
Memphis Religious Health Assets - FatCow Web Hostingmrhap.fatcow.com/binghampton_provider.pdf ·...
24
Memphis Religious Health Assets Health Provider-level Workshop Report Binghampton May 30 th , 2008 PIRHANA Workshop: Participatory Inquiry into Religious Health Assets, Networks and Agency Prepared by: Stephanie Doan, MPH* With Collaboration from: Sarah Kennedy † Emmanuel Nii Clottey * + Patience Jarrett † Stephen Nelson *‡ Katherine Pritchard † Ruthbeth Finerman † Teresa Cutts, PhD * * Methodist LeBonheur Healthcare † University of Memphis, Department of Anthropology + University of Iowa, College of Public Health ‡ Rice University, Poverty, Social Justice, and Human Capabilities Program This report is available online at: http://www.memphischamp.org
Transcript of Memphis Religious Health Assets - FatCow Web Hostingmrhap.fatcow.com/binghampton_provider.pdf ·...

Memphis Religious Health Assets
Health Provider-level Workshop Report
Binghampton
May 30th, 2008
PIRHANA Workshop: Participatory Inquiry into Religious Health
Assets, Networks and Agency
Prepared by: Stephanie Doan, MPH*
With Collaboration from:
Sarah Kennedy† Emmanuel Nii Clottey *+ Patience Jarrett† Stephen Nelson *‡ Katherine Pritchard† Ruthbeth Finerman† Teresa Cutts, PhD *
* Methodist LeBonheur Healthcare † University of Memphis, Department of Anthropology + University of Iowa, College of Public Health ‡ Rice University, Poverty, Social Justice, and Human Capabilities Program
This report is available online at: http://www.memphischamp.org

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 1
TABLE OF CONTENTS
SECTION A 1
1. AREA & LEVEL 1
2. DATE & PLACE OF WORKSHOP 1
3. FACILITATION TEAM 1
4. PHYSICAL DESCRIPTION 1
5. PREPARATORY WORK 2
6. PARTICIPANTS 2
7. INTRODUCTION TO PIRHANA WORKSHOPS 3
SECTION B 4
1. TIMELINE 4
2. AREAS OF ENGAGEMENT IN HEALTH AND WELL-BEING 8
3. RELIGION/ HEALTH INDEX 10
4. MAPPING 11
5. SOCIAL CAPITAL AND NETWORKING 113
6. CHARACTERISTICS OF GOOD PRACTICE 16
6. LOCAL ACTION 17
APPENDICES 18
TABLE 1: BINGHAMPTON DEMOGRAPHIC DATA 18
GIS MAP 1: BINGHAMPTON RELIGIOUS HEALTH ASSETS—ENTITIES IDENTIFIED BEFORE WORKSHOP 19
GIS MAP 2: BINGHAMPTON RELIGIOUS HEALTH ASSETS—ENTITIES IDENTIFIED DURING WORKSHOP 20
GIS MAP 3: BINGHAMPTON RELIGIOUS HEALTH ASSETS—COMBINED ENTITIES 21
TABLE 2: WAYS RELIGION CONTRIBUTES TO HEALTH (EXERCISE 3: ROUND 2) 22
ACKNOWLEDGMENTS 22

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 1
SECTION A
1. AREA & LEVEL
As a component of the Religious Health Assets Mapping project, a half-day workshop was held at the health provider level—focusing on the people and organizations that provide health and religious services in the Binghampton Community. The boundaries of the study area were formed by Jackson Avenue to the north, East Parkway to the west, Poplar Avenue to the south and Holmes to the East. The study area lies predominantly within zip code 38112. The basic demographics of the study area can be found in Appendix Table 2.
Map of study area
2. DATE & PLACE OF WORKSHOP The workshop took place from 8:15 AM to 1:30 PM on Friday, May 30thth, 2008 in the Caritas Village Upper Room located at 2509 Harvard, Memphis, TN 38112.
3. FACILITATION TEAM Lead Facilitator: Teresa Cutts, PhD Methodist LeBonheur Healthcare, University of Tennessee College of Medicine
Cecelia Sawyer Senior Vice President for Elder Care, Methodist LeBonheur Healthcare Facilitation Team: Chip Clay, MDiv Emmanuel Nii Clottey
Stephanie Doan, MPH Sarah Kennedy Stephen Nelson
Katherine Pritchard Rick Thomas, PhD
4. PHYSICAL DESCRIPTION The workshop was held in the upstairs room of Caritas Village, an old Masonic lodge. The front of the room was set up with several rows of chairs for seating as a large group, with several flip charts for recording information on the stage at the front of the room. In the center of the room were 2 tables for small group activities. Coffee and snacks were available at a table at the back of the room.
Room Layout
PIRHANA Health-Seeker Workshop Report—Binghampton
Page 2
5. PREPARATORY WORK Preparatory work for the PIRHANA workshops included several different activities including: background research, field study, data collection, map generation, facilitation team training, workshop planning, and workshop materials preparation. Background Research included a review of Religious Health Assets Mapping projects in southern Africa, various approaches to community mapping, and models for participatory research projects. Field Study included a series of transect drives through the study area with team members familiar with this area, as well as initial identification of key assets and potential key informants. These transect drives, in combination with the insights from key informants, were used to decide the preliminary boundaries for this mapping exercise. Data collection included the acquisition of basic demographic, socioeconomic and psychographic data in the study area. Study staff compiled lists of known assets and interviewed key community informants. Map Generation involved the processing and analysis of data on the study area, the incorporation of these data into a geographic information system, and the generation of geographical and spatial representation of area information through a series of GIS map layers. Facilitation Team Training occurred through team member’s participation in training events, past workshops held in similar locations, and a familiarity with the PIRHANA methodology and other participatory models for focused group discussion. Workshop Planning involved identifying potential participants for the health providers workshop, developing and disseminating a letter of invitation, and following up with potential participants. Workshop staff held face-to-face meetings, attended community meetings and local bible studies, sent emails, and made follow-up telephone calls during the 2 weeks prior to the workshop The workshop staff also identified Caritas Village as an appropriate site to hold the workshop and made the arrangements for AV equipment and lunch (catering by Caritas Village). Workshop Materials Preparation included the generation and printing of neighborhood maps, the printing of materials to be handed out, the packaging of these materials and the organization of all the materials needed for the workshop exercises (for example, large pieces of paper, post-it notes, writing utensils, flip charts, and beans).
6. PARTICIPANTS A total of nine ‘health providers’ participated in this workshop. The term ‘provider’ is used throughout this report to broadly include anyone who provides services in the community (including healthcare, religious, and social services). The workshop participants included 4 females and 5 males, with ages ranging from 22 to 69 years. Many of the participants have been long-time residents of Memphis—with the average participant spending nearly 2/3 of his or her life in Memphis. Participants represented a range of religious traditions including Baptist, United Methodist, Catholic, Disciples of Christ and other non-denominational traditions. Workshop participants represented a number of health and social service organizations in the Binghampton community, including Christ Community Health Services, Caritas Village, United Methodist Urban Ministries, School of Servant Leadership, Catholic Charities, and Binghampton Development Corporation. The participants were highly educated; all the participants received at least a college degree, with several participants holding advanced degrees. The selection of participants using a ‘snowballing technique’ often results in the creation of small pockets of similar people. While this workshop included some of the young and middle-aged adults that were not represented in the seeker-level workshop, there are many organizations and congregations that were not represented in this workshop. The results and data generated must be interpreted with an understanding of the composition of the workshop participants (and those groups that were not represented).

