Mesenteric ischemia presentation by Dr.NOSHI Capital Hospital Islamabad Pakistan.
38
MESENTERIC ISCHEMIA DR.NOSHI SURGERY DEPARTMENT CAPITAL HOSPITAL ISLAMABAD PAKISTAN
-
Upload
drfarhanali2008 -
Category
Health & Medicine
-
view
172 -
download
1
Transcript of Mesenteric ischemia presentation by Dr.NOSHI Capital Hospital Islamabad Pakistan.

MESENTERIC ISCHEMIADR.NOSHI
SURGERY DEPARTMENTCAPITAL HOSPITAL ISLAMABAD
PAKISTAN

BIO DATA :
Name : MR.XYZ .
Age: 36yrs, male . Religion: Islam , sunni .
Marital status: Married . Profession : ex director at
NADRA. Address: ISLAMABAD. DOA: 12-12-2015 at
05 PmSOA : ER

Lower abdominal pain 4 DAYS
Vomiting 1 DAY
PRESENTING COMPLAINTS:

HISTORY OF PRESENT ILLNESS :
My patient was living a healthy life 4 days back, when he developed Lower Abdominal pain, it was gradual in onset n later on it was sudden acute excruciating pain localized in lower abdomen non radiating Intermittent initially later on continous, colicky in character, INITIALLY mild in severity LATER on severe constant between meals NO aggravating factors NO relieving factors associated with bloating and vomiting. There is no h/o of Weight loss, retching No relation of posture with pain.
No h/o of haemetmesis, melena, heart burn, large bulky greasy stools and altered bowel habits.He consulted a local doctor on the same day and receive anti pyretics but didn’t relieved the pain.

He also developed intractable VomitingCommenced on the day of admissionFrequency was multiple episode of vomitingProjectile in nature, containing mostly semi digested food particals later on it was
watery in consistency. Clear with offensive smell. Associated with epigastric pain.anxiety,sweatingAggravated by intake of meal and relieved by limatation of
meal.No associated complain of hemetemasis ,RHC pain with or
without jaundice, polyuria, polydipsia, unconsciousness, headache or vertigo.

• Past medical HISTORY: pneumonia 2 yr back• PAST surgical history : nil• PAST allergic history: nil• PAST blood transfusion hx: nil• PAST drug history :nil• Drug addiction history: nil• Family history : Mother k/c cholithiasis &
Elder brother newly diagnosed htn
:

PERSONAL HISTORY :
MARRIED SINCE ONE & HALF YEAR. One baby girl of 3 months old.Bowel habits is normal.Sleep is not disturbed.Appetite is reduced.Living in well constructed home with proper
sanitation.Socioeconomic history is good.

GP EXAMINATION :
A gentleman of normal built, conscious alert and well oriented in time, space and person lying on the bed with discomfort due to pain
GCS 15/15I/V line maintained in left forarm Vitals:
• Pulse: 141/min .
• B.P: 100/70.
• RR: 29/min .
• BMI: 31.

Systemic Examination:
GIT: Abdomen tense , tenderness in lower abdomen with generalized guarding BS +ve
Respiratory system: • Normal B/L vesicular breathing• with no added sounds. CVS: S1+S2+0 CNS: GCS 15/15, agitated and in agony, well
oriented to time space ,person.

PRE OP Base line investigations:
Blood cp
WBC: 14.
HB: 15.0 mg/dl
Plt: : 211

On chest xray : Normal
On erect xray abdomen: Distended gut loop
On urine R/E: Normal
On u/s ABDOMEN & PELVIS: FATTY LIVER & MILD ASCITES

