Mending hearts Inequality and inequity in coronary heart disease Mending hearts Inequality and...
27
Mending hearts Inequality and inequity in coronary heart disease Mending hearts Inequality and inequity in coronary heart disease County Durham & Tees Valley 1993-2003 Michael Fleming Clare Eynon Mark Reilly Leon Green County Durham & Tees Valley Public Health Network
-
Upload
angela-pruiett -
Category
Documents
-
view
225 -
download
0
Transcript of Mending hearts Inequality and inequity in coronary heart disease Mending hearts Inequality and...

Mending heartsInequality and inequity in coronary heart disease
Mendinghearts
Inequality and inequityin coronary heart disease
County Durham & Tees Valley1993-2003
Michael FlemingClare EynonMark ReillyLeon Green
County Durham & Tees ValleyPublic Health Network

Mending heartsBackground
Somecontext
1. Coronary heart disease still presents a large burden of disease in the community
2. A great deal is known about inequalities (variations) in coronary heart disease risk and outcome
3. Much less is known about inequity - the nature of the gap between need and provision
4. Directors of Public Health are required to develop health equity profiles & conduct audits

Mending heartsMain aims
What didwe do?
1. Described the inequalities (variations) in coronary heart disease risk and outcome
2. Measured the size of the inequity (gap between need and provision) within and between places
3. Produced PCT locality profiles of coronary heart disease using the ‘life course’ model
All of this intended to provide evidence as the basis of reducing inequity systematically and effectively

Mending heartsOverview of methods
How didwe do it?Hospital
episodes (HES)
Deaths (PHMF)
Residentpopulation(Census)
ICD10 Disease definitions
1. Coronary heart disease (ICD10 I20-I25) Angina pectoris (I20) AMI (I21) Subsequent MI (I22) Comp after AMI (I23) Other ischaemic (I24) Chronic ischaemic (I25)
2. Acute myocardial infar (ICD10 I21)
Counts and rates for residents wherever treated
Excludes non-residents whowere treated in local hospitals

Mending heartsOverview of methods
How didwe do it?Hospital
episodes (HES)
Deaths (PHMF)
Residentpopulation(Census)
OPCS4 interventions
1. Angiography (K63-K65)
2. Revascularisation (K40-46 and K49-50)Cor art bypass graft (CABG) (K40-K46)
Perc Trans Cor Angio (PTCA)
(K49-K50)
Counts and rates for residents wherever treated
Excludes non-residents whowere treated in local hospitals

Mending heartsVarious options to assess inequality
Describinginequality
Inequalities in admission• coronary heart disease• acute myocardial infarction
Inequalities in interventions• angiography• revascularisation
Inequalities in mortality• coronary heart disease• acute myocardial infarction
Inequalities by:1. Gender (Person, Male, Female)
2. Area (SHA, PCT, ward)
3. Deprivation (IMD scores/ranks)
4. Time (from 1993 to 2003)

16,900 binge drinkers
440 admissions (el + em)
190 angiographies
100 revascularisations
70 CHD deaths (<75 yrs)
17,100 obese
21,100 current smokers
23,700 severely deprived
Iceberg of CHD risks and eventsOnly a fraction of ‘lifecourse’ experience is visible
Volumes ofCHD-related eventsoccurring every yearin Derwentside
25 AMI deaths (<75 yrs)

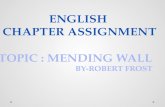
Mending heartsInequality in revascularisation between localities
1. Two-fold difference (Middlesbrough v Hartlepool)2. Some areas below England rates
Source: HESSource: HESRevascularisation per 100,000
0 20 40 60 80 100 120 140 160 180 200
Middlesbrough
Langbaurgh
Darlington
North Tees
Derwentside
Sedgefield
Easington
D & C-le-S
Durham Dales
Hartlepool
England CD&TV

M
Source: HESSource: HES
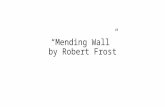
What about the effect of povertyon CHD admissions to hospital?
0100200300400500600700800900
1000
0 20 40 60 80
Deprivation Score
Em
erg
ency
Ad
m
Rat
e/10
0,00
0
Correlation Co-efficient = 0.6195% CI (0.52-0.68)
Emergency AdmissionsWard by Quintile
Quintile 1 (High Emergency Admissions)Quintile 2Quintile 3Quintile 4Quintile 5 (Low Emergency Admissions)
0100200300400500600700800900
1000
0 20 40 60 80
Deprivation Score
Ele
ctiv
e A
dm
Rat
e/1
00,0
00 Correlation Co-efficient = 0.2195% CI (0.09-0.33)
Elective admissions Emergency admissions
Rich Poor Rich Poor
Correlation r = 0.61Correlation r = 0.21
Stronger associationwith deprivation
No associationwith deprivation

Moments of truth
Assessing the scale of inequalities (variations) in risk or treatment or death
and looking at changes over time
is all very wellBUT
it still doesn’t tell us whether
the provision of health care is (in)equitable

Moments of truth
You’ve got to look atvariations in need
and variations in provision
and in comparable ways
Equity audit flat pack

Mending heartsInequality and inequity in coronary heart disease
Measuringinequity
2. Measure the gap in need• coronary heart disease mortality
3. Compare magnitudes of inequity• admissions v coronary heart disease mortality• revascularisation v coronary heart disease mortality
1. Measure the gap in provision
• elective admissions
• revascularisation

