Mental Health in the Elderly - douglas.qc.ca croisée 2015/Dr-Di... · Mental Health Disorders ......
36
Mental Health in the Elderly Maria Di Tomasso M.D. F.R.C.P
-
Upload
hoangxuyen -
Category
Documents
-
view
223 -
download
5
Transcript of Mental Health in the Elderly - douglas.qc.ca croisée 2015/Dr-Di... · Mental Health Disorders ......

Mental Health in the
Elderly Maria Di Tomasso M.D. F.R.C.P

Overview
• Demographics
• Epidemiology of Depressive, Anxiety, and
Psychotic Disorders
• Different clinical presentations between older and
younger adults with mental illness
• Risk Factors and Protective Factors
• Treatment

–Socrates
“I enjoy talking with very old people. They
have gone before us on a road by which we,
too, may have to travel, and I think we do well
to learn from them what it is like.”

Introduction
Demographics
• Canada met a milestone in July 2015, for the first time
ever there are more Canadians age 65 and over than
there are under age 15
• The growth rate of people over 65 is four times faster
than the population at large
• In 2011, centenarians were the second most rapidly
growing segment of the population, after those aged
60-64, which experienced the fastest increase
• By 2030 25% of Canadians will be over 65

Canada's Aging Population

Geriatric Psychiatry • An official subspecialty of the Royal College of Canada
since 1999
• Managing elderly patients requires special knowledge
• Mental illness should not be a normal part of aging
• Canadian Community Health Survey found that 68.9 %
of seniors reported their mental health as very good or
excellent
• The majority of older individuals remain mentally
healthy and aging can be a time of growth and tapping
into one's potential

Classification
• Mood Disorders
• Anxiety Disorders
• Suicidal Behaviour
• Neurocognitive Disorders due to a medical condition including
Dementia and Delirium
• Personality Disorders
• Substance Use Disorders including Prescription drugs and Alcohol
• Psychotic Disorders

Late Life Mental Health
Challenges
Age is NOT a risk factor for a mental disorder
• Chronic health conditions is the biggest risk factor
• Death of a loved one
• Caregiving
• Significant loss of independence and limitation of activities
• Loss of societal roles

Late Life Approach to
Mental Health Disorders • High index of suspicion
• Use cohort appropriate language
• Interview family members for collateral information
• Review the medical history including medications to rule out a
medical cause
• Medical investigations
• Elderly are often on multiple drug regimens therefore vigilance of
drug-drug interactions is necessary
• Always evaluate cognition
Late Life
Depression
Late life depression is not a
single disorder but rather a
heterogeneous disorder
made up of a number of
clinical syndromes

