Mental Health and Psychosocial Problems

of 28
-
Upload
simonpedra -
Category
Documents
-
view
223 -
download
0
Transcript of Mental Health and Psychosocial Problems
-
7/28/2019 Mental Health and Psychosocial Problems
1/28
-
7/28/2019 Mental Health and Psychosocial Problems
2/28
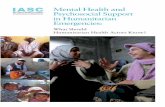
1. The Magnitude of the phenoaenon add its geographical distributionThe number o f re fugees throughout the w o r l d has been rising
substan tially over the last twenty years . According to official estimates ofthe High Commissioner fo r Refugees (Refugees , 1989) , twenty years ago therefugee population stood a t just under 2 .5 million . By 1980 it had risen to8 .2 million (Figure 1 and 2 ) . A t the beginning o f the nineties , the numbero f official refugees falling under UNHCR 's responsibility is approaching 15million . The large m ajority o f them are living in developing countries ,mainly in As ia and Afr ica . If we in f ac t look at the refugee population bycontinent (Figure 3) , we see that in Asia there are 6 .776 .000 refugees andin Afr ica 4 .587 .000 ; 1.380 .000 refugees live in Canada and the USA while inC e n t r a l and Latin A me r i ca ( including Mexico) there are approximately1.197 .000 refugees . Finally in Europe live 745 .000 refugees .
Look ing a t th e number o f refugees in se lec ted countries o f eachcontinent , we can see that in Asia , Pakistan and Iran are hosting thela rgest refugee population o f the wor ld , with respect ive ly 3 .257 .00 0 and2 .850 .00 0 Afghan refugees ; Thailand and ' Malaysia follow with substantiallysmaller numbers o f refugees ( 107 .000 and 104 .00 0 respect ive ly) (Figure 4 &5 ) .
In A f r i c a , S omal i a ( 8 3 4 .000 r e fu g e e s) , Sudan ( 745 .000 refugees ) ,Ethiopia ( 679 .000 refugees) , Malawi ( 628 .000 refugees ) and Zai re ( 34 0 .000
refugees ) are the most a f f e c te d countries (Figure 6 & 7) ; it should be notedthat some o f these countries are among the poores t o f the world . In Afr icaover the last 12 months only the number o f refugees has risen by around6 5 0 .0 0 0 ; in the last fe w months 150 .000 Liberians have fled into theneighbouring countries o f Cote d ' lvoire and Guinea . Presently one out o f
-
7/28/2019 Mental Health and Psychosocial Problems
3/28
every five African migrants is arefugee . Especially frequent in Africa is
border migration , with huge numberso f refugees crossing international
borders every day without any formality . In Africa70% o f the burden is
borne by 12 countries , and a o f the 16African countries among the least
developed in the world are affected by the refugeeproblem . An estimated 60%
o f the African refugees receive no assistance .
In North America , there are 1.000 .000refugees lving in the United
States , and 380 .000 in Canada (Figure 8).In Central America there are 278 .000 refugees
in Costa Rica , 237 .000 in
Honduras and 223 .000 in Guatemala (Figures9 & 10) .
In Europe , for a total number of refugeesapproaching 745 .000 people ,
184 .000 refugees live in France , 150 .000in West Germany , 139 .00 0 in Sweden
and 1 .000 in Ialy (Figures 1 & 12) .Even Europe has had to face sudden
and substantial increases in the numberso f refugees who flee : for instance ,
between June and September 1989 more than300 .000 Bulgarians crossed the
border into Turkey . Since 1983Western Europe as a whole has
received
700 ,000 asylum applicants . Host of them- some 300 .000 - have come from
Asia
and the Middle East .And even these figures do not include
over two mion Palestinians who
are assisted by UNRWA (the UN Reliefand Work Agency ) and the over 300 .000
Khmer displaced people assisted by UNBRO(the UN Border Relief Operations );
moreover they re fer only to thosepeople who have received the official
status o f refugees and who are coveredby the 1951 UN Convention relating
to
the status o f refugees and by thesubsequent protocol drafted in 1967 . They
do not incude the huge numbers o fso -called internally displaced
people and
migrants . Just to give an idea of themagnitude of these two phenomena , it
-
7/28/2019 Mental Health and Psychosocial Problems
4/28
is sufficient to remember that in Europe there are now some 20 millionimmigrants , and 35% o f them come from developing countries (Figure 13 )(Refugees , 1990) . The proportion o f foreign -bom in many European countriesamounts to between 10 and 15% , compared to 6% in USA and 16% in Canada . Lastyear there were more than 1.2 million arrivals from the East to the West .The year 1989 marked a turning point : if we consider refugees , asylumseekers , foreign workers , sett lers from the east , and family members , morethan 3 million people arrived in 1989 , twice as many as in previous years .
