MitraClip - Fonds de dotation ACTIONRepair, Replacement, LVAD, Transplantation) Patient Selection...
71
MitraClip Alec Vahanian, Dominique Himbert ,Eric Brochet Bichat Hospital, Paris
Transcript of MitraClip - Fonds de dotation ACTIONRepair, Replacement, LVAD, Transplantation) Patient Selection...
MitraClip
Alec Vahanian, Dominique Himbert ,Eric Brochet
Bichat Hospital, Paris

General comments

Mitral Valve Apparatus
Subvalvular apparatus
Leaflets
Commissures
Papillary
muscles
Annulus
Complex interaction

2008-Hugo Vanermen 2008-Hugo Vanermen
Principles of a reconstructive valve operation
• Preserve or restore full leaflet motion
• Create a large surface of coaptation
• Remodel and stabilise the entire annulus
« The duty of any valvular surgeon today is no longer to
correct a mitral valve regurgitation, but to correct a mitral
valve regurgitation for the rest of the patient’s life »
A .Carpentier
Surgery in Mitral Regurgitation
In expert centres, in patients with primary MR, the repair
rate is >90% and >90% of patients are alive and free
from reoperation after 10-15 years.
Surgery for secondary MR remains a challenge. Most
studies failed to demonstrate improved long-term clinical
outcome following surgical correction.

Rationale for Percutaneous
Valve Interventions
VHD is frequent and carries a poor prognosis
Patients are often elderly with several comorbidities
Surgery is « the gold standard » but may be high-risk
or even contraindicated
In practice, many patients are denied surgery

The natural evolution of a surgical into a
percutaneous procedure
Open Video assisted Robotic Percutaneous
Sternotomy
Skin incisions
CPB
X X
X
Direct vision Video assisted Echo-guided


(Maisano. J Am Coll Cardiol 2011;58: 2174–82)

years
14121086420
Fre
edom
fro
m r
eopera
tion a
nd M
R3-4
+
1,0
,9
,8
,7
,6
,5
,4
,3
,2
,1
0,0
At 12.5 years: 39±7%
Pts at risk:
51 42 39 30 20 13 1
Edge-to-edge without annuloplasty
Freedom from reoperation and MR 3+ or more
(Courtesy O.Alfieri))

General comments
The MitraClip procedure

www.escardio.org/guidelines
Treatment of Valve
disease
SURGEONS CARDIOLOGISTS
Imaging specialists (Echo, CT, MRI)
Anesthesiologists
The « Heart Team »
Other
specialists:HF,EP,
Geriatricians……
www.escardio.org/guidelines
Essential questions in the evaluation of a patient for valvular intervention
● Is valvular heart disease severe?
● Does the patient have symptoms?
● Are symptoms related to valvular disease?
● What are patient life expectancy and expected quality of life?
● Do the expected benefits of intervention (versus spontaneous
outcome) outweigh its risks?
● What are the patient's wishes?
● Are local resources optimal for planned intervention?
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs109 &
European Journal of Cardio-Thoracic Surgery 2012 -
doi:10.1093/ejcts/ezs455).

PMVR Surgery (Repair, Replacement, LVAD,
Transplantation)
Patient Selection for Percutaneous
Valve Intervention
Medical Rx
« Futility > Utility » Because of cardiac and
extra cardiac factors
The « Heart Team »

