Mentalizing and the mindful clinician - a prescription for
50
Mentalizing and the mindful clinician - a prescription for compassionate care. Prof Anthony W Bateman Visiting Professor University College, London; Affiliate Professor of Psychotherapy Copenhagen University
Transcript of Mentalizing and the mindful clinician - a prescription for

Mentalizing and the mindful
clinician - a prescription for
compassionate care.
Prof Anthony W Bateman
Visiting Professor University
College, London; Affiliate Professor
of Psychotherapy Copenhagen
University
Summary
Wards in same hospital show difference in:
Rates of violence
self-harm
absconding and other incidents
Use of manual restraint
Coercive use of medication
The problems tend to group together suggesting common cause(s)
Is it ‘us’; is it ‘them’; is it ‘both’; is it all/none of above.
Domains relevant to problems
Patient characteristics
Patient community
Outside hospital – e.g. home
Physical environment
Regulatory framework.
Staff team

Patient characteristics
Symptoms and demography
Paranoia; PD and BPD – interpersonal
problems and
abuse/irritability/reactivity/alcohol and drugs
Modifiers – psychotherapy; nursing
support; ward atmosphere
Patient community
Patient-patient interaction – contagion and
discord
Patient Modifiers – anxiety management;
psychological understanding; premorbid
personality
Staff modifiers – explanation; information;
role modelling; patient education; not too
little and not too much presence
Flashpoints – crowding; queuing; waiting;
noise; bullying; stealing

Outside hospital
Stressors – Visitors; relatives; dependency
and institutionalisation; demands from
home
Staff modifiers – carer relative involvement;
family therapy; active patient support
Flashpoints – Bad news; home crisis; loss
of relationship
Physical environment
Physical environment - Locked doors;
seclusion; fabric and comfort
Staff modifiers – care and attention to
property; décor maintenance;
Patient – modifiers – respect for property;
sharing; admission process
Regulatory framework
External factors – legal restrictions; national
policy; complaints; appeals; prosecutions;
hospital policy
Staff modifiers – Justice; respect for rights;
hope; information giving; flexibility.
Flashpoints – compulsory detention;
admission process; appeal refusal;
complaint not upheld; enforced treatment;
exit refused
Staff Team
Internal structure – rules; routine;
efficiency; ideology
Staff modifiers – leadership; staff anxiety;
control; psychological understanding;
teamwork and consistency; positive
appreciation
Flashpoints – denial if requests; demands;
limit setting; ignoring patients
Mentalizing
Mentalizing and the mindful
clinician
What is happening in the patient’s mind to
make him/her behave like this?
Can I, the clinician
talk to him to elicit his current mental state
Identify the dominant emotion and belief
Accept our contribution to creating this state
Be compassionate about his current narrative
What is mentalizing?
Mentalizing is a form of imaginative
mental activity about others or oneself,
namely, perceiving and interpreting
human behaviour in terms of
intentional mental states (e.g. needs,
desires, feelings, beliefs, goals,
purposes, and reasons).
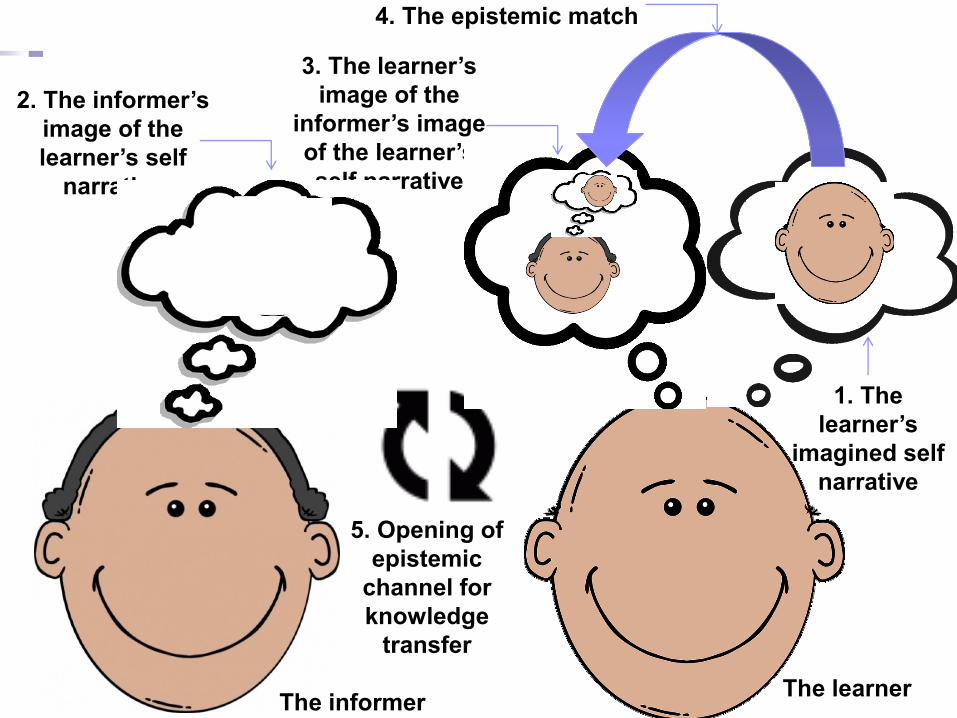
The learner
1. The
learner’s
imagined self
narrative
5. Opening of
epistemic
channel for
knowledge
transfer
4. The epistemic match
2. The informer’s
image of the
learner’s self
narrative
3. The learner’s
image of the
informer’s image
of the learner’s
self narrative
The informer

Creating a peaceful school
learning environment
Stuart W. Twemlow, Peter Fonagy,
Eric M. Vernberg, Jennifer A. Mize,
Edward J. Dill, Todd D. Little,
John A. Sargent

Assumptions, Aims and Adjuncts
The whole school community contributes
to bullying-related dysfunction
Peaceful collaboration with others
requires prioritizing their subjective
states, thus placing limits upon the urge
to violently control the behaviour of less
powerful members of the group

Assumptions, Aims and Adjuncts CAPSLE aims constantly to focus on the mental
states of all those involved in the power dynamics
of interpersonal violence (the bystander as well
as the bully and the victim) through:
a positive climate campaign to draw attention to the
subjective experiences of bully, victim, and bystander
a classroom management plan that requires teachers
to elaborate the thoughts and feelings associated with
acts of aggression in the classroom
a defensive martial arts program based on mindfulness
peer or adult mentorship that create additional
opportunities for reflective interpersonal interaction
reflection time which offers opportunities for the class
to consider shared immediate past experience together

