
mental-health-shared-care-for-ethnic-communities
45
Mental health shared care for ethnic communities – a handbook Brisbane Inner South Division of General Practice June 2001
-
Upload
michael-burville -
Category
Documents
-
view
212 -
download
0
description
Brisbane Inner South Division of General Practice June 2001 Mental health shared care for ethnic communities – a handbook Page 2 Mental health shared care for ethnic communities – a handbook Brisbane Inner South Division of General Practice June 2001 Mental health shared care for ethnic communities – a handbook Page 3
Transcript of mental-health-shared-care-for-ethnic-communities

Mental health shared care for ethnic communities – a handbook
Mental health shared care for ethnic communities – a handbook
Brisbane Inner South Division of General Practice June 2001

Mental health shared care for ethnic communities – a handbook
Page 2

Mental health shared care for ethnic communities – a handbook
Page 3
Mental health shared care for ethnic communities – a handbook
Brisbane Inner South Division of General Practice June 2001

Mental health shared care for ethnic communities – a handbook
Published by: Brisbane Inner South Division of General Practice PO Box 8004 Woolloongabba Qld 4102 Ph: (07) 3392 2822 Fax: (07) 339 22920 Email: [email protected] Queensland Transcultural Mental Health Centre Princess Alexandra Hospital Ipswich Rd Woolloongabba Qld 4102 Ph: (07) 3240 2833 Fax: (07) 3240 2282 Email:[email protected] © 2001 Brisbane Inner South Division of General Practice, Queensland Transcultural Mental Health Centre, Department of Health and Aged Care, Australian Transcultural Mental Health Network. This work is copyright. It may be reproduced in whole or part for study or training purposes subject to the inclusion of an acknowledgment of the source and no commercial usage or sale. Reproduction for purposes other than those indicated above requires permission from the Brisbane Inner South Division of General Practice and the Qld Transcultural Mental Health Centre. Contact details for these organisations are listed above. Additional copies of the handbook are available from the ATMHN. Tel: 02 98403333, Fax: 02 98403338, Email: [email protected] This handbook was funded by the Commonwealth Department of Health and Aged Care under the National Mental Health Strategy through the Australian Transcultural Mental Health Network and Queensland Health, through the Queensland Transcultural Mental Health Centre. ISBN 0-9579120-0-5 Written and designed by Marina Chand, [email protected]

Mental health shared care for ethnic communities – a handbook
Page 5
Table of contents
INTRODUCTION………..…….…………….7 PART ONE – ISSUES IN ETHNIC MENTAL HEALTH SHARED CARE Why use shared care?………..………10 Ethnic communities & mental health……………………………..…………10 General practice & ethnic mental health………..…………………..………….14 Shared care with ethnic communities………….…………………..16 Lessons learned………………………...19 Evaluation………………………………….21
PART TWO – SETTING UP ETHNIC MENTAL HEALTH SHARED CARE Components of ethnic shared care………………………………….………..24 Developing relationships, systems & protocols……………………..………….27 Care planning processes……...……..30 Maintaining shared care………….….31 Evaluating the program…….………...32 REFERENCES …..………………………..37 APPENDICES – Protocols used in Brisbane inner south project 1 – GP resources summary…….…..37 2 – Fax request form ……………......38 3 – GP quick reference guide ….….39 3 – GP resource guide ……….……...40

Mental health shared care for ethnic communities – a handbook
Page 6
List of tables: Table 1 – Factors relating to under-recognition of mental disorders p14 Table 2 – The GP role in ethnic mental health shared care p15 Table 3 – Shared care arrangements & resources in the Brisbane inner south shared care project p25 Table 4 – Strategies and considerations for program sustainability p31 Table 5 – Evaluation strategies in the Brisbane inner south project from the perspective of three participant groups p32 Table 6 – Evaluation framework for program effectiveness in the Brisbane inner south project p34 List of figures: Figure 1 – People of NESB with mental health problems in Australia p13 Figure 2 – Ethnic mental health shared care program framework p24 List of boxes: Box 1 – The Brisbane inner south mental health shared care project for ethnic
communities p 8 Box 3 – Accessing and using the Translating and Interpreting Service p29

Mental health shared care for ethnic communities – a handbook
This handbook contains practical strategies for the establishment of ethnic mental health shared care programs and arrangements, and offers insights into the issues affecting shared care for ethnic communities. Some of the issues that affect shared care service delivery to people of non-English speaking background (NESB) are similar to those for the community at large, however there are also distinct issues involved. The focus of this handbook is on these distinct issues. The general purpose of the handbook is to assist those planning to set up ethnic mental health shared care programs. The handbook guides the reader through the main issues that should be considered before setting up an ethnic shared care program and then provides practical information that may assist the implementation phase. More specifically the purpose of the handbook is to assist divisions of general practice and others to:
1. Plan and implement programs in shared-care that can meet the specific needs of clients of NESB;
2. Incorporate the needs of clients of NESB into existing shared care programs.
Much of the information in the hand-book is based on experience gained from an ethnic mental health shared care demonstration project in Brisbane. This project piloted a shared care approach between the Brisbane Inner South Division of General Practice and key services working with people of NESB with mental disorders.
Page 7
This handbook is divided into two sections: 1. Section one outlines pertinent issues in
shared care for ethnic communities 2. Section two is a how-to manual for
setting up shared care for ethnic communities
The handbook may be particularly useful to the following who are interested in setting up ethnic shared care programs and arrangements: • Divisions of general practice • Multicultural health organisations • Mental health organisations and
services
The aim of the project was to enhance general practitioners’ (GPs) skills and knowledge in an early intervention model where people of NESB exhibiting early signs and symptoms of mental disorder could be identified, assessed and treated. The project provided resources and support to GPs with assessment and diagnosis and ongoing support of their patients in a general practice setting. The project had a strong evaluation focus. The project report of the ‘Brisbane inner south project’ is available as an optional extra for those interested and is a valuable companion document, but is not necessary, to use and understand this handbook.
INTRODUCTION

Mental health shared care for ethnic communities – a handbook
The Brisbane Inner South Mental Health Shared Care P r o j e c t f o r E t h n i c Communities Who was involved? The Brisbane Inner South Division of General Practice, Qld Transcultural Mental Health Centre, West End and Coorparoo Mental Health Services, Qld Program of Assistance to Survivors of Torture and Trauma, the Ethnic Mental Health Program and the Qld Divisions of General Practice. What did the project do? The project established and piloted a shared care model for people of NESB exhibiting the early signs and symptoms of a mental disorder. How was shared care established? The project formed a reference group with representatives from the agencies participating in shared care and implemented the following strategies: • Undertook a comprehensive literature review
and developed an evaluation plan • Recruited 15 GPs with an interest in par-
ticipating in shared care • Developed and implemented a Transcultural
Mental Health Training Course for GPs • Introduced systems to facilitate and
formalise shared care through the development of a GP handbook consisting of referral guidelines, service request fax forms, interpreter booking forms, Enhanced Primary Care Items information and key contacts in mental health services.
• Undertook process and impact evaluation, pre and post training evaluation, and a cost analysis.
How did the project involve consumers? The project involved consumers in the project development phase through a consumer focus group and interviewed consumers at the conclusion phase to assess impact and satisfaction. Project information and data collection information was translation in six key languages and passed on to consumers through their GP.
What did the project find out? The GP sample was small and therefore results could not be generalised. However, the project found that a training course comprising both GPs and service providers was very important not only for information dissemination but also relationship building. Although the response to shared care arrangements from the project GPs was slow and gradual, the evaluation revealed that they offered significantly more options to their patients diagnosed with depression and/or anxiety compared to GPs who had not received the training. Some factors in the slow uptake to shared care by GPs was identified by GPs as being due to patient resistance to other service providers, lack of availability of culturally appropriate resources, lack of time, in house barriers in their current practice environment, hesitation to get too involved in fixed term projects, and difficulties in attending meetings. Implications of the project The project recommended that ethnic shared care programs be linked with mainstream shared care programs in order to maximise impact and ensure sustainability. It was clear from feedback from GPs and service providers that smaller projects are not well regarded. Training was a key factor to engage GPs with service providers and time needs to be build in for discussion and relationship development. Systems such as fax forms for easy contact and referral, guidelines on who to contact in what instance, contacts for direct access to staff in mental health services are all important components of a shared care project. The project found that the prevalence of depression and anxiety for people of non- English speaking background was similar to that of the general population but found that GPs who saw considerable numbers of patients from refugee backgrounds reported double the prevalence rates. It is therefore important that shared care programs include specific strategies to include bilingual GPs and ethnic health services.
Page 8
Box 1 – The Brisbane inner south mental health shared care project for ethnic communities
Introduction

Mental health shared care for ethnic communities – a handbook
Part one – issues in ethnic mental health shared care
Page 9