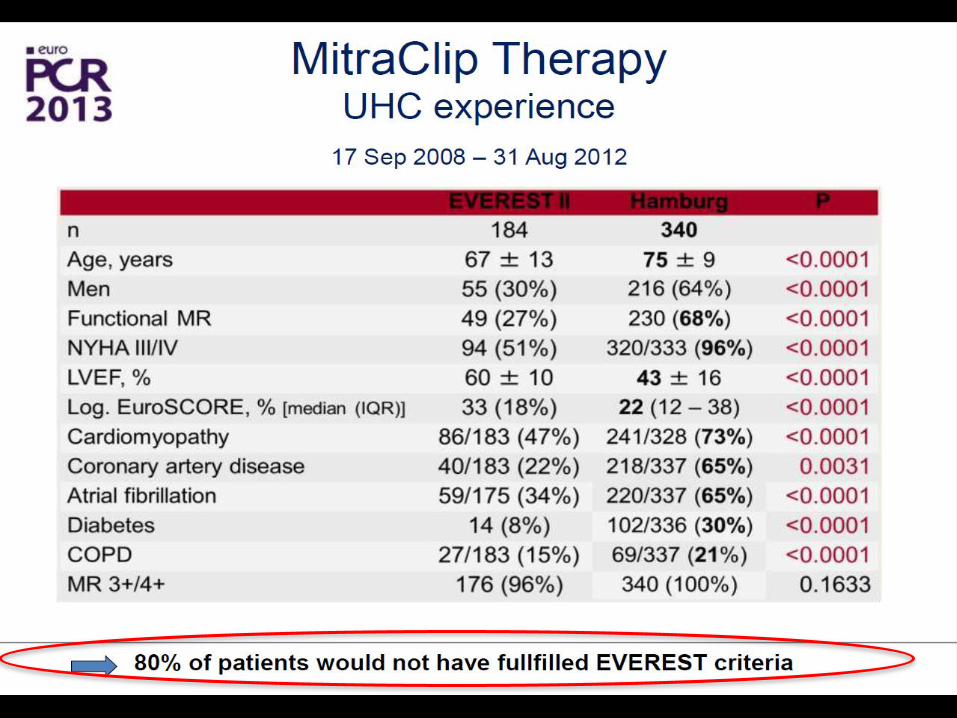
MitraClip Therapy
Selection of patients
TTE TEE 3D TEE
Comprehensive and systematic assessment
using multiple echo modalities - Quality of recordings
- Key echocardiographic views in each echo modality
- Optimal visualization of MR origin and valve pathology

Specific measurements
Flail gap Flail width
(Feldman T et al
JACC 2009;54:
686-94)
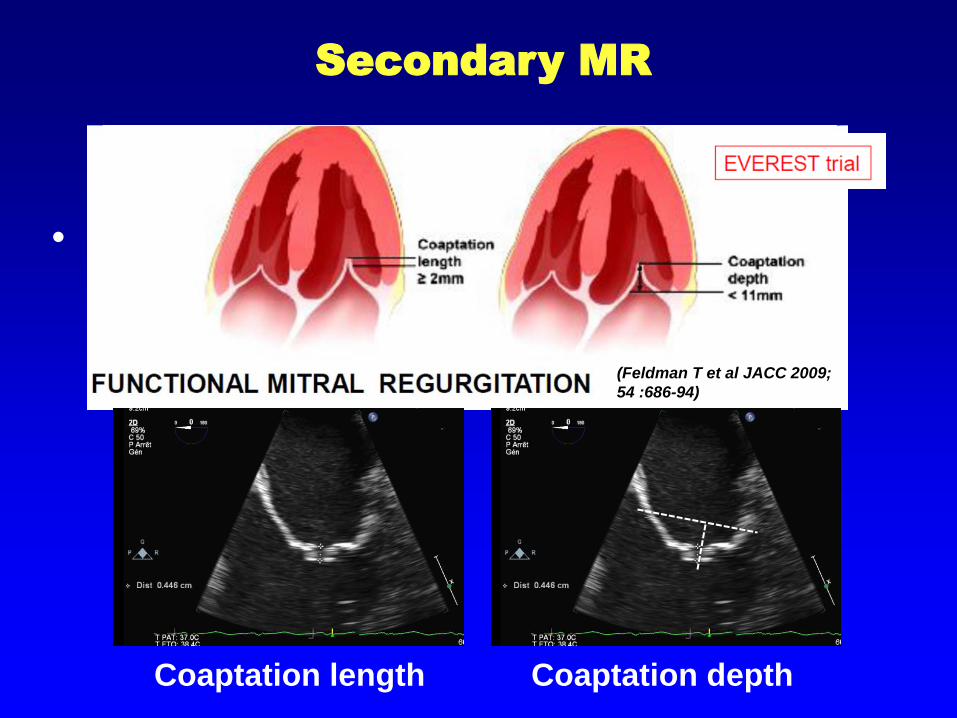
•
Secondary MR
(Feldman T et al JACC 2009;
54 :686-94)
Coaptation length Coaptation depth

(Boekstegers et al. Clin Res Cardiol (2014) 103:85–96)
Optimal Valve morphology
Central pathology in segment 2
No leaflet calcification
Mitral valve opening area >4cm2
Mobile length of the posterior leaflet ≥10mm
Coaption depth <11mm
Normal leaflet strength and mobility
Flail-width <15mm Flail-gap <10mm

(Boekstegers et al. Clin Res Cardiol (2014) 103:85–96)
Unsuitable valve morphology
Perforated mitral valve leaflet or cleft
Severe calcification in the grip-zone
Haemodynamically significant mitral stenosis (valve opening area
<3cm2, MPG ≥5mmHg)
Mobile length of the posterior leaflet <7mm
Rheumatic leaflet thickening and restriction in systole and diastole
(Carpentier IIIA)
Barlow’s syndrome with multisegment flail leaflets


