Mo1117 Intestinal Spirochetosis: an Enigmatic Disease
2
T regulatory: Th17 response contributes to recurrent CDI. Methods: Patients were identified as initial (never having CDI) or recurrent (having at least one documented CDI within 2 weeks-1 year after standard antibiotic treatment). Healthy controls and case controls (patients in hospital with similar comorbidities to CDI patients) were also examined. PBMC were isolated from heparinized blood using ficoll hypaque and divided into 2 groups. Both groups were placed in culture for 4 hours; one stimulated with PMA/ionomycin and the second was cultured in media alone. The detection of sufficient IL-17 and γIFN is dependent on PMA stimulation. After 4 hours both populations were collected and stained for CD8/CD3 and either Foxp3 (Treg), IL-17(Th17) or γIFN (Th1) and analyzed using flow cytometry. Gated lymphocytes were then gated on CD3+ cells. The CD4 cells surface antigen significantly diminishes/disappears after PMA stimulation; therefore the CD3+ CD8- population repres- ented the CD4+ CD3+ lymphocyte population. Patient samples were obtained only after IRB approved informed consent was signed. Results: Healthy and case controls have significantly greater numbers of CD3+ and fewer CD3- lymphocytes in their PBMC (Table 1), more of which were CD4+CD3+ cells. However, a greater number of CD4+CD3+ cells, as well as CD8+ CD3+ are Fox p3 in the CDI patients (both initial and recurrent). All patients have more IL-17+CD4+CD3+ cells than healthy controls. The recurrent patients trend to a larger % of CD4+CD3+ cells which are IL-17+. Interestingly, there is no difference in the γIFN+CD4+CD3+ population, but the γIFN +CD8+CD3+. The recurrent patients have the fewest γIFN +CD8+CD3+ cells. Conclusion: All CDI patients have fewer CD4CD3+ cells in their PBMC but significantly more CD4 cells co-express Foxp3. Healthy controls have the least CD4+ IL-17+ PBMC. At this time there are no significant differences between the Foxp3 and IL-17 PBMC percentages in initial and recurrent CDI patients. However, we believe that the trend, a greater % of CD4 IL-17+in the recurrent PBMC, may become significant as we accrue at least 20 patients, as well some of the initial patients may recur. From current data it appears that the recurrent population has both a larger CD4 Fox3 and CD4 IL17 population. T cell populations present in the PBMC from Healthy (H) and Case controls (CC) and Initial (I) and Recurrent (Rec) patients Mo1115 Quantifying the Incidence and Burden of Post-Infectious Enteric Sequelae and Well Established Deployment Related Health Outcomes Chad K. Porter, Wendy Munera, Nadia Thura, Mark S. Riddle Background. Military populations encounter unique exposures during deployment. Increased understanding of the effects of these exposures is fueling research to define the risk and the burden of several outcomes with significant health impacts. Specifically, post-traumatic stress disorder (PTSD) and mild traumatic brain injury (mTBI) adversely affect long term quality of life. Furthermore, travelers' diarrhea (TD) has gained increased awareness given its associ- ation with several conditions including irritable bowel syndrome (IBS), Guillain-Barré syn- drome (GBS), reactive arthritis (ReA) and inflammatory bowel disease (IBD). Given the high incidence of TD among deployed troops, studies are needed to quantify the burden of post-infectious (PI) sequelae in the context of well-established deployment-related health S-599 AGA Abstracts outcomes. Methods. We conducted a systematic review of the incidence of deployment- related health outcomes. We limited our review of mTBI and PTSD to military populations while including all studies of PI sequelae incidence following infectious diarrhea. Using median estimates of deployment-related incidence and published disability weights, we quantified disease burden for each outcome utilizing Disability-Adjusted Life years (DALYs) assuming one year duration for and an average age at onset of 29 