Metabolic Syndrome & CKD
59
Risk Factors in CKD Risk Factors in CKD Tevfik Ecder, MD Istanbul Faculty of Medicine Department of Internal Medicine Division of Nephrology
Transcript of Metabolic Syndrome & CKD

Risk Factors in CKDRisk Factors in CKD
Tevfik Ecder, MDIstanbul Faculty of Medicine
Department of Internal MedicineDivision of Nephrology

••
Therapy of uremia is wholly palliative.Therapy of uremia is wholly palliative.••
If a patient is depleted of salt and water, saline solution shouIf a patient is depleted of salt and water, saline solution should be ld be
infused.infused.••
The chief indication for active treatment of acidosis is the The chief indication for active treatment of acidosis is the
presence of distressing hyperpnea.presence of distressing hyperpnea.••
Tetani is an indication for intravenous calcium therapy.Tetani is an indication for intravenous calcium therapy.
••
The only effective treatment for the anemia is transfusion.The only effective treatment for the anemia is transfusion.••
When cardiac insufficiency complicates the uremic state, it is When cardiac insufficiency complicates the uremic state, it is
unwise to bleed a uremic patient with anemia unless there is a unwise to bleed a uremic patient with anemia unless there is a grave emergency.grave emergency.
••
In recent years the use of peritonal lavage or of some form of tIn recent years the use of peritonal lavage or of some form of the he soso‐‐called artificial kidney has been recommended in the called artificial kidney has been recommended in the
treatment of uremia.treatment of uremia.
Cecil Textbook of MedicineCecil Textbook of Medicine 19511951

( X 1000 )
( X 1000 )
8 63 159 272426
695
1,065
2,095
0
500
1000
1500
2000
2500
1970 1975 1980 1985 1990 1995 2000 2010
Dialysis Patients WorldwideDialysis Patients WorldwideThe Emerging EpidemicThe Emerging Epidemic
of Chronic Kidney Disease !of Chronic Kidney Disease !
Lysaght: J Am Soc Nephrol 13: S37Lysaght: J Am Soc Nephrol 13: S37‐‐S40, 2002S40, 2002

Lysaght: J Am Soc Nephrol 13: S37Lysaght: J Am Soc Nephrol 13: S37‐‐S40, 2002S40, 2002
0
200
400
600
800
1000
1200
1971-1980 1981-1990 1991-2000 2001-2010
$ B
illio
ns$
Bill
ions
$ 30 Billion$ 30 Billion $ 155 Billion$ 155 Billion
$ 470 Billion$ 470 Billion
$ 1.1 Trillion$ 1.1 Trillion
Medical Costs of Dialysis PopulationMedical Costs of Dialysis Population

Lysaght: J Am Soc Nephrol 13: S37Lysaght: J Am Soc Nephrol 13: S37‐‐S40, 2002S40, 2002
9900%%
Dialysis Patients WorldwideDialysis Patients Worldwide

Burden of Mortality from Kidney Disease Burden of Mortality from Kidney Disease Illustrated by Relative Country SizeIllustrated by Relative Country Size
Nugent et al.: Nephron Clin Pract 118: c269Nugent et al.: Nephron Clin Pract 118: c269‐‐c277, 2011 c277, 2011

05
10152025303540455055
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
Prevalence of Dialysis PatientsPrevalence of Dialysis Patientsin Turkeyin Turkey
Num
ber o
f Patients (x100
0)
49794979 71637163 811881181067210672 1261812618136261362616364
163642114121141
23698236982661526615
HemodialysisHemodialysis
Peritoneal DialysisPeritoneal Dialysis
28641286413188831888
3805338053
4457444574
Turkish Society of Nephrology DatabaseTurkish Society of Nephrology Database
4603846038
5206852068

0 5 10 15 20 25 30
Diabetes mellitusDiabetes mellitus
Chronic glomerulonephritisChronic glomerulonephritis
HypertensionHypertension
Cystic kidney diseasesCystic kidney diseases
Chronic pyelonephritisChronic pyelonephritis
Renal vascular diseaseRenal vascular disease
Unknown etiologyUnknown etiology
4.7
3.4
7.2
16.1
Percent (%)
27.627.6
Other causesOther causes
8.28.2
1.0
AmyloidosisAmyloidosis
No informationNo information
2.0
1.3
30.630.6
Turkish Society of Nephrology Database (2009) Turkish Society of Nephrology Database (2009)
Etiology in Prevalent HD PatientsEtiology in Prevalent HD Patientsin Turkeyin Turkey
58.2%58.2%

