Microbiology - HLS
47
Microbiology - HLS Done By Hani Titi Corrected By Leen Anwar Samah Freihat
Transcript of Microbiology - HLS
Microbiology - HLSDone By
Hani Titi
Corrected By Leen Anwar
Samah Freihat
Blood protozoa :Plasmodium & Babesia
Ass. Prof. Nader Alaridah MD, PhDBlue : not mentioned in 018 video
OverviewvAparasiteisanorganismthatlivesonorinahostorganismandgetsitsfood from orat the expense ofits host.
vProtozoa are unicellular eukaryotes that form anentire kingdom.vThe protozoa that are infectious to humans canbe classified into four groupsbased on their mode of movement and mode of reproduction :• Sarcodina – the ameba (They use pseudopods,asexual reproduction)• Mastigophora – the flagellates, Giardia, Leishmania (asexual reproduction)• Ciliophora – the ciliates, e.g., Balantidium (asexual reproduction)(asexual production = binary fission )
• Sporozoa – organisms whose adult stageis not motile (gliding movement) e.g., Plasmodium, Cryptosporidium undergo acomplex life cycle with alternatingsexual and asexual reproductive phases. The humanparasites Cryptosporidium,Cyclospora,and Toxoplasmaand themalarial parasites ( Plasmodium species) areall intracellular parasites.
3 kingdoms In parasitology :protozoa, helminths, and arthropods
• Malaria is an intracellular protozoal infection and it’s the most important parasitic disease. (the no.1 killer of all of them)
• Malaria is a vector-borne disease (the female anopheline mosquito). And the main targeted cells are RBCs.• Over 2 billion(41% world population) lives inmalaria-risk area.
• Infects 300-500 million peopleper year, 90% ofwhom are insub-Saharan Africa.
• Kills over 1 million peopleeach year and some estimate as many as 2.5 million.
• LeadingInfectiouskiller ofchildren in parasitic diseases. Worldwide a childdies of malariaevery 30 seconds.
• DiseaseBurden increasing due to: weakening public health, agricultural practices, globalwarming, lack of vaccine,drug resistance in parasiteandvector, populationgrowthin endemicareas, increased travel.
Epidemiology
Plasmodium• Plasmodium is a genus of parasitic alveolates, many of which causemalaria in their hosts.• Theparasitealwayshastwohostsinitslifecycle:Dipteraninsecthost and avertebrate host.
• Species:1.P. falciparum (most common , most serious , highest mortality rate)
2.P. malariacauses Quartan Malaria ( classical malaria , common in old ages)
3.P. vivax (mostcommon)4.P. ovale5.Plasmodium knowlesi(Simian malaria)
- Plasmodium falciparum is the major species associated with deadly infections throughout theworld. (associated with Malignant Tertian malaria)
v Both P.vivax and P.ovale causeBenign Tertian malaria which has 48 hr cycles
- Twosub-lifecycles:1- intrahepatic (exoerthrocytes )2- erthrocytic cycle• The vector for malaria is the femaleanopheline mosquito.• When thevectortakes a bloodmeal, sporozoites contained inthe salivary glands ofthemosquito aredischarged intothepuncture wound.
• Within an hour, these infective sporozoitesare carried via the blood to the liver, where theypenetrate hepatocytes and begin to grow, initiating the pre-erythrocytic or primaryexoerythrocytic cycle.
• The sporozoites (infectivestage) becomeround oroval and begindividing repeatedly.
• Schizogony results in (asexual multiplication)large numbers of exoerythrocytic merozoites.
• Oncethesemerozoites leave the liver, they invade the red blood cells (RBCs), initiating theerythrocytic cycle.
Mechanism of Infection
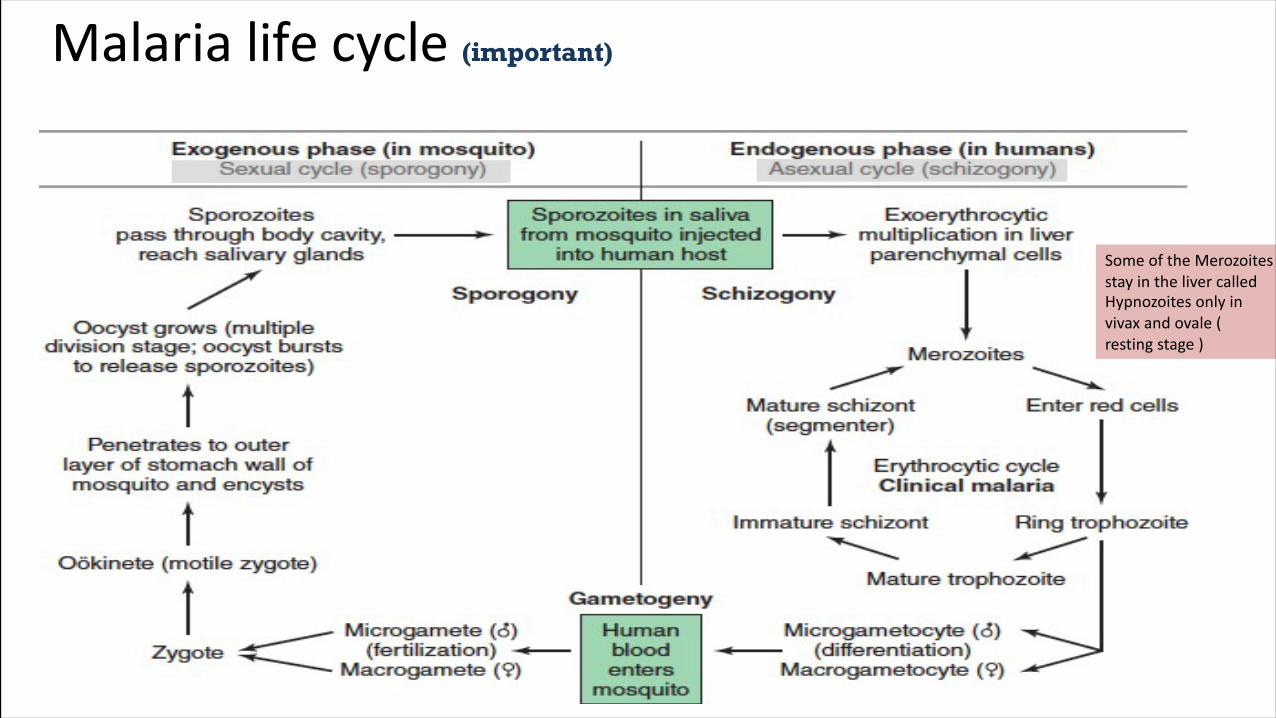
Malaria life cycle (important)
SomeoftheMerozoitesstayinthelivercalledHypnozoites only invivax andovale (restingstage)
• Adormant schizogonymay occur inP. vivax and P. ovale organisms,whichremain quiescent in theliver. (In extra-erythrocytic cycle)
• These resting stageshave been termedhypnozoitesand lead to a truerelapse (sleeping plasmodium) , often within 1 year or upto more than 5 years later.
• OncetheRBCsandreticulocyteshavebeeninvaded,theparasitesgrowandfeedonhemoglobin.
• Within the RBC, the merozoite (or young trophozoite) is vacuolated, ring shaped, moreor less ameboid, and uninucleate.
• The excess protein and hematinpresent from the metabolism ofhemoglobin combinetoformmalarial pigment.
• Oncethe nucleusbeginsto divide,the trophozoite iscalled a developing schizont.
• The matureschizont contains merozoites (whose number depends on thespecies),which are releasedinto the bloodstream.
