Meehan autoimmune lung disease 2015Keystonmeehandraft.ppt 2015/Meeh… · nodules, deformities,...
43
Autoimmune Lung Disease RICHARD MEEHAN, M.D. Professor of Medicine Rheumatology National Jewish Health February 6, 2015 Property of Presenter
-
Upload
hoanghuong -
Category
Documents
-
view
220 -
download
5
Transcript of Meehan autoimmune lung disease 2015Keystonmeehandraft.ppt 2015/Meeh… · nodules, deformities,...

Autoimmune Lung Disease
RICHARD MEEHAN, M.D.Professor of Medicine
Rheumatology National Jewish Health
February 6, 2015Prop
erty o
f Pres
enter

Disclosures
Other: Expert witness for RA-related bronchiolitis case
Propert
y of P
resen
ter

Pulmonary Manifestations of Connective Tissue Disease
Spectrum of Clinical presentations of patients with suspected pulmonary manifestations of CTD
Diagnostic evaluation of patients with suspected CTD
Radiographic and histological variationsof Autoimmune lung disease
Treatment goals, therapeutic options, and monitoring of disease progression
Propert
y of P
resen
ter

Common CTD with pulmonary manifestations
Systemic Sclerosis: Diffuse or limited “Scleroderma” (dcSSc, lcSSC) or Systemic sclerosis sine scleroderma
ANCA + vasculitis: Granulomatosis with polyangiitis(GPA, formerly Wegener’s granulomatosis)
Rheumatoid Arthritis: + Anti CCP Abs may precede synovitis by > 10 years and lung involvement may be first manifestation of RA
Inflammatory myopathies: Polymyositis, Dermatomyositis and antisynthetase syndrome.
Propert
y of P
resen
ter

CTD with pulmonary manifestations
Eosinophilic Granulomatosis with Polyangitits(EGPA) ,formerly Churg-Strauss Syndrome
Sjogren’s Syndrome (SS) Primary or secondary Systemic Lupus Erythematosis (SLE) and or
primary antiphospholipid Antibody syndrome Undifferentiated (UCTD) or overlap syndromes Rare: Vasculitis, Relapsing Polychondritis
(RPC), Inflammatory Bowel associated airway disease, Ankylosing Spondylitis (AS)
Propert
y of P
resen
ter

Thoracic manifestations of CTD
Airways:
Large (RP, limited ANCA+ vasculitis)
small- cellular and constrictive bronchiolitis (RA, SLE, SS, SSC), peri-bronchial inflammation (SS) R/O sarcoid, HP or Inflammatory bowel disease
Vascular - PAH (SSC),Vasculitis (SLE, UCTD), Anticardiolipin Antibodies (Primary APL AB syndrome or SLE), Pulmonary Hemorrhage (SLE, ACL Ab syndrome)
Propert
y of P
resen
ter

Thoracic Manifestations of Connective Tissue Diseases
Serositis: pleural and pericardial (SLE, RA) Diffuse Lung disease/ILD: Non Specific Interstitial Pneumonitis (NSIP) seen with
most systemic CTDs), Usual Interstitial Pneumonitis (UIP) seen with SSc, RA, lymphocytic Interstitial Pneumonitis (LIP) seen in SS and SLE
Ground glass opacification Crytogenic Organizing Pheumonia (COP), Diffuse Alveolar Damage (DAD) due : SLE, RA, Vasculitis, PM/DM, r/o aspiration
Consolidation PM/DM, r/o infection Nodules/Cysts large nodules (RA), thin wall cysts (SS), large
cysts & nodules – (ANCA + Vasculitis), r/o infectious abscess especially non tuberculous mycobacterial disease
Propert
y of P
resen
ter

Common Symptoms of CTD Related Lung Disease
Pulmonary symptoms of CTD- ILD are usually progressive exertional breathlessness and non-productive cough.
Pleurisy is common in CTD and commonly seen on VATS bx as pleural inflammation.
Other symptoms : Unintentional weight loss, fevers, and glucocorticoid responsiveness of joint pain, weakness, myalgias and fatigue.
Pulmonary manifestation may precede the onset of CTD and immunosuppressive therapy can mask CTD manifestations. (Ref)
Propert
y of P
resen
ter

SSC: Recent onset Raynauds in pts > 40, sclerodactyly, digital ulcers, dysphagia or refractory GERD
PM/DM: Painless proximal muscle weakness, Rash, “mechanics hands.”
SS: Progressive oral or ocular sicca symptoms unrelated to medications, accelerated dental caries, parotid or lymph node enlargements, refractory sinusitis, dysphagia relieved with increased fluid ingestion, bronchiectasis and or nontuberculous mycobacterium disease.
RA: symmetrical small joint swelling and synovitis on examination
EGPA: Adult onset progressively severe and refractory Asthma , mononeuritis multiplex and/or small vessel vasculitis on cutaneous biopsy.
Common CTD Specific Manifestations
Propert
y of P
resen
ter

