Mismanagement of the Neurosurgical Patient: Case Studiesce.unthsc.edu/assets/2618/Mismanagement -...
35
Mismanagement of the Neurosurgical Patient: Case Studies Atif Haque, M.D., F.A.A.N.S., F.A.C.S. Neurological Surgeon Adjunct Clinical Assistant Professor UNT 4th Annual Neuroscience Summit 9 September 2017
Transcript of Mismanagement of the Neurosurgical Patient: Case Studiesce.unthsc.edu/assets/2618/Mismanagement -...

Mismanagement of the Neurosurgical Patient: Case Studies
Atif Haque, M.D., F.A.A.N.S., F.A.C.S.Neurological Surgeon
Adjunct Clinical Assistant Professor
UNT 4th Annual Neuroscience Summit9 September 2017

Disclosures
Consultant for Medtronic

Mismanagement of Neurosurgical Patients
Objectives Case Studies

Objectives
Identify missteps in the treatment of selected neurosurgical conditions.
Understand the recommended best treatment strategies of these selected conditions.
Learn how to avoid the pitfalls presented in the case studies.

Case 1
Presentation 54 yo female 1 month h/o left upper extremity
generalized weakness Minimal neck pain No arm pain
Case 1
Exam 4/5 strength throughout LUE Hyperreflexic in LUE + Hoffman’s reflex LUE Otherwise normal exam
Case 1
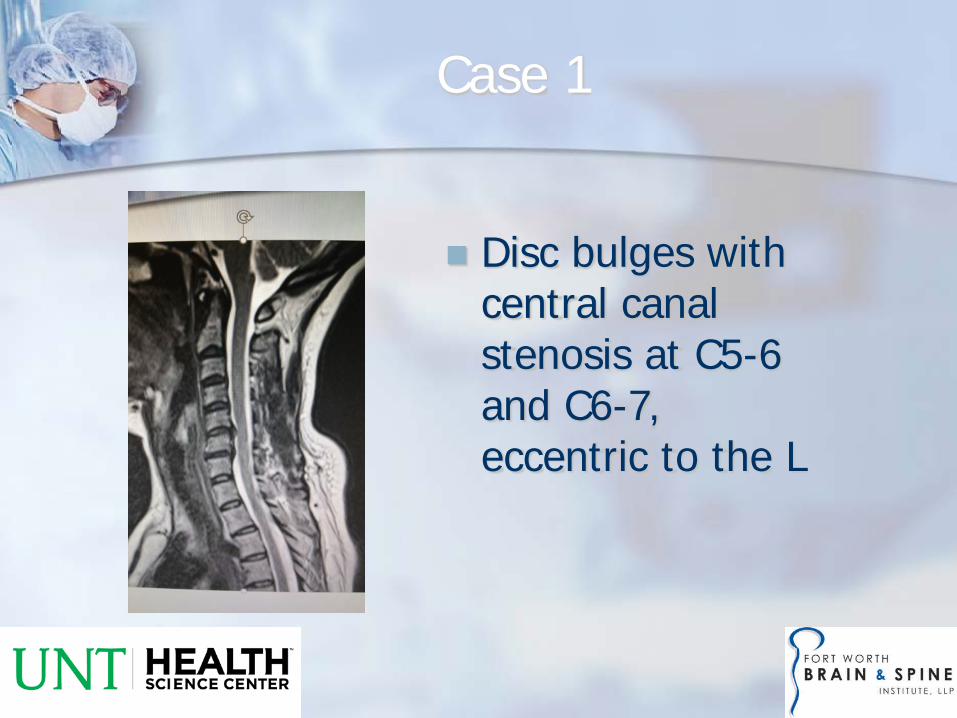
Disc bulges with central canal stenosis at C5-6 and C6-7, eccentric to the L

Case 1
First opinion—orthopedic spine surgeon Offered C5-7 ACDF
Came to me for a second opinion

