Middleware and the Clinical Hematology...
68
Middleware and the Middleware and the Clinical Hematology Clinical Hematology Laboratory Laboratory
Transcript of Middleware and the Clinical Hematology...

Middleware and the Middleware and the
Clinical Hematology Clinical Hematology
LaboratoryLaboratory

Balance? Balance? Clinical Needs vs. Laboratory RealityClinical Needs vs. Laboratory Reality
Accuracy
TAT
Costs
Resources

It doesn’t have to be a contest between
efficiency andpatient care!

Today’s OutlineToday’s Outline
Background of CBC and diffBackground of CBC and diff
Verification of the differential countVerification of the differential count
Practice modeling: prePractice modeling: pre--middlewaremiddleware
5 phases of middleware utilization5 phases of middleware utilization–– Automate Rules for Manual DifferentialsAutomate Rules for Manual Differentials
–– Focus on Patient Safety IssuesFocus on Patient Safety Issues
–– Enhance Laboratory EffectivenessEnhance Laboratory Effectiveness
–– Support Management GoalsSupport Management Goals
–– Unify MultiUnify Multi--site Practicessite Practices

Evolution of the Complete Blood Evolution of the Complete Blood Count (CBC)Count (CBC)
Early 1900’s: Counting Early 1900’s: Counting chamberschambers
Colorimetric methods for Colorimetric methods for hemoglobinhemoglobin
1940’s and 1950’s: 1940’s and 1950’s: Wintrobe and the Wintrobe and the hematocrit tube, MCV, hematocrit tube, MCV, MCH, MCHCMCH, MCHC
1956: Wallace Coulter 1956: Wallace Coulter and apertureand aperture--impedenceimpedencecell counting methodcell counting method
1970’s: Light scatter cell 1970’s: Light scatter cell counting counting
1980’s & 1990’s: Air1980’s & 1990’s: Air--cooled lasers, computers, cooled lasers, computers, etc.etc.
1990’s: Application of 1990’s: Application of immunologic methodsimmunologic methods
2000’s: Middleware and 2000’s: Middleware and other software other software approachesapproaches

Evolution of the Leukocyte Evolution of the Leukocyte Differential Count (Diff)Differential Count (Diff)
Early 1900’s: Evolution Early 1900’s: Evolution of manual techniquesof manual techniques
Early 1970’s: Image Early 1970’s: Image capture techniquescapture techniques
–– HematrakHematrak, IMI Micro 21, , IMI Micro 21, LAFIA system, LAFIA system, DifffmasterDifffmaster, , etc.etc.
1981: Technicon 1981: Technicon HemalogHemalog D D
–– First instrument to perform First instrument to perform automated differentialsautomated differentials
1983: Coulter Counter 1983: Coulter Counter Plus IVPlus IV
–– 33--part differentialspart differentials
1980’s/90’s: Coulter STKS, 1980’s/90’s: Coulter STKS, Sysmex 9000, Cell Dyne Sysmex 9000, Cell Dyne 35003500
–– 55--part differentialspart differentials
2000’s: Image recognition 2000’s: Image recognition software programssoftware programs
–– Still in its infancyStill in its infancy

Why Focus on the CBC and Diff?Why Focus on the CBC and Diff?CBC is the most frequently ordered single CBC is the most frequently ordered single laboratory testlaboratory test–– Highest reimbursed laboratory assay by CMSHighest reimbursed laboratory assay by CMS
Used in outpatient and inpatient settingsUsed in outpatient and inpatient settings–– Need 24/7 availabilityNeed 24/7 availability
Used as a screening tool for “health”Used as a screening tool for “health”–– Opens the door to the patient Opens the door to the patient -- looking for possible looking for possible
hematologic, infectious, inflammatory, and oncologic hematologic, infectious, inflammatory, and oncologic diseasesdiseases
Used specifically to evaluate for a variety of Used specifically to evaluate for a variety of acute and chronic hematologic diseasesacute and chronic hematologic diseases

The Manual DifferentialThe Manual DifferentialThe manual differentialThe manual differential–– Is labor intensive Is labor intensive
–– Requires both highly skilled and experienced Requires both highly skilled and experienced technologists and backtechnologists and back--up and availability by up and availability by pathologistspathologists
Errors with the manual differentialErrors with the manual differential–– Observer errorsObserver errors–– Slide distribution errorsSlide distribution errors–– Sampling errors with a 100 cell countSampling errors with a 100 cell count–– Data entry errorsData entry errors