years. Results. We identified a total of 7,847 studies of which 263 met inclusion criteria. The incidence of outcomes varied across publication year, study design and data source. Similarly variability was observed in disability weight estimates for each outcome. The incidence of deployment-related PI IBS and PTSD was higher than for other outcomes (16,243 and 2,440 per 100,000, respectively). Disability weights for PTSD were also high (0.42) as were estimates for GBS (0.39) and IBD (0.25). DALY estimates showed that while PTSD results in the highest overall disability (1,000 per 100,000), the impact of PI sequelae is similarly elevated with the greatest burden associated with IBS at 627 per 100,000 followed by ReA (139), IBD (10), and GBS (3). Conclusion. Our findings help place post-infectious enteric sequelae and their effect into the context of well-established deployment-related health outcomes. Given the impact infectious diarrhea has on troop readiness, and the association with long-term sequelae, the need for improved prevention strategies is evident. Follow up studies of deployed military populations with pathogen-specific infectious gastroenteritis will enable better estimates of PI sequelae risk. Additionally, detailed studies of patients with PI sequelae would afford an opportunity to better quantitate disease morbidity and related health care costs. Such studies will increase our understanding of the impact acute infections have on service member health and would serve as valuable guidance to policy and decision makers. Mo1116 The Efficacy and Safety of Rifaximin vs. Vancomycin in the Treatment of Mild to Moderate C. difficile Infection: A Randomized Double-Blind Active Comparator Trial Darrell S. Pardi, Robert Brennan, Mitchell Spinnell, Marcelo G. Gareca, Eugene Greenberg, Wei Tian, Enoch Bortey, William P. Forbes, Herbert L. DuPont Background: Clostridium difficile infection (CDI) is a frequent cause of infectious diarrhea and is one of the most common nosocomial infections causing a rise in morbidity and mortality. The use of antibiotics is associated with an increased risk for the development of CDI. Previously, studies have demonstrated the efficacy of rifaximin (RFX), a gut selective, non-systemic antibiotic, in the treatment of CDI. In addition, CDI and other enteric infections do not appear to increase with chronic long-term use of RFX in patients receiving RFX daily for the maintenance of remission from hepatic encephalopathy (HE). The efficacy and safety of RFX in the treatment of CDI was prospectively evaluated vs an active comparator, vancomycin (VA), in a randomized double blind trial. Methods: Patients with acute diarrhea, positive C. difficile stool toxin assay and at least one other sign of enteric infection (fever, nausea, loss of appetite, vomiting, severe abdominal pain or discomfort) within 48 hours of screening, were randomized to receive 10-days of either RFX 400 mg TID or VA 125 mg QID. Symptoms of abdominal pain, fever, stool frequency and consistency, were collected daily for 14 days and patients were assessed for clinical success at 14 ±1 day for test for cure (TOC). Any diarrhea recurrence was monitored to 28 days post TOC. The primary endpoint was a comparison of clinical success of RFX vs. VA. Clinical Success was defined as the absence of severe abdominal pain and fever (< 38°C); and < 3 unformed stools/day for 2 consecutive days at TOC. Non-inferiority analysis was used to test clinical success of RFX vs VA (the lower bound of the one-sided 97.5% confidence interval [CI] of the treatment difference [RFX-VA] >-15%). Adverse events were monitored throughout the study. Results: The modified ITT population included 117 subjects treated with RFX vs 115 treated with VA. Demographics and baseline characteristics were comparable between groups; the majority of subjects (92.7%) had mild CDI and very few patients (5%) reported a fever at baseline. Clinical success with RFX (57%) was similar to VA (64%) treatment: treatment difference