Mental health shared care for ethnic communities – a handbook
General practitioners and mental health services have worked together informally for many years, sharing the treatment and care of people with mental health problems. However, this has not necessarily been routine or systematised as a treatment and care approach. Shared care typically tends to focus on the development of systems and protocols to facilitate communication between the program participants through structured agreements about respective roles, responsibilities and expectations regarding patient care. In Australia, the majority of mental health shared care has been in the context of discharging stable patients from mental health services to the care of a general practitioner. However, there are many different models of shared care. Some of these are outlined below (SERU 1997): • up-skilling and educating program
participants in mental health assessment, diagnosis, treatment and management;
• enhancing and formalising communication, information and referral pathways between participating services, particularly between GPs and services;
• providing a mental health liaison o f f i c e r t o c o o r d i n a t e communication, facilitate access and transfer between services and general support;
• attachment of mental health workers to GPs; and
• attachment of GPs to mental health services.
These programs have however not been specifically designed to meet the needs of NESB clients. Mihalopolous et al (1999) identified the need to further pilot and evaluate shared care models before conclusions could be made about optimum shared care models for ethnic communities, given the paucity of information about the mental health outcomes of NESB clients within numerous shared care programs operating throughout Australia. The Brisbane inner south mental health shared care project, on which this handbook is based, was one such project. The Brisbane inner south project was a combination of models one and two outlined above. The focus was on up-skilling GPs to enhance their skills to detect and respond to NESB patients exhibiting the early signs and symptoms of mental illness. The secondary focus was to enhance and formalise communication and referral pathways between the program participants. The evaluation of the program revealed that: • patients generally had positive
feedback about their GP and mental health service providers;
• service providers perceived shared care as a priority despite not receiving as many referrals from GPs as anticipated and were still seeking more ‘mental health friendly’ GPs; and
• GPs who actively participated in shared care found it a positive experience but it was difficult to involve all GPs fully.
Page 10
“I found having a psychiatrist coming out to my surgery a great help, it w a s a f a n t a s t i c resource…” - GP in the Brisbane inner south project “I had depression before coming here, now my situation has worsened. I recommend the support I have received, I don’t know if I could manage on my own”. - patient in Brisbane inner south project “We really want GPs to be part of the treatment team, we will set up case conference times to suit the GP, we just need more GPs that we can w or k w i th! We acknowledge that it’s very difficult to find the time that suits both the GP and the case worker”. - service provider in the Brisbane inner south project
WHY USE SHARED CARE?

Mental health shared care for ethnic communities – a handbook
This section presents information about the prevalence of mental illness among people of NESB in Australia and their use of mental health services. The literature does not have consistent findings of mental disorder rates within NESB communities in Australia. This may be due to several factors. Firstly, measurement of the prevalence of mental disorders in people of NESB is fraught with difficulties because different cultural groups may express psychological symptoms in different ways, and research instruments are often not reliable nor cross-culturally valid. Secondly, people who do not speak English are often excluded from quantitative studies such as the National Survey of Mental Health and Wellbeing. Minas (2000) pointed out that there is a substantial and often confusing literature on the prevalence of mental illness in indigenous and immigrant populations. The results of prevalence studies vary widely according to the disorder studied, ethnic group and location of the study. In summary, in some studies prevalence rates for a particular ethnic group are higher than the host population, in others the rate is lower and in others the rate is the same. The National Survey of Mental Health and Wellbeing (1999) reported limited information on the mental health of people of NESB, but found that the prevalence of mental disorders was slightly lower in people born in non-English speaking countries (12.5 percent in males compared to 18.4
percent of Australian born males and 16.9 percent for females compared to 18.7 percent of Australian born females). The national survey concluded that these figures probably reflected a ‘healthy migrant effect’ - persons who do not have mental disorders are more likely to be interested in migration, and probably more likely to be accepted as immigrants. Refugees are singled out in the literature as having higher rates of long term medical an psychological conditions than other migrants, tend to report a poorer state of well being and visit health care providers more frequently (Lehn 1997). Refugee claimants have been documented as having even worse mental health status as a group separate from those whose refugee status has already been determined (Silove & Steele 1998). Minas commented that it is not immigrant status, in itself, that is associated with either a high or low prevalence of mental disorder but that there are many factors that are part of the experience of some immigrants (such as pre-migration experiences of trauma and disrupted families) that may be associated with increased vulnerability (2000). Other post-migration experiences that may increase vu lnerabi l i ty include u n e m p l oy m e n t , l ac k o f sk i l l recognition, social isolation, language barriers and lowered social status. Service access to appropriate mental health care is particularly pertinent for NESB people. Mihalopoulos et al
Page 11
“I don’t feel productive any more. The system forces people to be unproductive…” “...I’m grumpy, I’m isolated, not going out, I distrust people…” “My children have goals - I’m not financially able to give them. I have no plans for the future.” “The impossibility to adjust in this new society/country – I feel disabled!” “Put more effort into treating people like human beings. I was happy with the student, less with the psychiatrist.” - patients in the Brisbane inner south project
ETHNIC COMMUNITIES & MENTAL HEALTH SERVICES

Mental health shared care for ethnic communities – a handbook
(1999) reported several other Australian studies that suggest that people of NESB are at least as likely to visit a GP for a consultation for mental health problems, compared with their Australian-born counterparts. In a British study, Schurman et al (1984 in Mihalopoulos et al 1999) found that people of NESB were more likely to attend GPs for mental health problems than their English-born counterparts, but in Australia studies show that NESB people use their GPs as often as other patients. However, it has been established that NESB people prefer GPs who share their language and cultural background. Despite this, several Australian studies have confirmed that NESB people are less likely to receive treatment for their mental health problems and have their mental disorders diagnosed later in onset (McDonald and Steele 1997; Finlay-Jones and Burvill 1978 and
Lloyd 1993 in Mihalopoulos et al 1999). In Australia it has also been established that people of NESB are less likely to receive treatment and care from specialist mental health services in both hospital and community settings (McDonald and Stee le 1997; Stolk 1996 in M i h a l o p o u l o s e t a l 1 9 9 9 ) . Furthermore, once they do gain access to such services, people of NESB stay longer in hospital care, have higher or equal rates of involuntary admission but significantly lower rates of voluntary admission, have shorter face-to-face contacts in community settings, and are less likely to receive talking therapies than their English speaking counterparts (McDonald and Steele 1997; Stolk 1996, Trauer 1995, Lloyd 1993, Balabil and Dolan 1992 in Mihalopoulos et al 1999).
Page 12
“I find that when working with new arrivals, like people from the Horn of Africa or the Middle East there are so few culturally appropriate resources around that it is very difficult…” - GP in the Brisbane inner south project
Ethnic communities & mental health services

Mental health shared care for ethnic communities – a handbook
People who do not speak English are often excluded from quantitative studies such as the National Surveyof Mental Health and Wellbeing.
Refugees have a higher rate of long term medical and psychological conditions than other migrants, and report a poorer state of well being and visit health care providers more frequently.
Refugee claimants have even worse mental health status as a group separate from those whose refugee status has already been determined.
Are at least as likely to visit a GP for a consultation for mental health problems, astheir Australian-born counterparts.
Prefer GPs who share their language and cultural background.
Are less likely to receive treatment for their mental health problems and have their mental disorders diagnosed later in onset.
Are less likely to receive treatment and care from specialist mental health services in both hospital and community settings.
Once they do gain accessto mental health services, stay longer in hospital care,have higher or equal rates of involuntary admission but significantly lower ratesof voluntary admission.
Have shorter face-to-face contacts in community settings.
PPeeooppllee ooff NNEESSBB wwiitthh
mmeennttaall hheeaalltthh
pprroobblleemmss iinn AAuussttrraalliiaa……
Are less likely to receive talking therapies than theirEnglish speaking counterparts.
Fig 1 – People of NESB with mental health problems in Australia
Page 13 Ethnic communities & mental health services

Mental health shared care for ethnic communities – a handbook
The pathway to mental health care for people of NESB begins with the GP. Despite their reluctance to seek assistance from mental health services, NESB people do visit their GP for physical and mental health issues (Mihalopoulos et al 1999). People of NESB generally have a preference for a GP who shares their cultural and linguistic background. However, it has been documented that GPs tend to under-recognise
mental disorders within people of NESB and consequently diagnosis occurs later in onset of the illness. It is important that GPs have an awareness of the factors that contribute to the under-recognition of mental disorders in NESB people. According to Hickie (1999) these factors relate to the patient, doctor and service:
Page 14
“It would be good to provide more support to GPs who speak other languages. Apart from the fact that we can save money as we don’t need interpreters, we are a very important resource with the communities we work with and sometimes we are isolated. A project like this is excellent, for me anyway, it was a great opportunity”. - GP in the Brisbane inner south project “There are no people here with my condition. My doctor said my condition (diagnosis) is not in the book.” - patient in the Brisbane inner south project
Factors relating to under-recognition of mental disorders:
Patient re-lated factors
• tendency to present with somatic rather than psychological com-plaints,
• the co-occurrence of medical and psychological problems, • stigma associated with psychological diagnosis and treatments
Patients of NESB: all the above factors are applicable with very high levels of stigma in some ethnic communities; differences in expression of psychological distress and mental illness symptoms across cultural groups; and absence of notion of ‘mental health’ in some cultural groups.
• Insufficient interview and diagnostic skills, • Insufficient undergraduate and postgraduate training, • Inadequate time devoted to diagnostic assessment, • Lack of acquisition of new knowledge relevant to treatments, • Insufficient remuneration for long consultations
When treating patients of NESB: all the above factors are applicable and in addition a lack of awareness of the stages of settlement; lack of training in cross-cultural communication; and lack of cross-cultural clinical skills.
Doctor re-lated factors
Service re-lated factors
• insufficient remuneration for psychological interventions, • insufficient support from specialist public and private mental health
services, • inadequate access to non-medical mental health professionals
Services for patients of NESB: all the above factors are applicable and in addition, a lack of standardised processes for booking and using pro-fessional interpreters; and insufficient flexibility to cater for longer con-sultations that are required for the use of interpreters.
Table 1: Factors relating to under-recognition of mental disorders (adapted from Hickie 1999)
GENERAL PRACTICE & ETHNIC MENTAL HEALTH