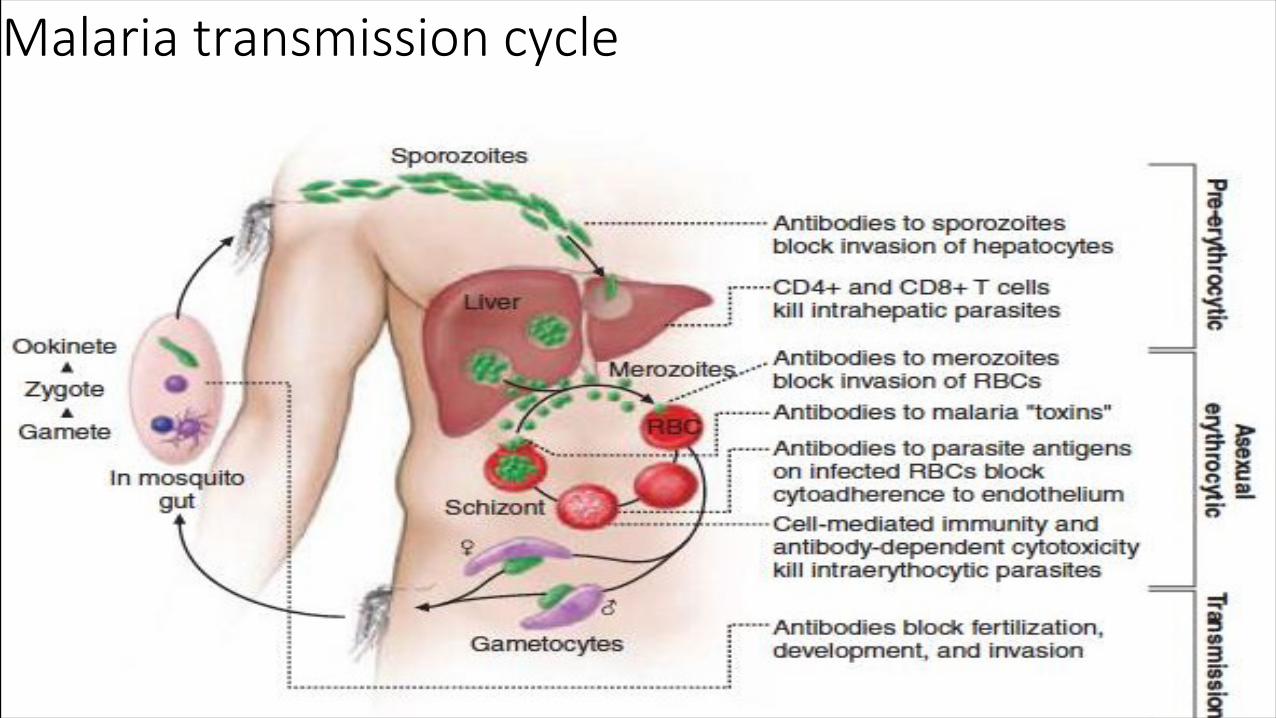
Malaria transmission cycle
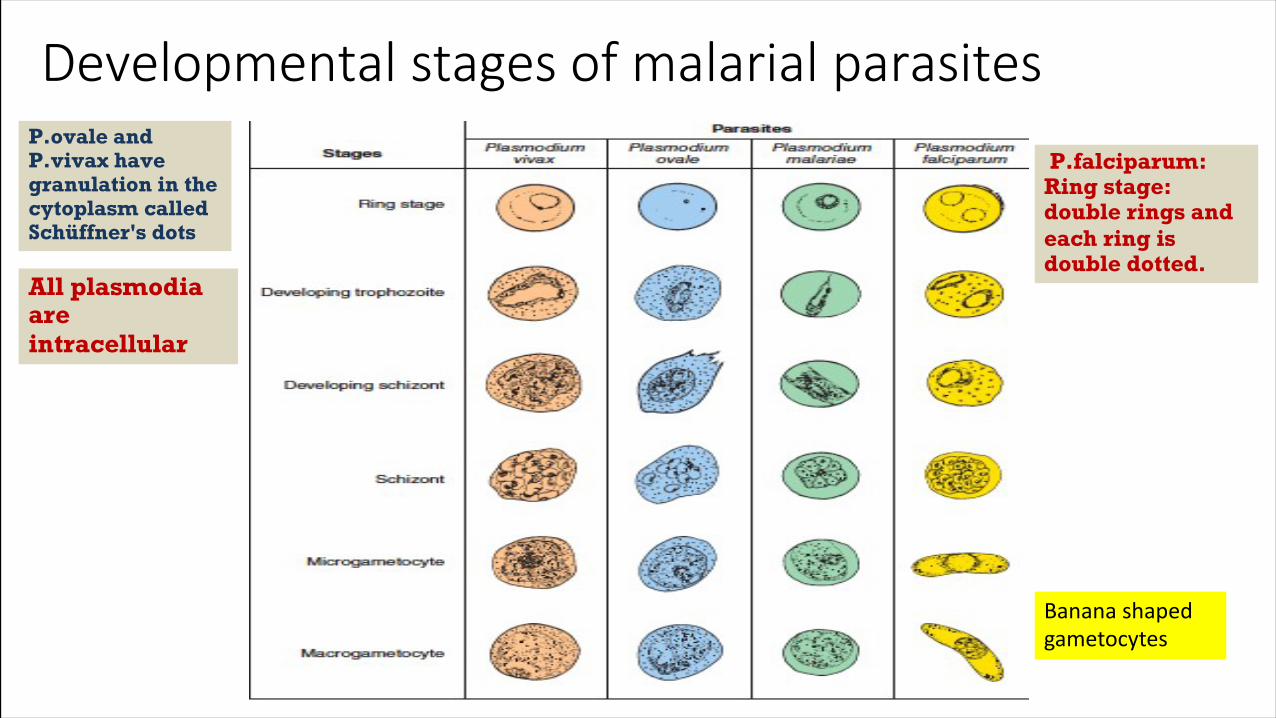
Developmental stages ofmalarial parasitesP.ovale and P.vivax have granulation in the cytoplasm called Schüffner's dots
P.falciparum: Ring stage: double rings and each ring is double dotted.
All plasmodia are intracellular
Bananashapedgametocytes
PLASMODIUMVIVAX (BENIGN TERTIAN MALARIA)Most wide spread malaria
After the incubation period the infection starts at the peripheral blood circulation which takes 48h
until ورجفنیام Merozoites from the RBCs the thing which effect the immune system causing fever
• P.vivax infects only thereticulocytes. (benign state which means parasitemia will be low unlike P.falciparum ; symptoms less frequent and less severe)
• *Tertian cycle is caused by erythrocytic cycle ; cycle of fever is repeated every 48hrs. (1 day of fever followed by 2 days of being well [repeatedly].
• Splenomegalyoccursduringthefirstfewweeksofinfection,andthespleenwill progress from being softandpalpabletohard, with continued enlargement during a chronic infection.
• Iftheinfectionistreatedduringtheearlyphases,thespleenwillreturntoitsnormal size.
• A secondaryordormant schizogony occurs in P. vivax and P. ovale, whichremain quiescentin the liver.The infected RBCs enlarge • These resting stageshave been termed hypnozoites.
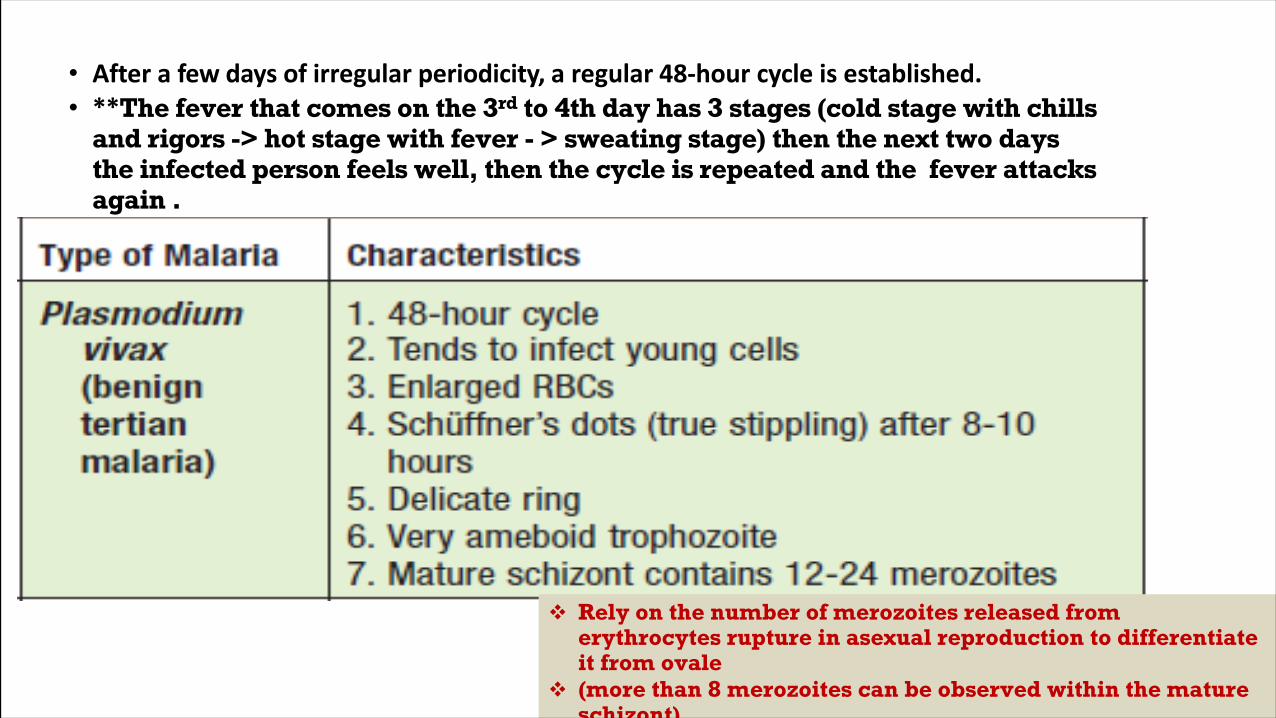
• After a few days ofirregular periodicity, a regular 48-hour cycleis established.• **The fever that comes on the 3rd to 4th day has 3 stages (cold stage with chills
and rigors -> hot stage with fever - > sweating stage) then the next two days the infected person feels well, then the cycle is repeated and the fever attacks again .