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 3
7. INTRODUCTION TO PIRHANA WORKSHOPS The workshop began with a short introduction of the workshop purpose and process as well as an introduction of each of the workshop participants and facilitation team. Participants were asked to share not only their names but also their connections to the neighborhood. Participatory Inquiry into Religious Health Assets, Networks, and Agency (PIRHANA) is a research tool developed by a group of researchers in sub-Saharan Africa known collectively as the African Religious Health Assets Program (ARHAP). Rather than focusing on the problems and deficiencies in communities, the purpose of the PIRHANA workshop is to identify the things that are good and positive in the community. The process is different from a traditional focus group or town hall meeting since the participants actually become ‘researchers’ during the workshop and the results are given back to the participants and the community to use for planning and future activities. The basic goals of the PIRHANA project in Memphis are to: 1) understand and assess the impact and growth of religious health assets in fostering health in all of its dimensions; 2) fuel research that will promote a greater and more complete understanding of the role of religion and religious institutions in health promotion and delivery; 3) strengthen leadership and organizational capacity to advance health and wellness. A similar workshop was held in this same community at the health-seeker level on May 29th. These workshops are just 2 of many workshops that will be held throughout the Memphis area over the next 3 years.
Introduction of participants and PIRHANA process

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 4
SECTION B
1. TIMELINE
a) Data The first exercise of the workshop focused on understanding the broader social, political, and religious context in which important Binghampton entities and assets have developed. Working together, participants created a timeline to this historical context; each participant was asked to fill out one post-it note for each of following categories, accompanied by an approximate date:
• One key significant social, political or economic event • The name of the organization they represent or belong to • A key event to do with religion or health
Participant writes post-its for the timeline
After each participant added his/her post-it notes to the blank timeline at the front of the room, participants were asked to continue to add important events that might be missing. Participants were given an opportunity to explain their additions to the time-line and were asked to comment on any trends emerging from the data. Throughout the conversation, participants continued to add additional events to the timeline.
Workshop staff adds additional post-its to the timeline

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 5
Key Religious or Health Events Formation of Organizations Key Social or Political Events 1870s—Yellow Fever Epidemic 1897—Church of God in Christ
(COGIC) founded/established — — —
1965—Medicare and Medicaid introduced by US Congress
1968—Merger of the Methodist
Church and the United Evangelical Brethren Church
1980s and 1990s—Sam Cooper
Corridor Mid 1980s and 1990s—Early Days
of AIDS Epidemic 1988—Church Health Clinic 1996—Merging of Methodist and
LeBonheur Hospitals 1999—Dr. Frank Anthony Thomas
becomes new pastor of Mississippi Blvd Christian Church
2001—Baptist leaves downtown 2004—Healthy Choices (Memphis
City Schools) 2005—Individuals dropped from
TennCare 2007—High Rate of Murder and
Violence 2008—Strong Me 2008—Not Even One Program
1907—Everett/Binghampton United
Methodist Church — — —
1968—MIFA (Metropolitan Interfaith Association)
1969—Community Foundation (of
Greater Memphis 1985—United Methodist
Neighborhood Center 1986—Service Over Self 1987—Physicians for a National
Health Program 1988—North Memphis Urban
Parish (5 United Methodist Churches)
1989—Tennessee Health Care Campaign
1993—Neighborhood School 1993—Metro Office of Urban
Ministries 1995—Memphis School of Servant
Leadership 1995—Christ Community Health
Services 1997—EIKON Ministries 1997—School of Servant
Leadership 1998—Christ Community Health
Services in Binghampton 1998—Rachel’s Kids, Inc. 1998—Hope Foundation 2000—Caritas Community 2003—Binghampton Development
Corporation 2003—Healthy Memphis Common
Table 2004—East High Foundation 2006—Caritas Village 2006—Memphis African American
Social Workers Association 2006—Memphis City Schools
Project— UTMG 2008—Common Ground Memphis 2008—Collegiate School of
Memphis
— — — 1957—Founding of Stax 1960s—Segregation 1964—Civil Rights Act
1968—Sanitation Worker Strike 1968 (April 3)—Dr. King’s Speech at
Clayborn Temple 1968—Dr. Martin Luther King, Jr
assassinated 1968—Desegregation of John
Gaston Hospital Late 1960s-Early 1970s—White
Flight 1970s—Social Pop Culture/Height
of Stax 1970-1972—Memphis City School
integration/busing 1976—Demise of Stax 1977—Elvis Presley Dies 1980s—Interstate cuts through
community—business and homes torn down
1991—First African-American Mayor of Memphis elected—W.W. Herenton
2000—Methodist Healthcare/UT merger
2000s—Broad Street Redevelopment Project
2000s—First Baptist Broad involved in Community—working closely with CCHS
2003—Dr. Lloyd takes over Crighton College
2005—Tennessee Waltz 2005—Brewster School built

