Medscape 1-7 - Nephrotic Syndrome_ Background, Pathophysiology, Etiology

of 9
-
Upload
sauzen-salazar -
Category
Documents
-
view
214 -
download
0
Transcript of Medscape 1-7 - Nephrotic Syndrome_ Background, Pathophysiology, Etiology
-
8/18/2019 Medscape 1-7 - Nephrotic Syndrome_ Background, Pathophysiology, Etiology
1/9
8/26/2015 Nephrotic Syndrome: Background, Pathophysiology, Etiology
http://emedicine.medscape.com/article/244631-overview#showall
Background
Nephrotic syndrome is kidney disease with proteinuria, hypoalbuminemia, andedema. Nephrotic-range proteinuria is 3 grams per day or more. On a single spoturine collection, it is 2 g of protein per gram of urine creatinine.
There are many specific causes of nephrotic syndrome. These include kidneydiseases such as minimal-change nephropathy, focal glomerulosclerosis, and
membranous nephropathy. Nephrotic syndrome can also result from systemicdiseases that affect other organs in addition to the kidneys, such as diabetes,amyloidosis, and lupus erythematosus.
Nephrotic syndrome may affect adults and children, of both sexes and of any race.It may occur in typical form, or in association with nephritic syndrome. The latter connotes glomerular inflammation, with hematuria and impaired kidney function.
Classification
Nephrotic syndrome can be primary, being a disease specific to the kidneys, or itcan be secondary, being a renal manifestation of a systemic general illness. In allcases, injury to glomeruli is an essential feature.
Primary causes of nephrotic syndrome include the following, in approximate order of frequency:
Minimal-change nephropathyFocal glomerulosclerosis
Membranous nephropathyHereditary nephropathies
Secondary causes include the following, again in order of approximate frequency:
Diabetes mellitusLupus erythematosus
Amyloidosis and paraproteinemiasViral infections (eg, hepatitis B, hepatitis C, human immunodeficiency virus [HIV] )Preeclampsia
Nephrotic-range proteinuria may occur in other kidney diseases, such as IgAnephropathy. In that common glomerular disease, one third of patients may have
nephrotic-range proteinuria.[1]
Nephrotic syndrome may occur in persons with sickle cell disease and evolve torenal failure. Membranous nephropathy may complicate bone marrow
ransplantation, in association with graft versus host disease.
Kidney diseases that affect tubules and interstitium, such as interstitial nephritis,will not cause nephrotic syndrome.
The above causes of nephrotic syndrome are largely those for adults, and thisarticle will concentrate primarily on adult nephrotic syndrome. However, nephroticsyndrome in infancy and childhood is an important entity. For discussion of thisopic, see the Medscape Reference article Pediatric Nephrotic Syndrome.
From a therapeutic perspective, nephrotic syndrome may be classified as steroidsensitive, steroid resistant, steroid dependent, or frequently relapsing.
Corticosteroids (prednisone), cyclophosphamide, and cyclosporine are used toinduce remission in nephrotic syndrome. Diuretics are used to reduce edema.
Angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockersare administered to reduce proteinuria. (See Treatment and Medication.)
Pathophysiology
In a healthy individual, less than 0.1% of plasma albumin may traverse the
glomerular filtration barrier.[2] Controversy exists regarding the sieving of albuminacross the glomerular permeability barrier. On the basis of studies in experimentalanimals, it has been proposed that there is ongoing albumin passage into the urine,in many grams per day, with equivalent substantial tubular uptake of albumin, the
result being that the urine has 80 mg per day or less of daily albumin. [3]
However, studies of humans with tubular transport defects suggest that the
glomerular urinary space albumin concentration is 3.5 mg/L.[4] With thisconcentration, and a normal daily glomerular filtration rate (GFR) of 150 liters, onewould expect no more than 525 mg per day of albumin in the final urine. Amountsabove that level point to glomerular disease.
The glomerular capillaries are lined by a fenestrated endothelium that sits on theglomerular basement membrane, which in turn is covered by glomerular epithelium,or podocytes, which envelops the capillaries with cellular extensions called footprocesses. In between the foot processes are the filtration slits. These 3 structures
http://emedicine.medscape.com/article/982920-overviewhttp://emedicine.medscape.com/article/989518-overviewhttp://emedicine.medscape.com/article/239927-overviewhttps://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBF7ynlSzdVfGyGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABYovuivLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5Gi48ojy8n_W5T7BcGBFKow8%2526sig%253DAOD64_259LLXv2NhZAKykBPhcRpwChU4ag%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_1ahttps://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBF7ynlSzdVfGyGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABYovuivLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5Gi48ojy8n_W5T7BcGBFKow8%2526sig%253DAOD64_259LLXv2NhZAKykBPhcRpwChU4ag%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_1ahttps://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBF7ynlSzdVfGyGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABYovuivLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5Gi48ojy8n_W5T7BcGBFKow8%2526sig%253DAOD64_259LLXv2NhZAKykBPhcRpwChU4ag%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_1ahttps://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBF7ynlSzdVfGyGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABYovuivLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5Gi48ojy8n_W5T7BcGBFKow8%2526sig%253DAOD64_259LLXv2NhZAKykBPhcRpwChU4ag%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_1ahttps://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBF7ynlSzdVfGyGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABYovuivLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5Gi48ojy8n_W5T7BcGBFKow8%2526sig%253DAOD64_259LLXv2NhZAKykBPhcRpwChU4ag%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_1ahttps://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBF7ynlSzdVfGyGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABYovuivLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5Gi48ojy8n_W5T7BcGBFKow8%2526sig%253DAOD64_259LLXv2NhZAKykBPhcRpwChU4ag%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_1ahttps://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBF7ynlSzdVfGyGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABYovuivLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5Gi48ojy8n_W5T7BcGBFKow8%2526sig%253DAOD64_259LLXv2NhZAKykBPhcRpwChU4ag%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_1ahttps://