Medicine Health RHODEISLAND
36
UNDER THE JOINT EDITORIAL SPONSORSHIP OF: Brown Medical School Richard Besdine, MD, Dean of Medicine & Biological Sciences Rhode Island Department of Health Patricia Nolan, MD, MPH, Director Quality Partners of Rhode Island David Gifford, MD, Chief Medical Officer Rhode Island Medical Society David B. Ettensohn, MD, President EDITORIAL STAFF Joseph H. Friedman, MD Editor-in-Chief Joan M. Retsinas, PhD Managing Editor Stanley M. Aronson, MD, MPH Editor Emeritus EDITORIAL BOARD Stanley M. Aronson, MD Edward M. Beiser, PhD, JD Jay S. Buechner, PhD John J. Cronan, MD James P. Crowley, MD Edward Feller, MD John P. Fulton, PhD Peter A. Hollmann, MD Anthony Mega, MD Marguerite A. Neill, MD Frank J. Schaberg, Jr., MD Fred J. Schiffman, MD Lawrence W. Vernaglia, JD, MPH Newell E. Warde, PhD William J. Waters, Jr., PhD OFFICERS David B. Ettensohn, MD President Fredric V. Christian, MD Vice President Tilak K. Verma, MD, MBA President-Elect Diane R. Siedlecki, MD Secretary Peter A. Hollmann, MD Treasurer Yul D. Ejnes, MD Immediate Past President DISTRICT & COUNTY PRESIDENTS Pamela A. Harrop, MD Bristol County Medical Society Gary A. L’Europa, MD Kent County Medical Society Jayanthi Parameswaran, MD Newport County Medical Society Stephen T. Conway, MD Pawtucket Medical Association Patrick J. Sweeney, MD, PhD, MPH Providence Medical Association R. Scott Hanson, MD Washington County Medical Society Naeem M. Siddiqi, MD Woonsocket District Medical Society R HODE I SLAND Medicine Health PUBLICATION OF THE RHODE ISLAND MEDICAL SOCIETY VOLUME 86, NO. 7 JULY, 2003 Medicine and Health\Rhode Island (USPS 464-820), a monthly publication, is owned and published by the Rhode Island Medical Society, 235 Promenade St., Suite 500, Providence, RI 02908, Phone: 401-331-3207. Single copies $5.00, individual subscriptions $50.00 per year, and $100 per year for institutional subscriptions. Published articles represent opinions of the authors and do not necessarily reflect the official policy of the Rhode Island Medical Society, unless clearly specified. Advertisements do not imply sponsorship or endorsement by the Rhode Island Medical Society. Periodicals postage paid at Providence, Rhode Island. ISSN 1086-5462. POSTMASTER: Send address changes to Medicine and Health\Rhode Island, 235 Promenade St., Suite 500, Providence, RI 02908. Classified Information: RI Medical Journal Marketing Department, P.O. Box 91055, Johnston, RI 02919, phone: (401) 383-4711, fax: (401) 383-4477, email: [email protected] Cover: “Beach Balls,” oil on canvas, by Lorraine Shemesh, formerly Assistant Professor of Fine Arts, Rhode Island School of Design. Private collection, www.lorraineshemesh.com, courtesy of the Allan Stone Gallery. COMMENTARIES 190 On Reviewing Manuscripts Joseph H. Friedman, MD 191 Where Are the Words To Heal? Stanley M. Aronson, MD, MPH DISASTER PREPAREDNESS: A CME ISSUE Guest Editor: Robert Woolard, MD 192 Introduction Robert Woolard, MD 193 The Hospital Emergency Incident Command System—Are You Ready? Liudvikas Jagminas, MD, and Gary Bubly, MD 196 Disaster Medicine: The Potential Role of High Fidelity Medical Simulation for Mass Casualty Incident Training Leo Kobayashi, MD Marc J. Shapiro, MD, Selim Suner, MD, and Kenneth A. Williams, MD 201 Biodefense: Medicine in the Time of Bioterrorism Andrew W. Artenstein, MD 204 Emergency Department Design After 9/11/2001 Robert Woolard, MD, Melisa Lai, MD, Marc J. Shapiro, MD, Leo Kobayashi, MD, Gregory Jay, MD, PhD, Selim