Menstrual cycle By Natalie Maltseva. Outline Preparation Ovulation Brief fertility Wait and See.
22
Menstrual cycle By Natalie Maltseva
-
Upload
julian-stafford -
Category
Documents
-
view
219 -
download
1
Transcript of Menstrual cycle By Natalie Maltseva. Outline Preparation Ovulation Brief fertility Wait and See.

Menstrual cycle
By Natalie Maltseva

Outline
PreparationOvulation Brief fertilityWait and See

Main facts:
• Menarche: Beginning of menstrual cycles• Menopause: End of menstrual cycles • Mean blood loss = 40ml (range 30-120ml)• Cycle length= first day of bleeding( LMP) in
one cycle to first day of bleeding in next cycle• Cycle length approx 28 days, (range21-42)

2 parts of the cycle: Ovarian and Menstrual

Phases of menstrual cycle: in the uterus
1. Menstruation
2. Proliferation
3. Secretory
Phases of ovarian cycle: in the ovary
1. Folicular phase – (early, middle, late)
2. Ovulation
3. Luteal


Control and Coordination• PULSATILE SECRETION of GnRH by the hypothalamus – stimulates anterior pituitary
gland
• Gonadotroph hormones secreted by the anterior pituitary: – Luteinising Hormone acts on theca cells androgens– Folicular Stimulating Hormone acts on granulosa cells inhibin and oestrogen
• Oestrogen secreted by the follicles – pay attention to the different effect at low/hgh levels– -ve feedback (at low levels) on hypothalamus, anterior pituitary– +ve feeback (at high levels in the absence of progesterone)
• Progesterone secreted by the follicles – Corpus luteum development– Endometrium etc.
• Inhibin secreted by granulosa cells negatively regulates FSH secretion at the anterior pituitary (This is important – it helps to lower level of FSH whilst LH level will rise – the difference in the levels of LH and FSH are important for Luteal SUrge)


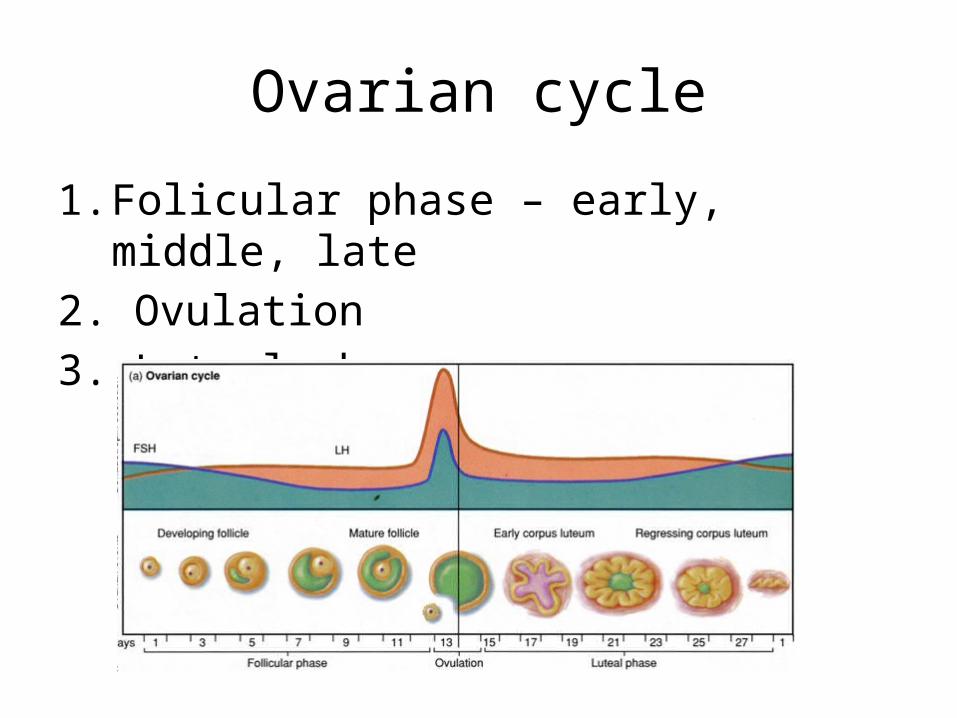
Ovarian cycle
1. Folicular phase – early, middle, late
2. Ovulation
3. Luteal phase

Early Follicular phase• Begins as menstrual shedding starts No corpus luteum present.• Follicles are small
– Very little oestrogen or inhibin hypothalamus and pituitary free from feedback inhibition
• FSH and LH begin to rise FSH more dramatic (because no inhibin present)• FSH binds to granulosa cells, develops follicle to form theca interna.• LH binds to theca cells • Follicles begin to grow• FSH stimulates the granulosa cells
(this produces inhibin and oestrogen)

Mid follicular phase
Oestrogen dominant
• Growing follicles secrete oestrogen and inhibin:– FSH falls rapidly compared to LH because of selective action of inhibin.
• Dominant oestrogen stimulates: – Oviduct motility– Thickening of endometrium– Growth and motility of myometrium– Thin cervical mucous – alkaline– Vaginal secretions– Changes in skin,
hair, calcium metabolism.

