Family Caregivers of Older Adults: NASW Standards for Social Work Practice
Mental Disorders,
Older Adults and Caregivers
Presented by:
Kate Mattias, MPH, JD Executive Director, NAMI Connecticut
Paloma Bayona Program Director, NAMI Connecticut
What Is NAMI?
National Alliance on
Mental Illness – Connecticut
NAMI’s Mission
Support,
education
& advocacy, for people living
with mental illnesses, their
family, friends, professionals
and the public

Audiences We Serve People living with mental illness
Family members/friends of loved ones
with mental illness adults & children
Policy makers and other community
stakeholders
Estimated that one
in five families are
impacted by serious
mental Illness each
year
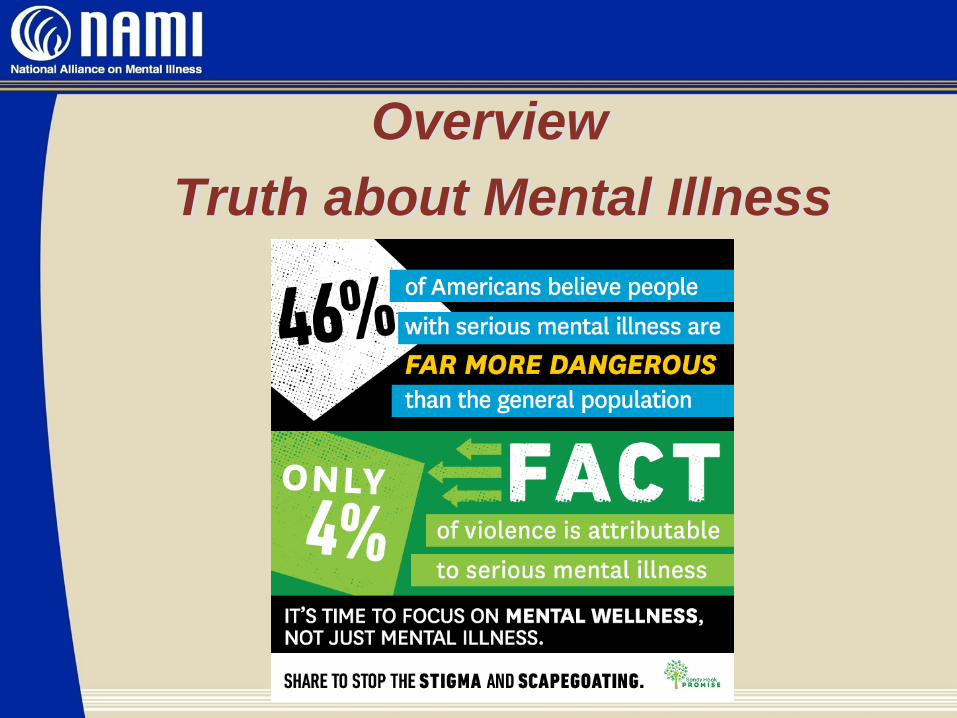
Overview
Truth about Mental Illness
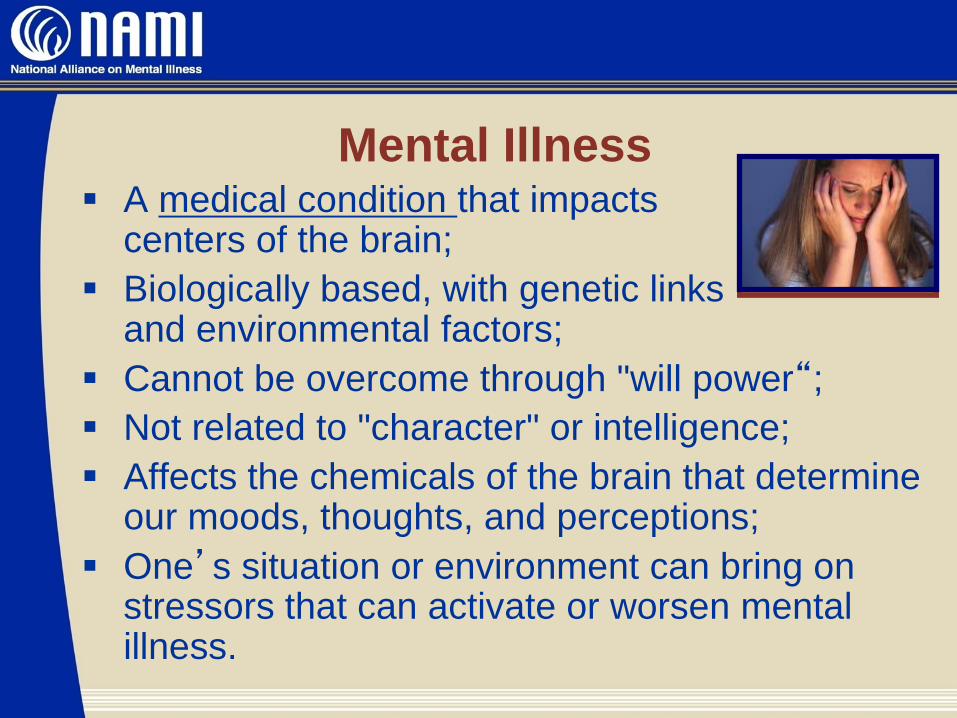
Mental Illness A medical condition that impacts
centers of the brain;
Biologically based, with genetic links and environmental factors;
Cannot be overcome through "will power“;
Not related to "character" or intelligence;
Affects the chemicals of the brain that determine our moods, thoughts, and perceptions;
One’s situation or environment can bring on stressors that can activate or worsen mental illness.