In the last tw o decades , nine million people have left the semi - developedcountries on the Southern side o f the Mediterranean sea to take up work inthe industrialized Nor t h . Accord ing to some demographers , a possiblescenario involving the depar ture o f some 25 million people during the nextfour dec ades cannot b e exc luded ( R i c c a, 1989 ) . Finally , as regardsmigration , it should be said that immigration to western European s ta tes ,taken t o g e t h e r , is presently bigger than immigration to North America(R e f u g e e s, 1 9 9 0) . Fac tua l l y speak ing , Europe has b e e n th e l ead ingimmigration area since the 1970s. A t the same time to tal unemploymen t inEurope runs a t a level o f some 20 million , and currently nearly 20% o f allforeign workers are unemployed .
As regards displaced people , in Afr ica an estimated 35 million live
ou t s i de their own count ry . In Ce n t ra l America , a part from officialrefugees , there is a total number o f around tw o million people displaced .According to some estimates , people fleeing from environmental degradationnow make up the largest class o f displaced people in the world , and theycould be in excess o f 10 million people worldwide . The degradation o fagricultura l and especially is currently displacing more people than any
-
7/28/2019 Mental Health and Psychosocial Problems
5/28
other form o f environmental degradation . Otherepidemiologieal estimates ,
obtained on the basis of the data collected bythe U.S . Off ice o f Foreign
Disaster Assistance (Agency for International Development , 1989) concerningthe major disasters which occurred worldwide
from 1900 up to 1988 , indicate
that , in these 9 decades , some 47 mion people became homeless because ofnatural disasters ; the large m ajority o f them were subsequently
displaced .
As for refugees , the displaced victims o f naturaldisasters are mainly made
up o f people living in the poorest countries andbelonging to the lowest
socioeconomic classes : as stated in the U.N.D.R.O . Manualon "
Disaster
Prevention and Mitigation " (1986) , "The smallestand poores t countries are
a f f e c t e d m o s t severely by natural disasters , and the poores t and mostdisadvantaged members o f a disaster a f fec ted community are likely to
experience the most serious consequences " .In general terms , the current refugee problem can be considered a
typical twentieth - century problem : it has been estimatedthat up to 140
million people have been forcibly uprooted in this century (Figure 14 )
(Harrel - Bond , 1988) .An important new characteristic o f the current
refugee situation to be
considered is that while in the past refugee emergenciestended to occur one
at a time , now refugee emergencies are occuringsimultaneously , on widely
scat tered fronts and often without warning .In terms o f sociodemographic characteristics o f the
refugee population ,
it is important to remember that half o f theworld refugee population is
made up o f children (Refugees , 1988) ; nearlyquarter o f a million o f them
suffer from acute malnutrition . Nearly 8 mionrefugees living in camps
and settlements now depend almost entirely onfood aid . Mortality rates in
-
7/28/2019 Mental Health and Psychosocial Problems
6/28
these populations during the acute phase o f displacement has been extremelyhigh , up to 60 times the expected rates (Toole & Waldman , 1990) . Displacedpopulations in Northern Ethiopia and southern Sudan have suggered thehighest mortality ra tes .
2 . MENTAL HEALTH AMD PSYCHOSOCIAL NEEDS OF REFUGEESThese f i gu res underscore the importance o f the overall phenomenon
currently represented by refugees and displaced populations ; however , until' recently , the mental health and psychosociai needs o f these people had been
neglected area o f investigation and act ion. It was felt tha t the basicneeds o f these populations were to be me t essentially in terms o f providingsh e l t e r , f o o d, sanitation and immunization aga ins t epidemics ; theirpsychosociai needs were seen as something too secondary to a t t rac t theattention o f relief agencies and relief workers . But over the last few years
different trend has become visible , and there is now wide recognition o fthe f ac t that refugees and displaced people represent populations at risk o fsuffering from various psychological s t ress- re la ted disorders ( (Miserez ,1987 ; W illiam s & Wes termeyer , 1986) .
