Saving the NHS_INVERTO & Mid Essex Hospital Services case study
20190416 900885 Post-inspection Evidence appendix template v4 Page 1
Mid Essex Hospital Services NHS Trust
Broomfield Hospital
Evidence appendix
Court Road,
Broomfield,
Chelmsford
CM1 7ET
Tel: 01245362000
www.meht.nhs.uk
Date of inspection visit:
5 November to 12 December 2019
Date of publication:
6 March 2020
This evidence appendix provides the supporting evidence that enabled us to come to our judgements of the quality of service provided by this trust. It is based on a combination of information provided to us by the trust, nationally available data, what we found when we inspected, and information given to us from patients, the public and other organisations. For a summary of our inspection findings, see the inspection report for this trust.
Facts and data about this trust
Mid Essex Hospital Services NHS Trust was established in 1992 and continues to provide local
elective and emergency acute medical services for adults and children for over 380,000 people
living in and around Chelmsford, Maldon, Braintree and Witham. The trust also includes Braintree
Community Hospital which covers the whole of Mid Essex and includes a variety of services
including x-rays, MRI scans, CT scans, ultrasound, day surgery, endoscopies, physiotherapy,
nursing and rehabilitation services.
In addition the trust provides a county-wide plastics, head and neck and upper gastrointestinal (GI)
surgical service to a population of 3.4 million and a supra-regional burns service to a population of
9.8 million. The trust employs over 5,000 staff and had a total turnover of £317m in 2018/19.
The trust continues to focus on performance and financial improvements, supported by NHS
Intelligence, NHS England and the CCG, to deliver their vision of becoming a financially stable,
modern health system that delivers integration and excellence in local and specialist services.
Mid Essex Hospitals NHS Trust remains a non-foundation trust. The trust began working closely
with Southend University Hospital NHS Foundation Trust and Basildon and Thurrock Hospitals
NHS Foundation trust in 2014. In 2015 the Essex Success Regime was announced and
collaborative working to have a joint clinical strategy began and continues. The leadership teams
restructure of the three trusts commenced in 2016 and was formalised as of 1 January 2017,
shared governance arrangements began in March 2017.

20190416 900885 Post-inspection Evidence appendix template v4 Page 2
This vision will continue through the proposed merger in 2020 of Mid Essex Hospital Services
NHS Trust with Basildon and Thurrock University Hospitals NHS Foundation Trust, and Southend
University Hospital NHS Foundation Trust.
(Source: Routine Provider Information Request (RPIR) – Acute context tab)
Acute hospital sites at the trust
A list of the acute hospitals at Mid Essex Hospital Services NHS Trust is shown below:
Name of acute hospital
site Address
Details of any specialist
services provided at the site
Broomfield Hospital
Broomfield Hospital
Court Road
Chelmsford
CM1 7ET
Acute and community-based
services. The site hosts regional
plastics, head and neck, and
upper gastrointestinal (upper GI)
surgical services and a supra-
regional burns service.
Braintree Community
Hospital
Braintree Community Hospital
Chadwick Drive
Braintree
CM7 2AL
A range of diagnostic tests, day
surgery, endoscopies,
physiotherapy, nursing and
rehabilitation services.
St Peter’s Hospital
St Peter's Hospital
Spital Road
Maldon
CM9 6EG
Maternity unit with a range of
outpatient clinics.
St Michael’s Hospital and
Birthing Centre
St Michael’s Hospital and Birthing
Centre
Chadwick Drive
Braintree
CM7 2AL
Birthing centre and a range of
therapy services.
(Sources: Trust Website / Routine Provider Information Request (RPIR) – Sites tab)
Due to the pending merger of the three trusts in April 2020 of; Mid Essex Hospital Services NHS
Trust with Basildon and Thurrock University Hospitals NHS Foundation Trust, and Southend
University Hospital NHS Foundation Trust. The decision was made to inspect core services at Mid
Essex Hospital Services NHS Trust and Southend University Hospital NHS Foundation Trust at
the same time which meant the executive team would be interviewed once at the well led part of
the inspection. Therefore there will be similarities in the report to the well led report for Southend
University Hospital NHS Foundation Trust.
20190416 900885 Post-inspection Evidence appendix template v4 Page 3
Is this organisation well-led?
Leadership
The executives of the trust had the right skills and abilities to run a service providing
sustainable care. The trust site leadership team had the appropriate range of skills,
knowledge and experience to perform its role.
The board executive team provided collaborative leadership between Mid Essex Hospital services
NHS Trust (MEHT), Basildon and Thurrock University Hospitals NHS Foundation Trust and
Southend University Hospital NHS Foundation Trust. The collaboration of the three trusts were
referred to as the MSB group which was adopted in January 2017 whilst options were considered.
In January 2018 the board approved the decision to merge, approved by NHS Improvement in
2018.
The key reasons for merging were to combine corporate services to sustain services for the local
communities, improve patient outcomes, provide further career opportunities to staff and financial
savings associated with the merger will improve services the trust delivers.
The executives were cohesive and experienced. The joint working board (JWB) consisted of a
chair, chief executive officer, chief medical officer, chief nurse, chief transformation officer, Chief
people and organisational, development director, chief finance officer, chief information officer,
chief of facilities and estates and a managing director from each trust.
The site leadership team were recruited by the executive team and are all substantive. The team
were developed under the management of the managing director. Leaders told us they had been
supported with training opportunities to enable them to do their role, and had been offered and/or
taken up external coaching.
The site leadership team at Mid Essex included a managing director, medical director, chief
operating officer, director of nursing, director of finance, head of human resources, director of
specialist services and trust secretary and director of strategy. Since our last inspection the trust
had a more stable experienced site level leadership team which enabled them to function
effectively. The site level leadership team were led by a managing director who was a member of
the JWB.
Senior leaders developed staff and in May 2019 the trust had commissioned a fifth senior staff
development programme to ensure staff were trained to take on leadership roles, there had been
positive feedback from the previous four cohorts.
The JWB met quarterly, and the executives were supported by the site leadership team.
Board Members
Of the executive board members at the trust, 8.3% were Black and Minority Ethnic (BME) and a
third (33.3%) were female.
Of the non-executive board members, 16.7% were BME and half (50.0%) were female.
Staff group BME % Female % Executive directors 8.3% 33.3% Non-executive directors 16.7% 50.0% All board members 11.1% 38.9%
(Source: Routine Provider Information Request (RPIR) – Board Diversity tab)
20190416 900885 Post-inspection Evidence appendix template v4 Page 4
Leaders told us that there was recognition that the board and senior leadership team was not
representative of the local population. To address this BME nurses had started to shadow leaders
and leaders planned to start peer mentoring BME members of staff. This is a process known as
reverse mentoring. This allows senior staff to better understand the issues that BME staff face.
All members of the board and site leadership teams we spoke with, demonstrated they had the
knowledge and leadership skills required of senior leaders. Leaders told us that the site leadership
structure was embedded, and clear lines of responsibility were now in place for governance and
safeguarding. Leaders acknowledged that governance arrangements remained complex, but were
the best they could be within the legal requirements for the three separate trusts the JWB was
responsible for.
We spoke with all the board members and found them to be cohesive, with shared visions of
continually improving care for patients and promoting the wellbeing of their workforce. It was
overwhelmingly evident that the board were all proud of the staff working within the organisation.
Both the executive directors and non-executive directors (NEDs), had the relevant operational and
financial experience, and organisational knowledge.
Leaders were aware of their current priorities and challenges leading up to the merger of the three
trusts. They had identified actions required to address them, which included sharing of good
practice, staff and building on areas of joint working not only for the benefit of Mid Essex Hospitals
Trust but for all three trusts. For example, leaders from the three trusts were implementing a
consistent approach to the use of bank and agency staff to support their own workforce and to
provide safe care to patients.
Although plans for the merger had been delayed due to a referral to the Secretary of State (of
which had now been resolved), leaders had continued working towards clinical reconfiguration and
pre-merger work. Two services were due to be reconfigured and go live; some planned
orthopaedics from December 2019 and vascular surgery pathways from January 2020 and
planned orthopaedic surgery.
The trust had a fit and proper persons policy that was in date and referenced. We reviewed five
personal files of executives to determine if employment checks had been performed in accordance
with the Fit and Proper Persons Requirement (FPPR) (Regulation 5 of the Health and Social Care
Act (Regulated Activities) Regulations 2014). This process ensured that directors are fit and
proper to carry out their role. We observed that FPPR checks were in place. The employment
process also included enhanced Disclosure and Barring Service (DBS) checks, insolvency and
bankruptcy checks, disqualified director register checks and occupational health checks of
directors appointed to the board. Further checks included annual self-declarations for additional
assurance.
It was evident from speaking with staff that the site leadership team, managers and staff worked
together to deliver a shared vision and used their individual strengths to improve services.
The trust had an operational structure which had five divisions; corporate operations, medicine
and emergency care, surgical anaesthetics and theatres, women and children’s, and burns,
plastics and outpatients. The divisions were encouraged and supported by the site leadership
team to take responsibility for their own their performance. A triumvirate team, consisting of a
divisional director, an associate director of operations and a divisional head of nursing/midwifery
led each division. The triumvirate team for each division were supported at a local level by
operational managers and matrons.
20190416 900885 Post-inspection Evidence appendix template v4 Page 5
The executives had appointed ten group clinical directors specifically to lead the changes of
service provision within their divisions across the three sites post-merger. All of the group clinical
directors were passionate about their role; however, some wanted more clarity of managerial
responsibilities from the executives.
The chief pharmacist (CP) we spoke with was managed by the medical director and had good
engagement with the trust executive and awareness of medicines optimisation challenges and
business plan.
Vision and strategy
The board and site senior leadership team had set a clear strategy for the forthcoming
merger. Their vision and values that were at the heart of all the work within the trust. They
were working hard to make sure staff at all levels understood the values in relation to their
daily roles.
The executive team had developed a Mid and South Essex, (MSE) strategy for the three hospital
trusts. The CEO told us: ‘Our ambition is to improve health and wellbeing through excellent,
financially sustainable services, provided by staff supported to develop, innovate and build
rewarding careers.’ The strategy had been developed with stakeholders, staff and consulted on
through engagement with the public.
There were four overarching strategic objectives:
• MSE Objective1:
Be a single, well led, high performing and innovative organisation which joins up care for
the people we serve.
• MSE Objective 2:
Deliver high quality, safe and responsive services shaped by best practice and our local
communities.
• MSE Objective 3:
Be an employer of choice for a supported, engaged and high-performing workforce.
• MSE Objective 4:
Be effective and efficient with all our resources, creating an organisation that residents and
staff can rely on for the long term.
We reviewed board agendas, board meeting minutes, board papers and a range of documents
including the board assurance framework. The board assurance framework is a key mechanism
which the board used to reinforce strategic focus and improve management of risk. All of which
referenced the strategic objectives which meant these were reflected during board meetings.
The trust was proud of their development of their transformation programme All the executives and
leaders we spoke with had a shared vision to integrate and reconfigure services for seamless care
and improved outcomes for patients.
20190416 900885 Post-inspection Evidence appendix template v4 Page 6
There was a trust medicines optimisation strategy monitored by the chief pharmacist. This
included for example, optimisation of the pharmacy workforce. Leaders recognised the need for
staff development and training to ensure safe and effective delivery of medicines optimisation.
We reviewed board minutes from September 2019, which showed detailed minutes were taken.
We attended a board meeting during our inspection, it was apparent that non-executive directors
were confident to make appropriate challenges, for example, non-executives asked for clarity and
assurances on a number of occasions.
Culture
Leaders across the trust continued to work to promote a positive culture that supported
and valued staff.
We found an improvement in culture during our inspection. The majority of staff told us culture was
positive since the appointment of the new site leadership team. Staff were more positive of the
proposed merger and spoke positively about new opportunities and sustainable services for
patients.
At our previous inspection we found that there had been some delays in some of the human
resource processes. Staff told us that there were some continued delays with human resource
processes in regard to the recruitment of staff although there had been improvements since our
last inspection.
The trust held daily staff briefings to encourage staff engagement and share important information
with staff, for example, feedback and learning from incidents. We observed these meetings and
saw good attendance from all grades of staff.
The executive team demonstrated a shared vision and encouraged and motivated staff to improve
and succeed. The trust had a chief transformation officer and had recruited further transformation
directors to improve relations with internal and external stakeholders to facilitate improvement
projects.
Directorate leaders we spoke with were all positive about the future merger and felt confident and
supported by the site leadership team to make improvements and changes within their own
services.
Freedom to speak-up guardians (FTSUG) were introduced following Sir Robert Francis’s
‘Freedom to Speak-up Review’ (2015). Their role is to work with leadership teams to create a
culture where people can speak-up to protect patient safety. The executive team recognised the
importance for staff to have a voice and be able to speak up freely. The trust recruited an external
company to facilitate and manage whistleblowing enquiries 24 hours a day. The company reported
directly to the trust’s people and organisational development committee. The company produced a
quarterly update and an annual report, from July 2018 to July 2019, 21 cases were reported. Staff
told us they were confident to report any concerns they had.
Appraisals were in place for providing executives with high quality annual reviews which included
career development conversations and setting objectives for the next year. All executives and
senior leaders told us that they had received a meaningful appraisal.

20190416 900885 Post-inspection Evidence appendix template v4 Page 7
The trust had a ‘Being Open and Duty of Candour policy’ in place. The duty of candour is a
regulatory duty that relates to openness and transparency and requires providers of health and
social care services to notify patients (or other relevant persons) of certain ‘notifiable safety
incidents’ and provide reasonable support to that person. During our core service inspection staff
explained the process and were aware of their responsibilities. We reviewed five serious incident
investigation reports and all had details that duty of candour had been followed correctly.
Staff told us throughout our core service inspection there was a no blame culture. They also stated
staff were actively encouraged to raise concerns and report incidents without fear of retribution.
Executives, the site leadership team and managers encouraged staff to be open and honest in
relation to issues arising and to challenge poor practice. We found in all serious incident reports
we reviewed that families and carers had been contacted explanations and an apology were
given. The patient and or families were invited to be part of the investigation process.
The majority of staff told us the site leadership team were approachable and visible, although they
would like the non-executive directors and executive team to be more visible. Executives were
aware of the challenges of being visible across the three trusts and had written a paper to try to
address staff concerns. Proposed improvements where the introduction of a walk about prior to
executive meetings which alternate at each trust, attending the morning team briefings and
offering mentoring and reverse mentoring to staff. To monitor compliance leaders kept a log when
the senior leaders and executives visited areas within the trust.
Staff side were active within the trust and held bi-monthly meetings with representation from the
chairs from the three trusts due to merge. The chairs met with the chief nurse, however, they
would like regular attendance from more of the executive directors. We were told that because of
this decision making and the pace of change was delayed.
Leaders told us that the non-executive directors, the executive team and the site leadership team
visited clinical and non clinical areas. Following a visit feedback was provided to the relevant
divisional teams.
Staff Diversity
The trust provided the following breakdowns of medical and dental staff, qualified nursing and
midwifery staff and qualified allied health professionals by ethnic group:
Ethnic group Medical and
dental staff (%) Qualified nursing
midwifery staff (%) Qualified allied health
professionals (%)
White British / Irish / Any other white background
25% 70% 83%
BME - British 23% 13% 4%
BME – Non-British 7% 2% 2%
Not stated 44% 15% 11%
(Source: Routine Provider Information Request (RPIR) – Diversity tab)

20190416 900885 Post-inspection Evidence appendix template v4 Page 8
NHS Staff Survey 2018 results – Summary scores
The following illustration shows how this provider compares with other similar providers on ten key
themes from the survey. Possible scores range from one to ten – a higher score indicates a better
result.
The trust’s scores were significantly lower (worse) than similar trusts in the 2018 staff survey for safe environment – bullying and harassment and staff engagement and about the same for the remaining eight themes.
There were no themes where the trust’s scores were significantly higher (better) or lower (worse)
when compared to the 2017 staff survey:
(Source: NHS Staff Survey 2018)
Leaders were disappointed with the outcome of the staff survey 2018, they felt they had
implemented a robust strategy for the merger, which had incorporated staff engagement plan. The
trust had developed a comprehensive action plan to address key areas for example, improving
communication, and dignity and respect. Actions were aligned to a member of staff with
timescales to adhere to.

20190416 900885 Post-inspection Evidence appendix template v4 Page 9
Leaders told us that they were proud of their teams and staff resilience was commended. Senior
managers felt that the workforce were coping well under extreme pressures. Earlier this year the
trust had a mass recruitment drive to employ over 190 overseas nurses. Although not reflected in
this survey leaders were confident that staff would feel the benefits and reduced work pressures
once all the nurses had started work.
Staff and leaders told us of regular staff engagement events to inform staff of the progress to the
merger of the three trusts. Communication to staff was in a variety of formats, face to face, by
email and social media platforms.
Workforce race equality standard
The Workforce Race Equality Standard (WRES) became compulsory for all NHS trusts in April
2015. Trusts have to show progress against nine measures of equality in the workforce.
The scores presented below are indicators relating to the comparative experiences of white and
black and minority ethnic (BME) staff, as required for the Workforce Race Equality Standard.
The data for indicators 1 to 4 and indicator 9 is supplied to CQC by NHS England, based on data
from the Electronic Staff Record (ESR) or supplied by trusts to the NHS England WRES team,
while indicators 5 to 8 are included in the NHS Staff Survey.
Notes relating to the scores:
• These scores are un-weighted, or not adjusted.
• There are nine WRES metrics which we display as 10 indicators. However, not all
indicators are available for all trusts; for example, if the trust has less than 11 responses
for a staff survey question, then the score would not be published.
• Note that the questions are not all oriented the same way: for 1a, 1b, 2, 4 and 7, a higher
percentage is better while for indicators 3, 5, 6 and 8 a higher percentage is worse.
• The presence of a statistically significant difference between the experiences of BME and
White staff may be caused by a variety of factors. Whether such differences are of
regulatory significance will depend on individual trusts' circumstances.
20190416 900885 Post-inspection Evidence appendix template v4 Page 10
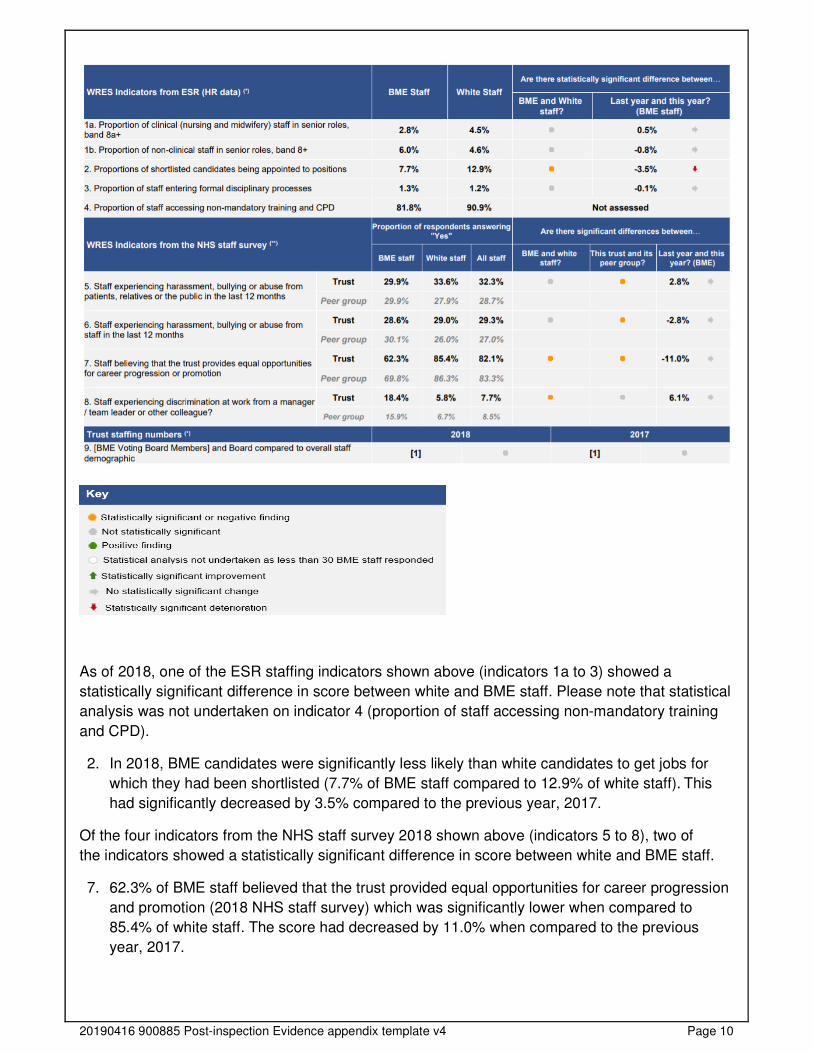
As of 2018, one of the ESR staffing indicators shown above (indicators 1a to 3) showed a
statistically significant difference in score between white and BME staff. Please note that statistical
analysis was not undertaken on indicator 4 (proportion of staff accessing non-mandatory training
and CPD).
2. In 2018, BME candidates were significantly less likely than white candidates to get jobs for
which they had been shortlisted (7.7% of BME staff compared to 12.9% of white staff). This
had significantly decreased by 3.5% compared to the previous year, 2017.
Of the four indicators from the NHS staff survey 2018 shown above (indicators 5 to 8), two of
the indicators showed a statistically significant difference in score between white and BME staff.
7. 62.3% of BME staff believed that the trust provided equal opportunities for career progression
and promotion (2018 NHS staff survey) which was significantly lower when compared to
85.4% of white staff. The score had decreased by 11.0% when compared to the previous
year, 2017.
20190416 900885 Post-inspection Evidence appendix template v4 Page 11
8. 18.4% of BME staff experienced discrimination from a colleague or manager in the past year
(2018 NHS staff survey) which was significantly higher when compared to 5.8% of white staff.
The score had increased by 6.1% when compared to the previous year, 2017.
There was one BME Voting Board Members at the trust, which was not significantly different to the
number expected, based on the overall percentage of BME staff.
(Source: NHS Staff Survey 2018; NHS England)
In response to the survey the trust had developed a workforce standard action plan, for example,
black, Asian and ethnic minority training was given to all recruiting line managers. The trust
introduced diversity and inclusion champions as part of recruitment panels. Actions were aligned
to a lead with timelines to achieve.
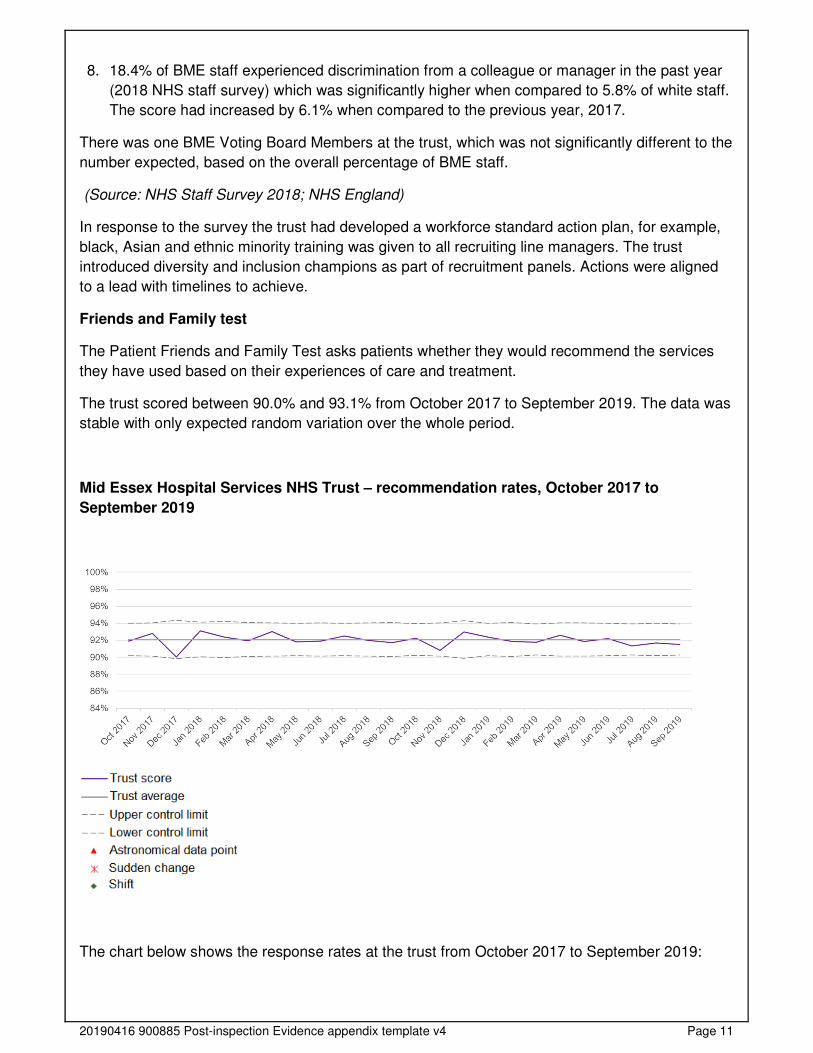
Friends and Family test
The Patient Friends and Family Test asks patients whether they would recommend the services
they have used based on their experiences of care and treatment.
The trust scored between 90.0% and 93.1% from October 2017 to September 2019. The data was
stable with only expected random variation over the whole period.
Mid Essex Hospital Services NHS Trust – recommendation rates, October 2017 to
September 2019
The chart below shows the response rates at the trust from October 2017 to September 2019:
20190416 900885 Post-inspection Evidence appendix template v4 Page 12
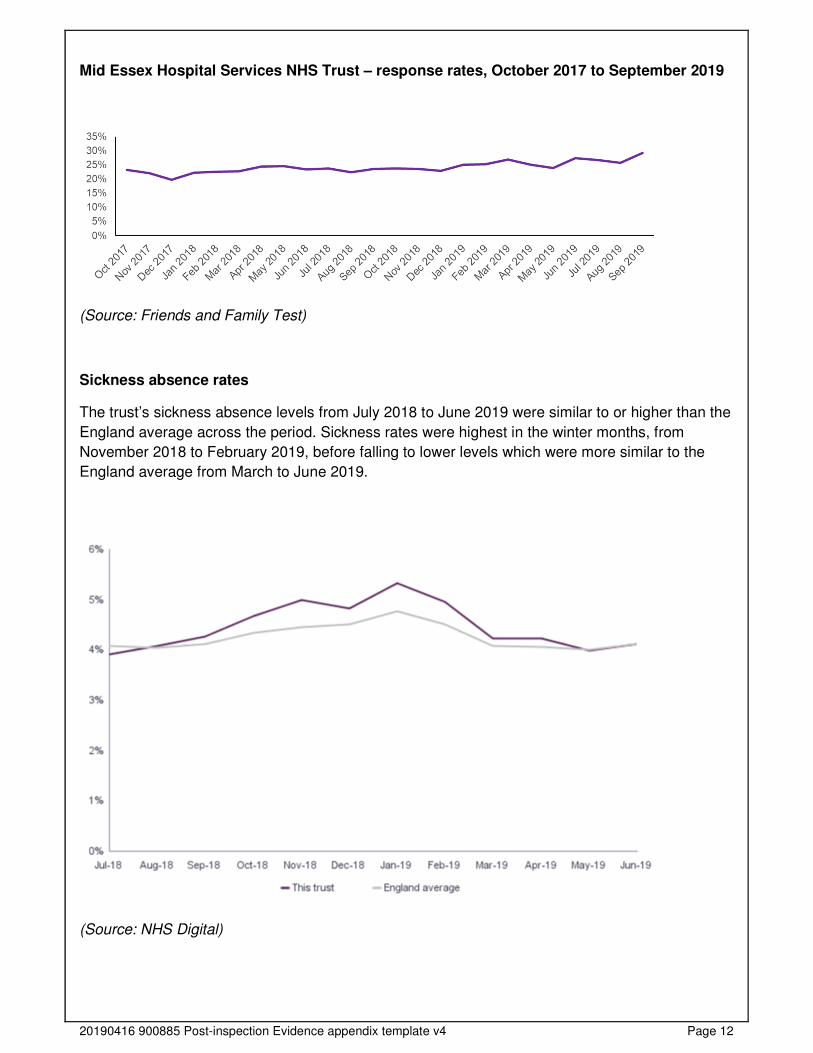
Mid Essex Hospital Services NHS Trust – response rates, October 2017 to September 2019
(Source: Friends and Family Test)
Sickness absence rates
The trust’s sickness absence levels from July 2018 to June 2019 were similar to or higher than the
England average across the period. Sickness rates were highest in the winter months, from
November 2018 to February 2019, before falling to lower levels which were more similar to the
England average from March to June 2019.
(Source: NHS Digital)

20190416 900885 Post-inspection Evidence appendix template v4 Page 13
General Medical Council – National Training Scheme Survey
In the 2019 General Medical Council Survey the trust performed worse than expected for two
indicators (curriculum coverage and local teaching), and the same as expected for the remaining
16 indicators.
(Source: General Medical Council National Training Scheme Survey)
The trust had a ‘Guardian of Safe Working Hours’ for junior doctors. The guardian’s role was to
ensure that providers identify and respond to issues around safe medical staffing, to deliver quality
care and keep patients and staff safe from avoidable harm. Safeguards around working hours of
doctors in training (junior doctors) had been designed to ensure that the risk was effectively
mitigated and that this mitigation was assured. The trust guardian reported to the medical director,
reviewed themes and trends from feedback from junior doctors. Since our last inspection the
guardian told us reporting had increased from 30% to 50%. This increase was following a
campaign through engagement meetings with junior doctors, the trust provided ‘pizza and pay slip’
meetings to highlight the importance of reporting.
Governance
The trust had a structure for overseeing performance, quality and risk, with a site
leadership managing director board member representing the trust at board level. This
gave them greater oversight of issues facing the services and they responded when
services needed more support.
Leaders operated effective governance processes, throughout the trust and with partner
organisations. Staff at all levels were clear about their roles and accountabilities. Staff had regular
opportunities to meet, discuss and learn from the performance of the service.
Executives told us over the last year since the formation of the site leadership team, they have
focused on developing management, leadership and governance within the trust to enable a
strong focus on integrated governance structures.
A trust governance improvement plan was in place and the senior team had implemented a plan
which was now embedded to provide a more consistent approach to governance across the MSB
group.
There were structures and systems in place to monitor governance and accountability throughout
the organisation to support the delivery of the strategy. There were site level divisional quality and
governance meetings, which reported to the site clinical outcomes and effectiveness meeting and
the corporate governance meeting which reported to the site governance forum and into the
quality committees in common (board level for the three trusts). This structure ensured that there
was board level oversight across the three hospital trusts through input from each of the managing
directors and other senior staff at the individual hospital.
The trust had an ‘Information Governance Strategy’ which incorporated an annual information
governance work plan. An information governance staff handbook was available on the staff
intranet and a weekly staff newsletter. All information governance policies had been reviewed and
aligned which included compliance with the General Data Protection Regulation and Data
Protection Act 2018.
20190416 900885 Post-inspection Evidence appendix template v4 Page 14
Governance arrangements for infection prevention control (IPC) had improved since our last
inspection. The IPC leadership team was strengthened and monitored by the director of nursing.
Leaders told us that systems have been embedded throughout the trust. The trust had recently
been reviewed by the IPC team at NHSI/E and had moved from being rated as red to green.
Papers and reports for board meetings and other committees, that we reviewed, were of a good
standard and contained appropriate information. For example, we reviewed three finance and
performance committee in common minutes from May to July 2019 and saw that the financial risks
on the BAF were discussed.
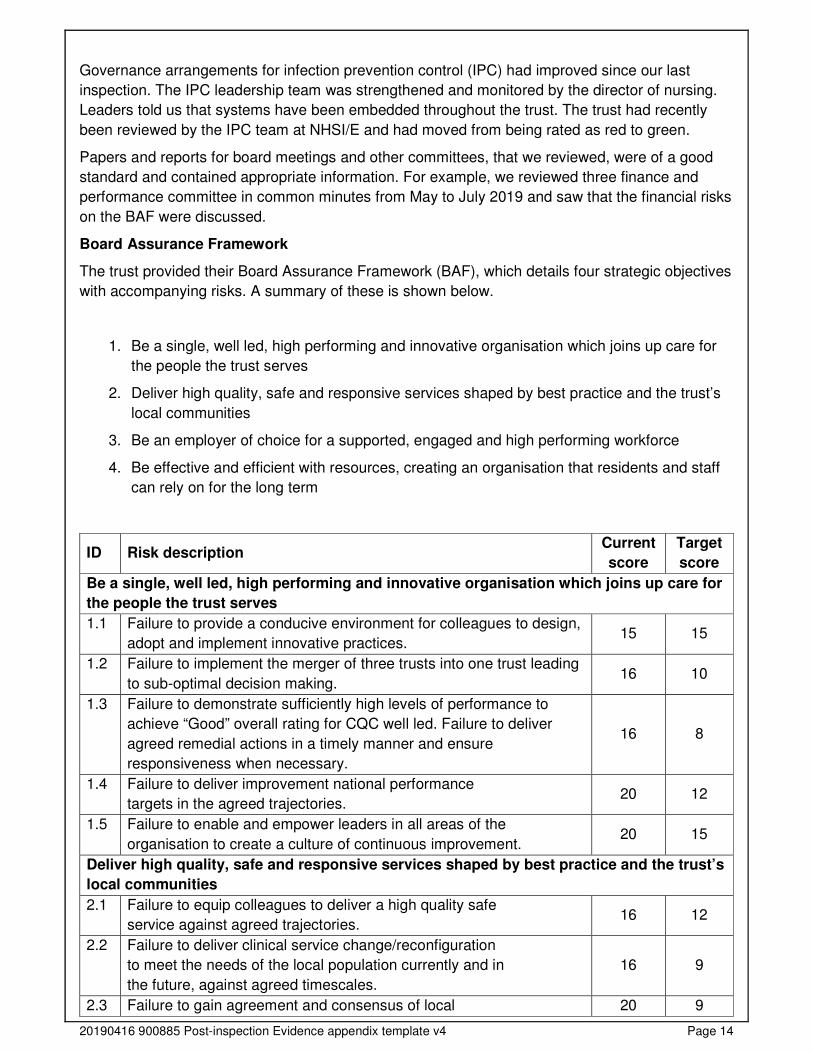
Board Assurance Framework
The trust provided their Board Assurance Framework (BAF), which details four strategic objectives
with accompanying risks. A summary of these is shown below.
1. Be a single, well led, high performing and innovative organisation which joins up care for
the people the trust serves
2. Deliver high quality, safe and responsive services shaped by best practice and the trust’s
local communities
3. Be an employer of choice for a supported, engaged and high performing workforce
4. Be effective and efficient with resources, creating an organisation that residents and staff
can rely on for the long term
ID Risk description Current
score
Target
score
Be a single, well led, high performing and innovative organisation which joins up care for
the people the trust serves
1.1 Failure to provide a conducive environment for colleagues to design,
adopt and implement innovative practices. 15 15
1.2 Failure to implement the merger of three trusts into one trust leading
to sub-optimal decision making. 16 10
1.3 Failure to demonstrate sufficiently high levels of performance to
achieve “Good” overall rating for CQC well led. Failure to deliver
agreed remedial actions in a timely manner and ensure
responsiveness when necessary.
16 8
1.4 Failure to deliver improvement national performance
targets in the agreed trajectories. 20 12
1.5 Failure to enable and empower leaders in all areas of the
organisation to create a culture of continuous improvement. 20 15
Deliver high quality, safe and responsive services shaped by best practice and the trust’s
local communities
2.1 Failure to equip colleagues to deliver a high quality safe
service against agreed trajectories. 16 12
2.2 Failure to deliver clinical service change/reconfiguration
to meet the needs of the local population currently and in
the future, against agreed timescales.
16 9
2.3 Failure to gain agreement and consensus of local 20 9
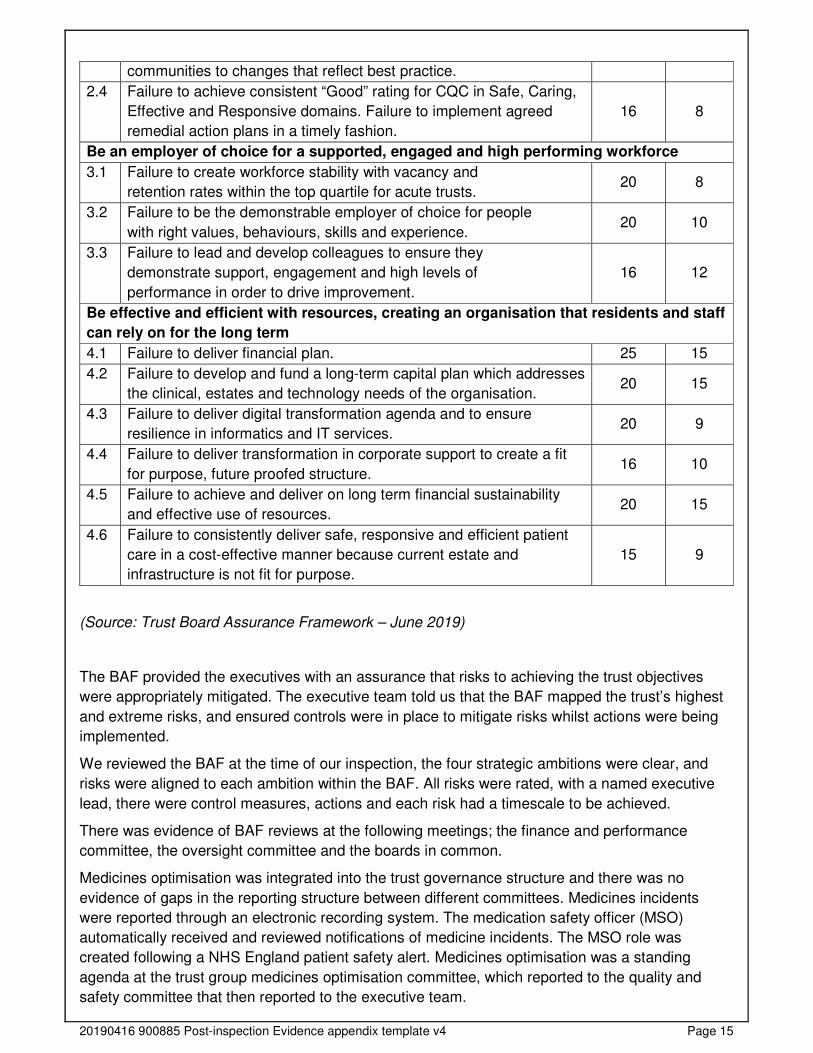
20190416 900885 Post-inspection Evidence appendix template v4 Page 15
communities to changes that reflect best practice.
2.4 Failure to achieve consistent “Good” rating for CQC in Safe, Caring,
Effective and Responsive domains. Failure to implement agreed
remedial action plans in a timely fashion.
16 8
Be an employer of choice for a supported, engaged and high performing workforce
3.1 Failure to create workforce stability with vacancy and
retention rates within the top quartile for acute trusts. 20 8
3.2 Failure to be the demonstrable employer of choice for people
with right values, behaviours, skills and experience. 20 10
3.3 Failure to lead and develop colleagues to ensure they
demonstrate support, engagement and high levels of
performance in order to drive improvement.
16 12
Be effective and efficient with resources, creating an organisation that residents and staff
can rely on for the long term
4.1 Failure to deliver financial plan. 25 15
4.2 Failure to develop and fund a long-term capital plan which addresses
the clinical, estates and technology needs of the organisation. 20 15
4.3 Failure to deliver digital transformation agenda and to ensure
resilience in informatics and IT services. 20 9
4.4 Failure to deliver transformation in corporate support to create a fit
for purpose, future proofed structure. 16 10
4.5 Failure to achieve and deliver on long term financial sustainability
and effective use of resources. 20 15
4.6 Failure to consistently deliver safe, responsive and efficient patient
care in a cost-effective manner because current estate and
infrastructure is not fit for purpose.
15 9
(Source: Trust Board Assurance Framework – June 2019)
The BAF provided the executives with an assurance that risks to achieving the trust objectives
were appropriately mitigated. The executive team told us that the BAF mapped the trust’s highest
and extreme risks, and ensured controls were in place to mitigate risks whilst actions were being
implemented.
We reviewed the BAF at the time of our inspection, the four strategic ambitions were clear, and
risks were aligned to each ambition within the BAF. All risks were rated, with a named executive
lead, there were control measures, actions and each risk had a timescale to be achieved.
There was evidence of BAF reviews at the following meetings; the finance and performance
committee, the oversight committee and the boards in common.
Medicines optimisation was integrated into the trust governance structure and there was no
evidence of gaps in the reporting structure between different committees. Medicines incidents
were reported through an electronic recording system. The medication safety officer (MSO)
automatically received and reviewed notifications of medicine incidents. The MSO role was
created following a NHS England patient safety alert. Medicines optimisation was a standing
agenda at the trust group medicines optimisation committee, which reported to the quality and
safety committee that then reported to the executive team.
20190416 900885 Post-inspection Evidence appendix template v4 Page 16
Following our inspection we reviewed the minutes of meetings such as but not limited to; the
mortality review group, the audit committee, the finance and performance committee in common,
and the boards in common (closed), and observed they did not follow the same format for minute
meeting templates. Attendance was good, actions were identified and allocated to staff, however,
timelines and progress were not always clearly identifiable.
Management of risk, issues and performance
Leaders and teams used systems to manage performance effectively. They identified and
escalated relevant risks and issues and identified actions to reduce their impact. They had
plans to cope with unexpected events. Staff contributed to decision-making to help avoid
financial pressures compromising the quality of care.
Governance meetings were held at service and division level which were reviewed at a monthly
division board. The division was led by a triumvirate including the divisional director, associate
director of nursing/head of midwifery and associate director. The site leadership team received risk
based exception reports, which contained for example, non-compliance to national best practice,
this meant executives monitored progress against actions implemented.
The trust had a policy for the management of incidents and serious incidents. Throughout our core
service and well led inspection we observed embedded systems within the trust to identify learning
from incidents and complaints.
All divisions produced patient and safety quality dashboards to enable reviews from ward to board
level. Wards held safety huddles to highlight any real time safety issues. The patient and safety
committee received a board performance report and provided assurance to the board.
We reviewed the trusts quality account for the year ending March 2019. It was comprehensive and
covered statements on quality, priorities for improvement and a review of quality performance from
March 2018 to March 2019. We saw quality improvements included for example, the
commencement of elective orthopaedics services and Braintree hospital which reduced the
number of cancellations and optimised the use of theatres and wards at that site.
Finances Overview
The executive team told us financial outcomes had an overarching group deficit, with the majority
belonging to Mid Essex hospital trust. Leaders recognised that their challenge was the successful
delivery of the trust’s cost improvement programme (CIP) plan and engaging clinicians to part of
the process.
Finance was discussed at local and divisional governance meetings, divisions discussed their
financial plans and delivery of their CIPs. The site leadership teams and executive team told us
that each CIP was subject to a quality assessment and would not be agreed if it compromised the
quality of patient care.
The trust had reviewed agency staffing spend and put in financial controls which capped agency
costs in the region, this had reduced spend from £17m to £18m last year to £10m this year.
Leaders were confident in reducing agency staffing spend further once all of the overseas nurses
had started work.
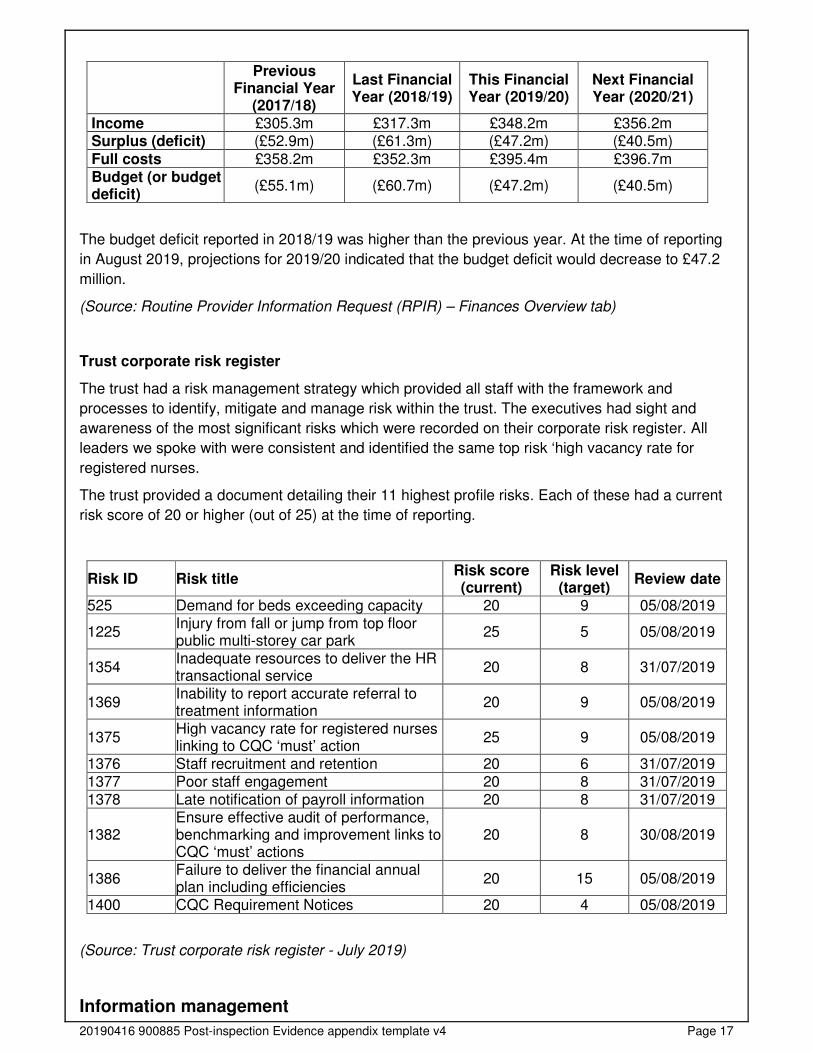
Financial metrics Historical data Projections
20190416 900885 Post-inspection Evidence appendix template v4 Page 17
Previous Financial Year
(2017/18)
Last Financial Year (2018/19)
This Financial Year (2019/20)
Next Financial Year (2020/21)
Income £305.3m £317.3m £348.2m £356.2m Surplus (deficit) (£52.9m) (£61.3m) (£47.2m) (£40.5m)
Full costs £358.2m £352.3m £395.4m £396.7m Budget (or budget deficit)
(£55.1m) (£60.7m) (£47.2m) (£40.5m)
The budget deficit reported in 2018/19 was higher than the previous year. At the time of reporting
in August 2019, projections for 2019/20 indicated that the budget deficit would decrease to £47.2
million.
(Source: Routine Provider Information Request (RPIR) – Finances Overview tab)
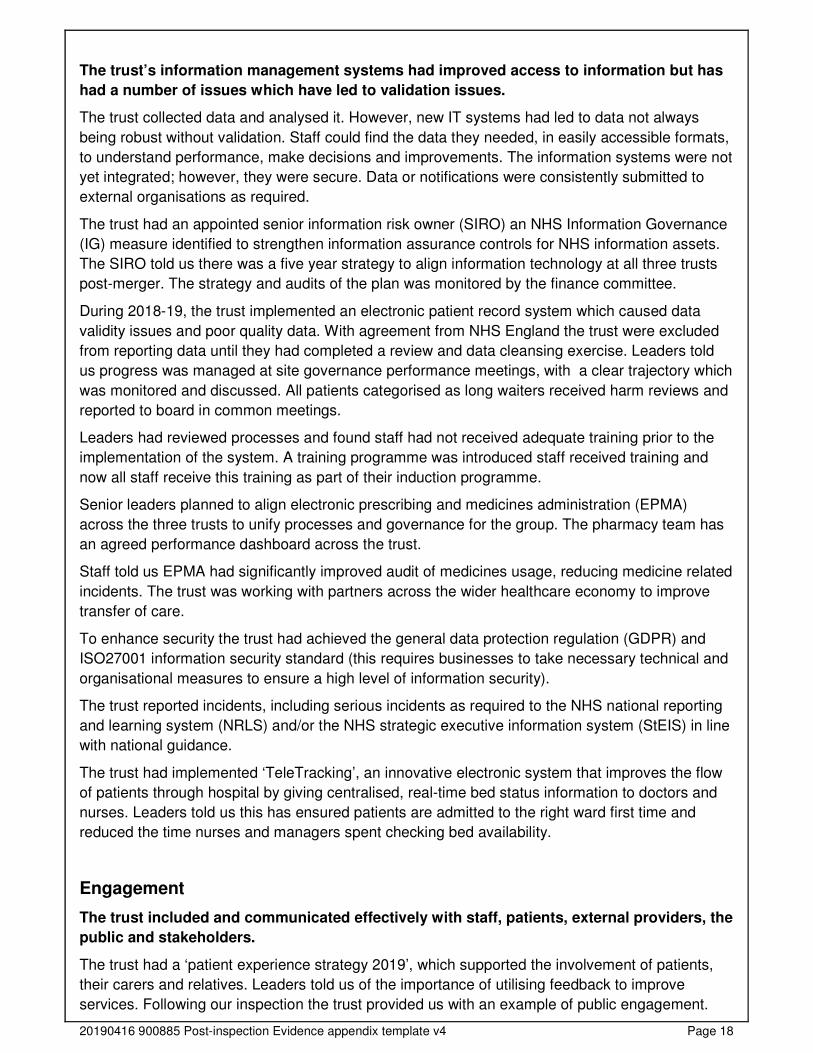
Trust corporate risk register
The trust had a risk management strategy which provided all staff with the framework and
processes to identify, mitigate and manage risk within the trust. The executives had sight and
awareness of the most significant risks which were recorded on their corporate risk register. All
leaders we spoke with were consistent and identified the same top risk ‘high vacancy rate for
registered nurses.
The trust provided a document detailing their 11 highest profile risks. Each of these had a current
risk score of 20 or higher (out of 25) at the time of reporting.
Risk ID Risk title Risk score (current)
Risk level (target)
Review date
525 Demand for beds exceeding capacity 20 9 05/08/2019
1225 Injury from fall or jump from top floor public multi-storey car park
25 5 05/08/2019
1354 Inadequate resources to deliver the HR transactional service
20 8 31/07/2019
1369 Inability to report accurate referral to treatment information
20 9 05/08/2019
1375 High vacancy rate for registered nurses linking to CQC ‘must’ action
25 9 05/08/2019
1376 Staff recruitment and retention 20 6 31/07/2019 1377 Poor staff engagement 20 8 31/07/2019 1378 Late notification of payroll information 20 8 31/07/2019
1382 Ensure effective audit of performance, benchmarking and improvement links to CQC ‘must’ actions
20 8 30/08/2019
1386 Failure to deliver the financial annual plan including efficiencies
20 15 05/08/2019
1400 CQC Requirement Notices 20 4 05/08/2019
(Source: Trust corporate risk register - July 2019)
Information management
20190416 900885 Post-inspection Evidence appendix template v4 Page 18
The trust’s information management systems had improved access to information but has
had a number of issues which have led to validation issues.
The trust collected data and analysed it. However, new IT systems had led to data not always
being robust without validation. Staff could find the data they needed, in easily accessible formats,
to understand performance, make decisions and improvements. The information systems were not
yet integrated; however, they were secure. Data or notifications were consistently submitted to
external organisations as required.
The trust had an appointed senior information risk owner (SIRO) an NHS Information Governance
(IG) measure identified to strengthen information assurance controls for NHS information assets.
The SIRO told us there was a five year strategy to align information technology at all three trusts
post-merger. The strategy and audits of the plan was monitored by the finance committee.
During 2018-19, the trust implemented an electronic patient record system which caused data
validity issues and poor quality data. With agreement from NHS England the trust were excluded
from reporting data until they had completed a review and data cleansing exercise. Leaders told
us progress was managed at site governance performance meetings, with a clear trajectory which
was monitored and discussed. All patients categorised as long waiters received harm reviews and
reported to board in common meetings.
Leaders had reviewed processes and found staff had not received adequate training prior to the
implementation of the system. A training programme was introduced staff received training and
now all staff receive this training as part of their induction programme.
Senior leaders planned to align electronic prescribing and medicines administration (EPMA)
across the three trusts to unify processes and governance for the group. The pharmacy team has
an agreed performance dashboard across the trust.
Staff told us EPMA had significantly improved audit of medicines usage, reducing medicine related
incidents. The trust was working with partners across the wider healthcare economy to improve
transfer of care.
To enhance security the trust had achieved the general data protection regulation (GDPR) and
ISO27001 information security standard (this requires businesses to take necessary technical and
organisational measures to ensure a high level of information security).
The trust reported incidents, including serious incidents as required to the NHS national reporting
and learning system (NRLS) and/or the NHS strategic executive information system (StEIS) in line
with national guidance.
The trust had implemented ‘TeleTracking’, an innovative electronic system that improves the flow
of patients through hospital by giving centralised, real-time bed status information to doctors and
nurses. Leaders told us this has ensured patients are admitted to the right ward first time and
reduced the time nurses and managers spent checking bed availability.
Engagement
The trust included and communicated effectively with staff, patients, external providers, the
public and stakeholders.
The trust had a ‘patient experience strategy 2019’, which supported the involvement of patients,
their carers and relatives. Leaders told us of the importance of utilising feedback to improve
services. Following our inspection the trust provided us with an example of public engagement.
20190416 900885 Post-inspection Evidence appendix template v4 Page 19
Relatives whose loved ones had passed away attended an event to share their experiences. Both
positive and negative experiences were captured and used to feedback to staff.
Leaders and staff we spoke with told us the trust had held engagement events to inform staff of
the changes to services in advance of the merger. In addition moving forward at mid daily meeting
continued to give staff the opportunity to share information and good practice across the
organisation.
The chief nurse told us in partnership with the chief medical officer they led clinical reconfiguration
workshops, to enable staff to be part of the journey and development of services into the merger.
Leaders and clinicians told us the merger is now a reality and more staff are involved and excited
about the opportunities which will result post-merger.
The trust had a strong volunteer service, who provided administrative assistance, supported
patients on arrival to the hospital, and staff in the clinical areas.
There was evidence of working with external stakeholders, for example, Healthwatch (the
independent champion for health and social care users) attended the trust’s patient experience
group meetings.
Social media platforms were utilised by the organisation as a way of sharing information and
receiving feedback from staff, patients and the public.
The patient council told us the team undertook ward visits to speak to patients about standards of
care they receive. This was fed back to ward managers and the matrons so that concerns could
be acted upon in a timely manner.
The equality and diversity group had been relaunched and now met bi-monthly. The trust had also
instigated the rainbow badge, the NHS rainbow badge aimed to make a positive difference by
promoting a message of inclusion for patients who identify as lesbian, gay, bisexual, transgender
(LGBT).
In the summer of 2019 the trust held an event to create network groups for staff which included,
BME, LGBT, disability and armed forces
The trust had produced a one minute video to promote apprenticeships within the hospital, it
included managers and apprentice’s views. This was launched during national apprenticeship
week.
Leaders gave examples of working with external organisations, nurses and discharge coordinators
worked with local care homes to reduce the number of community acquired pressure ulcers.
We reviewed the ‘Mid and South Essex group interim people strategy 2019 – 2020’ we saw that it
was detailed and aligned to the NHS long term plan and NHS interim people plan launched
January 2019. The strategy included the four main areas of focus:
• Making the NHS the best place to work
• Improving the leadership culture
• Tackling the nursing challenge
• Delivering 21st century care
• A new operating model for workforce
The trust had developed a leaflet for patients and the public which explained why the trust was
merging, all the proposed changes to services and the benefits for patients.

20190416 900885 Post-inspection Evidence appendix template v4 Page 20
Learning, continuous improvement and innovation
The leadership team worked well with the clinical leads and encouraged divisions to share
learning across the services.
Leaders had developed a number of transformational programmes and employed further directors
to encourage innovation and learning across the three trusts. The aim was to improve consistency
of practices and patient outcomes.
In line with national guidance the trust had recruited a medical examiner whose responsibility was
to review all inpatient deaths in line with the national quality board's 'learning from deaths
guidance’. The medical examiner role was to also work closely with the coroner and their
department and share learning across the trust.
The trust has had a history of raised mortality for the last three years. There had been some
coding issues which have been fixed and leaders are confident they are on a pathway of
improving mortality rates.
The pharmacy team worked with external partners and developed an audit tool that can be used
on smart phone. This provided live data to nursing staff on the wards which enabled effective
resolution and implementation of action plans in relation to safe and secure medicines audits.
The trust offered onsite functional skills maths and English classes for staff to access to promote
learning and development.
The trust implemented a scheme to retain staff known as the ‘retire to return initiative’. Staff were
given the option to stage their retirement, the process has been streamlined to enable staff to give
six months’ notice to arrange a package of flexible working to suit their needs.
The trust had signed the armed forces covenant (a promise ensuring that those who serve or who
have served in the armed forces, and their families, are treated fairly) and developed partnership
arrangements. The trust had been informed that they were to receive a military of defence silver
award for its support to the armed forces.
Complaints process overview
We reviewed a sample of complaints during the well led inspection. All patients received an
acknowledgment letter, an apology and an explanation of the trust’s complaints processes. The
final letter sensitively explained which staff were involved in the investigation, their expertise and
details of learning identified, actions and any national or local guideline where appropriate.
The trust was asked to comment on their targets for responding to complaints and current
performance against these targets for the last 12 months.
Question In days Current
performance What is your internal target for responding to complaints? 3 100%
What is your target for completing a complaint 25 65% If you have a slightly longer target for complex complaints please indicate what that is here
60 63%
Number of complaints resolved without formal process in the last 12 months?
August 2018 to July 2019 2,547
20190416 900885 Post-inspection Evidence appendix template v4 Page 21
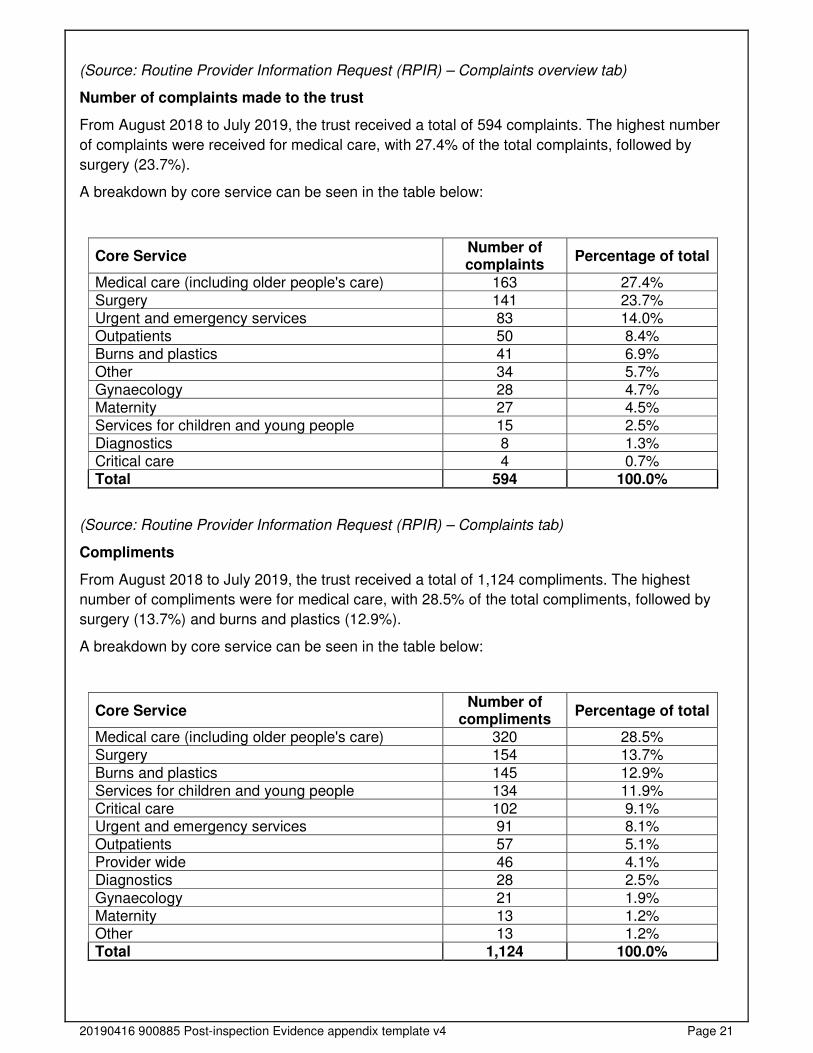
(Source: Routine Provider Information Request (RPIR) – Complaints overview tab)
Number of complaints made to the trust
From August 2018 to July 2019, the trust received a total of 594 complaints. The highest number
of complaints were received for medical care, with 27.4% of the total complaints, followed by
surgery (23.7%).
A breakdown by core service can be seen in the table below:
Core Service Number of complaints
Percentage of total
Medical care (including older people's care) 163 27.4% Surgery 141 23.7% Urgent and emergency services 83 14.0% Outpatients 50 8.4% Burns and plastics 41 6.9% Other 34 5.7% Gynaecology 28 4.7% Maternity 27 4.5% Services for children and young people 15 2.5% Diagnostics 8 1.3% Critical care 4 0.7% Total 594 100.0%
(Source: Routine Provider Information Request (RPIR) – Complaints tab)
Compliments
From August 2018 to July 2019, the trust received a total of 1,124 compliments. The highest
number of compliments were for medical care, with 28.5% of the total compliments, followed by
surgery (13.7%) and burns and plastics (12.9%).
A breakdown by core service can be seen in the table below:
Core Service Number of
compliments Percentage of total
Medical care (including older people's care) 320 28.5% Surgery 154 13.7%
Burns and plastics 145 12.9% Services for children and young people 134 11.9% Critical care 102 9.1% Urgent and emergency services 91 8.1% Outpatients 57 5.1% Provider wide 46 4.1% Diagnostics 28 2.5%
Gynaecology 21 1.9% Maternity 13 1.2% Other 13 1.2% Total 1,124 100.0%
20190416 900885 Post-inspection Evidence appendix template v4 Page 22
The trust stated that most of the compliments received related to overall care along the whole
pathway, with patients and relatives thanking staff for their kindness and compassion
during difficult and stressful times. These related to all staff from housekeepers,
porters and nurses, to consultants.
(Source: Routine Provider Information Request (RPIR) – Compliments)
Accreditations
NHS trusts are able to participate in a number of accreditation schemes whereby the services they
provide are reviewed and a decision is made whether or not to award the service with an
accreditation. A service will be accredited if they are able to demonstrate that they meet a certain
standard of best practice in the given area. An accreditation usually carries an end date (or review
date) whereby the service will need to be re-assessed in order to continue to be accredited.
The table below shows which of the trust’s services are engaged with or have been awarded an
accreditation.
Accreditation scheme name Service accredited
Joint Advisory Group on Endoscopy (JAG) • Achieved in March 2019, renewal
visit planned for October 2019 (service accredited not provided).
Gold Standards Framework Accreditation process, leading to the GSF Hallmark Award in End of Life Care
• Baddow, Feering and Braxted wards have completed the 2-year GSF programme.
• Bardfield ward will commence on the hospitals programme for GSF from October 2019.
Clinical Pathology Accreditation and its successor Medical Laboratories ISO 15189
• Microbiology, blood sciences and histology/mortuary currently accredited.
• Point of Care services is engaged with the scheme but has not yet achieved accreditation.
(Source: Routine Provider Information Request (RPIR) – Accreditations tab).
20190416 900885 Post-inspection Evidence appendix template v4 Page 23
Acute services
Broomfield Hospital
Court Road,
Broomfield,
Chelmsford
CM1 7ET
Tel: 01245362000
www.meht.nhs.uk
Urgent and emergency care
Facts and data about this service
Details of emergency departments and other urgent and emergency care services:
• Broomfield Hospital accident and emergency department
• Broomfield Hospital emergency care therapy
(Source: Routine Provider Information Request (RPIR) – Sites tab)
Emergency care at Broomfield Hospital is based in the emergency village, which comprises: the
adult emergency department (ED), acute medical unit (AMU), ambulatory care unit (ACU), and
emergency short stay ward (ESS) and frailty unit.
Emergency department patients are assessed, prioritised and streamed to agreed locations such
as gynaecology assessment, ACU, surgical assessment and GP within the emergency
department.
The emergency department is part of the East of England trauma network and has four adult
resuscitation bays with 10 acute majors cubicles and eight further majors trolleys. There are five
early senior assessment and treatment (ESAT) cubicles and a mental health interview room.
AMU is the primary route of admission and assessment for GP heralded medical patients with 10
assessment trolleys, two triage rooms and 20 assessment beds, with a target length of stay of less
than 24hrs. The unit is led by acute physicians who also lead the same day emergency care
service in ACU.
The ACU is a seven day service receiving patients streamed and referred from the ED and from
GPs supporting referrals from medical wards to facilitate earlier discharge when clinically
appropriate. There is in-reach into AMU from various specialty medical teams such as cardiology,
and community teams such as hospital at home and early supported discharge admissions
avoidance and resettlement (ESDAAR).
20190416 900885 Post-inspection Evidence appendix template v4 Page 24
Paediatric ED nursing sits within women’s and children’s services. Any child or young person is
triaged by a nurse, and then seen by an ED clinician, emergency nurse practitioner, GP or direct
referral to specialist services. In addition, the children's ED service has appointed four paediatric
consultants to work within the ED department.
(Source: Routine Provider Information Request (RPIR) – Acute context)
We used a variety of methods to help us gather evidence to inspect the emergency services at
Broomfield Hospital. We spoke with 40 members of staff, six patients and two relatives. We
reviewed 19 patient records during this inspection. We interviewed the department leads and we
spoke with a variety of different staff members. We observed the environment, checked the safety
and currency of equipment, we looked at records in relation to patients’ treatment and medication.
We also looked at a range of documents relevant to the service including policies, minutes of
meetings, action plans, risk assessments, and audit results.
Activity and patient throughput
From March 2018 to February 2019 there were 106,255 attendances at the trust’s urgent and
emergency care services as indicated in the chart below.
Total number of urgent and emergency care attendances at Mid Essex Hospital Services
NHS Trust compared to all acute trusts in England, March 2018 to February 2019
(Source: Hospital Episode Statistics)
20190416 900885 Post-inspection Evidence appendix template v4 Page 25
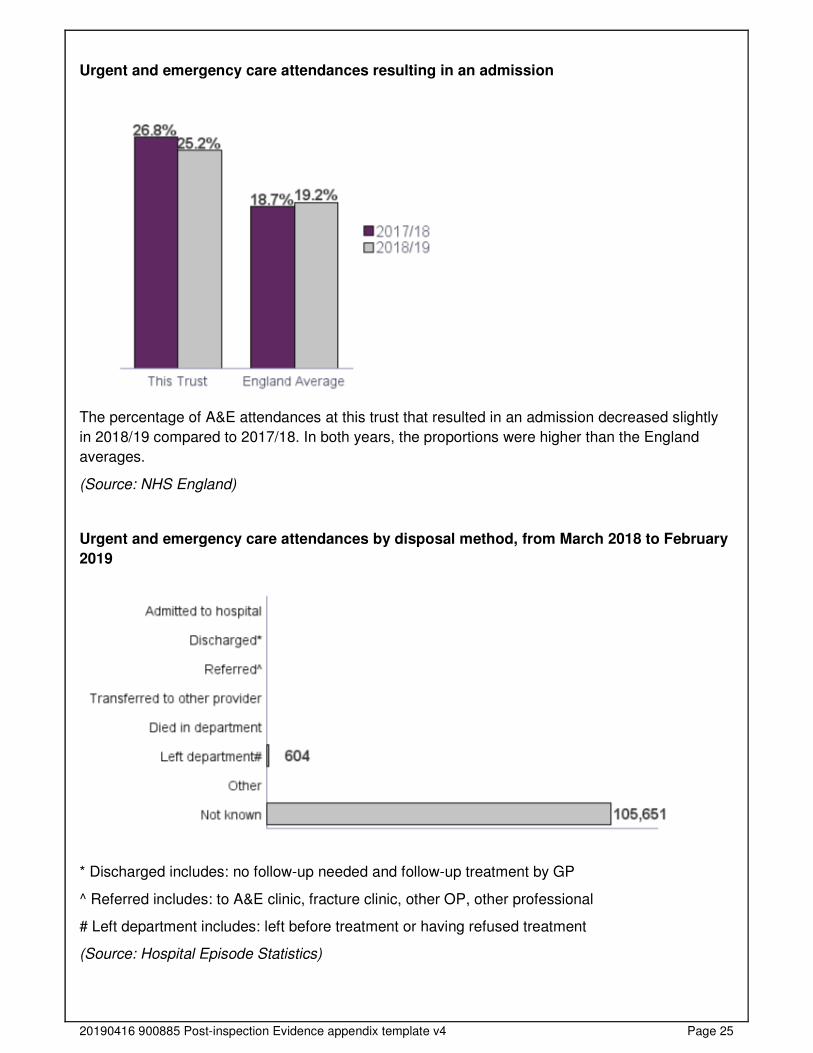
Urgent and emergency care attendances resulting in an admission
The percentage of A&E attendances at this trust that resulted in an admission decreased slightly
in 2018/19 compared to 2017/18. In both years, the proportions were higher than the England
averages.
(Source: NHS England)
Urgent and emergency care attendances by disposal method, from March 2018 to February
2019
* Discharged includes: no follow-up needed and follow-up treatment by GP
^ Referred includes: to A&E clinic, fracture clinic, other OP, other professional
# Left department includes: left before treatment or having refused treatment
(Source: Hospital Episode Statistics)
20190416 900885 Post-inspection Evidence appendix template v4 Page 26
Is the service safe?
By safe, we mean people are protected from abuse* and avoidable harm.
*Abuse can be physical, sexual, mental or psychological, financial, neglect, institutional or
discriminatory abuse.
Mandatory training
The service provided mandatory training in key skills including the highest level of life
support training to all staff, however not everyone had completed it.
Mandatory training completion rates
Nursing staff received and kept up-to-date with their mandatory training.
The trust set a target of 85% for the completion of all mandatory training modules, with the
exception of information governance which had a target of 95%.
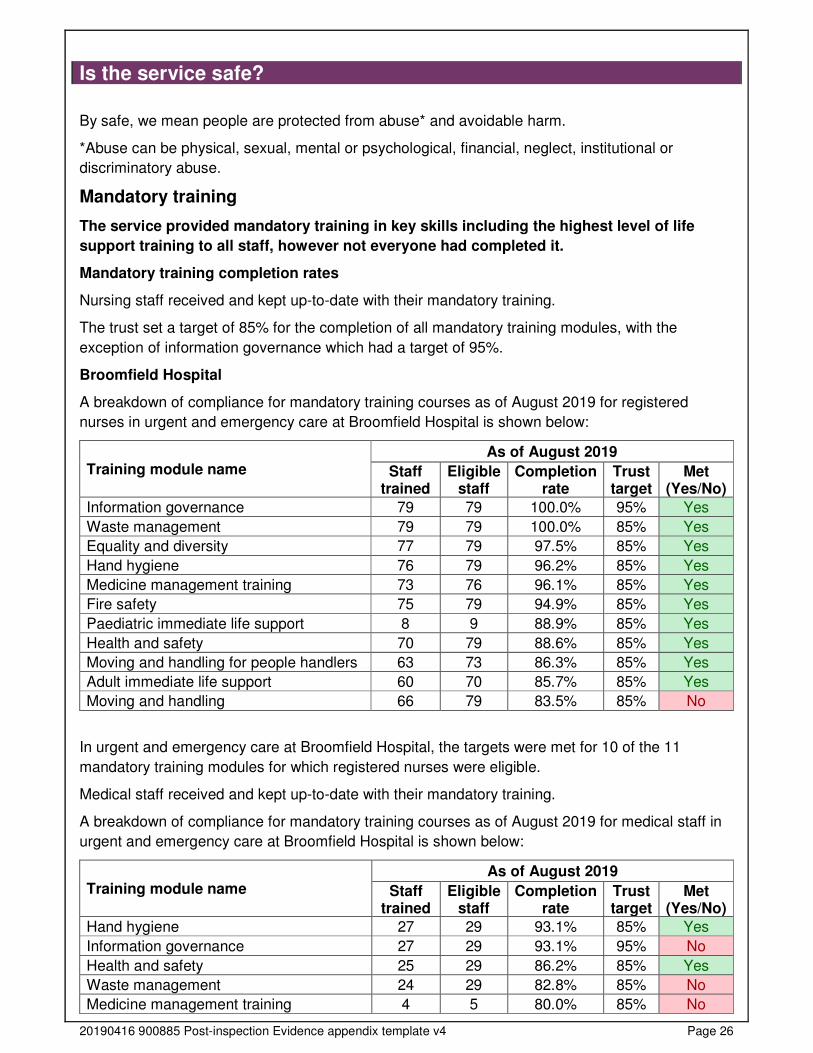
Broomfield Hospital
A breakdown of compliance for mandatory training courses as of August 2019 for registered
nurses in urgent and emergency care at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Information governance 79 79 100.0% 95% Yes
Waste management 79 79 100.0% 85% Yes
Equality and diversity 77 79 97.5% 85% Yes
Hand hygiene 76 79 96.2% 85% Yes
Medicine management training 73 76 96.1% 85% Yes
Fire safety 75 79 94.9% 85% Yes
Paediatric immediate life support 8 9 88.9% 85% Yes
Health and safety 70 79 88.6% 85% Yes
Moving and handling for people handlers 63 73 86.3% 85% Yes
Adult immediate life support 60 70 85.7% 85% Yes
Moving and handling 66 79 83.5% 85% No
In urgent and emergency care at Broomfield Hospital, the targets were met for 10 of the 11
mandatory training modules for which registered nurses were eligible.
Medical staff received and kept up-to-date with their mandatory training.
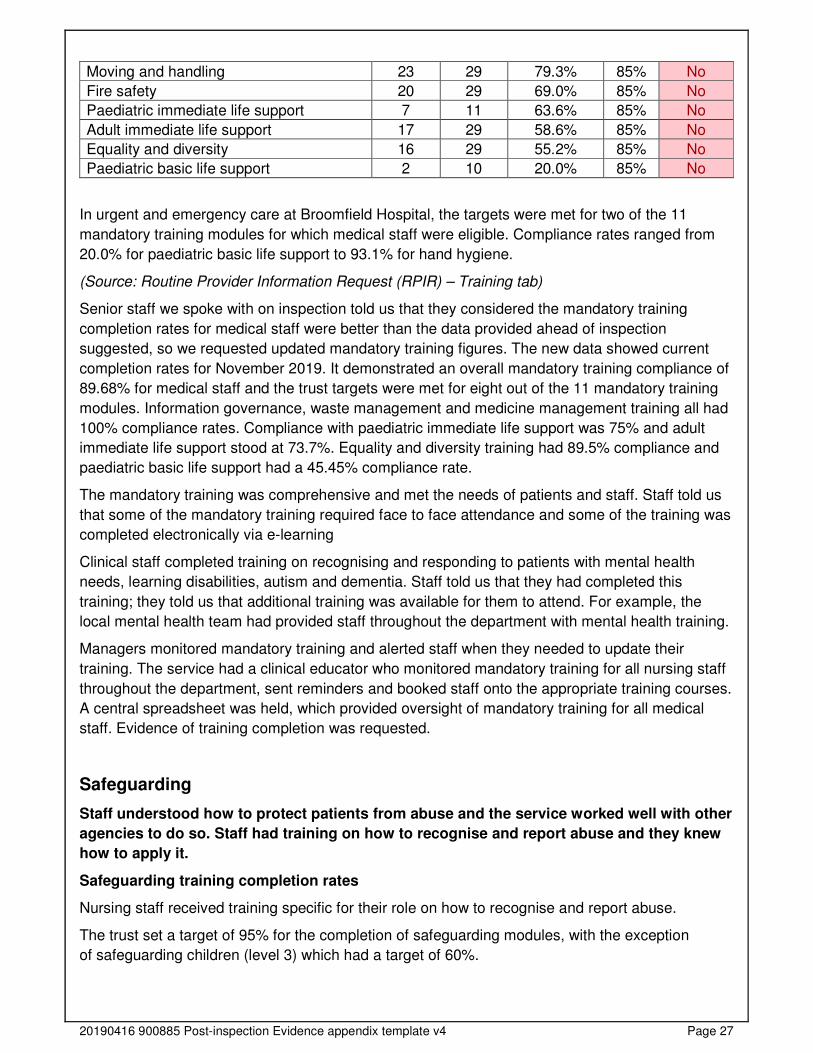
A breakdown of compliance for mandatory training courses as of August 2019 for medical staff in
urgent and emergency care at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Hand hygiene 27 29 93.1% 85% Yes
Information governance 27 29 93.1% 95% No
Health and safety 25 29 86.2% 85% Yes
Waste management 24 29 82.8% 85% No
Medicine management training 4 5 80.0% 85% No
20190416 900885 Post-inspection Evidence appendix template v4 Page 27
Moving and handling 23 29 79.3% 85% No
Fire safety 20 29 69.0% 85% No
Paediatric immediate life support 7 11 63.6% 85% No
Adult immediate life support 17 29 58.6% 85% No
Equality and diversity 16 29 55.2% 85% No
Paediatric basic life support 2 10 20.0% 85% No
In urgent and emergency care at Broomfield Hospital, the targets were met for two of the 11
mandatory training modules for which medical staff were eligible. Compliance rates ranged from
20.0% for paediatric basic life support to 93.1% for hand hygiene.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Senior staff we spoke with on inspection told us that they considered the mandatory training
completion rates for medical staff were better than the data provided ahead of inspection
suggested, so we requested updated mandatory training figures. The new data showed current
completion rates for November 2019. It demonstrated an overall mandatory training compliance of
89.68% for medical staff and the trust targets were met for eight out of the 11 mandatory training
modules. Information governance, waste management and medicine management training all had
100% compliance rates. Compliance with paediatric immediate life support was 75% and adult
immediate life support stood at 73.7%. Equality and diversity training had 89.5% compliance and
paediatric basic life support had a 45.45% compliance rate.
The mandatory training was comprehensive and met the needs of patients and staff. Staff told us
that some of the mandatory training required face to face attendance and some of the training was
completed electronically via e-learning
Clinical staff completed training on recognising and responding to patients with mental health
needs, learning disabilities, autism and dementia. Staff told us that they had completed this
training; they told us that additional training was available for them to attend. For example, the
local mental health team had provided staff throughout the department with mental health training.
Managers monitored mandatory training and alerted staff when they needed to update their
training. The service had a clinical educator who monitored mandatory training for all nursing staff
throughout the department, sent reminders and booked staff onto the appropriate training courses.
A central spreadsheet was held, which provided oversight of mandatory training for all medical
staff. Evidence of training completion was requested.
Safeguarding
Staff understood how to protect patients from abuse and the service worked well with other
agencies to do so. Staff had training on how to recognise and report abuse and they knew
how to apply it.
Safeguarding training completion rates
Nursing staff received training specific for their role on how to recognise and report abuse.
The trust set a target of 95% for the completion of safeguarding modules, with the exception
of safeguarding children (level 3) which had a target of 60%.
20190416 900885 Post-inspection Evidence appendix template v4 Page 28
The tables below include prevent training as a safeguarding course. Prevent works to
stop individuals from getting involved in or supporting terrorism or extremist activity. The trust set a
target of 85% for the completion of prevent awareness training modules.
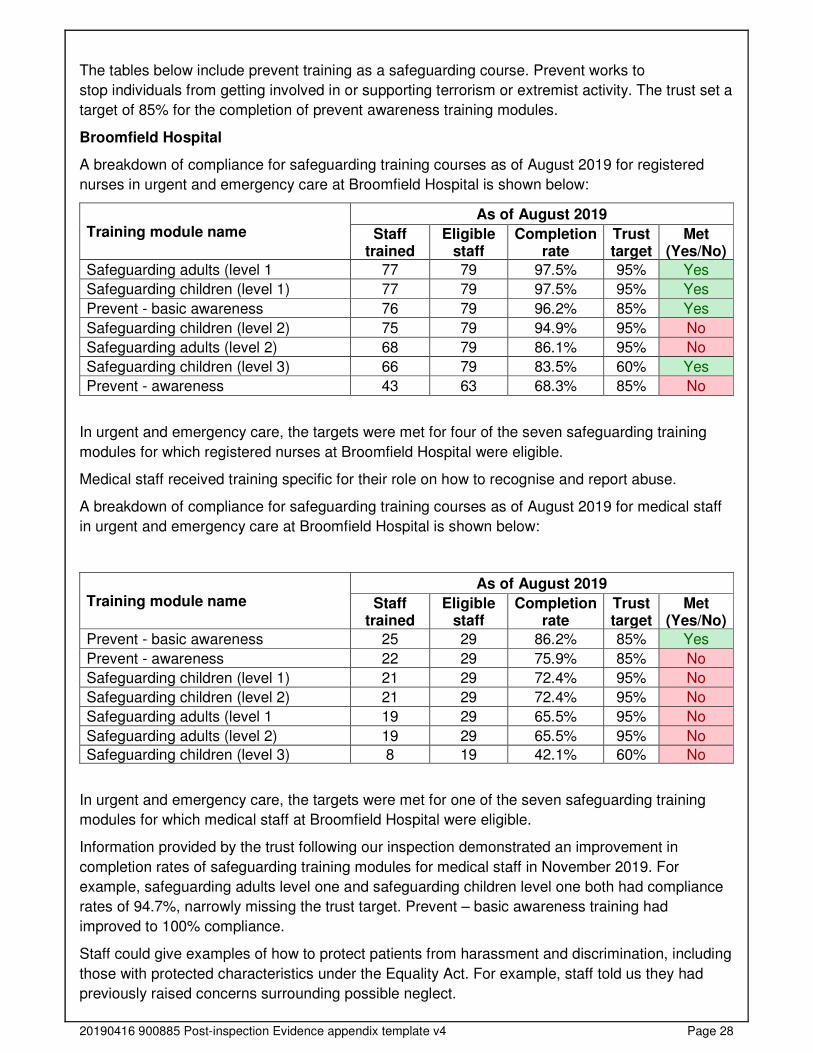
Broomfield Hospital
A breakdown of compliance for safeguarding training courses as of August 2019 for registered
nurses in urgent and emergency care at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Safeguarding adults (level 1 77 79 97.5% 95% Yes
Safeguarding children (level 1) 77 79 97.5% 95% Yes
Prevent - basic awareness 76 79 96.2% 85% Yes
Safeguarding children (level 2) 75 79 94.9% 95% No
Safeguarding adults (level 2) 68 79 86.1% 95% No
Safeguarding children (level 3) 66 79 83.5% 60% Yes
Prevent - awareness 43 63 68.3% 85% No
In urgent and emergency care, the targets were met for four of the seven safeguarding training
modules for which registered nurses at Broomfield Hospital were eligible.
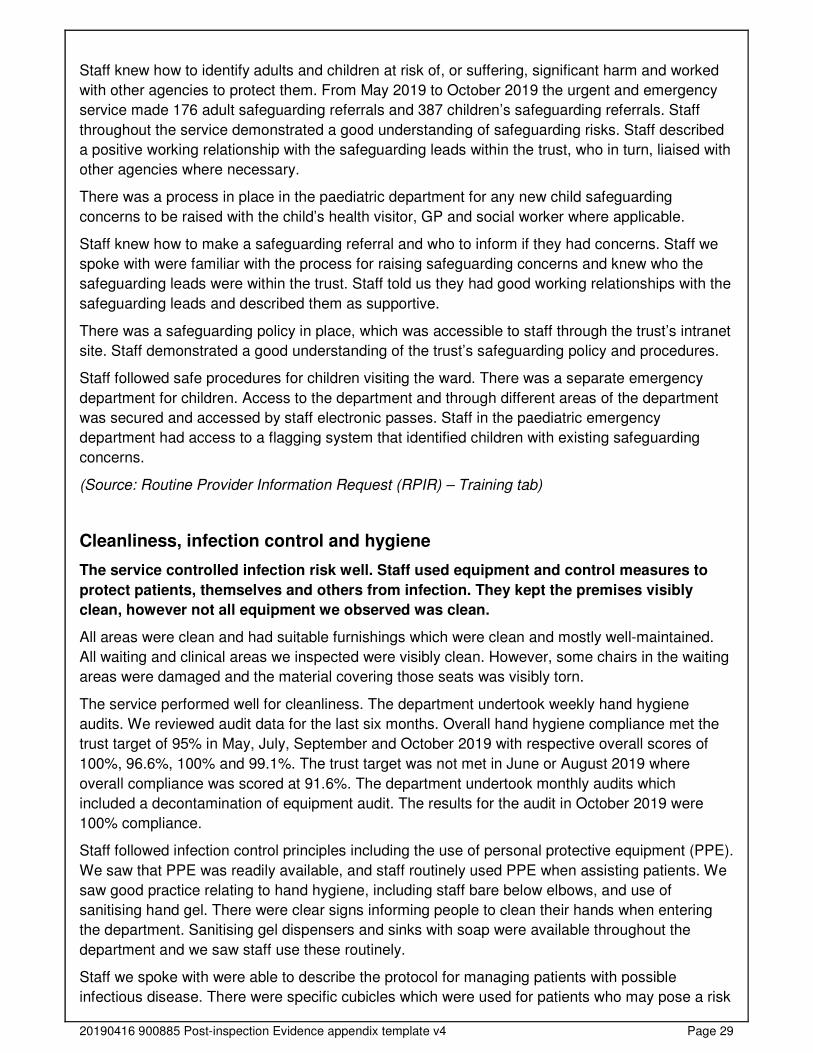
Medical staff received training specific for their role on how to recognise and report abuse.
A breakdown of compliance for safeguarding training courses as of August 2019 for medical staff
in urgent and emergency care at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Prevent - basic awareness 25 29 86.2% 85% Yes
Prevent - awareness 22 29 75.9% 85% No
Safeguarding children (level 1) 21 29 72.4% 95% No
Safeguarding children (level 2) 21 29 72.4% 95% No
Safeguarding adults (level 1 19 29 65.5% 95% No
Safeguarding adults (level 2) 19 29 65.5% 95% No
Safeguarding children (level 3) 8 19 42.1% 60% No
In urgent and emergency care, the targets were met for one of the seven safeguarding training
modules for which medical staff at Broomfield Hospital were eligible.
Information provided by the trust following our inspection demonstrated an improvement in
completion rates of safeguarding training modules for medical staff in November 2019. For
example, safeguarding adults level one and safeguarding children level one both had compliance
rates of 94.7%, narrowly missing the trust target. Prevent – basic awareness training had
improved to 100% compliance.
Staff could give examples of how to protect patients from harassment and discrimination, including
those with protected characteristics under the Equality Act. For example, staff told us they had
previously raised concerns surrounding possible neglect.
20190416 900885 Post-inspection Evidence appendix template v4 Page 29
Staff knew how to identify adults and children at risk of, or suffering, significant harm and worked
with other agencies to protect them. From May 2019 to October 2019 the urgent and emergency
service made 176 adult safeguarding referrals and 387 children’s safeguarding referrals. Staff
throughout the service demonstrated a good understanding of safeguarding risks. Staff described
a positive working relationship with the safeguarding leads within the trust, who in turn, liaised with
other agencies where necessary.
There was a process in place in the paediatric department for any new child safeguarding
concerns to be raised with the child’s health visitor, GP and social worker where applicable.
Staff knew how to make a safeguarding referral and who to inform if they had concerns. Staff we
spoke with were familiar with the process for raising safeguarding concerns and knew who the
safeguarding leads were within the trust. Staff told us they had good working relationships with the
safeguarding leads and described them as supportive.
There was a safeguarding policy in place, which was accessible to staff through the trust’s intranet
site. Staff demonstrated a good understanding of the trust’s safeguarding policy and procedures.
Staff followed safe procedures for children visiting the ward. There was a separate emergency
department for children. Access to the department and through different areas of the department
was secured and accessed by staff electronic passes. Staff in the paediatric emergency
department had access to a flagging system that identified children with existing safeguarding
concerns.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Cleanliness, infection control and hygiene
The service controlled infection risk well. Staff used equipment and control measures to
protect patients, themselves and others from infection. They kept the premises visibly
clean, however not all equipment we observed was clean.
All areas were clean and had suitable furnishings which were clean and mostly well-maintained.
All waiting and clinical areas we inspected were visibly clean. However, some chairs in the waiting
areas were damaged and the material covering those seats was visibly torn.
The service performed well for cleanliness. The department undertook weekly hand hygiene
audits. We reviewed audit data for the last six months. Overall hand hygiene compliance met the
trust target of 95% in May, July, September and October 2019 with respective overall scores of
100%, 96.6%, 100% and 99.1%. The trust target was not met in June or August 2019 where
overall compliance was scored at 91.6%. The department undertook monthly audits which
included a decontamination of equipment audit. The results for the audit in October 2019 were
100% compliance.
Staff followed infection control principles including the use of personal protective equipment (PPE).
We saw that PPE was readily available, and staff routinely used PPE when assisting patients. We
saw good practice relating to hand hygiene, including staff bare below elbows, and use of
sanitising hand gel. There were clear signs informing people to clean their hands when entering
the department. Sanitising gel dispensers and sinks with soap were available throughout the
department and we saw staff use these routinely.
Staff we spoke with were able to describe the protocol for managing patients with possible
infectious disease. There were specific cubicles which were used for patients who may pose a risk
20190416 900885 Post-inspection Evidence appendix template v4 Page 30
of cross infection. Staff knew where to locate isolation signs to be placed outside of cubicles to
identify what PPE staff were required to wear before entering the cubicle, depending on the
infection the patient had.
Information provided by the trust following inspection stated that the infection prevention and
control team undertook assurance audits in May, July, September and November 2019. These
audits included hand hygiene, cleaning and decontamination, waste management and segregation
and transmissible infections. We reviewed the audits for the paediatric emergency department
(ED) in July 2019 and the audit for the main emergency department which was carried out in May
2019. Paediatric ED had a compliance score of 93%. The main ED had a compliance score of
95%. Both were compliant as they scored above 90%. Both audits included an action plan which
included who was responsible for the action and the date of completion. This assured us that there
were processes in place to monitor whether staff cleaned equipment after patient contact and
actioned any changes that needed to be made.
We identified some equipment in the department that did not appear to have been recently
cleaned as they were visibly dusty. This was the case for four pieces of equipment we reviewed.
The items were; one cardiac monitor in resus, a cardiac monitor in majors and two suction units in
the minor assessment extension to ED. However, other equipment we reviewed was visibly clean.
We raised the dusty equipment with staff at the time of our inspection. When we reviewed the
equipment the following day, we found it had been cleaned.
Cleaning records were not always kept up-to-date. For example, documentation had not been
completed for three days of week commencing 23 September 2019 or week commencing 12
August 2019 in the majors lite area. The cleaning tasks that required documenting included
cleaning toilets, replenishing consumables, hoovering and mopping floors and emptying rubbish
bins. However, audit performance data showed that the department mostly achieved target scores
for cleanliness from 1 August to 28 October 2019. Therefore, the issue appeared to be with
documentation rather than the completion of cleaning tasks.
Environment and equipment
The design, maintenance and use of facilities, premises, vehicles and equipment kept
people safe. Staff were trained to use them. Staff managed clinical waste well.
The emergency department (ED) contained a main waiting area and reception close to the car
park where initial streaming took place. There were facilities for the assessment and treatment of
minor and major injuries and illnesses. There were 10 majors cubicles in the department, a bay
with five resuscitation spaces which included a dedicated space for paediatric patients. There was
a sixth resuscitation bay which was used for the storage of equipment. There was a separate
paediatric ED with its own waiting area. There were emergency nurse practitioner (ENP), and
general practitioner (GP) led services within the department. Early senior assessment and
treatment (ESAT) used five cubicles in majors to assess and triage patients who arrived through
the ambulance bay. There was an extended area to the emergency department which included a
minor assessment unit and two ‘fit to sit’ cubicles plus a waiting area. Patients who arrived by air
ambulance were transferred into the department via the onsite helipad.
The emergency department had a dedicated room for adult mental health patients which had been
specifically designed to meet the needs of mental health patients. The room was situated away
from the main treatment areas to offer people privacy and a safe environment with no ligature or
self-harm risks. This was in line with standards set by the Royal College of Psychiatrists
20190416 900885 Post-inspection Evidence appendix template v4 Page 31
psychiatric liaison accreditation network. The room was out of use at the time of our inspection as
a glass panel needed replacing, however when we returned for the unannounced inspection the
room was in use again.
The department also used majors cubicles for patients suffering with mental health problems. The
cubicles were situated close to the nursing station which meant that staff could directly observe
patients. Staff told us that they removed all potentially unsafe items from the rooms before
admitting patients into them. Healthcare support workers were able to carry out constant
observations where required and mental health nurses were sourced via an agency as needed.
Staff completed comprehensive mental health risk assessments and we were assured that they
were able to mitigate the risks of treating mental health patients in majors cubicles.
The paediatric ED was separate from the rest of the department. It had its own waiting area and
treatment rooms. Entrance in and out of the children’s ED was controlled by a locked door which
enabled staff to monitor who was entering or leaving the department.
The ambulatory care unit and emergency short stay ward were situated close to the emergency
department. Ambulatory care is same day care which meant that patients were assessed,
diagnosed, treated and able to go home the same day, without being admitted into hospital
overnight. The ambulatory care unit had its own waiting room, separate cubicles and an area with
reclining chairs. At the time of our unannounced inspection, the ambulatory care unit had moved
nearby to a different location and had been renamed same day emergency care (SDEC) unit.
Staff carried out daily safety checks of specialist equipment. We checked three resuscitation
trolleys within the department and found that checks were completed daily.
The service had enough suitable equipment to help them to safely care for patients. All electrical
items we reviewed had evidence of regular portable appliance testing. We found one suction unit
that was out of date for electronic testing, however it was not in use. The item was removed after
we notified a staff member. Equipment was monitored by the medical equipment library. Staff told
us they could access additional equipment if necessary.
Staff disposed of clinical waste safely. Clinical and non-clinical waste was disposed of separately.
Sharps bins containing used needles and other sharp objects were correctly signed and dated
which helped staff determine when they should be replaced.
We found patients could not reach call bells in part of the extension to the emergency department
which was known as the minor assessment unit. We saw that call bells were hanging on the walls
which were not within the reach of patients. We noticed that this area was staffed at all times while
patients were present, which mitigated the risk to patients. When we returned to the department
for an unannounced inspection we found that call bells were within reach of patients.
Assessing and responding to patient risk
Staff did not always complete risk assessments for each patient swiftly. They did not
always remove or minimise risks and update the assessments. Staff did not always identify
and quickly act upon patients at risk of deterioration.
Emergency Department Survey 2016
The trust scored about the same as other trusts for all five of the Emergency Department Survey
questions relevant to safety.
Question Score RAG
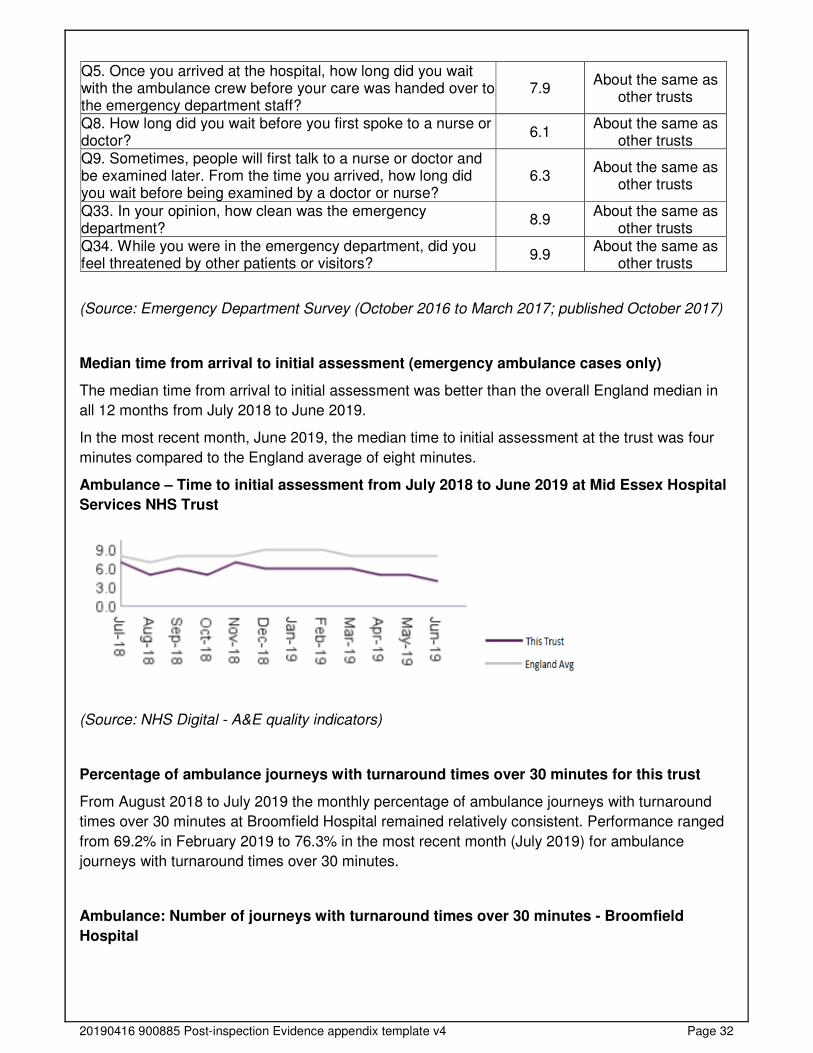
20190416 900885 Post-inspection Evidence appendix template v4 Page 32
Q5. Once you arrived at the hospital, how long did you wait with the ambulance crew before your care was handed over to the emergency department staff?
7.9 About the same as
other trusts
Q8. How long did you wait before you first spoke to a nurse or doctor?
6.1 About the same as
other trusts Q9. Sometimes, people will first talk to a nurse or doctor and be examined later. From the time you arrived, how long did you wait before being examined by a doctor or nurse?
6.3 About the same as
other trusts
Q33. In your opinion, how clean was the emergency department?
8.9 About the same as
other trusts Q34. While you were in the emergency department, did you feel threatened by other patients or visitors?
9.9 About the same as
other trusts
(Source: Emergency Department Survey (October 2016 to March 2017; published October 2017)
Median time from arrival to initial assessment (emergency ambulance cases only)
The median time from arrival to initial assessment was better than the overall England median in
all 12 months from July 2018 to June 2019.
In the most recent month, June 2019, the median time to initial assessment at the trust was four
minutes compared to the England average of eight minutes.
Ambulance – Time to initial assessment from July 2018 to June 2019 at Mid Essex Hospital
Services NHS Trust
(Source: NHS Digital - A&E quality indicators)
Percentage of ambulance journeys with turnaround times over 30 minutes for this trust
From August 2018 to July 2019 the monthly percentage of ambulance journeys with turnaround
times over 30 minutes at Broomfield Hospital remained relatively consistent. Performance ranged
from 69.2% in February 2019 to 76.3% in the most recent month (July 2019) for ambulance
journeys with turnaround times over 30 minutes.
Ambulance: Number of journeys with turnaround times over 30 minutes - Broomfield
Hospital
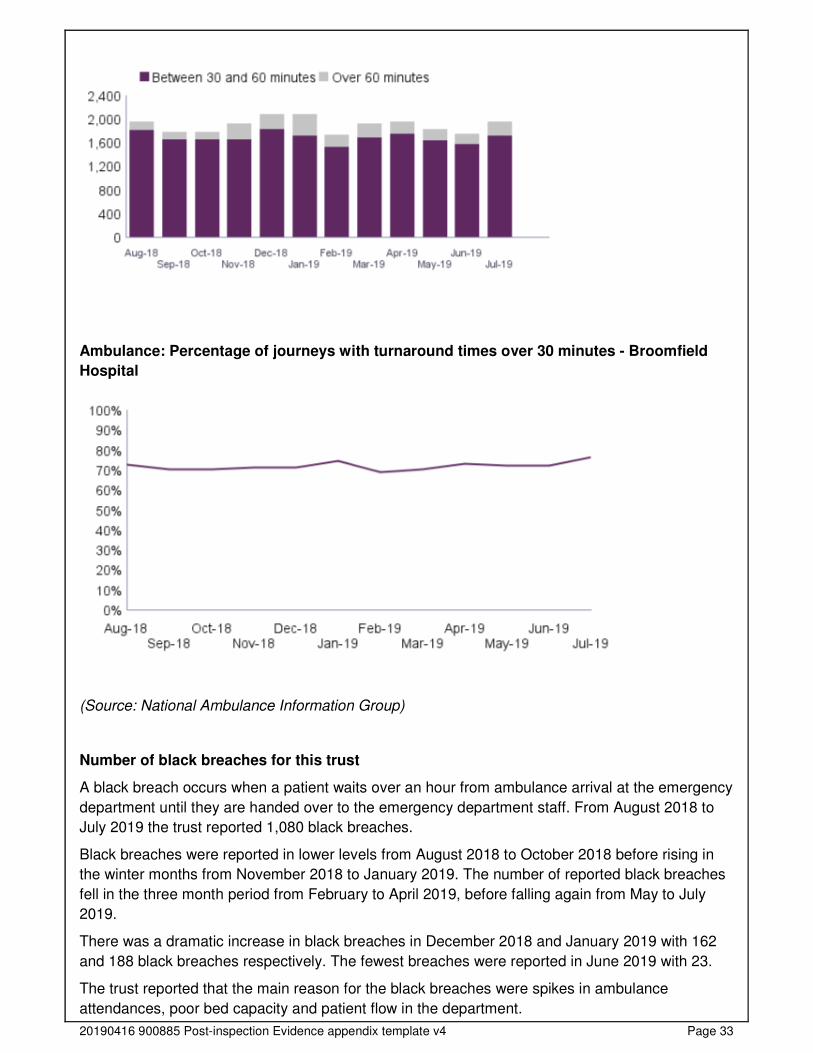
20190416 900885 Post-inspection Evidence appendix template v4 Page 33
Ambulance: Percentage of journeys with turnaround times over 30 minutes - Broomfield
Hospital
(Source: National Ambulance Information Group)
Number of black breaches for this trust
A black breach occurs when a patient waits over an hour from ambulance arrival at the emergency
department until they are handed over to the emergency department staff. From August 2018 to
July 2019 the trust reported 1,080 black breaches.
Black breaches were reported in lower levels from August 2018 to October 2018 before rising in
the winter months from November 2018 to January 2019. The number of reported black breaches
fell in the three month period from February to April 2019, before falling again from May to July
2019.
There was a dramatic increase in black breaches in December 2018 and January 2019 with 162
and 188 black breaches respectively. The fewest breaches were reported in June 2019 with 23.
The trust reported that the main reason for the black breaches were spikes in ambulance
attendances, poor bed capacity and patient flow in the department.