Upper vs. Lower Motor Neuron
UMN paralysis Flaccid then
spastic Hyperreflexic ± clonus Pathologic
reflexes Examples-
Stroke, SCI, TBI, myelopathy
LMN paralysis Flaccid Hyporeflexic Atrophy ± fasciculations Examples-
radiculopathy, nerve entrapment, polio
Case 1
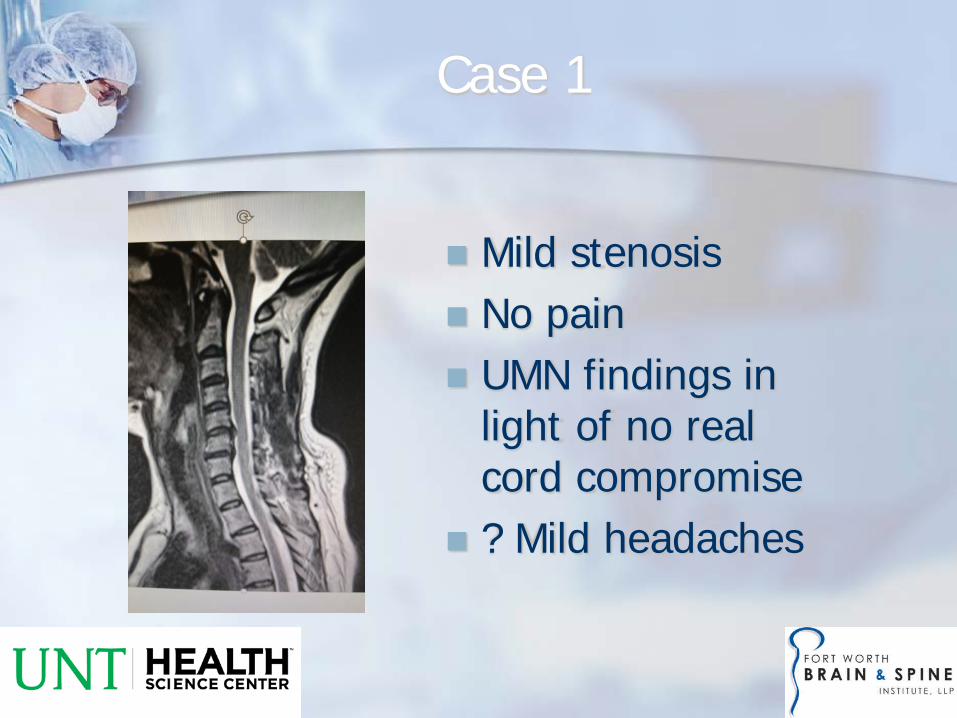
Mild stenosis No pain UMN findings in
light of no real cord compromise
? Mild headaches

Case 1
MRI brain Craniotomymeningioma
Case 2
Presentation 52 yo male Many month h/o left lower extremity
generalized weakness Moderate back pain Minimal leg pain No sensory issues Neck and arm pain

Case 2
Exam 4/5 strength left lower extremity diffusely Normal reflex exam in lowers,
hyporeflexic in uppers Normal strength elsewhere

Case 2
First opinion—orthopedic spine surgeon L4-5 fusion No improvement after 6 mos. MRI with minimal nerve
compromise on side of weakness Offered L3-4 fusion
Saw me for second opinion

Case 2

Case 2
Brain MRI Non-enhancing right
frontal/motor strip mass with edema
Brain biopsy—low-grade astrocytoma
Chemotherapy

Case 2
Cervical spine MRI Severe central
stenosis Kyphosis Foraminal stenosis

Case 2
C3-7 ACDF for stenosis, deformity, radiculopathy

Case 3
30 yo male inmate assaulted Rapid decline in
mental status at outside ER
Large extra-axial hematoma

Case 3
Apparent difficulty transferring out ER doctor attempted a
burr hole Patient worsened
afterward Intubated and sent to CT
with retractor in place Transferred to FW

Case 3
Epidural Hematoma Bi-lenticular Arterial injury (MMA) Usually associated with
fracture Lucid interval
Subdural Hematoma Crescent Torn bridging vein Often associated with
underlying brain injury

Case 3
Craniotomy Epidural hematoma Temporal bone
fracture Bleeding from MMA Complete recovery
within 24 hours

