Microbiologic Surrogate Endpoints in Clinical Trials-IDSA FDA/IDSA/ISAP Workshop April 15, 2004...
22
Microbiologic Surrogate Endpoints in Clinical Trials-IDSA FDA/IDSA/ISAP Workshop April 15, 2004 Sheldon L. Kaplan, MD Baylor College of Medicine Texas Children’s Hospital
-
date post
21-Dec-2015 -
Category
Documents
-
view
228 -
download
3
Transcript of Microbiologic Surrogate Endpoints in Clinical Trials-IDSA FDA/IDSA/ISAP Workshop April 15, 2004...

Microbiologic Surrogate Endpoints in Clinical Trials-IDSA
FDA/IDSA/ISAP WorkshopApril 15, 2004
Sheldon L. Kaplan, MD
Baylor College of Medicine
Texas Children’s Hospital
Houston, TX

Sridhara et al http://www.fda.gov/www.fda.gov/cder/Offices/Biostatistics/presentations.htm

Sridhara et al http://www.fda.gov/www.fda.gov/cder/Offices/Biostatistics/presentations.htm
Infections For Which Microbiologic Surrogate Endpoints
Are Useful for Clinical Trials
• Group A streptococcus pharyngitis
• Uncomplicated lower urinary tract infection
• Shigella gastroenteritis

Infections For Which Microbiologic Surrogate Endpoints
Are Useful for Clinical Trials• Group A Streptococcus Pharyngitis
-symptoms will resolve regardless of therapy; time to resolution can be compared
-suppurative and non-suppurative complications occur too infrequently to use as endpoints

Infections For Which Microbiologic Surrogate Endpoints
Are Not Useful or Unproven for Clinical Trials
• Skin and skin structure infections
• Pneumonia
• Acute hematogenous osteomyelitis or septic arthritis
• Intra-abdominal infections
• Viral meningitis or encephalitis
Infections For Which Microbiologic Surrogate Endpoints
Are Not Useful or Unproven for Clinical Trials
• Sites of infection are difficult to resample in order to document microbiologic eradication
• Lack of eradication of the organism may not equal clinical failure-VAP and tracheal aspirates
• Eradication of organism may not equal substantial clinical benefit-URI and pleconaril

Infections For Which Microbiologic Surrogate Endpoints
May be Useful for Clinical Trials
• Bacterial meningitis
• Acute otitis media and sinusitis
• VP shunt infections
• Coagulase-negative staphylococcus line-associated bacteremia
• Pertussis

Antimicrobial Drug Development for Acute Bacterial Meningitis
Joint FDA/IDSA/PhRMA Workshop
Imo Ibia, MD, MPH
Medical Officer
FDA/CDER/DSPIDP
November 20, 2002
Office of New Drugs IVOffice of New Drugs IV
Center for Drug Evaluation and ResearchCenter for Drug Evaluation and Research www.fda.gov
Outcomes• Are there data to show bacteriologic outcome is a good
surrogate for clinical outcome?• Would bacterial endpoint alone miss the potential
differential effect of drugs on inflammatory response?• How should clinical success/failure be defined and what
should constitute the primary efficacy population?– ITT or evaluable?
• How best can preclinical and early phase clinical trial data be used in meningitis trials to help address some of these issues?
Imo Ibia 2002 FDA/IDSA/PhRMA Workshop 2002
Evaluations• Timing of repeat lumbar puncture
– Is there data to establish the best time?– What factors could impact that time and how should they be
factored in?
• organism, baseline quantity, drug, host factors
• How many organisms in repeat LP constitute delayed sterilization and what is its utility in trials?
• Few and patient improving, optional (IDSA 1992)
• Quantification of baseline CSF pathogens– How feasible and consistent across multinational sites?
Imo Ibia 2002 FDA/IDSA/PhRMA Workshop 2002

Outcome of Bacterial meningitis
• IDSA Guidelines 1992: Endpoints of -cure -survival with mild neurologic sequelae -survival with severe neurologic sequelae (somewhat
dependent on the observer and some sequelae improve with time) -death• Mortality is low in US• Audiology testing is an objective and quantifiable
measure • As with other sequelae, hearing loss may improve over
time

Ceftriaxone vs Cefuroxime for Bacterial Meningitis in Children
• Prospective, randomized multicenter study • Ceftriaxone (n=53) or cefuroxime (n=53)• Repeat CSF culture at 18-36 hours • No significant differences in clinical
characteristics between the groups at enrollment
Schaad et al N Engl J Med 1990;332:141-7

