
Mental Hygiene Administration Mental Hygiene Annual Conference May 2,2012 Brian Hepburn, M.D.,...
22
Mental Hygiene Administration Mental Hygiene Annual Conference May 2,2012 Brian Hepburn, M.D., Executive Director Maryland Mental Health Administration
-
Upload
della-harvey -
Category
Documents
-
view
219 -
download
0
Transcript of Mental Hygiene Administration Mental Hygiene Annual Conference May 2,2012 Brian Hepburn, M.D.,...
Mental Hygiene Administration
Mental Hygiene Annual ConferenceMay 2,2012
Brian Hepburn, M.D.,Executive DirectorMaryland Mental Health Administration

Maryland’s Public Mental Health System (PMHS) is committed to the philosophy of providing safe and effective treatment at the least intensive level of care necessary to meet the individual’s need. MHA promotes a system that supports recovery and resilience across the life span.

State Psychiatric Facilities
The State of Maryland currently operates 5 State Psychiatric Facilities, including 1 Forensic hospital, and 2 Residential Institutes for Adolescents and Children (RICA)
Admissions to State hospitals have decreased by 57% since 2002. 80% of admissions in FY11 were Forensic.
Civil admissions have decreased as a result of a decision that civil admissions should go to the acute general or private psychiatric units. Recent implementation of EMTALA has also greatly affected civil admits.
Average Length of Stay (ALOS) has increased from the lowest recorded for the year in 2003 (n=132 days), to the highest logged ALOS in the past 3 years, 328, 380 and 311 days respectively.

State Admissions by Forensic Status FY 2002-11
Fiscal Year
Non-Forensic Forensic TOTAL Admissions
TOTAL Dischar
ges ALOS*
2002 2,306 862 3,168 3,196 149
2003 2,240 738 2,978 2,959 132
2004 2,348 777 3,125 3,256 207
2005 1,841 840 2,681 2,624 133
2006 1,783 838 2,621 2,667 177
2007 1,217 890 2,107 2,119 195
2008 883 935 1,818 1,853 257
2009 532 985 1,517 1,622 328
2010 379 989 1,368 1,353 380
2011 265 1,104 1,369 1,083 311
CT Perkins Included. RICAs excluded. *ALOS is calculated based on true admission and discharge date. Represented in days.

Public Mental Health System (PMHS)
In 1997, 1115 waiver implemented in Maryland, mental health services were carved out into the managed fee-for-service system. Many services that had previously been grant funded became funded on a fee-for-service basis.
Nearly all non-emergency service require pre-authorization. Services are authorized and claims processed and paid through an Administrative Services Organization (ASO). Current ASO-Value Options.
Eligibility data from Medicaid feeds daily into the ASO data system. Used to determine eligibility and authorization of services.
Majority of the services are delivered under the Fee-for-Service (FFS) system.
Evidence Based Practice-Assertive Community Treatment, Supported Employment
Core Service Agencies (CSAs)
Local authority with responsibility to manage services on the county level.
Nineteen CSAs-one in each county and Baltimore City. (1 CSA serves 5 Eastern Shore counties and 1 CSA serves both Somerset/Wicomico county)

Community and State Expenditures In FY 2011, 73 percent of total expenditures were for community-based services
(including those in the fee-for-service system and in grants and contracts).
MHA’s Actual Budget was $1,002,680,134 --- $738.1 million ($624.4 million from Medicaid) for community services, $256.4 million for state operated institutions, and $8 million for program administration.
Non-Medicaid expenditures include those for Medicaid-ineligible recipients, non-Medicaid reimbursable services provided to Medicaid recipients, and for services for individuals within state-only Medicaid eligibility categories.
Total Community and State Facility Expenditures-FY2011
State Facilities26%
Fee-For-Service62%
Program Administration
1%Grants/Contracts,
11%

Mental Hygiene Overview
The MHA oversees Mental Health care in Maryland
Children and Adolescents Adults and Older Adults Forensics Consumer Affairs Housing and Supported Employment Special Populations
Traumatic Brain Injury (TBI) Deaf and Hard of Hearing Suicide Prevention
Applied to all areas: Regulatory Compliance, Financial Oversight, Quality Assurance and Improvement, Medicaid Service Expansion