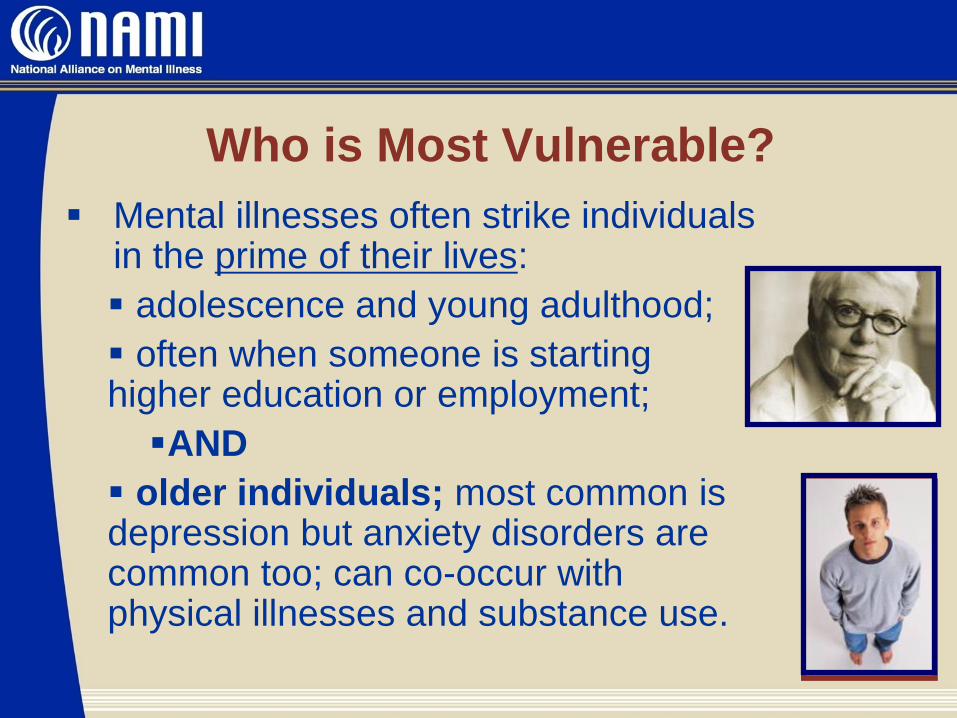
Who is Most Vulnerable?
Mental illnesses often strike individuals in the prime of their lives:
adolescence and young adulthood;
often when someone is starting higher education or employment;
AND
older individuals; most common is depression but anxiety disorders are common too; can co-occur with physical illnesses and substance use.