60,000 Patients with ESRD60,000 Patients with ESRD
7,500,000 Patients 7,500,000 Patients with Chronic Kidney Diseasewith Chronic Kidney Disease
(15.7% of the Adult Population)(15.7% of the Adult Population)
The CREDIT Study: Nephrol Dial Transplant, 2010

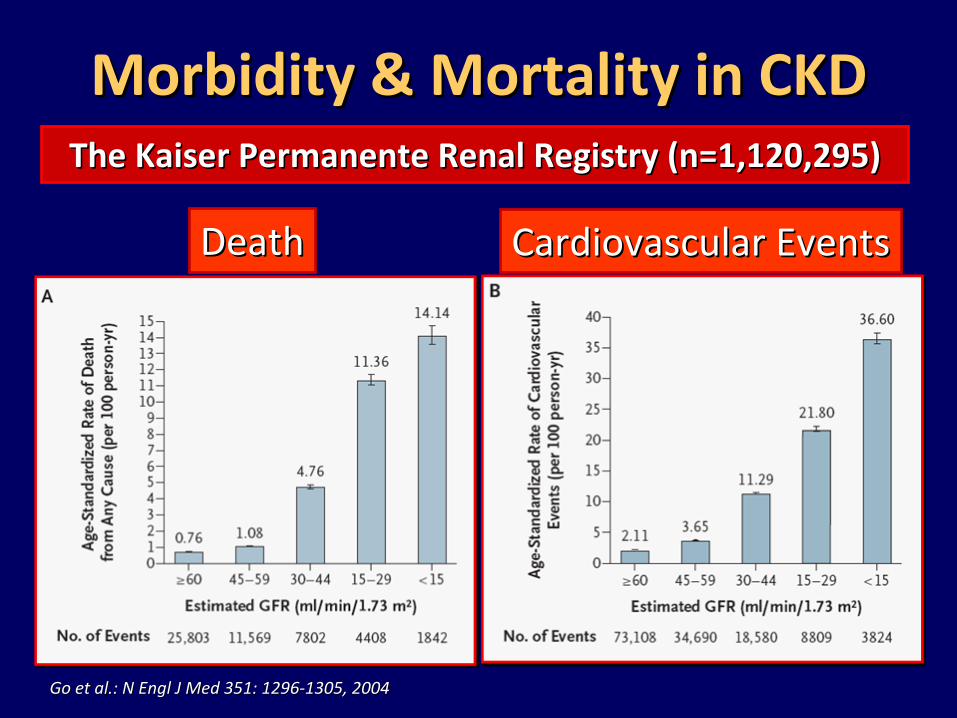
Morbidity & Mortality in CKDMorbidity & Mortality in CKD
Go et al.: N Engl J MedGo et al.: N Engl J Med
351351::
12961296‐‐13051305, 200, 2004 4
The Kaiser Permanente Renal Registry (n=1,120,295)The Kaiser Permanente Renal Registry (n=1,120,295)
DeathDeath Cardiovascular EventsCardiovascular Events

0
5
10
15
20
25
Klag et al: N Engl J Med 334Klag et al: N Engl J Med 334::1313‐‐1818, 19, 199696
Adjusted
Relative Risk
<120<80
>210>120
180‐209110‐119
160‐179100‐109
140‐15990‐99
130‐13985‐89
120‐12980‐84
SBP (mm Hg)DBP (mm Hg)
1 1.2 1.93.1*
6.0*
11.2*
22.1*
*P<0.001
Blood Pressure & ESRDBlood Pressure & ESRD
332,544 Males332,544 MalesAge: 35Age: 35‐‐5757
Multiple Risk Factor Intervention Trial (MRFIT)Multiple Risk Factor Intervention Trial (MRFIT)