Increasing Mentalization Should Reduce
Violence: The Peaceful Schools Project
9 schools randomly assigned to
CAPSLE
School Psychiatric Consultation
Treatment as usual
oProgrammes as usual
Design
3 year study
2 years of formal manualized intervention
3rd year test of generalisation

10 Schools, including 2,712
Children, Stratified and Cluster
Randomized
19 Eligible Elementary Schools,
Including 6,522 K-5th Grade Children
10 Elementary Schools Elected To
Participate, Including 2,712 Children
1 School
(178 Children)
Withdrew From
Treatment as
Usual
Condition
675 Children
Treatment as Usual
In 3 Schools
824 Children
SPC
In 3 Schools
1,035 Children
CAPSLE
In 3 Schools
Only 3rd-5th Grade Children
Completed Research Instruments
SPC Children
Participating
296 in Year 1
283 in Year 2
323 in Year 3
CAPSLE Children
Participating
391 in Year 1
356 in Year 2
395 in Year 3
Treatment as Usual
Children Participating
271 in Year 1
221 in Year 2
217 in Year 3

Key Results of The Peaceful Schools
Project: Peer Nomination
SPC vs TAU
Increase in helpful bystanding (p<.05)
o evident only in the first year of the intervention
CAPSLE vs TAU
significant on four out of the eight primary
outcome variables
peer-reported aggression (p < .05)
peer-reported victimization (p < .01)
aggressive bystanding (p < .05)
empathic mentalizing with victim (p < .01)
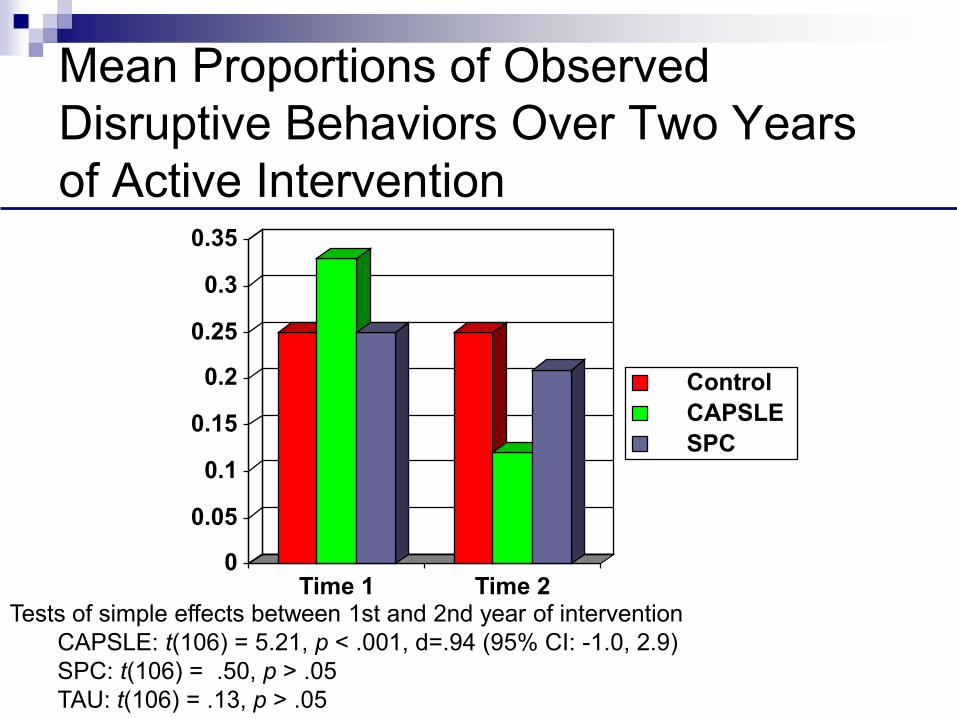
Mean Proportions of Observed
Disruptive Behaviors Over Two Years
of Active Intervention
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
Time 1 Time 2
Control
CAPSLE
SPC
Tests of simple effects between 1st and 2nd year of intervention
CAPSLE: t(106) = 5.21, p < .001, d=.94 (95% CI: -1.0, 2.9)
SPC: t(106) = .50, p > .05
TAU: t(106) = .13, p > .05

Mean Proportions of Observed Off-task
Behaviors Over Two Years of Active
Intervention
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
Time 1 Time 2
Control
CAPSLE
SPC
Tests of simple effects between 1st and 2nd year of intervention
CAPSLE: t(106) = 8.26, p < .001, Cohen’s d=1.61 (95% CI: -.38, 3.6)
SPC: t(106) = 1.19, p > .05
TAU: t(106) = .14, p > .05
Some basic
mentalizing interventions

Implications for understanding and treating borderline
personality disorder as a social
vulnerability disorder
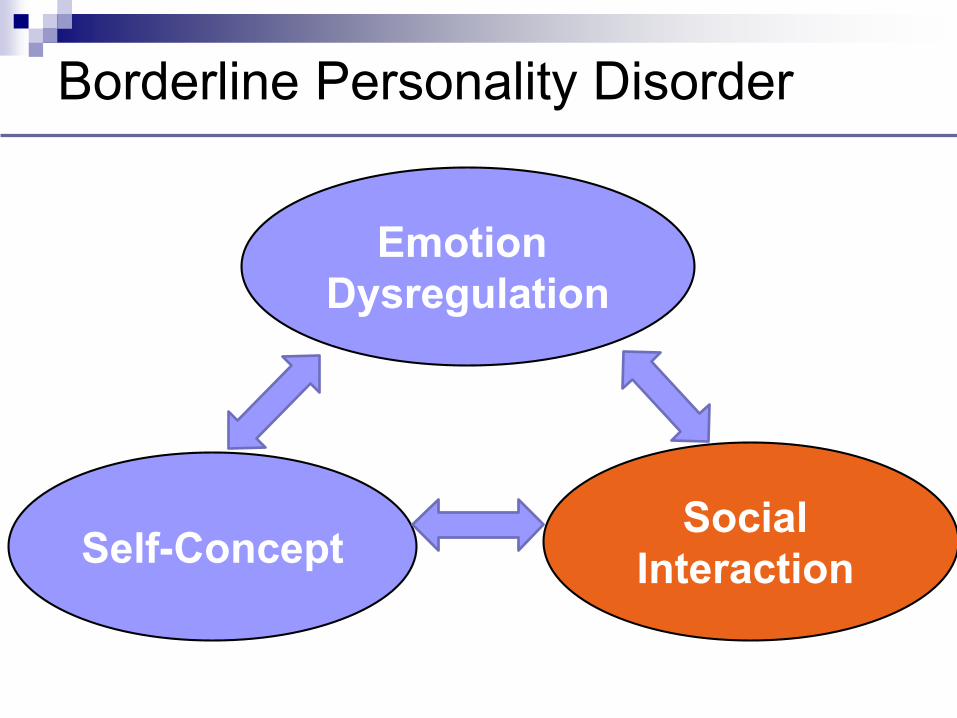
Borderline Personality Disorder
Self-ConceptSocial
Interaction
Emotion
Dysregulation

What do you feel looking at this picture?