The Automated DifferentialThe Automated Differential
The automated differentialThe automated differential
–– Is geared toward “not missing” anythingIs geared toward “not missing” anything
–– Must recognize a wide spectrum of white cell diff Must recognize a wide spectrum of white cell diff abnormalitiesabnormalities
Lymphoid and myeloid; acute and chronic; preLymphoid and myeloid; acute and chronic; pre-- and postand post--therapeutictherapeutic
No “single” cell type perfectly represents each disease processNo “single” cell type perfectly represents each disease process
Can’t consistently distinguish between reactive and diseaseCan’t consistently distinguish between reactive and disease
–– Every instrument technology has its own inherent Every instrument technology has its own inherent idiosyncrasies and will “overidiosyncrasies and will “over--capture” and “undercapture” and “under--capture” particular morphologic abnormalities capture” particular morphologic abnormalities

Manual vs. Automated Diff?Manual vs. Automated Diff?
The Challenges?The Challenges?
–– Need to identify important abnormal findings Need to identify important abnormal findings while minimizing the time required for either while minimizing the time required for either “normals” or “minimal abnormals”“normals” or “minimal abnormals”
–– In other words, maximize the use of In other words, maximize the use of automated differentialsautomated differentials while minimizing the while minimizing the number of number of manual differentialsmanual differentials
–– “The Technology” vs. “The Art”“The Technology” vs. “The Art”
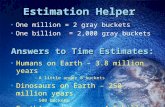
Verification of the Diff: Where?Verification of the Diff: Where?
“In the Lab”• Technologist• Middleware
LISAuto-verify rules
InstrumentAuto-verify rules

Verification of the Diff: How?Verification of the Diff: How?InstrumentInstrument–– Is geared toward “not missing” anythingIs geared toward “not missing” anything–– Quantitative flags (RBC & WBC)Quantitative flags (RBC & WBC)
Set by the laboratorySet by the laboratoryShould not be based on “normal values”Should not be based on “normal values”
–– Qualitative flagsQualitative flagsEstablished by the manufacturerEstablished by the manufacturer
–– Autoverification at the instrument is dependent Autoverification at the instrument is dependent on the local patient populationon the local patient population
Mayo Health System Clinics: 60% autoMayo Health System Clinics: 60% auto--release raterelease rateU of Michigan and Mayo: 40% autoU of Michigan and Mayo: 40% auto--release raterelease rate

Verification of the Diff: How?Verification of the Diff: How?LISLIS–– Dependent on vendor/systemDependent on vendor/system–– Many/Most have ruleMany/Most have rule--writing capabilitieswriting capabilities–– Easier for the lab to meet regulatory Easier for the lab to meet regulatory
requirementsrequirements–– IT support and backIT support and back--upup–– Often dependent on nonOften dependent on non--lab people to write lab people to write
the rulesthe rules–– Responsiveness can be at a bureaucratic, Responsiveness can be at a bureaucratic,
glacial pace; nonglacial pace; non--flexibleflexible

Verification of the Diff: How?Verification of the Diff: How?
Middleware:
– Usually purchased from instrument manufacturer
– Other non-instrument vendors are available
– Need information from both the instrument and LIS
– Need to bring middleware vendor, instrument manufacturer, and LIS resources together to understand the interface and what limitations the interface will impose
– Back-up and IT support is critical for a laboratory. Does the lab have to develop their own expertise?

Verification of the Diff: How?Verification of the Diff: How?
Middleware and Mayo Laboratory HematologyMiddleware and Mayo Laboratory Hematology–– Hematology Instrument Interface System Hematology Instrument Interface System
(HIIS; Coulter): November 1996(HIIS; Coulter): November 1996–– Aqueduct (Orchard Software): July 1999Aqueduct (Orchard Software): July 1999
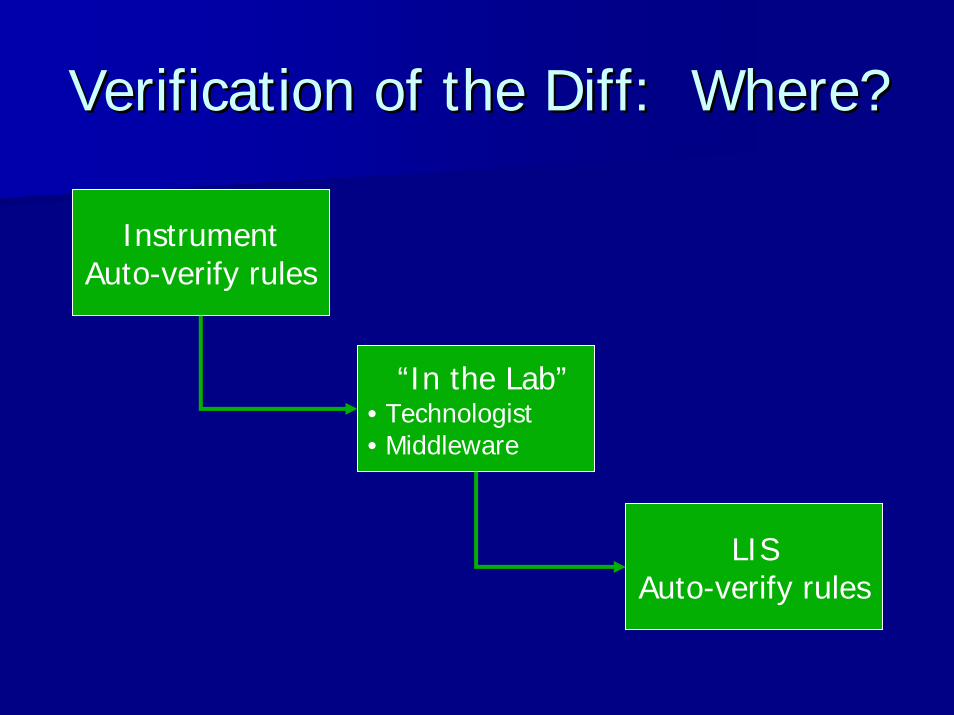
Differential?
Instrumentauto-verify
Scan and release Manual
LIS / EMRSignificantabnormal
Minimal abnormalor normal