20190416 900885 Post-inspection Evidence appendix template v4 Page 34
(Source: Routine Provider Information Request (RPIR) - Black Breaches tab)
Staff used a nationally recognised tool to identify deteriorating patients and escalated them
appropriately. Staff used the National Early Warning Score (NEWS2) and the Paediatric Early
Warning Score (PEWS) to monitor and identify deteriorating patients. However, we found that
NEWS2 scores were not always completed as frequently as they should have been. We found that
50% of the documentation we reviewed on inspection did not have NEWS2 scoring completed as
frequently as required. We raised our concerns during the inspection. The trust responded to the
concerns we raised by carrying out an audit of 10 sets of patient records. The audit reflected our
inspection findings with four out of 10 observations not recorded within recommended timescales.
The trust also conducted a harm review within the audit and there was no harm identified.
The trust reported that there had been some recent issues with the electronic devices that NEWS2
scoring was captured on. We were advised on inspection that the devices were set for two hourly
observations which needed to be overridden by staff. The matron reported there had been several
incidents raised for this issue and that a further incident had been raised at the time of our
inspection which prompted a system check of the devices.
The trust policy stated that all patients in majors required observation every 30 minutes until seen
by medical staff irrespective of clinical need or presenting complaint. The trust recognised this was
not achievable or clinically indicated. The trust agreed that frequency should be at least hourly or
more frequently dependant on the individual patient acuity determined by the NEWS2. This was
reflected in an update to the ED observation policy which was also in line with Royal College of
Emergency Medicine (RCEM) and NEWS2 best practice guidance.
We checked a further seven patient records when we returned for the unannounced inspection.
Five out of those seven records had NEWS2 scoring completed appropriately. This showed that
the frequency of NEWS2 scoring had improved in comparison to our findings from the initial
inspection. The electronic devices used for capturing NEWS2 scores were not working when we
returned for the unannounced inspection, so the data was being recorded on paper. The trust
formulated an action plan following our inspection which included an update to the ED observation
policy and training for additional staff members to be ‘super users’ of the electronic devices used
for NEWS2 scoring. The configuration of the electronic recording system was to be reviewed with
fortnightly task and finish group established that reported to the patient safety group. The trust also
planned to commence a daily local ‘snapshot’ audit to provide assurance of approved timeliness of
20190416 900885 Post-inspection Evidence appendix template v4 Page 35
observations. There were actions in place to improve clinical oversight by the senior team within
ED which included restructuring the nurse in charge station to clearly display NEWS2 scores.
Staff completed risk assessments for each patient on admission / arrival, using a recognised tool,
and reviewed this regularly, including after any incident. For example, staff completed
assessments of pressure areas and frailty assessments were completed where applicable.
Staff knew about and dealt with any specific risk issues. Nursing staff used the Manchester Triage
Tool (MTT) to assess patients. The MTT is used to triage patients and ascertain how critically
unwell a patient may be. Patients were treated in priority dependent on their condition. Triage
systems aimed to reduce risk by assessing patients and seeing them in order of clinical priority,
rather than order of attendance.
The reception staff were all trained in using a ‘red flag’ criteria to immediately highlight attending
patients to nursing and or medical staff, who may be seriously unwell.
We saw appropriate screening tools for sepsis used throughout the department. There was an
escalation policy in place for patients with presumed or confirmed sepsis who required an
immediate review and the service carried out monthly audits of sepsis management for a sample
of patients. The results of the audits identified the percentage of patients who required sepsis
screening that received intravenous antibiotics within one hour. The results of the audit were 91%
in August 2019, 100% in September 2019 and 75% in October 2019. The trust reported some
problems with the electronic system used for documentation, which at times meant staff had to
use paper documentation which could lead to duplication or omission of screening. Information
provided by the trust stated that this may account for some of the reduction in compliance in
October. The trust had implemented an action plan to improve compliance of the delivery of
antibiotics within one hour. Actions were assigned to individuals with completion and target
completion dates. We saw examples of patients receiving antibiotics within the recommended
sepsis pathway times.
Nurses working within the children’s ED had the necessary skills and expertise including advanced
life support. All ED healthcare support workers received paediatric basic life support training as
part of their mandatory training; and nurses received paediatric intermediate life support (PILS).
However, we were told it was not always possible to ensure there was a children’s nurse available
in the children’s ED. The service mitigated this risk by training adult nurses, and assessing and
ensuring they had the correct competencies to work in that environment.
The service had 24-hour access to mental health liaison and specialist mental health support. Staff
reported a positive working relationship with the local mental health team. Staff from the local
mental health team were based at the hospital site during the day to enable them to provide timely
support when needed.
Staff completed, or arranged, psychosocial assessments and risk assessments for patients
thought to be at risk of self-harm or suicide. Staff risk assessed all patients with a suspected
mental health condition upon arrival at the emergency department. Staff used a mental health
assessment tool that had been developed jointly with the local mental health team. It enabled staff
to calculate the level of risk that a patient presented with. Both adult and paediatric patients had a
specific risk assessment indicating their levels of risk, and any need for a referral to the local
mental health team. We saw that these assessments were detailed, comprehensive and
personalised.
Staff shared key information to keep patients safe when handing over their care to others. A
handover nurse completed a document based on situation, background, assessment,
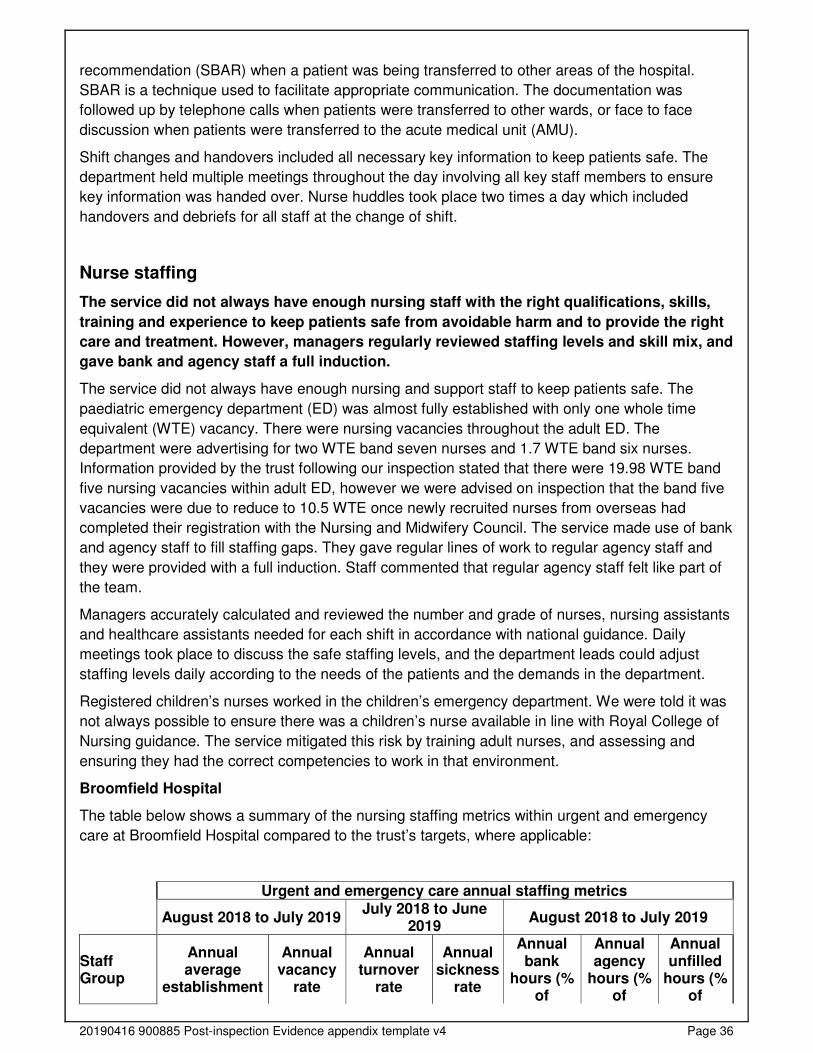
20190416 900885 Post-inspection Evidence appendix template v4 Page 36
recommendation (SBAR) when a patient was being transferred to other areas of the hospital.
SBAR is a technique used to facilitate appropriate communication. The documentation was
followed up by telephone calls when patients were transferred to other wards, or face to face
discussion when patients were transferred to the acute medical unit (AMU).
Shift changes and handovers included all necessary key information to keep patients safe. The
department held multiple meetings throughout the day involving all key staff members to ensure
key information was handed over. Nurse huddles took place two times a day which included
handovers and debriefs for all staff at the change of shift.
Nurse staffing
The service did not always have enough nursing staff with the right qualifications, skills,
training and experience to keep patients safe from avoidable harm and to provide the right
care and treatment. However, managers regularly reviewed staffing levels and skill mix, and
gave bank and agency staff a full induction.
The service did not always have enough nursing and support staff to keep patients safe. The
paediatric emergency department (ED) was almost fully established with only one whole time
equivalent (WTE) vacancy. There were nursing vacancies throughout the adult ED. The
department were advertising for two WTE band seven nurses and 1.7 WTE band six nurses.
Information provided by the trust following our inspection stated that there were 19.98 WTE band
five nursing vacancies within adult ED, however we were advised on inspection that the band five
vacancies were due to reduce to 10.5 WTE once newly recruited nurses from overseas had
completed their registration with the Nursing and Midwifery Council. The service made use of bank
and agency staff to fill staffing gaps. They gave regular lines of work to regular agency staff and
they were provided with a full induction. Staff commented that regular agency staff felt like part of
the team.
Managers accurately calculated and reviewed the number and grade of nurses, nursing assistants
and healthcare assistants needed for each shift in accordance with national guidance. Daily
meetings took place to discuss the safe staffing levels, and the department leads could adjust
staffing levels daily according to the needs of the patients and the demands in the department.
Registered children’s nurses worked in the children’s emergency department. We were told it was
not always possible to ensure there was a children’s nurse available in line with Royal College of
Nursing guidance. The service mitigated this risk by training adult nurses, and assessing and
ensuring they had the correct competencies to work in that environment.
Broomfield Hospital
The table below shows a summary of the nursing staffing metrics within urgent and emergency
care at Broomfield Hospital compared to the trust’s targets, where applicable:
Urgent and emergency care annual staffing metrics
August 2018 to July 2019 July 2018 to June
2019 August 2018 to July 2019
Staff Group
Annual average
establishment
Annual vacancy
rate
Annual turnover
rate
Annual sickness
rate
Annual bank
hours (% of
Annual agency
hours (% of
Annual unfilled
hours (% of
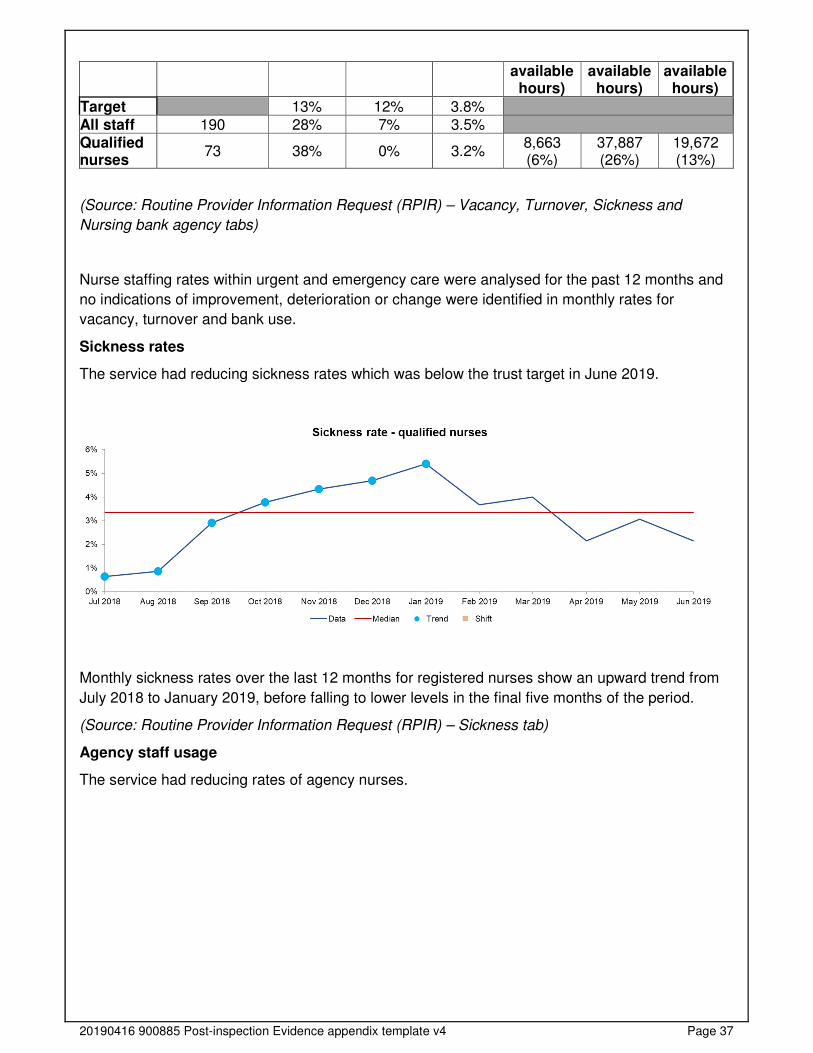
20190416 900885 Post-inspection Evidence appendix template v4 Page 37
available hours)
available hours)
available hours)
Target 13% 12% 3.8%
All staff 190 28% 7% 3.5% Qualified nurses
73 38% 0% 3.2% 8,663 (6%)
37,887 (26%)
19,672 (13%)
(Source: Routine Provider Information Request (RPIR) – Vacancy, Turnover, Sickness and
Nursing bank agency tabs)
Nurse staffing rates within urgent and emergency care were analysed for the past 12 months and
no indications of improvement, deterioration or change were identified in monthly rates for
vacancy, turnover and bank use.
Sickness rates
The service had reducing sickness rates which was below the trust target in June 2019.
Monthly sickness rates over the last 12 months for registered nurses show an upward trend from
July 2018 to January 2019, before falling to lower levels in the final five months of the period.
(Source: Routine Provider Information Request (RPIR) – Sickness tab)
Agency staff usage
The service had reducing rates of agency nurses.
20190416 900885 Post-inspection Evidence appendix template v4 Page 38
Monthly agency hours over the last 12 months for registered nurses show a downward shift from
February 2019 to July 2019, in line with decreasing sickness rates.
(Source: Routine Provider Information Request (RPIR) - Nursing bank agency tab)
Managers tried to limit the use of bank and agency staff and encouraged hospital staff to join the
hospital bank list for overtime. This helped ensure the bank staff used were familiar with the
service.
Medical staffing
The service did not always have enough medical staff with the right qualifications, skills,
training and experience to keep patients safe from avoidable harm and to provide the right
care and treatment. However, managers regularly reviewed staffing levels and skill mix, and
gave locum staff a full induction.
The service did not always have enough medical staff to keep patients safe. There were vacancies
across the adult emergency department (ED); information provided by the trust following
inspection stated that the trust had 0.9 whole time equivalent (WTE) consultant vacancies, 6.12
WTE vacancies for middle career staff and 1.4 WTE vacancies for registrars. The trust had an
action plan in place to support the recruitment and retention of middle career staff within the
emergency department. All actions were allocated to an individual with completion dates and/or
target completion dates. The risks were mitigated by the use of locum staff. Consultants told us
there had been times when they worked night shifts on occasions when no other medical cover
could be sourced. There were no paediatric medical vacancies within the department and there
were four paediatric consultants.
Broomfield Hospital
The table below shows a summary of the medical staffing metrics within urgent and emergency
care at Broomfield Hospital compared to the trust’s targets, where applicable:
Urgent and emergency care annual staffing metrics
August 2018 to July 2019 July 2018 to June
2019 August 2018 to July 2019
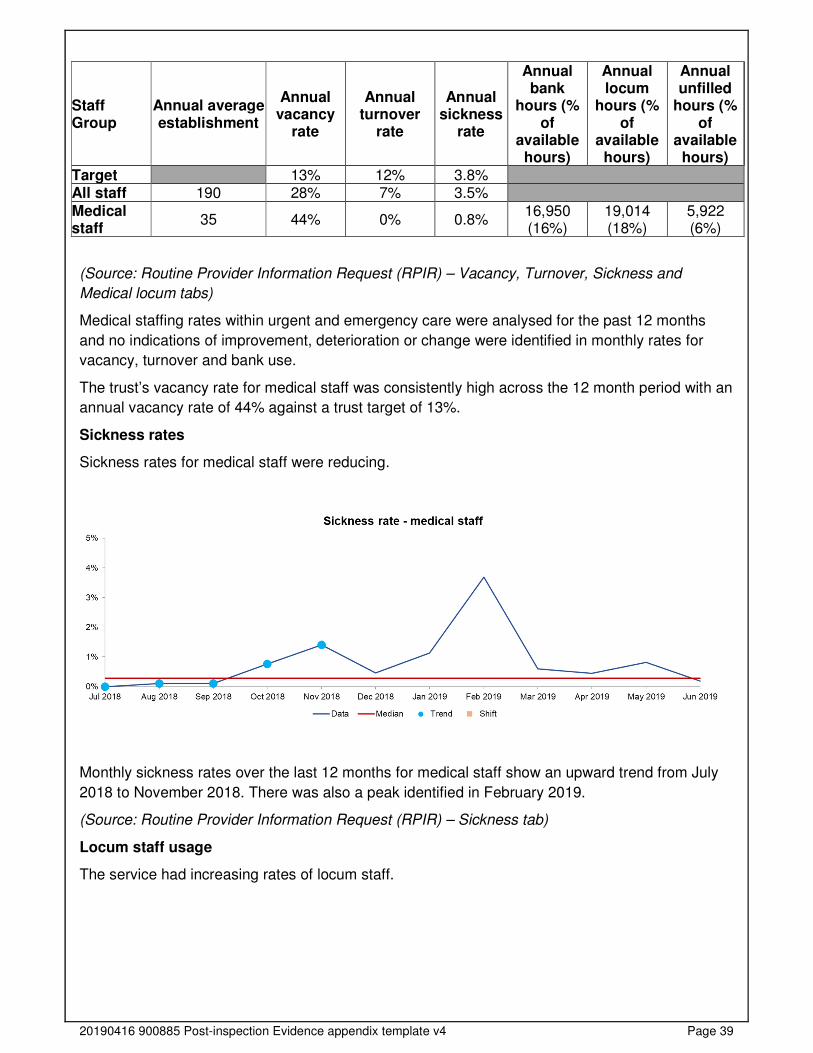
20190416 900885 Post-inspection Evidence appendix template v4 Page 39
Staff Group
Annual average establishment
Annual vacancy
rate
Annual turnover
rate
Annual sickness
rate
Annual bank
hours (% of
available hours)
Annual locum
hours (% of
available hours)
Annual unfilled
hours (% of
available hours)
Target 13% 12% 3.8% All staff 190 28% 7% 3.5%
Medical staff
35 44% 0% 0.8% 16,950 (16%)
19,014 (18%)
5,922 (6%)
(Source: Routine Provider Information Request (RPIR) – Vacancy, Turnover, Sickness and
Medical locum tabs)
Medical staffing rates within urgent and emergency care were analysed for the past 12 months
and no indications of improvement, deterioration or change were identified in monthly rates for
vacancy, turnover and bank use.
The trust’s vacancy rate for medical staff was consistently high across the 12 month period with an
annual vacancy rate of 44% against a trust target of 13%.
Sickness rates
Sickness rates for medical staff were reducing.
Monthly sickness rates over the last 12 months for medical staff show an upward trend from July
2018 to November 2018. There was also a peak identified in February 2019.
(Source: Routine Provider Information Request (RPIR) – Sickness tab)
Locum staff usage
The service had increasing rates of locum staff.
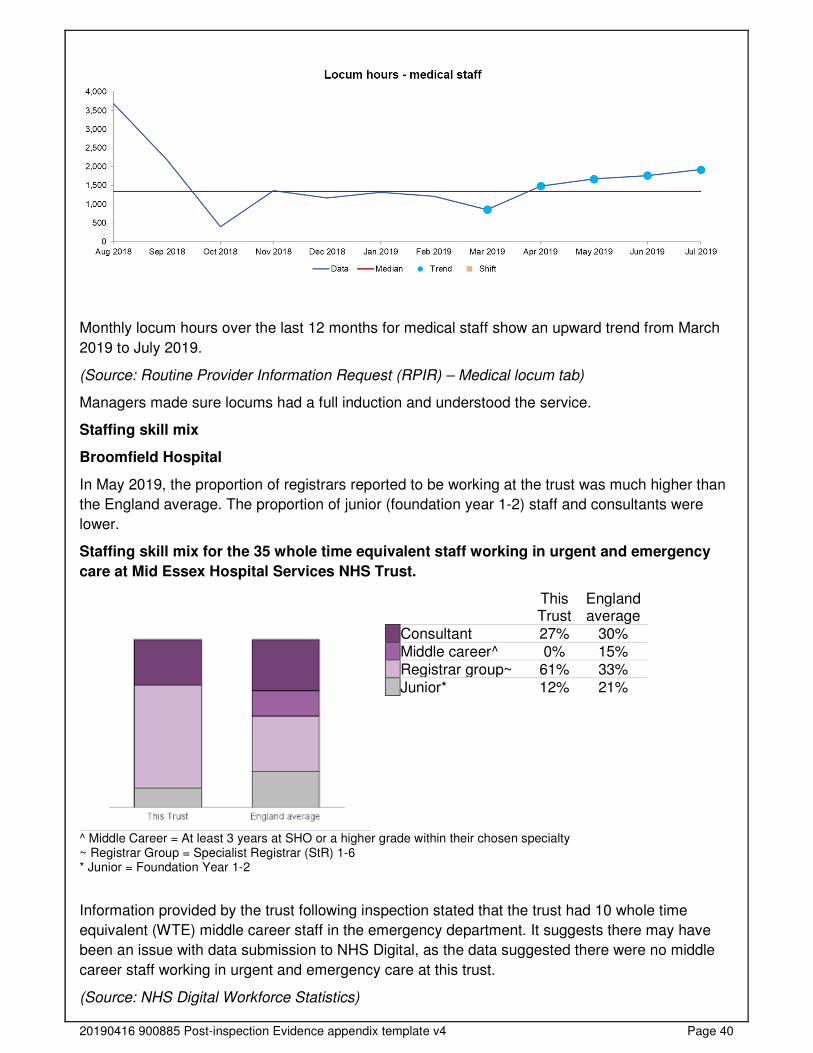
20190416 900885 Post-inspection Evidence appendix template v4 Page 40
Monthly locum hours over the last 12 months for medical staff show an upward trend from March
2019 to July 2019.
(Source: Routine Provider Information Request (RPIR) – Medical locum tab)
Managers made sure locums had a full induction and understood the service.
Staffing skill mix
Broomfield Hospital
In May 2019, the proportion of registrars reported to be working at the trust was much higher than
the England average. The proportion of junior (foundation year 1-2) staff and consultants were
lower.
Staffing skill mix for the 35 whole time equivalent staff working in urgent and emergency
care at Mid Essex Hospital Services NHS Trust.
This Trust
England average
Consultant 27% 30% Middle career^ 0% 15% Registrar group~ 61% 33% Junior* 12% 21%
^ Middle Career = At least 3 years at SHO or a higher grade within their chosen specialty ~ Registrar Group = Specialist Registrar (StR) 1-6 * Junior = Foundation Year 1-2
Information provided by the trust following inspection stated that the trust had 10 whole time
equivalent (WTE) middle career staff in the emergency department. It suggests there may have
been an issue with data submission to NHS Digital, as the data suggested there were no middle
career staff working in urgent and emergency care at this trust.
(Source: NHS Digital Workforce Statistics)
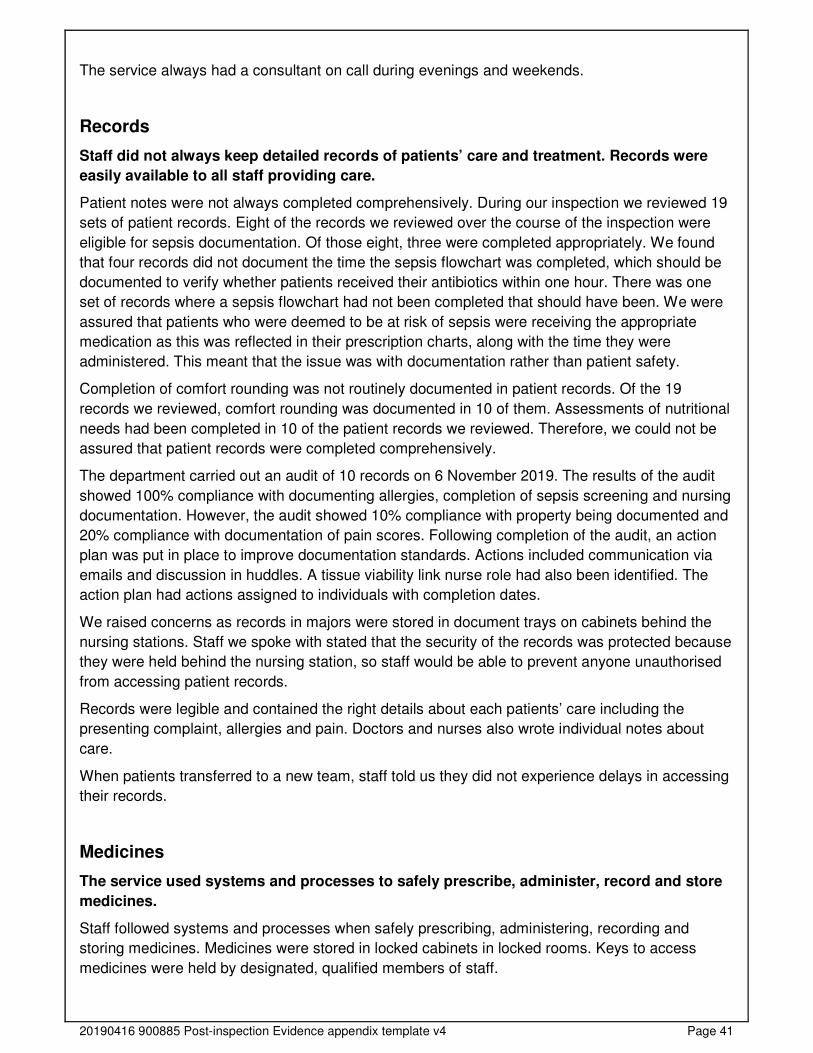
20190416 900885 Post-inspection Evidence appendix template v4 Page 41
The service always had a consultant on call during evenings and weekends.
Records
Staff did not always keep detailed records of patients’ care and treatment. Records were
easily available to all staff providing care.
Patient notes were not always completed comprehensively. During our inspection we reviewed 19
sets of patient records. Eight of the records we reviewed over the course of the inspection were
eligible for sepsis documentation. Of those eight, three were completed appropriately. We found
that four records did not document the time the sepsis flowchart was completed, which should be
documented to verify whether patients received their antibiotics within one hour. There was one
set of records where a sepsis flowchart had not been completed that should have been. We were
assured that patients who were deemed to be at risk of sepsis were receiving the appropriate
medication as this was reflected in their prescription charts, along with the time they were
administered. This meant that the issue was with documentation rather than patient safety.
Completion of comfort rounding was not routinely documented in patient records. Of the 19
records we reviewed, comfort rounding was documented in 10 of them. Assessments of nutritional
needs had been completed in 10 of the patient records we reviewed. Therefore, we could not be
assured that patient records were completed comprehensively.
The department carried out an audit of 10 records on 6 November 2019. The results of the audit
showed 100% compliance with documenting allergies, completion of sepsis screening and nursing
documentation. However, the audit showed 10% compliance with property being documented and
20% compliance with documentation of pain scores. Following completion of the audit, an action
plan was put in place to improve documentation standards. Actions included communication via
emails and discussion in huddles. A tissue viability link nurse role had also been identified. The
action plan had actions assigned to individuals with completion dates.
We raised concerns as records in majors were stored in document trays on cabinets behind the
nursing stations. Staff we spoke with stated that the security of the records was protected because
they were held behind the nursing station, so staff would be able to prevent anyone unauthorised
from accessing patient records.
Records were legible and contained the right details about each patients’ care including the
presenting complaint, allergies and pain. Doctors and nurses also wrote individual notes about
care.
When patients transferred to a new team, staff told us they did not experience delays in accessing
their records.
Medicines
The service used systems and processes to safely prescribe, administer, record and store
medicines.
Staff followed systems and processes when safely prescribing, administering, recording and
storing medicines. Medicines were stored in locked cabinets in locked rooms. Keys to access
medicines were held by designated, qualified members of staff.
20190416 900885 Post-inspection Evidence appendix template v4 Page 42
Staff reviewed patients' medicines regularly and provided specific advice to patients and carers
about their medicines. Pharmacy staff provided support to ward staff and ensured medicines were
restocked.
Staff stored and managed medicines and prescribing documents in line with the trust’s policy. We
checked a range of medicines in different areas of the urgent and emergency department.
Medicines were stored appropriately and were within expiry date. Controlled drugs were checked
daily to help ensure stock levels were correct. There was a dedicated pharmacist allocated to the
emergency department seven days per week. They supported the checking of medicines and
were able to offer support and guidance to staff if required.
Staff followed current national practice to check patients had the correct medicines. We observed
staff checking patients’ names and dates of birth before administering medicines. Patient Group
Directions (PGDs) were in place for nursing staff. PGDs allow healthcare professionals to supply
and administer specified medicines to pre-defined groups of patients without a prescription. The
department had introduced a sepsis PGD, which meant all staff were able to administer medicines
for sepsis patients, other than those staff who were on long term leave.
The service had systems to ensure staff knew about safety alerts and incidents, so patients
received their medicines safely. Any medicines incidents and errors were recorded on incident
recording systems and any alerts were disseminated to staff during huddles.
We checked three fridges in the emergency department and found two of them had temperatures
checked daily, however, the fridge in resus had nine dates in October 2019 where the temperature
had not been checked. The trust had an action plan in place to improve compliance. Actions were
assigned to individuals with completion dates. We found the fridge temperatures were in range.
Incidents
The service managed patient safety incidents well. Staff recognised and reported incidents
and near misses and reported them appropriately. Managers investigated incidents and
shared lessons learned with the whole team and the wider service. When things went
wrong, staff apologised and gave patients honest information and suitable support.
Managers ensured that actions from patient safety alerts were implemented and monitored.
Staff knew what incidents to report and how to report them. Staff understood their responsibilities
to raise concerns and report them using the trust’s electronic reporting system. There were
processes in place for investigating incidents and staff informed us that feedback was shared at a
local level by their managers.
Staff raised concerns and reported incidents and near misses in line with trust policy. Staff could
describe the types of incidents that required reporting. A patient fall occurred in the emergency
department during our inspection. We observed a staff member call for help and staff responded.
A doctor attended shortly after to review the patient. The incident was promptly documented via
the electronic reporting system.
Never Events
The service reported no never events.
Never events are serious patient safety incidents that should not happen if healthcare providers
follow national guidance on how to prevent them. Each never event type has the potential to cause
serious patient harm or death but neither need have happened for an incident to be a never event.
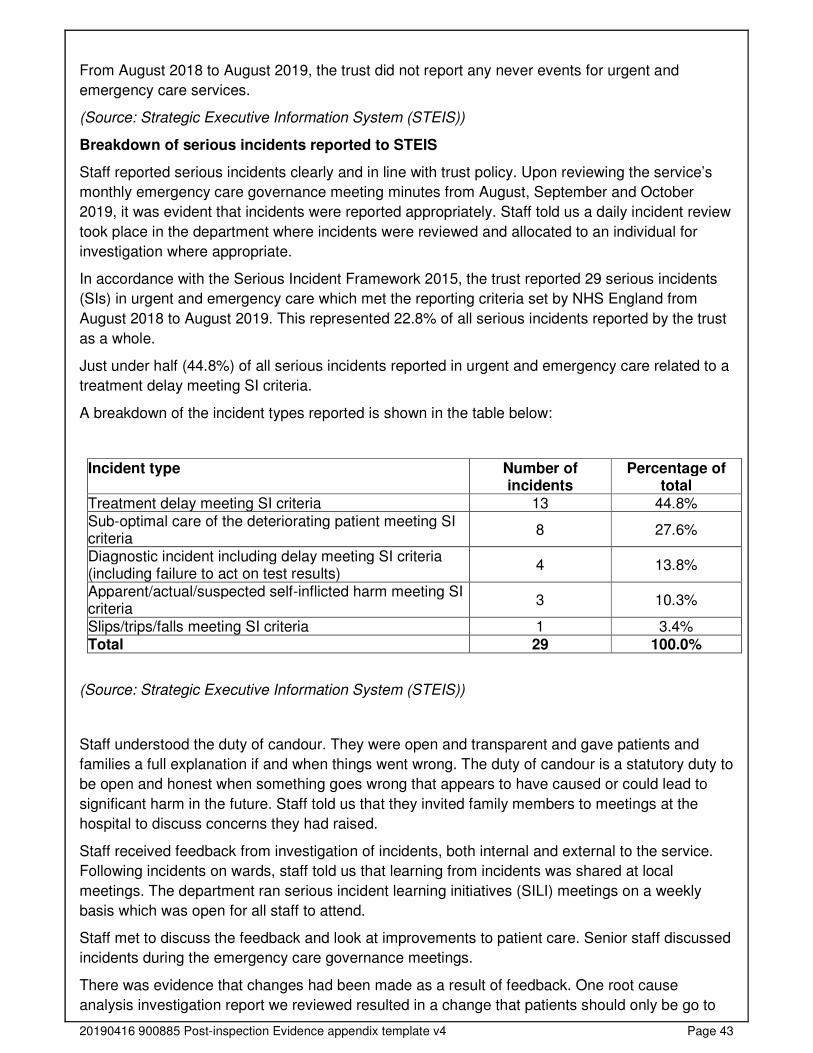
20190416 900885 Post-inspection Evidence appendix template v4 Page 43
From August 2018 to August 2019, the trust did not report any never events for urgent and
emergency care services.
(Source: Strategic Executive Information System (STEIS))
Breakdown of serious incidents reported to STEIS
Staff reported serious incidents clearly and in line with trust policy. Upon reviewing the service’s
monthly emergency care governance meeting minutes from August, September and October
2019, it was evident that incidents were reported appropriately. Staff told us a daily incident review
took place in the department where incidents were reviewed and allocated to an individual for
investigation where appropriate.
In accordance with the Serious Incident Framework 2015, the trust reported 29 serious incidents
(SIs) in urgent and emergency care which met the reporting criteria set by NHS England from
August 2018 to August 2019. This represented 22.8% of all serious incidents reported by the trust
as a whole.
Just under half (44.8%) of all serious incidents reported in urgent and emergency care related to a
treatment delay meeting SI criteria.
A breakdown of the incident types reported is shown in the table below:
Incident type Number of incidents
Percentage of total
Treatment delay meeting SI criteria 13 44.8% Sub-optimal care of the deteriorating patient meeting SI criteria
8 27.6%
Diagnostic incident including delay meeting SI criteria (including failure to act on test results)
4 13.8%
Apparent/actual/suspected self-inflicted harm meeting SI criteria
3 10.3%
Slips/trips/falls meeting SI criteria 1 3.4% Total 29 100.0%
(Source: Strategic Executive Information System (STEIS))
Staff understood the duty of candour. They were open and transparent and gave patients and
families a full explanation if and when things went wrong. The duty of candour is a statutory duty to
be open and honest when something goes wrong that appears to have caused or could lead to
significant harm in the future. Staff told us that they invited family members to meetings at the
hospital to discuss concerns they had raised.
Staff received feedback from investigation of incidents, both internal and external to the service.
Following incidents on wards, staff told us that learning from incidents was shared at local
meetings. The department ran serious incident learning initiatives (SILI) meetings on a weekly
basis which was open for all staff to attend.
Staff met to discuss the feedback and look at improvements to patient care. Senior staff discussed
incidents during the emergency care governance meetings.
There was evidence that changes had been made as a result of feedback. One root cause
analysis investigation report we reviewed resulted in a change that patients should only be go to
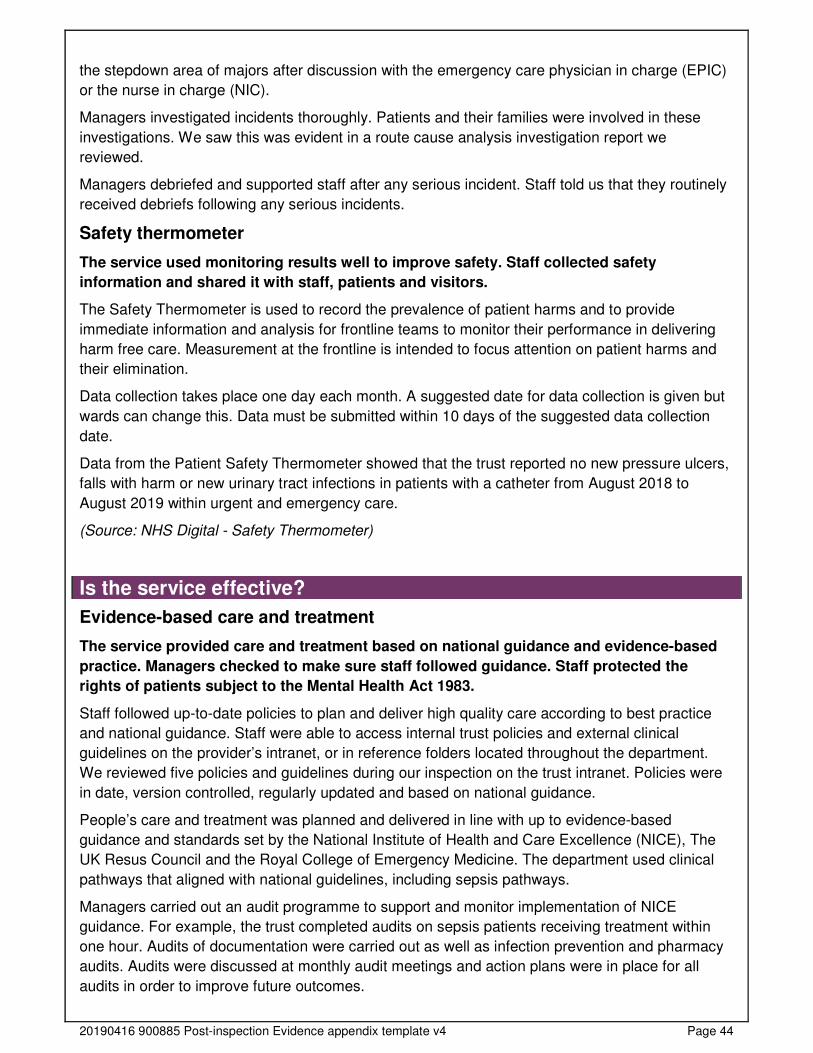
20190416 900885 Post-inspection Evidence appendix template v4 Page 44
the stepdown area of majors after discussion with the emergency care physician in charge (EPIC)
or the nurse in charge (NIC).
Managers investigated incidents thoroughly. Patients and their families were involved in these
investigations. We saw this was evident in a route cause analysis investigation report we
reviewed.
Managers debriefed and supported staff after any serious incident. Staff told us that they routinely
received debriefs following any serious incidents.
Safety thermometer
The service used monitoring results well to improve safety. Staff collected safety
information and shared it with staff, patients and visitors.
The Safety Thermometer is used to record the prevalence of patient harms and to provide
immediate information and analysis for frontline teams to monitor their performance in delivering
harm free care. Measurement at the frontline is intended to focus attention on patient harms and
their elimination.
Data collection takes place one day each month. A suggested date for data collection is given but
wards can change this. Data must be submitted within 10 days of the suggested data collection
date.
Data from the Patient Safety Thermometer showed that the trust reported no new pressure ulcers,
falls with harm or new urinary tract infections in patients with a catheter from August 2018 to
August 2019 within urgent and emergency care.
(Source: NHS Digital - Safety Thermometer)
Is the service effective?
Evidence-based care and treatment
The service provided care and treatment based on national guidance and evidence-based
practice. Managers checked to make sure staff followed guidance. Staff protected the
rights of patients subject to the Mental Health Act 1983.
Staff followed up-to-date policies to plan and deliver high quality care according to best practice
and national guidance. Staff were able to access internal trust policies and external clinical
guidelines on the provider’s intranet, or in reference folders located throughout the department.
We reviewed five policies and guidelines during our inspection on the trust intranet. Policies were
in date, version controlled, regularly updated and based on national guidance.
People’s care and treatment was planned and delivered in line with up to evidence-based
guidance and standards set by the National Institute of Health and Care Excellence (NICE), The
UK Resus Council and the Royal College of Emergency Medicine. The department used clinical
pathways that aligned with national guidelines, including sepsis pathways.
Managers carried out an audit programme to support and monitor implementation of NICE
guidance. For example, the trust completed audits on sepsis patients receiving treatment within
one hour. Audits of documentation were carried out as well as infection prevention and pharmacy
audits. Audits were discussed at monthly audit meetings and action plans were in place for all
audits in order to improve future outcomes.
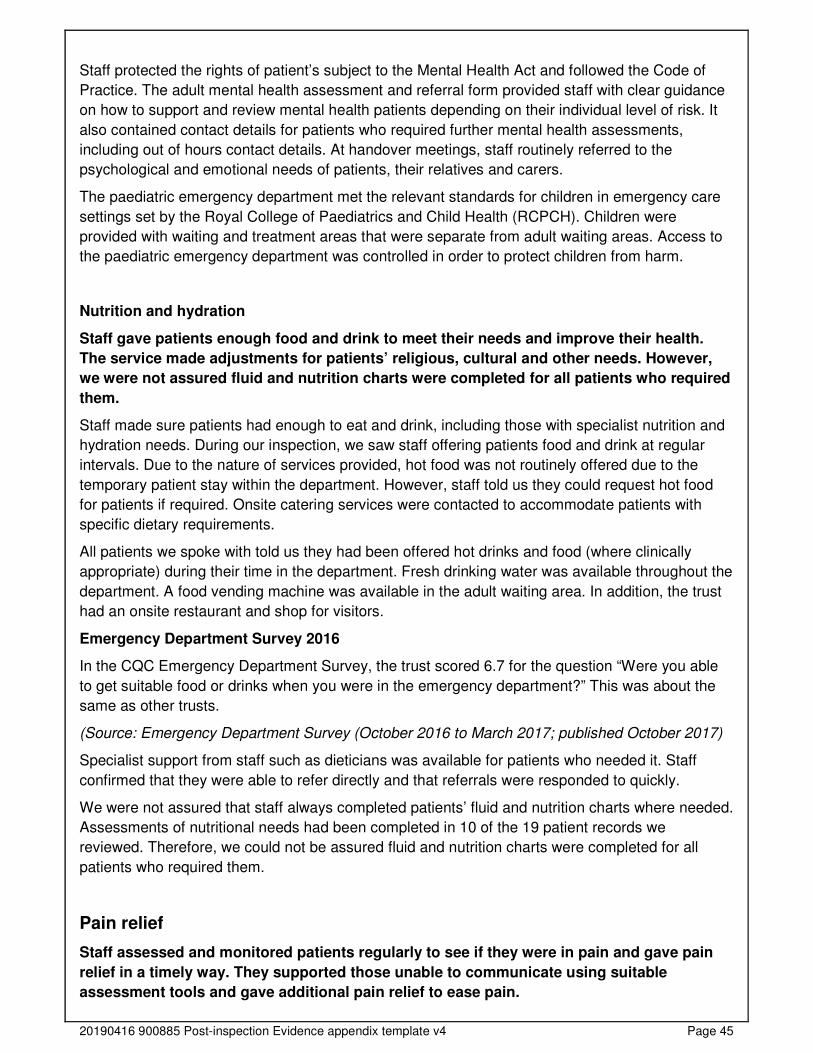
20190416 900885 Post-inspection Evidence appendix template v4 Page 45
Staff protected the rights of patient’s subject to the Mental Health Act and followed the Code of
Practice. The adult mental health assessment and referral form provided staff with clear guidance
on how to support and review mental health patients depending on their individual level of risk. It
also contained contact details for patients who required further mental health assessments,
including out of hours contact details. At handover meetings, staff routinely referred to the
psychological and emotional needs of patients, their relatives and carers.
The paediatric emergency department met the relevant standards for children in emergency care
settings set by the Royal College of Paediatrics and Child Health (RCPCH). Children were
provided with waiting and treatment areas that were separate from adult waiting areas. Access to
the paediatric emergency department was controlled in order to protect children from harm.
Nutrition and hydration
Staff gave patients enough food and drink to meet their needs and improve their health.
The service made adjustments for patients’ religious, cultural and other needs. However,
we were not assured fluid and nutrition charts were completed for all patients who required
them.
Staff made sure patients had enough to eat and drink, including those with specialist nutrition and
hydration needs. During our inspection, we saw staff offering patients food and drink at regular
intervals. Due to the nature of services provided, hot food was not routinely offered due to the
temporary patient stay within the department. However, staff told us they could request hot food
for patients if required. Onsite catering services were contacted to accommodate patients with
specific dietary requirements.
All patients we spoke with told us they had been offered hot drinks and food (where clinically
appropriate) during their time in the department. Fresh drinking water was available throughout the
department. A food vending machine was available in the adult waiting area. In addition, the trust
had an onsite restaurant and shop for visitors.
Emergency Department Survey 2016
In the CQC Emergency Department Survey, the trust scored 6.7 for the question “Were you able
to get suitable food or drinks when you were in the emergency department?” This was about the
same as other trusts.
(Source: Emergency Department Survey (October 2016 to March 2017; published October 2017)
Specialist support from staff such as dieticians was available for patients who needed it. Staff
confirmed that they were able to refer directly and that referrals were responded to quickly.
We were not assured that staff always completed patients’ fluid and nutrition charts where needed.
Assessments of nutritional needs had been completed in 10 of the 19 patient records we
reviewed. Therefore, we could not be assured fluid and nutrition charts were completed for all
patients who required them.
Pain relief
Staff assessed and monitored patients regularly to see if they were in pain and gave pain
relief in a timely way. They supported those unable to communicate using suitable
assessment tools and gave additional pain relief to ease pain.
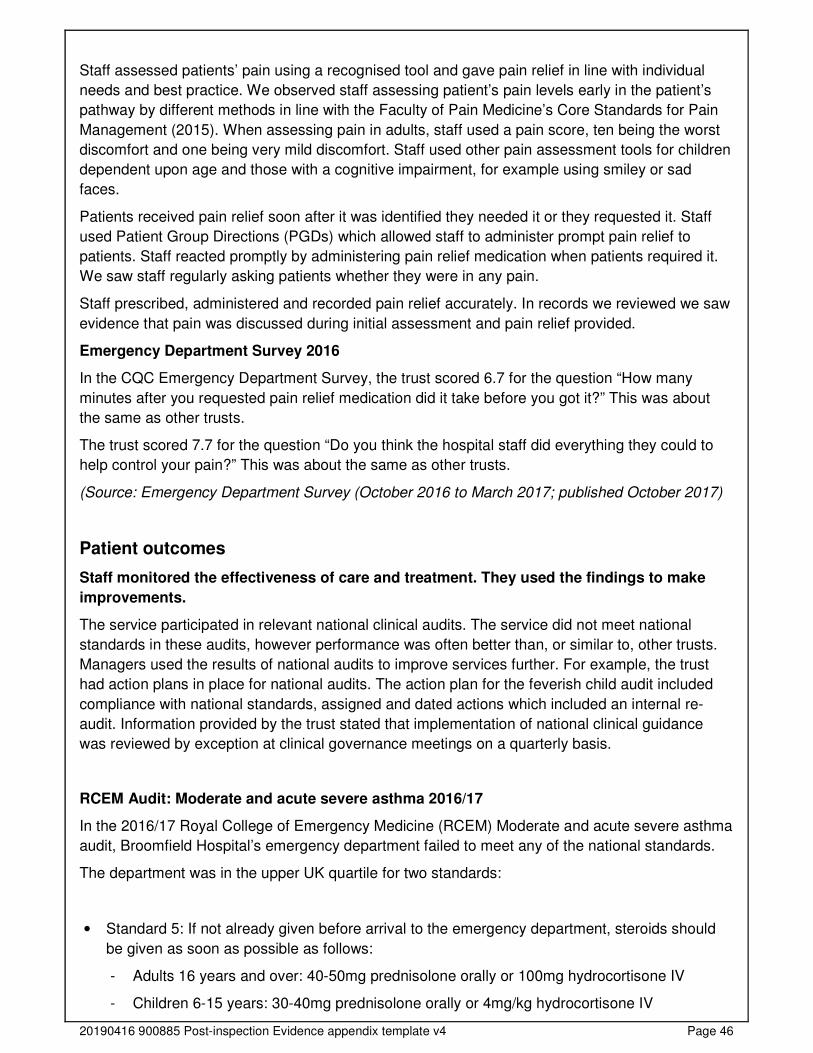
20190416 900885 Post-inspection Evidence appendix template v4 Page 46
Staff assessed patients’ pain using a recognised tool and gave pain relief in line with individual
needs and best practice. We observed staff assessing patient’s pain levels early in the patient’s
pathway by different methods in line with the Faculty of Pain Medicine’s Core Standards for Pain
Management (2015). When assessing pain in adults, staff used a pain score, ten being the worst
discomfort and one being very mild discomfort. Staff used other pain assessment tools for children
dependent upon age and those with a cognitive impairment, for example using smiley or sad
faces.
Patients received pain relief soon after it was identified they needed it or they requested it. Staff
used Patient Group Directions (PGDs) which allowed staff to administer prompt pain relief to
patients. Staff reacted promptly by administering pain relief medication when patients required it.
We saw staff regularly asking patients whether they were in any pain.
Staff prescribed, administered and recorded pain relief accurately. In records we reviewed we saw
evidence that pain was discussed during initial assessment and pain relief provided.
Emergency Department Survey 2016
In the CQC Emergency Department Survey, the trust scored 6.7 for the question “How many
minutes after you requested pain relief medication did it take before you got it?” This was about
the same as other trusts.
The trust scored 7.7 for the question “Do you think the hospital staff did everything they could to
help control your pain?” This was about the same as other trusts.
(Source: Emergency Department Survey (October 2016 to March 2017; published October 2017)
Patient outcomes
Staff monitored the effectiveness of care and treatment. They used the findings to make
improvements.
The service participated in relevant national clinical audits. The service did not meet national
standards in these audits, however performance was often better than, or similar to, other trusts.
Managers used the results of national audits to improve services further. For example, the trust
had action plans in place for national audits. The action plan for the feverish child audit included
compliance with national standards, assigned and dated actions which included an internal re-
audit. Information provided by the trust stated that implementation of national clinical guidance
was reviewed by exception at clinical governance meetings on a quarterly basis.
RCEM Audit: Moderate and acute severe asthma 2016/17
In the 2016/17 Royal College of Emergency Medicine (RCEM) Moderate and acute severe asthma
audit, Broomfield Hospital’s emergency department failed to meet any of the national standards.
The department was in the upper UK quartile for two standards:
• Standard 5: If not already given before arrival to the emergency department, steroids should
be given as soon as possible as follows:
- Adults 16 years and over: 40-50mg prednisolone orally or 100mg hydrocortisone IV
- Children 6-15 years: 30-40mg prednisolone orally or 4mg/kg hydrocortisone IV
20190416 900885 Post-inspection Evidence appendix template v4 Page 47
- Children 2-5 years: 20mg prednisolone orally or 4mg/kg hydrocortisone IV
o Standard 5b (fundamental): within 4 hours (moderate). This department: 61.2%; UK:
28%.
• Standard 9 (fundamental): Discharged patients should have oral prednisolone prescribed as
follows:
- Adults 16 years and over: 40-50mg prednisolone for 5 days
- Children 6-15 years: 30-40mg prednisolone for 3 days
- Children 2-5 years: 20mg prednisolone for 3 days
o This department: 76.2%; UK: 52%.
The department’s results for the remaining five standards were all within the middle 50% of
results.
• Standard 1a (fundamental): Oxygen should be given on arrival to maintain a saturation of 94-
98%. This department: 20.2%; UK: 19%.
• Standard 2a (fundamental): As per RCEM standards, vital signs should be measured and
recorded on arrival at the emergency department. This department: 26.3%; UK: 26%.
• Standard 3 (fundamental): High dose nebulised Beta 2 antagonist bronchodilator should be
given within 10 minutes of arrival at the emergency department. This department: 31.3%; UK:
25%.
• Standard 4 (fundamental): Add nebulised Ipratropium Bromide if there is a poor response to
nebulised Beta 2 antagonist bronchodilator therapy. This department: 82.8%; UK: 77%.
• Standard 5: If not already given before arrival to the emergency department, steroids should
be given as soon as possible as follows:
- Adults 16 years and over: 40-50mg prednisolone orally or 100mg hydrocortisone IV
- Children 6-15 years: 30-40mg prednisolone orally or 4mg/kg hydrocortisone IV
- Children 2-5 years: 20mg prednisolone orally or 4mg/kg hydrocortisone IV
o Standard 5a (fundamental): within 60 minutes of arrival (acute severe). This department:
32.3%; UK: 19%.
(Source: Royal College of Emergency Medicine)
RCEM Audit: Consultant sign-off 2016/17
In the 2016/17 Consultant sign-off audit, Broomfield Hospital’s emergency department failed to
meet any of the national standards.
The department was in the lower UK quartile for two standards:
20190416 900885 Post-inspection Evidence appendix template v4 Page 48
• Standard 1 (developmental): Consultant reviewed: atraumatic chest pain in patients aged 30
years and over. This department: 4.9%; UK: 11%.
• Standard 2 (developmental): Consultant reviewed: fever in children under 1 year of age. This
department: 0.0%; UK: 8%.
The department’s results for the remaining two standards were all within the middle 50% of
results.
• Standard 3 (fundamental): Consultant reviewed: patients making an unscheduled return to the
emergency department with the same condition within 72 hours of discharge. This department:
16.7%; UK: 12%.
• Standard 4 (developmental): Consultant reviewed: abdominal pain in patients aged 70 years
and over. This department: 5.9%; UK: 10%.
(Source: Royal College of Emergency Medicine)
RCEM Audit: Severe sepsis and septic shock 2016/17
In the 2016/17 Severe sepsis and septic shock audit, Broomfield Hospital’s emergency
department failed to meet any of the national standards.
The department was in the upper UK quartile for two standards:
• Standard 5: Blood cultures obtained within one hour of arrival. This department: 68.0%; UK:
44.9%.
• Standard 8: Urine output measurement/fluid balance chart instituted within four hours of
arrival. This department: 38.8%; UK: 18.4%.
The department’s results for the remaining six standards were all within the middle 50% of results.
• Standard 1: Respiratory rate, oxygen saturations (SaO2), supplemental oxygen requirement,
temperature, blood pressure, heart rate, level of consciousness (AVPU or GCS) and capillary
blood glucose recorded on arrival. This department: 70.0%; UK: 69.1%.
• Standard 2: Review by a senior (ST4+ or equivalent) emergency department medic or
involvement of critical care medic (including the outreach team or equivalent) before leaving
the emergency department. This department: 62.0%; UK: 64.6%.
• Standard 3: O2 was initiated to maintain SaO2>94% (unless there is a documented reason not
to) within one hour of arrival. This department: 55.6%; UK: 30.4%.
• Standard 4: Serum lactate measured within one hour of arrival. This department: 70.0%; UK:
60.0%.
• Standard 6: Fluids – first intravenous crystalloid fluid bolus (up to 30 mL/Kg) given within one
hour of arrival. This department: 49.0%; UK: 43.2%.
• Standard 7: Antibiotics administered: Within one hour of arrival. This department: 52.0%; UK:
44.4%.
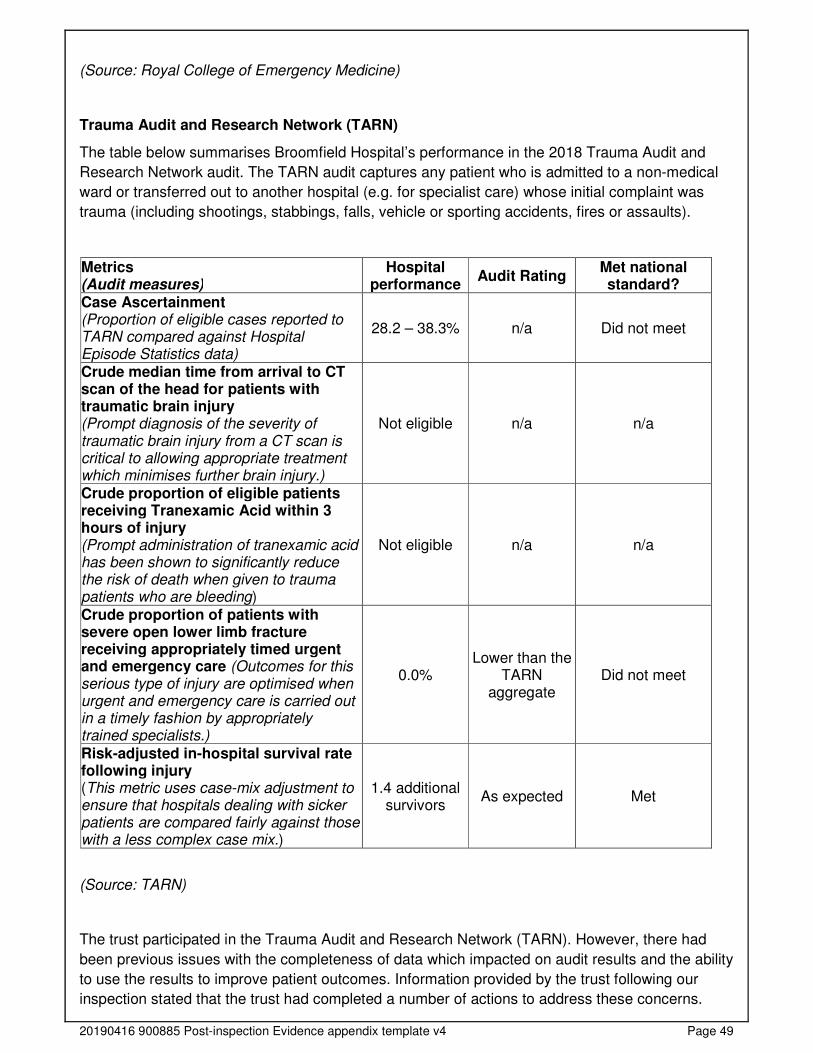
20190416 900885 Post-inspection Evidence appendix template v4 Page 49
(Source: Royal College of Emergency Medicine)
Trauma Audit and Research Network (TARN)
The table below summarises Broomfield Hospital’s performance in the 2018 Trauma Audit and
Research Network audit. The TARN audit captures any patient who is admitted to a non-medical
ward or transferred out to another hospital (e.g. for specialist care) whose initial complaint was
trauma (including shootings, stabbings, falls, vehicle or sporting accidents, fires or assaults).
Metrics (Audit measures)
Hospital performance
Audit Rating Met national standard?
Case Ascertainment (Proportion of eligible cases reported to TARN compared against Hospital Episode Statistics data)
28.2 – 38.3% n/a Did not meet
Crude median time from arrival to CT scan of the head for patients with traumatic brain injury (Prompt diagnosis of the severity of traumatic brain injury from a CT scan is critical to allowing appropriate treatment which minimises further brain injury.)
Not eligible n/a n/a
Crude proportion of eligible patients receiving Tranexamic Acid within 3 hours of injury (Prompt administration of tranexamic acid has been shown to significantly reduce the risk of death when given to trauma patients who are bleeding)
Not eligible n/a n/a
Crude proportion of patients with severe open lower limb fracture receiving appropriately timed urgent and emergency care (Outcomes for this serious type of injury are optimised when urgent and emergency care is carried out in a timely fashion by appropriately trained specialists.)
0.0% Lower than the
TARN aggregate
Did not meet
Risk-adjusted in-hospital survival rate following injury (This metric uses case-mix adjustment to ensure that hospitals dealing with sicker patients are compared fairly against those with a less complex case mix.)
1.4 additional survivors
As expected Met
(Source: TARN)
The trust participated in the Trauma Audit and Research Network (TARN). However, there had
been previous issues with the completeness of data which impacted on audit results and the ability
to use the results to improve patient outcomes. Information provided by the trust following our
inspection stated that the trust had completed a number of actions to address these concerns.
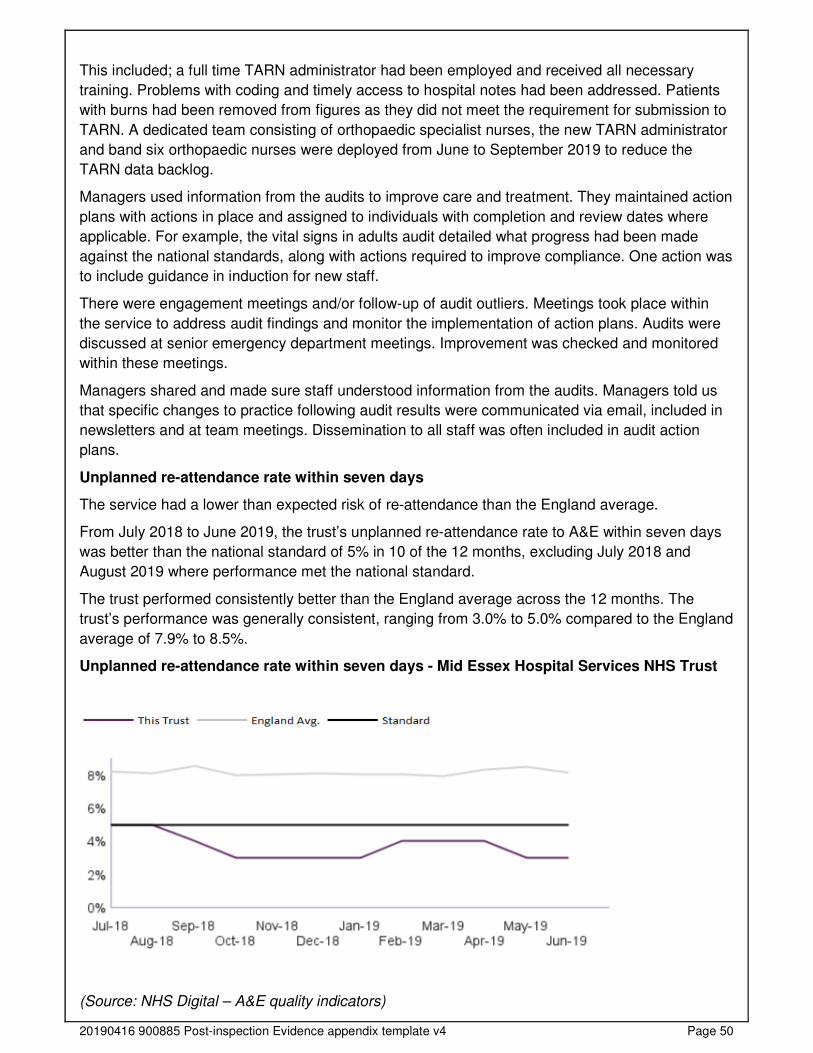
20190416 900885 Post-inspection Evidence appendix template v4 Page 50
This included; a full time TARN administrator had been employed and received all necessary
training. Problems with coding and timely access to hospital notes had been addressed. Patients
with burns had been removed from figures as they did not meet the requirement for submission to
TARN. A dedicated team consisting of orthopaedic specialist nurses, the new TARN administrator
and band six orthopaedic nurses were deployed from June to September 2019 to reduce the
TARN data backlog.
Managers used information from the audits to improve care and treatment. They maintained action
plans with actions in place and assigned to individuals with completion and review dates where
applicable. For example, the vital signs in adults audit detailed what progress had been made
against the national standards, along with actions required to improve compliance. One action was
to include guidance in induction for new staff.
There were engagement meetings and/or follow-up of audit outliers. Meetings took place within
the service to address audit findings and monitor the implementation of action plans. Audits were
discussed at senior emergency department meetings. Improvement was checked and monitored
within these meetings.
Managers shared and made sure staff understood information from the audits. Managers told us
that specific changes to practice following audit results were communicated via email, included in
newsletters and at team meetings. Dissemination to all staff was often included in audit action
plans.
Unplanned re-attendance rate within seven days
The service had a lower than expected risk of re-attendance than the England average.
From July 2018 to June 2019, the trust’s unplanned re-attendance rate to A&E within seven days
was better than the national standard of 5% in 10 of the 12 months, excluding July 2018 and
August 2019 where performance met the national standard.
The trust performed consistently better than the England average across the 12 months. The
trust’s performance was generally consistent, ranging from 3.0% to 5.0% compared to the England
average of 7.9% to 8.5%.
Unplanned re-attendance rate within seven days - Mid Essex Hospital Services NHS Trust
(Source: NHS Digital – A&E quality indicators)
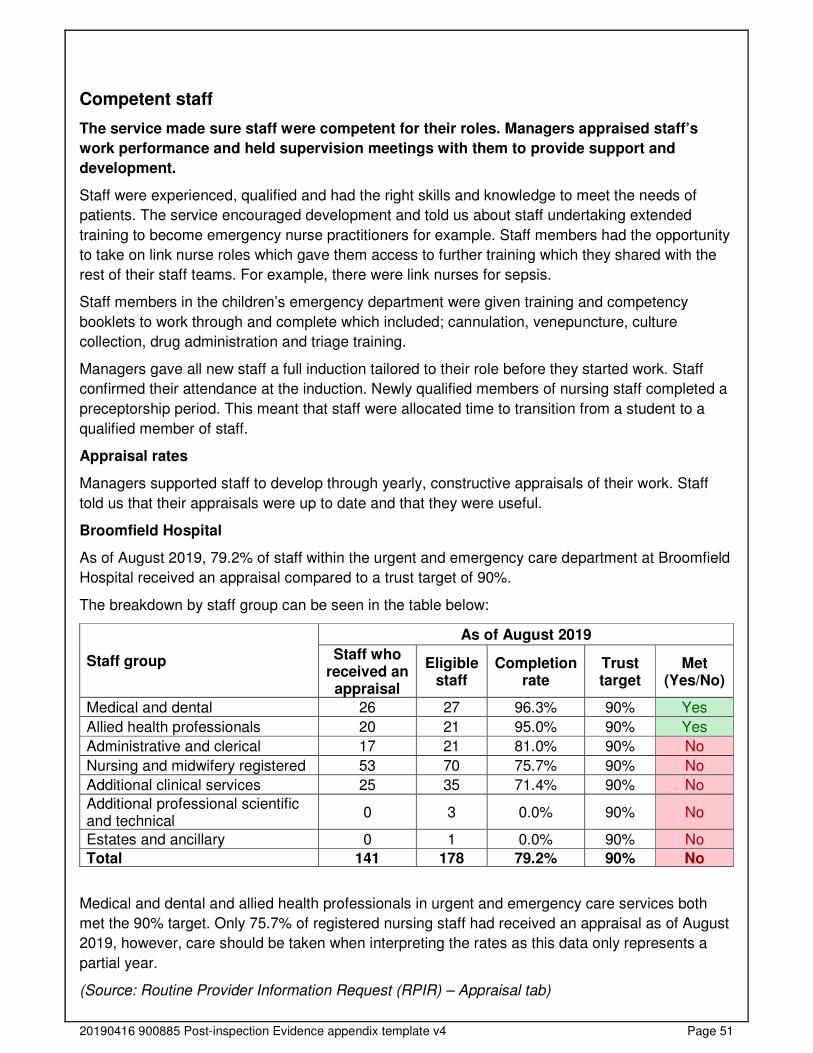
20190416 900885 Post-inspection Evidence appendix template v4 Page 51
Competent staff
The service made sure staff were competent for their roles. Managers appraised staff’s
work performance and held supervision meetings with them to provide support and
development.
Staff were experienced, qualified and had the right skills and knowledge to meet the needs of
patients. The service encouraged development and told us about staff undertaking extended
training to become emergency nurse practitioners for example. Staff members had the opportunity
to take on link nurse roles which gave them access to further training which they shared with the
rest of their staff teams. For example, there were link nurses for sepsis.
Staff members in the children’s emergency department were given training and competency
booklets to work through and complete which included; cannulation, venepuncture, culture
collection, drug administration and triage training.
Managers gave all new staff a full induction tailored to their role before they started work. Staff
confirmed their attendance at the induction. Newly qualified members of nursing staff completed a
preceptorship period. This meant that staff were allocated time to transition from a student to a
qualified member of staff.
Appraisal rates
Managers supported staff to develop through yearly, constructive appraisals of their work. Staff
told us that their appraisals were up to date and that they were useful.
Broomfield Hospital
As of August 2019, 79.2% of staff within the urgent and emergency care department at Broomfield
Hospital received an appraisal compared to a trust target of 90%.
The breakdown by staff group can be seen in the table below:
Staff group
As of August 2019
Staff who received an appraisal
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Medical and dental 26 27 96.3% 90% Yes
Allied health professionals 20 21 95.0% 90% Yes
Administrative and clerical 17 21 81.0% 90% No
Nursing and midwifery registered 53 70 75.7% 90% No
Additional clinical services 25 35 71.4% 90% No
Additional professional scientific and technical
0 3 0.0% 90% No
Estates and ancillary 0 1 0.0% 90% No
Total 141 178 79.2% 90% No
Medical and dental and allied health professionals in urgent and emergency care services both
met the 90% target. Only 75.7% of registered nursing staff had received an appraisal as of August
2019, however, care should be taken when interpreting the rates as this data only represents a
partial year.
(Source: Routine Provider Information Request (RPIR) – Appraisal tab)
20190416 900885 Post-inspection Evidence appendix template v4 Page 52
Managers supported nursing staff to develop through regular, constructive clinical supervision of
their work. Nursing staff told us that their development needs were identified in their annual
personal development plan meetings. Managers provided ad-hoc supervision and staff told us that
managers were approachable and highly supportive.
Managers supported medical staff to develop through regular, constructive clinical supervision of
their work. Medical staff worked together across the service to provide support, learning and
debriefs to their colleagues. Junior medical staff told us they received support and supervision
from their senior colleagues.
The clinical educator supported the learning and development needs of staff. Staff were assessed
across several competencies before they were allowed to perform certain procedures. This
ensured staff were experienced, qualified and had the right skills and knowledge to meet the
needs of patients.
Managers identified any training needs their staff had and gave them the time and opportunity to
develop their skills and knowledge. Managers made sure staff received specialist training to
support staff in their role. Managers arranged clinical skills days within the service. These took
place on a six monthly basis and included skills such as cannulas, plaster and wound care.
Multidisciplinary working
Doctors, nurses and other healthcare professionals mostly worked together as a team to
benefit patients. They supported each other to provide good care.
Staff held regular and effective multidisciplinary meetings to discuss patients and improve their
care. Doctors, nurses and other healthcare professionals supported each other to provide good
care. We saw good multidisciplinary working practices within the department. Nurses and doctors
spoke highly of each other and we observed a cohesive relationship when dealing with patients.
Staff told us that they liaised with other departments when they needed to gain specialist input.
Occupational therapists and physiotherapists regularly attended the department to assess and
treat patients.
Staff worked across health care disciplines and with other agencies when required to care for
patients. During our inspection we saw staff working together as a team to assess and plan
ongoing care and treatment. We saw evidence in one set of patient notes we reviewed of a
safeguarding referral being made to the local authority.
Staff referred patients for mental health assessments when they showed signs of mental ill health,
depression. Staff described positive working relationships with the local mental health team. Staff
liaised with the local mental health team to arrange mental health act assessments when required.
Mental health staff were located within the trust premises during the day which promoted
integrated care for patients.
However, we found there were limited pathways established for patients requiring hospital stay.
Other than referring patients directly to ambulatory care, staff told us that there was a lack of clear
pathways from the emergency department. For example, staff told us that there was previously a
clear pathway from ED to gynaecology, however this was stopped following an incident. Staff told
us that re-establishing this and other pathways would be a priority.
20190416 900885 Post-inspection Evidence appendix template v4 Page 53
Seven-day services
Key services were available seven days a week to support timely patient care.
Staff could call for support from doctors and other disciplines and diagnostic services, including
mental health services, 24 hours a day, seven days a week. The department had 24 hour access
to key support services, such as pathology, allowing for blood test results to be obtained at any
time. It also had 24-hour access to key diagnostic imaging tests, including x-rays, computerised
tomography (CT) scans and magnetic resonance imaging (MRI) scans.
Support from the local mental health service was available 24 hours a day, seven days a week.
Staff knew how to refer to this service and knew the processes to follow when a mental health act
assessment was required. Staff told us that the local mental health service responded promptly to
referrals.
Health promotion
Staff gave patients practical support and advice to lead healthier lives.
The service had relevant information promoting healthy lifestyles and support on wards. Varied
information was provided to patients and their relatives on a range of topics, for example, mental
health and lifestyle. Information signposted patients to other relevant agencies, where appropriate.
Staff assessed each patient’s health when admitted and provided support for any individual needs
to live a healthier lifestyle.
Consent, Mental Capacity Act and Deprivation of Liberty Safeguards
Staff supported patients to make informed decisions about their care and treatment. They
followed national guidance to gain patients’ consent. They knew how to support patients
who lacked capacity to make their own decisions or were experiencing mental ill health.
They used agreed personalised measures that limited patients' liberty.
Staff understood how and when to assess whether a patient had the capacity to make decisions
about their care. Staff demonstrated that they understood the Mental Capacity Act and how to
apply it. The trust had a Mental Capacity Act (2005) Policy for staff to follow, which included when
to assess capacity and guidance for documentation of decisions about capacity.
Staff gained consent from patients for their care and treatment in line with legislation and
guidance. We saw evidence that consent had been gained in all of the patient records we
reviewed. This was clearly recorded.
When patients could not give consent, staff made decisions in their best interest, taking into
account patients’ wishes, culture and traditions. If patients were not well enough to provide
consent, staff discussed care or treatment with relatives, or made decisions in the patient’s best
interests.
Staff understood Gillick Competence and supported children who wished to make decisions about
their treatment. Staff in the paediatric emergency department could describe the Gillick
competence and how this would be used when assessing children’s capacity. Gillick competence
is a legal principle for assessing a child’s capacity to consent to medical treatment.
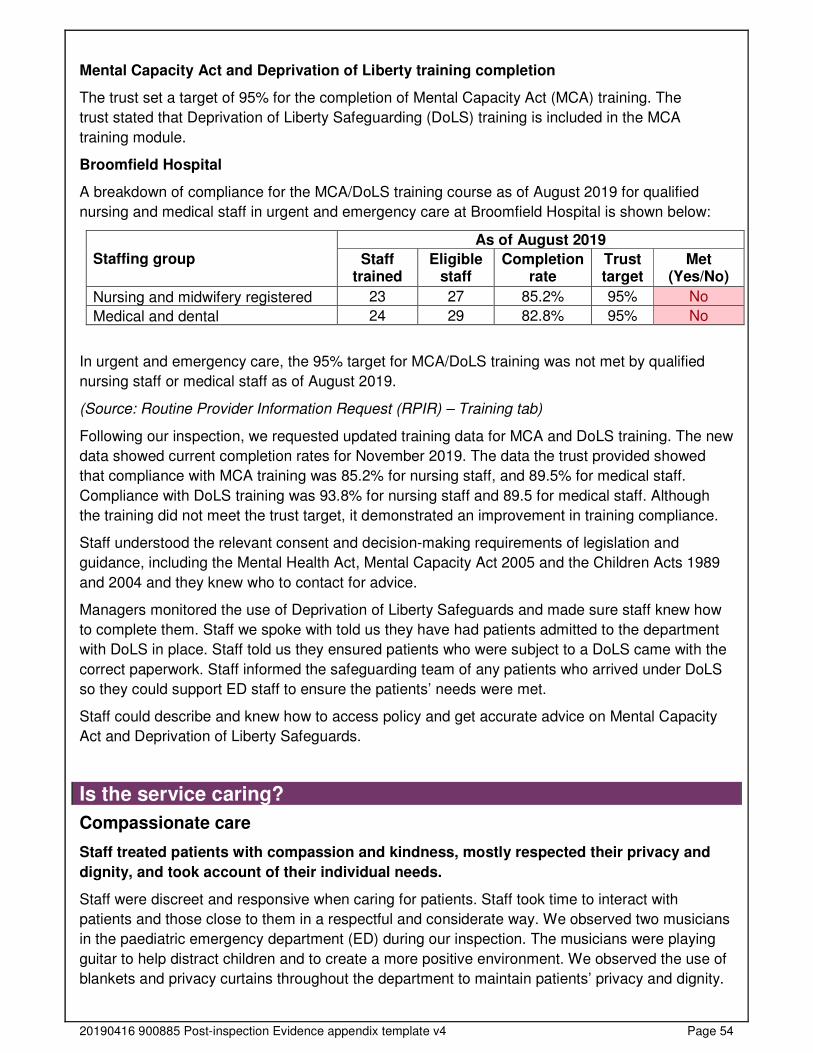
20190416 900885 Post-inspection Evidence appendix template v4 Page 54
Mental Capacity Act and Deprivation of Liberty training completion
The trust set a target of 95% for the completion of Mental Capacity Act (MCA) training. The
trust stated that Deprivation of Liberty Safeguarding (DoLS) training is included in the MCA
training module.
Broomfield Hospital
A breakdown of compliance for the MCA/DoLS training course as of August 2019 for qualified
nursing and medical staff in urgent and emergency care at Broomfield Hospital is shown below:
Staffing group
As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Nursing and midwifery registered 23 27 85.2% 95% No
Medical and dental 24 29 82.8% 95% No
In urgent and emergency care, the 95% target for MCA/DoLS training was not met by qualified
nursing staff or medical staff as of August 2019.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Following our inspection, we requested updated training data for MCA and DoLS training. The new
data showed current completion rates for November 2019. The data the trust provided showed
that compliance with MCA training was 85.2% for nursing staff, and 89.5% for medical staff.
Compliance with DoLS training was 93.8% for nursing staff and 89.5 for medical staff. Although
the training did not meet the trust target, it demonstrated an improvement in training compliance.
Staff understood the relevant consent and decision-making requirements of legislation and
guidance, including the Mental Health Act, Mental Capacity Act 2005 and the Children Acts 1989
and 2004 and they knew who to contact for advice.
Managers monitored the use of Deprivation of Liberty Safeguards and made sure staff knew how
to complete them. Staff we spoke with told us they have had patients admitted to the department
with DoLS in place. Staff told us they ensured patients who were subject to a DoLS came with the
correct paperwork. Staff informed the safeguarding team of any patients who arrived under DoLS
so they could support ED staff to ensure the patients’ needs were met.
Staff could describe and knew how to access policy and get accurate advice on Mental Capacity
Act and Deprivation of Liberty Safeguards.
Is the service caring?
Compassionate care
Staff treated patients with compassion and kindness, mostly respected their privacy and
dignity, and took account of their individual needs.
Staff were discreet and responsive when caring for patients. Staff took time to interact with
patients and those close to them in a respectful and considerate way. We observed two musicians
in the paediatric emergency department (ED) during our inspection. The musicians were playing
guitar to help distract children and to create a more positive environment. We observed the use of
blankets and privacy curtains throughout the department to maintain patients’ privacy and dignity.
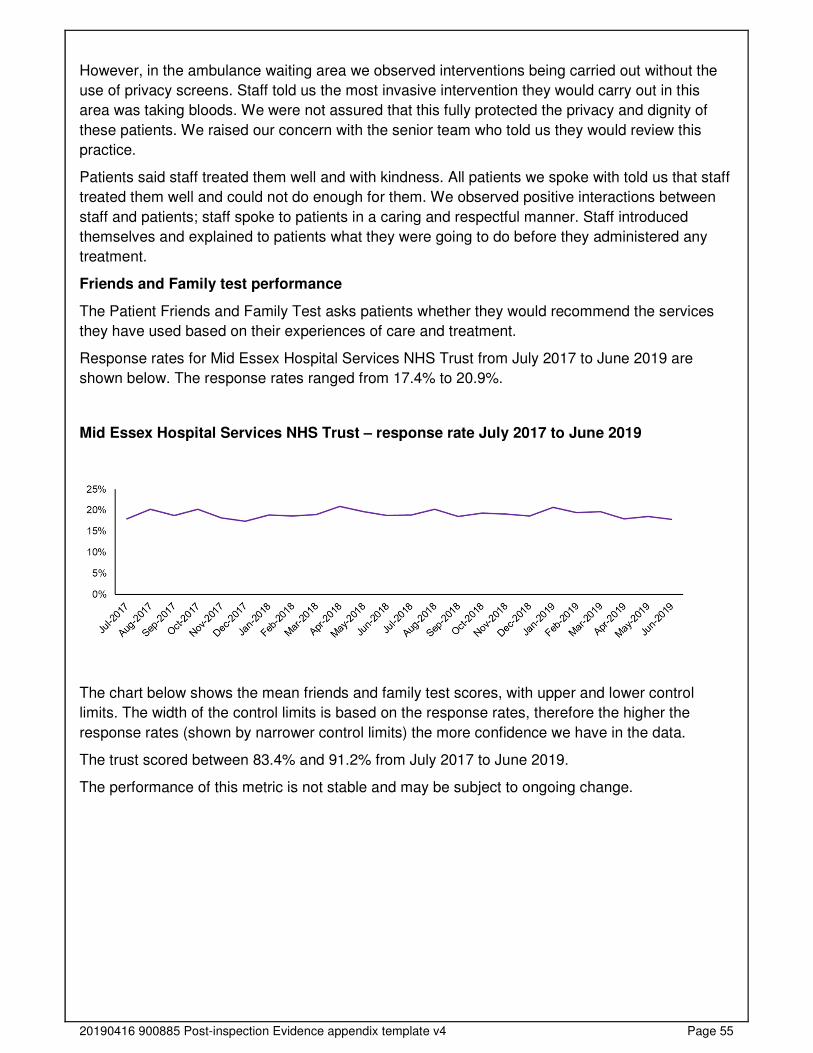
20190416 900885 Post-inspection Evidence appendix template v4 Page 55
However, in the ambulance waiting area we observed interventions being carried out without the
use of privacy screens. Staff told us the most invasive intervention they would carry out in this
area was taking bloods. We were not assured that this fully protected the privacy and dignity of
these patients. We raised our concern with the senior team who told us they would review this
practice.
Patients said staff treated them well and with kindness. All patients we spoke with told us that staff
treated them well and could not do enough for them. We observed positive interactions between
staff and patients; staff spoke to patients in a caring and respectful manner. Staff introduced
themselves and explained to patients what they were going to do before they administered any
treatment.
Friends and Family test performance
The Patient Friends and Family Test asks patients whether they would recommend the services
they have used based on their experiences of care and treatment.
Response rates for Mid Essex Hospital Services NHS Trust from July 2017 to June 2019 are
shown below. The response rates ranged from 17.4% to 20.9%.
Mid Essex Hospital Services NHS Trust – response rate July 2017 to June 2019
The chart below shows the mean friends and family test scores, with upper and lower control
limits. The width of the control limits is based on the response rates, therefore the higher the
response rates (shown by narrower control limits) the more confidence we have in the data.
The trust scored between 83.4% and 91.2% from July 2017 to June 2019.
The performance of this metric is not stable and may be subject to ongoing change.
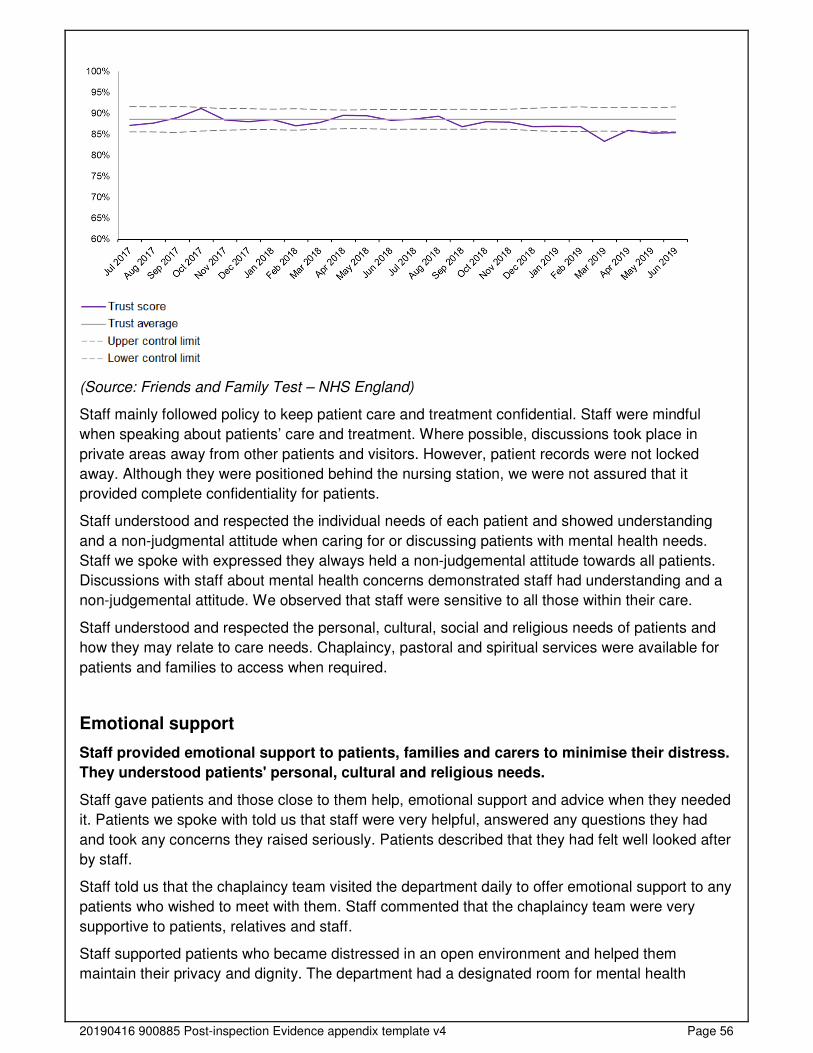
20190416 900885 Post-inspection Evidence appendix template v4 Page 56
(Source: Friends and Family Test – NHS England)
Staff mainly followed policy to keep patient care and treatment confidential. Staff were mindful
when speaking about patients’ care and treatment. Where possible, discussions took place in
private areas away from other patients and visitors. However, patient records were not locked
away. Although they were positioned behind the nursing station, we were not assured that it
provided complete confidentiality for patients.
Staff understood and respected the individual needs of each patient and showed understanding
and a non-judgmental attitude when caring for or discussing patients with mental health needs.
Staff we spoke with expressed they always held a non-judgemental attitude towards all patients.
Discussions with staff about mental health concerns demonstrated staff had understanding and a
non-judgemental attitude. We observed that staff were sensitive to all those within their care.
Staff understood and respected the personal, cultural, social and religious needs of patients and
how they may relate to care needs. Chaplaincy, pastoral and spiritual services were available for
patients and families to access when required.
Emotional support
Staff provided emotional support to patients, families and carers to minimise their distress.
They understood patients' personal, cultural and religious needs.
Staff gave patients and those close to them help, emotional support and advice when they needed
it. Patients we spoke with told us that staff were very helpful, answered any questions they had
and took any concerns they raised seriously. Patients described that they had felt well looked after
by staff.
Staff told us that the chaplaincy team visited the department daily to offer emotional support to any
patients who wished to meet with them. Staff commented that the chaplaincy team were very
supportive to patients, relatives and staff.
Staff supported patients who became distressed in an open environment and helped them
maintain their privacy and dignity. The department had a designated room for mental health
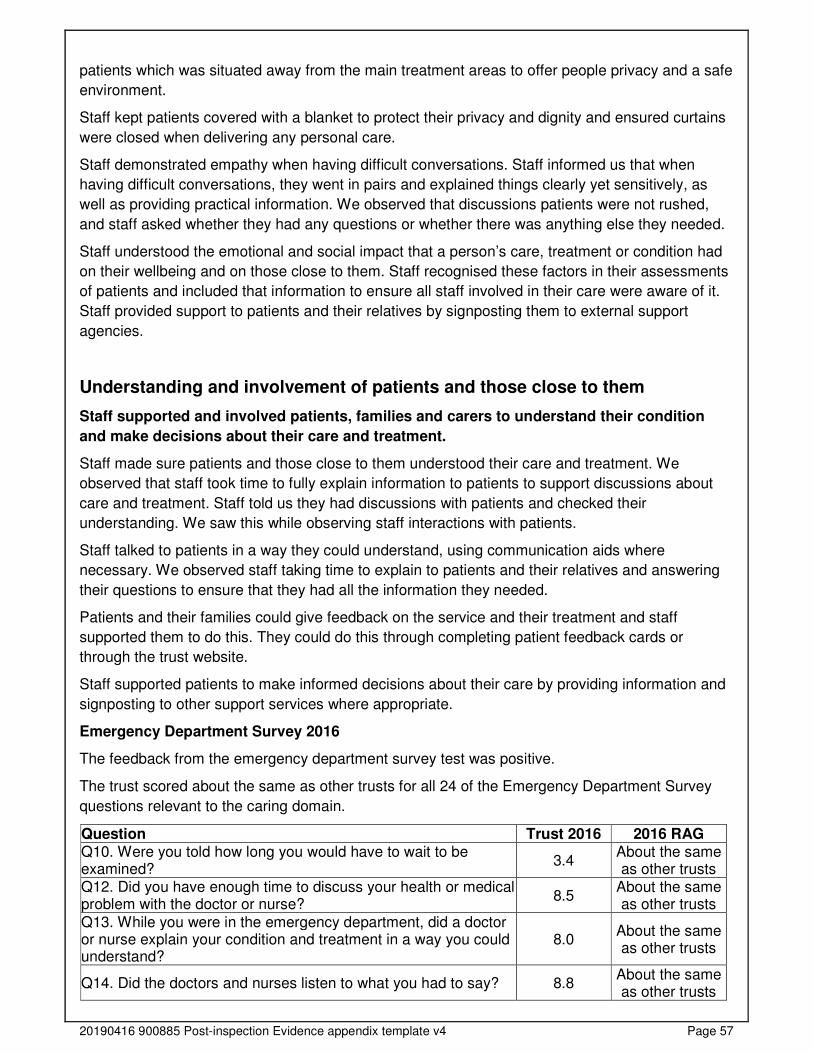
20190416 900885 Post-inspection Evidence appendix template v4 Page 57
patients which was situated away from the main treatment areas to offer people privacy and a safe
environment.
Staff kept patients covered with a blanket to protect their privacy and dignity and ensured curtains
were closed when delivering any personal care.
Staff demonstrated empathy when having difficult conversations. Staff informed us that when
having difficult conversations, they went in pairs and explained things clearly yet sensitively, as
well as providing practical information. We observed that discussions patients were not rushed,
and staff asked whether they had any questions or whether there was anything else they needed.
Staff understood the emotional and social impact that a person’s care, treatment or condition had
on their wellbeing and on those close to them. Staff recognised these factors in their assessments
of patients and included that information to ensure all staff involved in their care were aware of it.
Staff provided support to patients and their relatives by signposting them to external support
agencies.
Understanding and involvement of patients and those close to them
Staff supported and involved patients, families and carers to understand their condition
and make decisions about their care and treatment.
Staff made sure patients and those close to them understood their care and treatment. We
observed that staff took time to fully explain information to patients to support discussions about
care and treatment. Staff told us they had discussions with patients and checked their
understanding. We saw this while observing staff interactions with patients.
Staff talked to patients in a way they could understand, using communication aids where
necessary. We observed staff taking time to explain to patients and their relatives and answering
their questions to ensure that they had all the information they needed.
Patients and their families could give feedback on the service and their treatment and staff
supported them to do this. They could do this through completing patient feedback cards or
through the trust website.
Staff supported patients to make informed decisions about their care by providing information and
signposting to other support services where appropriate.
Emergency Department Survey 2016
The feedback from the emergency department survey test was positive.
The trust scored about the same as other trusts for all 24 of the Emergency Department Survey
questions relevant to the caring domain.
Question Trust 2016 2016 RAG Q10. Were you told how long you would have to wait to be examined?
3.4 About the same as other trusts
Q12. Did you have enough time to discuss your health or medical problem with the doctor or nurse?
8.5 About the same as other trusts
Q13. While you were in the emergency department, did a doctor or nurse explain your condition and treatment in a way you could understand?
8.0 About the same as other trusts
Q14. Did the doctors and nurses listen to what you had to say? 8.8 About the same as other trusts
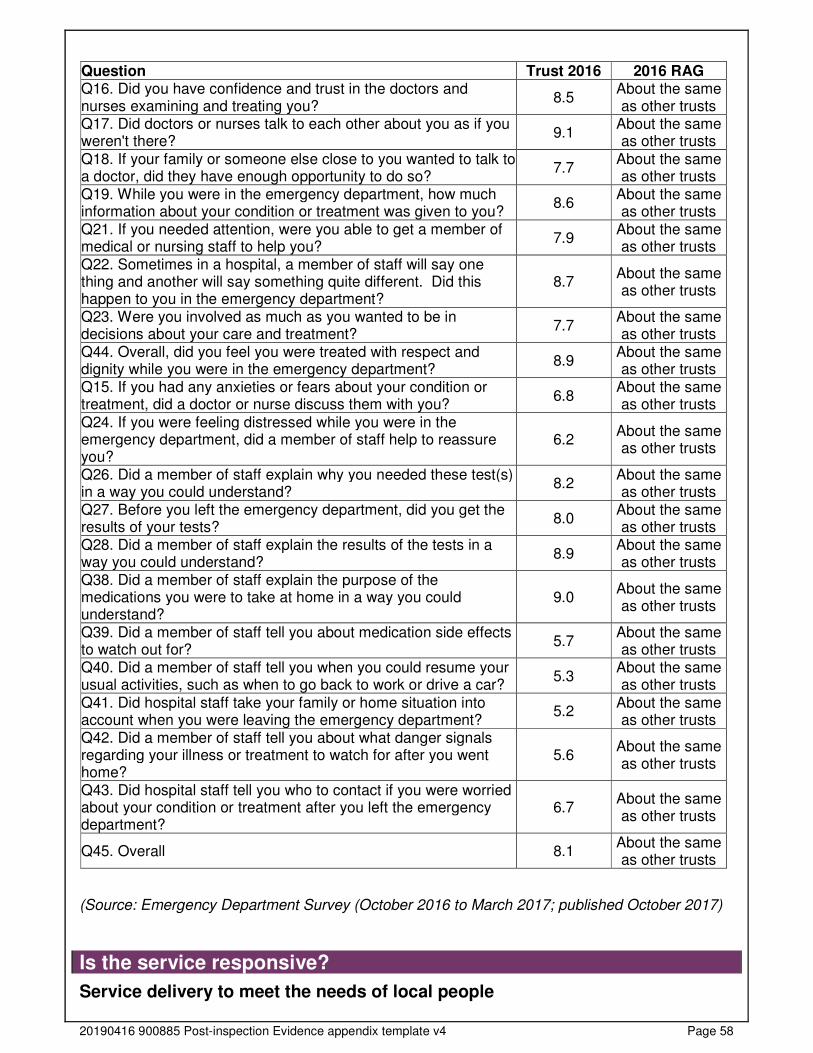
20190416 900885 Post-inspection Evidence appendix template v4 Page 58
Question Trust 2016 2016 RAG Q16. Did you have confidence and trust in the doctors and nurses examining and treating you?
8.5 About the same as other trusts
Q17. Did doctors or nurses talk to each other about you as if you weren't there?
9.1 About the same as other trusts
Q18. If your family or someone else close to you wanted to talk to a doctor, did they have enough opportunity to do so?
7.7 About the same as other trusts
Q19. While you were in the emergency department, how much information about your condition or treatment was given to you?
8.6 About the same as other trusts
Q21. If you needed attention, were you able to get a member of medical or nursing staff to help you?
7.9 About the same as other trusts
Q22. Sometimes in a hospital, a member of staff will say one thing and another will say something quite different. Did this happen to you in the emergency department?
8.7 About the same as other trusts
Q23. Were you involved as much as you wanted to be in decisions about your care and treatment?
7.7 About the same as other trusts
Q44. Overall, did you feel you were treated with respect and dignity while you were in the emergency department?
8.9 About the same as other trusts
Q15. If you had any anxieties or fears about your condition or treatment, did a doctor or nurse discuss them with you?
6.8 About the same as other trusts
Q24. If you were feeling distressed while you were in the emergency department, did a member of staff help to reassure you?
6.2 About the same as other trusts
Q26. Did a member of staff explain why you needed these test(s) in a way you could understand?
8.2 About the same as other trusts
Q27. Before you left the emergency department, did you get the results of your tests?
8.0 About the same as other trusts
Q28. Did a member of staff explain the results of the tests in a way you could understand?
8.9 About the same as other trusts
Q38. Did a member of staff explain the purpose of the medications you were to take at home in a way you could understand?
9.0 About the same as other trusts
Q39. Did a member of staff tell you about medication side effects to watch out for?
5.7 About the same as other trusts
Q40. Did a member of staff tell you when you could resume your usual activities, such as when to go back to work or drive a car?
5.3 About the same as other trusts
Q41. Did hospital staff take your family or home situation into account when you were leaving the emergency department?
5.2 About the same as other trusts
Q42. Did a member of staff tell you about what danger signals regarding your illness or treatment to watch for after you went home?
5.6 About the same as other trusts
Q43. Did hospital staff tell you who to contact if you were worried about your condition or treatment after you left the emergency department?
6.7 About the same as other trusts
Q45. Overall 8.1 About the same as other trusts
(Source: Emergency Department Survey (October 2016 to March 2017; published October 2017)
Is the service responsive?
Service delivery to meet the needs of local people
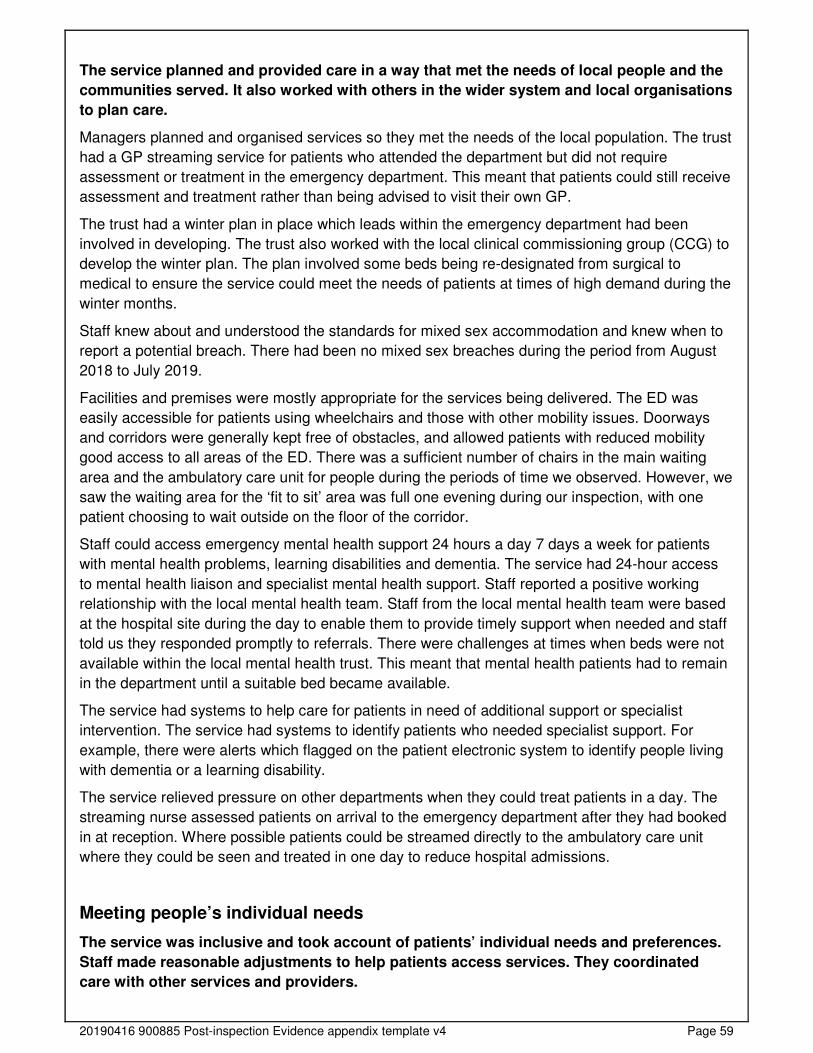
20190416 900885 Post-inspection Evidence appendix template v4 Page 59
The service planned and provided care in a way that met the needs of local people and the
communities served. It also worked with others in the wider system and local organisations
to plan care.
Managers planned and organised services so they met the needs of the local population. The trust
had a GP streaming service for patients who attended the department but did not require
assessment or treatment in the emergency department. This meant that patients could still receive
assessment and treatment rather than being advised to visit their own GP.
The trust had a winter plan in place which leads within the emergency department had been
involved in developing. The trust also worked with the local clinical commissioning group (CCG) to
develop the winter plan. The plan involved some beds being re-designated from surgical to
medical to ensure the service could meet the needs of patients at times of high demand during the
winter months.
Staff knew about and understood the standards for mixed sex accommodation and knew when to
report a potential breach. There had been no mixed sex breaches during the period from August
2018 to July 2019.
Facilities and premises were mostly appropriate for the services being delivered. The ED was
easily accessible for patients using wheelchairs and those with other mobility issues. Doorways
and corridors were generally kept free of obstacles, and allowed patients with reduced mobility
good access to all areas of the ED. There was a sufficient number of chairs in the main waiting
area and the ambulatory care unit for people during the periods of time we observed. However, we
saw the waiting area for the ‘fit to sit’ area was full one evening during our inspection, with one
patient choosing to wait outside on the floor of the corridor.
Staff could access emergency mental health support 24 hours a day 7 days a week for patients
with mental health problems, learning disabilities and dementia. The service had 24-hour access
to mental health liaison and specialist mental health support. Staff reported a positive working
relationship with the local mental health team. Staff from the local mental health team were based
at the hospital site during the day to enable them to provide timely support when needed and staff
told us they responded promptly to referrals. There were challenges at times when beds were not
available within the local mental health trust. This meant that mental health patients had to remain
in the department until a suitable bed became available.
The service had systems to help care for patients in need of additional support or specialist
intervention. The service had systems to identify patients who needed specialist support. For
example, there were alerts which flagged on the patient electronic system to identify people living
with dementia or a learning disability.
The service relieved pressure on other departments when they could treat patients in a day. The
streaming nurse assessed patients on arrival to the emergency department after they had booked
in at reception. Where possible patients could be streamed directly to the ambulatory care unit
where they could be seen and treated in one day to reduce hospital admissions.
Meeting people’s individual needs
The service was inclusive and took account of patients’ individual needs and preferences.
Staff made reasonable adjustments to help patients access services. They coordinated
care with other services and providers.
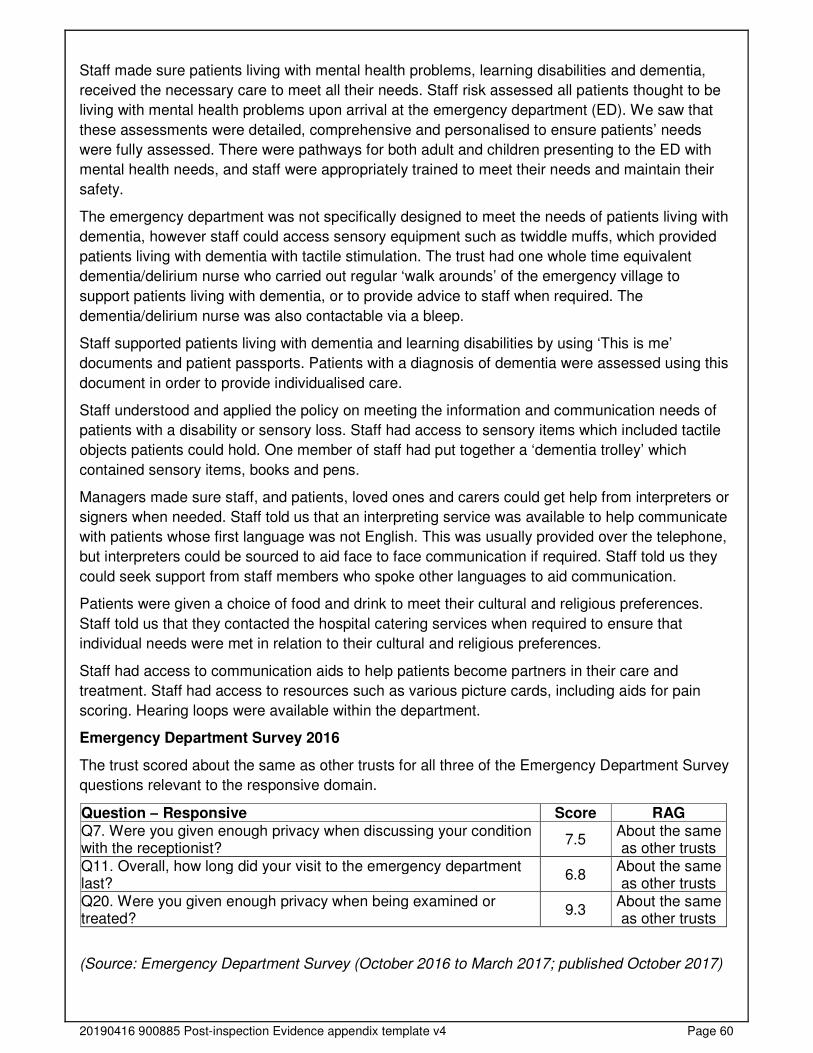
20190416 900885 Post-inspection Evidence appendix template v4 Page 60
Staff made sure patients living with mental health problems, learning disabilities and dementia,
received the necessary care to meet all their needs. Staff risk assessed all patients thought to be
living with mental health problems upon arrival at the emergency department (ED). We saw that
these assessments were detailed, comprehensive and personalised to ensure patients’ needs
were fully assessed. There were pathways for both adult and children presenting to the ED with
mental health needs, and staff were appropriately trained to meet their needs and maintain their
safety.
The emergency department was not specifically designed to meet the needs of patients living with
dementia, however staff could access sensory equipment such as twiddle muffs, which provided
patients living with dementia with tactile stimulation. The trust had one whole time equivalent
dementia/delirium nurse who carried out regular ‘walk arounds’ of the emergency village to
support patients living with dementia, or to provide advice to staff when required. The
dementia/delirium nurse was also contactable via a bleep.
Staff supported patients living with dementia and learning disabilities by using ‘This is me’
documents and patient passports. Patients with a diagnosis of dementia were assessed using this
document in order to provide individualised care.
Staff understood and applied the policy on meeting the information and communication needs of
patients with a disability or sensory loss. Staff had access to sensory items which included tactile
objects patients could hold. One member of staff had put together a ‘dementia trolley’ which
contained sensory items, books and pens.
Managers made sure staff, and patients, loved ones and carers could get help from interpreters or
signers when needed. Staff told us that an interpreting service was available to help communicate
with patients whose first language was not English. This was usually provided over the telephone,
but interpreters could be sourced to aid face to face communication if required. Staff told us they
could seek support from staff members who spoke other languages to aid communication.
Patients were given a choice of food and drink to meet their cultural and religious preferences.
Staff told us that they contacted the hospital catering services when required to ensure that
individual needs were met in relation to their cultural and religious preferences.
Staff had access to communication aids to help patients become partners in their care and
treatment. Staff had access to resources such as various picture cards, including aids for pain
scoring. Hearing loops were available within the department.
Emergency Department Survey 2016
The trust scored about the same as other trusts for all three of the Emergency Department Survey
questions relevant to the responsive domain.
Question – Responsive Score RAG Q7. Were you given enough privacy when discussing your condition with the receptionist?
7.5 About the same as other trusts
Q11. Overall, how long did your visit to the emergency department last?
6.8 About the same as other trusts
Q20. Were you given enough privacy when being examined or treated?
9.3 About the same as other trusts
(Source: Emergency Department Survey (October 2016 to March 2017; published October 2017)

20190416 900885 Post-inspection Evidence appendix template v4 Page 61
Access and flow
People could not always access the service when they needed it and did not always receive
care promptly. Waiting times from referral to treatment and arrangements to admit, treat
and discharge patients were not in line with national standards.
Median time from arrival to treatment (all patients)
Managers monitored waiting times but patients could not always access emergency services and
receive treatment within agreed timeframes and national targets. The leads within the department
were in the process of trialling an initiative to try to improve flow throughout the department. They
had extended the department and introduced a ‘fit to sit’ area. The area was used for patients who
were assessed as having stable conditions, did not require immediate intervention, cardiac
monitoring or high level of observation, and were deemed as low dependency. The ‘fit to sit’ area
ensured that these patients were not kept in the main waiting room but were cared for in a
dedicated area, which also supported the flow of the minors area. The trial of ‘fit to sit’ was subject
to a three month review, which was due on 4 December 2019.
There was an emergency department performance improvement plan in place which had actions
assigned to individuals and was red, amber, green (RAG) rated to indicate whether actions were
complete, on track, delayed, not complete or ongoing.
The Royal College of Emergency Medicine recommends that the time patients should wait from
time of arrival to receiving treatment should be no more than one hour. The trust did not report any
data for this quality indicator to NHS Digital from July 2018 to June 2019.
(Source: NHS Digital - A&E quality indicators)
Following our inspection, we requested the median time from arrival to treatment for all patients.
Information provided by the trust stated that the median time from arrival to treatment for all
patients from 1 May 2019 to 31 October 2019 was 90 minutes. This meant that the trust did not
meet the national recommendation.
Percentage of patients admitted, transferred or discharged within four hours (all
emergency department types)
The Department of Health’s standard for emergency departments is that 95% of patients should
be admitted, transferred or discharged within four hours of arrival in the emergency department.
From August 2018 to July 2019 the trust failed to meet the standard in all twelve months. The trust
also performed consistently poorer than the England average across the same period. The trust’s
performance remained relatively consistent across the period with improvements seen in August
and October 2018 and June 2019 (88%, 87% and 84% respectively).
Four hour target performance - Mid Essex Hospital Services NHS Trust
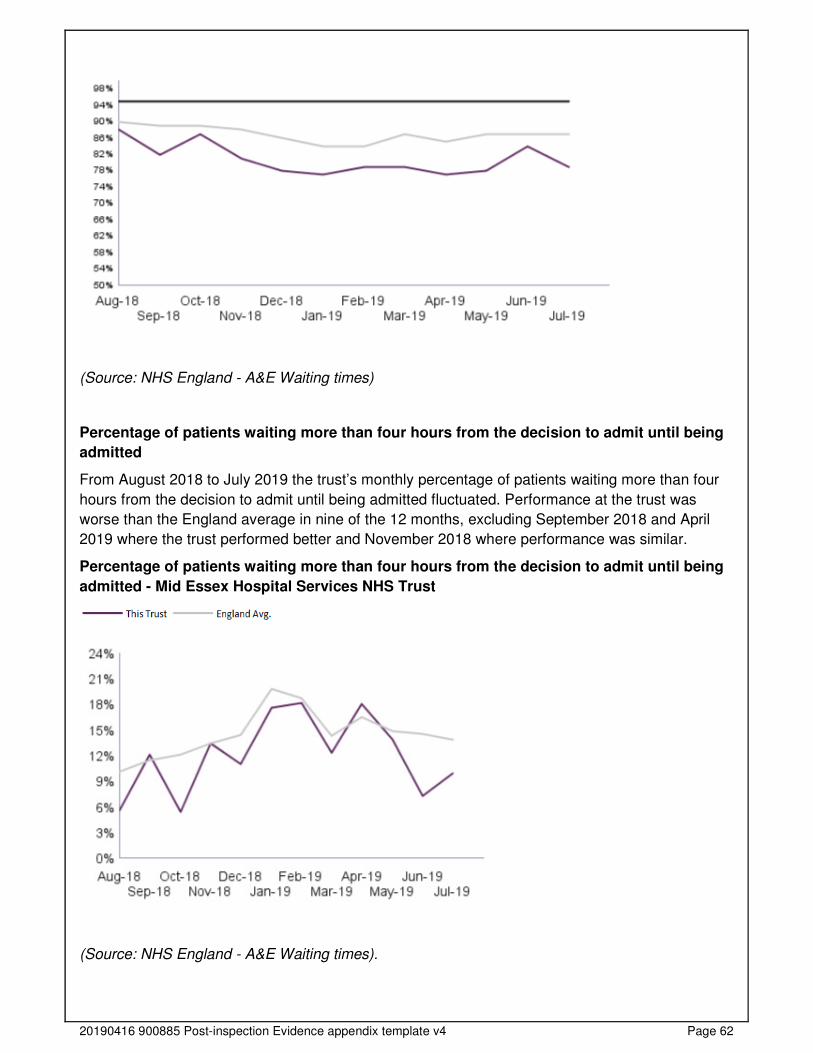
20190416 900885 Post-inspection Evidence appendix template v4 Page 62
(Source: NHS England - A&E Waiting times)
Percentage of patients waiting more than four hours from the decision to admit until being
admitted
From August 2018 to July 2019 the trust’s monthly percentage of patients waiting more than four
hours from the decision to admit until being admitted fluctuated. Performance at the trust was
worse than the England average in nine of the 12 months, excluding September 2018 and April
2019 where the trust performed better and November 2018 where performance was similar.
Percentage of patients waiting more than four hours from the decision to admit until being
admitted - Mid Essex Hospital Services NHS Trust
(Source: NHS England - A&E Waiting times).
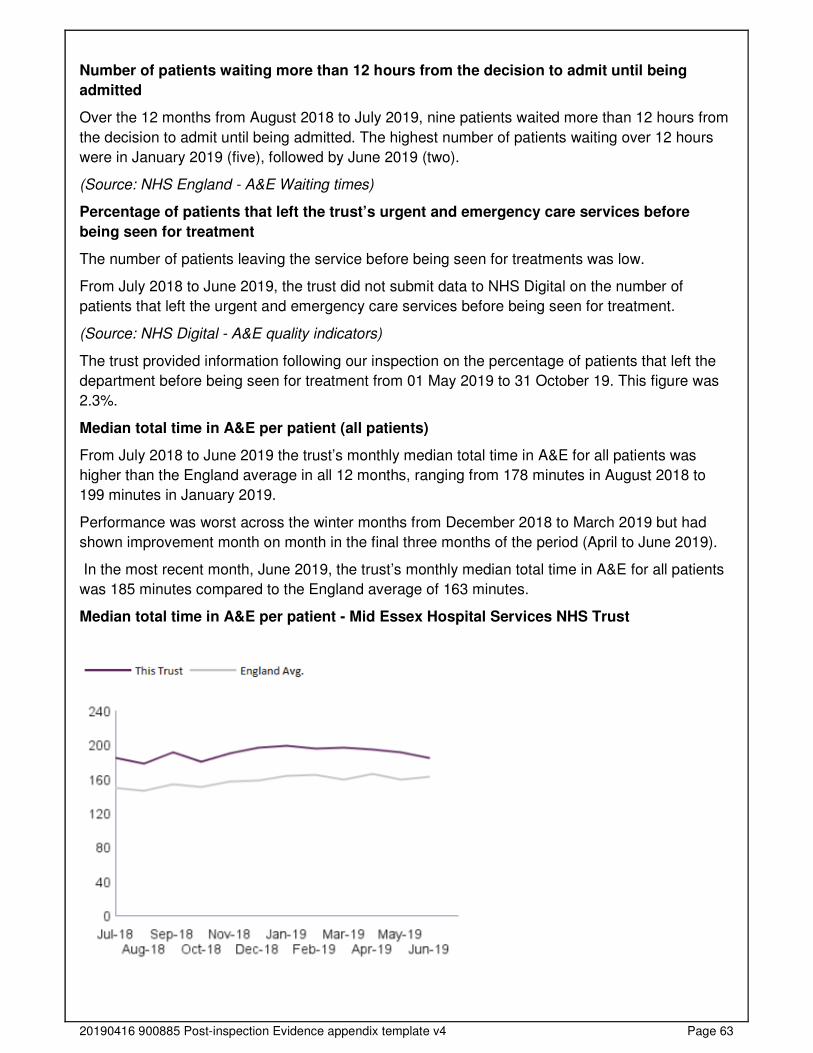
20190416 900885 Post-inspection Evidence appendix template v4 Page 63
Number of patients waiting more than 12 hours from the decision to admit until being
admitted
Over the 12 months from August 2018 to July 2019, nine patients waited more than 12 hours from
the decision to admit until being admitted. The highest number of patients waiting over 12 hours
were in January 2019 (five), followed by June 2019 (two).
(Source: NHS England - A&E Waiting times)
Percentage of patients that left the trust’s urgent and emergency care services before
being seen for treatment
The number of patients leaving the service before being seen for treatments was low.
From July 2018 to June 2019, the trust did not submit data to NHS Digital on the number of
patients that left the urgent and emergency care services before being seen for treatment.
(Source: NHS Digital - A&E quality indicators)
The trust provided information following our inspection on the percentage of patients that left the
department before being seen for treatment from 01 May 2019 to 31 October 19. This figure was
2.3%.
Median total time in A&E per patient (all patients)
From July 2018 to June 2019 the trust’s monthly median total time in A&E for all patients was
higher than the England average in all 12 months, ranging from 178 minutes in August 2018 to
199 minutes in January 2019.
Performance was worst across the winter months from December 2018 to March 2019 but had
shown improvement month on month in the final three months of the period (April to June 2019).
In the most recent month, June 2019, the trust’s monthly median total time in A&E for all patients
was 185 minutes compared to the England average of 163 minutes.
Median total time in A&E per patient - Mid Essex Hospital Services NHS Trust
20190416 900885 Post-inspection Evidence appendix template v4 Page 64
(Source: NHS Digital - A&E quality indicators)
Managers and staff worked to make sure that they started discharge planning as early as possible.
We saw this in patients’ notes and the board meetings we attended.
Staff planned patients’ discharge carefully, particularly for those with complex mental health and
social care needs. Staff liaised with discharge coordinators, ambulance services, patients’ GPs
and social care providers when relevant to ensure that appropriate patient care was provided for
discharge.
Staff liaised with the local mental health service to support patients with mental health needs to
help plan discharges to appropriate environments, depending on the needs of the patient.
Staff supported patients when they were referred or transferred between services. Staff told us
that they completed a document based on situation, background, assessment, recommendation
(SBAR) for all patients being transferred from the emergency department to other areas of the
hospital. This ensured the patients’ needs were communicated effectively to the accepting ward or
department.
Learning from complaints and concerns
It was easy for people to give feedback and raise concerns about care received. The
service treated concerns and complaints seriously, investigated them and shared lessons
learned with all staff. The service included patients in the investigation of their complaint.
Summary of complaints
Patients, relatives and carers knew how to complain or raise concerns. All patients and relatives
that we asked told us that they knew how to raise a complaint.
The service clearly displayed information about how to raise a concern in patient areas. Leaflets
which included information on how to raise concerns were displayed in ward areas. This included
Patient Advice and Liaison Service (PALS) details on how to make a formal complaint.
Staff understood the policy on complaints and knew how to handle them. Staff told us they would
try to resolve concerns before they progressed to complaints if possible. Staff directed people to
the complaints process and provided them with the details needed to make a complaint if needed.
Managers investigated complaints and identified themes. Managers shared feedback from
complaints with staff and learning was used to improve the service. We reviewed a recent
complaint received by the service. We found that the complainant was involved in the process and
remained updated regarding the process of the investigation. Actions were identified to address
concerns and learning from the complaint was shared with staff.
Broomfield Hospital
From August 2018 to July 2019 the trust received 83 complaints in relation to urgent and
emergency care at Broomfield Hospital (14.0% of the total complaints received by the trust). The
trust took an average of 38.9 days to investigate and close complaints. This was not in line with
their complaints policy, which states complaints should be completed within 25 working days.
The 12 complaints, that had not yet been closed, had been open for an average of 30.4 working
days at the time of data submission.
A breakdown of complaints by type is shown below:

20190416 900885 Post-inspection Evidence appendix template v4 Page 65
Type of complaint Number of complaints Percentage of total Clinical treatment - accident and emergency 65 78.3% Communications 5 6.0%
Clinical treatment - paediatric group 4 4.8% Values and behaviours (staff) 3 3.6% Clinical treatment - general medicine group 2 2.4% Admissions, discharge and transfer arrangements excluding delays due to absence of care package
2 2.4%
Appointments including delays and cancellations 1 1.2% Clinical treatment - obstetrics and gynaecology 1 1.2%
Total 83 100.0%
(Source: Routine Provider Information Request (RPIR) – Complaints tab)
Number of compliments made to the trust
Broomfield Hospital
From August 2018 to July 2019 there were 91 compliments about urgent and emergency care at
Broomfield Hospital (8.1% of all compliments received trust-wide). Of these, 92.3% were received
by the general accident and emergency department and 7.7% were received by paediatrics.
A breakdown of compliments by department is shown below:
Department Number of
compliments Percentage of total
Accident and emergency 84 92.3% Paediatric accident and emergency 7 7.7% Total 91 100.0%
The trust stated that most of the compliments received related to overall care along the whole
pathway with patients and relatives thanking staff for their kindness and compassion
during difficult and stressful times. These related to all staff from housekeepers,
porters and nurses to consultants.
Compliments and the associated learning and sharing of good practice is discussed at the patient
and carer experience group and also with individuals and their managers during appraisal. The
trust used its electronic reporting system to analyse themes from compliments.
(Source: Routine Provider Information Request (RPIR) – Compliments tab)
We spoke with staff regarding complaints that were not closed within 25 working days in line with
the trust’s policy. Staff commented that this was usually because the complaints involved other
departments, which meant it took longer to complete the complaints process.
Staff knew how to acknowledge complaints and patients received feedback from managers after
the investigation into their complaint. The trust sent feedback that addressed the entirety of
complaints and provided details to children, young people and their families of what to do if they
were not satisfied with the investigation into their complaint.
Managers shared feedback from complaints with staff and learning was used to improve the
service. Staff told us that managers shared feedback from complaints in local meetings. The
department held serious incident learning initiative (SILI) meetings on a weekly basis. Feedback
and learning from complaints was shared at these meetings as well as nursing safely huddles.
20190416 900885 Post-inspection Evidence appendix template v4 Page 66
Is the service well-led?
Leadership
Leaders had the skills, knowledge, experience and integrity to run a service providing high-
quality sustainable care.
Leaders had the skills, knowledge, experience and integrity that they needed. The trust had an
executive lead for urgent and emergency care. The service was led by the clinical director, director
of operations, service manager, associate director of nursing and matrons within the department.
Leaders understood issues within the service and wider organisation and were active in their roles.
Leaders understood the challenges to quality and sustainability within the service and identified
the actions needed to address them. For example, one of the challenges within the service was
nurse staffing within the department. Leaders spoke about it as a challenge during our inspection
and it is also featured on the department’s risk register. The risk was mitigated through the use of
regular bank and agency staff, ongoing recruitment and a daily staffing review.
Staff informed us that management were approachable and supportive and also stated that the
senior leadership team were visible. The leadership team provided support to teams following any
incidents.
Senior leaders told us that sustainable, compassionate, inclusive and effective leadership was a
priority within the emergency department. The department had strong working relationships with
the local mental health team, which meant that the service had access to the appropriate mental
health expertise.
Vision and strategy
The service had a vision for what it wanted to achieve, but no service specific strategy to
turn it into action, developed with all relevant stakeholders. The vision for developing the
department was focused on prioritising patient care and aligned to local plans within the
wider health economy. Leaders and staff understood and knew how to apply them and
monitor progress.
The emergency department was within the division of medicine and emergency care. The
paediatric emergency department was within the department for women and children.
There was a divisional and trust strategy in place which included the emergency department,
however there was not a service specific strategy in place. There was a clear set of values which
prioritised patient care. The service had an emergency improvement plan which was going to be
revised in December 2019. The plan included actions to improve performance of the service with a
central focus on patient care.
The majority of staff were aware of the trust’s vision and values and could tell us what they were.
The trust’s vision was “To be a healthcare organisation that puts patient care first and whose
reputation for excellence and innovation inspires our patients, staff and the population we serve”.
The trust values were that “At our best we are a kind, professional, positive, team.” The values
statement was developed following staff listening events.
20190416 900885 Post-inspection Evidence appendix template v4 Page 67
Culture
Staff felt respected, supported and valued. They were focused on the needs of patients
receiving care. The service had an open culture where patients, their families and staff
could raise concerns without fear.
The culture of the service centred on the needs and experiences of patients who used the service.
Senior staff in the department throughout our inspection told us that they were proud of the care
their staff delivered, and stated they were reliable with a positive attitude.
Staff felt supported, respected and valued. Staff spoke positively about their matrons, they told us
managers were always supportive and valued each member of staff. Staff described the service
as a positive environment to work within.
Medical and nursing staff we spoke with informed us that they had positive working relationships
with one another.
Medical staff described close working relationships within the medical team. They stated that as it
was a smaller department, they all knew each other well and felt supported by their managers.
One GP we spoke with described receiving significant support from the clinical director, despite
the fact that the GP’s were employed by the clinical commissioning group, rather than the trust.
Staff stated that the department leads had developed a cohesive working environment.
Staff we spoke with told us they felt confident that they could raise any concerns they had to their
manager and they felt they would be listened to and concerns would be acted upon.
There was a strong emphasis on staff wellbeing. The department leads told us they recently held
an emergency care wellness day. It was well supported and the leads were planning to run a
wellbeing event every six months.
Governance
Leaders operated effective governance processes, throughout the service and with partner
organisations. Staff at all levels were clear about their roles and accountabilities and had
regular opportunities to meet, discuss and learn from the performance of the service.
There were effective structures, processes and systems of accountability to support the delivery of
the strategy and a good quality sustainable service. There was a clear governance structure with
regular meetings. Emergency care governance meetings took place on a monthly basis
All levels of governance and management functioned effectively and interacted with each other
appropriately. We reviewed the minutes of the emergency care governance meetings for August,
September and October 2019. All of the minutes included whether there were any issues for
escalation to the board. Items discussed within the meetings included incidents, risks,
disseminating actions to all staff and review of the action log.
There was an integrated quality and performance report which was sent to the board. The
department leads provided data to contribute to the board report. The report included data relating
to the performance of the emergency department, including four hour performance, breaches, time
to assessment and time to treatment decision. This meant that the board had oversight of the
performance and challenges within the service.
20190416 900885 Post-inspection Evidence appendix template v4 Page 68
There was a governance display board within the department which was reviewed by all staff. The
board included the department’s risk register, incident reporting themes and review of the
department’s performance against the four hour standard.
Staff at all levels were clear about their roles and accountabilities and had regular opportunities to
meet, discuss and learn from the performance of the service. All staff we spoke with were clear
about their roles and understood what they were accountable for.
There was not a standard operating procedure in place for the ‘fit to sit’ area of the emergency
department. We highlighted this during our inspection A risk assessment was completed on 7
November 2019 for the ‘fit to sit’ service provision within the identified environment. The
assessment included the environment, capacity for the location and the category and cohort of
parents suitable for the area. There was a documented process for the use of the area and an
exclusion criteria in place.
Management of risk, issues and performance
The trust had effective systems for identifying risks, planning to eliminate or reduce them,
and demonstrated the ability to cope with both the expected and unexpected.
Risks were captured on the service’s comprehensive risk register which used the red, amber,
green (RAG) system to denote the level of risk and progress in resolving the risks. There were
robust arrangements for identifying, recording and managing risks, and mitigating actions. There
was alignment between the recorded risks on the register and what staff told us was ‘on their
worry list’. The frequency that risks were reviewed depended upon the severity of the risk. The
higher risk items on the risk register were reviewed monthly, or more frequently if required. All
risks had a review date on the risk register which were all within date.
Potential risks were taken into account when planning services, for example, the ‘fit to sit’ area
was introduced for patients who were deemed as low dependency. A risk assessment was
completed prior to the introduction of this extension to the department. There were lead owners of
the risks, actions and contingency plans put in place where relevant.
There were processes to manage current and future performance. The department held a live
performance dashboard which was reviewed by department leads on a daily basis. The dashboard
included time to triage, time to treatment, ambulance waiting times and number of attendances.
This meant that leads could review the performance of the service and identify areas of learning.
Data from this dashboard was included in the report to the board.
The service had a clinical and internal audit programme to monitor quality and operational
processes, as well as systems to identify where action should be taken. There was an audit lead
for the service who coordinated the audit programme. All audits, including national and local audits
had action plans in place to improve audit results. There were plans to re-audit as appropriate to
monitor improvement. National audit results were shared with staff at the weekly serious incident
learning initiatives (SILI) meetings held within the department.
The department had a full capacity policy. There had been no reported instances of it being
repeatedly used and there were no incidents of the emergency department being closed during
the period from November 2018 to October 2019.
Information management
20190416 900885 Post-inspection Evidence appendix template v4 Page 69
Appropriate and accurate information was being effectively processed, challenged and
acted upon. However, information technology systems were not always effective.
The service collected reliable data and analysed it. The service used performance dashboards to
provide assurance they had a good understanding of service performance. The live dashboard
was reviewed on a daily basis and shared in handovers with all staff. The data was measured
against key quality standards. The service manager compiled a weekly service improvement
report. This collected the data into triage streams, for example, mental health patients. The report
included rota fill and how capacity throughout the trust impacted the department. The data
collected provided service leads with good oversight of the department’s performance.
Staff had sufficient access to information about the service and challenged it appropriately. We
reviewed the minutes of the emergency department senior team meeting from 2 October, 23
October and 1 November 2019. There was evidence of scrutiny and challenge. For example, it
was documented that a consultant raised a concern about pathways for a particular patient group.
An action was agreed for a policy to be written and distributed. The action was assigned to a
specific individual and a due date was documented.
Information technology systems were not always used effectively to monitor and improve the
quality of care. During our inspection there were some issues with the electronic devices used to
calculate national early warning scores (NEWS2). The devices had been configured in a way that
required overriding manually by staff. If there were fluctuations in the internet connection, this at
times impacted the data being sent from the devices. The devices were also not working when we
returned for the unannounced inspection. Staff had raised incidents regarding the devices. The
trust had formulated an action plan which included that the configuration of the electronic
recording system was to be reviewed by a fortnightly task and finish group that had been
established. This group reported to the patient safety group.
Engagement
Leaders and staff actively and openly engaged with patients and staff to plan and manage
services. They collaborated with partner organisations to help improve services for
patients.
People’s views and experiences were gathered and used to shape and improve the service and
culture. The service participated in the friends and family test to gain feedback from patients. We
saw comments boxes were used throughout the emergency village to gain additional feedback
from patients. Feedback methods were also available via the trust website.
During our inspection, we attended one of the serious incident learning initiatives (SILI) meetings
where a previous patient provided feedback about their experience of attending the department.
They described the care they had been given and wanted to personally thank the staff involved in
their care for the treatment and support they provided.
The trust engaged with staff through a variety of methods including daily huddles, use of social
media, newsletters and emails. The service held safeguarding and wellbeing events. The
wellbeing event encouraged staff to reflect and share feedback on their experiences of working in
the department. The department leads recognised the importance of listening to staff suggestions
for improvement.
There were positive and collaborative relationships with external partners to meet the needs of the
population. Service leads engaged with the local clinical commissioning group (CCG). For
20190416 900885 Post-inspection Evidence appendix template v4 Page 70
example, the trust liaised with the local CCG in the development of their winter plan to ensure the
needs of the local population could be met during a time of increased demand and pressure.
Learning, continuous improvement and innovation
Staff were committed to continually learning and improving services. Leaders encouraged
innovation and participation in research.
Leaders and staff strived to achieve continuous learning, improvement and innovation. One
medical member of staff was in the process of developing a policy for the use of metal detector
wands for patients with mental health problems who claimed to have swallowed metal items. This
method was planned to reduce the inappropriate use of radiation for scans. Guidance was being
sought from another acute NHS trust in the development of the policy.
The introduction of the ‘fit to sit’ area in the department was a demonstration of the service’s
commitment to improving services for patients. It was still in the trial process at the time of our
inspection and was subject to a review in December 2019.
The trust continued to use serious incident learning initiative (SILI) meetings, which staff were
encouraged to attend to discuss incidents and share learning from incidents. The meeting was
embedded throughout the department as a tool for information sharing, shared learning and
improvement.
20190416 900885 Post-inspection Evidence appendix template v4 Page 71
Medical care (including older people’s care)
Facts and data about this service
Medical care at the trust consists of elective and non-elective services. All inpatient care is based
at Broomfield Hospital and there are 278 medical beds.
Acute medicine is based in the emergency village and consists of the acute medical unit, 20 short
stay beds (length of stay 24 hours) and 12 assessment trolleys. General practitioner (GP) referred
patients are also seen in this area. In addition, this area contains the emergency short stay ward
consisting of 10 beds with a length of stay of less than 72 hours. There is also a 7-day ambulatory
care unit.
Geriatric medicine is comprised of four wards, each with 26 beds, and a 16 bed frailty unit with
four assessment trolleys. The frailty unit provides a multi-disciplinary team seven days a week.
There are inpatient wards for gastroenterology, cardiology, respiratory and renal. Details of these
services are below:
• There is 24 hour a day seven days a week consultant cover for gastrointestinal bleed rota
and the five gastroenterology consultants provide two endoscopy sessions each week to
the endoscopy service.
• There is a dedicated 24/7 consultant led stroke service which includes a thrombolysis
service.
• There is a renal unit providing a haemodialysis service, 7am to midnight, six days a week,
and outpatient clinics.
• There is a large cardiology centre at Broomfield Hospital offering outpatient cardiac
imaging, angiography and cardio devices. Respiratory services provide inpatient non-
invasive ventilation (NIV) and outpatient lung function and sleep studies.
• Dermatology services offer consultant led and nurse led outpatient clinics and minor
operations.
• Neurology provide outpatient clinics and neurophysiology diagnostic testing.
• There is a diabetic centre providing both consultant-led and nurse-led outpatient clinics.
There is also an onsite HIV service.
(Source: Routine Provider Information Request (RPIR) – Acute context)
The trust had 37,323 medical admissions from March 2018 to February 2019. Emergency
admissions accounted for 18,120 (48.5%), 275 (0.7%) were elective, and the remaining 18,928
(50.7%) were day case.
Admissions for the top three medical specialties were:
• General medicine: 17,547 admissions
• Medical oncology: 5,995 admissions