was -6.2% (CI: -18.8%, 6.4%), but did not attain the non inferiority margin. albeit the resolution of diarrhea was 80% for RFX and 81% for VA. For patients who achieved clinical success, the incidence of CDI recurrence was 9% in RFX and 14% in VA. Treatment emergent adverse events were reported in 64 (53%) of RFX vs 68 (59%) of VA patients. Conclusions: Resolution of diarrhea and the safety profile of rifaximin 400 mg TID is similar to vancomycin 125 mg QID in the treatment of patients with CDI. Mo1117 Intestinal Spirochetosis: an Enigmatic Disease Nicholas Anthony, James Blackwell, William Ahrens, Roger D. Lovell, Martin Scobey INTRODUCTION: Intestinal spirochetosis (IS) is a condition in which colonic and appendiceal epithelial cells are colonized by one of two anaerobic spirochetes, either the Brachyspira aalborgi or Brachyspira pilosicoli. Many patients present with diarrhea, abdominal pain, or rectal bleeding, but some do not manifest significant symptoms. This has led to debate of the implication of IS as a pathogen or a commensal inhabitant. A recent case of IS at our institution prompted a retrospective database search and review of the literature. To date, our study is the largest case series that includes both endoscopic and pathologic descriptions of IS. METHODS: A retrospective review of the endoscopic and pathology reports for IS were performed at our institution from 2003-2007. The following data was collected: age, gender, nationality, HIV status, and other co-morbid conditions. All pathology slides were pulled and reviewed by one pathologist to confirm the diagnosis of spirochetosis— Steiner stains were used when necessary. We also attempted to determine whether patients were treated for IS and if so, the treatment regimen used as well as the results. RESULTS: The database search detected 29 patients with biopsies showing IS. Three patients were subsequently removed due to incorrect identification. A total of 26 patients showed an average age of 45 years, a female to male predominance (58% to 42%), and mostly Caucasian ethnicity (81%). The most common symptoms were abdominal pain, diarrhea, and rectal bleeding. Most patients did not exhibit inflammatory changes despite the presence of IS. Five patients exhibited mild inflammation by pathology, but only one of those showed mild erythema during endoscopy. We were able to obtain follow-up of two patients after treatment with metronidazole and both responded to therapy. DISCUSSION: To date, our study is AGA Abstracts
Transcript of Mo1117 Intestinal Spirochetosis: an Enigmatic Disease

T regulatory: Th17 response contributes to recurrent CDI.Methods: Patients were identifiedas initial (never having CDI) or recurrent (having at least one documented CDI within 2weeks-1 year after standard antibiotic treatment). Healthy controls and case controls (patientsin hospital with similar comorbidities to CDI patients) were also examined. PBMC wereisolated from heparinized blood using ficoll hypaque and divided into 2 groups. Both groupswere placed in culture for 4 hours; one stimulated with PMA/ionomycin and the secondwas cultured in media alone. The detection of sufficient IL-17 and γIFN is dependent onPMA stimulation. After 4 hours both populations were collected and stained for CD8/CD3and either Foxp3 (Treg), IL-17(Th17) or γIFN (Th1) and analyzed using flow cytometry.Gated lymphocytes were then gated on CD3+ cells. The CD4 cells surface antigen significantlydiminishes/disappears after PMA stimulation; therefore the CD3+ CD8- population repres-ented the CD4+ CD3+ lymphocyte population. Patient samples were obtained only after IRBapproved informed consent was signed. Results: Healthy and case controls have significantlygreater numbers of CD3+ and fewer CD3- lymphocytes in their PBMC (Table 1), more ofwhich were CD4+CD3+ cells. However, a greater number of CD4+CD3+ cells, as well asCD8+ CD3+ are Fox p3 in the CDI patients (both initial and recurrent). All patients havemore IL-17+CD4+CD3+ cells than healthy