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBF7ynlSzdVfGyGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABYovuivLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5Gi48ojy8n_W5T7BcGBFKow8%2526sig%253DAOD64_259LLXv2NhZAKykBPhcRpwChU4ag%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_1ahttps://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBe98glSzdVe-yGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABY8oCjvLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GiuPdhKbVtJJk6lUFZn2NRc%2526sig%253DAOD64_3Id_Bq4lW315Ds61BqVxCcKs5Myw%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_4https://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBe98glSzdVe-yGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABY8oCjvLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GiuPdhKbVtJJk6lUFZn2NRc%2526sig%253DAOD64_3Id_Bq4lW315Ds61BqVxCcKs5Myw%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_4https://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBe98glSzdVe-yGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABY8oCjvLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GiuPdhKbVtJJk6lUFZn2NRc%2526sig%253DAOD64_3Id_Bq4lW315Ds61BqVxCcKs5Myw%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_4https://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBe98glSzdVe-yGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABY8oCjvLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GiuPdhKbVtJJk6lUFZn2NRc%2526sig%253DAOD64_3Id_Bq4lW315Ds61BqVxCcKs5Myw%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_4https://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBe98glSzdVe-yGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABY8oCjvLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GiuPdhKbVtJJk6lUFZn2NRc%2526sig%253DAOD64_3Id_Bq4lW315Ds61BqVxCcKs5Myw%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_4https://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBe98glSzdVe-yGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABY8oCjvLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GiuPdhKbVtJJk6lUFZn2NRc%2526sig%253DAOD64_3Id_Bq4lW315Ds61BqVxCcKs5Myw%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_4https://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBe98glSzdVe-yGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABY8oCjvLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GiuPdhKbVtJJk6lUFZn2NRc%2526sig%253DAOD64_3Id_Bq4lW315Ds61BqVxCcKs5Myw%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_4https://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBe98glSzdVe-yGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABY8oCjvLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GiuPdhKbVtJJk6lUFZn2NRc%2526sig%253DAOD64_3Id_Bq4lW315Ds61BqVxCcKs5Myw%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_4https://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBe98glSzdVe-yGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABY8oCjvLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GiuPdhKbVtJJk6lUFZn2NRc%2526sig%253DAOD64_3Id_Bq4lW315Ds61BqVxCcKs5Myw%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_4https://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBe98glSzdVe-yGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABY8oCjvLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GiuPdhKbVtJJk6lUFZn2NRc%2526sig%253DAOD64_3Id_Bq4lW315Ds61BqVxCcKs5Myw%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_4https://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBF7ynlSzdVfGyGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABYovuivLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5Gi48ojy8n_W5T7BcGBFKow8%2526sig%253DAOD64_259LLXv2NhZAKykBPhcRpwChU4ag%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_1ahttp://emedicine.medscape.com/article/253960-overviewhttp://emedicine.medscape.com/article/989518-overviewhttp://emedicine.medscape.com/article/1957952-overviewhttp://emedicine.medscape.com/article/245915-overviewhttp://emedicine.medscape.com/article/429037-overviewhttp://emedicine.medscape.com/article/982920-overviewhttp://emedicine.medscape.com/article/239927-overviewhttps://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBNkwolSzdVfCyGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABY-v-ivLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GiBVdUld6HBNTBtOucVaZKY%2526sig%253DAOD64_0cPaLZO1zWuVxYWLhtT7_wJ8IRjQ%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_4http://emedicine.medscape.com/article/243597-overviewhttp://emedicine.medscape.com/article/239799-overviewhttp://emedicine.medscape.com/article/243348-overviewhttp://emedicine.medscape.com/article/246031-overview
-
8/18/2019 Medscape 1-7 - Nephrotic Syndrome_ Background, Pathophysiology, Etiology
2/9
8/26/2015 Nephrotic Syndrome: Background, Pathophysiology, Etiology
http://emedicine.medscape.com/article/244631-overview#showall
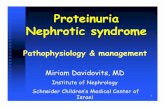
the fenestrated endothelium, glomerular basement membrane, and glomerular epithelium—are the glomerular filtration barrier. A schematic drawing of the
glomerular barrier is provided in the image below.
Schematic drawing of the glomerular barrier. Podo = podocytes; GBM = glomerular basementmembrane; Endo = fenestrated endothelial cells; ESL = endothelial cell surface layer (oftenreferred to as the glycocalyx). Primary urine is formed through the filtration of plasma fluidacross the glomerular barrier (arrows); in humans, the glomerular filtration rate (GFR) is 125mL/min. The plasma flow rate (Qp) is close to 700 mL/min, with the filtration fraction being 20%.The concentration of albumin in serum is 40 g/L, while the estimated concentration of albumin inprimary urine is 4 mg/L, or 0.1% of its concentration in plasma. Reproduced from Haraldsson etal, Physiol Rev 88: 451-487, 2008, and by permission of the American Physiological Society(www.the-aps.org).
Filtration of plasma water and solutes is extracellular and occurs through theendothelial fenestrae and filtration slits. The importance of the podocytes and thefiltration slits is shown by genetic diseases. Thus, in congenital nephrotic syndrome
of the Finnish type, the gene for nephrin, a protein of the filtration slit, is mutated,leading to nephrotic syndrome in infancy . Similarly, podocin, a protein of thepodocytes, may be abnormal in a number of children with steroid-resistant focalglomerulosclerosis.
The glomerular structural changes that may cause proteinuria are damage to theendothelial surface, the glomerular basement membrane, or the podocytes. One or more of these mechanisms may be seen in any one type of nephrotic syndrome.
Albuminuria alone may occur, or, with greater injury, leakage of all plasma proteins,(ie, proteinuria) may take place.