20190416 900885 Post-inspection Evidence appendix template v4 Page 72
• Clinical haematology: 3,659 admissions
(Source: Hospital Episode Statistics)
Due to the number of core services inspected, our inspection of Broomfield hospital was
announced. Prior to our inspection we reviewed data we held about the trust along with
information we requested from the trust. The medicine service was rated inadequate overall
following its last inspection in September 2018. Safe was rated as inadequate, effective, caring
and responsive were rated requires improvement and well led rated inadequate. We carried out a
focused inspection on 21 May 2019 to follow up on the concerns raised at our previous inspection
and found that the trust had made improvements to address these.
During our inspection, we spoke with 66 members of staff including doctors, nurses, therapists,
health care assistants and non-clinical staff. We visited all of the medicine wards, the endoscopy
department, acute medical assessment, frailty assessment bay, renal unit, discharge lounge,
angiography suite, day therapies and faith centre.
We reviewed 25 sets of patient records and considered other pieces of information and evidence
to come to our judgement and ratings. We spoke with nine patients and other family members to
gather their experience of the trust.
We carried out a further unannounced inspection on the 20 November 2019 in order to review
changes in the trust’s acute medical assessment centre, its frailty assessment bay and observe
staff handovers.
Is the service safe?
By safe, we mean people are protected from abuse* and avoidable harm.
*Abuse can be physical, sexual, mental or psychological, financial, neglect, institutional or
discriminatory abuse.
Mandatory training
The service provided mandatory training in key skills to all staff and made sure everyone
completed it.
Mandatory training completion rates
The trust set a target of 85% for the completion of all mandatory training, with the exception of
information governance which had a target of 95%.
Broomfield Hospital
Nursing and medical staff received and kept up-to-date with their mandatory training.
A breakdown of compliance for mandatory training courses as of August 2019 for qualified nursing
staff in medicine at Broomfield Hospital is shown below:
Training module name As of August, 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Paediatric basic life support 3 3 100.0% 85% Yes Hand hygiene 257 261 98.5% 85% Yes
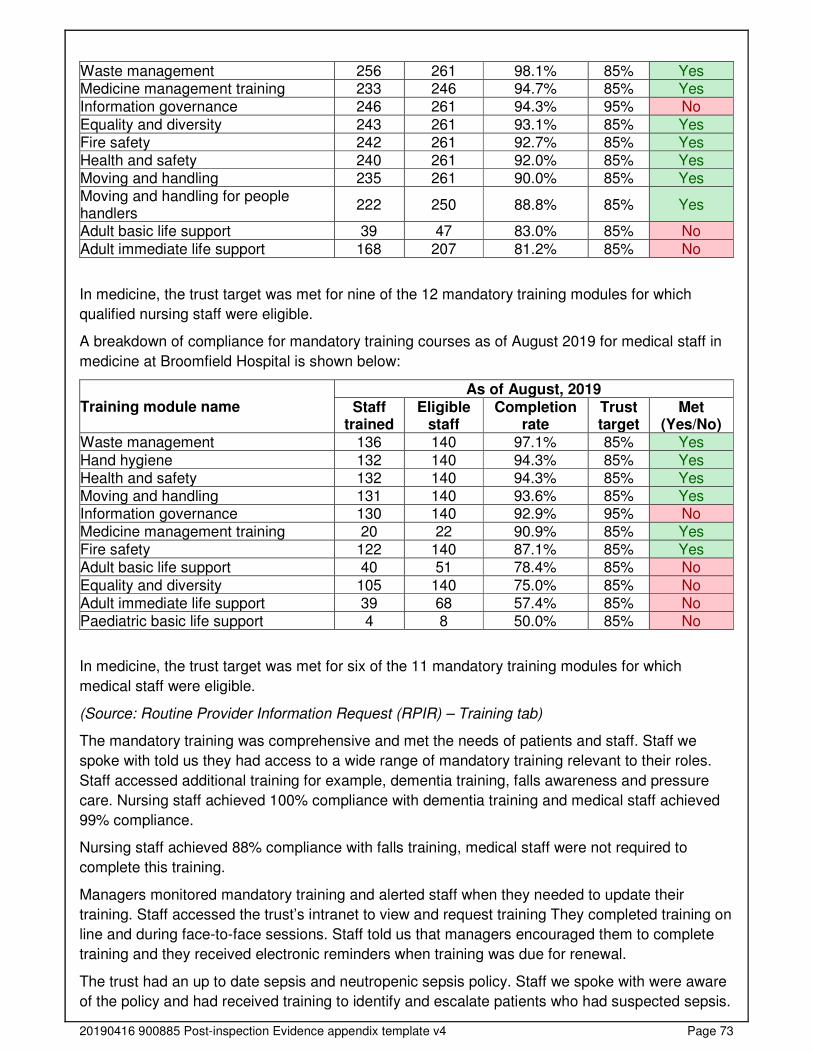
20190416 900885 Post-inspection Evidence appendix template v4 Page 73
Waste management 256 261 98.1% 85% Yes Medicine management training 233 246 94.7% 85% Yes Information governance 246 261 94.3% 95% No
Equality and diversity 243 261 93.1% 85% Yes Fire safety 242 261 92.7% 85% Yes Health and safety 240 261 92.0% 85% Yes Moving and handling 235 261 90.0% 85% Yes Moving and handling for people handlers
222 250 88.8% 85% Yes
Adult basic life support 39 47 83.0% 85% No
Adult immediate life support 168 207 81.2% 85% No
In medicine, the trust target was met for nine of the 12 mandatory training modules for which
qualified nursing staff were eligible.
A breakdown of compliance for mandatory training courses as of August 2019 for medical staff in
medicine at Broomfield Hospital is shown below:
Training module name As of August, 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Waste management 136 140 97.1% 85% Yes
Hand hygiene 132 140 94.3% 85% Yes Health and safety 132 140 94.3% 85% Yes Moving and handling 131 140 93.6% 85% Yes Information governance 130 140 92.9% 95% No Medicine management training 20 22 90.9% 85% Yes Fire safety 122 140 87.1% 85% Yes Adult basic life support 40 51 78.4% 85% No
Equality and diversity 105 140 75.0% 85% No Adult immediate life support 39 68 57.4% 85% No Paediatric basic life support 4 8 50.0% 85% No
In medicine, the trust target was met for six of the 11 mandatory training modules for which
medical staff were eligible.
(Source: Routine Provider Information Request (RPIR) – Training tab)
The mandatory training was comprehensive and met the needs of patients and staff. Staff we
spoke with told us they had access to a wide range of mandatory training relevant to their roles.
Staff accessed additional training for example, dementia training, falls awareness and pressure
care. Nursing staff achieved 100% compliance with dementia training and medical staff achieved
99% compliance.
Nursing staff achieved 88% compliance with falls training, medical staff were not required to
complete this training.
Managers monitored mandatory training and alerted staff when they needed to update their
training. Staff accessed the trust’s intranet to view and request training They completed training on
line and during face-to-face sessions. Staff told us that managers encouraged them to complete
training and they received electronic reminders when training was due for renewal.
The trust had an up to date sepsis and neutropenic sepsis policy. Staff we spoke with were aware
of the policy and had received training to identify and escalate patients who had suspected sepsis.
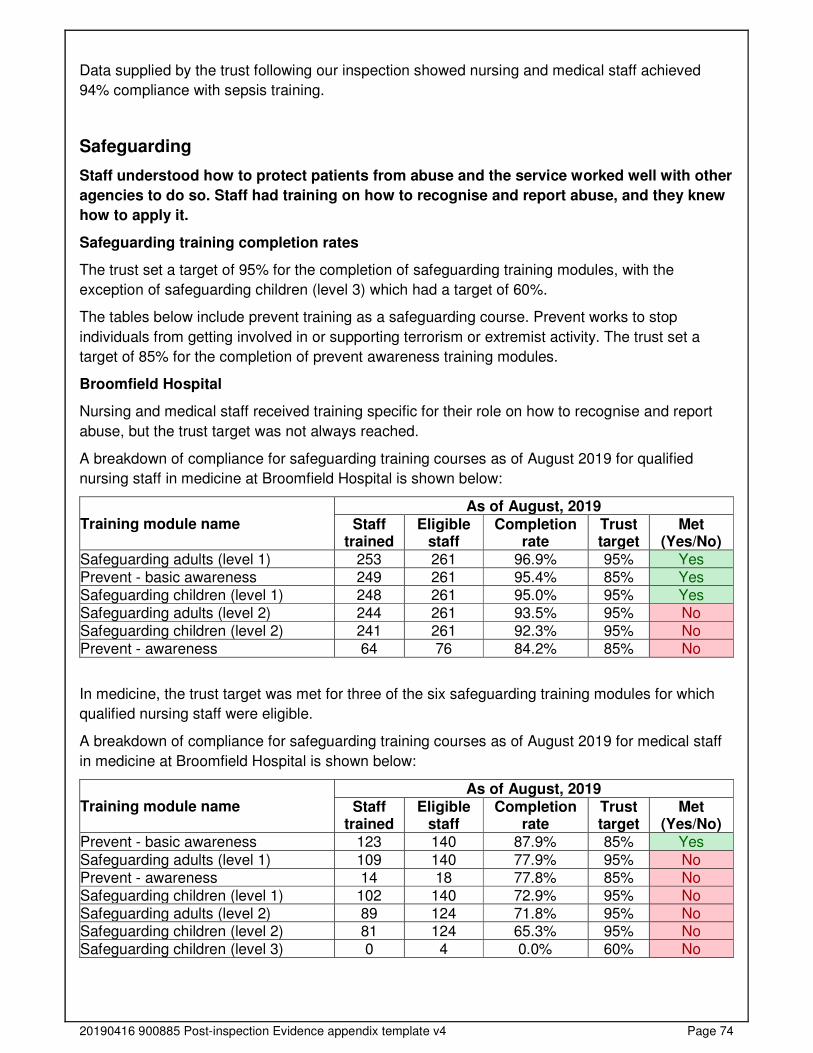
20190416 900885 Post-inspection Evidence appendix template v4 Page 74
Data supplied by the trust following our inspection showed nursing and medical staff achieved
94% compliance with sepsis training.
Safeguarding
Staff understood how to protect patients from abuse and the service worked well with other
agencies to do so. Staff had training on how to recognise and report abuse, and they knew
how to apply it.
Safeguarding training completion rates
The trust set a target of 95% for the completion of safeguarding training modules, with the
exception of safeguarding children (level 3) which had a target of 60%.
The tables below include prevent training as a safeguarding course. Prevent works to stop
individuals from getting involved in or supporting terrorism or extremist activity. The trust set a
target of 85% for the completion of prevent awareness training modules.
Broomfield Hospital
Nursing and medical staff received training specific for their role on how to recognise and report
abuse, but the trust target was not always reached.
A breakdown of compliance for safeguarding training courses as of August 2019 for qualified
nursing staff in medicine at Broomfield Hospital is shown below:
Training module name As of August, 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Safeguarding adults (level 1) 253 261 96.9% 95% Yes Prevent - basic awareness 249 261 95.4% 85% Yes Safeguarding children (level 1) 248 261 95.0% 95% Yes Safeguarding adults (level 2) 244 261 93.5% 95% No Safeguarding children (level 2) 241 261 92.3% 95% No Prevent - awareness 64 76 84.2% 85% No
In medicine, the trust target was met for three of the six safeguarding training modules for which
qualified nursing staff were eligible.
A breakdown of compliance for safeguarding training courses as of August 2019 for medical staff
in medicine at Broomfield Hospital is shown below:
Training module name As of August, 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Prevent - basic awareness 123 140 87.9% 85% Yes
Safeguarding adults (level 1) 109 140 77.9% 95% No Prevent - awareness 14 18 77.8% 85% No Safeguarding children (level 1) 102 140 72.9% 95% No Safeguarding adults (level 2) 89 124 71.8% 95% No Safeguarding children (level 2) 81 124 65.3% 95% No Safeguarding children (level 3) 0 4 0.0% 60% No
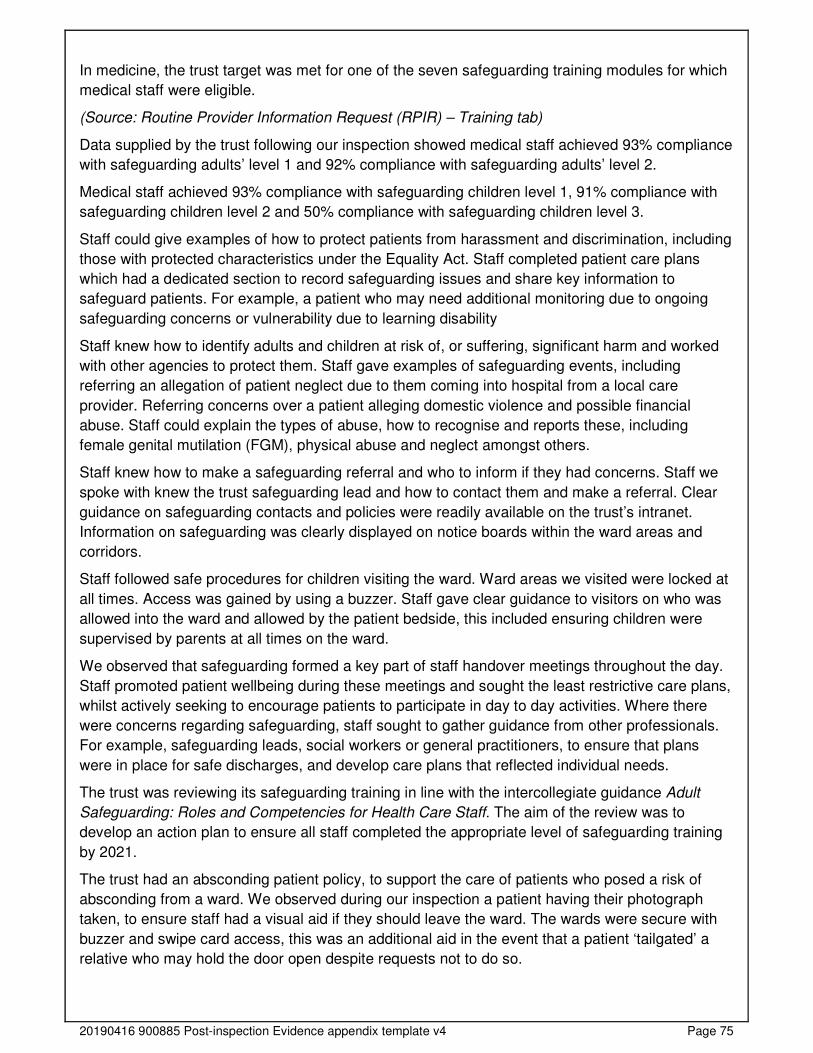
20190416 900885 Post-inspection Evidence appendix template v4 Page 75
In medicine, the trust target was met for one of the seven safeguarding training modules for which
medical staff were eligible.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Data supplied by the trust following our inspection showed medical staff achieved 93% compliance
with safeguarding adults’ level 1 and 92% compliance with safeguarding adults’ level 2.
Medical staff achieved 93% compliance with safeguarding children level 1, 91% compliance with
safeguarding children level 2 and 50% compliance with safeguarding children level 3.
Staff could give examples of how to protect patients from harassment and discrimination, including
those with protected characteristics under the Equality Act. Staff completed patient care plans
which had a dedicated section to record safeguarding issues and share key information to
safeguard patients. For example, a patient who may need additional monitoring due to ongoing
safeguarding concerns or vulnerability due to learning disability
Staff knew how to identify adults and children at risk of, or suffering, significant harm and worked
with other agencies to protect them. Staff gave examples of safeguarding events, including
referring an allegation of patient neglect due to them coming into hospital from a local care
provider. Referring concerns over a patient alleging domestic violence and possible financial
abuse. Staff could explain the types of abuse, how to recognise and reports these, including
female genital mutilation (FGM), physical abuse and neglect amongst others.
Staff knew how to make a safeguarding referral and who to inform if they had concerns. Staff we
spoke with knew the trust safeguarding lead and how to contact them and make a referral. Clear
guidance on safeguarding contacts and policies were readily available on the trust’s intranet.
Information on safeguarding was clearly displayed on notice boards within the ward areas and
corridors.
Staff followed safe procedures for children visiting the ward. Ward areas we visited were locked at
all times. Access was gained by using a buzzer. Staff gave clear guidance to visitors on who was
allowed into the ward and allowed by the patient bedside, this included ensuring children were
supervised by parents at all times on the ward.
We observed that safeguarding formed a key part of staff handover meetings throughout the day.
Staff promoted patient wellbeing during these meetings and sought the least restrictive care plans,
whilst actively seeking to encourage patients to participate in day to day activities. Where there
were concerns regarding safeguarding, staff sought to gather guidance from other professionals.
For example, safeguarding leads, social workers or general practitioners, to ensure that plans
were in place for safe discharges, and develop care plans that reflected individual needs.
The trust was reviewing its safeguarding training in line with the intercollegiate guidance Adult
Safeguarding: Roles and Competencies for Health Care Staff. The aim of the review was to
develop an action plan to ensure all staff completed the appropriate level of safeguarding training
by 2021.
The trust had an absconding patient policy, to support the care of patients who posed a risk of
absconding from a ward. We observed during our inspection a patient having their photograph
taken, to ensure staff had a visual aid if they should leave the ward. The wards were secure with
buzzer and swipe card access, this was an additional aid in the event that a patient ‘tailgated’ a
relative who may hold the door open despite requests not to do so.
20190416 900885 Post-inspection Evidence appendix template v4 Page 76
Cleanliness, infection control and hygiene
The service controlled infection risk well. Staff used equipment and control measures to
protect patients, themselves and others from infection. They kept equipment and the
premises visibly clean.
Ward areas were clean and had suitable furnishings which were clean and well-maintained. All of
the wards we visited were visibly clean and free from clutter.
The service performed well for cleanliness. Hand hygiene audits for October 2019 showed all
medicine wards achieved 100% compliance. Nursing staff working within the renal unit achieved
98% compliance with infection prevention and control (IPC) training and 92% of medical staff
achieved compliance. Nursing staff within the wards achieved 100% compliance with IPC training
and medical staff achieved 95% compliance.
The medicine team had developed the role of assistant infection prevention and control
practitioner to support the wards to deliver a comprehensive infection prevention and control
service. The post-holder provided a visible presence on the wards and was accessible to clinical
teams and patients. This role had been pivotal in increasing staff awareness of IPC across the
wards through offering additional training, providing face to face guidance and supporting hygiene
audits. There was a wide range of IPC information for staff on all the wards we visited. These
included posters offering advice on hand washing, how to reduce infection risk and the trust’s IPC
policy.
Cleaning records were up-to-date and demonstrated that all areas were cleaned regularly. We
spoke with housekeeping staff and reviewed cleaning rotas. The ward managers completed a
performance improvement book (PIB) and these contained routine audits of cleaning records and
hygiene standards. We found no gaps in cleaning records between August 2019 to November
2019.
Staff followed infection control principles including the use of personal protective equipment (PPE).
Wards we visited had a plentiful supply of PPE and we observed staff using equipment at
appropriate times. Staff were bare below the elbow and washed their hands routinely between
activities. The ward had hand sanitiser at each entrance and at key points within the ward areas.
There was clear guidance displayed to both staff and the public to cleanse their hands when
entering and leaving ward areas.
Staff cleaned equipment after patient contact and labelled equipment to show when it was last
cleaned. ‘I am clean’ stickers showed where staff had cleaned equipment and we observed staff
cleaning equipment between use. Housekeeping staff were present on the wards emptying bins,
cleaning work surfaces and equipment throughout our inspection.
For the financial year 2018/2019 there were changes to the trust’s Clostridium difficile Infection
(CDI) reporting algorithm adding a prior healthcare exposure element for community onset cases.
The trust objectives for 2019/20 were set using these two categories. Firstly, hospital acquired
healthcare associated infections: cases that are detected in the hospital two or more days after
admission. Secondly, community acquired healthcare associated infections: cases that occurred in
the community (or within two days of admission). The timeframe for reporting CDI reduced from 72
hours of admission in 2018/19 to 48 hours of admission in 2019/20.
The trust reported 26 hospital acquired CDI cases in medicine between November 2018 and
October 2019. This equated to a 0.23% infection rate against 11,269 patient admissions during the
same period.
20190416 900885 Post-inspection Evidence appendix template v4 Page 77
The trust set a zero tolerance to Methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia.
The trust reported two hospital acquired cases of MRSA in medicine between November 2018 and
October 2019. This equated to a 0.02% infection rate against 11,269 patient admissions during the
same period.
Environment and equipment
The design, maintenance and use of facilities, premises and equipment kept people safe.
Staff were trained to use them. Staff managed clinical waste well.
Patients could reach call bells and staff responded quickly when called. We observed staff
ensuring that patients had call bells within reach as well as other equipment, for example walking
aids.
Staff carried out daily safety checks of specialist equipment. Resuscitation equipment on all the
wards we visited was routinely checked by staff, with no gaps, between August to November
2019. Staff had a strong focus on checking equipment and managers completed audits to ensure
checks had been completed.
The service had enough suitable equipment to help them to safely care for patients. Ward areas
had a wide range of equipment appropriate for patients including pressure care mattresses,
manual handling hoists, monitors and other equipment. The trust had an engineering team that
routinely reviewed stock and all the equipment we checked had been serviced and labelled for
next service due date.
Store rooms were visibly clean and tidy. Staff carried out stock checks routinely to ensure that
equipment was in date. We checked store rooms and found no out of date consumables on any of
the wards we visited.
Staff disposed of clinical waste safely. Sharps bins were clearly labelled and signed by staff. We
observed staff separated hazardous waste appropriately and all wards had confidential waste bins
that were locked at all times.
At the last endoscopy Joint Advisory Group on Gastrointestinal Endoscopy (JAG) accreditation in
2018, the visiting JAG authorising engineer recognised the vulnerable state of the endoscopy
equipment and recommended a replacement programme.
The three washers were 10 years old and at the limits of their life. One of the machines was out of
action one day in 25, usually because it did not meet the water quality standards. The reverse
osmosis units were built into each machine. Staff we spoke with told us the hospital engineers
usually did the repairs quite quickly, but the units were no longer fully supported by the
manufacturers, and parts were becoming harder or impossible to get. An incident report was
completed every time there was a technical failure. The trust had a business case for replacement
equipment in place.
If a washer unit failed, the endoscopes were processed by another provider, this took time, so staff
had to work late to clear up. The plan for maintaining continuity if more than one unit failed was to
use vacuum packed scopes which were usable for one month from date of sealing, and
additionally having endoscopes processed at another location. Staff told us this had only ever
happened once, some time ago.
The department also provided a cleaning service for endoscopes used for evacuation of retained
products of conception (ERCP) and in urology.
20190416 900885 Post-inspection Evidence appendix template v4 Page 78
A good number of scopes were at the end of their useful clinical life. At the time of our inspection
the endoscopy team were trying to get approval for five new colonoscopes and four gastroscopes.
The trust did not have suitable facilities to meet the needs of patient families. The ward areas
lacked space for families and staff, this was noticeable on a number of occasions when families
needed to talk to staff and limited rooms were available. At the time of our inspection staff showed
us a ward that was being refurbished. This ward had additional space for patients, staff and
families and was due to open in the new year. Other wards were due to be refurbished to this
standard to provide staff with the additional space they needed to offer ongoing support to patients
and families.
Baddow and Braxted wards both had external garden spaces to enable patients to access a safe
outdoor space. The gardens had sensory areas, defined kerbs and ornaments to encourage
patients to spend time outside and enjoy the freedom of space from within the ward areas.
Assessing and responding to patient risk
Staff completed and updated risk assessments for each patient and removed or minimised
risks. Staff identified and quickly acted upon patients at risk of deterioration
Staff used a nationally recognised tool to identify deteriorating patients and escalated them
appropriately. The trust had made improvements from our last inspection. Staff used the National
Early Warning Score 2 (NEWS2) which improves the detection and response to clinical
deterioration in adult patients and is a key element of patient safety and improving patient
outcomes. Staff used a hand held IT tablet to record patient vital signs, and the system
automatically highlighted any patients that had an increased NEWS score and required staff
intervention.
Staff completed risk assessments for each patient on admission / arrival, using a recognised tool,
and reviewed this regularly, including after any incident. We reviewed 25 patient records and
found NEWS scores had been recorded appropriately, staff carried out patient vital signs and
venous thromboembolism (VTE) assessments on time this was an improvement from our last
inspection.
Staff knew about and dealt with any specific risk issues. Staff used the sepsis six care bundle to
identify patients whose NEWS score indicated they may have sepsis. Staff we spoke to knew how
to escalate deteriorating patients and the trust had an up to date policy to guide staff on actions to
take when patients deteriorated. The trust had a “TRIGGER” team which included key nursing
staff that responded to any patient with a NEWS score above 5. Any patient whose vital signs
indicated deterioration when recorded on the hand held IT tablets would automatically inform the
“TRIGGER” team remotely. The team would then head to the ward area and provide immediate
intervention with the sepsis bundle. The TRIGGER team were skilled in immediate and advanced
life support techniques and trained other staff in life saving skills across the trust.
Staff shared key information to keep patients safe when handing over their care to others. All staff
participated in ward handovers where key information was shared at regular intervals throughout
the day. This information included discharge planning, the patient’s current wellbeing, any
safeguarding issues, ongoing clinical needs and additional key information appropriate to the
patients care. We observed handovers between the day teams and night teams and found shift
changes and handovers included all necessary key information to keep patients safe.
20190416 900885 Post-inspection Evidence appendix template v4 Page 79
The trust had a dedicated falls prevention nurse and staff followed up to date guidance to
complete falls assessments and pressure care. All the patient records we reviewed showed that
patients had been assessed by a named consultant within twelve hours of ward admission and
medical staff responded quickly if additional reviews were required, for example within the hour.
The trust had an upper gastrointestinal bleed (UGI) rota in place and clear processes to support
any patients likely to deteriorate following any endoscopy procedure. The out of hours urgent
endoscopy rota included one gastrointestinal consultant and two trained nurses. Urgent
procedures were always done in theatres. Endoscopy lists were rarely cancelled, only if, for
example, a consultant was unwell. If this happened, their subsequent lists were modified to
accommodate these patients. Additionally, another consultant or a nurse endoscopist would take
the patients onto their lists.
Staff from the medicine department attended mortality reviews, these fed into governance
meetings and information from mortality reviews was shared at team meetings. This was an
improvement from our last inspection.
Inspired by the NHS England’s “Sign UP to Safety Kitchen Table Events”, the provider’s falls
service took the kitchen table to the wards. Using the idea of a table cloth and having tea, coffee,
biscuits and sweets, staff were invited to take a five minute break and have a chat about the
services frailty harm awareness document. This was a quick glance guide to assist staff unfamiliar
with clinical frailty to consider tissue viability, medication, bone health, end of life care, falls
interventions, nutrition, delirium, dementia and avoiding deconditioning. The document was
permanently hosted on the trust falls intranet page. The mobile kitchen table also promoted
dangers of deconditioning awareness.
The services falls clinical nurse specialist (CNS) and assistant director of nursing identified that
patients within the stroke unit had a known risk of falling but sat outside of the National Institute for
Health and Care Excellence (NICE) Falls in older people: assessing risk and prevention (CG 161).
This guideline covered assessment of falls risk and interventions to prevent falls in people aged 65
and over. It aimed to reduce the risk and incidence of falls and the associated distress, pain,
injury, loss of confidence, loss of independence and mortality. In order to address this issue, and
promote safety among this patient group, the service held a weekly meeting with the matron,
senior ward sister, and thrombolysis lead to review all patients with this area with a focus on
factors contributing to falls. For example, known falls risk, current mobility, witnessed impulsivity
and opportunities to fall. The process was Plan, Do, Study Act (PDSA) assessed and lead to
stroke-specific identification of falls risks and individualised interventions, pertinent to this specific
client group, being implemented.
Data supplied by the trust following our inspection showed nursing staff achieved 82% compliance
with adult basic life support training and 85% with immediate life support.
Medical staff achieved 67% compliance with adult basic life support, 69% compliance with
immediate life support and 50% compliance with paediatric basic life support.
Nurse staffing
The service had enough nursing and support staff with the right qualifications, skills,
training and experience to keep patients safe from avoidable harm and to provide the right
care and treatment. Managers regularly reviewed and adjusted staffing levels and skill mix,
and gave bank and agency staff a full induction.
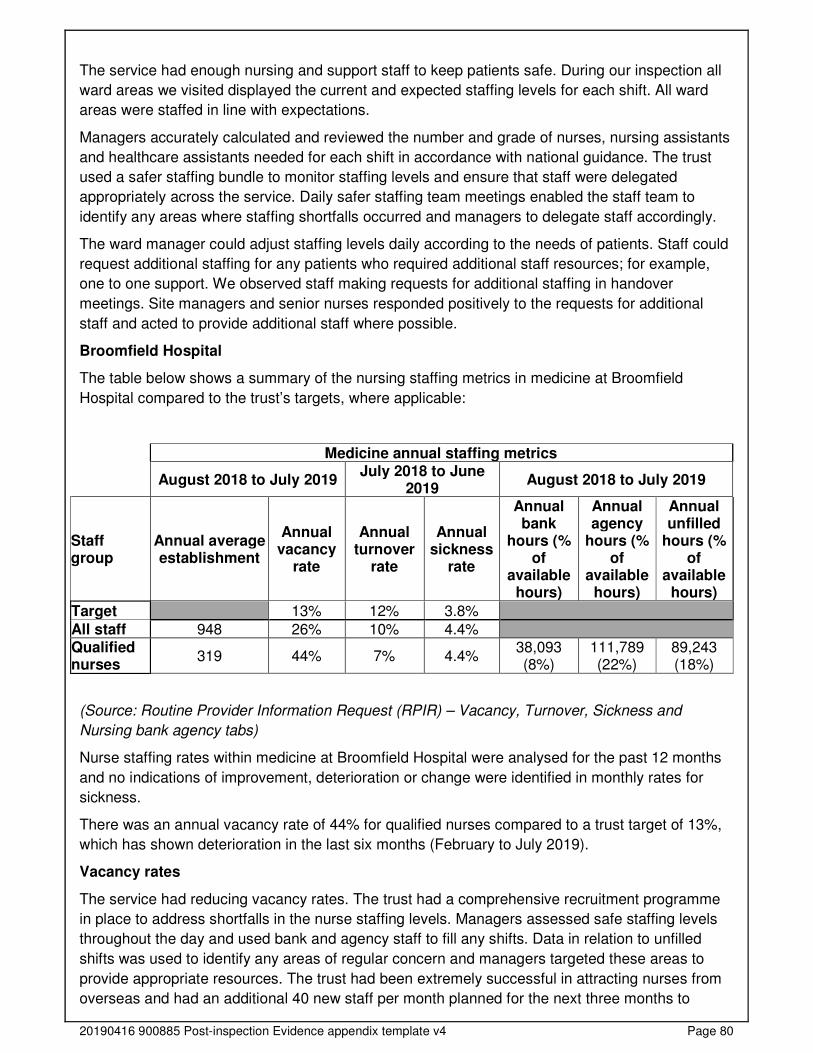
20190416 900885 Post-inspection Evidence appendix template v4 Page 80
The service had enough nursing and support staff to keep patients safe. During our inspection all
ward areas we visited displayed the current and expected staffing levels for each shift. All ward
areas were staffed in line with expectations.
Managers accurately calculated and reviewed the number and grade of nurses, nursing assistants
and healthcare assistants needed for each shift in accordance with national guidance. The trust
used a safer staffing bundle to monitor staffing levels and ensure that staff were delegated
appropriately across the service. Daily safer staffing team meetings enabled the staff team to
identify any areas where staffing shortfalls occurred and managers to delegate staff accordingly.
The ward manager could adjust staffing levels daily according to the needs of patients. Staff could
request additional staffing for any patients who required additional staff resources; for example,
one to one support. We observed staff making requests for additional staffing in handover
meetings. Site managers and senior nurses responded positively to the requests for additional
staff and acted to provide additional staff where possible.
Broomfield Hospital
The table below shows a summary of the nursing staffing metrics in medicine at Broomfield
Hospital compared to the trust’s targets, where applicable:
Medicine annual staffing metrics
August 2018 to July 2019 July 2018 to June
2019 August 2018 to July 2019
Staff group
Annual average establishment
Annual vacancy
rate
Annual turnover
rate
Annual sickness
rate
Annual bank
hours (% of
available hours)
Annual agency
hours (% of
available hours)
Annual unfilled
hours (% of
available hours)
Target 13% 12% 3.8%
All staff 948 26% 10% 4.4% Qualified nurses
319 44% 7% 4.4% 38,093 (8%)
111,789 (22%)
89,243 (18%)
(Source: Routine Provider Information Request (RPIR) – Vacancy, Turnover, Sickness and
Nursing bank agency tabs)
Nurse staffing rates within medicine at Broomfield Hospital were analysed for the past 12 months
and no indications of improvement, deterioration or change were identified in monthly rates for
sickness.
There was an annual vacancy rate of 44% for qualified nurses compared to a trust target of 13%,
which has shown deterioration in the last six months (February to July 2019).
Vacancy rates
The service had reducing vacancy rates. The trust had a comprehensive recruitment programme
in place to address shortfalls in the nurse staffing levels. Managers assessed safe staffing levels
throughout the day and used bank and agency staff to fill any shifts. Data in relation to unfilled
shifts was used to identify any areas of regular concern and managers targeted these areas to
provide appropriate resources. The trust had been extremely successful in attracting nurses from
overseas and had an additional 40 new staff per month planned for the next three months to
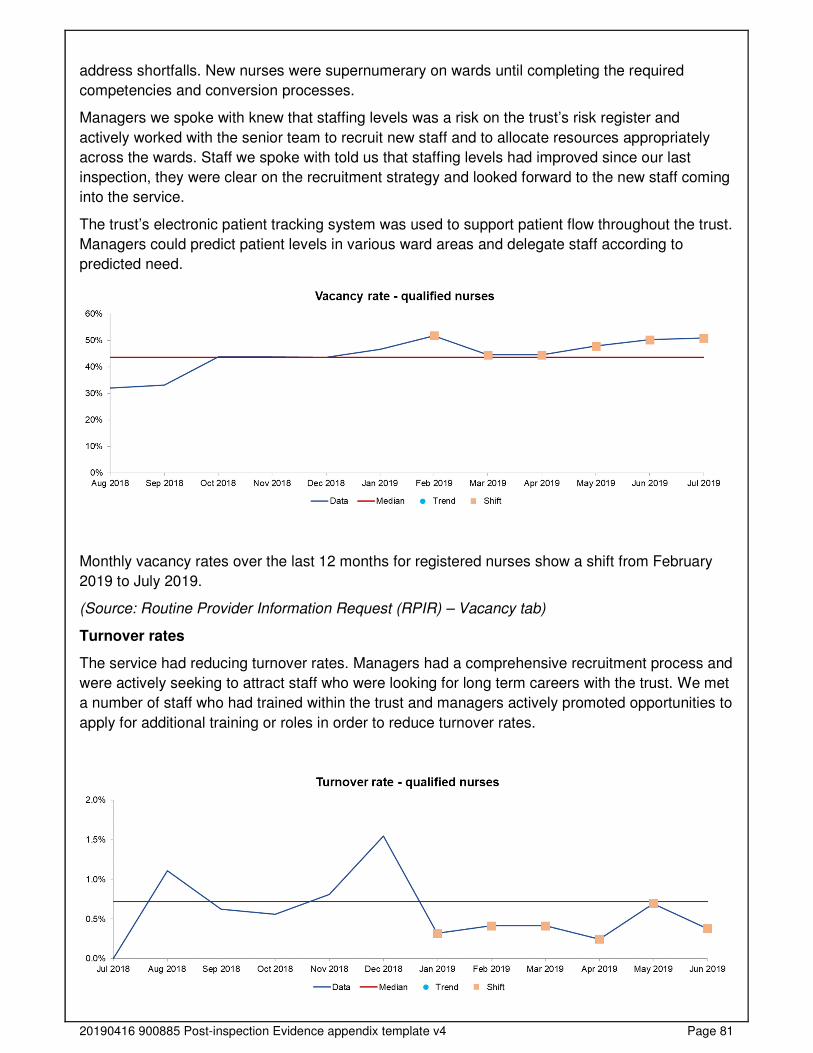
20190416 900885 Post-inspection Evidence appendix template v4 Page 81
address shortfalls. New nurses were supernumerary on wards until completing the required
competencies and conversion processes.
Managers we spoke with knew that staffing levels was a risk on the trust’s risk register and
actively worked with the senior team to recruit new staff and to allocate resources appropriately
across the wards. Staff we spoke with told us that staffing levels had improved since our last
inspection, they were clear on the recruitment strategy and looked forward to the new staff coming
into the service.
The trust’s electronic patient tracking system was used to support patient flow throughout the trust.
Managers could predict patient levels in various ward areas and delegate staff according to
predicted need.
Monthly vacancy rates over the last 12 months for registered nurses show a shift from February
2019 to July 2019.
(Source: Routine Provider Information Request (RPIR) – Vacancy tab)
Turnover rates
The service had reducing turnover rates. Managers had a comprehensive recruitment process and
were actively seeking to attract staff who were looking for long term careers with the trust. We met
a number of staff who had trained within the trust and managers actively promoted opportunities to
apply for additional training or roles in order to reduce turnover rates.

20190416 900885 Post-inspection Evidence appendix template v4 Page 82
Monthly turnover rates over the last 12 months for registered nurses show a shift from January
2019 to June 2019.
(Source: Routine Provider Information Request (RPIR) – Turnover tab)
Bank and agency staff usage
The service had reducing rates of bank and agency nurses used on the wards. This was due to
the comprehensive recruitment programme.
Monthly bank hours over the last 12 months for registered nurses show an upward trend from
August 2018 to February 2019 followed by a downward trend from February 2019 to July 2019.
Monthly agency hours over the last 12 months for registered nurses, health visitors and midwives
show a shift from February 2019 to July 2019.
(Source: Routine Provider Information Request (RPIR) - Nursing bank agency tab)
Managers limited their use of bank and agency staff and requested staff familiar with the service.
The trust was piloting a bank staffing ‘app’ designed by the trust. This innovation differed from
other staffing apps as it was skills-based and used the data to identify where skill gaps were, and
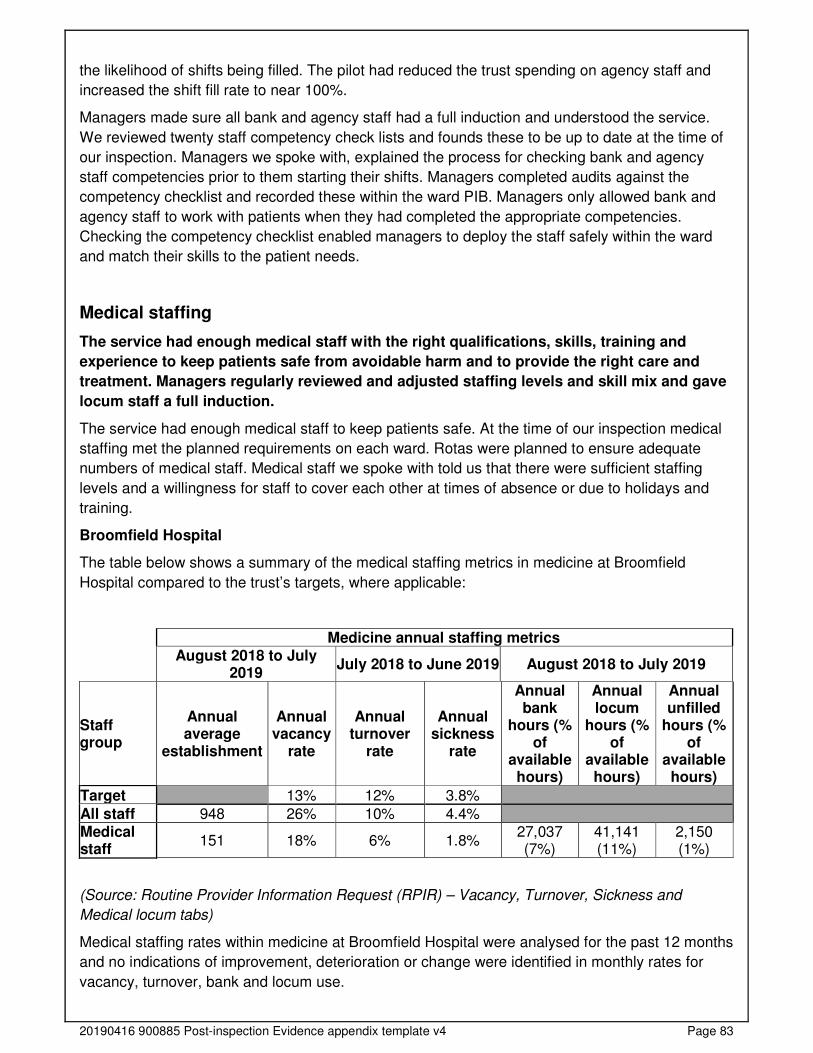
20190416 900885 Post-inspection Evidence appendix template v4 Page 83
the likelihood of shifts being filled. The pilot had reduced the trust spending on agency staff and
increased the shift fill rate to near 100%.
Managers made sure all bank and agency staff had a full induction and understood the service.
We reviewed twenty staff competency check lists and founds these to be up to date at the time of
our inspection. Managers we spoke with, explained the process for checking bank and agency
staff competencies prior to them starting their shifts. Managers completed audits against the
competency checklist and recorded these within the ward PIB. Managers only allowed bank and
agency staff to work with patients when they had completed the appropriate competencies.
Checking the competency checklist enabled managers to deploy the staff safely within the ward
and match their skills to the patient needs.
Medical staffing
The service had enough medical staff with the right qualifications, skills, training and
experience to keep patients safe from avoidable harm and to provide the right care and
treatment. Managers regularly reviewed and adjusted staffing levels and skill mix and gave
locum staff a full induction.
The service had enough medical staff to keep patients safe. At the time of our inspection medical
staffing met the planned requirements on each ward. Rotas were planned to ensure adequate
numbers of medical staff. Medical staff we spoke with told us that there were sufficient staffing
levels and a willingness for staff to cover each other at times of absence or due to holidays and
training.
Broomfield Hospital
The table below shows a summary of the medical staffing metrics in medicine at Broomfield
Hospital compared to the trust’s targets, where applicable:
Medicine annual staffing metrics
August 2018 to July
2019 July 2018 to June 2019 August 2018 to July 2019
Staff group
Annual average
establishment
Annual vacancy
rate
Annual turnover
rate
Annual sickness
rate
Annual bank
hours (% of
available hours)
Annual locum
hours (% of
available hours)
Annual unfilled
hours (% of
available hours)
Target 13% 12% 3.8%
All staff 948 26% 10% 4.4% Medical staff
151 18% 6% 1.8% 27,037 (7%)
41,141 (11%)
2,150 (1%)
(Source: Routine Provider Information Request (RPIR) – Vacancy, Turnover, Sickness and
Medical locum tabs)
Medical staffing rates within medicine at Broomfield Hospital were analysed for the past 12 months
and no indications of improvement, deterioration or change were identified in monthly rates for
vacancy, turnover, bank and locum use.
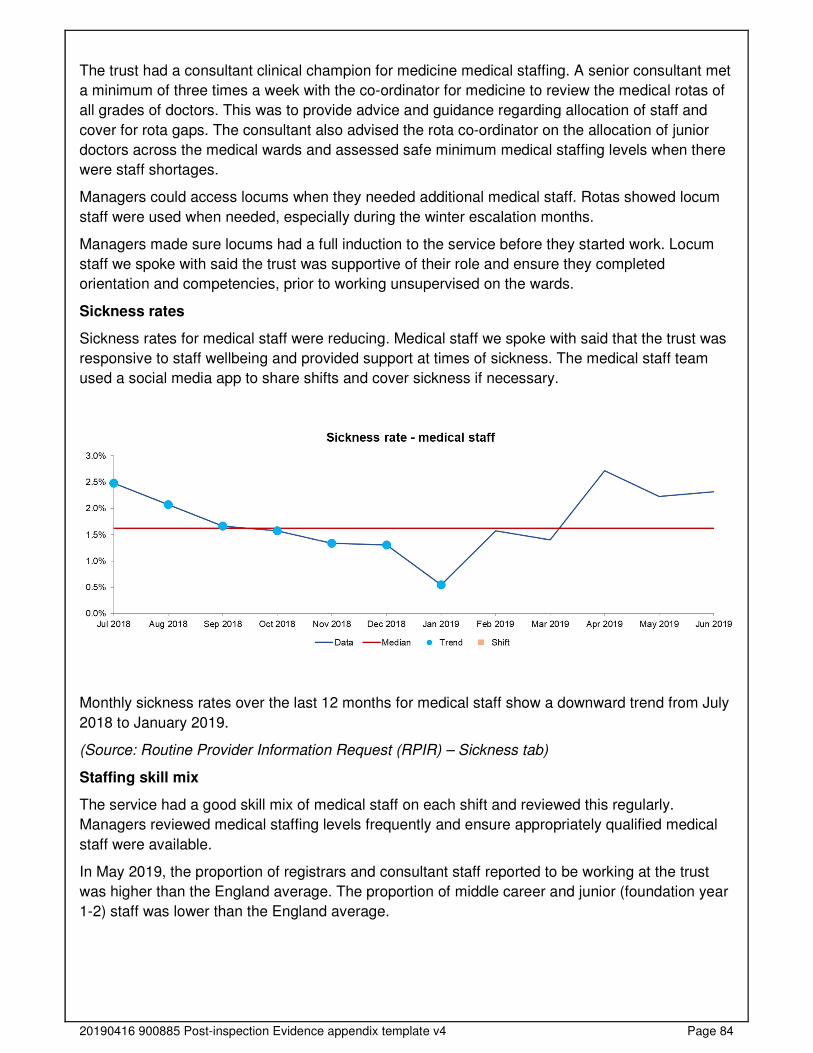
20190416 900885 Post-inspection Evidence appendix template v4 Page 84
The trust had a consultant clinical champion for medicine medical staffing. A senior consultant met
a minimum of three times a week with the co-ordinator for medicine to review the medical rotas of
all grades of doctors. This was to provide advice and guidance regarding allocation of staff and
cover for rota gaps. The consultant also advised the rota co-ordinator on the allocation of junior
doctors across the medical wards and assessed safe minimum medical staffing levels when there
were staff shortages.
Managers could access locums when they needed additional medical staff. Rotas showed locum
staff were used when needed, especially during the winter escalation months.
Managers made sure locums had a full induction to the service before they started work. Locum
staff we spoke with said the trust was supportive of their role and ensure they completed
orientation and competencies, prior to working unsupervised on the wards.
Sickness rates
Sickness rates for medical staff were reducing. Medical staff we spoke with said that the trust was
responsive to staff wellbeing and provided support at times of sickness. The medical staff team
used a social media app to share shifts and cover sickness if necessary.
Monthly sickness rates over the last 12 months for medical staff show a downward trend from July
2018 to January 2019.
(Source: Routine Provider Information Request (RPIR) – Sickness tab)
Staffing skill mix
The service had a good skill mix of medical staff on each shift and reviewed this regularly.
Managers reviewed medical staffing levels frequently and ensure appropriately qualified medical
staff were available.
In May 2019, the proportion of registrars and consultant staff reported to be working at the trust
was higher than the England average. The proportion of middle career and junior (foundation year
1-2) staff was lower than the England average.
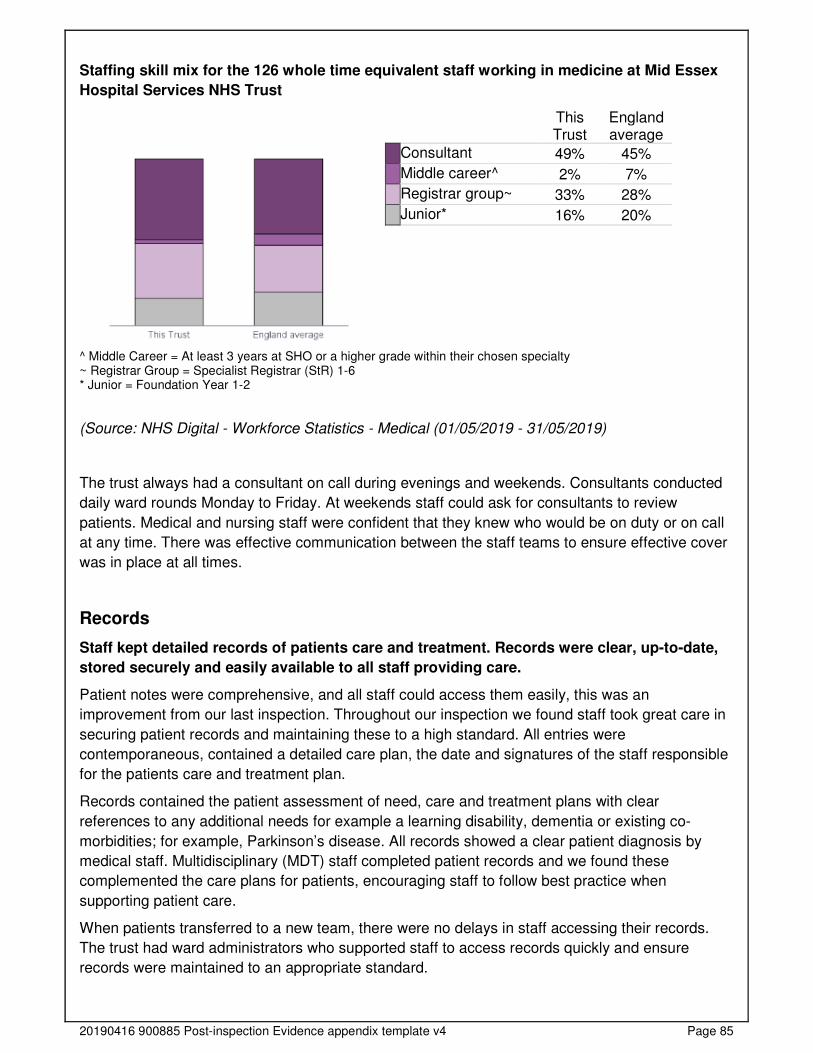
20190416 900885 Post-inspection Evidence appendix template v4 Page 85
Staffing skill mix for the 126 whole time equivalent staff working in medicine at Mid Essex
Hospital Services NHS Trust
This Trust
England average
Consultant 49% 45%
Middle career^ 2% 7%
Registrar group~ 33% 28%
Junior* 16% 20%
^ Middle Career = At least 3 years at SHO or a higher grade within their chosen specialty ~ Registrar Group = Specialist Registrar (StR) 1-6 * Junior = Foundation Year 1-2
(Source: NHS Digital - Workforce Statistics - Medical (01/05/2019 - 31/05/2019)
The trust always had a consultant on call during evenings and weekends. Consultants conducted
daily ward rounds Monday to Friday. At weekends staff could ask for consultants to review
patients. Medical and nursing staff were confident that they knew who would be on duty or on call
at any time. There was effective communication between the staff teams to ensure effective cover
was in place at all times.
Records
Staff kept detailed records of patients care and treatment. Records were clear, up-to-date,
stored securely and easily available to all staff providing care.
Patient notes were comprehensive, and all staff could access them easily, this was an
improvement from our last inspection. Throughout our inspection we found staff took great care in
securing patient records and maintaining these to a high standard. All entries were
contemporaneous, contained a detailed care plan, the date and signatures of the staff responsible
for the patients care and treatment plan.
Records contained the patient assessment of need, care and treatment plans with clear
references to any additional needs for example a learning disability, dementia or existing co-
morbidities; for example, Parkinson’s disease. All records showed a clear patient diagnosis by
medical staff. Multidisciplinary (MDT) staff completed patient records and we found these
complemented the care plans for patients, encouraging staff to follow best practice when
supporting patient care.
When patients transferred to a new team, there were no delays in staff accessing their records.
The trust had ward administrators who supported staff to access records quickly and ensure
records were maintained to an appropriate standard.
20190416 900885 Post-inspection Evidence appendix template v4 Page 86
Records were stored securely. Patient nursing records were stored at the end of the patient’s bed
in a closed folder and medical records were stored in a locked cabinet with key pad entry.
Medicines
The service used systems and processes to safely prescribe, administer, record and store
medicines.
Staff followed systems and processes when safely prescribing, administering, recording and
storing medicines. Patient records we reviewed showed allergies clearly documented and all
records were signed and dated by a clinician or nurse in charge of the patient’s care.
Staff reviewed patients’ medicines regularly and provided specific advice to patients and carers
about their medicines. Patient medication was reviewed daily during the ward rounds. Pharmacy
staff visited the wards to review patients, complete medication reconciliation and to arrange tablets
to take home.
Patients were provided with advice and information about their medications. We spoke with one
patient who explained how staff had guided them through their medications routine and explained
the way the medicines worked and any side effects.
Staff stored and managed medicines and prescribing documents in line with the provider’s policy.
We reviewed the controlled drugs records on the wards we visited. These demonstrated that staff
comprehensively reviewed and signed for controlled drugs in line with the trust’s medications
policy. On the ward’s medications were stored in a locked cupboard within a locked room. Access
to this room was limited to named roles and the key pad password was regularly changed. Staff
recorded ambient medication room temperatures and refrigeration temperatures accurately on all
the wards we visited. Records showed that between August 2019 to November 2019 checks were
completed daily. This was an improvement from our last inspection.
Staff followed current national practice to check patients had the correct medicines. Staff ensured
that the right patient had the right medications. All patients had barcodes on their wrist bands that
staff scanned prior to medication administration to ensure that the right patient was getting the
right medicine, right dose, at the right time and by the right route. Staff wore orange tabards whilst
undertaking medication rounds, which clearly stated, ‘do not disturb during medicine rounds’ to
minimise medication errors due to staff distraction.
The service had systems to ensure staff knew about safety alerts and incidents, so patients
received their medicines safely. Any medication safety alerts were shared at clinical governance
meetings, with the information shared through the hospital’s hot topic of the day, or during staff
handovers.
Decision making processes were in place to ensure people’s behaviour was not controlled by
excessive and inappropriate use of medicines. Staff ensured that patient behaviour was not being
controlled by inappropriate use of medicines, this was in line with the trust’s medication policy.
Staff discussed patient medicines and medication reviews during handovers and could seek
additional guidance from the trust’s pharmacy team. Staff recorded all medicines administered,
including those given PRN, which means “As needed”, to ensure patients were not taking
excessive amounts.
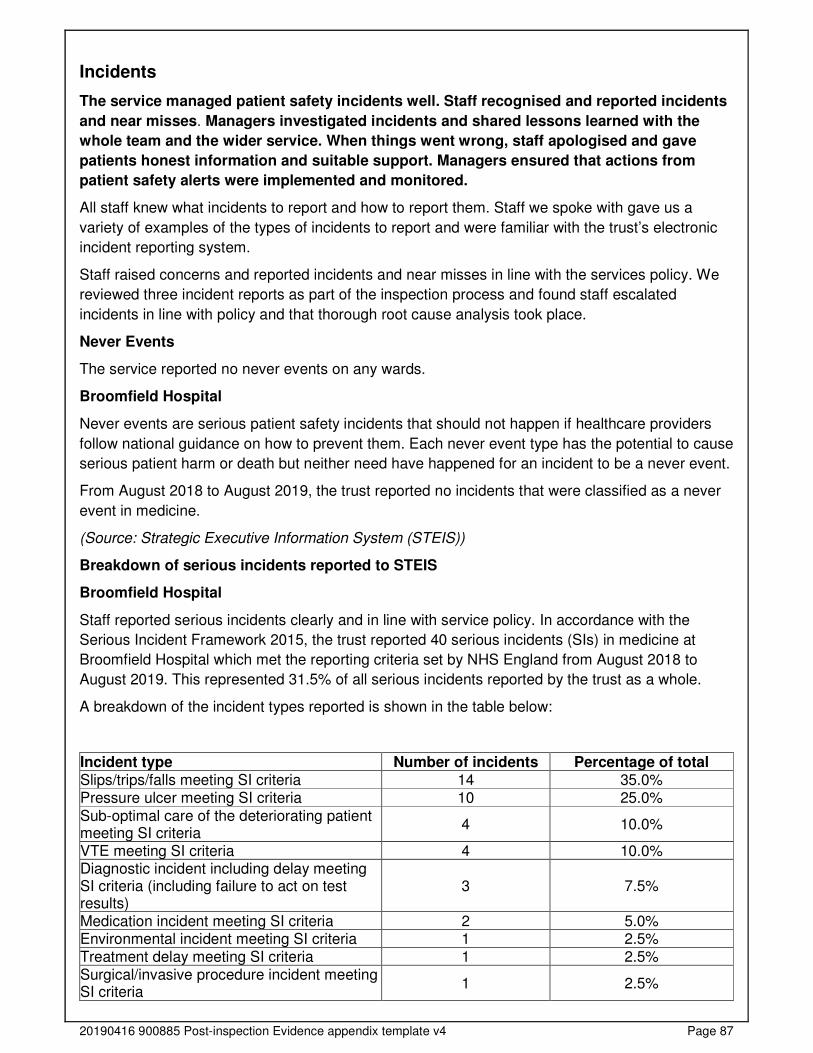
20190416 900885 Post-inspection Evidence appendix template v4 Page 87
Incidents
The service managed patient safety incidents well. Staff recognised and reported incidents
and near misses. Managers investigated incidents and shared lessons learned with the
whole team and the wider service. When things went wrong, staff apologised and gave
patients honest information and suitable support. Managers ensured that actions from
patient safety alerts were implemented and monitored.
All staff knew what incidents to report and how to report them. Staff we spoke with gave us a
variety of examples of the types of incidents to report and were familiar with the trust’s electronic
incident reporting system.
Staff raised concerns and reported incidents and near misses in line with the services policy. We
reviewed three incident reports as part of the inspection process and found staff escalated
incidents in line with policy and that thorough root cause analysis took place.
Never Events
The service reported no never events on any wards.
Broomfield Hospital
Never events are serious patient safety incidents that should not happen if healthcare providers
follow national guidance on how to prevent them. Each never event type has the potential to cause
serious patient harm or death but neither need have happened for an incident to be a never event.
From August 2018 to August 2019, the trust reported no incidents that were classified as a never
event in medicine.
(Source: Strategic Executive Information System (STEIS))
Breakdown of serious incidents reported to STEIS
Broomfield Hospital
Staff reported serious incidents clearly and in line with service policy. In accordance with the
Serious Incident Framework 2015, the trust reported 40 serious incidents (SIs) in medicine at
Broomfield Hospital which met the reporting criteria set by NHS England from August 2018 to
August 2019. This represented 31.5% of all serious incidents reported by the trust as a whole.
A breakdown of the incident types reported is shown in the table below:
Incident type Number of incidents Percentage of total Slips/trips/falls meeting SI criteria 14 35.0% Pressure ulcer meeting SI criteria 10 25.0%
Sub-optimal care of the deteriorating patient meeting SI criteria
4 10.0%
VTE meeting SI criteria 4 10.0% Diagnostic incident including delay meeting SI criteria (including failure to act on test results)
3 7.5%
Medication incident meeting SI criteria 2 5.0% Environmental incident meeting SI criteria 1 2.5% Treatment delay meeting SI criteria 1 2.5% Surgical/invasive procedure incident meeting SI criteria
1 2.5%
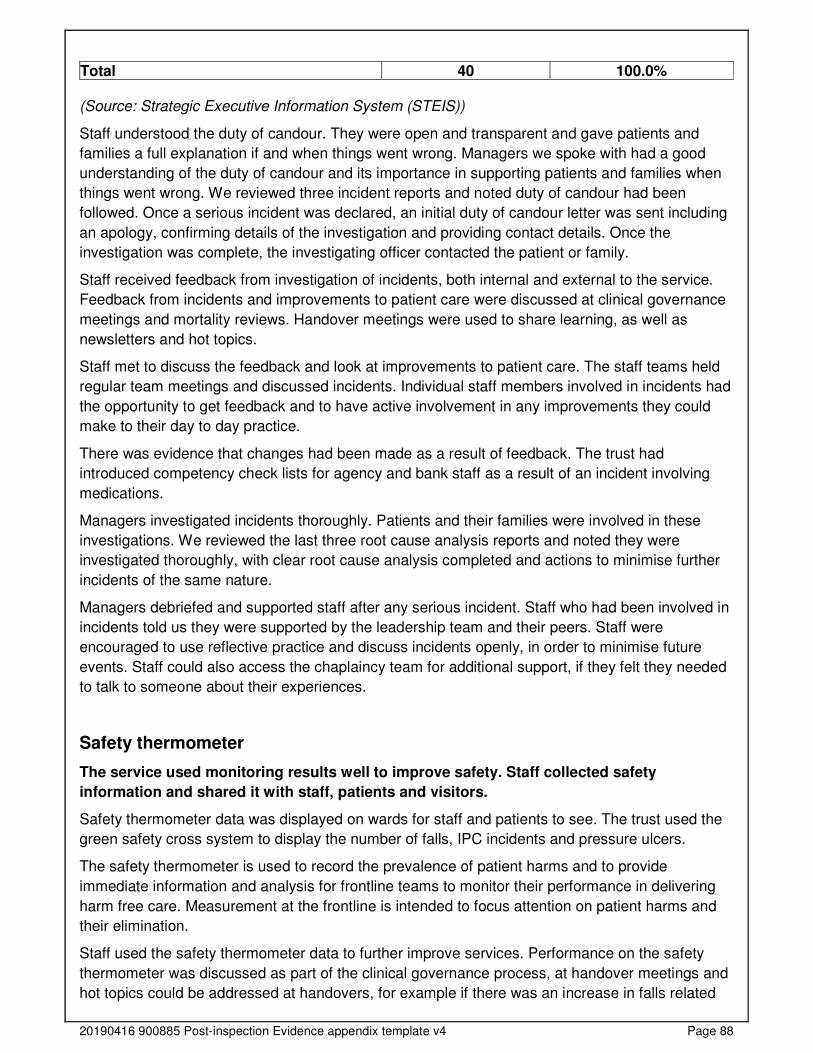
20190416 900885 Post-inspection Evidence appendix template v4 Page 88
Total 40 100.0% (Source: Strategic Executive Information System (STEIS))
Staff understood the duty of candour. They were open and transparent and gave patients and
families a full explanation if and when things went wrong. Managers we spoke with had a good
understanding of the duty of candour and its importance in supporting patients and families when
things went wrong. We reviewed three incident reports and noted duty of candour had been
followed. Once a serious incident was declared, an initial duty of candour letter was sent including
an apology, confirming details of the investigation and providing contact details. Once the
investigation was complete, the investigating officer contacted the patient or family.
Staff received feedback from investigation of incidents, both internal and external to the service.
Feedback from incidents and improvements to patient care were discussed at clinical governance
meetings and mortality reviews. Handover meetings were used to share learning, as well as
newsletters and hot topics.
Staff met to discuss the feedback and look at improvements to patient care. The staff teams held
regular team meetings and discussed incidents. Individual staff members involved in incidents had
the opportunity to get feedback and to have active involvement in any improvements they could
make to their day to day practice.
There was evidence that changes had been made as a result of feedback. The trust had
introduced competency check lists for agency and bank staff as a result of an incident involving
medications.
Managers investigated incidents thoroughly. Patients and their families were involved in these
investigations. We reviewed the last three root cause analysis reports and noted they were
investigated thoroughly, with clear root cause analysis completed and actions to minimise further
incidents of the same nature.
Managers debriefed and supported staff after any serious incident. Staff who had been involved in
incidents told us they were supported by the leadership team and their peers. Staff were
encouraged to use reflective practice and discuss incidents openly, in order to minimise future
events. Staff could also access the chaplaincy team for additional support, if they felt they needed
to talk to someone about their experiences.
Safety thermometer
The service used monitoring results well to improve safety. Staff collected safety
information and shared it with staff, patients and visitors.
Safety thermometer data was displayed on wards for staff and patients to see. The trust used the
green safety cross system to display the number of falls, IPC incidents and pressure ulcers.
The safety thermometer is used to record the prevalence of patient harms and to provide
immediate information and analysis for frontline teams to monitor their performance in delivering
harm free care. Measurement at the frontline is intended to focus attention on patient harms and
their elimination.
Staff used the safety thermometer data to further improve services. Performance on the safety
thermometer was discussed as part of the clinical governance process, at handover meetings and
hot topics could be addressed at handovers, for example if there was an increase in falls related
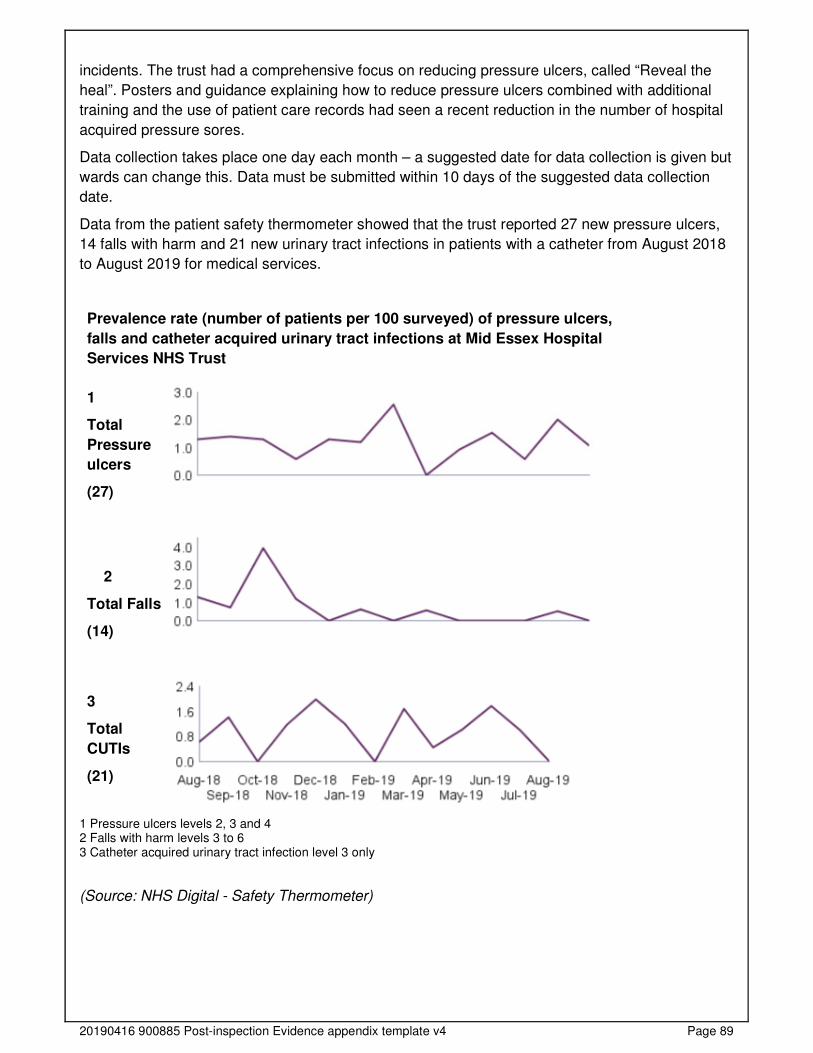
20190416 900885 Post-inspection Evidence appendix template v4 Page 89
incidents. The trust had a comprehensive focus on reducing pressure ulcers, called “Reveal the
heal”. Posters and guidance explaining how to reduce pressure ulcers combined with additional
training and the use of patient care records had seen a recent reduction in the number of hospital
acquired pressure sores.
Data collection takes place one day each month – a suggested date for data collection is given but
wards can change this. Data must be submitted within 10 days of the suggested data collection
date.
Data from the patient safety thermometer showed that the trust reported 27 new pressure ulcers,
14 falls with harm and 21 new urinary tract infections in patients with a catheter from August 2018
to August 2019 for medical services.
Prevalence rate (number of patients per 100 surveyed) of pressure ulcers,
falls and catheter acquired urinary tract infections at Mid Essex Hospital
Services NHS Trust
1
Total
Pressure
ulcers
(27)
2
Total Falls
(14)
3
Total
CUTIs
(21)
1 Pressure ulcers levels 2, 3 and 4 2 Falls with harm levels 3 to 6 3 Catheter acquired urinary tract infection level 3 only
(Source: NHS Digital - Safety Thermometer)

20190416 900885 Post-inspection Evidence appendix template v4 Page 90
Is the service effective?
Evidence-based care and treatment
The service provided care and treatment based on national guidance and evidence-based
practice. Managers checked to make sure staff followed guidance. Staff protected the
rights of patients subject to the Mental Health Act 1983.
Staff followed up-to-date policies to plan and deliver high quality care according to best practice
and national guidance. We reviewed eight policies on the trust’s intranet and they were all up to
date. Staff had access to up to date clinical guidance and the intranet provided a wide range of up
to date care pathways and advice for practitioners.
The trust had a process in place to identify new guidance published on the National Institute for
Health & Care Excellence (NICE) website monthly. This was directed to the relevant clinical
speciality lead. The lead carried out a baseline assessment who reviewed current practice against
the guidelines. Based on this assessment, the specialty lead agreed with the divisional triumvirate
any required implementation plan. The trust’s clinical effectiveness group received and monitored
the NICE internal compliance dashboard.
The trust had a dementia strategy which related to various best practice guidance including NICE
Quality Standard: Dementia (QS184), 2019. NICE Quality Standard: Delirium (QS63), 2014. NICE
Guideline: Dementia: assessment, management and support for people living with dementia and
their carers (NG97), 2018 and the Prime Minister’s Challenge on Dementia, 2020.
Staff protected the rights of patients subject to the Mental Health Act and followed the Code of
Practice. Staff were aware of patient rights under the Mental Health Act and knew how to reach
the mental health team to ensure patient care was being given appropriately. However, staff said
the response times for mental health support varied greatly.
At handover meetings, staff routinely referred to the psychological and emotional needs of
patients, their relatives and carers. Staff comprehensively discussed patient emotional and
psychological needs during handovers. This ensured that appropriate referrals to specialist staff
for example speech and language, occupational therapy, physiotherapy or the mental health team
were actively managed.
The renal service had measures in place for continued assessment of a patient’s vascular access
for example arteriovenous fistula and line rates, and processes for regular monitoring of vascular
access function. Managers maintained dialysis staff competency training records to ensure they
followed standard operating procedures to minimise the risk of infection. For example, electrolyte
imbalance, symptomatic dialysis-related hypotension and accidental venous needle/line
disconnection. The trust also provided clear pictorial guides for staff and patients to reduce
accidental venous needle/line disconnection.
Nutrition and hydration
Staff gave patients enough food and drink to meet their needs and improve their health.
They used special feeding and hydration techniques when necessary. The service made
adjustments for patients religious, cultural and other needs.
Staff made sure patients had enough to eat and drink, including those with special nutrition and
hydration needs. Patients on the medical wards had protected meal times to ensure that they had
time to eat and drink in a calm environment. Staff helped patients to eat when they were unable to
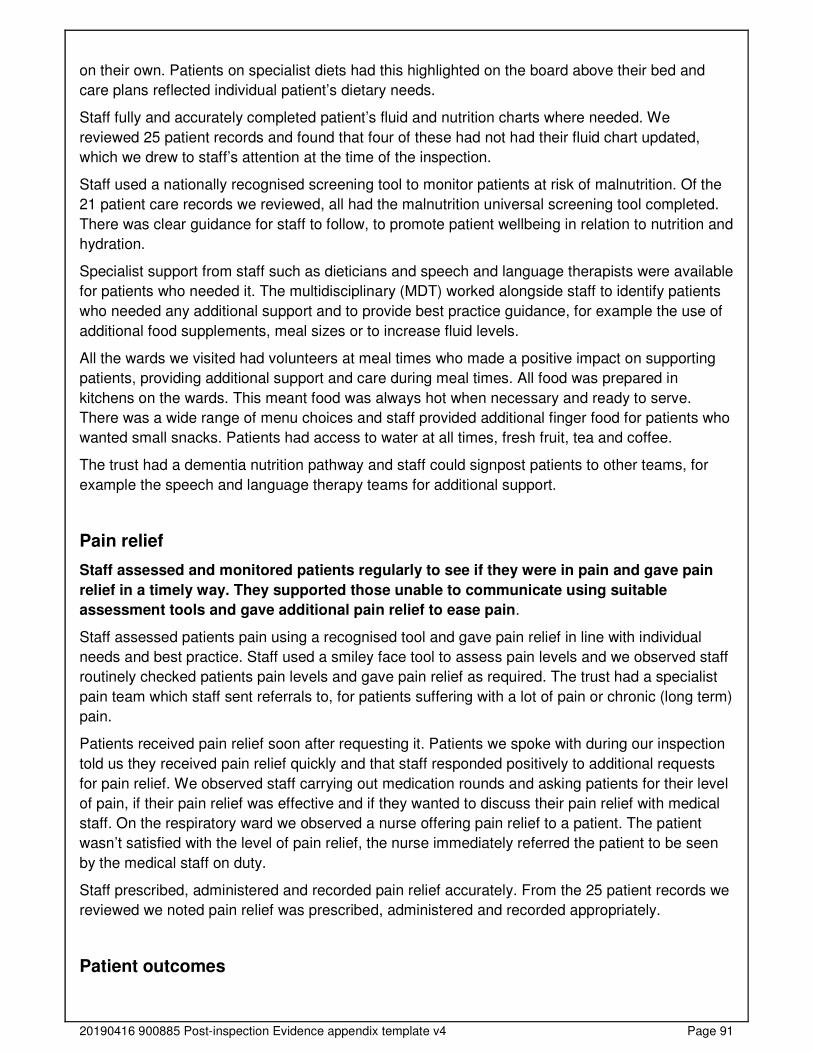
20190416 900885 Post-inspection Evidence appendix template v4 Page 91
on their own. Patients on specialist diets had this highlighted on the board above their bed and
care plans reflected individual patient’s dietary needs.
Staff fully and accurately completed patient’s fluid and nutrition charts where needed. We
reviewed 25 patient records and found that four of these had not had their fluid chart updated,
which we drew to staff’s attention at the time of the inspection.
Staff used a nationally recognised screening tool to monitor patients at risk of malnutrition. Of the
21 patient care records we reviewed, all had the malnutrition universal screening tool completed.
There was clear guidance for staff to follow, to promote patient wellbeing in relation to nutrition and
hydration.
Specialist support from staff such as dieticians and speech and language therapists were available
for patients who needed it. The multidisciplinary (MDT) worked alongside staff to identify patients
who needed any additional support and to provide best practice guidance, for example the use of
additional food supplements, meal sizes or to increase fluid levels.
All the wards we visited had volunteers at meal times who made a positive impact on supporting
patients, providing additional support and care during meal times. All food was prepared in
kitchens on the wards. This meant food was always hot when necessary and ready to serve.
There was a wide range of menu choices and staff provided additional finger food for patients who
wanted small snacks. Patients had access to water at all times, fresh fruit, tea and coffee.
The trust had a dementia nutrition pathway and staff could signpost patients to other teams, for
example the speech and language therapy teams for additional support.
Pain relief
Staff assessed and monitored patients regularly to see if they were in pain and gave pain
relief in a timely way. They supported those unable to communicate using suitable
assessment tools and gave additional pain relief to ease pain.
Staff assessed patients pain using a recognised tool and gave pain relief in line with individual
needs and best practice. Staff used a smiley face tool to assess pain levels and we observed staff
routinely checked patients pain levels and gave pain relief as required. The trust had a specialist
pain team which staff sent referrals to, for patients suffering with a lot of pain or chronic (long term)
pain.
Patients received pain relief soon after requesting it. Patients we spoke with during our inspection
told us they received pain relief quickly and that staff responded positively to additional requests
for pain relief. We observed staff carrying out medication rounds and asking patients for their level
of pain, if their pain relief was effective and if they wanted to discuss their pain relief with medical
staff. On the respiratory ward we observed a nurse offering pain relief to a patient. The patient
wasn’t satisfied with the level of pain relief, the nurse immediately referred the patient to be seen
by the medical staff on duty.
Staff prescribed, administered and recorded pain relief accurately. From the 25 patient records we
reviewed we noted pain relief was prescribed, administered and recorded appropriately.
Patient outcomes

20190416 900885 Post-inspection Evidence appendix template v4 Page 92
Staff monitored the effectiveness of care and treatment. They used the findings to make
improvements and achieved good outcomes for patients.
Managers and staff carried out a comprehensive programme of repeated audits to check
improvement over time and the service participated in relevant national clinical audits. The trust
participated in a range of national audits and shared its outcomes with staff and external
stakeholders.
Outcomes for patients were positive, consistent and met expectations, such as national standards.
For example, the trust took part in the quarterly Sentinel Stroke National Audit programme. On a
scale of A-E, where A is best, the trust achieved grade A in latest audit, covering the period from
January to March 2019. The hospital has achieved an overall grade A in each of the last four data
collection periods.
Managers and staff used the results to improve patient outcomes. The trust used audit data to
improve services, for example ongoing recruitment of consultant oncologists to support
assessment and delivery of treatment to patients with cancer in response to the National Lung
Cancer Audit.
Relative risk of readmission
Elective Admissions - Broomfield Hospital
From February 2018 to January 2019, patients at Broomfield Hospital had a lower than expected
risk of readmission for elective admissions when compared to the England average.
• Patients in medical oncology and clinical haematology had a lower than expected risk of
readmission for elective admissions compared to the England average.
• Patients in general medicine had a higher than expected risk of readmission for elective
admissions compared to the England average.
Note: Ratio of observed to expected emergency readmissions multiplied by 100. A value below
100 is interpreted as a positive finding, as this means there were fewer observed readmissions
than expected. A value above 100 represents the opposite. Top three specialties for specific site
based on count of activity.
Non-Elective Admissions - Broomfield Hospital
From February 2018 to January 2019, patients at Broomfield Hospital had a similar to expected
risk of readmission for non-elective admissions when compared to the England average.
• Patients in general medicine had a similar to expected risk of readmission for non-elective
admissions compared to the England average.

20190416 900885 Post-inspection Evidence appendix template v4 Page 93
• Patients in geriatric medicine had a higher than expected risk of readmission for non-
elective admissions compared to the England average.
• Patients in stroke medicine had a lower than expected risk of readmission for non-elective
admissions compared to the England average.
Note: Ratio of observed to expected emergency readmissions multiplied by 100. A value below
100 is interpreted as a positive finding, as this means there were fewer observed readmissions
than expected. A value above 100 represents the opposite. Top three specialties for specific site
based on count of activity.
(Source: Hospital Episode Statistics - HES - Readmissions (01/02/2018 - 31/01/2019))
Sentinel Stroke National Audit Programme (SSNAP)
Broomfield Hospital
Broomfield Hospital took part in the quarterly Sentinel Stroke National Audit programme. On a
scale of A-E, where A is best, the trust achieved grade A in latest audit, covering the period from
January to March 2019. The hospital has achieved an overall grade A in each of the last four data
collection periods.
The trust achieved either a grade A or grade B for all indicators in the audit other than the indicator
relating to the stroke unit where the hospital was awarded a grade C.
Overall Scores
Apr 18 -
Jun 18
Jul 18 -
Sep 18
Oct 18 -
Dec 18
Jan 19 -
Mar 19
SSNAP level A A A A
Case ascertainment band A A A A
Audit compliance band A A A A
Combined total key indicator level A A A A

20190416 900885 Post-inspection Evidence appendix template v4 Page 94
(Source: Royal College of Physicians London, SSNAP audit)
Lung Cancer Audit
The table below summarises Mid Essex Hospital Services NHS Trust’s performance in the 2018
National Lung Cancer Audit.
Metrics (Audit measures)
Trust performance
Comparison to other Trusts
Met national standard?
Patient centred performance
Apr 18 -
Jun 18
Jul 18 -
Sep 18
Oct 18 -
Dec 18
Jan 19 -
Mar 19
Domain 1: Scanning A A A A
Domain 2: Stroke unit C↓ B C↓ C
Domain 3: Thrombolysis A B↓ C↓ B↑
Domain 4: Specialist assessmentsA A A A
Domain 5: Occupational therapy C↓ A↑↑ A A
Domain 6: Physiotherapy B A↑ A B↓
Domain 7: Speech and language
therapyC↓ C B↑ B
Domain 8: Multi-disciplinary team
workingB B B B
Domain 9: Standards by dischargeA A A A
Domain 10: Discharge processes B↓ A↑ A A
Patient-centred total key indicator
levelA A A A
Team centred performance
Apr 18 -
Jun 18
Jul 18 -
Sep 18
Oct 18 -
Dec 18
Jan 19 -
Mar 19
Domain 1: Scanning A A A A
Domain 2: Stroke unit B↑ B C↓ C
Domain 3: Thrombolysis A B↓ C↓ B↑
Domain 4: Specialist assessmentsA A A A
Domain 5: Occupational therapy C↓↓ A↑↑ A A
Domain 6: Physiotherapy C↓ A↑↑ A B↓
Domain 7: Speech and language
therapyC C B↑ B
Domain 8: Multi-disciplinary team
workingB B B B
Domain 9: Standards by dischargeA A A A
Domain 10: Discharge processes A A A A
Team-centred total key indicator
levelA A A A

20190416 900885 Post-inspection Evidence appendix template v4 Page 95
Crude proportion of patients seen by a cancer nurse specialist (Access to a cancer nurse specialist is associated with increased receipt of anticancer treatment)
81.3% Does not meet the audit aspirational
standard Did not meet
Case-mix adjusted one-year survival rate (Adjusted scores take into account the differences in the case-mix of patients treated)
30.6% Within expected range No current standard
Case-mix adjusted percentage of patients with Non-Small Cell Lung Cancer (NSCLC) receiving surgery (Surgery remains the preferred treatment for early-stage lung cancer; adjusted scores take into account the differences in the case-mix of patients seen)
16.1% Within expected range Did not meet
Case-mix adjusted percentage of fit patients with advanced NSCLC receiving systemic anti-cancer treatment (For fitter patients with incurable NSCLC anti-cancer treatment is known to extend life expectancy and improve quality of life; adjusted scores take into account the differences in the case-mix of patients seen)
45.0% Worse than expected Did not meet
Case-mix adjusted percentage of patients with Small Cell Lung Cancer (SCLC) receiving chemotherapy (SCLC tumours are sensitive to chemotherapy which can improve survival and quality of life; adjusted scores take into account the differences in the case-mix of patients seen)
60.1% Within expected range Did not meet
(Source: National Lung Cancer Audit)
The trust participated in the Lung Cancer Audit and published its executive summary report in May
2019. The audit showed results were better than expected in five areas and the trust had an action
plan to address any shortfalls in the one remaining area.
National Audit of Inpatient Falls
Broomfield Hospital
The table below summarises Broomfield Hospital’s performance in the 2017 National Audit of
Inpatient Falls. The audit reports on the extent to which key indicators were met and grades
performance as red (less than 50% of patients received the assessment/intervention), amber
(between 50% and 79% of patients received the assessment/intervention) and green (more than
80% of patients received the assessment/intervention.
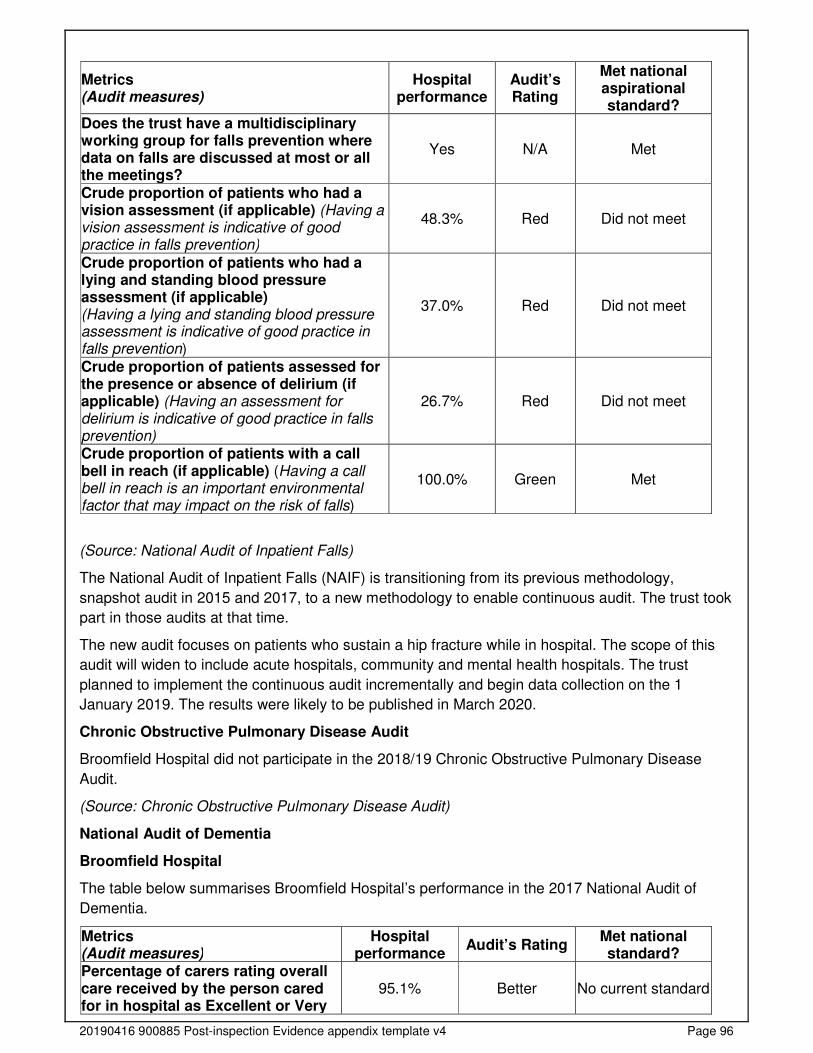
20190416 900885 Post-inspection Evidence appendix template v4 Page 96
Metrics (Audit measures)
Hospital performance
Audit’s Rating
Met national aspirational standard?
Does the trust have a multidisciplinary working group for falls prevention where data on falls are discussed at most or all the meetings?
Yes N/A Met
Crude proportion of patients who had a vision assessment (if applicable) (Having a vision assessment is indicative of good practice in falls prevention)
48.3% Red Did not meet
Crude proportion of patients who had a lying and standing blood pressure assessment (if applicable) (Having a lying and standing blood pressure assessment is indicative of good practice in falls prevention)
37.0% Red Did not meet
Crude proportion of patients assessed for the presence or absence of delirium (if applicable) (Having an assessment for delirium is indicative of good practice in falls prevention)
26.7% Red Did not meet
Crude proportion of patients with a call bell in reach (if applicable) (Having a call bell in reach is an important environmental factor that may impact on the risk of falls)
100.0% Green Met
(Source: National Audit of Inpatient Falls)
The National Audit of Inpatient Falls (NAIF) is transitioning from its previous methodology,
snapshot audit in 2015 and 2017, to a new methodology to enable continuous audit. The trust took
part in those audits at that time.
The new audit focuses on patients who sustain a hip fracture while in hospital. The scope of this
audit will widen to include acute hospitals, community and mental health hospitals. The trust
planned to implement the continuous audit incrementally and begin data collection on the 1
January 2019. The results were likely to be published in March 2020.
Chronic Obstructive Pulmonary Disease Audit
Broomfield Hospital did not participate in the 2018/19 Chronic Obstructive Pulmonary Disease
Audit.
(Source: Chronic Obstructive Pulmonary Disease Audit)
National Audit of Dementia
Broomfield Hospital
The table below summarises Broomfield Hospital’s performance in the 2017 National Audit of
Dementia.
Metrics (Audit measures)
Hospital performance
Audit’s Rating Met national standard?
Percentage of carers rating overall care received by the person cared for in hospital as Excellent or Very
95.1% Better No current standard
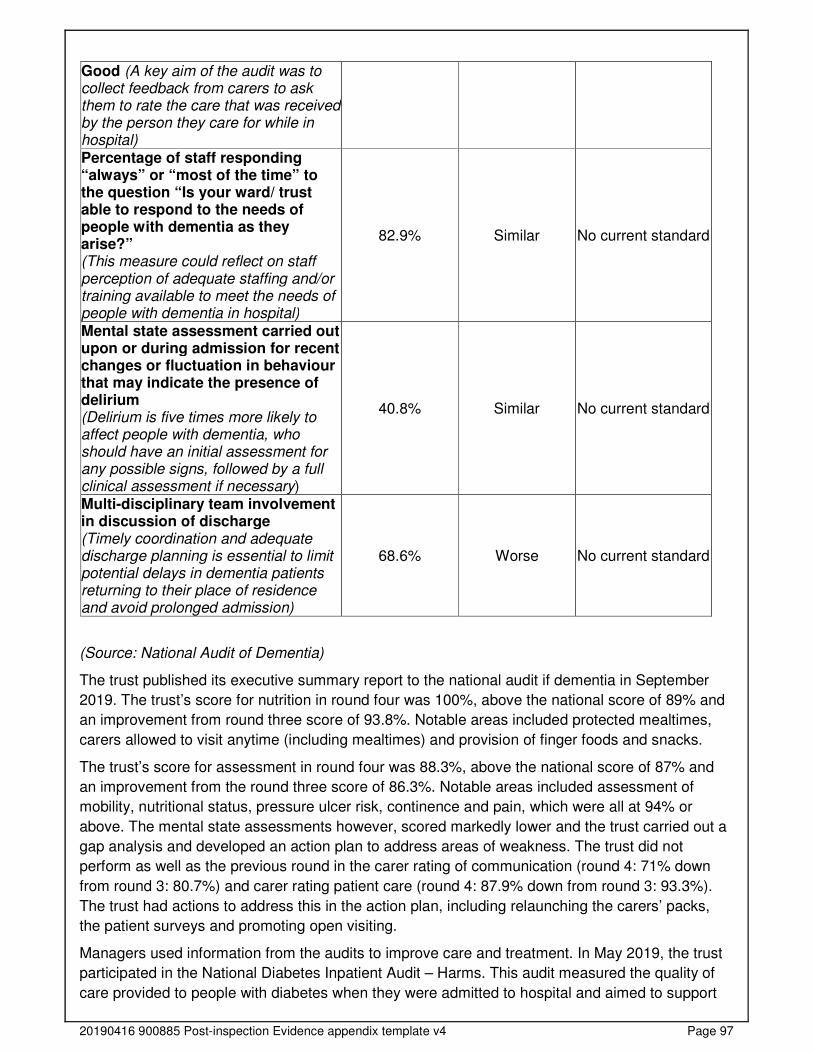
20190416 900885 Post-inspection Evidence appendix template v4 Page 97
Good (A key aim of the audit was to collect feedback from carers to ask them to rate the care that was received by the person they care for while in hospital) Percentage of staff responding “always” or “most of the time” to the question “Is your ward/ trust able to respond to the needs of people with dementia as they arise?” (This measure could reflect on staff perception of adequate staffing and/or training available to meet the needs of people with dementia in hospital)
82.9% Similar No current standard
Mental state assessment carried out upon or during admission for recent changes or fluctuation in behaviour that may indicate the presence of delirium (Delirium is five times more likely to affect people with dementia, who should have an initial assessment for any possible signs, followed by a full clinical assessment if necessary)
40.8% Similar No current standard
Multi-disciplinary team involvement in discussion of discharge (Timely coordination and adequate discharge planning is essential to limit potential delays in dementia patients returning to their place of residence and avoid prolonged admission)
68.6% Worse No current standard
(Source: National Audit of Dementia)
The trust published its executive summary report to the national audit if dementia in September
2019. The trust’s score for nutrition in round four was 100%, above the national score of 89% and
an improvement from round three score of 93.8%. Notable areas included protected mealtimes,
carers allowed to visit anytime (including mealtimes) and provision of finger foods and snacks.
The trust’s score for assessment in round four was 88.3%, above the national score of 87% and
an improvement from the round three score of 86.3%. Notable areas included assessment of
mobility, nutritional status, pressure ulcer risk, continence and pain, which were all at 94% or
above. The mental state assessments however, scored markedly lower and the trust carried out a
gap analysis and developed an action plan to address areas of weakness. The trust did not
perform as well as the previous round in the carer rating of communication (round 4: 71% down
from round 3: 80.7%) and carer rating patient care (round 4: 87.9% down from round 3: 93.3%).
The trust had actions to address this in the action plan, including relaunching the carers’ packs,
the patient surveys and promoting open visiting.
Managers used information from the audits to improve care and treatment. In May 2019, the trust
participated in the National Diabetes Inpatient Audit – Harms. This audit measured the quality of
care provided to people with diabetes when they were admitted to hospital and aimed to support
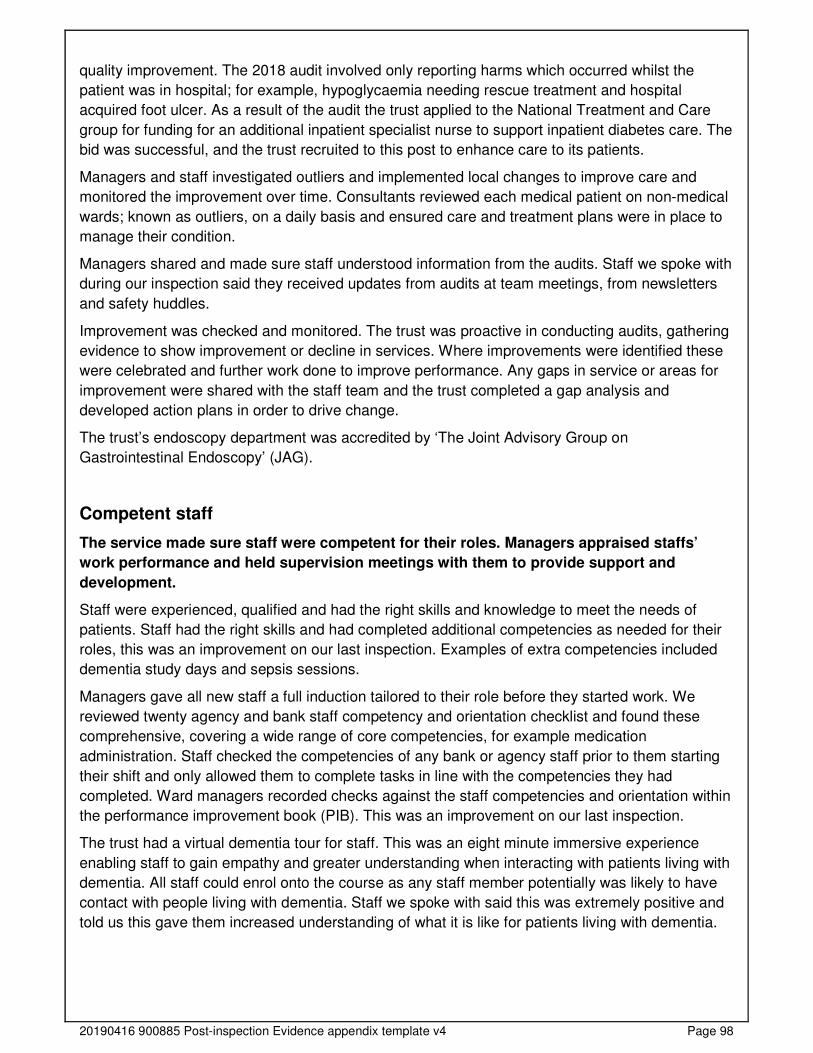
20190416 900885 Post-inspection Evidence appendix template v4 Page 98
quality improvement. The 2018 audit involved only reporting harms which occurred whilst the
patient was in hospital; for example, hypoglycaemia needing rescue treatment and hospital
acquired foot ulcer. As a result of the audit the trust applied to the National Treatment and Care
group for funding for an additional inpatient specialist nurse to support inpatient diabetes care. The
bid was successful, and the trust recruited to this post to enhance care to its patients.
Managers and staff investigated outliers and implemented local changes to improve care and
monitored the improvement over time. Consultants reviewed each medical patient on non-medical
wards; known as outliers, on a daily basis and ensured care and treatment plans were in place to
manage their condition.
Managers shared and made sure staff understood information from the audits. Staff we spoke with
during our inspection said they received updates from audits at team meetings, from newsletters
and safety huddles.
Improvement was checked and monitored. The trust was proactive in conducting audits, gathering
evidence to show improvement or decline in services. Where improvements were identified these
were celebrated and further work done to improve performance. Any gaps in service or areas for
improvement were shared with the staff team and the trust completed a gap analysis and
developed action plans in order to drive change.
The trust’s endoscopy department was accredited by ‘The Joint Advisory Group on
Gastrointestinal Endoscopy’ (JAG).
Competent staff
The service made sure staff were competent for their roles. Managers appraised staffs’
work performance and held supervision meetings with them to provide support and
development.
Staff were experienced, qualified and had the right skills and knowledge to meet the needs of
patients. Staff had the right skills and had completed additional competencies as needed for their
roles, this was an improvement on our last inspection. Examples of extra competencies included
dementia study days and sepsis sessions.
Managers gave all new staff a full induction tailored to their role before they started work. We
reviewed twenty agency and bank staff competency and orientation checklist and found these
comprehensive, covering a wide range of core competencies, for example medication
administration. Staff checked the competencies of any bank or agency staff prior to them starting
their shift and only allowed them to complete tasks in line with the competencies they had
completed. Ward managers recorded checks against the staff competencies and orientation within
the performance improvement book (PIB). This was an improvement on our last inspection.
The trust had a virtual dementia tour for staff. This was an eight minute immersive experience
enabling staff to gain empathy and greater understanding when interacting with patients living with
dementia. All staff could enrol onto the course as any staff member potentially was likely to have
contact with people living with dementia. Staff we spoke with said this was extremely positive and
told us this gave them increased understanding of what it is like for patients living with dementia.
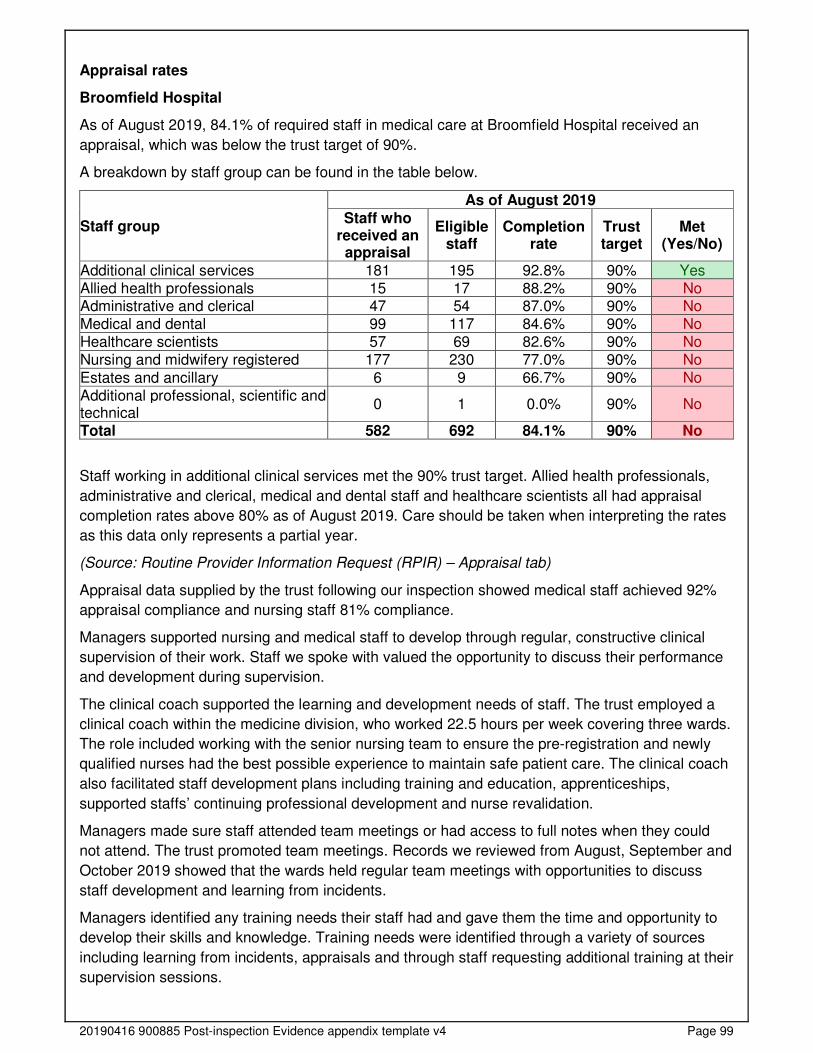
20190416 900885 Post-inspection Evidence appendix template v4 Page 99
Appraisal rates
Broomfield Hospital
As of August 2019, 84.1% of required staff in medical care at Broomfield Hospital received an
appraisal, which was below the trust target of 90%.
A breakdown by staff group can be found in the table below.
Staff group
As of August 2019
Staff who received an appraisal
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Additional clinical services 181 195 92.8% 90% Yes Allied health professionals 15 17 88.2% 90% No Administrative and clerical 47 54 87.0% 90% No Medical and dental 99 117 84.6% 90% No Healthcare scientists 57 69 82.6% 90% No Nursing and midwifery registered 177 230 77.0% 90% No
Estates and ancillary 6 9 66.7% 90% No Additional professional, scientific and technical
0 1 0.0% 90% No
Total 582 692 84.1% 90% No
Staff working in additional clinical services met the 90% trust target. Allied health professionals,
administrative and clerical, medical and dental staff and healthcare scientists all had appraisal
completion rates above 80% as of August 2019. Care should be taken when interpreting the rates
as this data only represents a partial year.
(Source: Routine Provider Information Request (RPIR) – Appraisal tab)
Appraisal data supplied by the trust following our inspection showed medical staff achieved 92%
appraisal compliance and nursing staff 81% compliance.
Managers supported nursing and medical staff to develop through regular, constructive clinical
supervision of their work. Staff we spoke with valued the opportunity to discuss their performance
and development during supervision.
The clinical coach supported the learning and development needs of staff. The trust employed a
clinical coach within the medicine division, who worked 22.5 hours per week covering three wards.
The role included working with the senior nursing team to ensure the pre-registration and newly
qualified nurses had the best possible experience to maintain safe patient care. The clinical coach
also facilitated staff development plans including training and education, apprenticeships,
supported staffs’ continuing professional development and nurse revalidation.
Managers made sure staff attended team meetings or had access to full notes when they could
not attend. The trust promoted team meetings. Records we reviewed from August, September and
October 2019 showed that the wards held regular team meetings with opportunities to discuss
staff development and learning from incidents.
Managers identified any training needs their staff had and gave them the time and opportunity to
develop their skills and knowledge. Training needs were identified through a variety of sources
including learning from incidents, appraisals and through staff requesting additional training at their
supervision sessions.

20190416 900885 Post-inspection Evidence appendix template v4 Page 100
Staff had the opportunity to discuss training needs with their line manager and were supported to
develop their skills and knowledge. Staff we spoke with said they valued their appraisals and
opportunities to discuss their training. Staff told us their line managers were supportive in
developing their skills and that they felt confident in requesting additional training.
Managers made sure staff received any specialist training for their role. Staff who required
specialist training for their role received this in order to carry out their roles, for example additional
dementia training for dementia support workers.
Managers recruited, trained and supported volunteers to support patients in the service.
Throughout the inspection we met dedicated and highly motivated volunteers that were focused on
providing additional support to the patients on the wards. Volunteers went through a strict
induction process and covered key areas of training required for their safety and in order to
understand the needs of patients, for example safeguarding and dementia care.
Multidisciplinary working
Doctors, nurses and other healthcare professionals worked together as a team to benefit
patients. They supported each other to provide good care.
Staff held regular and effective multidisciplinary meetings to discuss patients and improve their
care. We noted the trust held regular multidisciplinary (MDT) ‘red to green bed day’ meetings, with
input from nursing staff, medical staff, allied health professionals, mental health colleagues and
social care staff. Red and green bed days are a visual management system to assist in the
identification of wasted time in a patient’s journey in hospital. Applicable to in-patient wards in both
acute and community settings, this approach is used to reduce internal and external delays as part
of the “SAFER” patient flow bundle.
Staff worked across health care disciplines and with other agencies when required to care for
patients. Staff we spoke with gave numerous positive examples of cross sector working with
district nurses, social care and the clinical commissioning groups (CCGs) in order to care for
patients. A big focus of the MDT was the patient discharge process, this was an improvement from
our last inspection.
Staff referred patients for mental health assessments when they showed signs of mental ill health,
depression. Staff we spoke with during our inspection were aware of the mental health liaison
teams and could provide examples of cases where they referred patients to them.
Patients had their care pathway reviewed by relevant consultants. Consultants conducted daily
ward rounds Monday to Friday. At weekends staff could ask for medical staff to review patients.
Seven-day services
Key services were available seven days a week to support timely patient care.
Consultants led daily ward rounds on all wards. Patients were reviewed by consultants depending
on their care pathway. Consultant services were available seven days a week, out of hours an on-
call consultant was available. Specialist consultants were available on-call for gastrointestinal
bleeds, cardiologist pacing, haematology and microbiology.
20190416 900885 Post-inspection Evidence appendix template v4 Page 101
Consultant ward rounds on the general medicine wards occurred daily Monday to Friday. On
Saturday and Sunday consultants reviewed any new patients, any patients needing to be
discharged and any unstable patients.
Staff could call for support from doctors and other disciplines, including mental health services and
diagnostic tests, 24 hours a day, seven days a week. The pharmacy was open Monday to Friday
8.45am to 5.15pm, and Saturdays and bank holidays 10am to 4pm. Out of hours an on-call
pharmacist was available. Diagnostic tests, for example, CT, MRI and x-rays were available 24
hours a day, seven days a week.
Physiotherapists provided an on call respiratory service seven days a week, via on call out of
hours service.
Health promotion
Staff gave patients practical support and advice to lead healthier lives.
The service had relevant information promoting healthy lifestyles and support on wards/units. On
all the wards we visited we noted information available to guide patients and families on healthy
life styles. Information was available on a range of subjects, which included, but was not limited to,
managing healthy diets, diabetes, mental health and smoking cessation.
Staff assessed each patient’s health when admitted and provided support for any individual needs
to live a healthier lifestyle. Patients were weighed and had a medical history taken on admission to
the ward. Medical history could include information such as smoking and recreational drug use.
The cardiac rehabilitation service gave patients information, knowledge and tools to be able to
make healthier lifestyle choices. The patients were then invited to an eight-week cardiac
rehabilitation course consisting of exercise (individualised to the patient), and education, including
diet, stress management and benefits of exercise.
The alcohol liaison team visited all of the wards to give staff training on how to helpfully discuss
alcohol usage with patients and give leaflets and guidance. The trust had updated its inpatient
nursing booklets to make it easier for staff to assess patient alcohol and tobacco usage. Patients
in the stroke unit and transient ischaemic attack (TIA) clinics were offered verbal and written
advice about smoking, alcohol, diet and exercise.
Consent, Mental Capacity Act and Deprivation of Liberty Safeguards
Staff supported patients to make informed decisions about their care and treatment. They
followed national guidance to gain patients consent. They knew how to support patients
who lacked capacity to make their own decisions or were experiencing mental ill health.
They used measures that limit patients liberty appropriately.
Staff understood how and when to assess whether a patient had the capacity to make decisions
about their care. Staff were familiar with the test for identifying whether patients had mental
capacity to make decisions about their activities of day to day living, care and treatment. Staff
were able to explain factors that could affect capacity, whether capacity was fluctuating or affected
by delirium. Staff handovers had a keen focus on patients who lacked capacity and the decisions
that had been made in the patients best interest. Staff understood least restrictive care planning
and when to seek advice from the dementia specialist nurse or safeguarding team for additional
advice.
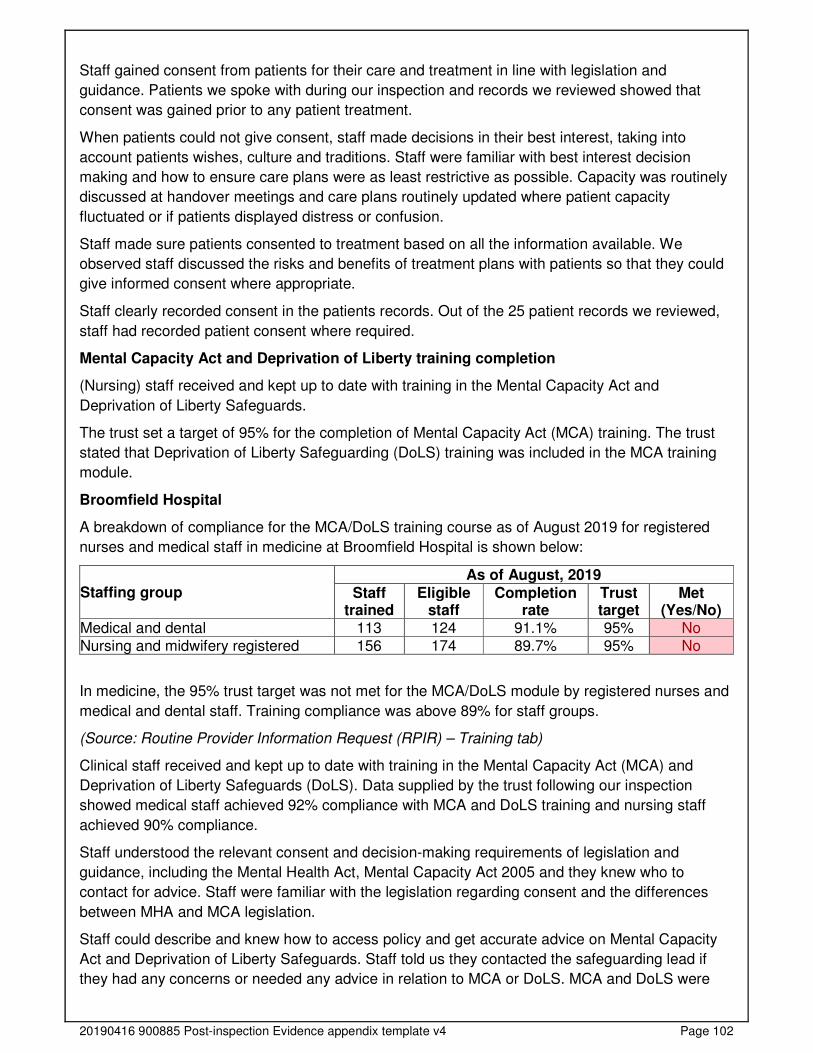
20190416 900885 Post-inspection Evidence appendix template v4 Page 102
Staff gained consent from patients for their care and treatment in line with legislation and
guidance. Patients we spoke with during our inspection and records we reviewed showed that
consent was gained prior to any patient treatment.
When patients could not give consent, staff made decisions in their best interest, taking into
account patients wishes, culture and traditions. Staff were familiar with best interest decision
making and how to ensure care plans were as least restrictive as possible. Capacity was routinely
discussed at handover meetings and care plans routinely updated where patient capacity
fluctuated or if patients displayed distress or confusion.
Staff made sure patients consented to treatment based on all the information available. We
observed staff discussed the risks and benefits of treatment plans with patients so that they could
give informed consent where appropriate.
Staff clearly recorded consent in the patients records. Out of the 25 patient records we reviewed,
staff had recorded patient consent where required.
Mental Capacity Act and Deprivation of Liberty training completion
(Nursing) staff received and kept up to date with training in the Mental Capacity Act and
Deprivation of Liberty Safeguards.
The trust set a target of 95% for the completion of Mental Capacity Act (MCA) training. The trust
stated that Deprivation of Liberty Safeguarding (DoLS) training was included in the MCA training
module.
Broomfield Hospital
A breakdown of compliance for the MCA/DoLS training course as of August 2019 for registered
nurses and medical staff in medicine at Broomfield Hospital is shown below:
Staffing group As of August, 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Medical and dental 113 124 91.1% 95% No Nursing and midwifery registered 156 174 89.7% 95% No
In medicine, the 95% trust target was not met for the MCA/DoLS module by registered nurses and
medical and dental staff. Training compliance was above 89% for staff groups.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Clinical staff received and kept up to date with training in the Mental Capacity Act (MCA) and
Deprivation of Liberty Safeguards (DoLS). Data supplied by the trust following our inspection
showed medical staff achieved 92% compliance with MCA and DoLS training and nursing staff
achieved 90% compliance.
Staff understood the relevant consent and decision-making requirements of legislation and
guidance, including the Mental Health Act, Mental Capacity Act 2005 and they knew who to
contact for advice. Staff were familiar with the legislation regarding consent and the differences
between MHA and MCA legislation.
Staff could describe and knew how to access policy and get accurate advice on Mental Capacity
Act and Deprivation of Liberty Safeguards. Staff told us they contacted the safeguarding lead if
they had any concerns or needed any advice in relation to MCA or DoLS. MCA and DoLS were
20190416 900885 Post-inspection Evidence appendix template v4 Page 103
discussed at all team handovers we observed, and staff had ample opportunity to advocate for
patients to ensure their needs were being met.
Managers monitored the use of Deprivation of Liberty Safeguards and Mental Capacity Act and
made sure staff knew how to complete them. Ward managers knew all patients who were subject
to a DoLS and ensured that applications were completed on time and reviewed where necessary.
Staff implemented Deprivation of Liberty Safeguards in line with approved documentation. We
reviewed MCA and DoLS assessments within patient records and found these were completed
appropriately and used least restrictive care practices.
Is the service caring?
Compassionate care
Staff treated patients with compassion and kindness, respected their privacy and dignity,
and took account of their individual needs.
Staff were discreet and responsive when caring for patients. Staff took time to interact with
patients and those close to them in a respectful and considerate way. Throughout our inspection
we observed positive interactions between staff members and patients and relatives. Staff
knocked on doors before entering toilets, introduced themselves and spoke kindly to patients and
their relatives.
Patients said staff treated them well and with kindness. We spoke with nine patients and other
family members. Eight of the patients gave positive feedback on the service saying that staff
always treated them or their relatives with kindness. One patient stated that the staff had not
followed their exercise plan and they had raised a complaint about this to the service.
Staff followed policy to keep patient care and treatment confidential. Staff understood the
importance of keeping patient care and treatment confidential. However, on one ward we
observed a patient handover at 7.15am that occurred at the end of a patient’s bed, with other
patients present in the bay. Staff told us this was based on feedback from managers who had told
them handover must be done in view of the patient, so they could physically see the patient’s
condition. This had arisen due to a previous safety concern.
We were concerned about the confidentially and privacy of patients in this area as well as all the
patients being woken up at the same time and staff switching all the lights on within the bay. At
one point there were ten staff handing over in the bay, with complex and often confused patients
present. We raised this issue with a senior member of staff, who said they would review the
practice.
On our follow up inspection on 21 November 2019 we again revisited a number of wards to
observe handovers. There had been no change in the handover process following our previous
inspection and the inconsistencies in practice remained.
On other wards handovers took place in side rooms, patients were asleep with lights off and staff
were calmly supporting patients to wake up and prepare for the day. This gave a calm and
reassuring environment for the patients and one that respected the individuality of the patients and
their complex needs.
Staff understood and respected the individual needs of each patient and showed understanding
and a non-judgmental attitude when caring for or discussing patients with mental health needs.
We observed consistently positive interaction between patients and staff, who were non-
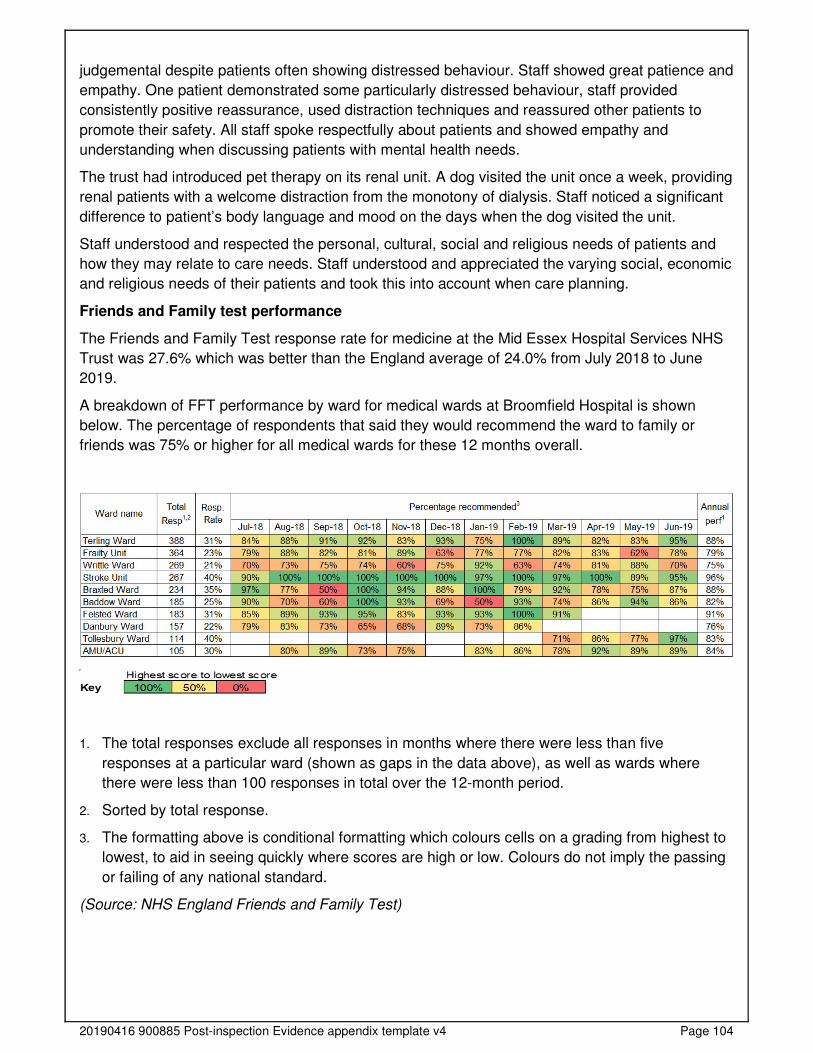
20190416 900885 Post-inspection Evidence appendix template v4 Page 104
judgemental despite patients often showing distressed behaviour. Staff showed great patience and
empathy. One patient demonstrated some particularly distressed behaviour, staff provided
consistently positive reassurance, used distraction techniques and reassured other patients to
promote their safety. All staff spoke respectfully about patients and showed empathy and
understanding when discussing patients with mental health needs.
The trust had introduced pet therapy on its renal unit. A dog visited the unit once a week, providing
renal patients with a welcome distraction from the monotony of dialysis. Staff noticed a significant
difference to patient’s body language and mood on the days when the dog visited the unit.
Staff understood and respected the personal, cultural, social and religious needs of patients and
how they may relate to care needs. Staff understood and appreciated the varying social, economic
and religious needs of their patients and took this into account when care planning.
Friends and Family test performance
The Friends and Family Test response rate for medicine at the Mid Essex Hospital Services NHS
Trust was 27.6% which was better than the England average of 24.0% from July 2018 to June
2019.
A breakdown of FFT performance by ward for medical wards at Broomfield Hospital is shown
below. The percentage of respondents that said they would recommend the ward to family or
friends was 75% or higher for all medical wards for these 12 months overall.
1. The total responses exclude all responses in months where there were less than five
responses at a particular ward (shown as gaps in the data above), as well as wards where
there were less than 100 responses in total over the 12-month period.
2. Sorted by total response.
3. The formatting above is conditional formatting which colours cells on a grading from highest to
lowest, to aid in seeing quickly where scores are high or low. Colours do not imply the passing
or failing of any national standard.
(Source: NHS England Friends and Family Test)
20190416 900885 Post-inspection Evidence appendix template v4 Page 105
Emotional support
Staff provided emotional support to patients, families and carers to minimise their distress.
They understood patients personal, cultural and religious needs.
Staff gave patients and those close to them help, emotional support and advice when they needed
it. Staff provided patients and relatives with emotional support when they needed it. Staff
explained how they helped patients understand their condition and signposted them to
organisations to help them manage their condition. For example, dementia or Parkinson’s self-help
groups. We spoke with one family who said the staff had been exceptionally understanding of their
personal situation. Staff had listened to their concerns and given additional time and care to them
as a family.
Staff supported patients who became distressed in an open environment and helped them
maintain their privacy and dignity. Staff were aware of the importance of maintaining patients
dignity and privacy, especially if they were distressed or confused. We spoke to the night team
who told us a patient with confusion had become upset and removed their clothes. Staff provided
support in a none judgmental way, saying, “That could be my family or a friend, it’s our role to
provide them with care and support, not judge them”.
Staff undertook training on breaking bad news and demonstrated empathy when having difficult
conversations. During our inspection we observed staff discussing the need to speak with patients
and their families regarding end of life care. In staff handovers staff demonstrated great empathy
and understanding for the patients and families, discussing plans in a sensitive and professional
manner. Staff prioritised patients with end of life plans and ensured they spoke to the patients and
families without any additional delays, so they were clear on the choices they could make. We
asked staff how they coped personally with having to have these conversations, they explained
they could always speak to colleagues or their line managers for additional support. On one
occasion we noted one of the medical staff having three of these conversations in the same shift.
They conducted themselves this with the utmost of dignity and professionalism putting the patient
and family needs first.
Staff understood the emotional and social impact that a person’s care, treatment or condition had
on their wellbeing and on those close to them. Staff explained that for many patients the ward was
a strange environment, they tried wherever possible to make it feel homely and encouraged
families to bring in small items form home to help orientate patients to their bed space. During
handover meetings staff routinely discussed the social and emotional impact of the patient’s
condition and how they could plan a discharge appropriate to the patient’s needs.
Understanding and involvement of patients and those close to them
Staff supported patients, families and carers to understand their condition and make
decisions about their care and treatment.
Staff made sure patients and those close to them understood their care and treatment. Patients
we spoke with told us that staff fully involved them in their care. One patient said, “They have been
brilliant, I know exactly what’s going to happen to me next and I am going home soon”. Another
patient said, “There is a routine on here, so the days go quite quickly, the staff tell me everything
they can, and give me time to ask questions”.
Staff talked with patients, families and carers in a way they could understand, using
communication aids where necessary. Staff had access to pictorial symbols to encourage
20190416 900885 Post-inspection Evidence appendix template v4 Page 106
communication with patients who were unable to speak. We observed staff used language that
patients understood and gave patients time to ask questions if they were unsure about anything.
Staff interacting with confused patients showed genuine empathy, gave patients extra time and
reassurance. Staff showed insight into the patient perspective and how it would feel to have a
sensory or physical impairment themselves.
Patients and their families could give feedback on the service and their treatment and staff
supported them to do this. Patients and their relatives provided feedback via the FFT and through
the complaints and compliments procedure. We noted rafts of thank you cards displayed on the
wards we visited. One card said, “Thank you so much for all the care to my dad, you made such a
difference”. Another card said, “Thank you so much for your kindness”.
Staff supported patients to make advanced decisions about their care. Staff we spoke with told us
they spoke to patients and families about the importance of making advanced decisions so that
they could have control over what happened to them. We noted in patient records that advanced
decisions were made about subjects such as resuscitation status and care planning for the future.
Staff supported patients to make informed decisions about their care. Staff spoke openly with
patients about the risks and benefits of procedures and treatment plans, so they could make
informed decisions about their care. We noted where patients lacked capacity that family members
had been involved in decision making and staff had a good understanding of the need to involve
families and those close to the patient in their care.
Is the service responsive?
Service delivery to meet the needs of local people
The service planned and provided care in a way that met the needs of local people and the
communities served. It also worked with others in the wider system and local organisations
to plan care.
Managers planned and organised services, so they met the changing needs of the local
population. Since our last inspection the trust had developed the frailty assessment bay (FAB)
which was a seven-day, multidisciplinary service that included a consultant geriatrician, junior
medical staff, frailty nurses, therapists, a social worker and dedicated dementia support. We
carried out a follow up unannounced inspection on 20 November 2019 and found the trust had
reconfigured the FAB to a standalone unit, no longer attached to the AMU. This was in response
to feedback from staff and service planning to reduce unnecessary patient admissions and focus
on coordinated and efficient discharges.
The service relieved pressure on other departments when they could treat patients in a day. The
aim of FAB was for frail old people to be seen quickly and undergo a comprehensive
multidisciplinary assessment early on in their admission. The team assessed, treated, and
diagnosed patients with a discharge plan, in rapid succession, to avoid admission to the hospital.
Staff knew about and understood the standards for mixed sex accommodation and knew when to
report a potential breach. There were three mixed sex breaches reported in January 2019, within
the discharge lounge. During periods when capacity across the trust and particularly within the
emergency department was challenged to the point that OPEL 3 triggers (The highest level of risk
due to patient capacity and flow through the trust), the trust escalation protocol allowed for
20190416 900885 Post-inspection Evidence appendix template v4 Page 107
decision making that minimised risk to patients. The trust would, at that point, declare a mix sex
breach to maintain patient safety.
Facilities and premises were appropriate for the services being delivered. The facilities and
premises provided adequate accommodation for the services being provided. Some areas of the
hospital were aged, some wards lacked storage space for equipment and there was a lack of
meeting/side rooms for patient activities. The trust was refurbishing one ward to improve these
areas and had additional plans to make similar changes across its existing wards.
Staff could access emergency mental health support 24 hours a day 7 days a week for patients
with mental health problems, learning disabilities and dementia. A mental health team worked on
site, employed by an external provider. The team operated an on-call system and staff from the
mental health team visited the ward for reviews of patients when required.
The service had systems to help care for patients in need of additional support or specialist
intervention. The trust employed dementia support workers on the elderly care wards. The
dementia support workers worked alongside the staff team to provide additional support to
patients living with dementia. They supported the dementia champions to update staff on new
skills and advice on supporting patients and their families. The trust also had access to dementia
specialist nurses, falls specialists, mental health staff and infection prevention and control (IPC)
staff.
Meeting people’s individual needs
The service was inclusive and took account of patients individual needs and preferences.
Staff made reasonable adjustments to help patients access services. They coordinated
care with other services and providers.
Staff made sure patients living with mental health problems, learning disabilities and dementia,
received the necessary care to meet all their needs. Activity boxes containing puzzles, books and
‘twiddlemuffs’ (a hand muff designed to provide sensory stimulation) were put together for patients
living with dementia to assist with agitation or confusion. Staff had purchased reminiscence
therapy in the form of interactive computers which provided additional stimulation to patients living
with dementia.
Staff promoted the use of “serene side rooms”. This process involved staff using a side room, if
one was free, for patients who may be confused or agitated. Staff used aromatherapy, serene
lighting and activity boxes to distract patients and provide a calm environment to reduce anxiety.
Wards were designed to meet the needs of patients living with dementia. Patient ward areas were
colour coded with male and female bays. Each bed had a famous person’s picture or a famous
brand on display above the patient’s bed. This was to encourage the patient to recognise their bed
space and orientate themselves on the ward.
Staff supported patients living with dementia and learning disabilities by using ‘This is me’
documents and patient passports. Staff used patient passports and “This is me” documents to help
staff know more about the patients likes, dislikes past experiences and their medical conditions
and how best to care for them. Often the books were completed by relatives or care home staff
and contained individual details, for example food preferences or particular actions staff could
follow if the patient became distressed.
20190416 900885 Post-inspection Evidence appendix template v4 Page 108
Staff understood and applied the policy on meeting the information and communication needs of
patients with a disability or sensory loss. Staff we spoke with knew how to meet the
communication needs of patients with a disability and where to go for more assistance if
necessary. Staff told us they would speak to the dementia nurse, learning disabilities nurse or
speech and language therapy staff if they were unsure how to communicate with patients.
The service had information leaflets available in languages spoken by the patients and local
community. All leaflets on display in the hospital were printed in English. Staff told us that the trust
could print them in other languages if required but they were not readily displayed or available.
Managers made sure staff, patients, loved ones and carers could get help from interpreters or
signers when needed. Staff could access a translation service for patients whose first language
was not English.
Patients were given a choice of food and drink to meet their cultural and religious preferences. The
service provided menus to patients each day so that they could make food choices that met their
cultural and religious preferences. Staff encouraged patients to actively make choices and be
involved in their menu options.
Staff had access to communication aids to help patients become partners in their care and
treatment. Staff had access to pictorial symbols as an aid to communication with patients who
were unable to speak or were cognitively impaired. The medicine team had developed a game for
patients with called "either, neither or both" to help initiate conversations with patients. Staff
providing one to one care or meaningful time with a patient used this game to enhance
conversation and stimulate dialogue. There was a pocket pack of 100 cards with a choice of two
subjects on the cards that staff used as an aid for conversation and getting to know patients better.
The service had a shared care programme in renal replacement therapies (DIY Dialysis). The
shared care (formerly self-care) programme was non-compulsory. The new programme allowed
patients to gain a better understanding of their chronic condition and a better understanding of
their treatment. Patients who signed up encouraged others to get involved to improve overall
health and well-being and 50 out of the 139 patients eligible had signed up at the time of our
inspection
The red bag scheme was launched within Mid-Essex to identify patients from care homes and to
improve two-way communication for this cohort of patients. The bags were held in the care homes
and when a patient was transferred to an acute trust the red bag was sent with all relevant
paperwork, medication and some personal belongings. The bag stayed with the patient all the way
through their hospital journey and ensured that vital information related to the patients, for
example, do not attempt cardiopulmonary resuscitation status (DNACPR) was shared with all
clinical teams and any updated status returned with the patient on discharge.
The wards had access to the chaplaincy team and faith centre. The chaplaincy team supported
those of all faiths and none and was a key part of providing both pastoral and spiritual support to
the patients and relatives.
Access and flow
People could access the service when they needed it and received the right care promptly.
Waiting times from referral to treatment and arrangements to admit, treat and discharge
patients were in line with national standards.
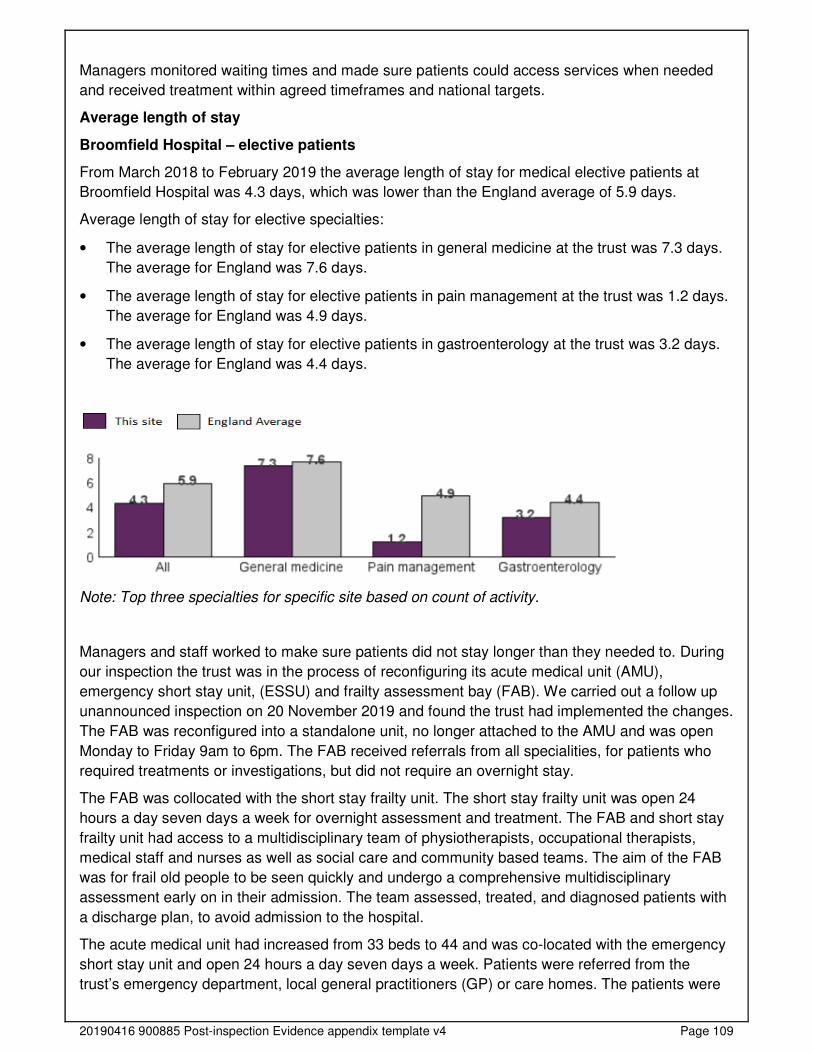
20190416 900885 Post-inspection Evidence appendix template v4 Page 109
Managers monitored waiting times and made sure patients could access services when needed
and received treatment within agreed timeframes and national targets.
Average length of stay
Broomfield Hospital – elective patients
From March 2018 to February 2019 the average length of stay for medical elective patients at
Broomfield Hospital was 4.3 days, which was lower than the England average of 5.9 days.
Average length of stay for elective specialties:
• The average length of stay for elective patients in general medicine at the trust was 7.3 days.
The average for England was 7.6 days.
• The average length of stay for elective patients in pain management at the trust was 1.2 days.
The average for England was 4.9 days.
• The average length of stay for elective patients in gastroenterology at the trust was 3.2 days.
The average for England was 4.4 days.
Note: Top three specialties for specific site based on count of activity.
Managers and staff worked to make sure patients did not stay longer than they needed to. During
our inspection the trust was in the process of reconfiguring its acute medical unit (AMU),
emergency short stay unit, (ESSU) and frailty assessment bay (FAB). We carried out a follow up
unannounced inspection on 20 November 2019 and found the trust had implemented the changes.
The FAB was reconfigured into a standalone unit, no longer attached to the AMU and was open
Monday to Friday 9am to 6pm. The FAB received referrals from all specialities, for patients who
required treatments or investigations, but did not require an overnight stay.
The FAB was collocated with the short stay frailty unit. The short stay frailty unit was open 24
hours a day seven days a week for overnight assessment and treatment. The FAB and short stay
frailty unit had access to a multidisciplinary team of physiotherapists, occupational therapists,
medical staff and nurses as well as social care and community based teams. The aim of the FAB
was for frail old people to be seen quickly and undergo a comprehensive multidisciplinary
assessment early on in their admission. The team assessed, treated, and diagnosed patients with
a discharge plan, to avoid admission to the hospital.
The acute medical unit had increased from 33 beds to 44 and was co-located with the emergency
short stay unit and open 24 hours a day seven days a week. Patients were referred from the
trust’s emergency department, local general practitioners (GP) or care homes. The patients were
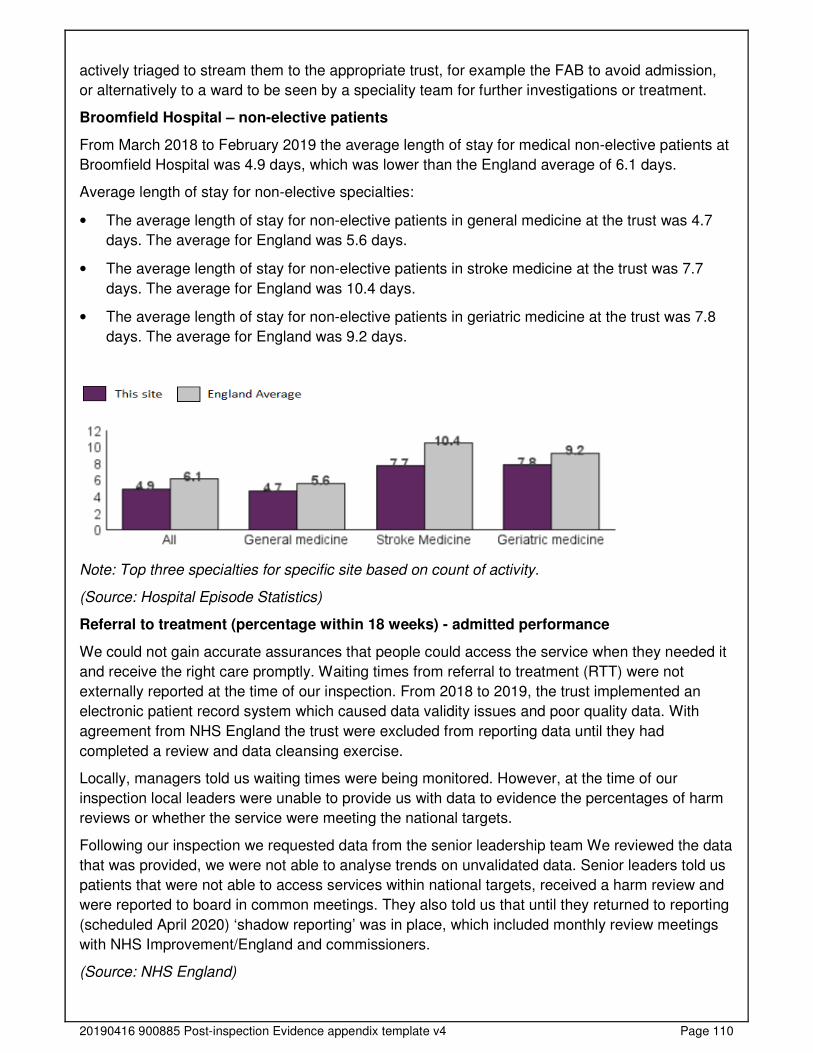
20190416 900885 Post-inspection Evidence appendix template v4 Page 110
actively triaged to stream them to the appropriate trust, for example the FAB to avoid admission,
or alternatively to a ward to be seen by a speciality team for further investigations or treatment.
Broomfield Hospital – non-elective patients
From March 2018 to February 2019 the average length of stay for medical non-elective patients at
Broomfield Hospital was 4.9 days, which was lower than the England average of 6.1 days.
Average length of stay for non-elective specialties:
• The average length of stay for non-elective patients in general medicine at the trust was 4.7
days. The average for England was 5.6 days.
• The average length of stay for non-elective patients in stroke medicine at the trust was 7.7
days. The average for England was 10.4 days.
• The average length of stay for non-elective patients in geriatric medicine at the trust was 7.8
days. The average for England was 9.2 days.
Note: Top three specialties for specific site based on count of activity.
(Source: Hospital Episode Statistics)
Referral to treatment (percentage within 18 weeks) - admitted performance
We could not gain accurate assurances that people could access the service when they needed it
and receive the right care promptly. Waiting times from referral to treatment (RTT) were not
externally reported at the time of our inspection. From 2018 to 2019, the trust implemented an
electronic patient record system which caused data validity issues and poor quality data. With
agreement from NHS England the trust were excluded from reporting data until they had
completed a review and data cleansing exercise.
Locally, managers told us waiting times were being monitored. However, at the time of our
inspection local leaders were unable to provide us with data to evidence the percentages of harm
reviews or whether the service were meeting the national targets.
Following our inspection we requested data from the senior leadership team We reviewed the data
that was provided, we were not able to analyse trends on unvalidated data. Senior leaders told us
patients that were not able to access services within national targets, received a harm review and
were reported to board in common meetings. They also told us that until they returned to reporting
(scheduled April 2020) ‘shadow reporting’ was in place, which included monthly review meetings
with NHS Improvement/England and commissioners.
(Source: NHS England)
20190416 900885 Post-inspection Evidence appendix template v4 Page 111
We asked the trust for additional data against national RTT standards. The trust told us they were
not currently reporting against this standard and therefore not in a position to formally respond to
our additional data requests. The trust has not reported against national 18 week RTT standards
since January 2018.
The decision to discontinue reporting was triggered by the identification of a number of data quality
issues, linked with the implementation of a new Electronic Patient Record (EPR) in May 2017.
Issues identified included migration of data, internal and external reporting, training and
operational processes.
Following the agreement of the trust board, a programme of work was established, with a
dedicated programme management team, reporting through the trust’s elective care group (ECG)
as a sub group of the senior management group (SMG). Key workstreams included validation,
data quality, training, demand and capacity.
From its implementation the programme had been supported by a dedicated resource from the
NHS Improvement Elective Intensive Support Team (IST). Ongoing support was in place (1 day
per week) until the trust returns to reporting. Regular gateway and progress reviews have been
undertaken between the trust and NHS England/Improvement and Clinical Commissioning Group
(CCG) colleagues, with all partners providing assurance of the current position. The latest meeting
was 24 October 2019. This issue was on the medicine risk register and an RTT recovery plan was
in place.
Patient moving wards per admission
The trust stated that the systems they have in place do not differentiate between clinical and non-
clinical reasons for patients moving wards and therefore this data is not recorded.
(Source: Routine Provider Information Request (RPIR) – Ward moves tab)
Patient moving wards at night
Staff did move patients between wards at night. From August 2018 to July 2019, there were 2,936
patients moving wards at night within medicine at Broomfield Hospital. The ward with the highest
number of ward moves at night was the acute medical unit with 2,247. This was followed by the
emergency short stay ward (203 ward moves) and the frailty unit (139 ward moves).
(Source: Routine Provider Information Request (RPIR) – Moves at night tab)
Managers monitored that patient moves between wards/ services were kept to a minimum.
Managers we spoke with were aware of patients being moved between wards at night and that
this could be detrimental to their care. Staff we spoke with told that patients who were very unwell
or nearing the end of their life would not be moved unless absolutely necessary.
At the time of our inspection the trust had implemented a tele tracking system across the three
trusts to embed new ways of working that automated and streamlined essential services in order
to improve patient outcomes.
The system had a shared control centre in Billericay, to aim to improve management of patient
flow across the three trusts. The key objective was to increase bed capacity across the group by
identifying and eliminating ‘idle bed time’ and reducing waste, resulting from structural
inefficiencies in hospital operations and implement a bed management model. Tele tracking
worked closely with each trust to agree improved work flows, reduce waste, and ensure every
patient was assigned the right bed, first time. Clinical and operational teams from each trust were
involved in the design process, ensuring the system was tailored to their pathways and work flows.

