
MHP Quality Metrics - transfusionontario
33
MHP – Quality Metrics Avery B. Nathens MD PhD, Surgeon-in Chief Sunnybrook Health Sciences Centre
Transcript of MHP Quality Metrics - transfusionontario

MHP – Quality Metrics
Avery B. Nathens MD PhD, Surgeon-in Chief
Sunnybrook Health Sciences Centre

2
Objectives
• Develop key quality metrics that are easily measured
and comparable
• Identify set targets for measureable patient outcomes
• Discuss options for formal provincial reporting
April 30, 2018

3
Dimensions of Quality
Accessible
• Right care at the right time
Effective
• Evidence based practices
Safe
• Avoid harm
Patient centred
• Needs and preferences of the patient
Equitable
• Same level of care for every patient
Efficient
• Maximize resource use, minimize waste
4
Structure Process
Outcome
• Was medicine
properly
practiced?
• Staff, physical
resources, policies
• Modifiable
Donabedian approach to quality
assessment

5
What is a good quality indicator?
• Important
– Must apply to a large number of patients OR
– Involve a high risk condition
• Scientifically acceptable
– Reliable – same result on repeated measures
– Valid – does it measure what its supposed to measure
• Feasibility
– Data must be readily available (opportunity costs)
• Usability
– Must be understood by intended audience to ensure PI can
happen
• Modifiable
April 30, 2018

6 April 30, 2018
Provincial reporting:
challenges

7
MHP Policy Effective care
• Hospitals should have a protocol to guide the
management of the severely bleeding patient
– Structural measure
• Hospitals should have a multidisciplinary QA committee
to review MHP activation
– Structural measure
April 30, 2018
…. ….that reports to the hospital Quality of Care
Committee [MAC]

8
Kaizen

9
Benefits of standardization
• Clarifies the process
• Documents the best way to achieve a goal
• Reduces variation
• Facilitates training
• Provides the baseline for improvement

10
Act
Plan
Do
Check

11
TXA administration
Effective care
• The proportion of patients receiving 2 g of tranexamic
acid within 1 hour of injury/onset of hemorrhage
– Process measure
– Modifiable
• Should it be time of onset of hemorrhage/injury or
recognition of hemorrhage – not usable in current form
• Is it 2 gm or first dose of TXA?
• Suggested: The proportion of patients receiving 1 g of
tranexamic acid within 30 min of activation of MHP
• Amenable to provincial reporting
April 30, 2018
12
Timely transfusion Accessibility
• The proportion of patients issued red cells either before
or within 10 minutes of protocol activation
• Process measure
– Is “issuing blood” the relevant measure?
• Blood might be issued and take 30 min to get to the patient
– Should it be time to bedside? Time to transfusion?
– Consider: The proportion of patients in whom transfusion is
initiated within 15 min of protocol activation
– Modifiable, measurable, relatively independent of case mix –
acceptable for provincial reporting
April 30, 2018

13
Hemorrhage control
Access
• The proportion of patients (of patients requiring transfer
for definitive care) with initiation of call for transfer within
15 minutes of protocol activation
– Process measure
• Modifiable? – very tight window, context dependent
• Activation might precede identification of source of
hemorrhage
– Might be faster to treat locally then transfer patient
• Acceptable for internal QI, not for provincial reporting
• Suggest extend window to an hour
April 30, 2018
14
Timely access to hemorrhage
control
• Additional consideration
• The proportion of patients with initiation of hemorrhage
control (where possible) within 60/90(?) min of protocol
activation
– Time to operative intervention, time to angioembolization,
endoscopic control, etc
– Modifiable, independent of case mix
• Acceptable for provincial reporting
April 30, 2018

15
Is one hour reasonable?
• PROPPR Study – 28 min to operating room
• Haas and Nathens, J Am College of Surgeons, 2009
– Time to OR among patients with penetrating truncal injury
presenting with shock – 1 hour in trauma centres, 50 min
in non-trauma centres
April 30, 2018

16
Pelvic angioembolization
TQIP experience
• Time to angiography from ED arrival among patients who
had this as their FIRST intervention
• Median 3.1 hours, most (75%) between 2-4 hrs; 1%
within 30 minutes
• Non-teaching hospital – 33 minutes quicker
• Higher volume centers (>10 per year) - 20 min shorter
17
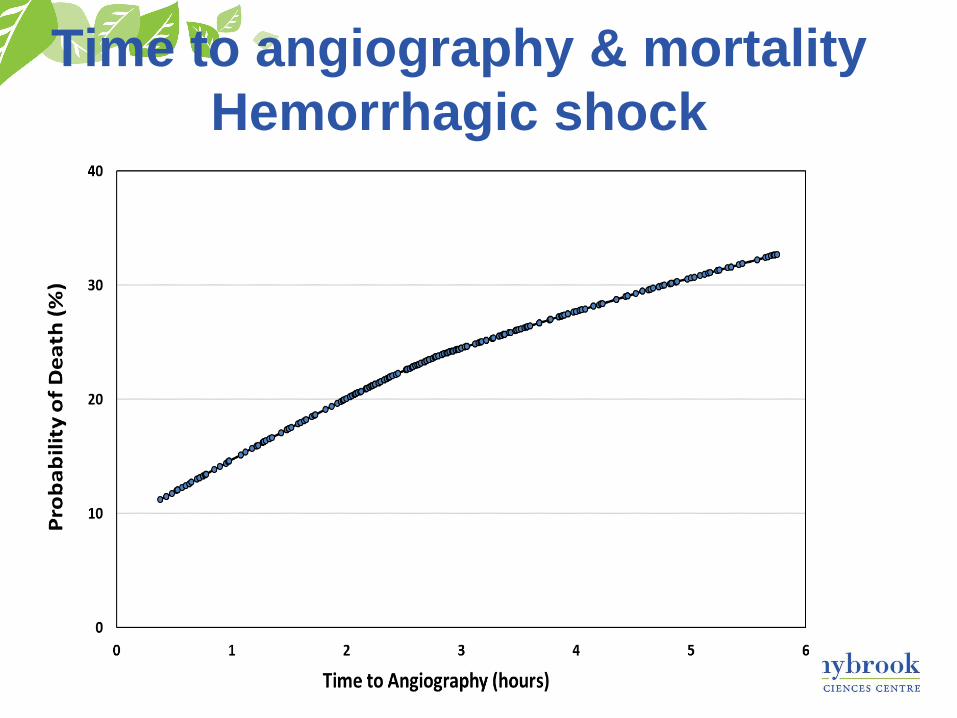
Time to angiography & mortality
Hemorrhagic shock