The mental health needs o f refugees r e f l e c t the problems o f uprootedpersons and the traumatic experiences encountered during their refugee -
seeking course . As a minimu m they include the following : 1) the e f f e c t so f conditions causing the person to f lee from his or her homeland ; 2)vicissitudes during flight ; 3 ) adjustment in the country o f first asylum ;and 4 ) problems arising in the land of resettlement which could indeed meanrepatriation . If unre leved, psychological problems occurring in one phaseaccumulate with those that emerge in subsequent phases .
-
7/28/2019 Mental Health and Psychosocial Problems
7/28
As regards the process o f fleeing one 's own country , it can be said
that when people are violently uprooted , placed in a alien and overcrowdedenvironment , or removed from the basic activities that give meaning andpurpose to their lives , there will inevitably develop psychological andadaptational problems . For example , those refugees who have made a last-minute decision to flee often exhibit gu , or conversely a feeling o finvulnerability and aggression . The guilt derives from the l oss o f loved
ones who might have survived had the decision to flee been made earlier .
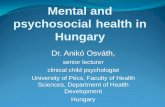
Camp e x p e r i e n c e, when it o c c u r s , becomes the next stage o f thetraumatic adjustment which the refugee undergoes upon arrival in the countryo f asylum , and it enahances the development o f dependency attitudes . Thecamp r e f u g e e can b e seen as someone facing a pas t world o f l oss , an
uncertain future , and a present sense o f being controlled (Figure 15 ) . The
main psychological consequences are the inability to make predictions , and a
sense o f incompe tence . Psychosocial adaptation in the host country becomesmore o r l e s s difficult depending on f a c to r s pertaining to the refugee
himself , to his country o f origin , and to those in the host community . As tothe first , the very process o f exile engenders in the refugee feelings o fgrief , bereavement , anxiety and fears , which have to be dealt with before asat i s fac to ry adjustment can be made . In the refugee situat ion one ob jec tloss becomes complicated by other l osses, and the result is a multiplebereavement which easily assumes pathological characteristics (Kohn & Levav ,1990) .
Where torture has been experienced , the psychological scars are deeper
and require treatment (Goldfield e t al . , 1988 ; Mollica e t al ., 1987) . In thehost or resettlement country , problems of accommodation , unemployment , and
-
7/28/2019 Mental Health and Psychosocial Problems
8/28
isolation f rom cultural and ethnic groups , as well as the degree o frejection within the local communities , and the length o f stay in camps insome countries , all a f fec t the refugee 's ability to integrate and to engagein meaningful activities and interpersonal relationships . Roles and statuschanges of ten occur in the country o f exile causing marital and familyproblems . Moreover , fo r many refugees camp life means a change from a ruralto an urban life- style, with related adaptationai problems . Where thecountry o f origin is characterized by large cultural dif ferences with thehost country , s t ress reactions are more severe . Therefore cultural factorsneed to be taken into account in counseling and in providing mental healthservices .
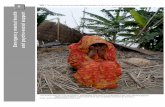
In Figure 16 the most common psychological disorders to be found amongcamp refugees are shown. These include depression and anxiety ; moreover , thespeci f ic features o f the severe s t r e sse s suf fe red by many refugees - such as
starvation , deprivation , witnessing killings or torture , physical injuriesand loss o f significant others - are likely t o produce a high number o fp o s t - traumatic s t r e s s disorders , Somatization disorders are very common aspeople in developing countries of ten express psychological i -health insomatic rather than in psychological terms (Goldberg & Bridges , 1988) . Thishas been confirmed by WHO collaborative studies carried out in differentdeveloping countr ies (Harding e t al. 1980) . Neurasthenia , which is adiagnostic category included in the ICD- lOth Edition, is another disorderparticularly f requent among some r e f u g e e populations , such as Asianpopulations .