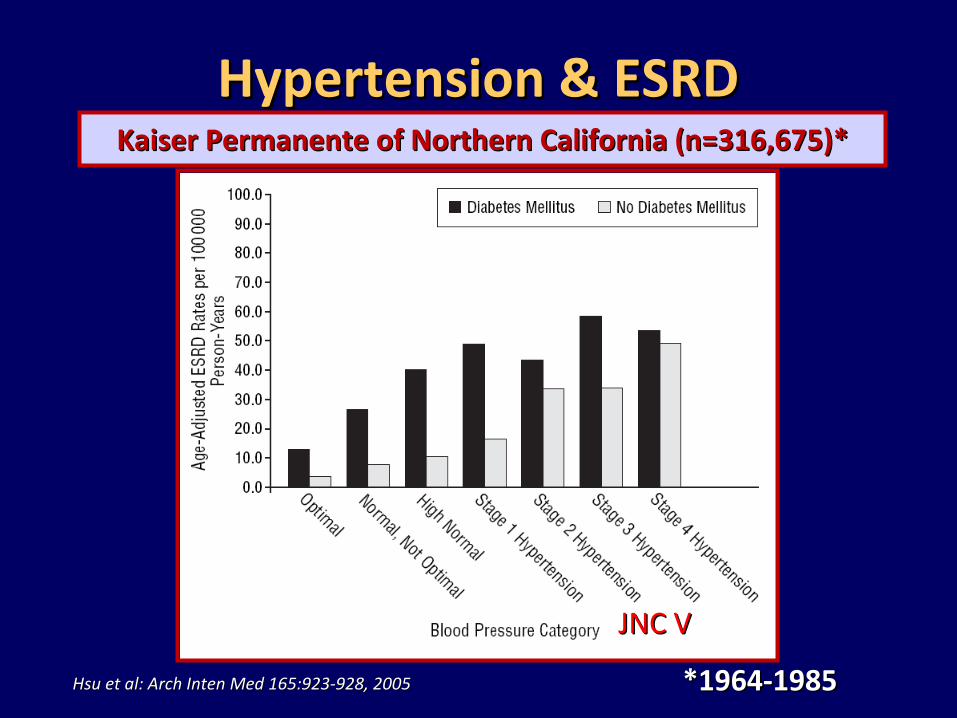
Hsu et al: Arch Inten Med 165Hsu et al: Arch Inten Med 165::923923‐‐928928, , 2005 2005
Hypertension & ESRDHypertension & ESRDKaiser Permanente of Northern California (n=316,675)*Kaiser Permanente of Northern California (n=316,675)*
JNC VJNC V
*1964*1964‐‐19851985

Hsu et al: Arch Inten Med 165Hsu et al: Arch Inten Med 165::923923‐‐928928, , 2005 2005
JNC VJNC V
*1964*1964‐‐19851985
Hypertension & ESRDHypertension & ESRDKaiser Permanente of Northern California (n=316,675)*Kaiser Permanente of Northern California (n=316,675)*
Hsu et al: Arch Inten Med 165Hsu et al: Arch Inten Med 165::923923‐‐928928, , 2005 2005
JNC VJNC V
*1964*1964‐‐19851985
Hypertension & ESRDHypertension & ESRDKaiser Permanente of Northern California (n=316,675)*Kaiser Permanente of Northern California (n=316,675)*

9595 9898 101101 104104 107107 110110 113113 116116 119119
r = 0.69; P
< 0.05
MAP (mmHg)
GFR
(mL/min/year)
GFR
(mL/min/year)
130/85 140/90
UntreatedHTN
00
‐‐22
‐‐44
‐‐66
‐‐88
‐‐1010
‐‐1212
‐‐1414Parving HH, et al. Br Med J. 1989.Parving HH, et al. Br Med J. 1989.
Moschio G, et al. N Engl J Med. 1996.Moschio G, et al. N Engl J Med. 1996.Viberti GC, et al. JAMA. 1993.Viberti GC, et al. JAMA. 1993.
Bakris GL, et al. Kidney Int. 1996.Bakris GL, et al. Kidney Int. 1996.Klahr S, et al. N Eng J. Med 1994.Klahr S, et al. N Eng J. Med 1994.
Bakris GL. Hypertension. 1997.Bakris GL. Hypertension. 1997.Hebert L, et al. Kidney Int. 1994.Hebert L, et al. Kidney Int. 1994.
The GISEN Group. Lancet. 1997.The GISEN Group. Lancet. 1997.Lebovitz H, et al. Kidney Int. 1994.Lebovitz H, et al. Kidney Int. 1994.
Bakris GL et alBakris GL et al::
Am J Kidney Dis. 36(3):646Am J Kidney Dis. 36(3):646‐‐661661, 2000, 2000
Lower MAP Results in Slower Rates of DeclineLower MAP Results in Slower Rates of Declinein GFR in Diabetics and Nonin GFR in Diabetics and Non‐‐DiabeticsDiabetics