Mental health shared care for ethnic communities – a handbook
The factors outlined in Table 1 are further complicated by cross-cultural communication and poor English language sk i l ls by pat ients. Recognition of the mental disorder by the GP will vary according to the patient’s ethnicity, cultural influences on clinical presentation and the explanatory model of his/her condition (Kleinman 1978). The GP has a particularly pivotal role in the assessment, diagnosis, treatment and management of
mental illness in people of NESB. With the growth of prevention and promotion strategies under the National Mental Health Strategy, there is also an expectation that GPs be involved in the prevention of mental illness and the promotion of mental health. The table below outlines the special role of GPs in relation to mental health care and more specifically, the additional factors that need to be considered when working with people of NESB (adapted from SERU 1997):
The role of the GP in mental health care for people of NESB is multi-dimensional and pivotal. The GP can easily be the primary service provider given NESB people’s reluctance to use specialist mental health services and their preference to seek assistance from their GP. GPs should be made a w a r e o f t h e opportunities that are now available for them to be care coordinators through the Enhanced Primary Care (EPC) items for care planning and case conferences. Part Two of this handbook has further information .
Aspect of mental health care
GP role Additional factors to consider with NESB patients
Detection & diagnosis
• Essential for provision of primary health care
• Rates are variable amongst GPs for complex reasons
• Often the first contact point
• GPs are often the only service sought out • Rates are lower than the community at
large • Diagnosis often requires cultural input • Tendency to present somatic complaints • The need to use professional interpreters
when there is a language barrier
Prescribing • Informed prescribing • Readily accessible advice • Regular reviews of medication
• Awareness of ethno-psychopharmacology • Extra care with instructions and advice
about medications
Non-pharmacologi-cal treatment
• Case management or coordination • Counselling • Support & advocacy • Information provision
• Awareness of ethnic support agencies • Awareness of multicultural counselling serv-
ices and specialist services • Multilingual information
Monitor of physical health
• Treatment and care of physical symptoms
• Receive patient feedback
• Awareness of tendency by NESB patients to only present with somatic complaints
Case man-ager
• Liaison with other service providers • Case planning • Case review • Receive patient feedback
• Awareness of ethnic and other specialist services
Prevention • Collaboration with self-help groups • Prevention & promotion activities • Receive patient feedback
• Partnerships with ethnic groups and ethnic health workers
Table 2: The GP role in ethnic mental health shared care
Page 15 General practice & ethnic mental health

Mental health shared care for ethnic communities – a handbook
Page 16
Working with patients of NESB means GPs and other program participants will: • Encounter different
world views • Encounter different
explanatory models for mental illness and symptoms
• Encounter different values and approaches to problem solving
• Need to consider working with non-traditional partners such as spiritual leaders, alternative health practitioners and ethnic voluntary groups.
• Need to consider strategies to facilitate patient input/feedback on services received.
Shared care programs for ethnic communities have many features in common with shared care programs for the community at large but also have a number of unique features that are explored in this section. Like other shared care programs, ethnic shared care programs also effect systemic change by changing the way service providers work with each other. However, the key difference is in the actual operation of the program - in the incorporation of ethnic groups and workers and language services. The special attention that bilingual GPs and ethnic workers require are also pertinent to the success of an ethnic shared care program. Transcultural clinical consultations One of the challenges for GPs can be to grasp and interpret their NESB patient’s cultural context, i.e. their bel ief system, cultural-specific expression of symptoms, norms for behaviour and general explanatory model. These are crucial factors for the identification of patients with a possible mental disorder. GPs cannot be expected to know about every culture and ethnic group that may present in their surgery. Hence, access to transcultural clinical consultations form an essential component of a shared care program for ethnic communities. Some states in Australia have transcultural mental health centres that provide precisely such a service.
These are state-wide services in states such as Queensland and can be accessed on a 1800 number. However, in areas where transcultural clinical consultation services are not available, the following may comprise an equally important component of an ethnic mental health shared care program:
• Welfare workers of NESB • GPs of NESB • Allied health workers of NESB • Multicultural settlement or
community workers • Voluntary multicultural groups These workers and groups could provide culturally-related information and in some cases, act as a cultural broker between the GP and the patient. However, a word of caution about confidentiality must be heeded as voluntary groups are generally not bound by a code of ethics nor work under policies of confidentiality.
Cross-cultural communication Every consultation with a patient involves a cross-cultural experience for the GP. Even if the patient is seemingly from the same cultural background as the GP, it is likely that they come from a different social status, geographical area or family background. According to Fitzgerald (1992) in every clinical interaction there are at least three cultures and medical systems involved: – the personal or familial culture of the provider (GP) – the culture of the client or patient
SHARED CARE with ethnic communities

Mental health shared care for ethnic communities – a handbook
For me the biggest plus out of this project has been working with interpreters. Before this I sort of knew that it was around but not sure how to go about doing it.” - GP in Brisbane inner south project “We have had the situation where we have booked an interpreter for 2 hrs and booked 3 patients from that language group and then we have a no show for 3 patients so the interpreter and GP is standing around with no patient. We know that for new arrivals there is trauma and people are disorganised as they have so much to deal with but from our point of view it is such as waste of precious resources. We only have access to interpreters from a very limited quota and you feel very bad when you know this resource is wasted due to no shows.” - GP in Brisbane inner south project
– the culture of the primary medical system And when the patient comes from a NESB, there is a fourth culture: – the traditional medical culture The GP may make assumptions about the patient’s behaviour or belief systems based on what makes sense in his/her own culture. With patients from non-English speaking countries, GPs may make even greater assumptions about their patients and the likelihood to make errors in judgement and understanding increases tremendously. It is also less likely that the GP’s values, beliefs or attitudes are shared by their NESB patient. Ethnic mental health shared care programs should incorporate a professional development component for GPs about cross-cultural communication and pertinent issues affecting health care in a culturally diverse society. It would be useful to address, at the very least, the following issues: • cu l tura l s tereotyping: the
categorisation of people and experiences. Unfortunately they are inadequate as sources of detailed information about an indiv idual patient from a particular background.
• attribution: the assumptions that
are made about the reasons a person is behaving in a particular way, based on what would make sense in the GP’s own culture.
• eliciting explanatory models: the way a patient understands his/her life, problems, relationships and illness, including spiritual, political, social and cultural beliefs. Western medicine has its own explanatory model that may not be acceptable to particular cultures.
• language issues: cross-cultural
communication involves more than having a common language but the need for professional i n t e r p r e t e r s s h o u l d b e emphasised in any training.
Language related issues An important consideration in an ethnic mental health shared care program is that of language services. Unfortunately, many GPs still don’t r o u t i n e l y u s e p r o f e s s i o n a l interpreters when there is a clear need to use one. GPs also need to be discouraged from using relatives as interpreters and should be made aware of the legal implications of doing so. The use of professional interpreters will need to be addressed both in the form of professional development, but also in the form of shared care protocols, forms and processes. Conversely, GPs also need to be prepared for some of the d i f f i c u l t i e s a n d c h a l l e n g e s surrounding the use of interpreters. If the use of professional interpreters is integrated into shared care program arrangements, it is more likely that they will be used. It will also be important to make GPs aware
Page 17 What is different about ethnic shared care

Mental health shared care for ethnic communities – a handbook
Page 18
“... I like to talk but I have no friends, I lost trust…” - patient in the Brisbane inner south project “They are doing what they are told. They go according to the book. It’s impossible to talk to them, they don’t listen. They use a language I don’t understand”. - patient in Brisbane inner south project
how interpreters can be booked and provide the correct information about the cost of professional interpreters. Part two contains more detailed information about accessing and using professional interpreters. Ethnic shared care programs will also need to translate written information about the program into the high demand community languages. This has a cost impact on the overall program budget. Working with ethnic workers, services and groups An ethnic shared care program will most often involve working with a range of ethnic workers and groups. Most metropolitan areas have ethnic welfare and even ethnic mental health workers. These workers are important partners in ethnic mental health shared care as they can
provide vital information about ethnic social support options and may even undertake indiv idual support themselves. Capital cities generally also have specialist refugee health services such as counselling services for survivors of torture and trauma. Once again, these organisations constitute important partners in the program or they may even be program participants. Ethnic social or cultural groups may constitute important social support options for clients of the ethnic mental health shared care program. It will be important for program staff to fully brief all the participants about such groups and organisations and/or provide information resources about finding and accessing such groups.
General practice & ethnic mental health