Y et , despite the magnitude o f the problem , we do not know much aboutthe percentage o f refugees suffering from speci f ic psychological disorders
-
7/28/2019 Mental Health and Psychosocial Problems
9/28
such as PTSD. The few existing studies havebeen carried out among refugees
lving in resettlement countries (Barudy , 1989; Beiser & Fleming , 1986 ;
Beiser e t al . , 1989 ; Berry & Blondell , 1982;Boehnlein , 1987 ; Kroll e t al .,
1989 ; Krupinsky e t al . , 1973 ; Ln e t a . , 1979 ;Ngyen 1982; Westermeyer ,
1985 , 1987 , 1988) , and their findings arehardly generalizable to refugees
living in crowded camps , often in staggeringlypoor conditions (de Girolamo
e t al . , 1989; Mollica Sc Jalbert , 1989; Urrutia ,1987) . Refugees fled to a
reset t lement country may represent anexceptionally healthy population ,
self - s e l e c t e d for the same f a c t o f havingbeing able to flee to a
resettlement country . Nor do we know about thenatural history and outcome
o f these disorders when they are untreated, and how the cultural norms and
beliefs o f the refugee populations couldhave a moderating e f f e c t on them .
Finally , it should be noted that therate of refugees attending PHC
centres and showing various degrees ofpsychological distress is often very
high : even if we do not have reliable data fromspecific surveys carried out
in refugee camps , we can take note that in amajor WHO collaborative study ,
carried out in PHC facilities in very poor areasin 4 developing countries ,
rate ranging from 1% up to 18% of attenderswere found to be suffering
f r om a significant psychiatric disorder(Harding e t a . , 1980) . If we
consider the exceptional st ress which them ajority o f refugees have endured ,
we can easily conclude that this percentagewill certainly be higher .
3 . MENTAL HEALTH PREVEKTIOH AND CAKE OF REFUGEES :WHO PROGRAMMES AND PRIORITIES
WHO has always been deeply involvedin providing health care fo r
refugees through the Emergency PreparednessProgramme , and is increasingly
-
7/28/2019 Mental Health and Psychosocial Problems
10/28
i nvo lved now t h r o u g h th e newly established Relief Programme . The maina c t i v i t i e s have t o do w i t h technical advice and support to other UNa g e n c i e s , such a s UNHCR ; w i t h making h e a l t h a s s e s s m e n t s of refugeesi tuat ions and providing sp ec i f i c recommendations in order to improve theheal th s ta tus of these populations ; and f ina l ly with monitoring th e mostimportant hea lth indicators of the refugee populations (WHO , 1987 , 1989a ,1989b , 1989c , 1989d) .
In view of the recognit ion of th e importance of th e mental heal th and
psychosocial needs of re fugees , WHO has become more and more involved inthese issues as we l l . A number o f p r o j e c t s a re underway : f o r instance , WHOhas been asked by UNBRO t o make an assessment of th e mental heal th andpsychosocial problems of Khmer displaced people l iving in border encampmentson the Thai -Kampuchean border , and to make recommendations f o r improving th es i t u a t i o n o f these popula t ions (de Girolamo e t al . , 1989 ) ; two missions havetaken place to chat area . Another p r o j e c t has been i n i t i a t e d jo in t ly withth e Rel ie f Programme f o r all disabled Afghan refugees and displaced people ,and a mission has recent ly taken place both in Pakistan r e fugee camps and inAfghanis tan < E1 Fawal , 1990) ; another mission was organized to look a t them e n t a l h e a l t h n e e d s o f Namib i an p o p u l a t i o n s s h o r t l y b e f o r e t h e i rindependence (Aboo -Baker & Chikara , 1990) .
Specific programmes can play a very important role in the prevention ofmental heal th and psychosocial problems among re fugee populations . Theseprogrammes should address in the f i r s t place high - r i s k , vulnerable groups ,such as children , women , elder ly and physical ly handicapped . The exist ings o c i a l n e t w o r k , su c h as s c h o o l s , communi ty o r g a n i z a t i o n s, religiousorganizations , self -help groups can play a crucia l role in this respect .
