Mental load: helping clinical learners
4
Mental load: helping clinical learners Geoff White, Clinical Education and Professional Development Unit, School of Primary Health Care, Monash University, Australia SUMMARY Background: The quality of an individual’s learning is influenced significantly by the quantity of mental processing they are required to manage in a clinical learning situation. Some clinical learning settings require the learner to process high levels of complex knowledge and skills, whilst simultaneously monitoring and responding to challenging social or emotional inputs. This paper introduces the concept of ‘cognitive load’, its negative impacts upon novice learners in particular, and its real-world implications for teaching and supervision. Method: Narrative review and discussion. Results: The concept of cognitive load is reviewed, and examples of its application to clinical learning and teaching are provided. Teaching and supervision strate- gies for managing the cognitive load of learners are presented. Discussion: The clinical teacher has significant capacity to reduce the cognitive load of learners by creating safe and supportive learning environments, establish- ing trusting relationships with the learner, and implementing structured learning experiences that are designed to support the learner’s growth in knowledge, understanding and skills. A threefold focus on the nature of the learning task, the learning environment and the learner’s perceptions of these elements, which characterises cognitive load, provides a useful framework for diagnosing poor learning behaviours and maximising learn- ing outcomes. The clinical teacher has significant capacity to reduce the cognitive load of learners Guiding the learner 168 Ó Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 168–171
-
Upload
geoff-white -
Category
Documents
-
view
213 -
download
0
Transcript of Mental load: helping clinical learners

Mental load: helpingclinical learnersGeoff White, Clinical Education and Professional Development Unit, School of PrimaryHealth Care, Monash University, Australia
SUMMARYBackground: The quality of anindividual’s learning is influencedsignificantly by the quantity ofmental processing they arerequired to manage in a clinicallearning situation. Some clinicallearning settings require thelearner to process high levels ofcomplex knowledge and skills,whilst simultaneously monitoringand responding to challengingsocial or emotional inputs. Thispaper introduces the concept of‘cognitive load’, its negativeimpacts upon novice learners in
particular, and its real-worldimplications for teaching andsupervision.Method: Narrative review anddiscussion.Results: The concept of cognitiveload is reviewed, and examplesof its application to clinicallearningandteachingareprovided.Teaching and supervision strate-gies for managing the cognitiveload of learners are presented.Discussion: The clinical teacherhas significant capacity to reducethe cognitive load of learners bycreating safe and supportive
learning environments, establish-ing trusting relationships withthe learner, and implementingstructured learning experiencesthat are designed to support thelearner’s growth in knowledge,understanding and skills. Athreefold focus on the nature ofthe learning task, the learningenvironment and the learner’sperceptions of these elements,which characterises cognitiveload, provides a useful frameworkfor diagnosing poor learningbehaviours and maximising learn-ing outcomes.
The clinicalteacher hassignificantcapacity toreduce the
cognitive loadof learners
Guidingthe learner
168 � Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 168–171

INTRODUCTION
Sam: a hypothetical nursingstudent
Sam, a nursing student onrotation in critical care,comes to the intensive care
unit as part of his mandatorycourse requirements. Stella is theclinical teacher assigned to hisclinical supervision. By week two ofSam’s rotation Stella has noticedthat Sam frequently ‘misses thepoint’ of concepts she is explainingto him, and also struggles withprocedures that involve multiplesteps.
Stella wonders what could be con-tributing to Sam’s learning prob-lems. Are the concepts and skillstoo difficult for him? Are thelearning activities too difficult? Isit a combination of both?
COGNITIVE LOAD
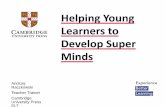
Cognitive load theory is a mem-ory-based model that sees learn-ing as involving the movement ofinformation from a learner’sshort-term memory (STM) to theirlong-term memory (LTM).1,2
Learning occurs when new infor-mation is linked to existingunderstanding in the LTM, result-ing in more complex and elabo-rate knowledge structures, knownas ‘schemas’.