Mental health shared care for ethnic communities – a handbook
“...a good project, I did not use it the way I should have…”
- GP in the Brisbane inner south project
“for us partnerships with GPs is a priority, in fact it is in our strategic plan…”
- service provider in the Brisbane inner south project
This section is based on the lessons learned about ethnic mental health shared care in the Brisbane inner south project. Given that the Brisbane i n n e r s o u t h p r o j e c t w a s a demonstration project, there were many issues both foreseen and unforeseen that impacted on the project. These are presented in this section. Limitations of ethnic shared care The Brisbane inner south project was a stand-alone program that was not attached to a larger or ‘mainstream’ shared care program. Throughout the project period it became more and more clear that the ethnic shared care project was regarded as a (small) competitor to other shared care projects by some services. Given the popularity of shared care as an approach to treatment and care in the mental health sector, several other shared care programs were operating in the same geographical area as the ethnic shared care project. Some of these shared care programs were better resourced than the ethnic program and were even in the position of providing financial resources to mental health services. This made it difficult for the ethnic program to ‘compete’ and had to solely rely on the goodwill of the participants. Ethnic shared care should be regarded as one stage in the implementation of an overall, culturally inclusive, shared care program. Because cultural diversity issues can be challenging to incorporate into a large program, the
special processes required are best developed in an exclusively ethnic shared care program that eventually will be integrated into a ‘mainstream’ shared care program. The ethnic shared care program should however be resourced in the same way as the overall program so that it is not marginalised. Once the ethnic shared care program is running smoothly it can be systematically integrated into the overall shared care program, paying special attention to the preservation of processes that address the complex issues of cultural diversity amongst patients and practitioners. GP recruitment The GP participants of any shared care program form an integral part of the program and therefore special attention should go towards the recruitment of GPs. In the Brisbane inner south project all the GP participants were fully briefed about the objectives and limitations of the project, yet a number of misconceptions remained, particularly about GPs needing to give up case coordination to other services. Other GPs thought they could use the shared care program to refer mental health patients on. It is also crucial to the success of the program that a good sample of bilingual GPs are involved. It is highly likely that the very GPs required, will have a relatively low profile with their local division of general practice, as some bilingual GPs have generally not been as actively involved in Division
Page 19
LESSONS LEARNED

Mental health shared care for ethnic communities – a handbook
Page 20
“ I am also aware that there are financial issues to working together. We have had the experience of co-locating with a number of GPs and this was discontinued as for the GPs it was no longer financially viable. They told us they could make three times as much money in the same time by not seeing our mental health patients.” - service provider in the Brisbane inner south project “I enjoyed talking to other GPs, training was good, it opened my eyes.” - GP in the Brisbane inner south project
programs. Ethnic community contacts and ethnic community health workers are a valuable source of information about popular bilingual GPs that many people in a particular community tend to use. It is important that these GPs be approached and invited into the shared care program. It is also recommended that the GP participants should comprise a small number of highly regarded GPs who are well known advocates of shared care programs and/or ethnic health issues. These GPs will champion the issue of ethnic health and display a great deal of commitment to the program. They may also motivate other GPs to accept the challenges of working in this area. Finally, the reluctance by GPs to use long consultations for mental health issues remains a difficult issue. Many GPs are under pressure to work within short appointment times and therefore cannot adequately deal with mental health issues that may require more time. This may be further exacerbated by the use of interpreters which place further time demands on GPs. This issue may also need to be addressed from the outset, during GP recruitment, as the reluctance to take the time necessary for a mental health consultation, may reduce the quality of care able to be offered by GPs. Training and up-skilling The training and up-skilling needs of GPs in relation to mental health and
transcultural clinical issues should not be underestimated. It is highly recommended that training needs be o v e r e s t i m a t e d r a t h e r t h a n underestimated! Training is also ideally conducted on an ongoing basis, rather than at the outset of the program. In this way, GPs and other participants can bring real practice issues to their training. There is also a real benefit in including other participants such as mental health service providers in the GP training. Their participation can facilitate the building of positive working relationships that are necessary in shared care programs. In the Brisbane inner south project the issue of motivating GPs to attend training was constantly grappled with. To date no conclusions have been drawn about this issue despite numerous attempts to dialogue with GPs about their low attendance at case discussions and ongoing training opportunities. It was observed that visiting GPs at their clinics and working on a one-to-one basis was the most effective way to engage with them but this was difficult to provide within the resource constraints of the project. The following strategies were used to encourage greater GP participation: • Six weekly short case discussion groups. • Motivational sessions with GP speakers
who were strong advocates of shared care.
• Discussion group about dealing with patient reluctance to be referred on.
• An offer to facilitate an actual case conference including case planning, support and follow-up.
Lessons learned

Mental health shared care for ethnic communities – a handbook
“The data collection was not explained adequately, some data was useless and it was hard to collect data from so many people.” - GP in the Brisbane inner south project
Evaluation forms an important component of a shared care program. Program impact and outcome evaluation is often a requirement of funding and may form the basis of the evaluation framework. However, as De Bruyn (1994) points out, there are a number of unique features of the mental health field that make outcome evaluation more difficult than in the medical field: • Diversity of theoretical constructs
and therapeutic approaches to mental health and mental illness
• Intangible qualities of mental health practitioners
• Difficulties for health care teams to come to a consensus on diagnosis and treatment
• Mix of contr ibut ing factors (treatment and non treatment) to outcomes during a period of care (i.e. confounding variables that may ‘contaminate’ evaluation findings)
• Chronicity of mental illness and difficulties in tracking patients and assessing care through multiple types of services and settings
• Difficulties in developing reliable and valid tests of the various aspects of quality care and quality of outcomes
• And lack of identification of data needed and appropriate information systems.
In the literature, the five most common and consistent dimensions of outcome evaluation, which have appeared in the m e nta l he a l th f i e l d inc lude: symptomatology, patient functioning, quality of life, patient satisfaction and
costs (health care utilisation) (De Bruyn 1994). It is suggested that a realistic and practical evaluation framework be developed, with the above mentioned complexities in mind. (Part two of this handbook provides a practical guide for evaluation.) There should also be a focus on consumer outcomes and gains in their quality of life, as a direct result of the program. De Bruyn (1994) has identified the following measures and operations used by researchers, administrators, and clinicians over the past two decades to evaluate approaches, programs, and outcomes in mental health care: • Quality assurance programs and
total quality management • Utilization review • Accreditation and certification of
mental health facilities • Measurement of quality of life • Measurement of outcome • Assessment of continuum of care,
and • Isolation of factors that contribute
to outcomes of care and quality of life
Whatever approach or method is employed, it is important to remember that program participants will be relied upon to obtain and record a significant proportion of the data. It is important that the methods and data chosen are feasible and accessible for those required to be involved. In the Brisbane inner south project, an
Page 21
EVALUATION

Mental health shared care for ethnic communities – a handbook
Page 22
attempt was made to conduct a prospective evaluation to determine: • The magnitude of the problem
addressed by the intervention (literature review)
• Whether the intervention worked according to the specified objectives of the project (program effectiveness evaluation).
• An indication of the cost of management of depression/ anxiety by a GP from the perspective of cost to the government (cost analysis)
The feasibility of conducting an economic evaluation was explored. However, due to the unavailability of data from a comparison group and other constraints in the project budget
and time-line, a cost analysis was done. The Canadian Journal of Psychiatry (1998) stated that a problem with economic evaluations is that many of the costs and benefits of treatments are extremely difficult to quantify economically and in addition, difficult to put a dollar value on what often may be the most important benefit of an effective intervention (i.e. increased satisfaction, wellbeing, self esteem and personal happiness in the recipient). Economic evaluations are certainly beneficial to do but particular conditions and resources are required and this must be borne in mind from the outset.
Evaluation

Mental health shared care for ethnic communities – a handbook
Part two – setting up ethnic mental health shared care
Page 23

Mental health shared care for ethnic communities – a handbook
Page 24
This section presents an ideal program framework for ethnic shared care and explores the key components of ethnic shared care. An overall program framework In developing the shared care program, it is important to consider the relationship of the program to other (mainstream) shared care programs. As discussed in the ‘Lessons Learned’ section, the experiences of the Brisbane inner south project led to the conclusion that ethnic shared care programs should have strong links with
a mainstream program, with a view to fully integrating the two. The ethnic program allows for the development of transcultural expertise that can be transferred into a mainstream program at a point when the expertise is fully developed and strong enough to withstand the pressures of a mainstream program. The mainstream program however, would be expected to incorporate transcultural practices and protocols into overall operations to facilitate the preservation of this expertise. This overall program framework can be conceptualised as follows:
Ethnic shared care program set up concurrently & in conjunction
with mainstream shared care program. Specialist expertise is
developed.
Mainstream shared care program set up in conjunction with ethnic
shared care program.
STEP 1
Ethnic shared care program once fully operational, is integrated
into mainstream program, with-out loss of transcultural prac-
tices.
Mainstream shared care program integrates ethnic component into
overall operations, including transcultural practices/ proc-esses for patients of NESB.
STEP 2
STEP 3 Culturally inclusive shared care
program.
Fig 2: Ethnic mental health shared care program framework
COMPONENTS OF ETHNIC SHARED CARE