Physical Examination HEENT: Nasal Septal perforation (SLE,
Wegner’s), parotid or submandibular enlargement and adenopathy (SS), scleritis, (SLE, RA, AS, IBD, RPC) decreased tear production Schirmer’s (SS)
CR: Elevated JVP/ fixed slit P2 (PAH), Rubs (SLE), dry crackles bases (ILD), expiratory wheezes (EGPA, Bronchiolitis), neck stridor (RP, WG).
GI: splenomegaly (SLE, SS).
MSK: synovitis, contractures, tapered digits, ulcers, nodules, deformities, proximal muscle weakness.
Propert
y of P
resen
ter

Skin: SSC: telangiectasias, sclerodactaly, calcinosis,
digital ulcers and abnormal NCM SLE: malar rash, alopecia, levido, nasal septal
perforation, oral ulcers, retinal changes, hand rash,
Nodules: SLE, SarcoidPM/DM: Heliotrope rash and Gottron’s
papules, “mechanics hands”.EGPA: E nodosum, palpable purpura, foot
or wrist drop
Physical Examination
Propert
y of P
resen
ter

Laboratory Evaluation Is there evidence of systemic inflammation?↑CRP, ↑ ESR, ↓ albumin, SPEP (polyclonal gammapathy), anemia (normochromicnormocytic) , ↑ Plt count, and ↓ WBC, ↑CPK and/or aldolase (myositis)
Hep B S Ag, C Ab and HIV screen in all patients.UA: proteinuria/hematuria (nephritis)Antiphospholipid Abs, anti-Beta 2 Glycoprotein
1 Abs, lupus anticoagulants (RVVT or prolonged PT which fails to correct), false positive RPR increases risk for PE/DVT
Propert
y of P
resen
ter

Serologic Studies
Most serologic studies are neither adequate, nor sufficient to diagnose or exclude CTDs due to poor specificity and sensitivity.
ANA and ANA Profile: Ds-DNA, and Sm are very specific for SLE, SSA and SSB can be positive in ANA negative SS pts,
Anti-nucleolar pattern common in dcSScAnti-centromere staining pattern is seen often
in lcSScProp
erty o
f Pres
enter

Serologic Studies continued
Scl 70 (anti-DNA topoisomerase I)- correlates with diffuse scleroderma related ILD and is rarely a false positive
Jo-1 (aminoacyl-tRNA synthestase) seen in Polymyositis and dermatomyositis associated ILD. There are many other anti-synthetase Abs, full myositis Ab panel may need to be ordered
Anti neutrophic cytoplasmic antibodies c-ANCA, and anti PR3 Abs (proteinase 3, in granulomatosis with
polyangitis) p-ANCA and anti MPO Abs, (myeloperoxidase) seen in EGPA,
microscopic polyangitis and inflammatory bowel diseaseProp
erty o
f Pres
enter

Physiology Studies
Complete PFTS, 6 MWT needed as baseline prior to therapy and q 3-6 months.
If low DLCO is out of proportion to ILD disease severity on HRCT suspect PAH, PEs or cardiac shunt
Very high RV with progressive decline in air flow rates with a negative bronchodilator response or negative methacholine challenge is suspious for constrictive bronchioloitis.
Propert
y of P
resen
ter

Thoracic Imaging Findings HRCT Chest: Valuable at documenting pathologic
processes, severity and irreversibility and may guide decisions as to whether additional invasive diagnostic studies are indicated.
UIP-Honeycombing, mild GGO, bilateral, basal predominance, traction bronchiectasis, ( RA, SSC)
NSIP- rare honeycombing, predominant GGO (may be confluent), basal predominance, traction bronchiectasis (SSC, PM/DM, RA)
Propert
y of P
resen
ter

Imaging Studies
OP (Organizing Pneumonia)- multifocal consolidation, GGO, subpleural or peribronchovascular (PM/DM,RA)
LIP (Lymphocytic Interstitial Pneumonitis)-multiple thin walled cysts,peribronchovascular, GGO (SS, RA)
Bronchiolitis- bronchiectasis, mosaic air trapping on expiration (RA, SS, IBD)
Propert
y of P
resen
ter