Suner, MD, MS, FACEP, Kenneth Williams, MD, FACEP, and Francis Sullivan, MD 207 Rhode Island Disaster Initiative Kenneth Williams, MD, Selim Suner, MD, Francis Sullivan, MD, and Robert Woolard, MD 211 CME Background Information COLUMNS 213 The Creative Clinican Case FIRST CASE OF WEST NILE INFECTION IN RHODE ISLAND Haris Mirza, MD, Shimae Cross, Maria Mileno, MD 216 Quality Partners of Rhode Island 217 Health by Numbers HEALTH RISK DISPARITIES AMONG RHODE ISLAND ADULTS, 2001 Jana E. Hesser, PhD 219 Public Health Briefing PROGRESS IN CONTROL OF OROPHARYNGEAL CANCER IN RHODE ISLAND, 1987–2000 John P. Fulton, PhD, Dorothy M. Darcy, CTR, and Leanne Chiaverini 222 A Physician’s Lexicon THE CEREBRAL HEMISPHERES Stanley M. Aronson, MD, MPH 222 Vital Statistics 224 Rhode Island Medical Journal Heritage
Transcript of Medicine Health RHODEISLAND

UNDER THE JOINTEDITORIAL SPONSORSHIP OF:
Brown Medical SchoolRichard Besdine, MD, Dean of Medicine& Biological Sciences
Rhode Island Department of HealthPatricia Nolan, MD, MPH, Director
Quality Partners of Rhode IslandDavid Gifford, MD, Chief Medical Officer
Rhode Island Medical SocietyDavid B. Ettensohn, MD, President
EDITORIAL STAFFJoseph H. Friedman, MD
Editor-in-ChiefJoan M. Retsinas, PhD
Managing EditorStanley M. Aronson, MD, MPH
Editor Emeritus
EDITORIAL BOARDStanley M. Aronson, MDEdward M. Beiser, PhD, JDJay S. Buechner, PhDJohn J. Cronan, MDJames P. Crowley, MDEdward Feller, MDJohn P. Fulton, PhDPeter A. Hollmann, MDAnthony Mega, MDMarguerite A. Neill, MDFrank J. Schaberg, Jr., MDFred J. Schiffman, MDLawrence W. Vernaglia, JD, MPHNewell E. Warde, PhDWilliam J. Waters, Jr., PhD
OFFICERSDavid B. Ettensohn, MD
PresidentFredric V. Christian, MD
Vice PresidentTilak K. Verma, MD, MBA
President-ElectDiane R. Siedlecki, MD
SecretaryPeter A. Hollmann, MD
TreasurerYul D. Ejnes, MD
Immediate Past President
DISTRICT & COUNTY PRESIDENTSPamela A. Harrop, MD
Bristol County Medical SocietyGary A. L’Europa, MD
Kent County Medical SocietyJayanthi Parameswaran, MD
Newport County Medical SocietyStephen T. Conway, MD
Pawtucket Medical AssociationPatrick J. Sweeney, MD, PhD, MPH
Providence Medical AssociationR. Scott Hanson, MD
Washington County Medical SocietyNaeem M. Siddiqi, MD
Woonsocket District Medical Society
RHODEISLANDMedicine Health�
PUBLICATION OF THE RHODE ISLAND MEDICAL SOCIETY
VOLUME 86, NO. 7 JULY, 2003
Medicine and Health\Rhode Island (USPS 464-820), a monthly publication, is owned and published by the Rhode Island Medical Society,235 Promenade St., Suite 500, Providence, RI 02908, Phone: 401-331-3207. Single copies $5.00, individual subscriptions $50.00 per year,and $100 per year for institutional subscriptions. Published articles represent opinions of the authors and do not necessarily reflect the officialpolicy of the Rhode Island Medical Society, unless clearly specified. Advertisements do not imply sponsorship or endorsement by the RhodeIsland Medical Society. Periodicals postage paid at Providence, Rhode Island. ISSN 1086-5462. POSTMASTER: Send address changes toMedicine and Health\Rhode Island, 235 Promenade St., Suite 500, Providence, RI 02908. Classified Information: RI Medical JournalMarketing Department, P.O. Box 91055, Johnston, RI 02919, phone: (401) 383-4711, fax: (401) 383-4477, email: [email protected]
Cover: “Beach Balls,” oil on canvas, byLorraine Shemesh, formerly AssistantProfessor of Fine Arts, Rhode IslandSchool of Design. Private collection,www.lorraineshemesh.com, courtesy ofthe Allan Stone Gallery.