Per -op findings:
• DATE: 13/12/16• SURGEON: DR TANSEER & DR YASMEEN• ANESTHESIA:GA• PROCEDURE: EXPLORATORY LAPAROTOMY• PER-OP FINDINGS:INFARCTED SMALL
INTESTINE FROM 5 CM FROM DJ JUNCTION TO 2 FEET AWAT FROM ILLEO-CECAL JUNSTION
• DOUBLE BARREL STOMA made on left side.
Post op orders:
• NPO TFO.• KEEP THE PATIENT IN ICU.• CVP was maintained & start with TPN.• STRICT HOURLY MONITORING of vitals .• TRANSFUSE BLOOD.• I/V ANTIBIOTICS AND I/V PAIN KILLERS.• URINE OUT PUT and NG was montiored.• Gut viability was visualized through stoma bag.
ON HISTOPATHOLOGY REPORT:• SHOWING FULL THICKNESS INFARCTION• EXCISION MARGINS ARE VIABLE..

Post op baselines
Blood cp
WBC: 8.7
HB: 13.0 mg/dl
Plt: : 444

Pre op optimization for illostomy reversal
• Encourage the oral intake• Counselling regarding the bowel habits • Special care of stoma bag to prevent any complications.
(stomal,peri-stomal or metabolic) • Proper care of wound • Stool softners• Effective antibiotics & pain killers• Gut preparation prior to surery AT 6PM,12AM,& 6AM• PASSED CVP ON 20/1/16 • WE PLANNED FOT CT ANGIOGRAPHY BUT NOT POSSIBLE DUE
TO derranged LFT’S & RFT’S.• WEIGHT WAS MARKEDLY REDEUCED TO 65 KG

PRE OP investigation for ILLOSTOMY IRREVERSAL
Blood cp
WBC: 11.1
HB: 13.8 mg/dl
Plt: : 270

surgery
• OPERATED ON 28/1/16• SURGEON DR.TANSEER & DR Ruqia &DR NOSHI• ANESTHESIA:GA• STEPS:– After Asceptic measure DOUBLE BARREL LUMEN was
dissected from surrounding structures.– EDGES were refreshed & antimesenteric border of both
lumen was stapled from 60mm staple (linear). Later on DOUBLE BARREL LUMEN was closed with 90mm linear stapler.
– Abdominal wound closed .

Post op illostomy reversal• Npo TFO• Antibiotics & PAIN KILLERS • STRICT MONITORING OF VITALS,NG & UO• START TPN • ENCOURAGE ORAL DIET AFTER NPO IS BREAK• If diet doesn’t improve situation then add up anti-
dirrhoeal ,softners.• COUNSELLING FOR BOWEL HABITS & Skin care( do not
use talcum powder or baby wipes instead use sudocrem.• Additional counselling of balanced diet & avoid food &
vegetables which alter the bowel habits.

Post op illostomy irreversal
Blood cp
WBC: 7.57
HB: 10.4 mg/dl
Plt: : 185

OFFICER SWD

ISCHEMIC BOWEL DISEASE LITERATURE

• INTESTINAL ISCHEMIA occurs when mesenteric perfusion is inadequate to meet intestinal metabolic demands for oxygen .
• IT may affect small or large bowel or both.• CAN develop suddenly(acute mesenteric
ischemia) or gradually over months( chronic Mesenteric Ischemia.
DEFINITION OF INTESTINAL ISCHEMIA

BLOOD SUPPLY

AETIOLOGY OF INTESTINAL ISCHEMIA
INADEQUATE INFLOW
• OCCLUDED(60%)• Embolism• Thrombosis• Volvulus• Mesenteric tear• AAA surgery• Aortic dissectin• Strangulated hernia
NON OCCLUSIVE•Cardiogenic shock•Hypovolumeia•Sepsis•Pancreatitis•Intra abdominal hypertension•Vasospasm due to drugs
INCREASED WALL TENSION
• CLOSED LOOP DESTRUCTION
• PSEUDO-OBSTRUCTION
REDUCED VENOUS OUTFLOW
•MESENTERIC VEIN THROMBOSIS
•MESENTERIC NODAL DISEASES
•PANCREATIC NEOPLASM