-
7/28/2019 Mental Health and Psychosocial Problems
11/28
Fundamenta l is the organization of work and activity programmes , becausenothing restores self -confidence and worth more than daily efforts at someuseful work or activity .Mental health care should be fuly integrated into the existing networkof general health care , and should not function as a separate system . Thereare a number of reasons for this :1) in developing countries , and in the refugee camps located there , theresources devo ted to mental health are often inadequa te to meet even theroutine needs ; the primary health care system is the first and often theonly health network available for socioeconomically deprived individuals ;2) Many potential users do not come to a facility which is openlylabeled as a mental health service , since they do not see themselves aspeople needing speciali zed help but consider themselves only as victims ofextreme adversity .
3) As s ta ted above , the m ajority of people in developing countries tendto e x p r e s s psychological distress in -somatic terms , and therefore thep r i m a r y health c a r e worker represents the crucial locus for theintervention . Moreover , it is well known that the large majority of cases ofpsychological distress among attenders of health centres go unrecognized , donot receive a proper care and represent an important burden for the heal thservices . Better and prompt recognition and management of these disorders ,including PTSD, can improve their outcome and reduce the burden on thehealth services .4) Finay , the primary health care network , thanks to its centralposition in the community , can guarantee proper follow -up of victims andheir families for as long as they need.
-
7/28/2019 Mental Health and Psychosocial Problems
12/28
Therefore , the training ofprimary health care workers
to give
treatment to people attendinghealth centres and showing
emotional distress deservesmaximum priority (Lima , 1986;
Lima e t al . ,
1989 ); such tranng represents one of theman preparedness activities
. The
training of health workersshould include basic
knowledge o f the
.psychological featuresassociated with the condition
o f being a refugee;
basic knowledge o f themost common psychological
and stress - related
disorders to be found amongrefugee populations ;
understanding and knowledge
of how to deal with themain psychosocial needs of
these populations ; and
dissemination o f simple and ef fective skillsto be used for the
recognition
and treatment of psychologicallydistressed refugees (interviewing
skis ,
counselling, brief and simplepsychotherapeut ic methods , t a rge ted
pharmaco therapy , group therapy , etc . ) .The training of local health
workers in dealing with psychosocial
problems related to thecondition of being a refugee
must be mandatory even
for socio -cultural reasons , as it isvery important that
assessment be
carried out by personnelwho are acceptable to
refugees (in terms of
language , religion , ethnici ty ,sex , etc . ) . Ths training
can also be an
important tool in fostering autonomyand self - reliance (List ,
1987 ; Simmonds
et a . , 1985) .
The traini .Tl Of healthworkers in mental health seems
to be effective
and long- lasting . I thecontext of a WHO collaborative
Study 111 SIX
developing coun tries , above mentioned, general health workers were
assessed
18 months after trainingaimed at improving their
knowledge , attitudes ,
sks and capacity o f managementin mental health care ; it was
shown that
the improvement was stvisible and was o f equa
magnitude in a
-
7/28/2019 Mental Health and Psychosocial Problems
13/28
countries (Ignacio e t a ., 1989) .In this framework , the role o f the specialized mental health teamshould essentially be one o f supervision and training , and only especially
difficult cases should be referred for direct treatment .While an adequate intervention fo r refugees
who have been victims of
violence is important , it should be borne in mindthe danger o f labelng
al victims as i for the possible induction o f a sick role (Harding , 1981)
and the "creation o f a stigmatizing 'victim status ' "(Hueting , 1986) .
Attent ion should also be paid to the mental healthneeds o f the care
givers themselves , who are faced with heavy demandsand who are themselves
exposed to a substantial risk o f stress - related disorders .As for service planning , it must be
remembered that services should be
provided on the basis o f the actual needsrather than on the basis o f the
demand o f the population : this applies both to the timing and magnitude o f
the interventions (Ross & Quarantelli , 1976) .Because o f the crucial importance o f the training
fo r health workers ,
WHO is preparing together with the HighCommissioner for Refugees a training
manual fo r relief workers dealing with refugeesfo r the identification and
management o f most common psychological andpsychosocial problems to be
encountered among refugees and displaced populations .
4 . CONCUJSIOHS iRefugees have generally been seen as a burden
for host communities and
as a threat for soc ie t ies . On thecontrary they can be an essential
component o f important development programmesin poor areas ; they can foster
the capacity o f the h o s t community to respond to difficult local
-
7/28/2019 Mental Health and Psychosocial Problems
14/28
circumstances , and they can also represent also a challenge for WHO , NGOsand various clinicians who have to meet the complex needs o f these specialpopulation groups , and have to plan and implement specific programmes in thearea o f mental health .