COMMENTARIES
190 On Reviewing ManuscriptsJoseph H. Friedman, MD
191 Where Are the Words To Heal?Stanley M. Aronson, MD, MPH
DISASTER PREPAREDNESS: A CME ISSUEGuest Editor: Robert Woolard, MD
192 IntroductionRobert Woolard, MD
193 The Hospital Emergency Incident Command System—Are You Ready?Liudvikas Jagminas, MD, and Gary Bubly, MD
196 Disaster Medicine: The Potential Role of High Fidelity Medical Simulation forMass Casualty Incident Training
Leo Kobayashi, MD Marc J. Shapiro, MD, Selim Suner, MD, andKenneth A. Williams, MD
201 Biodefense: Medicine in the Time of BioterrorismAndrew W. Artenstein, MD
204 Emergency Department Design After 9/11/2001Robert Woolard, MD, Melisa Lai, MD, Marc J. Shapiro, MD, Leo Kobayashi, MD,Gregory Jay, MD, PhD, Selim Suner, MD, MS, FACEP, Kenneth Williams, MD,FACEP, and Francis Sullivan, MD
207 Rhode Island Disaster InitiativeKenneth Williams, MD, Selim Suner, MD, Francis Sullivan, MD, andRobert Woolard, MD
211 CME Background Information
COLUMNS
213 The Creative Clinican CaseFIRST CASE OF WEST NILE INFECTION IN RHODE ISLAND
Haris Mirza, MD, Shimae Cross, Maria Mileno, MD
216 Quality Partners of Rhode Island
217 Health by NumbersHEALTH RISK DISPARITIES AMONG RHODE ISLAND ADULTS, 2001Jana E. Hesser, PhD
219 Public Health BriefingPROGRESS IN CONTROL OF OROPHARYNGEAL CANCER IN RHODE ISLAND,1987–2000John P. Fulton, PhD, Dorothy M. Darcy, CTR, and Leanne Chiaverini
222 A Physician’s LexiconTHE CEREBRAL HEMISPHERES
Stanley M. Aronson, MD, MPH
222 Vital Statistics
224 Rhode Island Medical Journal Heritage

190Medicine and Health / Rhode Island
COMMENTARIES� �
�On Reviewing Manuscripts
To the editor: I have not enjoyedreading a manuscript this much sincethe Journal of Irreproducible Resultsclosed down. Unfortunately I don’tthink the authors intended their ms toproduce these chuckles.
To the editor: Dr. Jones, and I as-sume that he wrote this piece himselfsince I doubt that anyone would wantto take credit for it, should be referredfor a brain MRI. He seems to be suf-fering both from aphasia andhypergraphia, suggesting the likelihoodof left posterior and right medial tem-poral lobe lesions.
To the editor: This case controlstudy is interesting only because of thecomparison group used. The relevanceof the comparators to the cases is nostronger than would be a control groupof Canadian geese. Or maybe not.