Diagnosing
Mental
Illnesses
Mood Disorders
Anxiety Disorders
Thought Disorders: Schizophrenia
General Categories of
Serious Mental Illness
Diagnosing Mental Illnesses No blood test
No brain scan
No “typical” behaviors or signs
No universal medication(s)
Providers have to go on:
The behavior(s) being exhibited
The person’s mood(s)
The person’s thoughts
The length of time the person has
experienced unusual thoughts or behaviors
Where Adults are Diagnosed
Emergency Departments
Rehab Hospitals
Other Health Facilities –
Primary Care Providers
Psychiatric Providers
Family Concerns
Court/Law Enforcement
Why Some Older Adults
Don’t Ask for Assistance
Stigma in seeking help
Not high on list of medical priorities
Concern over loss of independence or control over their life
Fear of being placed in a nursing home or on a “mental health” floor
Don’t want to be a burden
Fear cost of services and medications
Fear they may be exploited financially

Caregivers – Who Are They?
Caregivers – Who Are They?* • 8.4M provide care to adult with an emotional health issue;
• In their role an average of 8.7 years (4 yrs average for any
other kind of condition);
• 33% have been providing care for 10 or more years;
• Loved one typically has serious mental health issues;
typically bipolar disorder, schizophrenia or depression;
• Nearly all help with Instrumental Activities of Daily Living –
transportation, meals, shopping, arranging services;
• Average 31.8 hrs a week assisting loved one (typical
caregiver averages 24.4);
• 20% provide care to someone older than 65
• *(On Pins and Needles: Caregivers of Adults with Mental Illness; National Alliance for Caregiving; 2016)
Caregivers – Who Are They?* • One in seven care for a parent;
• 11% care for a spouse;
• 9% assist with a sibling;
• 45% say their loved one lives with them; 25% are within 20
minutes;
• 51% caring for a male;
• Average caregiver age 54.3 years of age;
• 82% of care recipients take prescription medication; 25% of
caregivers feel the condition not well managed by the
medication;
• 33% caregivers indicate difficulty in getting their loved one
to take prescribed medication • *(On Pins and Needles: Caregivers of Adults with Mental Illness; National Alliance on Caregiving; 2016)
• *(On Pins and Needles: Caregivers of Adults with Mental Illness; National Alliance for Caregiving; 2016)
Caregivers* • 80% help loved one manage finances or paperwork;
• 50% indicate their loved one is financially dependent upon
family or friends;
• 33% have some kind of legal responsibility – power of
attorney, guardianship;
• 40% have had any kind of mental health caregiver
training;
• 53% indicate they need help with own emotional and
physical stress (vs 40% for caregivers of adults without
mental health issues);
* (On Pins and Needles: Caregivers of Adults with Mental Illness; National Alliance on Caregiving; 2016)
Caregivers* • 30% would like a “care navigator” to
assist with accessing appropriate
services and supports;
• Services difficult to find;
• Most are employed;
• Stigma isolates caregivers
* (On Pins and Needles:
Caregivers of Adults with Mental Illness;
National Alliance on Caregiving; 2016)
Burnout – What it Looks Like • Poor sleeping habits;
• Abandoning leisure activities caregiver used to enjoy;
• Losing touch with close friend or family;
• Irritability, including towards the care recipient;
• Lack of energy for regular activities: cleaning, cooking, etc.
• Difficulty concentrating;
• Use of alcohol or drugs to relax;
• Headaches, body aches;
• Sense that no one cares for the caregiver;
• Sense of hopelessness for the future;
• Depression, anxiety
Issues Caregiver’s Face • Co-occurring disorders, both physical and
mental/substance use;
• Difficulty getting an accurate diagnosis;
• Appropriate medication; medication compliance;
• Lack of information and support;
• Personal health and mental health concerns;
• Personal Employment – most are employed
• Stigma;
• Isolation;
• Fractured healthcare system;
• Too few geriatric mental health providers and support
services
Caring for the Caregiver Taking care of yourself. Scheduling (and keeping!) doctors’
appointments. Asking for help. Taking a break. These are vital steps
caregivers can take to stay healthy.
Self-Care
• Important to acknowledge that stress is a normal,
sometimes difficult but definitely manageable,
part of caregiving. Stress can manifest itself
in both a physical and emotional way;
it is vital to find an outlet to relieve it!
• Caregiver may need to give him/herself
permission to take care of themselves.
That is fine, and good, and necessary!
Caring for the Caregiver Self-care/stress management can be achieved in many ways:
• General attention to daily activities like healthy eating,
exercising, sleeping, and talking with friends, is vital. Even for
the busiest of caregivers, mini-breaks can be lifesavers.
• Go to a quiet room or step outdoors and just breathe for ten
minutes; clear the mind and focus only on the breath.
• Write in a journal. Say a positive affirmation.