As we all know from our ownlearning experiences, this processcan be problematic. In compari-son with LTM, STM, also known as‘working memory’, has a limitedcapacity to hold and process newinformation and experiences:there is a bottleneck or constric-tion in the flow of informationfrom STM to LTM. The informationflow is not one-way, however, aslearning involves LTM beingdrawn upon by STM to make senseof new inputs, and the bottlenecksqueezes information in bothdirections (Figure 1).2
Anything that causes thelearner to divert their mental
processing away from this move-ment of information applies acognitive ‘load’ that narrows thebottleneck and reduces its flow(Figure 2).2
SamOn the second week of Sam’s rota-tion Stella is facilitating his clinicalsupport when he comments to herthat he is ‘feeling constantly over-whelmed by the clinical environ-ment’. He says he feels overwhelmedby the unfamiliar equipment andnoises on a daily basis. Sam alsotells Stella that he often feelsdistressed about the patients he iscaring for as they are very ill, and hefeels anxious every day.
Kirschner, Sweller and Clarkidentify three forms ofcognitive load: intrinsic,relevant and extraneous.3 Theintrinsic load is determined byboth the complexity of the con-tent or skill being learned andthe learner’s expertise. Therelevant load is related to themental effort required by theteaching and learningactivities, and the extraneousload is caused by anything thatdiverts the learner’s mentalactivity. Problem solving that isunsupported by the teacher orsupervisor is an example of alearning activity with highrelevant load. In the case of ourhypothetical student nurse, Sam,although the nature of thelearning tasks may hold somedegree of intrinsic and relevantload, his learning is limited bythe extraneous load resultingfrom anxiety-related stresscaused by the clinical learningenvironment.
COGNITIVE LOAD ANDPROBLEM SOLVING
Novice health professionals areoften engaged in problem solvingin clinical and formal learningsituations, and problem solvinghas high intrinsic and relevantload components. This load arisesfrom the learner having to allo-cate cognitive resources to con-sider questions such as: what isthe actual problem; what steps doI have to take to solve thisproblem; which do I do first;where would I find the requiredinformation?
GROUP PROBLEM SOLVING
Group work can often result inincreased cognitive load for bothnovice and expert learners beyondthat required by the problemsolving activity.4 This load isgenerally greater for novices,particularly when the group is notperforming optimally. The in-creased load arises from thelearner having to consider groupdynamics in addition to process-ing the solution to the problem.Questions such as: who’s doingthe various tasks required to solvethis problem; which ones am Iresponsible for; when do I have tofinish them; are the other group
a memory-basedlearning model
Short-term memory Long-term memoryLong-term memory
Working memoryWorking memory
working memory usesLTM content too
Figure 1. Bottleneck between long-term memory and short-tem memory
Cognitive load
Working memory Long-term memory
Figure 2. Diagram representing increased cog-
nitive load
Problem solvingthat isunsupported bythe teacher orsupervisor is anexample of alearning activitywith highrelevant load
� Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 168–171 169

members responsible workers;have they shown themselves to bereliable in the past; what will I doif they don’t contribute?
Group problem solving there-fore adds a higher risk of extra-neous load to what is already ahigh cognitive load activity.Clark, Nguyen and Sweller capturethe learners’ perspective on thiscomplexity:
We’re trying to sail the boatat the same time that we arebuilding it.4
TEACHER AND SUPERVISORGUIDANCE
In contrast to some proponentsof problem-oriented learning,Kirschner, Sweller and Clark3
advocate a greater involvementof teachers, tutors and supervi-sors in their students’ learning.
Clinical educators can reduceall three categories of cognitiveload by the provision of guidanceand close monitoring of groupprocesses. Guidance focused onreducing the load associated withthe nature of the learning task(intrinsic and relevant) can take anumber of forms, including: pro-viding carefully chosen examples;teacher modelling of the desiredlearning; helping students tobreak a task, sequence or complexconcept into component parts(‘chunking’); and providing qual-ity feedback.
A further example can befound in the Advanced TraumaLife Support (ATLS) model of skillsteaching.5 The ATLS approach is apowerful five-phase strategy forreducing cognitive load in theclinical setting by virtue of itsstructured support of the learneras they move towards skillsattainment (Figure 3).
Phase 1: overview• Instructor explains why the
skill is needed.
• Instructor explains how theskill is used in the delivery ofcare.