Instrumentauto-verify
Scan and release
Manual:•Normal/minimal •Abnormal (signif)
Practice ModelingPractice Modeling
How your practice cases are distributed in these How your practice cases are distributed in these “buckets” will determine your “buckets” will determine your middleware valuemiddleware value..
–– Is your instrument autoIs your instrument auto--verify at: 80% or 40%?verify at: 80% or 40%?
–– Is your “scan and release” at: 5% or 30%?Is your “scan and release” at: 5% or 30%?
–– Manual differentials: how many have Manual differentials: how many have truetrue value value added by morphologic review? 5% or 50%?added by morphologic review? 5% or 50%?

Practice Modeling Practice Modeling -- MayoMayo
Instrumentauto-verify
Scan and release
Manual:Normal /minimal
Manual:Abnormal
(significant)
Pre-Middleware (1995):
Current (2008):
40% 20% 30% 10%
82% 8% 2% 8%

QualityCost
Value = (satisfaction, outcomes,
safety, and service)
Practice Modeling: The Value Practice Modeling: The Value EquationEquation
“Value” must drive the process of whether and how middleware should be used in a
hematology laboratory.
Middleware

Today’s OutlineToday’s Outline
Background of CBC and diffBackground of CBC and diff
Verification of the differential countVerification of the differential count
Practice modeling: prePractice modeling: pre--middlewaremiddleware
5 phases of middleware utilization5 phases of middleware utilization–– Automate Rules for Manual DifferentialsAutomate Rules for Manual Differentials
–– Focus on Patient Safety IssuesFocus on Patient Safety Issues
–– Enhance Laboratory EffectivenessEnhance Laboratory Effectiveness
–– Support Management GoalsSupport Management Goals
–– Unify MultiUnify Multi--site Practicessite Practices

Five Phases of MiddlewareFive Phases of Middleware
Unify multi-site practices
Support management goals
Enhance laboratory effectiveness
Focus on patient safety issues
Automate rules for manual differentials

Five Phases of MiddlewareFive Phases of Middleware
Unify multi-site practices
Support management goals
Enhance laboratory effectiveness
Focus on patient safety issues
Automate rules for manual differentials

Differential?
Instrumentauto-verify
Scan and release
Manual
LIS / EMRSignificantabnormal
Minimal abnormalor normal

Automate Rules for Manual Automate Rules for Manual DifferentialsDifferentials
Simply write rules for what the technologist doesSimply write rules for what the technologist does
–– If they look up results in the computerIf they look up results in the computer
–– If they compare results to previous studiesIf they compare results to previous studies
–– If they base a decision on where the patient is or who If they base a decision on where the patient is or who their doctor istheir doctor is
–– If they minimize or ignore certain results or certain If they minimize or ignore certain results or certain instrument flagsinstrument flags
–– What are their algorithms for deciding whether a diff What are their algorithms for deciding whether a diff gets performed or not?gets performed or not?