CLASSIFICATION OF MIACUTE SUPERIOR MESENTERIC ISCHEMIA• Epidemiology
– ASMI is 1-2 episode/1000• Pathogenesis & Associations:
– SMA Embolism.– SMA Thrombosis.– Non-Occlusive Mesenteric Ischemia– SM Vein Thrombosis.
CHRONIC SUPERIOR MESENTERIC ISCHEMIA
• Epidemiology– CSMI is 1/100,000
• Pathogenesis & Associations:– Atherosclerosis– Fibrodysplasia– Vasculitis– takayasu’s disease– SM Vein Thrombosis
ASSOCIATED WITH :• Acute myocardial
Infarction• Cardiac ThrombI
(48%)• Atrial Fibrillation• Synchoronus
EMBOLI(68%)
Associated with:• Smoking• HTN(66%)• D.M• Coronary artery
disease(58%)• Hyperlipedemi• Peripheral
vascular disease(72%)
Superior Mesenteric Vein Thrombosis:• Hypercoguable states• Thrombophilia• Ocp
•Previous Thromboembolism•Dehydration•Obesity•Inflammatory bowel disease•Liver cirrhosis•Intra-abdominal malignancy•Post operatively.
• Generalized athersclerosis• Aortic• CMI • coronary artery• ceberovascular disease• peripheral vascular disease
• Disseminated Cancer.
•Critically ill patients.•Seen in elderly•Patients with severe cardiac diseases•Post cardiac – surgery.•Patients who are in sepsis•Patients who receive inotropes.•Other Drugs(digioxin,amphetaines,cocaine)\• Synchronous Infarction in Liver,Spleen &
Kidney.
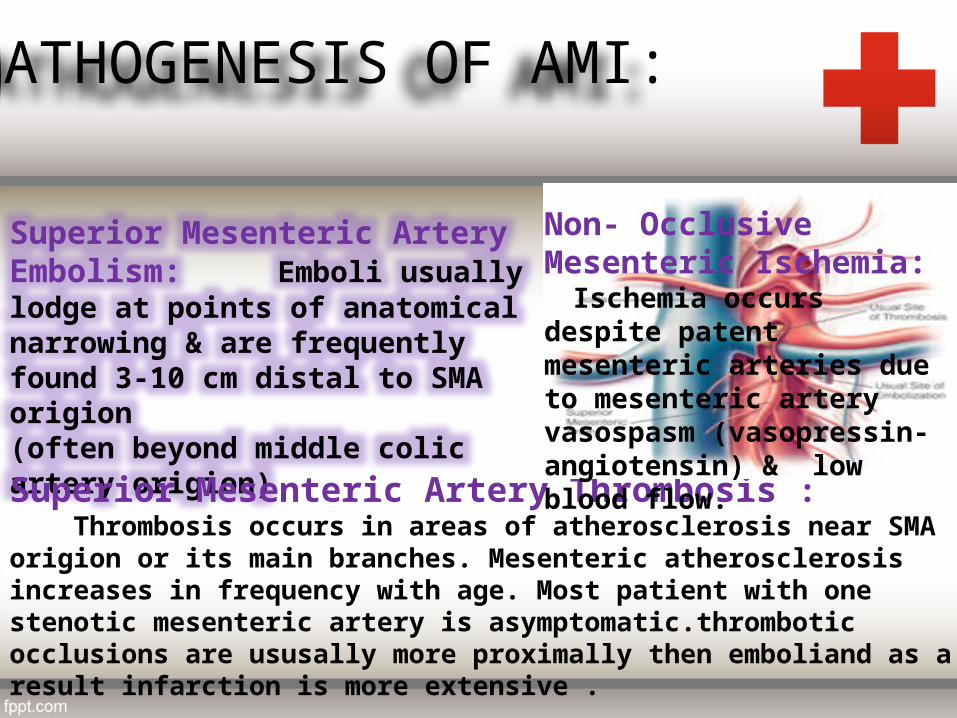
PATHOGENESIS OF AMI:
Superior Mesenteric Artery Embolism: Emboli usually lodge at points of anatomical narrowing & are frequently found 3-10 cm distal to SMA origion (often beyond middle colic artery origion)
Superior Mesenteric Artery Thrombosis : Thrombosis occurs in areas of atherosclerosis near SMA origion or its main branches. Mesenteric atherosclerosis increases in frequency with age. Most patient with one stenotic mesenteric artery is asymptomatic.thrombotic occlusions are ususally more proximally then emboliand as a result infarction is more extensive .
Non- Occlusive Mesenteric Ischemia: Ischemia occurs despite patent mesenteric arteries due to mesenteric artery vasospasm (vasopressin-angiotensin) & low blood flow.