When one reviews articles for peerreviewed journals there is an occasionaltemptation to be sarcastic, to displayone’s rapier wit, demonstrating, afterprolonged consideration, “le motjuste,” making up for all those disap-pointing moments when one’s repar-tee in real time falls short of the mark,followed by the thought of a devastat-ing response a few seconds too late. Idon’t think I’ve ever done this, takenthese pot shots. For one thing there’san unfair advantage, being an anony-mous reviewer and having a defense-less opponent. For another I am oftenon the receiving end of critical com-mentaries. Although these pot shotsare purely for the journal’s editors anddon’t go back to the authors, refereeslower themselves by debasing others’work.
I attended a meeting recently,which included the editors of threemajor journals. Despite my role aseditor of this journal (and two corpo-rate-sponsored journals, one for laypeople and one for neurologists,) I did
not consider myself in their league.They compared notes on numbers ofsubmissions, percentage of acceptan-ces, turn-around time and exchangeda few anecdotes. Their experiences andmine have been quite different.
However, the discussion thenturned to manuscript reviews and theplaying field leveled. I review all manu-scripts to this journal, but our accep-tance rate is pretty high since mostarticles are solicited and we don’t re-ceive too many unsolicited articles. Ialso submit my own manuscripts toother journals and review a fair num-ber of submissions to a variety of jour-nals.
I never thought too much aboutthe time I spent reviewing otherpeople’s works. After all, someone re-views mine. So I was shocked to learnthat some neurologist had persistentlyrefused to review submissions to a jour-nal in which he himself publishes. Hewas too busy. In other words, I maybe asked to provide a peer review ofhis work but he’s too busy to reviewmine. I wondered about the ethics ofbanning him from future submissionsto the journals he’s too busy to refereefor.
A more relevant issue, especiallyfor those of us who do review manu-scripts is how to do this. The editorswere lamenting the lack of skill of somereviewers and one told the followingstory.
When he was a post-doctoral fel-low in the lab of a famous scientist whosubsequently won a Nobel Prize, he wasasked to review a paper submitted to ajournal the famous scientist edited. Allsuch reviews are anonymous to encour-age both candor and honesty. Unfor-tunately anonymity can also provide amask for contempt and ill-will. Thepost-doc ardently reviewed the paper,tearing it to shreds. The older doctorgave it back and said, “You did a won-
derful job. Your analysis was com-pletely correct. I agree with everythingyou said. You found all the problemsand exposed all the weaknesses. Butyou need to remember that a paper islike the author’s child. She’s invested alot of time, effort and loving care soyou need to critique it in the same wayyou’d critique the performance of thechild of a friend. You should be hon-est but gentle and always keep in mindthat the paper’s “parents” love it evenif you think it’s rotten. So, be as care-ful in how you convey the message asyou are in formulating the message.”
I think this is good advice. I liketo think of the review process as beingakin to reading your child’s essay forschool. On the one hand, you wantthe child to get the best grade possible,so you try to provide constructive criti-cism, but on the other hand, you don’twant to undermine the child’s confi-dence by being overly critical or de-structive. Even if you recommendagainst publishing the article, yourcomments should be used by the au-thors as constructive advice in reword-ing the manuscript for submissionelsewhere.
– JOSEPH H. FRIEDMAN, MD

191Vol. 86 No. 7 July 2003
�Where Are the Words To Heal?
Toward the end of the 19th Century, and for the first time inthis nation’s history, there were more foreign-born than
native-born residents. The United States had truly become anation of immigrants. A steady flow of newcomers, both docu-mented and undocumented, continues to define the characterand ethnic composition of this country. And while a small frac-tion of the newly-arrived Americans originate from English-speaking nation, the great majority come from over one hundreddifferent nations speaking languages other than English.
In the last decade this nation has admitted 9,095,417 docu-mented immigrants. Presently there are an estimated 19 mil-lion adult American residents who speak no English.
The overwhelming majority of current immigrants are dis-tinguishable, on average, from their native-born neighbors by anumber of attributes: They are poorer, less educated, less con-versant in the English language and more likely to be burdenedby nutritional or infectious disease. Many possess no workingknowledge of English, its nuances, subtexts, ambiguities or col-loquialisms. And thus the very segment of the American popu-lation needing the greatest measure of medical help is also thatsegment with the least capacity to identify and explain theirsymptoms or provide a pertinent medical history. The medicalprofession now confronts an expanding portion of the Ameri-can population incapable of fully understanding therapeuticinstructions when rendered in English.