20190416 900885 Post-inspection Evidence appendix template v4 Page 112
The real time technology and system detected electronic badges and bracelets worn by patients. It
provided staff with visibility to all beds and patients across the trust. The system provided real time
bed status, patients that need to be allocated to a bed and housekeeping of portering
requirements to support staff to clean a bed or help transport a patient.
Managers and staff worked to make sure that they started discharge planning as early as possible.
Throughout our inspection we found that staff had a strong focus on the patient discharge process,
this was an improvement from our last inspection. All patients were given an expected discharge
date recorded in their notes, staff aimed to hit this date. We noted the trust held ‘red to green bed
day’ meetings, with input from nursing staff, medical staff, allied health professionals, mental
health colleagues and social care. Red and green bed days were a visual management system to
assist in the identification of wasted time in a patient’s journey. Applicable to in-patient wards in
both acute and community settings, this approach was used to reduce internal and external delays
as part of the SAFER patient flow bundle.
The trust held a daily medically fit patient review which took place in the operations centre. The
nurse in charge or patient flow co-ordinator from each ward had an opportunity to meet and get a
two-way update with representatives from the integrated discharge team to ensure all complex
discharge patients had a clear plan. This improved planning around patients and the added benefit
of supporting the education of the clinical teams around discharge pathways and processes
available to the patients.
The system was a key tool within the site status/capacity meetings and utilised to allocate the
elective and non-elective flow into confirmed and pending discharges, as well as further plan for
capacity throughout the day and into the next 24 and 48 hours.
Staff planned patients discharge carefully, particularly for those with complex mental health and
social care needs. Staff ensured that patients were discharged to a safe location and care
packages were in place, if required. Following our last inspection, the trust had trialled the role of a
flow coordinator on three of the wards as part of improving the safer patient flow bundle and safe
discharge. The flow co-ordinators played a pivotal role in supporting the nurse in charge with
planning robust daily patient discharge and acted as a link between the clinical team and the
integrated discharge team. The trust told us that the wards with flow co-ordinators had more
discharges before midday as all processes required were in put into place in a timely manner.
Following the trial, funding had been identified to appoint flow coordinators onto all medical wards.
This was an improvement on our last inspection.
The trust employed a trusted assessor to work with local community care providers and carry out
patient assessments to support the discharge process. This meant that care home staff no longer
needed to come into the hospital and hospital staff could assess patients to ensure the discharge
was safe and the preferred place of care could meet the patient’s needs.
Managers monitored the number of delayed discharges, knew which wards had the highest
number and acted to prevent them. We noted patients on several wards who were waiting for care
packages to be finalised so that they could be safely discharged. ‘Stranded patient’ reviews
happened twice a week, where staff discussed patients who had been admitted for longer than
seven, 14 and 21 days. The reviews led to increased activity with the local clinical commissioning
group (CCG) and social services to ensure these patients had a supportive discharge. The trust
closely motored patient discharge and had assigned additional resources to this area to improve
patient flow and safety. The use of the electronic patient tracking system had improved flow and
enabled staff to identify patients who were ready for discharge and to move patients to the most
appropriate area of the hospital, for their care and discharge planning.
20190416 900885 Post-inspection Evidence appendix template v4 Page 113
Discharge was affected by a number of factors including lack of social care locally, family
decisions, treatment plans changing and patients deteriorating or needing longer in hospital to
prevent an unsafe discharge.
Staff supported patients when they were referred or transferred between services. We observed
that staff explained why patients were being moved between services and accompanied them to
their new ward if needed. Ward administrators worked alongside the teams to ensure patient
records and details went with the patients to minimise any delays in communication of the patient’s
needs.
Managers made sure they had arrangements for medical staff to review any medical patients on
non-medical wards. Consultants reviewed each medical patient on non-medical wards; known as
outliers, on a daily basis and ensured care and treatment plans were in place to manage their
condition.
Managers worked to minimise the number of medical patients on non-medical wards. One of the
functionalities of the tele tracking system was the internal transfer worklist. The list incorporated
internal transfers that were to be moved from one speciality to another, which proactively
supported the movement of the patient into the right speciality bed. Should a patient be in an
outlying speciality ward the system highlighted these patients for ongoing movement.
From the 2nd December 2019 the tele tracking system will show a new “SNAP CAP”. This is a
capacity snap shot report generated from all three NHS trusts that will incorporate the outliers in
beds across all three sites. During our inspection outliers were discussed at every site meeting,
although the trust did not generate a report to view the quantity of outliers.
Learning from complaints and concerns
It was easy for people to give feedback and raise concerns about care received. The
service treated concerns and complaints seriously, investigated them and shared lessons
learned with all staff. The service included patients in the investigation of their complaint.
Summary of complaints
Patients, relatives and carers knew how to complain or raise concerns. Patients and families, we
spoke with confirmed that they knew who to contact if they had a complaint or wanted to raise any
concerns. One patient told us they had been unhappy with their care regime and had made a
complaint to the staff.
The service clearly displayed information about how to raise a concern in patient areas.
Information was displayed on the wards we visited that explained how to make a complaint and
how to contact the complaints team.
Staff understood the policy on complaints and knew how to handle them. Staff we spoke with were
familiar with the trust’s complaints policy and knew how to access it. Staff were confident in
dealing with complaints and escalating them where necessary.
Broomfield Hospital
Managers investigated complaints and identified themes. However, the investigations and
subsequent closure of individual complaints, did not comply with the service target.
From August 2018 to July 2019, the trust received 163 complaints about medicine (27.4% of the
total complaints received by the trust). The trust took an average of 41.3 days to investigate and
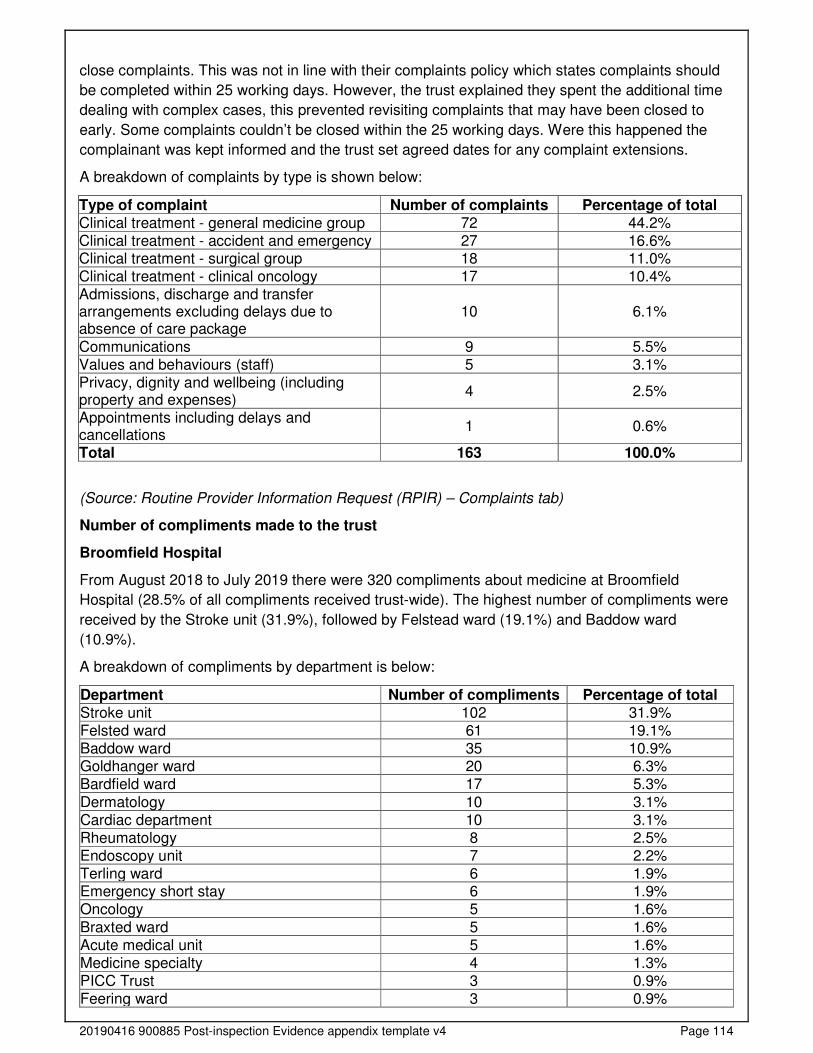
20190416 900885 Post-inspection Evidence appendix template v4 Page 114
close complaints. This was not in line with their complaints policy which states complaints should
be completed within 25 working days. However, the trust explained they spent the additional time
dealing with complex cases, this prevented revisiting complaints that may have been closed to
early. Some complaints couldn’t be closed within the 25 working days. Were this happened the
complainant was kept informed and the trust set agreed dates for any complaint extensions.
A breakdown of complaints by type is shown below:
Type of complaint Number of complaints Percentage of total Clinical treatment - general medicine group 72 44.2% Clinical treatment - accident and emergency 27 16.6% Clinical treatment - surgical group 18 11.0% Clinical treatment - clinical oncology 17 10.4% Admissions, discharge and transfer arrangements excluding delays due to absence of care package
10 6.1%
Communications 9 5.5% Values and behaviours (staff) 5 3.1% Privacy, dignity and wellbeing (including property and expenses)
4 2.5%
Appointments including delays and cancellations
1 0.6%
Total 163 100.0%
(Source: Routine Provider Information Request (RPIR) – Complaints tab)
Number of compliments made to the trust
Broomfield Hospital
From August 2018 to July 2019 there were 320 compliments about medicine at Broomfield
Hospital (28.5% of all compliments received trust-wide). The highest number of compliments were
received by the Stroke unit (31.9%), followed by Felstead ward (19.1%) and Baddow ward
(10.9%).
A breakdown of compliments by department is below:
Department Number of compliments Percentage of total Stroke unit 102 31.9% Felsted ward 61 19.1% Baddow ward 35 10.9% Goldhanger ward 20 6.3% Bardfield ward 17 5.3%
Dermatology 10 3.1% Cardiac department 10 3.1% Rheumatology 8 2.5% Endoscopy unit 7 2.2% Terling ward 6 1.9% Emergency short stay 6 1.9% Oncology 5 1.6%
Braxted ward 5 1.6% Acute medical unit 5 1.6% Medicine specialty 4 1.3% PICC Trust 3 0.9% Feering ward 3 0.9%
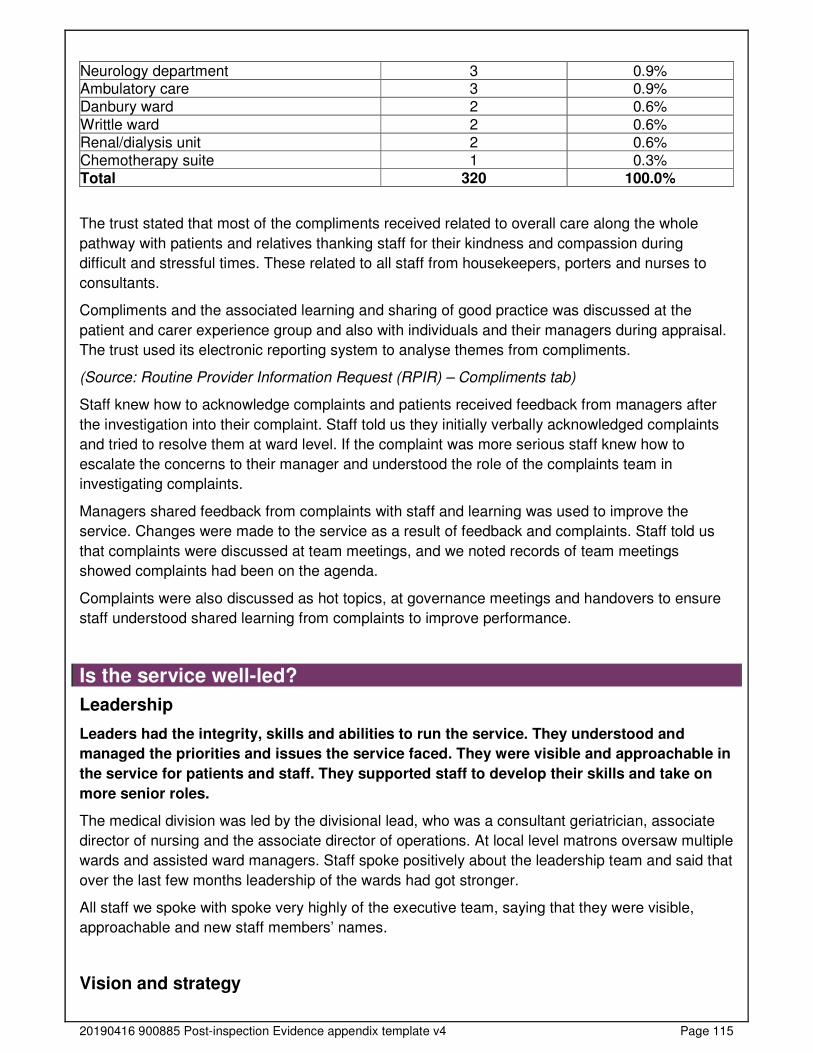
20190416 900885 Post-inspection Evidence appendix template v4 Page 115
Neurology department 3 0.9% Ambulatory care 3 0.9% Danbury ward 2 0.6%
Writtle ward 2 0.6% Renal/dialysis unit 2 0.6% Chemotherapy suite 1 0.3% Total 320 100.0%
The trust stated that most of the compliments received related to overall care along the whole
pathway with patients and relatives thanking staff for their kindness and compassion during
difficult and stressful times. These related to all staff from housekeepers, porters and nurses to
consultants.
Compliments and the associated learning and sharing of good practice was discussed at the
patient and carer experience group and also with individuals and their managers during appraisal.
The trust used its electronic reporting system to analyse themes from compliments.
(Source: Routine Provider Information Request (RPIR) – Compliments tab)
Staff knew how to acknowledge complaints and patients received feedback from managers after
the investigation into their complaint. Staff told us they initially verbally acknowledged complaints
and tried to resolve them at ward level. If the complaint was more serious staff knew how to
escalate the concerns to their manager and understood the role of the complaints team in
investigating complaints.
Managers shared feedback from complaints with staff and learning was used to improve the
service. Changes were made to the service as a result of feedback and complaints. Staff told us
that complaints were discussed at team meetings, and we noted records of team meetings
showed complaints had been on the agenda.
Complaints were also discussed as hot topics, at governance meetings and handovers to ensure
staff understood shared learning from complaints to improve performance.
Is the service well-led?
Leadership
Leaders had the integrity, skills and abilities to run the service. They understood and
managed the priorities and issues the service faced. They were visible and approachable in
the service for patients and staff. They supported staff to develop their skills and take on
more senior roles.
The medical division was led by the divisional lead, who was a consultant geriatrician, associate
director of nursing and the associate director of operations. At local level matrons oversaw multiple
wards and assisted ward managers. Staff spoke positively about the leadership team and said that
over the last few months leadership of the wards had got stronger.
All staff we spoke with spoke very highly of the executive team, saying that they were visible,
approachable and new staff members’ names.
Vision and strategy
20190416 900885 Post-inspection Evidence appendix template v4 Page 116
The service had a vision for what it wanted to achieve and a strategy to turn it into action,
developed with all relevant stakeholders. The vision and strategy were focused on
sustainability of services and aligned to local plans within the wider health economy.
Leaders and staff understood and knew how to apply them and monitor progress.
The trust had a vision that was to be a health care organisation that puts patient care first and
whose reputation for excellence and innovation inspires our patients, staff and the population we
serve. The staff values were based on, “We are a kind, professional positive team”.
The medical wards had their own philosophy of care displayed on each ward. This was a
philosophy that encouraged staff to work towards every day excellence in the service to provide
care to patients.
Throughout our inspection we noted that staff displayed behaviours which met the trust’s vision
and ward philosophies.
All wards displayed their improvement journeys on notice boards. These demonstrated
achievements towards achieving the trust’s vision and improvements.
Culture
All staff we spoke with said that there was a positive culture within the medicine division. Staff felt
supported and cared for and developed strong professional relationships with colleagues.
Staff knew the trust had freedom to speak up guardians but told us they felt able to speak up if
they felt something was wrong, or they felt something was not fair.
There was a culture of mutual respect amongst the multidisciplinary staff teams, with staff
respecting each other professional knowledge and how this could be best used to serve the
patient’s needs.
On all the wards we visited we found staff with positive attitudes, who were welcoming and
friendly, were proud to show us what they did and tell us how they were going to improve. Patients
benefited from a culture where staff were prepared to listen to each other and share ideas to
improve patient care.
Staff handovers were patient focused. We never heard staff on the wards talking about bed
capacity, they focused on the patients and their needs. Staff were focused on safe discharges and
finding the right treatment pathways to enable patients to leave the hospital safely and quickly.
Governance
Leaders operated effective governance processes, throughout the service and with partner
organisations. Staff at all levels were clear about their roles and accountabilities and had
regular opportunities to meet, discuss and learn from the performance of the service.
The trust had effective governance systems in place, this was an improvement from our last
inspection. Each division had a governance meeting monthly which reported into their divisional
board, chaired by the divisional director. The meetings focussed on the overarching finance,
performance, quality and workforce issues for their division. The divisional board informed the
monthly performance and accountability meetings held with the senior leadership team, as well as
the quality meetings held at service level. For example, risk and compliance, patient safety, patient
experience and clinical effectiveness all reported into the site governance forum.
20190416 900885 Post-inspection Evidence appendix template v4 Page 117
Safety and quality were a key part of the board agenda and agreed quality measures, based on
local and national priorities, were reviewed by the board through the integrated performance board
report. With effect from February 2019, following the trust merging with two other NHS trusts they
shared a quality committee across the three sites. This functioned as the trust’s umbrella clinical
governance committee, providing the board with assurance that the trust was delivering a quality
trust against each of the dimensions set out in High Quality Care for All (2008) for all and
enshrined in the Health and Social Care Act 2012.
In order to ensure that the non-executive directors had sufficient opportunity to scrutinise
performance in their respective trust’s, each site had a site governance forum (SGF). The SGF’s
were able to escalate issues to the committees and boards across the three sites on an exception
risk-basis. Patient stories were shared and discussed at Boards and SGF’s, and directors made
site visits to wards for additional assurance on quality and safety.
We reviewed governance meeting minute records from September and October 2019 and found
these to be comprehensive and covered areas of quality linked to performance, including mortality,
training and development, risk and strategy.
Management of risk, issues and performance
Leaders and teams had systems to manage performance. They identified and escalated
relevant risks and issues or identify actions to reduce their impact. They had plans to cope
with unexpected events. Staff contributed to decision-making to help avoid financial
pressures compromising the quality of care.
During our inspection we reviewed the trust’s risk register. The risk register was monitored within
the governance framework and regularly reviewed.
Managers that we spoke with were aware of risks within the medicine service and mitigating
actions to reduce these.
Risks included nurse staffing levels, lack of physical bed space and patient flow through the
hospital. The trust was actively using data and technology to increase flow, maximise on patient
bed space and reduce delayed discharges to improve flow throughout the wards.
The recruitment strategy and appointment of key staff, for example flow coordinators, trusted
assessors and specialist staff for dementia and falls, contributed significantly to responding to risks
across the trust in order to improve patient care.
Staff used data routinely to improve performance. The investment in the patient tele tracking
system meant that staff could use live data to improve performance across the wards and manage
flow to reduce delays and improve patient outcomes.
Audits were routine, staff used data to improve performance and identify any additional risks or
areas that required improvement within the trust.
Information management
The service collected reliable data and analysed it. Staff could find the data they needed, in
easily accessible formats, to understand performance, make decisions and improvements.
The information systems were integrated and secure. Data or notifications were
consistently submitted to external organisations as required.
20190416 900885 Post-inspection Evidence appendix template v4 Page 118
In May 2017, a new electronic patient record system led to problems with accurately tracking
patients and capturing validated accurate referral to treatment (RTT) data. At the time of our
inspection, RTT formal data submission was not taking place (ceased in January 2018 with the
support from NHS England), however, the trust had implemented a number of local measures to
monitor RTT times. All patients who did not meet RTT were reviewed for harm.
The trust intranet provided staff a wealth of up to date policies and guidance to help them plan,
deliver and monitor patient care and outcomes.
Staff were aware of how to use and store confidential information.
The trust used a combination of paper and electronic records for recording patient observations.
Staff also accessed key data from hand held IT tablets that were used to monitor patients
conditions and alert them to any deteriorating patients.
The trust had arrangements in place which ensured data was submitted to external providers as
required for example, serious incidents and never events.
Engagement
Leaders and staff actively and openly engaged with patients, staff, equality groups, the
public and local organisations to plan and manage services. They collaborated with partner
organisations to help improve services for patients.
Staff we spoke with said they could attend a wide range of meetings to participate in engagement
with managers and the senior team.
The 2018 staff survey showed 67% of staff felt supported by their immediate manager and 67% of
staff felt managers were invested in their health and wellbeing, and the hospital took positive
action in this area.
Stakeholders could provide feedback about their experience through the friends and family test
(FFT). The FFT was undertaken through text messaging (SMS) or intelligent voice messaging
(IVM). The trust also used hard copy questionnaires to supplement response rates in care of the
elderly wards.
The trust had a patient experience group with a diverse membership, who provided feedback
through this forum. Patient advice and liaison services (PALS) posters were displayed around the
wards which advised patients on how to give feedback or make a complaint. Patients could also
complete a ‘thank you’ card or feedback via websites, including Care Opinion or NHS Choices as
well as through social media forums.
The trust had a patient council that carried out regular patient surveys where the views and
opinions of patients were canvassed. Patients, relatives, and carers could feedback about their
experience to the local Health Watch.
The trust had a schedule of 'In Your Shoes' patient listening events, this previously included a
listening event for the bereaved. Patients were invited into the trust where they shared their
experience of the care that they had received.
When a patient died, their next of kin were sent a survey where they could give feedback about
theirs and their loved one’s experience.
The trust had a newsletter to share key information to staff.

20190416 900885 Post-inspection Evidence appendix template v4 Page 119
Learning, continuous improvement and innovation
All staff were committed to continually learning and improving services. They had a good
understanding of quality improvement methods and the skills to use them. Leaders
encouraged innovation and participation in research.
The medicine team had developed a game for patients with called "Either, neither or both" to help
initiate conversations with patients. Staff providing one to one care or meaningful time with a
patient used this game to enhanced conversation and stimulate dialogue. There was a pocket
pack of 100 cards with a choice of two subjects on the cards that staff used as an aid for
conversation and getting to know their patients better.
Inspired by the NHS England’s “Sign up to Safety Kitchen Table Events”, the provider’s falls
service took the kitchen table to the wards. Using the idea of a table cloth and having tea, coffee,
biscuits and sweets, staff were invited to take a five minute break and have a chat about the the
trust’s frailty harm awareness document. This was a quick glance guide to assist staff unfamiliar
with clinical frailty to consider tissue viability, medication, bone health, end of life care, falls
interventions, nutrition, delirium, dementia and avoiding deconditioning. The document was
permanently hosted on the trust’s falls intranet page. The mobile kitchen table also promoted the
dangers of deconditioning.
The trust introduced a virtual dementia tour for staff. This was an eight minute immersive
experience enabling staff to gain empathy and greater understanding when interacting with
patients living with dementia. All staff could enrol onto the course as any staff member potentially
could have contact with people living with dementia. Staff we spoke with were extremely positive
and told us this gave them increased understanding of what it was like for patients living with
dementia.
The trust had a consultant clinical champion for medicine medical staffing. A senior consultant met
a minimum of three times a week with the rota co-ordinator for medicine, to review the medical
rotas of all grades of doctors to provide advice and guidance regarding allocation of staff and
cover for rota gaps. The consultant also advised the rota co-ordinator the allocation of junior
doctors across the medical wards and assessed safe minimum medical staffing levels, when there
were staff shortages due to sickness.
Following our last inspection, the trust had trailed the role of a flow coordinator on three of the
wards as part of improving the safer patient flow bundle compliance and safe discharge. The flow
co-ordinators played a pivotal role in supporting the nurse in charge with planning patients
discharge and acted as a link between the clinical team and the integrated discharge team. The
trust told us that the wards with flow co-ordinators had more discharges before midday as all
processes were in place in a timely manner. Following the trial, funding had been identified to
support the introduction of patient flow coordinators onto all medical wards, to work alongside the
clinical teams to deal with all escalations around patient discharge pathways.
The medicine team had developed the role of an assistant infection prevention and control
practitioner to support the wards to deliver a comprehensive infection prevention and control trust.
The post-holder provided a visible presence and was accessible to clinical teams, patients and
trust users. They took an active role within the infection prevention and control trust, providing
support to clinical and non-clinical staff within the trust to help ensure that patients are cared for in
a clean and safe environment.
The trust had a shared care programme in renal replacement therapies (DIY Dialysis). The shared
care (formerly self-care) programme was non-compulsory. The new programme allowed patients
20190416 900885 Post-inspection Evidence appendix template v4 Page 120
to gain a better understanding of their chronic condition and a better understanding of their
treatment. Patients who signed up, encouraged others to get involved, to improve overall health
and well-being and 50 out of the 139 patients eligible had signed up at the time of our inspection
The trust had introduced pet therapy on its renal unit. A dog visited the unit once a week, providing
renal patients with a welcome distraction from the monotony of dialysis. Staff noticed a significant
difference to patient’s body language and mood on the days the dog visited the unit.
The trust’s falls clinical nurse specialist (CNS) and assistant director of nursing, identified that
patients within the stroke unit had a known risk of falling but sat outside of the National Institute
for Health and Care Excellence (NICE) Falls in older people: assessing risk and prevention
(CG 161). This guideline covered assessment of fall risk and interventions to prevent falls in
people aged 65 and over. It aimed to reduce the risk and incidence of falls and associated
distress, pain, injury, loss of confidence, independence and mortality.
In order to address this issue, and promote safety among this patient group, the trust held a
weekly meeting with the matron, senior ward sister, and thrombolysis lead, to review all patients
with this area with a focus on factors contributing to falls. For example, known falls risk, current
mobility, witnessed impulsivity and opportunities to fall. The process was plan, do, study act
(PDSA) assessed and lead to stroke-specific identification of falls risks and individualised
interventions pertinent to this specific client group being implemented.
The red bag scheme was launched within Mid-Essex to identify patients from care homes to
improve two-way communication for this cohort of patients. The bags were held in the care homes
and when a patient was transferred to an acute trust the red bag was sent with all relevant
paperwork, medication and some personal belongings. The bag stayed with the patient all the way
through their journey and ensured that vital information related to the patients, for example, do not
attempt cardiopulmonary resuscitation status (DNACPR) was shared with all clinical teams and
any updated status returned with the patient on discharge.
We noted the trust held ‘red to green bed day’ meetings, with input from nursing staff, medical
staff, allied health professionals, mental health colleagues and social care. Red and green bed
days are a visual management system to assist in the identification of wasted time in a patient’s
journey. It was applicable to in-patient wards in both acute and community settings, this approach
was used to reduce internal and external delays as part of the SAFER patient flow bundle.
The trust held a daily, medically fit patient review, which took place in the operations centre. The
nurse in charge or patient flow co-ordinator from each ward had an opportunity to meet and get a
two-way update with representatives from the integrated discharge team to ensure all complex
discharge patients had a clear plan. This improved planning around patients but and the added
benefit of supporting the education of the clinical teams around discharge pathways and
processes available to the patients.
The trust was piloting a bank staffing ‘app’ designed by the trust to work across organisations and
across care sectors. This innovation differed from other staffing apps by being skills-based and
used the data to identify where skill gaps were, and the likelihood of these shifts being filled. The
pilot has demonstrated that agency spends were reduced and there was an increased shift fill rate
to near 100%.
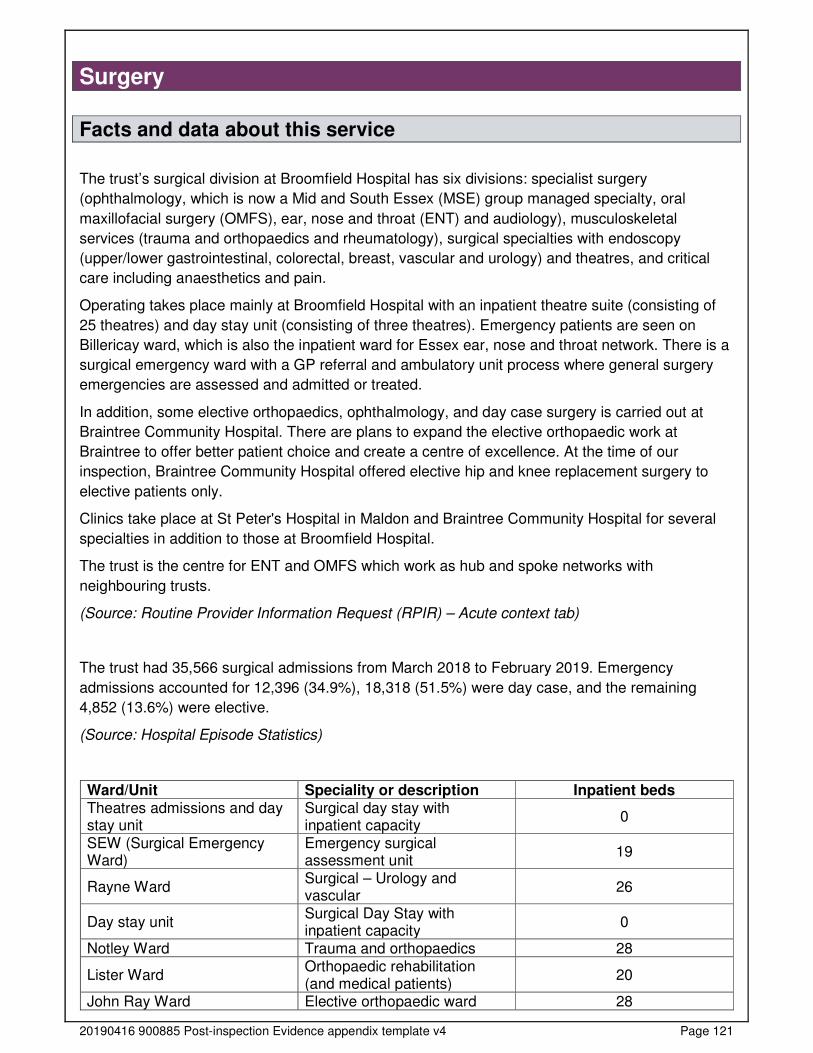
20190416 900885 Post-inspection Evidence appendix template v4 Page 121
Surgery
Facts and data about this service
The trust’s surgical division at Broomfield Hospital has six divisions: specialist surgery
(ophthalmology, which is now a Mid and South Essex (MSE) group managed specialty, oral
maxillofacial surgery (OMFS), ear, nose and throat (ENT) and audiology), musculoskeletal
services (trauma and orthopaedics and rheumatology), surgical specialties with endoscopy
(upper/lower gastrointestinal, colorectal, breast, vascular and urology) and theatres, and critical
care including anaesthetics and pain.
Operating takes place mainly at Broomfield Hospital with an inpatient theatre suite (consisting of
25 theatres) and day stay unit (consisting of three theatres). Emergency patients are seen on
Billericay ward, which is also the inpatient ward for Essex ear, nose and throat network. There is a
surgical emergency ward with a GP referral and ambulatory unit process where general surgery
emergencies are assessed and admitted or treated.
In addition, some elective orthopaedics, ophthalmology, and day case surgery is carried out at
Braintree Community Hospital. There are plans to expand the elective orthopaedic work at
Braintree to offer better patient choice and create a centre of excellence. At the time of our
inspection, Braintree Community Hospital offered elective hip and knee replacement surgery to
elective patients only.
Clinics take place at St Peter's Hospital in Maldon and Braintree Community Hospital for several
specialties in addition to those at Broomfield Hospital.
The trust is the centre for ENT and OMFS which work as hub and spoke networks with
neighbouring trusts.
(Source: Routine Provider Information Request (RPIR) – Acute context tab)
The trust had 35,566 surgical admissions from March 2018 to February 2019. Emergency
admissions accounted for 12,396 (34.9%), 18,318 (51.5%) were day case, and the remaining
4,852 (13.6%) were elective.
(Source: Hospital Episode Statistics)
Ward/Unit Speciality or description Inpatient beds Theatres admissions and day stay unit
Surgical day stay with inpatient capacity
0
SEW (Surgical Emergency Ward)
Emergency surgical assessment unit
19
Rayne Ward Surgical – Urology and vascular
26
Day stay unit Surgical Day Stay with inpatient capacity
0
Notley Ward Trauma and orthopaedics 28
Lister Ward Orthopaedic rehabilitation (and medical patients)
20
John Ray Ward Elective orthopaedic ward 28
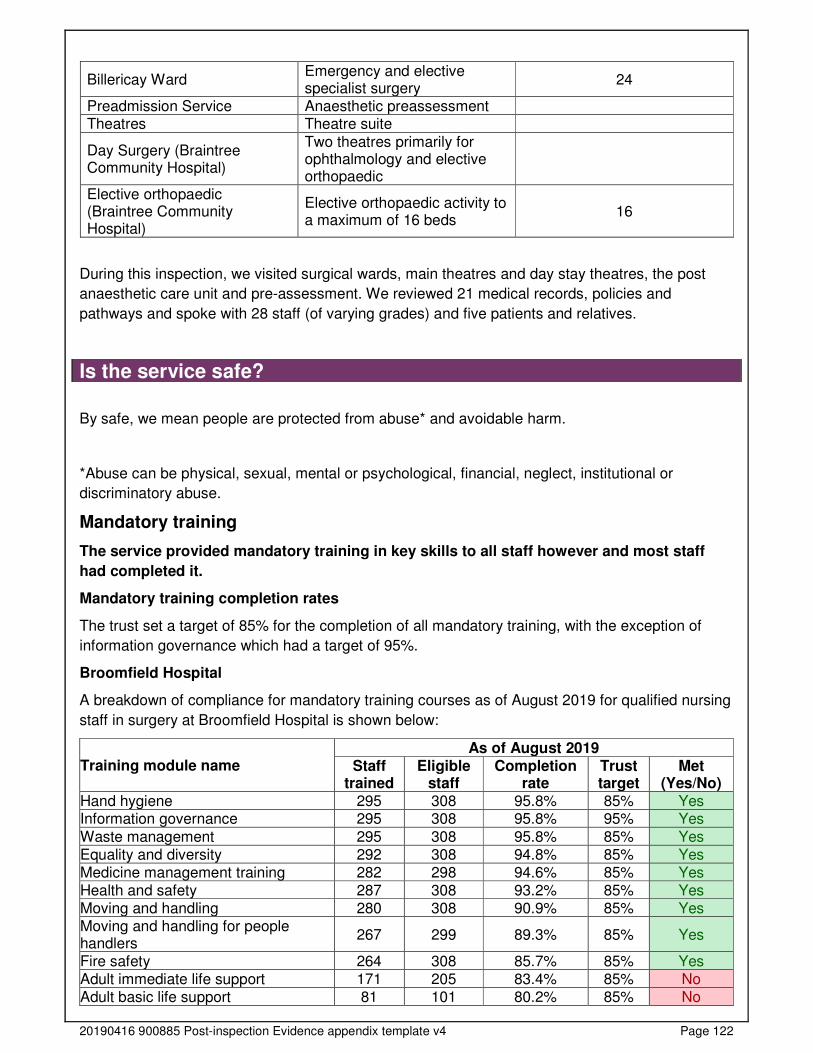
20190416 900885 Post-inspection Evidence appendix template v4 Page 122
Billericay Ward Emergency and elective specialist surgery
24
Preadmission Service Anaesthetic preassessment Theatres Theatre suite
Day Surgery (Braintree Community Hospital)
Two theatres primarily for ophthalmology and elective orthopaedic
Elective orthopaedic (Braintree Community Hospital)
Elective orthopaedic activity to a maximum of 16 beds
16
During this inspection, we visited surgical wards, main theatres and day stay theatres, the post
anaesthetic care unit and pre-assessment. We reviewed 21 medical records, policies and
pathways and spoke with 28 staff (of varying grades) and five patients and relatives.
Is the service safe?
By safe, we mean people are protected from abuse* and avoidable harm.
*Abuse can be physical, sexual, mental or psychological, financial, neglect, institutional or
discriminatory abuse.
Mandatory training
The service provided mandatory training in key skills to all staff however and most staff
had completed it.
Mandatory training completion rates
The trust set a target of 85% for the completion of all mandatory training, with the exception of
information governance which had a target of 95%.
Broomfield Hospital
A breakdown of compliance for mandatory training courses as of August 2019 for qualified nursing
staff in surgery at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Hand hygiene 295 308 95.8% 85% Yes Information governance 295 308 95.8% 95% Yes
Waste management 295 308 95.8% 85% Yes Equality and diversity 292 308 94.8% 85% Yes Medicine management training 282 298 94.6% 85% Yes Health and safety 287 308 93.2% 85% Yes Moving and handling 280 308 90.9% 85% Yes Moving and handling for people handlers
267 299 89.3% 85% Yes
Fire safety 264 308 85.7% 85% Yes Adult immediate life support 171 205 83.4% 85% No Adult basic life support 81 101 80.2% 85% No
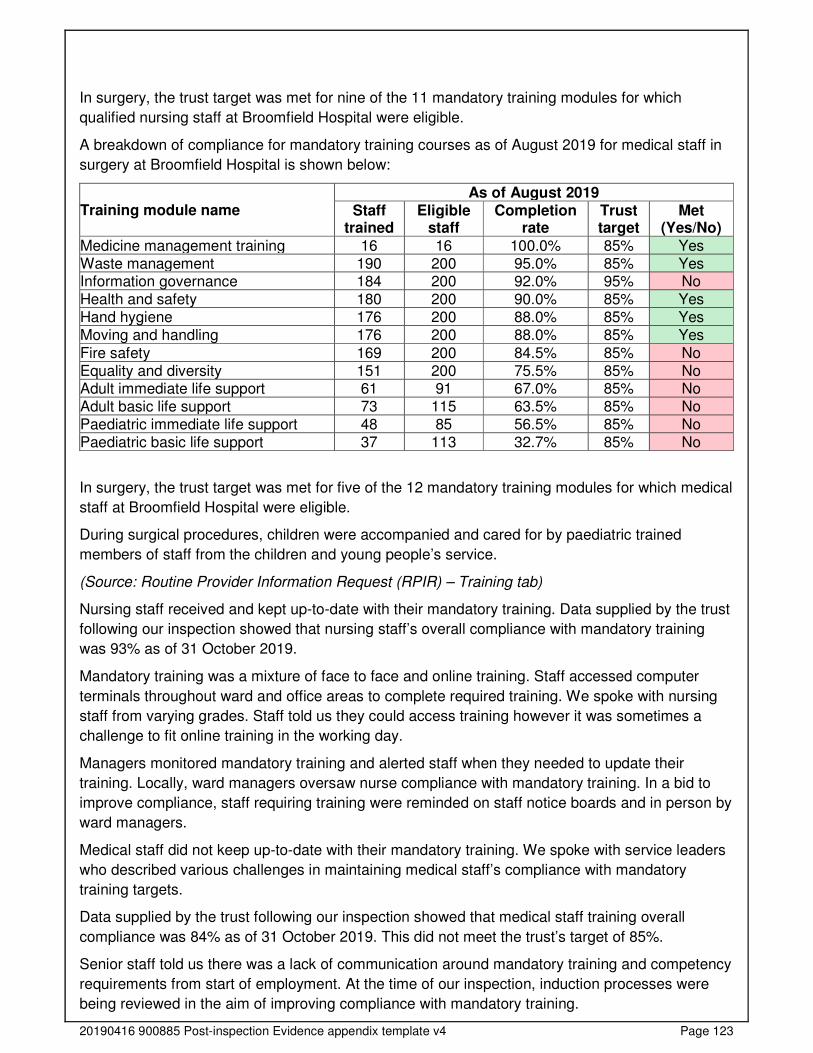
20190416 900885 Post-inspection Evidence appendix template v4 Page 123
In surgery, the trust target was met for nine of the 11 mandatory training modules for which
qualified nursing staff at Broomfield Hospital were eligible.
A breakdown of compliance for mandatory training courses as of August 2019 for medical staff in
surgery at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Medicine management training 16 16 100.0% 85% Yes Waste management 190 200 95.0% 85% Yes Information governance 184 200 92.0% 95% No Health and safety 180 200 90.0% 85% Yes Hand hygiene 176 200 88.0% 85% Yes Moving and handling 176 200 88.0% 85% Yes
Fire safety 169 200 84.5% 85% No Equality and diversity 151 200 75.5% 85% No Adult immediate life support 61 91 67.0% 85% No Adult basic life support 73 115 63.5% 85% No Paediatric immediate life support 48 85 56.5% 85% No Paediatric basic life support 37 113 32.7% 85% No
In surgery, the trust target was met for five of the 12 mandatory training modules for which medical
staff at Broomfield Hospital were eligible.
During surgical procedures, children were accompanied and cared for by paediatric trained
members of staff from the children and young people’s service.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Nursing staff received and kept up-to-date with their mandatory training. Data supplied by the trust
following our inspection showed that nursing staff’s overall compliance with mandatory training
was 93% as of 31 October 2019.
Mandatory training was a mixture of face to face and online training. Staff accessed computer
terminals throughout ward and office areas to complete required training. We spoke with nursing
staff from varying grades. Staff told us they could access training however it was sometimes a
challenge to fit online training in the working day.
Managers monitored mandatory training and alerted staff when they needed to update their
training. Locally, ward managers oversaw nurse compliance with mandatory training. In a bid to
improve compliance, staff requiring training were reminded on staff notice boards and in person by
ward managers.
Medical staff did not keep up-to-date with their mandatory training. We spoke with service leaders
who described various challenges in maintaining medical staff’s compliance with mandatory
training targets.
Data supplied by the trust following our inspection showed that medical staff training overall
compliance was 84% as of 31 October 2019. This did not meet the trust’s target of 85%.
Senior staff told us there was a lack of communication around mandatory training and competency
requirements from start of employment. At the time of our inspection, induction processes were
being reviewed in the aim of improving compliance with mandatory training.
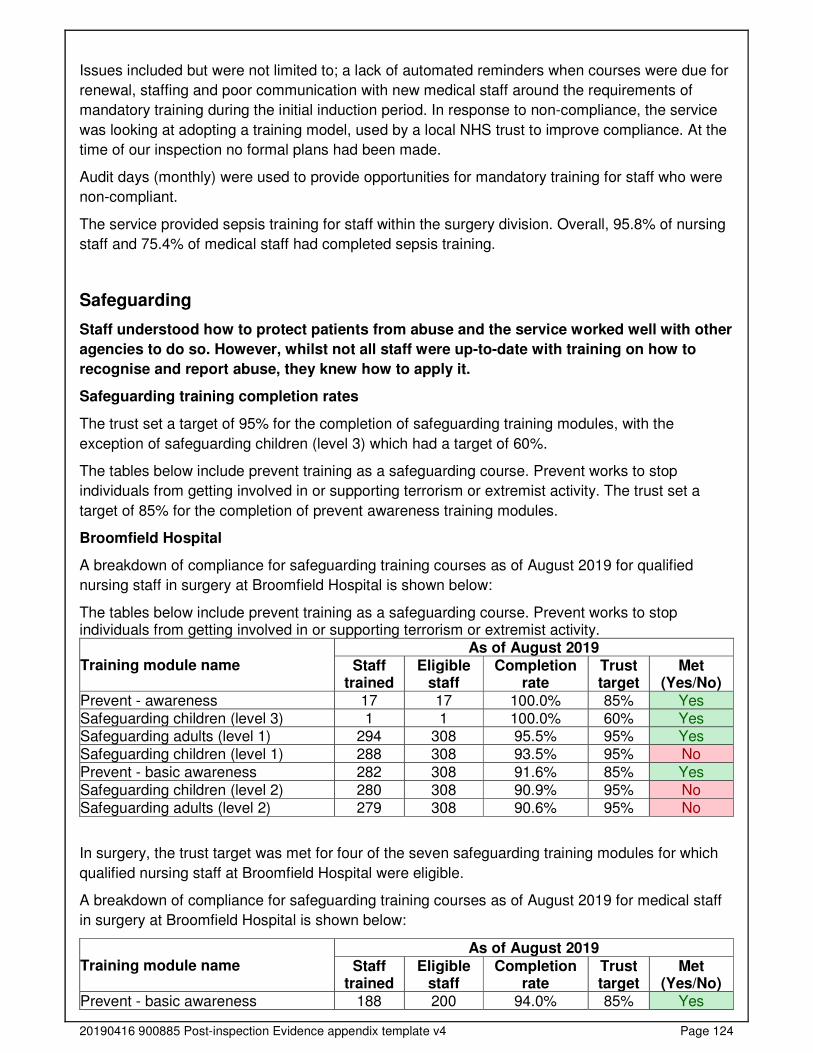
20190416 900885 Post-inspection Evidence appendix template v4 Page 124
Issues included but were not limited to; a lack of automated reminders when courses were due for
renewal, staffing and poor communication with new medical staff around the requirements of
mandatory training during the initial induction period. In response to non-compliance, the service
was looking at adopting a training model, used by a local NHS trust to improve compliance. At the
time of our inspection no formal plans had been made.
Audit days (monthly) were used to provide opportunities for mandatory training for staff who were
non-compliant.
The service provided sepsis training for staff within the surgery division. Overall, 95.8% of nursing
staff and 75.4% of medical staff had completed sepsis training.
Safeguarding
Staff understood how to protect patients from abuse and the service worked well with other
agencies to do so. However, whilst not all staff were up-to-date with training on how to
recognise and report abuse, they knew how to apply it.
Safeguarding training completion rates
The trust set a target of 95% for the completion of safeguarding training modules, with the
exception of safeguarding children (level 3) which had a target of 60%.
The tables below include prevent training as a safeguarding course. Prevent works to stop
individuals from getting involved in or supporting terrorism or extremist activity. The trust set a
target of 85% for the completion of prevent awareness training modules.
Broomfield Hospital
A breakdown of compliance for safeguarding training courses as of August 2019 for qualified
nursing staff in surgery at Broomfield Hospital is shown below:
The tables below include prevent training as a safeguarding course. Prevent works to stop individuals from getting involved in or supporting terrorism or extremist activity.
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Prevent - awareness 17 17 100.0% 85% Yes Safeguarding children (level 3) 1 1 100.0% 60% Yes Safeguarding adults (level 1) 294 308 95.5% 95% Yes Safeguarding children (level 1) 288 308 93.5% 95% No
Prevent - basic awareness 282 308 91.6% 85% Yes Safeguarding children (level 2) 280 308 90.9% 95% No Safeguarding adults (level 2) 279 308 90.6% 95% No
In surgery, the trust target was met for four of the seven safeguarding training modules for which
qualified nursing staff at Broomfield Hospital were eligible.
A breakdown of compliance for safeguarding training courses as of August 2019 for medical staff
in surgery at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Prevent - basic awareness 188 200 94.0% 85% Yes
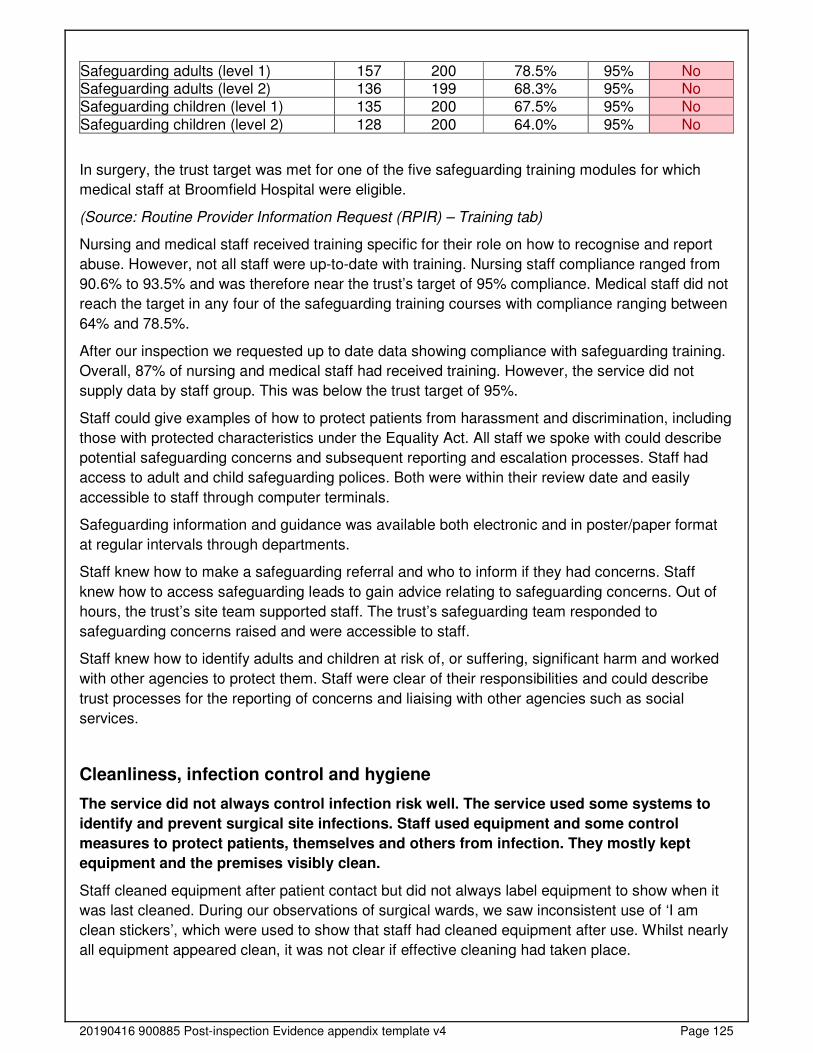
20190416 900885 Post-inspection Evidence appendix template v4 Page 125
Safeguarding adults (level 1) 157 200 78.5% 95% No Safeguarding adults (level 2) 136 199 68.3% 95% No Safeguarding children (level 1) 135 200 67.5% 95% No
Safeguarding children (level 2) 128 200 64.0% 95% No
In surgery, the trust target was met for one of the five safeguarding training modules for which
medical staff at Broomfield Hospital were eligible.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Nursing and medical staff received training specific for their role on how to recognise and report
abuse. However, not all staff were up-to-date with training. Nursing staff compliance ranged from
90.6% to 93.5% and was therefore near the trust’s target of 95% compliance. Medical staff did not
reach the target in any four of the safeguarding training courses with compliance ranging between
64% and 78.5%.
After our inspection we requested up to date data showing compliance with safeguarding training.
Overall, 87% of nursing and medical staff had received training. However, the service did not
supply data by staff group. This was below the trust target of 95%.
Staff could give examples of how to protect patients from harassment and discrimination, including
those with protected characteristics under the Equality Act. All staff we spoke with could describe
potential safeguarding concerns and subsequent reporting and escalation processes. Staff had
access to adult and child safeguarding polices. Both were within their review date and easily
accessible to staff through computer terminals.
Safeguarding information and guidance was available both electronic and in poster/paper format
at regular intervals through departments.
Staff knew how to make a safeguarding referral and who to inform if they had concerns. Staff
knew how to access safeguarding leads to gain advice relating to safeguarding concerns. Out of
hours, the trust’s site team supported staff. The trust’s safeguarding team responded to
safeguarding concerns raised and were accessible to staff.
Staff knew how to identify adults and children at risk of, or suffering, significant harm and worked
with other agencies to protect them. Staff were clear of their responsibilities and could describe
trust processes for the reporting of concerns and liaising with other agencies such as social
services.
Cleanliness, infection control and hygiene
The service did not always control infection risk well. The service used some systems to
identify and prevent surgical site infections. Staff used equipment and some control
measures to protect patients, themselves and others from infection. They mostly kept
equipment and the premises visibly clean.
Staff cleaned equipment after patient contact but did not always label equipment to show when it
was last cleaned. During our observations of surgical wards, we saw inconsistent use of ‘I am
clean stickers’, which were used to show that staff had cleaned equipment after use. Whilst nearly
all equipment appeared clean, it was not clear if effective cleaning had taken place.
20190416 900885 Post-inspection Evidence appendix template v4 Page 126
Steps and parallel bars within the therapy room were marked with ‘I am clean’ stickers. However,
equipment was visibly dusty, sticky in places and had hairs on surfaces. We raised our concerns
to the ward manager who advised they would rectify this issue.
Wards had side rooms for the isolation of patients with known or suspected infectious disease.
Clear signage was in place to restrict access to side rooms in the event of caring for a patient with
an infectious disease.
Staff did not always work effectively to prevent, identify and treat surgical site infections. Theatre
and post anaesthetic care unit staff were provided with gowns to cover surgical scrub clothing
when leaving theatre areas. During our inspection we saw that staff did not always use gowns and
that they were not always properly tied, leading to possible ineffective practices in preventing and
controlling the spread of infection. When we returned at our unannounced inspection, we saw on
six occasions that staff did not have gowns tied correctly and in two cases, we saw staff leaving
theatre areas without gowns in place. We escalated our concerns to the matron for the service.
The matron advised that this had previously been identified as a risk and in response to our raising
of concerns, the service circulated information to staff outlining the importance of gowns to prevent
and spread the risk of infection and placed signage in key areas within the department. However,
staff were still not using gowns as required.
Staff within the theatre department were not fully compliant with the surgical site infection (SSI)
bundle, used to prevent SSI’s. The National Institute for Health and Care Excellence, quality
standard QS49, Quality statement three, recommends the measurement and documenting of core
temperature in accordance with NICE’s guideline on ‘hypothermia: prevention and management in
adults having surgery’. This was also not in line with NICE guideline NG125, maintaining patient
homeostasis.
We raised our concerns at the time of our inspection relating to a lack of documented temperature
taking during surgical procedures. The trust reminded all staff of intraoperative warming guidance,
and complied an action plan to address any identified areas of non-compliance.
After our inspection we requested surgical site infection (SSI) data. In colorectal surgery, from
October 2018 to September 2019, inpatient infection rates ranged from 4.2% to 6.3%. This was
below the national average for all months.
In gastric surgery, from October 2018 to September 2019, inpatient infection rates were between
2.9% and 3.8%. Whilst this was above the England average, it is to be noted that this reflects a
small patient group with one inpatient surgical site infection during this period.
The service monitored SSI rates in orthopaedic services, which included total hip replacements
(THR), total knee replacements (TKR) , fractured neck of femur (NOF) and long bone fractures.
Surgical site infection rates for April 2018 to March 2019 can be seen in the table below:
Orthopaedic service Q1 Q2 Q3 Q4
THR 0% 0% 1.2% 1.5%
TKR 1.1% 1.2% 2.7% 2.7%
NOF 2.2% 2.0% 1.7% 2.2%
Long bone fractures 2.2% 0% 0% 1.5%
The SSI rates detailed above related to one or two patients per quarter.
Theatre changing areas (main theatres) were cramped and contained a lack of effective hanging
space and shoe storage. We raised concerns during our inspection that visibly dirty theatre clogs
20190416 900885 Post-inspection Evidence appendix template v4 Page 127
were in changing areas, mixed with outdoor shoes. Changing rooms also had areas of damaged
flooring. This potentially posed an infection prevention and control risk. Staff told us this point had
been raised but nothing had been done to date to address these concerns. We escalated our
concerns to a matron during our inspection The matron assured us that these concerns would be
addressed.
Pre-admission clinics for planned and elective surgery took place. Patients were screened for
methicillin-resistant staphylococcus aureus (MRSA) at this appointment. MRSA is a specific
bacteria that is resistant to the methicillin group of antibiotics. In the event of a positive result,
patients were offered treatment to further prevent and control the spread of infection.
MRSA screening for elective and non-elective patients was not consistently compliant with the
trust target (95% and above). Data supplied by the service after our inspection demonstrated that
compliance in theatres and anaesthetics from November 2018 to October 2019 varied. The target
was 95% and was not met in six months of this period for non-elective patients and in 10 months
for elective patients. Non-compliance ranged from 85% to 94.4% during this time. For the same
time frame in surgery, the target was not met any month months of this period for non-elective and
elective patients. Results varied from 81% to 93% for this timeframe.
Ward areas were clean and had suitable furnishings which were clean and well-maintained. All
clinical areas (including theatres) were visibility clean and free from dirt. Throughout the course of
our inspection we saw cleaning taking place at regular intervals.
Trolley beds, mattresses and wheelchairs were free from tears to prevent and control the spread
of infection and enable effective cleaning to take place.
However, one blood glucose monitoring box contained clean needles with blood on. We raised our
concerns to the senior nurse in charge who immediately removed this from service and replaced
with clean equipment.
Staff followed infection control principles including the use of personal protective equipment (PPE).
Personal protective equipment (PPE) was available at regular intervals throughout clinical areas.
PPE included, but was not limited to; gloves, masks and aprons. Staff had arms bare below the
elbow to prevent and control the spread of infection.
Hand cleansing gel was available at regular intervals in all areas we visited. Information displaying
the ‘five moments of hand hygiene’ was available for both staff and visitor information. This was in
line with the World Health Organisation (WHO) guidelines on hand hygiene in health care.
However, during our inspection, we saw that not all theatre staff used cleansing hand gel entering
the theatre department. This is not good practice to prevent and control the spread of infection.
The service carried out monthly local audits to assess if effective practices were in place to detect,
prevent and control the spread of infection. Audits covered various areas including, but not limited
to; hand hygiene, decontamination of equipment and urinary catheter care bundle (where
applicable).
Audit data provided after our inspection demonstrated that for October 2019, hand hygiene
compliance was 69% for Heybridge ward, 98% for Rayne ward, 100% for Billericay ward and 73%
for the surgical assessment ward. Staff were individually challenged if noted to be non-compliant
with hand hygiene guidance with local action plans in place to monitor and improve compliance.
Disposable curtains used to separate cubicles and provide privacy were visibly clean, undamaged
and replaced at regular intervals.
20190416 900885 Post-inspection Evidence appendix template v4 Page 128
Equipment was stored above floor level to enable effective cleaning to take place.
Staff could access an infection control policy to provide guidance on preventing and controlling the
spread of infection. In addition, other guidance was in place for safe handling of devices such as
intravenous cannulas (used to administer medicines and fluids). In addition, an infection
prevention and control link nurse was available for advice and support.
Pre-assessment clinics were carried out for all elective (planned) surgical patients where MRSA
screening took place prior to surgery.
Staff complied with the Control of Substances Hazardous to Health Regulations 2002. Cleaning
fluids were securely stored with risk assessments in place. We reviewed risk assessments and
saw all were within their review date and accessible to staff electronically.
Environment and equipment
The design, maintenance and use of facilities and premises kept people safe. Staff
managed clinical waste well. Staff were trained to check equipment however, staff did not
always check equipment in line with service policy and procedures.
Surgical areas and wards were located to minimise transfer times and improve patient access.
Patients could reach call bells and staff responded quickly when called. During our inspection, we
saw that call bells were answered in a timely manner. Patients had call bells within reach.
Staff carried out daily safety checks of specialist equipment. Emergency equipment including
resuscitation trolleys were checked on both a daily and weekly basis, in line with trust policy. We
saw that trolleys in ward areas had been checked on a regular basis since August 2019.
Emergency equipment was well maintained, accessible and tidy meaning staff could gain access
to vital equipment in a timely manner. Emergency equipment was tagged, with corresponding
documentation of tags numbers so staff could be assured equipment was complete and not
tampered with.
In the theatre department, staff completed daily checks on ‘technical check sheets’ to ensure
equipment including anaesthetic machines and resuscitation equipment were safe for use. We
reviewed check sheets from 1 to 6 November 2019 and saw a check had not been completed on 5
November 2019. In another theatre we looked at check sheets for anaesthetic machines. This had
not been completed on the day of our inspection. We raised our concerns with staff who advised
equipment had been checked but not documented.
Within recovery areas, staff had access to emergency resuscitation equipment. We reviewed one
trolley and checklists within recovery and equipment had been checked on a daily basis, in line
with trust policy.
Difficult airway trolleys were located within the theatre department and had been checked on a
regular basis to ensure the availability of equipment. Difficult airways equipment is used when
clinicians require specialist equipment to manage a patient’s airway.
Staff disposed of clinical waste safely. Clinical waste was clearly segregated from domestic waste
in colour coded bags. Sharps (needles) were disposed of in appropriate containers which were
within safe fill limits to prevent needlestick injuries to staff and others.
We reviewed a sample of consumable items from all wards we visited. All consumables were
found to be in date and well organised.
20190416 900885 Post-inspection Evidence appendix template v4 Page 129
Reusable surgical equipment was cleaned and sterilised offsite. We visited the sterile services
department (SSD) and saw equipment was sealed, tidy and well organised, with clear separation
of ‘clean’ and ‘dirty’ areas to prevent cross contamination. Operating equipment was prepared in
advance to ensure availability on the day of surgery.
Surgical equipment was tracked and colour coded, dependent on speciality, This meant in the
event of post-operative complications, equipment could be tracked and examined, should the need
arise.
Trust wide, registers were in place to monitor service requirements of individual pieces of
equipment. We inspected a number of items including defibrillators, blood pressure machines and
electrocardiographs. All demonstrated that service and maintenance had taken place at
recommended intervals.
Fire extinguishers throughout the surgical division were secured to the wall and serviced at
recommended intervals.
Assessing and responding to patient risk
Staff did not always complete and update risk assessments for each patient. However, staff
identified and quickly acted upon patients at risk of deterioration.
Pre-assessment clinics were carried out for all elective (planned) surgical patients. Clinics
assessed patient suitability and health prior to surgical procedures taking place.
Staff used a nationally recognised tool to identify deteriorating patients and escalated them
appropriately. In all records we reviewed, we saw that national early warning scores (NEWS) had
been recorded and acted upon in a timely manner, where applicable.
Staff within interventional radiology (managed by radiology services at the trust) utilised one of the
main theatres. Theatres provided anaesthetic support for patient’s undergoing sedation for
interventional radiology and at the time of our inspection.
Staff knew about and dealt with any specific risk issues. Staff had access to a clinical guideline
named ‘early identification and treatment of sepsis’. The guideline was within review data and
directed staff on actions to take in event of suspected or known sepsis. The guideline contained
sepsis screening and action tools/flowcharts, which we saw were prominently displayed in clinical
areas.
After our inspection we requested up-to-date compliance for sepsis training. The service provided
sepsis training for staff within the surgery division. Overall, 95.8% of nursing staff and 75.4% of
medical staff had completed sepsis training.
It is to be noted that a number of staff groups failed to meet the trust target of 90% including but
not limited to; medical staff (FY2, ST3+ and consultants).
Staff did not always complete risk assessments for each patient on admission / arrival. Staff were
required to complete venous thromboembolism (VTE) risk assessments for all patients. After our
inspection we requested audit data for VTE risk assessment compliance. The national target for
VTE risk assessment completion is 95%. From November 2018 to October 2019, surgery services
did not achieve the 95% target, with compliance ranging from 80.6% to 90.3%. Whilst failing to
meet the target, compliance had risen steadily from March 2019. When reviewing medical
records, we found that four did not contain a venous thromboembolism (VTE) risk assessment
(either paper or electronic). VTE risk assessment compliance was identified as a risk at our last
inspection in October 2018.
20190416 900885 Post-inspection Evidence appendix template v4 Page 130
VTE risk assessments were documented on a hand held electronic device. As the majority of
patient documentation was paper based, staff described the electronic recording of VTE as
disjointed and therefore difficult to achieve compliance with.
The World Health Organisation (WHO) checklist is a tool used in theatres to improve safety of
surgical procedures by bringing together the whole operating team. The checklist is used at
various stages of surgery, including prior to anaesthesia, prior to incision and before staff leave the
operating room.
Staff at the hospital used the WHO checklist for each patient having surgery. During our
inspection, we saw the ‘time out’ section of checks taking place which is used to check patient
identity, the site of surgery and what procedure is planned to take place. During this check, we
noted that the consultant surgeon was not involved in this process. Therefore, we could not gain
assurances that there was a positive safety culture in relation to the WHO checklist. A senior
member of staff described difficulties in ‘getting the consultants and anaesthetists on board’ with
WHO checklist completion. However, there was a focus within the service to improve compliance
with the WHO checklist which was discussed at regular intervals at meetings.
The Local Safety Standards for Invasive Procedures (LocSSIPs) Group oversaw implementation
of the WHO safer surgery checklists. In May 2019 the group requested more assurance with
compliance with the WHO checklist. As a result, an observational audit of theatres and the
endoscopy suite took place. Results demonstrated that in four out of 40 cases a debrief was not
conducted, in seven cases the debrief was conducted without the full attention of staff.
The theatre team carried out monthly self-assessment audits to improve compliance with the WHO
checklist. From April 2019 to September 2019, compliance was 100% for staff carrying out all
elements of the WHO checklist.
The service had 24-hour access to mental health liaison and specialist mental health support. Staff
had access to the 24 hour mental health liaison team in the event that support was required for a
patient. We saw that contact details and advice was available on the trust’s intranet.
Staff completed, or arranged, psychosocial assessments and risk assessments for patients
thought to be at risk of self-harm or suicide. Staff could contact the mental health team and
inpatient documentation contained risk assessments for patient with suspected or known mental
health illness.
Staff did not always share key information to keep patients safe when handing over their care to
others. On occasions, staff told us that patients arrived from the emergency department without a
handover. This meant that receiving staff were not fully aware of incoming patients acuity upon
arrival. Staff explained that whilst there was no evidence of harm to date, this practice led to a
poor patient experience and possible delays when arriving on the ward.
Shift changes and handovers included all necessary key information to keep patients safe.
Handovers were through and included a wide range of staff and other healthcare professionals.
The standard operating procedure for orthopaedic care at Braintree Community Hospital detailed
clear patient escalation in the event of a deteriorating patient, along with eligibility criteria for the
service (for elective patients only).
Nurse staffing
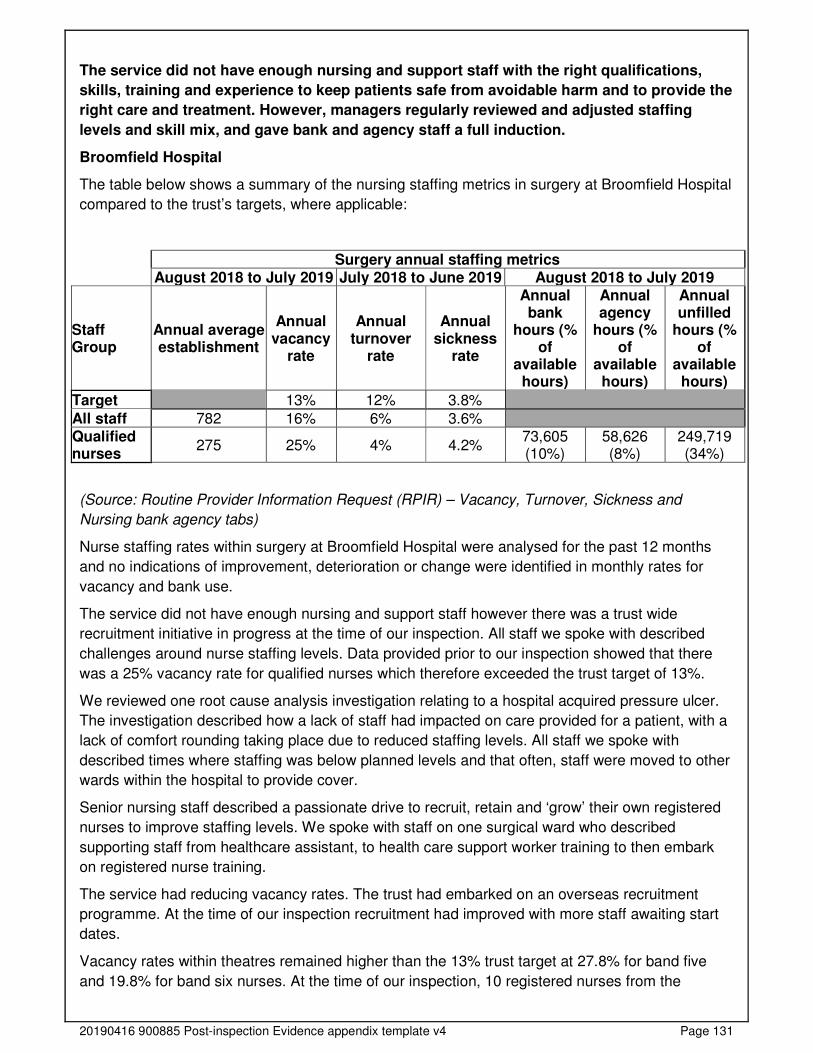
20190416 900885 Post-inspection Evidence appendix template v4 Page 131
The service did not have enough nursing and support staff with the right qualifications,
skills, training and experience to keep patients safe from avoidable harm and to provide the
right care and treatment. However, managers regularly reviewed and adjusted staffing
levels and skill mix, and gave bank and agency staff a full induction.
Broomfield Hospital
The table below shows a summary of the nursing staffing metrics in surgery at Broomfield Hospital
compared to the trust’s targets, where applicable:
Surgery annual staffing metrics August 2018 to July 2019 July 2018 to June 2019 August 2018 to July 2019
Staff Group
Annual average establishment
Annual vacancy
rate
Annual turnover
rate
Annual sickness
rate
Annual bank
hours (% of
available hours)
Annual agency
hours (% of
available hours)
Annual unfilled
hours (% of
available hours)
Target 13% 12% 3.8%
All staff 782 16% 6% 3.6% Qualified nurses
275 25% 4% 4.2% 73,605 (10%)
58,626 (8%)
249,719 (34%)
(Source: Routine Provider Information Request (RPIR) – Vacancy, Turnover, Sickness and
Nursing bank agency tabs)
Nurse staffing rates within surgery at Broomfield Hospital were analysed for the past 12 months
and no indications of improvement, deterioration or change were identified in monthly rates for
vacancy and bank use.
The service did not have enough nursing and support staff however there was a trust wide
recruitment initiative in progress at the time of our inspection. All staff we spoke with described
challenges around nurse staffing levels. Data provided prior to our inspection showed that there
was a 25% vacancy rate for qualified nurses which therefore exceeded the trust target of 13%.
We reviewed one root cause analysis investigation relating to a hospital acquired pressure ulcer.
The investigation described how a lack of staff had impacted on care provided for a patient, with a
lack of comfort rounding taking place due to reduced staffing levels. All staff we spoke with
described times where staffing was below planned levels and that often, staff were moved to other
wards within the hospital to provide cover.
Senior nursing staff described a passionate drive to recruit, retain and ‘grow’ their own registered
nurses to improve staffing levels. We spoke with staff on one surgical ward who described
supporting staff from healthcare assistant, to health care support worker training to then embark
on registered nurse training.
The service had reducing vacancy rates. The trust had embarked on an overseas recruitment
programme. At the time of our inspection recruitment had improved with more staff awaiting start
dates.
Vacancy rates within theatres remained higher than the 13% trust target at 27.8% for band five
and 19.8% for band six nurses. At the time of our inspection, 10 registered nurses from the
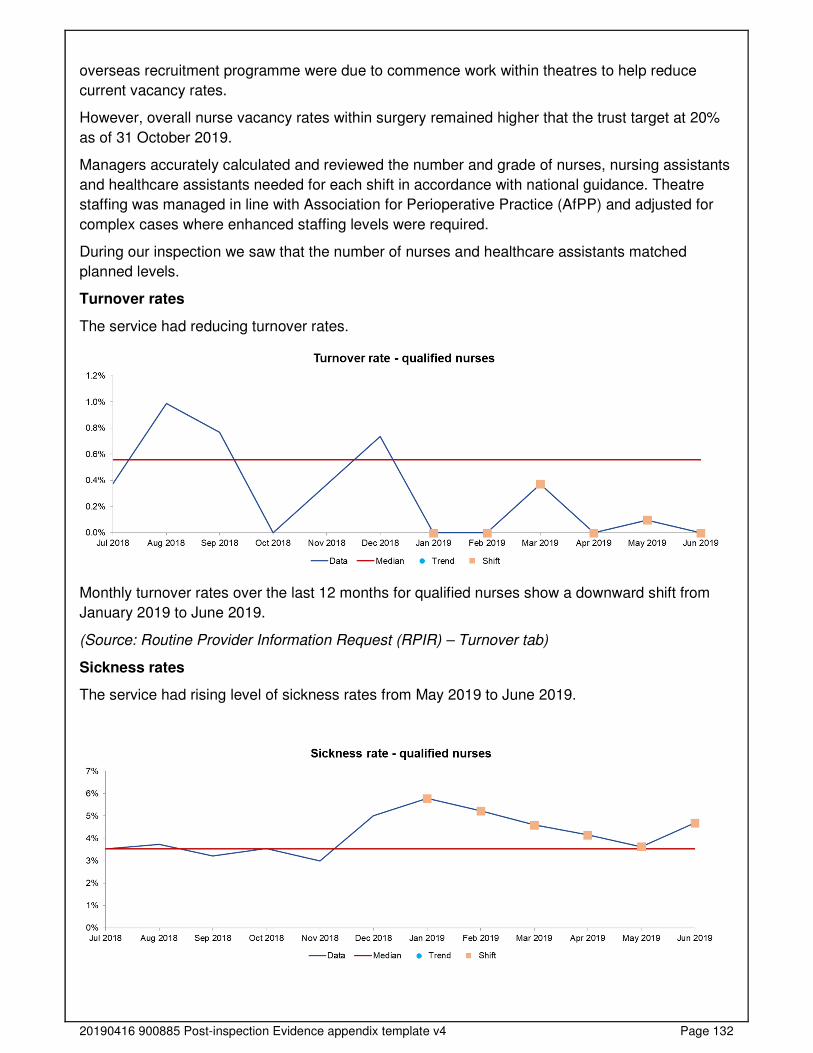
20190416 900885 Post-inspection Evidence appendix template v4 Page 132
overseas recruitment programme were due to commence work within theatres to help reduce
current vacancy rates.
However, overall nurse vacancy rates within surgery remained higher that the trust target at 20%
as of 31 October 2019.
Managers accurately calculated and reviewed the number and grade of nurses, nursing assistants
and healthcare assistants needed for each shift in accordance with national guidance. Theatre
staffing was managed in line with Association for Perioperative Practice (AfPP) and adjusted for
complex cases where enhanced staffing levels were required.
During our inspection we saw that the number of nurses and healthcare assistants matched
planned levels.
Turnover rates
The service had reducing turnover rates.
Monthly turnover rates over the last 12 months for qualified nurses show a downward shift from
January 2019 to June 2019.
(Source: Routine Provider Information Request (RPIR) – Turnover tab)
Sickness rates
The service had rising level of sickness rates from May 2019 to June 2019.
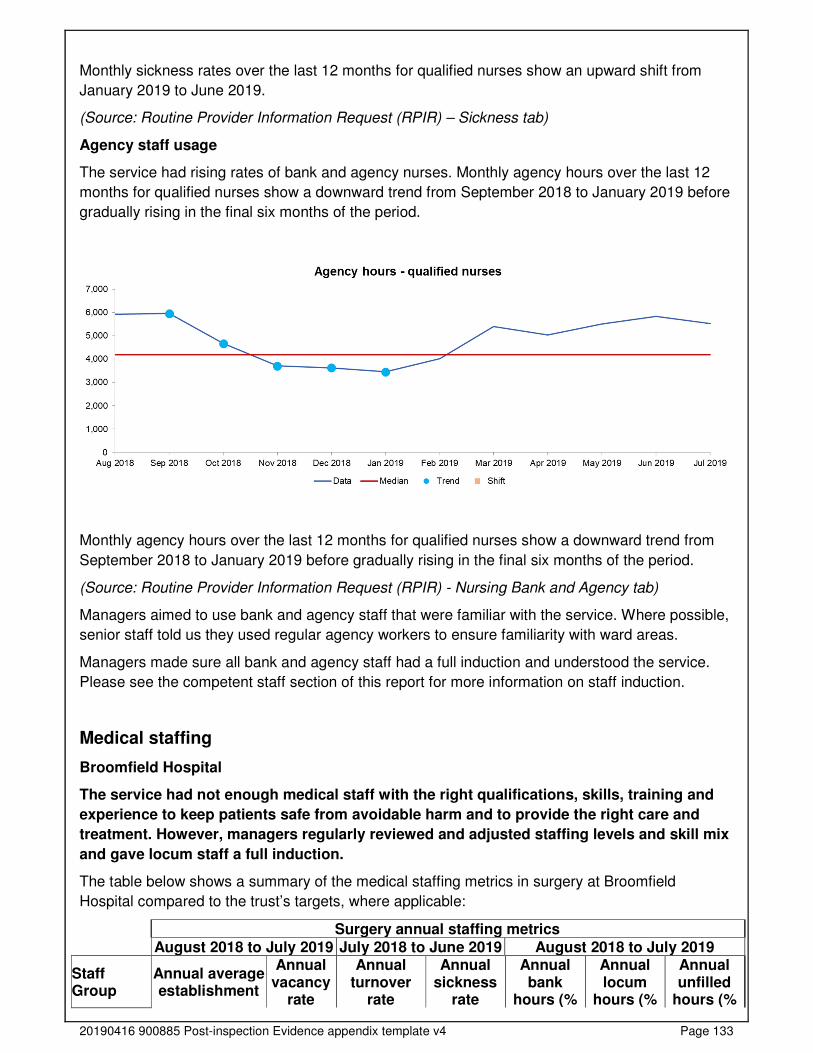
20190416 900885 Post-inspection Evidence appendix template v4 Page 133
Monthly sickness rates over the last 12 months for qualified nurses show an upward shift from
January 2019 to June 2019.
(Source: Routine Provider Information Request (RPIR) – Sickness tab)
Agency staff usage
The service had rising rates of bank and agency nurses. Monthly agency hours over the last 12
months for qualified nurses show a downward trend from September 2018 to January 2019 before
gradually rising in the final six months of the period.
Monthly agency hours over the last 12 months for qualified nurses show a downward trend from
September 2018 to January 2019 before gradually rising in the final six months of the period.
(Source: Routine Provider Information Request (RPIR) - Nursing Bank and Agency tab)
Managers aimed to use bank and agency staff that were familiar with the service. Where possible,
senior staff told us they used regular agency workers to ensure familiarity with ward areas.
Managers made sure all bank and agency staff had a full induction and understood the service.
Please see the competent staff section of this report for more information on staff induction.
Medical staffing
Broomfield Hospital
The service had not enough medical staff with the right qualifications, skills, training and
experience to keep patients safe from avoidable harm and to provide the right care and
treatment. However, managers regularly reviewed and adjusted staffing levels and skill mix
and gave locum staff a full induction.
The table below shows a summary of the medical staffing metrics in surgery at Broomfield
Hospital compared to the trust’s targets, where applicable:
Surgery annual staffing metrics
August 2018 to July 2019 July 2018 to June 2019 August 2018 to July 2019
Staff Group
Annual average establishment
Annual vacancy
rate
Annual turnover
rate
Annual sickness
rate
Annual bank
hours (%
Annual locum
hours (%
Annual unfilled
hours (%
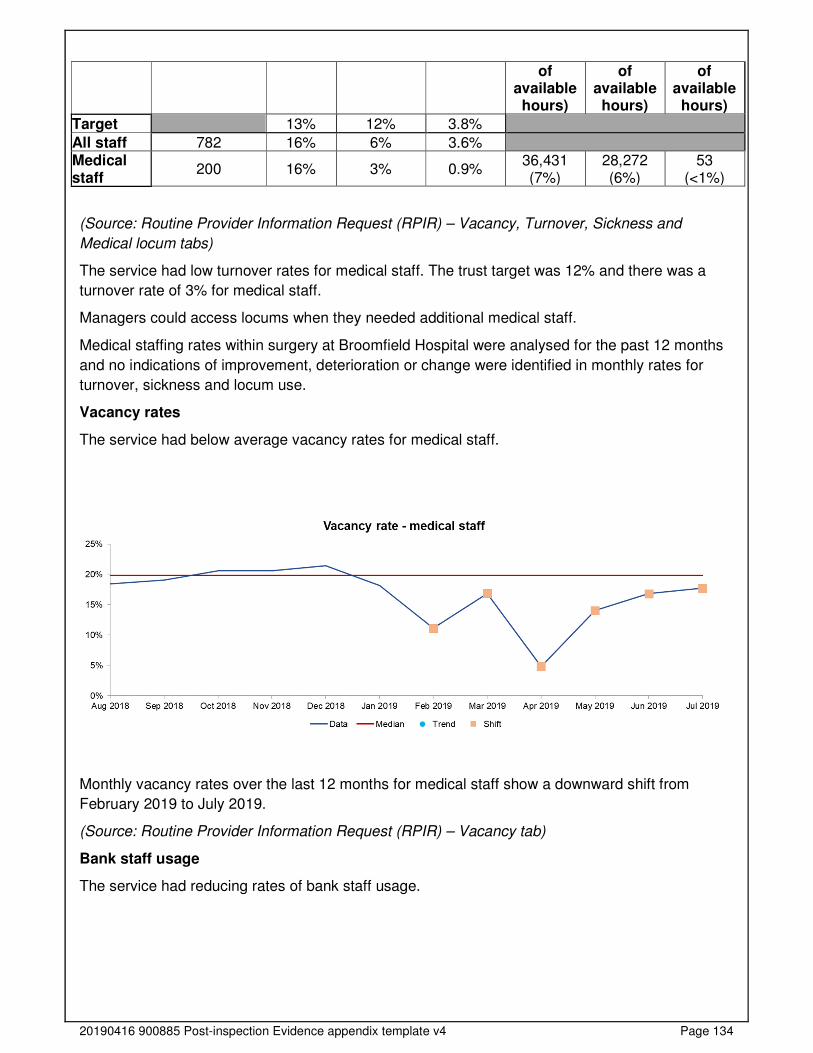
20190416 900885 Post-inspection Evidence appendix template v4 Page 134
of available hours)
of available hours)
of available hours)
Target 13% 12% 3.8%
All staff 782 16% 6% 3.6% Medical staff
200 16% 3% 0.9% 36,431 (7%)
28,272 (6%)
53 (<1%)
(Source: Routine Provider Information Request (RPIR) – Vacancy, Turnover, Sickness and
Medical locum tabs)
The service had low turnover rates for medical staff. The trust target was 12% and there was a
turnover rate of 3% for medical staff.
Managers could access locums when they needed additional medical staff.
Medical staffing rates within surgery at Broomfield Hospital were analysed for the past 12 months
and no indications of improvement, deterioration or change were identified in monthly rates for
turnover, sickness and locum use.
Vacancy rates
The service had below average vacancy rates for medical staff.
Monthly vacancy rates over the last 12 months for medical staff show a downward shift from
February 2019 to July 2019.
(Source: Routine Provider Information Request (RPIR) – Vacancy tab)
Bank staff usage
The service had reducing rates of bank staff usage.
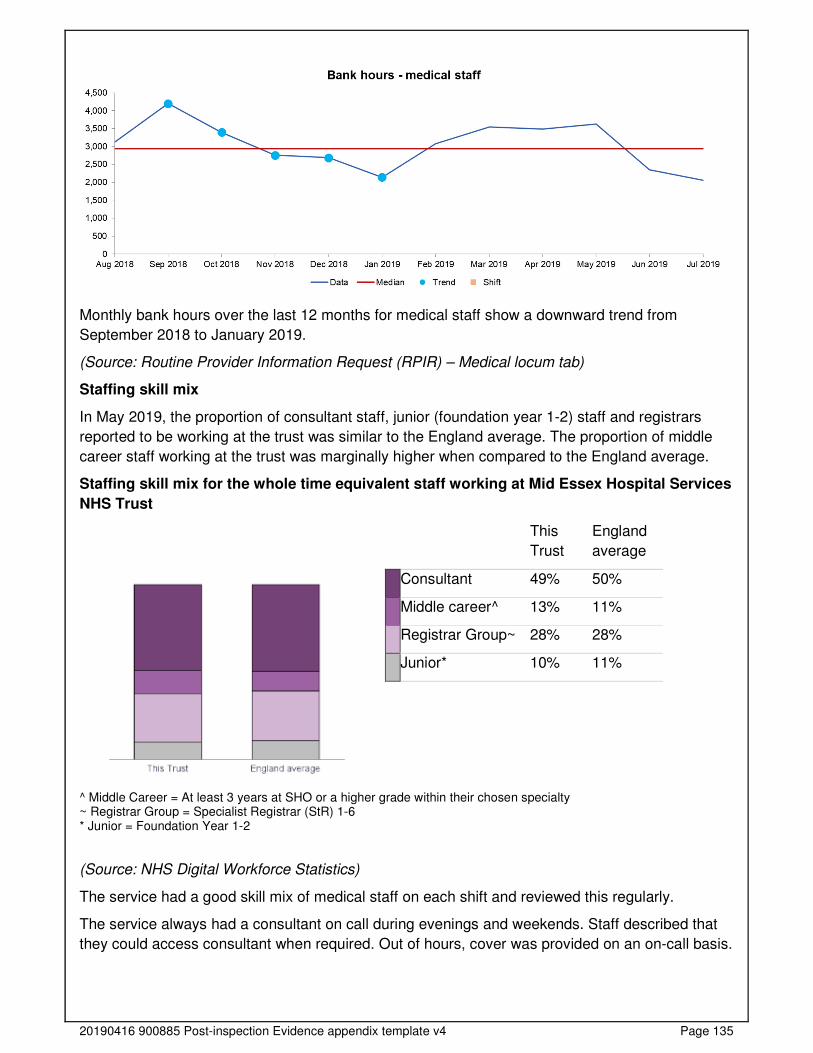
20190416 900885 Post-inspection Evidence appendix template v4 Page 135
Monthly bank hours over the last 12 months for medical staff show a downward trend from
September 2018 to January 2019.
(Source: Routine Provider Information Request (RPIR) – Medical locum tab)
Staffing skill mix
In May 2019, the proportion of consultant staff, junior (foundation year 1-2) staff and registrars
reported to be working at the trust was similar to the England average. The proportion of middle
career staff working at the trust was marginally higher when compared to the England average.
Staffing skill mix for the whole time equivalent staff working at Mid Essex Hospital Services
NHS Trust
This
Trust
England
average
Consultant 49% 50%
Middle career^ 13% 11%
Registrar Group~ 28% 28%
Junior* 10% 11%
^ Middle Career = At least 3 years at SHO or a higher grade within their chosen specialty ~ Registrar Group = Specialist Registrar (StR) 1-6 * Junior = Foundation Year 1-2
(Source: NHS Digital Workforce Statistics)
The service had a good skill mix of medical staff on each shift and reviewed this regularly.
The service always had a consultant on call during evenings and weekends. Staff described that
they could access consultant when required. Out of hours, cover was provided on an on-call basis.
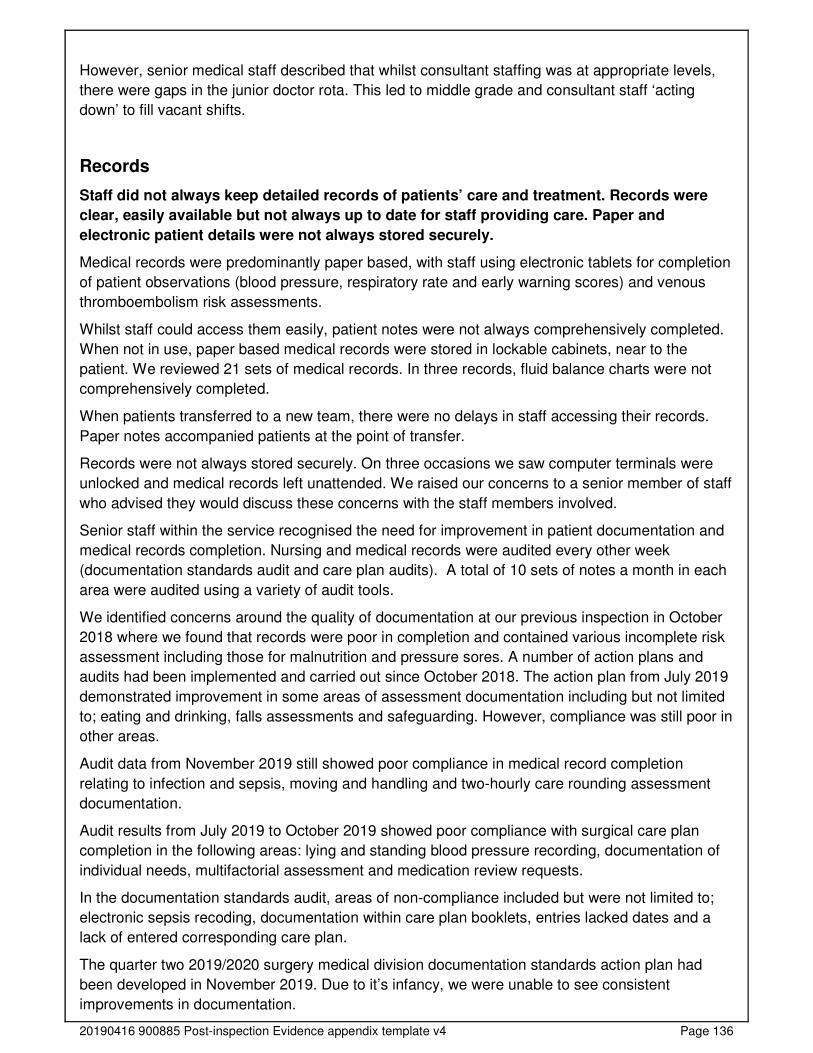
20190416 900885 Post-inspection Evidence appendix template v4 Page 136
However, senior medical staff described that whilst consultant staffing was at appropriate levels,
there were gaps in the junior doctor rota. This led to middle grade and consultant staff ‘acting
down’ to fill vacant shifts.
Records
Staff did not always keep detailed records of patients’ care and treatment. Records were
clear, easily available but not always up to date for staff providing care. Paper and
electronic patient details were not always stored securely.
Medical records were predominantly paper based, with staff using electronic tablets for completion
of patient observations (blood pressure, respiratory rate and early warning scores) and venous
thromboembolism risk assessments.
Whilst staff could access them easily, patient notes were not always comprehensively completed.
When not in use, paper based medical records were stored in lockable cabinets, near to the
patient. We reviewed 21 sets of medical records. In three records, fluid balance charts were not
comprehensively completed.
When patients transferred to a new team, there were no delays in staff accessing their records.
Paper notes accompanied patients at the point of transfer.
Records were not always stored securely. On three occasions we saw computer terminals were
unlocked and medical records left unattended. We raised our concerns to a senior member of staff
who advised they would discuss these concerns with the staff members involved.
Senior staff within the service recognised the need for improvement in patient documentation and
medical records completion. Nursing and medical records were audited every other week
(documentation standards audit and care plan audits). A total of 10 sets of notes a month in each
area were audited using a variety of audit tools.
We identified concerns around the quality of documentation at our previous inspection in October
2018 where we found that records were poor in completion and contained various incomplete risk
assessment including those for malnutrition and pressure sores. A number of action plans and
audits had been implemented and carried out since October 2018. The action plan from July 2019
demonstrated improvement in some areas of assessment documentation including but not limited
to; eating and drinking, falls assessments and safeguarding. However, compliance was still poor in
other areas.
Audit data from November 2019 still showed poor compliance in medical record completion
relating to infection and sepsis, moving and handling and two-hourly care rounding assessment
documentation.
Audit results from July 2019 to October 2019 showed poor compliance with surgical care plan
completion in the following areas: lying and standing blood pressure recording, documentation of
individual needs, multifactorial assessment and medication review requests.
In the documentation standards audit, areas of non-compliance included but were not limited to;
electronic sepsis recoding, documentation within care plan booklets, entries lacked dates and a
lack of entered corresponding care plan.
The quarter two 2019/2020 surgery medical division documentation standards action plan had
been developed in November 2019. Due to it’s infancy, we were unable to see consistent
improvements in documentation.
20190416 900885 Post-inspection Evidence appendix template v4 Page 137
Staff described the process of discharge letter completion. Doctors completed discharge letters
that were then sent to the patient’s GP by the ward clerk. We reviewed one discharge letter and
saw it was comprehensive and sent to the patient’s GP in a timely manner.
Medicines
The service used systems and processes to safely prescribe, administer, record and store
medicines. However, controlled drugs checking systems and processes were not
embedded or carried out in line with trust policy.
Staff followed systems and processes when safely prescribing, administering, recording and
storing medicines.
We reviewed seven prescription cards and saw that documentation was signed/dated, allergies
were documented, non-administrated medicines had a documented reason as to why this was the
case. Antibiotics had been prescribed as per guidelines (where required), writing was legible.
However, in two records, no documented patient weight was present.
Medicines were securely stored and locked in all areas we inspected. Access to drugs was
restricted to authorised personnel only. We reviewed medicines with theatre and on wards and
saw they were well organised and within their expiry dates.
Controlled drugs (CDs) cupboards were secured to walls, had robust locks in place and were
made of metal with strong hinges in line with The Misuse of Drugs Act 1971. Staff checked
controlled drugs in line with national guidance, ensuring two staff members were present at each
check.
We reviewed two months of controlled drugs checks on a surgical ward and saw medicines had
been checked on a daily basis from 1 October 2019 to 7 November 2019 with the exception of one
day.
However, staff did not always store and manage medicines in line with the provider’s medicines
policy. Ward staff described changes to local controlled drug checking processes that required two
CD checks per day. Staff found checking controlled drugs twice a day led to challenges around
compliance, estimating that each check with two members of staff took approximately 40 minutes.
We saw that twice daily checks had not taken place since 1 October 2019 with the exception of
five days within this period. This was not in line with the services controlled drugs policy
(ratification issue date June 2019) which stated: “a complete stock balance check must be
performed twice daily at the commencement of the shift. These checks may be performed with
staff from separate shifts i.e. night shift to early shift’.
Controlled drugs within the recovery area had been checked on a regular basis. In addition,
fridges within this area had daily checks carried out to maintain and ensure the integrity of
medicines stored within this area.
Medicines fridges on wards were checked on a daily basis in line with trust policy. If temperatures
were noted to be out of range, staff took appropriate action and notified pharmacy to ensure
medicines were safe for use. We saw evidence of escalation where fridges had been out of normal
range.
Intravenous fluid warming cabinets within the theatre department were maintained at
recommended temperatures and checked on a regular basis.
Medicines used within theatre were labelled and stored safely.
20190416 900885 Post-inspection Evidence appendix template v4 Page 138
Staff reviewed patients' medicines regularly and provided specific advice to patients and carers
about their medicines. We saw medicine reviews taking place during our inspection and patients
told us that they understood why medicines were prescribed and how to take them upon discharge
if applicable.
Staff followed current national practice to check patients had the correct medicines. Each ward
had access to a pharmacist who visited on a regular basis.
The service had systems to ensure staff knew about safety alerts and incidents, so patients
received their medicines safely.
Staff within theatres described occasions where some medicines were not available. In response
to concerns, they were exploring the possibility of having a dedicated pharmacy technician to help
with this issue. Main theatres had a named pharmacist to provide support where required.
Incidents
The service managed patient safety incidents well. Staff recognised and reported incidents
and near misses. Managers investigated incidents and shared lessons learned with the
whole team and the wider service.
When things went wrong, staff apologised and gave patients honest information and suitable
support. Managers ensured that actions from patient safety alerts were implemented and
monitored.
Never Events
Broomfield Hospital
Never events are serious patient safety incidents that should not happen if healthcare providers
follow national guidance on how to prevent them. Each never event type has the potential to cause
serious patient harm or death but neither need have happened for an incident to be a never event.
From August 2018 to August 2019, the trust reported two incidents that were classified as never
events in surgery. Both occurred at Broomfield Hospital.
One never event occurred in February 2019 and involved a wrong site block and the other
occurred in April 2019 due to a misplaced naso or orogastric tube.
(Source: Strategic Executive Information System (STEIS))
Breakdown of serious incidents reported to STEIS
Broomfield Hospital
In accordance with the Serious Incident Framework 2015, the trust reported 26 serious incidents
(SIs) in surgery which met the reporting criteria set by NHS England from August 2018 to August
2019. All of the incidents reported within surgery occurred at Broomfield Hospital and represented
20.5% of all serious incidents reported by the trust as a whole.
A breakdown of the incident types reported is shown in the table below:
Incident type Number of incidents Percentage of total Surgical/invasive procedure incident meeting SI criteria
9 34.6%
Pressure ulcer meeting SI criteria 4 15.4% Slips/trips/falls meeting SI criteria 3 11.5%

20190416 900885 Post-inspection Evidence appendix template v4 Page 139
VTE meeting SI criteria 3 11.5% HCAI/Infection control incident meeting SI criteria 2 7.7% Abuse/alleged abuse of adult patient by staff 1 3.8%
Substance misuse whilst inpatient meeting SI criteria
1 3.8%
Pending review (a category must be selected before incident is closed)
1 3.8%
Treatment delay meeting SI criteria 1 3.8% Diagnostic incident including delay meeting SI criteria (including failure to act on test results)
1 3.8%
Total 26 100.0%
(Source: Strategic Executive Information System (STEIS))
Staff knew what incidents to report and how to report them. All staff we spoke with could give
examples of potential incidents and describe the electronic incident reporting system in use. Staff
described a culture of feeling able to raise concerns when things went wrong and give examples of
learning from incidents where practice had changed.
Staff raised concerns and reported incidents and near misses in line with trust policy. We reviewed
a number of electronic incident reports and saw they had been reported and acted upon in a timely
manner.
Staff reported serious incidents clearly and in line with trust policy.
The service had identified non-compliance with venous thromboembolism (VTE) risk assessment
completion. From August 2018 to August 2019, the service had three serious incidents relating to
VTE’s. In response to concerns, there was a drive on VTE risk assessment awareness and regular
audits taking place. In addition, a video around VTE was produced by intensive care unit staff
outlining medication safety in response to previous serious incidents.
The service had two never events (from August 2018 to August 2019). Never events are serious
patient safety incidents that should not happen if healthcare providers follow national guidance on
how to prevent them. Each never event type has the potential to cause serious patient harm or
death but neither need have happened for an incident to be a never event. One never event
occurred in February 2019 and involved a wrong site block and the other occurred in April 2019
due to a misplaced naso or orogastric tube. Staff confirmed they were aware of never events and
could describe processes in place to prevent re-occurrence.
Theatre staff had introduced the ‘10,000 feet initiative’. This is based upon a safety initiative from
the airline industry where the aim was to reduce distractions and noise for pilots (used by another
healthcare provider within England). Surgeons called ’10,000 feet’ if they felt the environment was
noisy or distracting in the aim of reducing serious incidents within surgery.
Staff understood the duty of candour. They were open and transparent and gave patients and
families a full explanation if and when things went wrong. The duty of candour is a regulatory duty
that relates to openness and transparency and requires providers of health and social care
services to notify patients (or other relevant persons) of ‘certain notifiable safety incidents’ and
provide reasonable support to that person. Staff could describe the meaning of the duty of candour
and gave examples of when this had been used.
Managers debriefed and supported staff after any serious incident. Incident investigation
outcomes were shared with staff through a variety of methods. Staff received regular emails
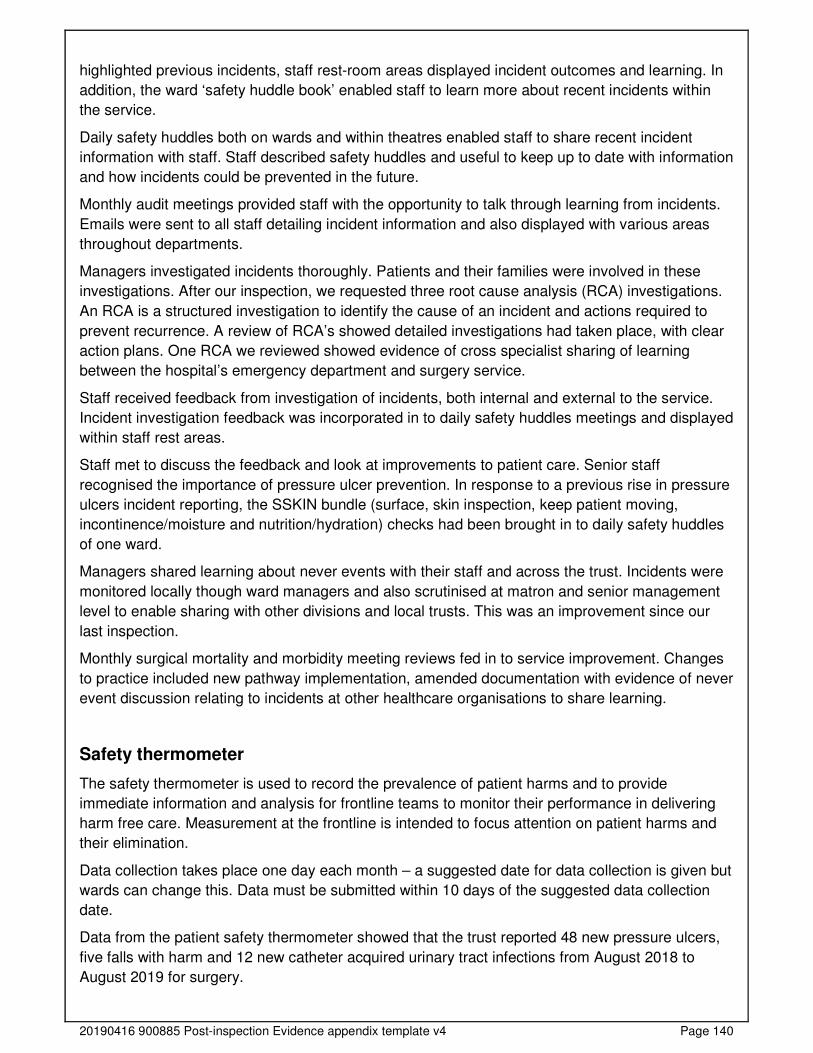
20190416 900885 Post-inspection Evidence appendix template v4 Page 140
highlighted previous incidents, staff rest-room areas displayed incident outcomes and learning. In
addition, the ward ‘safety huddle book’ enabled staff to learn more about recent incidents within
the service.
Daily safety huddles both on wards and within theatres enabled staff to share recent incident
information with staff. Staff described safety huddles and useful to keep up to date with information
and how incidents could be prevented in the future.
Monthly audit meetings provided staff with the opportunity to talk through learning from incidents.
Emails were sent to all staff detailing incident information and also displayed with various areas
throughout departments.
Managers investigated incidents thoroughly. Patients and their families were involved in these
investigations. After our inspection, we requested three root cause analysis (RCA) investigations.
An RCA is a structured investigation to identify the cause of an incident and actions required to
prevent recurrence. A review of RCA’s showed detailed investigations had taken place, with clear
action plans. One RCA we reviewed showed evidence of cross specialist sharing of learning
between the hospital’s emergency department and surgery service.
Staff received feedback from investigation of incidents, both internal and external to the service.
Incident investigation feedback was incorporated in to daily safety huddles meetings and displayed
within staff rest areas.
Staff met to discuss the feedback and look at improvements to patient care. Senior staff
recognised the importance of pressure ulcer prevention. In response to a previous rise in pressure
ulcers incident reporting, the SSKIN bundle (surface, skin inspection, keep patient moving,
incontinence/moisture and nutrition/hydration) checks had been brought in to daily safety huddles
of one ward.
Managers shared learning about never events with their staff and across the trust. Incidents were
monitored locally though ward managers and also scrutinised at matron and senior management
level to enable sharing with other divisions and local trusts. This was an improvement since our
last inspection.
Monthly surgical mortality and morbidity meeting reviews fed in to service improvement. Changes
to practice included new pathway implementation, amended documentation with evidence of never
event discussion relating to incidents at other healthcare organisations to share learning.
Safety thermometer
The safety thermometer is used to record the prevalence of patient harms and to provide
immediate information and analysis for frontline teams to monitor their performance in delivering
harm free care. Measurement at the frontline is intended to focus attention on patient harms and
their elimination.
Data collection takes place one day each month – a suggested date for data collection is given but
wards can change this. Data must be submitted within 10 days of the suggested data collection
date.
Data from the patient safety thermometer showed that the trust reported 48 new pressure ulcers,
five falls with harm and 12 new catheter acquired urinary tract infections from August 2018 to
August 2019 for surgery.
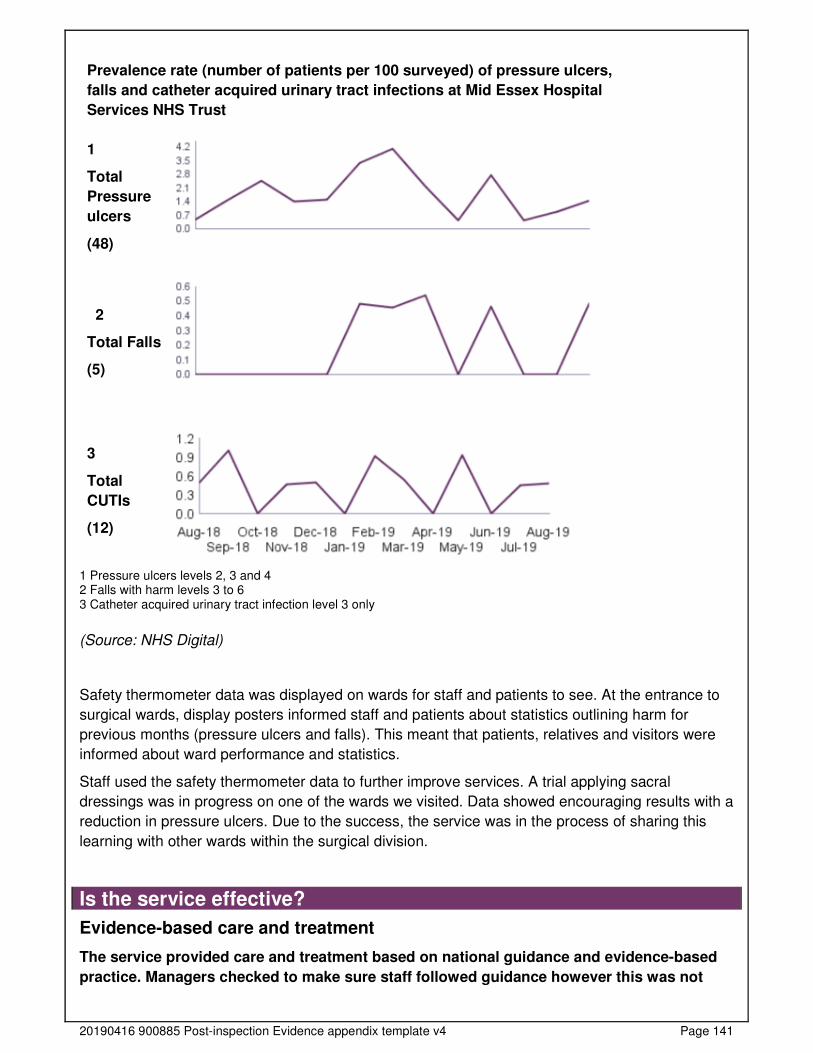
20190416 900885 Post-inspection Evidence appendix template v4 Page 141
Prevalence rate (number of patients per 100 surveyed) of pressure ulcers,
falls and catheter acquired urinary tract infections at Mid Essex Hospital
Services NHS Trust
1
Total
Pressure
ulcers
(48)
2
Total Falls
(5)
3
Total
CUTIs
(12)
1 Pressure ulcers levels 2, 3 and 4 2 Falls with harm levels 3 to 6 3 Catheter acquired urinary tract infection level 3 only
(Source: NHS Digital)
Safety thermometer data was displayed on wards for staff and patients to see. At the entrance to
surgical wards, display posters informed staff and patients about statistics outlining harm for
previous months (pressure ulcers and falls). This meant that patients, relatives and visitors were
informed about ward performance and statistics.
Staff used the safety thermometer data to further improve services. A trial applying sacral
dressings was in progress on one of the wards we visited. Data showed encouraging results with a
reduction in pressure ulcers. Due to the success, the service was in the process of sharing this
learning with other wards within the surgical division.
Is the service effective?
Evidence-based care and treatment
The service provided care and treatment based on national guidance and evidence-based
practice. Managers checked to make sure staff followed guidance however this was not
20190416 900885 Post-inspection Evidence appendix template v4 Page 142
always the case with staff completing venous thromboembolism risk assessments. Staff
protected the rights of patients subject to the Mental Health Act 1983.
Staff followed up-to-date policies to plan and deliver high quality care according to best practice
and national guidance. The service assessed for venous thromboembolism (VTE) in line with the
National Institute for Health and Care Excellence (NICE) guidelines (NG 89, Venous
thromboembolism in over 16s: reducing the risk of hospital-acquired deep vein thrombosis or
pulmonary embolism).
We reviewed the trust’s guideline on the prevention and treatment of VTE which referenced
national guidance and provided clear guidance on VTE treatment and prophylaxis, broken down
by type of surgery and patient (including bariatric surgery). For more information on VTE
assessments, please see the assessing and responding to patient risk section of this report.
Staff had access to a clinical guideline named ‘early identification and treatment of sepsis’. This
provided staff with clear guidance on how to identify and treat sepsis, and contained reference to
national guidance.
Patient documentation booklets and care records contained clear guidance and tools for staff on
the recognition and escalation of patients with known or suspected sepsis. In all records we
reviewed, sepsis documentation had been completed and escalated to senior clinicians where
required.
At handover meetings, staff routinely referred to the psychological and emotional needs of
patients, their relatives and carers. We saw staff thoroughly discussed the needs of patients and
their relatives/carers with other healthcare professionals including physiotherapists, occupational
therapists and social services if required.
The service’s safer surgery pathway (including patient site marking and safe transfer) guideline
was based on national guidance and within review date. The pre-operative fasting policy for adults
and children guideline was within review date, referenced guidelines from the European Society of
Anaesthesiology regarding peri-operative fasting in adults and children.
The peri-procedural anticoagulation in adult patients taking warfarin (blood thinner) and direct oral
anticoagulants guideline referenced national guidance and had been recently ratified in October
2019.
Staff had electronic access to pathways, policies and guidelines through the trust’s intranet.
Computer terminals were available at regular intervals to enable staff to access documentation in
a timely manner. However, some staff told us the system was difficult to navigate leading to
challenges in locating specific documentation.
Nutrition and hydration
Staff gave patients enough food and drink to meet their needs and improve their health.
They used special feeding and hydration techniques when necessary. The service made
adjustments for patients’ religious, cultural and other needs.
Staff followed national guidelines to make sure patients fasting before surgery were not without
food for long periods. Staff followed the services pre-operative fasting policy which had been
reviewed in January 2019. The policy contained clear guidance on fasting guidelines, dependent
on patient age and referenced the Royal College of Anaesthetist guidelines. Fasting is required
prior to surgery to prevent aspiration of stomach contents in to the lungs.
20190416 900885 Post-inspection Evidence appendix template v4 Page 143
Patient mealtimes were protected to ensure patients had quiet time to eat and drink without
interruption.
Staff made sure patients had enough to eat and drink, including those with specialist nutrition and
hydration needs. Dieticians were available to assess patients upon receipt of referral. At all times
during our inspection, we saw that patients had access to fresh drinking water (where clinically
safe to do so).
Staff regularly offered patients both hot and cold drinks. All patients we spoke with told us they had
received enough food and drink during their admission.
Staff did not always fully and accurately complete patients’ fluid charts where needed. In 21
records that we reviewed, five did not have an accurately completed fluid balance chart. We raised
our concerns with the trust during our inspection. In response, senior staff told us the results might
be due to staff sometimes used fluid balance charts for patients who did not require close
monitoring of their fluid balance Senior staff sent a briefing to staff to remind them when charts
should be completed in the aim of improving compliance.
Staff used a nationally recognised screening tool to monitor patients at risk of malnutrition. Staff
assessed patients to monitor for the risk of malnutrition using the Malnutrition Universal Screening
Tool (MUST). Records demonstrated MUST had been completed in all records we reviewed.
Specialist support from staff such as dieticians was available for patients who needed it. Staff
described the dietitian team as responsive and easy to access.
Patients waiting to have surgery were not left nil by mouth for long periods. Staff encouraged to
take clear fluids by mouth as near to surgery as possible to avoid prolonged periods without fluid
and subsequent dehydration. A theatre ‘floor co-ordinator’ contacted wards to advise of theatre
delays, where required.
Pain relief
Staff assessed and monitored patients regularly to see if they were in pain and gave pain
relief in a timely way. They supported those unable to communicate using suitable
assessment tools and gave additional pain relief to ease pain.
Staff assessed patients’ pain using a recognised tool and gave pain relief in line with individual
needs and best practice. Staff used pain scoring tools to assess for levels of pain. The early
warning score in use was also used to assess levels of pain. In addition, pictorial pain scoring was
offered to patients with additional needs such as dementia.
Patients received pain relief soon after requesting it. We saw that pain levels were assessed on a
regular basis, with timely prescribing and administration of pain relief, where required.
Staff prescribed, administered and recorded pain relief accurately. All records we reviewed
showed evidence of accurate prescribing, administration and recording of pain relief.
The trust’s pain team was available Monday to Friday, 9am to 4pm and Saturday 9am-12pm to
provide guidance and advice to staff on adequately managing pain levels for patients. Out of these
hours, support was available from the on call anaesthetic team. Staff described the pain team as
responsive and accessible.