Phase 2: silent demonstration• Instructor provides the learner
with a mental picture of whatthe skill looks like when per-formed correctly.
Phase 3: narrativedemonstration
• Instructor repeats the proce-dure while describing the pro-cess in detail.
Phase 4: learner narrative• Learner talks through the skill
whilst performing it for thefirst time.
• Instructor may perform theskill at the same time as thelearner.
Phase 5: learner performance• Learner performs the skill.
• Teacher observes, providesfeedback and coaches asnecessary.
WHAT CAN CLINICALTEACHERS DO TO MANAGEEXTRANEOUS LOAD?
Clinical teachers have asignificant capacity for influenc-ing a major cause of extraneousload: unsafe learning environ-ments. Learning environments inwhich learners do not feel safe,supported and included will inev-itably result in them divertingresources away from their learn-ing. We should be monitoring theways in which we relate to ourlearners, including the quality ofour feedback. We should also bemonitoring and managing thesocial dynamics within the groupswe teach with a view to ensuringthat our learners feel supported.These are key teacher behavioursthat will reduce extraneous load,and although ineffective learningenvironments impact upon bothnovice and expert learners, their
The teacher guidancecontinuum
Guided Unguided/minimal
guidance
Figure 3. The teacher guidance continuum
Cognitive load[can be
reduced] by theprovision of
guidance andclose
monitoring ofgroup processes
170 � Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 168–171

impact will be greater upon thenovices.
It should be noted, however,that the guidance strategieshelpful to novices have beenfound to reduce learning inexperts. Expert learners benefitfrom greater autonomy andreduced teacher guidance.
MANAGING SAM’SEXTRANEOUS COGNITIVELOAD
Now that Stella is aware of Sam’sconcerns and anxieties she looksfor ways to reduce his cognitiveload. As a first step, Stella tries tounderstand Sam’s situation betterby making time to talk with himoutside the intensive care unit(ICU). She then plans a progres-sive immersion process for Samthat allows him time to adjust to
the stressful learning environmentof the ICU over 5 or 6 days. Stellaalso uses the ALTS model to teachSam the skills he is required togain so that intrinsic and relevantloads are reduced, thereby allow-ing him more cognitive ‘space’ tomanage the extraneous load.
Stella also realises thatalthough Sam’s extraneous load isunusual in her experience, otherhealth professionals who aretransitioning into new learningand working environments wouldalso probably benefit from induc-tion programmes that recognisethe influence of cognitive load.
CONCLUSION
Although the concept of cognitiveload is one that we can all relateto, it provides a powerful lens for
viewing and understanding clini-cal learning. Whether applied toour own learning, the difficultcolleague or the strugglingstudent we are supervising, thenotions of intrinsic, relevant andextraneous load can lead us todeeper insights and improvedclinical education practice.
REFERENCES
1. van Merrienboer J, Sweller J.
Cognitive load theory in health
professional education: design
principles and strategies. Med Educ
2010;44:85–93.
2. van Merrienboer J, Kirschner P,
Kesterer L. Taking the load off a
learner’s mind: Instructional design
for complex learning. Psychologist
2003;38:5–13.
3. Kirschner P, Sweller J, Clark R. Why
minimal guidance during instruction
does not work: an analysis of the
failure of constructivist, discovery,
problem-based, experiential and
inquiry-based teaching. Educational
Psychologist 2006;41:75–86.
4. Clark R, Nguyen F, Sweller J. Efficiency
in learning: evidence-based guidelines
to manage cognitive load. San Fran-
cisco: Pfeiffer; 2006.
5. George J, Dotto F. A simple five-step
method for teaching clinical skills.
Family Medicine 2001;8:577–578.
6. Sweller J, Kirschner P, Clark R. Why
minimally guided teaching tech-
niques do not work: a reply to
commentaries. Educational
Psychologist 2007;42:115–121.
Corresponding author’s contact details: Geoff White, Clinical Education and Professional Development Unit, Level 1, Building 2, 270 FerntreeGully Road, Notting Hill, VIC 3168, Australia. E-mail: [email protected]
Funding: None.
Conflict of interest: None.
Ethical approval: Not required.
Cognitive loadprovides apowerful lensfor viewing andunderstandingclinical learning
� Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 168–171 171