CLINICAL PRESENTATIONS
ACUTE MESENTERIC ISCHEMIA• It presents with sudden,severe
abdominal pain becoming progressively worse associated with vomiting(70%) & diarrhoea (40-50%)
• Elderly presents with tachypnoea & confusion
• Pain seeming out of keeping ith physical finding.
• By the time b.s disappear,the abdomen distends & there is guarding & rigidity ischemia will usually have progressed to transmural infarction.
CHRONIC MESENTERIC ISCHEMIA•Patients are usually in their 60’s & 70’s with a colicky,psot-prandial epigastric pain(mesenteric angina) & unintentional weight loss( 10-15 kg)
•O/E they may reveal cachexia,smoke-related chest disease,scahphoid abdomen scarred by erythema abigne,abdominal bruit or reduced/absent peripheral pulses.
•D/D include biliary disease & peptic ulcer
DIFFERNTIAL DIAGNOSIS:•INTESTESTINAL OBSTRUCTION•PERFORATED VISCUS•PANCREATITIS•APPENDICITIS•DIVERTICULITIS•CHOLECYSTITIS
DIAGNOSISIT should be CONSIDERED & INVESTIGATED in any patient with ACUTE Severe Abdominal pain lasting longer then 2 hours ,out of keeping with physical signs and without obvious cause should be investigated for ASMI
•TYPICAL SYMPTOMS•DUPLEX ULTRASONOGRAPHIC evidence of occlusion or HIGH –GRADE STENOSIS of SMA & COELIAC ARTERY(peak systolic velocity of more then 275 & 200 cm/s respectively.

INVESTIGATIONS
ACUTE MESENTERIC ISCHEMIA
• BLOOD CP– WBC is raised– METABOLIC ACIDOSIS– ELEVATION IN PHOSPHATE (80%)– ELEVATION OF AMYLASE (50%)– ELEVATION OF LACTATE (100%S)– ELEVATED @glutathione s-
transferase(72%sen & 77% specf)
• PLAIN RADIOGRAPHY.• Duplex scanning of mesenteric
Vessels• CT ANGIOGRAPHY.
CHRONIC MESENTERIC ISCHEMIA
• DUPLEX ULTRASONOGRAPGH– Non invasive– Criteria are PEAK SYSTOLIC-
FLOW,END-DIASTOLIC VELOCITY & RETRO-GRADE FLOW IN HEPATIC ARTERY.(COLIAC STENOSIS)
• MESENTERIC ANGIOGRAPHY– Therapeutic( stent insertion)– Indicated to assess the
significant disease identified on DUPLEX & in obese patients
• CT ANGIOGRAPHY
•MAGNETIC RESONANCE ANGIOGRAPHY• NON-INVASIVE• EVALUATES PROXIMAL COLIAC
& SMA•MESENTERIC ANGIOGRAPHY• Sensitivity of 90-100%• Range of therapeutic options
• Intra-arterial vasodilators,thrombolysis, angioplasty & stenting
•DIAGNOSTIC LAPROSCOPY• Less invasive then laprotomy• Unable to assess mucosal
ischemia
•MAGNETIC RESONANCE ANGIOGRAPHY e GADOLINIUM• HAS high sensitivity &
specificity but there is gadolinium associated systemic fibrosis & renal failure