Invasive Procedures VATS BX: Most Definitive IPF (idiopathic pulmonary
fibrosis) versus HP (hypersensitivity pneumonitis) versus UIP (fibroblastic foci) versus NSIP (homogeneous inflammation and fibrosis). Connective Tissue Disease more likely to contain lymphoid hyperplasia, pleuritis and perivascular collagen deposition.
Bronchoscopy: BX may identify granulomas (sarcoidosis or Hypersensitivity pneumonitis) or Cancer. Cultures needed to exclude atypical mycobacterium disease, differential cell counts.
Sublabial BX: Positive Focus score of lymphocyte aggregates and fibrosis typical of an autoimmune exocrineopathy. 34% of 38 pts suspected of SS related ILD had a positive + thus reducing need for VATS Bx (Fischer et al CHEST 2009)
Propert
y of P
resen
ter

Other Studies Cardiac Echo: evaluate for PAH (Pulmonary Artery
Hypertension) suspected if an asymptomatic pericardial-effusion identified in Scleroderma patients cardiomyopathy (Fischer et al Chest 131:988, 2007)
Full Exercise study: if confusing physiology and co-exisitingcardiac dysfunction
Hand xray: erosions, cartilage loss and periarticularosteopenia (RA) but Ultrasound and especially MRI are more sensitive for documenting synovitis than physical exam, distal tuft resorption and calcinosis are seen in SSC
Selected: R heart cath, CT angio, Tailored barium swallow evaluate for aspiration risk, DEXA all patients at risk for low bone mass. Nailfold capillary microscopy (SSC)
Propert
y of P
resen
ter

Germinal center
Lymphoid Hyperplasia
Propert
y of P
resen
ter

Propert
y of P
resen
ter

Minor Salivary Gland Biopsy From Normal And Patient With SS
Normal Abnormal
Propert
y of P
resen
ter

Primary SS
Propert
y of P
resen
ter

LIP
Propert
y of P
resen
ter

NSIP, Cyst, Bronchiectasis
Propert
y of P
resen
ter

RA Pleural effusion
Propert
y of P
resen
ter

Post tx of COP with AZA 3 years
Propert
y of P
resen
ter

56 yo male Fibrotic NSIP (VATS) preclinical RA
2013 pre treatment 2014 post treatment
Propert
y of P
resen
ter

BO in RA Expiration images hrCT
Propert
y of P
resen
ter

Constrictive bronchiolitisProp
erty o
f Pres
enter

Environmental Induced BO/HP in Iraq
Propert
y of P
resen
ter

59 yo SLE patient fibrotic NSIP
Propert
y of P
resen
ter

Systemic Sclerosis
Propert
y of P
resen
ter

65 yo SSC PAH and ILD
2014 2004
Propert
y of P
resen
ter
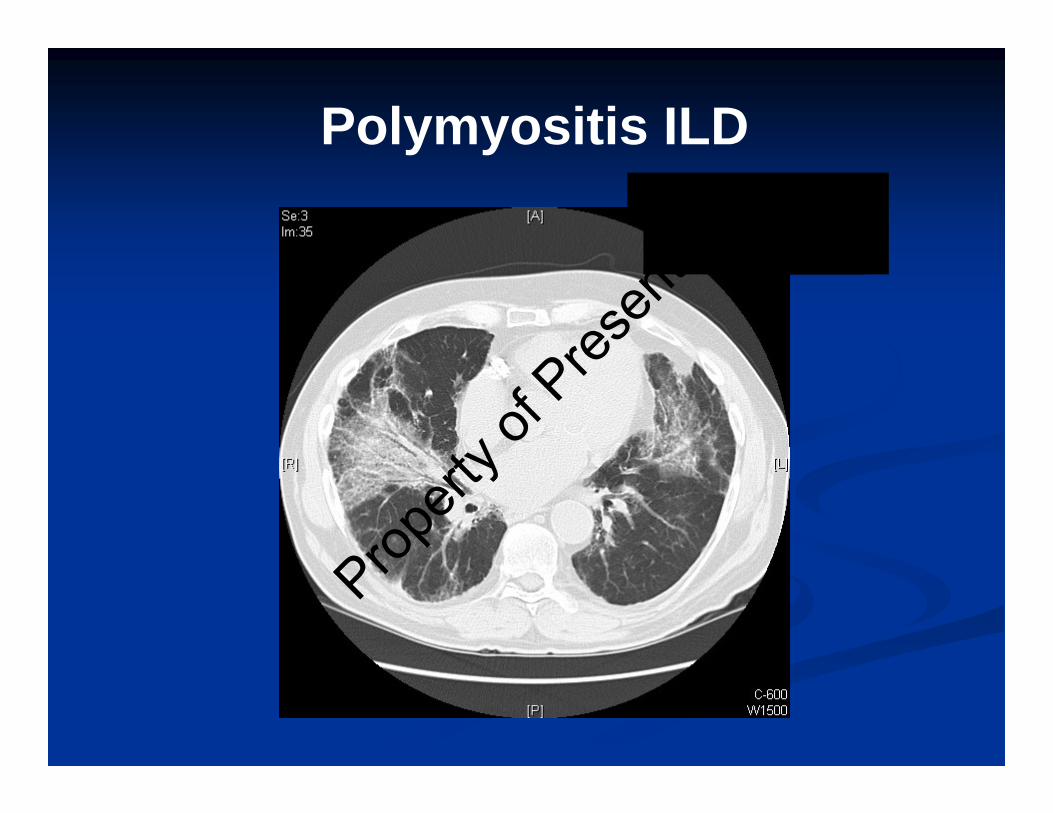
Polymyositis ILD
Propert
y of P
resen
ter