-
7/28/2019 Mental Health and Psychosocial Problems
15/28
ReferencesAboo - Baker , F. & Chikara , F. (1990) .
Report o f a mission on mental healthservices in Namibia .Geneva: World Health Organization .
Agency f o r InternationalDevelopment (1989 ) . D is a s te r History:
Significant D a t a on M a j o r D i s a s t e r sWorldwide . 1900 - Presen t .
Washington , DC: Off ice o f U.S . ForeignDisaster Assistance , Agency for
International Development .
Barudy , J . (1989) , A progra mme o fmental health for political refugees :
dealing with the invisible pain o fpolitical exile . Social Science and
Medicine . 28 :715 - 727 .Beiser , M. & Fleming , J .A .E. (1986).
Measuring psychiatric disorder among
Southeast Asianrefugees . Psychological Medicine . 16 :627 - 639 .
Beiser , M, Turner , R.J . & Ganesan ,S . (1989) . Catastrophic stress and
f a c t o r s af fecting its consequences amongSoutheast Asian refugees .
Social Science and Medicine . 28 :183 - 195 .Berry , J .W . & Blodell , T . (1982)
Psychological adaptation o f Vietnamese
refugees in Canada . Canadian Journal o fMental Health . 1:81- 88 .
Boehnlein , J .K . (1987) . Clinicalrelevance of grief and mourning
amongCambodian refugees . Social Science and Medicine . 25 :765- 772 .
de Girolamo , G, , Diekstra ,.R. & Williams , C . (1989
) . Report o f a visit to
border encampments on the Kampuchea -Thailand border . Geneva : WorldHealth Organization : MNH/PSF/90 .1.
El Fawal, K . (1990 ) . Mental healthprogramme for Afghanistan and for
Afghan
r e fuge e s in Pakistan . R e p o r t o f amission . Geneva : World Health
Organization .
Goldberg , D. & Bridges , K. (1988) .Somatic presentation o f psychiatric
illness in primary care settings . Journalo f Psychosomatic Research.
32 -.137 - U4.Goldfield , A .E. , Mollica , R.F . , Pesavento
, B.H. & Faraone , S .V . (1988) .
The physical and psychological sequelaeo f torture : Symptoma tology and
diagnosis . JAMA . 259 :2725 - 2729 .Harding , T . (1981) . Summary and recommendations
. In : Helping Victims o fViolence . Proceedings o f a WHO Working Group on the PsychosocialConsequences o f Violence . The Hague , 6 - 10
April 1981, pp . 160 - 170 .
Harding , T ., De Arango , M.V . , Baltazar , J .,Climent , C .E . , Ibrahim , H.H.A . ,
Ladrigo - Ignacio , L., Murthy , R .S . &Wig , N.N. (1980) . Mental disorders
in primary healh care : a study of theirfrequency and diagnosis in four
developing countries . Psychological Medicine . 10:231- 241.
-
7/28/2019 Mental Health and Psychosocial Problems
16/28
Harrel -Bond , B . (1988) . The non -material needs o f refugees . In : Medicine andMigration. Proceedings o f the 1st International Conference . Rome , 9 - 10April 1988 , pp . 42 - 52 .
Hueting , J . ( 1981) . Psychosocial mechanisms o f short - term and long - termreactions to violence . In : Helping Victims o f Violence . Proceedingso f a WHO Working Group on the Psvchosocial Consequences o f Violence .The Hague , 6 - 10 April 1981, pp . 13 - 19 .
Ignacio , L .L . , De Arango , M.V . , Baltazar , J . , D'Arrigo Busnello , E.,Climent , C .E . , Elkahim , A . , Giel , R . , Harding , T .W . , Ten Horn ,G .H.M.M. , Ibrahim , H.H.A . , Srinivasa Murthy , R. & Wig , N.N. (1989) .Knowledge and attitudes o f primary health care personnel concerningmental health problems in developing countries : A follow -up study .International Journal o f Epidemiology . 18 :669 - 673 .
Kohn , R. & Levav , I ( 1990) . Bereavement in disaster : an overview o f theresearch. International Journal o f Mental Health. 19 :61- 7 6 .