TS Puncture for Mitraclip
S. Y. Ho et al. Eur J of Echocardiography (2011)
SUP (SVC)
INF (IVC)
ANT (Ao)
POST (PV)
HIGH (PV)
LOW (AV Valve plane)
2
Bicaval SAX
4ch
Spatial orientation

Short-axis view at the
base (for anterior -
posterior orientation)
Bicaval view (for inferior.superior orientation)
Midesophageal 4-
chamber view (for
assessing height
above the valve
plane).
Silvestry et al JASE 2007
TS Puncture for MitraClip

Introduction of the Steerable Guide
Catheter into the LA
(Wunderlich NC, Siegel R. Eur Heart J Cardiovasc Imaging 2013;14:935-949)

Advancement of the Clip Delivery
System into the LA
(Wunderlich NC, Siegel R. Eur Heart J Cardiovasc Imaging 2013;14:935-949)

Steering and positioning of the
MitraClip above the mitral valve
(Wunderlich NC, Siegel R. Eur Heart J Cardiovasc Imaging 2013;14:935-949)

Advancement of the MitraClip into
the Left ventricle
(Wunderlich NC, Siegel R. Eur Heart J Cardiovasc Imaging 2013;14:935-949)

Grasping of the leaflets
(Wunderlich NC, Siegel R. J Eur Heart J Cardiovasc Imaging 2013;14:935-949)

Assessment of results
(Wunderlich NC, Siegel R. Eur Heart J Cardiovasc Imaging 2013;14:935-949)

Advanced techniques for
Degenerative MR
Implantation of 2 or more clips
Grasping during asystole (Adenosine infusion)
Grasping during rapid pacing
Volume control (ventilation manoeuvres)
Use of two delivery systems

Importance of the learning Curve
The learning curve: Procedure time reduction: 180min to 55min
Acute procedural success from 80% to 92%
*

Optimising the Initial Results
(Lim DS. JACC 2014;64;182-92)

General comments
The MitraClip procedure
Results

(Feldman T, N Engl J Med 2011;364:1395 – 1406)
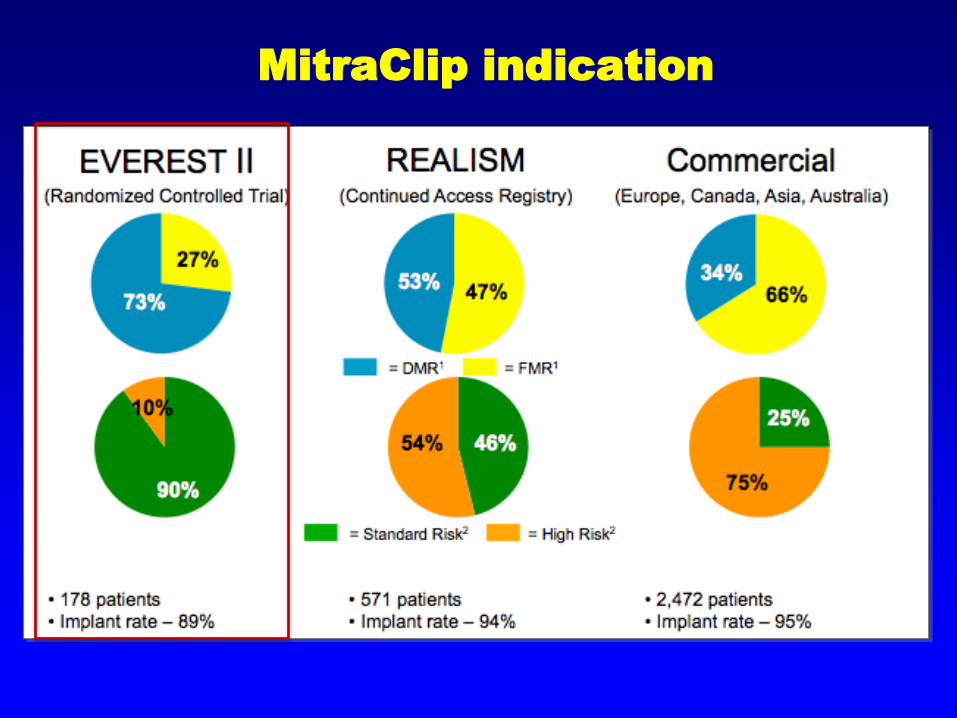
MitraClip indication

(Feldman T, N Engl J Med 2011;364:1395 – 1406)

