
Meetings 2012 - Primary Care Dermatology Society
20
The recent summer meeting in Warwickshire was an educational and social success and enjoyed by delegates and sponsors alike. The numbers however were less healthy and your committee have therefore decided to concentrate such meetings in major centres and to move the timing of this summer two day meeting to the spring when the pressure of holidays interferes much less. In addition we note the popularity of international speakers especially on dermoscopy which provided us with our biggest audience so far earlier this year. We have scheduled the main 2 day meeting next year for March 16th/17th in central Manchester when we are pleased to confirm the return of Professors Argenziano and Iris Zalaudek to continue their dermoscopy course and in addition there will be parallel sessions of more general dermatological interest for those less interested in dermoscopy. Delegates will be able to dip in and out as they wish. Please watch the website and email/postal invitations for more details in the Autumn. Please also consider passing on such notifications to your partners and colleagues who may be interested and/or in need of dermatological stimulation (whoops, that sounds like I am suggesting some form of massage therapy!) Advertising in the medical media is extremely expensive and we would rather spend our resources on educational events than on publishers profits so we rely on you, our members to help to promulgate the society, its ideals and advantages especially delivering quality education at reasonable cost. Primary Care Dermatology Society Autumn 2012 Bulletin pcds.org.uk Chairman’s Report The PCDS Trustee Committee Mr Peter Lapsley Dr Tom Poyner Dr Stephen Hayes Dr Jane Rakowski Gladys Edwards Sandra Webb Dr Andy Jordan
Transcript of Meetings 2012 - Primary Care Dermatology Society

The recent summer meeting in Warwickshire was an educational and social success
and enjoyed by delegates and sponsors alike. The numbers however were less
healthy and your committee have therefore decided to concentrate such meetings in
major centres and to move the timing of this summer two day meeting to the spring
when the pressure of holidays interferes much less. In addition we note the
popularity of international speakers especially on dermoscopy which provided us
with our biggest audience so far earlier this year.
We have scheduled the main 2 day meeting next year for March 16th/17th in central
Manchester when we are pleased to confirm the return of Professors Argenziano
and Iris Zalaudek to continue their dermoscopy course and in addition there will be
parallel sessions of more general dermatological interest for those less interested in
dermoscopy. Delegates will be able to dip in and out as they wish. Please watch the
website and email/postal invitations for more details in the Autumn.
Please also consider passing on such notifications to your partners and colleagues
who may be interested and/or in need of dermatological stimulation (whoops, that
sounds like I am suggesting some form of massage therapy!) Advertising in the
medical media is extremely expensive and we would rather spend our resources on
educational events than on publishers profits so we rely on you, our members to
help to promulgate the society, its ideals and advantages especially delivering quality
education at reasonable cost.
Primary Care Dermatology Society Autumn 2012
Bulletinpcds.org.uk
Chairman’s Report
The PCDS Trustee Committee
Mr Peter Lapsley Dr Tom PoynerDr Stephen Hayes Dr Jane RakowskiGladys EdwardsSandra Webb Dr Andy Jordan

Your requests and advice as to topics, good speakers and venues etc., is always
valuable and we are particularly keen to hear from those who do not regularly attend
meetings since we may not be providing what you want or need. Please let us know.
Something new is a joint Essential Dermatology meeting with the RCGP in the
Oxford region on 29th November which we hope represents a collaboration for future
development and we would be interested in talking to other regions of the RCGP.
Although I am not by inclination a reader of horror stories I always read the
“Cautionary Tales” in my recent MDU magazine. I was struck by a skin case that
went wrong but because the GP operator of a possible BCC on a woman’s back had
adhered to NICE and local guidelines the case was successfully defended. The
circumstances involved warfarin, valvular heart disease and subsequent bleeding and
infection eventually causing endocarditis. We may call them “guidelines” but failure
to follow them could result in expensive and distressing consequences even if
adherence does not guarantee perfection. My only question required the date of
surgery and the accreditation of the GP since a possible BCC should be referred to a
community skin cancer surgeon or secondary care according to the NICE IOG for skin
cancer. I wonder if the GP had a dermatoscope and the ability to use it? If not I could
recommend training provided by a well - known primary care organisation!
I have been informed that Leo Pharma are currently launching their Give your skin a
feel campaign which may involve some of you in promoting the awareness of skin
lesions as well as sun protection but many more are likely to receive patients with
lesions for diagnosis who have responded to this campaign. We would be interested
to hear of any consequences of such media emphasis.
I am delighted to inform you all of the MBE presented to Dr Julia Schofield for
services to dermatology. A more worthy recipient I could not imagine. She has long
supported the PCDS, provided clear and stimulating lectures and involved us in many
standard and accreditation stakeholder committees in which she has had a major
role. We congratulate her.
Stephen Kownacki
Executive Chair