controls. The recurrent patients trend to a larger% of CD4+CD3+ cells which are IL-17+. Interestingly, there is no difference in theγIFN+CD4+CD3+ population, but the γIFN +CD8+CD3+. The recurrent patients have thefewest γIFN +CD8+CD3+ cells. Conclusion: All CDI patients have fewer CD4CD3+ cellsin their PBMC but significantly more CD4 cells co-express Foxp3. Healthy controls havethe least CD4+ IL-17+ PBMC. At this time there are no significant differences between theFoxp3 and IL-17 PBMC percentages in initial and recurrent CDI patients. However, webelieve that the trend, a greater % of CD4 IL-17+in the recurrent PBMC, may becomesignificant as we accrue at least 20 patients, as well some of the initial patients may recur.From current data it appears that the recurrent population has both a larger CD4 Fox3 andCD4 IL17 population.T cell populations present in the PBMC from Healthy (H) and Case controls (CC) and Initial(I) and Recurrent (Rec) patients
Mo1115
Quantifying the Incidence and Burden of Post-Infectious Enteric Sequelae andWell Established Deployment Related Health OutcomesChad K. Porter, Wendy Munera, Nadia Thura, Mark S. Riddle
Background. Military populations encounter unique exposures during deployment. Increasedunderstanding of the effects of these exposures is fueling research to define the risk and theburden of several outcomes with significant health impacts. Specifically, post-traumatic stressdisorder (PTSD) and mild traumatic brain injury (mTBI) adversely affect long term qualityof life. Furthermore, travelers' diarrhea (TD) has gained increased awareness given its associ-ation with several conditions including irritable bowel syndrome (IBS), Guillain-Barré syn-drome (GBS), reactive arthritis (ReA) and inflammatory bowel disease (IBD). Given the highincidence of TD among deployed troops, studies are needed to quantify the burden ofpost-infectious (PI) sequelae in the context of well-established deployment-related health
S-599 AGA Abstracts
outcomes. Methods. We conducted a systematic review of the incidence of deployment-related health outcomes. We limited our review of mTBI and PTSD to military populationswhile including all studies of PI sequelae incidence following infectious diarrhea. Usingmedian estimates of deployment-related incidence and published disability weights, wequantified disease burden for each outcome utilizing Disability-Adjusted Life years (DALYs)assuming one year duration for and an average age at onset of 29 years. Results. We identifieda total of 7,847 studies of which 263 met inclusion criteria. The incidence of outcomesvaried across publication year, study design and data source. Similarly variability was observedin disability weight estimates for each outcome. The incidence of deployment-related PI IBSand PTSD was higher than for other outcomes (16,243 and 2,440 per 100,000, respectively).Disability weights for PTSD were also high (0.42) as were estimates for GBS (0.39) and IBD(0.25). DALY estimates showed that while PTSD results in the highest overall disability(1,000 per 100,000), the impact of PI sequelae is similarly elevated with the greatest burdenassociated with IBS at 627 per 100,000 followed by ReA (139), IBD (10), and GBS (3).Conclusion. Our findings help place post-infectious enteric sequelae and their effect into thecontext of well-established deployment-related health outcomes. Given the impact infectiousdiarrhea has on troop readiness, and the association with long-term sequelae, the need forimproved prevention strategies is evident. Follow up studies of deployed military populationswith pathogen-specific infectious gastroenteritis will enable better estimates of PI sequelaerisk. Additionally, detailed studies of patients with PI sequelae would afford an opportunityto better quantitate disease morbidity and related health care costs. Such studies will increaseour understanding of the impact acute infections have on service member health and wouldserve as valuable guidance to policy and decision makers.