(Feldman ACC 2014)
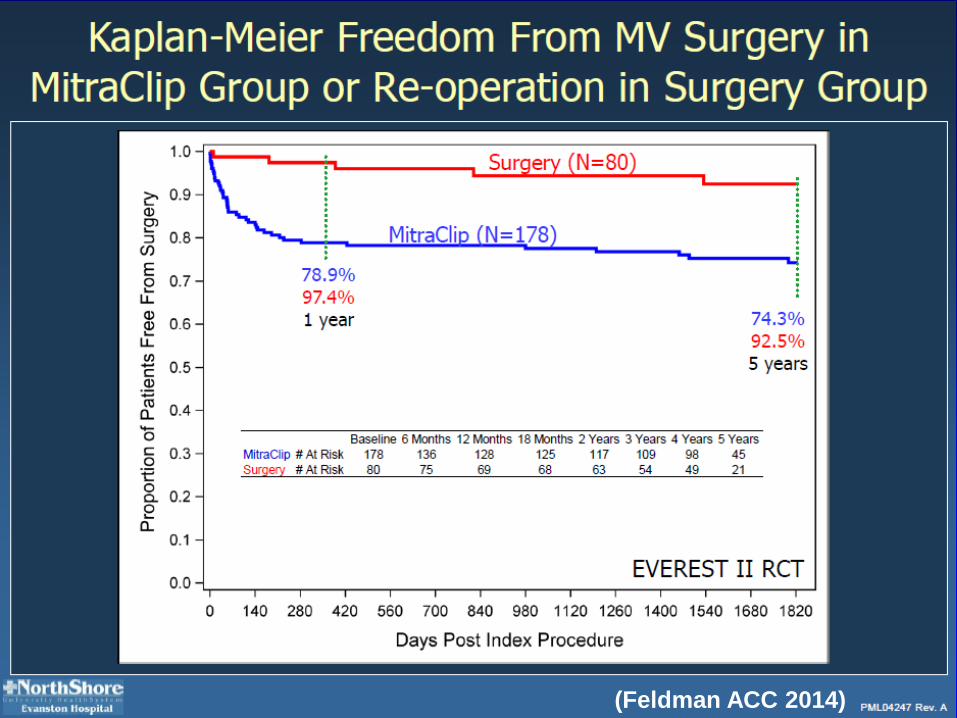
(Feldman ACC 2014)

(Feldman ACC 2014)

(Feldman ACC 2014)

Temporal Changes in MitraClip
indication
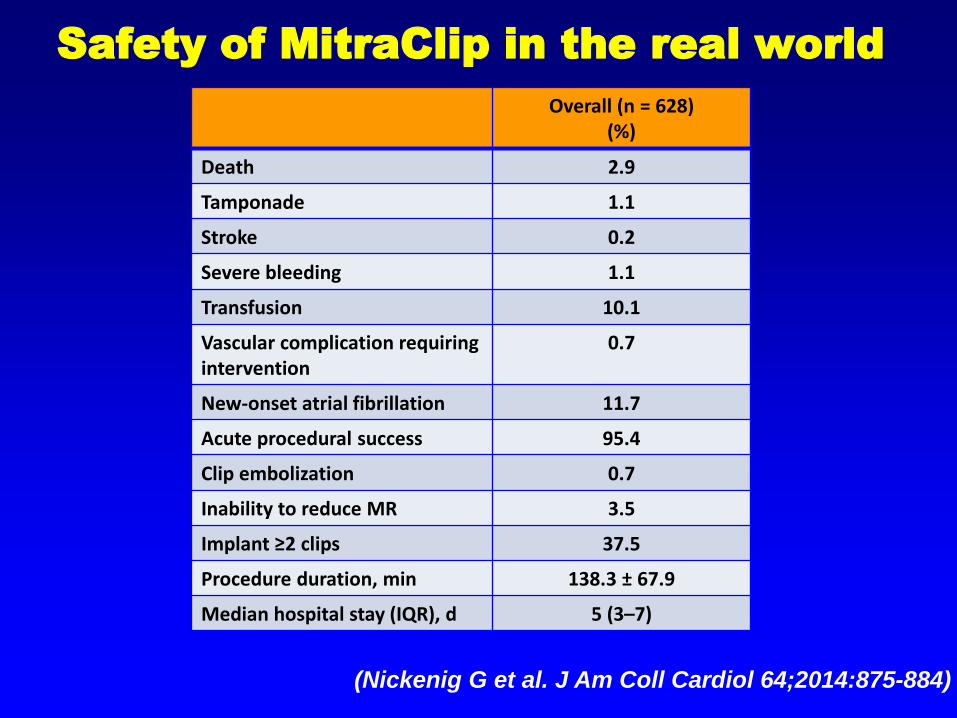
Safety of MitraClip in the real world
Overall (n = 628) (%)
Death 2.9
Tamponade 1.1
Stroke 0.2
Severe bleeding 1.1
Transfusion 10.1
Vascular complication requiring intervention
0.7
New-onset atrial fibrillation 11.7
Acute procedural success 95.4
Clip embolization 0.7
Inability to reduce MR 3.5
Implant ≥2 clips 37.5
Procedure duration, min 138.3 ± 67.9
Median hospital stay (IQR), d 5 (3–7)
(Nickenig G et al. J Am Coll Cardiol 64;2014:875-884)