I depend on others a lot
I can‘t manage when people don‘t respond
to me
I am an outsider
I am different from others (shame)
Others will reject me
I do not deserve being part of the group
(guilt)
I am ugly (self-contempt- self disgust)
Reported Social Cognitions in BPD
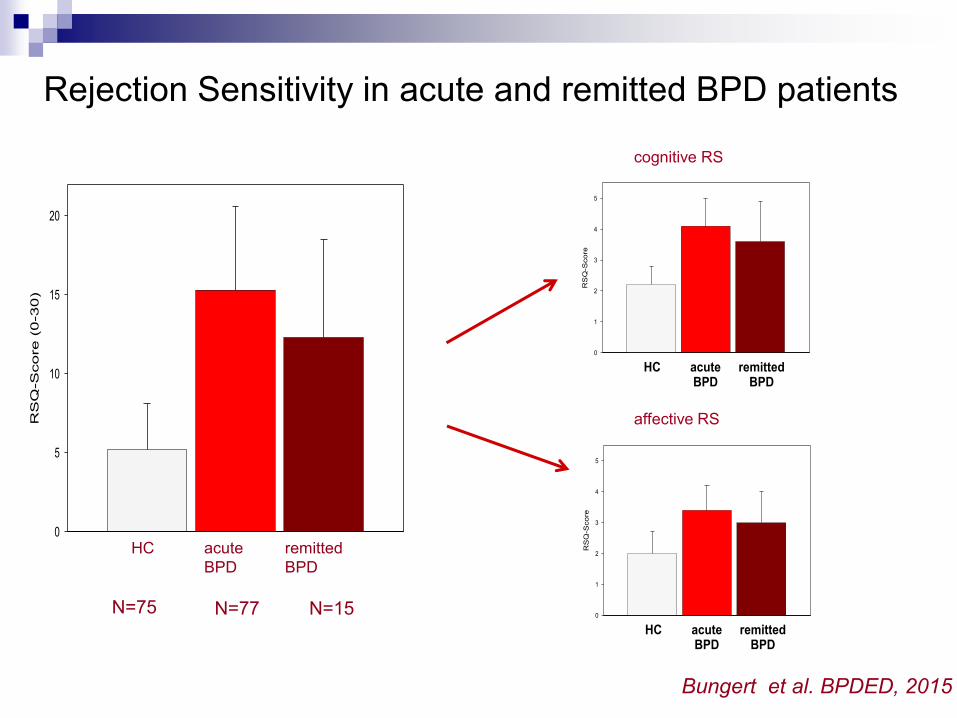
Rejection Sensitivity in acute and remitted BPD patients
HC
RS
Q-S
co
re
(0
-3
0)
0
5
10
15
20
acuteBPD
remittedBPD
HC
RS
Q-S
core
0
1
2
3
4
5
acuteBPD
remittedBPD
HC
RS
Q-S
co
re
0
1
2
3
4
5
acuteBPD
remittedBPD
cognitive RS
affective RS
HC acute
BPD
remitted
BPD
N=77 N=15N=75
Bungert et al. BPDED, 2015
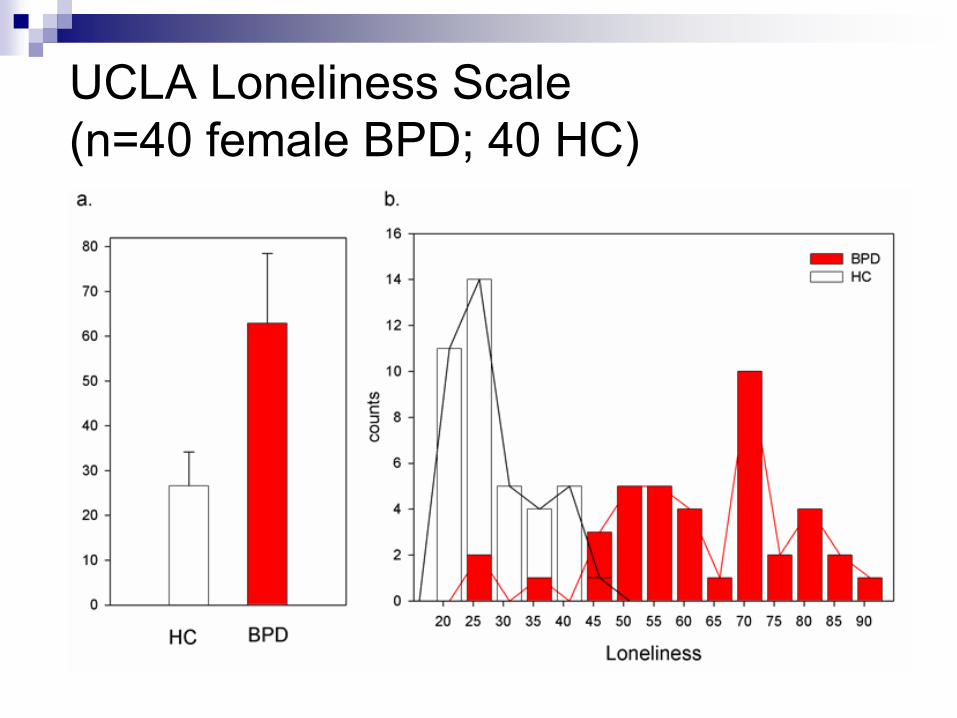
UCLA Loneliness Scale
(n=40 female BPD; 40 HC)
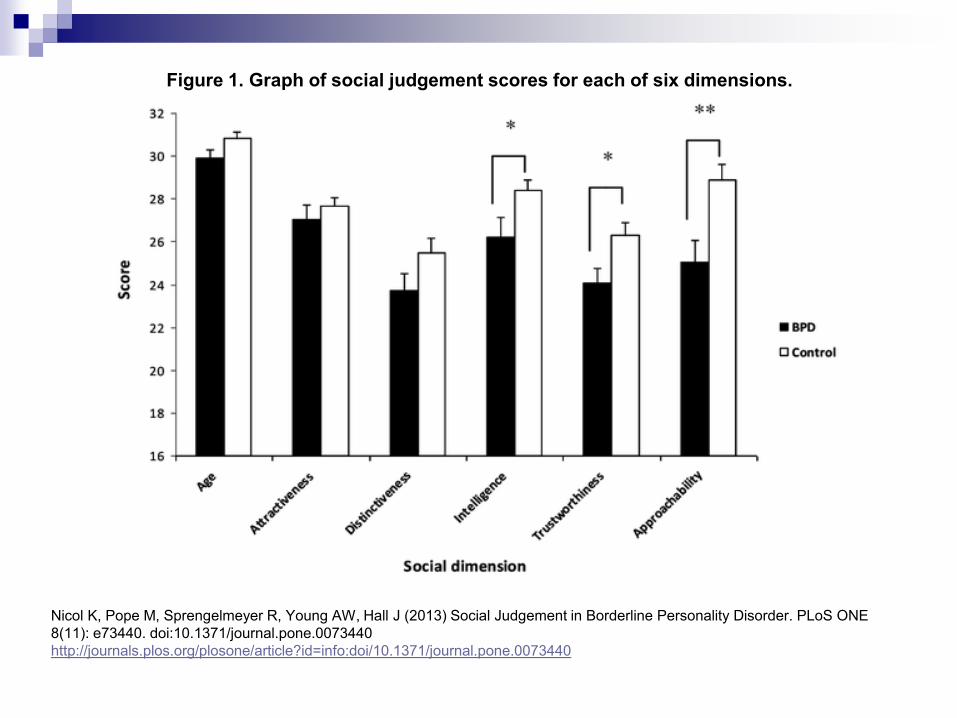
Figure 1. Graph of social judgement scores for each of six dimensions.
Nicol K, Pope M, Sprengelmeyer R, Young AW, Hall J (2013) Social Judgement in Borderline Personality Disorder. PLoS ONE
8(11): e73440. doi:10.1371/journal.pone.0073440
http://journals.plos.org/plosone/article?id=info:doi/10.1371/journal.pone.0073440
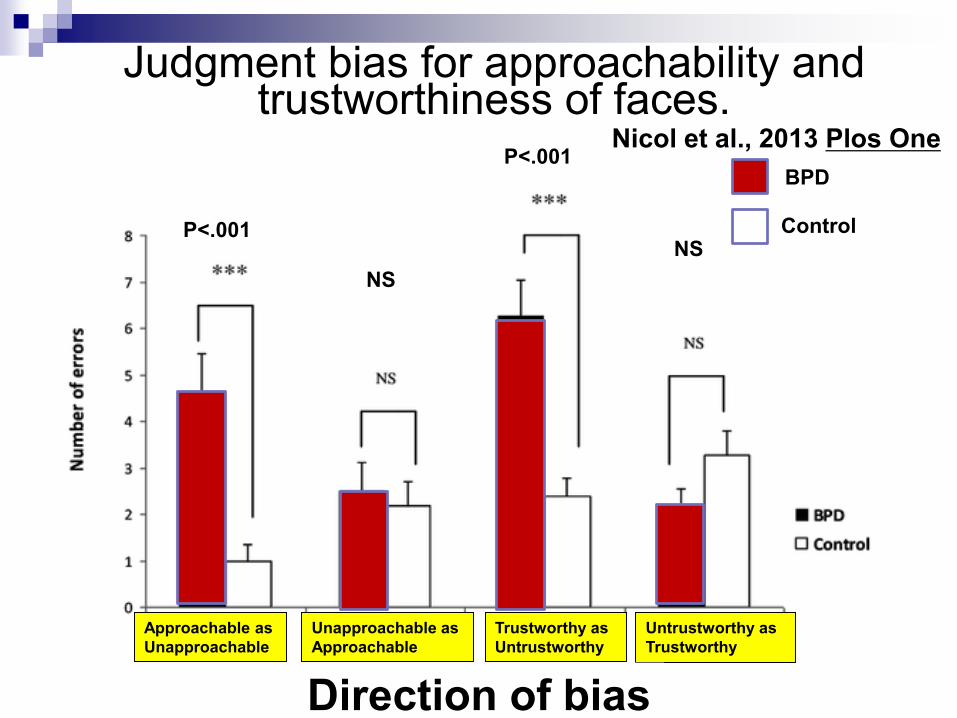
Approachable as
Unapproachable
Unapproachable as
Approachable