Quantitative numbers
Ranges sensitive to age and gender
Instrument flags
Delta check to hold
Delta check to release
Delta check on instrument flags
By physician
By type of CBC
By lab location
By patient location
By patient
Elapsed time between specimen testing
Automate Rules for Manual Automate Rules for Manual DifferentialsDifferentials

ISLH ISLH –– Consensus GuidelinesConsensus GuidelinesAGE
Parameter Primary and/or Secondary and/or Tertiary Action 1
Neonate First sample Slide review
Parameter Primary and/or Secondary and/or Tertiary Action 1
CBC
WBC <4.0 or > 30.0 and Deltafailed and < 3 days Slide review
PLT <100 or >1000 and First time Slide review
HGB<7g/dl or > 2g/dl above
upper referencerange for age and sex
and First time Slide review
RDW >22 and First time Slide review

ISLH ISLH –– Consensus GuidelinesConsensus Guidelines
DIFFERENTIAL
Parameter Primary and/or Secondary Action 1
No diff or incomplete diff Slide review
Neut # <1.0 or > 20.0 and First time Slide review
Lymph # >5.0 (adult) or >7.0 (<12 yrs old) and First time Slide review
Mono # >1.5 (Adult) or >3.0 (<12 yrs old) and First time Slide review
NRBC # any value and First time Slide review

INSTRUMENT FLAGS
Parameter Primary and/or Secondary and/or Tertiary Action 1
Suspect flag (except Imm G/B) Flag + and First time and Adult Slide review
Dimorphic RBC Flag + and First time Slide review
Left shift flag Flag + Follow lab SOP
Atypical lymphs Flag + and First time Slide review
PLT clump flag Any count Check samplefor clots
Immature granflag Flag + and Previous
confirmed result and Positive deltafail for WBC Slide review
Blast flag Flag + and Previous confirmed result and Positive delta
fail for WBC Slide review
NRBC flag Flag + Slide review
ISLH ISLH –– Consensus GuidelinesConsensus Guidelines

Mayo Mayo –– Aqueduct RulesAqueduct Rules
QUANTITATIVE FLAGSQUANTITATIVE FLAGS
TestsTests ActionAction LoLo HiHi Value Tests Held/Trapped Tests Pre-Transmitted Assigned
Panels
Hgb < X 6.1RBC, Hgb, Hct,
MCV, MCH, MCHC
WBC, 5-pt diff,RDW, Plt
CBC, CBCC,CBCN,
CBC4/NC
Plt < X 40.1 WBC, Plt 5-pt diff, RBC, Hgb, Hct,MCV, MCH, MCHC, RDW
CBC, CBCN,CBC4/NC
WBC < X 1.0 WBC5-pt diff, RBC, Hgb, Hct,
MCV, MCH, MCHC,RDW, Plt
CBC, CBCN,CBC4/NC
Plt Contains>
R39 WBC, Plt
5-pt diff, RBC, Hgb, Hct, MCV, MCH, MCHC,
RDW
CBC, CBCN,CBC4/NC

INSTRUMENT FLAGS
Value Tests Held/Trapped Tests Pre-Transmitted Assigned Panels
Imm. Ne 2 5-pt diff CBC CBC, CBC4/NC
Low Event # 5-pt diff CBC CBC, CBC4/NC
Ly Blasts 5-pt diff CBC CBC, CBC4/NC
Platelet Clumps CBC & diff None CBC, CBCN,CBC4/NC
RBC Interference CBC WBC, 5-pt diff CBC, CBCC, CBCN,CBC4/NC, CBCCG
Variant LY 5-pt diff CBC CBC, CBC4/NC
Mayo Mayo –– Aqueduct RulesAqueduct Rules

Mayo Mayo –– Aqueduct RulesAqueduct Rules
DELTA CHECKDELTA CHECK
TestsTests ActionAction LoLo HiHi Value Tests Held/Trapped
Tests Pre-Transmitted
Assigned Panels
Plt
Exceeds Hold Delta(Current is both + & -80%. New release
You can choose oneor the other or both)
80%/4 days CBC & diff None
CBC,CBCC,CBCN,
CBBCCG,CBC4/NC
RDW
Exceeds Release Delta
>
Location is not
X
10%/7 days
17.5
Spec.Sta.
RDWWBC, 5-pt diff, RBC,
Hgb, Hct, MCV,MCH, MCHC, Plt
CBC,CBC4/NC