(Nickenig G et al. J Am Coll Cardiol 64;2014:875-884)
MR Grade

(Nickenig G et al. J Am Coll Cardiol 64;2014:875-884)
NYHA Functional class
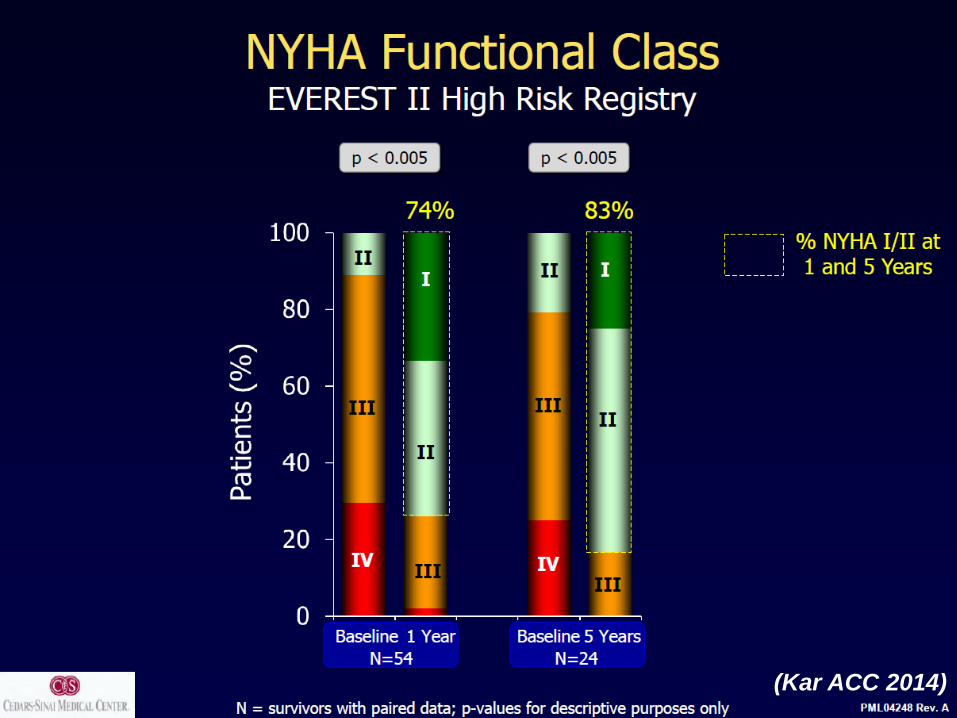
(Kar ACC 2014)