Mo1116
The Efficacy and Safety of Rifaximin vs. Vancomycin in the Treatment of Mildto Moderate C. difficile Infection: A Randomized Double-Blind ActiveComparator TrialDarrell S. Pardi, Robert Brennan, Mitchell Spinnell, Marcelo G. Gareca, EugeneGreenberg, Wei Tian, Enoch Bortey, William P. Forbes, Herbert L. DuPont
Background: Clostridium difficile infection (CDI) is a frequent cause of infectious diarrheaand is one of the most common nosocomial infections causing a rise in morbidity andmortality. The use of antibiotics is associated with an increased risk for the development ofCDI. Previously, studies have demonstrated the efficacy of rifaximin (RFX), a gut selective,non-systemic antibiotic, in the treatment of CDI. In addition, CDI and other enteric infectionsdo not appear to increase with chronic long-term use of RFX in patients receiving RFX dailyfor the maintenance of remission from hepatic encephalopathy (HE). The efficacy and safetyof RFX in the treatment of CDI was prospectively evaluated vs an active comparator,vancomycin (VA), in a randomized double blind trial.Methods: Patients with acute diarrhea,positive C. difficile stool toxin assay and at least one other sign of enteric infection (fever,nausea, loss of appetite, vomiting, severe abdominal pain or discomfort) within 48 hoursof screening, were randomized to receive 10-days of either RFX 400 mg TID or VA 125mg QID. Symptoms of abdominal pain, fever, stool frequency and consistency, were collecteddaily for 14 days and patients were assessed for clinical success at 14 ±1 day for test forcure (TOC). Any diarrhea recurrence was monitored to 28 days post TOC. The primaryendpoint was a comparison of clinical success of RFX vs. VA. Clinical Success was definedas the absence of severe abdominal pain and fever (< 38°C); and < 3 unformed stools/dayfor 2 consecutive days at TOC. Non-inferiority analysis was used to test clinical success ofRFX vs VA (the lower bound of the one-sided 97.5% confidence interval [CI] of the treatmentdifference [RFX-VA] >-15%). Adverse events were monitored throughout the study. Results:The modified ITT population included 117 subjects treated with RFX vs 115 treated withVA. Demographics and baseline characteristics were comparable between groups; the majorityof subjects (92.7%) had mild CDI and very few patients (5%) reported a fever at baseline.Clinical success with RFX (57%) was similar to VA (64%) treatment: treatment differencewas -6.2% (CI: -18.8%, 6.4%), but did not attain the non inferiority margin. albeit theresolution of diarrhea was 80% for RFX and 81% for VA. For patients who achieved clinicalsuccess, the incidence of CDI recurrence was 9% in RFX and 14% in VA. Treatment emergentadverse events were reported in 64 (53%) of RFX vs 68 (59%) of VA patients. Conclusions:Resolution of diarrhea and the safety profile of rifaximin 400 mg TID is similar to vancomycin125 mg QID in the treatment of patients with CDI.
Mo1117