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 6
b) Discussion After placing their post-it notes onto the timeline, the participants described in greater detail how some of the social and political (as well as religious) events on the timeline impacted the Memphis and Binghampton Community. One participant talked the early years of AIDS epidemic, remembering when all the people receiving services died as a result of the disease. Another participant talked about the push for education in the early days of AIDS and pointed out the huge amount of progress that has been made in the last 20 years. Another participant talked about the importance of Binghampton community organizations and churches coming together to resolve the issue about what would happen with Sam Cooper Blvd in the 1980s. One participant talked about the important leadership of Dr. Thomas in the discussion of faith and health in Memphis and that he has played an important role in empowering Mississippi Blvd Christian Church and others to become involved in their own communities. Participants went on to describe the work and activities of the various organizations on the timeline:
Service over Self—Started as a home repair project out of Christ United Methodist Church, has evolved into something much bigger. Every summer teams of youth from all over the country, led by groups of college-age counselors, go out into the Binghampton community to repair homes and form relationships with Binghampton residents. Under the surface, SOS helps to train young adults (including the college staff) to be in the business of providing services and ministries.
Christ Community Health Services—4 clinics throughout Memphis (one on Broad street in Binghampton). Clinic for the underserved populations in Memphis with no insurance—providing services in geriatrics, obstetrics and everything in between. Have outreach programs in the community including: Safe program (for victims of sexual assault), Marriage 101, Dynamic Dad, Memphis Healthy Churches, CHOICES (abstinence education program), social workers in local schools.
Memphis School of Servant Leadership—Raise up Christian leaders that had both the inner depth and the outer vision to serve people in the community, primarily through courses on a range of issues.
Binghampton Development Corporation—Bring healing to the community by working on real-estate to get land into the hands of local community residents—it’s more than just a real-estate program that also provides job and tax training, renovation assistance, senior housing, etc.
Healthy Memphis Common Table—Community collaborative venture that has held community forums and developed strategies for reversing the rising prevalence of obesity and diabetes and improving the quality of treatment associated with them. Community programs include Strong Me program (focused on decreasing obesity among adolescent girls) and Healthy Choices (focused on countering unhealthy behaviors among youth, like relationships, activity, diet, neighborhood, etc.)
Memphis City Schools Program—teams of teachers and therapists to work with children with ADHD (in elementary, middle and high schools)
East High Foundation—excellent example of public-private partnership; the foundation provides tutoring, sports, and resources to youth at East High School and Lester Elementary/Middle School.
EIKON Ministries—focused on “making reproducing disciples”—a couple of community houses and staff who live and work in the community who have activities for young people in Binghampton
Not Even One—A new program to bring awareness and find solutions to violence in Memphis through the development of “hope response teams.”
Broad Street Redevelopment Project—a series of community meetings and Tillman Master Plan
Rachel’s Kids—Began when neighborhood children wanted to help out at Rachel’s Flowers, now Rachel’s Kids provides services to a number of children and youth from the neighborhood.
Collegiate School of Memphis—a new school in Binghampton for grades 7 to 12, starting with 7th grade in 2008 adding a grade each year over the next 6 years.
First Baptist Broad—Deeply involved in the community—working closely with CCHS but also a number of services, including free dental examinations, parenting groups, etc.
PIRHANA Health-Seeker Workshop Report—Binghampton
Page 7
After discussing these organizations and events, the facilitator asked participants to describe how the religious organizations mentioned above are doing (and what they aren’t doing) in the community. A participant quickly said, “Not cooperating enough.” He went on to suggest that “power and money often get in the way of cooperation and efficiency” as people want to protect their own sources of funding. Another participant suggested that the religious organizations in Binghampton haven’t connected with the neighborhood like they should—most of the churches are white and do not reflect the racial composition of the neighborhood. In addition, while many of the organizations and ministries have done a good job of connecting with the children, they have done a poor job of connecting with the rest of the family. Other participants pointed out that community members often do not see strong connections between the religious organizations and the neighborhood churches. One participant suggested that organizations and individuals lack “real relationships,” especially relationships that cross both racial and socioeconomic divides. Others agreed and suggested that the idea of such relationships is not unique to Binghampton, Memphis, or our Nation. One participant suggested that the “white flight” of the 1960s and 1970s (and the current “Black Flight”) speak into this lack of real relationships, as our human nature makes us fearful of people who are different from us. Participants suggested that the ‘church’ has often been one of the most segregated places but that the churches could “overcome fear; they could begin the ball rolling” on creating meaningful relationships across traditional divides and on reaching outside their own congregations to attract and serve others.
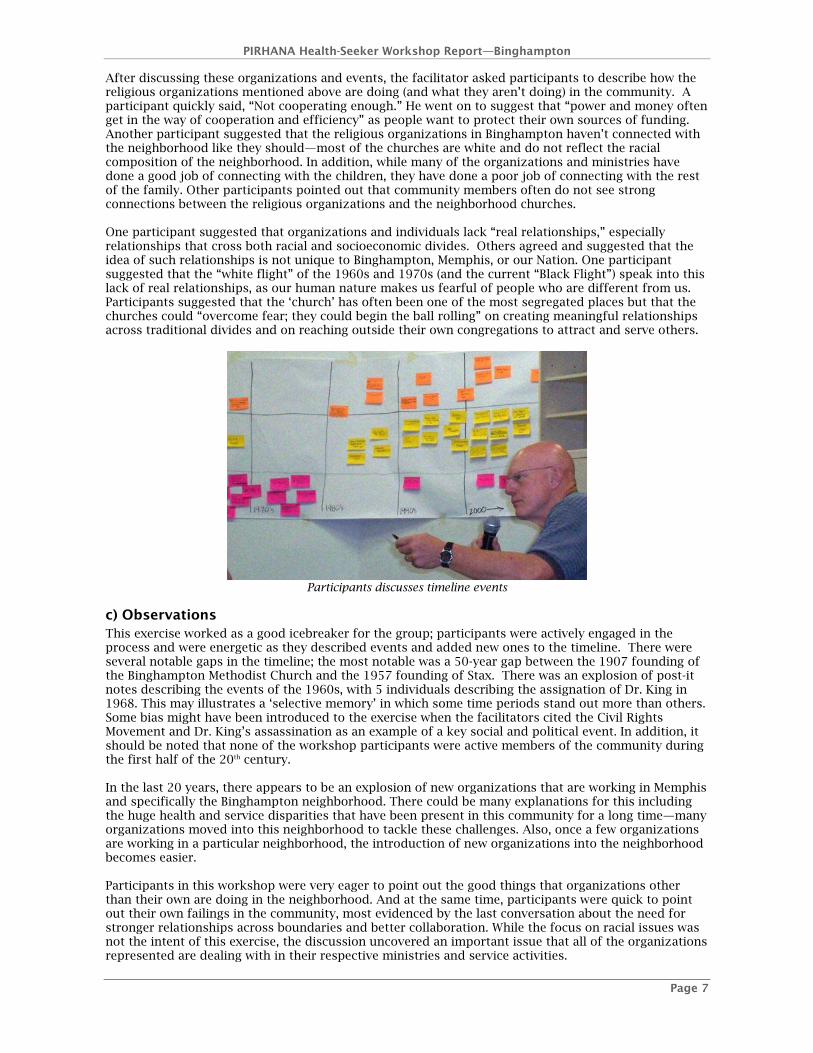
Participants discusses timeline events
c) Observations This exercise worked as a good icebreaker for the group; participants were actively engaged in the process and were energetic as they described events and added new ones to the timeline. There were several notable gaps in the timeline; the most notable was a 50-year gap between the 1907 founding of the Binghampton Methodist Church and the 1957 founding of Stax. There was an explosion of post-it notes describing the events of the 1960s, with 5 individuals describing the assignation of Dr. King in 1968. This may illustrates a ‘selective memory’ in which some time periods stand out more than others. Some bias might have been introduced to the exercise when the facilitators cited the Civil Rights Movement and Dr. King’s assassination as an example of a key social and political event. In addition, it should be noted that none of the workshop participants were active members of the community during the first half of the 20th century. In the last 20 years, there appears to be an explosion of new organizations that are working in Memphis and specifically the Binghampton neighborhood. There could be many explanations for this including the huge health and service disparities that have been present in this community for a long time—many organizations moved into this neighborhood to tackle these challenges. Also, once a few organizations are working in a particular neighborhood, the introduction of new organizations into the neighborhood becomes easier. Participants in this workshop were very eager to point out the good things that organizations other than their own are doing in the neighborhood. And at the same time, participants were quick to point out their own failings in the community, most evidenced by the last conversation about the need for stronger relationships across boundaries and better collaboration. While the focus on racial issues was not the intent of this exercise, the discussion uncovered an important issue that all of the organizations represented are dealing with in their respective ministries and service activities.