v Rely on the number of merozoites released from erythrocytes rupture in asexual reproduction to differentiate it from ovale
v (more than 8 merozoites can be observed within the mature schizont)
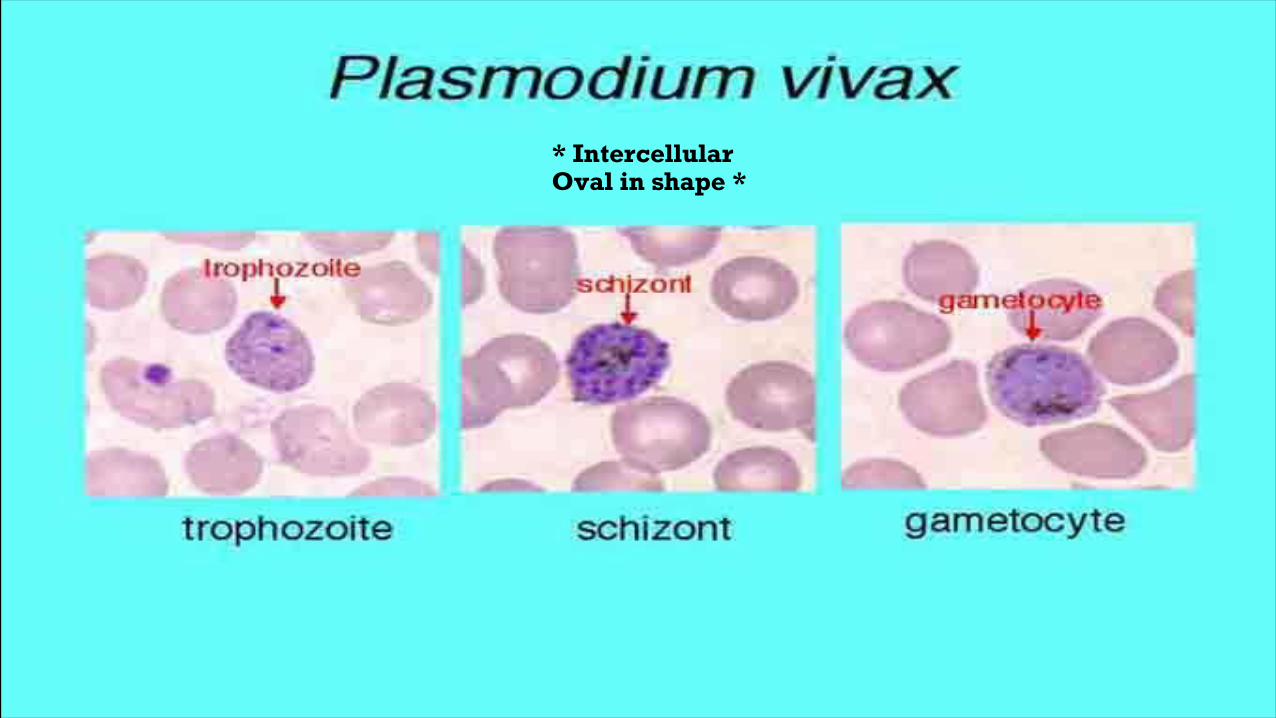
* IntercellularOval in shape *
Pathogenesis and Spectrum of Disease:
• In patients who have never been exposedto malaria:Symptomssuchasheadache,photophobia,muscleaches,anorexia,nausea,andsometimes vomitingmay occur before organismscan be detected in thebloodstream.
• In other patients with prior exposure tothe malaria:The parasites can befound inthe bloodstream several days before symptomsappear.
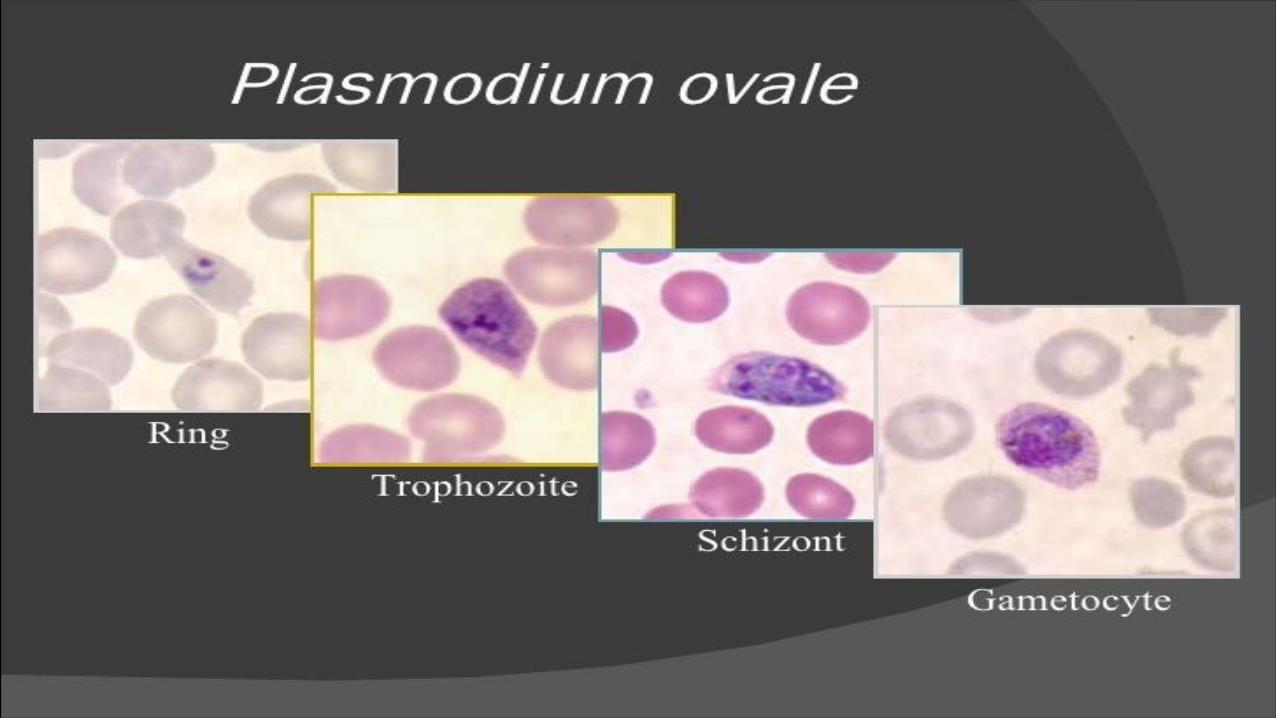
PLASMODIUMOVALE
• Although P.ovale and P. vivax infections are clinically similar, P.ovale malaria isusually less severe, tends to relapse less frequently, and usuallyends withspontaneous recovery.
• P. vivax, P. ovale infects only the reticulocytes.v Note that both have the same treatment
• Afterafewdaysofirregularperiodicity,aregular48-hourcycleisestablished.Over time,theparoxysms (fever attacks) becomelesssevereandmoreirregularinfrequencyandthen stopaltogether.