Lab Bldg
OutpatientClinics
Kasson
Kenyon
NW
NE
Gonda Lab(Chemo)
MH Lab(OR, ICUs)
SMH Lab(ER, OR, ICUs)
Methodist(MH)
St. Marys(SMH)
Lab Bldg
BloodDraw
CentralAuto. Lab
HemeLab
Lab Bldg
Lab
Lab
Lab
Lab
Middlewareauto-verify
n=1404
Scan and releasen=105
Manual diffn=168
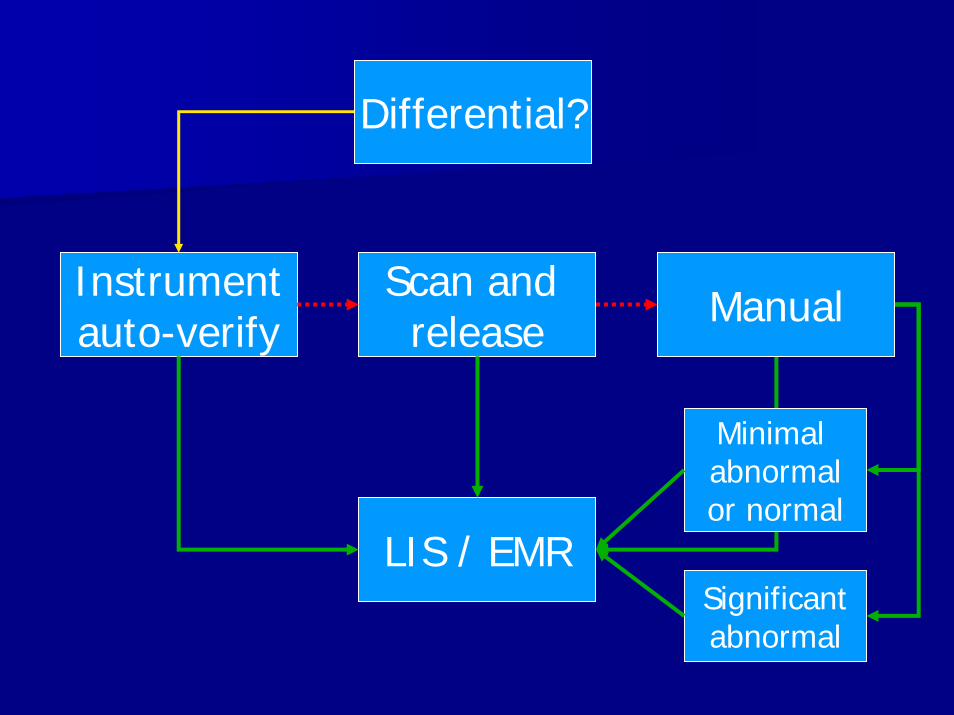
March 19, 2008March 19, 2008
LIS / EMR
Instrumentauto-verify
n=42
CentralAuto.Lab
n=1719
HemeLab
n=315
Trapped by Middleware:Quantitative – CBC: 195Quantitative – Diff: 168Instrument Flags: 302Individual Patients: 6
82%
18% 2% 6% 10%
13% 33% 54%

Middleware Middleware -- ImpactImpactInstrumentauto-verify
Scan and release
Manual:Normal /minimal
Manual:Abnormal
(significant)
Pre-Middleware:
Current:
40% 20% ~30% ~10%
82% 8% 2% 8%
Within 3 months of implementation:• Decreased 3.0 FTE• TAT of Priority 1 CBC’s: went from 50% to 85% released < 30 min.• Median TAT of all CBC’s went from 90 min. to 30 min.• Average CBC time in central automated lab: <20 min.

Automate Rules for Manual Automate Rules for Manual DifferentialsDifferentials
CBC CBC –– ChemotherapyChemotherapy–– Applied different rules for patients receiving Applied different rules for patients receiving
chemotherapy for myeloma and lymphoma chemotherapy for myeloma and lymphoma and certain leukemiasand certain leukemias
The entire clinical question is:The entire clinical question is:–– Are there enough platelets and neutrophils so Are there enough platelets and neutrophils so
that the hematologist can continue to give the that the hematologist can continue to give the next dose of chemotherapy? next dose of chemotherapy?

Automate Rules for Manual Automate Rules for Manual DifferentialsDifferentials
CBC CBC –– Chemotherapy (CBCChemotherapy (CBC--C)C)
–– Created a new type of orderable CBC available Created a new type of orderable CBC available only to the hematologists: only to the hematologists: CBCCBC--CC
–– Clinical needs:Clinical needs:The CBC is no longer a screening assay The CBC is no longer a screening assay –– it is a it is a therapeutic monitoring assay.therapeutic monitoring assay.
An accurate diff is not a concern, just: are there An accurate diff is not a concern, just: are there PMN’sPMN’s and platelets?and platelets?
A rare blast or a slight left shift is not importantA rare blast or a slight left shift is not important
Rapid turnRapid turn--aroundaround--time is the driving forcetime is the driving force

Automate Rules for Manual Automate Rules for Manual DifferentialsDifferentials
Separate autoSeparate auto--verify rules for the CBCverify rules for the CBC--CC
–– WBC>99.9; Hgb<6.1; MCHC>37; BA%>5WBC>99.9; Hgb<6.1; MCHC>37; BA%>5
–– 55--part R flag; Interference flags; nonpart R flag; Interference flags; non--resultsresults
–– PltPlt delta checkdelta check
Clinical awareness is importantClinical awareness is important
–– Cannot be used for other clinical scenariosCannot be used for other clinical scenarios
–– Need to call the lab to convert the CBC to a “real” CBC Need to call the lab to convert the CBC to a “real” CBC if there are any clinical findings that raise other if there are any clinical findings that raise other questions such as infection, etc.questions such as infection, etc.