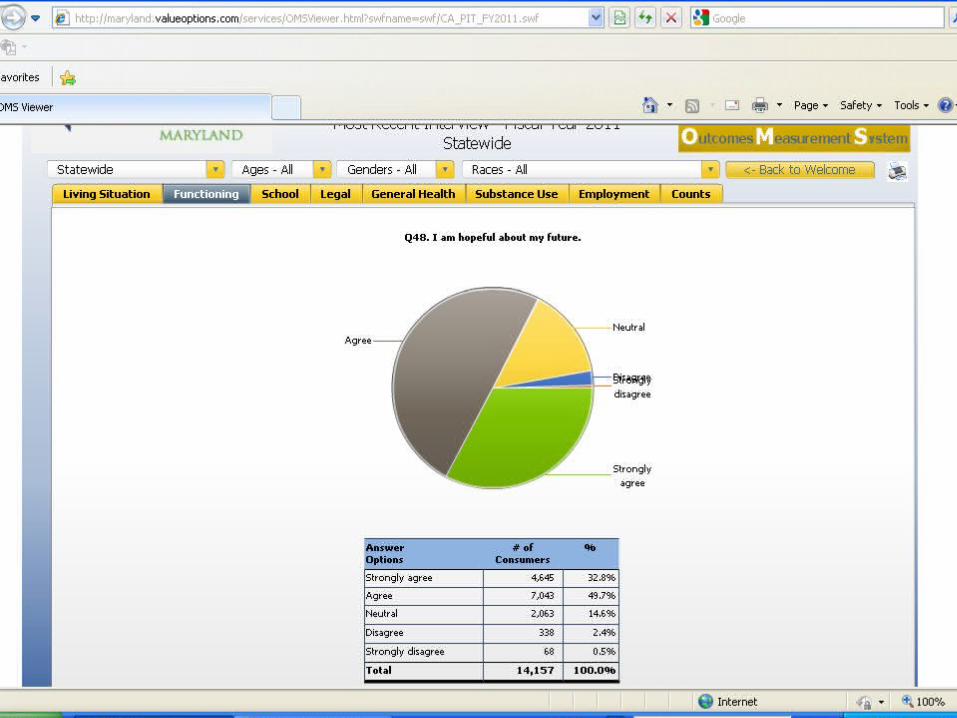
Maryland’s Outcome Measurement System (OMS)
The Outcome Measurement System (OMS), implemented statewide in FY 2007, was developed to collect information on several life domains (including symptoms, functioning, living situation, employment, school performance, alcohol and substance use, legal system involvement, and somatic health) from individuals, ages 6-64, who are receiving mental health services in outpatient settings from Maryland’s fee-for-service system.
OMS information, gathered directly through interviews between the clinician and consumer, is collected at the beginning of treatment and approximately every six months thereafter while an individual is receiving treatment.
Value Options, in collaboration with MHA and the Univ. of Md. SEC, developed an OMS datamart that has the ability to perform analysis and reports available to MHA, providers, CSAs, and the general public.
The OMS system provides Point-in-Time as well as Change-over-Time data.
Datamart Link: http://maryland.valueoptions.com/services/OMS_Welcome.html

Good and Modern System
We have a good system that can be better.
The challenge is to move to a financial system that includes risk sharing and integration of care for mental health, substance use and physical health care without losing the current strengths of the PMHS.

Integration of Care
The Affordable Care provides opportunities to increase access and quality of health care through the integration and coordination of health care which is a trend that has been seen nationwide already. We know that integration is important. We know that:
30% of all individuals with a mental health/substance use disorder may have 3 chronic conditions; that
Roughly 1/3 of all cigarette smokers have an mental health/substance use disorder; that
The cost of treating common diseases higher when a patient has untreated behavioral health problems: Hypertension – 2x the cost Coronary heart disease – 3x the cost Diabetes – 4x the cost.

Integration of Care Needs
SAMHSA/HRSA Center for Integrated Health Solutions which has been established to provide training and technical assistance on primary care and behavioral health integration. The Center is working to increase the number of:
Individuals trained in specific behavioral health related practices;
Organizations using integrated health care service delivery approaches;
Consumers credentialed to provide behavioral health related practices;
Model curriculums developed for bidirectional primary and behavioral health integrated practice; and,
Health providers trained in the concepts of wellness and behavioral health recovery.

Working Towards 2014
To assist States in preparing for 2014, SAMHSA is engaging state mental health commissioners and substance abuse authorities in focusing on the most critical areas in the implementation of the Affordable Care Act. Key areas where SAMHSA is engaged with states are:
1. Primary and behavioral health care integration;2. Identification of mental health/substance use
disorder services that should be offered by Medicaid and the Exchanges;
3. Education and enforcement of the Mental Health Parity and Addictions Equity Act of 2008; and
4. Outreach and enrollment to ensure the 11 million individuals with a behavioral health disorder is covered.

Focus Going Forward
Moving forward with Health Care Reform
The Triple Aim
Lower Per Capita CostsImproved Outcomes
Better Patient Experience……at the Same Time

Challenges for Behavioral Health
Is there capacity to provide MH & substance abuse services (workforce)?
Have strategies been developed to improve infrastructure (data, health IT, electronic health records)?
How can we facilitate linkages with primary care & other providers?
How will essential non-medical services (e.g., housing, employment) be funded?
Technology and Healthcare
Internet: e-Therapy, alternative source of service when traditional psychotherapy is not an option or not preferred.
Smart Phone Apps-applications available to help educate, maintain contact between appointments etc.
Telehealth-Maryland using Telemental Health services in Rural areas. PMHS reimbursable service.

Important websites
Network of Care http://networkofcare.org/home.cfm Portal to all Mental Health resources available at the county level.
National Suicide Prevention Lifeline http://www.suicidepreventionlifeline.org/
National Hotline or Chat service for those in emotional distress or suicidal crisis. Services for Youth and Veterans available.
American well http://www.americanwell.com/
Utilizing a web-based telehealth platform, brings healthcare into the home and workplace. Provider to patient via video, secure chat and phone.


