Mental health shared care for ethnic communities – a handbook
“The role of the GP is very ‘heavy’ when it comes to looking after people with mental health problems. For me the project was great, in fact it was uplifting to be supported, it assured me a lot that there are others that I can work with, that we can work together”. - GP in the Brisbane inner south project
The separate development of the ethnic component of the shared care program is important for the development of expertise and experience. Ethnic shared care is extremely complex and warrants special attention in the setting up phase of a shared care program. However, once developed, this expertise can be shared through the integration of the ethnic shared care program with the mainstream shared care program. Components of ethnic shared care The ‘components’ of shared care refers not only to the program participants but also to the arrangements and resources developed by the program. The chart below provides a snap-shot of the shared care arrangements that were put in place in the Brisbane
shared care project and the resources made available to participating GPs. In the Brisbane inner south project, the following participated in the ethnic shared care program: • selected GPs from the Brisbane
Inner South and Southside Central Divisions of General Practice
• selected adult mental health services
• Ethnic Mental Health Program (NGO)
• Queensland Transcultural Mental Health Centre (Queensland Health)
• Queensland Program of Assistance to Survivors of Torture and Trauma (NGO)
• Queensland Divisions of General Practice, Mental Health Support Strategy (NGO)
• Patients of NESB from different communities.
Phase of care Shared care arrange-ments put in place
Resources made available to GPs
Identification, assessment & diagnosis
Clinical consultation Transcultural clinical consultation
GPs could request consultations with the fol-lowing: 1 Psychiatrist 2 Transcultural clinical consultation serv-
ice, Queensland Transcultural Mental Health Centre
3 Joint assessment with workers from Eth-nic Mental Health Program or Queen-sland Program of Assistance to Survivors of Torture & Trauma
Management of patient care
Short-term clinical in-tervention
Access to bilingual mental health staff brokered by the Queensland Transcultural Mental Health Centre Joint case-management with Ethnic Mental Health Program and Queensland Program of Assistance to Survivors of Torture & Trauma and adult mental health services
Table 3: Shared care arrangements and resources in the Brisbane inner south project
Page 25 Components of ethnic shared care

Mental health shared care for ethnic communities – a handbook
Page 26
I n a r e a s w h e r e transcultural cl inical consultation services are not av a i l ab l e , t he following may comprise an equally important component of an ethnic mental health shared care program: • welfare or community
workers of NESB • allied health workers of
NESB • m u l t i c u l t u r a l
s e t t l e m e n t o r community workers
• voluntary multicultural groups
At the very least, an ethnic shared care program should aim to involve: • Selected GPs interested in the
program and who already see NESB patients/are willing to see NESB patients with mental health problems
• Mental health service/clinic • Ethnic mental health or welfare
workers, or even ethnic voluntary organisations if these are not available in the local area.
GPs – Since people of NESB prefer to see a bilingual or bicultural GP, it is important to consider the involvement of bilingual GPs. Furthermore, monolingual GPs working in areas with a high concentration of NESB people, may also have special skills and experience to offer the shared care program. Regardless of the linguistic background of participating GPs, it is essential that they have an interest in the program, an interest in NESB mental health issues and the time to allocate to extra tasks that may be required such as discussion groups or additional paperwork. In the Brisbane inner south project it also became apparent that the GPs who demonstrated high levels of commitment to the program became important role models for the other GPs. It is therefore suggested that GPs who are well known advocates of shared care are actively recruited to participate in the ethnic shared care program. The influence of peer education and positive role modelling by people who GPs respect, should not be underestimated. (Mazza 2000). Mental health services – These important services provide the mental health expertise to a shared care program. Most public mental health
services are restricted by geographical boundaries and also severity of mental illness and these issues should be considered from the outset. Many shared care programs work across a number of geographical areas and therefore involve more than one mental health service or clinic. Regional areas may not have a mental health clinic, but a visiting team of mental health workers or a part-time clinic. Some mental health services experience high rates of staff turn-over. For this reason it is important that the involvement of and communication with mental health workers is organised in a systemic way, for example through existing whole of agency processes such as team meetings or intake meetings. Mental health workers involved in the shared care program may need the support of shared care program staff to effect organisational change to institute processes such as changes in paper-work, referral protocols and intake protocols. Team leaders and managers should be involved wherever possible. Ethnic mental health, welfare or community organisations – These vital groups contribute the important cultural input into the ethnic shared care program. They often have e x c e l l e n t l i n k s w i t h e t h n i c communities, have ‘inside’ knowledge about community structure and networks, and have specialist knowledge about cross-cultural communication and practice issues. Depending on the location in Australia, the sophistication and range of ethnic resources available will vary. State transcultural mental health centres or psychiatry units are an excellent starting point.
Components of ethnic shared care

Mental health shared care for ethnic communities – a handbook
Key questions for GP recruitment:
• Why do you want to be in the program? (not just to refer mental health patients on)
• Are you willing to take on mental health patients? (is this a mental health friendly GP?)
• Are you prepared to be flexible and work differently?
• Are you willing to o f f e r l o n g e r con su l t a t i on s to m e n t a l h e a l t h patients?
• Are you prepared to be challenged? (and not feel defensive)
• Are you willing to collect the data required to be a participant?
• Are you willing to provide input into the processes and use them?
The foundation of shared care is the relationships developed between service providers participating in the program. Service providers may already have an informal working relationship but the aim of the shared care program is to formalise and systematise working relationships and processes between service providers. This chapter explores the important steps in this process. Identifying and engaging GPs In an ethnic shared care program, it is likely that the participating GPs will either be bilingual themselves, or work in geographical areas with high concentrations of people of NESB. It may be easy to readily identify the key GPs that could be approached to participate in the ethnic shared care program because they are well known to service providers or have visible clinics in the chosen geographical location. However, some GPs, particularly bilingual GPs, can be isolated from other service providers and have low visibility to organisations such as divisions of general practice. To identify these GPs it will be necessary to consult with ethnic health workers and ethnic consumer groups. It is important that these GPs are actively approached to be involved in the shared care program even if they are unknown to service providers. It is likely that these GPs are well known to the ethnic communities they serve. These important GPs may need special
visits to be briefed about the program and the possible benefits to them and their patients. Building personal relationships is an important factor in recruiting bilingual GPs in particular. In the Brisbane inner south project it was found that GPs who had not participated in previous divisional activities carried an enormous load of mental health patients and they formed a valuable component of the shared care program. Furthermore, the shared care program reduced the isolation experienced by these GPs by increasing their referral options and providing valuable clinical consultation opportunities. However, some GPs were reluctant to refer their patients on to other services, believing these to be culturally inappropriate. These GPs needed encouragement to raise these issues in the shared care program and also needed reassurance that they would remain in the role of case coordinator, despite referring patients to other services. GPs require ongoing contact from shared care program staff and may find it difficult to attend set meetings, instead preferring individual meetings with program staff. Negotiations may need to take place about how the program can realistically meet the individual needs of GPs . Skills development Simply having willing participants will not be enough to start setting up shared care arrangements. The participants will need to be trained in
Page 27
DEVELOPING RELATIONSHIPS, SYSTEMS & PROTOCOLS

Mental health shared care for ethnic communities – a handbook
Page 28
The Brisbane inner south project developed the f o l l o w i n g w r i t t e n communication tools. (They can be perused in the ‘appendices’ section.) • Fax service request
form • GP resource guide • GP resources summary The GP resource guide included a master copy of an interpreter request form, which is essential to include in ethnic shared care program written materials.
all aspects of transcultural mental health before the program can be implemented. Other program participants may also need skill enhancement on issues such as mental health, general practice and basic things such as using professional interpreters. The following page provides a snap-shot of issues to be covered in training about interpreters, as a guide. One of the major lessons learned from the Brisbane inner south project is that training should not be skimped on. Training is also most useful when it is conducted on an ongoing basis so that trainees can bring their real life practice issues to training. This not only enhances their learning but provides for a much more engaging training experience for all participants. Communication Mental health services and GPs participating in the shared care p r o g r a m s h o u l d e s t a b l i s h communication as early as possible. According to Keks et al (1998), the best kind of collaboration occurs when GPs and community mental health staff get to know about each other’s role and stay in personal contact. However, this may need to be a facilitated process. Educational meetings organised by the service and/or the local Division of General Practice are a useful opportunity for such networking. In the Brisbane inner south project, case discussion meetings were
organised but were poorly attended by GPs. Service providers demonstrated a high level of commitment by consistently attending such meetings but it was not possible in the project, to determine how GPs could be encouraged to participate in such meetings. However, the initial training seminars organised by the ethnic shared care program coordinator were well attended by GPs and service providers alike. Ongoing opportunities for face-to-face meetings are another important component of establishing good communication and goodwill. Program meetings, case discussion as well as training all provide an opportunity for this to take place. Protocols It is likely that the shared care program will develop its own written materials to facilitate the shared care procedures and protocols. These could include referral protocols, information sheets and referral feedback forms. It is essential that a representative from all participant services have input into the development of these communication tools so that they are shared, owned and relevant to all concerned. In ethnic shared care, the translation of some materials into community languages may have significant cost implications.
Developing relationships, systems & protocols