Three overlapping solutions to lessen this problem presentthemselves. First, train the primary care physicians to bepolylingual. [Actually, the Brown Medical School has offeredevening classes in Portuguese and Spanish to its students.] Sec-ond, more actively encourage the newly arrived immigrants tolearn English. And third, develop a cadre of bilingual transla-tors to assist in the process of medical history-taking.
Each of these solutions, though, presents substantial prob-lems.
The nature of modern medical education requires an in-creasingly stringent curriculum. More and more of the medicalstudent’s hours are now absorbed in learning newer technicalskills, newer bodies of data, leaving virtually no free time forlearning new languages.
Recruiting bilingual translators presents certain financialand ethical problems. The foundation of the patient-physicianrelationship is the unyielding promise of confidentiality. But atranslator, even one sworn to privacy, adds yet another poten-tial threat to this promise; and few clinics or hospitals can af-ford to maintain translators skilled in each of the many languagesspoken by their patients. Using family members also subvertsthe policy of medical confidentiality and may create intenseembarrassment for the adult patient, particularly so since theonly bilingual members of the family tend to be the children.
On the other hand, given the sophisticated nature of mod-ern diagnostic procedures such as CT scans, does it really makea difference whether or not the patient and the physician cancommunicate with each other in accurate English? Has accessto, and exploitation of, the health care system by many millionsof non-English speaking patients been compromised becauseof a language barrier between patient and physician?
Additionally, can we be certain that the translators faith-fully translate the crucial words from patient to doctor, and
then back again? Or are critical words – and therefore patients –being lost in translation? An analysis of the recorded translationsin a series of clinic encounters in Milwaukee and in Boston indi-cates that translators do represent a palpable risk. During thecourse of 13 taped clinic visits, the examiners noted 231 errors,over all of them judged to be potentially dangerous to the patient’swelfare. The authors of this study, appearing in Pediatrics, notedparenthetically that a single translational error caused one Floridahospital to lose a malpractice judgment for $22 million dollars.
Despite the intimidating machinery of modern medicine,the core, the very heart of medicine, remains the art of talkingand listening to the patient – in his or her language. Medicinefunctions best when there is mutual respect, time to exchangeviews, hopes and fears, a fervent belief in the confidentiality ofthe encounter, and the capacity of both parties to understandprecisely what the other is saying. Only then is there a high prob-ability of patient satisfaction and patient compliance. Increas-ingly, medical schools now insist on the critical importance ofaccurate communication, particularly so because many of thoseseeking medical attention are unfamiliar with English.
But even with those who speak and understand fluent En-glish, there remains the inescapable need for accurate communi-cation, precise words that diminish the likelihood of alternativeinterpretation. Physicians must rely upon language, accurate lan-guage, first to understand the messages spoken by their anguishedpatients, and second to provide explanations, prognostic specu-lations and therapeutic instructions to their patients. Has thisdistressed person, distracted by anxiety and with a shortened at-tention span, truly heard, understood and remembered thephysician’s instructions?
An incident in Bellevue Hospital, New York City, back inthe 1940s is worth recalling. At the Monday morning diabetesclinic a middle-aged, unmarried diabetic man, in order to pre-vent infections to his diseased toes, was instructed to put on afresh pair of clean white socks each morning. He did not appearfor his regularly scheduled clinic visit the next Monday morn-ing. A telephone call by a concerned social worker found outthat he couldn’t keep his appointment because his shoes wouldnot fit over all of those accumulated socks. This was not patientnon-compliance; rather, this was a vain attempt by the patient tofollow ambiguous instructions.
Another example of faulty communication: Some years agothe newspapers carried the story of a mother who bought a boxof animal crackers for her four year-old daughter. Instead of eat-ing the crackers, the child carefully spread out the animal pro-files upon the kitchen table, carefully examining each one. Thepuzzled mother asked: “What are you seeking?” The child re-sponded: “I’m looking for the seal.” “Why?” The child declared:“You told me not to eat any crackers if the seal is broken.”