18
Management of hypothermia Safe, effective care
• The proportion of patients achieving a temperature
>35⁰C at termination of the protocol
– Outcome measure
– Modifiability a challenge
– Risk adjustment would be necessary for provincial
reporting • GI bleed vs obstetrical hemorrhage, vs traumatic hemorrhage
• Dependent on exposure, extent/volume of resuscitation
• Acceptable for internal QI, not for provincial reporting
April 30, 2018

19
Transition to group specific
blood - efficiency
• The proportion of patients transitioned to group specific
blood within 90 minutes of arrival/onset of hemorrhage
– Process measure
• Needs more precision to ensure reliability and
usability….within 90 minutes of MHP activation
• Reflects ability of the provider(s) to obtain blood sample
& timely submission to lab
• Independent of case mix
• Case mix independence, modifiability suggest an
appropriate indicator for provincial reporting
April 30, 2018

20
Hemoglobin targets
• The proportion of patients with hemoglobin levels
maintained between 60-110 g/L during protocol activation
– Outcome measure
• Ability to achieve this target highly dependent on:
– Rate of bleeding (case mix)
– Ease with which hemorrhage control can be achieved (case
mix +/-)
– Turnaround time of labs (modifiable)
– Use of lab data (modifiable)
• Given case mix issues, not ideal for provincial reporting but
might have value for internal QI
April 30, 2018
21
Avoiding wastage
Efficient care
• The proportion of activations without any blood product
wastage (including plasma that is thawed and not used
within the 5 day limit on another patient)
– Outcome measure
• Some modifiability on the provider’s part but potentially case
mix dependent - early death, early hemorrhage control
• Incentivizes administration of product when it might not be
necessary
• As written, brings in other case mix issues (plasma thawed
to be used on another patient)
• Might be acceptable for internal QI only
April 30, 2018

22
Appropriateness of MHP activation Effectiveness, Efficiency
• The proportion of patients with appropriate activation
(non-survivors with hemorrhagic death transfused <6
units and patients transfused >6 RBC units)
• Process measure
• Needs element of time….within 4 hours
• True positive: activation among those who received>6
units in 4 hours or activation among those who received
transfusion yet died with hemorrhagic death within 4
hours
• False positive: activation among survivors who received
<6 units in 4 hrs
April 30, 2018
23
Appropriateness
• Appropriateness becomes the positive predictive value:
April 30, 2018
• PPV is influenced by case mix (prevalence)
• Not ideal for province wide reporting; good for internal
use and to track over time within specified populations
– E.g. trauma vs obstetric vs surgical

24
Appropriateness
April 30, 2018

25
Appropriateness
• What happens if we never activate MHP and we should?
• Balancing measure would be “Negative predictive value”
April 30, 2018
• TN = very large, undifferentiated population
• TN=any transfused patient? Any transfused patient
meeting specific criteria?
• Province wide reporting would be challenging
26
Appropriateness
• As part of the MHP quality assurance process, reviews
should be undertaken for every patient in whom MHP is
activated and for every patient who receives >6 units of
pRBC’s within 4 hours in whom MHP is not activated
• Reviews should address
– Appropriateness of activation (or lack of activation)
– Timeliness of activation and termination
– Administration of products and adjuncts (Ca, TXA)
– Avoidance of hypothermia
– Timeliness of hemorrhage control/transfer
April 30, 2018

27
Do quality indicators improve
care
• Providers need to have confidence in the data, its validity
and there must be a perceived component of
modifiability
• Most provincial reports get little air time
– No confidence
– Data reviewed in wrong forum
• Even if the data are correct and there is opportunity for
improvement, most don’t know how to affect change
April 30, 2018

28
NATIONAL SURGICAL QUALITY
IMPROVEMENT PROGRAM (NSQIP)
April 30, 2018

29
NSQIP Experience
• VA NSQIP
– Mortality: 3.16% to 1.7%
– Morbidity: 45% lower
• ACS NSQIP (2005-2008)
– Morbidity: 82% of centers improve
– Mortality: ~66% of centers improve
– Improvements identified in all groups
• High, low, and average performers
• Low performers improved the most

30
Quality Collaboratives
• Accelerate improvements
• Peers hold others
accountable for change
• Goal setting, sharing of
ideas, resources
• Sharing of successful
change strategies

31 April 30, 2018

32
Summary
• Several QI indicators acceptable for provincial reporting
– Current MHP policy
– TXA administration
– Timely transfusion
– Timely access to hemorrhage control
– Transition to group specific blood
• Others built into internal QI process with mandate for
review
• Empower providers to affect change through collaboratives
April 30, 2018

33
Excellence is a journey, not a
destination











![Mhp Gold The Automated Mhp Mgr[1].Revised](https://static.fdocuments.in/doc/165x107/55c343e3bb61ebe9438b45a3/mhp-gold-the-automated-mhp-mgr1revised-55c4568e3551f.jpg)