Ceftriaxone vs Cefuroxime for Bacterial Meningitis in Children
Variable Ceftriaxone Cefuroxime P value
+ CSF culture at
f/up (all Hib)
1/52 6/52 0.112
Hearing loss 2 (4%) 9 (17%) 0.052
Schaad et al N Engl J Med 1990;332:141-7
Ceftriaxone vs Cefuroxime for Bacterial Meningitis in Children
• Hearing loss for H. influenzae type b
Ceftriaxone-2/27 (7%); Cefuroxime-6/35 (17%)
• 2 of 6 children who had hearing loss after cefuroxime therapy for Hib had delayed sterilization of the CSF i.e. 4 did not have delayed sterilization of CSF
Schaad et al N Engl J Med 1990;332:141-7
Ceftriaxone vs Cefuroxime for Bacterial Meningitis in Children
• Hearing loss for S. pneumoniae
Ceftriaxone-0/7; Cefuroxime-2/6
None with hearing loss due to S. pneumoniae had delayed CSF sterilization
Schaad et al N Engl J Med 1990;332:141-7

Ceftriaxone vs Cefuroxime for Bacterial Meningitis in ChildrenHearing Repeat
CSF sterile
Repeat CSF
positive
Total
Normal 90 5 95
Impaired 9 2 11
Total 99 7 106
Sensitivity-90/99=91% Specificity-2/7=29%

Ceftriaxone vs Cefuroxime for Bacterial Meningitis in Children
• Four prospective studies conducted in Dallas-last 3 were dexamethasone trials. None of the studies were direct comparisons
• Ceftriaxone-174; Cefuroxime-159
• No significant differences between the groups at initiation of therapy
Lebel et al J Pediatr 1989;114:1049-54
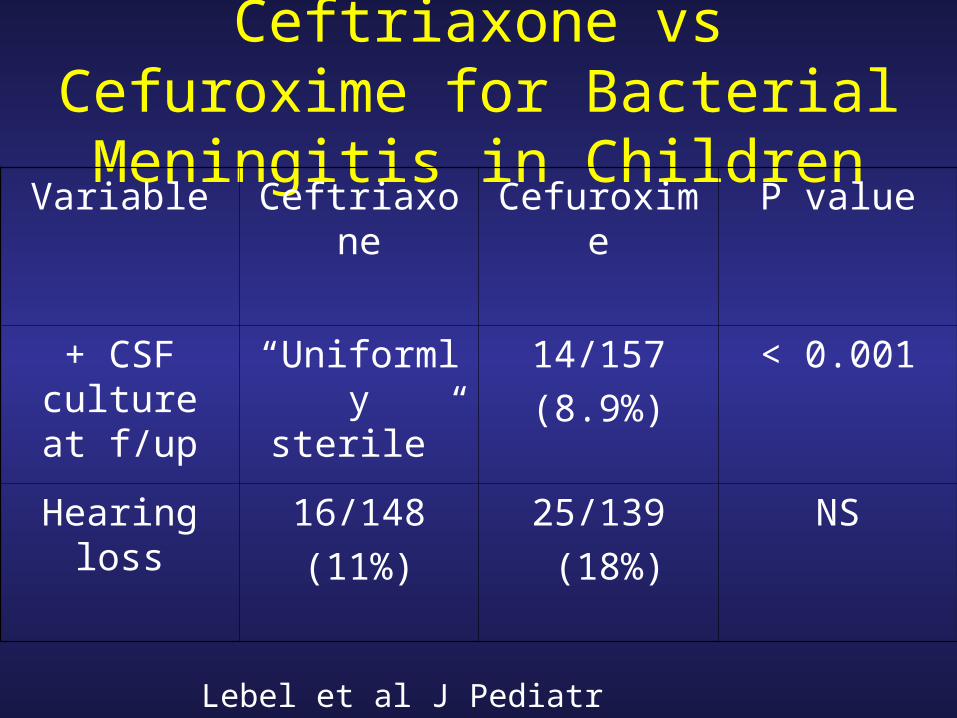
Ceftriaxone vs Cefuroxime for Bacterial Meningitis in Children
Variable Ceftriaxone Cefuroxime P value
+ CSF culture at
f/up
“Uniformly sterile”
14/157
(8.9%)
< 0.001
Hearing loss 16/148
(11%)
25/139
(18%)
NS
Lebel et al J Pediatr 1989;114:1049-54

Meropenem vs Cefotaxime for Bacterial Meningitis in Children
End of Treatment
Evaluable
Meropenem
N=79
Cefotaxime
N=75
Cure 36 (46%) 42 (58%)
Mild sequelae 21 20
Severe sequelae 20 10
2nd CSF sterile 75 (95%) 72 (96%)
2nd CSF delayed sterilization
2
Hib
1
Hib
Odio et al Pediatr Infect Dis J 1999;18:581-90

Trovafloxacin vs Ceftriaxone for Bacterial Meningitis in Children
End of Treatment
Evaluable
Trovafloxacin
N=108
Ceftriaxone
N=95
Cure 53 (49%) 57 (60%)
Mild sequelae 28 21
Severe sequelae 20 13
Failure 5 1
2nd CSF delayed sterilization
5 3
Sáez-Llorens et al Pediatr Infect Dis J 2002;21:14-22

Conclusions
• Not clear how well repeat CSF culture at 24-36 hours after initiation of treatment predicts hearing impairment or
overall outcome (vast majority of patients with severe sequelae have sterile 2nd CSF)
● Not clear if findings for Hib meningitis are applicable to pneumococcal or meningococcal meningitis