• P.ovale forms dormant schizogony (hypnozoites) in the liver
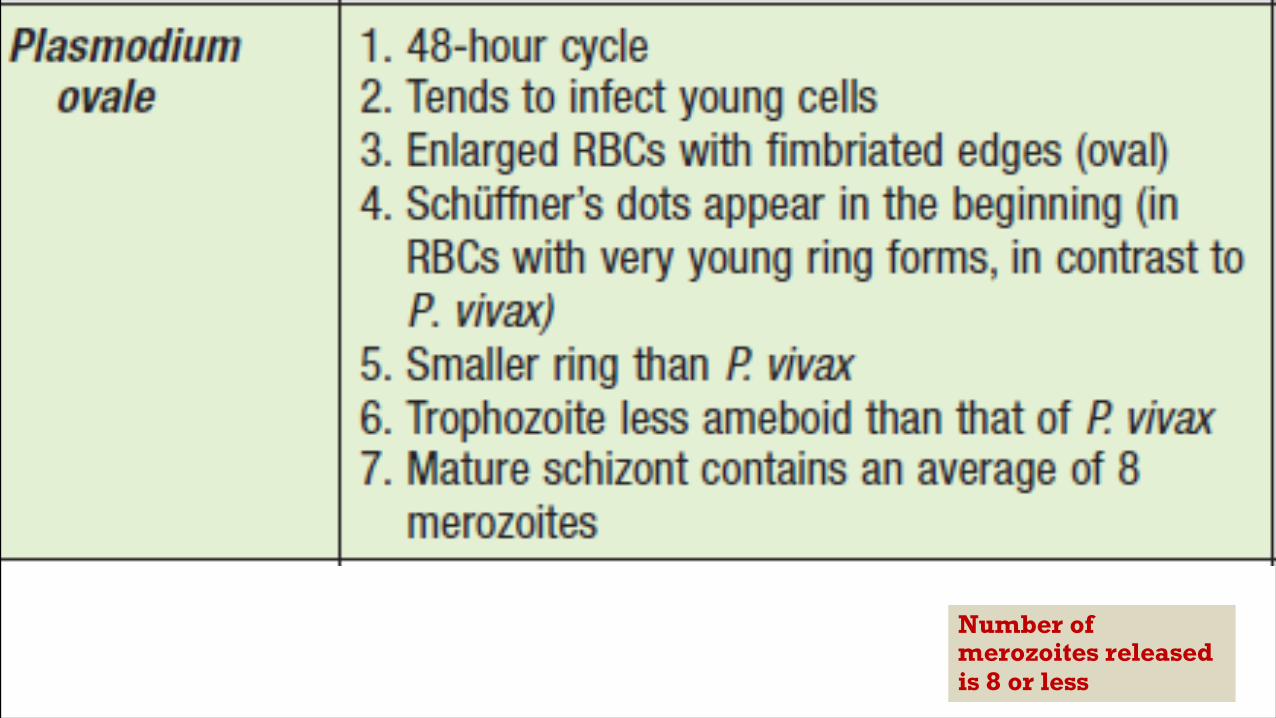
Number of merozoites released is 8 or less
Pathogenesis and Spectrum of Disease:
• TheincubationperiodissimilartothatforP.vivaxmalaria,butthefrequencyandseverityofthesymptoms are much less,witha lower fever and a lack of typical rigors.
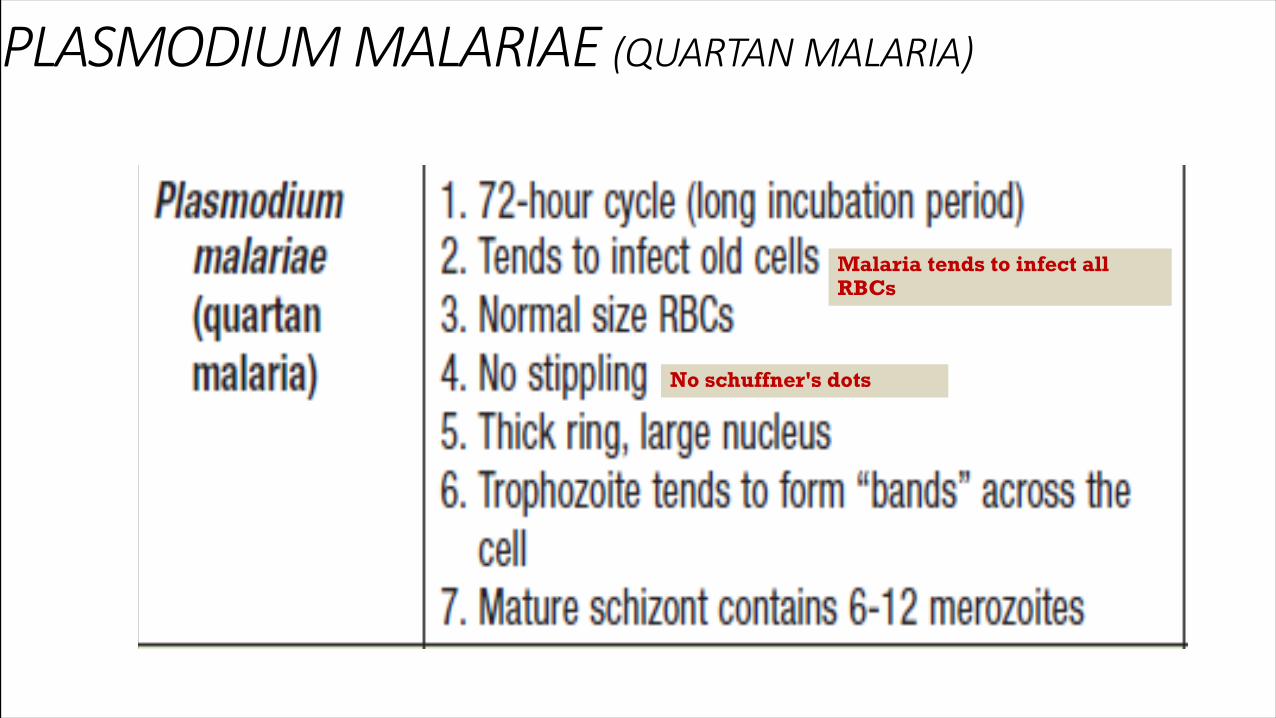
PLASMODIUMMALARIAE (QUARTANMALARIA)
Malaria tends to infect all RBCs
No schuffner's dots
Pathogenesis and Spectrum of Disease:
• ProteinuriaiscommoninP.malariae infectionsandmaybeassociatedwithclinicalsigns ofnephrotic syndrome.
• With a chronic infection, kidneyproblems result from depositionwithin the glomeruliof circulating antigen antibody complexes.
• A membrane proliferative type of glomerulonephritisis the mostcommon lesion seenin quartan malaria.
• Apply kidney functions test for patients with plasmodium malaria to check If there is protein in urine
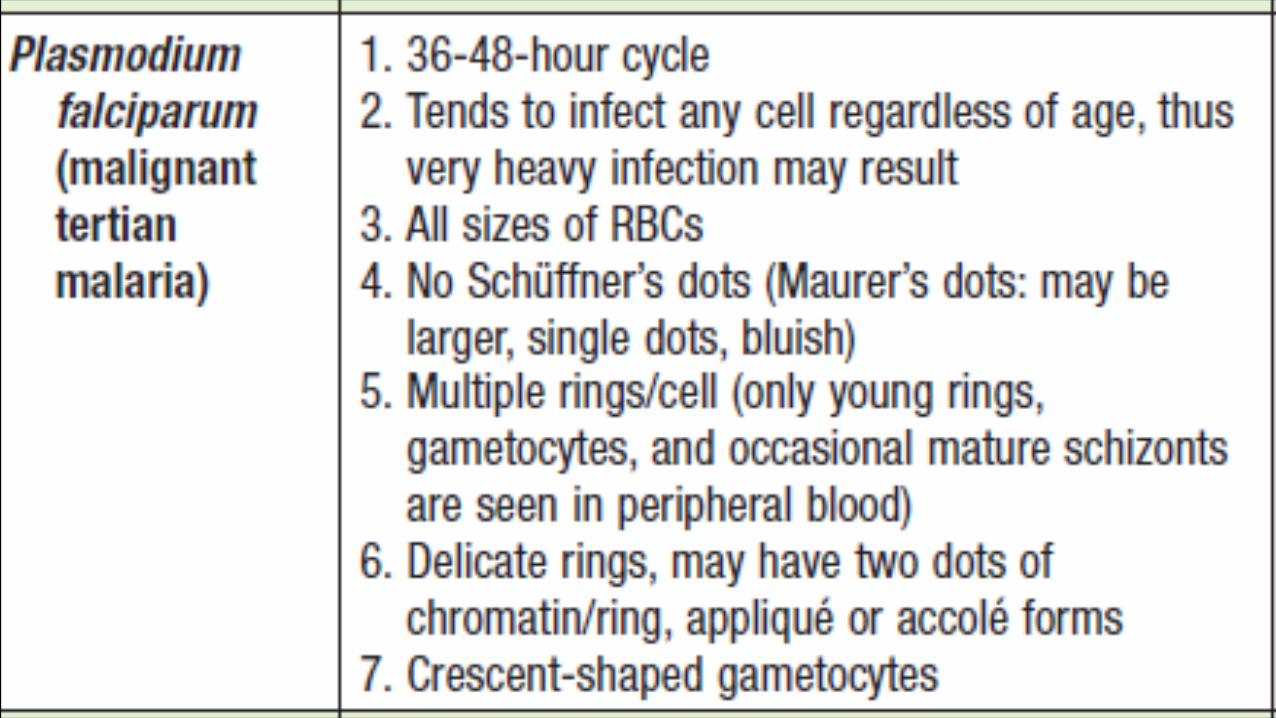
PLASMODIUMFALCIPARUM(MALIGNANT TERTIAN MALARIA)
• Plasmodium falciparum invades all ages of RBCs and sizes . [severe infections may result because the proportion of infected cells may exceed 50%] .
• Schizogonyoccursinthespleen,liver,andbonemarrowratherthaninthecirculating blood.