Trustworthy as
Untrustworthy
Untrustworthy as
Trustworthy
Judgment bias for approachability and trustworthiness of faces.
NS
NS
BPD
ControlP<.001
P<.001
Direction of bias
Nicol et al., 2013 Plos One
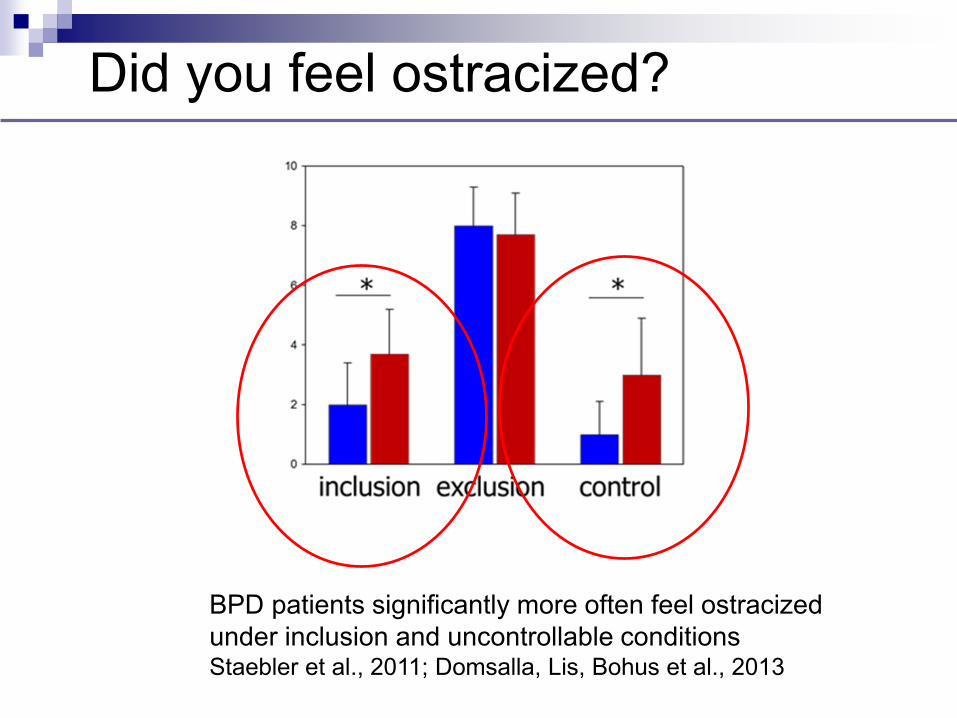
Did you feel ostracized?
BPD patients significantly more often feel ostracized
under inclusion and uncontrollable conditionsStaebler et al., 2011; Domsalla, Lis, Bohus et al., 2013
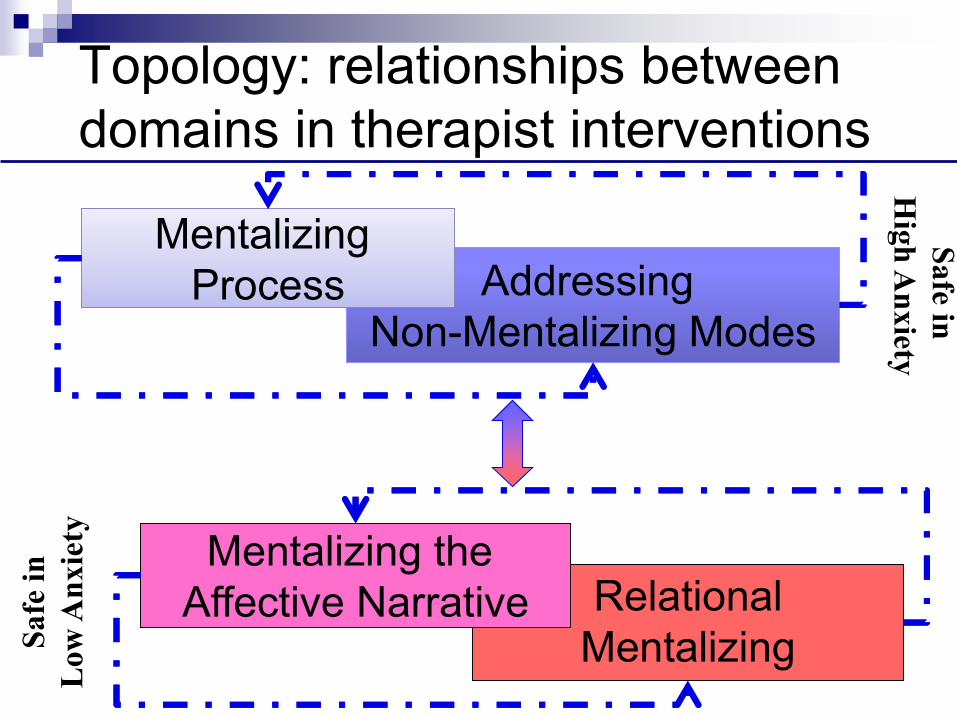
Topology: relationships between
domains in therapist interventions
Addressing
Non-Mentalizing Modes
Addressing
Non-Mentalizing Modes
Mentalizing
Process
Mentalizing
Process
Safe in
Hig
h A
nxiety
Relational
MentalizingSafe
in
Low
An
xie
ty
Mentalizing the
Affective Narrative
Aims of Formulation Aims
Organise thinking for therapist and patient – each sees different minds
Modelling a mentalising approach in formal way – do not assume that patient can do this (explicit, concrete, clear and exampled)
Modelling humility about nature of truth
Management of risk
Analysis of components of risk in intentional terms
Avoid over-stimulation through formulation
Beliefs about the self