Editorial Spring 2012
I hope that everyone has had a fantastic Summer. Having
just returned from a lovely 2 weeks in the South of France
I’m finding the weather outside is a little depressing. At
least I can now go for a run without fear of sunburn or
dehydration. It has been a really exciting Summer, starting
with our Summer meeting in Kenilworth. We had some
excellent speakers and it was particularly great to welcome
Dr Ralf Hartmann and his family, from Berlin, who gave a
fascinating talk about his experiences in Afghanistan. Then
came the spectacle that was the Olympics. There obviously
was a great atmosphere at the Olympic Park greatly enhanced
by Great Britain doing so well in the medals table. Many of us
are now feeling bereft and wondering what we will do as the
evenings draw in. Never fear, this edition of the Bulletin is well
worth a read!
Please find time to have a peek at Bob Sarkany’s article on
photodermatoses. It doesn’t disappoint in making a very
difficult subject seem very easy. Julian has been squirreling
away in piles of journals and done an excellent summary of the
salient points to save you time reading them yourselves. Iain
has given us some snippets from his travels in Rwanda and
4
promises more interesting cases in future editions. Sorry, in
advance for the jokes that come with the articles… There are
also more sewing tips from Christy and a short tutorial on
dermoscopy.
For future editions, Frances Humphreys has promised me an
article on urticaria made easy, everyone’s heart sink subject.
Many of you will have seen Ivan Bristow give some excellent
and humorous talks on podiatry. I have an article up my sleeve
by him for the next edition, which won’t disappoint.
If anyone has any ideas of interesting articles or case histories I
would be really happy to receive them via [email protected]
Finally an apology to Dr Jon Goulding and any observant
readers who may have noted that there was a photo of
calciphylaxis mimicking vasculitis and not of bullous change
with incipient skin necrosis, as stated,in his last article on
cutaneous vasculitis.Helen Frow
Dr Ralf Hartmann and his daughter join committee and society members for pre - dinner drinks at the Summer Meting in Kenilworth
5
Dermoscopy Tutorial
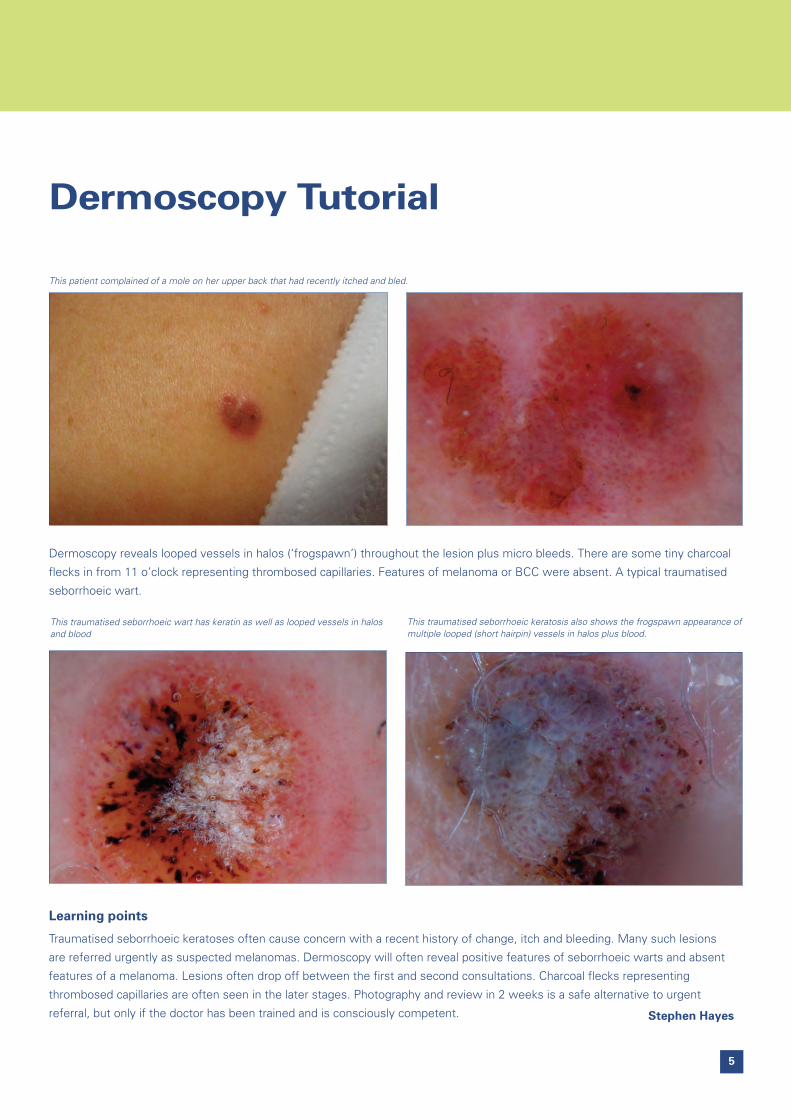
This traumatised seborrhoeic wart has keratin as well as looped vessels in halosand blood
This patient complained of a mole on her upper back that had recently itched and bled.
This traumatised seborrhoeic keratosis also shows the frogspawn appearance ofmultiple looped (short hairpin) vessels in halos plus blood.
Dermoscopy reveals looped vessels in halos (‘frogspawn’) throughout the lesion plus micro bleeds. There are some tiny charcoal
flecks in from 11 o’clock representing thrombosed capillaries. Features of melanoma or BCC were absent. A typical traumatised
seborrhoeic wart.
Learning points
Traumatised seborrhoeic keratoses often cause concern with a recent history of change, itch and bleeding. Many such lesions
are referred urgently as suspected melanomas. Dermoscopy will often reveal positive features of seborrhoeic warts and absent
features of a melanoma. Lesions often drop off between the first and second consultations. Charcoal flecks representing
thrombosed capillaries are often seen in the later stages. Photography and review in 2 weeks is a safe alternative to urgent
referral, but only if the doctor has been trained and is consciously competent. Stephen Hayes

6
My previous articles have set out to address what I
consider to be some essential aspects of skin surgery.
The final stage of your procedure and, just as crucial is
how you are going to close the wound once you have
performed your biopsy or surgical excision. It is this skill
which significantly affects the cosmetic outcome and the
suturing process should not be underestimated. It is
important not to relax mentally at this stage but take enough
care to ensure the wound is closed correctly. Bear in mind
that the scar may be the only detail of the operation which
concerns your patient.
The reason for suturing any wound is to bring opposing skin
edges together to allow the healing process to take place.
Your decision about suture technique, suture placement
and type of suture depends on the anatomical site, depth of
skin and degree of tension. A badly designed excision
which creates difficulty bringing skin edges together or,
over tightening the sutures will cause strangulation at the
wound edges. Excessive wound tension and strain
following suturing also increases the risk of wound
dehiscence and will inevitably lead to a poor cosmetic
result.
Photo 1 Photo2
Sewing with ChristyChristy’s tips and advice for safe andefficient operating

7
In this first of two articles I will look at the instruments and
materials required for suturing as well as some basic principles
and techniques. Suturing methods and indications for use will
be covered in the next issue of the journal.
When thinking about instruments the suture holder has a very
important function in your instrument pack and ideally should
be of good quality. The suture holder not only allows you to
hold onto the needle itself but it is also used to grasp the
suture filament when tying knots. Suture filaments can be
extremely fine, the 6-0 Ethilon used on the face, is the same
diameter as human hair. Some disposable instruments are not
delicate enough to hold this fine thread resulting in the filament
slipping through the jaws of the holder. As I have said in
previous articles try to invest in the best instruments within
your budget as they will help to make skin surgery a lot less
frustrating.
Suture holders have a ratchet mechanism for grasping the
needle, only close the holder to the first click of the ratchet as
excessive pressure can damage both the needle and the
needle holder. The correct way to hold the suture holder is to
put your thumb and forth finger through the holes in the
handle, use the middle and little fingers to stabilise the base
and extend the index finger along the suture holder towards
the tip to guide the needle accurately (photo 1). Alternatively
the needle holder can be held in the palm (photo 2) this is a
useful technique to use when the needle is entering and
exiting the skin. The palming technique allows 360 degree
control of needle movement making it much easier to enter
the needle into the skin at 90 degrees. Holding the suture
holder in the conventional way can force your wrist, elbow and
shoulder into very awkward positions. Suture needles are
usually curved and a quick rotational movement of the wrist is
needed to direct the needle where you need it to go.
In skin surgery, two main types of needle are used; cutting or
reverse cutting. The reverse cutting needle is less likely to tear
the skin edges due to its design as it presents a flat triangular
section to the skin rather than a sharp tip. It is worth
mentioning the prime reverse cutting needles which are less
traumatic to the skin as they have a smaller cross sectional
body, but they are of course more expensive. Loading the
suture needle correctly is essential. The needle is made up of
three sections; the sharp tip which penetrates the tissue, the
mid section or body and, the swage which is the thick end
where the suture material is attached. The needle should be
grasped close to the tip of the suture holder jaw, right angles
to the jaw and approximately 2/3 from the tip of the needle
(photo 3). If the needle is incorrectly inserted into the suture
holder there is an increased risk of bending the needle,
difficulty in penetrating the skin and poor angle of penetration.
Photo 3 Photo 4

