Michel Jadoul, Brussels, Belgium Chairs: Pablo Urena ...
15
Phosphate and cardiovascular disease beyond CKD: is phosphate a new cholesterol? Michel Jadoul, Brussels, Belgium Chairs: Pablo Urena Torres, Saint-Ouen, France Carmine Zoccali, Reggio Calabria, Italy Prof. Michel Jadoul Cliniques universitaires St-Luc Université Catholique de Louvain Brussels, Belgium Slide 1 Thank you very much. I want to thank the scientific committee for the opportunity to discuss with you an interesting topic and a rapidly moving field. My topic, as mentioned, is phosphate and cardiovascular disease beyond or in the absence of CKD. Is phosphate a new cholesterol? Slide 2
Transcript of Michel Jadoul, Brussels, Belgium Chairs: Pablo Urena ...
Phosphate and cardiovascular disease beyond CKD: is phosphate a new cholesterol? Michel Jadoul, Brussels, Belgium
Chairs: Pablo Urena Torres, Saint-Ouen, FranceCarmine Zoccali, Reggio Calabria, Italy
Prof. Michel JadoulCliniques universitaires St-Luc
Université Catholique de LouvainBrussels, Belgium
Slide 1
Thank you very much. I want to thank the scientific committee for the opportunity to discusswith you an interesting topic and a rapidly moving field. My topic, as mentioned, is phosphateand cardiovascular disease beyond or in the absence of CKD. Is phosphate a newcholesterol?
Slide 2
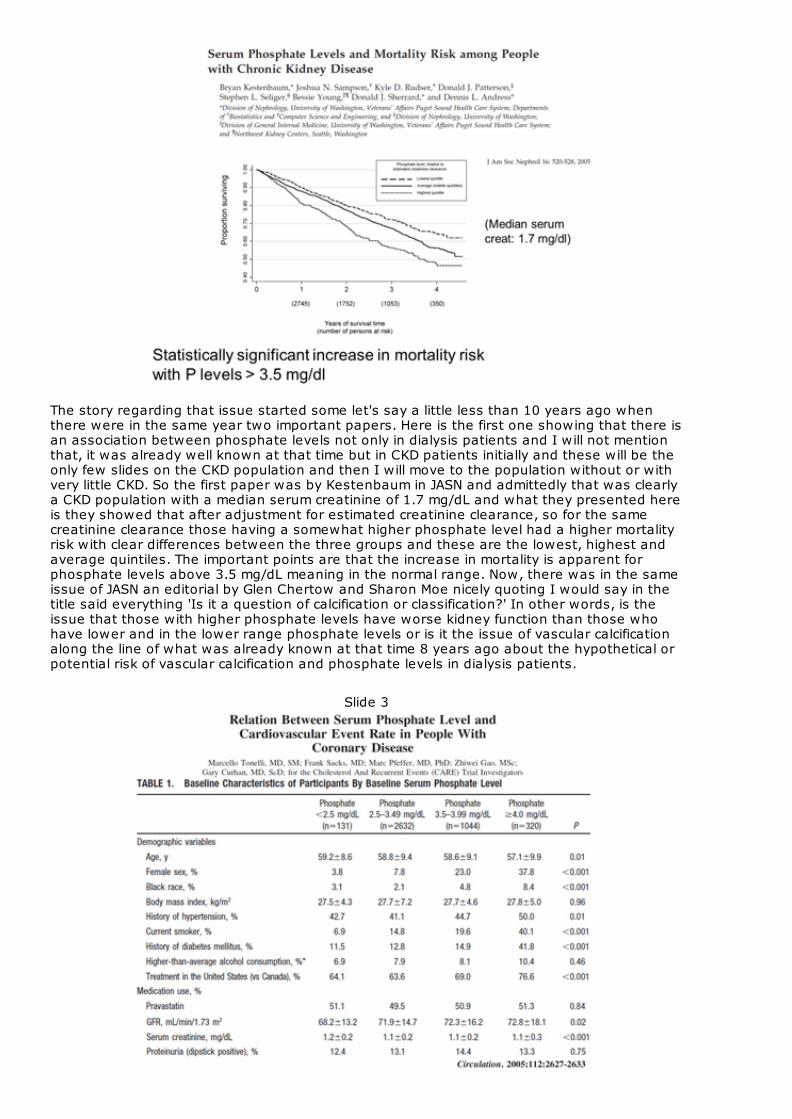
The story regarding that issue started some let's say a little less than 10 years ago whenthere were in the same year two important papers. Here is the first one showing that there isan association between phosphate levels not only in dialysis patients and I will not mentionthat, it was already well known at that time but in CKD patients initially and these will be theonly few slides on the CKD population and then I will move to the population without or withvery little CKD. So the first paper was by Kestenbaum in JASN and admittedly that was clearlya CKD population with a median serum creatinine of 1.7 mg/dL and what they presented hereis they showed that after adjustment for estimated creatinine clearance, so for the samecreatinine clearance those having a somewhat higher phosphate level had a higher mortalityrisk with clear differences between the three groups and these are the lowest, highest andaverage quintiles. The important points are that the increase in mortality is apparent forphosphate levels above 3.5 mg/dL meaning in the normal range. Now, there was in the sameissue of JASN an editorial by Glen Chertow and Sharon Moe nicely quoting I would say in thetitle said everything 'Is it a question of calcification or classification?' In other words, is theissue that those with higher phosphate levels have worse kidney function than those whohave lower and in the lower range phosphate levels or is it the issue of vascular calcificationalong the line of what was already known at that time 8 years ago about the hypothetical orpotential risk of vascular calcification and phosphate levels in dialysis patients.
Slide 3