M
County Durham & Tees Valley
Elective Admission
0
50
100
150
200
250
300
0 0.2 0.4 0.6 0.8 1
Relative Rank
Ele
ctiv
e A
dm
iss
ion
Ra
te
RII = 23%
AffluentDeprivedRich Poor
Rel Index Inequality
1. Measuring gap in provision - admissions
Slope index inequality = 37

M
County Durham & Tees Valley
3. Comparingthe two gaps
0102030405060708090
100
Admissions Mortality
Magnitudeof inequity
in provisionrelative to need
70%
Elective Admission
0
50
100
150
200
250
300
0 0.2 0.4 0.6 0.8 1
Relative Rank
Ele
ctiv
e A
dm
iss
ion
Ra
te
RII = 23%
AffluentDeprivedRich Poor
Rel Index Inequality
1. Measuring gap in provision - admissions
CHD Mortality
020
406080
100
120140160
180200
0 0.2 0.4 0.6 0.8 1
Relative Rank
Ele
ctiv
e A
dm
iss
ion
Ra
te
RII = 93%
AffluentDeprived
2. Measuring gap in need - mortality
Rich Poor
Slope index inequality = 37
Slope index inequality = 72

Comparing the size of inequity
-50 0 50 100 150 200
Middlesbrough
North Tees
Sedgefield
Darlington
Easington
Durham Dales
Hartlepool
Langbaurgh
Derwentside
Durham & C-le-S
Admissions
Mortality
Mag Inequity
Lower provision
in more deprived areas
Higher provision/need
in more deprived areas
Relative index of inequality
1. Inequalities in need between affluent and deprived areas are worse than inequalities in provision
2. Provision of care does not vary sufficiently to meet different needs and so inequity occurs
3. The inverse care law operates in Sedgefield & Easington
4. Similar resultsoccur when usingrevascularisationfor provision

Someconclusions
1. Inequalities in CHD mortality reflect differences in exposure to risk & access to appropriate healthcare
2. The provision of care for CHD is inequitable in all localities and, at the worst, some inverse care occurs
3. The ability to reduce inequity requires much more understanding of:• patient care pathways;• whole system engineering; and • resource allocation at all levels
Mending heartsWhat does it all mean?

Mending heartsWhere might we start to reduce inequity?
…andquestions
1. Planning & commissioning Do current ‘systems’ create/entrench inequity?
2. Pathways & protocols To what extent are these influencing (in)equity?
3. Patients & professionals How does clinician-patient interaction affect equity?
4. Possible & practical What to do to reduce inequity given other constraints?

Reflections on the processWhat are we learning by studying inequity
1. Does it matter if (in)equity means different things to different people if all working toward the same end?
2. Is available ‘guidance’ for (in)equity measurement sufficient for practical needs in the real world?
3. Are we (the Public Health community) capable of ensuring that the actions we take will really reduce inequity rather than make it worse?
Perceptions
Techniques
Proportionality of response

PerceptionsThe blind men and the elephant
It’s a ropeIt’s a wallIt’s a spear

PerceptionsThe blind men and the elephant
It’s all of these things and yet none of them... …and this is still an elephant.

TechniquesThey forgot to include the instructions
Let me guess.Step 2, add sand
More ‘instructions’
needed at every stage
Illusory simplicity

TechniquesThey forgot to include the instructions
The real 6 stages
ofaudit
1. Enthusiasm
2. Despair
3. Panic
4. Search for the guilty
5. Punishmentof the innocent
6. Praise & honourfor those
never involved

Proportionality of responseI was wondering which of you men would spot that
We need to do somethingto reduce inequity
Wilson
Yes - there is rather a lot of it about
Sir

Proportionality of responseI was wondering which of you men would spot that
Is the response appropriate to the point(s) in the disease life stage where inequity is known/assumed to start?
Where is inequity ‘caused’ and howdoes it vary within adjacent systems?
• Inequity in disease prevention?• Inequity at diagnosis/referral?• Inequity in admissions?• Inequity in surgery?• Inequity in rehabilitation?
Knowledge is patchy & inconsistent

Proportionality of responseIs action happening where it’s needed most?
Do we know if the locality actions are proportional to the size of inequity?
0 20 40 60 80 100 120 140
Durham &C-le-S
Derwentside
Langbaurgh
Hartlepool
Dur Dales
Easington
Darlington
Sedgefield
N Tees
MiddlesbroughCould some types of inequity - like property values -get better even if there was no formal intervention?

Reflections on the processWhat are we learning by studying inequity
1. Does it matter if (in)equity means different things to different people if all working toward the same end?
2. Is available ‘guidance’ for (in)equity measurement sufficient for practical needs in the real world?
3. Are we (the Public Health community) capable of ensuring that the actions we take will really reduce inequity rather than make it worse?
Not if we recognise the perceptions held
Not remotely
We may be capable but there is no evidence of what impact the differences in current activities will have on desired reductions in inequity

Thanks to those involved
Report authorsMichael Fleming
Clare EynonLeon Green
County Durham & Tees ValleyPublic Health Network
Steering GroupMichael Fleming
Alyson LearmonthAnne Low
Mark ReillyToks Sangowawa
Ken Snider
Equity measurementAllan Low
Louise Unsworth
Clinical adviceCoast to Coast Network
Various clinicians
Mending heartsInequality and inequity in coronary heart disease