Proteinuria that is more than 85% albumin is selective proteinuria. Albumin has anet negative charge, and it is proposed that loss of glomerular membrane negativecharges could be important in causing albuminuria. Nonselective proteinuria, beinga glomerular leakage of all plasma proteins, would not involve changes inglomerular net charge but rather a generalized defect in permeability. This constructdoes not permit clear-cut separation of causes of proteinuria, except in minimal-change nephropathy, in which proteinuria is selective.
Pathogenesis of edema
An increase in glomerular permeability leads to albuminuria and eventually tohypoalbuminemia. In turn, hypoalbuminemia lowers the plasma colloid osmoticpressure, causing greater transcapillary filtration of water throughout the body andhus the development of edema.
Capillary hydrostatic pressure and the gradient of plasma to interstitial fluid oncoticpressure determine the movement of fluid from the vascular compartment to theinterstitium. The oncotic pressure is mainly determined by the protein content. Theflux of water across the capillary wall can be expressed by the following formula:
Qw = K ([Pc - Pi] - [pp - pi]
In this formula, Qw is net flux of water, K is the capillary filtration coefficient, Pc is
capillary hydrostatic pressure, and Pi is the interstitial fluid hydrostatic pressure,
while pp is the plasma oncotic pressure, and pi is the interstitial fluid oncotic
pressure.
ith a high enough capillary hydrostatic pressure or a low enough intravascular oncotic pressure, the amount of fluid filtered exceeds the maximal lymphatic flow,and edema occurs. In patients with nephrotic syndrome, this causes a reduction inplasma volume, with a secondary increase of sodium and water retention by thekidneys.
An alternative hypothesis is that a condition of renal sodium retention occursbecause of the proteinuria, but this is not related to intravascular volume or toserum protein concentration. The evidence supporting this so-called overfillhypothesis includes the facts that (1) sodium retention is observed even before theserum albumin level starts falling and (2) intravascular volume is normal or evenincreased in most patients with nephrotic syndrome. This could occur if intraluminal
protein directly stimulated renal epithelial sodium reabsorption. [5]
A third possible mechanism is an enhanced peripheral capillary permeability toalbumin, as shown by radioisotopic technique in human studies of 60 patients with
nephrotic syndrome.[6] This would then lead to increased tissue oncotic pressure
http://refimgshow%281%29/
-
8/18/2019 Medscape 1-7 - Nephrotic Syndrome_ Background, Pathophysiology, Etiology
3/9
8/26/2015 Nephrotic Syndrome: Background, Pathophysiology, Etiology
http://emedicine.medscape.com/article/244631-overview#showall
and fluid retention in the peripheral tissues.
Metabolic consequences of proteinuria
Metabolic consequences of the nephrotic syndrome include the following:
InfectionHyperlipidemia and atherosclerosisHypocalcemia and bone abnormalitiesHypercoagulabilityHypovolemia
Acute renal failure may indicate an underlying glomerulonephritis but is more oft enprecipitated by hypovolemia or sepsis. Edema of the kidneys that causes a
pressure-mediated reduction in the GFR has also been hypothesized.
Hypertension related to fluid retention and reduced kidney function may occur.
Failure to thrive may develop in patients with chronic edema, including ascites andpleural effusion. Failure to thrive may be caused by anorexia, hypoproteinemia,increased protein catabolism, or frequent infectious complications. Edema of thegut may cause defective absorption, leading to chronic malnutrition.
Infection
Infection is a major concern in nephrotic syndrome; patients have an increasedsusceptibility to infection with Streptococcus pneumoniae, Haemophilus influenzae,Escherichia coli , and other gram-negative organisms. Varicella infection is alsocommon. The most common infectious complications are bacterial sepsis, cellulitis,pneumonia, and peritonitis.
Proposed explanations include the following:
Urinary immunoglobulin lossesEdema fluid acting as a culture mediumProtein deficiencyDecreased bactericidal activity of the leukocytesImmunosuppressive therapyDecreased perfusion of the spleen caused by hypovolemiaUrinary loss of a complement factor (properdin factor B) that opsonizescertain bacteria
Hyperlipidemia and atherosclerosis
Hyperlipidemia may be considered a typical feature of the nephrotic syndrome,rather than a mere complication. It is related to the hypoproteinemia and low serumoncotic pressure of nephrotic syndrome, which then leads to reactive hepatic protein
synthesis, including of lipoproteins.[7] In addition, reduced plasma levels of lipoprotein lipase results in diminution of lipid catabolism. Some of the elevatedserum lipoproteins are filtered at the glomerulus, leading to lipiduria and theclassical findings of oval fat bodies and fatty casts in the urine sediment.
Atherosclerotic vascular disease appears to occur in greater frequency in personswith nephrotic syndrome than in healthy persons of the same age. Curry andRoberts showed that the frequency and extent of coronary artery disease stenoseswere greater in patients with nephrotic syndrome than in nonnephrotic control
subjects. [8]
hen their study was published, in 1977, lipid-lowering treatments were less widelyused than they are today. Accordingly, the average highest serum total cholesterolin this series was over 400 mg/dL. That is in the range of serum cholesterol seen infamilial hypercholesterolemia, a disease that predisposes individuals to myocardialinfarction.
Hypocalcemia
Hypocalcemia is common in the nephrotic syndrome, but rather than being a truehypocalcemia, it is usually caused by a low serum albumin level. Nonetheless, lowbone density and abnormal bone histology are reported in association with nephroticsyndrome. This could be caused by urinary losses of vitamin D–binding proteins,
with consequent hypovitaminosis D and, as a result, reduced intestinal calciumabsorption. [9]
Tessitore et al reported that when the GFR was normal, persons with the nephrotic
syndrome had no consistent calcium or bony abnormalities. [10] Yet in that samestudy, when the GFR was reduced, bone mineralization defects were found bybiopsy. A later study found osteomalacia on bone biopsy in over half of adults who
had longstanding nephrotic syndrome but whose GFR was preserved. [9]
A further complication derives from therapies, especially prednisone use. Low bone
mass may be found in relation to cumulative steroid dose. [11] This subject remainscontroversial; as reported by Leonard et al, intermittent corticosteroid treatment of childhood steroid-sensitive nephrotic syndrome does not appear to be associated
with bone mineral deficits. [12] It is possible that long duration of either the nephroticsyndrome or treatments for it are the important risk factors for bone disease inhese patients.