Therapeutic Approach and Management
Immune suppressive drugs. Must balance the risk of irreversible loss of lung function vs increased risk of drug toxicity in particular patient.
Determine rate of deterioration based upon prior PFTs, SaO2 and or hrCT imaging especially fibrosis
Determine responsiveness of prior immunosuppressive regiments as this also affects prognosis.
Propert
y of P
resen
ter

Therapeutic Approach and Management
General guidelines: Achieve and document maximum improvement in physiology before tapering immunosuppressive agents (12 months). Then try to maintain the clinical response with less toxic or lower doses of immune suppressive agents.
Be vigilant of extra-pulmonary manifestations of disease or drugs; GERD (risk of aspiration), steroid myopathy, digit necrosis, disabling arthritis or osteoporosis.
Clinical respiratory deterioration could be the result of drug toxicity, infection or AIP (disease flare during taper of drugs)
Future multicenter SSC treatment trials for ILD are ongoing at NJH, Aryeh Fisher as PI now enrolling for SLS II trial (Cytoxan vs MMF) and SCOT trial (hi dose immunosuppressive with Autologous stem Cell transplantation) shouldallow us to better define optimum therapy in selected patient populations.
Propert
y of P
resen
ter

Treatment OptionsPrednisone: 40-60mg daily or pulse solumedrol 1 gm daily
times 3 may be used initially to achieve a more rapid response until prednisone sparing agent is efficacious which may take 4-6 weeks.
Azathioprine (AZA): Azathioprine may be used for serositis, or mild disease which is slowly progressive or in patients unlikely to tolerate CYC or MMF (due to expenses).
Cyclophosphamide (Cytoxan, CYC): Probable most effective against CTD-ILD, daily oral route carries greater toxicity than monthly iv (500-1,000mg/M2).
Mycophenolate Mofetil (MMF): less toxic than cytoxanand usually better tolerated than AZA and appears superior to AZA in treating SSC, PM and UCTD related CTD, expensive (Swigris, et al. Chest 2006).
Propert
y of P
resen
ter

Other Treatment Options
Cyclosporine: May be effective in patients with intolerance to above agents due to cytopenias or infections.
Tacrolimus: Similar to cyclosporine but more expensive yet better tolerated (author’s experience)
Combinations: Infliximab 5mg/kg and MMF or AZA may be helpful in RA associated Bronchiolitis whereas sever BO may need CYC (author’s experience).
Rituximab: May be of benefit in LIP (RA, SS or SLE) or ANCA + lung disease.
Propert
y of P
resen
ter

Bibliography
1. Casteline FV, Goldberg H, Dellaripa. The impact of rheumatological evaluation in the management of patients with interstitial lung disease
2. Sakamoto O, Saita N, Ando M, Kohrogi H, Suga M, Ando M. Two cases of Sjogren's syndrome with multiple bullae. Intern Med 2002;41(2):124-8.
3. Chang B, Wigley FM, White B, Wise RA. Scleroderma patients with combined pulmonary hypertension and interstitial lung disease. J Rheumatol 2003;30(11):2398-405.
4. Solomon JJ, Olson AL, Fischer A, Bull T, Brown K Raghu G. Scleroderma lung Disease. Eur Resp Rev 2013;22: 6-19.
5. Medications with pulmonary toxicity www.pneumotox.com6. Fathi M, Lundberg IE. Interstitial lung disease in polymyositis and dermatomyositis. Curr
Opin Rheumatol 2005;17(6):701-6.7. Lee HK, Kim DS, Yoo B, et al. Histopathological pattern and clinical features of
rheumatoid arthritis-associated interstitial lung disease. Chest 2005;127(6):2019-27.8. Kocheril SV, Appleton BE, Somers EC, et al. Comparison of disease progression and
mortality of connective tissue disease-related interstitial lung disease and idiopathic interstitial pneumonia. Arthritis Rheum 2005;53(4):549-57.
9. King, TE, Kim EJ, Kinder BW. Chapter 26 Connective Tissue Diseases in Interstitial Lung Disease, 5th Edition, Schwarz ML and King TE (eds), 2011. Peoples Medical Publishing House Shelton, CT-USA.
Propert
y of P
resen
ter