0
10
20
30
40
50
60
4 8 12 16 20
Retarding Progression of CKDRetarding Progression of CKDwith Blood Pressure Controlwith Blood Pressure Control
Time (years)Time (years)
GFR
(ml/m
in)
GFR
(ml/m
in)
8 ml/min/yr8 ml/min/yr
6 ml/min/yr6 ml/min/yr4 ml/min/yr4 ml/min/yr
2 ml/min/yr2 ml/min/yr1 ml/min/yr1 ml/min/yr


Gender Number Mean SD24 hour NaCl intake (gr/day)
WholeGroup
1767 18.04 8.34
Males 857 19,31 8,67Females 910 16,83 7,86
Gender Number Mean SD24 hour urinary Na+ (mEq/day)
Whole Group
1767 306.7 142.1
Male 857 328.4 147.5Female 910 286.2 133.7
SALTurk TrialSALTurk Trial
www.turkhipertansiyon.orgwww.turkhipertansiyon.org



AtherosclerosisAtherosclerosis
Type 2Type 2DiabetesDiabetesMellitusMellitus
HypertensionHypertension
HyperlipidemiaHyperlipidemia
InsulinInsulinResistanceResistance
NephropathyNephropathy
OBESITYOBESITY


••
There was a tenThere was a ten‐‐fold fold increase in the incidence increase in the incidence
of obesityof obesity‐‐related related glomerulopathy over 15 glomerulopathy over 15
years. years.
••
80% of the cases were 80% of the cases were due to FSGS.due to FSGS. 0
1
2
1986 2000Kambham et al: Kidney Int 59: 1498Kambham et al: Kidney Int 59: 1498‐‐1509, 20011509, 2001
%%
Analysis of 6818 Kidney BiopsiesAnalysis of 6818 Kidney Biopsies
ObesityObesity‐‐related Glomerulopathyrelated Glomerulopathy


Wang et al: Kidney Int 73: 19Wang et al: Kidney Int 73: 19‐‐33, 2008 33, 2008
Obesity & Kidney DiseaseObesity & Kidney Disease

Wang et al: Kidney Int 73: 19Wang et al: Kidney Int 73: 19‐‐33, 2008 33, 2008
Obesity & Kidney DiseaseObesity & Kidney Disease

Renal Effects of AdipocyteRenal Effects of Adipocyte‐‐Derived FactorsDerived Factors
Saxena, ChopraSaxena, Chopra: : Dial Transplant 33Dial Transplant 33::
1111‐‐2020, , 2004 2004

BMI is Associated with Altered RenalBMI is Associated with Altered RenalHemodynamics in NonHemodynamics in Non‐‐Obese Healthy SubjectsObese Healthy Subjects
Bosma et al: Kidney Int 65: 259‐265, 2004
P<0.001P<0.001 P<0.001P<0.001
102 healthy, non102 healthy, non‐‐obese subjects (59 males, 43 females)obese subjects (59 males, 43 females)

PREVENDPREVEND(Prevention of REnal and Vascular ENdstage Disease)(Prevention of REnal and Vascular ENdstage Disease)
de Jong et al: International Journal of Obesity 26: Suppl 4, S21de Jong et al: International Journal of Obesity 26: Suppl 4, S21‐‐S24, 2002 S24, 2002
NonNon‐‐Diabetic and NonDiabetic and Non‐‐Hypertensive Subjects (n=8050)Hypertensive Subjects (n=8050)

de Jong et al: International Journal of Obesity 26: Suppl 4, S21de Jong et al: International Journal of Obesity 26: Suppl 4, S21‐‐S24, 2002 S24, 2002
9.5%9.5%
18.3%18.3%
29.3%29.3%
6.6%6.6%9.2%9.2%
16.0%16.0%
PREVENDPREVEND(Prevention of REnal and Vascular ENdstage Disease)(Prevention of REnal and Vascular ENdstage Disease)
NonNon‐‐Diabetic and NonDiabetic and Non‐‐Hypertensive Subjects (n=8050)Hypertensive Subjects (n=8050)