8
The skin needs to be stable to allow entry and
exiting of the needle. Depending on preference a
fine toothed forceps or skin hook can be used to
steady the skin edges but, be very gentle. Avoid
using your fingers to stabilise the skin when exiting
as there is a risk of needle stick injury, use your
forceps. Grasp the needle with your forceps once
through the skin taking care not to grab the tip
which will result in damage to the needle.
The needle should always enter the skin at a 90
degree angle as this minimises trauma and ensures
capture of the full skin thickness. Once the skin has
been penetrated rotate the wrist so that when
exiting on the opposite side you take a ‘tissue bite’
of the same depth. Try using the ‘palming method’
described earlier as this allows for greater for
dexterity. Wound edges which meet at the same
level minimise the risk of ‘stepping’. Always insert
the needle 3 to 4mm from the wound edge and exit
at the same distance on the opposite side, placing
your suture less than 2mm from the wound edges
can result in necrosis. The spacing of each suture
along the length of the wound depends on location,
degree of skin tension and the condition of the skin.
Generally on the head and neck a 3 to 5mm gap
between sutures is average but, if there is a high
degree of skin tension or if the wound lies over a
joint then the distancing is less.
Once you are happy with the placement of your
suture it must be held in position by tying a surgical
knot. Tying knots with your instruments is
preferable as it uses less suture material and
reduces the likelihood of over tightening. In skin
surgery the square knot is commonly used as it cuts
down the risk of your knot slipping or unravelling
following surgery. The easiest way to describe this
is to imagine you are looking at the wound as a
vertical line in front of you. Start suturing from the
right hand side of the wound and exit on the left,
the loose end of the suture will now be on the right
hand side. Pull the suture gently through the skin
leaving the loose end approximately 2-3 cm long,
release the needle, and allow this to fall onto the
sterile drape. Place the suture holder between the
two ends of the thread. Rotate the thread clockwise
around the needle holder twice, then take hold of
the short, loose end of the suture and pull through
the loops crossing your hands so the loose end of
the suture and the end attached to the needle swap
sides. As gently as possible pull the wound edges
together.
The next step is virtually the same, place the suture
holder back between the two threads, the loose
end is on the left hand side and the needle end on
the right hand side. Now do exactly the same, but
perform a single rotation of the thread counter
clockwise around the suture holder. Again grab the
loose end pull through the loop and swap hands,
tighten the knot enough to approximate not
strangulate the wound edges. Repeat step one with
a single rotation for the final ‘throw’. This technique
automatically creates the square knot designed not
to slip. This is the most conventional way of tying
surgical knots; sufficient for polyfilament sutures
such as Silk or Vicryl. When using a single filament
nylon suture like Prolene you may want to add an
additional single throw to make sure the knots are
fully secure. Place the knots to one side of the
wound, leaving them directly over the top of wound
will increase the possibility of post op infection.
When you are not using the suture needle it is very
important to store it safely to prevent accidental
injury, this is achieved by ‘parking’ the needle in the
suture holder. Clip the needle on the ‘swage’ with
the needle point towards the body of the holder, do
not grasp the tip in case you need to use the suture
again (photo 4).
The suture packet holds a lot of information for the
surgeon about the needle and thread/filament
(photo 5). When choosing the suture needle a
Photo 5
9
reverse cutting or, reverse cutting prime needle
would be my first choice, they are less traumatic
and therefore less likely to tear the delicate skin
edges. This pack contains a 3/8 of a circle needle
which is ideal for skin surgery and 19mm indicates
the needle diameter. The illustration of the needle
on the outer packaging is true to size. Underneath
this illustration is the information about the filament;
in this case it is 45cms in length and the number,
5.0 signifies the diameter.
The diameter of your suture is dependent on the
anatomical site. My practice is to use either 6.0 or
5.0 for the face, head and neck area as this
diameter produces very little scarring there is also
less skin tension around the face. On the trunk and
legs a thicker thread is required and here a 3.0 or
4.0 would be more suitable. The smaller the
number on the packet, the thicker the thread, each
size increases in thickness by approximately 50%
which is worth bearing in mind when thinking about
scarring. Finally, the product code on this pack of
5.0 Ethilon is W1618, there are many variations of
needles and sutures so be careful when ordering.
Suture material falls into basic groups;
Non-absorbable or Absorbable, Monofilament or
Polyfilament.
Non-absorbable sutures retain their strength
indefinitely. For skin surgery my preference would
be a nylon monofilament such as Ethilon or Novafil
(Ethilon is generally considered to be a superior
suture material). Another option is Prolene which is
a stronger suture however, it is more elastic and
slippery making it difficult to handle and less user
friendly. When first taking your nylon
(monofilament) suture out of the packet it is worth
giving the thread a good tug to get rid of the elastic
memory which can make suturing awkward as it
curls and tangles. The advantage of monofilament
sutures is that they are easier and less traumatic to
insert and remove on the other hand they are more
difficult to knot.
Polyfilament sutures are made from braided
materials making them stronger and easier to
handle, the fibres are twisted together to give extra
strength. There is a higher infection risk with
polyfilament sutures as bacteria can collect
between the braids however, this has been
minimised in those with an anti-microbial coating
such as Vicryl plus. Silk sutures are rarely used now
as they can cause excessive scarring, whenever
possible do not use a Silk suture on the face.
Absorbable sutures widely available are Vicryl which
is polyfilament or the single filament Monocryl, a
transparent suture that can be difficult to see
however, dyed variations available.
Vicryl rapide is a useful polyfilament suture as it is
designed to be absorbed within 8 to 14 days. It can
be used as a superficial skin suture for interrupted
suturing or for sub dermal techniques. The quick
absorption rate makes it ideal for use in children or
genital areas where suture removal causes anxiety
or embarrassment, it can also be useful for the
older person where transport or mobility problems
can be an issue.
Remember your choice of suture and needle is
determined by the location of the wound, thickness
of the skin and the amount of tension to bring the
wound edges together.
Look out for suturing methods and indications in the
next issue.
Christy Chou
Trust Surgeon
Department of Plastic Surgery
University Hospital of Durham
and Primary Care Skin Surgeon
Darlington and County Durham PCT