Bibliography10. Swigris, JJ, Olson, AL, Fischer, et al. Mycophenolate mofetil is safe, well-tolerated,
and preserves lung function in patients with connective tissue diseases-related interstitial lung disease. Chest 2006;130:30-36.
11. Fischer A, Meehan RT, Feghali-Boswick CA, West SG and Brown KK. Unique Characteristics of systemic Sclerosis sine Scleroderma-associated interstitial lung disease. Chest 2006;130:976-981k
12. Fischer A, West SG, Swigris JJ. Connective tissue-associated interstitial lung disease a call for clarification. Chest. 2010;138-251-256.
13. Tanaka, N, Kim S, Newell, J, Brown, K, Cool, C, Meehan, R, Emoto, T, Matsumoto, T, Lynch, D. Rheumatoid Arthritis-related lung diseases: CT findings. Radiology 2004;232:1:81-91.
14. Swigris JJ, Fischer A, Gillis, Meehan RT, and Brown K. Pulmonary and thrombotic Manifestations of Systemic Lupus Erythematosus. Chest 2008; 133: 271-280.
15. Frankel SK, Brown KK. Collagen Vascular Diseases of the Lung. Clinical Pulmonary Medicine 2006; 13:25-35.
16. Bongartz T, Nannini C, Medina-Velasquez YF et al. Incidence and mortality of interstitial lung disease in rheumatoid arthritis a population-based study. Arthritis & Rheumatism 2010; 62: 1583-1591.
17. Lynch DA. Lung disease related to collagen vascular disease. J Thorac Imaging 2009; 24: 299-309.
18. Swigris JJ, Brown KK, Flaherty KR. The idiopathic interstitial pneumonias and connective tissue disease-associated interstitial lung disease. Current Rheumatology Reviews 2010; 6: 91-98
Propert
y of P
resen
ter

Bibliography: Lung involvement in preclinical RA
19. Reynisdottir G, Karimi R, Joshua V, Olsen H et al. Structural changes and antibody enrichment in the lungs are early features of anti-citrullinated protein antibody-positive rheumatoid arthritis. Arthritis Rheum 2014:66: 31-39.
20. Willis VC, Demoruelle MK, Derber LA, Chartier-Logan CJ et al. Sputum autoantibodies in patients with established rheumatoid arthritis and subjects at risk of future clinically apparent disease. Arthritis Rheum 2013; 65L 2545-2555.
21. Demoruelle MK, Weisman MH, Simonian PL, Lunch DA et al. Airways abnormalities and rheumatoid arthritis-related autoantibodies in subjects without arthritis: early injury or initiating sire of autoimmunity? Arthritis Rheum. 2012; 64: 1756-1761.
22. Majka DS, Deane KD, Parrish LA, Lazar AA et al. Duration of preclinical rheumatoid arthritis-related autoantibody positivity increases in subjects with older age at time of disease diagnosis. Ann Rheum Dis 2008; 67: 801-807.
23. Fischer A, Solomon JJ, Du Bois RM, Deane KD et al. Lung disease with anti-CCP antibodies but not rheumatoid arthritis or connective tissue disease. Respiratory Medicine 2012; 106: 1040-1047.
24. Demoruelle MK, Solomon JJ, Fischer A, Deane KD. The lung may play a role in the pathogenesis of rheumatoid arthritis. Int J Clin Rheumatol 2014; 9: 295-309.
Propert
y of P
resen
ter

Pulmonary Manifestations Associated with Various Connective Tissue Diseases
Diseases Serositis Fibrotic ILD COP PAH Hemorrhage Airway
RA ++ ++ ++ + Rare +
Systemic Sclerosis + +++ + +++ Rare +
Polymyositis/Dermatomyositis
+ +++ ++ + Rare +
Systemic lupus erthematosus
+++ + ++ ++ ++ Rare
Sjogren’s syndrome + ++ + Rare Rare ++
Ankylosing spondylitis Rare + Rare Rare Rare +
Relapsing polychondritis Rare Rare Rare Rare Rare +++
Wegener’s granulomatosis Rare ++ ++ Rare ++ +
Propert
y of P
resen
ter