Hypercoagulability
Nephrotic Syndrome
Author: Eric P Cohen, MD; Chief E ditor: Vecihi B atuman, MD, FACP, FASN more...
Updated: Dec 09, 2014
http://emedicine.medscape.com/article/121298-overview
-
8/18/2019 Medscape 1-7 - Nephrotic Syndrome_ Background, Pathophysiology, Etiology
4/9
8/26/2015 Nephrotic Syndrome: Background, Pathophysiology, Etiology
http://emedicine.medscape.com/article/244631-overview#showall
Venous thrombosis and pulmonary embolism are well-known complications of thenephrotic syndrome. Hypercoagulability in these cases appears to derive fromurinary loss of anticoagulant proteins, such as antithrombin III and plasminogen,along with the simultaneous increase in clotting factors, especially factors I, VII,VIII, and X.
A study by Mahmoodi et al of almost 300 patients with nephrotic syndromeconfirmed that venous thromboembolism (VTE) was almost 10 times higher in
hese persons than in the normal population (1% vs 0.1-0.2%). [13] Moreover, thatrisk appeared especially elevated during the first 6 months of nephrotic syndrome,being at almost 10%. This high incidence may justify the routine use of preventiveanticoagulation treatment during the first 6 months of a persistent nephroticsyndrome.
Mahmoodi's study also showed an increased risk of arterial thrombotic events,including coronary and cerebrovascular ones, in nephrotic syndrome. Unlike the riskof VTE, which was related to proteinuria, this arterial risk was related to usual riskfactors for arterial disease, such as hypertension, diabetes, smoking, and reducedGFR.
Hypovolemia
Hypovolemia occurs when hypoalbuminemia decreases the plasma oncoticpressure, resulting in a loss of plasma water into the interstitium and causing adecrease in circulating blood volume. Hypovolemia is generally observed only whenhe patient's serum albumin level is less than 1.5 g/dL. Symptoms include vomiting,
abdominal pain, and diarrhea. The signs include cold hands and feet, delayedcapillary filling, oliguria, and tachycardia. Hypotension is a late feature.
Etiology
Common primary causes of nephrotic syndrome include kidney diseases such as
minimal-change nephropathy, membranous nephropathy, and focalglomerulosclerosis. Secondary causes include systemic diseases such as diabetesmellitus, lupus erythematosus, and amyloidosis. Congenital and hereditary focalglomerulosclerosis may result from mutations of genes that code for podocyteproteins, including nephrin, podocin, or the cation channel 6 protein. Nephroticsyndrome can result from drugs of abuse, such as heroin.
Nephrotic-range proteinuria occurring in the third trimester of pregnancy is theclassical finding of preeclampsia. In that condition, also known as toxemia,hypertension develops as well. It may occur de novo or it may be superimposed onanother chronic kidney disease. In the latter case, there will have been preexistingproteinuria that will have worsened during pregnancy.
Medication can cause nephrotic syndrome. This includes the very infrequentoccurrence of minimal-change nephropathy with NSAID use, and the occurrence of membranous nephropathy with the administration of gold and penicillamine, whichare older drugs used for rheumatic diseases; there have also been reports of focalglomerulosclerosis in association with intravenous bisphosphonates. Lithium andinterferon therapy also are implicated in focal glomerulosclerosis of the collapsingype.
Nephrotic-range proteinuria could occur with the use of anticancer agents, such as
bevacizumab, that inhibit vascular endothelial growth factor (VEGF). [14] However,he clinical picture of this complication is of a thrombotic microangiopathy rather han of nephrotic syndrome per se.
The association of membranous nephropathy with cancer is a clinical dilemma. Thisassociation presumably results from immune complex injury to the glomeruluscaused by cancer antigens.
hile there are about 6000 new cases of membranous nephropathy per year in theUnited States, there are 1.5 million new cases of nonskin cancer. Therefore, fromhe oncologist’s standpoint, the problem of paraneoplastic membranous
nephropathy is trivial.
Nonetheless, a carefully performed analysis from France suggested that the cancer rate in persons with membranous nephropathy is approximately 10-fold higher than
it is in the general population, especially in individuals over age 65 years. [15] In thatstudy, 50% of membranous nephropathy cases were diagnosed before the diagnosisof cancer. Thus, in some patients with membranous nephropathy, one shouldconsider the possibility of an undiagnosed cancer.
Epidemiology
United States statistics
The figure below shows the incidence per million population of important causes of nephrotic syndrome. Diabetic nephropathy with nephrotic syndrome is mostcommon, at an estimated rate of at least 50 cases per million population. That is anunderestimation, however, since the rate of end-stage renal disease from diabeteshas reached 100 cases per million population in some Western countries. Inchildren, nephrotic syndrome may occur at a rate of 20 cases per million children.[16]
http://emedicine.medscape.com/article/280744-overviewhttp://emedicine.medscape.com/article/1476919-overview
-
8/18/2019 Medscape 1-7 - Nephrotic Syndrome_ Background, Pathophysiology, Etiology
5/9
8/26/2015 Nephrotic Syndrome: Background, Pathophysiology, Etiology
http://emedicine.medscape.com/article/244631-overview#showall
Incidence of important causes of nephrotic syndrome, in number per million population. The leftpanel shows systemic causes, and the right panel lists primary renal diseases that can cause
nephrotic syndrome. fgs = focal glomerulosclerosis, MN = membranous nephropathy, minchange = minimal-change nephropathy. Data are in part from Swaminathan et al and Bergesio etal.