20190416 900885 Post-inspection Evidence appendix template v4 Page 144
Patient outcomes
Staff monitored the effectiveness of care and treatment. However, we could not always see
that findings were used to make improvements in a timely manner.
Managers used information from the audits to improve care and treatment. Managers and staff
carried out a comprehensive programme of repeated audits to check improvement over time.
Audits covered a number of areas including but not limited to; infection prevention and control,
pressure ulcers and falls.
Managers shared and made sure staff understood information from the audits. Information from
audits was shared through ward meetings, information boards and daily huddles on the ward.
Relative risk of readmission
The service had a higher than expected risk of readmission for elective care than the England
average.
Outcomes for patients were mixed, with some national audits not meeting the national standards.
Please see data below for more information.
Elective Admissions - Broomfield Hospital
From February 2018 to January 2019, patients at Broomfield Hospital had a higher than expected
risk of readmission for elective admissions when compared to the England average.
• Plastic surgery patients at Broomfield Hospital had a higher than expected risk of readmission
for elective admissions when compared to the England average.
• Urology patients at Broomfield Hospital had a higher than expected risk of readmission for
elective admissions when compared to the England average.
• Upper gastrointestinal surgery patients at Broomfield Hospital had a higher than expected risk
of readmission for elective admissions when compared to the England average.
Note: Ratio of observed to expected emergency readmissions multiplied by 100. A value below
100 is interpreted as a positive finding, as this means there were fewer observed readmissions
than expected. A value above 100 represents the opposite. Top three specialties for specific site
based on count of activity
Non-Elective Admissions - Broomfield Hospital
The service had a lower than expected risk of readmission for non-elective care than the England
average.
From February 2018 to January 2019, patients at Broomfield Hospital had a lower expected risk of
readmission for non-elective admissions when compared to the England average.
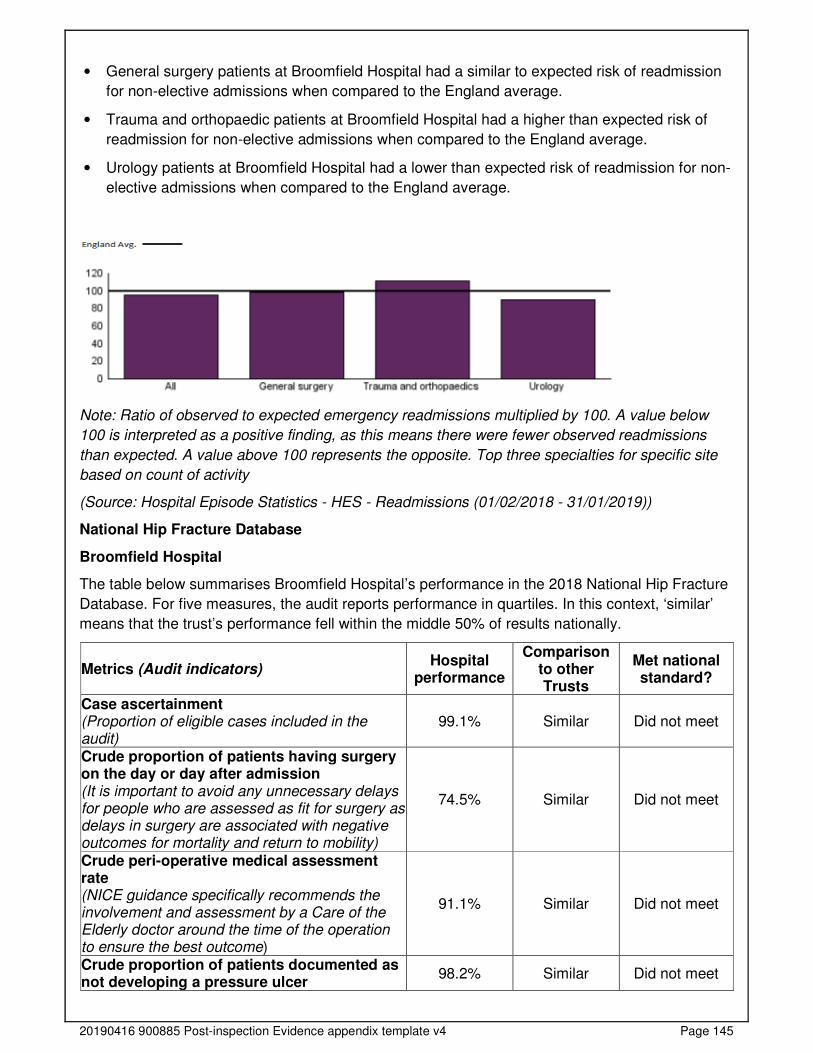
20190416 900885 Post-inspection Evidence appendix template v4 Page 145
• General surgery patients at Broomfield Hospital had a similar to expected risk of readmission
for non-elective admissions when compared to the England average.
• Trauma and orthopaedic patients at Broomfield Hospital had a higher than expected risk of
readmission for non-elective admissions when compared to the England average.
• Urology patients at Broomfield Hospital had a lower than expected risk of readmission for non-
elective admissions when compared to the England average.
Note: Ratio of observed to expected emergency readmissions multiplied by 100. A value below
100 is interpreted as a positive finding, as this means there were fewer observed readmissions
than expected. A value above 100 represents the opposite. Top three specialties for specific site
based on count of activity
(Source: Hospital Episode Statistics - HES - Readmissions (01/02/2018 - 31/01/2019))
National Hip Fracture Database
Broomfield Hospital
The table below summarises Broomfield Hospital’s performance in the 2018 National Hip Fracture
Database. For five measures, the audit reports performance in quartiles. In this context, ‘similar’
means that the trust’s performance fell within the middle 50% of results nationally.
Metrics (Audit indicators) Hospital
performance
Comparison to other Trusts
Met national standard?
Case ascertainment (Proportion of eligible cases included in the audit)
99.1% Similar Did not meet
Crude proportion of patients having surgery on the day or day after admission (It is important to avoid any unnecessary delays for people who are assessed as fit for surgery as delays in surgery are associated with negative outcomes for mortality and return to mobility)
74.5% Similar Did not meet
Crude peri-operative medical assessment rate (NICE guidance specifically recommends the involvement and assessment by a Care of the Elderly doctor around the time of the operation to ensure the best outcome)
91.1% Similar Did not meet
Crude proportion of patients documented as not developing a pressure ulcer
98.2% Similar Did not meet

20190416 900885 Post-inspection Evidence appendix template v4 Page 146
(Careful assessment, documentation and preventative measures should be taken to reduce the risk of hospital-acquired pressure damage (grade 2 or above) during a patient’s admission); this measures an organisation’s ability to report ‘documented as no pressure ulcer’ for a patient Crude overall hospital length of stay (A longer overall length of stay may indicate that patients are not discharged or transferred sufficiently quickly; a too short length of stay may be indicative of a premature discharge and a risk of readmission)
15.0 days Better No current standard
Risk-adjusted 30-day mortality rate (Adjusted scores take into account the differences in the case-mix of patients treated)
7.5% Within
expected range No current standard
(Source: National Hip Fracture Database)
Managers and staff used the results to improve patients' outcomes. After our inspection we
requested the service’s action plan for the National Hip Fracture Database. The action plan
outlined areas for improvement including reducing the time to theatre and improvements with pre
and post-operative mental tests and delirium scores. However, the action plan had been
implemented after our inspection and therefore there was little opportunity to see progress with
actions.
Bowel Cancer Audit
The table below summarises Mid Essex Hospital Services NHS Trust’s performance in the 2018
National Bowel Cancer Audit.
Metrics (Audit measures)
Trust performance
Comparison to other Trusts
Met national standard?
Case ascertainment (Proportion of eligible cases included in the audit)
53.4% Fair Good is over
80%
Risk-adjusted post-operative length of stay >5 days after major resection (A prolonged length of stay can pose risks to patients)
50.0% Better than
national aggregate
No current standard
Risk-adjusted 90-day post-operative mortality rate (Proportion of patients who died within 90 days of surgery; post-operative mortality for bowel cancer surgery varies according to whether surgery occurs as an emergency or as an elective procedure)
0.0% Within
expected range No current standard
Risk-adjusted 2-year post-operative mortality rate (Variation in two-year mortality may reflect, at least in part, differences in surgical care, patient characteristics and provision of chemotherapy and radiotherapy)
21.4% Within
expected range No current standard
Risk-adjusted 30-day unplanned readmission rate
8.0% Within
expected range No current standard
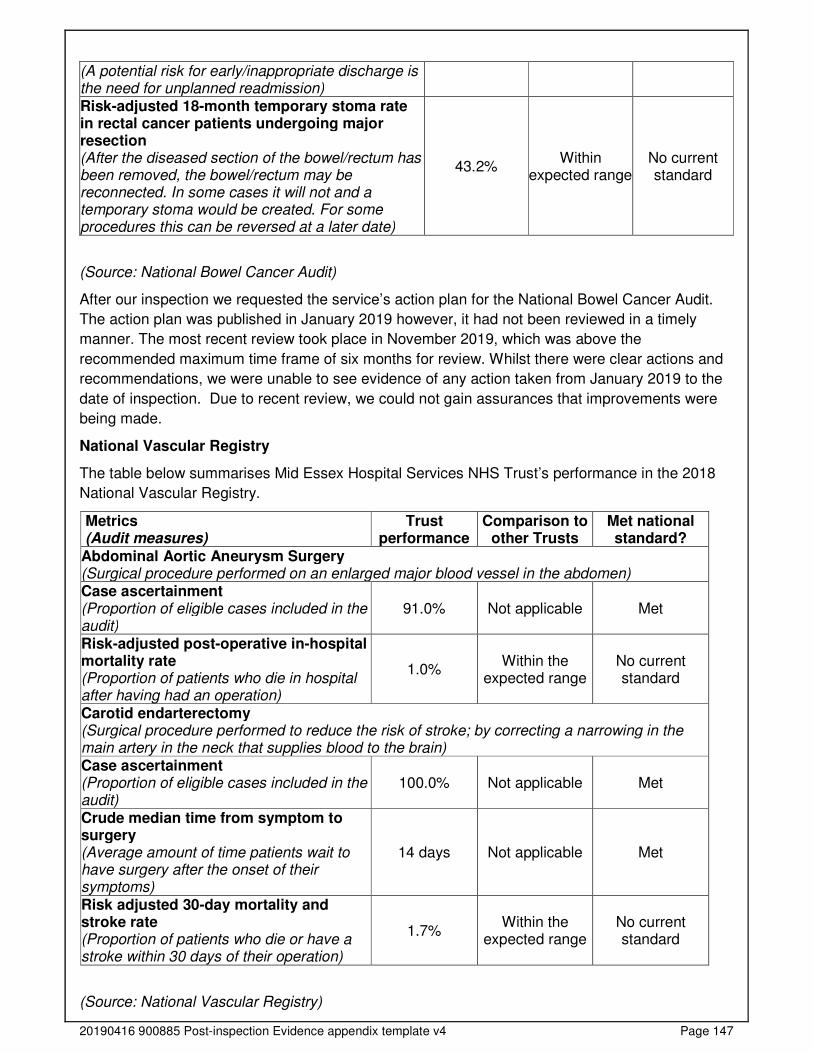
20190416 900885 Post-inspection Evidence appendix template v4 Page 147
(A potential risk for early/inappropriate discharge is the need for unplanned readmission) Risk-adjusted 18-month temporary stoma rate in rectal cancer patients undergoing major resection (After the diseased section of the bowel/rectum has been removed, the bowel/rectum may be reconnected. In some cases it will not and a temporary stoma would be created. For some procedures this can be reversed at a later date)
43.2% Within
expected range No current standard
(Source: National Bowel Cancer Audit)
After our inspection we requested the service’s action plan for the National Bowel Cancer Audit.
The action plan was published in January 2019 however, it had not been reviewed in a timely
manner. The most recent review took place in November 2019, which was above the
recommended maximum time frame of six months for review. Whilst there were clear actions and
recommendations, we were unable to see evidence of any action taken from January 2019 to the
date of inspection. Due to recent review, we could not gain assurances that improvements were
being made.
National Vascular Registry
The table below summarises Mid Essex Hospital Services NHS Trust’s performance in the 2018
National Vascular Registry.
Metrics (Audit measures)
Trust performance
Comparison to other Trusts
Met national standard?
Abdominal Aortic Aneurysm Surgery (Surgical procedure performed on an enlarged major blood vessel in the abdomen) Case ascertainment (Proportion of eligible cases included in the audit)
91.0% Not applicable Met
Risk-adjusted post-operative in-hospital mortality rate (Proportion of patients who die in hospital after having had an operation)
1.0% Within the
expected range No current standard
Carotid endarterectomy (Surgical procedure performed to reduce the risk of stroke; by correcting a narrowing in the main artery in the neck that supplies blood to the brain) Case ascertainment (Proportion of eligible cases included in the audit)
100.0% Not applicable Met
Crude median time from symptom to surgery (Average amount of time patients wait to have surgery after the onset of their symptoms)
14 days Not applicable Met
Risk adjusted 30-day mortality and stroke rate (Proportion of patients who die or have a stroke within 30 days of their operation)
1.7% Within the
expected range No current standard
(Source: National Vascular Registry)
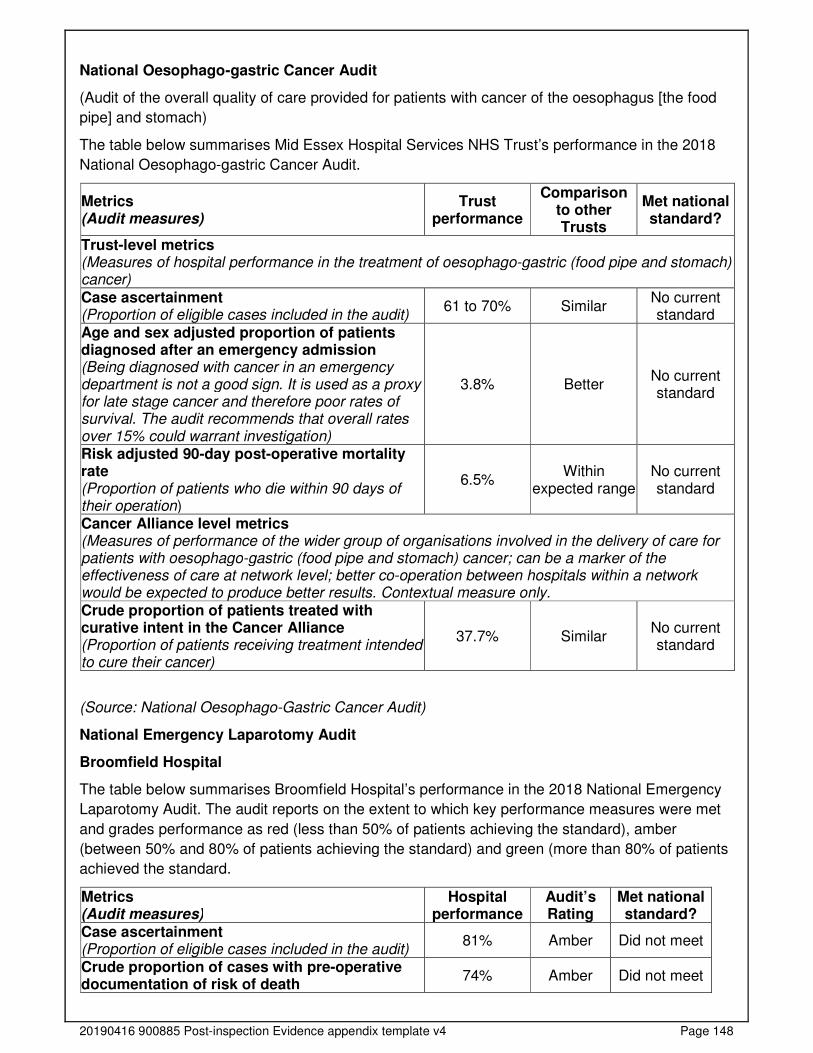
20190416 900885 Post-inspection Evidence appendix template v4 Page 148
National Oesophago-gastric Cancer Audit
(Audit of the overall quality of care provided for patients with cancer of the oesophagus [the food
pipe] and stomach)
The table below summarises Mid Essex Hospital Services NHS Trust’s performance in the 2018
National Oesophago-gastric Cancer Audit.
Metrics (Audit measures)
Trust performance
Comparison to other Trusts
Met national standard?
Trust-level metrics (Measures of hospital performance in the treatment of oesophago-gastric (food pipe and stomach) cancer)
Case ascertainment (Proportion of eligible cases included in the audit)
61 to 70% Similar No current standard
Age and sex adjusted proportion of patients diagnosed after an emergency admission (Being diagnosed with cancer in an emergency department is not a good sign. It is used as a proxy for late stage cancer and therefore poor rates of survival. The audit recommends that overall rates over 15% could warrant investigation)
3.8% Better No current standard
Risk adjusted 90-day post-operative mortality rate (Proportion of patients who die within 90 days of their operation)
6.5% Within
expected range No current standard
Cancer Alliance level metrics (Measures of performance of the wider group of organisations involved in the delivery of care for patients with oesophago-gastric (food pipe and stomach) cancer; can be a marker of the effectiveness of care at network level; better co-operation between hospitals within a network would be expected to produce better results. Contextual measure only. Crude proportion of patients treated with curative intent in the Cancer Alliance (Proportion of patients receiving treatment intended to cure their cancer)
37.7% Similar No current standard
(Source: National Oesophago-Gastric Cancer Audit)
National Emergency Laparotomy Audit
Broomfield Hospital
The table below summarises Broomfield Hospital’s performance in the 2018 National Emergency
Laparotomy Audit. The audit reports on the extent to which key performance measures were met
and grades performance as red (less than 50% of patients achieving the standard), amber
(between 50% and 80% of patients achieving the standard) and green (more than 80% of patients
achieved the standard.
Metrics (Audit measures)
Hospital performance
Audit’s Rating
Met national standard?
Case ascertainment (Proportion of eligible cases included in the audit)
81% Amber Did not meet
Crude proportion of cases with pre-operative documentation of risk of death
74% Amber Did not meet
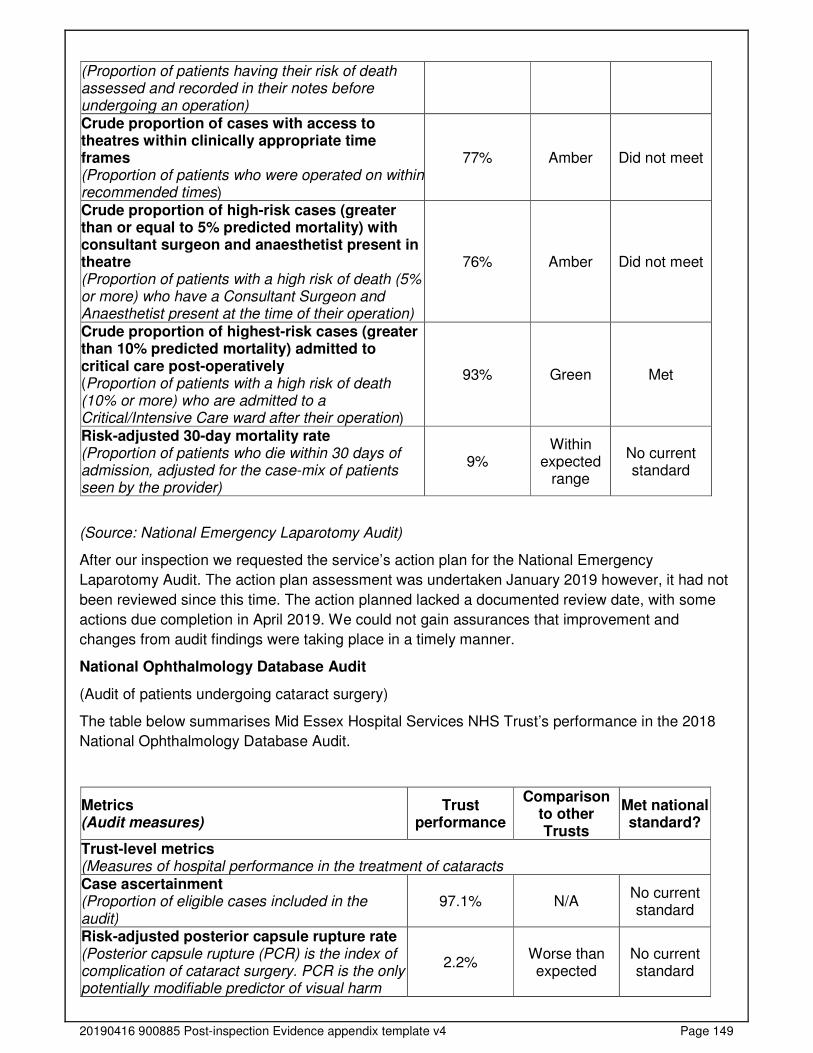
20190416 900885 Post-inspection Evidence appendix template v4 Page 149
(Proportion of patients having their risk of death assessed and recorded in their notes before undergoing an operation) Crude proportion of cases with access to theatres within clinically appropriate time frames (Proportion of patients who were operated on within recommended times)
77% Amber Did not meet
Crude proportion of high-risk cases (greater than or equal to 5% predicted mortality) with consultant surgeon and anaesthetist present in theatre (Proportion of patients with a high risk of death (5% or more) who have a Consultant Surgeon and Anaesthetist present at the time of their operation)
76% Amber Did not meet
Crude proportion of highest-risk cases (greater than 10% predicted mortality) admitted to critical care post-operatively (Proportion of patients with a high risk of death (10% or more) who are admitted to a Critical/Intensive Care ward after their operation)
93% Green Met
Risk-adjusted 30-day mortality rate (Proportion of patients who die within 30 days of admission, adjusted for the case-mix of patients seen by the provider)
9% Within
expected range
No current standard
(Source: National Emergency Laparotomy Audit)
After our inspection we requested the service’s action plan for the National Emergency
Laparotomy Audit. The action plan assessment was undertaken January 2019 however, it had not
been reviewed since this time. The action planned lacked a documented review date, with some
actions due completion in April 2019. We could not gain assurances that improvement and
changes from audit findings were taking place in a timely manner.
National Ophthalmology Database Audit
(Audit of patients undergoing cataract surgery)
The table below summarises Mid Essex Hospital Services NHS Trust’s performance in the 2018
National Ophthalmology Database Audit.
Metrics (Audit measures)
Trust performance
Comparison to other Trusts
Met national standard?
Trust-level metrics (Measures of hospital performance in the treatment of cataracts Case ascertainment (Proportion of eligible cases included in the audit)
97.1% N/A No current standard
Risk-adjusted posterior capsule rupture rate (Posterior capsule rupture (PCR) is the index of complication of cataract surgery. PCR is the only potentially modifiable predictor of visual harm
2.2% Worse than expected
No current standard
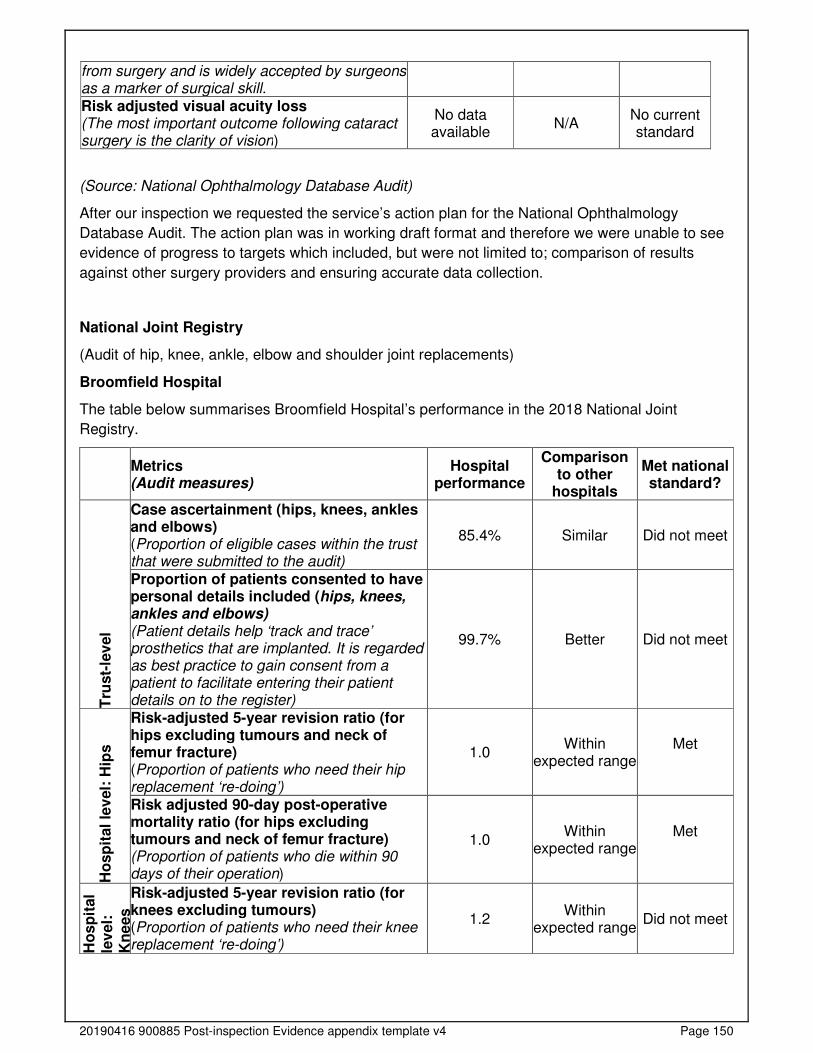
20190416 900885 Post-inspection Evidence appendix template v4 Page 150
from surgery and is widely accepted by surgeons as a marker of surgical skill. Risk adjusted visual acuity loss (The most important outcome following cataract surgery is the clarity of vision)
No data available
N/A No current standard
(Source: National Ophthalmology Database Audit)
After our inspection we requested the service’s action plan for the National Ophthalmology
Database Audit. The action plan was in working draft format and therefore we were unable to see
evidence of progress to targets which included, but were not limited to; comparison of results
against other surgery providers and ensuring accurate data collection.
National Joint Registry
(Audit of hip, knee, ankle, elbow and shoulder joint replacements)
Broomfield Hospital
The table below summarises Broomfield Hospital’s performance in the 2018 National Joint
Registry.
Metrics (Audit measures)
Hospital performance
Comparison to other
hospitals
Met national standard?
Tru
st-
lev
el
Case ascertainment (hips, knees, ankles and elbows) (Proportion of eligible cases within the trust that were submitted to the audit)
85.4% Similar Did not meet
Proportion of patients consented to have personal details included (hips, knees, ankles and elbows) (Patient details help ‘track and trace’ prosthetics that are implanted. It is regarded as best practice to gain consent from a patient to facilitate entering their patient details on to the register)
99.7% Better Did not meet
Ho
sp
ital
lev
el:
Hip
s
Risk-adjusted 5-year revision ratio (for hips excluding tumours and neck of femur fracture) (Proportion of patients who need their hip replacement ‘re-doing’)
1.0 Within
expected range Met
Risk adjusted 90-day post-operative mortality ratio (for hips excluding tumours and neck of femur fracture) (Proportion of patients who die within 90 days of their operation)
1.0 Within
expected range Met
Ho
sp
ital
lev
el:
K
ne
es
Risk-adjusted 5-year revision ratio (for knees excluding tumours) (Proportion of patients who need their knee replacement ‘re-doing’)
1.2 Within
expected range Did not meet

20190416 900885 Post-inspection Evidence appendix template v4 Page 151
Risk adjusted 90-day post-operative mortality ratio (for knees excluding tumours) (Proportion of patients who die within 90 days of their operation)
1.7 Within
expected range Did not meet
(Source: National Joint Registry)
National Prostate Cancer Audit
Broomfield Hospital
The table below summarises Broomfield Hospital’s performance in the 2018 National Prostate
Cancer Audit. Please note, the trust was not eligible the final three metrics. These metrics relate to
specific procedures and therefore it was likely that the trust did not have any patients who
underwent those specific procedures.
Metrics (Audit measures)
Hospital performance
Comparison to other trusts
Met national standard?
Men with complete information to determine disease status (This is a classification that describes how advanced the cancer is and includes the size of the tumour, the involvement of lymph nodes and whether the cancer has spread to different part of the body)
91.9% N/A Did not meet
Percentage of patients who had an emergency readmission within 90 days of radical prostatectomy (A radical prostatectomy involves the surgical removal of the whole prostate and the cancer cells within it; emergency readmission may reflect that patients experienced a complication related to the surgery after discharge from hospital)
No data available N/A No current standard
Percentage of patients experiencing a severe urinary complication requiring intervention following radical prostatectomy (Complications following surgery may reflect the quality of surgical care)
No data available N/A No current standard
Percentage of patients experiencing a severe gastrointestinal complication requiring an intervention following external beam radiotherapy (External beam radiotherapy uses high-energy beams to destroy cancer cells)
No data available N/A No current standard
(Source: National Prostate Cancer Audit)
Patient Reported Outcome Measures
In the Patient Reported Outcomes Measures (PROMS) survey, patients are asked whether they
feel better or worse after receiving the following operations:

20190416 900885 Post-inspection Evidence appendix template v4 Page 152
• Groin hernias
• Varicose veins
• Hip replacements
• Knee replacements
Proportions of patients who reported an improvement after each procedure can be seen on the
right of the graph, whereas proportions of patients reporting that they feel worse can be viewed on
the left. These changes are measured in a number of different ways, descriptions of some of the
indicators presented are below.
The visual analogue scale (EQ VAS) asks patients to mark their health status on the day of the
interview on a vertical scale. The bottom rate (0) corresponds to "the worst health you can
imagine", and the highest rate (100) corresponds to "the best health you can imagine".
The EQ-5D-5L questionnaire has two parts. Five domain questions ask about specific issues;
namely mobility, self-care, usual activities, pain or discomfort, anxiety or depression. The EQ-5D-
5L uses five levels of responsiveness to measure problems. The range is; no problem to
disabling/extreme.
The Oxford Hip Score (OHS) is a patient self-completion report on outcomes of hip operations
containing 12 questions about activities of daily living. A simple scoring and summing system
provides an overall scale for assessing outcome of hip interventions.
In 2016/17 performance on groin hernias was better than the England average for both metrics
reported in the PROMs survey.
For varicose veins, performance was better than the England average for scores relating to the
EQ-5D index. In relation to EQ-VAS scores, the percentage of patients who reported feeling worse
following their procedure was lower than the England average and the percentage of patients who
reported an improvement was similar to the England average.
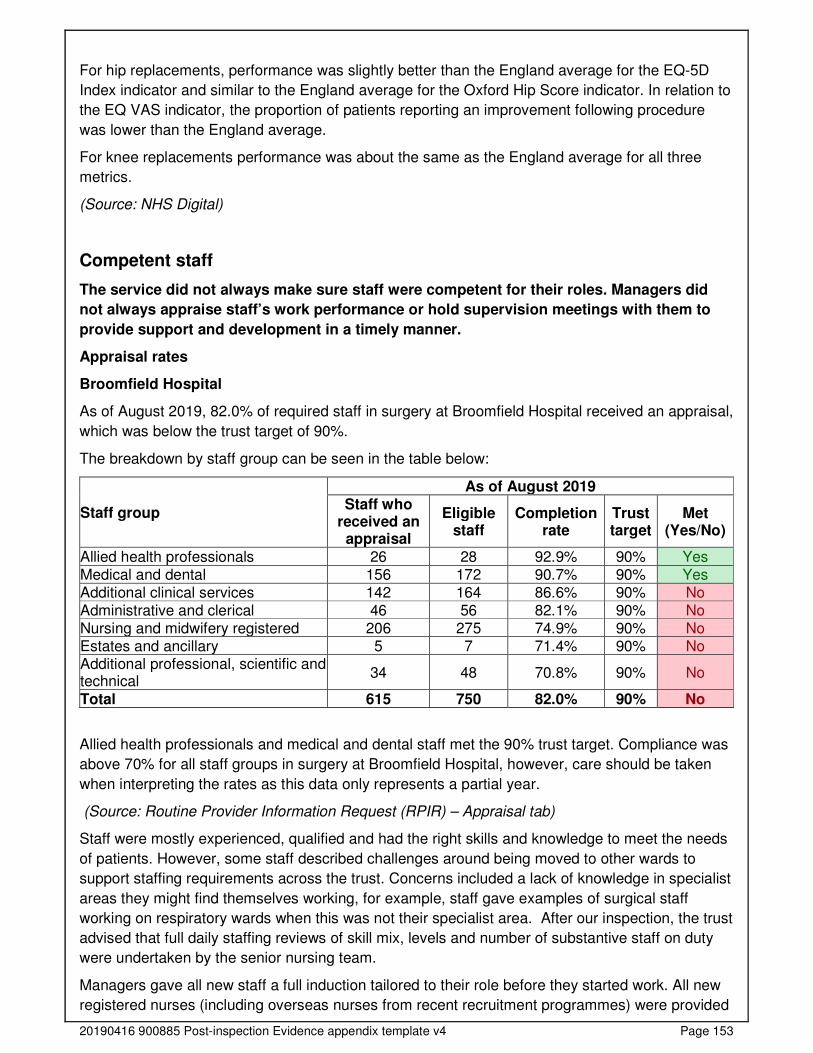
20190416 900885 Post-inspection Evidence appendix template v4 Page 153
For hip replacements, performance was slightly better than the England average for the EQ-5D
Index indicator and similar to the England average for the Oxford Hip Score indicator. In relation to
the EQ VAS indicator, the proportion of patients reporting an improvement following procedure
was lower than the England average.
For knee replacements performance was about the same as the England average for all three
metrics.
(Source: NHS Digital)
Competent staff
The service did not always make sure staff were competent for their roles. Managers did
not always appraise staff’s work performance or hold supervision meetings with them to
provide support and development in a timely manner.
Appraisal rates
Broomfield Hospital
As of August 2019, 82.0% of required staff in surgery at Broomfield Hospital received an appraisal,
which was below the trust target of 90%.
The breakdown by staff group can be seen in the table below:
Staff group
As of August 2019 Staff who
received an appraisal
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Allied health professionals 26 28 92.9% 90% Yes Medical and dental 156 172 90.7% 90% Yes Additional clinical services 142 164 86.6% 90% No Administrative and clerical 46 56 82.1% 90% No Nursing and midwifery registered 206 275 74.9% 90% No Estates and ancillary 5 7 71.4% 90% No Additional professional, scientific and technical
34 48 70.8% 90% No
Total 615 750 82.0% 90% No
Allied health professionals and medical and dental staff met the 90% trust target. Compliance was
above 70% for all staff groups in surgery at Broomfield Hospital, however, care should be taken
when interpreting the rates as this data only represents a partial year.
(Source: Routine Provider Information Request (RPIR) – Appraisal tab)
Staff were mostly experienced, qualified and had the right skills and knowledge to meet the needs
of patients. However, some staff described challenges around being moved to other wards to
support staffing requirements across the trust. Concerns included a lack of knowledge in specialist
areas they might find themselves working, for example, staff gave examples of surgical staff
working on respiratory wards when this was not their specialist area. After our inspection, the trust
advised that full daily staffing reviews of skill mix, levels and number of substantive staff on duty
were undertaken by the senior nursing team.
Managers gave all new staff a full induction tailored to their role before they started work. All new
registered nurses (including overseas nurses from recent recruitment programmes) were provided
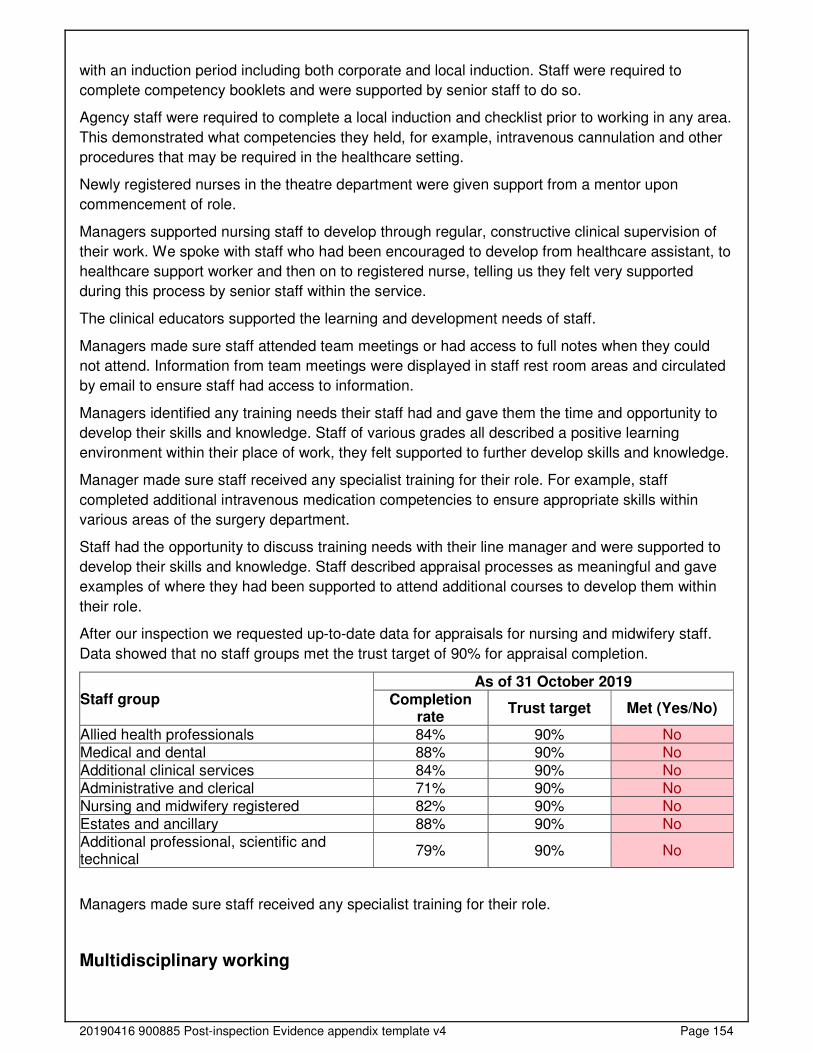
20190416 900885 Post-inspection Evidence appendix template v4 Page 154
with an induction period including both corporate and local induction. Staff were required to
complete competency booklets and were supported by senior staff to do so.
Agency staff were required to complete a local induction and checklist prior to working in any area.
This demonstrated what competencies they held, for example, intravenous cannulation and other
procedures that may be required in the healthcare setting.
Newly registered nurses in the theatre department were given support from a mentor upon
commencement of role.
Managers supported nursing staff to develop through regular, constructive clinical supervision of
their work. We spoke with staff who had been encouraged to develop from healthcare assistant, to
healthcare support worker and then on to registered nurse, telling us they felt very supported
during this process by senior staff within the service.
The clinical educators supported the learning and development needs of staff.
Managers made sure staff attended team meetings or had access to full notes when they could
not attend. Information from team meetings were displayed in staff rest room areas and circulated
by email to ensure staff had access to information.
Managers identified any training needs their staff had and gave them the time and opportunity to
develop their skills and knowledge. Staff of various grades all described a positive learning
environment within their place of work, they felt supported to further develop skills and knowledge.
Manager made sure staff received any specialist training for their role. For example, staff
completed additional intravenous medication competencies to ensure appropriate skills within
various areas of the surgery department.
Staff had the opportunity to discuss training needs with their line manager and were supported to
develop their skills and knowledge. Staff described appraisal processes as meaningful and gave
examples of where they had been supported to attend additional courses to develop them within
their role.
After our inspection we requested up-to-date data for appraisals for nursing and midwifery staff.
Data showed that no staff groups met the trust target of 90% for appraisal completion.
Staff group As of 31 October 2019
Completion rate
Trust target Met (Yes/No)
Allied health professionals 84% 90% No Medical and dental 88% 90% No Additional clinical services 84% 90% No Administrative and clerical 71% 90% No Nursing and midwifery registered 82% 90% No Estates and ancillary 88% 90% No Additional professional, scientific and technical
79% 90% No
Managers made sure staff received any specialist training for their role.
Multidisciplinary working
20190416 900885 Post-inspection Evidence appendix template v4 Page 155
Doctors, nurses and other healthcare professionals worked together as a team to benefit
patients. They supported each other to provide good care.
Staff held regular and effective multidisciplinary meetings to discuss patients and improve their
care. Multidisciplinary team (MDT) meetings took place on a regular basis and included a wide
range of healthcare professionals. Staff knew who was responsible for each patient’s care with a
named consultant and nurse in place.
Staff worked across health care disciplines and with other agencies when required to care for
patients. Staff described positive working relationship with other clinicians including doctors,
anaesthetists, consultants and physiotherapists/occupational therapists. During our inspection we
saw a range of healthcare professional including physiotherapist and occupational therapists
discussing patient care.
There was a good relationship between ward staff and theatre staff, including the day surgery unit.
Staff could access up to date patient information through medical records booklets and care plans.
Staff had access to a range of clinical nurse specialist including stoma care, diabetes and learning
disability and they shared information at MDT meetings to improve patient care.
Staff shared information amongst various departments. For example from theatres to wards. Ward
based staff could describe recent never events and changes in practice.
Externally, work was in progress with forging strong working relationships as part of the Mid and
South Essex success Regime, with a planned merger taking place in April 2020. Staff described
ear, nose and throat services working as part of an effective network and that foundations were
being laid prior to the merger in April 2020.
Staff referred patients for mental health assessments when they showed signs of mental ill health
or depression.
Seven-day services
Key services were available seven days a week to support timely patient care.
Access to emergency surgical services was available 24 hours a day, seven days a week. Medical
staff were available on a rota system when outside of normal working hours. An on call consultant
was available for response to the hospital within 30 minutes out of hours.
Registrars led daily ward rounds on all wards, including weekends. Patients were reviewed by
consultants depending on the care pathway. Staff told us that consultants were readily available to
discuss patients requiring senior input, for example emergency trauma patients. In addition, ward
rounds were attended by senior nursing staff.
Staff could call for support from doctors and other disciplines, including mental health services and
diagnostic tests, 24 hours a day, seven days a week. Diagnostic imaging services (including x-ray,
magnetic resonance imaging and computed tomography) were available 24 hours a day, seven
days a week. This was in line with standard five (priority standard) of the NHS seven day services.
Pharmaceutical, anaesthetic and pathology services were accessible 24 hours a day, seven days
a week to ensure access to service in a timely manner to aid clinical decision making (on an on
call basis when out of hours).
Dietician support was available Monday to Friday, 9am to 5pm. The pain management team was
available six days a week, with access to an on call anaesthetic outside of normal working hours.
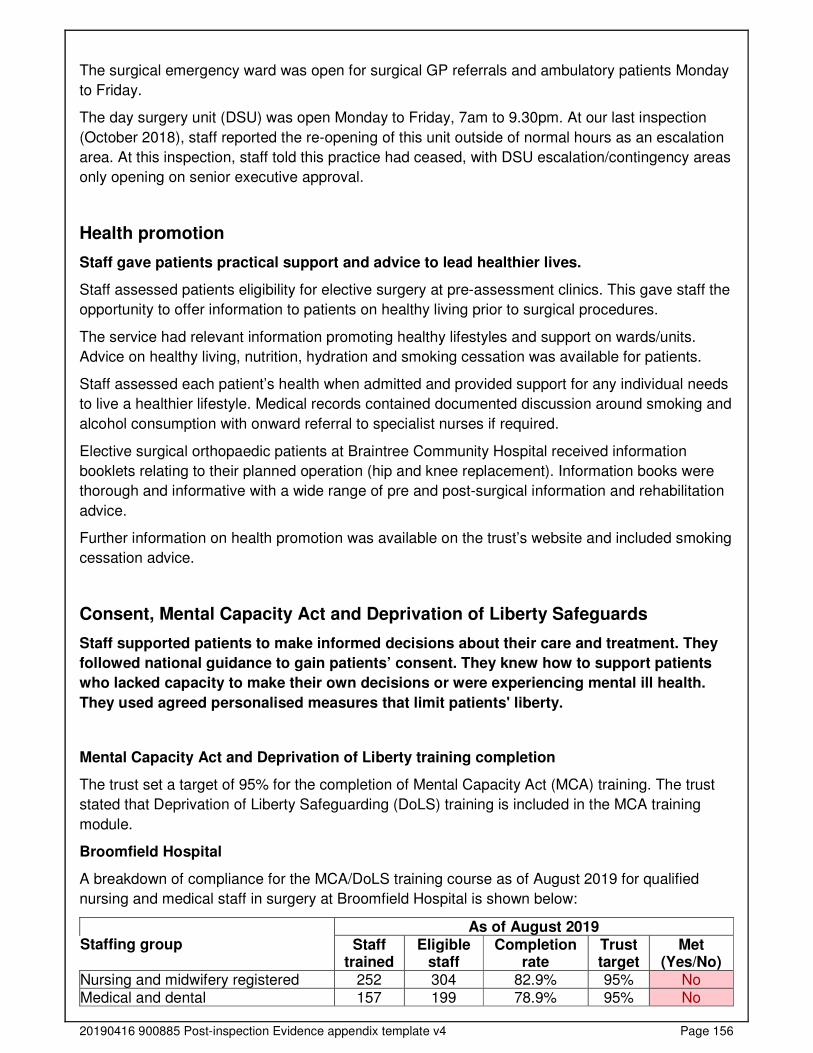
20190416 900885 Post-inspection Evidence appendix template v4 Page 156
The surgical emergency ward was open for surgical GP referrals and ambulatory patients Monday
to Friday.
The day surgery unit (DSU) was open Monday to Friday, 7am to 9.30pm. At our last inspection
(October 2018), staff reported the re-opening of this unit outside of normal hours as an escalation
area. At this inspection, staff told this practice had ceased, with DSU escalation/contingency areas
only opening on senior executive approval.
Health promotion
Staff gave patients practical support and advice to lead healthier lives.
Staff assessed patients eligibility for elective surgery at pre-assessment clinics. This gave staff the
opportunity to offer information to patients on healthy living prior to surgical procedures.
The service had relevant information promoting healthy lifestyles and support on wards/units.
Advice on healthy living, nutrition, hydration and smoking cessation was available for patients.
Staff assessed each patient’s health when admitted and provided support for any individual needs
to live a healthier lifestyle. Medical records contained documented discussion around smoking and
alcohol consumption with onward referral to specialist nurses if required.
Elective surgical orthopaedic patients at Braintree Community Hospital received information
booklets relating to their planned operation (hip and knee replacement). Information books were
thorough and informative with a wide range of pre and post-surgical information and rehabilitation
advice.
Further information on health promotion was available on the trust’s website and included smoking
cessation advice.
Consent, Mental Capacity Act and Deprivation of Liberty Safeguards
Staff supported patients to make informed decisions about their care and treatment. They
followed national guidance to gain patients’ consent. They knew how to support patients
who lacked capacity to make their own decisions or were experiencing mental ill health.
They used agreed personalised measures that limit patients' liberty.
Mental Capacity Act and Deprivation of Liberty training completion
The trust set a target of 95% for the completion of Mental Capacity Act (MCA) training. The trust
stated that Deprivation of Liberty Safeguarding (DoLS) training is included in the MCA training
module.
Broomfield Hospital
A breakdown of compliance for the MCA/DoLS training course as of August 2019 for qualified
nursing and medical staff in surgery at Broomfield Hospital is shown below:
Staffing group As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Nursing and midwifery registered 252 304 82.9% 95% No Medical and dental 157 199 78.9% 95% No
20190416 900885 Post-inspection Evidence appendix template v4 Page 157
In surgery, the 95% trust target was not met for the MCA/DoLS module by qualified nurses and
medical and dental staff as of August 2019.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Clinical (medical and nursing) staff did not always receive or keep up to date with training in the
Mental Capacity Act and Deprivation of Liberty Safeguards. After our inspection we requested up-
to-date data for MCA and DoLS training. Data showed 83% of nursing and medical staff had
completed this training at required intervals. This was below the service’s target of 95%.
Staff understood the relevant consent and decision-making requirements of legislation and
guidance, including the Mental Health Act, Mental Capacity Act 2005 and the Children Acts 1989
and 2004 and they knew who to contact for advice. A policy named consent to examination or
treatment was available for staff to access electronically. The policy had recently been reviewed in
August 2019. The policy provided guidance for staff on determining if a patient had capacity, the
seeking of consent and processes for recoding written consent.
Staff gained consent from patients for their care and treatment in line with legislation and
guidance. Staff clearly recorded consent in the patients’ records. We reviewed 21 patient records.
In all cases we saw consent had been documented.
Staff understood how and when to assess whether a patient had the capacity to make decisions
about their care. The trust wide safeguarding team reviewed all MCA and DoLs documentation to
ensure correct processes were being followed. Staff had access to clinical nurse specialists for
learning disability and dementia in the event that further advice and support was required.
Staff made sure patients consented to treatment based on all the information available. We
observed staff explaining treatment and procedures in detail with patients during our inspection.
Managers monitored the use of Deprivation of Liberty Safeguards and made sure staff knew how
to complete them. Staff describe the meaning of deprivation of liberty and managers maintained
oversight of this.
Staff could describe and knew how to access policy and get accurate advice on Mental Capacity
Act and Deprivation of Liberty Safeguards. The trust’s liberty safeguard policy and procedure was
available for staff to access electronically. The policy was within review date. It provided guidance
for staff on requirements for the MCA and DoLS, how to apply for a deprivation of liberty
authorisation and the roles and responsibilities of staff.
Is the service caring?
Compassionate care
Staff treated patients with compassion and kindness, respected their privacy and dignity,
and took account of their individual needs.
Friends and Family test performance
Broomfield Hospital
The Friends and Family Test response rate for surgery at Mid Essex Hospital Services NHS Trust
was 22.9% which was worse than the England average of 24.0% from July 2018 to June 2019.
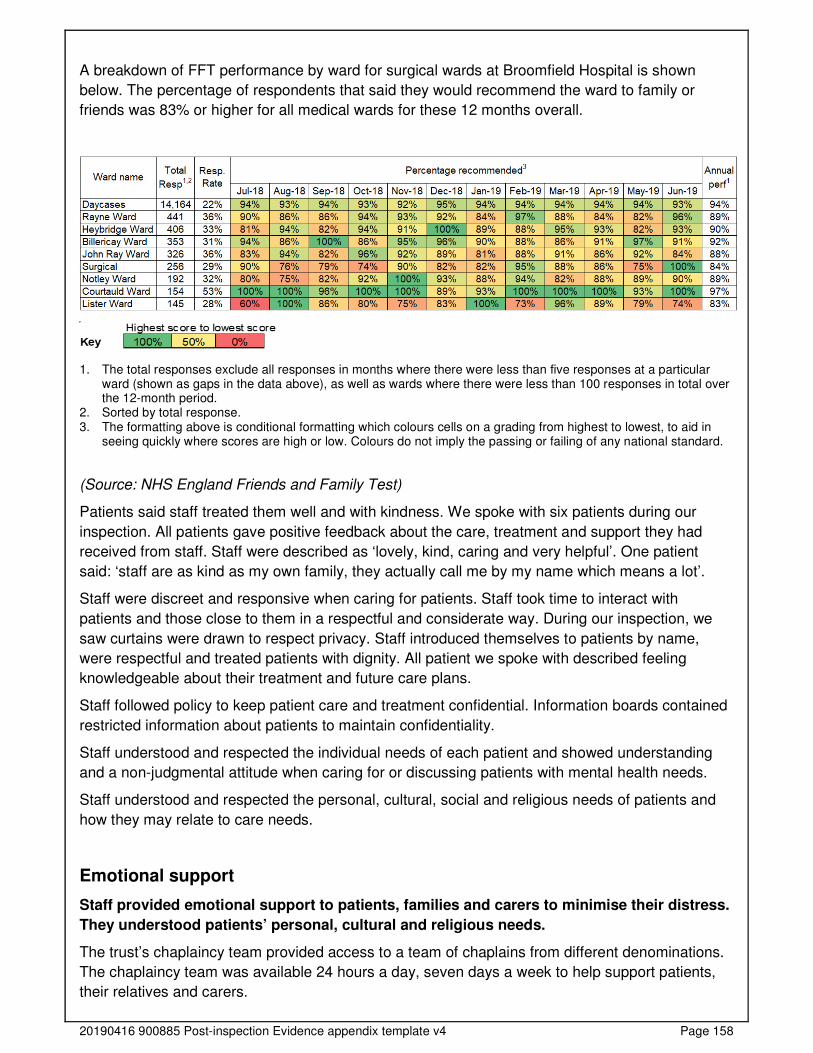
20190416 900885 Post-inspection Evidence appendix template v4 Page 158
A breakdown of FFT performance by ward for surgical wards at Broomfield Hospital is shown
below. The percentage of respondents that said they would recommend the ward to family or
friends was 83% or higher for all medical wards for these 12 months overall.
1. The total responses exclude all responses in months where there were less than five responses at a particular ward (shown as gaps in the data above), as well as wards where there were less than 100 responses in total over the 12-month period.
2. Sorted by total response. 3. The formatting above is conditional formatting which colours cells on a grading from highest to lowest, to aid in
seeing quickly where scores are high or low. Colours do not imply the passing or failing of any national standard.
(Source: NHS England Friends and Family Test)
Patients said staff treated them well and with kindness. We spoke with six patients during our
inspection. All patients gave positive feedback about the care, treatment and support they had
received from staff. Staff were described as ‘lovely, kind, caring and very helpful’. One patient
said: ‘staff are as kind as my own family, they actually call me by my name which means a lot’.
Staff were discreet and responsive when caring for patients. Staff took time to interact with
patients and those close to them in a respectful and considerate way. During our inspection, we
saw curtains were drawn to respect privacy. Staff introduced themselves to patients by name,
were respectful and treated patients with dignity. All patient we spoke with described feeling
knowledgeable about their treatment and future care plans.
Staff followed policy to keep patient care and treatment confidential. Information boards contained
restricted information about patients to maintain confidentiality.
Staff understood and respected the individual needs of each patient and showed understanding
and a non-judgmental attitude when caring for or discussing patients with mental health needs.
Staff understood and respected the personal, cultural, social and religious needs of patients and
how they may relate to care needs.
Emotional support
Staff provided emotional support to patients, families and carers to minimise their distress.
They understood patients’ personal, cultural and religious needs.
The trust’s chaplaincy team provided access to a team of chaplains from different denominations.
The chaplaincy team was available 24 hours a day, seven days a week to help support patients,
their relatives and carers.
20190416 900885 Post-inspection Evidence appendix template v4 Page 159
Staff gave patients and those close to them help, emotional support and advice when they needed
it. Patients had access to a number of clinical nurse specialist to provide both physical and
emotional support. One patient told us they had felt supported by the stoma care team and that
they were offered psychological support at regular intervals.
Whilst staff did not receive formal training in the chaperone role, staff could support patients where
requested.
Staff supported patients who became distressed in an open environment and helped them
maintain their privacy and dignity.
Staff understood the emotional and social impact that a person’s care, treatment or condition had
on their wellbeing and on those close to them.
Understanding and involvement of patients and those close to them
Staff supported and involved patients, families and carers to understand their condition
and make decisions about their care and treatment. Staff made sure patients and those
close to them understood their care and treatment.
We spoke with six patients who all described feeling informed about their care and that they had
received enough information about what to expect.
The service had developed comprehensive information books for patients undergoing hip or knee
replacement. The books provided a wide range of information including pre-surgery, post-surgery
and rehabilitation advice.
Staff talked with patients, families and carers in a way they could understand, using
communication aids where necessary. Staff used a range of tools to help communication with
patients who had additional needs. Tools included picture books and pictorial pain scoring.
Patients and their families could give feedback on the service and their treatment and staff
supported them to do this. Staff welcomed feedback and information in ward areas encouraged
patients, relatives and carers to provide feedback about the care received.
Staff supported patients to make advanced decisions about their care.
Staff supported patients to make informed decisions about their care. All patients we spoke with
described feeling well informed about their care and future treatment plans.
Patients gave positive feedback about the service. All patients we spoke with gave positive
feedback about the care and treatment they were receiving.
Is the service responsive?
Service delivery to meet the needs of local people
The service planned and provided care in a way that met the needs of local people and the
communities served. It also worked with others in the wider system and local organisations
to plan care.
Managers planned and organised services, so they met the changing needs of the local
population. At the time of our inspection, plans were in place to merge with two other local NHS
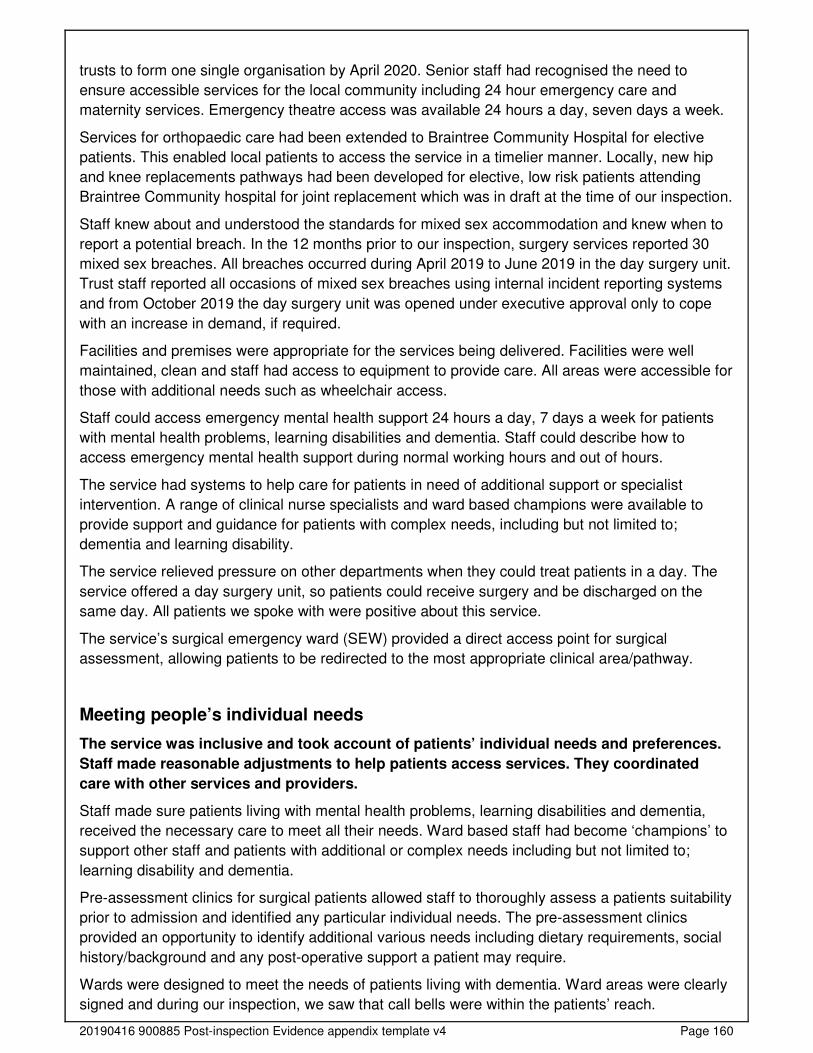
20190416 900885 Post-inspection Evidence appendix template v4 Page 160
trusts to form one single organisation by April 2020. Senior staff had recognised the need to
ensure accessible services for the local community including 24 hour emergency care and
maternity services. Emergency theatre access was available 24 hours a day, seven days a week.
Services for orthopaedic care had been extended to Braintree Community Hospital for elective
patients. This enabled local patients to access the service in a timelier manner. Locally, new hip
and knee replacements pathways had been developed for elective, low risk patients attending
Braintree Community hospital for joint replacement which was in draft at the time of our inspection.
Staff knew about and understood the standards for mixed sex accommodation and knew when to
report a potential breach. In the 12 months prior to our inspection, surgery services reported 30
mixed sex breaches. All breaches occurred during April 2019 to June 2019 in the day surgery unit.
Trust staff reported all occasions of mixed sex breaches using internal incident reporting systems
and from October 2019 the day surgery unit was opened under executive approval only to cope
with an increase in demand, if required.
Facilities and premises were appropriate for the services being delivered. Facilities were well
maintained, clean and staff had access to equipment to provide care. All areas were accessible for
those with additional needs such as wheelchair access.
Staff could access emergency mental health support 24 hours a day, 7 days a week for patients
with mental health problems, learning disabilities and dementia. Staff could describe how to
access emergency mental health support during normal working hours and out of hours.
The service had systems to help care for patients in need of additional support or specialist
intervention. A range of clinical nurse specialists and ward based champions were available to
provide support and guidance for patients with complex needs, including but not limited to;
dementia and learning disability.
The service relieved pressure on other departments when they could treat patients in a day. The
service offered a day surgery unit, so patients could receive surgery and be discharged on the
same day. All patients we spoke with were positive about this service.
The service’s surgical emergency ward (SEW) provided a direct access point for surgical
assessment, allowing patients to be redirected to the most appropriate clinical area/pathway.
Meeting people’s individual needs
The service was inclusive and took account of patients’ individual needs and preferences.
Staff made reasonable adjustments to help patients access services. They coordinated
care with other services and providers.
Staff made sure patients living with mental health problems, learning disabilities and dementia,
received the necessary care to meet all their needs. Ward based staff had become ‘champions’ to
support other staff and patients with additional or complex needs including but not limited to;
learning disability and dementia.
Pre-assessment clinics for surgical patients allowed staff to thoroughly assess a patients suitability
prior to admission and identified any particular individual needs. The pre-assessment clinics
provided an opportunity to identify additional various needs including dietary requirements, social
history/background and any post-operative support a patient may require.
Wards were designed to meet the needs of patients living with dementia. Ward areas were clearly
signed and during our inspection, we saw that call bells were within the patients’ reach.
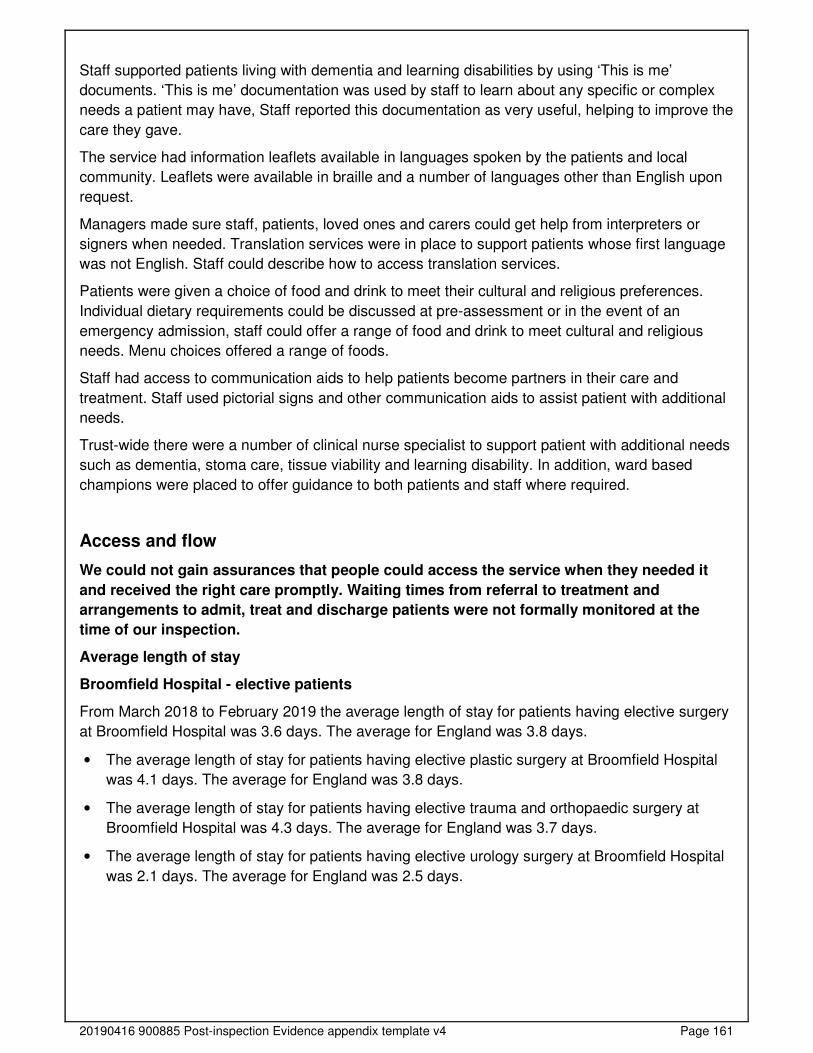
20190416 900885 Post-inspection Evidence appendix template v4 Page 161
Staff supported patients living with dementia and learning disabilities by using ‘This is me’
documents. ‘This is me’ documentation was used by staff to learn about any specific or complex
needs a patient may have, Staff reported this documentation as very useful, helping to improve the
care they gave.
The service had information leaflets available in languages spoken by the patients and local
community. Leaflets were available in braille and a number of languages other than English upon
request.
Managers made sure staff, patients, loved ones and carers could get help from interpreters or
signers when needed. Translation services were in place to support patients whose first language
was not English. Staff could describe how to access translation services.
Patients were given a choice of food and drink to meet their cultural and religious preferences.
Individual dietary requirements could be discussed at pre-assessment or in the event of an
emergency admission, staff could offer a range of food and drink to meet cultural and religious
needs. Menu choices offered a range of foods.
Staff had access to communication aids to help patients become partners in their care and
treatment. Staff used pictorial signs and other communication aids to assist patient with additional
needs.
Trust-wide there were a number of clinical nurse specialist to support patient with additional needs
such as dementia, stoma care, tissue viability and learning disability. In addition, ward based
champions were placed to offer guidance to both patients and staff where required.
Access and flow
We could not gain assurances that people could access the service when they needed it
and received the right care promptly. Waiting times from referral to treatment and
arrangements to admit, treat and discharge patients were not formally monitored at the
time of our inspection.
Average length of stay
Broomfield Hospital - elective patients
From March 2018 to February 2019 the average length of stay for patients having elective surgery
at Broomfield Hospital was 3.6 days. The average for England was 3.8 days.
• The average length of stay for patients having elective plastic surgery at Broomfield Hospital
was 4.1 days. The average for England was 3.8 days.
• The average length of stay for patients having elective trauma and orthopaedic surgery at
Broomfield Hospital was 4.3 days. The average for England was 3.7 days.
• The average length of stay for patients having elective urology surgery at Broomfield Hospital
was 2.1 days. The average for England was 2.5 days.
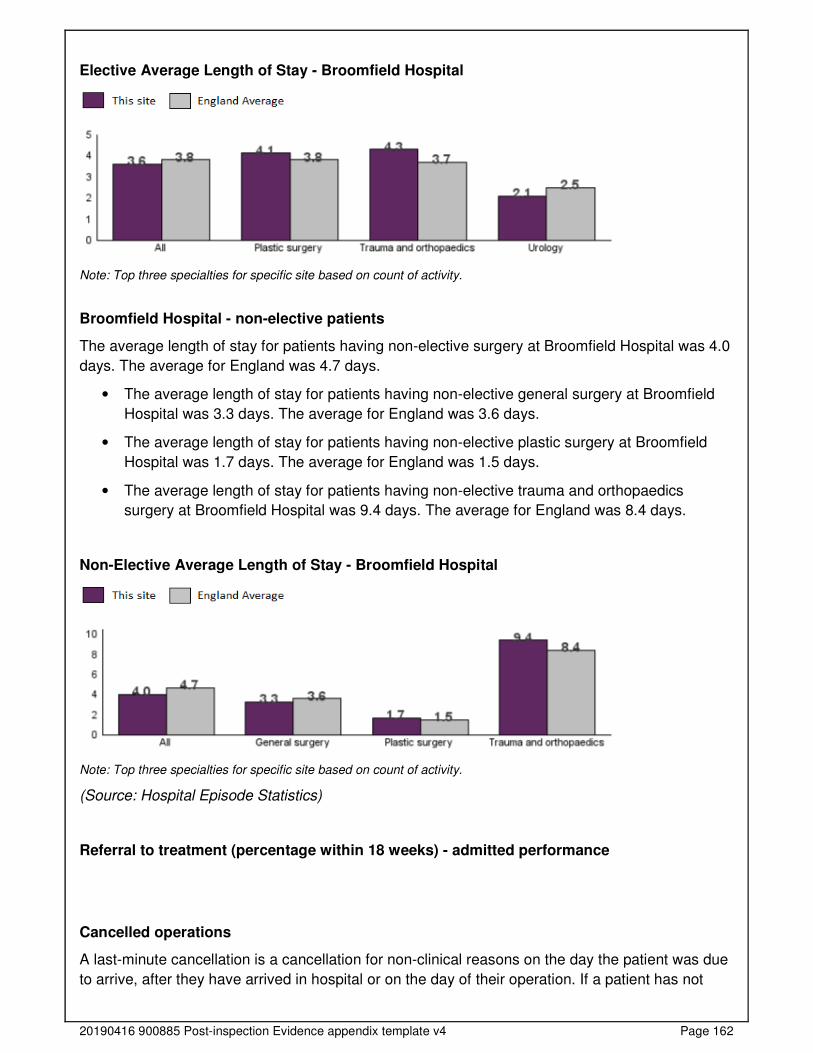
20190416 900885 Post-inspection Evidence appendix template v4 Page 162
Elective Average Length of Stay - Broomfield Hospital
Note: Top three specialties for specific site based on count of activity.
Broomfield Hospital - non-elective patients
The average length of stay for patients having non-elective surgery at Broomfield Hospital was 4.0
days. The average for England was 4.7 days.
• The average length of stay for patients having non-elective general surgery at Broomfield
Hospital was 3.3 days. The average for England was 3.6 days.
• The average length of stay for patients having non-elective plastic surgery at Broomfield
Hospital was 1.7 days. The average for England was 1.5 days.
• The average length of stay for patients having non-elective trauma and orthopaedics
surgery at Broomfield Hospital was 9.4 days. The average for England was 8.4 days.
Non-Elective Average Length of Stay - Broomfield Hospital
Note: Top three specialties for specific site based on count of activity.
(Source: Hospital Episode Statistics)
Referral to treatment (percentage within 18 weeks) - admitted performance
Cancelled operations
A last-minute cancellation is a cancellation for non-clinical reasons on the day the patient was due
to arrive, after they have arrived in hospital or on the day of their operation. If a patient has not
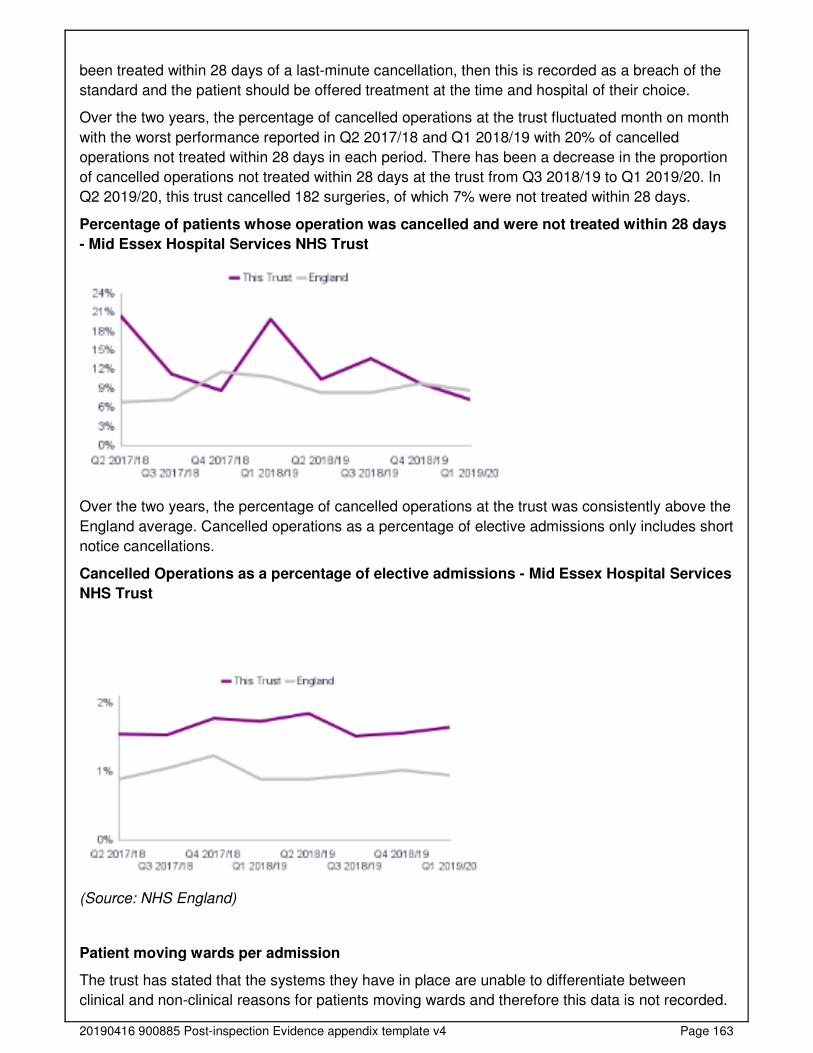
20190416 900885 Post-inspection Evidence appendix template v4 Page 163
been treated within 28 days of a last-minute cancellation, then this is recorded as a breach of the
standard and the patient should be offered treatment at the time and hospital of their choice.
Over the two years, the percentage of cancelled operations at the trust fluctuated month on month
with the worst performance reported in Q2 2017/18 and Q1 2018/19 with 20% of cancelled
operations not treated within 28 days in each period. There has been a decrease in the proportion
of cancelled operations not treated within 28 days at the trust from Q3 2018/19 to Q1 2019/20. In
Q2 2019/20, this trust cancelled 182 surgeries, of which 7% were not treated within 28 days.
Percentage of patients whose operation was cancelled and were not treated within 28 days
- Mid Essex Hospital Services NHS Trust
Over the two years, the percentage of cancelled operations at the trust was consistently above the
England average. Cancelled operations as a percentage of elective admissions only includes short
notice cancellations.
Cancelled Operations as a percentage of elective admissions - Mid Essex Hospital Services
NHS Trust
(Source: NHS England)
Patient moving wards per admission
The trust has stated that the systems they have in place are unable to differentiate between
clinical and non-clinical reasons for patients moving wards and therefore this data is not recorded.
20190416 900885 Post-inspection Evidence appendix template v4 Page 164
(Source: Routine Provider Information Request (RPIR) – Ward moves tab)
Patient moving wards at night
From August 2018 to July 2019, there were 673 patients moving wards at night within surgery. Of
these, 672 occurred at Broomfield Hospital. The wards with the highest number of patient ward
moves at night were the surgical emergency ward with 285 ward moves, Notley ward with 113
ward moves and Billericay ward with 80 ward moves.
(Source: Routine Provider Information Request (RPIR) – Moves at night tab)
We could not gain accurate assurances that people could access the service when they needed it
and receive the right care promptly. Waiting times from referral to treatment (RTT) were not
externally reported at the time of our inspection. From 2018 to 2019, the trust implemented an
electronic patient record system which caused data validity issues and poor quality data. With
agreement from NHS England the trust were excluded from reporting data until they had
completed a review and data cleansing exercise.
Locally, managers told us waiting times were being monitored. However, at the time of our
inspection local leaders were unable to provide us with data to evidence the percentages of harm
reviews or whether the service were meeting the national targets.
Following our inspection we requested data from the senior leadership team We reviewed the data
that was provided, we were not able to analyse trends on unvalidated data. Senior leaders told us
patients that were not able to access services within national targets, received a harm review and
were reported to board in common meetings. They also told us that until they returned to reporting
(scheduled April 2020) ‘shadow reporting’ was in place, which included monthly review meetings
with NHS Improvement/England and commissioners.
Managers monitored waiting times and made sure patients could access emergency services
when needed and received treatment within agreed timeframes and national targets. Theatre lists
were managed in advance using an electronic tool to assess utilisation. Previously, staff described
that lists were frequently overbooked, leading to late finishing for staff, In response to this, staff
challenge consultant surgeons in advance, with evidence to show the impact of over booking lists
to prevent over booking and subsequent lists over running. Staff reported a significant
improvement in late finishes over recent months.
After our inspection we requested theatre utilisation data. Senior staff monitored data to try and
ensure that theatres were utilised in an efficient way. Data showed from April 2019 to September
2019 theatres were utilised 72% to 78% of the time. However, future alignment and improved
utilisation was a focus upon merging with other NSH trusts in April 2020.
On a daily basis at 2.30pm, the next day’s lists were reviewed, enabling staff to pull forward
planned work or accommodate emergency surgery if cancellations occurred.
However, staff with theatres expressed concerns about the frequent overrunning of elective
surgery lists. They described overruns being problematic as they often led to a delay in the theatre
lists for emergency patients.
Staff also described challenges around capacity as Lister Ward (previously surgical) had been
relocated to medical care therefore placing pressure on current bed capacity.
Managers and staff worked to make sure patients did not stay longer than they needed to.
Discharge planning was discussed at regular intervals, with forward planning and estimation of

20190416 900885 Post-inspection Evidence appendix template v4 Page 165
when patients may be fit for discharge. However, out of 21 records we reviewed, four records did
not contain a completed discharge checklist.
Whilst most patients were discharged from the ward, the service had access to a discharge lounge
if required. Staff described difficulties with timely discharge when waiting for confirmation of social
and reablement care in the community. At the time of our inspection, one patient on the ward had
been waiting seven days for a social care package to be put in place.
Managers worked to keep the number of cancelled operations to a minimum. We spoke with
theatre services managers during our inspection. In response to cancelled operations, theatre lists
were reviewed in advance, and a work stream was in place to decrease cancelled operations. The
work stream had demonstrated a month on month reduction in cancellations. Staff had recognised
a proportion of cancellations were at short notice due to coughs and colds. In response to this,
staff called patients one to two days prior to surgery to reduce the risk of short notice cancellation
due to coughs and colds. Therefore, vacant slots could be allocated elsewhere, improving theatre
productivity.
When patients had their operations cancelled at the last minute, managers made sure they were
rearranged as soon as possible and within national targets and guidance. Senior nursing staff
within the surgery division spoke with patients who had operations cancelled at short notice. All
patients were rebooked at the earliest opportunity, some being offered a new date on the day of
cancellation. The service had a work stream in place which was demonstrating month on month
reduction in cancellations.
National targets state that patients should begin their first treatment for cancer within 62 days,
following an urgent GP referral for suspected cancer. After our inspection we requested 62 day
standard data which can be seen in the table below:
Oct 18
Nov 18
Dec 18
Jan 19
Feb 19
Mar 19
Apr 19
May 19
Jun 19
Jul 19
Aug 19
Sep 19
Performance 69.5%
64.4%
69.8% 55.2% 67.2%
66.4%
71.8%
67.9% 59.8% 59.1% 59.9%
60.2%
Patients within 62 days
91 65 75 66.5 55.5 73 94 84.5 65.5 69.5 72.5 62
Patients above 62 days
40 36 32.5 54 32.5 37 37 40 44 48 48.5 41
Total Patients
131 101 107.5 120.5 99 110 131 124.5 109.5 117.5 121 103
As data shows, the service did not see 95% of patients within the recommended national 62 day
cancer treatment timeframe.
The service moved patients only when there was a clear medical reason or in their best interest.
There had been no occasions in the last 12 months where intensive care patients had been cared
for within recovery areas to create capacity for patients in intensive care in the last 12 months.
Staff could not always avoid moving patients between wards at night. A proportion of patient were
admitted to the service from the emergency department, for example, fracture neck of femur (hip).
As a result, the pathways in place sometimes meant that patients were required to move due to
capacity. Locally, senior managers were aware of keeping night moves to a minimum, where
possible.

20190416 900885 Post-inspection Evidence appendix template v4 Page 166
Staff planned patients’ discharge carefully, particularly for those with complex mental health and
social care needs. Staff regularly reviewed patients awaiting discharge with involvement of other
healthcare professional such as physiotherapists, occupational therapists and social services.
Staff supported patients when they were referred or transferred between services.
Managers made sure they had arrangements for surgical staff to review any surgical patients on
non-surgical wards. Surgical outlier patients (those not placed on surgical wards) were regularly
reviewed both locally and at trust-wide bed meetings to ensure that patients were identified and
reviewed on a regular basis. Manager worked to minimise the number of surgical patients on non-
surgical wards, where possible.
Senior staff within the service described challenges around patient access to services including
endoscopy. In response to this, a capacity and demand model had recently been completed,
which led to consideration of weekend opening. At the time of our inspection, this was in the
process of discussion.
During our inspection we saw that the theatre recovery area was staffed overnight between the
days of Monday to Wednesday. Staff expressed concerns that patients were regularly exposed to
prolonged stays within this area if beds were not available within the hospital. During our
inspection, we saw that one patient had been within the recovery area for 20 hours.
Learning from complaints and concerns
It was easy for people to give feedback and raise concerns about care received. The
service treated concerns and complaints seriously, investigated them and shared lessons
learned with all staff. The service included patients in the investigation of their complaint.
Summary of complaints
Broomfield Hospital
From August 2018 to July 2019, the trust received 137 complaints in relation to surgery at
Broomfield Hospital (23.1% of the total complaints received by the trust). The trust took an
average of 37.2 days to investigate and close complaints. This was not in line with their complaints
policy, which states complaints should be completed within 25 working days
A breakdown of complaints by type is shown below:
Type of complaint Number of complaints Percentage of total Clinical treatment - surgical group 104 75.9% Communications 8 5.8%
Appointments including delays and cancellations
8 5.8%
Clinical treatment - general medicine group 5 3.6% Values and behaviours (staff) 4 2.9% Clinical treatment - obstetrics and gynaecology 2 1.5% Clinical treatment - anaesthetics 2 1.5% Facilities services (including; access for people with disability, cleanliness, food, parking, maintenance and portering)
1 0.7%
Admissions, discharge and transfer arrangements excluding delays due to absence of care package
1 0.7%
Clinical treatment - accident and emergency 1 0.7%
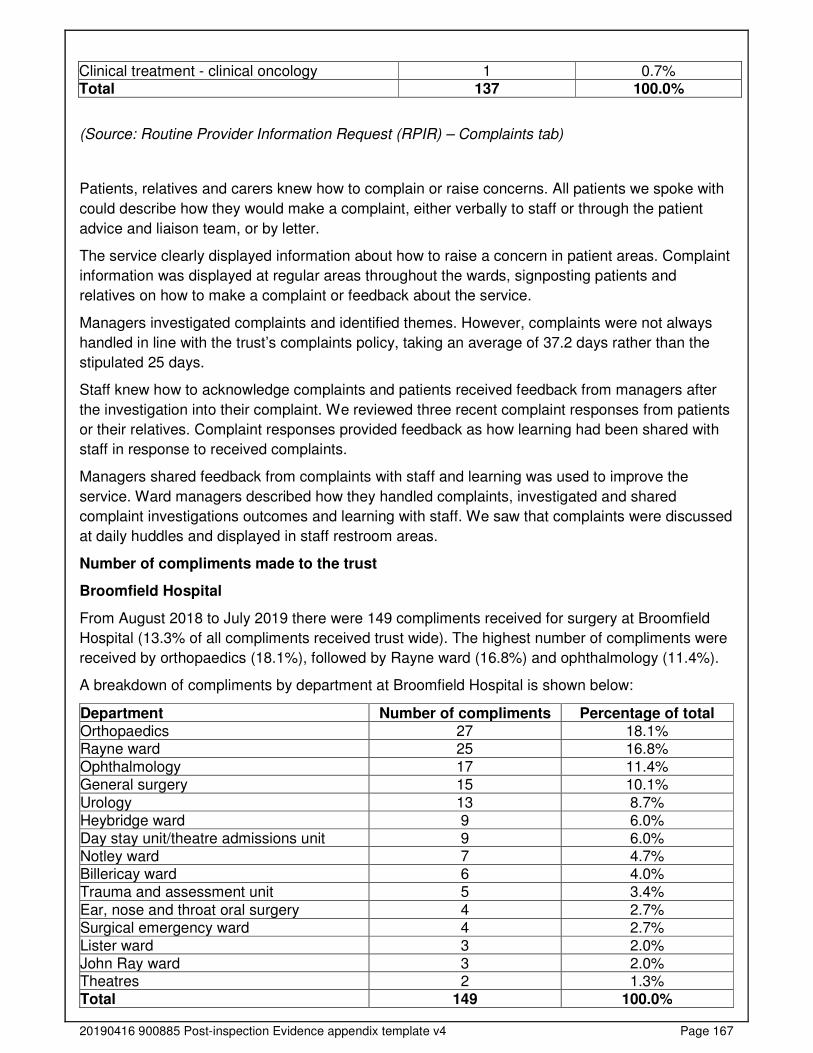
20190416 900885 Post-inspection Evidence appendix template v4 Page 167
Clinical treatment - clinical oncology 1 0.7% Total 137 100.0%
(Source: Routine Provider Information Request (RPIR) – Complaints tab)
Patients, relatives and carers knew how to complain or raise concerns. All patients we spoke with
could describe how they would make a complaint, either verbally to staff or through the patient
advice and liaison team, or by letter.
The service clearly displayed information about how to raise a concern in patient areas. Complaint
information was displayed at regular areas throughout the wards, signposting patients and
relatives on how to make a complaint or feedback about the service.
Managers investigated complaints and identified themes. However, complaints were not always
handled in line with the trust’s complaints policy, taking an average of 37.2 days rather than the
stipulated 25 days.
Staff knew how to acknowledge complaints and patients received feedback from managers after
the investigation into their complaint. We reviewed three recent complaint responses from patients
or their relatives. Complaint responses provided feedback as how learning had been shared with
staff in response to received complaints.
Managers shared feedback from complaints with staff and learning was used to improve the
service. Ward managers described how they handled complaints, investigated and shared
complaint investigations outcomes and learning with staff. We saw that complaints were discussed
at daily huddles and displayed in staff restroom areas.
Number of compliments made to the trust
Broomfield Hospital
From August 2018 to July 2019 there were 149 compliments received for surgery at Broomfield
Hospital (13.3% of all compliments received trust wide). The highest number of compliments were
received by orthopaedics (18.1%), followed by Rayne ward (16.8%) and ophthalmology (11.4%).
A breakdown of compliments by department at Broomfield Hospital is shown below:
Department Number of compliments Percentage of total Orthopaedics 27 18.1% Rayne ward 25 16.8% Ophthalmology 17 11.4% General surgery 15 10.1%
Urology 13 8.7% Heybridge ward 9 6.0% Day stay unit/theatre admissions unit 9 6.0% Notley ward 7 4.7% Billericay ward 6 4.0% Trauma and assessment unit 5 3.4%
Ear, nose and throat oral surgery 4 2.7% Surgical emergency ward 4 2.7% Lister ward 3 2.0% John Ray ward 3 2.0% Theatres 2 1.3% Total 149 100.0%
20190416 900885 Post-inspection Evidence appendix template v4 Page 168
The trust stated that most of the compliments received related to overall care along the whole
pathway with patients and relatives thanking staff for their kindness and compassion during
difficult and stressful times. These related to all staff from housekeepers, porters and nurses to
consultants.
Compliments and the associated learning and sharing of good practice is discussed at the patient
and carer experience group and also with individuals and their managers during appraisal. The
trust uses its Datix system to analyse themes from compliments.
(Source: Routine Provider Information Request (RPIR) – Compliments tab)
Is the service well-led?
Leadership
Leaders had the skills and abilities to run the service. They understood and managed the
priorities and issues the service faced. They were visible and approachable in the service
for patients and staff. They supported staff to develop their skills and take on more senior
roles.
Surgery was located in the surgical, anaesthetics and theatres division which encompassed:
general surgery, specialist surgery (ophthalmology, oral maxillofacial surgery (OMFS), ear nose
and throat (ENT) and audiology, musculoskeletal (MSK - trauma and orthopaedics and
rheumatology), anaesthetics, theatres and critical care and surgical specialities with endoscopy
(upper and lower gastrointestinal, colorectal, breast, vascular and urology.
The divisional director, associate director of operation and two associate directors of nursing
oversaw the division and in turn reported to the executive team.
Locally, both theatres and surgical wards were led by matrons who were supported by ward
managers, who in turn supported ward and theatre based staff.
The divisional leads told us they felt well supported by the executive team. However, some staff
within the surgical division reported a lack of visibility and support from the executive team and
that concerns were not always listened too or acted upon. Concerns centred around a feeling that
the executive team were focused on the upcoming merger, rather than current issues within the
department. Staff expressed concerns that ‘goodwill’ was running out, and a focus was put on
financial targets rather that patients and staff. Other staff described a ‘gap’ in access to the
executive team.
Vision and strategy
The service had a vision for what it wanted to achieve and a strategy to turn it into action,
developed with all relevant stakeholders. The vision and strategy were focused on
sustainability of services and aligned to local plans within the wider health economy.
Leaders and staff understood and knew how to apply them and monitor progress.
At the time of our inspection, Mid Essex Hospital Service was planning to become one new single
NHS Organisation in conjunction with two other local NHS trusts, by an expected date of 1 April
2020. The vision included running all three hospitals under one leadership team.
20190416 900885 Post-inspection Evidence appendix template v4 Page 169
Staff we spoke with were aware of the strategy and recognised the challenges that this strategy
posed and staff within the service felt passionate about providing the best care possible. Staff
described future plans for more cohesive working with other local NHS trust staff.
Part of the merger included Mid Essex hospital becoming the major elective surgical site for the
three hospitals.
The trust’s vision was: ‘to be a healthcare organisation that puts patient care first and whose
reputation for excellence and innovation inspires our patients, staff and the population we serve’.
The service’s values underpinned the vision and in 2015 the following values statement was
agreed; ‘We are a kind, professional, positive team’.
During our inspection we saw that staff demonstrated the service’s values through their course of
work. Patient feedback also described staff as adhering to the vision and values statement.
The service had a cancer improvement plan in place and was working in collaboration with other
stakeholders and the East of England Cancer Alliance.
Culture
Staff mostly felt respected, supported and valued. However, the service promoted equality
and diversity in daily work and provided opportunities for career development. The service
had an open culture where patients and their families could raise concerns without fear.
The majority of staff described an open culture, feeling they could raise concerns without a fear of
reprisal. However, there were some staff who did not feel supported by the senior leadership
team.
There was a strong focus on recruiting, retaining and developing staff currently in employment. At
ward level, senior nursing staff were passionate about create a nurturing environment to support
and develop staff knowledge and expertise.
In the theatre department, a focus had been placed on improving the culture which historically had
been poor due to the attitude of some clinicians. Senior nursing staff described an ‘open door’
policy to improve their visibility to staff within the service. All nursing staff we spoke with described
feeling well supported by senior leaders, describing them as ‘supportive and helpful’.
As identified at our previous inspection in September 2018, concerns were highlighted around
medical staff displaying behaviours that prohibited a positive safety culture. Whilst overall culture
had improved, some staff’s compliance with venous thromboembolism risk assessments and
thorough completion of the World Health Organisation (WHO) checklist still showed room for
improvement.
Senior staff had identified ‘group quality priorities 2019/2020’, aiming for zero tolerance of never
events and increased focus to sharing learning at cross site level, in particular from previous never
events.
In April 2019, the trust introduced a new external guardian service, providing staff with a
confidential and independent opportunity to raise concerns therefore ensuring anonymity. The
external service reported back to the trust’s organisational development committee with
information for staff being shared on the trust’s intranet, on corporate induction days and through
leaflets and staff events.
20190416 900885 Post-inspection Evidence appendix template v4 Page 170
Governance
We could not gain assurance that leaders always operated effective governance processes
throughout the service. Staff at all levels were clear about their roles and accountabilities
and had regular opportunities to meet, discuss and learn from the performance of the
service, however, performance did not always show steady and sustainable signs of
improvement.
Clinical governance meetings took place on a monthly basis for anaesthetics and theatres,
musculoskeletal surgery, specialist surgery and general surgery. We reviewed meeting minutes for
October 2019 and saw meetings were generally well attended. Meeting minutes discussed a
number of topics including but not limited to; workforce, mandatory training and incidents.
For the month of October 2019, meeting minutes highlighted that there were 241 incidents classed
as requiring investigation or closure. We could not gain assurances that incidents were
investigated in a timely manner.
General surgical audit meetings took place on a monthly basis and offered local medical students
the opportunity to attend.
However, a number of areas of concern remained from our previous inspection in October 2018.
Issues included; poor medical records documentation and poor infection prevention and control
processes. We could not gain assurances that there were effective governance processes in place
to embed and sustain improvement in performance.
Management of risk, issues and performance
Leaders and teams used systems to manage performance effectively. However, not all risks
were identified and escalated with identified actions to reduce their impact.
The surgical division held and maintained an electronic risk register. Top risks included but were
not limited to; nurse staffing, junior doctor staffing, late notice cancellations of surgery and the
inability to accommodate elective and non-elective surgical patient in an appropriate environment.
Risks were RAG (red, amber, green) rated to indicate the level risks posed. Each risk had a
named lead, detailed actions taken to mitigate risk and when further review was due.
However, areas of poor compliance with medical record completion was not identified as a risk on
the risk register. This had been identified at our previous inspection in October 2018. In addition,
infection prevention and control concerns within the theatre department were not identified as a
risk.
Cramped condition within theatre changing areas were not reflected on the service’s risk register.
The services top five theatre risks were displayed in staff areas:
• Overbooked theatre lists
• Day surgery Unit – use as a contingency area
• A lack of patient pre-assessment
• Availability of pharmacy medicines
• Ageing instruments (a repair and replacement programme was in progress at the time of
our inspection).
20190416 900885 Post-inspection Evidence appendix template v4 Page 171
Compliance with completion of venous thromboembolism (VTE) risk assessments had been
identified by senior staff as a risk to the service. In response to this, a ‘focus month’ took place in
June 2019 in the aim of improving awareness with staff. Learning was shared through a variety of
methods including but not limited to; trust safety alerts, governance meetings and patient safety
meetings. Whilst VTE risk assessment compliance was not meeting the 95% target, it is to be
noted that data showed an improvement in performance from March 2019, however, this was not
reflected on the service’s risk register.
We could not gain accurate assurances that people could access the service when they needed it
and receive the right care promptly. Waiting times from referral to treatment (RTT) were not
externally reported at the time of our inspection. From 2018 to 2019, the trust implemented an
electronic patient record system which caused data validity issues and poor quality data. With
agreement from NHS England the trust were excluded from reporting data until they had
completed a review and data cleansing exercise.
Locally, managers told us waiting times were being monitored. However, at the time of our
inspection local leaders were unable to provide us with data to evidence the percentages of harm
reviews or whether the service were meeting the national targets.
Following our inspection we requested data from the senior leadership team We reviewed the data
that was provided, we were not able to analyse trends on unvalidated data. Senior leaders told us
patients that were not able to access services within national targets, received a harm review and
were reported to board in common meetings. They also told us that until they returned to reporting
(scheduled April 2020) ‘shadow reporting’ was in place, which included monthly review meetings
with NHS Improvement/England and commissioners. Electronic scorecards (broken down to
surgery and theatre/anaesthetic areas) enabled senior staff to oversee and monitor key safety
information including but not limited to; serious incidents, falls resulting in injury and pressure
ulcers. Senior staff attended monthly meetings to discuss dashboard data.
The service carried out regular audits to monitor performance, including but not limited to;
controlled drugs storage, transient workers, drug trolley and VTE risk assessments.
At our previous inspection in October 2018, incomplete records, poor compliance with venous
thromboembolism risk assessment completion, infection prevention control processes and
mandatory training compliance were previously identified as a risk. Whilst mandatory training
compliance had improved, issues still remained around IPC processes, medical records
documentation and VTE assessment completion. Therefore we could not gain assurances that
effective governance frameworks and oversight of risk were in place to enable sustained changes
and improvements.
Information management
The service did not always collect reliable data and analyse it. Staff could not always find
the data they needed, in easily accessible formats, to understand performance, make
decisions and improvements. Information systems were not always integrated but were
secure. Data or notifications were not always consistently submitted to external
organisations as required.
In May 2017, a new electronic patient record system led to problems with accurately tracking
patients and capturing validated accurate referral to treatment (RTT) data. At the time of our
inspection, RTT formal data submission was not taking place (ceased in January 2018 with the
20190416 900885 Post-inspection Evidence appendix template v4 Page 172
support from NHS England), however, the trust had implemented a number of local measures to
monitor RTT times. All patients who did not meet RTT were reviewed for harm.
However, the electronic system for patient records did not communicate with the system used to
track and maintain patient flow, therefore leading to difficulties. In response to this the trust had
implemented an interim director for improvement, who commenced in post in October 2019.
In addition, senior staff told us that records relating to mandatory training compliance were not
always accurate. For example, medical staffing records contained staff that had left the service,
leading to possible inaccurate data.
Engagement
Leaders and staff actively and openly engaged with patients and staff. They collaborated
with partner organisations to help improve services for patients.
Senior staff welcomed feedback from staff and described ‘open door’ policies. Staff within the
theatre department had adopted the ‘Greatex’ system, used so staff could nominate colleagues for
outstanding work or going above and beyond. This had been well received and welcomed by staff.
The service facilitated patient and carer experience groups, enabling feedback about the service.
Listening events provided patients and their relatives/carers with an opportunity to feedback about
their experience.
An Oscar nomination scheme was in use for staff to nominate colleagues for outstanding work or
going above and beyond.
Learning, continuous improvement and innovation
All staff were committed to continually learning and improving services. Leaders
encouraged innovation and participation in research.
Staff from Notley ward were passionate about reducing the number of hospital acquired sacral
pressure ulcers. Previous data showed Notley ward as having a high prevalence of pressure
ulcers in the last two years. In response to findings the ‘react to red’ project was trialled from July
2019 to August 2019 which focussed on the prevention of sacral pressure ulcers using
preventative sacrum dressings for patients with fractured neck of femur (hip). Results were
positive, with no patients in the trial acquiring a sacral pressure ulcer.
The service offered a one-stop clinic for lower limb care and treatment as this had been identified
as being underutilised.
The service had expanded the number of robotic procedures on offer which included; upper
gastrointestinal, colorectal, urology and head and neck surgery.

20190416 900885 Post-inspection Evidence appendix template v4 Page 173
Maternity
Facts and data about this service
Mid Essex Hospital Services NHS Trust provides a range of hospital and community-based
maternity services across three sites; Broomfield Hospital in Chelmsford, St Peter’s Hospital in
Maldon and St Michael’s Hospital (also known as William Julien Courtauld Hospital) in Braintree.
The trust has 62 maternity beds.
Broomfield Hospital provides consultant and midwife led care for high and low risk women.
Inpatient maternity services include a consultant led delivery suite, midwife led birthing suite and
postnatal ward. Delivery suite has 10 ensuite delivery rooms, one bereavement suite and two
dedicated obstetric theatres. The birthing suite has four delivery rooms, two of which have static
birthing pools. The postnatal ward has 20 beds. There is also a 14-bedded antenatal day
assessment unit open 24 hours a day, seven days a week. Outpatient maternity services are
provided on the hospital site and in conjunction with community services.
St Peter’s Hospital and St Michael’s Hospital both have birthing centres which provide midwife led
care to women with uncomplicated pregnancies and labours. The birthing centres also act as hubs
for community and acute outreach provision, including consultant led clinics.
There are three community midwifery teams based at each hospital site. They provide antenatal
and postnatal care from GP surgeries, children’s centres and birthing centres, as well as home
visits. A home birth service is also available.
From August 2018 to July 2019 there were 4,300 deliveries at the trust. The number of deliveries
per location is show below:
• 3,192 (74.2%) - Broomfield Hospital consultant led unit
• 682 (15.9%) - Broomfield Hospital midwife led birthing suite
• 107 (2.5%) - Home births
• 138 (3.2%) - St Peter’s midwife led birthing centre
• 181 (4.2%) - St Michael’s midwife led birthing centre
(Source: Routine Provider Information Request (RPIR) – Maternity overview)
From January to December 2018 there were 3,941 deliveries at the trust.
A comparison from the number of deliveries at the trust and the national totals during this period is
shown below.

20190416 900885 Post-inspection Evidence appendix template v4 Page 174
Number of deliveries at Mid Essex Hospital Services NHS Trust – Comparison with other
trusts in England.
(Source: Hospital Episode Statistics (HES))
A profile of all deliveries and gestation periods from January to December 2018 can be seen in the
tables below. Both the profile of deliveries in terms of single and multiple births and profile of
mother’s age was similar at the trust when compared with the England average.
Notes: A single birth includes any delivery where there is no indication of a multiple birth. This table does not
include deliveries where delivery method is 'other' or 'unrecorded'.

20190416 900885 Post-inspection Evidence appendix template v4 Page 175
Notes: This table does not include deliveries where delivery method is 'other', 'Missing' or 'unrecorded'.
We inspected inpatient, outpatient and community maternity services provided at Broomfield
Hospital on 5 to 7 November 2019. We did not inspect the maternity services located at St Peter’s
Hospital and St Michael’s Hospital. We visited:
• Antenatal clinic (A401)
• Delivery suite (A402); including obstetric theatres and recovery area, and the midwifery led
birthing unit
• Antenatal day assessment unit (A404)
• Postnatal ward (A405)
• Early pregnancy assessment unit
At the last inspection in June 2016, we rated the maternity and gynaecology service good for all
five key questions (safe, effective, caring, responsive and well-led). Since then the inspection
methodology has changed. We no longer inspect maternity jointly with gynaecology, so we cannot
compare our new ratings directly with previous ratings. This is the first inspection of maternity as a
single core service.
Our inspection was announced (staff knew we were coming) because of the number of core
services we inspected. We also returned for an unannounced inspection (staff did not know we
were coming) to enable us to observe routine activity. Before the inspection visit, we reviewed
information that we held about the service and information requested from the trust, including
performance data, policies and meeting minutes.
During our inspection visit, the inspection team:
• Spoke with 10 women who were using the service and one partner
• Spoke with 54 staff members; including midwives, doctors, managers, specialist midwives and
maternity care assistants
• Observed two handover meetings
• Observed the environment and care provided to women and their babies
• Reviewed 21 maternity care records and 22 prescription charts.
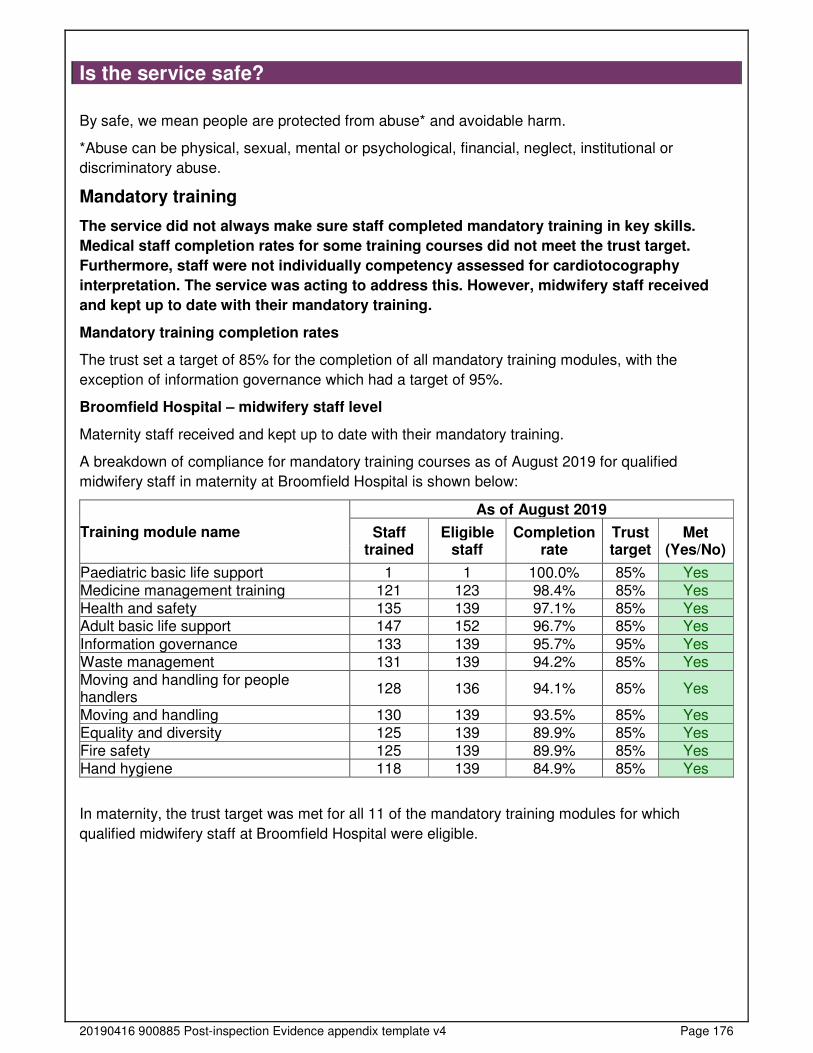
20190416 900885 Post-inspection Evidence appendix template v4 Page 176
Is the service safe?
By safe, we mean people are protected from abuse* and avoidable harm.
*Abuse can be physical, sexual, mental or psychological, financial, neglect, institutional or
discriminatory abuse.
Mandatory training
The service did not always make sure staff completed mandatory training in key skills.
Medical staff completion rates for some training courses did not meet the trust target.
Furthermore, staff were not individually competency assessed for cardiotocography
interpretation. The service was acting to address this. However, midwifery staff received
and kept up to date with their mandatory training.
Mandatory training completion rates
The trust set a target of 85% for the completion of all mandatory training modules, with the
exception of information governance which had a target of 95%.
Broomfield Hospital – midwifery staff level
Maternity staff received and kept up to date with their mandatory training.
A breakdown of compliance for mandatory training courses as of August 2019 for qualified
midwifery staff in maternity at Broomfield Hospital is shown below:
Training module name
As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Paediatric basic life support 1 1 100.0% 85% Yes Medicine management training 121 123 98.4% 85% Yes Health and safety 135 139 97.1% 85% Yes Adult basic life support 147 152 96.7% 85% Yes
Information governance 133 139 95.7% 95% Yes Waste management 131 139 94.2% 85% Yes Moving and handling for people handlers
128 136 94.1% 85% Yes
Moving and handling 130 139 93.5% 85% Yes Equality and diversity 125 139 89.9% 85% Yes Fire safety 125 139 89.9% 85% Yes Hand hygiene 118 139 84.9% 85% Yes
In maternity, the trust target was met for all 11 of the mandatory training modules for which
qualified midwifery staff at Broomfield Hospital were eligible.
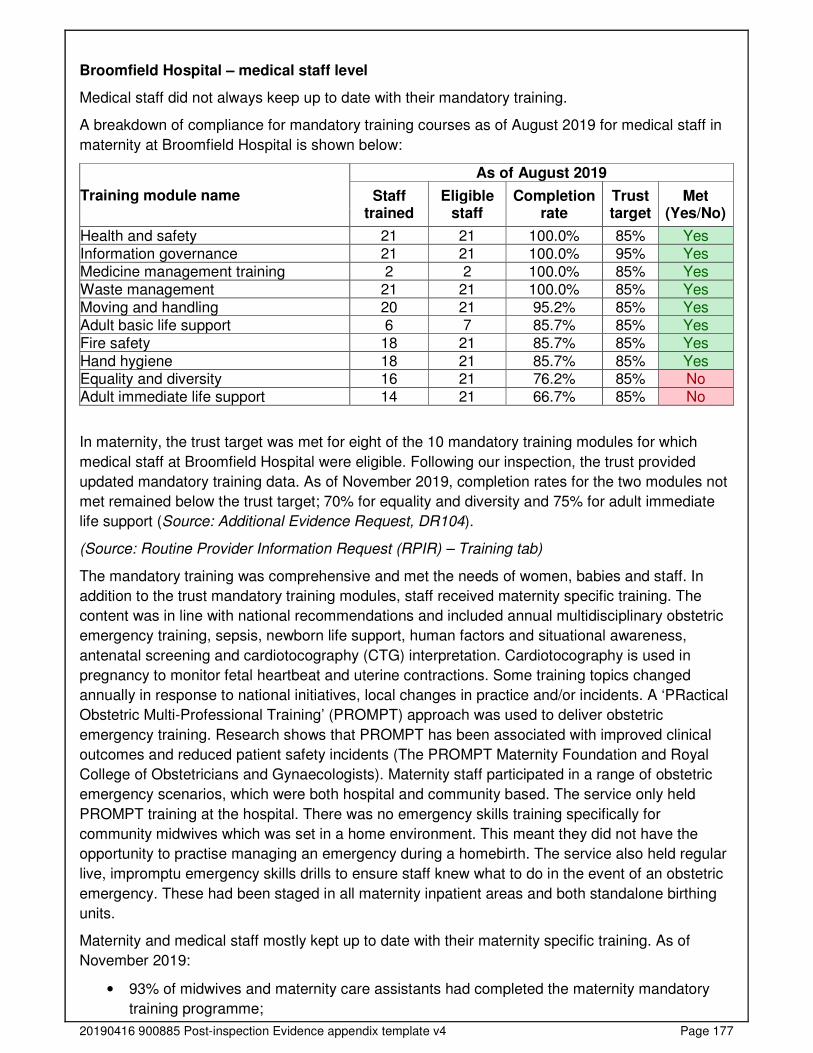
20190416 900885 Post-inspection Evidence appendix template v4 Page 177
Broomfield Hospital – medical staff level
Medical staff did not always keep up to date with their mandatory training.
A breakdown of compliance for mandatory training courses as of August 2019 for medical staff in
maternity at Broomfield Hospital is shown below:
Training module name
As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Health and safety 21 21 100.0% 85% Yes Information governance 21 21 100.0% 95% Yes Medicine management training 2 2 100.0% 85% Yes Waste management 21 21 100.0% 85% Yes Moving and handling 20 21 95.2% 85% Yes Adult basic life support 6 7 85.7% 85% Yes Fire safety 18 21 85.7% 85% Yes
Hand hygiene 18 21 85.7% 85% Yes Equality and diversity 16 21 76.2% 85% No Adult immediate life support 14 21 66.7% 85% No
In maternity, the trust target was met for eight of the 10 mandatory training modules for which
medical staff at Broomfield Hospital were eligible. Following our inspection, the trust provided
updated mandatory training data. As of November 2019, completion rates for the two modules not
met remained below the trust target; 70% for equality and diversity and 75% for adult immediate
life support (Source: Additional Evidence Request, DR104).
(Source: Routine Provider Information Request (RPIR) – Training tab)
The mandatory training was comprehensive and met the needs of women, babies and staff. In
addition to the trust mandatory training modules, staff received maternity specific training. The
content was in line with national recommendations and included annual multidisciplinary obstetric
emergency training, sepsis, newborn life support, human factors and situational awareness,
antenatal screening and cardiotocography (CTG) interpretation. Cardiotocography is used in
pregnancy to monitor fetal heartbeat and uterine contractions. Some training topics changed
annually in response to national initiatives, local changes in practice and/or incidents. A ‘PRactical
Obstetric Multi-Professional Training’ (PROMPT) approach was used to deliver obstetric
emergency training. Research shows that PROMPT has been associated with improved clinical
outcomes and reduced patient safety incidents (The PROMPT Maternity Foundation and Royal
College of Obstetricians and Gynaecologists). Maternity staff participated in a range of obstetric
emergency scenarios, which were both hospital and community based. The service only held
PROMPT training at the hospital. There was no emergency skills training specifically for
community midwives which was set in a home environment. This meant they did not have the
opportunity to practise managing an emergency during a homebirth. The service also held regular
live, impromptu emergency skills drills to ensure staff knew what to do in the event of an obstetric
emergency. These had been staged in all maternity inpatient areas and both standalone birthing
units.
Maternity and medical staff mostly kept up to date with their maternity specific training. As of
November 2019:
• 93% of midwives and maternity care assistants had completed the maternity mandatory
training programme;
20190416 900885 Post-inspection Evidence appendix template v4 Page 178
• 95.4% of midwives and 100% of medical staff had completed PROMPT;
• 97.1% of midwives and 78.9% of medical staff had completed annual CTG training;
• 90% of midwives and medical staff had completed newborn life support training
(Source: Additional Evidence Request, DR72 to DR75).
Senior staff told us the four doctors who were not up to date with CTG training had completed it,
but they had not yet seen evidence to confirm this when we requested this information. However,
we found staff were not individually competency assessed for CTG interpretation. The service
assessed CTG competency through a group interactive session. This was not in line with national
recommendations (NHS England, Saving Babies’ Lives Version Two: A care bundle for reducing
perinatal mortality (March 2019)). We raised this with managers who took immediate action to
address this concern. When we returned for the unannounced inspection, managers told us they
had introduced an individual CTG competency assessment which eligible staff completed when
they attended their maternity specific training. Managers told us they hoped to introduce a full-day
dedicated to CTG training and a compulsory on-line competency assessment for eligible staff.
Clinical staff completed training on recognising and responding to women with mental health
needs, learning disabilities and autism. Topics covered included maternal mental health disorders,
risk assessment and referral pathways.
Managers monitored mandatory training and alerted staff when they needed to update their
training. Staff could monitor their own training needs through the trust’s electronic system, which
sent an email alert when due. The practice development midwife had oversight of training needs
and completion rates, which they monitored monthly. They were supported by two clinical
facilitators. Staff who needed to update their training were booked on the next available course.
Safeguarding
Staff understood how to protect women and babies from abuse and worked well with other
agencies to do so. However, medical staff completion rates for safeguarding adults training
courses did not meet the trust target. Furthermore, not all staff were aware of the abduction
policy. This meant there was a risk that some staff would not know what to do if a baby was
abducted from the maternity unit.
Staff received safeguarding training specific for their role on how to recognise and report abuse.
Safeguarding training was delivered in line with national recommendations and included scenario-
based discussion and learning from incidents and serious case reviews. The training programme
included professional responsibilities, categories of abuse, safeguarding processes, female genital
mutilation (FGM), child sexual exploitation (CSE), domestic violence and preventing radicalisation.
Staff said they learned from safeguarding training and put what they learned into practice.
However, completion rates for some safeguarding training modules was below the trust target. All
registered professionals working in direct contact with children, young people and families were
required to complete safeguarding children training at level three. This was in line with national
recommendations (RCPCH, Safeguarding Children and Young People; Roles and Competencies
for Healthcare Staff. Intercollegiate Document (January 2019)).
Safeguarding training completion rates
Midwifery staff kept up to date with their safeguarding training however, not all medical staff did.
The trust set a target of 95% for the completion of safeguarding modules.
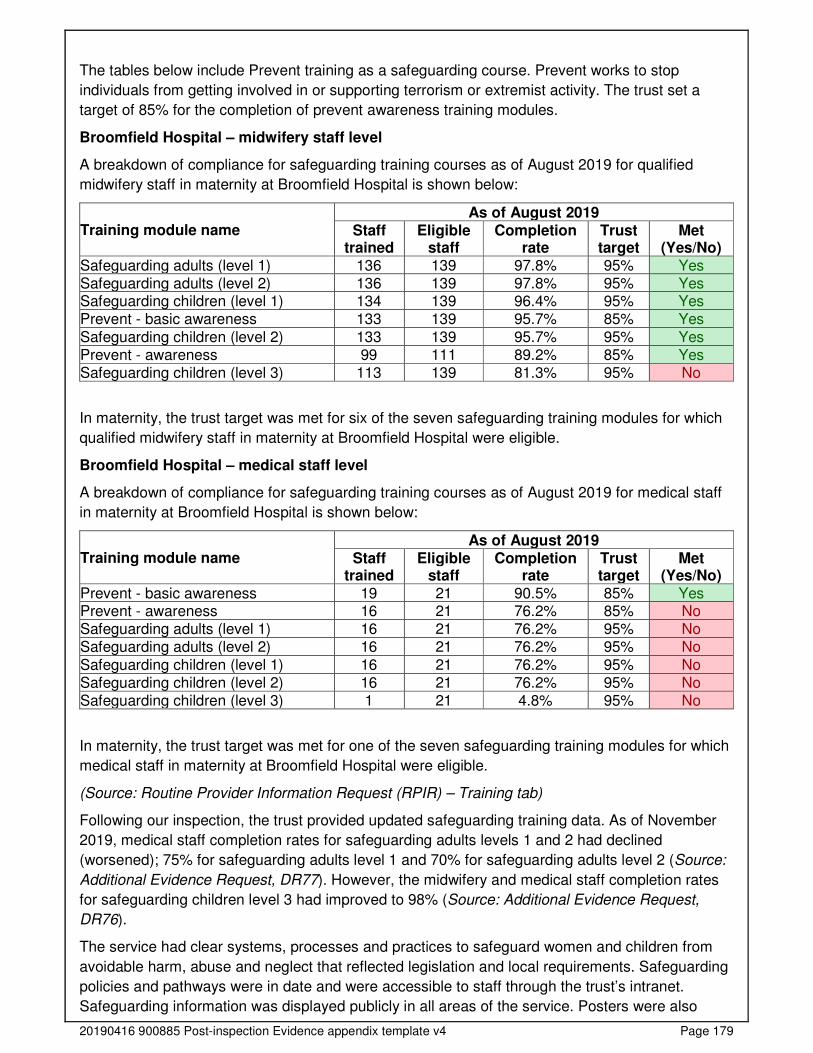
20190416 900885 Post-inspection Evidence appendix template v4 Page 179
The tables below include Prevent training as a safeguarding course. Prevent works to stop
individuals from getting involved in or supporting terrorism or extremist activity. The trust set a
target of 85% for the completion of prevent awareness training modules.
Broomfield Hospital – midwifery staff level
A breakdown of compliance for safeguarding training courses as of August 2019 for qualified
midwifery staff in maternity at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Safeguarding adults (level 1) 136 139 97.8% 95% Yes Safeguarding adults (level 2) 136 139 97.8% 95% Yes Safeguarding children (level 1) 134 139 96.4% 95% Yes Prevent - basic awareness 133 139 95.7% 85% Yes
Safeguarding children (level 2) 133 139 95.7% 95% Yes Prevent - awareness 99 111 89.2% 85% Yes Safeguarding children (level 3) 113 139 81.3% 95% No
In maternity, the trust target was met for six of the seven safeguarding training modules for which
qualified midwifery staff in maternity at Broomfield Hospital were eligible.
Broomfield Hospital – medical staff level
A breakdown of compliance for safeguarding training courses as of August 2019 for medical staff
in maternity at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Prevent - basic awareness 19 21 90.5% 85% Yes Prevent - awareness 16 21 76.2% 85% No Safeguarding adults (level 1) 16 21 76.2% 95% No Safeguarding adults (level 2) 16 21 76.2% 95% No
Safeguarding children (level 1) 16 21 76.2% 95% No Safeguarding children (level 2) 16 21 76.2% 95% No Safeguarding children (level 3) 1 21 4.8% 95% No
In maternity, the trust target was met for one of the seven safeguarding training modules for which
medical staff in maternity at Broomfield Hospital were eligible.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Following our inspection, the trust provided updated safeguarding training data. As of November
2019, medical staff completion rates for safeguarding adults levels 1 and 2 had declined
(worsened); 75% for safeguarding adults level 1 and 70% for safeguarding adults level 2 (Source:
Additional Evidence Request, DR77). However, the midwifery and medical staff completion rates
for safeguarding children level 3 had improved to 98% (Source: Additional Evidence Request,
DR76).
The service had clear systems, processes and practices to safeguard women and children from
avoidable harm, abuse and neglect that reflected legislation and local requirements. Safeguarding
policies and pathways were in date and were accessible to staff through the trust’s intranet.
Safeguarding information was displayed publicly in all areas of the service. Posters were also