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 8
2. AREAS OF ENGAGEMENT IN HEALTH AND WELL-BEING
a) Data The goal of the second exercise was to create a categorized list of organizations and the services they provide in respect to health (prevention, treatment, care-giving, support services, other) as well as to examine the religious or non-religious nature of each organization or entity. Participants were asked to place the organizations they represent (plus others in the community) into the matrix on the board. After participants added entities to each category, participants discussed the organizations they put up and the trends that emerged out of the data.
CCHS CCHS CCHS CCHS BDC
BDC BDC UMUM MSSL (teaching)
Crichton MSSL EIKON CV (micro-lending)
NEO UMUM SOS HF
UMUM CV CV CF
MSSL SSL
Religious/ Faith-based
CV
Prevention Treatment Care Support Other
MAASWA MAASWA MAASWA BDC MAASWA (scholarship)
PNHP HMCT EHF
MCS PNHP MAASWA Secular/Public
HMCT THCC CCHS Key:
BDC Binghampton Development Corporation CCHS Christ Community Health Services CF Community Foundation CV Caritas Village/Caritas Community EHF East High Foundation HF Hope Foundation HMCT Healthy Memphis Common Table MAASWA Memphis African American Social Workers Association MCS Memphis City Schools MSSL Memphis School of Servant Leadership NEO Not Even One PNHP Physician for National Health Program THCC Tennessee Health Care Campaign UMUM United Methodist Urban Ministries
Health entities Matrix