International statistics
Biopsy studies in children with nephrotic syndrome have shown similar types of histology in India and Turkey, compared with what one would expect in Western
countries. [17, 18] In Pakistani adults with nephrotic syndrome, the spectrum of histologies of kidney biopsies has been found to be similar to that seen in western
countries. [19]
In parts of Africa and the Middle East (eg, Egypt), glomerular disease may be
associated with urogenital schistosomal infection.[20] However, so-called "tropicalnephrotic syndrome" (eg, from parasitic diseases such as schistosomiasis or malaria) may not be a true entity.
Doe et al reviewed causes of nephrotic syndrome in African children and found no
evidence for a dominating role of steroid-resistant tropical glomerulopathies; rather,kidney biopsy most often showed typical histologic findings (focal and segmental
glomerulosclerosis and minimal change disease).[21]
The connection of nephrotic syndrome to quartan malaria is not well-established.Indeed, Pakasa and Sumaili call attention to the apparent decline of parasite-
associated nephrotic syndrome in the Congo.[22, 23] It is possible that the perceivedassociation between nephrotic syndrome and parasitic infections was coincidental,as supported by the ongoing and probably increasing occurrence of chronic kidney
disease in the Congo. [23]
Race-, sex-, and age-related demographics
Because diabetes is major cause of nephrotic syndrome, American Indians,Hispanics, and African Americans have a higher incidence of nephrotic syndromehan do white persons. HIV nephropathy is a complication of HIV infection that is
unusual in whites; it is seen with greater frequency in African Americans. [24] Focalglomerulosclerosis appears to be overrepresented in African-American children, as
compared with white children, as a cause of nephrotic syndrome.[25]
There is a male predominance in the occurrence of nephrotic syndrome, as there isfor chronic kidney disease in general. This male overrepresentation is also seen in
paraneoplastic membranous nephropathy.[15] However, lupus nephritis affectsmostly women.
The image below shows typical ages at which a given cause of nephrotic syndromemay occur. It does not show every possible cause of nephrotic syndrome, such aslupus nephritis, which typically affects young black women. The ages shown areaverages.
A sc hema of the average patient ages associated with various common forms of nephroticsyndrome.
Prognosis
In the preantibiotic era, infection was a major factor in the mortality rate among
patients with nephrotic syndrome.[26] Treatments for nephrotic syndrome and itscomplications appear to have reduced the morbidity and mortality once associatedwith the syndrome. Currently, the prognosis for patients with primary nephrotic
syndrome depends on its cause.
http://refimgshow%282%29/http://refimgshow%283%29/
-
8/18/2019 Medscape 1-7 - Nephrotic Syndrome_ Background, Pathophysiology, Etiology
6/9
8/26/2015 Nephrotic Syndrome: Background, Pathophysiology, Etiology
http://emedicine.medscape.com/article/244631-overview#showall
Infants with congenital nephrotic syndrome have a dismal prognosis: survivalbeyond several months is possible only with dialysis and kidney transplantation.
Only approximately 20% of patients with focal glomerulosclerosis undergo remissionof proteinuria; an additional 10% improve but remain proteinuric. Many patientsexperience frequent relapses, become steroid-dependent, or become steroid-resistant. End-stage renal disease develops in 25-30% of patients with focalsegmental glomerulosclerosis by 5 years and in 30-40% of these patients by 10years.
The prognosis for patients with minimal-change nephropathy is very good. Mostchildren respond to steroid therapy; still, about 50% of children have 1 or 2 relapseswithin 5 years and approximately 20% of them continue to relapse 10 years after diagnosis. Only 30% of children never have a relapse after the initial episode.
Approximately 3% of patients who initi ally respond t o steroids become steroid-resistant.
Adults with minimal-change nephropathy have a burden of relapse similar to that of children. However, the long-term prognosis for kidney function in patients with thisdisease is excellent, with little risk of renal failure.
Poor patient response to steroid therapy may predict a poor outcome. Children whopresent with hematuria and hypertension are more likely to be steroid-resistant andhave a poorer prognosis than are those who do not present with these conditions.
A study by Donadio et al of 140 patients with idiopathic membranous nephropathy,89 of whom received no treatment with corticosteroids or immunosuppressive drugsand 51 of whom were treated primarily with short-term courses of prednisone alone,found that survival rates in these patients were the same as those expected for the
general population.[27]
The prognosis may worsen because of (1) an increased incidence of renal failureand the complications secondary to nephrotic syndrome, including thrombotic
episodes and infection, or (2) treatment-related conditions, such as infectiouscomplications of immunosuppressive treatments.
In secondary nephrotic syndromes, morbidity and mortality are related to theprimary disease process (eg, diabetes, lupus, amyloidosis). In diabetic nephropathy,
however, the magnitude of proteinuria itself relates directly to mortality.[28]
In diabetic nephropathy with nephrotic syndrome, there is usually a good responseo angiotensin blockade, with reduction of proteinuria to low, sub-nephrotic levels.
True remission is uncommon, however. Cardiovascular morbidity and mortalityincrease as kidney function declines, and some patients will eventually need dialysisor a kidney transplant.
In primary amyloidosis, prognosis is not good, even with intensive chemotherapy. Insecondary amyloidosis, remission of the underlying cause, such as rheumatoidarthritis, is followed by remission of the amyloidosis and its associated nephroticsyndrome.
Patient EducationPediatric nephrotic syndrome is a chronic illness characterized by relapses andremissions, which can extend throughout childhood. There will be illness from thedisease and from its treatment. Parents may monitor their child's urine and recordhe results in a diary. The diary can also be used to write down an agreed-upon plan
for the management of relapses. Information booklets should be given to the family.Peer support and psychological counseling may be helpful for some families.
Progression to renal failure will require preparation for dialysis and/or kidneyransplantation. Similarly, adults with forms of nephrotic syndrome that cannot be
cured may progress to renal failure and the need for dialysis or kidneyransplantation.