• Ischemia caused by theobstruction of vessels within theseorgans byparasitizedRBCs will produce various symptoms, dependingontheorgan involved.
High level of parasitaemia
• AdecreaseintheabilityoftheRBCstochangeshape( projecting nopes ) whenpassing throughcapillariesorthesplenicfiltermayleadtopluggingofthevessels Also, only P. falciparum causes cytoadherence, a feature that is associatedwithsevere malaria.
• InP. falciparum infections, as the parasite grows, theRBC membrane becomesstickyandthecellsadheretotheendothelialliningofthe capillaries oftheinternal organs.(spleen ,liver and kidneys).
• Thus,onlytheringformsandthegametocytes(occasionallymature schizonts)normallyappear inthe peripheral blood.
A decrease in the viscosity followed by ischemia,hypoxia then organ failure
Two common complications associated with plasmodium falciparum: 1.cerebral malaria 2. Black water fever ( in kidneys, intravascular hemolysis)
Pathogenesis and Spectrum of Disease
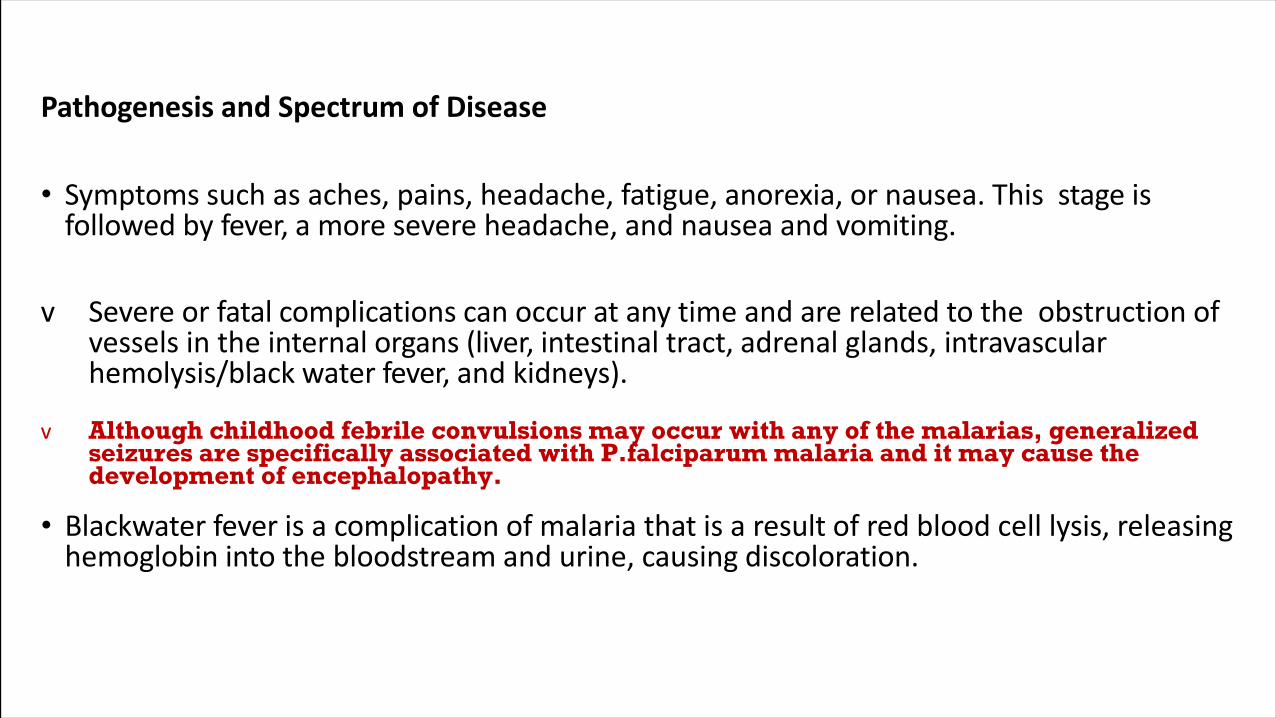
• Symptomssuchasaches,pains,headache,fatigue,anorexia,ornausea.This stage isfollowed by fever, a more severe headache,and nauseaand vomiting.
v Severe orfatal complications can occur at any time andare related to the obstruction ofvessels intheinternal organs (liver, intestinal tract, adrenal glands, intravascularhemolysis/black water fever, and kidneys).
v Although childhood febrile convulsions may occur with any of the malarias, generalized seizures are specifically associated with P.falciparum malaria and it may cause the development of encephalopathy.
• Blackwaterfeverisacomplicationofmalariathatisaresultofredbloodcelllysis, releasinghemoglobin into thebloodstream andurine, causing discoloration.
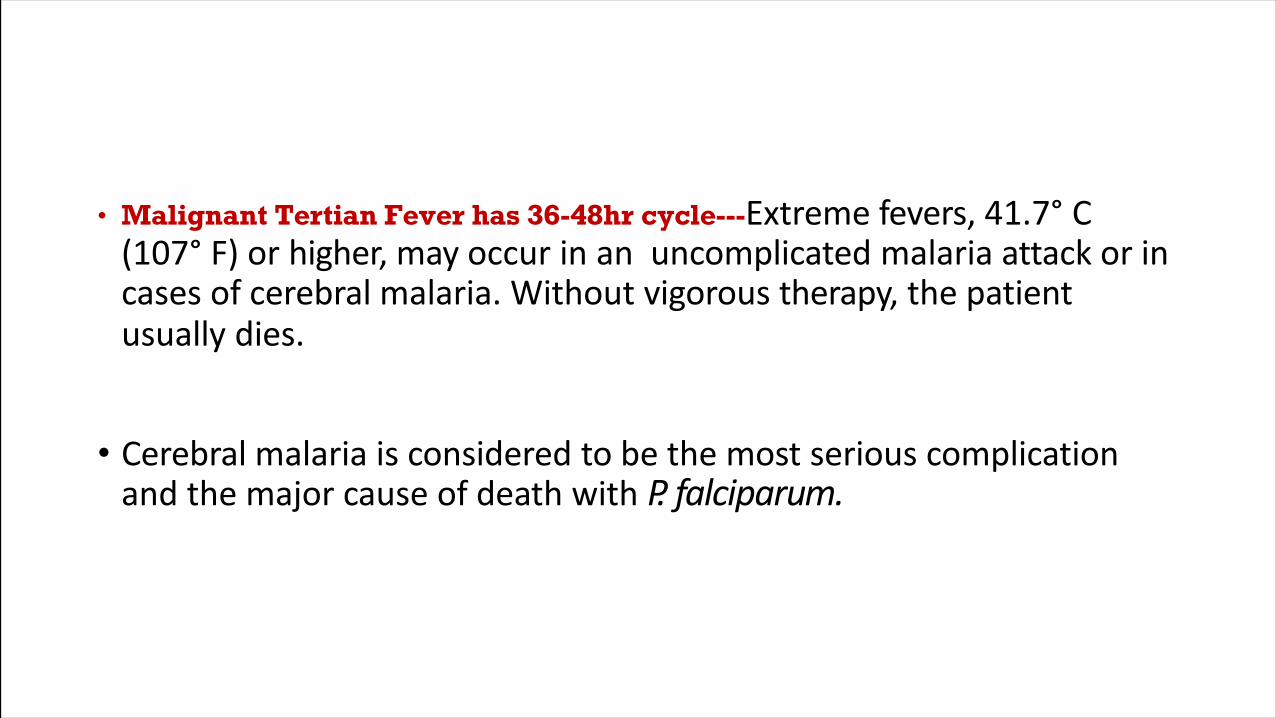
• Malignant Tertian Fever has 36-48hr cycle---Extremefevers, 41.7° C(107° F) or higher, may occur in an uncomplicated malaria attack or incases ofcerebral malaria. Without vigorous therapy, thepatientusually dies.
• Cerebral malaria is considered to be the most serious complicationand the major cause ofdeath with P. falciparum.