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 9
b) Discussion Participants were given the opportunity to describe in more detail the organizations that they placed onto the board and why they placed organizations into particular categories. Participants talked about the details of services for many of the organizations on the entities in the timeline exercises. Participants brought out the idea that the BDC really touches each of the different categories of services, including treatment to some extent. Caritas Village suggested that support services are the thrust of their ministry (affordable housing, care-giving, mentoring, etc.); while they didn’t add treatment, they suggested that they “treat skins and bruises and hurt feelings and a lot of the ‘isms.’” Participants also talked about the focus on prevention and counseling that is present at Christ Community Health Services, including a mobile van to serve homeless populations. Participants also talked about the mentoring that many of these organizations provide, including SOS, EIKON, SSL, UMUM and CV. A participant representing the Memphis African American Social Workers Association (MAASWA) described the work of MAASWA to connect social workers in different organizations and ministries. While MAASWA itself doesn’t provide direct services in any of these categories, the people involved in MAASWA are involved in these different categories. In the Other category, MAASWA gives a scholarship to aid in the training of new social workers. MAASWA is involved in some community development projects and mentoring projects with the Girl Scouts and LeMoyne-Owen College. One participant talked about the importance of prevention in the elimination of disparities, most of which are linked to poverty and racism—introducing the topic of race and poverty to the discussion will continue to be central in decreasing disparities. Participants went on to talk about the religious nature of the entities on the matrix. The Caritas Community/Village representative suggested that CV is like a ‘church in the marketplace.’ The participant representing Christ Community Health Services (CCHS) designated CCHS as a religious entity because it is a faith-based clinic and because staff read scripture, pray with patients, and hand out Bibles. However, the participant also placed CCHS in the public category since the services are made available to all members of the community, not just people who belong to a certain church.
Participant add organizations to the matrix
c) Observations The service categories with the largest number of organizations mentioned were prevention and support, highlighting the large number of social service organizations that are working in the Binghampton neighborhood. While it was addressed in the timeline exercise, this workshop activities again brought out the fact that a large number of the organizations working in Binghampton have a religious nature. In fact, most of the organizations in the public category are Memphis-wide organizations that do not provide services solely, or even primarily, within the Binghampton neighborhood.

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 10
3. RELIGION/ HEALTH INDEX
a) Data For the third exercise, participants were each given two post-it notes and were asked the following question: “If the Health Department asked you to identify the two most important ways that religion/faith/spirituality contributes to health/wellbeing in your community – what would you say?” A list was created based on the answers provided. Participants were then asked to repeat the activity by filling out two additional post-it notes to ‘vote’ for the factors that the participant deemed the most important. These factors were mentioned by participants during the first ‘brainstorming’ round:
• Faith-based Hospital Systems/Religious motivation behind healthcare providers (2) • Faith-based organizations can act as an incubator for health programs, discussions and
advocacy • One's faith contributes to wellness which impacts health—emotional, physical, spiritual • Provides means and structure for believing in something greater than self & provides a way
to move out of destructive habits • Security and Support • At CCHS—give patients a positive feeling of God and love and provides a caring staff to help
patients cope with health issues • Parish nursing programs (mainly in white churches) • Church Preaching—emphasis on physical and mental health (mainly in black churches)
The answers in the 2nd ground were grouped into 3 main categories: (Factors grouped together, for full list, see Appendix Table 3)
Empowerment (4)
Education (3) Relationships (2) Providing services Hope in healthcare
Weekly fitness program Breaks down love affair that Americans have with medical technology
b) Discussion Participants were given the opportunity to comment on what they meant on their cards and their reasons for thinking that a particular factor was important. One participant talked about the importance of having caring people and strong relationships and a shared (“higher”) belief , especially when caring for people who do not have strong support systems. When talking about faith-based organizations as incubators for services, participants talked about the role of churches in mobilization efforts (for example, the civil rights movement). Often in these communities, churches are the places where people come together to talk about important topics (whether it’s a health fair, round-table discussion or supporting advocacy organizations). Participants also suggested that believing in something greater than yourself is important when dealing with mental health issues, especially drug and alcohol abuse. Participants also suggested that in many churches there hasn’t been enough emphasis on health. For example, you walk into a church and you will see many overweight people. One participant suggested that black churches actually do a better job of addressing those health issues collectively. However, participants suggested that Catholic, Episcopal and Lutheran churches have developed and trained parish nurses to address these issues.
c) Observations Especially in the first round, participants touched on broad range of different ways that religious organizations and religion contribute to health. In the second round, there were several more participants who identified empowerment as an important contribution of religion to health. While this concept was not discussed in detail with the group, perhaps this is due to the large number of participants involved in social work, counseling, and mentoring. The final grouping into categories was perhaps the least participatory part of the workshop process. While participants were given a chance to explain their cards, the facilitators were the ones who made decisions about the grouping of the factors mentioned by participants.

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 11
4. MAPPING
a) Data For the third exercise, the participants were divided into two groups. The groups were provided with pre-printed maps and were asked to verify the entities listed on the maps and to add any other entities that they thought were missing. Participants noted new additions to the maps with small post-it notes. Group A identified the following entities:
• First Baptist Church Broad • Early Grove Baptist Church • Christ Community Health Services • Caritas House (on Everett) • Blessed Sacrament
• Park • Caritas Village • No Grocery Store • Ugly Mug Coffee • Rachel’s Kids
Group A adds entities to the Binghampton map
Group B identified the following entities:
• De LaSalle School • First Baptist Church Broad • Lester Community Center • Police Precinct • School • EIKON • Tillman Apartments • The Neighborhood School • Senior Center • Red Oak • Early Grove • Lester Middle/Elementary School • After School Program • Pleasant Hill Missionary Baptist Church • Memphis School of Servant Leadership • Veterinary Office • Central Library • Tech Center East HS (East Career and
Technology Center) • Southeast Mental Health Center
(SEMHC) • East High School • Chickasaw Oaks Plaza • Lester Community Center
• J. O. Patterson Mortuary • Caritas Village • Republic Coffee • Agape • NH Owens Funeral Home • Exchange Club • Big Brothers/Big Sisters • Bank of America • Everett Memorial Binghampton Church • Memphis City Schools’ Teaching &
Learning Academy • Binghampton Park • After School Program • Open Heart Spiritual Center • Broadway Pizza • Brewster Elementary School • Family Services of the Mid-south • Service Over Self • Rachel’s Florist / Rachel’s Kids • Memphis Theological Seminary • Lindenwood Christian Church • LeBonheur CCP • Christ Community Health Services