0
24
68
1012
1416
18
Chen et al.: Ann Intern MedChen et al.: Ann Intern Med
140140::
167167‐‐174174, 200, 20044
P re va le n
c e of
P re va le n
c e of
Microalbu
minuria (%
)Microalbu
minuria (%
)
Blood PressureBlood Pressure>>130/85 mm Hg130/85 mm Hg
HDL CholesterolHDL Cholesterol<40 mg/dL (M)<40 mg/dL (M)<50 mg/dL (F)<50 mg/dL (F)
TriglycerideTriglyceride>>150 mg/dL150 mg/dL
GlucoseGlucose>>110 mg/dL110 mg/dL
Waist CircumferenceWaist Circumference>>102 cm (M)102 cm (M)>>88 cm (F)88 cm (F)
P<0.001P<0.001
P=0.039P=0.039
P<0.001P<0.001YesYes
NoNo
Metabolic Syndrome & MicroalbuminuriaMetabolic Syndrome & Microalbuminuria

0
5
10
15
20
25
0 1 2 3 4 5
Pre valen
ce (%
)Pre valen
ce (%
)
3.03.04.94.9
6.86.89.89.8
14.614.6
20.120.1
Metabolic Syndrome Risk Factors (n)Metabolic Syndrome Risk Factors (n)
Chen et al.: Ann Intern MedChen et al.: Ann Intern Med
140140::
167167‐‐174174, 200, 20044
Metabolic Syndrome & MicroalbuminuriaMetabolic Syndrome & Microalbuminuria

0
1
2
3
4
5
6
7
8
P re va le n
c e of C
K D (%
)P re va le n
c e of C
K D (%
) P<0.001P<0.001
P=0.002P=0.002P=0.004P=0.004
P=0.044P=0.044
P<0.001P<0.001
YesYes
NoNo
Chen et al.: Ann Intern MedChen et al.: Ann Intern Med
140140::
167167‐‐174174, 200, 20044
Metabolic Syndrome & CKDMetabolic Syndrome & CKD
Blood PressureBlood Pressure>>130/85 mm Hg130/85 mm Hg
HDL CholesterolHDL Cholesterol<40 mg/dL (M)<40 mg/dL (M)<50 mg/dL (F)<50 mg/dL (F)
TriglycerideTriglyceride>>150 mg/dL150 mg/dL
GlucoseGlucose>>110 mg/dL110 mg/dL
Waist CircumferenceWaist Circumference>>102 cm (M)102 cm (M)>>88 cm (F)88 cm (F)

0123456789
10
0 1 2 3 4 5
0.3 0.9
2.9
4.9
7.0
9.2
Chen et al.: Ann Intern MedChen et al.: Ann Intern Med
140140::
167167‐‐174174, 200, 20044
Metabolic Syndrome Risk Factors (n)Metabolic Syndrome Risk Factors (n)
Metabolic Syndrome & CKDMetabolic Syndrome & CKDPre valen
ce (%
)Pre valen
ce (%
)

0
20
40
60
NonNon‐‐Metabolic SyndromeMetabolic Syndrome(n=823)(n=823)
Metabolic SyndromeMetabolic Syndrome(n=802)(n=802)
P=0.01P=0.01
Microalb u
minu ri a
Mi cr oa lb u
minu ri a
mg /2 4
ho u
r smg /2 4
ho u
r sHypertensive Renal Damage in Metabolic Syndrome is Hypertensive Renal Damage in Metabolic Syndrome is
Associated with Glucose Metabolism DisturbancesAssociated with Glucose Metabolism Disturbances
1625 Patients with Essential Hypertension1625 Patients with Essential Hypertension
Segura et al: J Am Soc Nephrol 15: S37Segura et al: J Am Soc Nephrol 15: S37‐‐S42, 2004 S42, 2004

0
20
40
60
80
NormoglycemiaNormoglycemia(n=319)(n=319)
Impaired FastingImpaired FastingGlucose (n=237)Glucose (n=237)
DiabetesDiabetes(n=246)(n=246)
Microalbu
minuria
Microalbu
minuria
mg /2 4
ho u
r smg /2 4
ho u
r s
P=0.001P=0.001
Patients with Metabolic Syndrome (n=802)Patients with Metabolic Syndrome (n=802)
Segura et al: J Am Soc Nephrol 15: S37Segura et al: J Am Soc Nephrol 15: S37‐‐S42, 2004 S42, 2004
Hypertensive Renal Damage in Metabolic Syndrome is Hypertensive Renal Damage in Metabolic Syndrome is Associated with Glucose Metabolism DisturbancesAssociated with Glucose Metabolism Disturbances