Relationship of these to specific (varying) internal states
Historical aspects placed into context
Central current concerns in relational terms
Identification of attachment patterns – what is activated
Challenges that are entailed
Positive aspects
When mentalisation worked and had effect of improving situation
Anticipation for the unfolding of treatment
Impact of individual and group therapy
Empathic Validation:
Underpinning mentalizing process
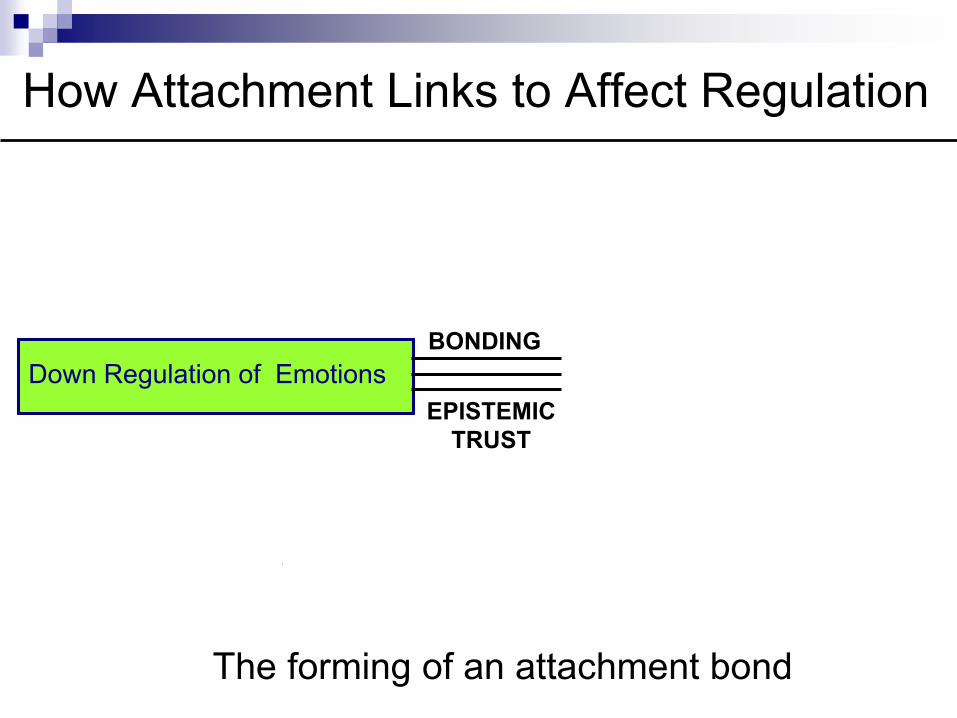
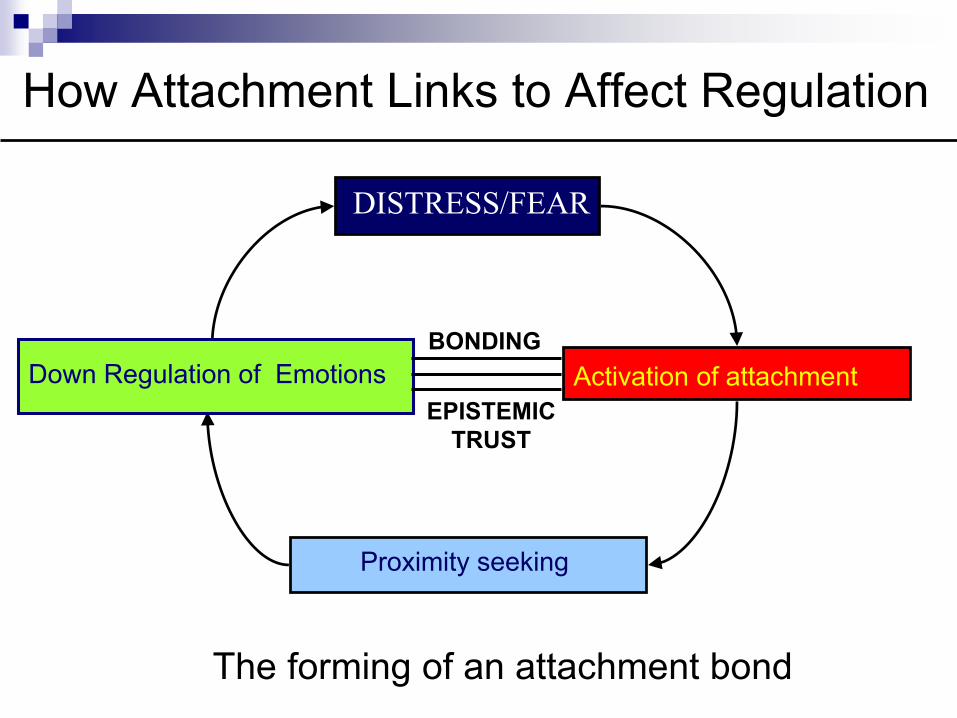
How Attachment Links to Affect Regulation
DISTRESS/FEAR
Exposure to Threat
Proximity seeking
Activation of attachment
The forming of an attachment bond
Down Regulation of Emotions
EPISTEMIC
TRUST
BONDING
How Attachment Links to Affect Regulation
DISTRESS/FEAR
Exposure to Threat
Proximity seeking
Activation of attachment
The forming of an attachment bond
Down Regulation of Emotions
EPISTEMIC
TRUST
BONDING
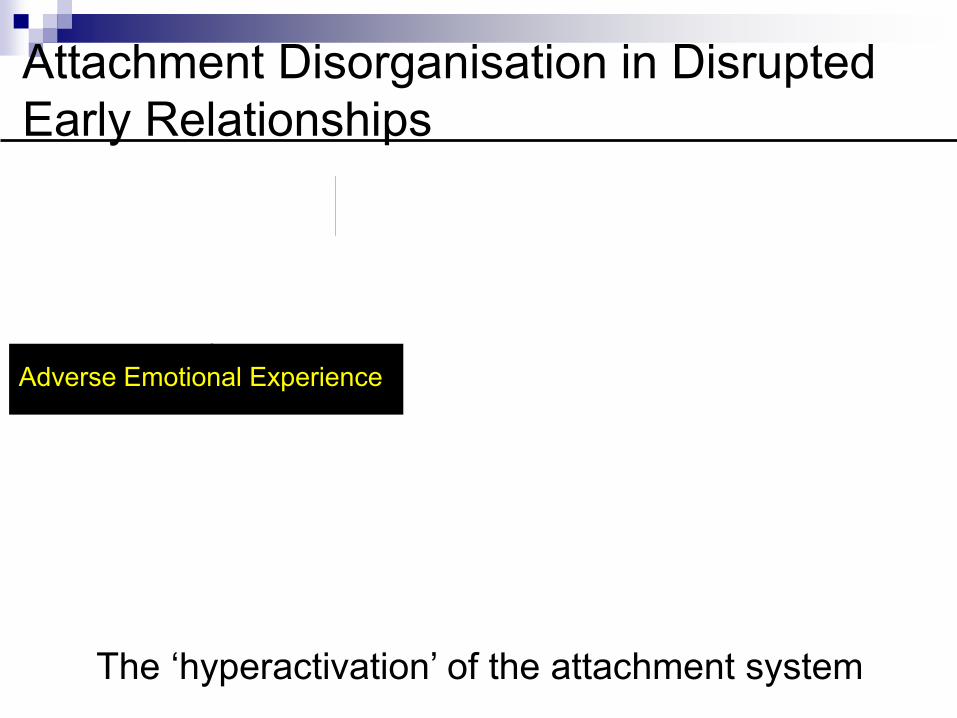
Attachment Disorganisation in Disrupted
Early Relationships
DISTRESS/FEAR
Exposure to threat
Proximity seeking
Activation of attachment
The ‘hyperactivation’ of the attachment system
Adverse Emotional Experience