20190416 900885 Post-inspection Evidence appendix template v4 Page 180
displayed on the back of toilet doors advising people how to access support if they were
experiencing domestic violence and/or abuse.
Staff could give examples of how to protect women from harassment and discrimination, including
those with protected characteristics under the Equality Act. Staff screened all women for
safeguarding risks. The risk assessment covered all types of abuse such as physical, emotional,
financial and sexual. Women and/or babies found to be at risk of abuse were referred
appropriately for additional care and support as needed.
Staff knew how to identify adults, children and babies at risk of, or suffering, significant harm and
worked with other agencies to protect them. Staff told us they worked collaboratively with health
visitors, GPs, the police, the perinatal mental health team and social workers to protect vulnerable
women and children. We reviewed 21 sets of maternity care records which showed women were
routinely asked about domestic abuse. This was in line with national recommendations (National
Institute for Health and Care Excellence (NICE), domestic violence and abuse: multi-agency
working [PH50] (February 2014). Staff understood their mandatory duty to report all cases of
female genital mutilation (FGM) in girls under the age of 18 and those at risk of FGM being
performed. The Female Genital Mutilation Information Sharing (FGM-IS) system was used by staff
to alert healthcare professionals to girls under the age of 18 who were at risk of FGM. The FGM-IS
is a national electronic system which supports the early intervention and ongoing safeguarding of
girls under the age of 18, who have a family history of FGM.
Staff knew how to make a safeguarding referral and who to inform if they had concerns. Staff we
spoke with were confident to make safeguarding referrals and were able to provide examples of
how they had responded to safeguarding concerns. The trust’s electronic patient record (EPR)
system enabled staff to create an alert for women with safeguarding concerns, and those subject
to a child protection or child in need plan. This meant staff could easily identify when any woman
with known safeguarding concerns attended the service. Individual safeguarding records were
electronic and stored on the EPR system, such as referrals, child protection conference meeting
minutes and management plans. This meant staff had immediate access to up to date
safeguarding information. The trust had a lead midwife for safeguarding who was available to
provide support, supervision, training and updates for staff. Staff could contact the lead midwife for
safeguarding, or other members of the trust’s safeguarding team, if they needed advice and
support with any safeguarding concerns. The lead midwife for safeguarding also visited the wards
daily, Monday to Friday, to support women and staff with any safeguarding concerns.
There were arrangements for safeguarding supervision and peer review. Community midwives
participated in quarterly safeguarding supervision, where they reflected on safeguarding cases to
enhance their knowledge and skills and promote positive outcomes for women and their children.
This was in line with national recommendations (HM Government, Working Together to Safeguard
Children: A guide to interagency working to safeguard and promote the welfare of children (July
2018).
Staff followed safe procedures for children visiting the ward. Women’s and their partners children
only could visit the maternity unit.
The service had an abduction policy, but four out of six staff we spoke with were not aware of it.
Nor had staff undertaken baby abduction drills. This meant there was a risk that some staff may
not know what to do if a baby was abducted from the maternity unit. However, in line with the
trust’s policy, most staff could describe what actions they would take if they suspected a baby had
been abducted. Furthermore, there were measures and controls in place to minimise the risk of a
baby being abducted. Access to and exit from the inpatient wards was by means of swipe card
20190416 900885 Post-inspection Evidence appendix template v4 Page 181
access or an intercom buzzer system. There was also closed-circuit camera television video
(CCTV) at ward entrance and exit points. This meant staff could monitor who was entering and
leaving the wards. Babies had identification labels applied to each ankle after birth to ensure
correct identification of the infant, in case mother and baby were separated at any time. The labels
were checked on transfer to the postnatal ward and then daily by staff as part of the routine
postnatal check. Staff told us if they found a baby with both labels missing they would check the
identity of all babies on the ward to ensure each baby was with their mother. When we returned for
our unannounced inspection, managers told us they had a mock baby abduction exercise planned
for December 2019.
Cleanliness, infection control and hygiene
The service controlled infection risk well. Staff used equipment and control measures to
protect women, babies, themselves and others from infection. However, staff did not
always label equipment to show when they last cleaned it.
Most ward areas were clean and had suitable furnishings which were clean and well-maintained.
However, we found areas in the midwife led birthing suite which were dusty, including a cot and
trolleys where equipment was stored. When we returned for our unannounced inspection, we
found all areas in the midwife led unit were clean.
Cleaning records were up to date and demonstrated that all areas were cleaned regularly. The
service had housekeeping staff who were responsible for cleaning patient and public areas, in
accordance with daily and weekly checklists. Infection prevention and control (IPC) audits were
undertaken and the results were used to improve IPC practice where needed. The trust’s IPC
team audited the antenatal day assessment unit in October 2019 and the delivery suite and
postnatal ward in November 2019. We requested the audit compliance results but were not
provided with these. However, the action plans showed four areas of non-compliance for delivery
suite, six for the postnatal ward and eight for the antenatal day assessment unit. We saw all
actions had been completed (Source: Additional Evidence Request, DR60). Side rooms were
available on the antenatal and postnatal wards, which could be used to admit women with a
known or suspected infection. Staff could describe what they would do if a woman required
isolation due to infection.
Staff told us they cleaned equipment after patient contact. However, they did not always label
equipment to show when it was last cleaned. We saw equipment that was not in use on the
antenatal day assessment unit and midwife led birthing suite was not labelled to show when it had
been cleaned. However, equipment on the postnatal ward and delivery suite was labelled. All the
equipment we saw appeared visibly clean and well-maintained.
Staff followed infection control principles including the use of personal protective equipment (PPE).
There was access to hand washing facilities, hand sanitising gel and PPE, such as gloves and
aprons, in all areas. Community staff carried a supply of IPC equipment for use when they visited
women at home, such as hand sanitising gel, gloves and cleaning wipes. We saw staff washed
their hands before and following patient contact. This was in accordance with national guidance
(National Institute for Health and Care Excellence (NICE), Infection prevention and control: QS61,
Quality statement 3 (April 2014)). Women we spoke with confirmed staff washed their hands.
Hand hygiene audits were completed monthly and the results were used to improve hand hygiene
practice where needed. Audit results for the service showed hand hygiene compliance was
consistently 100% (Source: Additional Evidence Request, DR61). We observed staff adhered to
20190416 900885 Post-inspection Evidence appendix template v4 Page 182
the trust’s ‘arms bare below the elbows’ policy to enable effective hand washing and reduce the
risk of spreading infections.
Managers monitored postnatal readmission rates for infection. From November 2018 to October
2019, 23 women were readmitted within 42 days of delivery because of suspected or known
infection. In relation to the total number of deliveries for this period, this equated to a postnatal
readmission rate of 0.5% for maternal infection (Source: Additional Evidence Rest, DR220).
Women were screened for MRSA during pregnancy if they had an induction of labour, planned or
emergency caesarean section or any risk factors for MRSA. Women were offered treatment before
they had their baby if they screened positive. This was to reduce the risk of developing an infection
in a wound, such as caesarean section scar. From November 2018 to October 2019 compliance
with MRSA screening for women with planned procedures was 96.5% on average. This was in line
with the trust target of 95%. However, compliance for women who underwent emergency
caesarean section was 85.1% on average. Managers had acted to improve compliance. For
example, MRSA swabs and pathology request forms were added to emergency caesarean section
packs (Source: Additional Evidence Request, DR96a and DR96b).
Environment and equipment
The design, maintenance and use of facilities, premises and equipment kept people safe.
Staff managed clinical waste well.
During our announced inspection, we found not all equipment had been safety tested to ensure it
was fit for purpose and safe for patient use. We looked at 33 items of equipment, of which 20 had
either expired safety test dates or had no label to show the item had been safety tested. However,
12 of these items had expired four days before our inspection. We raised this as a concern and
managers told us medical engineers were in the process of safety testing the equipment. When
we returned for our unannounced inspection, we looked at 50 items of equipment all of which had
up to date safety test dates.
Staff carried out daily safety checks of specialist equipment. Staff checked adult and neonatal
emergency equipment daily. We reviewed eight checklists which were mostly completed.
The service had enough suitable equipment to help them to safely care for women and babies.
This included cardiotocograph (CTG) machines (used to monitor fetal heartbeat and uterine
contractions), resuscitaires (used to support newborn babies who may need resuscitation after
delivery) and ultrasound machines. A fetal blood gas analyser was available on delivery suite. This
was in line with national recommendations (Royal College of Obstetricians and Gynaecologists
(RCOG), Safer Childbirth: Minimum Standards for the Organisation and Delivery of Care in Labour
(2007)). Community midwives had the equipment they needed, such as baby scales, carbon
monoxide monitors and Doppler fetal monitors. However, they did not have transcutaneous
bilirubinometers (a non-invasive device used to measure the serum bilirubin level of babies with
suspected jaundice). Staff told us if they suspected jaundice they would refer the baby to the
hospital for testing and paediatric review. We checked a range of consumable items for expiration
dates and all were in-date, such as syringes, needles, dressings and delivery packs. Store rooms
were tidy and well-organised.
Women could reach call bells and staff responded quickly when called. We observed call bells
were answered in a timely manner during the inspection. Women we spoke with told us staff
responded to them quickly when called.
20190416 900885 Post-inspection Evidence appendix template v4 Page 183
The design of the environment followed national guidance. The service had two dedicated
obstetric theatres and recovery area. All maternity departments and wards were situated on the
fourth floor, alongside the neonatal unit. This enabled timely transfer when needed. All the delivery
rooms on the delivery suite and midwifery led birthing suite had ensuite facilities. This was in line
with national guidance (Department of Health (DH), Children, young people and maternity
services. Health Building Note 09-02: Maternity care facilities (2013)). Laboratory facilities with
blood and blood products was available on site. We observed fire exits were kept clear and free
from obstruction.
The service had suitable facilities to meet the needs of women. There were two static birthing
pools in the midwife led birthing suite for women who wanted to labour and/or birth in water.
Staff disposed of clinical waste safely. Waste management was handled appropriately with
separate colour coded arrangements for general waste and clinical waste. Sharps, such as
needles, were disposed of in sharps containers which were dated and labelled with the hospital’s
details for traceability purposes. This was in line with national guidance (Health and Safety
Executive Health and Safety (Sharp Instruments in Healthcare) Regulations 2013: Guidance for
employers and employees (March 2013)). Arrangements for the control of substances hazardous
to health (COSHH) were adhered to. Cleaning equipment was stored securely in locked
cupboards. This meant unauthorised persons could not access hazardous cleaning materials.
Assessing and responding to patient risk
Staff completed and updated risk assessments for each woman and baby and took action
to remove or minimise risks. Staff identified and quickly acted upon women and babies at
risk of deterioration.
There was a designated four-bedded triage unit in the antenatal day assessment unit. This
provided 24-hour assessment, review and care planning for pregnant women from 17 weeks
gestation. Women could telephone for advice if they had any concerns or health issues such as
reduced fetal movements or suspected labour. Staff documented all telephone calls and a full
history was taken using the situation, background, assessment, recommendation (SBAR)
communication tool. If a woman called three times in 24-hours they were invited to the unit for
assessment, as staff recognised that frequent calls could be because of domestic violence or
mental health concerns. Birthing equipment was available in the triage unit if a woman presented
in advanced labour and could not be transferred to delivery suite. Staff told us they did not use a
system to determine the time in which a woman should be seen by a midwife and/or doctor based
on the symptoms they had, such as a traffic light RAG (red, amber, green) rating. Staff told us they
used their clinical judgement and prioritised women as needed. For example, they would aim to
see women who reported no fetal movements as soon as they arrived and aimed to see all women
within 30 minutes of arrival. This was in line with national guidance (National Institute for Health
and Care Excellence (NICE), Safe midwifery staffing for maternity settings overview (September
2019).
Staff used a nationally recognised tool to identify deteriorating women and escalated them
appropriately. The service used a modified early obstetric warning score (MEOWS) tool. This was
designed to aid early recognition of acutely unwell women by monitoring physical parameters such
as breathing rate, heart rate, temperature and blood pressure. We reviewed 19 MEOWS charts
and found they were completed and scored. We also saw women were referred promptly to the
medical team for review when indicated by their MEOWS score. Managers audited the completion
20190416 900885 Post-inspection Evidence appendix template v4 Page 184
of MEOWS charts quarterly and acted to improve completion when needed. From April to June
2019, 65% of MEOWS charts audited were fully and correctly completed. To improve completion,
managers shared the results with staff and gave improvement practice points. The most recent
audit from July to September 2019 showed compliance had improved to 90% (Source: Additional
Evidence Request, DR94a and DR94b).
Staff used a nationally recognised tool to identify women at risk of developing a pressure ulcer.
Staff assessed women routinely in accordance with trust policy, such as on admission during
pregnancy and labour, if they had a body mass index of 40 or above and if an epidural was sited.
Specialist equipment was used for women who were identified as high risk, such as air
mattresses.
Staff used a buddy system to review cardiotocography (CTG) interpretation. This was in line with
national recommendations (NHS England, Saving Babies’ Lives Version Two: A care bundle for
reducing perinatal mortality (March 2019)). The service used the ‘fresh eyes’ approach. This
meant a second midwife was required to review the CTG recording hourly during labour, to ensure
it had been interpreted correctly and escalated when needed. The maternity records we reviewed
showed CTG peer reviews were performed hourly and were escalated appropriately.
Staff completed risk assessments for each woman at their initial booking appointment and updated
them throughout pregnancy, labour and the postnatal period as needed. We reviewed 21
maternity care records which confirmed this. These included social, medical, obstetric and mental
health risk assessments. The outcome of these risk assessments was used to plan future care
provision. Women who were high-risk and unsuitable for midwife led care were referred to an
obstetrician for review and management.
Staff knew about and dealt with any specific risk issues such as gestational diabetes, blood clots
and smoking. Women who were at high risk of gestational diabetes were offered diagnostic
testing. Staff completed venous thromboembolism (VTE) risk assessments (used to determine a
patient’s risk of developing a blood clot) at booking, antenatal admissions and postnatally. This
was in line with national recommendations (RCOG, Reducing the Risk of Venous
Thromboembolism during Pregnancy and the Puerperium: Green-top Guideline No. 37a (April
2015). From May to October 2019, 100% of VTE assessments audited were complete, correctly
assessed and the appropriate action pathway had been followed (Source: Additional Evidence
Request, DR95).
Staff offered women carbon monoxide screening at booking and mostly recorded the outcome. We
reviewed 21 records, four of which had no carbon monoxide level recorded. We were unable to
determine whether these women had declined the test. Staff risk assessed women for fetal growth
restriction and used customised fetal growth charts to help identify babies who were not growing
as expected. Women who were identified at risk were referred for serial growth scans during
pregnancy. In quarter 1 (April to June 2019) and quarter 2 (July to September 2019), 100% and
98% of pregnancies were appropriately screened and monitored according to risk. For the same
period, 92% and 98% of all fundal height measurements were plotted on individualised GROW
charts (Source: Additional Evidence Request, DR97). However, managers recognised the current
scanning capacity would not enable them to meet national recommendations. They had added this
to the service’s risk register and developed an action plan to increase scanning capacity, which
included the recruitment of additional sonographers.
There was a pathway for the management of sepsis. Staff we spoke with could describe what
actions they would take if a woman was admitted with suspected or known sepsis including
prompt administration of fluids and antibiotics.
20190416 900885 Post-inspection Evidence appendix template v4 Page 185
Swabs used for vaginal birth and perineal suturing were counted for completeness by two
members of staff. This was in line with national recommendations (NSPA, Reducing the risk of
retained swabs after vaginal birth and perineal suturing: 1229 (May 2010). We reviewed 16
records and saw two members of staff had verified the swab count.
The service had 24-hour access to mental health liaison and specialist mental health support (if
staff were concerned about a woman’s mental health. Staff could contact the crisis team for urgent
mental health support when needed. Staff told us they responded promptly.
Staff completed, or arranged, psychosocial assessments and risk assessments for women thought
to be at risk of self-harm or suicide. Staff routinely asked women about their mental health when
they had their booking appointment, throughout pregnancy and postnatally. Women at risk were
referred to the specialist perinatal mental health midwife and local perinatal mental health team for
review, support and treatment.
Staff shared key information to keep women safe when handing over their care to others. The
service used the SBAR communication tool when handing over care. SBAR is a structured method
for communicating critical information that requires immediate attention and action. From June to
November 2019, records audited showed staff completed SBAR handovers. The delivery suite
‘patient safety at a glance’ (PSAG) whiteboard was configured with SBAR. It included key
information about each woman’s history, observations, risks and management plan which health
professionals could see at a glance.
Shift changes and handovers included all necessary key information to keep women safe.
Midwifery handovers took place at the start of each shift, with a further three medical handovers a
day. We observed two handovers which were structured and detailed. Staff handed over all
necessary information about each woman such as history, risks, observations, medicines
prescribed and management care plans.
The World Health Organisation (WHO) surgical safety checklist ‘Five Steps to Safer Surgery’ was
used in maternity theatres. However, compliance was variable. In August 2019, an observational
audit showed compliance was 75% for the safety briefing, 87% for sign in, 89% for time out, 74%
for sign out, 81% for swab count and 58% for debrief. The observers reported staff completed the
WHO checklist well for women who had a planned caesarean section but there was poor
compliance with emergency cases, particularly in terms of debrief. We saw an action plan had
been developed to improve compliance. The service planned to re-audit completion of surgical
safety checklists in January 2020 (Source: Additional Evidence Request, DR93). We reviewed six
WHO checklists and found they were fully completed.
Midwifery staffing
The service had enough maternity staff with the right qualifications, skills, training and
experience to keep women and babies safe from avoidable harm and to provide the right
care and treatment. Managers regularly reviewed staffing levels and skill mix, and gave
bank and agency staff a full induction.
The service had enough maternity staff of all grades to keep women and babies safe. All maternity
staff we spoke with told us staffing levels had improved since the new head of midwifery had
joined the service in September 2019. This was because the establishment (planned staffing
levels) had increased, most vacancies had been recruited to and flexible working had been
introduced. Staff mostly felt there was enough maternity staff to meet the demands of the service.
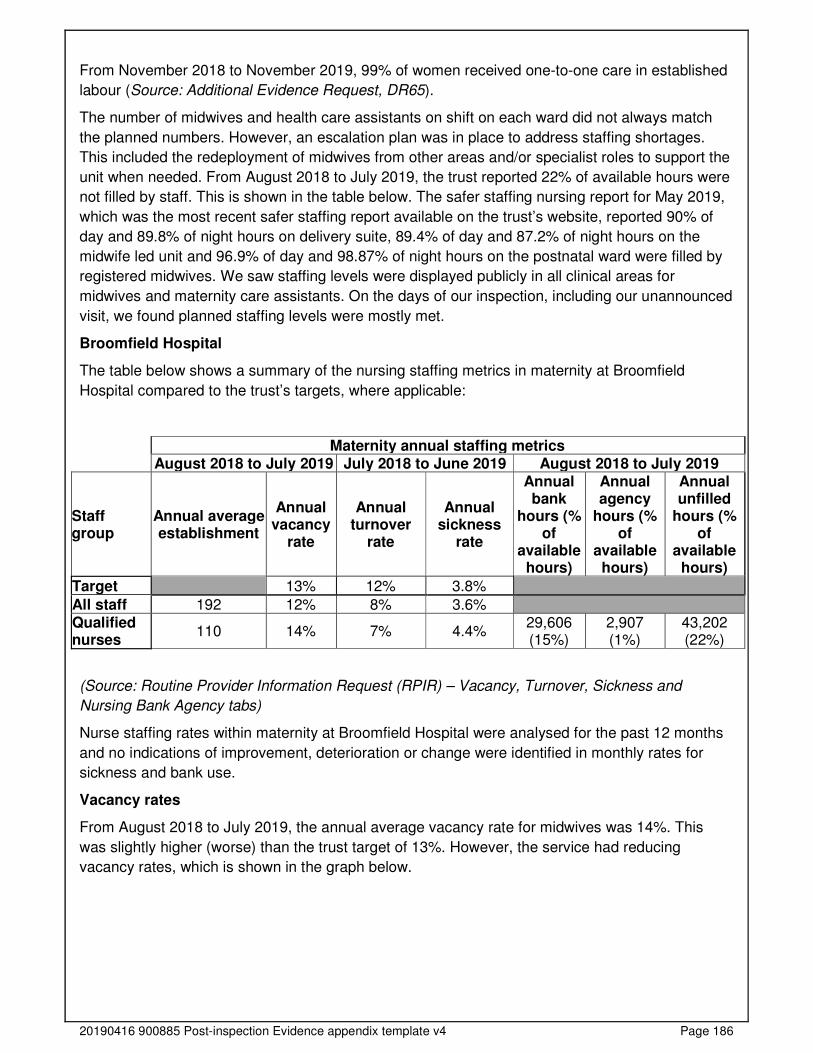
20190416 900885 Post-inspection Evidence appendix template v4 Page 186
From November 2018 to November 2019, 99% of women received one-to-one care in established
labour (Source: Additional Evidence Request, DR65).
The number of midwives and health care assistants on shift on each ward did not always match
the planned numbers. However, an escalation plan was in place to address staffing shortages.
This included the redeployment of midwives from other areas and/or specialist roles to support the
unit when needed. From August 2018 to July 2019, the trust reported 22% of available hours were
not filled by staff. This is shown in the table below. The safer staffing nursing report for May 2019,
which was the most recent safer staffing report available on the trust’s website, reported 90% of
day and 89.8% of night hours on delivery suite, 89.4% of day and 87.2% of night hours on the
midwife led unit and 96.9% of day and 98.87% of night hours on the postnatal ward were filled by
registered midwives. We saw staffing levels were displayed publicly in all clinical areas for
midwives and maternity care assistants. On the days of our inspection, including our unannounced
visit, we found planned staffing levels were mostly met.
Broomfield Hospital
The table below shows a summary of the nursing staffing metrics in maternity at Broomfield
Hospital compared to the trust’s targets, where applicable:
Maternity annual staffing metrics August 2018 to July 2019 July 2018 to June 2019 August 2018 to July 2019
Staff group
Annual average establishment
Annual vacancy
rate
Annual turnover
rate
Annual sickness
rate
Annual bank
hours (% of
available hours)
Annual agency
hours (% of
available hours)
Annual unfilled
hours (% of
available hours)
Target 13% 12% 3.8%
All staff 192 12% 8% 3.6% Qualified nurses
110 14% 7% 4.4% 29,606 (15%)
2,907 (1%)
43,202 (22%)
(Source: Routine Provider Information Request (RPIR) – Vacancy, Turnover, Sickness and
Nursing Bank Agency tabs)
Nurse staffing rates within maternity at Broomfield Hospital were analysed for the past 12 months
and no indications of improvement, deterioration or change were identified in monthly rates for
sickness and bank use.
Vacancy rates
From August 2018 to July 2019, the annual average vacancy rate for midwives was 14%. This
was slightly higher (worse) than the trust target of 13%. However, the service had reducing
vacancy rates, which is shown in the graph below.
20190416 900885 Post-inspection Evidence appendix template v4 Page 187
Monthly vacancy rates over the last 12 months for qualified nurses, health visitors and midwives at
Broomfield Hospital showed a downwards shift from February 2019 to July 2019. This indicated an
improvement in vacancy rates. The service had employed 13 full-time equivalent (FTE) band 5
midwives in September 2019. We were told the service had 7.5 full-time equivalent (FTE) midwife
band 6 vacancies and five FTE maternity care assistant vacancies when we inspected.
(Source: Routine Provider Information Request (RPIR) – Vacancy tab)
Turnover rates
The service had low turnover rates. The turnover rate was below the trust target of 12%.
Monthly turnover rates over the last 12 months for qualified nurses, health visitors and midwives at
Broomfield Hospital showed a shift from January 2019 to June 2019, with an increase from April
2019. However, the turnover rate remained below the trust target.
(Source: Routine Provider Information Request (RPIR) – Turnover tab)
Agency staff usage
Managers limited their use of bank and agency staff and requested staff familiar with the service.
From August 2018 to July 2019, the service reported 15% of shifts were covered by bank staff and
1% by agency staff. All staff we spoke with told us the use of bank and agency midwives had
reduced. This was partly because the new head of midwifery had introduced flexible working hours
and allowed staff to work reduced hours if they wished. Prior to this, we were told permanent staff
had to work a minimum of 30 hours per week. Those who wanted to work less had to do so
through the bank. Agency staff were not used in the community.
Managers made sure all bank and agency staff had a full induction and understood the service.
Most bank staff had been employed or were still employed as substantive (permanent) staff within

20190416 900885 Post-inspection Evidence appendix template v4 Page 188
the trust. Bank staff were required to complete the same trust and service specific mandatory
training as permanent staff. Agency staff had an induction before they commenced duties. This
was undertaken by a senior midwife.
Monthly agency hours over the last 12 months for qualified nurses, health visitors and midwives at
Broomfield Hospital showed a shift from February 2019 to July 2019.
(Source: Routine Provider Information Request (RPIR) - Nursing bank agency tab)
Midwife to birth ratio
From January to December 2018 the trust had a ratio of one midwife to every 29.4 births. This was
similar to the England average of one midwife to every 24.6 births. However, the maternity
dashboard showed this had increased (worsened) from April to October 2019, with an average of
one midwife to every 33.4 births. This corresponded with a general increase in deliveries during
this period.
(Source: Electronic Staff Records – EST Data Warehouse)
Managers accurately calculated and reviewed the number and grade of midwives and maternity
care workers needed for each shift, in accordance with national guidance. A midwifery staffing
establishment review was undertaken and presented to the board in June 2019. The trust used the
Birthrate Plus midwifery workforce tool to calculate the midwifery staff needed based on activity,
case mix and demographics. Birthrate Plus is recommended by the Department of Health,
endorsed by the Royal College of Midwives and is incorporated within the national maternity safety
strategy (NHS Resolution, Maternity incentive scheme - year two (2018)). The establishment
review showed the service had a shortfall of 3.47 full-time equivalent (FTE) midwives for clinical
care and 6.20 FTE non-clinical midwives. Managers told us they had recruited several specialist
midwives to lead on improvement and safety initiatives, in accordance with national
recommendations. These included a fetal surveillance lead midwife, quality improvement lead
midwife and a Better Births lead midwife. At the time of our inspection, the service was also
recruiting for an additional perinatal mental health and bereavement midwife to help meet the
increasing demands for these services.
Staffing incidents were reported through the trust’s electronic reporting system. From 20
November 2018 to 19 November 2019, the service reported 45 incidents related to staffing. Most
of these were categorised as unit closure of one of the standalone birthing units (53.3%) or failure
and/or delay in access and admission (22.2%). Managers acted to minimise the risk from staffing
shortages to women and/or babies, such as the redeployment of staff.

20190416 900885 Post-inspection Evidence appendix template v4 Page 189
The ward manager could adjust staffing levels daily according to the needs of women. Staffing
levels, skill mix and patient acuity were monitored and reported regularly throughout the day. A
senior midwife was the designated daily ‘bleep holder’ from 8am to 4pm. Their role was to monitor
and manage any staffing issues. Staff could contact them for assistance with any staffing issues
when needed. Out of these hours, the delivery suite coordinator and manager on-call were
available. Staffing levels were also reviewed at the daily safety huddle and handovers. An acuity
tool was used to monitor staffing levels and patient acuity four-hourly. The tool flagged whether a
shift was safe or unsafe by a traffic light system. Green indicated staffing numbers were safe,
amber indicated staffing numbers were safe but required escalation to maintain safety and red
indicated staffing numbers were unsafe and required escalation. We reviewed the acuity tool for
October 2019 and found 10 occasions when staffing levels were red rated (5.4%). This meant
most shifts in October 2019 were rated safe for staffing (94.6%).
Student midwives were supernumerary and not included in the midwife-staffing establishment.
Every student was assigned a midwife to work with on shift.
Medical staffing
While planned medical staffing levels were met, the service did not always have enough
medical staff with the right qualifications, skills, training and experience to keep women
and babies safe from avoidable harm and to provide the right care and treatment.
The service did not always have enough medical staff to keep women and babies safe. Most staff
we spoke with felt there was not always enough medical staff to meet the needs of women and/or
babies in a timely manner. They also told us medical staffing levels had not increased despite an
increase in activity. The service provided 68 hours of consultant obstetric on-site cover per week
(Source: Mid and South Essex University Hospitals Group, Maternity Staffing Strategy (October
2019)). When not on site, a consultant was on-call from home. However, the consultant on-call
was also responsible for covering any emergencies in the gynaecology service. This meant there
was a risk they may not always be available to attend maternity emergencies in a timely manner.
A middle grade/registrar doctor and junior doctor supported the on-call consultant and were on-site
24 hours a day, seven days a week. Managers had recognised medical staffing was a risk and
funding had been allocated to mitigate this risk by providing a second registrar at nights and
weekends to manage activity. Staff told us this worked well. However, from Monday to Thursday
the service had one doctor at middle grade/registrar level who covered both the maternity and
gynaecology service. Staff told us this meant women were not always reviewed in a timely
manner, particularly those awaiting review on the antenatal day assessment unit.
Obstetric anaesthetic cover was available 24 hours a day, seven days a week. Emergency work
on delivery suite was covered by a staff grade/specialist anaesthetist. A consultant anaesthetist
was also available from 8am to 6pm to cover the elective caesarean section list. There was a
designated lead anaesthetist for obstetrics. This was in line with national recommendations (Royal
College of Anaesthetists (RCoA), Guidelines for the Provision of Anaesthesia Services for an
Obstetric Population 2019 (January 2019)).
There were three consultant-led ward rounds per day, where activity was discussed, and women
were reviewed. Women were prioritised according to their risk.
The medical staff matched the planned number on all shifts in each department. As the table
below shows, from August 2018 to July 2019 on average, there were no vacancies for medical
staff and all available hours were filled.
20190416 900885 Post-inspection Evidence appendix template v4 Page 190
Broomfield Hospital
The table below shows a summary of the medical staffing metrics in maternity at Broomfield
Hospital compared to the trust’s targets, where applicable.
The trust has reported that there are no medical staff working exclusively in maternity at St Peter’s
Hospital and St Michael’s Hospital.
Maternity annual staffing metrics August 2018 to July 2019 July 2018 to June 2019 August 2018 to July 2019
Staff group
Annual average establishment
Annual vacancy
rate
Annual turnover
rate
Annual sickness
rate
Annual bank
hours (% of
available hours)
Annual locum
hours (% of
available hours)
Annual unfilled
hours (% of
available hours)
Target 13% 12% 3.8%
All staff 234 13% 8% 3.9% Medical staff
28 0% 8% 0.3% 1,918 (3%)
2,619 (5%)
0 (0%)
(Source: Routine Provider Information Request (RPIR) – Vacancy, Turnover, Sickness and
Medical locum tabs)
Medical staffing rates within maternity were analysed for the past 12 months and no indications of
improvement, deterioration or change were identified in monthly rates for turnover, sickness, bank
use and locum use.
Vacancy rates
The service had low vacancy rates for medical staff. As of June 2019, the service reported a
medical vacancy rate of 2% which was below (better than) the trust target of 13%.
Monthly vacancy rates over the last 12 months for medical staff show a downward trend from
November 2018 to April 2019 and medical staff in maternity at the trust were over established in
February, March and April 2019.
(Source: Routine Provider Information Request (RPIR) – Vacancy tab)
20190416 900885 Post-inspection Evidence appendix template v4 Page 191
Sickness rates for medical staff were low. From July 2018 to June 2019, the sickness rate for
medical staff was 0.3%. This was below (better than) the trust target of 3.8%.
The service had low turnover rates for medical staff. From July 2018 to June 2019, the turnover
rate for medical staff was 8%. This was below (better than) the trust target of 12%.
The service had low rates of bank and locum staff used. From August 2018 to July 2019, 3% of
shifts were filled by bank medical staff and 5% by locum medical staff. Managers could access
locums when they needed additional staff. There were no medical shifts unfilled by substantive
and temporary staff.
Managers made sure locums had a full induction to the service before they started work. Locum
doctors received an induction before they commenced duties. Managers we spoke with told us
locums who were familiar with the service were used where possible.
Staffing skill mix
The service had a good skill mix of medical staff on each shift and reviewed this regularly. The
service always had a consultant, middle grade/registrar level doctor, junior doctor and anaesthetist
on-call 24 hours a day, seven days a week. Staff told us they could contact the on-call obstetric
team whenever they needed them.
In April 2019, the proportion of consultant staff and registrars reported to be working at the trust
was lower than the England average. The proportion of junior (foundation year 1-2) and middle
career staff was higher.
Staffing skill mix for the 27.2 whole time equivalent staff working in maternity at Mid Essex
Hospital Services NHS Trust.
This
Trust
England
average
Consultant 36% 42%
Middle career^ 15% 9%
Registrar group~ 38% 44%
Junior* 11% 6%
^ Middle Career = At least 3 years at SHO or a higher grade within their chosen specialty ~ Registrar Group = Specialist Registrar (StR) 1-6 * Junior = Foundation Year 1-2
(Source: NHS Digital Workforce Statistics)

20190416 900885 Post-inspection Evidence appendix template v4 Page 192
Records
Staff kept detailed records of women’s care and treatment. Records were clear, up-to-date
and mostly available to all staff providing care.
Women’s notes were comprehensive, and staff could mostly access them easily. The service
mainly used paper-based records, with some information held on the trust’s electronic patient
record system. Community staff told us there could be a delay in booking information being
available to hospital staff. This was because most community midwives did not have laptops and
had to return to the hospital to update the electronic patient record system. To address this, four
community hubs were opening in January 2020 (Source: Additional Evidence Request, DR83).
These would be equipped with computer terminals so that community staff could record women’s
information on the electronic patient record system in a timely manner. Furthermore, all women
had their handheld pregnancy records which included all their booking information. Staff told us it
was uncommon for women’s records to be unavailable for clinics.
Records were contemporaneous, legible, dated and signed. We reviewed 21 sets of maternity
records and found these were mostly completed in line with professional standards (NMC, The
Code: Professional standards of practice and behaviour for nurses, midwives and nursing
associates (October 2018). Handheld records contained a complete record of antenatal test
results. This was in line with national guidance (NICE, Antenatal care: QS22, Quality statement 3
(April 2016). Regular maternal and fetal assessment was evident, such as blood pressure, urine
analysis, symphysis-fundal height measurement and fetal movements. Relevant past and current
medical, obstetric, social and mental health information was documented. Risk assessments were
completed with details of further action taken when indicated. It was evident from the records if
women had additional needs, such as language and literacy, sight and hearing. Staff had access
to up to date management plans for women with safeguarding and mental health concerns. These
were stored on the electronic patient record system. All authorised staff could access, and update
safeguarding management plans as needed.
Managers audited records to ensure staff completed them in line with national standards and trust
policy. Audits carried out from June to November 2019 showed staff were mostly compliant with
record keeping standards. There were two occasions when staff had not documented the time the
entry was made. A letter detailing where improvement was needed was sent to these staff
members (Source: Additional Evidence Request, DR92).
When women were transferred from the community to the hospital, to different wards and/or
discharged home, there were no delays in staff accessing their records. Women carried their own
handheld pregnancy records which they were advised to bring to each antenatal appointment and
when they attended the hospital. Discharge summaries were sent to community midwives, health
visitors and GPs to help ensure continuity of care in the community. The summary included
information about the woman’s pregnancy, birth and postnatal care, medicines prescribed, and
ongoing risks and/or follow-up care needed. Women were given the personal child health record
(also known as the ‘red book’). Staff completed the required sections and told women what the
record was for and how to use it. The red book is a national standard health and development
record which is used to monitor growth and development of the child, up to the first four years of
life.
Records were stored securely. Women’s maternity records were stored in lockable trolleys on the
delivery suite and postnatal ward. We observed these were locked when not in use. The maternity
records of women on the antenatal day assessment unit were stored behind the midwives’ station.

20190416 900885 Post-inspection Evidence appendix template v4 Page 193
These were not secured. However, we observed the station was not left unattended by staff.
Electronic records were password protected. We saw computer terminals were locked when not in
use.
Medicines
Prescription charts were not always completed with women’s weight and allergy status.
Furthermore, storage temperatures were not always checked daily and temperature
checklists were not always completed fully. However, staff followed systems and
processes when safely administering and recording medicines.
We found prescription charts were not always fully completed. We reviewed 22 charts and found
three did not have the woman’s allergy status documented. This is essential to avoid serious
medication errors from being made. Furthermore, women’s weight was not documented in seven
charts. This is important because the correct dose of some medicines is determined by patient
weight, such as anti-clotting medicine. Women at risk of developing a blood clot were routinely
prescribed anti-clotting medicine to reduce this risk; the correct dose of which was determined by
the woman’s weight. However, staff told us they used the woman’s booking weight to determine
the correct dose which was in line with national guidance (RCOG, Reducing the Risk of Venous
Thromboembolism during Pregnancy and the Puerperium: Green-top Guideline No. 37a (April
2015). All the prescription charts were signed, legible and medicines were given as prescribed.
Antibiotics were prescribed and reviewed in line with trust policy.
Staff did not always store and manage all medicines and prescribing documents in line with the
trust’s policy. Ambient and fridge temperatures were not always checked daily to ensure
medicines stored were effective and safe for patient use. We reviewed 18 checklists completed
from 1 September to 5 November 2019 for delivery suite, the antenatal day assessment unit
(ADAU) and postnatal ward and found 65 occasions when the fridge and/or ambient temperature
had not been checked daily. Furthermore, according to the ambient checklists for the ADAU, the
temperature had exceeded 25°C for seven consecutive days. However, staff had not recorded
what escalation and corrective action they had taken. This was not in line with the trust’s policy
(Source: Additional Evidence Request, DR101). Managers told us this had been escalated to
pharmacy staff, who had checked and confirmed the medicines stored were safe and effective at
up to 30°C. We raised these concerns with senior staff and when we revisited the service on our
unannounced inspection we found all checklists had since been completed with details of
escalation and action taken when indicated.
Medicines were stored securely in all clinical areas we visited. Controlled drugs (medicines subject
to additional security measures) were stored correctly in locked cupboards and stock was checked
by two qualified members of staff twice a day. The keys for medicine cupboards and fridges were
stored in a safe which only qualified members of staff had access to. This prevented unauthorised
personnel from accessing medicines. We found medicine storage areas were well organised and
tidy, with effective processes in place to ensure stock was regularly rotated. All medicines we
checked were within their use by date, including intravenous fluids (fluid given through a vein).
Staff reviewed women’s medicines regularly and provided specific advice to women and carers
about their medicines. Staff showed women or their carer how to administer anti-clotting medicine
when this was prescribed for them to take at home. Women we spoke with confirmed this. Staff
provided advice to women about medicine options for pain relief during labour, which included the
20190416 900885 Post-inspection Evidence appendix template v4 Page 194
risks and benefits of each option. Staff could contact pharmacy staff for advice about women’s
medicines when needed.
Staff followed current national practice to check women had the correct medicines. Midwives
undertook additional drug administration training if they were involved in medication incidents and
had not followed current national practice. We saw staff checked women’s identification to ensure
they had the correct medicines before they gave them. Staff checked women had the correct
medicines to take home before they discharged them.
The service had systems to ensure staff knew about safety alerts and incidents, so women
received their medicines safely. Staff knew how to report medicine errors and incidents and we
saw these were investigated and learning was shared with staff. From August 2018 to August
2019 the service reported 40 medication incidents through the National Reporting and Learning
System. This equated to 2.6% of total incidents reported by the service. All incidents were graded
as having caused no harm. Common themes included missed and/or delayed administration and
wrong dose, wrong frequency and/or wrong route. We saw learning from medicine incidents were
shared with staff.
Decision making processes were in place to ensure women’s behaviour was not controlled by
excessive and inappropriate use of medicines. Women with known drug and alcohol misuse were
referred to the local specialist treatment and recovery service for assessment. This included
whether stabilising drug use or detoxification programme was appropriate before delivery.
Incidents
The service managed patient safety incidents well. Staff recognised incidents and near
misses and reported them appropriately. Managers investigated incidents and shared
lessons learned with the whole team and the wider service. When things went wrong, staff
apologised and gave women honest information and suitable support. Managers ensured
that actions from patient safety alerts were implemented and monitored.
All staff knew what incidents to report and how to report them. The trust used an electronic
reporting system which all grades of staff had access to. Staff we spoke with said they were
encouraged to report incidents and felt confident to do so. They described a “good reporting
culture” within the service and trust.
Staff reported all incidents that they should report. The service had up to date guidance on what
should be reported as an incident which staff could access easily. We saw staff reported a wide
range of incidents including near misses. From August 2018 to August 2019, staff reported 1,518
maternity incidents through the National Reporting and Learning System (NRLS). Incidents were
graded as having caused no harm, low harm or severe harm. Most incidents were graded as
having caused no harm (95.3%). The most common themes for incidents reported were related to
treatment and/or procedure, access, admission, transfer, discharge (including missing patient)
(20.3%) and other (13.6%) (Source: RPM Analysis, NRLS Notifications and StEIS incidents
Detail).
Never events
The service had no never events on any maternity wards and departments.
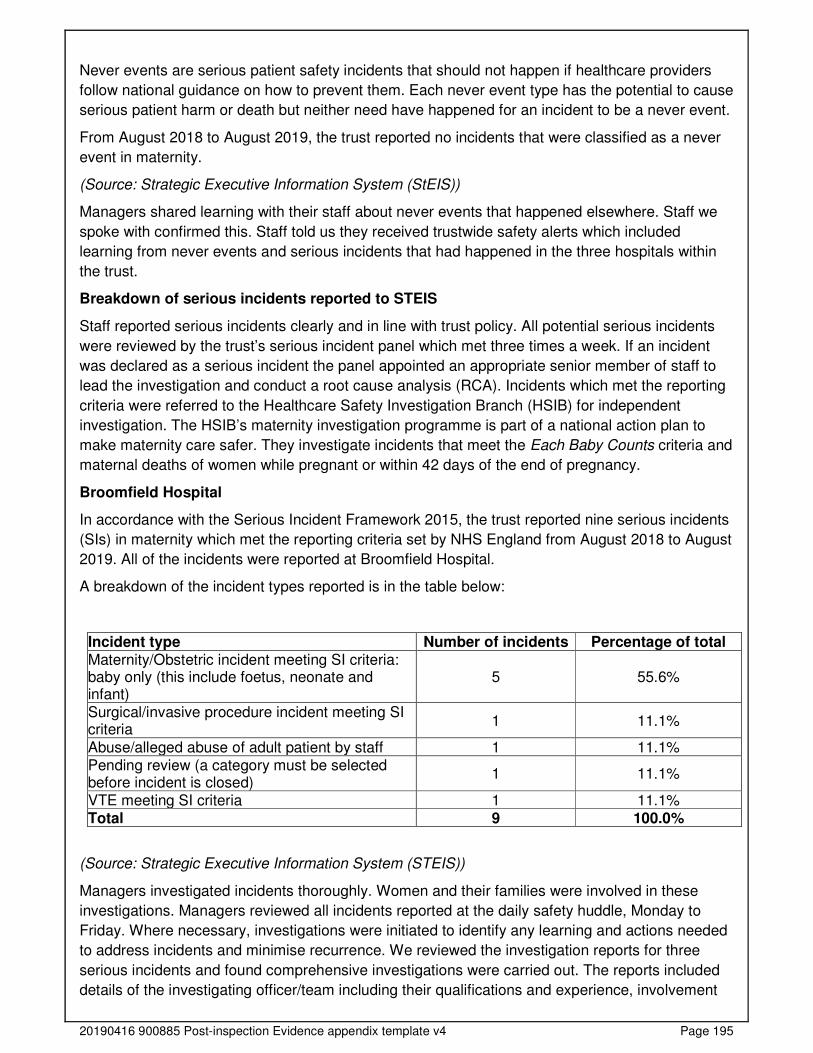
20190416 900885 Post-inspection Evidence appendix template v4 Page 195
Never events are serious patient safety incidents that should not happen if healthcare providers
follow national guidance on how to prevent them. Each never event type has the potential to cause
serious patient harm or death but neither need have happened for an incident to be a never event.
From August 2018 to August 2019, the trust reported no incidents that were classified as a never
event in maternity.
(Source: Strategic Executive Information System (StEIS))
Managers shared learning with their staff about never events that happened elsewhere. Staff we
spoke with confirmed this. Staff told us they received trustwide safety alerts which included
learning from never events and serious incidents that had happened in the three hospitals within
the trust.
Breakdown of serious incidents reported to STEIS
Staff reported serious incidents clearly and in line with trust policy. All potential serious incidents
were reviewed by the trust’s serious incident panel which met three times a week. If an incident
was declared as a serious incident the panel appointed an appropriate senior member of staff to
lead the investigation and conduct a root cause analysis (RCA). Incidents which met the reporting
criteria were referred to the Healthcare Safety Investigation Branch (HSIB) for independent
investigation. The HSIB’s maternity investigation programme is part of a national action plan to
make maternity care safer. They investigate incidents that meet the Each Baby Counts criteria and
maternal deaths of women while pregnant or within 42 days of the end of pregnancy.
Broomfield Hospital
In accordance with the Serious Incident Framework 2015, the trust reported nine serious incidents
(SIs) in maternity which met the reporting criteria set by NHS England from August 2018 to August
2019. All of the incidents were reported at Broomfield Hospital.
A breakdown of the incident types reported is in the table below:
Incident type Number of incidents Percentage of total Maternity/Obstetric incident meeting SI criteria: baby only (this include foetus, neonate and infant)
5 55.6%
Surgical/invasive procedure incident meeting SI criteria
1 11.1%
Abuse/alleged abuse of adult patient by staff 1 11.1% Pending review (a category must be selected before incident is closed)
1 11.1%
VTE meeting SI criteria 1 11.1% Total 9 100.0%
(Source: Strategic Executive Information System (STEIS))
Managers investigated incidents thoroughly. Women and their families were involved in these
investigations. Managers reviewed all incidents reported at the daily safety huddle, Monday to
Friday. Where necessary, investigations were initiated to identify any learning and actions needed
to address incidents and minimise recurrence. We reviewed the investigation reports for three
serious incidents and found comprehensive investigations were carried out. The reports included
details of the investigating officer/team including their qualifications and experience, involvement
20190416 900885 Post-inspection Evidence appendix template v4 Page 196
and support of the woman and relatives, lessons learned and recommendations. Each report had
an action plan to minimise recurrence (Source: Additional Evidence Request, DR67).
Managers debriefed and supported staff after any serious incident. The serious incident reports we
reviewed included details of the involvement and support provided for staff. Professional midwifery
advocates offered restorative clinical supervision sessions to midwives involved in an
investigation. One of the reports we reviewed showed staff were given group psychological
support after a distressing event. One-to-one psychological support was offered to those who
needed it. Staff we spoke with told us they received support from their managers and peers if they
were involved in a serious incident. Staff were provided with additional training if identified as a
learning action.
Staff understood the duty of candour. They were open and transparent and gave women and
families a full explanation when things went wrong. The trust had an up to date duty of candour
policy which staff could access through the trust’s intranet. The duty of candour is a regulatory
duty that relates to openness and transparency and requires providers of health and social care
services to notify patients (or other relevant persons) of certain notifiable safety incidents and
provide reasonable support to that person, under Regulation 20 of the Health and Social Care Act
2008 (Regulated Activities) Regulations 2014. A notifiable safety incident includes any incident
that could result in, or appears to have resulted in, the death of the person using the service or
severe, moderate or prolonged psychological harm. Staff we spoke with were aware of the
importance of being open and honest with women and families when something went wrong, and
of the need to offer an appropriate remedy or support to put matters right and explain the effects of
what had happened. We saw the duty of candour regulation was followed in the incident reports
we reviewed. Women and families were involved in the investigation process and informed of the
outcome. The investigation report was shared with the woman, her family and/or representative(s)
on completion (Source: Additional Evidence Request, DR67).
Staff received feedback from investigation of incidents, both internal and external to the service.
Staff could indicate if they wanted feedback from incidents they had reported through the
electronic reporting system. Feedback from incidents was shared with staff in a variety of ways
such as safety huddles and handovers, hot topics, email, newsletters and staff noticeboards. We
read two copies of the women’s and children’s divisional quarterly newsletter which included
learning from maternity, gynaecology and paediatric related incidents. Staff told us they felt well
informed about incidents.
Staff met to discuss the feedback and look at improvements to women’s and babies care.
Incidents were a standing agenda item at monthly team and governance meetings. We reviewed
three sets of mortality and morbidity meeting minutes which showed incident themes and areas for
improvement were discussed. Individual cases of maternal and perinatal morbidity and mortality
were also presented, including learning and recommendations. The meetings were well attended
by members of the multidisciplinary team (Source: Additional Evidence Request, DR68). All cases
of perinatal mortality were reviewed with the aid of a national perinatal mortality tool. This was in
line with national recommendations (MBRRACE-UK, Perinatal Mortality Review Tool (February
2018).
There was evidence that changes had been made as a result of feedback. For example, in July
2019 the service commenced a 12-month quality improvement project to reduce the rate of
postpartum haemorrhage (PPH) (excessive blood loss following delivery) of 1,500mls or more by
50% by May 2020. This was in response to an increase in incidents of this. From March to June
2019, the average rate of births at the trust with PPH greater than/or equal to 1,500mls was 5.3%
20190416 900885 Post-inspection Evidence appendix template v4 Page 197
This was higher than the national rate of 2.7%. Actions taken to reduce the PPH rate included
completion of PPH risk assessment on admission to delivery suite, second midwife to be present
at delivery and the administration of medicine for management of the third stage (delivery of the
placenta and membranes) with delivery of the anterior shoulder (the shoulder of the baby that
faces the pubic symphysis of the mother during delivery) (Source: Additional Evidence Request,
DR98a).
Safety thermometer
The service used monitoring results well to improve safety. While safety thermometer data
was not shared with staff, women and visitors, other safety information was displayed
publicly.
Safety thermometer data was not displayed on wards for staff and women to see. While managers
collected data for the maternity safety thermometer, the results were not displayed. However,
other safety information was displayed publicly. For example, we saw television screens in each
department with learning from incidents and audit results displayed on a loop.
Managers submitted data monthly to the national maternity safety thermometer. The safety
thermometer was designed to support improvements in patient care and experience. Harms
associated with maternity were recorded such as perineal trauma, infection and babies with an
Apgar score less than seven at five minutes.
The safety thermometer data showed the service did not achieve over 95% harm free care for the
last 12 months. From August 2018 to July 2019, the trust’s average combined harm free score
was 49.9%. This was significantly lower (worse) than the England average of 75.1%. Managers
told us this was because some of the figures submitted had been wrongly recorded by staff. This
had significantly skewed some of the data submitted.
Staff used the safety thermometer data to further improve services. For example, from August
2018 to July 2019, the percentage proportion of women that had a PPH greater than 1,000mls
was 22.5%. This was significantly higher (worse) than the England average of 10.1%. In response,
the service had commenced a 12-month quality improvement project to reduce the rate of PPH.
Is the service effective?
Evidence-based care and treatment
The service provided care and treatment based on national guidance and best practice.
Managers checked to make sure staff followed guidance. Staff protected the rights of
women subject to the Mental Health Act 1983.
Staff followed up to date policies to plan and deliver high quality care according to best practice
and national guidance. Antenatal records showed women received care in accordance with
national guidance and standards. For example, all pregnant women were offered fetal anomaly
screening (NICE, Antenatal care: QS22, Quality statement 10 (April 2016)). Staff offered pregnant
women testing for gestational diabetes if they were identified at risk of it at booking (NICE,
Antenatal care: QS22, Quality statement 6 (April 2016)). Staff offered women who had had one or
more previous caesarean sections the opportunity to discuss birth options in their current
pregnancy (NICE, Caesarean section: QS32, Quality statement 1 (June 2013)).

20190416 900885 Post-inspection Evidence appendix template v4 Page 198
Managers checked to make sure staff followed guidance and used the results to improve.
Compliance with the Saving Babies’ Lives care bundle was monitored and reported quarterly. An
audit of compliance in quarter 2 (July to September 2019) showed most recommendations were
being met. For example, women were offered carbon monoxide screening at booking and the
outcome was recorded when accepted. Information and advice leaflet on reduced fetal movement
was given to and discussed with all pregnant women by 24 weeks of pregnancy. Symphysis-
fundal height measurement was routinely monitored from 24 weeks of pregnancy. Where
compliance was not 100%, we saw action was taken to improve. For example, staff who had not
completed cardiotocography (CTG) training and assessment were asked to evidence this within
the month (Source: Additional Evidence Request, DR97).
Managers made sure guidelines reflected current evidence-based guidance and quality standards.
Guidelines were reviewed every three years or when national guidance was published. Staff were
informed of updated guidelines through email. Managers were working collaboratively to develop
network guidelines to standardise care across the local maternity system. The guidelines we
reviewed were in line with and referenced current national guidance. All maternity guidelines were
within review date. We saw staff could access guidelines easily through the trust’s intranet. Trust
policies were assessed to ensure guidance did not discriminate because of race, ethnic origin,
nationality, gender, culture, religion or belief, sexual orientation and/or age.
Staff protected the rights of women subject to the Mental Health Act and followed the Code of
Practice. Staff knew how to access support and advice to best meet the needs of women with
mental health concerns. Staff assessed all women for risk of mental health issues at booking and
monitored psychological wellbeing throughout the perinatal period. Women identified at risk were
referred to the specialist perinatal mental health midwife. Mental health assessment, care and
treatment was also available from the local perinatal mental health service. Women with current or
history of moderate and/or severe psychiatric disorder had a pre-birth planning meeting at 32
weeks gestation. This involved the prospective parents and all involved health care professionals.
A care pathway for the management of psychiatric emergencies was in place.
At handover meetings, staff routinely referred to the psychological and emotional needs of women,
their relatives and carers. We saw staff discussed all aspects of women’s care including
psychological and emotional needs at handover meetings.
Nutrition and hydration
Staff gave women and babies enough food and drink to meet their needs and improve their
health. They used special feeding and hydration techniques when necessary.
Staff made sure women and babies had enough to eat and/or drink, including those with specialist
nutrition and hydration needs. Women were encouraged to eat and drink as normal in the early
stages of labour to maintain hydration and energy. Staff checked women’s hydration regularly
during labour and treated dehydration with oral or intravenous fluids when needed. Staff supported
women with feeding their baby and respected women’s choice of feeding method. Staff educated
and helped women who wanted to breastfeed. This was confirmed from women we spoke with
and feedback we read. For example, one woman wrote, “[staff member] went out of her way to
help me breastfeed throughout the night and nothing was too much trouble”. From January to
October 2019, 77.2% of women on average initiated breastfeeding at birth. For the same period,
85.3% of women were breastfeeding 10 days after birth. Both breastfeeding rates were higher
(better) than the trust’s target. Community midwives and maternity care assistants provided
20190416 900885 Post-inspection Evidence appendix template v4 Page 199
feeding support to women at home. Staff followed up to date guidance and infant feeding
pathways. Babies were routinely weighed and monitored for jaundice to ensure their nutritional
and hydration needs were being met.
The service did not provide infant formula to women who chose not to breastfeed. Women were
told to bring formula and feeding equipment with them, such as bottles and teats. Infant formula
was provided for babies when clinically indicated, such as concerns with weight and blood sugar
levels, following paediatric review. Staff monitored babies at risk of hypoglycaemia (low blood
sugar) after delivery to ensure blood sugar levels were within the normal range.
There was a milk kitchen on the postnatal ward where women could store expressed breast milk
or formula. Checklists showed the fridge temperature was checked daily to ensure milk was stored
within the recommended range. The fridge was locked which meant milk could not be taken or
tampered with. Stored milk was labelled with the date, time and mother’s name.
Staff fully and accurately completed women’s fluid and baby feeding charts where needed.
Maternity care records we reviewed confirmed this. We saw staff put infant feeding plans in place
and escalated babies for medical review when indicated.
Specialist support from staff such as dietitians, ear, nose and throat (ENT) specialists, cleft lip and
palate specialists and infant feeding specialists was available for women and babies who needed
it. For example, dietetic support was provided for women with pre-existing or gestational diabetes
and women who had a body mass index (BMI) of 40 or higher.
Staff used a nationally recognised screening tool to assess babies with tongue tie who would
benefit from frenulotomy (a procedure that separates tongue tie). Babies with suspected tongue tie
and breastfeeding difficulties were referred to the midwife led frenulotomy clinic for assessment
and division, if appropriate.
Women admitted for planned caesarean section were not left nil by mouth for long periods. Staff
gave women intravenous fluid during and after the procedure to ensure they kept hydrated. After
caesarean section, women could eat and drink as soon as they wished if they were recovering
well with no complications.
Pain relief
Staff assessed and monitored women regularly to see if they were in pain and gave pain
relief in a timely way. They supported those unable to communicate using suitable
assessment tools and gave additional pain relief to ease pain.
Staff assessed women’s pain using a recognised tool and gave pain relief in line with individual
needs and best practice. We saw women’s pain levels were regularly assessed using a numerical
pain scale. Staff could access pain assessment tools for women with communication difficulties
when needed.
Women received pain relief soon after requesting it. Women we spoke with told us they were
asked if they needed pain relief regularly and were given it promptly. Managers did not monitor
epidural waiting times. This meant we could not determine if women were ready to receive an
epidural within 30 minutes from request, in line with national recommendations (OAA/AAGBI,
Guidelines for Obstetric Anaesthetic Services (2013)). Managers told us women were rarely
delayed in having an epidural because a dedicated obstetric anaesthetist was available 24 hours a
20190416 900885 Post-inspection Evidence appendix template v4 Page 200
day, seven days a week. In the event the anaesthetist was busy in theatre, for example, a second
on-call anaesthetist was called. Staff offered women alternative analgesia while they waited.
Staff prescribed, administered and recorded all pain relief accurately. Pain relief could be
prescribed as suppositories or injection if women were unable to tolerate oral medication. We saw
post-operative women were prescribed and given regular pain relief to keep them comfortable.
Women were routinely given local anaesthetic before perineal suturing and were offered non-
steroidal anti-inflammatory drug (NSAID) suppository medicine following suturing, unless
contraindicated. Women who had undergone caesarean section were given pain relief for use at
home when they were discharged.
Midwives provided pregnant women with evidence-based information about the availability and
provision of different types of analgesia. Pharmacological (medicine based) methods of pain relief
were readily available, including ‘gas and air’, opioids (such as pethidine and morphine) and
patient controlled epidural anaesthesia. Non-pharmacological methods of pain relief were also
available, such as transcutaneous electrical nerve stimulation (TENS), hydrotherapy (water) and
aromatherapy. Pain relief options for women who wanted a homebirth were gas and air, TENS or
hydrotherapy. The birthing units offered TENS, hydrotherapy, gas and air, oral morphine and
pethidine. Women who needed stronger pain relief in labour were transferred to delivery suite for
epidural.
Outcomes
Staff monitored the effectiveness of care and treatment. They used the findings to make
improvements and achieved good outcomes for women and babies. The service had been
accredited under the UNICEF UK Baby Friendly Initiative.
The service participated in all relevant national clinical audits. The service performed well in
clinical outcome audits and managers used the results to improve services further. For example,
the service participated in the Avoiding term admissions into neonatal units (Atain) programme.
This was designed to reduce avoidable causes of harm that could lead to infants born at term
(from 37 weeks gestation) being admitted to a neonatal unit. In partnership with neonatal care
staff, the service had introduced initiatives to reduce the number of unexpected term admissions.
This included workstreams for hypoglycaemia, respiratory distress, jaundice, hypothermia and
birth asphyxia (Source: Additional Evidence Request, DR85). From January to October 2019, the
percentage of unexpected term admissions was 2% on average. This was in line with the trust
target.
The tables below summarise the trust’s performance in two national maternity and neonatal audits.
In the latest national audit of perinatal mortality, the trust’s perinatal mortality rate was more than
5% and up to 15% lower (better) than the national average. The trust performed within the
expected range in the National Neonatal Audit Programme for measures related to maternity care.
National Neonatal Audit Programme
Broomfield Hospital
The table below summarises Broomfield Hospital’s performance in the 2018 National Neonatal
Audit Programme against measures related to maternity care.
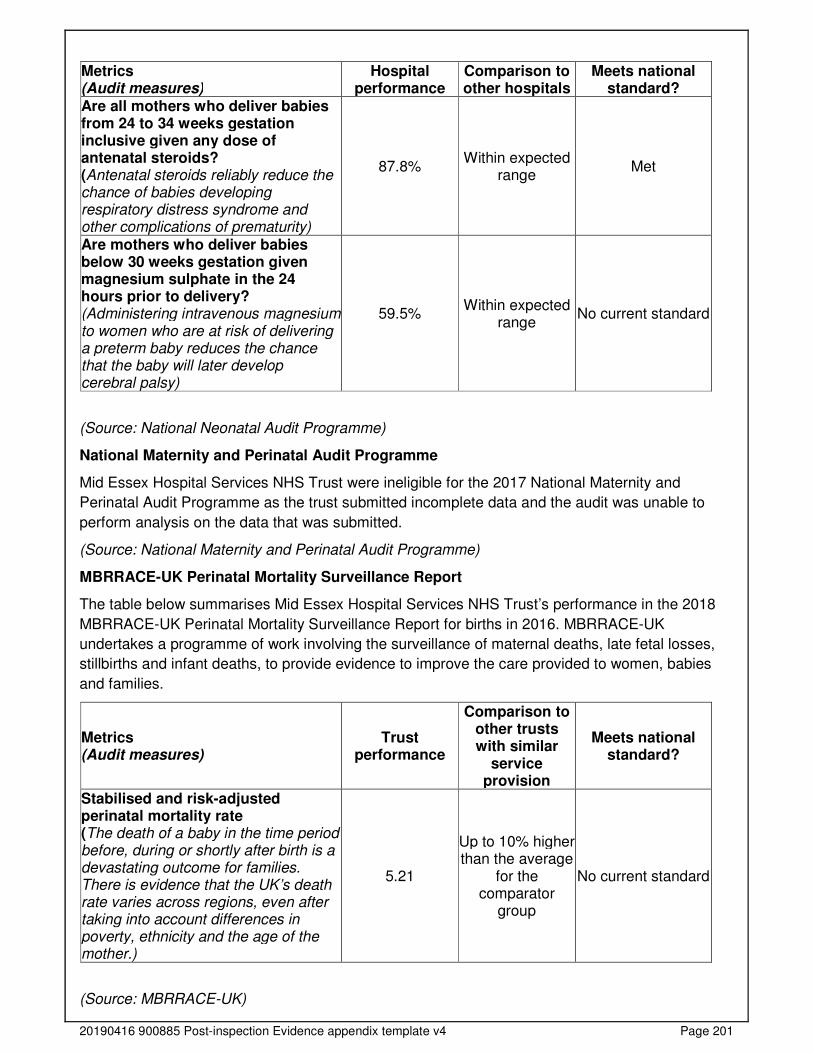
20190416 900885 Post-inspection Evidence appendix template v4 Page 201
Metrics (Audit measures)
Hospital performance
Comparison to other hospitals
Meets national standard?
Are all mothers who deliver babies from 24 to 34 weeks gestation inclusive given any dose of antenatal steroids? (Antenatal steroids reliably reduce the chance of babies developing respiratory distress syndrome and other complications of prematurity)
87.8% Within expected
range Met
Are mothers who deliver babies below 30 weeks gestation given magnesium sulphate in the 24 hours prior to delivery? (Administering intravenous magnesium to women who are at risk of delivering a preterm baby reduces the chance that the baby will later develop cerebral palsy)
59.5% Within expected
range No current standard
(Source: National Neonatal Audit Programme)
National Maternity and Perinatal Audit Programme
Mid Essex Hospital Services NHS Trust were ineligible for the 2017 National Maternity and
Perinatal Audit Programme as the trust submitted incomplete data and the audit was unable to
perform analysis on the data that was submitted.
(Source: National Maternity and Perinatal Audit Programme)
MBRRACE-UK Perinatal Mortality Surveillance Report
The table below summarises Mid Essex Hospital Services NHS Trust’s performance in the 2018
MBRRACE-UK Perinatal Mortality Surveillance Report for births in 2016. MBRRACE-UK
undertakes a programme of work involving the surveillance of maternal deaths, late fetal losses,
stillbirths and infant deaths, to provide evidence to improve the care provided to women, babies
and families.
Metrics (Audit measures)
Trust performance
Comparison to other trusts with similar
service provision
Meets national standard?
Stabilised and risk-adjusted perinatal mortality rate (The death of a baby in the time period before, during or shortly after birth is a devastating outcome for families. There is evidence that the UK’s death rate varies across regions, even after taking into account differences in poverty, ethnicity and the age of the mother.)
5.21
Up to 10% higher than the average
for the comparator
group
No current standard
(Source: MBRRACE-UK)
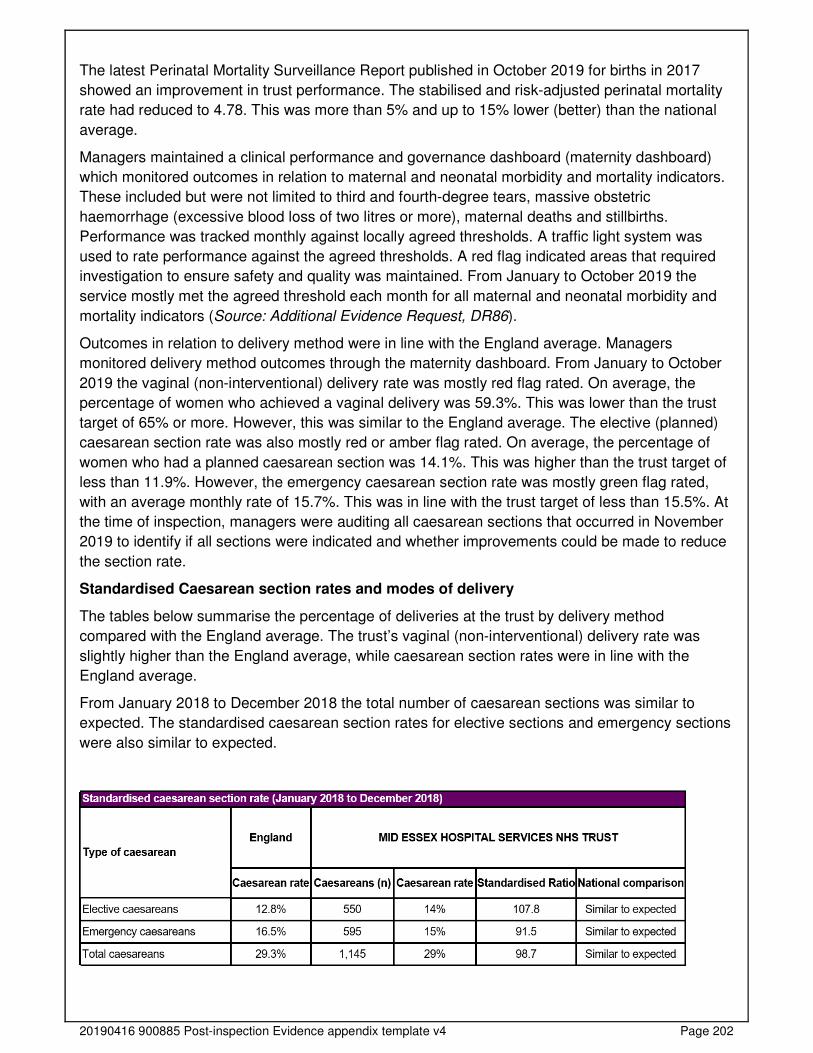
20190416 900885 Post-inspection Evidence appendix template v4 Page 202
The latest Perinatal Mortality Surveillance Report published in October 2019 for births in 2017
showed an improvement in trust performance. The stabilised and risk-adjusted perinatal mortality
rate had reduced to 4.78. This was more than 5% and up to 15% lower (better) than the national
average.
Managers maintained a clinical performance and governance dashboard (maternity dashboard)
which monitored outcomes in relation to maternal and neonatal morbidity and mortality indicators.
These included but were not limited to third and fourth-degree tears, massive obstetric
haemorrhage (excessive blood loss of two litres or more), maternal deaths and stillbirths.
Performance was tracked monthly against locally agreed thresholds. A traffic light system was
used to rate performance against the agreed thresholds. A red flag indicated areas that required
investigation to ensure safety and quality was maintained. From January to October 2019 the
service mostly met the agreed threshold each month for all maternal and neonatal morbidity and
mortality indicators (Source: Additional Evidence Request, DR86).
Outcomes in relation to delivery method were in line with the England average. Managers
monitored delivery method outcomes through the maternity dashboard. From January to October
2019 the vaginal (non-interventional) delivery rate was mostly red flag rated. On average, the
percentage of women who achieved a vaginal delivery was 59.3%. This was lower than the trust
target of 65% or more. However, this was similar to the England average. The elective (planned)
caesarean section rate was also mostly red or amber flag rated. On average, the percentage of
women who had a planned caesarean section was 14.1%. This was higher than the trust target of
less than 11.9%. However, the emergency caesarean section rate was mostly green flag rated,
with an average monthly rate of 15.7%. This was in line with the trust target of less than 15.5%. At
the time of inspection, managers were auditing all caesarean sections that occurred in November
2019 to identify if all sections were indicated and whether improvements could be made to reduce
the section rate.
Standardised Caesarean section rates and modes of delivery
The tables below summarise the percentage of deliveries at the trust by delivery method
compared with the England average. The trust’s vaginal (non-interventional) delivery rate was
slightly higher than the England average, while caesarean section rates were in line with the
England average.
From January 2018 to December 2018 the total number of caesarean sections was similar to
expected. The standardised caesarean section rates for elective sections and emergency sections
were also similar to expected.
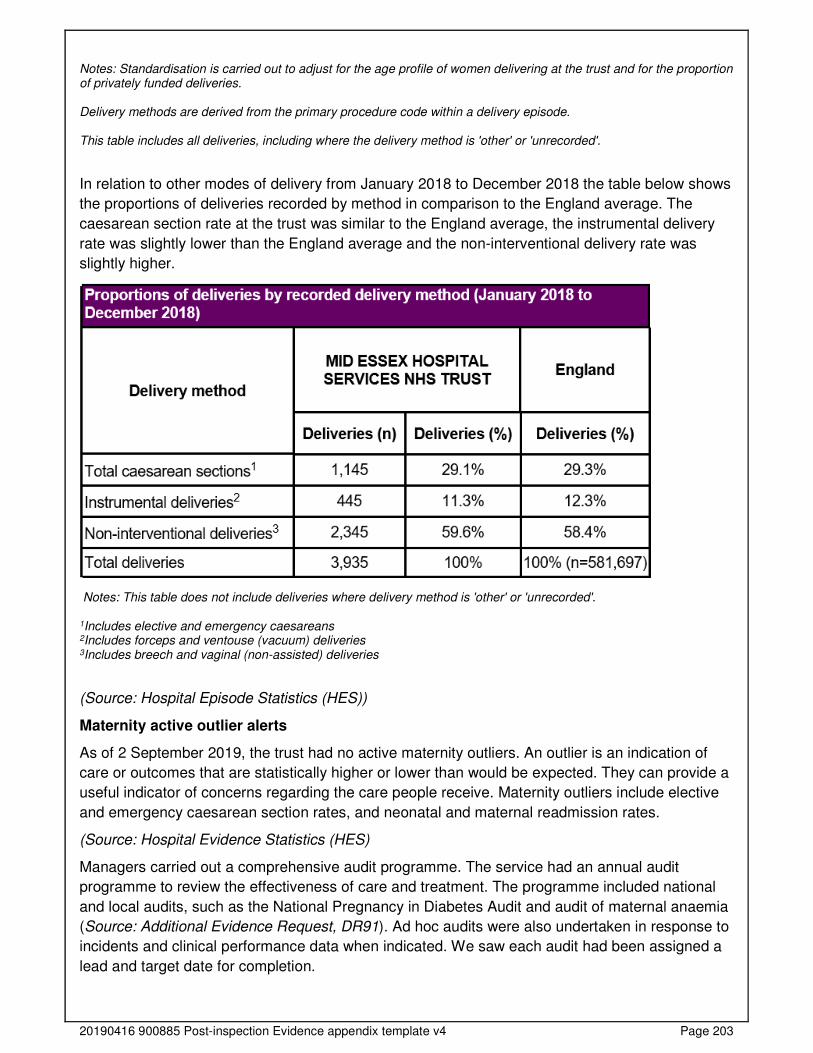
20190416 900885 Post-inspection Evidence appendix template v4 Page 203
Notes: Standardisation is carried out to adjust for the age profile of women delivering at the trust and for the proportion of privately funded deliveries. Delivery methods are derived from the primary procedure code within a delivery episode. This table includes all deliveries, including where the delivery method is 'other' or 'unrecorded'.
In relation to other modes of delivery from January 2018 to December 2018 the table below shows
the proportions of deliveries recorded by method in comparison to the England average. The
caesarean section rate at the trust was similar to the England average, the instrumental delivery
rate was slightly lower than the England average and the non-interventional delivery rate was
slightly higher.
Notes: This table does not include deliveries where delivery method is 'other' or 'unrecorded'. 1Includes elective and emergency caesareans 2Includes forceps and ventouse (vacuum) deliveries 3Includes breech and vaginal (non-assisted) deliveries
(Source: Hospital Episode Statistics (HES))
Maternity active outlier alerts
As of 2 September 2019, the trust had no active maternity outliers. An outlier is an indication of
care or outcomes that are statistically higher or lower than would be expected. They can provide a
useful indicator of concerns regarding the care people receive. Maternity outliers include elective
and emergency caesarean section rates, and neonatal and maternal readmission rates.
(Source: Hospital Evidence Statistics (HES)
Managers carried out a comprehensive audit programme. The service had an annual audit
programme to review the effectiveness of care and treatment. The programme included national
and local audits, such as the National Pregnancy in Diabetes Audit and audit of maternal anaemia
(Source: Additional Evidence Request, DR91). Ad hoc audits were also undertaken in response to
incidents and clinical performance data when indicated. We saw each audit had been assigned a
lead and target date for completion.
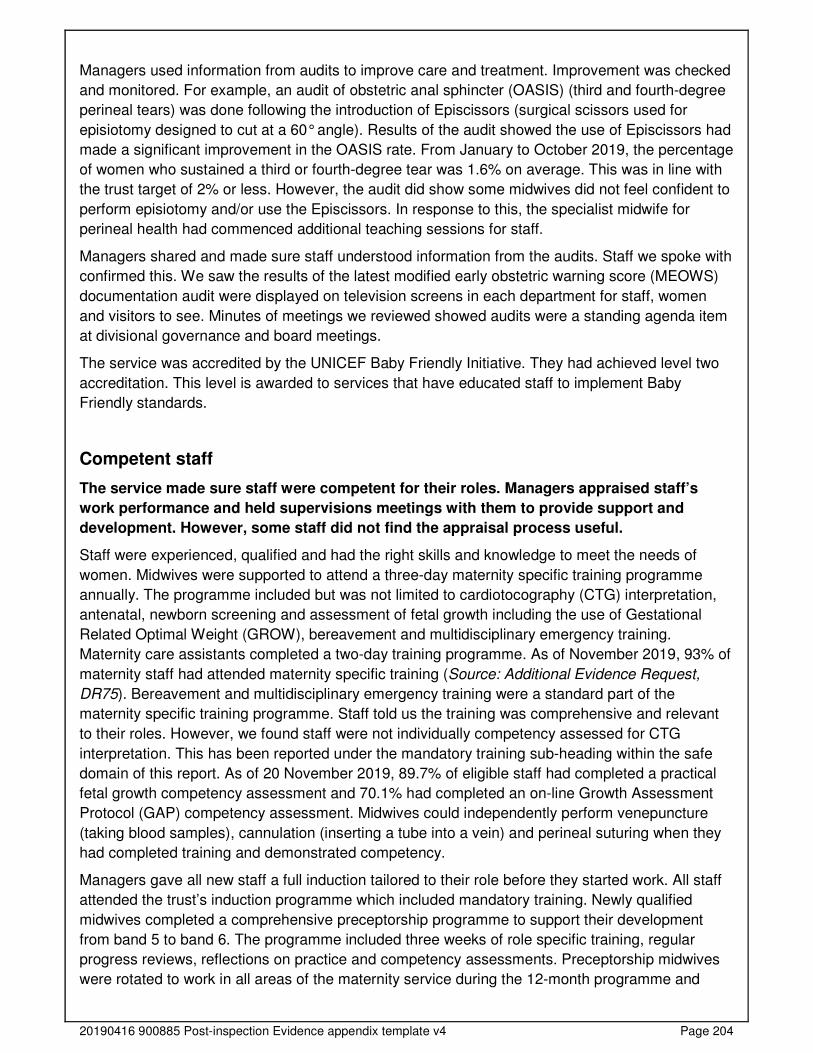
20190416 900885 Post-inspection Evidence appendix template v4 Page 204
Managers used information from audits to improve care and treatment. Improvement was checked
and monitored. For example, an audit of obstetric anal sphincter (OASIS) (third and fourth-degree
perineal tears) was done following the introduction of Episcissors (surgical scissors used for
episiotomy designed to cut at a 60° angle). Results of the audit showed the use of Episcissors had
made a significant improvement in the OASIS rate. From January to October 2019, the percentage
of women who sustained a third or fourth-degree tear was 1.6% on average. This was in line with
the trust target of 2% or less. However, the audit did show some midwives did not feel confident to
perform episiotomy and/or use the Episcissors. In response to this, the specialist midwife for
perineal health had commenced additional teaching sessions for staff.
Managers shared and made sure staff understood information from the audits. Staff we spoke with
confirmed this. We saw the results of the latest modified early obstetric warning score (MEOWS)
documentation audit were displayed on television screens in each department for staff, women
and visitors to see. Minutes of meetings we reviewed showed audits were a standing agenda item
at divisional governance and board meetings.
The service was accredited by the UNICEF Baby Friendly Initiative. They had achieved level two
accreditation. This level is awarded to services that have educated staff to implement Baby
Friendly standards.
Competent staff
The service made sure staff were competent for their roles. Managers appraised staff’s
work performance and held supervisions meetings with them to provide support and
development. However, some staff did not find the appraisal process useful.
Staff were experienced, qualified and had the right skills and knowledge to meet the needs of
women. Midwives were supported to attend a three-day maternity specific training programme
annually. The programme included but was not limited to cardiotocography (CTG) interpretation,
antenatal, newborn screening and assessment of fetal growth including the use of Gestational
Related Optimal Weight (GROW), bereavement and multidisciplinary emergency training.
Maternity care assistants completed a two-day training programme. As of November 2019, 93% of
maternity staff had attended maternity specific training (Source: Additional Evidence Request,
DR75). Bereavement and multidisciplinary emergency training were a standard part of the
maternity specific training programme. Staff told us the training was comprehensive and relevant
to their roles. However, we found staff were not individually competency assessed for CTG
interpretation. This has been reported under the mandatory training sub-heading within the safe
domain of this report. As of 20 November 2019, 89.7% of eligible staff had completed a practical
fetal growth competency assessment and 70.1% had completed an on-line Growth Assessment
Protocol (GAP) competency assessment. Midwives could independently perform venepuncture
(taking blood samples), cannulation (inserting a tube into a vein) and perineal suturing when they
had completed training and demonstrated competency.
Managers gave all new staff a full induction tailored to their role before they started work. All staff
attended the trust’s induction programme which included mandatory training. Newly qualified
midwives completed a comprehensive preceptorship programme to support their development
from band 5 to band 6. The programme included three weeks of role specific training, regular
progress reviews, reflections on practice and competency assessments. Preceptorship midwives
were rotated to work in all areas of the maternity service during the 12-month programme and
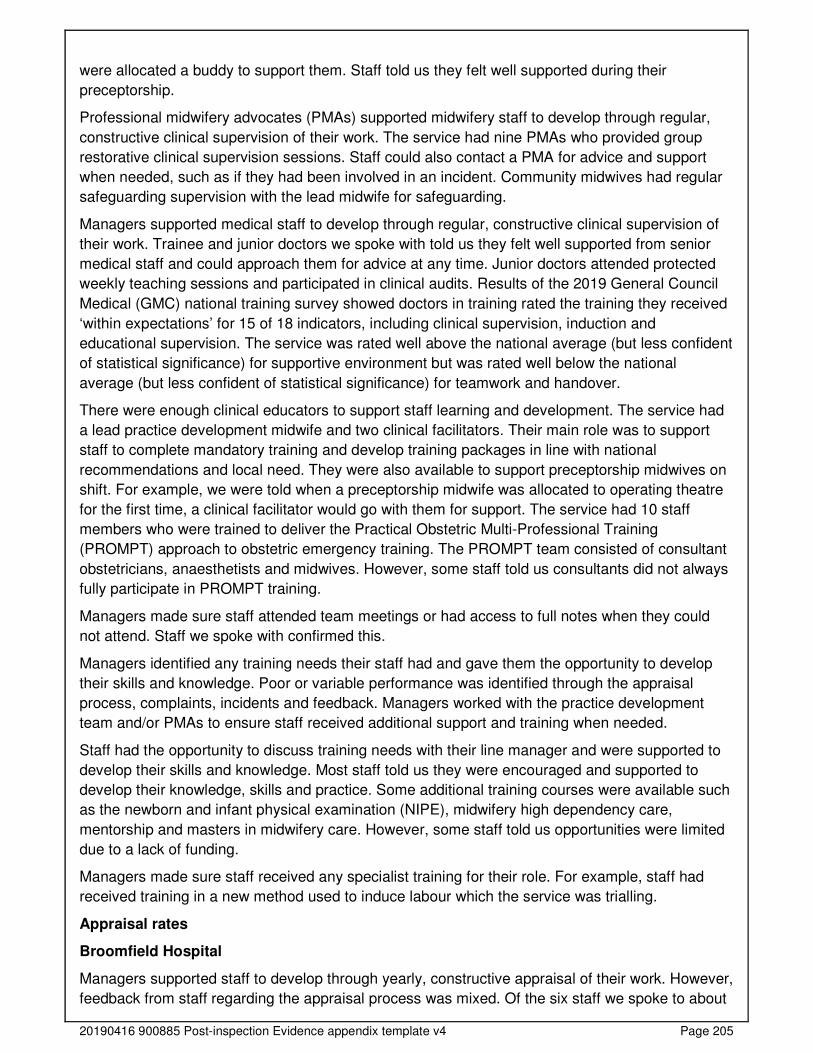
20190416 900885 Post-inspection Evidence appendix template v4 Page 205
were allocated a buddy to support them. Staff told us they felt well supported during their
preceptorship.
Professional midwifery advocates (PMAs) supported midwifery staff to develop through regular,
constructive clinical supervision of their work. The service had nine PMAs who provided group
restorative clinical supervision sessions. Staff could also contact a PMA for advice and support
when needed, such as if they had been involved in an incident. Community midwives had regular
safeguarding supervision with the lead midwife for safeguarding.
Managers supported medical staff to develop through regular, constructive clinical supervision of
their work. Trainee and junior doctors we spoke with told us they felt well supported from senior
medical staff and could approach them for advice at any time. Junior doctors attended protected
weekly teaching sessions and participated in clinical audits. Results of the 2019 General Council
Medical (GMC) national training survey showed doctors in training rated the training they received
‘within expectations’ for 15 of 18 indicators, including clinical supervision, induction and
educational supervision. The service was rated well above the national average (but less confident
of statistical significance) for supportive environment but was rated well below the national
average (but less confident of statistical significance) for teamwork and handover.
There were enough clinical educators to support staff learning and development. The service had
a lead practice development midwife and two clinical facilitators. Their main role was to support
staff to complete mandatory training and develop training packages in line with national
recommendations and local need. They were also available to support preceptorship midwives on
shift. For example, we were told when a preceptorship midwife was allocated to operating theatre
for the first time, a clinical facilitator would go with them for support. The service had 10 staff
members who were trained to deliver the Practical Obstetric Multi-Professional Training
(PROMPT) approach to obstetric emergency training. The PROMPT team consisted of consultant
obstetricians, anaesthetists and midwives. However, some staff told us consultants did not always
fully participate in PROMPT training.
Managers made sure staff attended team meetings or had access to full notes when they could
not attend. Staff we spoke with confirmed this.
Managers identified any training needs their staff had and gave them the opportunity to develop
their skills and knowledge. Poor or variable performance was identified through the appraisal
process, complaints, incidents and feedback. Managers worked with the practice development
team and/or PMAs to ensure staff received additional support and training when needed.
Staff had the opportunity to discuss training needs with their line manager and were supported to
develop their skills and knowledge. Most staff told us they were encouraged and supported to
develop their knowledge, skills and practice. Some additional training courses were available such
as the newborn and infant physical examination (NIPE), midwifery high dependency care,
mentorship and masters in midwifery care. However, some staff told us opportunities were limited
due to a lack of funding.
Managers made sure staff received any specialist training for their role. For example, staff had
received training in a new method used to induce labour which the service was trialling.
Appraisal rates
Broomfield Hospital
Managers supported staff to develop through yearly, constructive appraisal of their work. However,
feedback from staff regarding the appraisal process was mixed. Of the six staff we spoke to about
20190416 900885 Post-inspection Evidence appendix template v4 Page 206
the appraisal process, three told us they found it beneficial while the other three felt it was a ‘tick
box exercise’.
As of August 2019, 86.6% of required staff in maternity at Broomfield Hospital received an
appraisal, which was lower than the trust target of 90%. We found appraisal completion rates had
improved on inspection. As of November 2019, 94% of midwives, medical staff and maternity care
assistants had received an annual appraisal (Source: Additional Evidence Request, DR79).
A breakdown by staff group can be found in the table below:
Staff group
As of August 2019 Staff who
received an appraisal
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Healthcare scientists 1 1 100.0% 90% Yes Additional clinical services 26 27 96.3% 90% Yes Nursing and midwifery registered 94 106 88.7% 90% No Administrative and clerical 19 24 79.2% 90% No Medical and dental 15 21 71.4% 90% No Total 155 179 86.6% 90% No
(Source: Routine Provider Information Request (RPIR) – Appraisal tab)
Multidisciplinary working
Doctors, midwives and other healthcare professionals worked together as a team to benefit
women and babies. They supported each other to provide good care.
Staff held regular and effective multidisciplinary meetings to discuss women and babies and
improve their care. All necessary staff were involved in assessing, planning and delivering
women’s care and treatment. We observed a multidisciplinary handover and ward round, which
was attended by the obstetric medical team, delivery suite coordinator, anaesthetists and
midwifery staff. Women with known risks were reviewed with care and treatment planned.
Staff worked across health care disciplines and with other agencies when required to care for
women and babies. Staff worked together with other specialties to benefit women and babies. This
included endocrinology for women with diabetes, paediatrics, haematology, psychiatry,
anaesthetics and physiotherapy. Women with a high body mass index (40 or above) were
reviewed by a consultant anaesthetist around 32 weeks gestation to discuss management plans
for labour and delivery. Physiotherapy staff attended the postnatal ward daily, Monday to Friday, to
provide care and treatment to women who would benefit from their input, such as women who had
a caesarean section or had sustained a third or fourth-degree tear. A multidisciplinary team cared
for women with multiple pregnancies, which included a multiple pregnancy specialist midwife and
fetal medicine specialist obstetrician. Women and babies who needed higher levels of care were
referred to neighbouring trusts with tertiary fetal medicine centres as needed. Obstetric and
midwifery staff were involved in the management and care of pregnant or postnatal women who
were admitted to non-maternity wards for medical reasons. A member of the safeguarding team
visited the wards daily, Monday to Friday, to support the care of women with safeguarding
concerns. The team worked closely with other professionals and agencies, such as health visitors
and social workers.
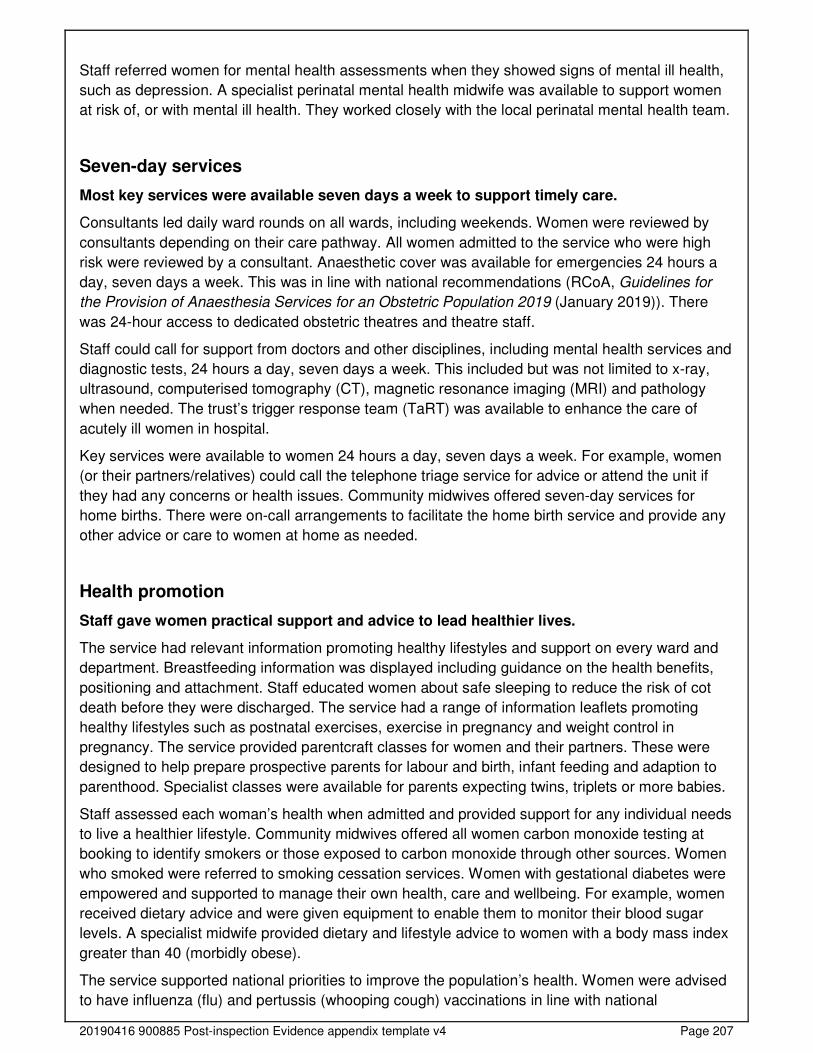
20190416 900885 Post-inspection Evidence appendix template v4 Page 207
Staff referred women for mental health assessments when they showed signs of mental ill health,
such as depression. A specialist perinatal mental health midwife was available to support women
at risk of, or with mental ill health. They worked closely with the local perinatal mental health team.
Seven-day services
Most key services were available seven days a week to support timely care.
Consultants led daily ward rounds on all wards, including weekends. Women were reviewed by
consultants depending on their care pathway. All women admitted to the service who were high
risk were reviewed by a consultant. Anaesthetic cover was available for emergencies 24 hours a
day, seven days a week. This was in line with national recommendations (RCoA, Guidelines for
the Provision of Anaesthesia Services for an Obstetric Population 2019 (January 2019)). There
was 24-hour access to dedicated obstetric theatres and theatre staff.
Staff could call for support from doctors and other disciplines, including mental health services and
diagnostic tests, 24 hours a day, seven days a week. This included but was not limited to x-ray,
ultrasound, computerised tomography (CT), magnetic resonance imaging (MRI) and pathology
when needed. The trust’s trigger response team (TaRT) was available to enhance the care of
acutely ill women in hospital.
Key services were available to women 24 hours a day, seven days a week. For example, women
(or their partners/relatives) could call the telephone triage service for advice or attend the unit if
they had any concerns or health issues. Community midwives offered seven-day services for
home births. There were on-call arrangements to facilitate the home birth service and provide any
other advice or care to women at home as needed.
Health promotion
Staff gave women practical support and advice to lead healthier lives.
The service had relevant information promoting healthy lifestyles and support on every ward and
department. Breastfeeding information was displayed including guidance on the health benefits,
positioning and attachment. Staff educated women about safe sleeping to reduce the risk of cot
death before they were discharged. The service had a range of information leaflets promoting
healthy lifestyles such as postnatal exercises, exercise in pregnancy and weight control in
pregnancy. The service provided parentcraft classes for women and their partners. These were
designed to help prepare prospective parents for labour and birth, infant feeding and adaption to
parenthood. Specialist classes were available for parents expecting twins, triplets or more babies.
Staff assessed each woman’s health when admitted and provided support for any individual needs
to live a healthier lifestyle. Community midwives offered all women carbon monoxide testing at
booking to identify smokers or those exposed to carbon monoxide through other sources. Women
who smoked were referred to smoking cessation services. Women with gestational diabetes were
empowered and supported to manage their own health, care and wellbeing. For example, women
received dietary advice and were given equipment to enable them to monitor their blood sugar
levels. A specialist midwife provided dietary and lifestyle advice to women with a body mass index
greater than 40 (morbidly obese).
The service supported national priorities to improve the population’s health. Women were advised
to have influenza (flu) and pertussis (whooping cough) vaccinations in line with national

20190416 900885 Post-inspection Evidence appendix template v4 Page 208
recommendations (NICE, Antenatal care for uncomplicated pregnancies: CG62, (February 2019)).
Maternity records we reviewed confirmed this.
Consent, Mental Capacity Act and Deprivation of Liberty Safeguards
Staff supported women to make informed decisions about their care and treatment. They
followed national guidance to gain women’s consent. They knew how to support women
who lacked capacity to make their own decisions or were experiencing mental ill health.
However, not all staff were up to date with Mental Capacity Act and Deprivation of Liberty
Safeguards training.
Staff understood the relevant consent and decision-making requirements of legislation and
guidance, including the Mental Health Act, Mental Capacity Act 2005 and the Children Acts 1989
and 2004 and they knew who to contact for advice. Staff could explain their roles and
responsibilities if a woman lacked capacity to make their own decisions or was experiencing
mental ill health.
Staff knew how to access policy and get accurate advice on the Mental Capacity Act and
Deprivation of Liberty Safeguards. Staff understood Gillick competence and Fraser Guidelines and
supported young women who wished to make decisions about their treatment. Up to date policies
were available on the trust’s intranet regarding consent, Deprivation of Liberty Safeguards and the
Mental Capacity Act (MCA) 2005, including the treatment of young people and children in
accordance with Gillick Competence and Fraser Guidelines. Gillick Competence is a term used in
medical law to decide whether a child (under 16 years of age) can consent to his or her own
medical treatment, without the need for parental consent. Fraser Guidelines are used specifically
to decide if a young person can consent to contraceptive or sexual health advice and treatment.
Staff demonstrated how to access policies through the trust’s intranet. Staff could contact
specialist midwives, nurses and other professionals who had expertise with supporting women in
vulnerable circumstances for advice when needed, such as teenagers and women experiencing
mental ill health.
Staff gained consent from women for their care and treatment in line with legislation and guidance.
We saw staff gained verbal and/or written consent from women prior to undertaking any
procedures or treatment. Women told us staff explained care and treatment and sought their
consent. One woman told us, “consent is always gained before treatment”. This was in line with
national legislation (Health and Social Care Act 2008 (Regulated Activities) Regulations 2014:
Regulation 11 Need for consent (November 2014) and national guidance (Department of Health,
Reference guide to consent for examination or treatment (July 2009)).
Staff clearly recorded consent in women’s records. Staff documented consent for care and
treatment given, such as vaginal examinations. Medical staff obtained written consent from women
prior to surgery, such as caesarean section. The maternity care records we reviewed confirmed
this.
Staff made sure women consented to treatment based on all the information available. We
observed staff clearly explained the benefits and risks of induction of labour to a woman and her
partner. This enabled them to make an informed decision about their care.
Mental Capacity Act and Deprivation of Liberty training completion
20190416 900885 Post-inspection Evidence appendix template v4 Page 209
Not all clinical staff had completed training on the Mental Capacity Act and Deprivation of Liberty
Safeguards.
The trust set a target of 95% for the completion of Mental Capacity Act (MCA) training. The trust
stated that Deprivation of Liberty Safeguarding (DoLS) training was included in the MCA training
module.
Broomfield Hospital
A breakdown of compliance for the MCA/DoLS training course as of August 2019 for qualified
nursing and medical staff in maternity at Broomfield Hospital is shown below:
Staffing group As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Medical and dental 18 21 85.7% 95% No Nursing and midwifery registered 15 22 68.2% 95% No
In maternity, the target was not met for MCA/DoLS training module by medical staff or qualified
midwives at Broomfield Hospital.
(Source: Routine Provider Information Request (RPIR) – Training tab)
As of November 2019, completion rates remained below the trust target. The service reported
80% of medical and midwifery staff had completed MCA/DoLS training.
Is the service caring?
Compassionate care
Staff treated women with compassion and kindness, respected their privacy and dignity,
and took account of their individual needs.
Staff were discreet and responsive when caring for women. Staff took time to interact with women
and those close to them in a respectful and considerate way. Staff introduced themselves to
women and their birthing partners and made them aware of their roles and responsibilities. We
observed staff were polite, friendly and warm with women and their families.
Women said staff treated them well and with kindness. Women and partners we spoke with were
positive about the care they had received. One woman told us, “The midwives are incredible,
100% excellent”. Several other women described the staff as, really kind, friendly and supportive
and told us they felt, safe, secure and cared for. We also read many compliments and thank you
cards from women regarding their care. One woman wrote, “Every single midwife treated me with
kindness, compassion and respect”.
Staff followed policy to keep women’s care and treatment confidential. Women’s preferences for
sharing information with their partner and family members was established and respected. We
saw staff discussed women’s care and treatment in non-public areas to minimise the risk of
confidential information being overheard. Women’s privacy and dignity was respected. Staff closed
curtains and doors to protect women’s privacy and knocked on doors before they entered rooms.
Birthing rooms had “in use” signs by the door to alert staff when they were occupied and prevent
anyone from entering without consent.
20190416 900885 Post-inspection Evidence appendix template v4 Page 210
Staff understood and respected the individual needs of each woman and showed understanding
and a non-judgmental attitude when caring for or discussing women with mental health needs. We
observed staff discussed women in vulnerable circumstances at handovers with compassion,
respect and sensitivity. Women with mental health concerns could be referred to the perinatal
mental health team for additional support, care and advice. Staff responded in a compassionate,
timely and appropriate way when women were in pain or were anxious and distressed. For
example, we saw staff took time to listen to women who were worried about their baby’s
movements and invited them to attend the unit for timely review.
Staff understood and respected the personal, cultural, social and religious needs of women and
how they may relate to care needs. Women we spoke with, maternity care records we reviewed
and observations we made confirmed this.
Friends and Family test performance
Friends and family test performance (antenatal), Mid Essex Hospital Services NHS Trust
From July 2018 to June 2019 the trust did not receive any responses to the maternity Friends and
Family Test (antenatal).
Friends and family test performance (birth), Mid Essex Hospital Services NHS Trust
From July 2018 to June 2019 the trust’s maternity Friends and Family Test (birth) performance (%
recommended) fluctuated around the England average. The trust’s performance was 90% or
greater in all months. Performance was lowest in October 2018 (91%) and February 2019 (90%).
Friends and family test performance (postnatal ward), Mid Essex Hospital Services NHS
Trust
From July 2018 to June 2019 the trust’s maternity Friends and Family Test (postnatal ward)
performance (% recommended) fluctuated around the England average. The trust’s performance
was 90% or greater in all months.
20190416 900885 Post-inspection Evidence appendix template v4 Page 211
Friends and family test performance (postnatal community), Mid Essex Hospital Services
NHS Trust
From July 2018 to June 2019 the trust’s maternity Friends and Family Test (postnatal community)
fluctuated around the England average. The trust’s performance was 94% or greater in all months.
(Source: Friends and Family Test – NHS England)
CQC Survey of women’s experiences of maternity services 2018
The trust performed similarly to other trusts for 17 out of 19 questions in the CQC maternity survey
2018. The trust performed worse than other trusts for the two remaining survey questions. Both
questions were related to staff during labour and birth.
Area Question Score (0-10)
RAG
Labour and birth
At the very start of your labour, did you feel that you were given appropriate advice and support when you contacted a midwife or the hospital?
8.1 About the
same
During your labour, were you able to move around and choose the position that made you most comfortable?
7.4 About the
same
Did you have skin to skin contact (baby naked, directly on your chest or tummy) with your baby shortly after the birth?
9.1 About the
same
If your partner or someone else close to you was involved in your care during labour and birth, were they able to be involved as much as they wanted?
9.4 About the
same
Staff during labour and birth
Did the staff treating and examining you introduce themselves?
9.3 About the
same
Were you and/or your partner or a companion left alone by midwives or doctors at a time when it worried you?
6.6 Worse
If you raised a concern during labour and birth, did you feel that it was taken seriously?
7.0 Worse
If attention was needed during labour and birth, did a staff member help you within a reasonable amount of time
8.8 About the
same
Thinking about your care during labour and birth, were you spoken to in a way you could understand?
9.5 About the
same
Thinking about your care during labour and birth, were you involved enough in decisions about your care?
8.3 About the
same
Thinking about your care during labour and birth, were you treated with respect and dignity?
9.1 About the
same
Did you have confidence and trust in the staff caring for you during your labour and birth?
8.6 About the
same
20190416 900885 Post-inspection Evidence appendix template v4 Page 212
Care in hospital after the birth
Looking back, do you feel that the length of your stay in hospital after the birth was appropriate?
7.2 About the
same
Looking back, was there a delay in being discharged from hospital?
5.3 About the
same
Thinking about response time, if attention was needed after the birth, did a member of staff help within a reasonable amount of time?
7.2 About the
same
Thinking about the care you received in hospital after the birth of your baby, were you given the information or explanations you needed?
7.5 About the
same
Thinking about the care you received in hospital after the birth of your baby, were you treated with kindness and understanding?
8.2 About the
same
Thinking about your stay in hospital, was your partner who was involved in your care able to stay with you as much as you wanted?
5.6 About the
same
Thinking about your stay in hospital, how clean was the hospital room or ward you were in?
9.2 About the
same
(Source: CQC Survey of Women’s Experiences of Maternity Services 2018)
Emotional support
Staff provided emotional support to women, partners and families to minimise their
distress. They understood women’s personal, cultural and religious needs. Staff were
committed to doing all they could to support the emotional needs of bereaved women, their
partners and families.
Staff gave women and those close to them help, emotional support and advice when they needed
it. Staff recognised when women needed time to talk to them and they went out of their way to
provide this. We saw staff provided open and honest answers to questions and gave as much
reassurance as possible. Women we spoke with said staff were supportive and they knew who to
contact for advice if they had any concerns.
Staff supported women who became distressed in an open environment and helped them maintain
their privacy and dignity. Women who were separated from their baby were given a side room to
minimise any distress caused by being with other mothers and their babies. Staff met women with
a known pregnancy loss at the entrance to delivery suite and escorted them to their birthing room.
Staff undertook training on breaking bad news and demonstrated empathy when having difficult
conversations. The service had a specialist bereavement midwife who provided training for staff.
Staff were committed to doing all they could to support the emotional and individual needs of
women, partners and families whose baby had died. The specialist bereavement midwife
supported parents from their initial loss, throughout their time in hospital and their return home. We
saw many compliments from bereaved parents about the care and support they had received. One
mother wrote, “Your support pre and post our bereavement has gone above and beyond what we
could ever have imagined”. Another wrote, “The midwives who cared for me and my baby were
great and did an amazing job. [Staff] made an unbearable night more bearable, thank you”.
Another wrote, “Lovely staff, could not have asked for better…incredible and thoughtful in every
way”.
20190416 900885 Post-inspection Evidence appendix template v4 Page 213
Staff understood the emotional and social impact that a person’s care, treatment or condition had
on their wellbeing and on those close to them. Staff routinely assessed women’s mental health
and emotional wellbeing throughout the antenatal and postnatal period. They recognised when
women would benefit from additional care and support and referred to specialist services when
needed, such as the perinatal mental health team. A debriefing service was also available. This
provided women and their partners with the opportunity to discuss any unresolved concerns or
issues they had regarding their pregnancy or birth experience. Women and their families were
given time with the baby they had lost.
Feedback showed 90% of bereaved parents felt they were given the opportunity to spend the time
they wanted with their baby. The service had a memorial frame for bereaved parents to let them
know they were not alone. Parents could write their baby’s name on a wooden butterfly and place
it in the memorial frame. The hospital held an annual service of remembrance for bereaved
families who had lost a child before or after birth. Women had access to other support services
who provided both practical advice and emotional support. Examples included local and national
baby loss charities, such as Aching Arms and Sands (Stillbirth and neonatal death), and TAMBA
(twins and multiple births association).
Understanding and involvement of patients and those close to them
Staff supported and involved women, partners and families to understand their condition
and make decisions about their care and treatment.
Staff made sure women and those close to them understood their care and treatment. All the
women and partners we spoke with felt involved in their care and had received the information
they needed to make informed decisions about their care. Feedback we read confirmed this. For
example, one woman wrote, “We felt so supported in every decision we made and were given time
to make these”. Feedback from bereaved parents showed 90% felt they were involved in any
decisions about their baby, and 100% felt they were given time and an opportunity to express their
wishes regarding funeral and memorial arrangements for their baby.
Staff talked with women, families and carers in a way they could understand, using communication
aids where necessary. Staff clearly explained planned care and treatment with women and their
partners. We observed this during the inspection. We saw staff made sure women understood
what was said to them and took time to answer any questions they had.
Staff supported women to make informed decisions about their care. Women were involved in
decisions about their choice of birth at booking and throughout their pregnancy. Staff encouraged
them to make birth plans which met their individual needs. Partners were included and involved
where possible. For example, they could cut their baby’s cord at delivery where appropriate and
have skin-to-skin contact with their baby. Professional midwifery advocates were also available to
support women to develop care plans that met their individual needs. Bereaved women and
families had the opportunity to create memories with their baby if they wished, such as bathing
and dressing them. Feedback from bereaved parents showed 100% felt they were given the
opportunity to create memories with their baby in the time they needed without feeling rushed.
Women and their families could give feedback on the service and their treatment and staff
supported them to do this. Staff sought feedback from women and those close to them through a
range of methods, including national patient survey schemes such as the Friends and Family Test
and local surveys. For example, the specialist bereavement midwife sent a questionnaire to all
bereaved parents, so care provision could be improved where needed. The survey included
20190416 900885 Post-inspection Evidence appendix template v4 Page 214
questions on their experience of the environment, how they were communicated with and if their
individual needs and wishes were met. Feedback showed most parents were very positive about
all aspects of care and support they received.
A high proportion of women gave positive feedback about the service in the Friends and Family
Test survey. In September 2019, 98% of women who completed the survey after the birth of their
baby would recommend the service to their family and friends.
Is the service responsive?
Service delivery to meet the needs of local people
The service planned and provided care in a way that met the needs of local people and the
communities served. It also worked with others in the wider system and local organisations
to plan care. However, the service did not have the capacity to meet national requirements
for ultrasound scanning services. The service was acting to address this.
Managers planned and organised services, so they met the changing needs of the local
population. The service was working with local stakeholders and neighbouring hospitals within the
trust to establish a local maternity system (LMS) to improve maternal and neonatal safety across
the clinical network. The purpose of the LMS was to deliver the national priorities for maternity
care provision (National Maternity Review, Better Births: Improving outcomes of maternity services
in England (2016)). Priorities for the LMS included delivering all five aspects of the Saving Babies’
Lives care bundle (version two) and achieving 35% continuity of carer by March 2020 (Source:
Additional Evidence Request, DR66).
Managers identified where people’s needs and choices were not being met and acted to develop
and improve services. For example, the service did not have transitional care for babies who
needed more nursing care and monitoring than that routinely provided on a postnatal ward. Babies
had to be taken to the neonatal intensive care unit (NICU) if they needed treatment such as
antibiotics. This meant babies could sometimes be separated from their mothers if the mother was
unable to attend NICU with them for any reason. Managers told us they were developing a
transitional care model to minimise the number of babies that had to leave their mother for
treatment. This model would enable babies to receive treatment on the postnatal ward next to their
mother. Managers had set aside two beds on the postnatal ward for transitional care and were
recruiting for neonatal nurses to staff the service at the time of our inspection.
Women did not always have access to ultrasound scanning services in a timely manner.
Managers recognised this was a risk and added the lack of scanning availability to the service’s
risk register in May 2019. Managers told us the radiology department had developed an action
plan to address this risk, which included the recruitment of additional sonographers. Minutes of the
women’s and children’s risk register review meeting held in October 2019 reported scans were
currently being undertaken in line with national recommendations. However, the current capacity
would not enable them to meet the recommendations of Saving Babies’ Lives care bundle (version
two), which must be implemented by March 2020 (Source: Additional Evidence Request, DR83).
Feedback from bereaved parents showed they were not able to access counselling services when
they needed it. Counselling services were provided by another provider and we were told by a
lead midwife the waiting list was eight months. The specialist bereavement midwife had acted on
this feedback and funding had been secured for a pilot counselling service at the hospital. This
would be provided by the hospital’s psychotherapy and counselling services department.

20190416 900885 Post-inspection Evidence appendix template v4 Page 215
Antenatal care was accessible to pregnant women. Women accessed maternity services through
their community midwife or GP. Women could also email the service to arrange their first booking
appointment. Women were given an informed choice about where they gave birth, and with
consideration of their risk. Midwifery led models of care were offered to women with an
uncomplicated pregnancy. This included home birth or delivery in either the standalone birthing
units or hospital-based midwife led unit (MLU). This was in line with national guidance (NICE,
Antenatal care: QS22, statement 2 (April 2016)). Women with an existing medical condition,
complication of pregnancy or previous complications in pregnancy and/or labour were advised to
have their baby in the consultant led unit (CLU) (delivery suite).
The service was developing continuity of carer models at the time of our inspection. Managers told
us 11% to 19% of women on average received continuity of carer throughout their pregnancy, birth
and postnatal period. The service hoped to increase this to 35% by March 2020, in line with
national recommendations (National Maternity Review, Better Births: Improving outcomes of
maternity services in England (2016)). Actions taken to increase continuity of carer included the
recruitment of a lead midwife for Better Births and additional midwives. Community midwives we
spoke with told us they tried to provide continuity of carer for at least two women per midwife per
month. They told us they prioritised vulnerable women for continuity of carer where possible. A
named midwife cared for women throughout their pregnancy. Care was shared with a named
consultant if the woman was considered high-risk. Most women we spoke with told us they had
seen the same midwife throughout their pregnancy.
The service had systems to help care for women in need of additional support or specialist
intervention. Specialist midwife clinics were provided for women with diabetes, multiple
pregnancies and who were morbidly obese (body mass index over 40). Specialist consultant
clinics were provided for diabetes, fetal medicine and maternal medicine. The service had a
midwife led birth after caesarean section clinic. This meant women who have had a previous
caesarean could explore birth choices for their current pregnancy. This was in line with national
guidance (NICE, Caesarean section: QS32, statement 1 (June 2013)).
Staff could access emergency mental health support 24 hours a day, seven days a week for
women with mental health problems and learning disabilities. Staff working at the hospital or in the
community could contact the crisis team for urgent support when needed. The service had a
specialist perinatal mental health midwife. They held weekly clinics at either the hospital or
standalone birthing units for women with moderate or high mental health risks. They worked
closely with the local perinatal mental health liaison team to plan care, treatment and support for
women who needed it. There was a mother and baby unit located close to the hospital for mothers
who had severe mental health concerns and needed admission for specialist care and treatment.
The trust had a learning disability hospital liaison nurse who was available to support women with
learning disabilities.
Facilities and premises were mostly appropriate for the services being delivered. The service had
a dedicated bereavement room to ensure women and families were cared for while grieving. The
room was decorated and furbished to create a homely environment, with double bed, sofa,
nursery, kitchen and bathroom facilities. However, the room was located at one end of the delivery
suite. This meant bereaved parents could hear other activity. This was not in line with national
recommendations (Stillbirth and neonatal death charity (Sands), Stillbirth: how professionals can
make a difference (2015)). Staff were mindful of this and told us they would not use the
neighbouring delivery room if the bereavement room was in use, wherever possible. Staff also met
women with a known pregnancy loss at the entrance to delivery suite and escorted them to their
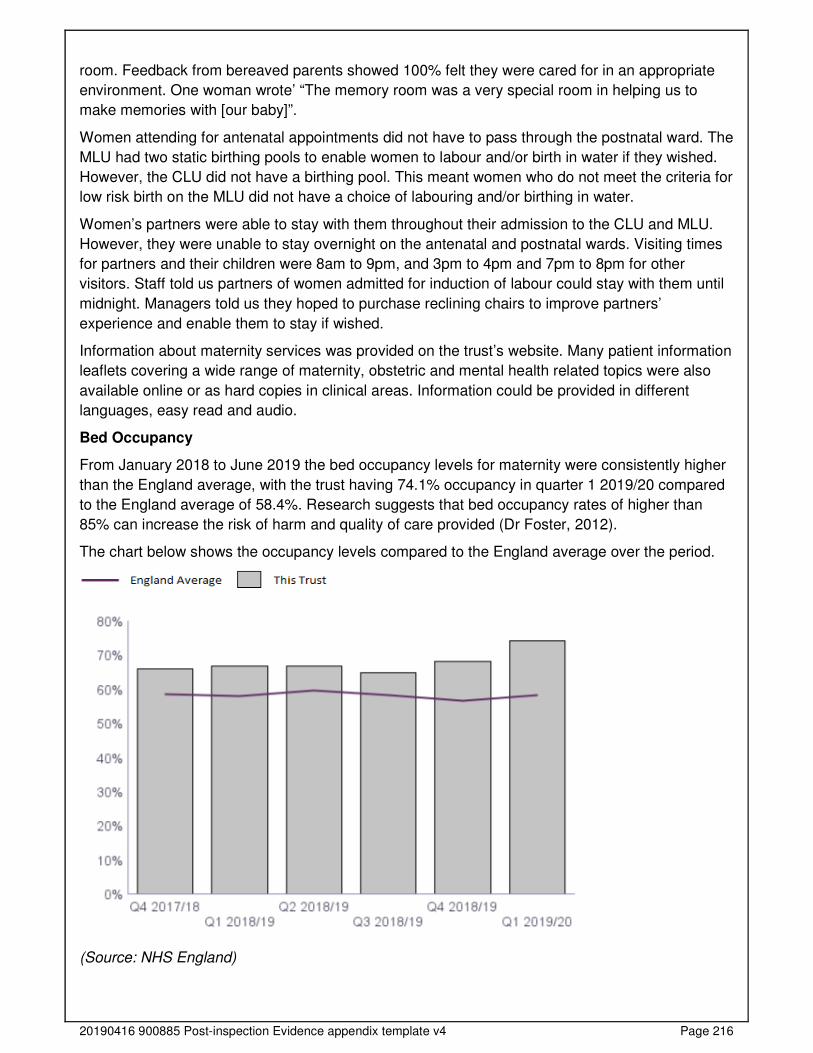
20190416 900885 Post-inspection Evidence appendix template v4 Page 216
room. Feedback from bereaved parents showed 100% felt they were cared for in an appropriate
environment. One woman wrote’ “The memory room was a very special room in helping us to
make memories with [our baby]”.
Women attending for antenatal appointments did not have to pass through the postnatal ward. The
MLU had two static birthing pools to enable women to labour and/or birth in water if they wished.
However, the CLU did not have a birthing pool. This meant women who do not meet the criteria for
low risk birth on the MLU did not have a choice of labouring and/or birthing in water.
Women’s partners were able to stay with them throughout their admission to the CLU and MLU.
However, they were unable to stay overnight on the antenatal and postnatal wards. Visiting times
for partners and their children were 8am to 9pm, and 3pm to 4pm and 7pm to 8pm for other
visitors. Staff told us partners of women admitted for induction of labour could stay with them until
midnight. Managers told us they hoped to purchase reclining chairs to improve partners’
experience and enable them to stay if wished.
Information about maternity services was provided on the trust’s website. Many patient information
leaflets covering a wide range of maternity, obstetric and mental health related topics were also
available online or as hard copies in clinical areas. Information could be provided in different
languages, easy read and audio.
Bed Occupancy
From January 2018 to June 2019 the bed occupancy levels for maternity were consistently higher
than the England average, with the trust having 74.1% occupancy in quarter 1 2019/20 compared
to the England average of 58.4%. Research suggests that bed occupancy rates of higher than
85% can increase the risk of harm and quality of care provided (Dr Foster, 2012).
The chart below shows the occupancy levels compared to the England average over the period.
(Source: NHS England)
20190416 900885 Post-inspection Evidence appendix template v4 Page 217
Meeting people’s individual needs
The service was inclusive and took account of women’s individual needs and preferences.
Staff made reasonable adjustments to help women access services. They coordinated care
with other services and providers.
Staff made sure women in vulnerable circumstances and those with mental health problems and
learning disabilities, received the necessary care to meet all their needs. Staff spoke sensitively
and confidently about the differing needs of women in vulnerable circumstances and described
arrangements to help them access services. Staff referred women to specialist midwives when
needed. The service had specialist midwives for safeguarding, perinatal mental health and
vulnerable women, such as teenagers and women for whom English was not their first language.
Staff could also refer to other health care professionals or agencies for additional support and
advice. These included the trust’s learning disability liaison nurse, local substance misuse teams,
the link outreach worker for Gypsy, Roma, Traveller (GRT) communities and independent
domestic violence advisors. The specialist perinatal mental health midwife worked in partnership
with the local perinatal mental health service. This service provided community-based treatment
and support to women who had a moderate to severe mental health issue or had in the past
experienced a serious mental health issue.
Staff made sure women, partners and families who experienced the death of their baby during
pregnancy, birth or soon after, received bereavement care and support to meet their needs. A
specialist bereavement midwife provided care and support to all bereaved parents, as well as
training and education for staff. Specialist equipment was available to enable bereaved parents
time with their baby, such as cold and cuddle cots. These slow down the natural deterioration
process and mean stillborn babies can stay longer with their parents. Baby and remembrance
items were provided to help parents create memories with their baby. These included story books,
a baby bath, pram, baby clothing and blankets. Parents could choose remembrance items, such
as ‘hand in heart’ keyrings and olive wood hearts. Comfort teddy bears had been gifted by other
bereaved parents. These helped signpost parents to support agencies, as well as being a physical
comforter and a means for staff to discuss the mental and emotional needs of parents following
their baby’s death. Each bear had been gifted by a bereaved family, to remind parents they were
not alone. A local professional photographer volunteered their photography services and created
personalised photo boxes of their baby for them. Memory boxes were also offered to all bereaved
families. Parents who had experienced a stillbirth or neonatal death were offered a post-mortem
examination to enhance future pregnancy counselling. Parents were supported with making
funeral arrangements. A chaplaincy service was available which provided spiritual care and
religious support for women, partners and families when needed. The chaplaincy team supported
all faiths and beliefs and could facilitate visits from local faith group leaders when asked. Staff
asked women who had experienced the loss of a baby if a sticker could be placed on their medical
records to alert health professionals to their loss. These are advocated by baby loss charities
because they help bereaved parents show rather than have to repeat their story to different health
professionals and signify to staff that the woman and her partner may need additional
understanding and support.
Staff understood and applied policy on meeting the information and communication needs of
women with a disability or sensory loss. The trust’s website had a ‘Browsealoud’ function. This
added speech and reading support tools to online content for people that required reading support,
such as those with dyslexia, learning disabilities, mild visual impairments and those with English
as a second language. Women could access information about maternity services through this
20190416 900885 Post-inspection Evidence appendix template v4 Page 218
function. Staff wore badges with their name clearly displayed in large font against a yellow
background. This made the name badges easier for visually impaired women and visitors to read
and promoted open communication across all levels of staff.
Managers made sure staff and women, relatives and carers could get help from interpreters or
signers when needed. Staff accessed interpreting services for women with English as a second
language. These were provided face to face or through a dedicated telephone translation service.
Sign language interpreters were available for women with hearing difficulties.
Information leaflets were available in languages spoken by women and the local community.
Leaflets could be provided in different languages and Braille, for blind or partially sighted women
through the patient advisory liaison service (PALS). The trust’s website had a translation function
which translated online content into any recognised world language.
Staff had access to communication aids to help women become partners in their care and
treatment. The trust worked with local providers to ensure communication guides were available
for people with sight and hearing difficulties, such as the Royal Association for Deaf people and
the Royal National Institute of Blind People. Information leaflets could be provided in easy read
formats. Pictorial aids were available to help women position and attach their baby correctly when
breastfeeding. Special dolls were offered to siblings of babies who had died to help them talk
about their lost brother or sister.
The service was accessible to women and visitors with mobility difficulties and wheelchair users.
Lifts were available to the fourth floor, where all maternity departments were located. Disabled
access bathroom and toilet facilities were available. Hearing loop was available for women and
visitors with hearing difficulties.
Women were given a choice of food and drink to meet their cultural and religious preferences.
Access and flow
Women could access the service when they needed it and received the right care promptly.
Managers made sure women could access services when needed and received care and
treatment within agreed timeframes and national targets. Women could access maternity services
through their GP, community midwife or by contacting the hospital directly. From January to
October 2019, 94.8% of women on average had accessed antenatal care by 12 weeks and six
days gestation. This was in line with the trust target of 95%. Routine antenatal care appointments
were scheduled in line with national guidance (NICE, Antenatal care for uncomplicated
pregnancies: CG62 (February 2019)). The maternity care records we reviewed confirmed this.
National guidance recommends that women should ideally be able to access antenatal care by 10
weeks so screening tests can be provided in a timely manner (NICE, Antenatal care: QS22,
Quality statement 1 (April 2016)). The service had an action plan to improve access to antenatal
care by 10 weeks. This included piloting a drop-in clinic for early screening bloods. The maternity
pages on the trust’s website had also been updated to make it easier for women to self-refer. An
audit of antenatal booking figures was being undertaken at the time of inspection. This was due to
be completed in January 2020. Data reported quarterly showed an upward trend (improvement) in
the percentage of women who had screening bloods taken by 10 weeks; from 42.8% in quarter 1
2018/19 to 51.6% in quarter 1 2019/20. The national acceptable threshold was 50% (Source:
Additional Evidence Request, DR100a and DR100b).
20190416 900885 Post-inspection Evidence appendix template v4 Page 219
The newborn and infant physical examination (NIPE) was performed on babies within 72 hours of
birth. In quarter 4 (January to March 2019), 99.5% of babies born at the trust had the NIPE within
72 hours. This was in line with the national achievable threshold of 99.5% and was better than the
England average of 96.7% (Public Health England, Screening KPI data summary factsheets
(August 2019)).
Women who were concerned or thought they were in labour could call the telephone triage service
24 hours a day, seven days a week for advice. This was staffed by midwives on the antenatal day
assessment unit (ADAU). Staff advised women to attend the unit when indicated by the symptoms
and/or concerns described. Staff told us they aimed to see all women within 30 minutes of arrival.
From July to October 2019 2,249 women attended triage. Of these, 91.5% were seen within 30
minutes of arrival, 5.5% within 60 minutes and 2.6% within 120 minutes. Staff took over 120
minutes to see the remaining 0.4%.
From November 2018 to October 2019 there was no suspension of the homebirth service or
maternity services at the hospital However, there were 23 occasions when one of the two stand-
alone midwifery led birthing units were suspended. Neither of the units were closed at the same
time (Source: Additional Evidence Request, DR64).
Managers worked to keep the number of delayed transfers and procedures to a minimum. When
women had their procedure cancelled at the last minute, managers made sure they were
rearranged as soon as possible. Planned caesarean section operating lists were scheduled daily,
Monday to Friday. They were staffed by a dedicated team to minimise cancellations or delays due
to staffing issues. Staff told us planned caesareans were rarely cancelled on the day. From August
2018 to July 2019 the average time (in hours) from admission to delivery for all planned
caesareans at term was 3.8 hours (Source: Routine Provider Information Request – Maternity
overview tab). From 20 November 2018 to 19 November 2019 one planned caesarean section
was cancelled and rescheduled. From August 2018 to August 2019, seven incidents regarding
delayed transfers from the ADAU to delivery suite were reported through the National Reporting
and Learning System (NRLS). All incidents resulted in no harm. Up to four inductions of labour
were commenced daily. These were mostly for women whose pregnancy had extended 10 days or
more past their expected due date. Staff told us low-risk women whose induction was commenced
on the antenatal day assessment unit were usually transferred to delivery suite two to four hours
after their waters were broken for ongoing treatment. From August 2018 to July 2019 the average
time (in hours) from admission to delivery for all inductions at term was 22.2 hours for women who
had their baby in the CLU and 18.1 hours for women in the MLU (Source: Routine Provider
Information Request – Maternity overview tab). Women were offered an induction of labour 24
hours after their waters had broken if they were not in labour and with consideration of risks.
Women rarely gave birth in areas not designated as labour ward. From August 2018 to August
2019 two incidents of this were reported through NRLS. Both incidents resulted in no harm. From
January to October 2019, 18 babies were born before arrival or in transit to the hospital. This
equated to 0.5% of total births.
Managers and staff worked to make sure women did not stay longer than they needed to and
started discharge planning as early as possible. Women were offered an early discharge where
appropriate. Staff told us women and babies suitable for early discharge were generally
discharged home within six hours after birth. Women who had a caesarean section were
discharged home one to two days after birth where appropriate. Eligible women were offered an
induction of labour as an outpatient. This meant they could return home to await labour for up to
23 hours after the induction was started if all observations were normal. Staff told us antenatal
20190416 900885 Post-inspection Evidence appendix template v4 Page 220
clinics generally ran on time, which we observed. Staff informed women if the clinic was running
late. Women could arrange an appointment on the ADAU on a day and time that suited them if
they needed regular monitoring during their pregnancy. We saw most women who attended were
seen promptly and did not stay longer than needed.
Staff planned women’s discharge carefully, particularly for those with complex mental health and
social care needs. Postnatal care was arranged with community midwives as part of the discharge
process. A discharge letter was also sent to each woman’s GP and health visitor to enable
continuity of care. Other professionals were informed when women with complex mental health
and social care needs were discharged, such as social workers and the perinatal mental health
team. Women were routinely seen by a midwife at home on day one, day five and day 10, when
they were discharged to the health visiting service if all observations were normal. Staff told us
they would continue to visit women up to 28 days after birth when needed, such as those in
vulnerable circumstances.
Staff supported women when they were referred or transferred between services. Women who
required transfer in labour to the hospital from the standalone birthing units or home were escorted
by the midwife caring for them.
Managers monitored and acted to minimise missed appointments. Women were offered future
appointments prior to leaving their consultation. This helped ensure appointments were not missed
because they were jointly agreed. Community midwives held clinics at the hospital at weekends
and Monday evenings for women who had difficulty attending their GP surgery during the week.
Staff ensured that women who did not attend appointments were contacted. Staff followed trust
policy if a woman did not attend their appointment. Women were offered a further appointment,
and/or their community midwife was informed who contacted or visited the woman at home. Staff
told us they would escalate to the safeguarding team if two or more appointments were missed.
Learning from complaints and concerns
It was easy for women to give feedback and raise concerns about care received. The
service treated concerns and complaints seriously, investigated them and shared lessons
learned with all staff.
Staff understood the policy on complaints and knew how to handle them. They told us that where
possible complaints were resolved when raised. If concerns could not be resolved informally,
women and/or those close to them were supported to make a formal complaint. The service had
processes to ensure complaints were dealt with effectively. This included prompt acknowledgment
of the complaint, written response to the complaint and whether changes had been made because
of the complaint.
Women, relatives and carers knew how to complain or raise concerns. Women we spoke with
confirmed this.
The service clearly displayed information about how to raise a concern in all maternity wards and
departments. Leaflets regarding the complaints process were available for women and details of
how to raise a complaint was published on the trust’s website. Women were also signposted to the
trust’s patient advice and liaison service (PALS). PALS provided advice and support to women
(and those close to them) who wished to raise a concern or complaint.
20190416 900885 Post-inspection Evidence appendix template v4 Page 221
Summary of complaints
Broomfield Hospital
Managers investigated complaints and identified themes. Managers told us most complaints were
managed promptly and in line with trust policy.
From August 2018 to July 2019 the trust received 26 complaints in relation to maternity at
Broomfield Hospital. The trust took an average of 32.8 working days to investigate and close
complaints. This was not in line with their complaints policy, which states complaints should be
closed within 25 working days. However, complex complaints could take up to 60 working days to
close.
Managers routinely monitored performance for complaints response times. In October 2019, 100%
of complaints received for maternity were responded to in line with trust policy. This exceeded
(was better than) the trust target of 85%.
A breakdown of complaints by type is shown below:
Type of complaint Number of complaints Percentage of total
Clinical treatment - Obstetrics and gynaecology
23 88.5%
Values and behaviours (staff) 2 7.7% Clinical treatment - paediatric group 1 3.8% Total 26 100.0%
(Source: Routine Provider Information Request (RPIR) – Complaints tab)
Staff knew how to acknowledge complaints and women received feedback from managers after
the investigation into their complaint. We reviewed three complaint responses and saw thorough
investigations of the concerns raised had been conducted. The response letters were sensitively
written and included an apology. A detailed response was provided to each concern raised. Any
learning or action taken in response to the complaint was included. Women and those close to
them were also offered a debriefing session known as a birth reflection. This enabled them to
review their maternity notes and gave them the opportunity to discuss their birth experience with
an experienced midwife. Women and/or those close to them who were dissatisfied with the
response to their complaint were signposted to the Parliamentary and Health Service Ombudsman
(PHSO). From August 2018 to July 2019 no complaints received by the service were referred to
the PHSO (Source: Routine Provider Information Request (RPIR) - Complaints overview tab).
Managers shared feedback from complaints with staff and learning was used to improve the
service. Learning from complaints and feedback was shared with staff through a variety of means
such as newsletters, team meetings and noticeboards. Staff confirmed they received feedback on
complaints. Action was taken in response to complaints received to improve patient experience
and care provision. Where individual members of staff were the cause of the complaint, managers
discussed the concerns raised with them, so they could reflect and make changes to their practice
accordingly.
Number of compliments made to the trust
Broomfield Hospital
20190416 900885 Post-inspection Evidence appendix template v4 Page 222
From August 2018 to July 2019 there were 11 compliments received for maternity at Broomfield
Hospital (1.0% of all received trust wide).
A breakdown of compliments by ward/team is shown below:
Ward/team Number of compliments Percentage of total Maternity 9 81.8% Postnatal ward 1 9.1% Antenatal clinic 1 9.1% Total 11 100.0%
The trust stated that most of the compliments received related to overall care along the whole
pathway and women and relatives thanking staff for their kindness and compassion during difficult
and stressful times. These related to all staff from housekeepers, porters and midwives to
consultants.
Compliments and the associated learning and sharing of good practice was discussed at the
patient and carer experience group and with individuals and their managers during appraisal. The
trust used its electronic incident reporting and risk management system to analyse themes from
compliments.
(Source: Routine Provider Information Request (RPIR) – Compliments tab)
Managers shared compliments received with staff. The divisional quarterly newsletter included
examples of positive comments and thank you letters received.
Is the service well-led?
Leadership
Leaders had the skills and abilities to run the service and deliver high-quality, woman-
centred care. They understood and managed the priorities and issues the service faced.
They were visible and approachable in the service for women and staff.
There was a clear management structure with defining lines of responsibility and accountability.
The maternity service formed part of the women’s and children’s division, which was led by the
divisional clinical director, associate director of operations, head of midwifery (HOM) and head of
children. They were supported by a clinical director for obstetrics, service manager, lead midwife
for clinical governance, consultant lead for labour ward, matrons, ward managers and specialist
midwives. We met with the senior leadership team who demonstrated knowledge of the service’s
performance, challenges they faced and priorities for their service. They had the right skills,
knowledge and experience required to deliver high-quality, woman-centred sustainable care.
The senior leadership team had direct access to the trust board when maternity was under
consideration. Minutes of board meetings we reviewed for June and September 2019 showed the
trust board had oversight of the service. The executive lead for maternity services at board level
was the chief nursing officer. The trust’s maternity safety champions were the head of midwifery
and clinical director for obstetrics. They met regularly with the chief nursing officer to monitor
information about quality, including safety and to escalate any concerns to the board which
required necessary action. There was also a non-executive director (NED) with responsibility for
maternity services. This was in line with national recommendations (National Maternity Review,
Better Births: Improving outcomes of maternity services in England (2016)). The senior leadership

20190416 900885 Post-inspection Evidence appendix template v4 Page 223
team told us the chief nursing officer and NED were actively engaged with the service and they felt
maternity services were a priority for the trust and were well represented at board level. For
example, in September 2019 a report was presented to the board to provide assurance that the 10
maternity safety actions required by the Clinical Negligence Scheme for Trusts (CNST) had been
evidenced by the service and through review by the Quality Committee and the maternity safety
champions. Staff we spoke with confirmed the chief nursing officer was visible and were aware of
visits to the unit by the NED.
At the time of our inspection, the HOM had been in post approximately two months. All staff we
talked to spoke very highly of the HOM and described them as being “dynamic”, “very supportive”
and “really open”. Staff told us leaders were very visible, approachable and they felt well
supported. We observed the HOM frequently visited the wards to check-in with staff during our
inspection.
The service’s maternity safety strategy included a focus on leadership and creating strong
leadership at every level. This was in response to concerns raised by band 7 midwives who felt
disempowered to challenge some staffing issues. Actions to address this had been taken. For
example, two band 7 leadership workshops were held, as well as bi-monthly manager’s meetings
to support staff with management duties. A designated daily ‘bleep holder’ was also introduced.
They were responsible for monitoring and managing any staffing issues.
The delivery suite was coordinated by an experienced senior midwife who, wherever possible, was
supernumerary. This meant they could maintain oversight of activity and risks and could support
staff as needed.
The service had processes to ensure midwives were adequately supervised and received clinical
supervision. The service had nine professional midwifery advocates (PMAs) who provided
restorative clinical supervision and support to staff. Restorative clinical supervision has been found
to reduce stress and has had a positive impact on physical and emotional well-being, job
satisfaction and relationships with colleagues (NHS England, A-EQUIP: a model of clinical
midwifery supervision (2017)).
The trust provided development programmes for staff that supported them to develop leadership
and management skills, which staff we spoke with confirmed. Leadership and development
programmes were available for first line managers, middle managers and senior managers.
Vision and strategy
The service had a vision for what it wanted to achieve and a strategy to turn it into action
developed with all relevant stakeholders. The vision and strategy were focused on
sustainability of services and aligned to local plans within the wider health economy.
Leaders and staff understood and knew how to apply them and monitor progress.
The service had a clear vision and strategy, central to which was the ‘provision of the safest and
highest quality care’. The vision for the maternity service was:
• Drive forward the choice and safety agenda, ensure women were central to the service,
work collaboratively with local, regional and national systems, and listen to staff and
women;
• Work in partnership with the multidisciplinary team;
• Foster a culture of learning for improvements in outcomes, using evidence-based practice;
20190416 900885 Post-inspection Evidence appendix template v4 Page 224
• Increase the use of midwifery-led units and breastfeeding rates and implement continuity of
care;
• Promote health and normality at every opportunity and embrace women to achieve a
positive experience;
• A cohesive and supportive team, a culture of support and respect and visible clinical
leadership (Source: Additional Evidence Request, DR245).
In addition to the local vision, the senior leadership team and managers were working
collaboratively with senior staff from the other hospitals within the trust to establish a local
maternity system (LMS). The LMS strategy detailed 12 national planning deliverables which were
aligned with national recommendations and ambitions for maternity care services. These included
full implementation of the Saving Babies’ Lives care bundle (version two) and increasing the
number of women on continuity of care pathways by March 2020 (National Maternity Review,
Better Births: Improving outcomes of maternity services in England (2016)). Progress against
achieving the national planning deliverables was regularly monitored and reported. The
September 2019 LMS highlight report showed one of the 12 national planning deliverables had
been completed within the specified timeframe. This was achievement of the Clinical Negligence
Scheme for Trusts (CNST) maternity incentive scheme. Of the 11 remaining deliverables, eight
were ‘on track’ and three were ‘at risk’ of not being completed within the specified timeframe.
These were mostly in relation to providing continuity of care pathways and an inability to deliver all
five aspects of the Saving Babies’ Lives care bundle because of gaps in the sonography workforce
(Source: Additional Evidence Request, DR66). We saw these risks were detailed on the service’s
risk register.
The trust had an established values statement which was, “We are a kind, professional, positive
team”.
Staff we spoke with knew and understood what the vision, strategy and values were and their role
in achieving them.
Culture
Staff felt respected, supported and valued. They were focused on the needs of women
receiving care. The service had an open culture where women, their families and staff could
raise concerns without fear.
All staff we met were welcoming, friendly and helpful. It was evident that staff were passionate
about the care they provided to women and babies and were proud to work at the trust. Staff told
us they loved their job and loved working at the trust.
Multidisciplinary teams worked collaboratively and were focused on improving women’s care and
service provision. During our inspection, we observed positive and respectful interactions which
were focused on meeting women’s needs and providing safe care and treatment.
Staff told us they felt well supported, valued and respected. All staff we spoke with felt the culture
of the service had improved since the new head of midwifery had started. One staff member felt
there was, “a real buzz about the place”. None of the staff we spoke with raised any concerns
about bullying or other inappropriate behaviours from colleagues. Leaders promoted an ‘open
door’ culture and staff were encouraged to speak up and raise concerns. Trust policies and
procedures positively supported this process. We saw information on how staff could raise
20190416 900885 Post-inspection Evidence appendix template v4 Page 225
concerns and who the trust freedom to speak up guardians were detailed in multiple editions of the
women’s and children’s newsletter. An independent guardian service was also available to staff 24
hours a day, seven days a week. This was a confidential service for staff to discuss matters
relating to patient care and safety, whistle-blowing, bullying and harassment and work grievances.
The culture encouraged openness and honesty. The trust had processes to ensure the duty of
candour was met. Where incidents had caused harm or could have significant caused harm, we
saw the duty of candour was complied with.
The senior leadership team and managers spoke with pride about the work and care their staff
delivered daily. They celebrated staff success by sharing positive feedback received and positive
contributions made by staff. We saw many examples of these in the newsletters we read. Staff
were invited to nominate colleagues for ‘Star of the Month’. This was awarded to staff who had
gone the extra mile. In August 2019, the lead midwife for governance won the award for working
tirelessly and selflessly to keep women safe and free from harm. In September 2019, the
bereavement lead midwife won the ‘improving patient experience’ award at the trust’s annual
Outstanding Care and Service Awards (OSCAs).
There were arrangements in place to promote the safety and wellbeing of staff. Staff could contact
the trust’s security team for support and assistance if women or visitors became verbally and/or
physically abusive. Staff who worked alone and within teams spread across the community had
mobile phones and some community midwives had personal safety devices, but not all. Managers
told us they planned to replace all mobile phones with smart phones, which would enable them to
track staff when needed. Professional midwifery advocates provided a formal mechanism for
debriefing and supporting staff when needed, such as if they were involved in an incident. Staff
could also access the trust’s occupational health, physiotherapy and counselling services if they
needed additional support at any time.
There were mechanisms for providing staff with the development they needed. These included
personal development reviews and appraisals. Staff spoke positively about the training and
development opportunities available. However, some staff told us they felt the appraisal process
was not constructive and described it as a ‘tick box exercise’. Action was taken to address
behaviour and performance that was inconsistent with the vision and values, regardless of
seniority. Managers gave examples of when this had occurred.
Governance
Leaders operated effective governance processes, throughout the service. Staff at all levels
were clear about their roles and accountabilities and had regular opportunities to meet,
discuss and learn from the performance of the service.
The service had a clear governance structure and processes to support the delivery of quality
services and safeguard high standards of care. There was an up to date policy which detailed the
clinical governance structure for the women’s and children’s division. All staff could access this
through the trust’s intranet. The policy included the governance strategy and objectives, the
meetings, forums and groups with responsibility for governance and risk management, and staff
roles and responsibilities.
The service had a lead midwife for clinical governance. They were responsible for coordinating
and implementing clinical risk management, audit, clinical effectiveness and midwifery practice
developmental processes within the maternity service. They reported to the head of midwifery.