Intestinal Spirochetosis: an Enigmatic DiseaseNicholas Anthony, James Blackwell, William Ahrens, Roger D. Lovell, Martin Scobey
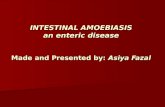
INTRODUCTION: Intestinal spirochetosis (IS) is a condition in which colonic andappendiceal epithelial cells are colonized by one of two anaerobic spirochetes, either theBrachyspira aalborgi or Brachyspira pilosicoli. Many patients present with diarrhea, abdominalpain, or rectal bleeding, but some do not manifest significant symptoms. This has led todebate of the implication of IS as a pathogen or a commensal inhabitant. A recent case ofIS at our institution prompted a retrospective database search and review of the literature.To date, our study is the largest case series that includes both endoscopic and pathologicdescriptions of IS. METHODS: A retrospective review of the endoscopic and pathologyreports for IS were performed at our institution from 2003-2007. The following data wascollected: age, gender, nationality, HIV status, and other co-morbid conditions. All pathologyslides were pulled and reviewed by one pathologist to confirm the diagnosis of spirochetosis—Steiner stains were used when necessary. We also attempted to determine whether patientswere treated for IS and if so, the treatment regimen used as well as the results. RESULTS:The database search detected 29 patients with biopsies showing IS. Three patients weresubsequently removed due to incorrect identification. A total of 26 patients showed anaverage age of 45 years, a female to male predominance (58% to 42%), and mostly Caucasianethnicity (81%). The most common symptoms were abdominal pain, diarrhea, and rectalbleeding. Most patients did not exhibit inflammatory changes despite the presence of IS.Five patients exhibited mild inflammation by pathology, but only one of those showed milderythema during endoscopy. We were able to obtain follow-up of two patients after treatmentwith metronidazole and both responded to therapy. DISCUSSION: To date, our study is
AG
AA
bst
ract
s
AG
AA
bst
ract
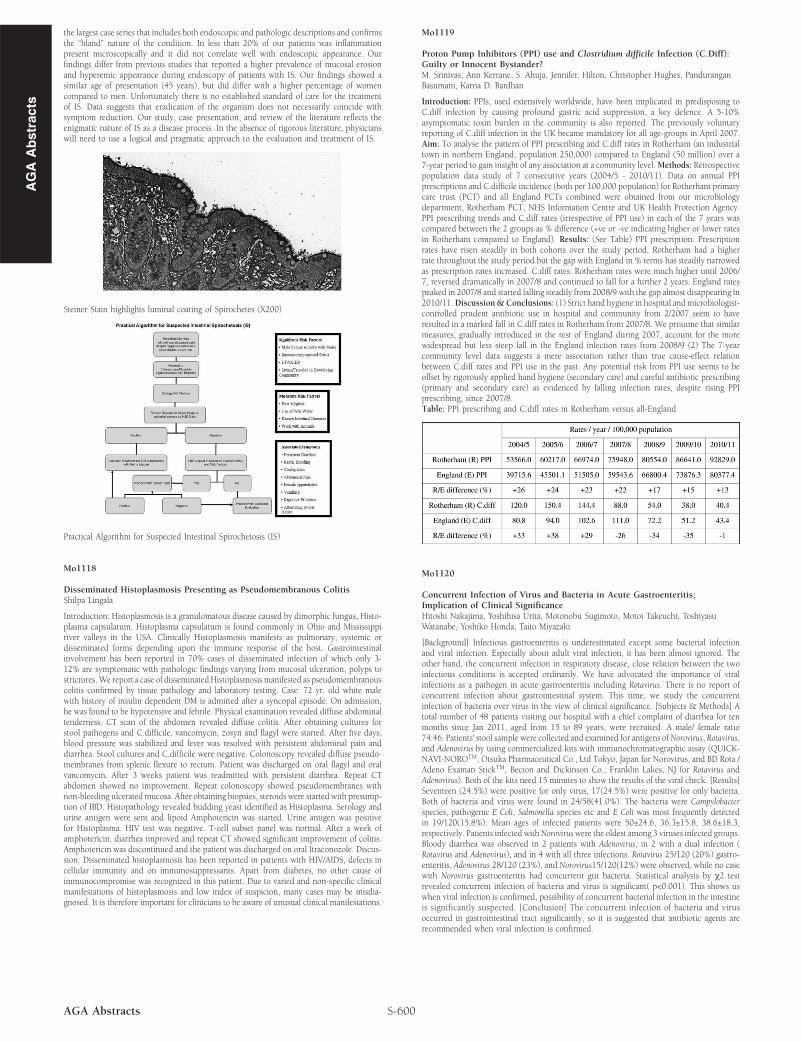
sthe largest case series that includes both endoscopic and pathologic descriptions and confirmsthe “bland” nature of the condition. In less than 20% of our patients was inflammationpresent microscopically and it did not correlate well with endoscopic appearance. Ourfindings differ from previous studies that reported a higher prevalence of mucosal erosionand hyperemic appearance during endoscopy of patients with IS. Our findings showed asimilar age of presentation (45 years), but did differ with a higher percentage of womencompared to men. Unfortunately there is no established standard of care for the treatmentof IS. Data suggests that eradication of the organism does not necessarily coincide withsymptom reduction. Our study, case presentation, and review of the literature reflects theenigmatic nature of IS as a disease process. In the absence of rigorous literature, physicianswill need to use a logical and pragmatic approach to the evaluation and treatment of IS.