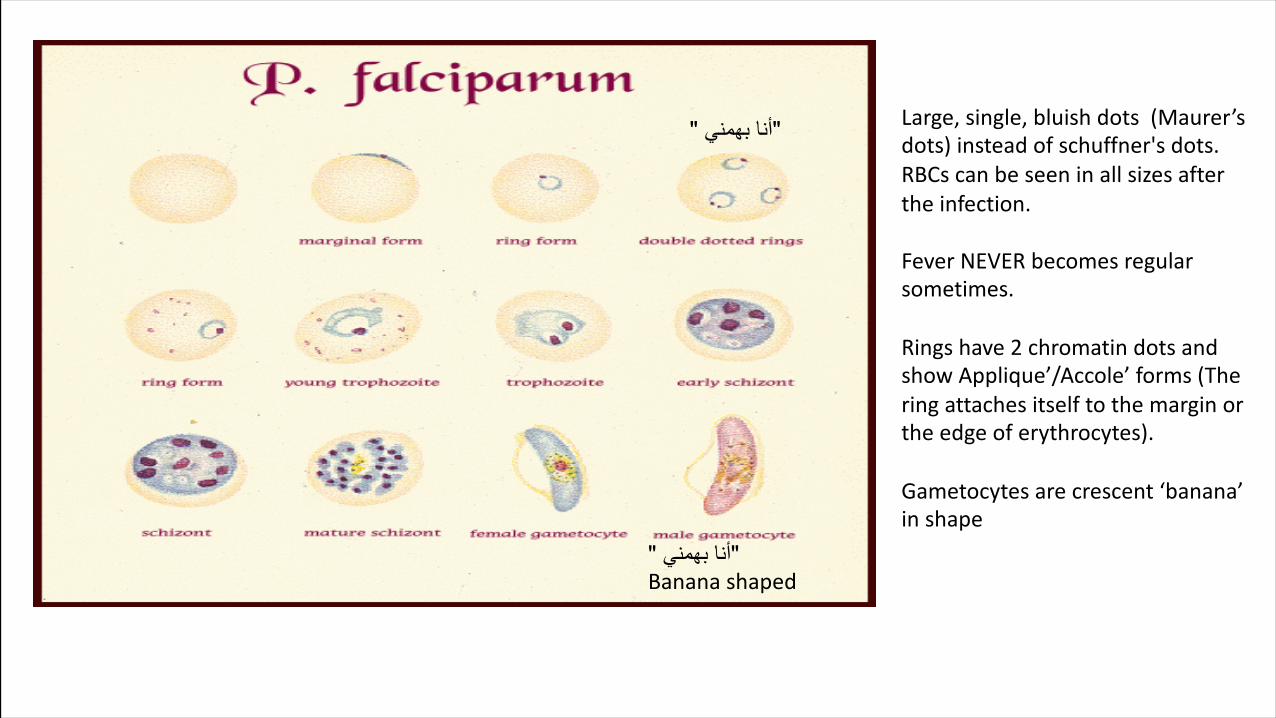
Large,single,bluishdots (Maurer’sdots)insteadofschuffner'sdots.RBCscanbeseeninallsizesaftertheinfection.
FeverNEVERbecomes regularsometimes.
Ringshave2chromatindotsandshowApplique’/Accole’forms(Theringattachesitselftothemarginortheedgeoferythrocytes).
Gametocytesarecrescent‘banana’inshape
" ينمھب انأ"
" ينمھب انأ"Bananashaped
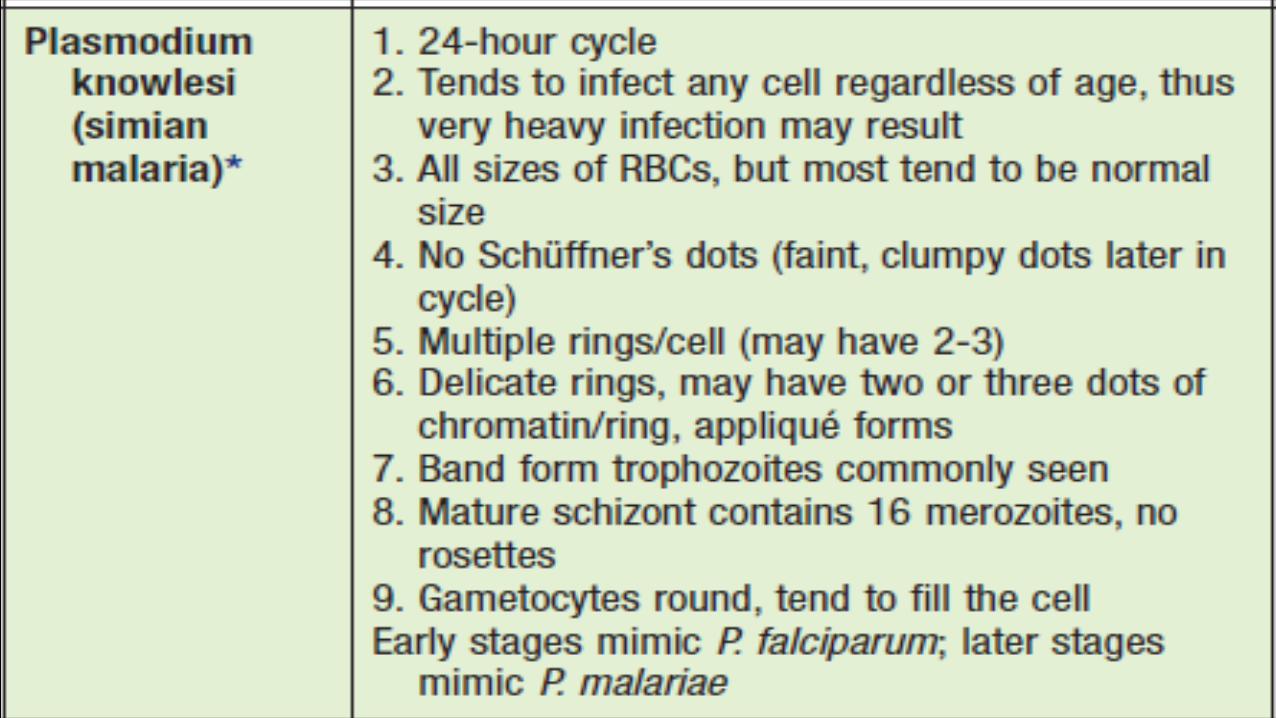
PLASMODIUM KNOWLESI(SIMIANMALARIA,THE FIFTH HUMANMALARIA)
• P. knowlesi invades all ages of RBCs.
• The early blood stages of P. knowlesi resemble those of P. falciparum.
• Whereas the mature blood stages and gametocytes resemble thoseof P.malariae.
• Unfortunately, these infections are often misdiagnosed as the relativelybenignP.malariae;however,infectionswithP.knowlesicanbe fatal.
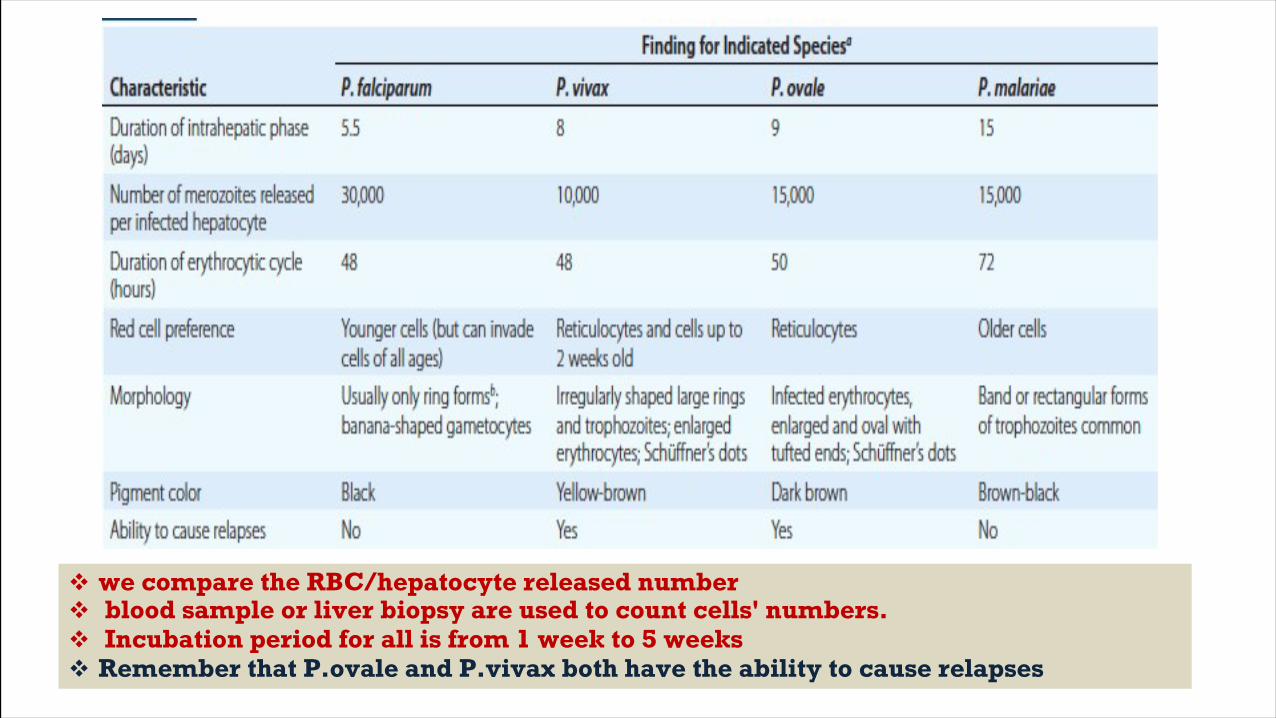
v we compare the RBC/hepatocyte released numberv blood sample or liver biopsy are used to count cells' numbers.v Incubation period for all is from 1 week to 5 weeksv Remember that P.ovale and P.vivax both have the ability to cause relapses
CLINICAL FEATURES• Malariaisaverycommoncauseoffeverintropicalcountries.Thefirstsymptoms ofmalariaarenonspecific;thelackofasenseofwellbeing,headache,fatigue, abdominaldiscomfort,andmuscleachesfollowedbyfeverareallsimilartothe symptoms ofa minorviral illness.