Late Life Depression
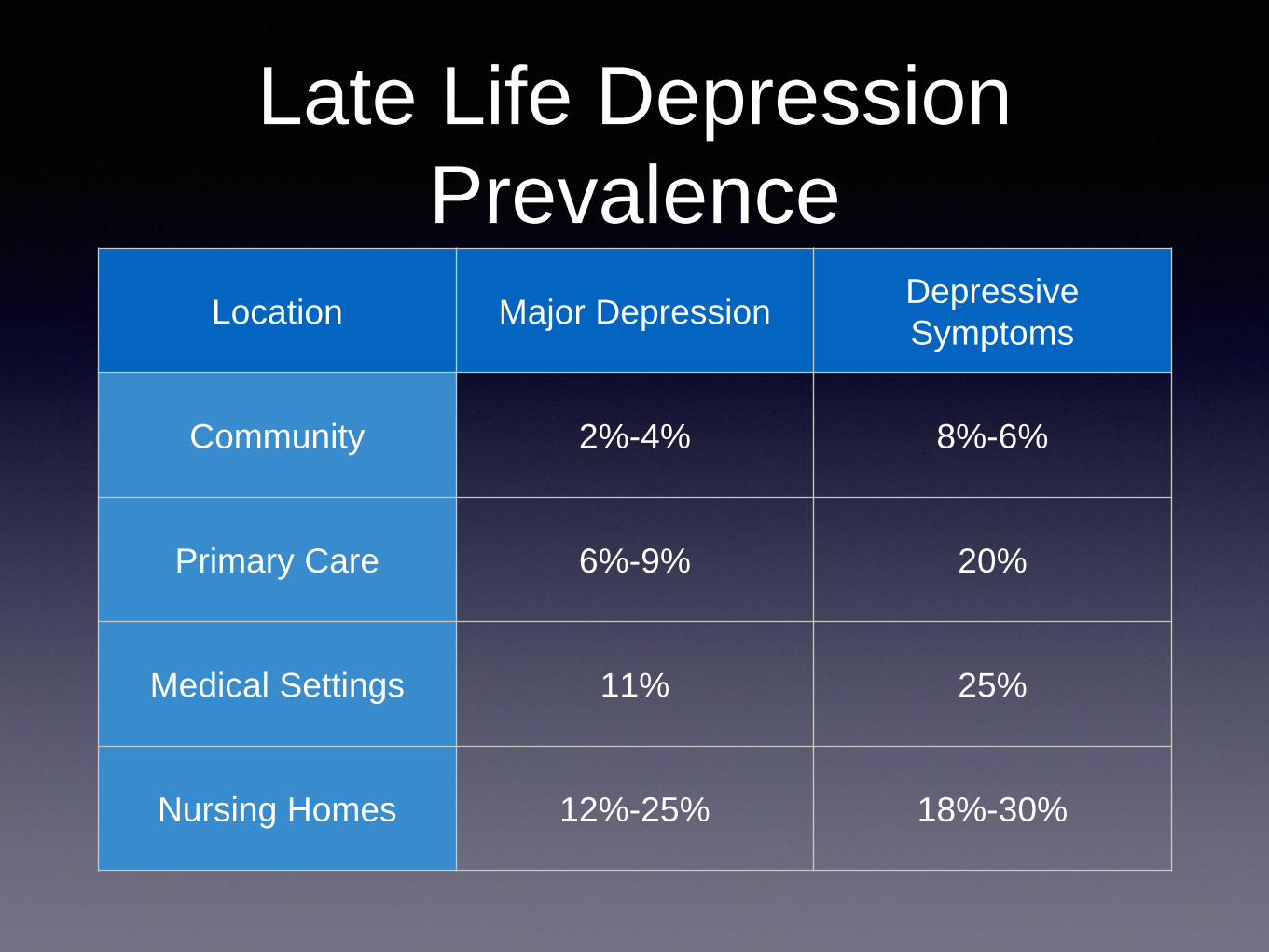
Late Life Depression
Prevalence
Location Major Depression Depressive
Symptoms
Community 2%-4% 8%-6%
Primary Care 6%-9% 20%
Medical Settings 11% 25%
Nursing Homes 12%-25% 18%-30%

Barriers to Diagnosis • Patient Factors
- May not complain of sadness or depression
- Symptoms are different than younger adults
- Patients present with more somatic and cognitive symptoms
- Often do not seek mental health services, view depression as a
sign of weakness, stigma
- May be isolated with limited transportation
• Physician Factors
- Depression is seen as a normal response to aging
- Misattribute depressive symptoms to a physical illness
- Therapeutic nihilism
Late Life Depression
Common Presentations • Melancholic: anhedonia, early morning awakening, severe guilt,
psychomotor slowing
• Agitated: insomnia, restlessness, pacing, irritability
• Masked: somatic complaints, anxiety, hypochondriasis, negativity
• Psychotic: ego-syntonic delusions, auditory hallucinations
• Late Onset Depression: > age 60, silent strokes on CT or MRI,
cognitive deficits, loss of energy, physical disability
• Long-Term Care: signs observable by caregivers, new
oppositional behaviour, decreased socialization or self care