Mental health shared care for ethnic communities – a handbook
Translating and interpreter service
The Translating and Interpreter Service (TIS) provides both over-the-phone interpreters at short notice and on-site interpreters that are booked a couple of days in advance. It is important to establish language, ethnic and gender preferences for interpreters and to request these from TIS. The TIS telephone number is 131 450. Telephone interpreters can be accessed 24 hours per day.
Accessing telephone interpreters: 1. Call TIS on 131 450. 2. Explain the purpose of your call and nominate the
language (and gender/ethnic preference) required. 3. State that the interpreter is required for a doctor’s
consultation. 4. You will then be connected to an interpreter in the
language you require. 5. The telephone interpreter service can also be pre-
booked for an extra fee. If the call is booked in advance this will ensure that any special requirements can be catered for.
Accessing on-site interpreters: 1. Determine the language, ethnicity and gender
required. 2. Complete an Interpreter Request Form (available
from TIS). 3. Fax the completed Interpreter Request Form to TIS
on 1300 654 151 with reasonable notice – at least a couple of days in advance.
4. TIS will confirm the booking by sending a return fax. Using phone interpreters
These can be used if you are with the patient or if the patient is at another location:
Same location: 1. Sit with the patient next to a telephone. Put the
telephone on the ‘speaker’ function. 2. Call TIS on 131 450 and the operator will connect
you to an interpreter in the language you require. 3. Sit facing the patient. Be aware of facial expressions
and body language. 4. Speak in the first person at all times. 5. Be sure that the interpreter can hear clearly.
6. Keep the amount of information to be interpreted at any one time short, with one idea per sentence.
7. So that the participants do not talk over each other, include a pause after each sentence.
Different locations: 1. Call TIS on 131 450 and ask the officer to
contact the required interpreter, who will then call the patient.
2. A three-way conversation can then take place. 3. In the same way, patients can use this service
to contact the GP. Using on-site interpreters 1. Introduce everyone and establish roles. 2. Arrange seating to facilitate communication
between yourself and the patient. The ideal seating arrangement is a triangle, with participants at equal distances from each other, so that eye contact can be maintained at all times.
3. Maintain eye contact with the patient if culturally appropriate (rather than engaging with the interpreter). Avoid private discussions with the interpreter.
4. Speak directly to the patient, on first person terms.
5. Speak slowly and clearly but naturally. Avoid jargon. If jargon is unavoidable e.g. medical terminology, ensure that the interpreter understands the concept.
6. If you feel that the patient and interpreter are speaking together and excluding you to the extent that you are not establishing communication with the patient, you should stop the interview. Restate the ground rules and start again.
7. Summarise your discussion periodically throughout the interview to ensure shared understanding of what is being said.
8. With consecutive interpreting, use short sentences.
Box 2: Accessing and using the Translating and Interpreting Service
Page 29 Developing relationships, systems & protocols
GPs can access interpreters from TIS free of charge

Mental health shared care for ethnic communities – a handbook
Page 30
“We really want the GP to be part of the treatment team, we will set up case conference times to suit the GP, we just need more GPs to work with!” - service provider in the Brisbane inner south project
Care planning is a critical component of shared or integrated care. The contents of a care plan are partly influenced by the program and its aims, but there are generally three models of care: acute, intermediate and long-term. The Brisbane inner south project found that key elements of a care plan included:
· A list of who was involved in the care and treatment of the person and how to contact them.
· A person’s met and unmet needs and goals for activity, to be addressed by any clinician or the consumer.
· A person’s early warning signs of acute and/or worsening illness
· A brief summary of a person’s mental health history, including d iagnosis , date of last admission and reasons for admission.
· A person’s medication history and a clear outline of who is responsible for managing repeat prescriptions, changes i n medicat ion and the monitoring of side effects.
· Date of plan and review date. It can be a challenge to set up a system or process that facilitates the creation of care plans. In the Brisbane inner south project, attempts were made by the project to organise case conferences through the provision of opportunities for GPs and service providers to meet for case discussion.
However, it was a challenge to get GPs to bring cases along to these meetings. MBS and case management The MBS items for care planning and case conferencing can be used advantageously for shared care. It allows for GP involvement in the development of patient care plans and case conferences, and the opportunity to clearly outline individual roles and responsibilities in patient care. These are all essential components of a shared care program. These MBS items mean that GP involvement is feasible and GPs can be remunerated for their involvement. It is important that the availability of the MBS items be communicated to GPs as early as the recruitment stage, as some GPs may not be aware about the use of these items. Furthermore, MBS utilisation should be addressed in preliminary training. Such training should be attended not only by GPs but all other service providers so that an accurate and sound knowledge is developed by all program participants. This is particularly important as GP involvement in case conferences and care planning can be initiated and requested by service providers.
CARE PLANNING PROCESSES

Mental health shared care for ethnic communities – a handbook
“We vaguely know what is around but don’t have the opportunity to really find out, unless you get involved in a project like this. It is great to build the relationship and we must continue to build the relationship.” - GP in the Brisbane inner south project
Shared care projects are an opportunity to establish relationships and develop systems to facilitate ongoing collaboration. However, as most shared care programs operate on time-limited funding, one of the challenges is to sustain the impact and benefit of the program for as long as is feasible. However, it may not be possible to maintain all aspects of the shared care program, particularly if certain functions were carried out by program staff, rather than program participants themselves. These tasks could include: • Facilitation of case discussions • Ongoing training • Administrative support
• Coordination of meetings • Liaison between program
participants • Trouble shooting • Ongoing recruitment of GPs Such tasks should be considered from the outset to determine if they are time-limited by the establishment phase, or ongoing and essential to program operation. There were a number of issues that the Br isbane inner south project considered from the outset to maximise the project’s sustainability and maintenance beyond the funded life of the project. These appear in Table 4 below.
Strategy to sustain the program Specific issues to consider
Ongoing meetings between program par-ticipants to monitor and review shared care processes.
• Commitment of all parties to the program
• Time commitments necessary to participate and attend meetings
Ongoing training and professional devel-opment to maintain interest and rele-vance.
• Training program to be drawn up from the outset
• Some training at commencement but ongoing training thereafter
Integration of ethnic shared care into a mainstream program.
• Partnership with a relevant main-stream program from the outset
• Establishment of parallel processes • Clear integration plan from the out-
set
Table 4: Strategies and considerations for program sustainability
Page 31
MAINTAINING SHARED CARE

Mental health shared care for ethnic communities – a handbook
Page 32
The evaluation framework ideally should be developed at the planning stage of the program. An evaluation framework usually involves the collection of data to answer questions about program process, impact and sometimes, outcome. Thus the first step in developing an evaluation framework is to set the evaluation questions. These may i nc l u de quest ions about the effectiveness of program processes, the impact of training or the program
itself on participants, or any intended or unintended outcomes. The next step is to develop data collection tools that will answer the evaluation questions. It may also be possible to use existing data collection processes such as statist ical in formation that organisations routinely collect, for the evaluation. The perspective of the three main participant groups (consumers, GPs and services) should guide the development of data collection tools to ensure that the tools will be accessible
Measures Accessibility & feasibility
Patients Levels of satisfaction Levels of access Tool: personal in-depth interviews
GPs required for access to patients and to obtain consent. Interviews were accessible and feasible once ground-work was achieved.
Service providers
Referral numbers Program processes – satisfaction and effi-ciency Tool: focus group
Service data could not be relied on be-cause inadequate records were kept by services. Focus group was used for feedback.
GPs Program processes – satisfaction and effi-ciency Use of referral options Use of program resources Tool: pre and post-training questionnaires, focus group, telephone interviews, GP check list, GP case studies
Focus group was used for feedback but was poorly attended. Individual telephone interviews were used to augment information from focus group. GP check list relied on intervention & control groups to compare impact of in-tervention. This was difficult to facilitate and only small numbers of GPs partici-pated. Case study data provided rich informa-tion.
Table 5: Evaluation strategies in the Brisbane inner south project from the perspective of three participant groups
EVALUATING THE PROGRAM

Mental health shared care for ethnic communities – a handbook
and realistic. Considerable negotiations with the participant groups will need to take place from the outset of the program to discuss the type of data that is required from them. Groups should also be given input into the development of tools to ensure that they will be used. Step three involves the development of indicators that will answer the evaluation questions. Some examples of indicators are: • A 25 per cent increase in referral
to mental health services by GPs • Demonstrated improvement in
knowledge by mental health workers in transcultural mental health practices.
Fourthly, all the participants who are required to collect data must be trained and briefed about the evaluation and what is required of them. Time-frames should be set and regular contact should be made with participants to ensure that the data collection tools are being used correctly. Finally, an analysis framework should be developed. An analysis framework guides the analysis of the evaluation data. The framework may contain information about the weighting of different perspectives. For example, the perspective of consumers may take p recedence over othe r
perspectives about the program, or, the perspectives of the three groups may be triangulated and considered equally. The analysis framework may also provide a guide on the methodology for data analysis. Group processes such as evaluation workshops involving program participants could be used, or program staff could themselves analyse the data or perhaps an external consultant could be used. The table on the next page provides an example of the evaluation strategies used in the Brisbane inner south pro ject , to measure program effectiveness (excluding the cost analysis).
Page 33 Evaluation

Mental health shared care for ethnic communities – a handbook
Page 34
Training course
Evaluation question Data collection tool Indicator Who to collect
Has the training increased GP knowledge and under-standing of transcultural mental health issues?
Pre and post question-naire
Improvements in knowledge and understanding demon-strated by GPs
Project coordi-nator
Has the training course in-creased GP skills in identify-ing mental illness in patients of NESB?
Pre and post question-naire GP checklist
Identification rates by GPs who undertook training and GPs in the control group (non-trained)
Project coordi-nator
Has the training course in-creased GP awareness of available mental health services?
Pre and post question-naire GP checklist
Improvements in GP aware-ness of services
Project coordi-nator
Has the training enabled GPs to be active participants in shared care?
Content evaluation questionnaire GP check list Number of communi-cations/referrals to mental health services
GP stated intention to par-ticipate in shared care GP actual participation in shared care
Project coordi-nator
Has the training increased GP confidence in identifying mental illness in patients of NESB?
Self reporting by GPs in questionnaire/ inter-view GP check list
Increased level of confi-dence Increased number of men-tal illnesses identified by ac-tive GPs
Project coordi-nator
Shared care
What are the systems devel-oped and implemented by the project of facilitate shared care?
Project data Utilisation rates by service providers - GP check list - Service data
Number of systems imple-mented Systems are utilised by rele-vant service providers as agreed within the program Quality and frequency of communication between services
All service pro-viders
Are GPs able to make appro-priate referrals to mental health services?
Service data Number of referrals Appropriateness of referrals
Service pro-viders
Are GPs using the new MBS items to participate in shared care?
GP check list Number of items claimed per GP
Project coordi-nator
What is the impact of the shared care program on the level of satisfaction of key stakeholders?
Service provider and GP focus group Patient interviews
Stakeholder satisfaction Project coordi-nator
Table 6 – Evaluation framework for program effectiveness in the Brisbane inner south project
Evaluation

Mental health shared care for ethnic communities – a handbook
It is hoped that the issues and practical strategies outlined in this handbook will assist others to plan, implement and evaluate their own ethnic mental health shared care programs. Ethnic mental health shared care can improve the quality of services received by people of NESB with mental health problems and should therefore be considered to be an important component of all mainstream mental health shared care programs. The Brisbane inner south ethnic mental health shared care project, although a
Page 35
CONCLUSION small demonstration project, did contribute valuable information and insights into ethnic mental health shared care. In particular, the project demonstrated the positive impact of GP training, with significant differences recorded in GP responses to patients of NESB with mental health problems. The primary pathway to mental health care for people of NESB often starts with the GP and therefore, despite the challenges of setting up shared care, it is well worth persevering, to achieve more equitable outcomes for people of NESB with mental health problems.