Clinical Presentation
Contributor Information and Disclosures
Author
Eric P Cohen, MD Professor, Department of Medicine, Division of Nephrology, Medical College of Wisconsin;Nephrology Section Chief, Zablocki Veterans Affairs Hospital
Eric P Cohen, MD is a member of the following medical societies: American S ociety of Nephrology, RadiationResearch Society, Central Society for Clinical and Translational Research, International Society of Nephrology
Disclosure: Nothing to disclose.
Coauthor(s)Ramapriya Sinnakirouchenan, MD Assistant Professor, Division of Nephrology, Medical College of Wisconsin
Ramapriya Sinnakirouchenan, MD is a member of the following medical societies: American Society of Nephrology, Indian Medical Association
Disclosure: Nothing to disclose.
Specialty Editor BoardFrancisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College
http://www.asn-online.org/http://www.cscr.com/http://www.theisn.org/http://emedicine.medscape.com/article/244631-clinicalhttp://www.radres.org/http://www.asn-online.org/http://www.ima-india.org/
-
8/18/2019 Medscape 1-7 - Nephrotic Syndrome_ Background, Pathophysiology, Etiology
7/9
8/26/2015 Nephrotic Syndrome: Background, Pathophysiology, Etiology
http://emedicine.medscape.com/article/244631-overview#showall
of Pharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Received salary from Medscape for employment. for: Medscape.
Eleanor Lederer, MD Professor of Medicine, Chief, Nephrology Division, Director, Nephrology Training Program,Director, Metabolic Stone Clinic, Kidney Disease Program, University of Louisville School of Medicine; ConsultingStaff, Louisville Veterans Affairs Hospital
Eleanor Lederer, MD is a member of the following medical societies: American Association for the Advancementof Science, International Society of Nephrology, American S ociety for Biochemistry and Molecular Biology,
American Federation for Medical Research, American S ociety for Bone and M ineral Research, American S ocietyof Nephrology, American Society of Transplantation, Kentucky Medical Association, National Kidney Foundation,Phi Beta Kappa
Disclosure: Received grant/research funds from Dept of Veterans Affairs for research; Received salary from American Society of Nephrology f or asn council position; Received salary from University of Louisville for employment; Received salary from University of Louisville Physicians for employment; Received contractpayment from American Physician Institute for Advanced Professional Studies, LLC for independent contractor;Received contract payment from Healthcare Quality Strategies, Inc for independent cont.
Chief Editor Vecihi Batuman, MD, FACP, FASN Huberwald Professor of Medicine, Section of Nephrology-Hypertension,Tulane University School of Medicine; Chief, Renal Section, Southeast Louisiana Veterans Health Care System
Vecihi Batuman, MD, FACP, FASN is a member of the following medical societies: American College of Physicians, American S ociety of Hypertension, American S ociety of Nephrology, International Society of Nephrology
Disclosure: Nothing to disclose.
Additional ContributorsLaura Lyngby Mulloy, DO, FACP Professor of Medicine, Chief, Section of Nephrology, Hypertension, andTransplantation Medicine, Glover/Mealing Eminent Scholar Chair in Immunology, Medical College of Georgia,Georgia Regents University
Disclosure: Nothing to disclose.
References
1. Neelakantappa K, Gallo GR, Baldwin DS. Proteinuria in IgA nephropathy. Kidney Int . 1988 Mar. 33(3):716-21. [Medline].
2. Haraldsson B, Nyström J, Deen WM. Properties of the glomerular barrier and mechanisms of proteinuria.Physiol Rev . 2008 Apr. 88(2):451-87. [Medline].
3. Russo LM, B akris GL, Comper WD. Renal handling of albumin: a critical review of basic concepts andperspective. Am J K idney Dis. 2002 May. 39(5):899-919. [Medline].
4. Norden AG, Lapsley M, Lee PJ, Pusey CD, Scheinman SJ, Tam FW. Glomerular protein sieving andimplications for renal failure in Fanconi syndrome. Kidney Int . 2001 Nov. 60(5):1885-92. [Medline].
5. Hamm LL, Batuman V. Edema in the nephrotic syndrome: new aspect of an old enigma. J Am Soc Nephrol . 2003 Dec. 14(12):3288-9. [Medline].
6. Rostoker G, Behar A, Lagrue G. Vascular hyperpermeability in nephrotic edema. Nephron. 2000 Jul.85(3):194-200. [Medline].
7. Appel GB, Blum CB, Chien S, K unis CL, Appel AS. The hyperlipidemia of the nephrotic syndrome.Relation to plasma albumin concentration, oncotic pressure, and viscosity. N Engl J Med . 1985 Jun 13.312(24):1544-8. [Medline].
8. Curry RC Jr, Roberts WC. Status of the coronary arteries in the nephrotic syndrome. Analysis of 20necropsy patients aged 15 to 35 years to determine if coronary atherosclerosis is accelerated. Am J M ed .1977 Aug. 63(2):183-92. [Medline].
9. Mittal S K, Dash SC, Tiwari SC, Agarwal SK, S axena S, Fishbane S. Bone histology in patients withnephrotic syndrome and normal renal function. Kidney Int . 1999 May. 55(5):1912-9. [Medline].
10. Tessitore N, Bonucci E, D'Angelo A, Lund B, Corgnati A, Lund B, et al. B one histology and calcium
metabolism in patients with nephrotic syndrome and normal or reduced renal function. Nephron. 1984.37(3):153-9. [Medline].
11. Gulati S, Godbole M, Singh U, Gulati K, Srivastava A. Are children with idiopathic nephrotic syndrome atrisk for metabolic bone disease?. Am J K idney Dis. 2003 Jun. 41(6):1163-9. [Medline].
12. Leonard MB, Feldman HI, Shult s J, Zemel BS, Foster BJ, Stallings VA. Long-term, high-doseglucocorticoids and bone mineral content in childhood glucocorticoid-sensitive nephrotic syndrome. N Engl J Med . 2004 Aug 26. 351(9):868-75. [Medline].