Now the same year, the third speaker of this session Professor Tonelli published a post-hocanalysis of the CARE study which as you'll remember, randomised patients to Pravastatin orplacebo. You have here the breakdown of the 4 groups with phosphate below 2.5mg/dL, 2.5-3.5mg/dL, 3.5-3.99mg/dL and above 4mg/dL. You will note that there are differences inseveral respects between these four groups but importantly below well as you would expect50% of the patients were under pravastatin average but GFR average was 68ml/min,71ml/min, 72ml/min, slight differences between groups significant but not impressive. Serumcreatinine was 1.1- 1. 2 mg/dL and they had importantly in that study also a dipstick anddipstick was only positive in 12-14% for proteinuria.
Slide 4
The results still were I would say along the same line as the previous study, an impressiveincrease of the risk of all-cause death, coronary death or non-fatal MI, new CHF or fatal andnon-fatal MI where a dose-dependent let's relationship has a function of phosphate afteradjustment for a number of other confounders.
Slide 5
Then some other groups moved the topic a step further or some steps further and the groupof Alan Collins at USRDS published some years later that paper entitled 'Serum phosphorous

levels associated with coronary atherosclerosis in young adults' and the strength of thatstudy is that the mean age at inclusion in those over 5000 people was 25 years. In 3 UScities the phosphate level was measured in the late 80s and many of those people, not all ofthem, returned 15 years later. They had calcium scoring together with fortunately, an initialphosphate level available in the vast majority of them.
Slide 6
Along I would say the same line but here as you have noticed these were really young guys,along the same line there was an association that becomes significant here somewhere inthe range of 4 mg/dL, the calcium score above 100, the risk is increased already whenphosphate is still within the normal range.
Slide 7
You can imagine that those young guys, there were few patients with CKD and here are the

overall results from the same paper. On the top, overall population and below after exclusionof the few patients with a GFR below 60 ml/min and you will notice that the association withphosphorous level of coronary calcification. It's virtually the same picture even though there isno association with calcium or calcium phosphorous.
Slide 8
Very recently another group from Brazil published another interesting study much smaller butthey had importantly elective coronary angiography and a creatinine clearance above 60ml/min. There are two outcomes or two endpoints for that study: one is an Agatston score ofabove 10 so meaning significant coronary calcification. The other one is a Friesinger score andfor those of you who are not familiar with the coronary lesions it's a way of measuring theextent of coronary stenosis.
Slide 9

Here is the result of the logistic regression of the risk of having an Agatston score above 10and you will notice that phosphorous is among others with age like you would expect olderage, male gender, hypertension, diabetes even though it's borderline significant but not PTHand FGF23, there is an independent association with phosphate.
Slide 10

Here for coronary stenosis and no longer calcification, the same is true even though it's muchless significant but it's still significant even though here FGF23 again is independentlyassociated together with a number of other factors.
Slide 11
Now I must confess that when reviewing the literature in that respect, it's not a consistentfinding in all studies and I will show briefly two. And of those two the first one is a prospectiveobservational study of 3381 men in their 60s and 70s without history of MI or stroke with amean eGFR 72 ml/min who were followed up for 11 years published some weeks ago,
Slide 12
in fact only on the web meaning that it's hard and poorly readable because of that ATVBthat's the name of the journal visible on the proofs that I downloaded I apologise for this. Buthere the message is that for CVD events, coronary heart disease there is no association withphosphate for stroke, no association. For cardiovascular death, there is some association butafter exclusion of CKD patients and other determinants there is no longer a significantassociation for major CVD events similarly. In fact, if you look at the paper at what is a

cardiovascular event here whereas there is no association with CHD and stroke, you will findthat it's mostly borderline that associates due to aortic aneurism surgery, peripheral vasculardisease, cardiomyopathy or pulmonary heart disease in other words a mix of little bit ofvarious items that may be unrelated to each other in my opinion.
Slide 13
If you then look at the link with the total mortality still serum phosphate is significantlyassociated like alkaline phosphatase. I will not discuss that for the sake of time.
Slide 14
The last slide I'll show in that respect is again a recent one on calcium phosphate and risk ofcardiovascular events and all-cause mortality. Again of course, a different population. 1200subjects who had 3 weeks rehabilitation after an acute cardiovascular event, mostly maleswith an average age of 62 and they had creatinine calcium and phosphate measured at theend of rehabilitation before starting the follow-up. We learned from the paper that thecreatinine clearance was above 60-95% and the follow-up was 8 years.
Slide 15