Mental health shared care for ethnic communities – a handbook
Page 36
ACCESS SERU, Sharing Mental Health Care A Guide for Divisions of General Practice, SERU, 1997 Andrews, G Hall W, Teesson M & Henderson, S, The Mental Health of Australians, Commonwealth Department of Health and Aged Care, Mental Health Branch, Canberra, 1999 De Bruyn, Evaluation of programs for the treatment of schizophrenia: a health economic perspective, Health Canada, 1994, www.hc-sc.gc.ca/hppb/mentalhealth/pubs/evaluation Fitzgerald, M (1992) ‘Multicultural Clinical Interactions’, Journal of Rehabilitation, April-June, 38-42. Hickie, I B, ‘Primary care psychiatry is not specialist psychiatry in general practice’ in Medical Journal of Australia, 1999; 170: 171-173 (http://www.mja.com.au/public/issues/feb15/hickie/hickie.html) Keks N, Altson B, Sacks T, Hustig H and Tanaghow A, ‘Collaboration between general practice and community psychiatric services for people with chronic mental illness’, Medical Journal of Australia, 1998, www.mja.com.au/public/mental_health/articles/keks2/keks2.htm/, pp1-2 Kleinman, A Esenberg, I and Good, B, ‘Culture, illness and care: clinical lessons from anthropological and cross-cultural research‘, Annals of Internal Medicine, 1978:88 Lehn A, ‘Recent Immigrant’s Health and their Utilisation of Medical Services. Results from a longitudinal Survey of Immigrants to Australia‘, Department of Immigration and Multicultural Affairs Immigration update, March Quarter, 1997 Mazza, D ‘A coordinated national approach to clinical practice guideline implementation for GPs’ To Their Full Potential: Evidence based guideline uptake in primary mental health care. Conference Proceedings, Centre for General Practice Integration Studies, UNSW, 2000 McDonald R and Steele Z, Immigrants and mental health: an epidemiological analysis, TMHC NSW 1997 Mihalopolous C, Pirkis C, Naccarella L and Dunt D, The Role of General Practitioners and other Primary Care Agencies in Transcultural Mental Health Care, ATMHN, Vic, 1999 Minas, H, Texbook of Community Psychiatry , Oxford Press, Melbourne, 2000 Nelson K, Cumming J, MacEwan V, ‘Early lessons in shared care: experience from a pilot involving general practitioners in the care and treatment of people with ongoing needs from mental health services’, Geigy Psychiatric Symposium, Dec 1997, pp 71-71. Silove D and Steele Z, The mental health and well-being of on-shore asylum seekers in Australia, Psychiatry Research & Teaching Unit, Liverpool Hospital, NSW 1998
REFERENCES

Mental health shared care for ethnic communities – a handbook
Page 37
appendices
Appendix 1 – Protocols used in Brisbane inner south project: GP re-sources summary
1. TIS Fax Booking Form
Use when an on-site interpreter or pre-booked telephone interpreter is required. At least 48 hrs notice is required.
2. Fax request Form Use when access to staff from the following organisations is required to discuss follow up support for your patient:
• Ethnic Mental Health Program (bilingual support workers) • Qld Program of Assistance to Survivors of Torture and Trauma • Transcultural Clinical Consultation Service • Psychiatry consultation and liaison service (BISDIV)
3. MHS Intake and Referral Form
If you have diagnosed your patient, use this form when making a referral to the Adult Mental Health Service. When filled in completely the referral will go straight through to a team review meeting and bypass the assessment process. A photocopy is acceptable so you can keep the form for your records if you wish.
IMPORTANT COMMUNICATION TOOLS:

Mental health shared care for ethnic communities – a handbook
I request the following service(s) for my patient:
Page 38
appendices Appendix 2 – Protocols used in Brisbane inner south project: fax request form
To (tick service required)
Name of service Fax number
Ethnic Mental Health Program Fax 3891 7922 Ph 3891 7911
Qld Program of Assistance to Survivors of Torture and Trauma
Fax 3391 6388 Ph 3391 6677
Qld Transcultural Mental Health Centre Clinical Consultation Service
Fax 3240 2282 Ph 3240 2833
Brisbane Inner Sth Division of General Practice Psychiatry consultation and liaison
Fax 3392 2920 Ph 3392 2822
Patie
nt d
etai
ls:
Ethn
icity
:
Pref
erre
d la
ngua
ge:
Gen
der:
M
F A
ge:
D
urat
ion
in A
ust:
Dur
atio
n of
illn
ess:
NESB MENTAL HEALTH SHARED CARE PROJECT FAX REQUEST FORM
Ethnic Mental Health Program
Patient support Support and follow up for patient Support and education for family Case discussion re ongoing management of patient Joint assessment and interview with patient
Information Regarding culture of patient Regarding other support services within cultural group Regarding mental health services Mental health information
Shared care Follow up on shared patient Case conference requested Update on care plan
Patient support Support and follow up for patient Case discussion re ongoing management of patient Specialist counselling for refugee patient Request for joint assessment and interview with patient
Shared care Follow up information on shared patient Case conference requested Update on care plan
Transcultural Mental Health Centre Clinical Consultation
Assessment & diagnosis and short-term intervention
Case discussion re cross cultural and clinical input into as-sessment Information about available services for patient Request for joint assessment and interview with patient Short term counselling for patient Psycho-education for patient/family
BISDIV Psychiatry Consultation and Liaison
Assessment & diagnosis Case discussion with a psychiatrist Request for joint assessment and interview with patient
QPASTT
From: Dr Phone: Fax: Mobile: Date: Best time to ring me back:

Mental health shared care for ethnic communities – a handbook
NESB Mental Health Shared Care Project When to use fax request form Resources available to project GPs
1. Clinical Consultation and liaison Dr Frances Dark will visit your surgery at a time convenient to you for case discussion or joint consultation with patient for assessment and diagnosis. Use fax request form to request a visit from Dr Dark
2. Clinical Consultation and liaison (Transcultural) Contact Polly Nip at Transcultural Mental Health Centre for access to a bilingual/bicultural mental health professional to provide input into assessment, diagnosis or other care management issues. Can also provide short term interventions such as counselling. Use fax request form to request a service from Polly.
3. Bilingual mental health support worker The Ethnic Mental Health Program has mental health support workers who are Vietnamese, Chinese, Spanish speaking, Croatian, Greek and Italian who can provide one on one support to your patient and their family. The program also has a range of support groups. Use fax request from to request a service from Valentina, coordinator Ethnic Mental Health Program
4. QPASTT Specialist services available through QPASTT for refugees who are survivors of torture and trauma. These services include counselling, case work support, youth program, children’s program and natural therapies program Use fax request form to request a service from QPASTT
appendices Appendix 3 – Protocols used in Brisbane inner south project: GP quick reference guide
Page 39