Automate Rules for Manual Automate Rules for Manual DifferentialsDifferentials
Pre CBCPre CBC--CC–– ~150 CBC’s per week ~150 CBC’s per week
from chemo unitfrom chemo unit–– Autoverify through Autoverify through
AqueductAqueduct35%35%
–– Average TAT: Average TAT: 20 min. vs. 2.5 hours20 min. vs. 2.5 hours
–– Not a happy clinical Not a happy clinical group!group!
CBCCBC--C implemented in C implemented in 20012001
Post CBCPost CBC--CC–– Autoverify: 88%Autoverify: 88%–– TAT = 20 min from TAT = 20 min from
blood drawblood draw–– Audits:Audits:
NeutropeniaNeutropeniaThrombocytopeniaThrombocytopeniaLeft shiftLeft shiftRBC RBC poikpoik (non(non--specific)specific)Rare blast (LEBR)Rare blast (LEBR)Rare lymphoma or Rare lymphoma or plasma cellplasma cell
–– ~1 CBC~1 CBC--C converted to C converted to routine CBC per monthroutine CBC per month

Five Phases of MiddlewareFive Phases of Middleware
Unify multi-site practices
Support management goals
Enhance laboratory effectiveness
Focus on patient safety issues
Automate rules for manual differentials

Focus on Patient Safety IssuesFocus on Patient Safety Issues
Why call it patient safety?Why call it patient safety?–– In the hematology laboratory, true primary In the hematology laboratory, true primary
sentinel events are blessedly raresentinel events are blessedly rare–– BUTBUT: Revised reports from labs do contribute : Revised reports from labs do contribute
to unnecessary clinical steps, which may lead to unnecessary clinical steps, which may lead to unnecessary patient eventsto unnecessary patient events
–– Every lab needs to look at all their revised Every lab needs to look at all their revised reports and near misses. Why did they reports and near misses. Why did they happen? What was wrong with the happen? What was wrong with the processprocess??
–– Until you collect the info, you will Until you collect the info, you will underestimate the severity of the issueunderestimate the severity of the issue

Focus on Patient Safety IssuesFocus on Patient Safety Issues
Revised reports and near missesRevised reports and near misses–– Revised diff counts Revised diff counts (instrument or tech)(instrument or tech)
After pathologist review of a bone marrowAfter pathologist review of a bone marrowAfter tech review of a subsequent PB smearAfter tech review of a subsequent PB smearAfter a call from a clinicianAfter a call from a clinician
–– Revised platelet count due to clotted Revised platelet count due to clotted specimens or EDTAspecimens or EDTA--associated clumpingassociated clumping
After tech review of a subsequent PB smearAfter tech review of a subsequent PB smearAfter a call from a clinicianAfter a call from a clinician
–– Dependency on “sticky notes” and memoryDependency on “sticky notes” and memory

Focus on Patient Safety IssuesFocus on Patient Safety Issues
Revised reports and near misses Revised reports and near misses ((con’tcon’t.).)
–– Didn’t follow through per SOP Didn’t follow through per SOP (memory)(memory)Did a scan and release instead of a manual diffDid a scan and release instead of a manual diff“Forgot” to have a second review by senior tech “Forgot” to have a second review by senior tech or MDor MDEtc.Etc.
–– Manual reporting / clerical error Manual reporting / clerical error (direct (direct interface)interface)
–– Mixing up slides and paperwork Mixing up slides and paperwork (barcodes)(barcodes)

Focus on Patient Safety IssuesFocus on Patient Safety Issues
Individual patients act like individuals Individual patients act like individuals –– they they don’t always follow the rules for the group.don’t always follow the rules for the group.Let’s call our patient: “Mrs. Johnson”Let’s call our patient: “Mrs. Johnson”–– Blasts may be missed on followBlasts may be missed on follow--upsups–– Lymphoma cells may be missed on followLymphoma cells may be missed on follow--upsups–– Morphologic features may be difficult to interpretMorphologic features may be difficult to interpret–– EDTA platelet “clumpers” create problemsEDTA platelet “clumpers” create problems–– Red cell agglutination create problemsRed cell agglutination create problems–– Clinician or pathologist need specific followClinician or pathologist need specific follow--up on up on
Mrs. JohnsonMrs. Johnson–– Protocol/clinical trial requirementsProtocol/clinical trial requirements