When to Suspect Depression
Special Clinical Features and Clues
• Prominent loss of interest and pleasure in activities
• Prominent cognitive complaints
• Irritability
• Heightened pain complaints
• Unexplained health worries
• Multiple visits to G.P. without resolution of the problem
• Slow recovery post surgery
• Refusal of treatment
• Prolonged hospitalization
• Excess disability
• Social withdrawal and avoidance of social interaction
• Unexplained functional decline

Causes of LLD
Etiological and Risk Factors
• Medical: High measures of medical burden triples the risk of depression
Theres is a reciprocal relationship between depression and medical illness.
Physical health impacts mental health and mental health impacts physical health.
- Neurological disease: Parkinson's disease, Stroke, Alzheimer's disease,
Silent Strokes or WMH
- Cardiovascular Disease
- Malignancies: Pancreatic cancer
- Endocrine disorders: Hypothyroidism
- Medications, polypharmacy, drug-drug interactions
- Sleep disturbance
• Disability alone ( measured by activities of daily living ) in the absence of medical illness
increases the risk of developing depression by a factor of 4 for elderly living in the community

Causes of LLD
Etiological and Risk Factors
• Psychosocial:
-Personality Attributes: Neuroticism, Insecure Attachment
Obsessional traits
Personality Disorder
- Behaviour: Learned helplessness
- Poor perceived health
- Loss of a spouse or loved one
- Caregiving
- Lack of social supports
- Marital separation, divorce or widowhood
- Low socioeconomic status
- Living in a nursing home

Comorbidity LLD and
Medical Illness • Stroke 22-50%
• Myocardial Infarction 15-19%
• Cancer 18-39%
• Rheumatoid Arthritis 13%
• Parkinson's Disease 10-37%
• Diabetes Mellitus 5-11%

Consequences of LLD Depression impacts older adults differently than younger adults
• Decrease in functional status
• Decreased compliance with medical care
• Poor outcome following MI, CVA, Hip
• Increased risk of osteoporosis in women
• Increase in death:
Post MI mortality rates are 5X higher
Post CVA mortality rates are 3.5X higher
• Increased risk of death in nursing homes is 2 fold
• Suicide

Graph


Suicide in Older Adults • Adults 65 and over have the highest suicide rate of any other age group
• Men 65 and older have the highest rate in Canada
• Older adults tend to use more lethal means, firearms, hanging and poisoning
• Older adults less likely to discuss their plans, give fewer warning signs
• Nonviolent deaths from suicide may be mistakenly attributed to an illness: not taking
medications, refusal to eat,
• 50% of older adults who have committed suicide saw their GP within one month of the
suicide
• Depression is the foremost risk factor for suicide in older adults
• Passive suicidal ideation, the desire to die and the belief that life is not worth living, is not
normative in late life
• Suicide is PREVENTABLE
Late Life Depression
Protective Factors
• Spiritual and Religious Affiliations
• Social, Family, Community Supports
• Wisdom
• Physical Activity
• Socio-Emotional Selectivity

Depression and Dementia
• Depression and dementia frequently coexist and the differential diagnosis
can be challenging
• Historically major depression with cognitive deficits, "Pseudodementia" ,
was considered a reversible and benign condition
• However a subset of patients will continue to have cognitive impairment
even after remission of symptoms, with as many as 40% developing
dementia within 3-5 years
• Late onset depression with cognitive impairment is a risk factor for
dementia, may also be a prodrome or psychological reaction to an
already present cognitive deficit
• Additionally early onset depression is also considered to be a risk factor
for dementia
Treatment • The elderly have similar response rates as younger adults
• Antidepressants may take longer to start working
• Start low, go slow, but go
• Choice of antidepressant depends on previous response to treatments,
side effect profile, other medical problems, existing medications, type of
depression
• SSRI's, SNRI's, Bupropion, Mirtazapine
• Psychotherapy: Cognitive Behaviour Therapy, Interpersonal Therapy,
Problem Solving Therapy
• Electroconvulsive Therapy ECT