• Insomeinstances,aprominenceofheadache,chestpain,abdominalpain, cough,arthralgia,myalgia,ordiarrheamaysuggestanotherdiagnosis.[But are excluded by their specific symptoms] .
• Although headache may besevere inmalaria, theneck stiffness and photophobia seenin meningitisdonotoccur.Whilemyalgiamaybeprominent,itisnotusuallyas severe asin dengue fever, and the muscles are not tender as in leptospirosis or typhus.Nausea,vomiting, and orthostatic hypotension are common.
• Then patterns start (cycles of 48-72 hrs); The fever that comes on the third to forth day has 3 stages (cold stage with chills and rigors -----hot stage ------sweating stage) then there are two days of feeling well, then the fever attacks again.
• The classic malarial paroxysms, in which fever spikes, chills, and rigors occurat regular intervals, are relatively unusual and suggest infection with P. vivax orP.ovale.
• Thefeverisusuallyirregularatfirst(thatoffalciparummalariamaynever becomeregular);thetemperatureofnonimmuneindividualsandchildrenoften risesabove40Cinconjunctionwithtachycardiaandsometimesdelirium. Although childhoodfebrile convulsionsmay occur with any ofthemalarias, generalizedseizuresarespecificallyassociatedwithfalciparummalariaandmay heraldthe development ofencephalopathy (cerebral malaria).
• Anemia can show (due to hemolysis) but mostly in P.falciparum due to high parasitemia
LABORATORY DIAGNOSIS(ALL SPECIES) Definitive diagnosis by seeing plasmodium in the peripheral blood
1.Routine Methods:
- Thick and thin blood films .
- At least 200to 300oil immersion fields should be examined onboth films before anegative report is issued.
- Stains:1. Giemsa stain.2. Wright’s stain.3. Fluorescent nucleic acid stains, such asacridine orange.
- Blood collected using (EDTA) anticoagulant.
Thick – blood drop Thin – "ةحسم" to see fine details
2.Serologic Methods:
- Several rapid malaria tests (RMTs):
1.Some ofwhich use monoclonal antibodies against the histidine-rich protein 2(HRP2).
2.Whereas others detectspecies-specific parasite lactatedehydrogenase (pLDH).
- These procedures are basedonan antigen captureapproach indipstick orcartridge formats.
3. Molecular Diagnostics:
• OthermethodsincludedirectdetectionofthefivespeciesbyusingaspecificDNA probe after PCR amplification of target DNA sequences.
4. AutomatedInstruments:
• Usingautomatedflowcytometryhematologyinstruments,therearepotentiallimitations related to thediagnosis of blood parasite infections.
THERAPY
• Antimalarialdrugsareclassifiedaccordingtothestageofmalariaagainstwhich they aretargeted.
• QUINOLINES , ARTEMISININS• Tetracycline, doxycycline, and clindamycin are used increasingly in combination with otherantimalarials to improve their efficacy
• For prophylaxis you can take quinolones if you’re travelling to endemic areas like mefloquine
• These drugs are referred to as :
1.Tissue schizonticides (which kill tissue schizonts).2.Blood schizonticides (which kill blood schizonts).3.Gametocytocides (which kill gametocytes).4.Sporonticides (which prevent formation of sporozoites within the mosquito).
All falciparum are resistance to Quinolines "ينمھب يلی وھ اذھ " Because it works on active motile producing form -we use primaqines for hepnozoids
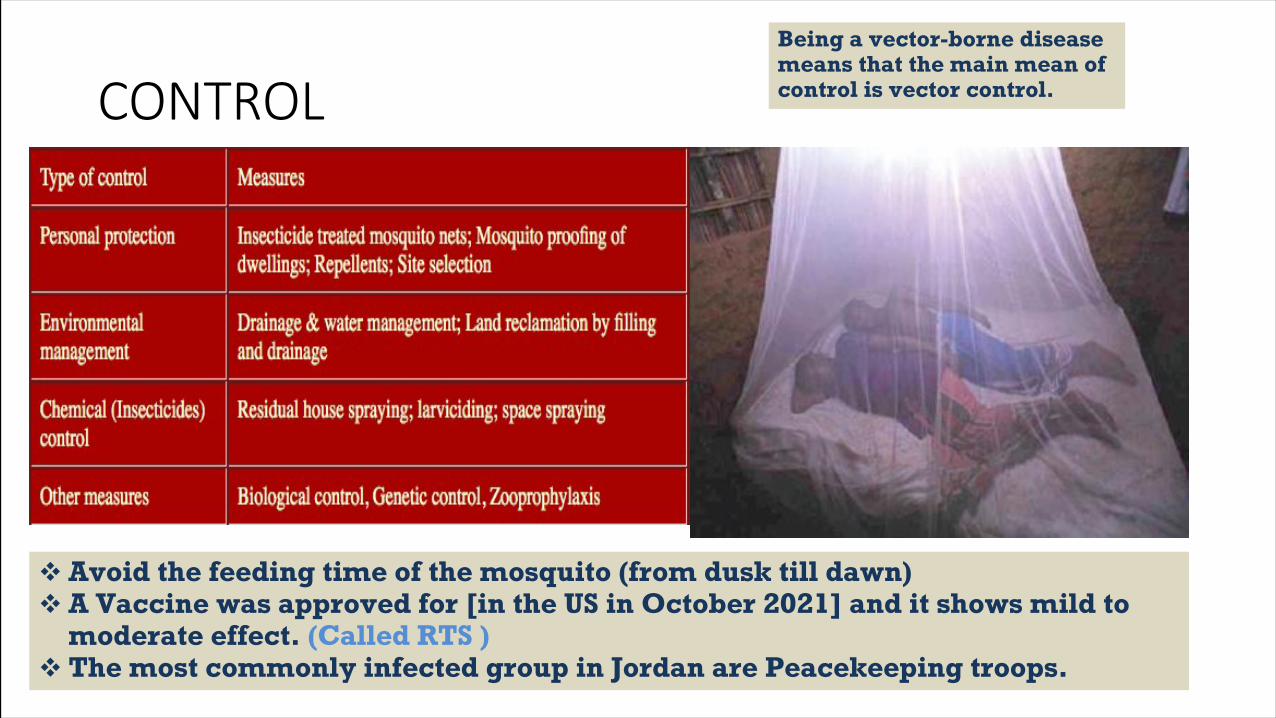
CONTROLBeing a vector-borne disease means that the main mean of control is vector control.
v Avoid the feeding time of the mosquito (from dusk till dawn)v A Vaccine was approved for [in the US in October 2021] and it shows mild to
moderate effect. (Called RTS )v The most commonly infected group in Jordan are Peacekeeping troops.
Babesiosis vector borne • Babesiosisisanemergingtick-borneinfectiousdiseasecausedbyprotozoanparasitesofthe genus Babesia that invade and eventually lyse red blood cells(RBCs).
• MostcasesareduetoBabesia microti.B.microti,aparasiteofsmallrodents,isthemostcommonetiologic agent of human babesiosis
• TheprimarycausativeagentofhumanbabesiosisinEuropeisB.divergens,butBabesia venatorum and B. microti also have been reported.
• The infectiontypically is mild in youngandotherwise healthyindividuals butcan be severe and sometimes fatal inpersons>50 years ofage and inimmunocompromisedpatients.Sporadic caseshave been reported in Europeand the rest of the world.
Modes of Transmission
• B. microti is transmittedto humans primarily by the nymphal stage ofthedeer tick(Ixodesscapularis),thesametickthattransmitsthecausativeagentsofLyme disease . [No exo-erythrocytic cycle; directly to RBCs and their mainstay of pathogenesis is hemolysis ]
• The vectorsfor transmission of B. duncani andB. divergens– like organisms arethought to be Ixodespacificus and Ixodesdentatus, respectively.