Focus on Patient Safety IssuesFocus on Patient Safety Issues
Middleware can helpMiddleware can help–– Immediately in the lab can create a rule to Immediately in the lab can create a rule to
“trap” the next sample that comes through “trap” the next sample that comes through from Mrs. Johnsonfrom Mrs. Johnson
–– A time line is added to the rule; e.g., expires A time line is added to the rule; e.g., expires in one month or three monthsin one month or three months
–– Doesn’t matter where in the system Mrs. Doesn’t matter where in the system Mrs. Johnson walks into Johnson walks into –– main clinic, ER, outlying main clinic, ER, outlying clinic, etc.: same outcome for the CBCclinic, etc.: same outcome for the CBC

Focus on Patient Safety IssuesFocus on Patient Safety Issues
PrePre--““MrsMrs. Johnson”. Johnson”
Revised differentialsRevised differentials–– 2.5 “A” events / mo.2.5 “A” events / mo.
Communicate by Communicate by sticky notes and sticky notes and emailsemails
PostPost--““MrsMrs. Johnson”. Johnson”
Revised differentialsRevised differentials–– <1 “A” event / mo.<1 “A” event / mo.
5 to 10 “Mrs. Johnson 5 to 10 “Mrs. Johnson rules” in place at any rules” in place at any given timegiven time< 2 hrs. from request < 2 hrs. from request to being “live”to being “live”

Five Phases of MiddlewareFive Phases of Middleware
Unify multi-site practices
Support management goals
Enhance laboratory effectiveness
Focus on patient safety issues
Automate rules for manual differentials

Enhance Laboratory EffectivenessEnhance Laboratory Effectiveness
Use middleware to streamline the Use middleware to streamline the presentation and flow of data from presentation and flow of data from instrument to workstation instrument to workstation –– regardless regardless of where data was acquiredof where data was acquired
Minimize the number of manual steps Minimize the number of manual steps between instrument and slide reviewbetween instrument and slide review
Blends with patient safety issuesBlends with patient safety issues

Enhance Laboratory EffectivenessEnhance Laboratory Effectiveness
Use middleware to make the lab paperlessUse middleware to make the lab paperless–– At each workstation:At each workstation:
Transmit scatterplots to any workstationTransmit scatterplots to any workstationMake all CBC/diff data easily visibleMake all CBC/diff data easily visibleApply color coding to aid visual recognition Apply color coding to aid visual recognition Visually see trapped vs. released data Visually see trapped vs. released data Display invoked rules for trapped dataDisplay invoked rules for trapped data
–– Multiple ways to review old dataMultiple ways to review old dataBy CBC dateBy CBC dateBy each analyteBy each analyte





Lab continues to run if LIS is downLab continues to run if LIS is downUse rules as SOP remindersUse rules as SOP reminders–– E.g.: new employee can’t report out E.g.: new employee can’t report out
schistocytes without 2schistocytes without 2ndnd reviewreview–– All new adult All new adult lymphocytoseslymphocytoses needs MD reviewneeds MD review–– All blasts >1% need initial MD reviewAll blasts >1% need initial MD review
Disease processesDisease processes–– Set frequency of review after initial diagnosis Set frequency of review after initial diagnosis
of a disease: e.g., CLL, MDS, etc.of a disease: e.g., CLL, MDS, etc.
Enhance Laboratory EffectivenessEnhance Laboratory Effectiveness

The instrument’s QC package (The instrument’s QC package (12s N=2 or 3) is not is not optimal for each of the CBC’s components. A high optimal for each of the CBC’s components. A high false rejection rate breeds complacency:false rejection rate breeds complacency:
Can you use middleware as your QC manager?Can you use middleware as your QC manager?
LH750LH750 Sigma Metric QC Rule
Hgb 8.75 13.5s N=3
WBC 8.82 13.5s N=3
RBC 7.50 13.5s N=3
Plt 7.57 13.5s N=3
Enhance Laboratory EffectivenessEnhance Laboratory Effectiveness

Five Phases of MiddlewareFive Phases of Middleware
Unify multi-site practices
Support management goals
Enhance laboratory effectiveness
Focus on patient safety issues
Automate rules for manual differentials
Support Management GoalsSupport Management Goals
Is there laboratory information that cannot Is there laboratory information that cannot be gathered through “routine” reports?be gathered through “routine” reports?
–– Technologist productivityTechnologist productivity
–– Type of cases released by technologistType of cases released by technologist
–– Number and type of cases trapped by each ruleNumber and type of cases trapped by each rule
Monitor utilization of rulesMonitor utilization of rules
Identify new clinical scenarios for potential new Identify new clinical scenarios for potential new rulesrules

Technologist ProductivityTechnologist Productivity
0102030405060708090
100
A C E G I K M O Q S U W Y AA CC
Avg
. PB
cas
es /
sh
ift