40
60
80
100
DiabetesDiabetes(n=246)(n=246)
Creatin
i ne C le ar an ce
C re at in
i ne C le ar an ce
ml/ m
in/ 1.73 m
ml/ m
in/ 1.73 m
22
P=0.0007P=0.0007
Segura et al: J Am Soc Nephrol 15: S37Segura et al: J Am Soc Nephrol 15: S37‐‐S42, 2004 S42, 2004
Hypertensive Renal Damage in Metabolic Syndrome is Hypertensive Renal Damage in Metabolic Syndrome is Associated with Glucose Metabolism DisturbancesAssociated with Glucose Metabolism Disturbances
Patients with Metabolic Syndrome (n=802)Patients with Metabolic Syndrome (n=802)
NormoglycemiaNormoglycemia(n=319)(n=319)
Impaired FastingImpaired FastingGlucose (n=237)Glucose (n=237)

Muntner et al: Kidney Int 58: 293Muntner et al: Kidney Int 58: 293‐‐301, 2000 301, 2000
Plasma Lipids & Risk of Renal DysfunctionPlasma Lipids & Risk of Renal DysfunctionAtherosclerosis Risk in Communities Study (n=12,728)Atherosclerosis Risk in Communities Study (n=12,728)
Baseline serum creatinine: <2.0 mg/dL (M), <1.8 mg/dL (F)Baseline serum creatinine: <2.0 mg/dL (M), <1.8 mg/dL (F)

The Benefits of Weight Loss in Patients The Benefits of Weight Loss in Patients with CKDwith CKD

Navaneethan et al: Clin J Am Soc Nephrol 4: 1565‐1574, 2009
The Benefits of Weight Loss in Patients The Benefits of Weight Loss in Patients with CKDwith CKD

A prospective observational study of 20A prospective observational study of 20‐‐yr durationyr durationto examine the association between hypertension and to examine the association between hypertension and
smoking on the future risk of CKDsmoking on the future risk of CKD

Stage 2Stage 2
Stage 1Stage 1
Stage 2Stage 2
Stage 1Stage 1
Stage 1Stage 1
Stage 2Stage 2

CurrentCurrentSmokerSmoker
Former/NeverFormer/NeverSmokerSmoker

Ritz et al.: JASN 9:1798‐1804, 1998
80 90 100 110 120 40 60 80 100
Basal
Cigarette
Mean Arterial PressureMean Arterial Pressure
P<0.0001 P<0.001
mm Hg min‐1
Effects of Smoking on Renal HemodynamicsEffects of Smoking on Renal Hemodynamicsin Healthy Volunteersin Healthy Volunteers
Heart RateHeart Rate

0 50 100 150 200 250 300 0 2 4 6 8 10
P<0.01 P<0.01
pg/ml ng/ml
Basal
Cigarette
Effects of Smoking on Renal HemodynamicsEffects of Smoking on Renal Hemodynamicsin Healthy Volunteersin Healthy Volunteers
Ritz et al.: JASN 9:1798‐1804, 1998
EpinephrinEpinephrin Active ReninActive Renin

80 100 120 140 80 100 120 140
P<0.001 P<0.006
ml/min/1.73m2 mmHg.min/ml.1.73m2
Effects of Smoking on Renal HemodynamicsEffects of Smoking on Renal Hemodynamicsin Healthy Volunteersin Healthy Volunteers
Ritz et al.: JASN 9:1798‐1804, 1998
Basal
Cigarette
Glomerular Filtration RateGlomerular Filtration Rate Renovascular ResistanceRenovascular Resistance