10
Photosensitivity is a common presentation in the
Dermatology Clinic and the management of these patients
poses unique challenges.
In practice, there are two ways that photosensitivity can
present. Patients who complain of a reaction to sun exposure,
and patients with a rash which the Doctor notices is in a
light-exposed distribution.
This review will provide a framework to begin to diagnose and
manage photosensitive patients.
Why does sunlight cause so much skin disease?
Ultraviolet radiation (UV) makes up a small part of sunlight but
UV is uniquely damaging to the skin (Fig. 1). UV chemically
reacts with, and alters, proteins, lipids and, more worryingly,
DNA in skin cells. Although there is a sophisticated and
effective set of defences in the skin against UV damage, when
these responses go wrong, the photosensitive diseases result.
Photodermatoses versus photoaggravateddermatoses
Photosensitive skin diseases are divided into two groups. The
photoaggravated dermatoses are ‘normal’ dermatoses which,
in some patients, worsen with sun exposure. The most
common is atopic eczema which flares after sun exposure in
15-20% of patients. Many other dermatoses are sometimes
aggravated by ultraviolet, from lupus which is almost always
photoaggravated, to pemphigoid where photoaggravation is
rare (Table 1).
The photodermatoses (Table 2) are true sun-induced skin
diseases: they do not occur in the absence of sunlight.
Patients with photoaggravated dermatoses are managed for
the underlying dermatosis, apart from the extra UV
photoprotection they require. This review will cover the
management of patients with photodermatoses.
What types of diseases are the photodermatoses?
Most of the photodermatoses are inflammatory diseases. This
is less mysterious than it might seem. Ultraviolet has profound
effects on the skin’s immune system. For a few days after UV
exposure, immune responses in the skin are suppressed. UV
alters molecules in the skin which can then appear ‘foreign’ to
lymphocytes, potentially inducing autoimmunity. So UV can
Managing the Photosensitive Patient
Dr Robert Sarkany FRCP MD
Head of Photodermatology, St John’s Institute of Dermatology, London
Figure 1. Ultraviolet is the portion of the spectrum of light in sunlight which isuniquely damaging to the skin, and is the cause of much Dermatological disease

11
cause autoimmune and other inflammatory reactions. The
commonest inflammatory photodermatosis is polymorphic
light eruption. Chronic actinic dermatitis and actinic prurigo are
not rare. Solar urticaria and hydroa vacciniforme are
(fortunately) uncommon.
Not all photodermatoses are inflammatory. In drug
photosensitivity and porphyria, light directly activates
molecules in the skin (i.e drugs and porphyrins) to become
destructive. These are the ‘phototoxic’ photodermatoses.
Drug phototoxicity is very common.
The rarest photodermatoses are the DNA repair disorders.
Repairing the damage that UV in daylight constantly does to
keratinocyte and melanocyte DNA is crucial to prevent skin
cancer. Faulty DNA repair causes Xeroderma pigmentosum
and other severe inherited diseases.
The main photodermatoses ‘in a nutshell’
Inflammatory Photodermatoses
• Polymorphic Light Eruption: Affects 1 in 6 young women.
Causes itchy papules, plaques and vesicles. Often spares
the face and hands.
• Actinic Prurigo: commoner in children. Flares in summer.
Causes multiple small nodular prurigo-type lesions on the
arms and face, and sometimes a more confluent
eczematous rash on the face. Can be treatment resistant.
• Chronic Actinic Dermatitis: a severe exposed site eczema,
worse in summer. Can be lichenified and even
pseudolymphomatous and nodular. It is an allergic dermatitis
to UVB. Often associated with non-photosensitive contact
allergic dermatitis to multiple allergens. Commoner in the
elderly.
• Solar urticaria: rare and severe. Life-limiting urticaria on
exposure to daylight often even in winter. Generally in young
adults and may persist for decades and be
treatment-resistant.
• Photoallergic contact dermatitis: a light-dependent form of
contact allergic dermatitis. Presents with an acute eczema
starting within a day or two of sun exposure. Since the allergy
(in the UK) is usually to a sunscreen ingredient, it occurs only
where sunscreen has been applied.
• Lupus: subacute lupus (and sometimes systemic lupus) can
cause a PLE-like eruption, but it tends to persist longer than
PLE. Always think of lupus and check ANA in a photosensitive
patient.
• Hydroa vacciniforme: a severe inflammatory scarring
photodermatosis that affects young children and is often
treatment resistant. It usually resolves after two to three
years but can leave severe facial scarring.
Phototoxic Photodermatoses
• Drug photosensitivity: often presents with pain, redness and
swelling in exposed skin which persists for hours after sun
exposure. It is most commonly caused by tetracyclines,
non-steroidal anti-inflammatories, amiodarone, thiazides or
quinine. Drug photosensitivity is the great mimicker in
photosensitivity. Always take a drug history in photosensitive
patients.
• Erythropoietic Protoporphyria (EPP) (Fig. 2): inherited. Causes
severe pain and swelling of the hands and face within
minutes of summer sun exposure. The reaction is to visible
violet light. Diagnosed on blood test.
Table 1: The common Photoaggravated Dermatoses
Eczema:• atopic • seborrhoeic
Connective tissue: • lupus• Dermatomyositis
Infection: • herpes simplex
Other inflammatory skin diseases• Psoriasis• Rosacea• Actinic lichen planus• Erythema multiforme• Acne
Acantholytic diseases: • pemphigus, Grover’s, Darier’s
Pigmentary: • chloasma
Table 2: The photodermatoses
Immunologically based:• Polymorphic light eruption• Chronic actinic dermatitis• Actinic prurigo• Hydroa vacciniforme• Solar urticaria• Photoallergic contact dernatitis
Chemical photoxicity:• Exogenous: drugs• Endogenous: porphyrias
DNA repair disorders:• Xeroderma pigmentosum