Both miscommunication and the lack of communicationbring an unwanted menace to the practice of medicine. And thatelusive thing called humanism in medicine rests principally inthe words exchanged between patient and physician. Certainlywithout accurate and meaningful verbal interchange, as one phy-sician observed, it is like practicing veterinary rather than hu-man medicine.
– STANLEY M. ARONSON, MD, MPH

192Medicine and Health / Rhode Island
�Introduction
This issue of Medicine & Health/ Rhode Island is thefirst of a two-part series, 10 articles that will address
disaster response and preparedness both in Rhode Islandand by Rhode Island physicians. This first issue is dedi-cated to disaster preparedness. After 9/11/01, physicians,health care workers, public officials and the public at largewant to know whether we are prepared for other foresee-able terror-related disasters.
This issue describes many of the pre-hospital and emer-gency medicine efforts that have made us prepared in RI.Many of these efforts will continue into the next few years.There are efforts within agencies such as state police, emer-gency management and the department of health that havenot been detailed in this issue. No doubt we are better pre-pared than before 9/11/01 and will be even better preparedover the next two years as an anticipated $11,000,000 flowsinto R.I. from Homeland Security and other sources. Ar-ticles in this issue address information needs, pre-hospitalsystem needs, educational needs, Emergency Departmentand hospital capacity needs and ED-based hospital pre-paredness—issues all being addressed in Rhode Island.
Rhode Island has the opportunity to demonstrate amodel “disaster ready” system for the nation due to theexpertise of local emergency physicians, the manageablepopulation and geographic size, the ease of access to fed-eral programs and the potential coordination between agen-cies. To help this coordination, efforts of the Rhode IslandDisaster Initiative began before 9/11/01 and are fundedinto 5/05/05.
Many disaster and terrorism experts consider an eventwith up to 4,000 victims needing decontamination likelyand much of our planning focuses on preparing to meetthese needs. Even the best plan can be overwhelmed. Adisaster or mass casualty event is defined as one that over-
whelms local or routinely available resources. All physiciansshould become and stay familiar with their hospital and com-munity disaster plans, identify websites with informationon response to terrorism and participate in disaster drills,including planning and debriefing. Even with better tech-nology, more equipment, new surge capacity, immunizationand new paradigm for more coordinated response, many localand regional drills must be conducted with physician par-ticipation to develop and maintain readiness. For the read-ership of this journal the message must be “act locally”, getinvolved in disaster efforts.
Clearly much of our approach to prepare ourselves fora large-scale event (4,000 victims) will be on paper. Few ofour drills will test our system to this level. Resources re-quired for this magnitude of casualties will tax the New En-gland region.
National Disaster Medical System with D-MAT teamswill be called into action. Sharing admitted patients regionaltertiary and trauma centers will be needed. However, pre-paring locally will provide the backbone of the response todisaster at all magnitudes of casualties.
– ROBERT WOOLARD, MD
Robert Woolard, MD, is Chairman of the Section of Emer-gency Medicine, and Associate Professor of Medicine, BrownMedical School.
CORRESPONDENCE:Robert Woolard, MDChairman of the Section of Emergency MedicineBrown Medical School593 Eddy StreetProvidence, RI 2903Phone: (401) 444-5826Fax: (401) 444-4307E-mail: [email protected]
ACKNOWLEDGEMENT: Special thanks to Alana Ducharmefor organization and continuous improvement of the articlesin these two issues.

193Vol. 86 No. 7 July 2003
�The Hospital Emergency Incident Command System
—Are You Ready?
Liudvikas Jagminas, MD, and Gary Bubly, MD
Medical disasters often cause greatconfusion and inefficiency in
hospitals. Disasters can overwhelm ahospital’s resources: staff, space, or sup-plies. Mass casualty incidents challengehospitals already running at seeminglymaximal capacity and struggling to rem-edy inpatient and emergency depart-ment overcrowding. In addition,hospitals must prepare for the possibil-ity of being the victim or site of a disas-ter.