Smoking & CKDSmoking & CKD

Smoking & CKDSmoking & CKD

Proposed Mechanism of Fetal ProgrammingProposed Mechanism of Fetal Programmingof Hypertension and Renal Diseaseof Hypertension and Renal Disease
Zandi-Nejad et al. Hypertension 47: 502-508, 2006
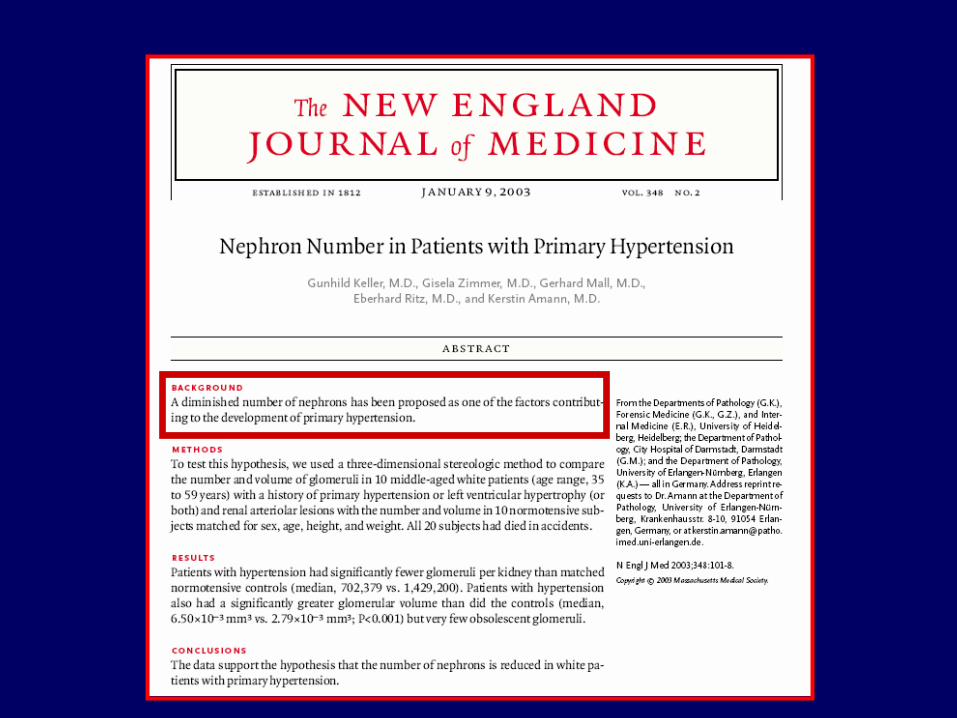

Nephron Number in Patients with Nephron Number in Patients with Primary HypertensionPrimary Hypertension
Keller et al. N Engl J Med 348: 101‐108, 2003
10 Hypertensive & 10 Normotensive Subjects Who Had Died in Accid10 Hypertensive & 10 Normotensive Subjects Who Had Died in Accidentsents
Hypertensive Hypertensive Patients (n=10)Patients (n=10)
Normotensive Normotensive Subjects (n=10)Subjects (n=10)
P P ValueValue
Age (yr)Age (yr) 45.545.5 46.546.5 NS*NS*
Sex (M/F)Sex (M/F) 9/19/1 9/19/1 NSNS
Height (cm)Height (cm) 178178 177177 NSNS
Body Weight (kg)Body Weight (kg) 90.590.5 84.584.5 NSNS
Heart Weight / Body Weight (g/kg) Heart Weight / Body Weight (g/kg) 6.086.08 4.924.92 <0.001<0.001
Absolute Kidney Weight (g)Absolute Kidney Weight (g) 184184 173173 NSNS
Relative Kidney Weight (g/kg)Relative Kidney Weight (g/kg) 2.062.06 1.861.86 NSNS
Weight of Renal CortexWeight of Renal Cortex 120120 102102 NSNS
*NS: Not Significant*NS: Not Significant

Number of GlomeruliNumber of GlomeruliPer KidneyPer Kidney
Volume of Volume of GlomeruliGlomeruli
Nephron Number in Patients with Nephron Number in Patients with Primary HypertensionPrimary Hypertension
Keller et al. N Engl J Med 348: 101‐108, 2003

NormotensiveNormotensiveControlControl
HypertensiveHypertensivePatientPatient
Nephron Number in Patients with Nephron Number in Patients with Primary HypertensionPrimary Hypertension
Keller et al. N Engl J Med 348: 101‐108, 2003


ThankThank
youyou
forfor
youryour
attentionattention……


![Metabolic Syndrome[1]](https://static.fdocuments.in/doc/165x107/577cd7141a28ab9e789dffc3/metabolic-syndrome1.jpg)