12
• Porphyria Cutanea Tarda (PCT)(Fig.3): a metabolic disease
strongly associated with liver disease and haemochromatosis.
Causes fragile skin and blistering on the hands and face.
Accurate biochemical diagnosis is vital to exclude potentially
life-threatening variegate porphyria.
• Pseudoporphyria: a presentation of drug photosensitivity
which mimics PCT. Can also be caused by haemodialysis.
DNA repair disorders
• Xeroderma pigmentosum (XP): A rare inherited disease in
which the process of repair of UV-induced damage to DNA is
impaired. It causes multiple skin cancers and eye disease
from childhood, and a fatal degenerative neurological disease
in some patients. Early diagnosis is crucial so that absolute
and drastic UV photoprotection can be started as soon as
possible, which prolongs survival. Think of the diagnosis in
any child with exaggerated prolonged sunburn reactions, or
exaggerated early freckling in exposed skin, (rare versions
present in adults).
Managing the patient who complains of asun-induced rash
As every comedian knows, ‘timing is everything’. In patients in
whom there is no rash to see, the history is the key to
diagnosis. If the eruption flares up within seconds or minutes of
first going out in the sun, the diagnosis is most likely to be one
of the three causes of immediate photosensitivity:- drug
photosensitivity, solar urticaria or erythropoietic protoporphyria
(EPP). The other photosensitive eruptions tend to flare up a few
hours after sun exposure.
The classic presentations are:
Immediate photosensitivity (within minutes):
• Drug photosensitivity: pain , redness and swelling in
exposed skin which persists for hours after sun exposure.
Drug photosensitivity is the great mimicker in photosensitivity.
Always take a drug history in photosensitive patients.
• Solar urticaria: itching with redness and swelling in exposed
skin, resolving within an hour once the patient gets away
from the sun
• Erythropoietic protoporphyria: onset in early childhood. Pain
and swelling on the hands and face which lasts 2-3 days.
Delayed photosensitivity (within hours):
• Polymorphic light eruption (PLE): itchy red papules,
sometimes plaques or vesicles, in exposed areas, lasting up
to 10 days
• Lupus: can present like PLE, but tends to last weeks or longer.
• Chronic actinic dermatitis: there may be no history of
photosensitivity, but there can be a history of flaring of
existing eczema which can last for weeks or until topical
steroids are applied.
• Photoallergic contact dermatitis: presents with an acute
eczema starting within a day or two of sun exposure. Since
the allergy (in the UK) is usually to a sunscreen ingredient, it
occurs only where sunscreen has been applied.
• Actinic prurigo: itchy papules appearing within hours of sun,
which persist for months. Commoner in children.
Figure 2. Oedema during an acute painful attack in achild with erythropoietic protoporphyria (EPP)Reproduced with permission from ref. 3
Figure 3. Porphyria cutanea tarda causes fragility and blistering. It is often the presenting feature ofliver disease or haemochromatosis. Reproduced with permission from ref. 3

• Porphyria Cutanea Tarda (PCT): the patient is usually not
aware of a link to sun exposure. Presents with fragility and
sometimes blistering with scarring and milia formation, on
the hands and face, worse in the summer.
• Hydroa vacciniforme: papules, bullae and pustules within
hours of sun exposure. Can take weeks to resolve and leave
vacciniform scars.
Managing the patient in whom the doctornotices that a rash is distributed in alight-sensitive distribution
In some photodermatoses the doctor will notice that the rash is
in an exposed site distribution. The patient may not be aware
that there is any link to sun exposure. This is often the case in
chronic actinic dermatitis and porphyria cutanea tarda. If a
patient has an exposed site rash, the hallmarks of it being due
to light are sharp cut-off at clothes lines, and sparing in
relatively shaded areas (below the chin, behind the ears, around
the eyes, under watch straps).
In patients where you suspect a connection to sunlight, always
ask whether it is better or worse in the sun and what happens
after bright sun exposure and on hot holidays. If the rash clears
up on the beach in Majorca, it is not a photodermatosis
whatever it may look like!
Exposed site eczema (Fig. 4): Dermatologists often see
patients with eczema which is predominantly in an exposed
site distribution. Although this may be due to photosensitivity
(photoaggravated atopic eczema, chronic actinic dermatitis or
photoallergic contact dermatitis), there are other possibilities.
Contact allergic dermatitis to an airborne allergen affects
exposed sites, and sometimes normal atopic eczema just
happens to be worse on the face and hands (and seborrhoeic
dermatitis tends to be facial). Careful history taking and
relevant investigations (patch tests, photopatch tests,
phototests) are the key to accurate diagnosis and effective
treatment.
Investigating patients with suspectedphotosensitivity
Blood tests:
• Always check the ANA: along with drug photosensitivity,
lupus can present in many ways and is important not to
miss.
• Have a low threshold for checking plasma porphyrins: this is
a good screen for the cutaneous porphyrias. It is essential in
any immediate photosensitivity and any bullous
photodermatosis
• If you suspect actinic prurigo, check the HLA class 2 type:
HLA DR4 and DRB1*0407 are strongly associated with this
disease.
Patch tests: important in any exposed site eczema, (a) to
exclude a non-photosensitive contact allergic dermatitis as the
diagnosis; (b) because Chronic actinic dermatitis, is usually
accompanied by non-photosensitive contact allergies.
Photopatch tests: the diagnostic test for photoallergic contact
dermatitis.
Phototesting: only available in specialist Photodermatology
Units. It is the diagnostic test for chronic actinic dermatitis
and solar urticaria. It can be helpful in other photodermatoses.
It involves challenging small areas of skin on the back with a
series of different doses of each wavelength of UV light in
turn and assessing the response 24 hours later
(‘monochromator test’). Patients’ skin is also exposed to
broader spectrum ‘sun-like’ UV in order to induce the eruption
(‘provocation test’).
Treating the photosensitive patient
Photoprotection
The sunscreen must protect against the wavelength causing
the disease. The SPF (sun protection factor) only measures
protection against short wavelength UV (UVB). For many
photosensitive patients (including most PLE patients), longer
wavelength UV (UVA) is the main problem, so a broad
spectrum sunscreen with high UVA protection (as well as a
high SPF) is needed. UV sunscreens do not protect against
visible light, and for visible light photosensitivity (EPP and
Figure 4 (a, b and c). Exposed site eczema has a wide differential diagnosis ofphotosensitive and non-photosensitive causes. Careful history taking is crucial.The relative sparing here around the eyes and under the chin is a clue that thiscase is photosensitive. This patient had chronic actinic dermatitis.
13