PRE-OPERATIVE PROCEDURE:
• GIVE 100 %OXYGEN• I/V ANTIBIOTICS & PAIN KILLERS.• HEMODYNAMIC & FLUID/ELECTROLYTES/ACID-BASE
DISTURBANCES are CORRECTED.• ASSOCIATED CONDITIONS are TREATED.• HEPARIN is ADMINISTERED EARLY unless ACTIVE BLEEDING.• INVASIVE MONITORING in CRITICAL CARE is ADVISED• PATIENT need INOTROPES if fluid rususcitation fails to
correct hemodynamic disturbances,although VASOPRESSORS may exacerbate MI.
• Start with TPN

COMPLICATION OF PARENTERAL NUTRITION
•RELATED TO OVER FEEDING• Excess glucose: Hyperglycemia,hyperosmolar dehdration, hepatis steatosis ,
hypercapnia,increased sympathetic activity , fluid retention ,electrolyte abnormalities
• EXCESS FAT: Hypercholesterolemia & formation of lipo protein X, hypertriglyceridemia
• EXCESS AMINOACIDS: Hypercholerimc metabolic acidosis ,hypercalcemia, aminoacedmia,uremia
•RELATED TO SEPSIS:• Catheter related sepsis• Increased pre disposition to synthetic sepsis
•RELATED TO LINE• ON INSERTION: pneumothorax, damage to adjacent artery,air embolism, thoracic
duct damage,cardiac perforation,or tamponade ,pleural effusion • Long term occlusion, venous thrombosis
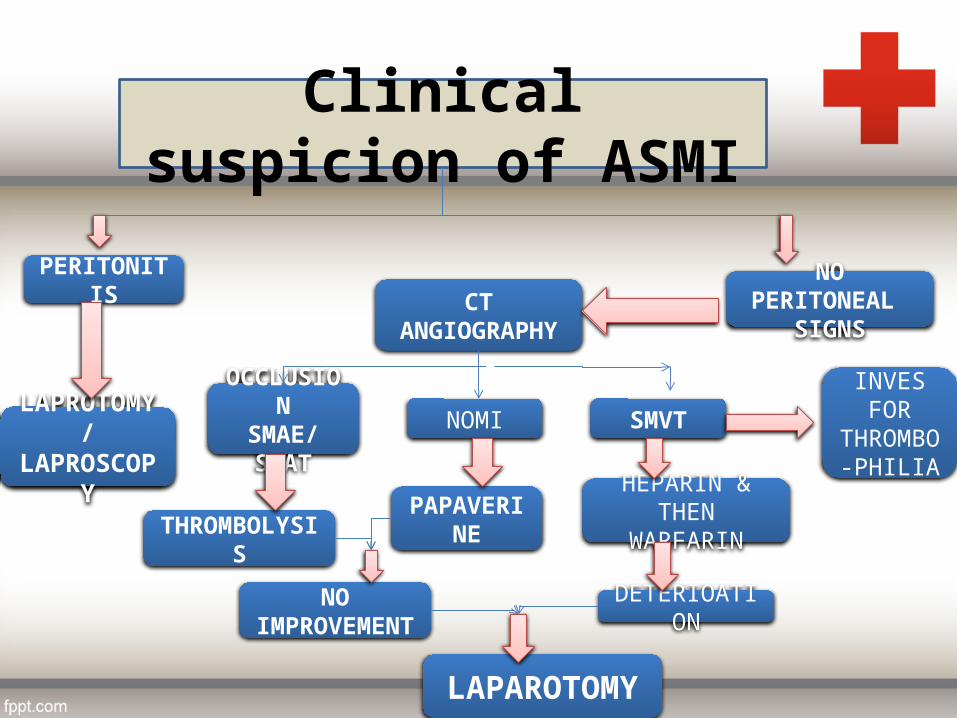
Clinical suspicion of ASMI
NO PERITONEAL SIGNS
PERITONITIS
INVES FORTHROMBO
-PHILIASMVTNOMIOCCLUSION
SMAE/SMATLAPROTOMY/LAPROSCOPY
NO IMPROVEMENT
PAPAVERINETHROMBOLYSIS
CT ANGIOGRAPHY
DETERIOATION
HEPARIN & THEN WARFARIN
LAPAROTOMY