Propensity-matched analysis of survival
of MitraClip vs Controls
(IN-HF registry 32 centres from ANMCO database) Heart
failure patients with MR>3+
MitraClip treated patients
Medically treated patients
(Source: CERGAS Dr Tarricone)
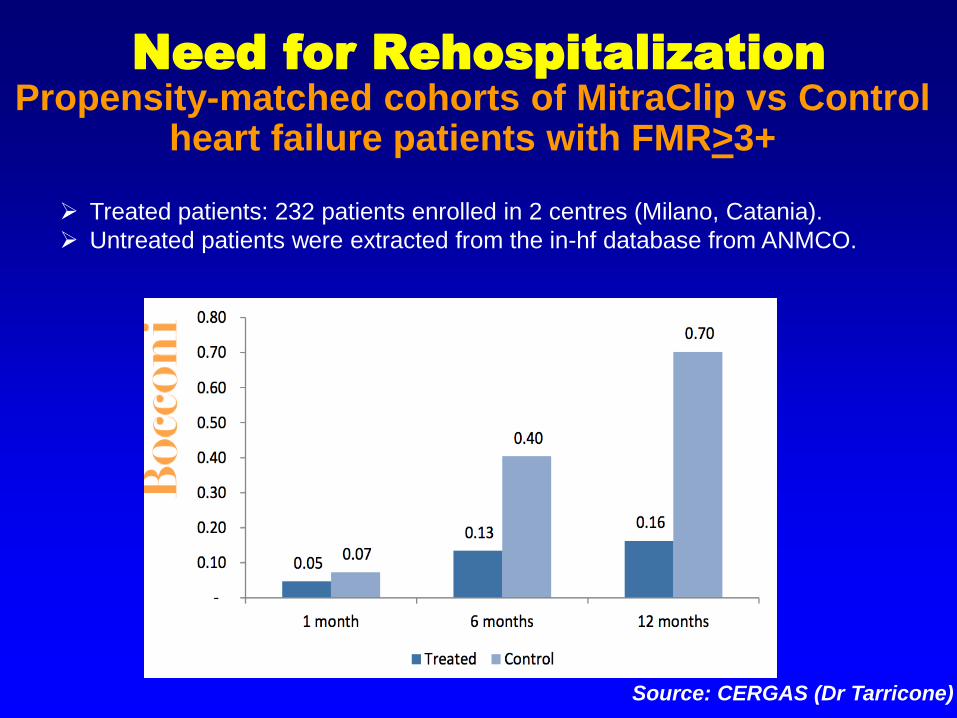
Need for Rehospitalization
Source: CERGAS (Dr Tarricone)
Treated patients: 232 patients enrolled in 2 centres (Milano, Catania).
Untreated patients were extracted from the in-hf database from ANMCO.
Propensity-matched cohorts of MitraClip vs Control heart failure patients with FMR>3+

Primary/secondary MR: Freedom from
heart failure rehospitalization
(Rudolph V et al. Eur J Heart Fail 2013;15:796-807)
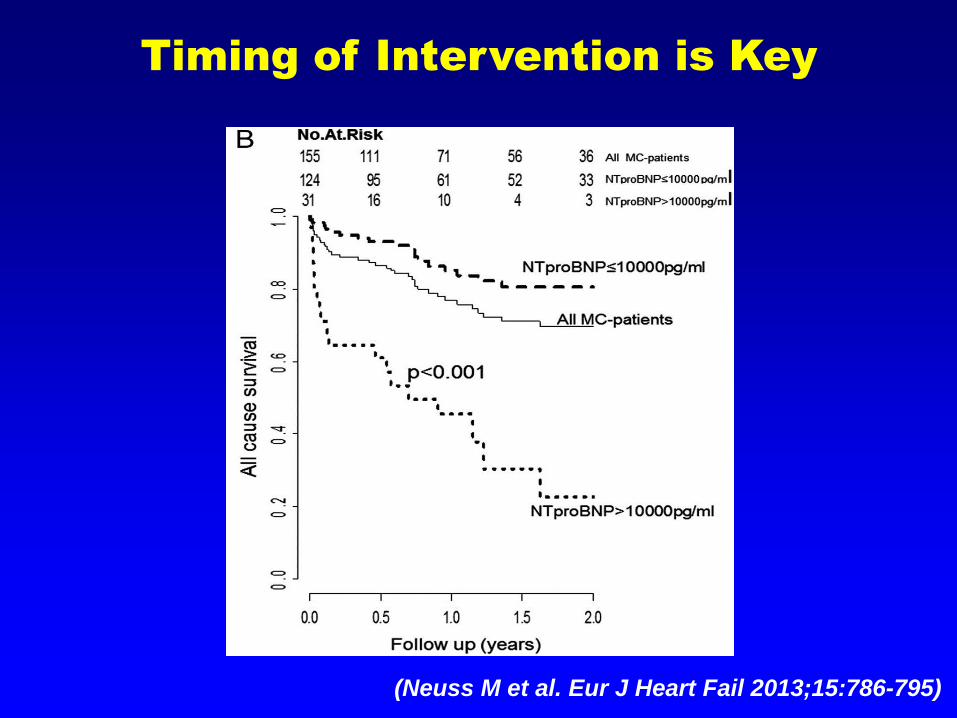
Timing of Intervention is Key
(Neuss M et al. Eur J Heart Fail 2013;15:786-795)