• Light a candle.
• Listen to music.
• Call a good friend.
• You might consider attending a support group. Groups of
individuals who share a common experience and provide each
other with various types of help, i.e., information, resources, and
emotional support.
Mental Illnesses and
Older Adults
Mental Illnesses and Older Adults • Dramatic recent and projected growth in population;
Population aged 65 and older will increase from 20
million in 1970 to 69.4 million in 2030;
Major direct and indirect impact on health outcomes,
service use and costs;
We know treatment works, but effective services
are not reaching those in need;
Lack of rehabilitative interventions;
An alarming under-investment in knowledge
dissemination, service development, and research to
meet future need. Source: Dartmouth Psychiatric Research Center
Poor Quality of Care for Older
Persons with Mental Disorders Increased risk for inappropriate medication treatment
(Bartels, et al., 1997, 2002)
> 1 in 5 older (20%) persons given an
inappropriate prescription (Zhan, 2001)
Research shows older adults are
getting medication but inconsistent
follow up by providers (Psychiatric News; Jan. 2013)
Less likely to get psychotherapy services;(Bartels, et al., 1997)
Lower quality of general health care
and associated increased mortality(Druss, 2001)
Mental Disorders in Older Adults:
The Silent Epidemic Alzheimer’s and other memory disorders (30-
40% co-occurring depression or psychosis);
Most common: depression, anxiety disorders,
severe mental illness, alcohol abuse;
Often overlooked by community
providers and clinicians;
Majority of individuals over age 65
who commit suicide saw primary
care provider the week before.
Dimensions of the Challenge
Less than 3% of older adults
receive outpatient mental health
treatment by specialty mental health
providers; (Olfson et al, 1996).
Only 1/3 of older persons who live
in the community and who need
mental health services receive
them. (Shapiro et al, 1986).
Older adults with mental illness on
target to reach 15 million in 2030. (Jeste, et al., 1999; www.census.gov)
Dimensions of the Challenge
Community Mental Health Services Under-serve older persons
Lack staff trained to address needs of
older adults
Often lack age-appropriate services
Principal Providers: Primary Care and Long-term Care –
insufficient depth of knowledge about
mental illness;
False belief that MH Services are not
covered by Medicare.
Late Life Depression
Co-Existing Medical Conditions
About 25% of people who have heart
attacks suffer from depression post event;
20 – 50% of people who have a stroke will
develop depression within one year;
In one study, elderly people who were
depressed were 4x as likely to die within
four months of a heart attack than those
without depression. Abebaw Mengistu Yohannes, PhD and
Robert C. Baldwin, MD ; Medical Comorbidities in Late-Life Depression; Dec
1, 2008 Psychiatric Times. Vol. 25 No. 14;
Dementia – About 17% with Alzheimer’s
also have major depression;
Symptoms of depression may
precede development of dementia
or Alzheimer’s;
When depression and cognitive
impairment develop simultaneously,
deficits may be mistaken for dementia or
a problem known as “pseudo-
dementia”; Cognitive function may
improve if depression treated.
Co-Existing Medical Conditions
•
Substance Use
Numbers of Older Adults Impacted
by Depression
1-5 % - who live in the community;
12% - who are hospitalized;
14% - who require health care at home;
29-52% - who live in nursing homes;
39-47% - being treated for cancer, heart attack, or stroke.
Risk Factors for Late Life
Depression Female gender
Widowed or divorced; loss of close
friends or poor family relations;
Chronic & disabling illness;
Lack of social support;
Recently bereaved;
Prior history of depression;
family history of mental illness;
Lack of regular physical activity;
Recent placement in nursing home
Late Life Depression
Clinically significant
depression affects
15-20% of older adults
(2M with clinical
depression; 5M with less
severe condition that
impacts quality of life)
Late life depression
associated with:
– Lower physical
functioning;
– Poorer adaptation to
medical illness;
– Lower quality of life;
– Higher health care costs;
– Dementia and Heart
Disease
– Increased mortality from
suicide and illness.
Depression Symptoms in Older Adults Symptoms different than that of younger person;
An older person more likely to have sleep or eating
problems (insomnia is a risk factor);
Ambien and Lunesta increasingly prescribed for older
individuals instead of Klonopin or Xanax;
Tends to last longer period of time in older adults; may
increase risk for physical health problems or death;
Depression in older adults is more likely to lead to suicide.