Krol l , J . , Habenicht , M . , Mackenzie , T . , Yang , M . , Chan , S . , Nguyen , T . ,Ly , M. . , Phommasouvanh , B . , Nguyen , H . , Vang , Y . , Souvannasoth , L . &Cabugao , R . ( 1989) . Depression and pos t t raumat ic s t r e s s disorders inSoutheas t Asian re fugees . American Journal o f Psyc h i a t ry . 146 :1592-1597.
Krupinsky , J . , Stoller , A . & Wallace , L . ( 1973) . Psychiatric disorders inE as t European refugees now in Australia . Soc ia l Science and Medicine .7 :31- 49 .
Lima , B.R. ( 1986) . P rimary mental health care for disaster victims indeveloping countries . Disas ters. 10 :203 - 204 .Lima . B .R . , Chavez , H . , Samaniego , N. , Pompei , M .S . , Pai , S . , Santacruz , H.
Lozano , J . ( 1989a) . Disaster sever i ty and emotional disturbance :Implications fo r primary mental health care in developing countries ,Ada Psychiatr ica Scandinavica . 79 :74 - 82 .
L in , K .M . , Tazuma L . & Masuda , M . ( 1 97 9) . Adap ta t i o n a l problems i nVietnamese re fugees : I . Health and mental hea l th s t a t u s . Archives ofGeneral Psychiatry . 36 :955 - 961 .List , A .L . (1988) . Great expectations : the retraining o f refugee health carepersonnel . M igration World . 14 :31- 34 .
Miserez (Ed . ) (1988) . Refugees : The Trauma o f Exile . Published on behalf o fthe League o f Red C r o s s and Red C r e s c e n t Societ ies by Nijhoff :Dordrecht .Mollica , R. & Jalbert , R.R. ( 1989) . Community or confinement : mental healthcrisis in S i te Two (Evacuation camp on the Thai - Kampuchean border ) .
Washington : World Federation fo r Mental Health .
-
7/28/2019 Mental Health and Psychosocial Problems
17/28
Mollica , R.F . , Wyshak , G. & Lavelle , J. (1987 ) . The psychosocial impact
of
war trauma and torture on SoutheastAsian refugees . American Journal o f
Psychiatr y . 144 :1567 - 1572.Nguyen , S .D . (1982). The psychological adjustment
and the mental health
needs of Southeast asianre fugees . Psychiatric Journal o f the
University o f Ottawa . 7 :26 - 35 .Refugees (1988) . Refugee children , 70 , 6 .
Refugees (1989 ) . Towards 1990 :efugees around the world , 71, 12 .
Refugees (1990) . Europe in flux , 72 , 5 .
R i c c a, S . (1 9 8 9) . Internationalmigration in Africa: legal and
administrative aspects . Geneva: Interna tional Labour Office .
Ross , G .A . & Quarantelli , E .L,(1976 ) . Delivery o f mental
health services
in disasters : The Xenia tornadoand some implications . In : The Ohio
S t a t e University : The DisasterResearch Center Book and Monograph
Series .
Simmonds , S ., Cutts , F . 6c Dick , B.(1985) . Training refugees as
primary
health care workers : Past imperfect ,future conditional . Disasters .
9 :61- 68 .Toole , M.J . & Waldman , R.J . (1990) .
Prevention o f excess mortality in
re fugee and displacedpopulations in developing countries .
JAMA .
263:3296- 3302.U.N.D.R.O . (1986) . Disaster
Prevention and Mitigation Manual.Geneva ; United
Nations Disaster Relief Operations .
Urrutia , G . (1987) . Mental healthproblems o f encamped refugees .
Bulletin o f
the Menninger Clnic . 51:170 - 185 .Westermeyer , J . (1985) . Mental health
o f south e a s t Asian refugees .
observations over two decades fromLaos and the United States .
In :
Cowan, T .C . (Ed , ) . Sout eas t asianmental health : Treatment . Prevention .
Services . Training and Research. Washington : NIMH , pp . 65 - 69 ,Westermeyer , J . (1987 ) . Prevention o f
psychiatric disorders among Hmong
refugees in the United States : Lessonsfrom the period 1976- 1985 .