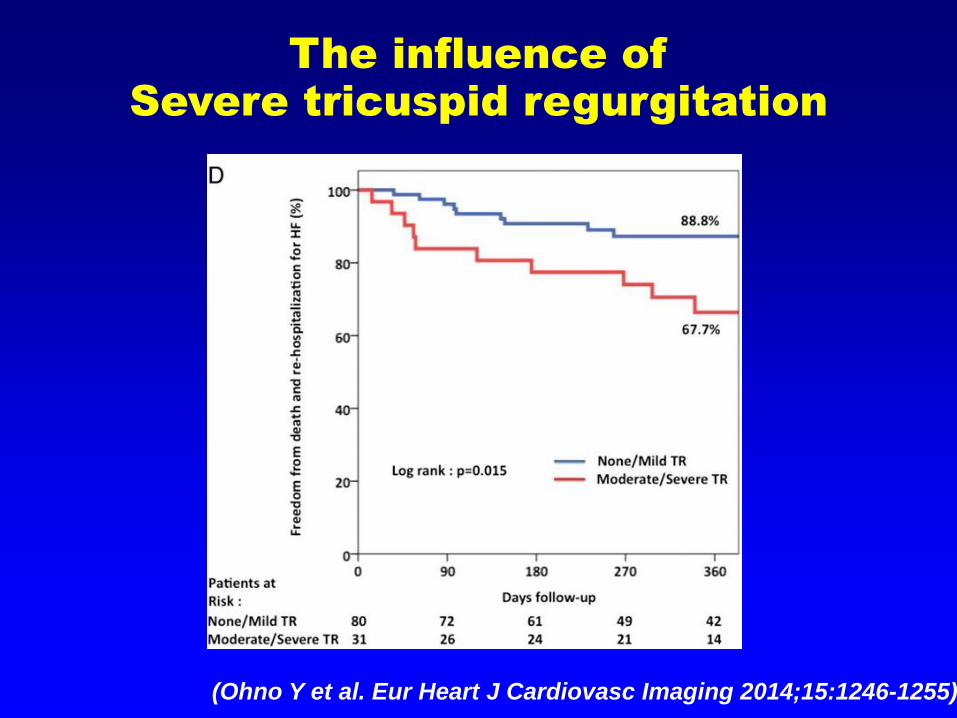
The influence of
Severe tricuspid regurgitation
(Ohno Y et al. Eur Heart J Cardiovasc Imaging 2014;15:1246-1255)
www.escardio.org/guidelines
ESC/ EACTS Guidelines for the
Management of Valvular Heart Disease
« The percutaneous MitraClip procedure may be considered in symptomatic patients with severe primary or secondary MR despite optimal medical therapy, who fulfil the echo criteria of eligibility, are judged inoperable or at high risk for surgery by a heart team, and who have a life expectancy greater than one year »
(Recommendation class IIb, level of Evidence C)
European Heart Journal 2012 - doi:10.1093/eurheartj/ehs109 &
European Journal of Cardio-Thoracic Surgery 2012 -
doi:10.1093/ejcts/ezs455).