14
some cases of solar urticaria) a visible light sunscreen is
necessary and blocks out blue and violet light.
Photoprotection is not just about sunscreens. Sun avoidance,
broad-brimmed hats, long sleeves and long trousers all play a
vital role. In the most severe photosentivity, transparent
adhesive UV films can be applied to house and car windows.
Treatment of the common photodermatoses
PLE: Short causes of prednisolone (25mg od for 5 days) will
control the bouts. For patients who suffer severe and
frequent bouts of PLE in the spring and summer, TL01 UVB
desensitisation in the early spring can be an effective, though
not always straightforward, option.
Chronic actinic dermatitis: this can be severe, even in winter,
and despite vigorous photoprotection and topical steroids.
Some patients require systemic immunosuppression though
often only in summer.
Actinic prurigo: even with excellent photoprotection this often
requires systemic therapy or UV desensitisation in the early
spring. In some treatment resistant cases, oral thalidomide is
effective.
Solar urticaria: photoprotection can be difficult in cases
caused by visible light. Antihistamines, often in combination
and at high doses, may be effective. Second line treatments
include ciclosporin, IV immune globulin, plasmapheresis and
omalizumab. UV desensitisation is possible but exceptionally
difficult. In some cases,solar urticaria is a very severe,
disabling, treatment-resistant and persistent disease.
Erythropoietic Protoporphyria: in the absence of any more
effective treatment, photoprotection is critical but difficult
because the painful attacks are caused by visible violet light.
Regular monitoring of liver function tests is crucial since
rapidly progressive liver disease requiring liver transplant is an
unpredictable complication in 1% of patients.
Xeroderma pigmentosum (XP): Early diagnosis is crucial so
that absolute and drastic UV photoprotection can be started
as soon as possible. This prolongs survival in this severe
inherited childhood disease in which minimal UV exposure
causes multiple skin cancers from childhood. Think of the
diagnosis in any child with exaggerated prolonged sunburn
reactions, or exaggerated early freckling in exposed skin, (rare
versions present in adults).
Photoallergic contact dermatitis: the diagnosis will not be
made unless it is thought of and photopatch tests carried out.
Avoidance of the relevant sunscreen photoallergen cures the
problem.
Hydroa vacciniforme: affects young children and can be severe
and treatment resistant. Rigorous UV protection and UV
desensitisation are the mainstays of treatment. It usually
resolves after two or three years, but can leave severe
vacciniform facial scarring.
Porphyria Cutanea Tarda: look for an underlying cause
(haemochromatosis, hepatitis C, alcoholism, HRT or the OCP).
Responds to low dose chloroquine or venesection but relapse
once off treatment is common.
Vitamin D in Photosensitive patients
Many photosensitive patients are vitamin D insufficient or
deficient as a result of the necessary photoprotection. Vitamin
D does need to be monitored and supplemented when
necessary.
Learning points
• Ultraviolet in sunlight is a major environmental stress on the
skin
• Careful history taking is vital to diagnose the photodermatoses
• Timing of photosensitive reactions is particularly important
diagnostically
• Drug photosensitivity and lupus can both mimic other
photosensitive diseases.
• Phototesting is the diagnostic test in Chronic Actinic Dermatitis
and Solar Urticaria
• First line treatment in Polymorphic Light Eruption is a broad
spectrum sunscreen, with oral prednisolone for the bouts
• A child with pain on sun exposure usually has Erythropoietic
Protoporphyria.
• Exaggerated freckling, with or without exaggerated sunburn,
is the usual presentation of Xeroderma Pigmentosum.
• Porphyria Cutanea Tarda is often a sign of internal disease.
• The SPF of a sunscreen only tells you about its UVB protection.
Further Reading
1. Photodermatology. Eds. Ferguson J and Dover JS.
Manson Publishing, London (2006)
2. Photodermatology. Eds. Lim HW, Honigsmann H, Hawk
JLM. Informa Healthcare, New York (2007)
3. Sarkany RP.Making sense of the porphyrias. Photodermatol
Photoimmunol Photomed.24:102-8. (2008).
We would like to thank Wiley publishing for allowing us to use
the 2 images used in reference 3.

15
What a year we’ve had for big events
but the biggest has yet to come!
The Queen’s Diamond Jubilee – a mere
bauble!
The European Championships – a mere
footie note!
The Olympics – a mere bagatelle!
The Annual Scottish PCDS meeting
at the Dundee Apex on 10th/11th
November – now you’re talking…..or
if you’re not talking at least you’re
listening to some sparkling speakers
and some great topics.
Book your place now.
Dundee – the city that has more
Premier League Football teams than
Glasgow and Father’s Day causes a lot
of confusion. (Apologies to everyone
from Dundee but I got these from a
St Johnstone fan.)
Other educational events are the
Dermoscopy workshop in Glasgow 5th
September followed by the Essential
Dermatology day in Stirling on the 6th.
One of the key objectives of the PCDS is
to encourage an interest and provide an
arena to promote and establish a clearer
understanding of dermatology in primary
care. So once again I would urge anyone
who hears of anything which looks
interesting in the dermatological
educational field to let me know at
[email protected] and I will
try and disseminate it to appropriate
places.
The Dermatology Council for Scotland
met on 7th June where it was reported
that the update to the melanoma SIGN
Guidelines will probably commence in
2013 and that the initial scoping work
was underway for the guidelines on SCC.
The Council continues to campaign for
inclusion of dermatological conditions
into QoF and it hopes to provide data
from the Psoriasis Integrated Care Clinics
that have been held in Scotland to add
weight to the recommendations of SIGN
121 – “The diagnosis and management
of psoriasis and psoriatic arthritis in
adults.”
News from North of the Border
Skin Care Campaign Scotland continues
to contribute to Cross Party Groups of
the Scottish Parliament on psoriasis, skin
cancer and health inequality.
Dermatology in Practice is now back in
publication and the first hard copy of the
revamped journal has been sent out. If
you didn’t receive one you can register
and log in at
http://www.dermatologyinpractice.co.uk.
One final joke ….
Q. Two Dundee kids in a car without any
music - who is driving?
A. The policeman.
Iain Henderson