13. Mahmoodi BK, t en Kate MK, Waanders F, Veeger NJ, Brouwer JL, Vogt L. High absolute risks andpredictors of venous and arterial thromboembolic events in patients with nephrotic syndrome: results from alarge retrospective cohort study. Circulation. 2008 Jan 15. 117(2):224-30. [Medline].
14. George BA, Zhou XJ, Toto R. Nephrotic syndrome after bevacizumab: case report and lit erature review. Am J K idney Dis. 2007 Feb. 49(2):e23-9. [Medline].
15. Lefaucheur C, St engel B, Nochy D, et al. Membranous nephropathy and cancer: Epidemiologic evidenceand determinants of high-risk cancer association. Kidney Int . 2006 Oct. 70(8):1510-7. [Medline].
https://adclick.g.doubleclick.net/aclk%253Fsa%253DL%2526ai%253DBoAF4lSzdVfKyGIqnoAP5vZdIur2E2gcAAAAQASC6_NYeOABYmvyivLsCYOmCgICEDrIBFmVtZWRpY2luZS5tZWRzY2FwZS5jb226AQlnZnBfaW1hZ2XIAQnaATVodHRwOi8vZW1lZGljaW5lLm1lZHNjYXBlLmNvbS9hcnRpY2xlLzI0NDYzMS1vdmVydmlld8ACAuACAOoCIy80MzEyNDM0L3Byb2Zwcm9tby9tZWRzY3ByZWZkZXNrdG9w-AL-0R6QA_QImAPgA6gDAdAEkE7gBAGQBgGgBh_YBwA%2526num%253D0%2526cid%253D5GjyA83XC5ejvOqB43jYi2Kw%2526sig%253DAOD64_1edSjDEFzjK5RN0LIQgr4qp0cEUQ%2526client%253Dca-pub-3100878564080714%2526adurl%253Dhttp://www.medscape.com/invitation/viewTracker.do?src=house_1ahttp://www.asn-online.org/http://www.ash-us.org/http://reference.medscape.com/medline/abstract/18391170http://reference.medscape.com/medline/abstract/10867533http://reference.medscape.com/medline/abstract/18158362http://www.afmr.org/http://reference.medscape.com/medline/abstract/14638928http://reference.medscape.com/medline/abstract/11703607http://www.acponline.org/http://www.aaas.org/http://www.myast.org/http://reference.medscape.com/medline/abstract/16941021http://www.kyma.org/http://www.pbk.org/home/index.aspxhttp://www.kidney.org/http://reference.medscape.com/medline/abstract/17261417http://reference.medscape.com/medline/abstract/6738766http://reference.medscape.com/medline/abstract/11979334http://www.asbmb.org/http://reference.medscape.com/medline/abstract/12776267http://reference.medscape.com/medline/abstract/888841http://www.asbmr.org/http://reference.medscape.com/medline/abstract/15329424http://www.theisn.org/http://reference.medscape.com/medline/abstract/10231454http://reference.medscape.com/medline/abstract/3858668http://reference.medscape.com/medline/abstract/3367561http://www.asn-online.org/http://www.theisn.org/
-
8/18/2019 Medscape 1-7 - Nephrotic Syndrome_ Background, Pathophysiology, Etiology
8/9
8/26/2015 Nephrotic Syndrome: Background, Pathophysiology, Etiology
http://emedicine.medscape.com/article/244631-overview#showall
16. Wong W. Idiopathic nephrotic syndrome in New Zealand children, demographic, clinical features, initialmanagement and outcome after twelve-month follow-up: results of a three-year national surveillance study.J Paediatr Child Health. 2007 May. 43(5):337-41. [Medline].
17. Kumar J, Gulati S, Sharma AP, S harma RK, Gupta RK. Histopathological spectrum of childhood nephroticsyndrome in Indian children. Pediatr Nephrol . 2003 Jul. 18(7):657-60. [Medline].
18. Ozkaya N, Cakar N, Ekim M, Kara N, Akkök N, Yalçinkaya F. Primary nephrotic syndrome during childhoodin Turkey. Pediatr Int . 2004 Aug. 46(4):436-8. [Medline].
19. Kazi JI, Mubarak M. Pattern of glomerulonephritides in adult nephrotic patients--report from SIUT. J Pak Med Assoc . 2007 Nov. 57(11):574. [Medline].
20. Barsoum R. The changing face of schistosomal glomerulopathy. Kidney Int . 2004. 66:2472-2484.
21. Doe JY, Funk M, Mengel M, et al. Nephrotic syndrome in Af rican children: lack of evidence for 'tropicalnephrotic syndrome'?. Nephrol Dial Transplant . 2006. 21:672-676.
22. Pakasa NM, Sumaili EK. The nephrotic syndrome in the Democratic Republic of Congo. N Engl J Med .2006 Mar 9. 354(10):1085-6. [Medline].
23. Sumaili EK , Krzesinski JM, Zinga CV, Cohen EP, Delanaye P, Munyanga SM, et al. Prevalence of chronickidney disease in Kinshasa: results of a pilot study from the Democratic Republic of Congo. Nephrol Dial Transplant . 2009 Jan. 24(1):117-22. [Medline].
24. Kopp JB, Winkler C. HIV-associated nephropathy in African Americans. Kidney Int Suppl . 2003 Feb. S43-9. [Medline].
25. Bonilla-Felix M, Parra C, Dajani T, Ferris M, Swinford RD, Portman RJ. Changing patterns in thehistopathology of idiopathic nephrotic syndrome in children. Kidney Int . 1999 May. 55(5):1885-90.[Medline].
26. Arneil GC, Lam CN. Long-term assessment of steroid therapy in childhood nephrosis. Lancet . 1966 Oct 15.2(7468):819-21. [Medline].
27. Donadio JV Jr, Torres VE, Velosa JA, Wagoner RD, Holley KE, Okamura M. Idiopathic membranousnephropathy: the natural history of untreated patients. Kidney Int . 1988 Mar. 33(3):708-15. [Medline].