surgery
• PLAN URGENT EXPOLARTORY LAPRATOMY• OPTIMIZE THE PATIENT CONDITION DURING &
AFTER SURGERY• STOMA CARE• COUNSELLING REGARDING HIGH PROTIEN
DIET• MONITOR ELECTROLYE IMBALANCE & BSR• CORRECT THE ABNORMALITIES BECAUSE OF
SHORT BOWEL SYNDROME

TREATMENT OF CSMI• AIM OF TREATMENT– To relieve SYMPTOMS– TO restore WEIGHT– TO prevent INTESTINAL INFARCTION
• DECISION to TREAT depends upon– Symptom severity– Presence of MULTI-VESSEL DISEASE– Severity of STENOSIS

INVASIVE TREATMENT FOR CSMITX OPTIONS FOR
CSMI
ENDOVASCULAR MESENTERIC ANGIOPLASTY & STENTING 90-95%(OPEN SMA REVASCULARISATION)
OPEN MESENTERIC BYPASS
•ANGIOPLASTY alone for short,non-ostial,focal stenosis
•ANGIOPLASTY & a ballon expandable STENT are deployed for long occlusions flush with the aorta
•STENTING has higher technical success then angioplasty & used in 70% of CSMI PATIENT
•Done when two or more vessels are critically stenosed.
•IF ITS NOT TECHNICALLY POSSIBLE ,ANGIOPLASTY OR STENTING OF COLIAC AXIS OR IMA MAY BENEFIT.
•ANTEGRADE/RETEROGRADE•SINGLE/MULTIPLE VESSELS•WITH AN AORTIC/ILLIAC BASED ORIGION
•IT IS reserved for failed PERCUTANEOUS INTERVENTION,OCCLUDED OR STENOSD STENTS.
•IT has lower restenosis & symmtomatic recurrence then angioplasty & stenting
TRANSAORTIC ENDARTERECTOMY
OUTCOME
ACUTE MESENTERIC ISCHEMIA• IT has high peri-operative mortality
rate 32-69% & 5 year survival rate.• MORATLITY depends upon
cause,speed of diagnosis & intervention.– HIGHEST IS NOMI.(70%)– LOWER FOR SMA OCCLUSION– LOWEST FOR SMVT (20%)
• MORTALITY is higher for SMAT then SAME,possibly due to more proximal SMA OCCLUSION with SMAT(more extensive infarction)
• Short bowel syndome may result in 23% of patients
CHRONIC MESENTERIC ISCHEMIA• ENDOVASCULAR SUCCESS IS 90-95 %.
– PERI-PROCEDURE MORTALITY IS 3-5% & MORBIDITY IS 20%.
– RISKS:• PUNCTURE-SITE PROBLEMS.• CONTRAST-INDUCED NEPHROTOXITY.• ARTERIAL DISSECTION(or rupture can
be manges using covered stent.)• DISTAL EMBOLISATION.(may respond
to thrombolysis or thromboaspiration.
• OPEN MESENTERIC BYPASS has a high mortality (0-15%) & morbidity (10-38%) due to cardiac & pulmonary complications.

KEY POINTS OF MANAGMENT
• RECOGNITION(high index of suspicion)• RESUSCITATION• REVASCULARISATION• RESECTION of intestine(limited initially to necrotic &
perforated bowel)• REASSESSMENT(after revascularisation & a second
look laprotomy)• REDUCTION of recurrence( critical care post
operatively to prevent secondary ischemia;long term anticoagulation)