Attachment Disorganisation in Disrupted
Early Relationships
DISTRESS/FEAR
Exposure to threat
Proximity seeking
Activation of attachment
The ‘hyperactivation’ of the attachment system
Adverse Emotional Experience
Empathic Validation – Affect and Effect
Interest in and Reflection on Affect
Identification of feelings
Normalising when possible in context of
present and past
Seeing it through their eyes
What effect does this experience have on
them


Staff Teams
And
Working together
Anna Freud National Centre for Children and Families
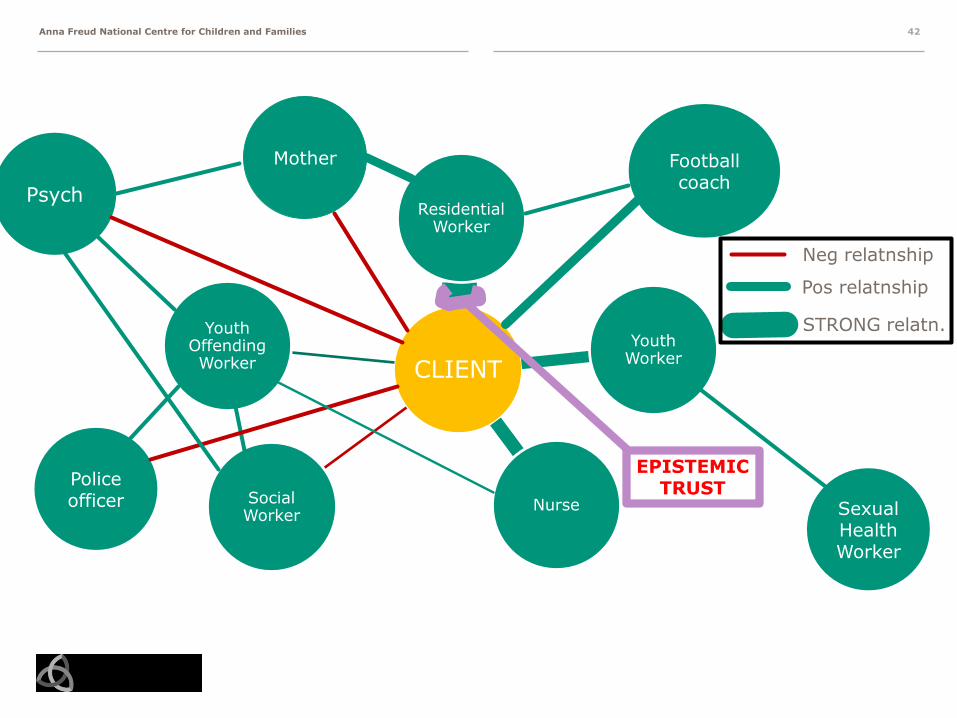
CLIENT
Residential Worker
Youth Worker
NurseSocial Worker
Youth Offending Worker
42
Psych
Mother
Sexual Health Worker
Police officer
Football coach
Neg relatnship
Pos relatnship
STRONG relatn.
EPISTEMICTRUST
Anna Freud National Centre for Children and Families
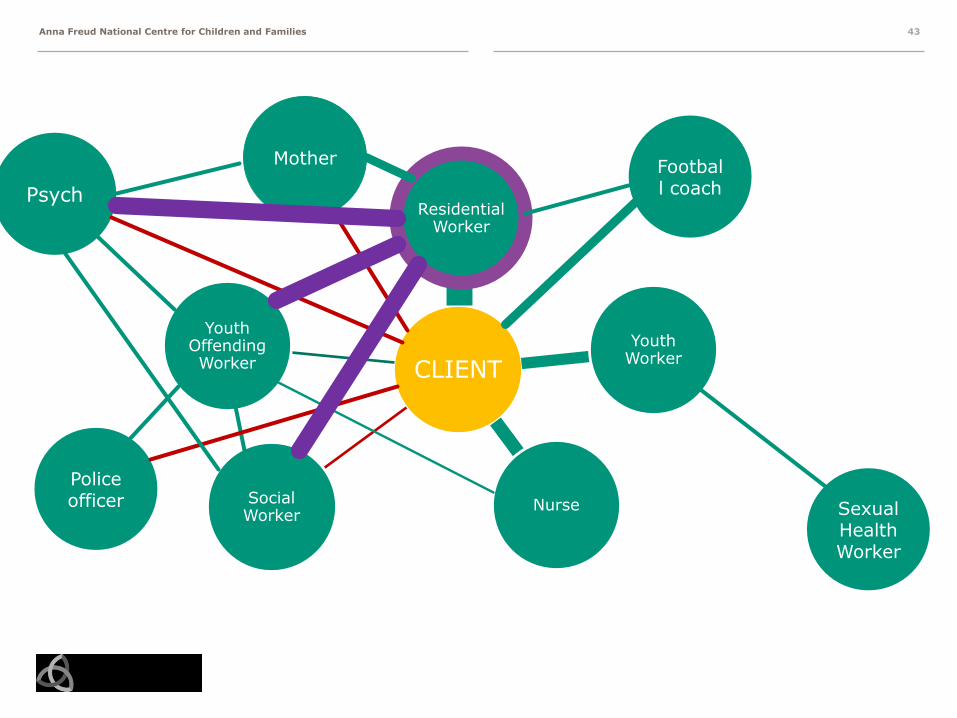
CLIENT
Residential Worker
Youth Worker
NurseSocial Worker
Youth Offending Worker
43
Psych
Mother
Sexual Health Worker
Police officer
Football coach