28. Jude EB, Anderson SG, Cruickshank JK, et al. Natural history and prognostic factors of diabeticnephropathy in type 2 diabetes. Quart J Med . 2002. 95:371-7. [Medline].
29. Varghese SA, Powell TB, B udisavljevic MN, et al. Urine biomarkers predict the cause of glomerular disease. J Am Soc Nephrol . 2007. 18:913-22. [Medline].
30. Cohen EP, Lemann J. The role of the laboratory in evaluation of kidney function. Clin Chem. 1991. 37:785-796.
31. Gupta K, Iskandar SS, Daeihagh P, et al. Distribution of pathologic findings in individuals with nephroticproteinuria according to serum albumin. Nephrol Dial Transplant . 2008 May. 23(5):1595-9. [Medline].
32. Beck LH Jr, Bonegio RG, Lambeau G, et al. M-type phospholipase A2 receptor as target antigen inidiopathic m embranous nephropathy. N Engl J Med . 2009 Jul 2. 361(1):11-21. [Medline]. [Full Text].
33. Hofstra JM, Beck LH Jr, Beck DM, Wetzels JF, Salant DJ. Anti -phospholipase A2 receptor antibodiescorrelate with clinical status in idiopathic membranous nephropathy. Clin J Am Soc Nephrol . 2011 Jun.6(6):1286-91. [Medline]. [Full Text].
34. Palmer SC, Nand K, S trippoli GF. Interventions for minimal change disease in adults with nephroticsyndrome. Cochrane Database Syst Rev . 2008 Jan 23. CD001537. [Medline].
35. Waldman M, Crew RJ, Valeri A, Busch J, Stokes B, Markowitz G, et al. Adult mi nimal-change disease:clinical characteristics, treatment, and outcomes. Clin J Am Soc Nephrol . 2007 May. 2(3):445-53.[Medline].
36. Fervenza FC, Abraham RS, Erickson SB, et al. Rit uximab therapy in idiopathic membranous nephropathy:a two year study. Clin J Am Soc Nephrol . 2010. 5:2188-2198. [Medline].
37. Hibino S, Uemura O, Nagai T, Yamakawa S, Iwata N, It o H, et al. Three year outcome of childhoodidiopathic nephrotic syndrome under a unified immunosuppressive protocol. Pediatr Int . 2014 Sep 15.[Medline].
38. du Buf-Vereijken PW, Branten AJ, Wetzels JF. Idiopathic membranous nephropathy: outline and rationale
of a treatment strategy. Am J K idney Dis
. 2005 Dec. 46(6):1012-29. [Medline].39. Chen Y, Schieppati A, Chen X, Cai G, Zamora J, Giuliano GA, et al. Im munosuppressive treatment for
idiopathic membranous nephropathy in adults with nephrotic syndrome. Cochrane Database Syst Rev .2014 Oct 16. 10:CD004293. [Medline].
40. Gulati A, Si nha A, Jordan SC, Hari P, Dinda AK, Sharma S, et al. E fficacy and safety of treatment withrituximab for difficult steroid-resistant and -dependent nephrotic syndrome: multicentric report. Clin J AmSoc Nephrol . 2010 Dec. 5(12):2207-12. [Medline]. [Full Text].
41. Bomback AS, Tumlin JA, Baranski J, et al. T reatment of nephrotic syndrome with adrenocorticotropichormone (ACTH) gel. Drug Des Devel Ther . 2011 Mar 14. 5:147-53. [Medline]. [Full Text].
42. Bomback AS, Canetta PA, Beck LH Jr, Ayalon R, Radhakrishnan J, Appel GB. Treatment of resistantglomerular diseases with adrenocorticotropic hormone gel: a prospective trial. Am J Nephrol . 2012.36(1):58-67. [Medline].
43. Chen M, Li H, Li XY, et al. Tacrolimus Combined With Corticosteroids in Treatment of Nephrotic IdiopathicMembranous Nephropathy: A Multicenter Randomized Controlled Trial. Am J M ed Sci . 2010 Mar.
http://reference.medscape.com/medline/abstract/10231451http://reference.medscape.com/medline/abstract/3367560http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2994081/http://reference.medscape.com/medline/abstract/18253993http://reference.medscape.com/medline/abstract/12037245http://reference.medscape.com/medline/abstract/17489822http://reference.medscape.com/medline/abstract/12743793http://reference.medscape.com/medline/abstract/17699450http://reference.medscape.com/medline/abstract/4162167http://reference.medscape.com/medline/abstract/16310567http://reference.medscape.com/medline/abstract/20798255http://reference.medscape.com/medline/abstract/15310309http://reference.medscape.com/medline/abstract/20705965http://reference.medscape.com/medline/abstract/17301191http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3109923/http://reference.medscape.com/medline/abstract/22722778http://reference.medscape.com/medline/abstract/18715963http://reference.medscape.com/medline/abstract/25318831http://reference.medscape.com/medline/abstract/21474589http://reference.medscape.com/medline/abstract/21448451http://reference.medscape.com/medline/abstract/16525148http://reference.medscape.com/medline/abstract/12864874http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3063118/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2762083/http://reference.medscape.com/medline/abstract/19571279http://reference.medscape.com/medline/abstract/18065791http://reference.medscape.com/medline/abstract/18062530http://reference.medscape.com/medline/abstract/25225083
-
8/18/2019 Medscape 1-7 - Nephrotic Syndrome_ Background, Pathophysiology, Etiology
9/9
8/26/2015 Nephrotic Syndrome: Background, Pathophysiology, Etiology
http://emedicine medscape com/article/244631 overview#showall
Medscape Reference © 2011 WebMD, LLC
339(3):233-8. [Medline].
44. Roberti I, Vyas S. Long-term outcome of children with steroid-resistant nephrotic syndrome treated withtacrolimus. Pediatr Nephrol . 2010 Mar 9. [Medline].
http://reference.medscape.com/medline/abstract/20217433http://reference.medscape.com/medline/abstract/20220333