MLAB 1227: Coagulation Keri Brophy-Martinez
16
Coagulation Disorders: Secondary Hemostasis Part One MLAB 1227: Coagulation Keri Brophy-Martinez
description
MLAB 1227: Coagulation Keri Brophy-Martinez. Coagulation Disorders: Secondary Hemostasis Part One. Disorders of the Proteins of Fibrin Formation. Fibrin formation ineffective and slowed so patient presents with abnormal bleeding Two categories Inheritance of a defective gene - PowerPoint PPT Presentation
Transcript of MLAB 1227: Coagulation Keri Brophy-Martinez

Coagulation Disorders: Secondary Hemostasis
Part One
MLAB 1227: CoagulationKeri Brophy-Martinez

Disorders of the Proteins of Fibrin FormationFibrin formation ineffective and slowed so
patient presents with abnormal bleedingTwo categories
Inheritance of a defective geneFailure of synthesis of a hemostatic
protein Malfunction or impaired molecule
Acquired Acquisition of a deficiency secondary
to another condition

TermsQuantitative: amount of a coagulation
proteinQualitative: Present in plasma but
functionally defective
General Lab Features Lab
PT prolongedaPTT prolongedPlatelet count normal
Clinical FindingsCoagulation Factor Disorders Platelet DisordersBleed from
ruptured arteriolesDeep muscular &
joint bleedingDelayed bleedingEcchymosesHematuriaNo petechiae
Bleed from capillaries
Superficial bleeding
Acute bleedingEcchymosesHematuriaPetechiae
Hereditary Disorders of Secondary Hemostasis
Involve a single factorBleeding originates from one site

Factor VIII DeficiencyVon Willebrand's Disease – lack of or
defective VIII:vWFAutosomal dominant – seen in both
males and femalesMost common inherited blood disorderPlatelet abnormalities – adhesiveness
and aggregation, bleeding times

Von Willebrand's DiseaseClinical Features Lab FindingsMild bleeding in
mucosal & cutaneous tissues
Easy bruisingHallmark is
variability of symptoms
PTT normal or increased
PT normalPlatelet count
normalBT/ PFA abnormal

Factor VIII DeficiencyHemophilia A – classical hemophilia
Sex-linked recessive carried by female, manifested in the male Accounts for 80% of all hemophiliacs
Deficiency of factor VIII portion of VIII/vWf complex
Patient has normal circulating vWfAbnormal bleeding
Caused by delayed and inadequate fibrin formationCaused by a secondary increase in fibrinolysis
Failure of TAFI

Factor VIII TherapyReplace clotting factors to achieve
hemostasisDDAVP (desamino-D-vasopressin)
Stimulates storage cells to release VIII and vWF into plasma.
Disadvantage is not all patients can take it

Factor IX Deficiency – Hemophilia B, Christmas Disease
<20% of all hemophiliacsSex-linked recessiveNo Factor IX functionClinically indistinguishable from hemophilia
A, so we see the same disease course
Clinical Findings of Hemophilias
Bleeding occurs with NO trauma or trivial injury
HemarthrosisSpontaneous bleeding into joints, causes
extreme pain and destroys cartilage of knees, elbows, ankles
Deep tissue hemorrhage – internallyHematuriaCNS bleeding

Factor XI Deficiency – Rosenthal's Disease or Hemophilia C
<5% of all hemophiliacsAutosomal recessiveHighest incidence in Jewish persons of
Russian decentMucosal bleedingRequires therapy only following childbirth
or surgery
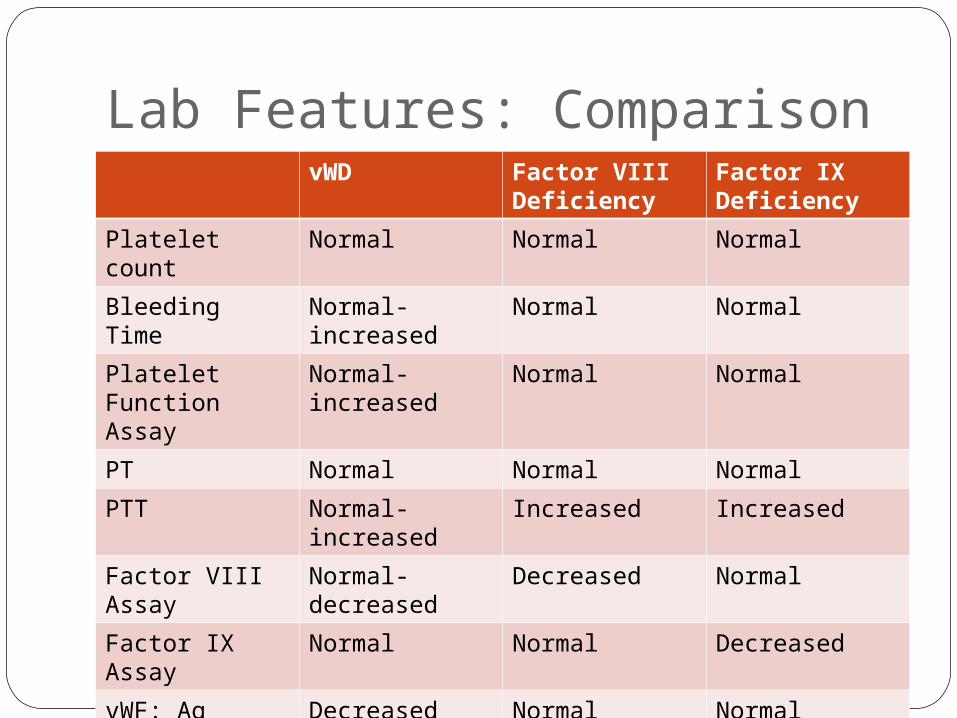
Lab Features: ComparisonvWD Factor VIII
DeficiencyFactor IX Deficiency
Platelet count Normal Normal NormalBleeding Time Normal-
increasedNormal Normal
Platelet Function Assay
Normal-increased
Normal Normal
PT Normal Normal NormalPTT Normal-
increasedIncreased Increased
Factor VIII Assay
Normal-decreased
Decreased Normal
Factor IX Assay Normal Normal DecreasedvWF: Ag Assay Decreased Normal Normal

Congenital Disorders of the Other Factors
The following factors are rarely deficient or defective to the extent that coagulation is slowed – I, II, V, VII, X, XII, XIII
Severity of bleeding dependent upon concentration of factor present
PK and HMWK disorders do exist but patients do not have bleeding tendencies.

References
McKenzie, Shirlyn B., and J. Lynne. Williams. "Chapter 32." Clinical Laboratory Hematology. Boston: Pearson, 2010. Print.