Anna Freud National Centre for Children and Families
CLIENT
Residential Worker
Youth Worker
NurseSocial Worker
Youth Offending Worker
44
Psych
Mother
Sexual Health Worker
Police officer
Football coach
THE “KEY” WORKER IS NOT AN ORGANISATIONAL ROLE,IT IS WHO THE CLIENT SEES AS “GETTING ME” AT THAT TIME

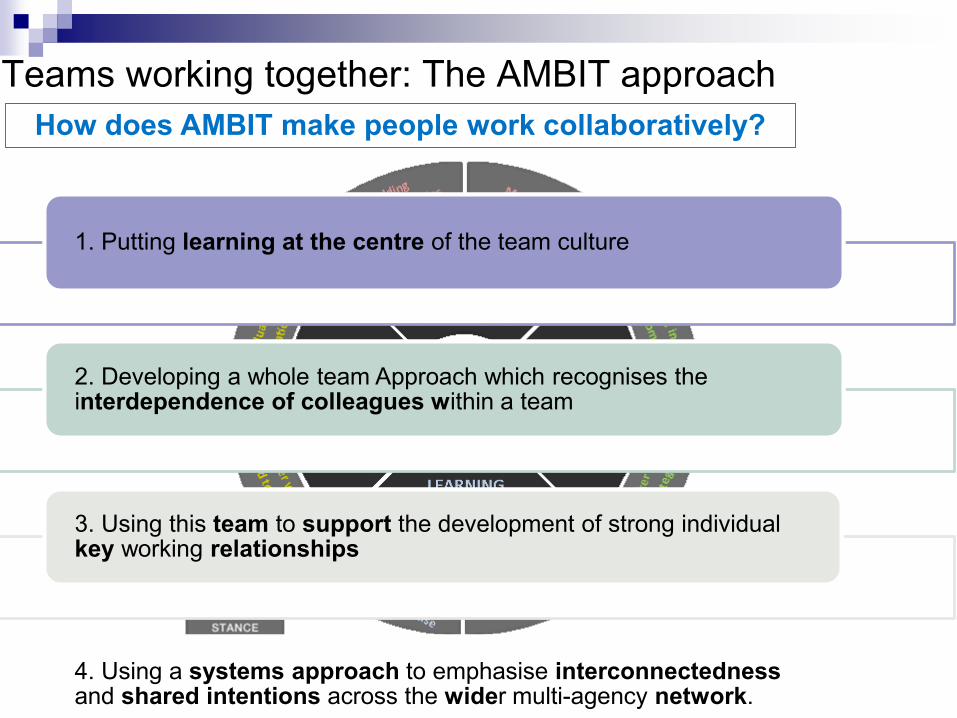
Teams working together: The AMBIT approach
MentalizingMentalizing
© Bevington & Fugglehttp://ambit.tiddlyspace.com/
Teams working together: The AMBIT approach
MentalizingMentalizing
© Bevington & Fuggle
How does AMBIT make people work collaboratively?
1. Putting learning at the centre of the team culture1. Putting learning at the centre of the team culture
2. Developing a whole team Approach which recognises the interdependence of colleagues within a team2. Developing a whole team Approach which recognises the interdependence of colleagues within a team
3. Using this team to support the development of strong individual key working relationships3. Using this team to support the development of strong individual key working relationships
4. Using a systems approach to emphasise interconnectednessand shared intentions across the wider multi-agency network. 4. Using a systems approach to emphasise interconnectednessand shared intentions across the wider multi-agency network.
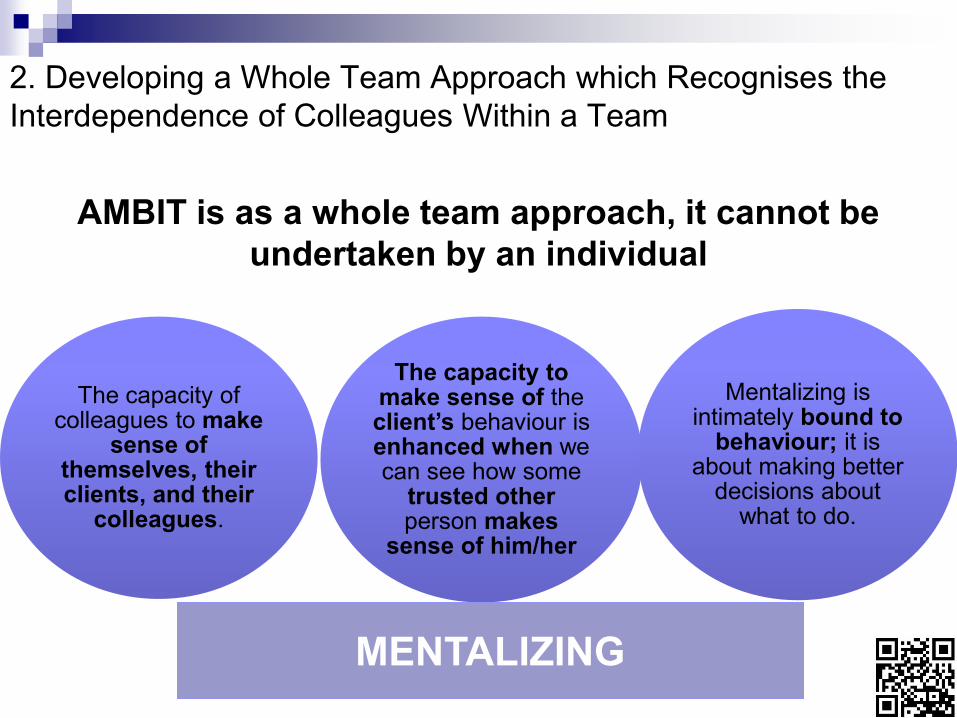
AMBIT is as a whole team approach, it cannot be
undertaken by an individual
The capacity to make sense of the client’s behaviour isenhanced when we can see how some
trusted other person makes
sense of him/her
Mentalizing is intimately bound to
behaviour; it is about making better
decisions about what to do.
The capacity of colleagues to make
sense of themselves, their clients, and their
colleagues.
MENTALIZINGMENTALIZING
2. Developing a Whole Team Approach which Recognises the
Interdependence of Colleagues Within a Team