Here a smaller number of items but still long follow up and you have virtually with phosphateno association so the finding has not been completely consistent.
Slide 16
Last, sorry I forgot I had another one which is a recent one from AJKD from the osteoporoticfractures in men study which looked at something complementary.
Slide 17

Firstly, they showed like the previous ones I've shown, a dose-dependent let's sayrelationship for all-cause mortality and annual cardiovascular mortality with phosphate levels.Especially here for cardiovascular mortality as you can see but they interestingly showed thatthere is no relationship between cardiovascular mortality and urine phosphorous overcreatinine ratio or the fractional excretion of phosphate, which may be of interest of course,because of the hormones involved in the regulation of phosphate.
Slide 18
Now, after having shown a number of observational studies, you might wonder what themechanisms are and if there is a mechanism and it's not residual confounding and due toother factors what are the potential mechanisms and I must say that in that respect it's acomplex topic. I'm not a super expert; we may discuss it in a few minutes but it's a verycomplex topic. I would just point to one important study, even though as you will note it'sonly 11 patients. It was published in JASN some 4 years ago and the title is 'Dietaryphosphorous acutely impairs endothelial function'.
Slide 19

The baseline characteristics of those 11 healthy male Japanese subjects are here, aged 24average and they were given in random order double blind but still they had I guess strikinglydifferent breakfasts with 400 or 1200 mg of phosphate. We are even told that it wasconsumed over 7-14 minutes.
Slide 20
The next slide gives you the main results of that part of the paper where you will notice thatwhen they had the 1200 mg of phosphate diet, well as you would expect phosphateincreased as compared with baseline and there is a correlation between the vasodilatation,so impaired vasodilatation meaning worse endothelial function. There is a correlationbetween the impaired vasodilatation and the change in phosphate level. Now of course, as Imentioned, this is a nice study but in 11 subjects that has not yet been repeated to the bestof my knowledge.

Slide 21
The authors are of course, enthusiastic about that. They have proposed a number ofpotential explanations that I will not discuss and I'm not a lab scientist and I will not discussthe potential pathways that may link phosphate to endothelial dysfunction and eventuallycardiovascular disease.
Slide 22

Now the topic of today was probably proposed by the organising committee, was probablysuggested by that paper establishing somewhat an analogy between phosphate andcholesterol. Now if you think about that there are similarities, both are essential for life, forcell membranes, for energy metabolism and a number of other aspects. Both have increasedin our typical Western dietary intake but there are genetic determinants. Both are found inexcess in pathologic samples, in lesions and both correlate, associate with vascular diseasewithin the range considered normal in the West. Eventually, last both change the phenotypeof cells found in vascular lesions but we should not forget that that is true in vascular lesionsonly at hyperphosphatemic levels and not within the normal range. Now still there are twomajor differences between phosphate and cholesterol and those differences are that there isa much tighter hormonal control for phosphate than for cholesterol number one. Number twointerestingly we should keep in mind that the normal range for phosphate is higher in childrenthan in adults even though children have no cardiovascular disease because of their ageamong others but I mean that should at least put into perspective the hypothetical analogybetween phosphate and cholesterol.
Slide 23

If you then want to discuss the potential mechanism, I will refrain from that and perhapsfinish a little bit early because there are so many. I will try to summarise what we could do forthe next steps and probably at the end of the symposium after the presentation of ProfessorZoccali and Professor Tonelli but I mean there are so many, as you know stimulatory factorson this slide even though if we take only those actors: phosphate, calcium, bone, FGF23, PTH,parathyroid cells, the gut, the kidney and the vitamin D system.
Slide 24
So I think I would suggest as take home messages that in observational studies, I haveshown you several a high normal or normal but on the high side phosphate level associatedwith coronary calcification. In some studies with atherosclerosis or atheroma burden withcardiovascular events and mortality. That was in the absence of CKD in several or in some ofthese studies or at least adjustment for CKD present in a minority did not change the resultsthat much even though residual confounding in any observational study will remain apotential concern. Second, that the mechanisms of the association are complex. If there iscausality which is not proven at all, it may be direct or indirect, you can speculate about whatI've mentioned briefly and what was suggested by the investigators along the progression ofthe mind of the studies I've shown. I wasn't able to show all of them but I've shown severalimportant ones, there have been others and I apologise for having been unable to show allof them.
Slide 25

The second part of my take home messages would be that the role of the actors FGF23, PTH,the bone vascular access, calcium and others, clearly further studies are required,observational, experimental not to say interventional in humans and that's a different topicand probably we may turn back to that after the talk of professor Tonelli. So we have knownfor decades that cholesterol is a well-known cardiovascular risk factor. As you have seen inthe last part of my talk phosphate shares some interesting characteristics with cholesterol.There are also important differences and whether intervention, especially in the populationI've mentioned in the absence of CKD could reduce the risk remains to be investigated. Thankyou for your attention. I was told that because there is some recording I should leave theslides so I will leave the slide, so the recording goes on.