Disasters can impact a hospital’sphysical plant in ways that radically al-ter the environment of care, such asstructural damage occurring in an earth-quake or hurricane, or the sudden lossof electricity or water. Experience withseveral disasters in the last few decadesdemonstrates that an organized disasterresponse system for hospitals is invalu-able and can reduce mortality.1 Integralcomponents of an organized responseinclude clearly identified leadership,well-outlined responsibilities, effectivecommunication, and the capacity tointeract and coordinate with other hos-pitals and governmental agencies. Inci-dent command systems are responseplans designed to incorporate these fea-tures in the management of disasters.The Joint Commission on Accredita-tion of Healthcare Organizations(JCAHO) mandates hospitals developdisaster plans which identify their com-mand structure and recommends theyshare this information with surround-ing facilities.2 These systems have beenmodified for use in hospitals and areavailable on the Internet as the Hospi-tal Emergency Incident CommandSystem (HEICS).3 This article reviewsthe history and features of the HEICS.
HEICS’ origins can be traced backto the 1980s, when a multi-jurisdic-tional committee represented by local,state, and federal authorities created thefirst Incident Command System,known as FIRESCOPE. This system
eventually became the command systemof choice for almost every fire depart-ment in the country. In 1987, the Hos-pital Council of Northern Californiaadapted FIRESCOPE for use in re-sponse to earthquakes.
California’s Orange County Emer-gency Medical System (EMS) devel-oped HEICS in 1991, customizing thecommand system to the hospital envi-ronment and management system. Thisinitial version underwent modificationtwice before the third and currently usededition was developed. This final ver-sion is being implemented across thecountry as hospitals strive for greatercertainty and accountability in the wakeof recent disasters around the nation.This system has been successfully usedin several disasters. In a 1997 survey ofCalifornia hospitals, 39 of 115 had usedHEICS in an actual hospital response.4
Of those who used HEICS in a disas-ter, 82% reported their experience as“positive.” Although HEICS is not apanacea, hospitals using it reportedlyfunctioned better in response to the1993 earthquake in Northridge thanthose not using the plan.5
HEICS offers benefits not foundwith other disaster management sys-tems. These include:
• Predictable chain of command• Applicability to varying types
and magnitudes of disasters• Accountability for specific func-
tions• Thorough documentation of
actions taken• Common terminology to pro-
mote communication• Flexibility and cost effectiveness
within organizations
HEICS does not replace butcomplements a hospital’s existing disas-ter/emergency preparedness plan.Proper emergency preparedness requiresup-to-date policies and procedures fordealing with specific issues such as mass
casualty, nuclear, biological, chemical aswell as natural disasters to be in place.In addition, hospital emergency pre-paredness policies must specify who isable to initiate the Disaster Plan, out-line staff recall procedures, designate adecontamination location and proce-dures for specific agents if required, tri-age sites, staging and assembly areas,debriefing, etc.
The benefits of the HEICS plan tofunction during any sort of mass casu-alty incident, regardless of its etiology,lies in the plan’s predictable, reproduc-ible chain of command, accountabilityof position function, the flexibility ofresponse to specific emergencies, priori-tized response checklists and the use ofcommon language to facilitate interac-tion with the hospital, other hospitalsusing the HEICS plan and governmentagencies.
Once the plan is activated, HEICSis implemented within a hospital by as-signing jobs to managers, their desig-nees, or the most competent personavailable at the time the command sys-tem is initiated. While hospitals shouldplan who will optimally fill specific po-sitions, theoretically anyone can fill anyrole in the chain of command. The In-cident Commander role is assigned firstand has overall responsibility for man-agement of the entire facility during theoperation. This may be the hospitalpresident or designee, or may tempo-rarily be an individual on-site such as anight nursing supervisor or emergencyphysician. Activities under the supervi-sion of the Incident Commander arebroadly divided into the areas of logis-tics, planning, finance, and operations.A Section Chief is appointed to headeach of these four divisions. They over-see the remaining staff leadership posi-tions in each division, and report to theIncident Commander.