October 2012 – December 2012
So, what a summer eh? One or two
special events, a mixed bag of weather
and a few records broken. It’s a good
job that we have the journals to fall
back on to give us a bit of security in
these trying times...
I believe I may have mentioned before
Peace’s first law of human hair – there is
either too much, too little or it is in the
wrong place. A new guideline from the
BAD on the management of alopecia
areata1 is, therefore, a welcome sight to
start this article with. Less welcome is
the paucity of new recommendations for
alopecia is a singularly frustrating disease
to treat. Sadly, although a number of
treatments have been shown to induce
hair growth, none has been shown to
alter the long term course of the disease.
Topical and intralesional steroids remain
the mainstay of treatment options, but
the latter are not appropriate in rapidly
progressive or extensive disease. It is a
sad reflection on our impotence to treat
this distressing condition that no
intervention reaches an evidence level
above concensus and case reports.
I include the next article to demonstrate
the lengths that researchers have to go to
to obtain evidence for our otherwise
accustomed activities. A team from Brazil2
has been looking at the efficacy and
safety of topical antifungal agents. They
looked at a total of 4443 articles and
excluded all but 104 (slightly over 2%!) as
unsuitable for inclusion in this meta-analysis. After all this careful work, their
conclusion is that, although all agents studied were better than placebo, none was
statistically more effective than any other. So now we know.
To continue a slightly depressing theme, oral lichen planus (OLP) is another
common, well, relatively common condition without a recognised treatment
regime. It is 10 years since the last Cochrane review of treatment for OLP was
published, so this was updated by a multinational team3. Sadly, once again, no firm
conclusion was reached. Topical corticosteroids are considered the treatment of
choice and yet there is no trial evidence of their efficacy. The authors reach the
conclusion that, as topical corticosteroids are recognised as a first line treatment,
it would be considered unethical to perform a randomised, controlled trial to prove
their efficacy. Such are the machinations within dermatological research. Of other
treatments studied, topical calcineurin inhibitors, including ciclosporin, could not
be recommended on the balance of evidence, but there was weak evidence to
suggest that Aloe Vera gel could be useful in reducing pain and some clinical signs
of OLP.
Time for a good scratch. Another multinational team has been looking in to the
psychology of scratching4 – the rationale appearing to be that, although it has long
been recognised that scratching an itch is a pleasurable experience, no one has
really looked at why this may be so, and, indeed, if scratching is more pleasurable
at one body site compared to another. A word of caution, however. The
experiment design involved induction of itch using cowhage spicules (individually
counted cowhage spicules, no less) and then scratching was performed by the
investigator using a cervical cytology brush. Nonetheless, conclusions were
reached. The forearm has traditionally been used as the preferred site of itch
investigation, but it was found that itch, itch intensity and pleasurability ratings
were considerably higher on the back and the ankle of test subjects. This also
demonstrated that the more intense the itch, the more pleasure could be obtained
from having it scratched. The next studies suggest the scalp and the anogenital
region as future test sites. I think I may pass on that one, the mental image is not
too pleasant.
We are often reminded of the ‘tsunami’ of skin cancers that are approaching our
troubled dermatological shores. A small, but significant, part of this deluge comes
from non melanoma skin cancers in organ transplant recipients. As these patients
Journal Watch
16

often grow multiple synchronous lesions, a study5 – the first such published –
looking at the use of photodynamic therapy to treat selected basal cell carcinomas
is to be applauded. At first sight, it all appears good – only one recurrence was
reported in the 18 patients studied – but the number of test subjects was small
and the follow up period varied between 2 months and 4 years. A more rigourous
– and standardised - study needs to be performed before this could be considered
a viable treatment option.
This may be the first time that restless leg syndrome (RLS) has been mentioned
in this bulletin, but my magpie eye was caught by an article6 showing that the
incidence of RLS in those suffering from atopic dermatitis is up to four times that
of a healthy control population. Although first described in 1685 as anxietas
tibarium, and more formally classified by Karl-Axem Ekbom in 1945, we have little
or no idea what causes RLS. It is worth, however, considering discussing it with
your atopic patients as their sleep may be disturbed by more than just itch.
A brief mention for the least surprising result of a systematic review7 – no
evidence could be found that homeopathy is an efficacious treatment for eczema.
Fancy!
Whilst I am both an advocate and an enthusiastic practitioner of the dark art of
dermoscopy, there are worrying signs that it is starting to move in to areas for
which it is not really ideally suited. In the first paper8, dermoscopic features of
lichen planus, psoriasis, pityriasis versicolor and dermatitis are delineated and
discussed. This, to me, is like trying to determine the make of car by closely
studying its paintwork. A return to holistic medicine seems timely... The second
paper9 looks at the dermoscopic evolution of melanomas that were identified after
long term monitoring. I’m sorry, but this seems madness – these melanomas
were monitored over the course of a year, and their evolution studied. Although
the study was retrospective and, in most cases, the lesions were only identified
as melanomas after excision, I can’t help feeling this paper sends out the wrong
message. If it’s a melanoma after 12 months, it was a melanoma to start with.
The dermoscope should not be a tool that stops the excision of suspicious
lesions, but a tool to stop the wasteful excision of benign lesions. Rant over.
Another new topic – skin disorders surrounding stomas. These are remarkably
common, representing perhaps a third of all visits to stoma nurse clinics. It is not
unreasonable to consider contact dermatitis as being significant in this group –
occlusive, adhesive appliances applied directly to the skin. This study10, however,
did a load of patch tests on sufferers and found a positive result in only around
5% of ostomates (a new word to me , too). More likely is an irritant dermatitis to
the contents of the bags and the cleansers that it is necessary to use.
Imiquimod cream is licensed for the treatment of superficial basal cell carcinomas,
so a study looking at its use in nodular lesions seems to be of interest. A
randomised, controlled study11 looked at pretreating nodular lesions in preparation
for Mohs surgery. Four weeks of Imiquimod reduced the size of the surgical
defect, reduced the number of stages of Mohs that were necessary and
significantly reduced the reconstruction time. Although the authors recommend
further research to look into cost effectiveness, it is hard to believe that this will
not be seen to be of great interest in future. Watch this space.
As ‘any ful knos’, much of what we perceive to be treatment failure actually
represents poor compliance with the prescribed medication. Methotrexate is a
drug that seems to have both a variable
response and a variable side effect
profile. The reasons for this variability in
toxicity and response are poorly
understood – my reader will remember in
the last bulletin we mentioned genetic
variability in response. A new study12
looks at the presence of Methotrexate
polyglutamates (Methotrexate to which
glutamic acid is sequentially added) in red
blood cells. These were found to be
present early in therapy and then reached
a steady state with continuing therapy. It
was not the scope of the study to
determine if these were a measure of
clinical response, but they do seem to be
a good marker of patient compliance.
So there you have it. It always feels like
an Olympian task to summarize these
August journals. This summer, that has
been more apt than ever. Enjoy!Julian Peace
References1. Messenger et al – British Association ofDermatologists’ guidelines for the management ofalopecia areata 2012. BJD2012:166;916-926.
2. Rotta et al – Efficacy and safety of topicalantifungals in the treatment of dermatomycosis: asystematic review. BJD2012:166;927-933.
3. Lodi et al – Interventions for treating oral lichenplanus: a systematic review. BJD2012:166;938-947.
4. Bin Saif et al – The pleasurability of scratching anitch: a psychological and topographical assessment.BJD2012:166;981-985.
5. Guleng and Helsing – Photodynamic therapy forbasal cell carcinomas in organ transplant recipientsCED2012:37;367-369.
6. Cicek et al – Increased frequency of restless legsyndrome in atopic dermatitis. CED2012:37;469-476.
7. Ernst – Homeopathy for eczema: a systematicreview of controlled clinical trials.BJD2012:166;1170-1172
8. Lallas et al – Accuracy of dermoscopic criteria forthe diagnosis of psoriasis, dermatitis, lichen planusand pityriasis rosea. BJD2012:166;1198-1205
9. Terushkin et al – Changes observed in slowgrowing melanomas during long term dermoscopicmonitoring.BJD2012:166;1213-1220.
10. Al-Niaimi et al – The relevance of patch testing inperistomal dermatitis. BJD2012:167;103-109.
11. Van der Geer et al – Imiquimod 5% cream aspretreatment of Mohs micrographic surgery fornodular basal cell carcinoma in the face: aprospective randomised controlled study.BJD2012:167;110-115.
12. Woolf et al – Methotrexate polyglutamates as amarker of patient compliance and clinical response inpsoriasis: a single centre prospective studyBJD2012:167;165-173.
17