Steiner Stain highlights luminal coating of Spirochetes (X200)
Practical Algorithm for Suspected Intestinal Spirochetosis (IS)
Mo1118
Disseminated Histoplasmosis Presenting as Pseudomembranous ColitisShilpa Lingala
Introduction: Histoplasmosis is a granulomatous disease caused by dimorphic fungus, Histo-plasma capsulatum. Histoplasma capsulatum is found commonly in Ohio and Mississippiriver valleys in the USA. Clinically Histoplasmosis manifests as pulmonary, systemic ordisseminated forms depending upon the immune response of the host. Gastrointestinalinvolvement has been reported in 70% cases of disseminated infection of which only 3-12% are symptomatic with pathologic findings varying from mucosal ulceration, polyps tostrictures.We report a case of disseminatedHistoplasmosismanifested as pseudomembranouscolitis confirmed by tissue pathology and laboratory testing. Case: 72 yr. old white malewith history of insulin dependent DM is admitted after a syncopal episode. On admission,he was found to be hypotensive and febrile. Physical examination revealed diffuse abdominaltenderness. CT scan of the abdomen revealed diffuse colitis. After obtaining cultures forstool pathogens and C.difficile, vancomycin, zosyn and flagyl were started. After five days,blood pressure was stabilized and fever was resolved with persistent abdominal pain anddiarrhea. Stool cultures and C.difficile were negative. Colonoscopy revealed diffuse pseudo-membranes from splenic flexure to rectum. Patient was discharged on oral flagyl and oralvancomycin. After 3 weeks patient was readmitted with persistent diarrhea. Repeat CTabdomen showed no improvement. Repeat colonoscopy showed pseudomembranes withnon-bleeding ulceratedmucosa. After obtaining biopsies, steroids were started with presump-tion of IBD. Histopathology revealed budding yeast identified as Histoplasma. Serology andurine antigen were sent and lipoid Amphotericin was started. Urine antigen was positivefor Histoplasma. HIV test was negative. T-cell subset panel was normal. After a week ofamphotericin, diarrhea improved and repeat CT showed significant improvement of colitis.Amphotericin was discontinued and the patient was discharged on oral Itraconozole. Discus-sion: Disseminated histoplasmosis has been reported in patients with HIV/AIDS, defects incellular immunity and on immunosuppressants. Apart from diabetes, no other cause ofimmunocompromise was recognized in this patient. Due to varied and non-specific clinicalmanifestations of histoplasmosis and low index of suspicion, many cases may be misdia-gnosed. It is therefore important for clinicians to be aware of unusual clinical manifestations.
S-600AGA Abstracts
Mo1119
Proton Pump Inhibitors (PPI) use and Clostridium difficile Infection (C.Diff):Guilty or Innocent Bystander?M. Srinivas, Ann Kerrane, S. Ahuja, Jennifer. Hilton, Christopher Hughes, PanduranganBasumani, Karna D. Bardhan
Introduction: PPIs, used extensively worldwide, have been implicated in predisposing toC.diff infection by causing profound gastric acid suppression, a key defence. A 5-10%asymptomatic toxin burden in the community is also reported. The previously voluntaryreporting of C.diff infection in the UK became mandatory for all age-groups in April 2007.Aim: To analyse the pattern of PPI prescribing and C.diff rates in Rotherham (an industrialtown in northern England; population 250,000) compared to England (50 million) over a7-year period to gain insight of any association at a community level.Methods: Retrospectivepopulation data study of 7 consecutive years (2004/5 - 2010/11). Data on annual PPIprescriptions and C.difficile incidence (both per 100,000 population) for Rotherham primarycare trust (PCT) and all England PCTs combined were obtained from our microbiologydepartment, Rotherham PCT, NHS Information Centre and UK Health Protection Agency.PPI prescribing trends and C.diff rates (irrespective of PPI use) in each of the 7 years wascompared between the 2 groups as % difference (+ve or -ve indicating higher or lower ratesin Rotherham compared to England). Results: (See Table) PPI prescription: Prescriptionrates have risen steadily in both cohorts over the study period. Rotherham had a higherrate throughout the study period but the gap with England in % terms has steadily narrowedas prescription rates increased. C.diff rates: Rotherham rates were much higher until 2006/7, reversed dramatically in 2007/8 and continued to fall for a further 2 years. England ratespeaked in 2007/8 and started falling steadily from 2008/9 with the gap almost disappearing in2010/11.Discussion&Conclusions: (1) Strict hand hygiene in hospital and microbiologist-controlled prudent antibiotic use in hospital and community from 2/2007 seem to haveresulted in a marked fall in C.diff rates in Rotherham from 2007/8. We presume that similarmeasures, gradually introduced in the rest of England during 2007, account for the morewidespread but less steep fall in the England infection rates from 2008/9 (2) The 7-yearcommunity level data suggests a mere association rather than true cause-effect relationbetween C.diff rates and PPI use in the past. Any potential risk from PPI use seems to beoffset by rigorously applied hand hygiene (secondary care) and careful antibiotic prescribing(primary and secondary care) as evidenced by falling infection rates, despite rising PPIprescribing, since 2007/8.Table: PPI prescribing and C.diff rates in Rotherham versus all-England
Mo1120
Concurrent Infection of Virus and Bacteria in Acute Gastroenteritis;Implication of Clinical SignificanceHitoshi Nakajima, Yoshihisa Urita, Motonobu Sugimoto, Motoi Takeuchi, ToshiyasuWatanabe, Yoshiko Honda, Taito Miyazaki
[Background] Infectious gastroenteritis is underestimated except some bacterial infectionand viral infection. Especially about adult viral infection, it has been almost ignored. Theother hand, the concurrent infection in respiratory disease, close relation between the twoinfectious conditions is accepted ordinarily. We have advocated the importance of viralinfections as a pathogen in acute gastroenteritis including Rotavirus. There is no report ofconcurrent infection about gastrointestinal system. This time, we study the concurrentinfection of bacteria over virus in the view of clinical significance. [Subjects & Methods] Atotal number of 48 patients visiting our hospital with a chief complaint of diarrhea for tenmonths since Jan 2011, aged from 15 to 89 years, were recruited. A male/ female ratio74:46. Patients' stool sample were collected and examined for antigens ofNorovirus, Rotavirus,and Adenovirus by using commercialized kits with immunochromatographic assay (QUICK-NAVI-NOROTM, Otsuka Pharmaceutical Co., Ltd Tokyo, Japan for Norovirus, and BD Rota /Adeno Examan StickTM, Becton and Dickinson Co., Franklin Lakes, NJ for Rotavirus andAdenovirus). Both of the kits need 15 minutes to show the results of the viral check. [Results]Seventeen (24.5%) were positive for only virus, 17(24.5%) were positive for only bacteria.Both of bacteria and virus were found in 24/58(41.0%). The bacteria were Campylobacterspecies, pathogenic E Coli, Salmonella species etc and E Coli was most frequently detectedin 19/120(15.8%). Mean ages of infected patients were 50±24.6, 36.3±15.8, 38.6±18.3,respectively. Patients infected withNoroviruswere the oldest among 3 viruses infected groups.Bloody diarrhea was observed in 2 patients with Adenovirus, in 2 with a dual infection (Rotavirus and Adenovirus), and in 4 with all three infections. Rotavirus 25/120 (20%) gastro-enteritis, Adenovirus 28/120 (23%), and Norovirus15/120(12%) were observed, while no casewith Norovirus gastroenteritis had concurrent gut bacteria. Statistical analysis by χ2 testrevealed concurrent infection of bacteria and virus is significant( p<0.001). This shows uswhen viral infection is confirmed, possibility of concurrent bacterial infection in the intestineis significantly suspected. [Conclusion] The concurrent infection of bacteria and virusoccurred in gastrointestinal tract significantly, so it is suggested that antibiotic agents arerecommended when viral infection is confirmed.