Models for the organisation of palliative care for patients with cancer and dementia
14
Models for the organisation of palliative care for patients with cancer and dementia Professor Steve Iliffe, Nathan Davies, Dr Mareeni Raymond Dr Alex Warner & Laura Maio in Primary Care at UCL Professor Sam Ahmedzai , Department of Oncology, Sheffield University Professor Jill Manthorpe, Social Care Workforce Research Unit, Kings College London
description
Models for the organisation of palliative care for patients with cancer and dementia. Professor Steve Iliffe, Nathan Davies, Dr Mareeni Raymond Dr Alex Warner & Laura Maio in Primary Care at UCL Professor Sam Ahmedzai , Department of Oncology, Sheffield University - PowerPoint PPT Presentation
Transcript of Models for the organisation of palliative care for patients with cancer and dementia

Models for the organisation of palliative care for patients with cancer and dementia
Professor Steve Iliffe, Nathan Davies, Dr Mareeni RaymondDr Alex Warner & Laura Maio in Primary Care at UCL
Professor Sam Ahmedzai , Department of Oncology, Sheffield University
Professor Jill Manthorpe, Social Care Workforce Research Unit, Kings College London

Aim
To develop and test a tool to assess the quality of palliative care:• For cancer & dementia• In different health care systems• In different settings (home, care home,
hospital, hospice)

European centres
• Nijmegen, Holland• Bonn, Germany• Trondheim, Norway• Bologna, Italy• London, England

Methodology
Modelling palliative care for people with dementia or with cancer (nominal groups, Delphi processes)Developing quality indicator sets (technology development, co-design)Field testing QIs in primary care, care homes, hospitals and hospices (before and after study)

Technology development & co-design 2Rapid appraisal of the literature
Research team reaches consensus on key themes for qualitative interviews
Review of national policies in England, Germany, Italy, the Netherlands & Norway
List of questions developed and asked of subject
matter experts
Generic model discussed with subject matter expert
groups to refine and develop it further
Research team constructs generic model of palliative
care

Modelling• Detailed system description drawn up using subject matter
experts (SMEs)• In policy, service organisation, service delivery, patient
groups, & research in palliative care• Matrix of macro-, meso-,micro- level organisation• In four settings: own home, care home, hospitals, hospices• Interviews & focus groups with SMEs
Kotiadis K, Robinson S Conceptual modelling: knowledge acquisition and model abstraction in Mason S, Hill R, Moench L, Rose O, Jefferson T, Fowler J (eds) Proceedings of the 2008 Winter Simulation Conference 951-8 Kaulio, M. (1998) Customer, consumer and user involvement in product development: a framework and a review of selected methods, Total Quality Management and Business Excellence 9(1) pp. 141-49

Technology development & co-design 1
• Modified nominal group technique for ill-structured problems to synthesise findings :
• Allow for disagreements over problem definition, potential solutions that overlap or vary widely in specificity.
• Generate ideas, confirm they are addressing the same problem, analyse the content of the ideas, categorise ideas and clarify the items in each category
Bartunek JM & Murningham JK (1984) The nominal group technique: expanding the basic procedure and underlying assumptions Group & Organisation Studies 1984;9(3): 417-432

Core themes of palliative care
1. Division of labour2. Structure & function of care planning3. Managing rising risk and complexity4. Boundaries5. Process of bereavement

Grief, Loss and Bereavement from family, professionals and person with dementia
ComprehensiveDiagnosis and
Prognosis
Structured, iterative needs assessment & care planning, managing and monitoring
Options of treatment/self-care with shared decision making Death End-of-life care Rising support needs
Professionals
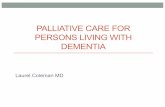
Basic model for dementia

Grief, Loss and Bereavement from family, professionals and person with dementia
ComprehensiveDiagnosis and
Prognosis
Structured, iterative needs assessment & care planning, managing and monitoring
Options of treatment/self-care with shared decision making Death End-of-life care Rising support needs
Professionals
Quality indicators of good end-of-life care and of “a good death” related to outcome
UK example: Liverpool Care Pathway
Fidelity to prior and current preferences, symptoms controlled,
family satisfaction, appropriate setting (home or hospital),
psychosocial and spiritual needs met
Prior/current preferences established with carer or family involvement.

Grief, Loss and Bereavement from family, professionals and person with dementia
ComprehensiveDiagnosis and
Prognosis
Structured, iterative needs assessment & care planning, managing and monitoring
Options of treatment/self-care with shared decision making Death End-of-life care Rising support needs
Professionals
Quality indicators of good palliative care related to process & structure
Evidence of increased skill
Evidence of care coordinationCommunity orientation
UK example: Gold Standard Framework in operation; pain control: use of assessment tools, psycho-social needs met; nutrition assessed, few PEG/NG tubes
used; Infection management agreed; Prognostication tools used
Training and continuous learning; audit of outcomes
Stable leadership & workforce, staff skill mix

Full descriptionIliffe S, Davies N, Vernooij-Dassen M, van Riet Paap J, Sommerbakk R, Mariani E, Jaspers B, Radbruch L, Manthorpe J, Maio L, Engels Y for the IMPACT research team
Modelling the landscape of palliative care for people with dementia: a European mixed methods study Submitted to BMC Palliative Care April 2013

Field testing
• Modified Delphi process with SMEs to choose a QI package
• Use QIs to identify strengths and weaknesses in volunteer services
• Focus on correcting weaknesses• Re-assess using QIs

Before & after study
In each country we are engaging with:• Hospital wards• Hospices• Care Homes• Community services (General practitioners) to test QI packages