Social Science and Medicine . 25 :941947 . .Wescermeyer , J . (1988) . DSM-I psychiatric
disorders among Hmong refugees
in the United States . American Journalo f Psychiatry . 145 :197 - 202 .
Williams , C .L. & Westermeyer , J . (eds . ) (1986) . Refugee Mental
Health in
Resettlement Countries . Washington ; Hemisphere .World Health
Organization (1987). Eight GeneralProgramme o f Work , covering
-
7/28/2019 Mental Health and Psychosocial Problems
18/28
the period 1990- 1995 . Geneva : World Health Organization .World Health Organization (1989a) . Emergency preparedness and response :Annual report 1988 . Geneva : PC O/EPR/ 89 .3 .World Health Organization (1989b) . Emergency preparedness and response :
Programme 1989 - 1991. Geneva : PCO/EPR/ 89 .5 .World Healh Organization (1989c) . Emergency preparedness and response :Consultative meetings fo r programme development 1986- 1989 . Geneva :PCO/EPR/89 .7 .Wor ld Heal th Organization ( 1 9 8 9 d) . WHO a c t i o n in emergenc ies anddisasters : WHO Manual revision. Geneva : PCO/EPR/ 89 .6 .
-
7/28/2019 Mental Health and Psychosocial Problems
19/28
Figure 1 Changes in world refugeepopulations over time (1970-90),8 -1' _ 15_^\ / A f14 412 ! 8.2^\ ^^^^^^^^^^^^^^^^^^^^^^^
1970
1980 CZ3 1990
Source:UNHCR
-
7/28/2019 Mental Health and Psychosocial Problems
20/28
Figure 3
World Refugee Population By Continentas of 31 December 1989 (X 1.000)
6 .773_ ^ ^ ^ ,_ i 4 .587^^^^^^^^^\
-
7/28/2019 Mental Health and Psychosocial Problems
21/28
Tr-.n Thailand and Malaysia )
^K'BS'S^SST 7 !?^ W^^ '^f l i ^
-
7/28/2019 Mental Health and Psychosocial Problems
22/28
Figure 6 Countries hosting the largest refugee population in Africa (omalia, Sudan , Ethiopia , Malawi and Zaire)
-
7/28/2019 Mental Health and Psychosocial Problems
23/28
Figure 9 Countries hosting the largest refugee population in Central America (Costa Rica , Honduras and Guatemala )
fttBJBHJ.j-s..Mtaa~tai S&B-i3"-r-aSi.yB*.BBi5 S J-J-i J - -. - .^,... . . . . i
-
7/28/2019 Mental Health and Psychosocial Problems
24/28
Figure 13
Europe some 20 mion immigrants
5% from developing countries
I 1989 more than 3 mion arrivalsom Eastern countriesIn Central America 2 mion
people
-
7/28/2019 Mental Health and Psychosocial Problems
25/28
Figure 14
In this century up to 140 mionforcibly uprootedBetween 1900 -1988 47 mion becomebecause of natural disastersHalf of the world refugee population
made up by children and adolescents14 of a mion suffer from acutemalnutritionIn Africa 35 mion live outside their
own country
-
7/28/2019 Mental Health and Psychosocial Problems
26/28
Figure 15
PSYCHOLOGICAL FEATURES OFREFUGEE LIFE IN CAMPSPast -world of lossFuture uncertain lifePresent sense of being controlledInability to make predictions andsense of inco mpetence
Loss of self -respect and trust in othersD e v e l o p m e n t o f a 'dependency
syndrome '
-
7/28/2019 Mental Health and Psychosocial Problems
27/28
Figure 16
ost common psychological disorderso be found amongrefugees in camps
DepressionAnxietyPosttraumatic stress disordersSomatization disordersNeurastheniaIn a major WHO study carried out in 4developing countries , 11 -18% of primarycare attenders w er e ' suffering from apsychiatric disorder
-
7/28/2019 Mental Health and Psychosocial Problems
28/28
Figure 16
Mental health care fully integratedthe existing network of generalcare because of:a) shortage of resourcesb) somatic presentation ofsymptomsc ) reluctance to use 'mentalhealth services 'd) proper follow -up by the PHCnetwork
Training of PHC workers deservespriorityDevelopment o f a WHO /UNHCRManual in mental health forworkers