End of follicular pre-ovulatory phase
• One follicle becomes dominant• Rising oestrogen levels flip into positive feedback (absence of progesterone) • LH surge stimulates ovulation.
• Ovulation timing can be affected by stress and environment
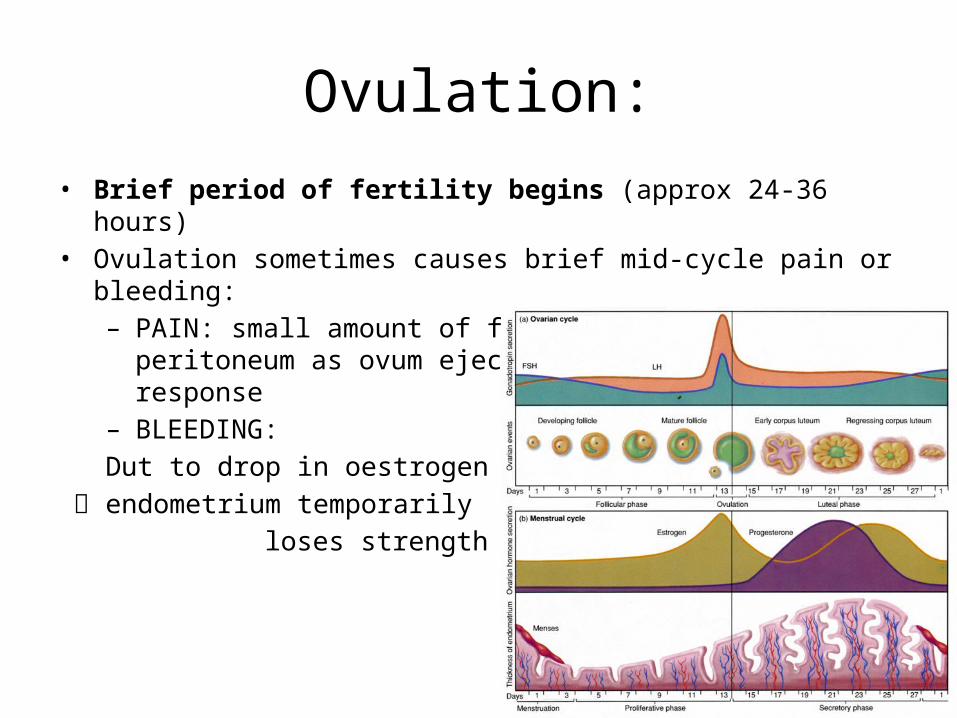
Ovulation:• Brief period of fertility begins (approx 24-36 hours)• Ovulation sometimes causes brief mid-cycle pain or bleeding:
– PAIN: small amount of fluid passes into the peritoneum as ovum ejected = inflammatory response
– BLEEDING:
Dut to drop in oestrogen levels
endometrium temporarily
loses strength

Luteal phase• Disrupted follicle forms corpus luteum rapid rise in progesterone and
also oestrogen levels
• LH, FSH and GnRH remain suppressed, corpus luteum lasts for 14 days.
• Dominant progesterone: – Acts on oestrogen primed cells, • Further thickening
of endometrium into secretory form • Thickening of myometrium • Thick mucus • Changes in breast tissue• Increased body temperature.

Luteal phase 2• Corpus luteum programmed cell death after 14 days. • Steroid levels fall, endometrium begins to shed.• Pituitary and hypothalamus freed from feedback inhibition FSH and LH
start to rise for a new cycle - UNLESS CONCEPTION

IF PREGNANCY IS ANNOUNCED:
• Developing trophoblast and placenta secrete hCG (human chorionic gonadotrophin)
• Preserves the corpus luteum until the placenta takes over at 10-12 weeks.

Endometrium:
• Stimulated by oestrogen….proliferates• Stimulated by oestrogen AND
progesterone……. secretory change• Conceptus arrives and takes control……or• Steroids withdrawn…..flushed away

Menopause:
• Occurs 45-60 years, mean age 51.• Decline in ovarian oestrogen production
increased FSH & LH.• Occurs because degeneration of follicles
(atresia) increases from age 35, fertility wanes from age 37, increased risk of miscarriage.

3 stages of menopause:
• 1. Pre-menopause:– From age 40years – Changes in menstrual cycle follicular phase shortens – Ovulation early or absent– Decreasing oestrogen– LH&FSH rise (FSH more due to inhibin) – Reduced feedback. – Leads to reduced fertility meiotic non disjunction, miscarriage increases
• 2. Menopause: • Cessation of menses. • Average 49-50 but variable. • No follicles to develop oestrogen falls dramatically • FSH rises dramatically as no inhibin.
• 3. Post-menopause:

Symptoms of Menopause:• CLASSIC SYMPTOM TRIAD affects 80%
– Hot flushes– Sweats– Vaginal dryness
• Non-specific symptoms:– Headache– Migraine– Palpitations– Disturbed sleep
• Periods become infrequent (oligomenorrhea) and then cease.• Urogenital symptoms
– Vaginal dryness– Cystitis– Urinary frequency– Incontinence.
• Psychologic symptoms – Loss of concentration– Poor memory– Irritability– Loss of libido– Panic attack.
• Atrophy of connective tissue – Skin thinning, hair loss, brittle nails, aches & pains.
• Osteoporosis – loss of bone matrix (esp vertebral column), loss of height, deformity, fractures.