18
Dermatology in Pigmented SkinA Rwandan Sojourn
When my practice found that we had to
entertain 3 GP registrars for the month
of February 2012 and that consulting
rooms were at a premium I unselfishly
gave mine up to go on a 3 week
sabbatical to Gahini Hospital in rural
eastern Rwanda.
My connections to Rwanda go back to
both my sons. In 2008 my elder son
was working for the International
Justice Mission in the capital, Kigali and
we visited him while he was there. With
the connections we made at that time,
my younger son then went on his senior
medical election in 2010 to Gahini
hospital.
Within clinical practice as a GP in an
increasingly multicultural practice and as
a hospital practitioner in dermatology I
have become aware of the challenges of
being presented with dermatological
conditions in pigmented skin. These
include the diagnosis of common skin
conditions as well as conditions more
peculiar to pigmented skin. There are
also specific challenges in the
biopsychosocial aspects that can
influence the management and
concordance of them.
I contacted Wim Schonbee the senior
doctor who my son shadowed while at
Gahini and he kindly agreed to host my
Gahini Hospital, rural eastern Rwanda Podoconiosis
wife who is a physiotherapist and me
during our stay. He informed me that
there is no specific dermatology service
in the hospital and dermatological
conditions are treated at the open access
daily general medical clinics.
The hospital had no mains water supply
but it did have internet connection!
This sabbatical, therefore, was an
opportunity to help at the hospital and set
up a teledermatology service.
I applied and was successful in receiving
the Alastair Short Memorial Travel
Fellowship ,which funded my airfare and
equipment for the service. This included
a compact SLR digital camera with a
macro attachment, illuminated
magnifying glasses and a battery
operated angle poise lamp. All the
batteries were rechargeable.
I contacted five Dermatology
Consultants who all agreed to receive
and give advice on pictures sent to
them by email and to whom I am
eternally grateful.
We also took out scalpels, blades,
sutures, crutches, aircast boots,
footballs and football jerseys.
Our first night in Rwanda was in Hotel
de Milles Collines, which is the Hotel
Rwanda and had our last mains supply
hot shower for 3 weeks.
For the next 3 weeks I shadowed the
inspirational Wim, a South African who
had worked as a GP in a township
practice in his home country. He first
entered Rwanda one month after the
genocide in 1994. He kept going back
and has been at Gahini hospital
permanently except for holidays for the
last 10 years. He upskilled as an
ophthalmologist but also had training in
obstetrics.
The first patient I saw was a
dermatological one on the way to the
hospital and we invited him to the clinic.
He had podoconiosis, a non-filarial
for malarial prophylaxis but there were
no topical treatments for acne. The
nearest equivalent of an emollient cream
was udder cream they used for milking
goats and cows.
While I was there Wim came up with
other uses for the camera such as
monitoring cervical dysplasia treatment
as the focal length of the macro lens
was the length of a speculum. He was
going to buy some small LED strip lights
to stick to inside the speculum for
illumination.
He was also going to use it to
photograph theatre packs for various
operations as the instruments were
often all piled into one pack and when
opened only 2 or 3 instruments may be
used and the rest had to be resterilised
again.
His wife Bertha helped at the local blind
school and disabled centre and was
using it to photograph hand made cards
for the centre’s website catalogue.
Over the next few bulletins I will present
a few of the conditions I encountered.
We may complain about the NHS and all
its faults but having worked for a short
period in rural Rwanda we should be
very grateful for it.
Iain Henderson
elephantiasis caused by walking barefoot
in volcanic dust. I took a picture of this on
my compact digital camera and sent it to
the consultants for comment on delivery,
picture quality etc.
I then sent them other photographs
during my stay taken on the SLR camera.
The size of these photographs was much
bigger at 5-6 Mb compared to around
1Mb on the compact camera but
although slower, managed to get through
to the consultants. Consent was verbal
through translation and the patient was
always shown the photograph to confirm
they were happy with it.
My first operation was a curettage and
cautery of a pyogenic granuloma on a
thumb. The next was a debridement of
what we thought was a soft tissue
infection of the foot from a snake bite.
I also helped out with hernia repairs,
deliveries including Caesarian sections
mainly at the wound closure stage.
During my stay I felt challenged
especially with the language barrier, lack
of resources and slowing to African time
but I admired the Rwandans’ patience
and fortitude.
Dermatological products were sparse.
Liquid paraffin was frequently used
making follicular conditions common.
Doxycycline was plentiful as it was used

PCDS 2012:
Skin Surgery13th & 14th OctoberCopthorne Hotel Newcastle
Scottish Meeting10th & 11th NovemberApex Hotel Dundee
2nd Floor, Titan Court, 3 Bishop Square, Hatfield AL10 9NA T: 01707 226024 F: 01707 226001 E: [email protected] W: pcds.org.uk
Forthcoming Meetings 2012
Members of the corporate membership scheme
Essential Dermatology2012:l 27th September PRESTON
l 11th October LEEDS
l 1st November MAIDSTONE
Essential DermatologyLevel 2 2012:l 4th October LONDON
l 22nd November MANCHESTER
PCDS 2013:
Spring meeting16th & 17th MarchManchester
Summer Meeting6th JuneLondon
Autumn Meeting12th SeptemberNottingham
Scottish Meeting9th & 10th NovemberEdinburgh
The New PCDS Website
At long last the new PCDS website is nearly upon us. It is due to be re-launched on Ist October2013. The domain address will remain unchanged.
The advantages of the new website are many and include the following:
n The clinical chapters
n The clinical contents have all been updated
n Each chapter is written in the same format
n Clinical images can be enlarged and / or downloaded
n Improved linkage between different chapters
n Events
n An easy guide to our various dermatological, dermoscopic and surgical meetings
n On-line payments for subscriptions and events
n An online ‘self-examination of moles’ toolkit that can be used by GPs to teach patients
Some features have been removed such as the forum, as these were not used except for spam!
The website is still in its evolution and there are some 20 new clinical chapters waiting to be added,and more after that.
I would like to take this opportunity to thank Neil Evans who is the technical wizard behind thewebsite and the PCDS committee, all of who work equally hard in their different capacities for thesociety, and who have supported me in the development of the new website over the past twoyears.
Dr Tim Cunliffe


