Late Life Anxiety Disorders
Epidemiology • Anxiety disorders are more prevalent among younger adults than older adults
• In the ECA study: 7.3% of adults 18-64
vs. 5.5% of adults >65
• Late onset anxiety disorders are infrequent, 90% of anxiety disorders begin before age of 41,
75% before the age of 21
• Different forms of anxiety occur later in life
• Generalized Anxiety Disorder and Phobias account for most anxiety in late life
• Panic Disorder is rare
• Agoraphobia and possibly Obsessive Compulsive Disorder in females, may occur for the first
time in old age
• Simple Phobia, Obsessive Compulsive Disorder in males, and Panic Disorder either persist
from younger years or arise in the context of another psychiatric or medical disorder
• Fear of falling is a unique geriatric anxiety syndrome



Clinical Presentation
• GAD: Worry is different in the elderly, focus is on health and illness in self or
spouse, not work and interpersonal issues, new onset GAD is often related to a
depressive disorder
• Agoraphobia: most common phobia, usually no history of Panic Disorder, may
appear for the first time following a stroke or medical condition
• Panic Disorder: fewer and less severe symptoms, lower levels of arousal, late
onset is very rare, suspect medical condition
• Obsessive Compulsive Disorder: more religious than contamination obsessions
and more hand washing compulsions and less symmetry and counting, more
hoarding, late onset OCD may be secondary to a neurological disorder
• PTSD: less frequent after a traumatic event, delayed onset or re-emergence of
symptoms, 30% of MI patients, correlates with impaired memory

Comorbidities
• Up to 25% of medically ill have anxiety symptoms, most common
comorbidites are with cardiovascular disease, COPD, gastrointestinal
problems,vestibular conditions, hyperthyroidism, and diabetes
• Anxiety often leads to depression, approx. half of elderly with
depression have a comorbid anxiety disorder
• All late onset anxiety should raise suspicion of a cognitive disorder
• MCI with comorbid anxiety may indicate an underlying
neurodegenerative process, twice as likely to develop Alzheimer's
Dementia in 3 years
• Substance misuse with alcohol, hypnotics and anxiolytics may be an
attempt to self medicate

Late Life Anxiety Disorders
Treatment
• Avoid benzodiazepines, benefits must outweigh the risks,
risks include falls, ataxia, cognitive impairment, short term
use only
• Citalopram, Escitalopram, Sertraline, Venlafaxine XR are
effective
• CBT, relaxation therapy, sleep hygiene, supportive therapy
• Memory aides and between session reminder telephone
calls lead to better compliance and greater treatment effect
Late Life Psychosis
Psychosis is a
symptom not a
disorder Prevalence is up to 23% of elderly
Risk Factors
Female Gender
Social isolation
Low socio-economic status
Sensory Deficits
Cognitive decline
Polypharmacy

Late Life Psychosis • Most common cause of psychosis in later life is Dementia, occurs mainly
during middle stages, hallucinations are visual> auditory, delusions of theft,
spousal infidelity, abandonment, house is not one's home, and persecution
• Second most common cause of psychosis in the elderly is Major Depression,
especially late onset depression, mood congruent delusions of guilt, poverty,
nihilism and somatization
• Most common cause of acute onset psychosis is Delirium or Substance
Induced Psychosis ( drugs/alcohol/medications, especially with anticholinergic,
sedative and analgesic medications
• Late Onset Schizophrenia ( age 40-60 ) and Very Late Onset Schizophrenia (
after age 60 ), higher rates of visual, olfactory and tactile hallucinations
• Very Late Onset Schizophrenia tends to be a prodrome of a neurodegenerative
disorder

Etiology
• What is the most common etiology of psychosis?
• Dementia 40%
• Major Depression 33%
• Delirium 7%
• Medical conditions 7%
• Mania 5%
• Substance induced 4%
• Delusional disorder 2%
• Schizophrenia 1%

Peggy Freydberg
• Began writing poetry at age 90
• Published her first poetry
book, Poems from the Pond,
at 107 years of age

Inga Rapaport
• Neonatologist who received a
doctorate in medicine at age 102