Case 4
Presentation 66 yo female Comatose for about 2 weeks and unresponsive and
on ventilator Found to have R > L subdural hematomas Recent diagnosis of leukemia Being treated by another neurosurgeon without any
improvement in spine of multiple procedures Further surgery was being recommended I was asked to give a third opinion
Case 4
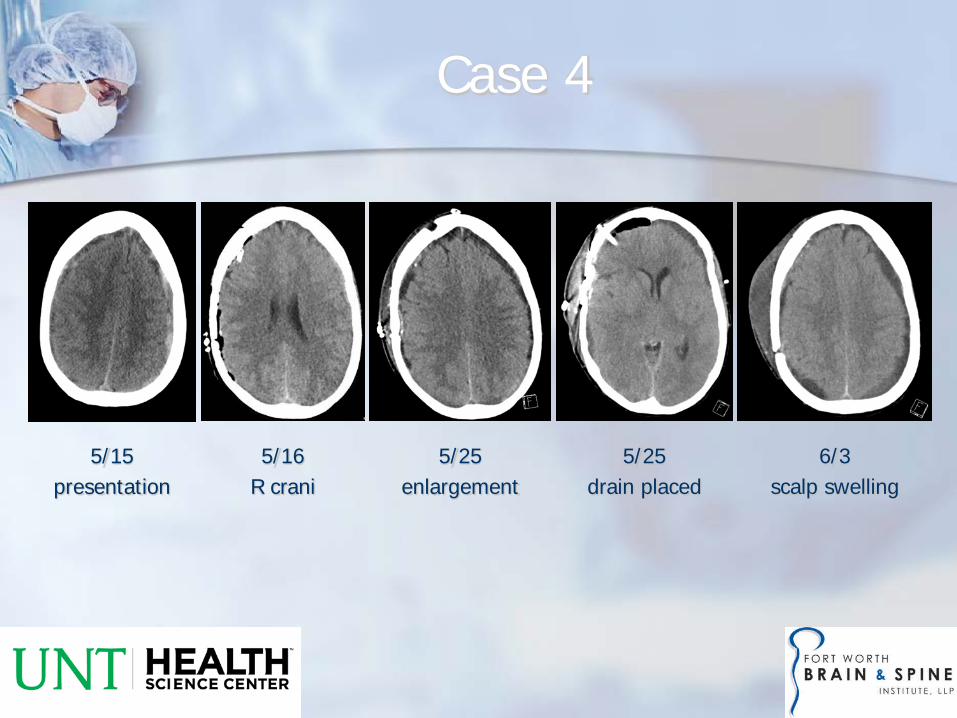
5/15presentation
5/16R crani
5/25enlargement
5/25drain placed
6/3scalp swelling

Case 4
Upon further investigation, Had severe headaches immediately following LP 5
days prior to presentation, as well as getting intrathecal chemotherapy
Headache worsened with standing/sitting and improved with laying flat
Progressive nausea Progressive lethargy; obtunded at presentation

Case 4
Intracranial hypotension Spontaneous vs. post-traumatic vs. iatrogenic Orthostatic headache classically Other presentations—encephalopathy, myelopathy, parkinsonism “CSF hypovolemia” Low or normal intracranial pressure Imaging—brain and spine
± Pachymeningeal enhancement ± Sagging brain/tonsils ± Subdural hygromas/hematomas ± Small ventricles/cisterns ± Obvious site of CSF leak

Case 4
MRI spine without obvious CSF leak MRI brain
BilateralSDH’s
Cisternaleffacement
Brainsagging
Low-lyingtonsils

Case 4
Treatment options for intracranial hypotension HOB flat/bedrest Pain control Hydration Caffeine Epidural blood patch Fix underlying leak

Case 4
Our patient Epidural blood patch 17 days after admission and of being
comatose No obvious response in first 24 hours
ICP monitor insertion for 24 hours Essentially normal pressures with occasional low readings
Patient turned back over for comfort care, possible tracheostomy/G-tube
Slowly became more responsive over next couple of weeks Subsequent removal of R bone flap for possible infection
cultures negative Following commands and talking 2 weeks after blood patch

Case 5
18 yo female College-bound athlete Occipital headaches Numbness/tingling
bilateral upper extremities
Worsening with coughing/sneezing

Chiari I Malformation Herniation of cerebellar
tonsils Brainstem typically normal
30-70% with associated syrinx
Young adult presentation
Case 5

Case 5
PCPEvaluation
MRI withherniated“tonsils”
PCPrefers to
ENT
ENTEvaluation
ENTrefers to
Ortho Spine
Ortho Spinestarts
migraine meds
Patient’sgrandmother
(former patient)recommends
me
Neurosurgeryevaluation
with surgeryoffered

Case 6
67 yo female s/p MVC Sizeable
intraparenchymal hematoma
Taken to OR emergently Congenital occipital
encephalocele

References
Chiari and Syringomyelia Foundation website. Greenberg, M.S. Handbook of Neurosurgery.

Thank you.
Questions?