20190416 900885 Post-inspection Evidence appendix template v4 Page 226
Monthly governance meetings were held at service and divisional level. These included the
maternity multidisciplinary risk management group meeting and the women’s and children’s
divisional governance and board meeting. Matters which required escalation to the board were
done so through direct reporting to the executive lead for maternity, trust mortality meetings and/or
the trust’s risk and compliance group meetings. This meant there was oversight of the service at
ward to board level.
Monthly and divisional governance meetings followed standing agendas. We reviewed six sets of
meeting minutes which confirmed governance matters such as incidents, risks, performance,
guidance, audits and complaints were discussed. Minutes were sufficiently detailed however, the
lead person responsible for ensuring any required actions were followed up was not always
documented. The more recent copies of minutes we were sent did include this detail (Source:
Additional Evidence Request, DR80 and DR81).
Managers reviewed all incidents reported daily at the safety huddle, Monday to Friday. This
ensured any immediate action required to address safety concerns was identified and promptly
shared with staff through handovers and ‘hot topics’. Where necessary, investigations were
undertaken to identify learning and actions needed to address incidents and minimise recurrence.
Incidents were also reviewed to ensure they had been graded in terms of harm appropriately. Any
potential serious incidents were brought to the trust’s serious incident for review which met three
times a week.
The clinical governance facilitator prepared an incidents and clinical effectiveness report monthly.
The purpose of the report was to update the women’s and children’s governance group on matters
which required note or response with actions to facilitate service improvement and/or compliance
with legislative and regulatory requirements. We reviewed the October 2019 report which included
details of incidents, risks, audits and guidelines, including those which were overdue and required
action. The report also included a list of all National Institute for Health and Care Excellence
(NICE) advice and guidance published in the previous month and all active national and trust
patient safety alerts (Source: Additional Evidence Request, DR89), with identified actions where
needed.
Staff at all levels were clear about their roles and understood their accountabilities and who they
reported to. They confirmed they were kept informed about governance matters and performance
of the service.
Management of risk, issues and performance
Leaders and teams identified and escalated risks and issues. They identified actions to
reduce their impact. They had plans to cope with unexpected events.
There were clear and effective processes for identifying, recording, managing and mitigating risks.
The trust had an up to date risk management policy and related policies, such as the business
continuity policy and plan. Staff used an electronic incident reporting and risk management system
to record and manage risks. A clinical governance facilitator supported managers to ensure risks
were appropriately described, assessed and recorded. Risk registers were managed at
department, division, divisional and/or trust level, depending on the level of risk identified. We
reviewed the maternity risk register. It included a description of each risk, the named risk owner
and review date, alongside mitigating actions and controls in place to minimise the risk. Each risk
was scored according to the likelihood of the risk occurring and its potential impact.
20190416 900885 Post-inspection Evidence appendix template v4 Page 227
The risk register was reviewed at governance meetings. Managers told us they had also
introduced a divisional risk register meeting. We reviewed the minutes of the women’s and
children’s risk register review meeting held in October 2019. Each risk was updated, and actions
identified had a named person responsible for ensuring they were completed. Risks were
regraded when indicated and closed when they had been addressed.
There was alignment between the recorded risks and what staff identified as risks within the
service. Staff told us they were kept informed about risks in a variety of ways, including team
meetings, staff noticeboards and emails. We saw posters displayed which detailed the top three
risks for the trust and the women’s and children’s division. The top three risks for the maternity
service concerned:
• The service’s inability to archive cardiotocography traces electronically;
• The lack of scanning availability which meant the service was unable to meet national
recommendations;
• The service’s inability to provide continuity of care in line with national recommendations.
(Source: RPIR and SHIPP Landing Pad, RQ8 documents – P106; Additional Evidence Request,
DR63a)
The trust had an up to date business continuity and emergency planning policy which was
accessible to staff and detailed what action should be taken and by who in the event of a critical
incident, such as fire or loss of utilities.
Information management
The service collected reliable data and analysed it. Staff could find the data they needed, in
easily accessible formats, to understand performance, make decisions and improvements.
The information systems were integrated and secure. Data or notifications were
consistently submitted to external organisations as required.
There was a holistic understanding of performance which sufficiently covered and integrated
people’s views with information on quality, operations and finances. Clear service performance
measures were reported and monitored. For example, staff had access to quality and performance
data through the maternity dashboard which was used to monitor activity, workforce, outcomes
and performance. Areas of good and poor performance were highlighted and used to challenge
and drive forward improvements, where indicated. Performance thresholds and targets had been
set in agreement with clinical commissioning groups and were in line with national targets where
available. A traffic light Red, Amber, Green (RAG) rating was used to flag performance against
agreed thresholds. This meant staff could identify at a glance, areas that required investigation
and improvement. Managers regularly discussed performance at governance meetings and
actions were taken to investigate and address areas of concern where indicated. For example, in
response to the ‘red rated’ caesarean section rate, managers were auditing all caesarean sections
that occurred in November 2019 to identify if all sections were indicated and whether
improvements could be made to reduce the section rate.
Staff mostly had access to up to date and comprehensive information regarding women’s care and
treatment. However, the service was unable to archive cardiotocographs (CTGs) electronically.
This meant there was a risk CTGs would fade and could not be used in the event of a medico-
legal case. This risk was listed on the service’s risk register and an electronic solution had been
20190416 900885 Post-inspection Evidence appendix template v4 Page 228
requested. All CTGs related to a serious incident were photocopied to reduce this risk. There were
arrangements to ensure the confidentiality of patient information held electronically and staff were
aware of how to use and store confidential information. The electronic patient record system was
password protected. We observed computer terminals were locked when not in use to prevent
unauthorised persons for accessing confidential patient information.
There were effective arrangements to ensure data was submitted to external bodies as required,
such as local commissioners, Public Health England and M-BRRACE-UK. This enabled the
service to benchmark performance against other maternity providers and national outcomes.
Engagement
Leaders and staff actively and openly engaged with women, staff, the public and local
organisations to plan and manage services. They collaborated with partner organisations
to help improve services for women.
Women’s views and experiences were gathered and acted on to shape and improve the service
and culture. Women and partners were encouraged to share their views to help improve services.
For example, women who used maternity services were encouraged to give feedback on the
quality of service they received through the Friends and Family Test (FFT). Feedback was
reviewed by staff and used to inform improvements and learning, where possible. Information
about making a complaint and the patient advisory liaison service (PALS) was available in all
areas of the service. Feedback was also gathered through social media forums.
Parents whose baby had died during pregnancy, birth, or soon after were sent a questionnaire to
help identify any areas where bereavement care and support could be improved. The
questionnaire had been designed collaboratively with members of the Sands charity and bereaved
families. The questionnaire was posted to parents with a blossom sticker on the envelope, so they
knew what it was and could open it if and/or when they wanted. We reviewed 20 feedback forms
which showed most parents rated their care and the service very highly. Any areas of care that did
not meet family’s needs were acted on by the bereavement lead midwife. For example, feedback
from bereaved parents showed they were able to access counselling services when they needed
it. In response, the service had secured funding to pilot a counselling service at the hospital.
Women were involved in decision-making and activities to help shape services and the culture.
For example, the service worked collaboratively with the local Maternity Voices Partnership (MVP).
This user group was made up people involved in planning, providing and receiving maternity care,
such as midwives, health visitors, GPs, parents, parents-to-be and maternity service stakeholders.
An ‘in your shoes’ event was held to understand women’s, partner’s and staff views and feedback
from this event was used to develop action plans to improve the service.
The service participated in events to engage women, families, the public and staff. For example, in
September 2019 the service participated in the World Health Organisation’s annual world patient
safety day. The aim was to raise public awareness about patient safety and improve the quality of
healthcare. Staff had a stand in the hospital’s main foyer to share work that had been done to
improve services. The trust promoted baby loss awareness week. The external lights of the
hospital were changed to blue and pink, memory trees were placed in the foyer along with
information stands and singers were invited in to perform. The bereavement lead midwife ran a
social media group for bereaved parents. This acted as a means of support and helped parents
form social support connections with others who understood what they were going through.
Feedback from the service’s community of bereaved families was, “one you’d never choose to join
20190416 900885 Post-inspection Evidence appendix template v4 Page 229
but it’s the best and most supportive group you could be part of”. In the Summer, staff held their
first maternity festival (“MatFest”) at a staff member’s farm. Everyone in the unit was invited for an
evening of food and music under the stars. Staff told us the event had been great for staff morale
and they hoped to make it an annual event.
Staff’s views and experiences were gathered and acted on to shape and improve the service and
culture. Staff were encouraged to share their views to help improve services. For example, the
service had introduced breakfast meetings where the leads for the service provided breakfast to
staff on duty and gave them an open forum to discuss any issues they wished to raise. The
meetings were colleague-led with no fixed agenda to ensure conversations flowed. Managers
reported the breakfast meeting had already proven to mitigate grievances and work-related stress,
as well as providing key target areas for increased training (Source: Routine Provider Information
Request, Innovation tab – P65). Feedback from restorative clinical supervision and staff feedback
sessions was used to develop an action plan for maternity and neonatal safety. Safety concerns
identified by staff were aligned to five key drivers; leadership, learning and best practice, teams,
data and innovation. We saw actions to address each concern were identified. For example,
managers ensured staff had support from their line manager, psychotherapy and/or restorative
clinical supervision in response raised to concerns about psychological trauma experienced by
staff following an incident or stressful situation (Source: Additional Evidence Request, DR69).
More flexible working and core staff had also been introduced in response to staff feedback, which
all staff spoke very positively about.
From the conversations we had with staff and observations were made during our inspection, it
was evident staff were engaged in the service and felt empowered to help improve services.
Information was shared with staff in a variety of ways, such as daily handovers, email,
noticeboards and staff events. The service also used social media forums to engage with staff.
The service engaged with external partners to build a shared understanding of challengers within
maternity, the needs of the local community and to deliver services to meet those needs. The
service was working collaboratively with service users, neighbouring hospitals and commissioners
by means of the local maternity system to ensure national recommendations for maternity services
were implemented across the region.
Learning, continuous improvement and innovation
Staff were committed to continually learning and improving services. They had a good
understanding of quality improvement methods and the skills to use them. Leaders
encouraged innovation and participation in research.
Staff of all grades were committed to continually learning and improving services. Staff we spoke
with told us they were encouraged to share any ideas or suggestions they had for service
improvement. Staff gave examples of new initiatives within the service. For example, all
preceptee’s were given a blue flower badge to wear to discretely signify to other staff they were
newly qualified and may need additional support and help. This innovation was developed by
preceptee’s. The service was participating in the Maternity and Neonatal Safety Improvement
Programme to reduce the postpartum haemorrhage rate of births of 1,500mls or more by 50% by
May 2020. A recognised quality improvement tool known as Plan, Do, Study, Act (PDSA) cycles
was being used to trial the model for improvement (Source: Additional Evidence Request, DR98).
The service had employed a lead midwife for quality improvement.

20190416 900885 Post-inspection Evidence appendix template v4 Page 230
The service participated in research projects which contributed to learning, continuous
improvement and innovation. For example, the service was trialling a non-medicinal method of
labour induction. The benefits of which included a very low risk of uterine hyperstimulation, which
is a serious complication of induction where the uterus contracts for longer or more frequently than
normal and can lead to uterine rupture or fetal distress.
Staff were committed to giving high quality care to women and their families and had improved
services to meet their needs. For example, we heard many examples of improvements made to
bereavement care. The service was actively recruiting for an additional midwife to support the
bereavement team. Once recruited, their focus would be rainbow pregnancies (pregnancies that
follow the loss of a baby).
In December 2019, the maternity bereavement team were awarded a Judge’s Award at the NHS
Elect Patient Experience and Quality Improvement Awards. The team were praised for
demonstrating leadership and compassion for women, partners and families and inspiring their
colleagues. Their nomination was described as “moving” and “made unforgettable reading”.
The service was committed to training and staff development. Staff told us they were encouraged
and supported to complete additional training.
20190416 900885 Post-inspection Evidence appendix template v4 Page 231
Gynaecology
Facts and data about this service
The trust provides a range of gynaecology services including the early pregnancy unit, acute
gynaecology, outpatient services including colposcopy, fertility, hysterosalpingo contrast
sonography (HyCoSy), urodynamics and hysteroscopy clinics as well as a specialist oncology
service.
The service has eight obstetrics and gynaecology consultants who covered both specialties. Each
consultant has area of expertise in women’s health to provide a range of specialist clinic services.
The gynaecology service offered the following specialist clinics:
• Colposcopy Clinic
• Early Pregnancy Assessment Unit
• Fast Track Clinic
• Fertility Clinic
• Gynaecology Outpatient’s
• Gynae-oncology
• Hysteroscopy Clinic
• Menstrual Disorder Clinic
• Outreach Clinics
• Pre-assessment Clinic
• Termination of Pregnancy Clinic
• Uro-gynaecology Clinic
• Urodynamics Clinic
Gynaecology services has one inpatient ward, Gosfield Ward is a 10-bedded inpatient ward for
gynaecological services at Broomfield Hospital. There is 24-hour consultant coverage for the
service with close working with two other hospitals in relation to the oncology patient care
pathways.
The gynaecology ambulatory care unit has four trolleys for patient assessments and accepts direct
referrals from the emergency department and GP’s. The gynaecology ambulatory care unit and
the early pregnancy unit were located on Gosfield ward.
The trust has undertaken a number of service developments, including specialist nurse training
courses to allow the introduction of nurse-led ultrasound scanning in the early pregnancy unit on
completion of the training. The training has been completed by an advanced nurse colposcopist
and is being rolled out to other nurses.
The trust is developing an outpatient endometrial ablation clinic to reduce the pressure on
inpatient services. The trust is also in the final phase of implementing manual vacuum aspiration
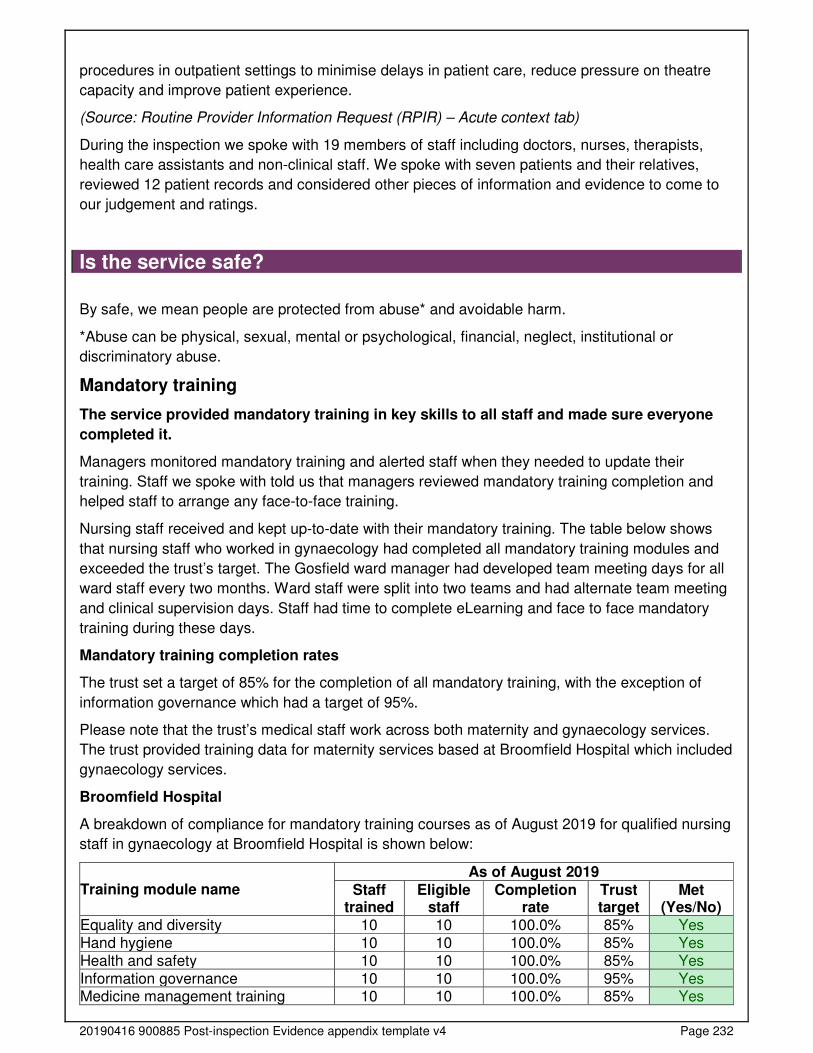
20190416 900885 Post-inspection Evidence appendix template v4 Page 232
procedures in outpatient settings to minimise delays in patient care, reduce pressure on theatre
capacity and improve patient experience.
(Source: Routine Provider Information Request (RPIR) – Acute context tab)
During the inspection we spoke with 19 members of staff including doctors, nurses, therapists,
health care assistants and non-clinical staff. We spoke with seven patients and their relatives,
reviewed 12 patient records and considered other pieces of information and evidence to come to
our judgement and ratings.
Is the service safe?
By safe, we mean people are protected from abuse* and avoidable harm.
*Abuse can be physical, sexual, mental or psychological, financial, neglect, institutional or
discriminatory abuse.
Mandatory training
The service provided mandatory training in key skills to all staff and made sure everyone
completed it.
Managers monitored mandatory training and alerted staff when they needed to update their
training. Staff we spoke with told us that managers reviewed mandatory training completion and
helped staff to arrange any face-to-face training.
Nursing staff received and kept up-to-date with their mandatory training. The table below shows
that nursing staff who worked in gynaecology had completed all mandatory training modules and
exceeded the trust’s target. The Gosfield ward manager had developed team meeting days for all
ward staff every two months. Ward staff were split into two teams and had alternate team meeting
and clinical supervision days. Staff had time to complete eLearning and face to face mandatory
training during these days.
Mandatory training completion rates
The trust set a target of 85% for the completion of all mandatory training, with the exception of
information governance which had a target of 95%.
Please note that the trust’s medical staff work across both maternity and gynaecology services.
The trust provided training data for maternity services based at Broomfield Hospital which included
gynaecology services.
Broomfield Hospital
A breakdown of compliance for mandatory training courses as of August 2019 for qualified nursing
staff in gynaecology at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Equality and diversity 10 10 100.0% 85% Yes Hand hygiene 10 10 100.0% 85% Yes Health and safety 10 10 100.0% 85% Yes Information governance 10 10 100.0% 95% Yes Medicine management training 10 10 100.0% 85% Yes

20190416 900885 Post-inspection Evidence appendix template v4 Page 233
Moving and handling 10 10 100.0% 85% Yes Moving and handling for people handlers
10 10 100.0% 85% Yes
Waste management 10 10 100.0% 85% Yes
Adult immediate life support 9 10 90.0% 85% Yes Fire safety 9 10 90.0% 85% Yes
In gynaecology, the trust target was met for all 10 of the mandatory training modules for which
qualified nursing staff were eligible.
Medical staff received and kept up-to-date with their mandatory training. The average completion
rate for mandatory training was 89.5% which was above the trust completion target. Although
medical staff had not completed two modules to the trust’s target of 85%.
A breakdown of compliance for mandatory training courses as of August 2019 for medical staff in
gynaecology at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Health and safety 21 21 100.0% 85% Yes Information governance 21 21 100.0% 95% Yes
Medicine management training 2 2 100.0% 85% Yes Waste management 21 21 100.0% 85% Yes Moving and handling 20 21 95.2% 85% Yes Adult basic life support 6 7 85.7% 85% Yes Fire safety 18 21 85.7% 85% Yes Hand hygiene 18 21 85.7% 85% Yes
Equality and diversity 16 21 76.2% 85% No Adult immediate life support 14 21 66.7% 85% No
In gynaecology, the target was met for eight of the 10 mandatory training modules for which
medical staff were eligible.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Clinical staff completed training on recognising and responding to patients with mental health
needs, learning disabilities, autism and dementia. The completion rate for Mental Capacity Act and
Deprivation of Liberty Safeguards training was 100% for nursing staff which was above the trust’s
target of 95%. The completion rate for medical staff was 85.7% which was below the trust’s target.
Safeguarding
Staff understood how to protect patients from abuse and the service worked well with other
agencies to do so. Nursing staff had training on how to recognise and report abuse and
they knew how to apply it. Although not all medical staff had completed all elements of
safeguarding training.
Staff knew how to identify adults and children at risk of, or suffering, significant harm and worked
with other agencies to protect them. The trust had a safeguarding adults policy and safeguarding
children policy in place which were within the review date. The policies set out staff responsibilities
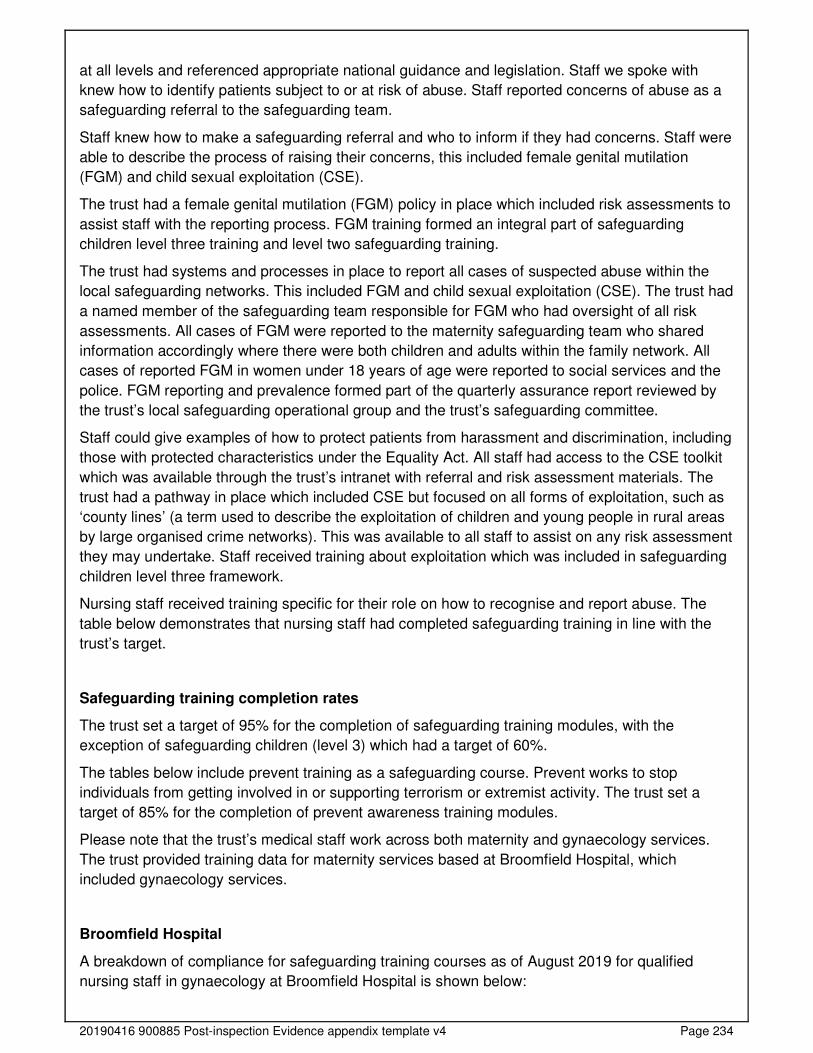
20190416 900885 Post-inspection Evidence appendix template v4 Page 234
at all levels and referenced appropriate national guidance and legislation. Staff we spoke with
knew how to identify patients subject to or at risk of abuse. Staff reported concerns of abuse as a
safeguarding referral to the safeguarding team.
Staff knew how to make a safeguarding referral and who to inform if they had concerns. Staff were
able to describe the process of raising their concerns, this included female genital mutilation
(FGM) and child sexual exploitation (CSE).
The trust had a female genital mutilation (FGM) policy in place which included risk assessments to
assist staff with the reporting process. FGM training formed an integral part of safeguarding
children level three training and level two safeguarding training.
The trust had systems and processes in place to report all cases of suspected abuse within the
local safeguarding networks. This included FGM and child sexual exploitation (CSE). The trust had
a named member of the safeguarding team responsible for FGM who had oversight of all risk
assessments. All cases of FGM were reported to the maternity safeguarding team who shared
information accordingly where there were both children and adults within the family network. All
cases of reported FGM in women under 18 years of age were reported to social services and the
police. FGM reporting and prevalence formed part of the quarterly assurance report reviewed by
the trust’s local safeguarding operational group and the trust’s safeguarding committee.
Staff could give examples of how to protect patients from harassment and discrimination, including
those with protected characteristics under the Equality Act. All staff had access to the CSE toolkit
which was available through the trust’s intranet with referral and risk assessment materials. The
trust had a pathway in place which included CSE but focused on all forms of exploitation, such as
‘county lines’ (a term used to describe the exploitation of children and young people in rural areas
by large organised crime networks). This was available to all staff to assist on any risk assessment
they may undertake. Staff received training about exploitation which was included in safeguarding
children level three framework.
Nursing staff received training specific for their role on how to recognise and report abuse. The
table below demonstrates that nursing staff had completed safeguarding training in line with the
trust’s target.
Safeguarding training completion rates
The trust set a target of 95% for the completion of safeguarding training modules, with the
exception of safeguarding children (level 3) which had a target of 60%.
The tables below include prevent training as a safeguarding course. Prevent works to stop
individuals from getting involved in or supporting terrorism or extremist activity. The trust set a
target of 85% for the completion of prevent awareness training modules.
Please note that the trust’s medical staff work across both maternity and gynaecology services.
The trust provided training data for maternity services based at Broomfield Hospital, which
included gynaecology services.
Broomfield Hospital
A breakdown of compliance for safeguarding training courses as of August 2019 for qualified
nursing staff in gynaecology at Broomfield Hospital is shown below:
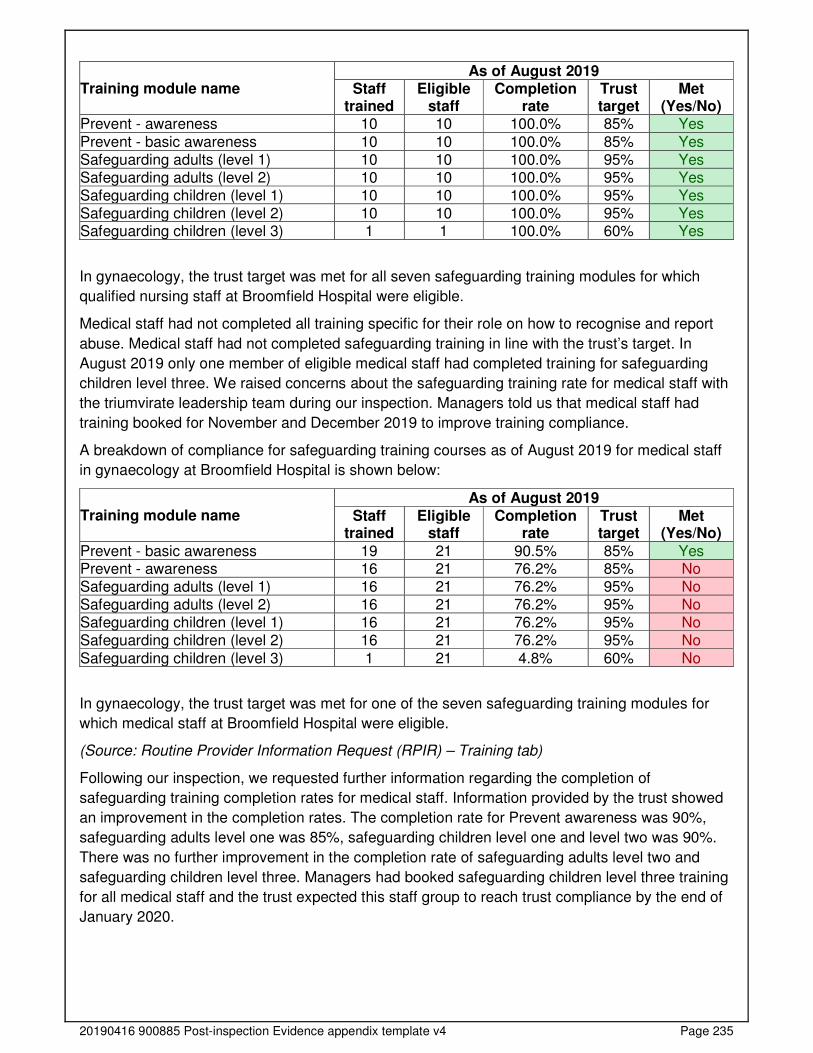
20190416 900885 Post-inspection Evidence appendix template v4 Page 235
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Prevent - awareness 10 10 100.0% 85% Yes
Prevent - basic awareness 10 10 100.0% 85% Yes Safeguarding adults (level 1) 10 10 100.0% 95% Yes Safeguarding adults (level 2) 10 10 100.0% 95% Yes Safeguarding children (level 1) 10 10 100.0% 95% Yes Safeguarding children (level 2) 10 10 100.0% 95% Yes Safeguarding children (level 3) 1 1 100.0% 60% Yes
In gynaecology, the trust target was met for all seven safeguarding training modules for which
qualified nursing staff at Broomfield Hospital were eligible.
Medical staff had not completed all training specific for their role on how to recognise and report
abuse. Medical staff had not completed safeguarding training in line with the trust’s target. In
August 2019 only one member of eligible medical staff had completed training for safeguarding
children level three. We raised concerns about the safeguarding training rate for medical staff with
the triumvirate leadership team during our inspection. Managers told us that medical staff had
training booked for November and December 2019 to improve training compliance.
A breakdown of compliance for safeguarding training courses as of August 2019 for medical staff
in gynaecology at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Prevent - basic awareness 19 21 90.5% 85% Yes Prevent - awareness 16 21 76.2% 85% No Safeguarding adults (level 1) 16 21 76.2% 95% No Safeguarding adults (level 2) 16 21 76.2% 95% No Safeguarding children (level 1) 16 21 76.2% 95% No Safeguarding children (level 2) 16 21 76.2% 95% No
Safeguarding children (level 3) 1 21 4.8% 60% No
In gynaecology, the trust target was met for one of the seven safeguarding training modules for
which medical staff at Broomfield Hospital were eligible.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Following our inspection, we requested further information regarding the completion of
safeguarding training completion rates for medical staff. Information provided by the trust showed
an improvement in the completion rates. The completion rate for Prevent awareness was 90%,
safeguarding adults level one was 85%, safeguarding children level one and level two was 90%.
There was no further improvement in the completion rate of safeguarding adults level two and
safeguarding children level three. Managers had booked safeguarding children level three training
for all medical staff and the trust expected this staff group to reach trust compliance by the end of
January 2020.
20190416 900885 Post-inspection Evidence appendix template v4 Page 236
Cleanliness, infection control and hygiene
The service controlled infection risk well. The service used systems to identify and prevent
surgical site infections. Staff used equipment and control measures to protect patients,
themselves and others from infection. They kept equipment and the premises visibly clean.
Ward areas were clean and had suitable furnishings which were clean and well-maintained. We
visited all clinical areas that cared for gynaecology patients, we found all areas were visibly clean
and had disposable privacy curtains. The curtains were dated on commissioning, all of the curtains
we reviewed were dated appropriately.
Cleaning records were up-to-date and demonstrated that all areas were cleaned regularly.
Cleaning records we reviewed showed that cleaning had taken place in ward areas, clinics and
theatres.
Staff followed infection control principles including the use of personal protective equipment (PPE).
In all areas we visited, staff decontaminated their hands appropriately before and after patient
care. Staff wore uniforms with short sleeves and were bare below the elbows. They used personal
protective equipment in line with the trust’s infection prevention and control policy and disposed of
the items correctly.
The service completed monthly hand hygiene audits. We reviewed the hand hygiene audit results
from May to October 2019 which consistently scored 100% compliance.
Staff cleaned equipment after patient contact and labelled equipment to show when it was last
cleaned. We observed reusable medical equipment such as dressing trolleys, intravenous infusion
stands, and commodes were visibly clean and had dated green “I am clean” stickers attached to
signify that the equipment had been cleaned and was ready for use. Clinic staff cleaned
equipment between patients’ appointments, such as examination couches and ultrasound
equipment.
Elective gynaecology patients were screened for hospital associated infections such as methicillin
resistant staphylococcus aureus (MRSA). Elective surgical patients received screening during their
pre-assessment appointment prior to their admission to hospital. Pre-assessment staff referred
any patient that had a positive result to the infection prevention and control team for treatment.
Patients on the emergency gynaecology pathway of care were screened during the admission
process and isolated appropriately if there were any concerns about hospital associated infections.
We reviewed the MRSA screening audits conducted from October 2018 to September 2019 which
showed that gynaecology patients were screened in line with trust’s 95% target for seven out of 12
months. The data showed that screening was just below the trust’s target in October 2018,
November 2018, May 2019 and July 2019, however in February 2019 only 88% of elective
gynaecology patients received screening.
Managers we spoke with told us that the staff completed a fast track MRSA swab test for patients
that had been missed during the pre-assessment process. The ward received MRSA swab results
within two hours.
Environment and equipment
The design, maintenance and use of facilities, premises and equipment kept people safe.
Staff were trained to use them. Staff managed clinical waste well.
20190416 900885 Post-inspection Evidence appendix template v4 Page 237
Patients could reach call bells and staff responded quickly when called. Each bed space on
Gosfield ward had a call bell system. We observed call bells were within the reach of patients, and
when patients called for help, staff were prompt responding to their needs.
The design of the environment followed national guidance. Gynaecology had ten protected beds
on Gosfield ward, the gynaecology ambulatory care unit had four trolleys for patient assessments,
two procedure rooms within the gynaecology treatment unit and outpatient clinic rooms.
Gynaecological surgeries were performed within a designated theatre in the main theatre suite.
Staff carried out daily safety checks of specialist equipment. Ward and clinic staff completed daily
checks of the emergency resuscitation trolleys. We reviewed records in outpatient clinics and on
Gosfield ward which demonstrated staff had completed daily and weekly checks. We checked the
resuscitation trolley on Gosfield ward and we found all equipment listed was available and within
their expiry date.
The service had enough suitable equipment to help them to safely care for patients. The service
used a range of single use consumable equipment items such as syringes, needles and
intravenous infusion lines. We randomly checked 32 items of single use equipment and found they
were stored appropriately and were within their expiry date.
The trust had a team of engineers who were responsible for the management of medical device
maintenance. The trust had a medical device database in place for the oversight of medical device
maintenance and safety testing. The biomedical engineering department submitted quarterly
reports of compliance and performance to the health and safety group and the medical device
group. We checked eight items of electrical equipment such as examination couches, diathermy
machines and blood pressure machines. All equipment was up-to-date with electrical safety
testing and servicing in line with manufacturers guidance.
Staff disposed of clinical waste safely. Waste bins were monitored throughout the day and staff
disposed of clinical and domestic waste appropriately. Staff disposed of sharp items, such as
injection needles, in clinical waste sharps bins. We reviewed six sharps bins and found these were
labelled, dated, included the clinical area and were not overfilled.
Assessing and responding to patient risk
Staff completed and updated risk assessments for each patient and removed or minimised
risks. Staff identified and quickly acted upon patients at risk of deterioration.
Staff used a nationally recognised tool to identify deteriorating patients and escalated them
appropriately. Staff used the NEWS2 tool to monitor patients and identify a deteriorating patient.
NEWS2 is a nationally standardised assessment of illness severity and determines the need for
escalation based on a range of patient vital observations. The trust had a central team that
monitored patient vital observations electronically and alerted teams if a NEWS2 score triggered
escalation. The Trigger team had oversight of patients that triggered the NEWS2 assessment
through electronic clinical observation tracking throughout the trust to reduce delays in the
identification and treatment of sepsis. We reviewed 12 patient records and we found that all
patients had vital observations recorded at the right time and staff had escalated patients in line
with trust policy.
Staff had access to the sepsis six care bundle to manage patients with suspected sepsis. Sepsis
is rare but a serious complication to an infection which requires timely identification and antibiotic
management to prevent long term organ damage or death. At the time of our inspections no
20190416 900885 Post-inspection Evidence appendix template v4 Page 238
patients had triggered the NEWS2 for suspected sepsis. Staff we spoke with knew how to
implement the sepsis six care bundle and escalate their patients when the NEWS2 triggered signs
of sepsis.
Staff had access to consultant support either on site or on-call 24 hours a day, seven days a week
in the event of a deteriorating patient. Consultants worked an on-call rota to ensure staff had
access to consultant support when required.
Staff did not always fully complete all risk assessments for each patient on admission or arrival
and updated them when necessary and used recognised tools. The service did not always
complete venous thromboembolism risk screening in line with the trust’s target. Manages
monitored the completion of venous thromboembolism (VTE) risk screening in gynaecology. The
trust’s target for VTE risk screening was 95% of patients. We reviewed the VTE risk screening
audits from November 2018 to October 2019 which showed that the service only met the target in
December 2018 and January 2019. Managers for the service included VTE risk screening
completion within the weekly safety briefing from October 2019.
Staff completed risk assessments such as the Waterlow pressure ulcer risk, malnutrition universal
scoring tool and fall risk assessments as part of the patient admission process. Staff reviewed
these risk assessments daily and updated the assessments as the patient’s condition changed.
Staff knew about and dealt with any specific risk issues. Theatres had a major haemorrhage
protocol in place. The matron for maternity and gynaecology planned to provide additional major
haemorrhage training for gynaecology ward staff. The matron had additional resources on order to
staff had medications and equipment in place to manage a major haemorrhage once the training
was completed.
All patients admitted for elective gynaecology procedures had pre-admission assessments which
included an anaesthetist review where pre-assessment staff identified increased risks such as
high blood pressure and respiratory abnormalities.
Gynaecological procedures were undertaken within a designated theatre in the main theatre suite.
The theatre teams had completed competencies specific to gynaecological procedures. Theatres
used the World Health Organisation (WHO) five steps to safer surgery checklist. Staff used an
electronic system to audit compliance, with briefing, sign in, time out, sign out and debrief stages
of the World Health Organisation (WHO) five steps to safer surgery checklist in main theatres.
Theatres had local safety standards for invasive procedures in place. Theatre staff had a process
called ‘pause for gauze’ to ensure that all gauze swabs were accounted for before the surgical
wound was closed. Staff followed this safety standard in the allocated gynaecology theatre.
Gynaecology services did not routinely provide termination of pregnancy, a partner private
provider had a contract for the provision of termination of pregnancies. However, the service
carried out a small number of medical termination of pregnancies where foetal abnormalities were
detected through routine pregnancy monitoring.
The service had 24-hour access to mental health liaison and specialist mental health support (if
staff were concerned about a patient’s mental health). Staff could refer their patients for a mental
health assessment if they had concerns that a patient was at risk of harm due to new or existing
mental health condition. Staff contacted the hospital site management team to request either a
mental health review or support.
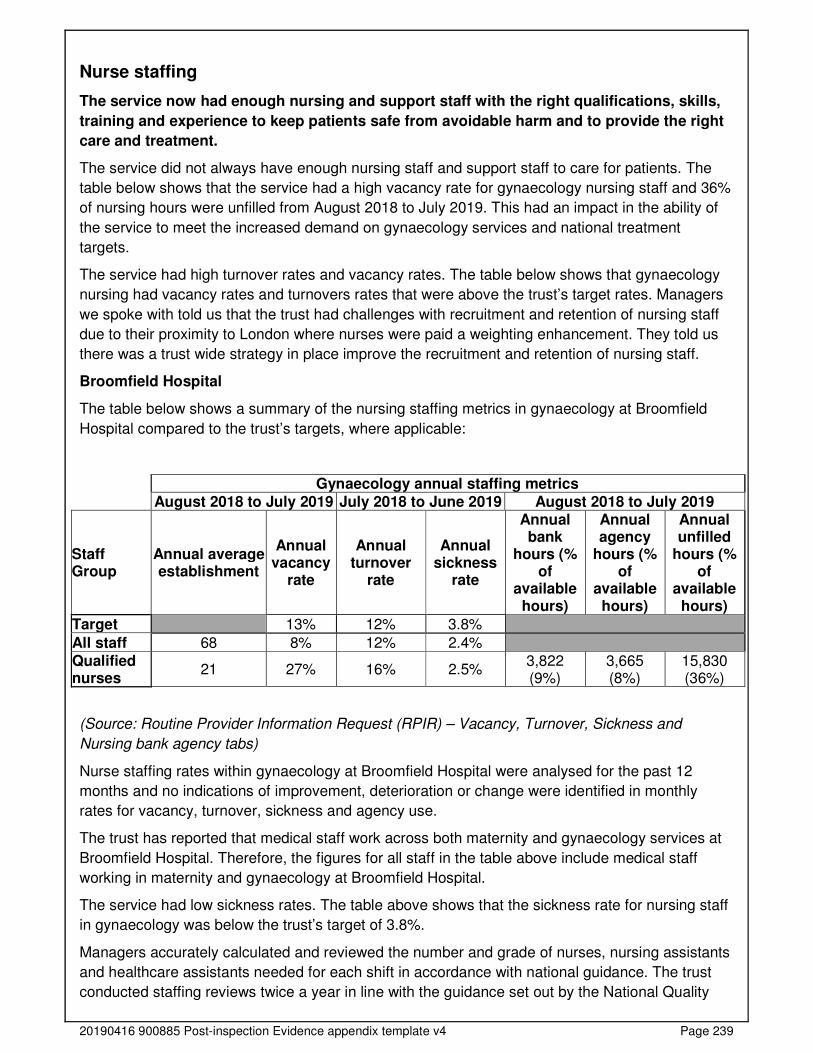
20190416 900885 Post-inspection Evidence appendix template v4 Page 239
Nurse staffing
The service now had enough nursing and support staff with the right qualifications, skills,
training and experience to keep patients safe from avoidable harm and to provide the right
care and treatment.
The service did not always have enough nursing staff and support staff to care for patients. The
table below shows that the service had a high vacancy rate for gynaecology nursing staff and 36%
of nursing hours were unfilled from August 2018 to July 2019. This had an impact in the ability of
the service to meet the increased demand on gynaecology services and national treatment
targets.
The service had high turnover rates and vacancy rates. The table below shows that gynaecology
nursing had vacancy rates and turnovers rates that were above the trust’s target rates. Managers
we spoke with told us that the trust had challenges with recruitment and retention of nursing staff
due to their proximity to London where nurses were paid a weighting enhancement. They told us
there was a trust wide strategy in place improve the recruitment and retention of nursing staff.
Broomfield Hospital
The table below shows a summary of the nursing staffing metrics in gynaecology at Broomfield
Hospital compared to the trust’s targets, where applicable:
Gynaecology annual staffing metrics
August 2018 to July 2019 July 2018 to June 2019 August 2018 to July 2019
Staff Group
Annual average establishment
Annual vacancy
rate
Annual turnover
rate
Annual sickness
rate
Annual bank
hours (% of
available hours)
Annual agency
hours (% of
available hours)
Annual unfilled
hours (% of
available hours)
Target 13% 12% 3.8%
All staff 68 8% 12% 2.4%
Qualified nurses
21 27% 16% 2.5% 3,822 (9%)
3,665 (8%)
15,830 (36%)
(Source: Routine Provider Information Request (RPIR) – Vacancy, Turnover, Sickness and
Nursing bank agency tabs)
Nurse staffing rates within gynaecology at Broomfield Hospital were analysed for the past 12
months and no indications of improvement, deterioration or change were identified in monthly
rates for vacancy, turnover, sickness and agency use.
The trust has reported that medical staff work across both maternity and gynaecology services at
Broomfield Hospital. Therefore, the figures for all staff in the table above include medical staff
working in maternity and gynaecology at Broomfield Hospital.
The service had low sickness rates. The table above shows that the sickness rate for nursing staff
in gynaecology was below the trust’s target of 3.8%.
Managers accurately calculated and reviewed the number and grade of nurses, nursing assistants
and healthcare assistants needed for each shift in accordance with national guidance. The trust
conducted staffing reviews twice a year in line with the guidance set out by the National Quality

20190416 900885 Post-inspection Evidence appendix template v4 Page 240
Board (NQB). Managers used the Shelford Group Safer Nursing Care Tool (SNCT) to assess staff
requirements for each clinical area. The last data collection was undertaken in June 2019. At the
time of our inspection Gosfield ward had no staff vacancies.
The trust held bed meetings four times each day where safe staffing levels were reviewed at each
bed meeting, to identify areas that had lower than expected staff or that required further support.
Matrons for the division conducted daily safety huddles to mitigate any risk areas. They escalated
any areas with reduced staffing at a daily staffing meeting with the deputy director of nursing to
ensure that cross divisional support was addressed. Managers reviewed the daily acuity and
dependency risk assessment tool to ensure that managers utilised workforce effectively in clinical
areas.
The ward manager could adjust staffing levels daily according to the needs of patients. The
divisional senior nursing team reviewed ward staffing levels and mitigated staff shortages which
they recorded within the electronic staffing system. Managers had access to bank and agency
staff where they had vacant shifts.
Incident reporting of staffing issues and red flags as described by the NQB are captured within the
trust's incident reporting system and reviewed monthly within the monthly ward staffing review
paper.
Bank staff usage
Monthly bank hours over the last 12 months for qualified nurses show an upward shift from
February 2019 to July 2019.
(Source: Routine Provider Information Request (RPIR) - Nursing Bank and Agency tab)
The service had an increased bank staffing rate from February 2019 to July 2019 to cover vacant
shifts due to staff vacancies. Managers had recruited staff to vacancies during this period and staff
numbers met establishment at the time of our inspection.
The trust introduced a preferred supplier list arrangement for general nursing agencies in 2019,
which adhered to the NHS employer standard checks. This ensured that agency staff had
clearances such as identity checks, references and employment history, qualifications and
professional registration, occupational health and Disclosure and Baring Service (DBS). The ward
manager completed a local induction checklist. We checked completed agency induction
checklists and we found that documents were completed correctly, dated and signed.
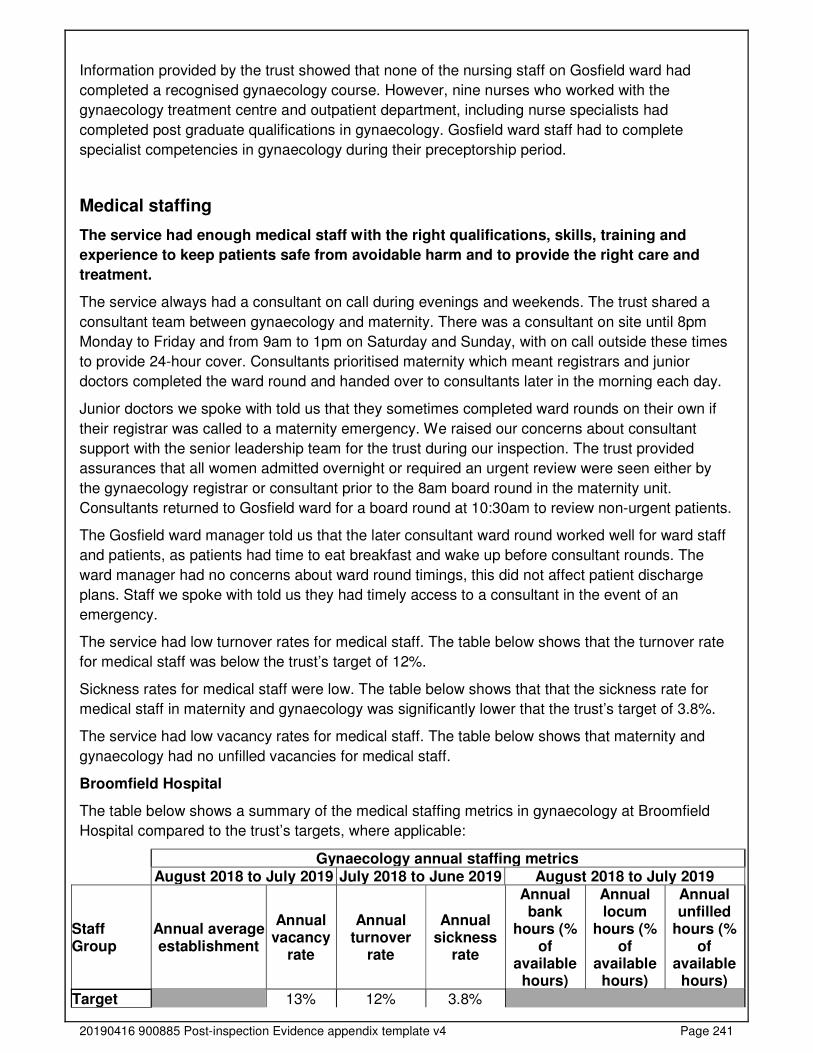
20190416 900885 Post-inspection Evidence appendix template v4 Page 241
Information provided by the trust showed that none of the nursing staff on Gosfield ward had
completed a recognised gynaecology course. However, nine nurses who worked with the
gynaecology treatment centre and outpatient department, including nurse specialists had
completed post graduate qualifications in gynaecology. Gosfield ward staff had to complete
specialist competencies in gynaecology during their preceptorship period.
Medical staffing
The service had enough medical staff with the right qualifications, skills, training and
experience to keep patients safe from avoidable harm and to provide the right care and
treatment.
The service always had a consultant on call during evenings and weekends. The trust shared a
consultant team between gynaecology and maternity. There was a consultant on site until 8pm
Monday to Friday and from 9am to 1pm on Saturday and Sunday, with on call outside these times
to provide 24-hour cover. Consultants prioritised maternity which meant registrars and junior
doctors completed the ward round and handed over to consultants later in the morning each day.
Junior doctors we spoke with told us that they sometimes completed ward rounds on their own if
their registrar was called to a maternity emergency. We raised our concerns about consultant
support with the senior leadership team for the trust during our inspection. The trust provided
assurances that all women admitted overnight or required an urgent review were seen either by
the gynaecology registrar or consultant prior to the 8am board round in the maternity unit.
Consultants returned to Gosfield ward for a board round at 10:30am to review non-urgent patients.
The Gosfield ward manager told us that the later consultant ward round worked well for ward staff
and patients, as patients had time to eat breakfast and wake up before consultant rounds. The
ward manager had no concerns about ward round timings, this did not affect patient discharge
plans. Staff we spoke with told us they had timely access to a consultant in the event of an
emergency.
The service had low turnover rates for medical staff. The table below shows that the turnover rate
for medical staff was below the trust’s target of 12%.
Sickness rates for medical staff were low. The table below shows that that the sickness rate for
medical staff in maternity and gynaecology was significantly lower that the trust’s target of 3.8%.
The service had low vacancy rates for medical staff. The table below shows that maternity and
gynaecology had no unfilled vacancies for medical staff.
Broomfield Hospital
The table below shows a summary of the medical staffing metrics in gynaecology at Broomfield
Hospital compared to the trust’s targets, where applicable:
Gynaecology annual staffing metrics August 2018 to July 2019 July 2018 to June 2019 August 2018 to July 2019
Staff Group
Annual average establishment
Annual vacancy
rate
Annual turnover
rate
Annual sickness
rate
Annual bank
hours (% of
available hours)
Annual locum
hours (% of
available hours)
Annual unfilled
hours (% of
available hours)
Target 13% 12% 3.8%
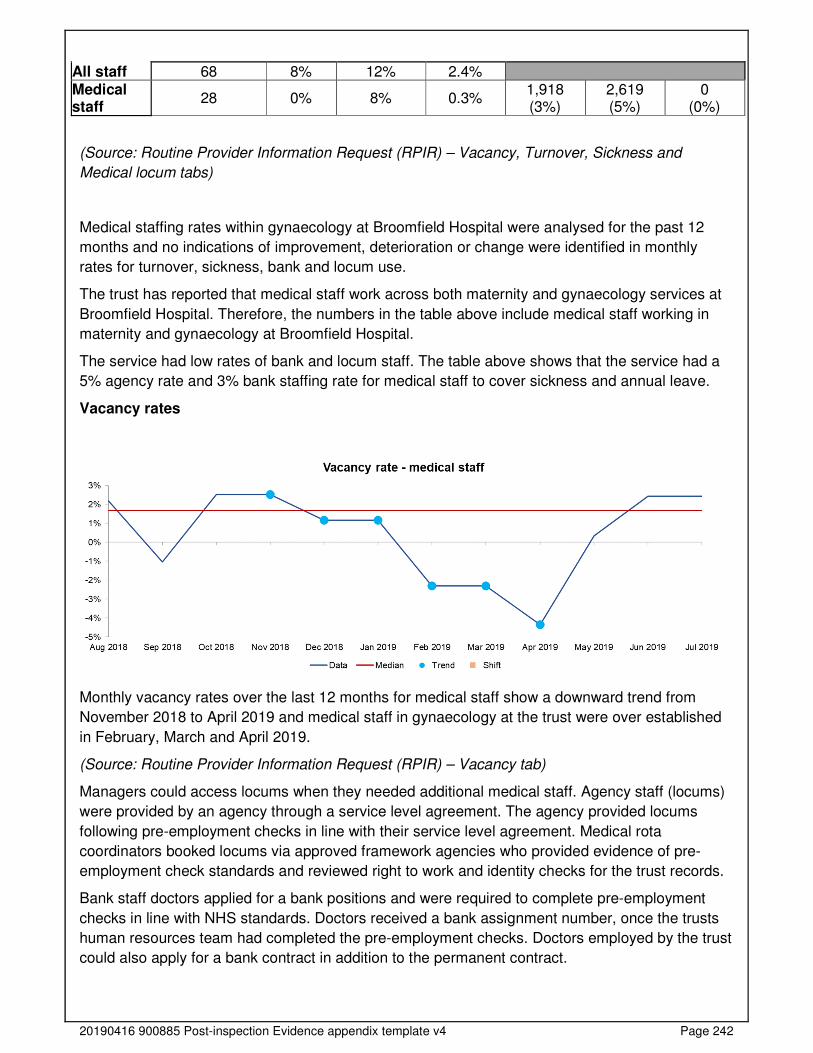
20190416 900885 Post-inspection Evidence appendix template v4 Page 242
All staff 68 8% 12% 2.4% Medical staff
28 0% 8% 0.3% 1,918 (3%)
2,619 (5%)
0 (0%)
(Source: Routine Provider Information Request (RPIR) – Vacancy, Turnover, Sickness and
Medical locum tabs)
Medical staffing rates within gynaecology at Broomfield Hospital were analysed for the past 12
months and no indications of improvement, deterioration or change were identified in monthly
rates for turnover, sickness, bank and locum use.
The trust has reported that medical staff work across both maternity and gynaecology services at
Broomfield Hospital. Therefore, the numbers in the table above include medical staff working in
maternity and gynaecology at Broomfield Hospital.
The service had low rates of bank and locum staff. The table above shows that the service had a
5% agency rate and 3% bank staffing rate for medical staff to cover sickness and annual leave.
Vacancy rates
Monthly vacancy rates over the last 12 months for medical staff show a downward trend from
November 2018 to April 2019 and medical staff in gynaecology at the trust were over established
in February, March and April 2019.
(Source: Routine Provider Information Request (RPIR) – Vacancy tab)
Managers could access locums when they needed additional medical staff. Agency staff (locums)
were provided by an agency through a service level agreement. The agency provided locums
following pre-employment checks in line with their service level agreement. Medical rota
coordinators booked locums via approved framework agencies who provided evidence of pre-
employment check standards and reviewed right to work and identity checks for the trust records.
Bank staff doctors applied for a bank positions and were required to complete pre-employment
checks in line with NHS standards. Doctors received a bank assignment number, once the trusts
human resources team had completed the pre-employment checks. Doctors employed by the trust
could also apply for a bank contract in addition to the permanent contract.
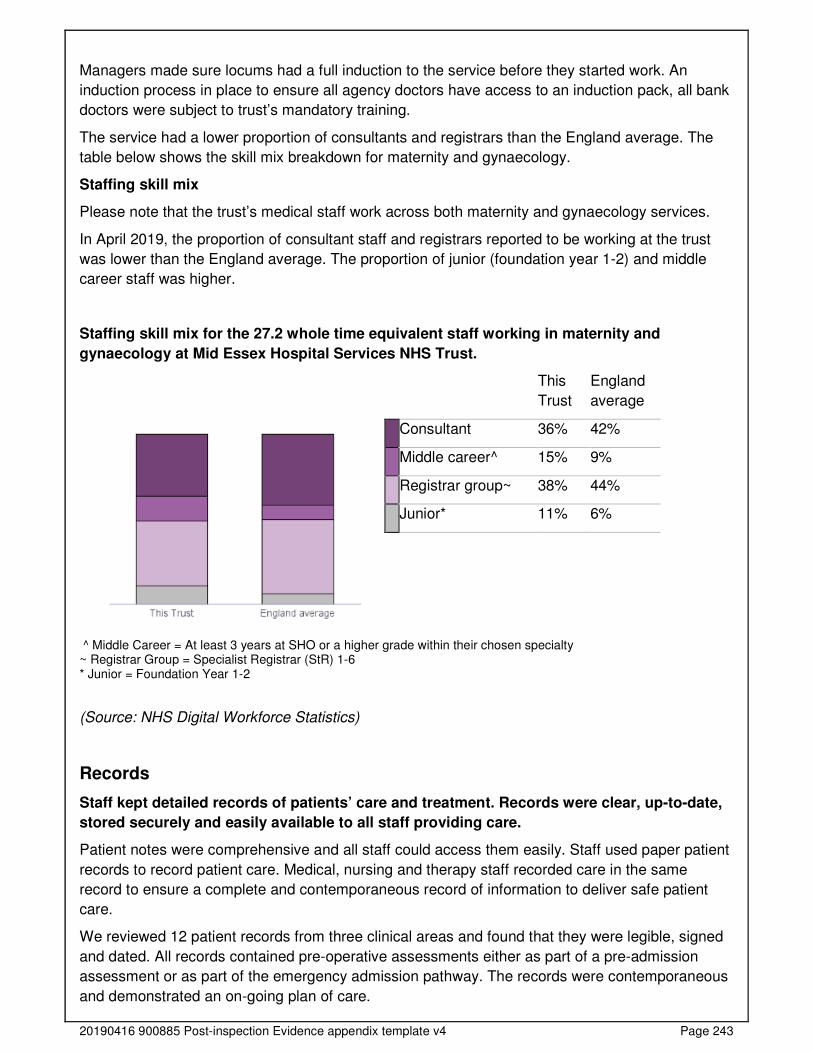
20190416 900885 Post-inspection Evidence appendix template v4 Page 243
Managers made sure locums had a full induction to the service before they started work. An
induction process in place to ensure all agency doctors have access to an induction pack, all bank
doctors were subject to trust’s mandatory training.
The service had a lower proportion of consultants and registrars than the England average. The
table below shows the skill mix breakdown for maternity and gynaecology.
Staffing skill mix
Please note that the trust’s medical staff work across both maternity and gynaecology services.
In April 2019, the proportion of consultant staff and registrars reported to be working at the trust
was lower than the England average. The proportion of junior (foundation year 1-2) and middle
career staff was higher.
Staffing skill mix for the 27.2 whole time equivalent staff working in maternity and
gynaecology at Mid Essex Hospital Services NHS Trust.
This
Trust
England
average
Consultant 36% 42%
Middle career^ 15% 9%
Registrar group~ 38% 44%
Junior* 11% 6%
^ Middle Career = At least 3 years at SHO or a higher grade within their chosen specialty ~ Registrar Group = Specialist Registrar (StR) 1-6 * Junior = Foundation Year 1-2
(Source: NHS Digital Workforce Statistics)
Records
Staff kept detailed records of patients’ care and treatment. Records were clear, up-to-date,
stored securely and easily available to all staff providing care.
Patient notes were comprehensive and all staff could access them easily. Staff used paper patient
records to record patient care. Medical, nursing and therapy staff recorded care in the same
record to ensure a complete and contemporaneous record of information to deliver safe patient
care.
We reviewed 12 patient records from three clinical areas and found that they were legible, signed
and dated. All records contained pre-operative assessments either as part of a pre-admission
assessment or as part of the emergency admission pathway. The records were contemporaneous
and demonstrated an on-going plan of care.
20190416 900885 Post-inspection Evidence appendix template v4 Page 244
We reviewed seven patient records on Gosfield ward which demonstrated that staff had completed
intentional rounding. All the records we reviewed had up to date risk assessments such as
Waterlow pressure ulcer risk, malnutrition universal scoring tool (MUST) and a falls risk
assessment.
Managers monitored staff completion of medical records and completed monthly patient record
audits on Gosfield ward. We reviewed the audit results for September and October 2019 where
the compliance rate for record keeping was 99% and 100% respectively.
When patients transferred to a new team, there were no delays in staff accessing their records.
Staff ensured patients records were transferred with patients from one area to another within the
hospital. Medical staff completed discharge summaries electronically which were sent directly to
the patient’s general practitioner (GP) through the electronic system. Staff printed a copy of the
discharge summary, which was given to the patient.
Staff kept records securely within gynaecology services. We observed ward staff kept records
securely in keypad secured trolleys in a staff area. In the gynaecology treatment centre, staff kept
all patient records in a locked office when they were not in use. Staff had access to the office to
retrieve records for patient appointments and they returned records to the office following patients’
treatments.
Medicines
The service used systems and processes to safely prescribe, administer, record and store
medicines.
Staff followed systems and processes when safely prescribing, administering, recording and
storing medicines. Staff used paper prescription records. We reviewed seven prescription records
on Gosfield ward which demonstrated patients had received their medicines at the right time.
Staff reviewed patients' medicines regularly and provided specific advice to patients and carers
about their medicines. We reviewed seven prescription records of Gosfield ward evidenced that
staff reviewed patients’ medicines daily during ward rounds. Staff provided information to their
patients about their medicines when they administered medicine and during patient discharge
process.
Staff stored and managed medicines and prescribing documents in line with the trust’s policy. Staff
kept medicine securely within a swipe access storage room which was only accessed by staff.
Staff stored controlled drugs within a locked wall mounted cupboard in line with legislation. We
reviewed the controlled drug reconciliation records and we found that the stock matched the
records. Records we reviewed demonstrated that staff checked controlled drugs daily in line with
the trust’s policy.
Staff kept medicines securely within the gynaecology treatment unit. The treatment centre did not
hold controlled drugs within the department. We checked a variety of pain-relieving medicines
such as Voltarol (an anti-inflammatory) and paracetamol and found all medicines were within their
expiry date.
We observed that staff kept medicines fridges locked and monitored the temperatures daily. We
reviewed the fridge temperature records on Gosfield ward and in outpatient clinics and found
these were completed daily without gaps.
20190416 900885 Post-inspection Evidence appendix template v4 Page 245
Staff followed current national practice to check patients had the correct medicines. We observed
staff administering medicines on the wards, they checked medicine prescription, allergies, dosage.
and patients’ wrist identity bands against the prescription chart before they gave patients their
medicines.
The service had systems to ensure staff knew about safety alerts and incidents, so patients
received their medicines safely. Staff completed service specific training and competencies which
included areas such as medical management of miscarriage to ensure they administered these
medicines safely. Managers shared key safety messages during daily safety briefing which
included information about safety alerts and medicines incidents.
Incidents
The service managed patient safety incidents well. Staff recognised and reported incidents
and near misses. Managers investigated incidents and shared lessons learned with the
whole team and the wider service. When things went wrong, staff apologised and gave
patients honest information and suitable support. Managers ensured that actions from
patient safety alerts were implemented and monitored.
Staff knew what incidents to report and how to report them. Staff we spoke with knew how to
report an incident or a near miss. Staff gave examples of incidents they had reported such as,
incidents of violence and aggression from patients or their relatives. Staff demonstrated to us the
electronic system they used to report incidents. Staff reported incidents through an electronic
system which alerted managers that an incident had occurred and required follow up and
investigation.
Staff raised concerns and reported incidents and near misses in line with trust policy. The trust
had an incident reporting policy which set out the responsibilities of staff at all levels in reporting
and investigation of safety incidents. The policy was within the review date and referenced
national guidance and legislation. Staff knew how to access the policy via the trust’s electronic
policy library.
The service had no never events in any of the gynaecology clinical areas. The service had no
reported never events from August 2018 to July 2019.
Never Events
Broomfield Hospital
Never events are serious patient safety incidents that should not happen if healthcare providers
follow national guidance on how to prevent them. Each never event type has the potential to cause
serious patient harm or death but neither need have happened for an incident to be a never event.
From August 2018 to August 2019, the trust reported no incidents that were classified as a never
event in gynaecology at Broomfield Hospital.
(Source: Strategic Executive Information System (STEIS))
Staff understood the duty of candour. They were open and transparent, and gave patients and
families a full explanation if and when things went wrong. Duty of candour is a regulatory duty that
relates to openness and transparency and requires providers of health and social care services to
notify patients (or other relevant persons) of certain ‘notifiable safety incidents’ and provide
reasonable support to that person. Staff received training on the duty of candour during their trust
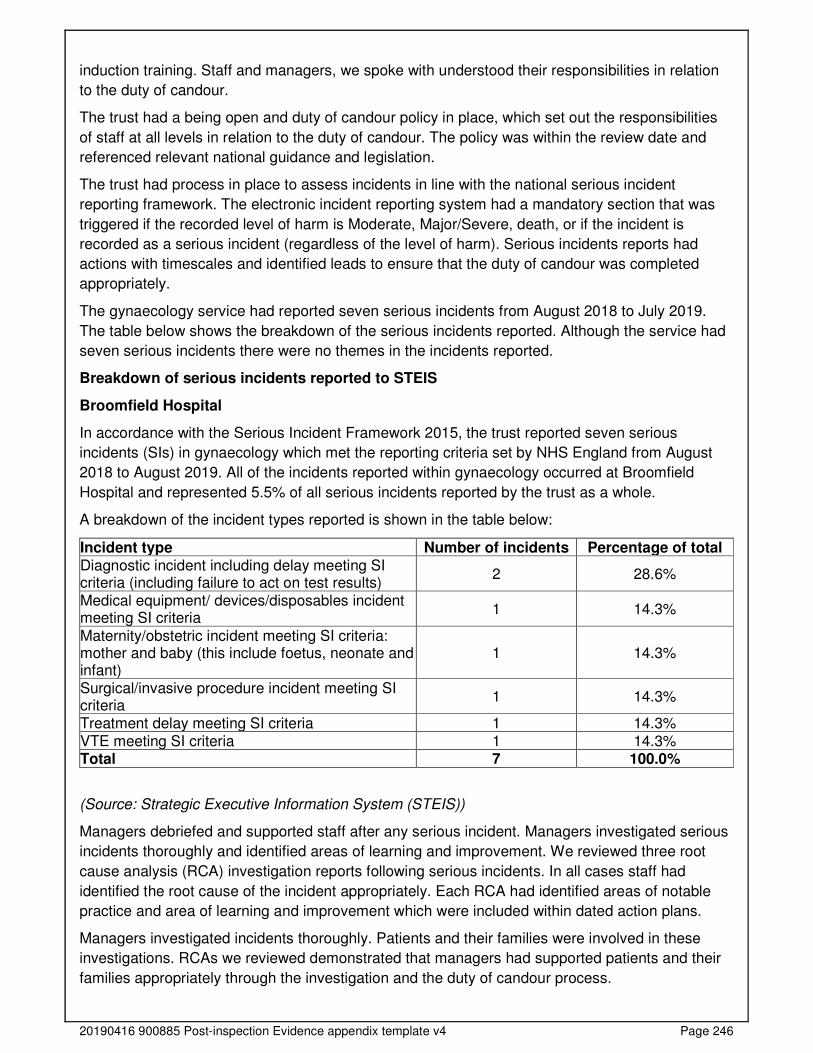
20190416 900885 Post-inspection Evidence appendix template v4 Page 246
induction training. Staff and managers, we spoke with understood their responsibilities in relation
to the duty of candour.
The trust had a being open and duty of candour policy in place, which set out the responsibilities
of staff at all levels in relation to the duty of candour. The policy was within the review date and
referenced relevant national guidance and legislation.
The trust had process in place to assess incidents in line with the national serious incident
reporting framework. The electronic incident reporting system had a mandatory section that was
triggered if the recorded level of harm is Moderate, Major/Severe, death, or if the incident is
recorded as a serious incident (regardless of the level of harm). Serious incidents reports had
actions with timescales and identified leads to ensure that the duty of candour was completed
appropriately.
The gynaecology service had reported seven serious incidents from August 2018 to July 2019.
The table below shows the breakdown of the serious incidents reported. Although the service had
seven serious incidents there were no themes in the incidents reported.
Breakdown of serious incidents reported to STEIS
Broomfield Hospital
In accordance with the Serious Incident Framework 2015, the trust reported seven serious
incidents (SIs) in gynaecology which met the reporting criteria set by NHS England from August
2018 to August 2019. All of the incidents reported within gynaecology occurred at Broomfield
Hospital and represented 5.5% of all serious incidents reported by the trust as a whole.
A breakdown of the incident types reported is shown in the table below:
Incident type Number of incidents Percentage of total Diagnostic incident including delay meeting SI criteria (including failure to act on test results)
2 28.6%
Medical equipment/ devices/disposables incident meeting SI criteria
1 14.3%
Maternity/obstetric incident meeting SI criteria: mother and baby (this include foetus, neonate and infant)
1 14.3%
Surgical/invasive procedure incident meeting SI criteria
1 14.3%
Treatment delay meeting SI criteria 1 14.3% VTE meeting SI criteria 1 14.3% Total 7 100.0%
(Source: Strategic Executive Information System (STEIS))
Managers debriefed and supported staff after any serious incident. Managers investigated serious
incidents thoroughly and identified areas of learning and improvement. We reviewed three root
cause analysis (RCA) investigation reports following serious incidents. In all cases staff had
identified the root cause of the incident appropriately. Each RCA had identified areas of notable
practice and area of learning and improvement which were included within dated action plans.
Managers investigated incidents thoroughly. Patients and their families were involved in these
investigations. RCAs we reviewed demonstrated that managers had supported patients and their
families appropriately through the investigation and the duty of candour process.
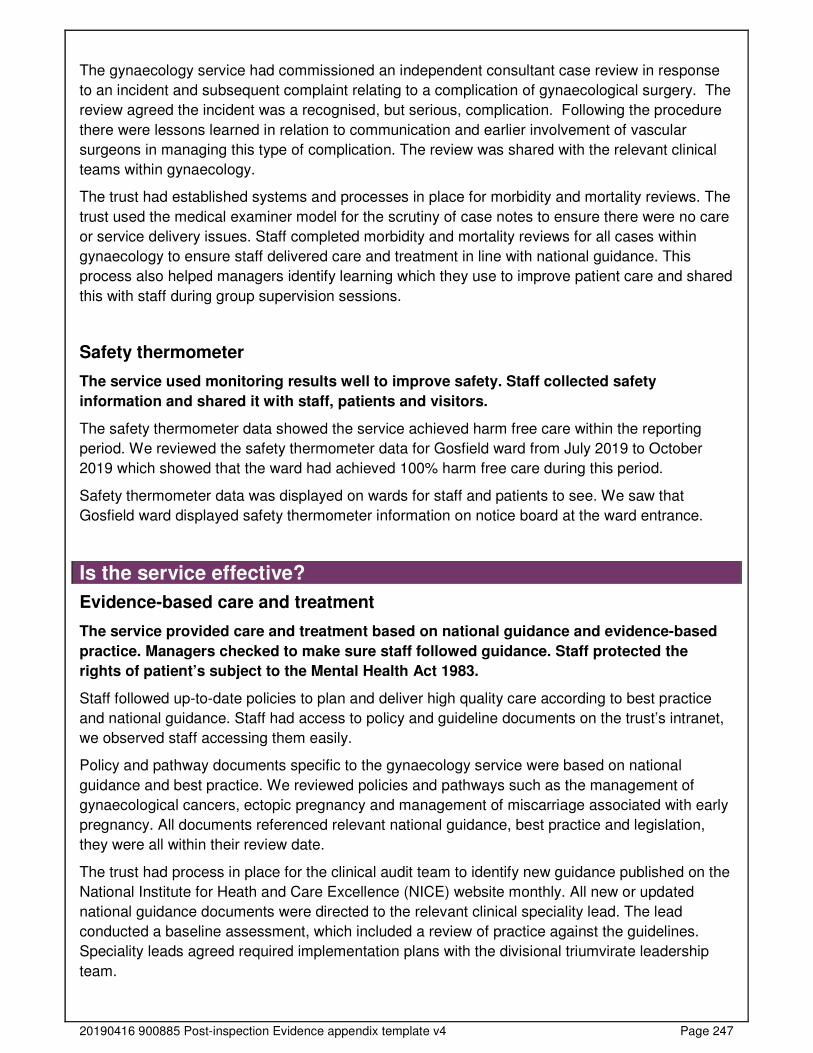
20190416 900885 Post-inspection Evidence appendix template v4 Page 247
The gynaecology service had commissioned an independent consultant case review in response
to an incident and subsequent complaint relating to a complication of gynaecological surgery. The
review agreed the incident was a recognised, but serious, complication. Following the procedure
there were lessons learned in relation to communication and earlier involvement of vascular
surgeons in managing this type of complication. The review was shared with the relevant clinical
teams within gynaecology.
The trust had established systems and processes in place for morbidity and mortality reviews. The
trust used the medical examiner model for the scrutiny of case notes to ensure there were no care
or service delivery issues. Staff completed morbidity and mortality reviews for all cases within
gynaecology to ensure staff delivered care and treatment in line with national guidance. This
process also helped managers identify learning which they use to improve patient care and shared
this with staff during group supervision sessions.
Safety thermometer
The service used monitoring results well to improve safety. Staff collected safety
information and shared it with staff, patients and visitors.
The safety thermometer data showed the service achieved harm free care within the reporting
period. We reviewed the safety thermometer data for Gosfield ward from July 2019 to October
2019 which showed that the ward had achieved 100% harm free care during this period.
Safety thermometer data was displayed on wards for staff and patients to see. We saw that
Gosfield ward displayed safety thermometer information on notice board at the ward entrance.
Is the service effective?
Evidence-based care and treatment
The service provided care and treatment based on national guidance and evidence-based
practice. Managers checked to make sure staff followed guidance. Staff protected the
rights of patient’s subject to the Mental Health Act 1983.
Staff followed up-to-date policies to plan and deliver high quality care according to best practice
and national guidance. Staff had access to policy and guideline documents on the trust’s intranet,
we observed staff accessing them easily.
Policy and pathway documents specific to the gynaecology service were based on national
guidance and best practice. We reviewed policies and pathways such as the management of
gynaecological cancers, ectopic pregnancy and management of miscarriage associated with early
pregnancy. All documents referenced relevant national guidance, best practice and legislation,
they were all within their review date.
The trust had process in place for the clinical audit team to identify new guidance published on the
National Institute for Heath and Care Excellence (NICE) website monthly. All new or updated
national guidance documents were directed to the relevant clinical speciality lead. The lead
conducted a baseline assessment, which included a review of practice against the guidelines.
Speciality leads agreed required implementation plans with the divisional triumvirate leadership
team.
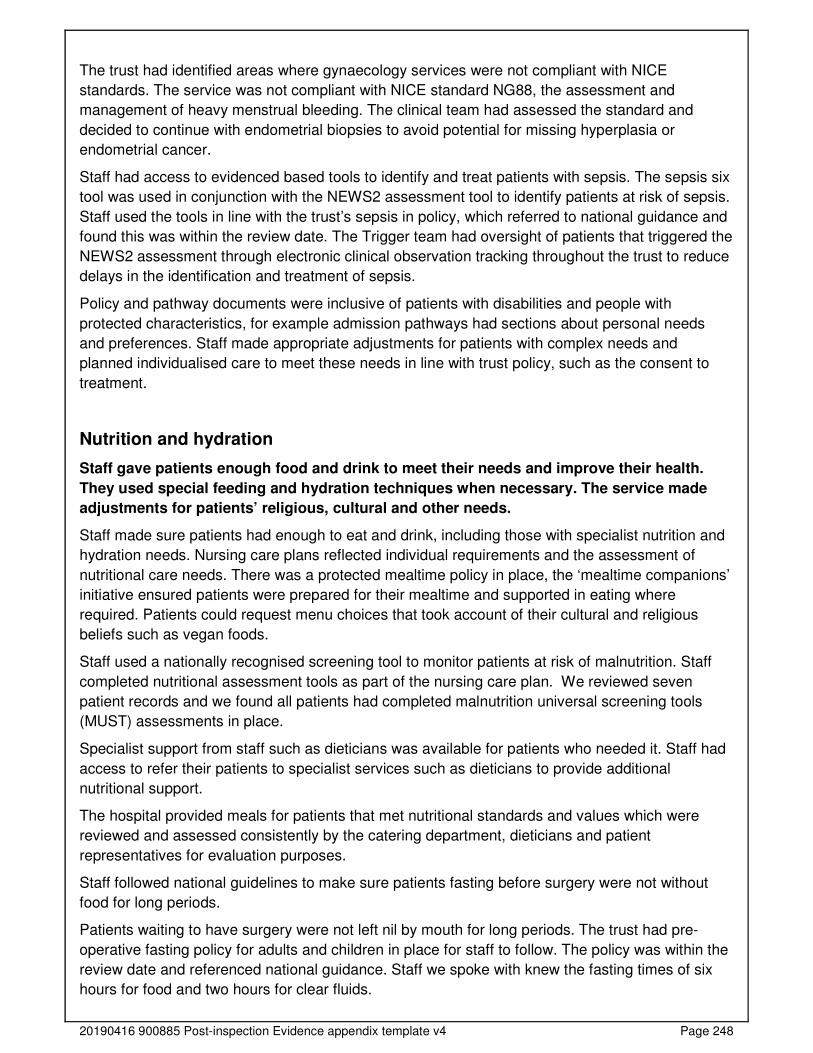
20190416 900885 Post-inspection Evidence appendix template v4 Page 248
The trust had identified areas where gynaecology services were not compliant with NICE
standards. The service was not compliant with NICE standard NG88, the assessment and
management of heavy menstrual bleeding. The clinical team had assessed the standard and
decided to continue with endometrial biopsies to avoid potential for missing hyperplasia or
endometrial cancer.
Staff had access to evidenced based tools to identify and treat patients with sepsis. The sepsis six
tool was used in conjunction with the NEWS2 assessment tool to identify patients at risk of sepsis.
Staff used the tools in line with the trust’s sepsis in policy, which referred to national guidance and
found this was within the review date. The Trigger team had oversight of patients that triggered the
NEWS2 assessment through electronic clinical observation tracking throughout the trust to reduce
delays in the identification and treatment of sepsis.
Policy and pathway documents were inclusive of patients with disabilities and people with
protected characteristics, for example admission pathways had sections about personal needs
and preferences. Staff made appropriate adjustments for patients with complex needs and
planned individualised care to meet these needs in line with trust policy, such as the consent to
treatment.
Nutrition and hydration
Staff gave patients enough food and drink to meet their needs and improve their health.
They used special feeding and hydration techniques when necessary. The service made
adjustments for patients’ religious, cultural and other needs.
Staff made sure patients had enough to eat and drink, including those with specialist nutrition and
hydration needs. Nursing care plans reflected individual requirements and the assessment of
nutritional care needs. There was a protected mealtime policy in place, the ‘mealtime companions’
initiative ensured patients were prepared for their mealtime and supported in eating where
required. Patients could request menu choices that took account of their cultural and religious
beliefs such as vegan foods.
Staff used a nationally recognised screening tool to monitor patients at risk of malnutrition. Staff
completed nutritional assessment tools as part of the nursing care plan. We reviewed seven
patient records and we found all patients had completed malnutrition universal screening tools
(MUST) assessments in place.
Specialist support from staff such as dieticians was available for patients who needed it. Staff had
access to refer their patients to specialist services such as dieticians to provide additional
nutritional support.
The hospital provided meals for patients that met nutritional standards and values which were
reviewed and assessed consistently by the catering department, dieticians and patient
representatives for evaluation purposes.
Staff followed national guidelines to make sure patients fasting before surgery were not without
food for long periods.
Patients waiting to have surgery were not left nil by mouth for long periods. The trust had pre-
operative fasting policy for adults and children in place for staff to follow. The policy was within the
review date and referenced national guidance. Staff we spoke with knew the fasting times of six
hours for food and two hours for clear fluids.
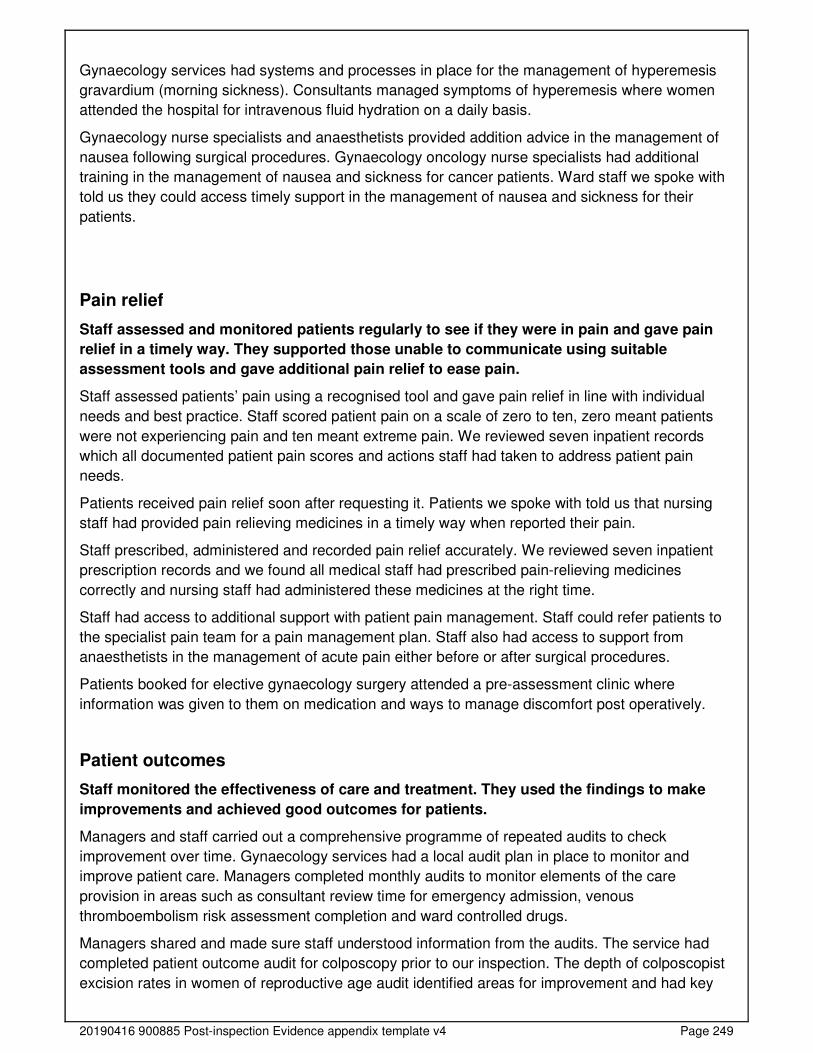
20190416 900885 Post-inspection Evidence appendix template v4 Page 249
Gynaecology services had systems and processes in place for the management of hyperemesis
gravardium (morning sickness). Consultants managed symptoms of hyperemesis where women
attended the hospital for intravenous fluid hydration on a daily basis.
Gynaecology nurse specialists and anaesthetists provided addition advice in the management of
nausea following surgical procedures. Gynaecology oncology nurse specialists had additional
training in the management of nausea and sickness for cancer patients. Ward staff we spoke with
told us they could access timely support in the management of nausea and sickness for their
patients.
Pain relief
Staff assessed and monitored patients regularly to see if they were in pain and gave pain
relief in a timely way. They supported those unable to communicate using suitable
assessment tools and gave additional pain relief to ease pain.
Staff assessed patients’ pain using a recognised tool and gave pain relief in line with individual
needs and best practice. Staff scored patient pain on a scale of zero to ten, zero meant patients
were not experiencing pain and ten meant extreme pain. We reviewed seven inpatient records
which all documented patient pain scores and actions staff had taken to address patient pain
needs.
Patients received pain relief soon after requesting it. Patients we spoke with told us that nursing
staff had provided pain relieving medicines in a timely way when reported their pain.
Staff prescribed, administered and recorded pain relief accurately. We reviewed seven inpatient
prescription records and we found all medical staff had prescribed pain-relieving medicines
correctly and nursing staff had administered these medicines at the right time.
Staff had access to additional support with patient pain management. Staff could refer patients to
the specialist pain team for a pain management plan. Staff also had access to support from
anaesthetists in the management of acute pain either before or after surgical procedures.
Patients booked for elective gynaecology surgery attended a pre-assessment clinic where
information was given to them on medication and ways to manage discomfort post operatively.
Patient outcomes
Staff monitored the effectiveness of care and treatment. They used the findings to make
improvements and achieved good outcomes for patients.
Managers and staff carried out a comprehensive programme of repeated audits to check
improvement over time. Gynaecology services had a local audit plan in place to monitor and
improve patient care. Managers completed monthly audits to monitor elements of the care
provision in areas such as consultant review time for emergency admission, venous
thromboembolism risk assessment completion and ward controlled drugs.
Managers shared and made sure staff understood information from the audits. The service had
completed patient outcome audit for colposcopy prior to our inspection. The depth of colposcopist
excision rates in women of reproductive age audit identified areas for improvement and had key

20190416 900885 Post-inspection Evidence appendix template v4 Page 250
actions for further monitoring. The service leads were in the process of developing a full action
plan and audit tools to monitor improvements.
Managers monitored the trust’s compliance with termination of pregnancy reporting in line with
legislation through the termination of pregnancy audit. We reviewed the audit data from November
2018 to October 2019 which showed 100% compliance for each month with the exception of
February 2019 where there was a breach of two days due to confusion whether a patient had a
spontaneous pregnancy loss or a termination of pregnancy.
Managers used information from the audits to improve care and treatment. The service had an
action plan in place following a risk summit for the service. The risk summit identified gaps in the
service, which took account of serious incident root cause analysis reports and complaint
investigations. The service had completed actions in response to the audit such as staff
competencies and protected emergency ultrasound scanning appointments. Managers were on
track to complete other action within the proposed time scales with full completion due by April
2020. Each action had a named manager responsible for the completion of the action.
Competent staff
The service made sure nursing staff were competent for their roles. Managers appraised
staff’s work performance and held supervision meetings with them to provide support and
development. Medical staff did not always participate in the appraisal process in line with
the trust’s target.
Staff were experienced, qualified and had the right skills and knowledge to meet the needs of
patients. Staff we spoke with had completed the appraisal process and had individual
development plans. Managers kept records of staff competence and qualifications. Staff on
Gosfield ward had group clinical supervision every two months. Ward staff also had an opportunity
to visit the local sexual assault referral centre, so they understood the evidence gathering process,
to support women if they were admitted to the ward following a sexual assault.
Managers gave all new staff a full induction tailored to their role before they started work. All new
nursing staff on Gosfield ward received a local induction. The local induction followed the
corporate trust induction process and included a competency portfolio that required a mentor sign
off process. The competency portfolio covered skills and knowledge such early pregnancy, patient
admission process and patient escalation.
Managers supported staff to develop through yearly, constructive appraisals of their work. Clinical
staff such as registered nurses, doctors and health care assistants participated in a meaningful
appraisal.
Staff had the opportunity to discuss training needs with their line manager and were supported to
develop their skills and knowledge. All staff we spoke with told us they had participated in the
appraisal process with their manager where they reviewed their educational needs and set
mutually agreed objectives. One member of staff we spoke with had been supported to keep their
skills up-to-date, they completed ‘keep in touch’ clinical sessions during the maternity leave. The
staff member worked with another clinician during the sessions to gain confidence.
The table below shows that nursing and clinical services staff had participated in the appraisal
process from August 2018 to July 2019 in line with the trust’s target of 90%. However, the
appraisal rate for medical staff and administrative and clerical staff was below the trust’s target
completion rate.
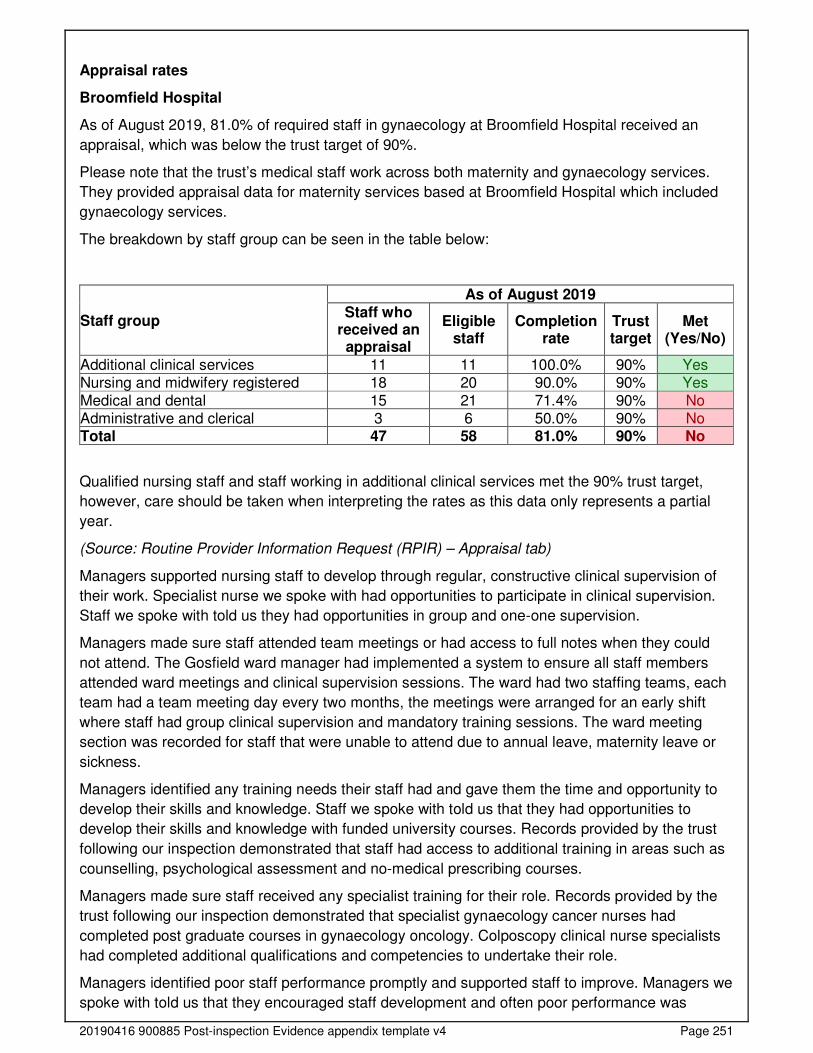
20190416 900885 Post-inspection Evidence appendix template v4 Page 251
Appraisal rates
Broomfield Hospital
As of August 2019, 81.0% of required staff in gynaecology at Broomfield Hospital received an
appraisal, which was below the trust target of 90%.
Please note that the trust’s medical staff work across both maternity and gynaecology services.
They provided appraisal data for maternity services based at Broomfield Hospital which included
gynaecology services.
The breakdown by staff group can be seen in the table below:
Staff group
As of August 2019 Staff who
received an appraisal
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Additional clinical services 11 11 100.0% 90% Yes Nursing and midwifery registered 18 20 90.0% 90% Yes Medical and dental 15 21 71.4% 90% No Administrative and clerical 3 6 50.0% 90% No Total 47 58 81.0% 90% No
Qualified nursing staff and staff working in additional clinical services met the 90% trust target,
however, care should be taken when interpreting the rates as this data only represents a partial
year.
(Source: Routine Provider Information Request (RPIR) – Appraisal tab)
Managers supported nursing staff to develop through regular, constructive clinical supervision of
their work. Specialist nurse we spoke with had opportunities to participate in clinical supervision.
Staff we spoke with told us they had opportunities in group and one-one supervision.
Managers made sure staff attended team meetings or had access to full notes when they could
not attend. The Gosfield ward manager had implemented a system to ensure all staff members
attended ward meetings and clinical supervision sessions. The ward had two staffing teams, each
team had a team meeting day every two months, the meetings were arranged for an early shift
where staff had group clinical supervision and mandatory training sessions. The ward meeting
section was recorded for staff that were unable to attend due to annual leave, maternity leave or
sickness.
Managers identified any training needs their staff had and gave them the time and opportunity to
develop their skills and knowledge. Staff we spoke with told us that they had opportunities to
develop their skills and knowledge with funded university courses. Records provided by the trust
following our inspection demonstrated that staff had access to additional training in areas such as
counselling, psychological assessment and no-medical prescribing courses.
Managers made sure staff received any specialist training for their role. Records provided by the
trust following our inspection demonstrated that specialist gynaecology cancer nurses had
completed post graduate courses in gynaecology oncology. Colposcopy clinical nurse specialists
had completed additional qualifications and competencies to undertake their role.
Managers identified poor staff performance promptly and supported staff to improve. Managers we
spoke with told us that they encouraged staff development and often poor performance was
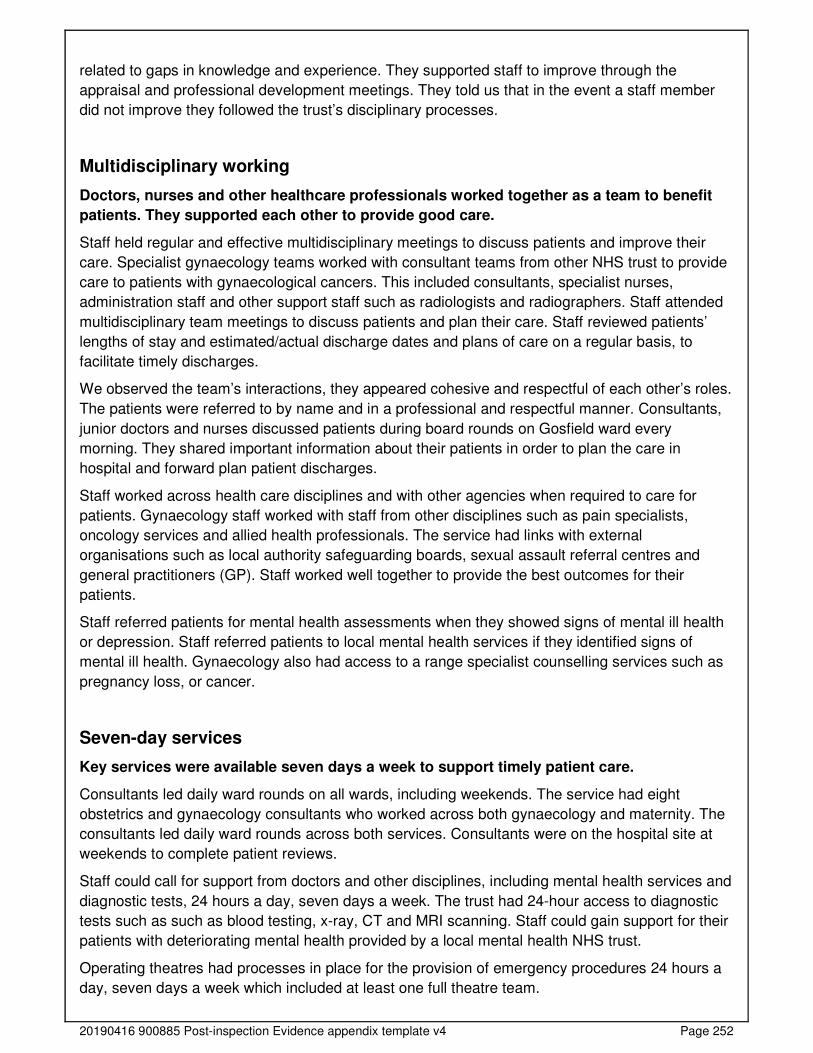
20190416 900885 Post-inspection Evidence appendix template v4 Page 252
related to gaps in knowledge and experience. They supported staff to improve through the
appraisal and professional development meetings. They told us that in the event a staff member
did not improve they followed the trust’s disciplinary processes.
Multidisciplinary working
Doctors, nurses and other healthcare professionals worked together as a team to benefit
patients. They supported each other to provide good care.
Staff held regular and effective multidisciplinary meetings to discuss patients and improve their
care. Specialist gynaecology teams worked with consultant teams from other NHS trust to provide
care to patients with gynaecological cancers. This included consultants, specialist nurses,
administration staff and other support staff such as radiologists and radiographers. Staff attended
multidisciplinary team meetings to discuss patients and plan their care. Staff reviewed patients’
lengths of stay and estimated/actual discharge dates and plans of care on a regular basis, to
facilitate timely discharges.
We observed the team’s interactions, they appeared cohesive and respectful of each other’s roles.
The patients were referred to by name and in a professional and respectful manner. Consultants,
junior doctors and nurses discussed patients during board rounds on Gosfield ward every
morning. They shared important information about their patients in order to plan the care in
hospital and forward plan patient discharges.
Staff worked across health care disciplines and with other agencies when required to care for
patients. Gynaecology staff worked with staff from other disciplines such as pain specialists,
oncology services and allied health professionals. The service had links with external
organisations such as local authority safeguarding boards, sexual assault referral centres and
general practitioners (GP). Staff worked well together to provide the best outcomes for their
patients.
Staff referred patients for mental health assessments when they showed signs of mental ill health
or depression. Staff referred patients to local mental health services if they identified signs of
mental ill health. Gynaecology also had access to a range specialist counselling services such as
pregnancy loss, or cancer.
Seven-day services
Key services were available seven days a week to support timely patient care.
Consultants led daily ward rounds on all wards, including weekends. The service had eight
obstetrics and gynaecology consultants who worked across both gynaecology and maternity. The
consultants led daily ward rounds across both services. Consultants were on the hospital site at
weekends to complete patient reviews.
Staff could call for support from doctors and other disciplines, including mental health services and
diagnostic tests, 24 hours a day, seven days a week. The trust had 24-hour access to diagnostic
tests such as such as blood testing, x-ray, CT and MRI scanning. Staff could gain support for their
patients with deteriorating mental health provided by a local mental health NHS trust.
Operating theatres had processes in place for the provision of emergency procedures 24 hours a
day, seven days a week which included at least one full theatre team.
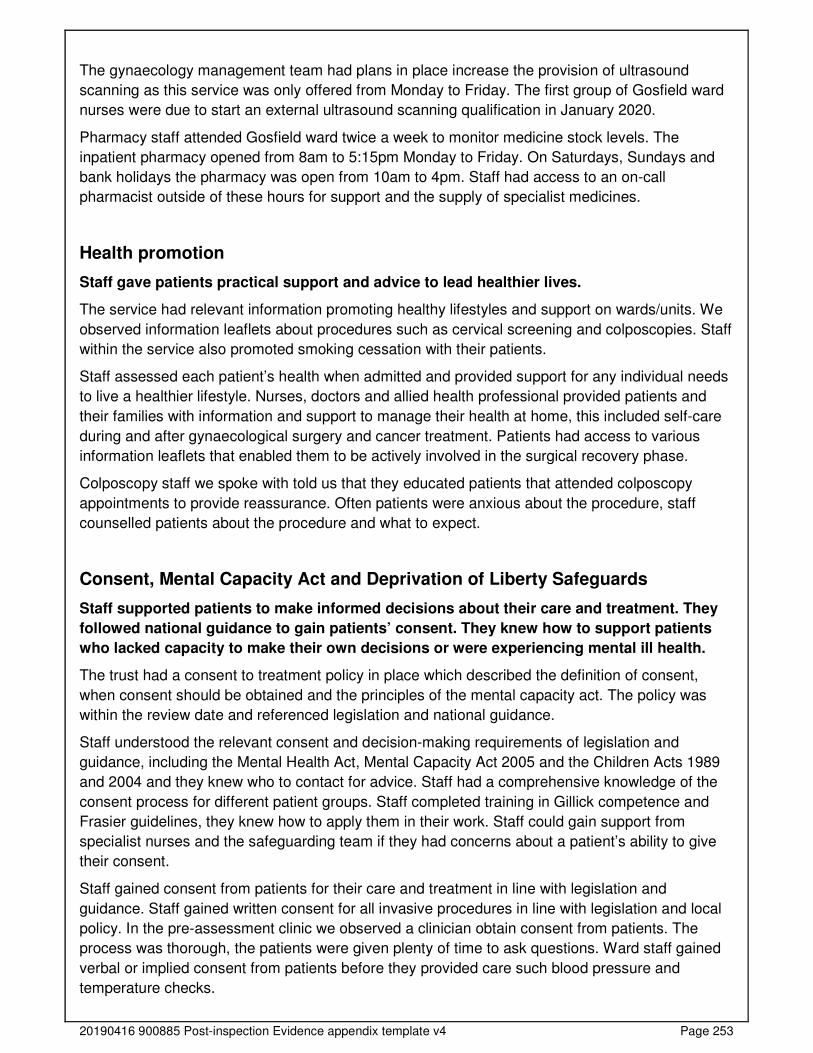
20190416 900885 Post-inspection Evidence appendix template v4 Page 253
The gynaecology management team had plans in place increase the provision of ultrasound
scanning as this service was only offered from Monday to Friday. The first group of Gosfield ward
nurses were due to start an external ultrasound scanning qualification in January 2020.
Pharmacy staff attended Gosfield ward twice a week to monitor medicine stock levels. The
inpatient pharmacy opened from 8am to 5:15pm Monday to Friday. On Saturdays, Sundays and
bank holidays the pharmacy was open from 10am to 4pm. Staff had access to an on-call
pharmacist outside of these hours for support and the supply of specialist medicines.
Health promotion
Staff gave patients practical support and advice to lead healthier lives.
The service had relevant information promoting healthy lifestyles and support on wards/units. We
observed information leaflets about procedures such as cervical screening and colposcopies. Staff
within the service also promoted smoking cessation with their patients.
Staff assessed each patient’s health when admitted and provided support for any individual needs
to live a healthier lifestyle. Nurses, doctors and allied health professional provided patients and
their families with information and support to manage their health at home, this included self-care
during and after gynaecological surgery and cancer treatment. Patients had access to various
information leaflets that enabled them to be actively involved in the surgical recovery phase.
Colposcopy staff we spoke with told us that they educated patients that attended colposcopy
appointments to provide reassurance. Often patients were anxious about the procedure, staff
counselled patients about the procedure and what to expect.
Consent, Mental Capacity Act and Deprivation of Liberty Safeguards
Staff supported patients to make informed decisions about their care and treatment. They
followed national guidance to gain patients’ consent. They knew how to support patients
who lacked capacity to make their own decisions or were experiencing mental ill health.
The trust had a consent to treatment policy in place which described the definition of consent,
when consent should be obtained and the principles of the mental capacity act. The policy was
within the review date and referenced legislation and national guidance.
Staff understood the relevant consent and decision-making requirements of legislation and
guidance, including the Mental Health Act, Mental Capacity Act 2005 and the Children Acts 1989
and 2004 and they knew who to contact for advice. Staff had a comprehensive knowledge of the
consent process for different patient groups. Staff completed training in Gillick competence and
Frasier guidelines, they knew how to apply them in their work. Staff could gain support from
specialist nurses and the safeguarding team if they had concerns about a patient’s ability to give
their consent.
Staff gained consent from patients for their care and treatment in line with legislation and
guidance. Staff gained written consent for all invasive procedures in line with legislation and local
policy. In the pre-assessment clinic we observed a clinician obtain consent from patients. The
process was thorough, the patients were given plenty of time to ask questions. Ward staff gained
verbal or implied consent from patients before they provided care such blood pressure and
temperature checks.
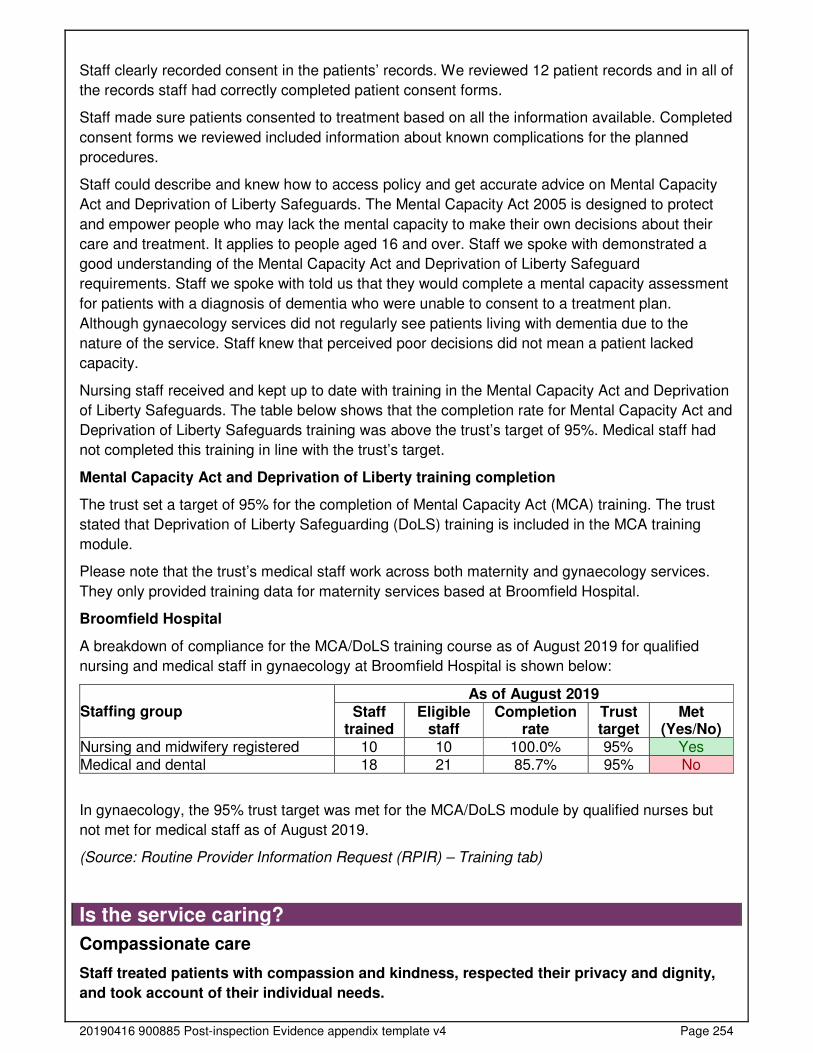
20190416 900885 Post-inspection Evidence appendix template v4 Page 254
Staff clearly recorded consent in the patients’ records. We reviewed 12 patient records and in all of
the records staff had correctly completed patient consent forms.
Staff made sure patients consented to treatment based on all the information available. Completed
consent forms we reviewed included information about known complications for the planned
procedures.
Staff could describe and knew how to access policy and get accurate advice on Mental Capacity
Act and Deprivation of Liberty Safeguards. The Mental Capacity Act 2005 is designed to protect
and empower people who may lack the mental capacity to make their own decisions about their
care and treatment. It applies to people aged 16 and over. Staff we spoke with demonstrated a
good understanding of the Mental Capacity Act and Deprivation of Liberty Safeguard
requirements. Staff we spoke with told us that they would complete a mental capacity assessment
for patients with a diagnosis of dementia who were unable to consent to a treatment plan.
Although gynaecology services did not regularly see patients living with dementia due to the
nature of the service. Staff knew that perceived poor decisions did not mean a patient lacked
capacity.
Nursing staff received and kept up to date with training in the Mental Capacity Act and Deprivation
of Liberty Safeguards. The table below shows that the completion rate for Mental Capacity Act and
Deprivation of Liberty Safeguards training was above the trust’s target of 95%. Medical staff had
not completed this training in line with the trust’s target.
Mental Capacity Act and Deprivation of Liberty training completion
The trust set a target of 95% for the completion of Mental Capacity Act (MCA) training. The trust
stated that Deprivation of Liberty Safeguarding (DoLS) training is included in the MCA training
module.
Please note that the trust’s medical staff work across both maternity and gynaecology services.
They only provided training data for maternity services based at Broomfield Hospital.
Broomfield Hospital
A breakdown of compliance for the MCA/DoLS training course as of August 2019 for qualified
nursing and medical staff in gynaecology at Broomfield Hospital is shown below:
Staffing group As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Nursing and midwifery registered 10 10 100.0% 95% Yes Medical and dental 18 21 85.7% 95% No
In gynaecology, the 95% trust target was met for the MCA/DoLS module by qualified nurses but
not met for medical staff as of August 2019.
(Source: Routine Provider Information Request (RPIR) – Training tab)
Is the service caring?
Compassionate care
Staff treated patients with compassion and kindness, respected their privacy and dignity,
and took account of their individual needs.
20190416 900885 Post-inspection Evidence appendix template v4 Page 255
Staff were discreet and responsive when caring for patients. Staff took time to interact with
patients and those close to them in a respectful and considerate way. Staff demonstrated caring,
respectful and supportive relationships with their patients and those close to them. We observed
staff delivering care to patients on Gosfield ward, outpatients and during their pre-assessment
appointments. Staff interactions with patients were professional, friendly, and kind. Staff
demonstrated an understanding of the importance of treating patients, and those who were
important to them, in a caring and sensitive manner.
Staff followed policy to keep patient care and treatment confidential. Staff treated patients with
privacy, respect, and dignity by closing curtains in ward bays and doors of side rooms whilst
administering physical and or intimate care. We saw staff maintained patient privacy and dignity in
the gynaecology treatment centre where patients had a separate changing area linked to the main
treatment room. All of the treatment rooms had curtains around doors to maintain patient privacy.
Staff understood and respected the personal, cultural, social and religious needs of patients and
how they may relate to care needs. Staff asked patients about their spiritual or religious
preferences on admission and this information was used to support patients to receive visits from
the chaplaincy team if this was their wish. Staff tailored care to meet patients personal, cultural,
social needs and respected their beliefs. Staff ensured they recorded information about patients
such as if they were vegetarian or vegan to ensure they had appropriate menu choices and
products derived from animals were not used in their care.
Patients said staff treated them well and with kindness. All of the staff we spoke with took pride in
their work and were committed to providing the best care they could to their patients. We spoke
with five patients and two relatives who told us they would recommend the service to others.
Patients felt the staff cared about them, had been very kind and attended to their needs in a timely
way. They said, “Staff are fantastic” and “Nurses are lovely”.
The service had a varied response from patients who completed the friends and family test from
October 2018 to September 2019. The percentage of patients that said they would recommend
Gosfield ward to their friends and family scored from 76% to 100%.
Emotional support
Staff provided emotional support to patients, families and carers to minimise their distress.
They understood patients’ personal, cultural and religious needs.
The trust had a chaplaincy service in place to support patients and those close to them. A team of
trust chaplains and volunteer chaplains delivered spiritual and religious care during daily ward
rounds or following referrals from patients, relatives, staff and community faith leaders.
The trust’s multifaith centre provided resources for those of all faiths for meditation or simply a
quiet space to sit.
The trust had a service level agreement with a mental health service to provide a psychiatric
liaison service to patients when the need for additional support was identified.
Staff gave patients and those close to them help, emotional support and advice when they needed
it. The service had staff with additional counselling skills to provide emotional support to patients.
Four nurses who worked within the gynaecology service had completed additional training in
counselling skills. Staff had additional skills to support patients in areas such as pregnancy loss
and gynaecological cancer support.
20190416 900885 Post-inspection Evidence appendix template v4 Page 256
Staff supported patients who became distressed in an open environment and helped them
maintain their privacy and dignity. Staff had access to quiet rooms where they could comfort
women and their families when they received distressing news. Staff we spoke with demonstrated
empathy about the importance of supporting patients in a way that maintained their privacy and
dignity both on Gosfield ward and in outpatient clinics.
Staff undertook training on breaking bad news and demonstrated empathy when having difficult
conversations. Managers had implemented training for nursing staff in breaking bad news for
nursing staff within gynaecology. Managers we spoke with told us they had plans to roll out the
training to medical staff and emergency departments staff as many women who experienced
pregnancy loss presented in the emergency department. Staff spoke compassionately about
patients they had supported emotionally. Two members of staff gave an example of care and
support they had provided to a patient and their family at the end of their life.
Staff understood the emotional and social impact that a person’s care, treatment or condition had
on their wellbeing and on those close to them. Staff we spoke with understood the emotional
impact of diagnosis’ and treatments had on patients and those close to them. Staff could signpost
patients and their families to specialist counselling and support services especially in cases of
pregnancy loss and cancer diagnosis and treatment.
Understanding and involvement of patients and those close to them
Staff supported and involved patients, families and carers to understand their condition
and make decisions about their care and treatment.
Staff made sure patients and those close to them understood their care and treatment. We
observed staff explaining treatments and discharge arrangements with patients. Staff answered
patients’ questions in a way they understood.
Staff talked with patients, families and carers in a way they could understand. We observed staff
used language that patients understood and gave patients time to ask questions if they were
unsure about anything. In gynaecology treatment centre and the pre-assessment department staff
asked patients if they had any questions about their care and treatment, they answered patient
questions and provided reassurance about any concerns for fears raised.
Patients and their families could give feedback on the service and their treatment and staff
supported them to do this. Where patients or their families raised concerns, staff took time to listen
to the concerns and resolve any issues at the earliest opportunity. Staff we spoke with felt
empowered and able to act on concerns or escalate these to a senior member of the team to
resolve these at the earliest opportunity.
Staff supported patients to make advanced decisions about their care. Specialist gynaecology
oncology nurses coordinated care for patients with a cancer diagnosis and supported patients to
make decisions related to their care. Staff supported patients to make decision about care at the
end of their life.
Staff supported patients to make informed decisions about their care. All patients we spoke with
told us staff had provided information about their care and treatment, so they could make
decisions. Patients felt they had input into decisions about their care and treatment. We observed
that pre-assessment staff prepared patients well for their admission and gynaecological
procedure.
20190416 900885 Post-inspection Evidence appendix template v4 Page 257
Staff could give examples of how they used patient feedback to improve daily practice. Managers
had provided training in counselling skills following feedback from patients. Staff we spoke with
found the training had helped them to hold difficult conversations with patients and their families.
Is the service responsive?
Service delivery to meet the needs of local people
The service planned and provided care in a way that met the needs of local people and the
communities served. It also worked with others in the wider system and local organisations
to plan care.
Managers planned and organised services so they met the changing needs of the local population.
The trust had plans to merge with two other local NHS trust in April 2020. Managers from both
trusts were in the process of mapping services across both trusts in preparation for the merger.
The trust worked closely with other providers within the sustainability and transformation
partnership.
The service relieved pressure on other departments when they could treat patients in a day. The
service was developing an outpatient endometrial ablation clinic to reduce the pressure on
inpatient services. The trust was also in the final phase of implementing manual vacuum aspiration
procedures in outpatient settings to minimise delays in patient care, reduce pressure on theatre
capacity and improve patient experience.
Facilities and premises were appropriate for the services being delivered. The ward, outpatient
clinics, the gynaecology treatment centre and theatres were well equipped and complied with
department of health guidelines. The layout of all clinical areas meant that all areas were
accessible for people using a wheelchair or walking aids.
Staff could access emergency mental health support 24 hours a day, 7 days a week for patients
with mental health problems, learning disabilities and dementia. The trust worked closely with the
local mental health NHS trust in the provision of mental health assessments and treatments that
patients required while they were in hospital. Staff had access to mental health support for their
patients 24 hours a day either face-to-face of by telephone out of hours.
The service had systems to help care for patients in need of additional support or specialist
intervention. The gynaecology service worked closely with local termination of pregnancy
providers. The service had arrangements in place to treat women with complex termination of
pregnancy needs and accepted referrals from local providers to meet the needs of women.
The service worked with local NHS trust in the provision of gynaecological cancer services. The
service worked within the local cancer multidisciplinary network to assess and plan cancer care for
women based on their individual needs and preferences.
Managers monitored and took action to minimise missed appointments. The service used a text
message reminder service for all hospital appointments. The trust sent patient’s a text message
two days before their appointment with information about how to cancel an appointment if they
were unable to attend.
Managers ensured that patients who did not attend appointments were contacted. Managers we
spoke with told us that gynaecology staff contacted patients that did not attend their appointments,
however, this was rare. They told us that the service also advised the patient’s general practitioner
(GP) if they did not attend their appointment.
20190416 900885 Post-inspection Evidence appendix template v4 Page 258
Meeting people’s individual needs
The service was inclusive and took account of patients’ individual needs and preferences.
Staff made reasonable adjustments to help patients access services. They coordinated
care with other services and providers.
Staff made sure patients living with mental health problems, learning disabilities and dementia,
received the necessary care to meet all their needs. The trust had dementia and delirium nurse
specialist in post to support staff to meet the needs of patients living with dementia. The electronic
patient records system had flags for staff to easily identify patients living with dementia, learning
disabilities and mental health diagnosis. The flags provided staff with information about individual
patients with cognitive impairment, which prompted staff that reasonable adjustments may be
required.
The service did not routinely care for patients living with dementia due to the age of the women
that used the service. Staff knew how to support patients living with mental health problems,
dementia and learning disabilities. Staff we spoke with knew how to gain support from specialist
teams to make adjustments to meet the complex needs of their patients.
Staff understood and applied the policy on meeting the information and communication needs of
patients with a disability or sensory loss. Patients with a diagnosis of dementia were assessed
using tools like the 'This is me' document to personalise and individualise care. Staff we spoke
with knew about the personalised care document, although they did not routinely care for patients
with complex needs.
The service had information leaflets available in languages spoken by the patients and local
community. Staff had access to information leaflets in different languages, provided by third-party
provider through a service level agreement. They printed leaflets in different languages when they
needed them.
Managers made sure staff, patients, loved ones and carers could get help from interpreters or
signers when needed. Staff had access to full translation services provided by third-party provider
through a service level agreement with the trust. This service included full translation and
interpreting services including face to face, spoken, written, Braille and sign language. Contact
information was on display in the consulting rooms and available on the staff intranet site.
Gynaecology patients could choose Gosfield ward to provide their end of life care. Staff we spoke
with told us that patients had chosen to be on the ward at the end of their lives because of the
relationships they had built with patients. Staff coordinated end of life care with oncologists, the
pain team and specialist nurses.
The Gosfield ward manager had contributed within the working group that produced the disposal
of fetal remains and other human tissue policy. The policy provided women and their families
choice about what happened to pregnancy loss remains. This meant that women and their families
could arrange cremations and memorial services following pregnancy loss.
The gynaecology service followed up all women after third and fourth degree vaginal tears during
child birth in the perianal assessment clinic. Consultant gynaecologist and urogynaecology
specialists reviewed women in a specialist clinic following vaginal tears to monitor healing and any
complications.