ACC/AHA Recommendations for
chronic primary MR
Recommendations COR LOE
Transcatheter mitral valve repair may be considered for severely symptomatic patients with chronic severe primary MR who have a reasonable life expectancy but a prohibitive surgical risk because of severe comorbidities
IIb
B
(Nishimura et al. J Am Coll Cardiol 2014 In Press. DOI:
10.1016/j.jacc.2014.02.537)

Global experience > 20000 patients worlwide

General comments
The MitraClip procedure
Results
How to move forward

annuloplasty replacement

Cardioband Implant
(Maisano. JACC Cardiovasc Interv. 2014;7:1326 -1328)

Combination of
Techniques

Transcatheter Mitral Valve Implantation
EndoValve CardiAQ( n=3)
Neovasc – Tiara( n=3) Lutter Valve (n=2) Fortis (n=12)
Medtronic
HF patients with Severe MR and Low EF
Edge-to-Edge Medical therapy
Symptoms despite Optimal Medical Management
(including Revascularisation and/or CRT)
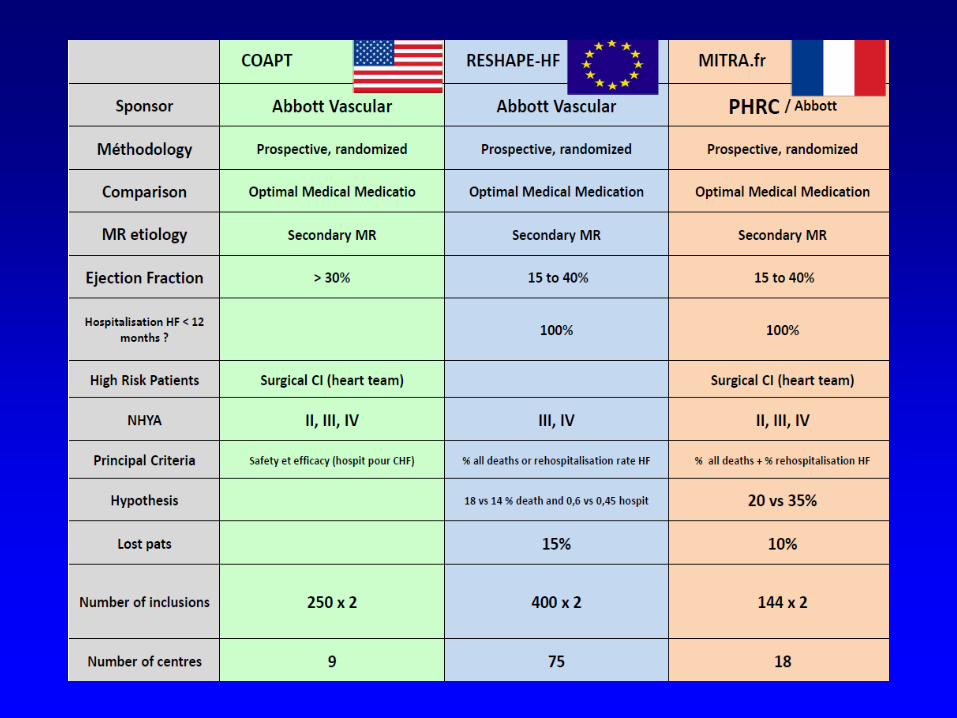
The Trials we need
COAPT, and Mitra-FR are ongoing .RESHAPE will
restart
> 300 Pts included
Mitral VARC will be published in 2015

HiRiDe
High Risk Degenerative Mitral
Regurgitation
Objective: To evaluate safety and efficacy of MitraClip® vs. surgery in
high-risk but operable patients with DMR
Elderly (>65yo) and with significant comorbidities
STS 3-10%
NYHA ≥ III
Study size: n=294
Follow up: up to 12 months
Endpoints:
Safety: Major Adverse Event Composite (MAE) including all-cause death,
prolonged ventilation (>48h), renal failure, stroke and need for non-elective
cardiovascular or thoracic surgery in order to show superiority of MitraClip to
surgery
Efficacy: In order to show non-inferiority to surgery, it will be a composite of
all-cause death, NYHA Functional Class and HF Hospitalization.

A dedicated “Heart Team” is key at all steps of the new transcatheter
procedures.
Pre-procedural evaluation relies on a comprehensive evaluation of cardiac
and extra-cardiac conditions combining clinical assessment, multimodality
imaging, and other investigations if needed.
The current results of the Edge-to-Edge technique, in > 19000 patients,
suggest that in selected high-risk patients:
- Safety is good
- “It gives life to years and may add years of life”
- The results are stable up to 5 years
In the future improvement may be expected from:
• Better evaluation including long-term follow-up and RCT to evaluate the
effect on mortality and refine the indications
• Combination of techniques
Conclusions

(Treede. J Thorac Cardiovasc Surg 2012;143:78-84)
The Future of the Treatment of
Mitral Regurgitation

STOP


• Comparison of MitraClip therapy vs optimal medical
management in patients with severe secondary mitral
regurgitation after 12 months:
• All-cause mortality
• Hopsitalisation for heart failure
Primary objective

• Death
All cause @ 30d, 6m,12m, 24m
Cardiovascular death @ 30d, 6m,12m, 24m
• Survival without major cardiovascular event @ 30d,
6m,12m, 24m
• Safety of MitraClip @30d, 6m,12m
• Medicoeconomic study @12m
• QOL, biomarkers, LV remodelling @ 6-12m
Secondary objectives
• Open, Multicentric, comparative, randomized
study
• Patients with severe secondary MR with CI to
surgery
• MitraClip vs optimal medical management
• Total duration of the study: 4 years
Start: December 2013
Patient enrollment: 24m
Follow-up: 24m
Protocol

• Severe secondary MR (Carpentier type III)
• Severity assessed by TTE/TEE
• NYHA class >= II
• LVEF 15-40%
• >= 1 heart failure hospitalisation <12m
• Optimal medical management
• Contraindication to mitral valve surgery decided by the Heart team
• Confirmation of inclusion echo criteria by Echo CoreLab
Inclusion criteria

• Absence of CI to surgery
• Primary MR
• MI or CABG< =3m
• CRT<= 3m
• Other surgery planned
• PCI<= 1m
• Previous mitral valve repair
• Active Infection
• Dialysis for renal failure
• Severe hepatic insufficiency
• Stroke<=3m
• Life expectancy<=1year
• Uncontrolled HTN
• Allergy to Nitinol
Exclusion criteria