, Plentz RR. Activationof Notch signaling is required for cholangiocarcinoma progression and isenhanced by inactivation of p53 in vivo. PLoS ONE 2013;8:e77433.
67. Zender S, Nickeleit I, Wuestefeld T, Sorensen I, Dauch D, Bozko P, et al. Acritical role for notch signaling in the formation of cholangiocellularcarcinomas. Cancer Cell 2013;23:784–95.
68. Huntzicker EG, Hotzel K, Choy L, Che L, Ross J, Pau G, et al. Differentialeffects of targeting Notch receptors in a mouse model of liver cancer.Hepatology 2015;61:942–52.
69. Boulter L, Guest RV, Kendall TJ, Wilson DH, Wojtacha D, Robson AJ, et al.WNT signaling drives cholangiocarcinoma growth and can be pharmaco-logically inhibited. J Clin Invest 2015;125:1269–85.
70. Goeppert B, Konermann C, Schmidt CR, Bogatyrova O, Geiselhart L,Ernst C, et al. Global alterations of DNA methylation in cholangio-carcinoma target the Wnt signaling pathway. Hepatology 2014;59:544–54.
71. Loilome W, Bungkanjana P, Techasen A, Namwat N, Yongvanit P, Pua-pairoj A, et al. Activatedmacrophages promoteWnt/beta-catenin signalingin cholangiocarcinoma cells. Tumour Biol 2014;35:5357–67.
72. Arai Y, Totoki Y, Hosoda F, Shirota T, Hama N, Nakamura H, et al.Fibroblast growth factor receptor 2 tyrosine kinase fusions define aunique molecular subtype of cholangiocarcinoma. Hepatology 2014;59:1427–34.
73. Wu YM, Su F, Kalyana-Sundaram S, Khazanov N, Ateeq B, Cao X, et al.Identification of targetable FGFR gene fusions in diverse cancers. CancerDiscov 2013;3:636–47.
74. Dienstmann R, Rodon J, Prat A, Perez-Garcia J, Adamo B, Felip E, et al.Genomic aberrations in the FGFR pathway: opportunities for targetedtherapies in solid tumors. Ann Oncol 2014;25:552–63.
75. Graham RP, Barr Fritcher EG, Pestova E, Schulz J, Sitailo LA, Vasmatzis G,et al. Fibroblast growth factor receptor 2 translocations in intrahepaticcholangiocarcinoma. Hum Pathol 2014;45:1630–8.
76. Tanizaki J, Ercan D, Capelletti M, Dodge M, Xu C, Bahcall M, et al.Identification of oncogenic and drug-sensitizing mutations in the extra-cellular domain of FGFR2. Cancer Res 2015;75:3139–46.
77. Gu TL, Deng X, Huang F, Tucker M, Crosby K, Rimkunas V, et al. Survey oftyrosine kinase signaling reveals ROS kinase fusions in human cholangio-carcinoma. PLoS ONE 2011;6:e15640.
78. Saborowski A, Saborowski M, Davare MA, Druker BJ, Klimstra DS, LoweSW. Mouse model of intrahepatic cholangiocarcinoma validates FIG-ROSas a potent fusion oncogene and therapeutic target. ProcNatl Acad SciU SA2013;110:19513–8.
79. Jinawath N, Chamgramol Y, Furukawa Y, Obama K, Tsunoda T, Sripa B,et al. Comparison of gene expression profiles between Opisthorchisviverrini and non-Opisthorchis viverrini associated human intrahepaticcholangiocarcinoma. Hepatology 2006;44:1025–38.
80. Ong CK, Subimerb C, Pairojkul C, Wongkham S, Cutcutache I, YuW, et al.Exome sequencing of liver fluke-associated cholangiocarcinoma. NatGenet 2012;44:690–3.
81. Eckel F, Schmid RM. Chemotherapy in advanced biliary tract carcinoma: apooled analysis of clinical trials. Br J Cancer 2007;96:896–902.
Clin Cancer Res; 22(2) January 15, 2016 Clinical Cancer Research300
Moeini et al.
on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296

2016;22:291-300. Published OnlineFirst September 24, 2015.Clin Cancer Res Agrin Moeini, Daniela Sia, Nabeel Bardeesy, et al. CholangiocarcinomaMolecular Pathogenesis and Targeted Therapies for Intrahepatic
Updated version
10.1158/1078-0432.CCR-14-3296doi:
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/22/2/291.full#ref-list-1
This article cites 81 articles, 15 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/22/2/291To request permission to re-use all or part of this article, use this link
on April 27, 2018. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 24, 2015; DOI: 10.1158/1078-0432.CCR-14-3296