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 12
b) Discussion Participants had a chance to talk about the entities that they identified on their maps. The spokesperson from Group A suggested that no other maps of this neighborhood include the house churches that meet in this neighborhood that are important to the neighborhood. Blessed Sacrament Church has Latino and Vietnamese congregations. The spokesperson also pointed out the lack of a good grocery store in this neighborhood and pointed out that the diversity was an important thing that the participants valued in this community. The group also pointed out the importance of a good pharmacy. The spokesperson from Group B described their process for mapping—simply writing down everything that came to mind. They identified many different types of entities—schools, after-school programs, churches, apartments, social services, apartment complexes, etc. They pointed out that Lindenwood Church has an afterschool program. The map also identified business like banks and mortuaries. The group was unsure whether LeBonheur CCP was still located in Binghampton.
The group B representative reports on their map
c) Observations The most notable observation made by the facilitation team was the disparity between the two groups concerning the number of entities mapped. This was probably due to the fact that most of the participants in Group B were social workers, who are very familiar with the services and businesses of the neighborhood. However, while Group A generated a much smaller list, they located several entities that were not mentioned by Group B.
Group A map Group B map
PIRHANA Health-Seeker Workshop Report—Binghampton
Page 13
5. SOCIAL CAPITAL AND NETWORKING
a) Data (Step 1) Participants were asked: We are now interested in understanding more fully the types of relationships that exist among you and your organizations and also among others who may not be with us today. We often think of ‘assets’ as physical things – but in fact, relationships (the spaces between things) can also be an asset. Participants were provided with blank forms on which they could write the names of different organizations and entities with which their organization has a relationship. Summarized data from completed forms (* Potential Relationships):
Binghampton Development Corporation (BDC) connected to: SOS, Lester Community Center, EIKON, Church Health Center, Lester Elementary/Middle School, Healthy Memphis Common Table
Christ Community Health Services (CCHS) connected to: Methodist, Police, DHS, UT Medical, Fresh Start, Department of Mental Retardation Services, Sycamore Church of Christ Counseling Services, BDC, CSA, Baptist, the MED MAASWA is connected to: Lester Community Center, Girl Scouts, Mental Health Centers*, Churches*, Local Colleges*, Memphis City Schools*, Community Organizations*, Criminal Justice System* Healthy Memphis Common Table is connected to: Caritas Village, Memphis City Schools (East High, Lester, Brewster), School of Servant Leadership, Church congregations, Memphis Healthy Churches, Green Organization, Memphis Health Loop Clinic
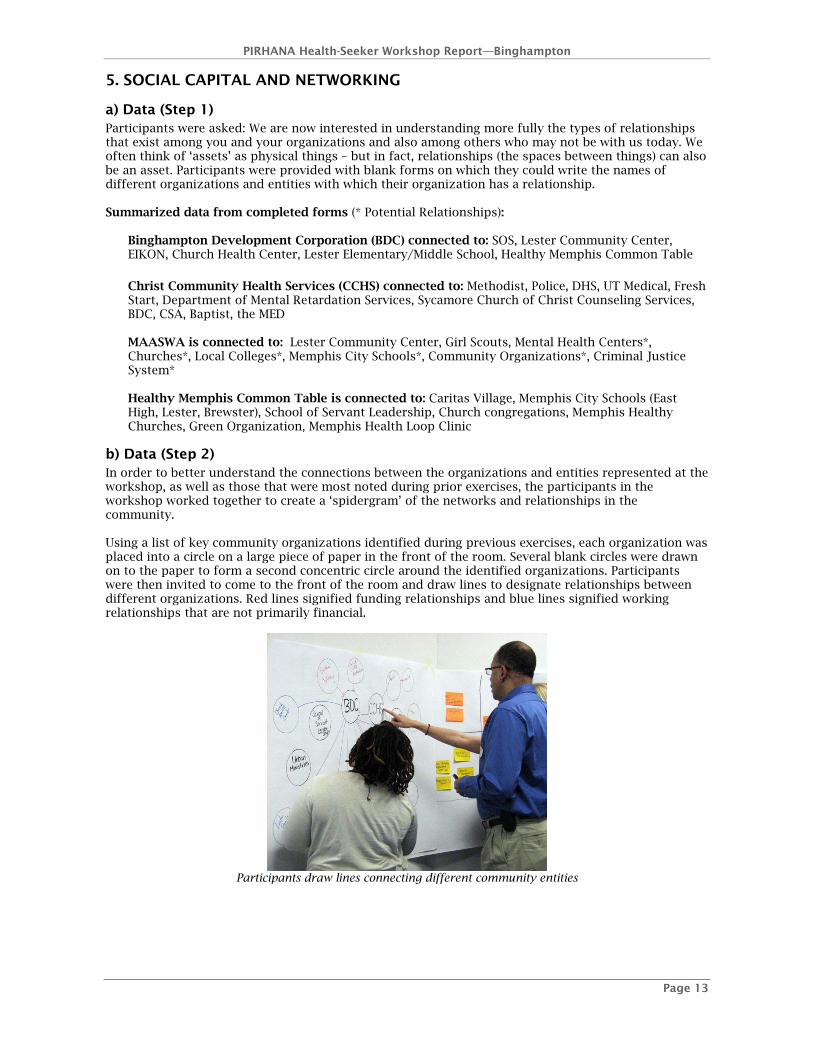
b) Data (Step 2) In order to better understand the connections between the organizations and entities represented at the workshop, as well as those that were most noted during prior exercises, the participants in the workshop worked together to create a ‘spidergram’ of the networks and relationships in the community. Using a list of key community organizations identified during previous exercises, each organization was placed into a circle on a large piece of paper in the front of the room. Several blank circles were drawn on to the paper to form a second concentric circle around the identified organizations. Participants were then invited to come to the front of the room and draw lines to designate relationships between different organizations. Red lines signified funding relationships and blue lines signified working relationships that are not primarily financial.
Participants draw lines connecting different community entities