3. Using this Team to Support the Development of
strong Individual Key Working Relationships
The person needs to experience his/her mind being held accurately,
respectfully and safely in the mind of a trusted other
The person needs to experience his/her mind being held accurately,
respectfully and safely in the mind of a trusted other
AMBIT invests in a single key helping relationship
that the person may, perhaps over some time, come to
trust.
AMBIT invests in a single key helping relationship
that the person may, perhaps over some time, come to
trust.
The ‘keyworker’ is the worker who is the “key” professional in the mind of the person -the worker who they feel
most understood by.
The ‘keyworker’ is the worker who is the “key” professional in the mind of the person -the worker who they feel
most understood by.
Worker must be well integrated and supported by a team that understands the maintenance of their mentalizing as a shared
responsibility
Worker must be well integrated and supported by a team that understands the maintenance of their mentalizing as a shared
responsibility
Establishment of Individual Trusting
Relationships between Person and
Key Worker
Establishment of Individual Trusting
Relationships between Person and
Key Worker
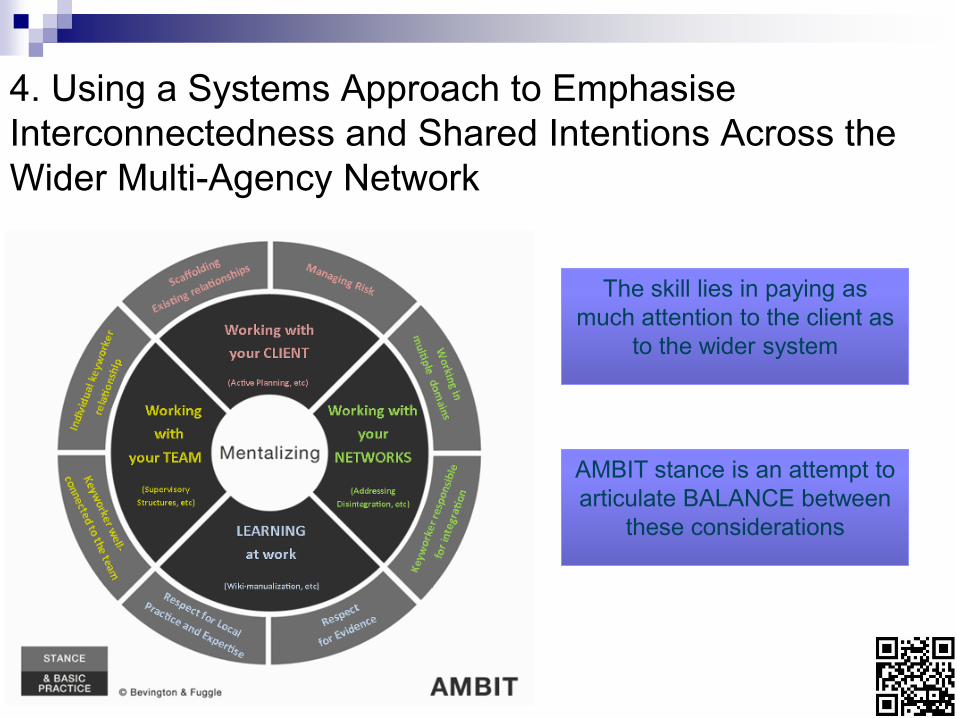
The skill lies in paying as
much attention to the client as
to the wider system
The skill lies in paying as
much attention to the client as
to the wider system
AMBIT stance is an attempt to
articulate BALANCE between
these considerations
AMBIT stance is an attempt to
articulate BALANCE between
these considerations
4. Using a Systems Approach to Emphasise
Interconnectedness and Shared Intentions Across the
Wider Multi-Agency Network
Thank you for
considering mentalizing!
For further information
Slides available at:
http://www.ucl.ac.uk/psychoanalysis/people/bateman