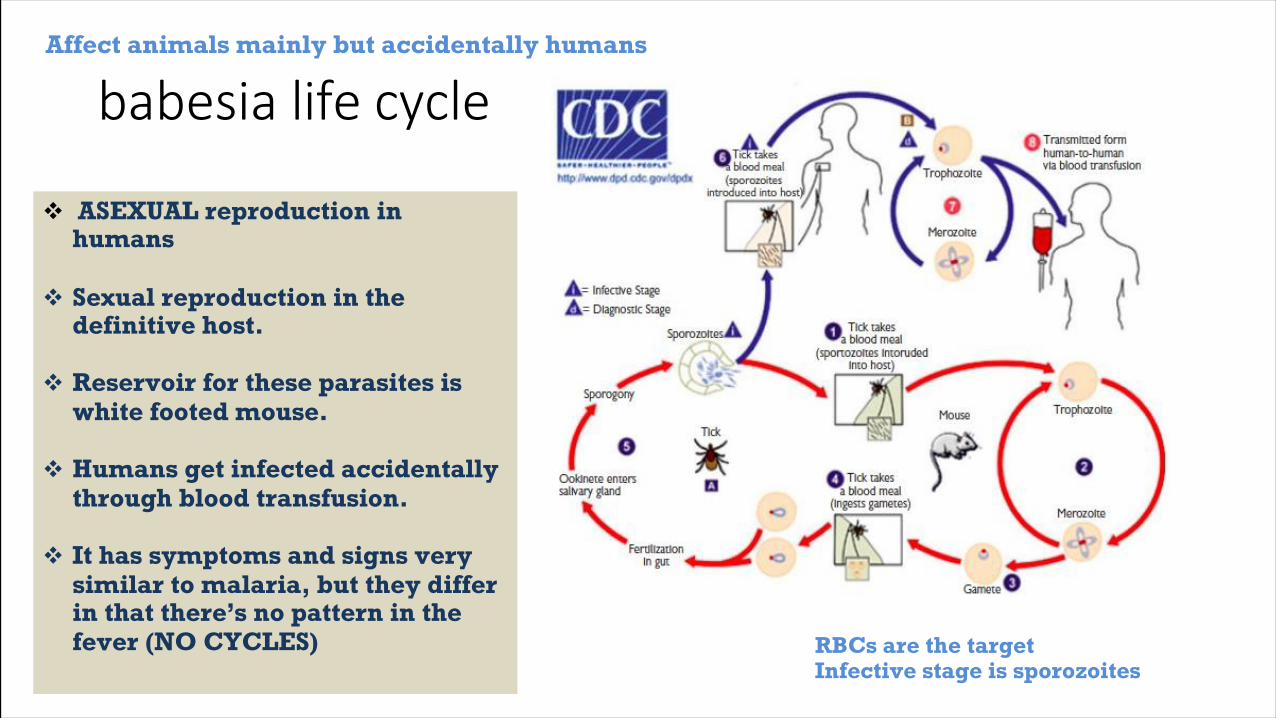
babesia life cycle
v ASEXUAL reproduction in humans
v Sexual reproduction in the definitive host.
v Reservoir for these parasites is white footed mouse.
v Humans get infected accidentally through blood transfusion.
v It has symptoms and signs very similar to malaria, but they differ in that there’s no pattern in the fever (NO CYCLES)
Affect animals mainly but accidentally humans
RBCs are the targetInfective stage is sporozoites
CLINICAL MANIFESTATIONS• AsymptomaticB.microtiInfection:Atleast20%ofadultsand40%ofchildrendonot experience symptoms following B. microti infection.There isno evidence oflong-term complicationsfollowingasymptomaticinfection;however,peoplewhoare asymptomatically infected may transmit theinfection whenthey donate blood.[It mimics malaria starting with non-specific symptoms similar to viral illnesses and then later on fever becomes the chief complaint]
• MildtoModerateB.microtiIllnessSymptomstypicallydevelopfollowinganincubation periodof1–4weeksaftertickbiteand1–9weeks(butaslongas6months)after transfusionofbloodproducts.Patientsexperienceagradualonsetofmalaise,fatigue,and weakness.Fevercanreach40.9Candisaccompaniedbyoneormoreofthefollowing: chills, sweats, headache,myalgia, arthralgia, nausea, anorexia, and dry cough.
• Severe B. microti Illness Severe babesiosis requires hospital admission and typically occurs inpatientswithoneormoreofthefollowing:ageof>50years,neonatalprematurity,male gender,asplenia, HIV/AIDS, malignancy, hemoglobinopathy, and immunosuppressive therapy.
PATHOGENESIS• Anemiaisakeyfeatureofthepathogenesisofbabesiosis.Hemolyticanemiacausedby ruptureofinfectedRBCsgeneratescelldebristhatmayaccumulateinthekidneyand cause renal failure.
• Anemia also resultsfromthe clearance ofintact RBCs as they pass through thesplenicred pulpand encounter resident macrophages.
• BabesiaantigensexpressedattheRBCmembranepromoteopsonizationandfacilitate uptake by splenic macrophages. In addition, RBCs are poorlydeformable asaresult of oxidationgeneratedbytheparasiteandthehostimmuneresponseandarefilteredout as theyattempt to squeeze across the venous vasculature. Bone marrowsuppression duetocytokine production may also contribute to anemia.
DIAGNOSIS
• Microscopic examination of Giemsa-stained thinblood smears
• Polymerase chain reaction (PCR)
• Serologycansuggestorconfirmthediagnosisofbabesiosis.Anindirectimmunofluorescent antibody testfor B. microti is most commonly used.
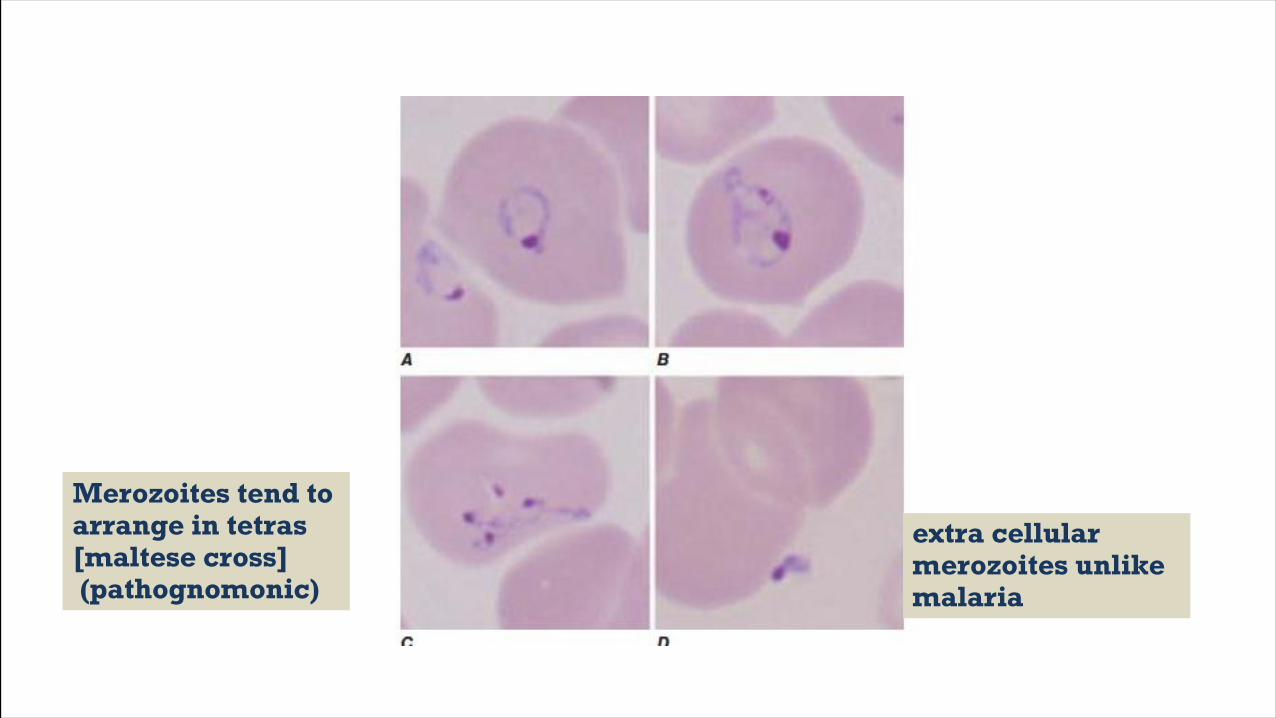
extra cellular merozoites unlike malaria
Merozoites tend to arrange in tetras [maltese cross](pathognomonic)
TREATMENT
• Atovaquone plus azithromycin isthe recommended antibiotic treatmentcombination for mild tomoderate babesiosis.
• Clindamycin plus quinonesisthe choice for severe infections.
Prevention
• Wearclothingthatcoversthelowerpartofthebody,applytickrepellents(suchasDEET)toclothing,andlimitoutdooractivitieswhereticksmayaboundfromMay through October.
The End