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 14
LesterCommunity
Center(3)
MSSL(5)
BDC(13)
CCHS(9)
CaritasVillage
(16)
MAASWA(2)
Rachel’sKids
(1)
UrbanMinistries
(2)
HMCT(10)
SOS(2)
ChurchHealthCenter
UnitedWay
ChristUMC
LesterElem/Middle
School
EIKON
WH BrewsterElementary
School
Colleges
LeadershipFoundation
Baptist
MethodistHealthcare
St Francis
MCS
Recreation of Spidergram
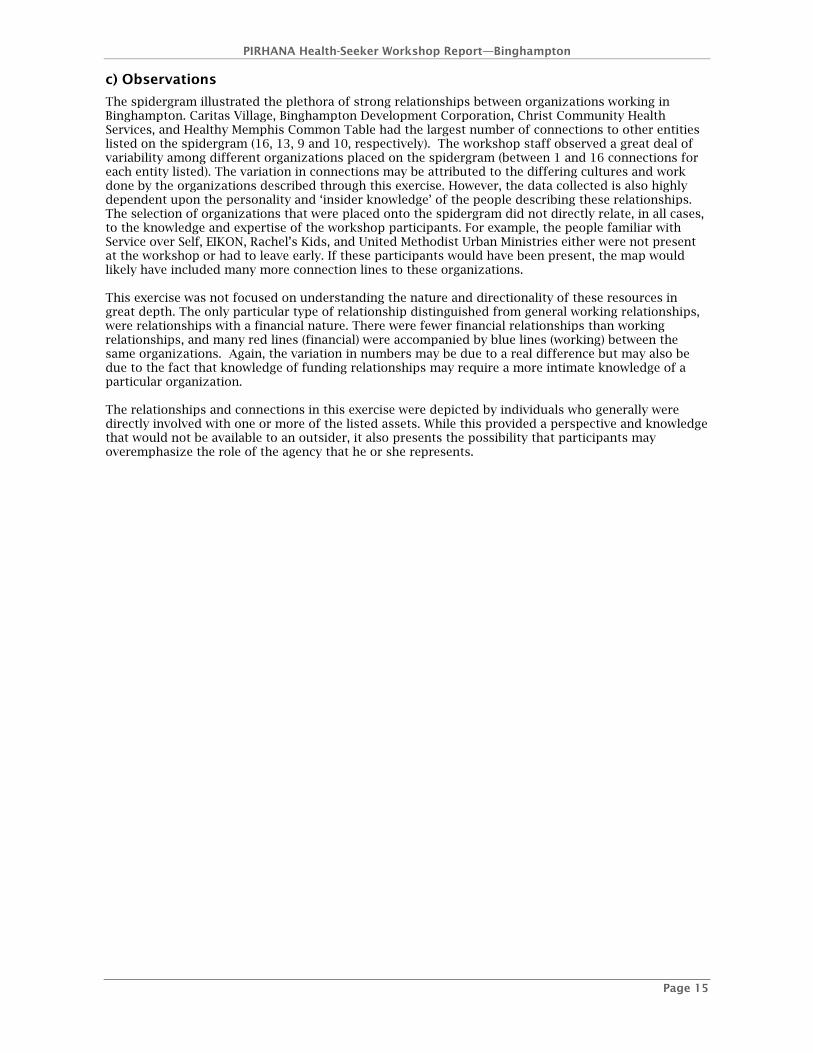
After each participant had the opportunity to add additional lines to the ‘spidergram,’ the moderator lead a discussion concerning the interrelationships that exist between these community assets and the extent to which the provision of services has been integrated. Ten organizations were placed into the first group of concentric circles. An additional twelve organizations were added to the outer circle by participants. Of the twenty-two organizations included in the spidergram, five could be described as healthcare providers, nine as social service agencies, two as networking agencies and four as education providers. Only one specific religious congregation was added to the spidergram—Christ UMC.
Other participants add connection lines
PIRHANA Health-Seeker Workshop Report—Binghampton
Page 15
c) Observations
The spidergram illustrated the plethora of strong relationships between organizations working in Binghampton. Caritas Village, Binghampton Development Corporation, Christ Community Health Services, and Healthy Memphis Common Table had the largest number of connections to other entities listed on the spidergram (16, 13, 9 and 10, respectively). The workshop staff observed a great deal of variability among different organizations placed on the spidergram (between 1 and 16 connections for each entity listed). The variation in connections may be attributed to the differing cultures and work done by the organizations described through this exercise. However, the data collected is also highly dependent upon the personality and ‘insider knowledge’ of the people describing these relationships. The selection of organizations that were placed onto the spidergram did not directly relate, in all cases, to the knowledge and expertise of the workshop participants. For example, the people familiar with Service over Self, EIKON, Rachel’s Kids, and United Methodist Urban Ministries either were not present at the workshop or had to leave early. If these participants would have been present, the map would likely have included many more connection lines to these organizations. This exercise was not focused on understanding the nature and directionality of these resources in great depth. The only particular type of relationship distinguished from general working relationships, were relationships with a financial nature. There were fewer financial relationships than working relationships, and many red lines (financial) were accompanied by blue lines (working) between the same organizations. Again, the variation in numbers may be due to a real difference but may also be due to the fact that knowledge of funding relationships may require a more intimate knowledge of a particular organization. The relationships and connections in this exercise were depicted by individuals who generally were directly involved with one or more of the listed assets. While this provided a perspective and knowledge that would not be available to an outsider, it also presents the possibility that participants may overemphasize the role of the agency that he or she represents.