Risk of suicide is serious. Elderly white men are at the
greatest risk, and those ages 80-84 have a suicide rate
more than twice that of the general population.
Depression is a predictor of suicide
Depression Symptoms in Older Adults Somatic or physical symptoms more
common than in other age groups, including heart palpitations, restlessness, fatigue, aches and pains, nausea and vomiting, dizziness, tremors, shortness of breath, fainting;
Because physical symptoms are common, many providers overlook or don’t consider screening for depression;
Cognitive problems, including inability to concentrate or remember things;
Mood disturbances, including irritability, anxiety, or preoccupation with death.
Late Life Depression
No one cause; onset of late-life depression can be
attributed to genetic, biological, or neurological factors;
life changes; illnesses; or a combination;
Some older adults with depression have suffered from
the illness for most of their lives and gone undiagnosed;
Depression in late life is more common in women,
widowed individuals, those who lack a supportive social
network, and those with physical health problems;
Important to recognize that the depression is NOT just “ being down” about one’s condition.
Treating Late Life Depression
Only 10 to 40 percent of elderly patients with
depression are prescribed antidepressant
medication;
Underuse or misuse of antidepressants
and prescribing inadequate dosages are
common mistakes physicians make when treating
the elderly with depression;
Treatments believed to be beneficial in late-life
depression include antidepressants, psychotherapy,
electroconvulsive therapy (ECT) and transcranial
magnetic stimulation (TMS); http://www.narsad.org/dc/pdf/facts.latelifedep.pdf
Treating Late Life Depression
More than 20 antidepressants available;
Some antidepressants may not be as
effective for people over age 60 as they
are for younger persons;
Treatment may take longer to work; may
need to take higher doses;
Treating physician needs to know all the
medications someone is taking —
including vitamins, herbal supplements,
alcohol and tobacco, and recreational
drugs — combination of medications can
impact the effectiveness of treatment.
Treating Late Life Depression Support and education important part of depression
treatment for individual and caregivers;
Studies show older patients with depression benefit
most from aggressive, persistent treatment;
therefore, therapy for older patients should be
continued for a sufficient duration; www.narsad.org/dc/pdf/facts.latelifedep.pdf
Psychotherapy can involve just the person or a
whole family;
Cognitive therapy especially helpful with older adults
once depression is under control;
Group therapy – can provide a communal experience
of guidance and education;
What works is what is important
Community Response to Late Life
Mental Illness
Depression Screening Agencies and staff serving home or
facility-bound individuals need to provide
information on late life depression to
clients and family members;
Screening results can provide the
physician/provider with a reason to
discuss depression and/or other mental
illnesses
Depression Screening Community support to reduce stigma;
Primary care, geriatric physicians,
psychologists and psychiatrists use special
assessments, such as the Geriatric Depression
Scale;
Touted as a “best practice” in primary
care settings;
Caregivers and Older Adults may need to ask
that a screening be performed;
Primary Care physicians need to know where
mental health resources are in the community;
Community agencies need to know about
resources.
Evidence-Based Practices
Mental health outreach services – key role
for community agencies and providers
Integrated service delivery in primary care
Mental health consultation and treatment
teams in long-term care
Family/caregiver support and education
interventions
Psychological and pharmacological
treatments Draper, 2000; Unützer, et al., 2001; Schulberg, et al., 2001;
Bartels et al., 2002, 2003; Sorenson, et al., 2002;
Successful Mental Health &
Aging Coalition Education of Primary Care Physicians/Community
Social Service Providers • Educational Seminars
• Brochures on Aging Mental Health Issues
• Community Resources
• Peer Organizations share successful treatment programs
Education of primary caregivers • NAMI’s Family to Family course
• Introduction to easy screening tools to de-mystify process
Public Education • Public Service Announcements
• Speakers Bureau
• Library Focus – National Depression Day; Mental Illness
Awareness Day
• Aging Mental Health Conferences
Resources
NAMI: www.nami.org;
Education Courses for Family Members
Support Groups for Family Members and People
living with Mental Illness
Professional Education
Older Americans Substance Abuse and
Mental Health Technical Assistance Ctr. www.SAMHSA.gov/OlderAdultsTAC
National Institutes of Mental Health (NIMH)
Mental Health Connecticut (MHC)
Questions and Answers
NAMI Connecticut
www.namict.org