Mental health shared care for ethnic communities – a handbook
appendices Appendix 4 – Protocols used in Brisbane inner south project: GP resource guide
Page 40
Shared Mental Health Care for people from non English speaking backgrounds
Brisbane Inner South Division of General Practice Brisbane Southside Central Division of General Practice
Queensland Transcultural Mental Health Centre Ethnic Mental Health Program
Queensland Program of Assistance to Survivors of Torture and Trauma Adult Mental Health Services (Coorparoo, West End, Inala)
The following information is for General Practitioners, Mental Health Professionals and non-government agencies supporting NESB people with mental health problems with the objective of promoting better communication and systems between health professionals to facilitate shared care. The aim of this document is to provide you with an easy to follow reference guide and checklist on who you can contact and liaise with to support you in providing optimum care to your patient. We hope you find this information useful and easy to use and invite you to make use of the support and resources that are available to you and your patients and that the enclosed referral forms will facilitate easy access to services. You may also find that as you are using this information, that you have questions or suggestions to improve this information. Please contact us at: Brisbane Inner South Division of General Practice PO Box 8004 Woolloongabba Q 4102 Ph 3392 2822 Fax 33922920
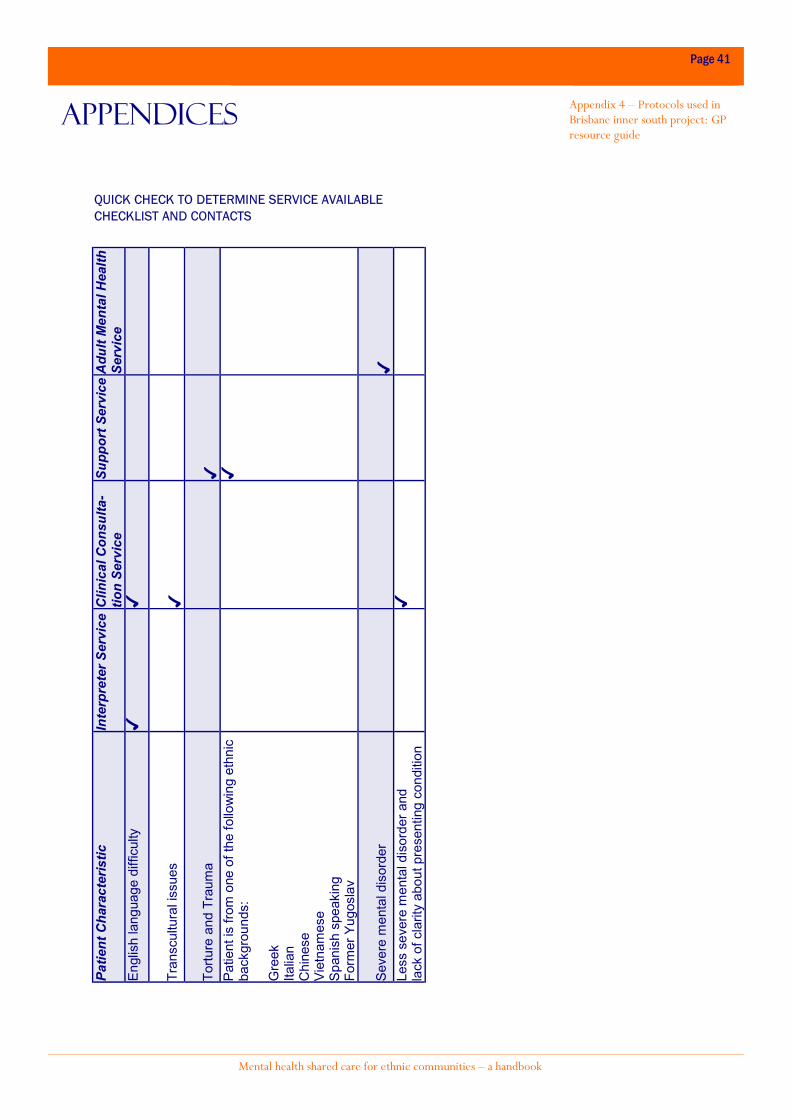
Mental health shared care for ethnic communities – a handbook
appendices Appendix 4 – Protocols used in Brisbane inner south project: GP resource guide
Page 41
Patie
nt C
hara
cter
istic
In
terp
rete
r Ser
vice
Clin
ical
Con
sulta
-tio
n Se
rvic
e Su
ppor
t Ser
vice
Adu
lt M
enta
l Hea
lth
Serv
ice
Engl
ish
lang
uage
diff
icul
ty
Tran
scul
tura
l iss
ues
Tortu
re a
nd T
raum
a
Patie
nt is
from
one
of t
he fo
llow
ing
ethn
ic
back
grou
nds:
G
reek
Ita
lian
Chi
nese
Vi
etna
mes
e Sp
anis
h sp
eaki
ng
Form
er Y
ugos
lav
Seve
re m
enta
l dis
orde
r
Less
sev
ere
men
tal d
isor
der a
nd
lack
of c
larit
y ab
out p
rese
ntin
g co
nditi
on
QUICK CHECK TO DETERMINE SERVICE AVAILABLE CHECKLIST AND CONTACTS

Mental health shared care for ethnic communities – a handbook
appendices Appendix 4 – Protocols used in Brisbane inner south project: GP resource guide
Page 42
Patie
nt C
hara
cter
is-
tics
Key
pha
se o
f car
e Se
rvic
e/R
esou
rce
avai
l-ab
le
Con
tact
Ac
cess
/ R
efer
ral P
ro-
toco
l U
nabl
e to
com
mun
icat
e in
En
glis
h
All p
hase
s of
car
e Tr
ansl
atin
g an
d In
terp
retin
g Se
rvic
e
13
14
50
Fax
book
ing
form
for o
nsite
in
terp
retin
g an
d pr
e bo
oked
te
leph
one
inte
rpre
ter.
Tran
scul
tura
l iss
ues
Adm
issi
on/i
ntak
e Co
nsul
tatio
n to
est
ab-
lish
hist
ory
Asse
ssm
ent,
diag
nosi
s D
evel
opm
ent o
f tre
at-
men
t pla
n
Spec
ialis
t con
sulta
tion
by s
es-
sion
al b
iling
ual w
orke
r for
as-
sess
men
t and
dia
gnos
is
Case
dis
cuss
ion
for o
ngoi
ng
man
agem
ent o
f pat
ient
Sh
ort t
erm
cou
nsel
ling
Tran
scul
tura
l Clin
ical
co
nsul
tatio
n Se
rvic
e Ph
32
40
28
33
Fax
32
40
228
2
Fax
requ
est f
orm
Ref
ugee
Bac
kgro
und
Surv
ivor
of T
ortu
re a
nd
Trau
ma
All p
hase
s of
car
e H
ealth
sup
port
Sp
ecia
list c
ouns
ellin
g
Qld
Pro
gram
of A
ssis
-ta
nce
to S
urvi
vors
of
Tort
ure
and
Trau
ma
Ph 3
39
1 6
67
7
Fax
requ
est f
orm
Patie
nt is
from
the
follo
w-
ing
ethn
ic b
ackg
roun
d Ch
ines
e Vi
etna
mes
e G
reek
Ita
lian
Form
er Y
ugos
lav
(Cro
atia
n,
Serb
ian,
Bos
nian
) Sp
anis
h sp
eaki
ng
All p
hase
s of
car
e, e
s-pe
cial
ly o
ngoi
ng c
are
Bili
ngua
l sup
port
wor
ker
to
supp
ort p
atie
nt w
ith tr
eatm
ent
and
follo
w u
p
Educ
atio
n fo
r ca
rer/
fam
ily
Ethn
ic M
enta
l Hea
lth
Prog
ram
Ph
38
91
79
11
Fax
38
91
792
2
Fax
requ
est f
orm

Mental health shared care for ethnic communities – a handbook
appendices Appendix 4– Protocols used in Brisbane inner south project: GP resource guide
Page 43
Seve
re m
enta
l illn
ess
(acu
te)
Non
acu
te
Asse
ssm
ent
Inta
ke, a
sses
smen
t and
re
ferr
al
Coor
paro
o M
on-F
ri 8
.30
am
- 3.0
0 p
m
(in p
erso
n)
Coor
paro
o M
on –
Fri
8.3
0 a
m –
5.0
0 pm
(by
phon
e)
PAH
Men
tal H
ealth
Ass
essm
ent T
eam
M
on-F
ri 3.
00
am
– 1
1.0
0 pm
PA
H M
enta
l Hea
lth A
sses
smen
t Tea
m
Wee
kend
s an
d Pu
blic
Hol
iday
s
10
.00
am
– 6
.00
pm
If pa
tient
is d
iag-
nose
d by
GP
the
In-
take
Ref
erra
l For
m
can
be c
ompl
eted
by
GP
and
forw
arde
d to
lo
cal m
enta
l hea
lth
serv
ice,
whi
ch w
ill g
o to
a te
am re
view
m
eetin
g. T
his
is p
ref-
erab
le fo
r pat
ient
s w
ho h
ave
a la
n-gu
age
barr
ier
as a
n in
terp
rete
r can
be
book
ed b
y th
e se
rv-
Less
sev
ere
men
tal i
llnes
s La
ck o
f cla
rity
abou
t pre
-se
ntin
g co
nditi
on
Asse
ssm
ent,
diag
no-
sis,
and
dev
elop
-m
ent o
f tre
atm
ent
plan
Clin
ical
con
sulta
tion
from
a
psyc
hiat
rist
Bris
bane
Inne
r St
h D
ivis
ion
of G
ener
al
Prac
tice
Ph 3
39
2 2
82
2 Fa
x 3
39
2 2
920
Fax
requ
est f
orm

Mental health shared care for ethnic communities – a handbook
Page 44
This handbook was developed by Marina Chand on behalf of the Brisbane Inner South Division of General Practice. It was developed with the assistance and input from Marco Ramirez, Brisbane Inner South Division of General Practice and Rita Prasad-Ildes from the Queensland Transcultural Mental Health Centre. Special thanks and appreciation to the following members of the project reference group who found time in their busy schedules to provide valuable comments and feedback: Sue Gargett School of Public Health, Queensland University of Technology Amanda Kivic Team Leader, Coorparoo Adult Mental Health Service Alison Smith Brisbane Southside Central Division of General Practice Dr Robert Zubeshaw General Practitioner Thank you also to other members of the reference group: Dr Frances Dark, Robyn Prince, Glenys Powell, Donata Rossi, Valentina Dimoska and Damian Stanley-Jones and all the consumers and service providers who agreed to be interviewed and/or attend feedback meetings.
acknowledgments

Mental health shared care for ethnic communities – a handbook


