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 16
6. CHARACTERISTICS OF GOOD PRACTICE
a) Data In order to identify which religious assets provide an example of an effective contribution to the health of the community, participants were asked, “In light of the previous discussion, what do you think are the two most important religious organizations that contribute to health in your community.” Each participant was once again given two post-it notes each. The collected post-it notes were made into a bar graph. Participants were then given the opportunity to describe the characteristics of these organizations that make them exemplary. The group identified the following religious organizations:
Christ Community Health Services (6) Caritas Village (2) First Baptist Church Broad (2) Memphis School of Servant Leadership(1) Agape (1) Baptist Hospital Mobile Health Van (1)
b) Discussion Participants described the exemplary organizations in the following ways:
Christ Community Health Services: They provide affordable and quality healthcare and “also do a lot of handholding.” They are available to people who have nowhere else to go; if they didn’t go to CCHS, they would probably not receive services anywhere. Many of the physicians live in the neighborhood among the people they are serving. They have a long history of performing well, they have a great mission, and have a model for spreading into new areas of need. Caritas Village: Described as an ‘urban oasis’ with a strong feeling of love and hospitality First Baptist Broad: One of the oldest African American congregations in Binghampton. They have excellent services for the members of the congregations as well as many services for the community. For example, they played a large role in activities surrounding the aftermath of the Lester Street tragedy, attempting to heal people in the community.
c) Observations In both the health-seeker and health-provider workshops in Binghampton, Christ Community Health Services received the highest number of votes in this exercise. In both workshops, participants cited the affordability of care, the faith-based nature/mission of the clinic, and the excellence of the staff as just a few of CCHS’s exemplary characteristics.
Participant describes an exemplary Binghampton organization

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 17
6. LOCAL ACTION As the final exercise of the workshop, participants were asked, “Now that we’ve talked about all the assets in the community, like organizations, relationships and networks, what do you think would be the next steps to bring this process forward?” The discussion generated the following suggestions:
• While there are many assets, we need to identify the deficits in Binghampton. • More collaborative efforts among Binghampton entities. Duplication of services is a big
problem; entities need to break away from mindsets of individuality to build collaborative partnerships.
• Address the lack of economic development in Binghampton. • Resource booklet and ongoing meetings to put together the things we do have and things we
don’t have so we can work together more effectively. • Share contact information between people and organizations who are involved in this process.
Need transparency and forums for communication.
Participant discusses next steps

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 18
APPENDICES
TABLE 1: BINGHAMPTON DEMOGRAPHIC DATA
Binghampton Demographic Information Source: US Census 2000
Bin
gh
amp
ton
*
Shel
by
Cou
nty
Un
ited
Stat
es
Total Population 17,851 897,472 281,421,906Gender
Male 46.3% 47.8% 49.1% Female 53.7% 52.2% 50.9%
Race White 24.4% 47.3% 75.1% Black or African American 69.0% 48.6% 12.3% Other 5.5% 3.1% 10.2% More than one race 1.1% 1.0% 2.4%
Educational Achievement (25 years and older) High School Diploma or highter 64.1% 80.8% 80.4% Bachelor's Degree or higher 13.5% 25.3% 24.4%
Marital Status (15 years and older) Never Married 40.2% 31.8% 27.1% Married 32.1% 46.6% 54.4% Seperated, Divorced, Widowed 27.7% 21.6% 18.5%
Employment (16 years and older) In labor force 55.5% 65.6% 63.9%
Employed 48.1% 61.1% 60.2% Unemployed 7.4% 4.5% 3.7%
Not in labor force 44.5% 34.4% 36.1%
Nativity: Born in USA 93.5% 95.5% 87.7%
Median Age 32.5 yrs 32.9 yrs 35.3 yrs
Total Households 6,909 338,366 105,480,101Families (Family Household) 58.8% 67.6% 68.1%
Married-couple family 24.2% 42.8% 51.7% Female-householder, no husband present 29.3% 20.1% 12.2%
Non-family Households 41.2% 32.4% 31.9%
Households with individuals <18 years 36.3% 39.0% 36.0% Households with individuals >65 years 23.6% 19.5% 23.4%
Income Median Household Income (1999) $25,082 $39,593 $41,994 Households with Social Security Income 26.0% 21.4% 25.7% Households with Public Assistance Income 9.2% 4.5% 3.4%
Poverty Family households below poverty line 30.7% 12.9% 9.2% Non-family households below poverty line 27.0% 19.1% 17.4%
Families with grandparent responsible for own grandchildren <18 years
9.5% 5.2% 3.4%
Average Household Size 2.54 2.6 2.59 Average Family Size 3.30 3.18 3.14
Total Housing Units 7,673 362,954 105,480,101Owner-occupied 43.0% 58.8% 60.2% Renter Occupied 47.0% 34.4% 30.8% Vacant 10.0% 6.8% 9.0%
*Compilation of Census Tracts 0046, 0047, 0048, 0049, 0050, 0058, 0059

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 19
GIS MAP 1: BINGHAMPTON RELIGIOUS HEALTH ASSETS—
ENTITIES IDENTIFIED BEFORE WORKSHOP

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 20
GIS MAP 2: BINGHAMPTON RELIGIOUS HEALTH ASSETS—
ENTITIES IDENTIFIED DURING WORKSHOP

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 21
GIS MAP 3: BINGHAMPTON RELIGIOUS HEALTH ASSETS—
COMBINED ENTITIES

PIRHANA Health-Seeker Workshop Report—Binghampton
Page 22
TABLE 2: WAYS RELIGION CONTRIBUTES TO HEALTH (EXERCISE 3: ROUND 2) Factors listed by Participants Factors Grouped Empowerment Promotes personal responsibility Self-Motivation Positive Self Esteem/image
Empowerment
Positive Holistic message Awareness Re. Problem issues Monthly Health tip sheet
Education
Relationships
Patients/ Health Care Providers have a service with not being alone in receiving or giving (at CCHS)
Relationships
Providing healthcare, counseling, and services Hope in Health Care - Higher Beliefs (at CCHS) Weekly Fitness program
Breaks down the love affair that Americans have with medical technology
ACKNOWLEDGMENTS We gratefully acknowledge the support of Paula Jacobson and the Methodist
Healthcare Foundation, Cerner Corporation, and CIGNA for their grant funding and interest and passion for the Memphis community. We wish to thank the
Urban Child Institute, Cindy Martin and the Shared Urban Data System for their contributions to the GIS portion of this work. Also, we thank Dr. Ruthbeth
Finerman, the University of Memphis Department of Anthropology, and the many graduate students who worked to help staff the workshops and to compile the
database and GIS maps.


