20190416 900885 Post-inspection Evidence appendix template v4 Page 259
Patients were given a choice of food and drink to meet their cultural and religious preferences.
Patients had access to a range of menu choices which met their religious and cultural beliefs. Staff
understood and respected the beliefs of their patients and ensured they had access to food and
drink which supported their beliefs.
Access and flow
We could not assess if people could access the service when they needed it and received
the right care promptly. The trust had suspended the reporting of waiting times from
referral to treatment and arrangements to admit, treat.
We could not gain accurate assurances that people could access the service when they needed it
and receive the right care promptly. Waiting times from referral to treatment (RTT) were not
externally reported at the time of our inspection. From 2018 to 2019, the trust implemented an
electronic patient record system which caused data validity issues and poor quality data. With
agreement from NHS England the trust were excluded from reporting data until they had
completed a review and data cleansing exercise.
Locally, managers told us waiting times were being monitored. However, at the time of our
inspection local leaders were unable to provide us with data to evidence the percentages of harm
reviews or whether the service were meeting the national targets.
Following our inspection we requested data from the senior leadership team We reviewed the data
that was provided, we were not able to analyse trends on unvalidated data. Senior leaders told us
patients that were not able to access services within national targets, received a harm review and
were reported to board in common meetings. They also told us that until they returned to reporting
(scheduled April 2020) ‘shadow reporting’ was in place, which included monthly review meetings
with NHS Improvement/England and commissioners.
Patients did not always receive treatment within agreed timeframes and national targets.
Managers provided information regarding the national two week and 62 day referral to treatment
targets. The service did not consistently meet the national referral to treatment target within 62
days for suspected gynaecology cancers. Although the trust consistently met the two week urgent
referral target from November 2018 to September 2019.
The percentage of people seen by a specialist within 62 days of an urgent GP referral from
November 2018 to September 2019 ranged from 0% (in January 2019 and March 2019) to 100%
(in November 2018, February 2019 and August 2019). The trust met the 85% operational standard
in five of the 11 months.
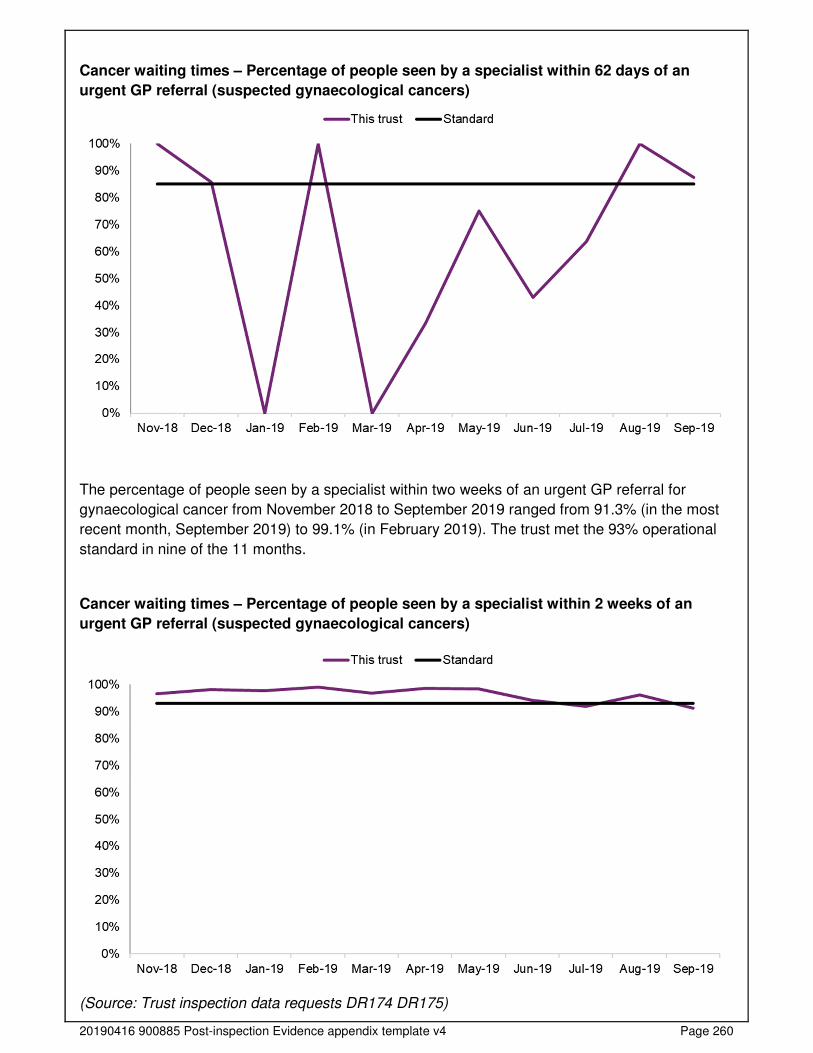
20190416 900885 Post-inspection Evidence appendix template v4 Page 260
Cancer waiting times – Percentage of people seen by a specialist within 62 days of an
urgent GP referral (suspected gynaecological cancers)
The percentage of people seen by a specialist within two weeks of an urgent GP referral for
gynaecological cancer from November 2018 to September 2019 ranged from 91.3% (in the most
recent month, September 2019) to 99.1% (in February 2019). The trust met the 93% operational
standard in nine of the 11 months.
Cancer waiting times – Percentage of people seen by a specialist within 2 weeks of an
urgent GP referral (suspected gynaecological cancers)
(Source: Trust inspection data requests DR174 DR175)
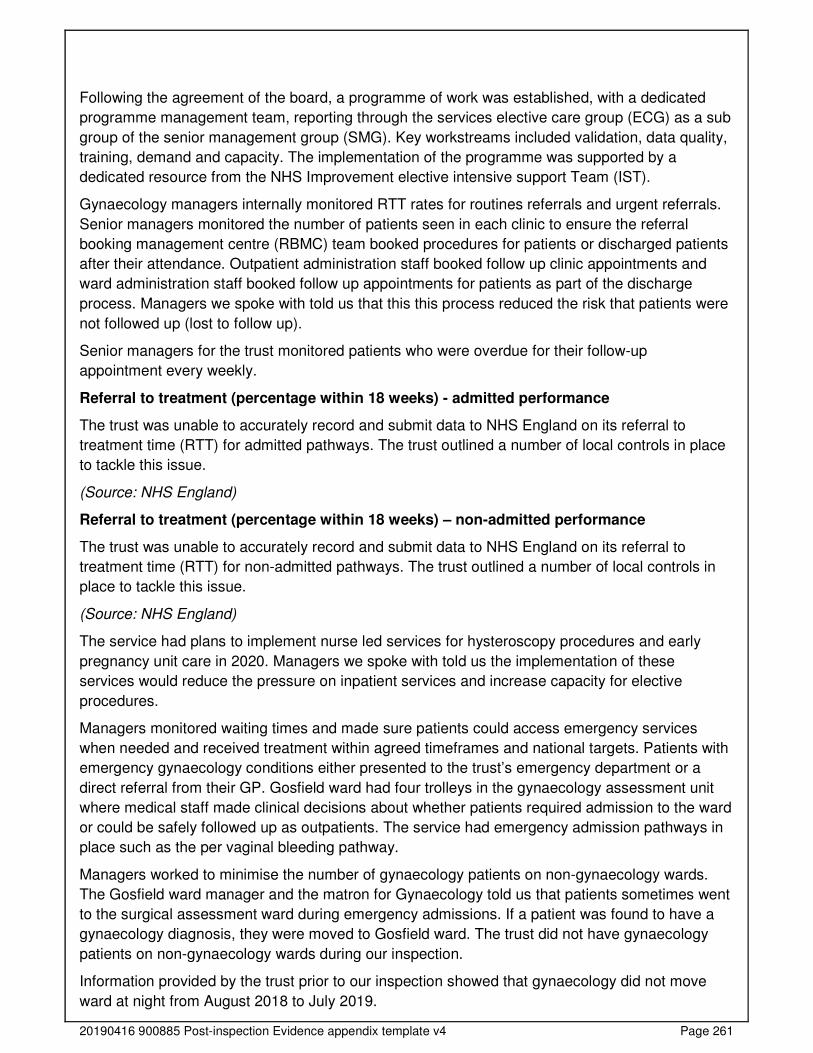
20190416 900885 Post-inspection Evidence appendix template v4 Page 261
Following the agreement of the board, a programme of work was established, with a dedicated
programme management team, reporting through the services elective care group (ECG) as a sub
group of the senior management group (SMG). Key workstreams included validation, data quality,
training, demand and capacity. The implementation of the programme was supported by a
dedicated resource from the NHS Improvement elective intensive support Team (IST).
Gynaecology managers internally monitored RTT rates for routines referrals and urgent referrals.
Senior managers monitored the number of patients seen in each clinic to ensure the referral
booking management centre (RBMC) team booked procedures for patients or discharged patients
after their attendance. Outpatient administration staff booked follow up clinic appointments and
ward administration staff booked follow up appointments for patients as part of the discharge
process. Managers we spoke with told us that this this process reduced the risk that patients were
not followed up (lost to follow up).
Senior managers for the trust monitored patients who were overdue for their follow-up
appointment every weekly.
Referral to treatment (percentage within 18 weeks) - admitted performance
The trust was unable to accurately record and submit data to NHS England on its referral to
treatment time (RTT) for admitted pathways. The trust outlined a number of local controls in place
to tackle this issue.
(Source: NHS England)
Referral to treatment (percentage within 18 weeks) – non-admitted performance
The trust was unable to accurately record and submit data to NHS England on its referral to
treatment time (RTT) for non-admitted pathways. The trust outlined a number of local controls in
place to tackle this issue.
(Source: NHS England)
The service had plans to implement nurse led services for hysteroscopy procedures and early
pregnancy unit care in 2020. Managers we spoke with told us the implementation of these
services would reduce the pressure on inpatient services and increase capacity for elective
procedures.
Managers monitored waiting times and made sure patients could access emergency services
when needed and received treatment within agreed timeframes and national targets. Patients with
emergency gynaecology conditions either presented to the trust’s emergency department or a
direct referral from their GP. Gosfield ward had four trolleys in the gynaecology assessment unit
where medical staff made clinical decisions about whether patients required admission to the ward
or could be safely followed up as outpatients. The service had emergency admission pathways in
place such as the per vaginal bleeding pathway.
Managers worked to minimise the number of gynaecology patients on non-gynaecology wards.
The Gosfield ward manager and the matron for Gynaecology told us that patients sometimes went
to the surgical assessment ward during emergency admissions. If a patient was found to have a
gynaecology diagnosis, they were moved to Gosfield ward. The trust did not have gynaecology
patients on non-gynaecology wards during our inspection.
Information provided by the trust prior to our inspection showed that gynaecology did not move
ward at night from August 2018 to July 2019.
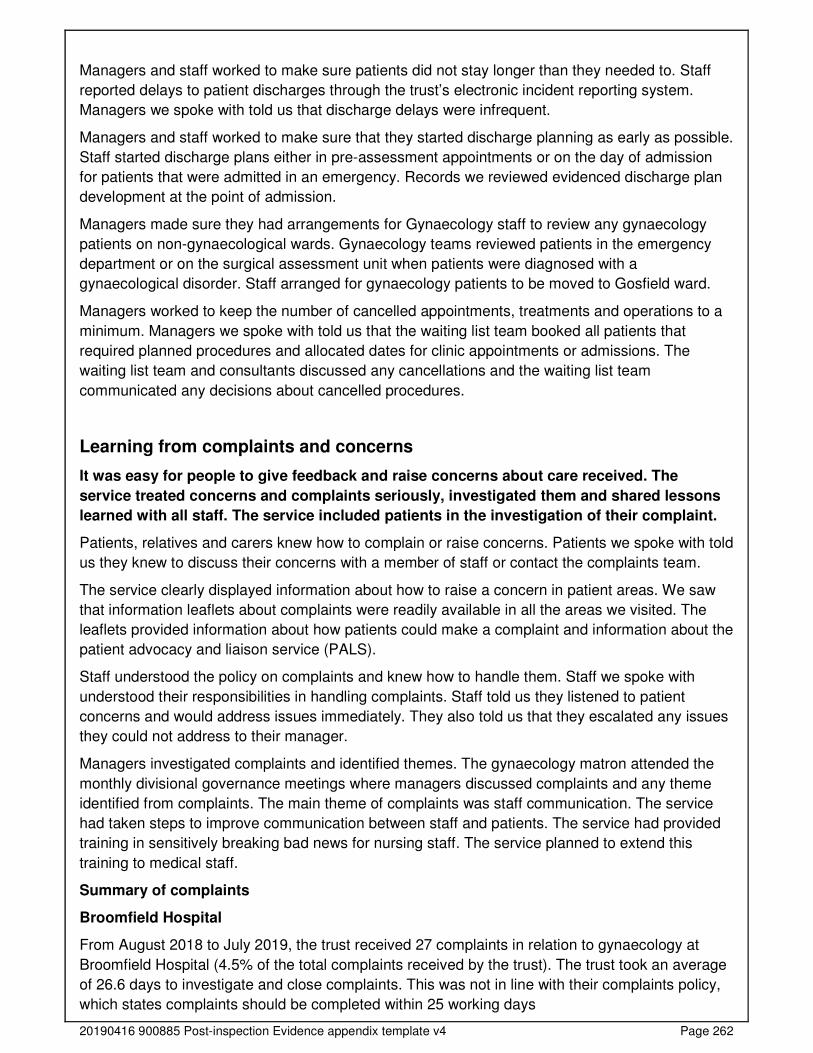
20190416 900885 Post-inspection Evidence appendix template v4 Page 262
Managers and staff worked to make sure patients did not stay longer than they needed to. Staff
reported delays to patient discharges through the trust’s electronic incident reporting system.
Managers we spoke with told us that discharge delays were infrequent.
Managers and staff worked to make sure that they started discharge planning as early as possible.
Staff started discharge plans either in pre-assessment appointments or on the day of admission
for patients that were admitted in an emergency. Records we reviewed evidenced discharge plan
development at the point of admission.
Managers made sure they had arrangements for Gynaecology staff to review any gynaecology
patients on non-gynaecological wards. Gynaecology teams reviewed patients in the emergency
department or on the surgical assessment unit when patients were diagnosed with a
gynaecological disorder. Staff arranged for gynaecology patients to be moved to Gosfield ward.
Managers worked to keep the number of cancelled appointments, treatments and operations to a
minimum. Managers we spoke with told us that the waiting list team booked all patients that
required planned procedures and allocated dates for clinic appointments or admissions. The
waiting list team and consultants discussed any cancellations and the waiting list team
communicated any decisions about cancelled procedures.
Learning from complaints and concerns
It was easy for people to give feedback and raise concerns about care received. The
service treated concerns and complaints seriously, investigated them and shared lessons
learned with all staff. The service included patients in the investigation of their complaint.
Patients, relatives and carers knew how to complain or raise concerns. Patients we spoke with told
us they knew to discuss their concerns with a member of staff or contact the complaints team.
The service clearly displayed information about how to raise a concern in patient areas. We saw
that information leaflets about complaints were readily available in all the areas we visited. The
leaflets provided information about how patients could make a complaint and information about the
patient advocacy and liaison service (PALS).
Staff understood the policy on complaints and knew how to handle them. Staff we spoke with
understood their responsibilities in handling complaints. Staff told us they listened to patient
concerns and would address issues immediately. They also told us that they escalated any issues
they could not address to their manager.
Managers investigated complaints and identified themes. The gynaecology matron attended the
monthly divisional governance meetings where managers discussed complaints and any theme
identified from complaints. The main theme of complaints was staff communication. The service
had taken steps to improve communication between staff and patients. The service had provided
training in sensitively breaking bad news for nursing staff. The service planned to extend this
training to medical staff.
Summary of complaints
Broomfield Hospital
From August 2018 to July 2019, the trust received 27 complaints in relation to gynaecology at
Broomfield Hospital (4.5% of the total complaints received by the trust). The trust took an average
of 26.6 days to investigate and close complaints. This was not in line with their complaints policy,
which states complaints should be completed within 25 working days

20190416 900885 Post-inspection Evidence appendix template v4 Page 263
A breakdown of complaints by type is shown below:
Type of complaint Number of complaints Percentage of total Clinical treatment - obstetrics and gynaecology 24 88.9% Facilities services (including; access for people with a disability, cleanliness, food, parking, maintenance and portering)
1 3.7%
Communications 1 3.7% Clinical treatment - surgical group 1 3.7% Total 27 100.0%
(Source: Routine Provider Information Request (RPIR) – Complaints tab)
Number of compliments made to the trust
Broomfield Hospital
From August 2018 to July 2019 there were 21 compliments received for gynaecology at
Broomfield Hospital (1.9% of all compliments received trust wide). Over half (52.4%) of the
compliments received for gynaecology at Broomfield Hospital related to the gynaecology
outpatients department.
A breakdown of compliments by department at Broomfield Hospital is shown below:
Department Number of compliments Percentage of total Gynaecology outpatients 11 52.4% Gosfield ward 8 38.1% Gynaecology surgery 2 9.5% Total 21 100.0%
The trust stated that most of the compliments received related to overall care along the whole
pathway with patients and relatives thanking staff for their kindness and compassion during
difficult and stressful times. These related to all staff from housekeepers, porters and nurses to
consultants.
Compliments and the associated learning and sharing of good practice was discussed at the
patient and carer experience group and also with individuals and their managers during appraisal.
The trust used its Datix system to analyse themes from compliments.
(Source: Routine Provider Information Request (RPIR) – Compliments tab)
Staff knew how to acknowledge complaints and patients received feedback from managers after
the investigation into their complaint. We reviewed two complaints investigation reports and the
response letters. In both cases the trust apologised about the circumstance of the complaint.
Response letters sent by managers to patients following a complaint evidenced that the patients
had been involved in the complaints process.
Managers shared feedback from complaints with staff and learning was used to improve the
service. The ward manager from Gosfield ward used anonymised complaints for role play learning
on team meeting days. The manager told us that the aim of this learning was to encourage staff to
view events from a patient’s perspective.
Staff we spoke with gave examples of changes to ward processes which were developed following
patient complaints. Staff checked each bed space for hazards following a patient discharge, this
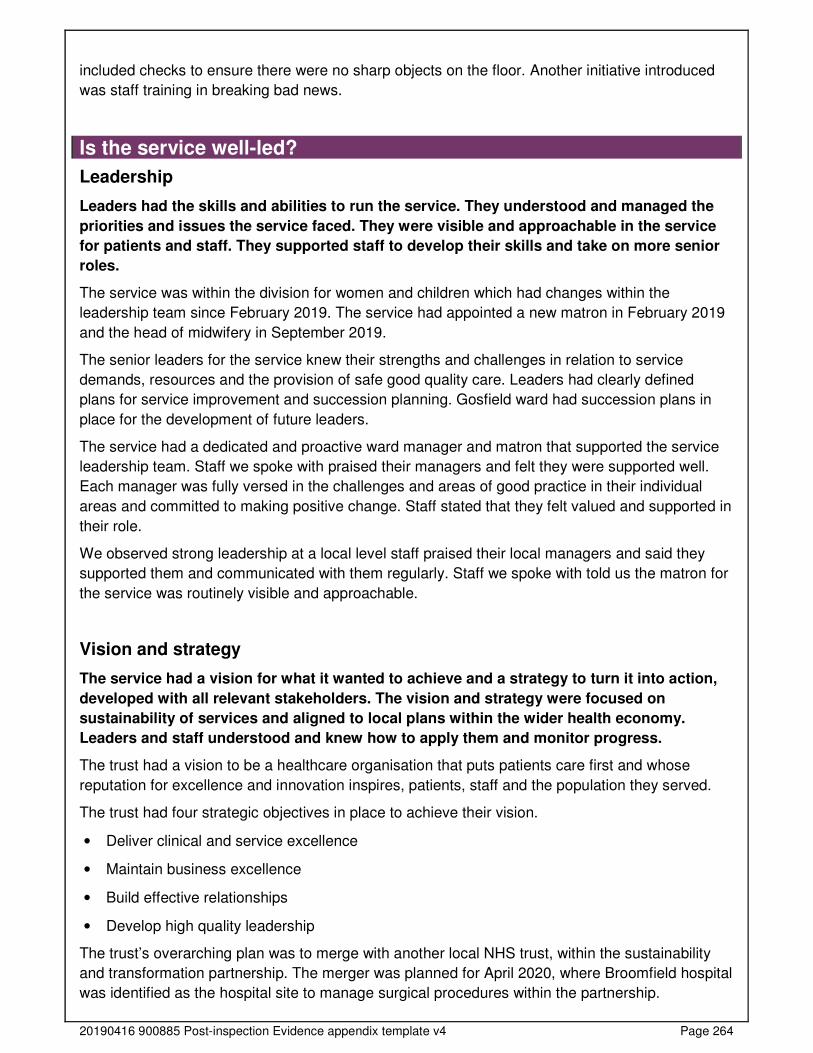
20190416 900885 Post-inspection Evidence appendix template v4 Page 264
included checks to ensure there were no sharp objects on the floor. Another initiative introduced
was staff training in breaking bad news.
Is the service well-led?
Leadership
Leaders had the skills and abilities to run the service. They understood and managed the
priorities and issues the service faced. They were visible and approachable in the service
for patients and staff. They supported staff to develop their skills and take on more senior
roles.
The service was within the division for women and children which had changes within the
leadership team since February 2019. The service had appointed a new matron in February 2019
and the head of midwifery in September 2019.
The senior leaders for the service knew their strengths and challenges in relation to service
demands, resources and the provision of safe good quality care. Leaders had clearly defined
plans for service improvement and succession planning. Gosfield ward had succession plans in
place for the development of future leaders.
The service had a dedicated and proactive ward manager and matron that supported the service
leadership team. Staff we spoke with praised their managers and felt they were supported well.
Each manager was fully versed in the challenges and areas of good practice in their individual
areas and committed to making positive change. Staff stated that they felt valued and supported in
their role.
We observed strong leadership at a local level staff praised their local managers and said they
supported them and communicated with them regularly. Staff we spoke with told us the matron for
the service was routinely visible and approachable.
Vision and strategy
The service had a vision for what it wanted to achieve and a strategy to turn it into action,
developed with all relevant stakeholders. The vision and strategy were focused on
sustainability of services and aligned to local plans within the wider health economy.
Leaders and staff understood and knew how to apply them and monitor progress.
The trust had a vision to be a healthcare organisation that puts patients care first and whose
reputation for excellence and innovation inspires, patients, staff and the population they served.
The trust had four strategic objectives in place to achieve their vision.
• Deliver clinical and service excellence
• Maintain business excellence
• Build effective relationships
• Develop high quality leadership
The trust’s overarching plan was to merge with another local NHS trust, within the sustainability
and transformation partnership. The merger was planned for April 2020, where Broomfield hospital
was identified as the hospital site to manage surgical procedures within the partnership.
20190416 900885 Post-inspection Evidence appendix template v4 Page 265
The service had a vision to expand nurse led pathways for the early pregnancy unit and
hysteroscopy. The leadership team aimed to free consultant capacity to meet referral to treatment
times. Managers of the service had implemented training programmes for staff, this included
nationally recognised external courses in specialist skills such as ultrasound sonography.
The service strategy aligned with the trust’s strategy for the recruitment and retention of staff as
managers had provided opportunities to develop a more diverse skill set and further career
progression within the speciality.
The trust had a shared set of staff values. All staff we spoke knew the trust’s values of ‘we are
kind, professional, positive team’.
Culture
Staff felt respected, supported and valued. They were focused on the needs of patients
receiving care. The service promoted equality and diversity in daily work and provided
opportunities for career development. The service had an open culture where patients, their
families and staff could raise concerns without fear.
Staff reported an open and honest culture and said they felt able to raise any concerns with their
managers. All staff we spoke with confirmed that the needs and experience of their patients was at
the centre of the service. Staff told us they could raise concerns without fear or reprimand and
they were confident action would be taken as a result.
Staff had access to independent freedom to speak up guardians to express any concerns outside
of their immediate teams if they needed to.
Staff we spoke with told us morale was good and staff we spoke with confirmed they felt valued
and well supported by colleagues and managers within their roles. Managers praised staff for their
commitment and team working to meet the needs of patients and the service.
The trust had an active programme of recognition and reward for staff including Star of the Month
and the annual OSCARS.
The trust had the rainbow badge scheme in place to promote inclusion and equity.
Governance
Leaders operated effective governance processes, throughout the service and with partner
organisations. Staff at all levels were clear about their roles and accountabilities and had
regular opportunities to meet, discuss and learn from the performance of the service.
The service set out clear roles, responsibilities, and systems of accountability to support the
governance and management of the service. Staff we spoke with described the service’s
management and governance structure and their specific roles and responsibilities.
The service had data collection processes, which provided the management team with service
level assurance. The gynaecology governance committee was responsible for reviewing clinical
governance information from audits, and safety and quality improvement initiatives. The
gynaecology governance committee reported into their divisional board chaired by the divisional
director. Senior managers discussed the overarching finance, performance, quality and workforce
issues for their division.
20190416 900885 Post-inspection Evidence appendix template v4 Page 266
The divisional board reported to performance, safety and quality reports to the trust board through
sub committees such as performance and accountability meetings, risk and compliance committee
and patient experience committee.
Managers we spoke with told us, there were additional specialty governance meetings across the
division and organisation which provided opportunities for shared learning including the mortality
and morbidity meetings and local audit meetings.
Ward managers for the whole trust met monthly to discuss incidents, learning, key messages and
audit results. This provided peer support and networking opportunities for ward managers.
The Gosfield ward manager shared key messages and safety updates during daily safety briefings
with staff. The briefing sheet was updated weekly to ensure all staff were updated and did not miss
key information. All ward staff were expected to attend ward meetings and update days every two
months. Gosfield had monthly team meetings, the ward Manager had allocated staff into two
teams which attended ward meeting on alternate months. This way of working ensured all staff
had the opportunity to attend the meetings and clinical supervision sessions.
Management of risk, issues and performance
Leaders and teams used systems to manage performance effectively. They identified and
escalated relevant risks and issues and identified actions to reduce their impact. They had
plans to cope with unexpected events. Staff contributed to decision-making to help avoid
financial pressures compromising the quality of care.
The service had clear processes for managing risks issues and performance. The service had an
electronic risk register linked to the incident reporting system. The trust used risk registers based
on the potential consequence of the risk and the likelihood of the risk happening again. The trust
used a red, amber, green risk rating system, to denote the extreme, high, medium and low risk.
Each risk had a rating on entry to the register and a rating once mitigations were in place. All risks
had a review date, a named owner, and an action plan.
The gynaecology service had three risks on their risk register. Each risk entry had a clear
description of the risk and mitigation in place to reduce the impact of the identified risk. There were
regular updates added to the risk register by the risk owner. The service had one risk rated as high
for ultrasound scanning which were not available in the early pregnancy unit on Saturday and
Sunday. Managers had plans in place to mitigate this risk with ultrasound sonography training
secured for nursing staff.
Service leads had identified that colposcopy referral to treatment (RTT) rates were not in line with
national targets due to a high demand for the procedure. They acknowledged that changes to the
cervical screening process had increased urgent referral rates. Managers had implemented extra
clinics to meet the additional demand. Divisional board meeting minutes noted that the trust
performed better than the other trusts in the RTT despite not meeting the national target.
Managers had not included external RTT reporting on the service risk register. However this was
on the trust’s risk register.
Gynaecology service risks were on the women and children’s divisional risk register. Senior
managers discussed the divisional risks within the divisional risk register review meeting. We
reviewed the divisional risk register review action log from October 2019 which evidenced all risks
were reviewed and discussed. The action log also evidenced that risk closed appropriately, for
20190416 900885 Post-inspection Evidence appendix template v4 Page 267
example, managers had closed the risk for Gosfield ward staffing as the ward was fully
established.
Wards and clinical areas did not hold an individual risk register, all risks were held on a service
wide risk register. Ward managers took ownership of risks directly related to their area of
responsibility, they monitored risks and discussed risk mitigation actions taken with their
managers.
Managers made sure staff knew the risks for the gynaecology service. We saw posters displayed
in staff rooms in all clinical areas we visited. The poster’s provided information about the top three
risks and what action managers had taken to reduce the impact of the risk. Managers we spoke
with told us that it was important that staff knew and understood the service risks, to encourage
team ownership and team working to address the risks.
The division board monitored the performance of the service against key local safety and quality
safety measures. We reviewed the division board meeting minutes from July 2019 to October
2019 which showed managers had discussed areas such as staffing, mandatory training
compliance and incidents. The gynaecology service had a risk summit in September 2019 which
identified areas for improvement within the service. Managers had action plans in place to address
issues identified such as the availability of ultrasound scans at weekend in the early pregnancy
unit staff recruitment.
Information management
The service collected reliable data and analysed it. Staff could find the data they needed, in
easily accessible formats, to understand performance, make decisions and improvements.
The information systems were integrated and secure. Although the trust did not submit
data against national treatment targets.
In May 2017, a new electronic patient record system led to problems with accurately tracking
patients and capturing validated accurate referral to treatment (RTT) data. At the time of our
inspection, RTT formal data submission was not taking place (ceased in January 2018 with the
support from NHS England), however, the trust had implemented a number of local measures to
monitor RTT times. All patients who did not meet RTT were reviewed for harm.
Staff across the trust accessed information from the trust intranet which included policies and
national guidance. Staff knew how to access information through the intranet in each of the areas
we visited.
The service used both paper and electronic patient records. Care planning, records of care and
medicine prescriptions were hand written in paper records, the patient admission discharge
system were electronic. Staff had access to up-to-date, accurate, and comprehensive information
about their patients’ care and treatment. They knew how to use and store confidential information.
Staff kept paper records in locked trolleys within staff areas, to prevent visitor and members of the
public access to confidential information. Electronic records were secured through individual login
and passwords.
The service had arrangements in place which ensured data was submitted to external
organisations as required for example, serious incidents and never events.
Engagement
20190416 900885 Post-inspection Evidence appendix template v4 Page 268
Leaders and staff actively and openly engaged with patients, staff, equality groups, the
public and local organisations to plan and manage services. They collaborated with partner
organisations to help improve services for patients.
Staff had opportunities to engage at work through a range of team meetings and wider trust wide
meetings. The senior leadership team for the trust held daily ‘Moving Forward @ Mid’ meetings to
update staff with what was happening within the trust. Staff could attend these meetings from
Monday to Friday which brought corporate, clinical and non-clinical staff together.
Managers shared information about service performance on wall displays in the staff rooms of all
clinical areas we visited. Staff also received key messages and safety updates during the daily
safety briefing on Gosfield ward.
The trust participated in the NHS staff survey. The 2018 staff survey showed 67% of staff felt
supported by their immediate manager and 67% of staff felt managers were invested in their
health and wellbeing, and the hospital took positive action in this area.
Divisional managers had regular engagement with other stakeholders in the local sustainability
and transformation partnership. Stakeholders included service commissioners, partner
organisations such as termination pregnancy services, community services and GPs, who worked
collaborative to provide patient care.
The service actively sought feedback from their patients to improve the quality and safety of care
provided. Patients could provide their feedback through the NHS friends and family test or through
the patient advocacy and liaison service. Managers used feedback during clinical supervision
sessions for staff learning.
Gynaecology services had links with patient support services such as counselling and support
groups for both patients and their relatives.
Learning, continuous improvement and innovation
All staff were committed to continually learning and improving services. They had a good
understanding of quality improvement methods and the skills to use them. Leaders
encouraged innovation and participation in research.
The service had undertaken a risk summit of gynaecology services to identify areas of the service
which required improvement in service provision and delivery. The service leads had actions in
place to improve these areas of the service.
The ward manager on Gosfield ward had developed monthly team meeting and clinical
supervision shifts. The ward had two teams which alternated so that all staff attended a team
meeting shift every two months. The organisation of this style of team meetings had improved staff
compliance with mandatory training, clinical supervision and enabled managers to complete staff
appraisals.
Gynaecology had a nurse-led colposcopy service and had plans to increase nurse-led pathways to
include hysteroscopy and the early pregnancy unit. Managers had booked specialist training
courses for staff in specialist skill such as ultrasound sonography.
20190416 900885 Post-inspection Evidence appendix template v4 Page 269
Outpatients
Facts and data about this service
Outpatient services at Mid Essex Hospital Services NHS Trust cover multiple sites including:
Broomfield Hospital, St Peter’s Hospital, St Michael’s Hospital and Braintree Community Hospital.
The main outpatient area of Broomfield Hospital is located in the atrium. This was purpose-built
and opened in 2010 with interactive self check-in kiosks throughout and a co-located pharmacy.
There is also an information pod which opened in 2013 for cancer and other life limiting illnesses.
This is delivered in collaboration with Macmillan and Farleigh Hospice.
The remainder of the outpatient services are located in the older part of the building. The trust
covers a wide range of specialities such as ophthalmology, musculoskeletal, surgical and medical,
in addition to the St Andrew’s burns and plastics regional unit at Broomfield hospital.
The trust had over 600,000 outpatient attendances from April 2018 to March 2019, with the
majority undertaken at the Broomfield Hospital site. Outpatient appointments are available Monday
to Friday between 8.30am and 5.00pm with regular evening and weekend clinics.
The trust is delivering a transformation programme to streamline patient pathways, reduce the
number of follow-up appointments and improve the patient experience.
(Source: Routine Provider Information Request (RPIR) – Acute context)
During our inspection, we visited the outpatient department located at Broomfield Hospital. We
inspected and observed areas across main outpatients including; gynaecology, ophthalmology,
ear, nose and throat (ENT), phlebotomy, booking team and the St Andrews burns and plastics
centre.
In addition to consultant-led clinics, there are nurse-led clinics across a range of specialities. We
spoke with patients, relatives, and members of staff. During our inspection we spoke with 32
members of staff including; nurses, healthcare assistants, receptionist staff, medical staff, service
managers, bookings team administration assistants, and directors of nursing.
We observed interactions between patients and staff and considered the environment. We also
reviewed national data and performance information about the trust, and a range of policies,
procedures and other documents relating to the operation of the outpatient department.
The service was last inspected in September 2018, where safe, responsive and well-led were
rated as requires improvement and caring was rated as good. We do not rate effective for
outpatients. This led to an overall rating of requires improvement.
Total number of first and follow up appointments compared to England
The trust had 528,816 first and follow up outpatient appointments from March 2018 to February
2019. The graph below represents how this compares to other trusts.
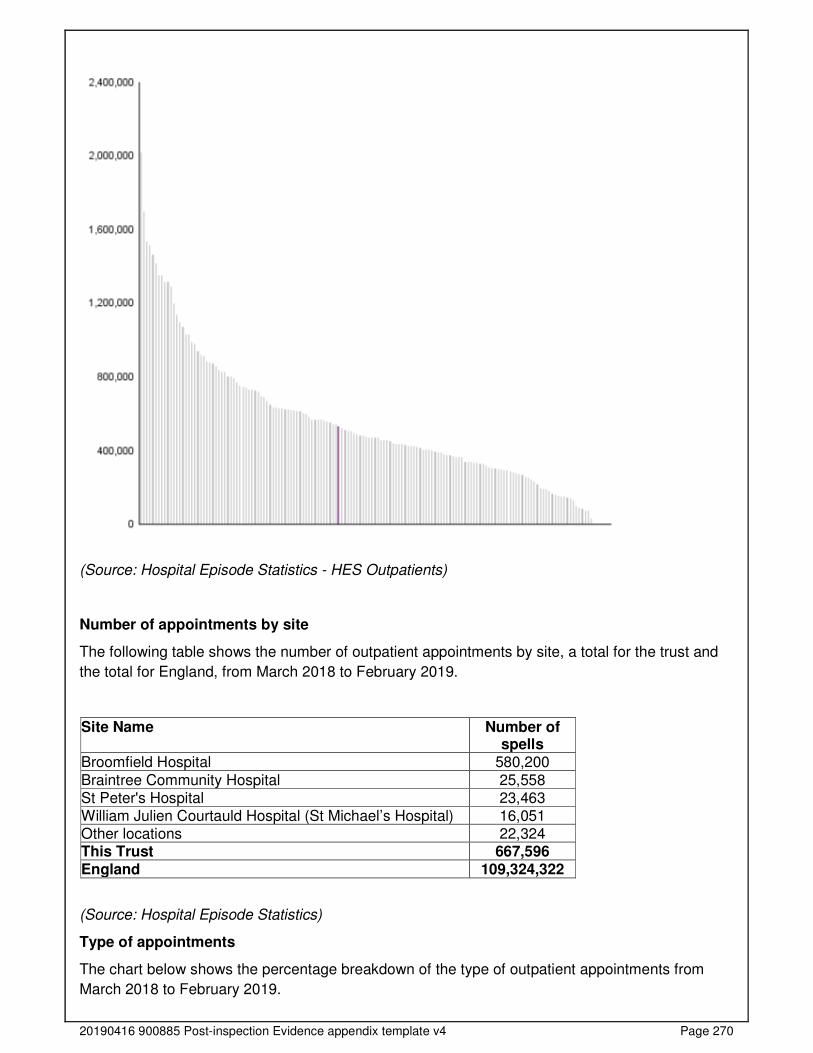
20190416 900885 Post-inspection Evidence appendix template v4 Page 270
(Source: Hospital Episode Statistics - HES Outpatients)
Number of appointments by site
The following table shows the number of outpatient appointments by site, a total for the trust and
the total for England, from March 2018 to February 2019.
Site Name Number of spells
Broomfield Hospital 580,200
Braintree Community Hospital 25,558 St Peter's Hospital 23,463 William Julien Courtauld Hospital (St Michael’s Hospital) 16,051 Other locations 22,324 This Trust 667,596 England 109,324,322
(Source: Hospital Episode Statistics)
Type of appointments
The chart below shows the percentage breakdown of the type of outpatient appointments from
March 2018 to February 2019.
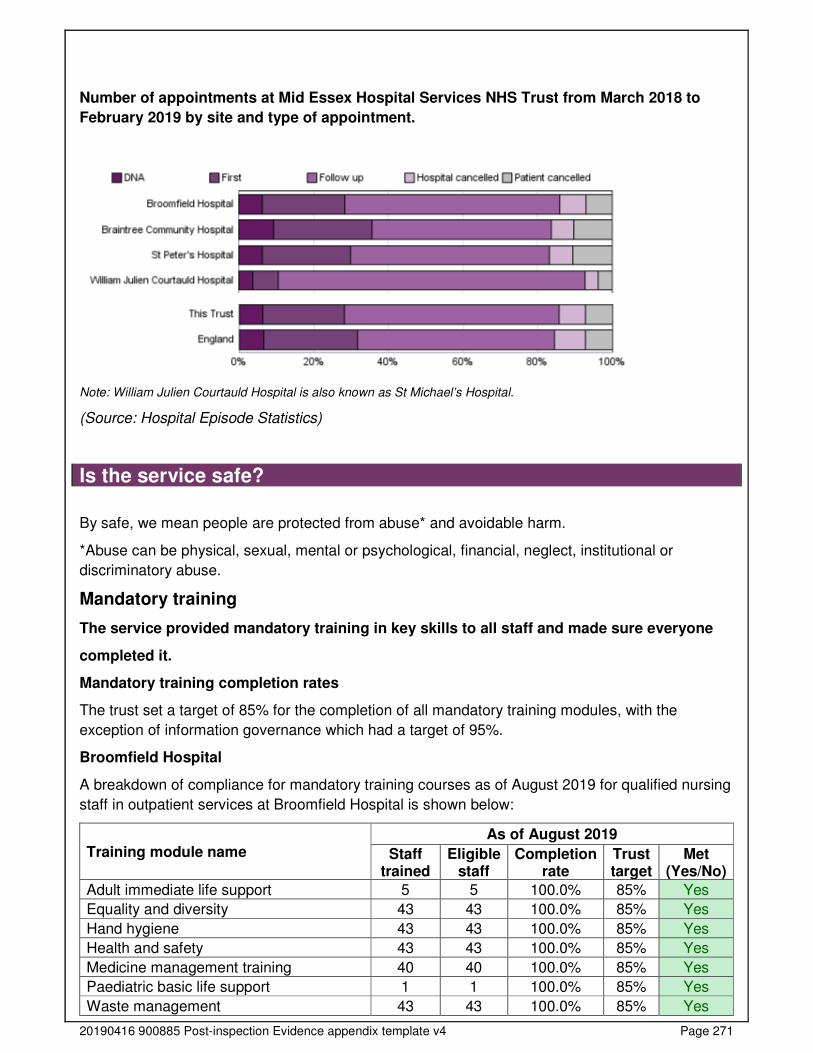
20190416 900885 Post-inspection Evidence appendix template v4 Page 271
Number of appointments at Mid Essex Hospital Services NHS Trust from March 2018 to
February 2019 by site and type of appointment.
Note: William Julien Courtauld Hospital is also known as St Michael’s Hospital.
(Source: Hospital Episode Statistics)
Is the service safe?
By safe, we mean people are protected from abuse* and avoidable harm.
*Abuse can be physical, sexual, mental or psychological, financial, neglect, institutional or
discriminatory abuse.
Mandatory training
The service provided mandatory training in key skills to all staff and made sure everyone
completed it.
Mandatory training completion rates
The trust set a target of 85% for the completion of all mandatory training modules, with the
exception of information governance which had a target of 95%.
Broomfield Hospital
A breakdown of compliance for mandatory training courses as of August 2019 for qualified nursing
staff in outpatient services at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Adult immediate life support 5 5 100.0% 85% Yes
Equality and diversity 43 43 100.0% 85% Yes
Hand hygiene 43 43 100.0% 85% Yes
Health and safety 43 43 100.0% 85% Yes
Medicine management training 40 40 100.0% 85% Yes
Paediatric basic life support 1 1 100.0% 85% Yes
Waste management 43 43 100.0% 85% Yes
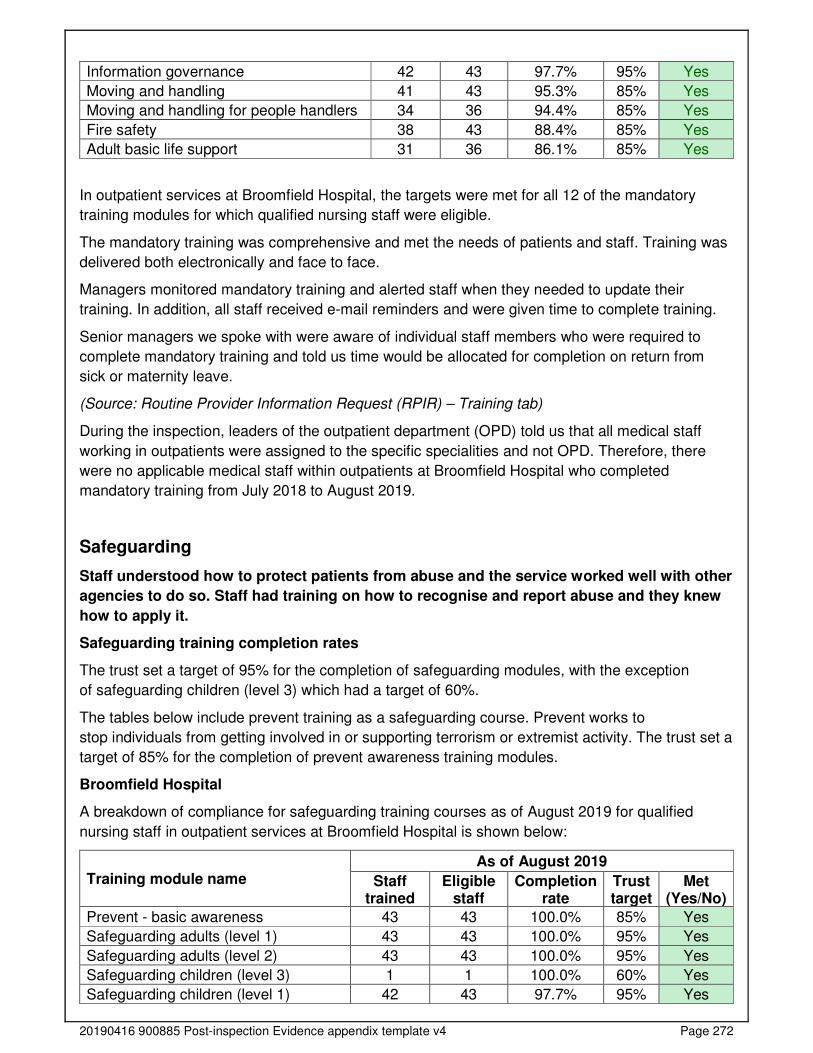
20190416 900885 Post-inspection Evidence appendix template v4 Page 272
Information governance 42 43 97.7% 95% Yes
Moving and handling 41 43 95.3% 85% Yes
Moving and handling for people handlers 34 36 94.4% 85% Yes
Fire safety 38 43 88.4% 85% Yes
Adult basic life support 31 36 86.1% 85% Yes
In outpatient services at Broomfield Hospital, the targets were met for all 12 of the mandatory
training modules for which qualified nursing staff were eligible.
The mandatory training was comprehensive and met the needs of patients and staff. Training was
delivered both electronically and face to face.
Managers monitored mandatory training and alerted staff when they needed to update their
training. In addition, all staff received e-mail reminders and were given time to complete training.
Senior managers we spoke with were aware of individual staff members who were required to
complete mandatory training and told us time would be allocated for completion on return from
sick or maternity leave.
(Source: Routine Provider Information Request (RPIR) – Training tab)
During the inspection, leaders of the outpatient department (OPD) told us that all medical staff
working in outpatients were assigned to the specific specialities and not OPD. Therefore, there
were no applicable medical staff within outpatients at Broomfield Hospital who completed
mandatory training from July 2018 to August 2019.
Safeguarding
Staff understood how to protect patients from abuse and the service worked well with other
agencies to do so. Staff had training on how to recognise and report abuse and they knew
how to apply it.
Safeguarding training completion rates
The trust set a target of 95% for the completion of safeguarding modules, with the exception
of safeguarding children (level 3) which had a target of 60%.
The tables below include prevent training as a safeguarding course. Prevent works to
stop individuals from getting involved in or supporting terrorism or extremist activity. The trust set a
target of 85% for the completion of prevent awareness training modules.
Broomfield Hospital
A breakdown of compliance for safeguarding training courses as of August 2019 for qualified
nursing staff in outpatient services at Broomfield Hospital is shown below:
Training module name As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Prevent - basic awareness 43 43 100.0% 85% Yes
Safeguarding adults (level 1) 43 43 100.0% 95% Yes
Safeguarding adults (level 2) 43 43 100.0% 95% Yes
Safeguarding children (level 3) 1 1 100.0% 60% Yes
Safeguarding children (level 1) 42 43 97.7% 95% Yes
20190416 900885 Post-inspection Evidence appendix template v4 Page 273
Safeguarding children (level 2) 42 43 97.7% 95% Yes
In outpatient services the targets were met for all six safeguarding training modules for which
qualified nursing staff at Broomfield Hospital were eligible.
(Source: Routine Provider Information Request (RPIR) – Training tab)
During the inspection, leaders of the outpatient department (OPD) told us that all medical staff
working in outpatients were assigned to the specific specialities and not OPD. Therefore, there
were no applicable medical staff within outpatients at Broomfield Hospital who completed
safeguarding training from July 2018 to August 2019.
Outpatient department staff received training on level 1 and level 2 safeguarding modules,
however this did not meet recommendations of the Safeguarding Children and Young People:
Roles and Competencies for Healthcare Staff Fourth edition: January 2019 Intercollegiate
document which states that all clinical staff working with children, young people and/or their
parents/carers and/or must be trained to level three.
We raised this during our inspection with department senior staff who were reviewing children
safeguarding training trust wide.
Safeguarding policies and procedures were available for staff to access electronically and we saw
posters in place across the outpatient departments, providing information on who to contact, staff
responsibilities and a flowchart detailing safeguarding principles.
Staff we spoke with knew how to make a safeguarding referral and who to inform if they had
concerns. The names and contact details of the safeguarding team were displayed in the staff
room and staff confirmed that the safeguarding team were responsive and provided support when
needed.
Staff we spoke to knew how to identify adults and children at risk of, or suffering, significant harm
and worked with other agencies to protect them.
Staff followed safe procedures for children visiting the service /department. The trauma and
orthopaedic outpatients held specific clinics for children twice weekly. Similarly, ophthalmology
had clinics led by a children’s nurse with the level three of safeguarding training.
Cleanliness, infection control and hygiene
The service mostly controlled infection risk well. Staff generally kept themselves,
equipment and the premises visibly clean. They used control measures to prevent the
spread of infection.
Most clinical areas were clean and had suitable furnishings which were clean and well-maintained.
Each outpatient area displayed the cleaning schedule for the month on the wall. The schedules
had signatures against the daily cleaning performed. Most areas we visited used ‘I am clean’
stickers to indicate that equipment and rooms had been cleaned. However, in the chemotherapy
day unit staff did not routinely label equipment with ‘I am clean’ stickers. Staff confirmed that they
cleaned equipment after patient contact but did not label equipment to show when it was last
cleaned. This meant it was not clear which pieces of equipment had been cleaned and were ready
for use.
20190416 900885 Post-inspection Evidence appendix template v4 Page 274
We saw an area used for the lung function test in the main outpatients which was not visibly clean
with the lung function equipment covered in dust. We highlighted this to the staff present and on
our unannounced inspection 20 November 2019 we found the equipment was visibly clean.
In the chemotherapy unit, the area where chemotherapy drugs were prepared appeared to be an
office and storage area and not a formal clinical treatment room. The work surfaces where the
drugs were being prepared were cluttered with consumables and we were concerned regarding
infection prevention control in this area. We escalated our concerns to the senior leadership team.
Hand sanitiser was generally available throughout the departments. We saw posters displaying
the five moments of hand hygiene near handwashing facilities.
Staff used personal protective equipment (PPE). We observed staff were bare below the elbows
and used gloves and aprons where indicated and washed their hands between patient contacts.
All clinic rooms had disposable aprons, gloves in various sizes, hand washing facilities including
filled soap dispensers, paper towels, disposable bed sheets, hand sanitiser, and clinical waste
disposal.
Staff in the ear, nose and throat (ENT) clinics cleaned naso-endoscopes using the three-wipe
system between patients before sending to the decontamination unit at the end of clinics.
Infection prevention and control was monitored by senior staff and the audit results reported
monthly. We viewed the audit reports from January to June 2019 for general outpatients,
ophthalmology and St Andrews burns OPD clinic and saw that the hand hygiene compliance was
100%.
Environment and equipment
The design, maintenance and use of facilities, premises and equipment did not always keep
people safe. Staff managed clinical waste well.
The outpatient service generally had suitable facilities to meet the needs of patient’s and their
families. The outpatient clinics were well signposted. The majority of clinics took place in the main
outpatients department, some clinics were spread throughout the hospital in different departments.
The chemotherapy day unit had its own reception and waiting area. The treatment area was
designed 10 years ago to treat 14 patients simultaneously, on 12 chairs and two beds. However,
due to high demand for the service, the service now treated 30 patients simultaneously. At the
time of our inspection the treatment room was very busy. There was very limited space between
patients, no screens to maintain patient privacy and dignity and in an emergency, there was
limited space for the emergency trolley. Staff told us in an emergency they would have to move
the patient safely to the middle of the room, and put a screen around the patient. We escalated our
concerns with the overcrowded area with the senior leadership team, they acknowledged the issue
and had already put a protocol in place to ensure patient’s safety, should a patient require
emergency support following a hypersensitivity or anaphylaxis reaction to their treatment.
Each outpatient clinic area had its own reception and waiting area. On occasions some clinic
areas could become overcrowded and did not always have enough space to seat all patients and
their families/carers. During the inspection, we observed the waiting area for the phlebotomy clinic
and the eye clinic were overcrowded during busy periods.
The service had enough suitable equipment to help them to safely care for patients. We saw that
equipment was stored appropriately and neatly. Consumable items, for example, dressings were
20190416 900885 Post-inspection Evidence appendix template v4 Page 275
stored in cupboards and drawers. We randomly checked a number of consumable items and were
within date. We checked a number of electrical equipment and all had evidence of electrical safety
testing and maintenance testing.
There were processes in place to ensure that equipment was maintained and serviced.
Equipment servicing, and repairs were undertaken by the trust’s clinical engineering department,
who were responsible for monitoring when equipment was due for servicing. Staff could contact
the department to highlight concerns about any items of equipment and told us that they were
responsive.
During our inspection we checked resuscitation equipment in all the outpatient areas we visited.
Resuscitation trolleys or emergency grab bags were easily accessible and locked with anti-tamper
tags. We reviewed resuscitation trolley records and saw that daily checks and weekly checks were
completed from August to November 2019. This showed a consistent and regular approach to
safety checks.
Staff disposed of clinical waste safely. The trust had a waste segregation system in place and we
found separate bins and bags in place throughout outpatient clinics. Staff disposed waste correctly
and followed the trust’s policy. Sharps bins were correctly assembled dated and labelled and not
overfilled. The outpatient departments stored control of substances hazardous to health (COSHH)
materials correctly in locked cupboards which ensured patients and the public could not access
substance.
Assessing and responding to patient risk
Staff completed and updated risk assessments for each patient and identified and quickly
acted upon patients at risk of deterioration.
A policy was in place to identify deteriorating patients. Staff we spoke with told us that they
responded promptly a patient suddenly deteriorated. As per trust policy, outpatient staff told us
they would call the trust’s resuscitation team to any patient or relative who collapsed or escort
them to the emergency department if appropriate. Medical staff arranged admission for patients if
required.
Each clinic room had an emergency call bell to summon assistance if needed in an emergency
situation.
Staff completed risk assessments for each patient on arrival where appropriate and used
recognised tools.
Staff were trained to provide life support to patients. This ranged from basic life support and
immediate life support for adults and children, depending upon staff grade. Out of the 36 staff in
the main outpatients 31 (86.1%) had an up to date basic life support training. In addition, five
senior members of staff in the main outpatients had an up to date immediate life support training.
Staff knew how to deal with any specific risk issues. For example, staff told us that if a patient was
known to have an infectious disease, to minimise infection risk to others attending clinic, they
would be treated in a separate room preferably at the end of clinic
Systems and process were in place to ensure patients with urgent clinical needs were seen in a
timely manner. Staff tracked referrals through the electronic patient information management
system. Referrals were triaged by the outpatient appointment booking team and this was overseen
by the outpatient bookings manager.
20190416 900885 Post-inspection Evidence appendix template v4 Page 276
Staff shared key information to keep patients safe when handing over their care to others. We saw
clinic staff completing routine assessments for patients attending clinics, including blood pressure,
pulse, and weight. Staff reported abnormal results to the consulting clinician, details were also
included in letters sent to the patients GP for monitoring and follow up as required.
A modified ‘World Health Organisation (WHO) five steps to safer surgery checklist’ was used in
the procedure rooms for invasive procedures. We reviewed four checklists used in the eye
treatment unit and two for dermatology procedures, all six checklists were completed appropriately
as per trust policy and procedures. The outpatient service audited the WHO checklists every six
months.
Nurse staffing
The service had enough nursing staff with the right qualifications, skills, training and
experience to keep patients safe from avoidable harm and to provide the right care and
treatment. Managers regularly reviewed staffing levels and skill mix, and gave bank and
agency staff a full induction.
Broomfield Hospital
The table below shows a summary of the nursing staffing metrics within outpatient services at
Broomfield Hospital compared to the trust’s targets, where applicable:
Outpatients annual staffing metrics
August 2018 to July 2019 July 2018 to June
2019 August 2018 to July 2019
Staff Group
Annual average establishment
Annual vacancy
rate
Annual turnover
rate
Annual sickness
rate
Annual bank
hours (% of
available hours)
Annual agency
hours (% of
available hours)
Annual unfilled
hours (% of
available hours)
Target 13% 12% 3.8% All staff 134 19% 5% 5.6% Qualified nurses
45 30% 0% 4.2% 2,457 (3%) 0
(0%) 38,365 (44%)
(Source: Routine Provider Information Request (RPIR) – Vacancy, Turnover, Sickness and
Nursing bank agency tabs)
Nurse staffing rates within outpatient services were analysed for the past 12 months and no
indications of improvement, deterioration or change were identified in monthly rates for turnover.
The trust reported that no agency staff were used in outpatients at Broomfield Hospital from
August 2018 to July 2019.
At the time of inspection, the service leads provided us with updated information regarding
staffing. Qualified nursing establishment was 12.1 whole time equivalent (WTE) and data from
November 2019 showed actual staffing was 9.09 WTE. The vacancy was for band 5 registered
nurses and the OPD matron told us that interviews were scheduled for later on in November.
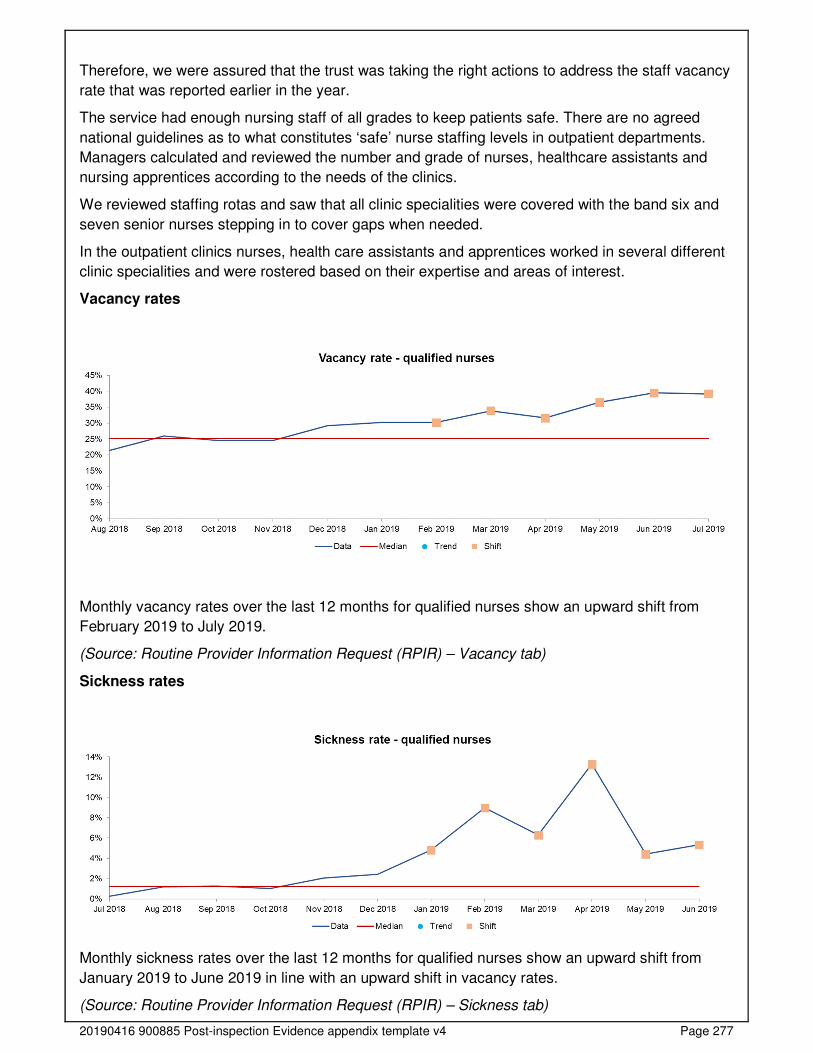
20190416 900885 Post-inspection Evidence appendix template v4 Page 277
Therefore, we were assured that the trust was taking the right actions to address the staff vacancy
rate that was reported earlier in the year.
The service had enough nursing staff of all grades to keep patients safe. There are no agreed
national guidelines as to what constitutes ‘safe’ nurse staffing levels in outpatient departments.
Managers calculated and reviewed the number and grade of nurses, healthcare assistants and
nursing apprentices according to the needs of the clinics.
We reviewed staffing rotas and saw that all clinic specialities were covered with the band six and
seven senior nurses stepping in to cover gaps when needed.
In the outpatient clinics nurses, health care assistants and apprentices worked in several different
clinic specialities and were rostered based on their expertise and areas of interest.
Vacancy rates
Monthly vacancy rates over the last 12 months for qualified nurses show an upward shift from
February 2019 to July 2019.
(Source: Routine Provider Information Request (RPIR) – Vacancy tab)
Sickness rates
Monthly sickness rates over the last 12 months for qualified nurses show an upward shift from
January 2019 to June 2019 in line with an upward shift in vacancy rates.
(Source: Routine Provider Information Request (RPIR) – Sickness tab)
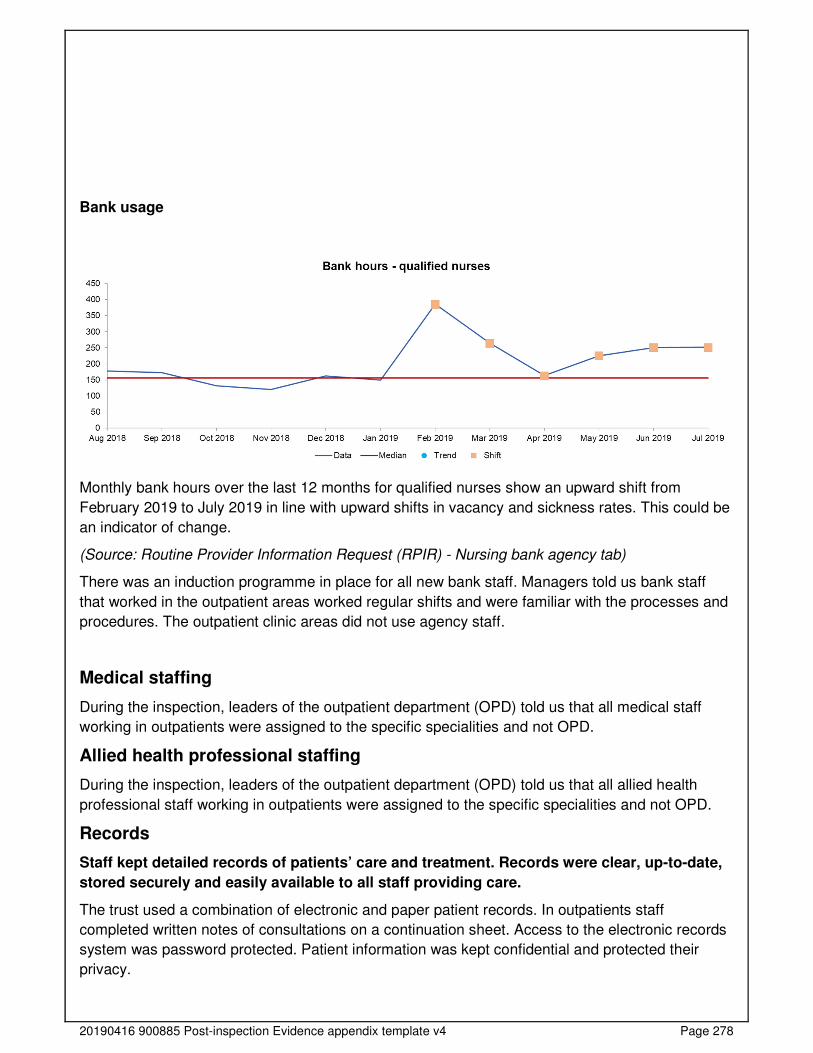
20190416 900885 Post-inspection Evidence appendix template v4 Page 278
Bank usage
Monthly bank hours over the last 12 months for qualified nurses show an upward shift from
February 2019 to July 2019 in line with upward shifts in vacancy and sickness rates. This could be
an indicator of change.
(Source: Routine Provider Information Request (RPIR) - Nursing bank agency tab)
There was an induction programme in place for all new bank staff. Managers told us bank staff
that worked in the outpatient areas worked regular shifts and were familiar with the processes and
procedures. The outpatient clinic areas did not use agency staff.
Medical staffing
During the inspection, leaders of the outpatient department (OPD) told us that all medical staff
working in outpatients were assigned to the specific specialities and not OPD.
Allied health professional staffing
During the inspection, leaders of the outpatient department (OPD) told us that all allied health
professional staff working in outpatients were assigned to the specific specialities and not OPD.
Records
Staff kept detailed records of patients’ care and treatment. Records were clear, up-to-date,
stored securely and easily available to all staff providing care.
The trust used a combination of electronic and paper patient records. In outpatients staff
completed written notes of consultations on a continuation sheet. Access to the electronic records
system was password protected. Patient information was kept confidential and protected their
privacy.
20190416 900885 Post-inspection Evidence appendix template v4 Page 279
We reviewed 10 sets of patient records including electronic records and found that the records
were legible, signed and dated. Results from pathology and diagnostic imaging were available
electronically meaning staff could readily access to up to date results.
Staff told us when patients transferred to a new team, there were no delays in accessing their
records.
Medicines
The service used systems and processes to safely prescribe, administer, record and store
medicines.
Staff in the outpatient clinics stored medicines securely in locked cupboards in key coded locked
clinical rooms. We reviewed two medicines cupboards and had no concerns regarding medicines
storage in these areas. We looked at 15 medicines and saw that they were within their use by
date. Staff consistently recorded maximum / minimum temperatures on medicines fridges and
ambient room temperatures of clinical rooms where medication was stored.
Controlled drugs (CDs) were not stored in outpatient clinics. Controlled drugs are prescription
medicines that are controlled under the Misuse of Drugs legislation (and subsequent
amendments).
The outpatient clinics did not regularly use external (FP10) prescriptions. In exceptional
circumstances when FP10 prescriptions had to be used, the trust had clear processes and
procedures in place. When an FP10 was used the prescription number was recorded and
reconciled in the trust pharmacy. An FP10 is an external green prescription that can be dispensed
by a high street pharmacy as well as the hospital pharmacy.
In the eye clinic, staff used patient group directives (PGDs) for some medications. PGDs provided
a legal framework which allowed some registered health professionals to supply and/or administer
specified medicines, such as painkillers, to a predefined group of patients without them having to
see a doctor. We reviewed the PGDs used in the eye clinic and saw that they were within date and
were signed off by both a doctor and a pharmacist.
Incidents
The service managed patient safety incidents well. Staff recognised incidents and near
misses and reported them appropriately. Managers investigated incidents and shared
lessons learned with the whole team and the wider service. When things went wrong, staff
apologised and gave patients honest information and suitable support. Managers ensured
that actions from patient safety alerts were implemented and monitored.
From June to November 2019, the OPD reported 112 incidents. Of these 15 were recorded as
near miss, eight as low harm and 89 as no harm. The most common reported incident was to do
with administrative/clerical, followed by delay/failure to treatment or procedure and data quality.
Staff reported all incidents that they should report. Staff we spoke with knew what incidents to
report and how to report them on the trust’s electronic reporting system. They gave us examples
of when they had reported incidents and were satisfied that they had a good understanding of
what incidents should be reported and how to report.
20190416 900885 Post-inspection Evidence appendix template v4 Page 280
Staff understood their responsibility to raise concerns, to record safety incidents, concerns and
near misses.
Outcomes from incidents and associated trends and themes were communicated to staff face to
face by the senior nurses. The outpatient teams held daily safety huddles, learning from incidents
was shared.
All action plans from incidents were monitored through the relevant business unit meetings and
reported to the quality and risk management group.
Managers investigated incidents thoroughly. Patients and their families were involved in these
investigations. We reviewed four recently reported and investigated incidents which showed
detailed description of incident, actions taken and recommendation for lessons learnt.
Staff received feedback from investigation of incidents. Staff told us that they received feedback
after reporting an incident. There were processes to share learning from incidents which included;
staff meetings, emails and notices to ensure that action was taken to improve safety.
Never Events
Never events are serious patient safety incidents that should not happen if healthcare providers
follow national guidance on how to prevent them. Each never event type has the potential to cause
serious patient harm or death but neither need have happened for an incident to be a never event.
From August 2018 to August 2019, the trust did not report any never events for outpatient
services.
(Source: Strategic Executive Information System (STEIS))
Breakdown of serious incidents reported to STEIS
In accordance with the Serious Incident Framework 2015, the trust reported two serious incidents
(SIs) in outpatient services which met the reporting criteria set by NHS England from August 2018
to August 2019. This represented 1.6% of all serious incidents reported by the trust as a whole.
Both of the incidents occurred at Broomfield Hospital.
One serious incident reported in outpatient services related to a diagnostic incident including delay
meeting SI criteria (including failure to act on test results) and occurred in September 2017. The
other incident which occurred in July 2017 was still pending review at the time of data submission.
(Source: Strategic Executive Information System (STEIS)
Staff understood the duty of candour. They were open and transparent and gave patients and
families a full explanation when things went wrong. Duty of candour is a regulatory duty under the
Health and Social Care Act (Regulated Activities Regulations) 2014 that relates to openness and
transparency and requires providers of health and social care services to notify patients (or other
relevant persons) of certain ‘notifiable safety incidents’ and provide reasonable support to that
person.
Is the service effective?
Evidence-based care and treatment
20190416 900885 Post-inspection Evidence appendix template v4 Page 281
The service provided care and treatment based on national guidance and evidence-based
practice. Managers checked to make sure staff followed guidance. Staff protected the
rights of patients subject to the Mental Health Act 1983.
The service followed up to date policies and staff delivered care according to best practice and
national guidance. Staff accessed a range of guidelines through the trust intranet. Staff we spoke
with said that it was easy to access the information.
We reviewed several guidelines and found they followed National Institute for Health and Care
Excellence (NICE) best practice where relevant. For example; breast care services clinical
operational policy, which referred to Improving Outcomes in Breast Cancer –NICE health &
wellbeing guidance (CSG1) and the diabetes care clinical operational policy which referred to the
Type 2 diabetes in adults: management (2015) NICE guideline (NG28).
Staff had access to a range of information which was displayed on staff notice boards in the staff
room and in the sister’s office. For example, in the staff area of the fracture clinic, we saw
information on safeguarding and wound care.
The outpatient department did not have an overall audit plan. However, all clinical services which
provided care in outpatients had their own specialty audit plans.
Staff protected the rights of patients subject to the Mental Health Act and followed the Code of
Practice by ensuring that they had access to services. Staff told us that patients were given extra
time in clinics and referred to other organisations when appropriate for specialist help.
Nutrition and hydration
Staff ensured patients who required it had enough food and drink to meet their needs.
Water dispensers were available throughout the outpatient’s departments and were clearly
signposted.
There were shops and café facilities, where patients and visitors could purchase refreshments.
Staff told us they would provide hot drinks and sandwiches to those who had to wait a long time
and had specific nutritional needs such as patients who had diabetes.
Pain relief
Staff assessed and monitored patients to see if they were in pain and gave pain relief in a
timely way. They supported those unable to communicate using suitable assessment tools
and gave additional pain relief to ease pain.
Pain relief was prescribed and used within some of the outpatient departments. In the
ophthalmology and dermatology clinics, staff had access to both oral and local analgesia where
patients were undergoing minor procedures.
In the ophthalmology clinic and fracture clinic (plaster room), during treatment we observed staff
asking patients about their pain and comfort levels. Patients we spoke with raised no concerns
about their pain management during appointments.
Patient outcomes

20190416 900885 Post-inspection Evidence appendix template v4 Page 282
Staff monitored the effectiveness of care and treatment and reported this in patient
records. There was minimal evidence of staff using the findings to make improvements and
achieve good outcomes for patients.
There were no specific national clinical audits for outpatient services, but within the division staff
contributed to relevant local and national audits and collected information on patient outcomes.
For example, the ophthalmology department took part in the national ‘Patient Reported Outcome
Measures’ (PROMS) ophthalmology audit, the orthopaedic team took part in the ‘National Hip
Fracture’ audit and Joint Registry programme and staff in neurology clinic participated in the
‘National Parkinson's UK’ audit. Further details are reported in the surgery and medicine sections
of this report.
The national clinical audits are used to benchmark the quality of the trust’s services compared with
other NHS trusts, and highlight both best and substandard practices to drive continuous
improvement across services.
Follow-up to new rate
Broomfield Hospital
From March 2018 to February 2019 the follow-up to new rate for Broomfield Hospital was
marginally higher than the England average in all months and followed the same trend.
Follow-up to new rate, Mid Essex Hospital Services NHS Trust.
Note: William Julien Courtauld Hospital is also known as St Michael’s Hospital.
(Source: Hospital Episode Statistics)
Competent staff
The service made sure staff were competent for their roles. Managers held supervision
meetings with staff to provide support and development. Although not all nursing staff had
an annual appraisal.
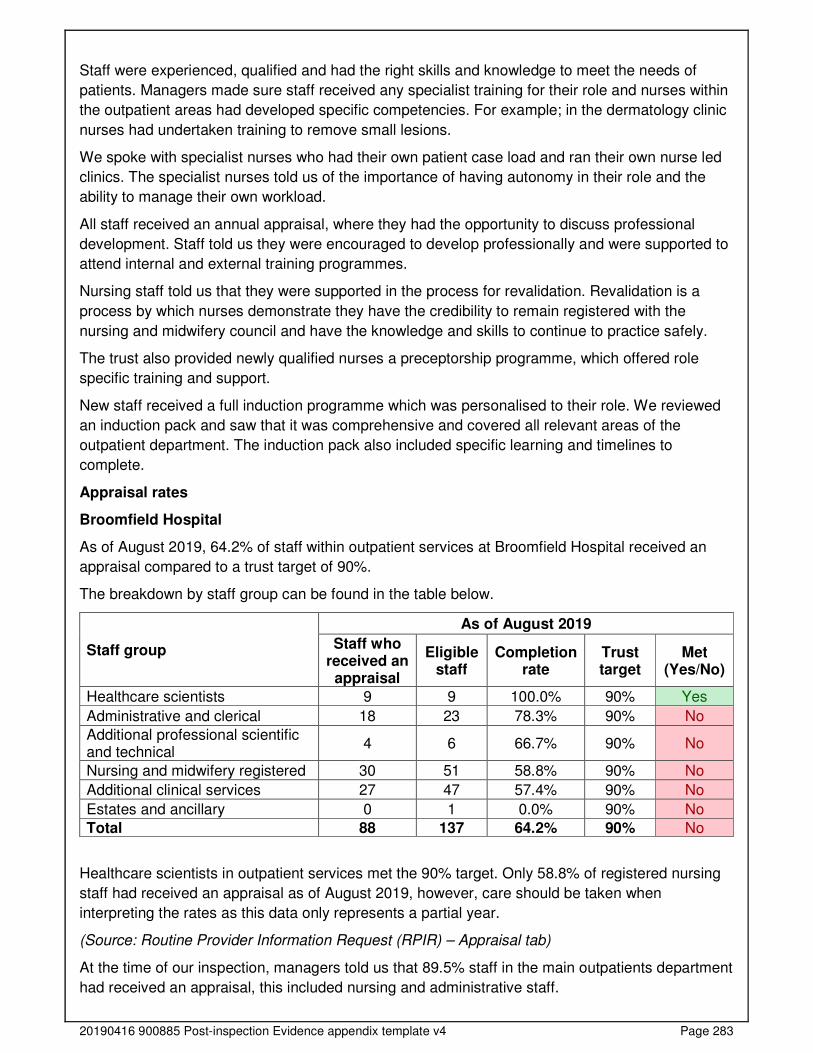
20190416 900885 Post-inspection Evidence appendix template v4 Page 283
Staff were experienced, qualified and had the right skills and knowledge to meet the needs of
patients. Managers made sure staff received any specialist training for their role and nurses within
the outpatient areas had developed specific competencies. For example; in the dermatology clinic
nurses had undertaken training to remove small lesions.
We spoke with specialist nurses who had their own patient case load and ran their own nurse led
clinics. The specialist nurses told us of the importance of having autonomy in their role and the
ability to manage their own workload.
All staff received an annual appraisal, where they had the opportunity to discuss professional
development. Staff told us they were encouraged to develop professionally and were supported to
attend internal and external training programmes.
Nursing staff told us that they were supported in the process for revalidation. Revalidation is a
process by which nurses demonstrate they have the credibility to remain registered with the
nursing and midwifery council and have the knowledge and skills to continue to practice safely.
The trust also provided newly qualified nurses a preceptorship programme, which offered role
specific training and support.
New staff received a full induction programme which was personalised to their role. We reviewed
an induction pack and saw that it was comprehensive and covered all relevant areas of the
outpatient department. The induction pack also included specific learning and timelines to
complete.
Appraisal rates
Broomfield Hospital
As of August 2019, 64.2% of staff within outpatient services at Broomfield Hospital received an
appraisal compared to a trust target of 90%.
The breakdown by staff group can be found in the table below.
Staff group
As of August 2019
Staff who received an appraisal
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Healthcare scientists 9 9 100.0% 90% Yes
Administrative and clerical 18 23 78.3% 90% No
Additional professional scientific and technical
4 6 66.7% 90% No
Nursing and midwifery registered 30 51 58.8% 90% No
Additional clinical services 27 47 57.4% 90% No
Estates and ancillary 0 1 0.0% 90% No
Total 88 137 64.2% 90% No
Healthcare scientists in outpatient services met the 90% target. Only 58.8% of registered nursing
staff had received an appraisal as of August 2019, however, care should be taken when
interpreting the rates as this data only represents a partial year.
(Source: Routine Provider Information Request (RPIR) – Appraisal tab)
At the time of our inspection, managers told us that 89.5% staff in the main outpatients department
had received an appraisal, this included nursing and administrative staff.
20190416 900885 Post-inspection Evidence appendix template v4 Page 284
Managers made sure all staff attended team meetings or had access to full minutes when they
could not attend. We saw that team meeting minutes were displayed in the departments for staff to
read.
Managers identified any training needs their staff had and gave them the time and opportunity to
develop their skills and knowledge.
Staff told us that they had the opportunity to discuss training needs at their appraisals and were
supported by their line manager to develop their skills and knowledge.
Staff received specialist or additional training that was needed for their role. Staff in the
orthopaedic and fracture clinic told us that they received training in wound recognition as they
were often responsible for checking and redressing wounds post-surgery or on removal of plaster
casts.
Multidisciplinary working
Doctors, nurses and other healthcare professionals worked together as a team to benefit
patients. They supported each other to provide good care.
Staff held regular multidisciplinary meetings to discuss patients and improve their care. Outpatient
teams worked together to plan and deliver care and treatment. Staff in different teams and
services worked together to assess, plan and deliver co-ordinated care.
Staff in the outpatient department told us that specialist nurses attended clinics to support staff
and patients. These included; dementia nurses, breast care nurses and diabetes nurses.
Outpatient clinics were run by multidisciplinary teams (MDTs). We saw nursing staff, healthcare
assistants and doctors working collaboratively in all of the OPD clinics we visited.
We saw in the patient medical records clear evidence of outcomes and decisions from MDT
discussions and staff told us these were shared with patients and their relatives.
During clinics, doctors were always supported by a healthcare assistant or registered nurse.
The service provided one-stop clinics so that patients could see all the health professionals
involved in their care at the same time. We saw this in the breast clinic, rheumatology and
diabetes clinics.
Seven-day services
Key services were available five days a week to support timely patient care.
Outpatients’ clinics operated from 8.30am to 5pm Monday to Friday. There were no regular
weekend clinic appointments in the outpatients department. None of the services offered any
evening clinics or regular weekend clinics.
Staff reported that some specialties ran the occasional additional weekend clinics to address
patient backlogs.
Health promotion
Staff gave patients practical support and advice to lead healthier lives.
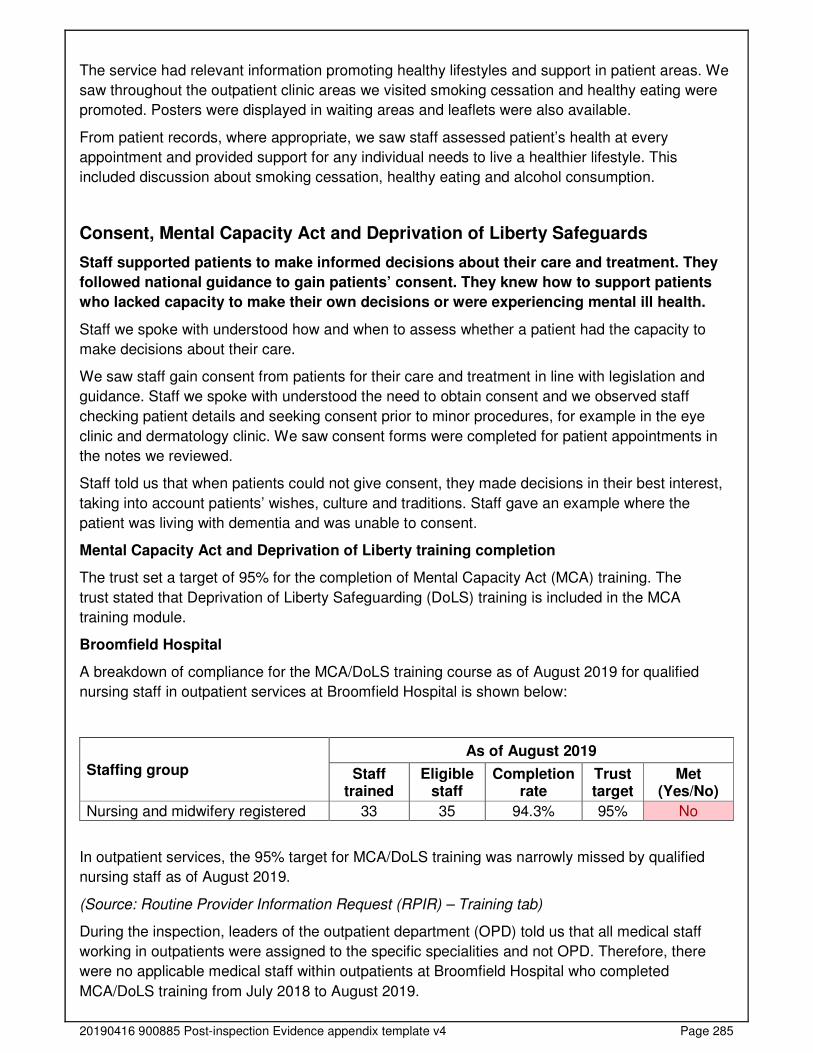
20190416 900885 Post-inspection Evidence appendix template v4 Page 285
The service had relevant information promoting healthy lifestyles and support in patient areas. We
saw throughout the outpatient clinic areas we visited smoking cessation and healthy eating were
promoted. Posters were displayed in waiting areas and leaflets were also available.
From patient records, where appropriate, we saw staff assessed patient’s health at every
appointment and provided support for any individual needs to live a healthier lifestyle. This
included discussion about smoking cessation, healthy eating and alcohol consumption.
Consent, Mental Capacity Act and Deprivation of Liberty Safeguards
Staff supported patients to make informed decisions about their care and treatment. They
followed national guidance to gain patients’ consent. They knew how to support patients
who lacked capacity to make their own decisions or were experiencing mental ill health.
Staff we spoke with understood how and when to assess whether a patient had the capacity to
make decisions about their care.
We saw staff gain consent from patients for their care and treatment in line with legislation and
guidance. Staff we spoke with understood the need to obtain consent and we observed staff
checking patient details and seeking consent prior to minor procedures, for example in the eye
clinic and dermatology clinic. We saw consent forms were completed for patient appointments in
the notes we reviewed.
Staff told us that when patients could not give consent, they made decisions in their best interest,
taking into account patients’ wishes, culture and traditions. Staff gave an example where the
patient was living with dementia and was unable to consent.
Mental Capacity Act and Deprivation of Liberty training completion
The trust set a target of 95% for the completion of Mental Capacity Act (MCA) training. The
trust stated that Deprivation of Liberty Safeguarding (DoLS) training is included in the MCA
training module.
Broomfield Hospital
A breakdown of compliance for the MCA/DoLS training course as of August 2019 for qualified
nursing staff in outpatient services at Broomfield Hospital is shown below:
Staffing group
As of August 2019
Staff trained
Eligible staff
Completion rate
Trust target
Met (Yes/No)
Nursing and midwifery registered 33 35 94.3% 95% No
In outpatient services, the 95% target for MCA/DoLS training was narrowly missed by qualified
nursing staff as of August 2019.
(Source: Routine Provider Information Request (RPIR) – Training tab)
During the inspection, leaders of the outpatient department (OPD) told us that all medical staff
working in outpatients were assigned to the specific specialities and not OPD. Therefore, there
were no applicable medical staff within outpatients at Broomfield Hospital who completed
MCA/DoLS training from July 2018 to August 2019.
20190416 900885 Post-inspection Evidence appendix template v4 Page 286
Staff we spoke with understood the relevant consent and decision-making requirements of
legislation and guidance, including the Mental Health Act, Mental Capacity Act 2005 and the
Children Acts 1989 and 2004 and they knew who to contact for advice.
Staff knew how to access the trust’s policy on Mental Capacity Act and Deprivation of Liberty
Safeguards.
Is the service caring?
Compassionate care
Staff treated patients with compassion and kindness, respected their privacy and dignity,
and took account of their individual needs.
Staff were discreet and responsive when caring for patients. We observed staff treating patients
with dignity, courtesy and respect. We observed that staff introduced themselves and interacted
well with patients.
Patients we spoke with said staff were friendly and treated them well and with kindness. All six
patients and the one relative we spoke with described positive experiences of care.
We observed patients being greeted when arriving in the department and staff taking the time to
interact with patients. Staff introduced themselves and took time to interact with patients. We
observed that staff were respectful and considerate during consolations.
Staff respected patient’s dignity. For example, we saw staff knocking before entering consultation
rooms and covering patients with blankets during procedures.
All outpatients’ clinics had nursing staff available to chaperone patients and staff commented that
this was always available. In the 10 patients’ records we reviewed, a stamp was used to indicate
that chaperone was present with the patient.
Emotional support
Staff provided emotional support to patients, families and carers to minimise their distress.
They understood patient's personal, cultural and religious needs.
Staff gave patients and those close to them help, emotional support and advice when they needed
it. Staff were sensitive and respectful of patients. Staff supported patients who became distressed
or anxious and spent time discussing their concern.
Patients’ privacy was observed when speaking with receptionists on arrival. Patients waited
behind a line to book in to ensure information could be communicated with the reception staff
without being overheard.
The hospital had a multi-faith chapel available with prayer facilities. A chaplain was present within
the hospital to provide support to patients, carers and staff. The chaplains were available to
provide support for managers in breaking bad news to other staff, offer listening and support for
staff, and hold short acts of remembrance for staff members who passed away.
Patients we spoke with told us they had received support from staff, emotionally, as well as
physically where there had been bad news following diagnostic results.
20190416 900885 Post-inspection Evidence appendix template v4 Page 287
Staff signposted patients to other support organisations. For example, on the hospital site there
was a Macmillan cancer support service, and a volunteer service to help support patients
undergoing cancer treatment.
Understanding and involvement of patients and those close to them
Staff supported patients, families and carers to understand their condition and make
decisions about their care and treatment.
Staff made sure patients and those close to them understood their care and treatment. Care was
planned and delivered in a way that involved patients and their carers. We saw Staff gave patients
and their relatives time to explain their symptoms and they were encouraged to ask questions. We
observed that staff answered patients’ questions appropriately, and in a way they could
understand.
Staff talked with patients, families and carers in a way they could understand. For example, we
saw staff using communication aids where necessary. Staff also simplified medical terminology to
ensure the patient understood what they were explaining.
Staff used communication aids for patients with learning difficulties and those with communication
needs, these included picture cards. Staff also had access to the learning disabilities nurse to
support patients where appropriate.
Patients told us that staff kept them informed of what was happening with their care, including
waiting times. We saw staff informing patients of current waiting times for their clinic.
Staff supported patients to make informed decisions about their care. Patients we spoke with said
they felt comfortable asking questions about their care and that they had been given time with the
nurses and doctors to ask questions.
Is the service responsive?
Service delivery to meet the needs of local people
The service planned and provided care in a way that met the needs of local people and the
communities served.
Managers planned and organised services, so they met the changing needs of the local
population.
The hospital site was accessible by public transport and the main entrance had an electronic
board with ‘live’ public transport timetable information. There was also an on-site car park,
however both staff and patients stated that it was difficult to find parking space .
The facilities in the main outpatient was appropriate for the services being delivered. The main
outpatient department was on the ground floor main atrium of the hospital. Clinics were clearly
signposted from the main entrance throughout the reception area.
The outpatient areas generally had enough seating for patients and relatives, but we did see
congestion and patients standing at the phlebotomy clinic during busy times during the day.
There were suitable toilet facilities in all clinic areas we visited. In the waiting areas, magazines
and water dispensing machines was available for patients to use.
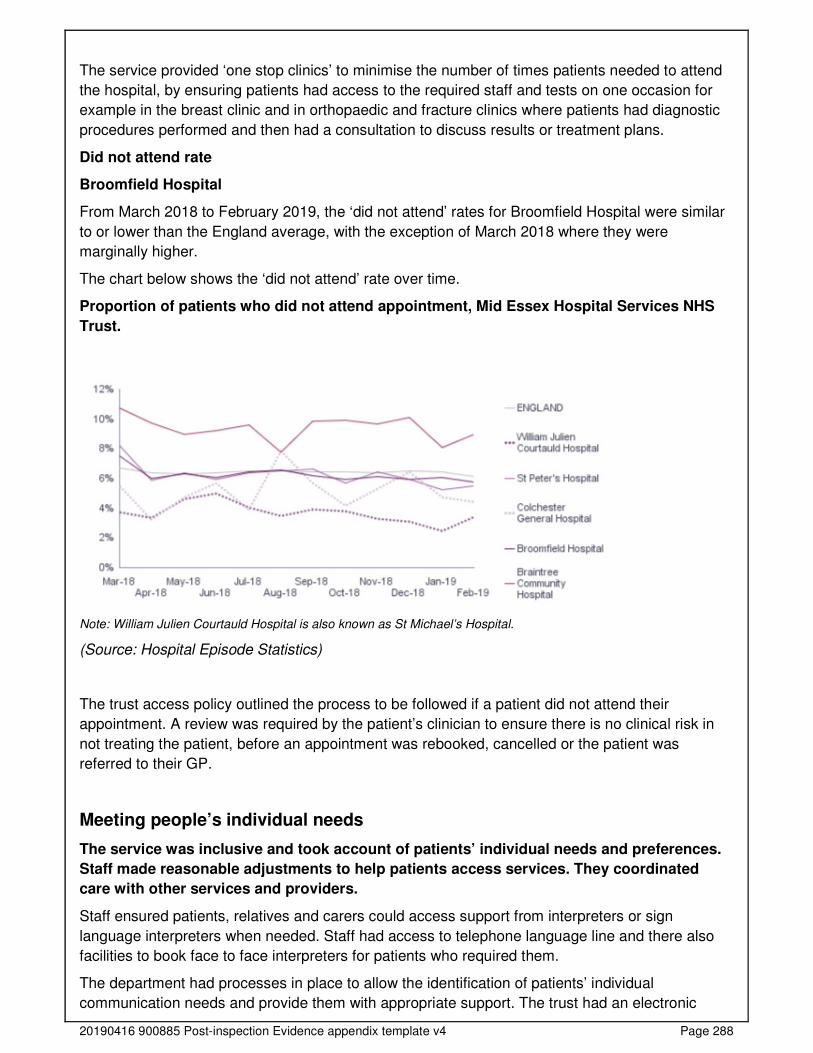
20190416 900885 Post-inspection Evidence appendix template v4 Page 288
The service provided ‘one stop clinics’ to minimise the number of times patients needed to attend
the hospital, by ensuring patients had access to the required staff and tests on one occasion for
example in the breast clinic and in orthopaedic and fracture clinics where patients had diagnostic
procedures performed and then had a consultation to discuss results or treatment plans.
Did not attend rate
Broomfield Hospital
From March 2018 to February 2019, the ‘did not attend’ rates for Broomfield Hospital were similar
to or lower than the England average, with the exception of March 2018 where they were
marginally higher.
The chart below shows the ‘did not attend’ rate over time.
Proportion of patients who did not attend appointment, Mid Essex Hospital Services NHS
Trust.
Note: William Julien Courtauld Hospital is also known as St Michael’s Hospital.
(Source: Hospital Episode Statistics)
The trust access policy outlined the process to be followed if a patient did not attend their
appointment. A review was required by the patient’s clinician to ensure there is no clinical risk in
not treating the patient, before an appointment was rebooked, cancelled or the patient was
referred to their GP.
Meeting people’s individual needs
The service was inclusive and took account of patients’ individual needs and preferences.
Staff made reasonable adjustments to help patients access services. They coordinated
care with other services and providers.
Staff ensured patients, relatives and carers could access support from interpreters or sign
language interpreters when needed. Staff had access to telephone language line and there also
facilities to book face to face interpreters for patients who required them.
The department had processes in place to allow the identification of patients’ individual
communication needs and provide them with appropriate support. The trust had an electronic
20190416 900885 Post-inspection Evidence appendix template v4 Page 289
flagging system in place for all patients known to have a formal diagnosis of dementia or learning
disabilities (LD).
Within each clinic area staff confirmed that they tried to reduce the impact on patients living with
dementia or with learning disabilities by offering a quiet space to wait prior to appointments. Staff
also confirmed that they had access to support from the learning disability and dementia nurses,
and they prioritised patients to reduce their waiting.
The outpatient departments had hearing loop in place. This is a special type of sound system for
use by people with hearing aids.
Staff were aware of the support available and knew how to access it for patients presenting with
mental health conditions.
The service had access to information leaflets in languages spoken by the patients and local
community. An interpreting service was available for patients whose first language was not
English. The interpreting service was available through a telephone line service or face to face and
was arranged for patients requiring it.
There were volunteers located at the front entrance to the hospital to direct patients to the correct
outpatient area.
Access and flow
We could not gain accurate assurances that people could access the service when they needed it
and receive the right care promptly. Waiting times from referral to treatment (RTT) were not
externally reported at the time of our inspection. From 2018 to 2019, the trust implemented an
electronic patient record system which caused data validity issues and poor quality data. With
agreement from NHS England the trust were excluded from reporting data until they had
completed a review and data cleansing exercise.
Locally, managers told us waiting times were being monitored. However, at the time of our
inspection local leaders were unable to provide us with data to evidence the percentages of harm
reviews or whether the service were meeting the national targets.
Following our inspection we requested data from the senior leadership team We reviewed the data
that was provided, we were not able to analyse trends on unvalidated data. Senior leaders told us
patients that were not able to access services within national targets, received a harm review and
were reported to board in common meetings. They also told us that until they returned to reporting
(scheduled April 2020) ‘shadow reporting’ was in place, which included monthly review meetings
with NHS Improvement/England and commissioners.
A standard operating procedure (SOP) was in place relating to clinic cancellations. All clinics
cancelled at short notice (within six weeks) had to be signed off by the appropriate management
team.
Managers told us that they ensured that there was full utilisation of the outpatient clinic rooms.
Booking staff and clinical teams worked together to ensure that additional clinics were
accommodated, and all clinic rooms were used.
Referral to treatment (percentage within 18 weeks) – non-admitted pathways
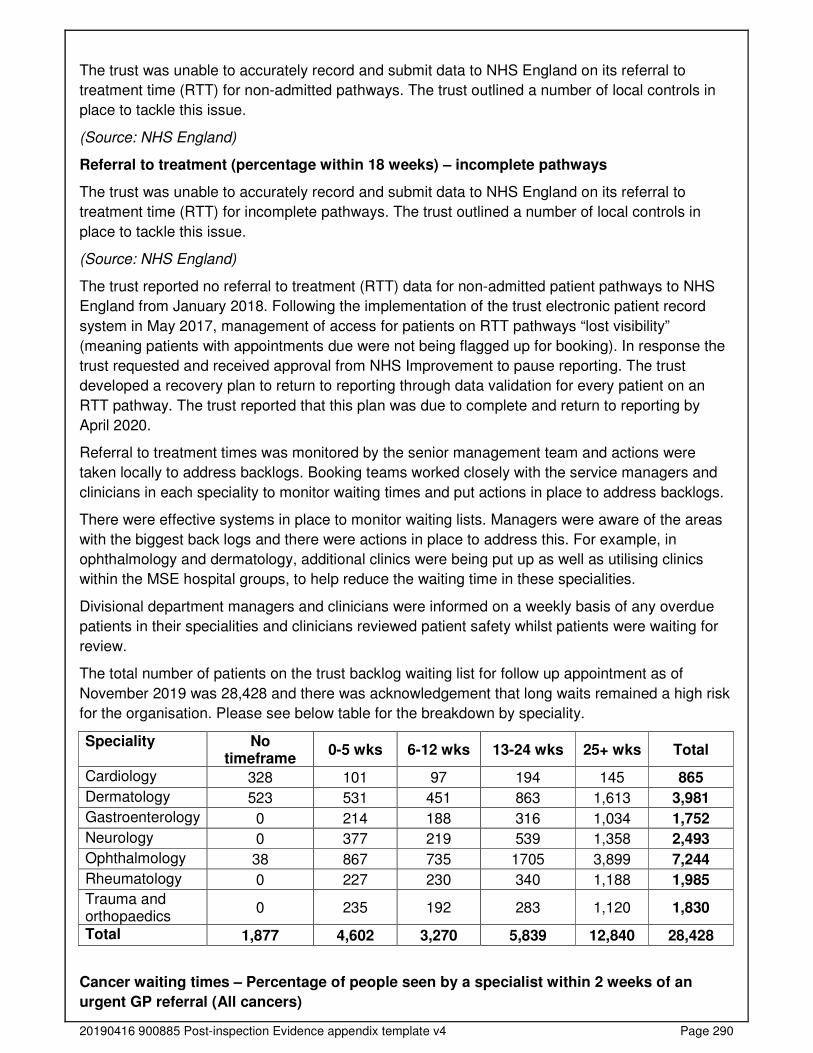
20190416 900885 Post-inspection Evidence appendix template v4 Page 290
The trust was unable to accurately record and submit data to NHS England on its referral to
treatment time (RTT) for non-admitted pathways. The trust outlined a number of local controls in
place to tackle this issue.
(Source: NHS England)
Referral to treatment (percentage within 18 weeks) – incomplete pathways
The trust was unable to accurately record and submit data to NHS England on its referral to
treatment time (RTT) for incomplete pathways. The trust outlined a number of local controls in
place to tackle this issue.
(Source: NHS England)
The trust reported no referral to treatment (RTT) data for non-admitted patient pathways to NHS
England from January 2018. Following the implementation of the trust electronic patient record
system in May 2017, management of access for patients on RTT pathways “lost visibility”
(meaning patients with appointments due were not being flagged up for booking). In response the
trust requested and received approval from NHS Improvement to pause reporting. The trust
developed a recovery plan to return to reporting through data validation for every patient on an
RTT pathway. The trust reported that this plan was due to complete and return to reporting by
April 2020.
Referral to treatment times was monitored by the senior management team and actions were
taken locally to address backlogs. Booking teams worked closely with the service managers and
clinicians in each speciality to monitor waiting times and put actions in place to address backlogs.
There were effective systems in place to monitor waiting lists. Managers were aware of the areas
with the biggest back logs and there were actions in place to address this. For example, in
ophthalmology and dermatology, additional clinics were being put up as well as utilising clinics
within the MSE hospital groups, to help reduce the waiting time in these specialities.
Divisional department managers and clinicians were informed on a weekly basis of any overdue
patients in their specialities and clinicians reviewed patient safety whilst patients were waiting for
review.
The total number of patients on the trust backlog waiting list for follow up appointment as of
November 2019 was 28,428 and there was acknowledgement that long waits remained a high risk
for the organisation. Please see below table for the breakdown by speciality.
Speciality No timeframe
0-5 wks 6-12 wks 13-24 wks 25+ wks Total
Cardiology 328 101 97 194 145 865
Dermatology 523 531 451 863 1,613 3,981
Gastroenterology 0 214 188 316 1,034 1,752
Neurology 0 377 219 539 1,358 2,493
Ophthalmology 38 867 735 1705 3,899 7,244
Rheumatology 0 227 230 340 1,188 1,985
Trauma and orthopaedics
0 235 192 283 1,120 1,830
Total 1,877 4,602 3,270 5,839 12,840 28,428
Cancer waiting times – Percentage of people seen by a specialist within 2 weeks of an
urgent GP referral (All cancers)
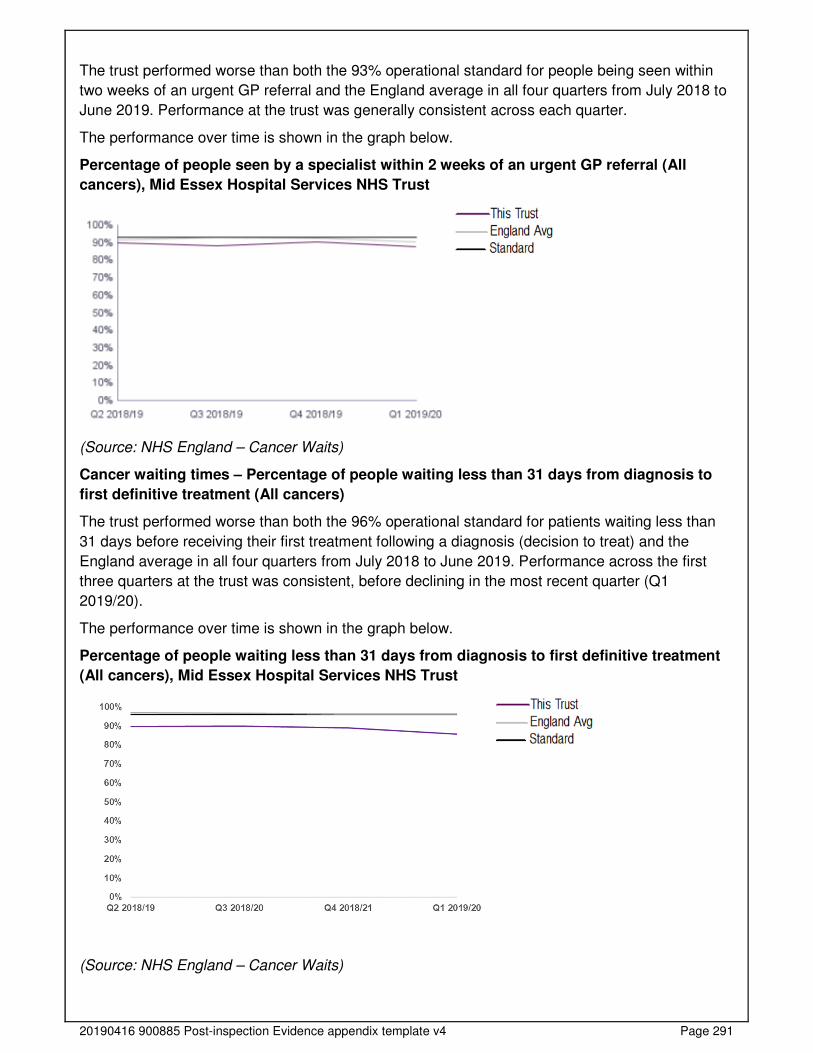
20190416 900885 Post-inspection Evidence appendix template v4 Page 291
The trust performed worse than both the 93% operational standard for people being seen within
two weeks of an urgent GP referral and the England average in all four quarters from July 2018 to
June 2019. Performance at the trust was generally consistent across each quarter.
The performance over time is shown in the graph below.
Percentage of people seen by a specialist within 2 weeks of an urgent GP referral (All
cancers), Mid Essex Hospital Services NHS Trust
(Source: NHS England – Cancer Waits)
Cancer waiting times – Percentage of people waiting less than 31 days from diagnosis to
first definitive treatment (All cancers)
The trust performed worse than both the 96% operational standard for patients waiting less than
31 days before receiving their first treatment following a diagnosis (decision to treat) and the
England average in all four quarters from July 2018 to June 2019. Performance across the first
three quarters at the trust was consistent, before declining in the most recent quarter (Q1
2019/20).
The performance over time is shown in the graph below.
Percentage of people waiting less than 31 days from diagnosis to first definitive treatment
(All cancers), Mid Essex Hospital Services NHS Trust
(Source: NHS England – Cancer Waits)

20190416 900885 Post-inspection Evidence appendix template v4 Page 292
Cancer waiting times – Percentage of people waiting less than 62 days from urgent GP
referral to first definitive treatment
The trust performed worse than the 85% operational standard for patients receiving their first
treatment within 62 days of an urgent GP referral and the England average in all four quarters
from July 2018 to June 2019. Performance at the trust declined in Q4 2018/19 before improving in
Q1 2019/20 in line with the first two quarters.
The performance over time is shown in the graph below.
Percentage of people waiting less than 62 days from urgent GP referral to first definitive
treatment, Mid Essex Hospital Services NHS Trust
(Source: NHS England – Cancer Waits)
Learning from complaints and concerns
It was easy for people to give feedback and raise concerns about care received. The
service treated concerns and complaints seriously, investigated them and shared lessons
learned with all staff.
Staff understood the policy on complaints and knew how to handle them. The trust had an up to
date complaints policy which was available to all staff through the trust’s intranet. The policy set
out the process for investigating, responding to and learning from complaints.
Staff told us they usually tried to address complaints or concerns at the time the concern was
raised. However, If the complaint could not be resolved by the team, patients were provided with
the contact details of the patient advice and liaison service (PALS). Patients we spoke with knew
how to complain or raise concerns.
Information about how to raise a concern was clearly displayed in patient areas. We saw posters
and leaflets displayed in all outpatient areas and information about how to feed back to the service
was readily available in the outpatient department.
Managers we spoke to told us that they had received the appropriate training to investigate
complaints. Outpatient staff told us that mangers feedback from complaints and concerns at the
team meetings and during daily safety huddle.
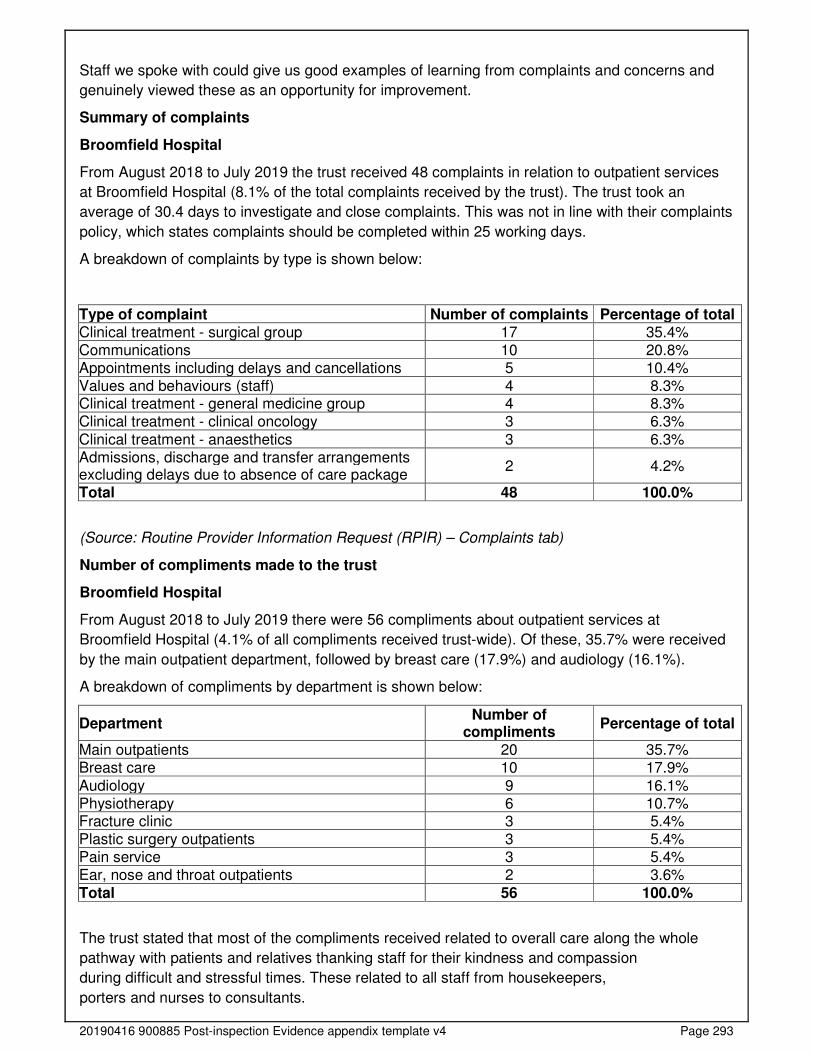
20190416 900885 Post-inspection Evidence appendix template v4 Page 293
Staff we spoke with could give us good examples of learning from complaints and concerns and
genuinely viewed these as an opportunity for improvement.
Summary of complaints
Broomfield Hospital
From August 2018 to July 2019 the trust received 48 complaints in relation to outpatient services
at Broomfield Hospital (8.1% of the total complaints received by the trust). The trust took an
average of 30.4 days to investigate and close complaints. This was not in line with their complaints
policy, which states complaints should be completed within 25 working days.
A breakdown of complaints by type is shown below:
Type of complaint Number of complaints Percentage of total Clinical treatment - surgical group 17 35.4% Communications 10 20.8% Appointments including delays and cancellations 5 10.4% Values and behaviours (staff) 4 8.3% Clinical treatment - general medicine group 4 8.3% Clinical treatment - clinical oncology 3 6.3%
Clinical treatment - anaesthetics 3 6.3% Admissions, discharge and transfer arrangements excluding delays due to absence of care package
2 4.2%
Total 48 100.0%
(Source: Routine Provider Information Request (RPIR) – Complaints tab)
Number of compliments made to the trust
Broomfield Hospital
From August 2018 to July 2019 there were 56 compliments about outpatient services at
Broomfield Hospital (4.1% of all compliments received trust-wide). Of these, 35.7% were received
by the main outpatient department, followed by breast care (17.9%) and audiology (16.1%).
A breakdown of compliments by department is shown below:
Department Number of
compliments Percentage of total
Main outpatients 20 35.7% Breast care 10 17.9%
Audiology 9 16.1% Physiotherapy 6 10.7% Fracture clinic 3 5.4% Plastic surgery outpatients 3 5.4% Pain service 3 5.4% Ear, nose and throat outpatients 2 3.6%
Total 56 100.0%
The trust stated that most of the compliments received related to overall care along the whole
pathway with patients and relatives thanking staff for their kindness and compassion
during difficult and stressful times. These related to all staff from housekeepers,
porters and nurses to consultants.
20190416 900885 Post-inspection Evidence appendix template v4 Page 294
Compliments and the associated learning and sharing of good practice is discussed at the patient
and carer experience group and with individuals and their managers during appraisal. The trust
uses its Datix system to analyse themes from compliments.
(Source: Routine Provider Information Request (RPIR) – Compliments tab)
Is the service well-led?
Leadership
Leaders had the integrity, skills and abilities to run the service. They understood and
managed the priorities and issues the service faced. They were visible and approachable in
the service for patients and staff.
The main outpatient department (OPD) was within the division of burns, plastics and outpatients.
The division was managed by the triumvirate team which consisted of a divisional director,
associated director of operations and an associated director of nursing supported by the OPD
service manager and matron.
Specialist staff were managed by their own divisions, for example, the head and neck unit and the
orthopaedic and fracture clinics were managed by similar systems within the surgical division.
Outpatient clinics were managed on a day to day basis by band six or band seven nurses. The
outpatient teams were made up of nurses, healthcare assistants, administration and clerical staff.
The OPD frontline clinical managers reported to the matron of the division in which the outpatient
department belonged to. Matrons were allocated to variety of areas within the OPD based on their
skills, experience and expertise.
All of the outpatient leaders and senior staff we met demonstrated understanding of the issues in
their service and appeared knowledgeable about their service and competent in their roles.
All staff we spoke with knew who their local leaders were and felt supported. Staff commented that
local leaders were approachable and supportive.
Vision and strategy
The service had a vision for what it wanted to achieve and a strategy to turn it into action.
Leaders and staff understood and knew how to apply them and monitor progress.
The outpatient vision and strategy were based on the trust’s vision “patient care first…always” and
the values.
The outpatient strategy identified eight key areas of focus for 2019/2020. These were; improve
patient experience and safety, right size clinic templates, improve clinic utilisation, reduce
unnecessary follow ups, streamlining the booking process, reduce less than six weeks clinic
cancellations, review non-medical workforce and going digital.
Culture
Staff felt respected, supported and valued. They were focused on the needs of patients
receiving care. The service promoted equality and diversity in daily work and provided

20190416 900885 Post-inspection Evidence appendix template v4 Page 295
opportunities for career development. The service had an open culture where patients, their
families and staff could raise concerns without fear.
All staff we spoke with said they felt supported, respected and valued by their line managers. We
observed good teamwork in the outpatient clinics between all staff groups.
Staff of all grades confirmed that they were encouraged to be open and transparent, reporting
adverse events and incidents in a way which helped improve things within the service.
Staff told us that they were able to raise any concerns with their managers and said that they
received support from local leadership team and their peers.
Staff were aware of the trust’s ‘Guardian’ service, an independent service commissioned by the
trust to facilitate ‘Freedom to Speak Up Guardian’ (all NHS trusts must nominate a guardian to
ensure staff can raise concerns safely) who was available for confidential advice.
There were processes in place to provide staff with career development opportunities. Staff told us
that they received regular appraisals and these included discussions around career development.
Staff told us that the trust was supportive of training and they felt encouraged to undertake
additional training when funding and scheduling allowed.
Governance
Leaders operated effective governance processes, throughout the service and with partner
organisations. Staff at all levels were clear about their roles and accountabilities and had
regular opportunities to meet, discuss and learn from the performance of the service.
There were effective processes and systems of accountability within outpatients. Outpatient
specialities were split over different clinical divisions. There was a central outpatient function for a
number of general clinics in surgery and medicine. Specialist clinics were run from specific areas
across the trust. The management of these specialist clinics were within the division responsible
for the service such as gynaecology, trauma and orthopaedics, ENT, dermatology, ophthalmology
and oncology.
Governance systems were in place to support the functions of outpatient services. Monthly
meetings were conducted to allow oversight of the service which reported into divisional
governance meetings. All senior outpatient managers and clinical managers were encouraged to
attend these meetings. Governance meetings had a set agenda and we saw this was followed
during meetings. We reviewed the minutes from June, July and September 2019.
There was an effective process to share governance systems and updates with staff. Daily safety
huddles were held in the OPD. We reviewed a sample of the daily huddle sheet from August,
September, October and November 2019 and saw that they had a list of items to discuss and
governance was included. Items discussed included incidents, complaints, clinic start times and
changes in processes (new policies or procedures).
Staff of all grades appeared clear about their roles and what they were accountable for and to
whom.
Management of risk, issues and performance
The trust had systems for identifying risks, planning to eliminate or reduce them, and
coping with both the expected and unexpected.
20190416 900885 Post-inspection Evidence appendix template v4 Page 296
OPD clinical delivery unit had a risk register in place. Each risk was rated and had a named
manager responsible for overseeing the risk and there were details of the actions taken to mitigate
the risk and updates provided as the risks were reviewed. The risk register was reviewed and
updated at the monthly clinical governance meeting. Specialist clinics risks, where reported within
the division responsible for the service.
Clinical delivery groups held monthly meetings where performance concerns were discussed
addressed and performance reports presented. We reviewed the last three meeting minutes (from
July to September 2019) for outpatients and saw they detailed areas of risk and performance,
including number of referrals received and number of patients waiting for 6 week appointments.
Clinicians undertook clinical harm reviews for follow up patients and a risk assessment was
completed for patients waiting over six weeks beyond their due date. There were robust processes
in place to give leaders oversight of patients waiting for appointments and RTT performance and
these were used to plan to deliver improved access for patients.
The trust had not reported against the national 18 week referral to treatment (RTT) standards
since January 2018. The trust had established a programme of work with key workstreams
including validation, data quality, training and demand and capacity. At the time of our inspection
the programme was in progress and likely to return to national reporting in April 2020.
The monthly OPD performance dashboard enabled senior staff to oversee and monitor key
performance information including but not limited to; service demand, activity and productivity.
Senior staff attended monthly meetings to discuss the dashboard data.
The service carried out regular audits provide assurance on safety and effectiveness in the OPD
areas, including but not limited to; medicines management, chaperone audit, environment and
safety, availability of notes and quality of documentation.
Information management
The service did not always collect reliable data and analyse it. Staff could not always find
the data they needed, in easily accessible formats, to understand performance, make
decisions and improvements. Information systems were not always integrated but were
secure. Data or notifications were not always consistently submitted to external
organisations as required.
In May 2017, a new electronic patient record system led to problems with accurately tracking
patients and capturing validated accurate referral to treatment (RTT) data. At the time of our
inspection, RTT formal data submission was not taking place (ceased in January 2018 with the
support from NHS England), however, the trust had implemented a number of local measures to
monitor RTT times. All patients who did not meet RTT were reviewed for harm.
Staff had access to policies, standard operating procedures and patient information leaflets
electronically through the document pages on the intranet. Staff confirmed that this ensured that
information was easily accessible and up to date.
Patient information was managed securely. Computer terminals were secured when not in use to
protect patient confidentiality. Reception desk terminals were not visible to the public. All paper
patients’ record was stored in secure locked cabinets when not in use.
Engagement

20190416 900885 Post-inspection Evidence appendix template v4 Page 297
Leaders and staff actively and openly engaged with patients, staff, equality groups, the
public and local organisations to plan and manage services. They collaborated with partner
organisations to help improve services for patients.
Patients were encouraged to complete the NHS Friends and Family Test (FFT). This is a national
programme that gives patients the opportunity to feedback on the care they have received.
Staff working in outpatients felt they were involved by their managers about plans for the services
they delivered.
Staff at all levels told us that senior leaders were visible and offered opportunities to listen and
feedback to staff.
Service leaders were working with clinical commissioning groups (CCGs) and primary care to
assess and reviewed patient pathways across a number of specialities to improve access and
care for patients.
Learning, continuous improvement and innovation
All staff were committed to continually learning and improving services. They had a good
understanding of quality improvement methods and the skills to use them.
In the last 12 months the outpatient department had a programme of work designed to streamline
pathways of care across the trust. Various clinical specialities including cardiology,
gastroenterology, nephrology, neurology, endocrinology, respiratory, ophthalmology, trauma and
orthopaedics, general surgery, urology, and plastics have reviewed their pathways and
benchmarked their performance against peers in the same speciality to inform pathway changes.
The proposals had been presented to executive team and been approved.