Differential?
Instrumentauto-verify
Scan and release
Manual
LIS / EMRSignificantabnormal
Minimal abnormalor normal

Technologist ProductivityTechnologist Productivity
0
10
20
30
40
50
60
70
80
E R S W X CC DD
Scan Manual
Avg
. PB
cas
es /
sh
ift

Five Phases of MiddlewareFive Phases of Middleware
Unify multi-site practices
Support management goals
Enhance laboratory effectiveness
Focus on patient safety issues
Automate rules for manual differentials
Future Needs: Unify MultiFuture Needs: Unify Multi--site site PracticesPractices
Multiple sites within a hospital/clinicMultiple sites within a hospital/clinic
Multiple hospitals and clinics within an Multiple hospitals and clinics within an organization organization –– local, regional, nationallocal, regional, national
–– May have different instrumentationMay have different instrumentation
–– Different clinical needs at each siteDifferent clinical needs at each site
–– Different patient characteristics at each siteDifferent patient characteristics at each site
–– Not all sites may do manual differentialsNot all sites may do manual differentials
–– May or may not have a common EMRMay or may not have a common EMR

Future Needs: Unify MultiFuture Needs: Unify Multi--site site PracticesPractices
Middleware offers you a common Middleware offers you a common language through which laboratories language through which laboratories can communicatecan communicate
Middleware offers you a starting point Middleware offers you a starting point for standardization / integration of for standardization / integration of your medical practiceyour medical practice

Middleware ConclusionsMiddleware ConclusionsBefore you purchase / implement:Before you purchase / implement:
–– Model your lab practice to understand where you Model your lab practice to understand where you might benefit from middleware and to what extentmight benefit from middleware and to what extent
–– Keep in mind the “Value Equation” Keep in mind the “Value Equation” –– both quality and both quality and costs can be improved with middlewarecosts can be improved with middleware
–– Envision the coordinated roles that your instrument, Envision the coordinated roles that your instrument, LIS, and potential middleware system will play in your LIS, and potential middleware system will play in your lab practicelab practice
Instrument and LIS might be sufficient in some labsInstrument and LIS might be sufficient in some labs
–– Work with your IT people to understand their needs Work with your IT people to understand their needs and their willingness to help provide support in the laband their willingness to help provide support in the lab

Automate rules for differentials Automate rules for differentials –– this is the this is the easy part! Benefits include:easy part! Benefits include:
–– Reduce costs / FTE’sReduce costs / FTE’s
–– Improve TATImprove TAT
–– Improve employee satisfactionImprove employee satisfaction
–– Improve accuracy of differential resultsImprove accuracy of differential results
Challenge your concept of the CBC and diff Challenge your concept of the CBC and diff and think differently about specific patient and think differently about specific patient populations and their needspopulations and their needs
Middleware ConclusionsMiddleware Conclusions

Focus on patient safety issues. Every lab needs Focus on patient safety issues. Every lab needs to look at all their revised reports and near to look at all their revised reports and near misses. Why did they happen? What was misses. Why did they happen? What was wrong with the wrong with the processprocess? ?
Use middleware to fill in gaps in your patient Use middleware to fill in gaps in your patient safety processes:safety processes:
–– “The Mrs. Johnson Rules”“The Mrs. Johnson Rules”
–– SOP and diseaseSOP and disease--specific “Popspecific “Pop--Up” reminders for the Up” reminders for the techstechs
Middleware ConclusionsMiddleware Conclusions

Enhance laboratory effectivenessEnhance laboratory effectiveness–– Create the paperless labCreate the paperless lab
–– Ensure the ideal screen presentations of dataEnsure the ideal screen presentations of data
–– Minimize the steps between CBC analyzer and the Minimize the steps between CBC analyzer and the microscope/work stationmicroscope/work station
–– Improve your QC approach in the labImprove your QC approach in the lab
Support management goalsSupport management goals–– Middleware is another source of information about your Middleware is another source of information about your
laboratorylaboratory
Unify multiUnify multi--site practicessite practices–– A common language to crossA common language to cross--communicate with other labscommunicate with other labs
–– A starting point for standardization / integration of your multiA starting point for standardization / integration of your multi--site laboratory practicesite laboratory practice
Middleware ConclusionsMiddleware Conclusions

Middleware!
Balance Achieved! Balance Achieved! Clinical Needs and Laboratory RealityClinical Needs and Laboratory Reality
Accuracy
TAT
Costs
Resources
Satisfaction Patient safety
Management Outcomes
Balance? Balance? Clinical Needs vs. Laboratory RealityClinical Needs vs. Laboratory Reality

Thank You!Thank You!


