From a mass casualty perspective,the cause of the event does not affectthe HEICS system. The inciting event,

194Medicine and Health / Rhode Island
�
HEICS has been used infacilities as diverse as
Level I Trauma Centersand small community
hospitals.
however, may require mobilization ofdifferent parts of HEICS. For example,in a fire such as the recent Station firein Rhode Island, the mass casualty as-pect would mobilize all hospital person-nel since multi-system injuries shouldbe expected, even though the bulkwould be primarily focused on burn careand pulmonary injuries. However, if amass casualty event were secondary to achemical or biological incident, thenHEICS along with the decontaminationprocedures already in place at the hos-pital would be activated.
The responsibilities of every posi-tion in the tree are delineated on “jobaction sheets,” which are distributed tothe individual assigned to each role.(Figure 1) These “job actions” are sub-divided into “immediate”, “intermedi-ate”, and “extended” time frames to helpthe assigned individuals prioritize theirtasks. Hospitals should customize thelist of job actions for each position tosuit their facilities’ needs. These may beeasily adapted from their facilities’ ex-isting disaster plans. Each job actionsheet also explicitly states whom the as-signed individual should report to, andwhom they need to get reports from.Thus, the job action sheets prompt in-dividuals to perform critical duties andenhance communication, keeping themfocused during times of chaos.
A large part of the flexibility ofHEICS lies in the tree and the job ac-tion sheets. For example, more than oneposition and job action sheet can begiven to a particular individual, or cer-tain parts of the plan may not be usedat all. The entire tree of positions may
be deployed in a mass casualty incident,which necessitates utilizing the full spec-trum of a hospital’s staff and resources.On the other hand, an internal prob-lem such as a power outage on one floormay be more efficiently managed byactivating only part of the tree, with onlya few individuals providing critical roles.Because key staff may be unavailable,or may even be victims of a disaster, thejob action sheets help guide remainingpersonnel in managing the event.
These features of HEICS also con-
fer adaptability for use in differenthealth care settings. HEICS has beenused in facilities as diverse as Level ITrauma Centers and small commu-nity hospitals. (Figure 1) A modifiedversion for outpatient clinics and urgentcare centers entitled the Medical AidStation Incident Command Center hasalso been developed.4 Large-scale disas-ters may require the involvement of ur-gent care centers to manage high patientvolumes. Again, coordination withother facilities and agencies would beenhanced if all involved understandHEICS terminology.
The number of hospitals usingHEICS grows, perhaps due to its obvi-
ous advantages, perhaps due to regula-tory compliance issues. In Californiaalone, 56% of hospitals surveyed in1997 were already using HEICS.4 In a1999 survey of hospitals in New YorkCity, 90% of respondents described us-ing the incident command systemmodel in their disaster plans.5 Further-more, hospitals in Canada are using it,and requests for implementation assis-tance have been received from Germany,New Zealand, Japan, South America,and Saudi Arabia.
Rhode Island has been no excep-tion, having made great strides in adopt-ing HEICS. According to the HospitalAssociation of Rhode Island, several ofthe 15 participating hospitals in the statereport some degree of implementationof HEICS. For example, Rhode IslandHospital and The Miriam Hospital haverewritten their disaster plans in theHEICS format. Both hospitals haveheld training sessions to introduce man-agers and staff to HEICS, run tabletopexercises to increase familiarity with thesystem, and conducted live drills inHEICS to evaluate its effectiveness. Inaddition, HEICS was tested in many ofthe area hospitals participating in thestatewide disaster exercise in June, 2002,with excellent results. It is expected thatrepeated exercises will build competencein using the system. The HEICS manualand other references6,7 include sugges-tions on how to apply the plan and pro-vide scenarios for exercises. The RhodeIsland Emergency Management Agencyis urging Rhode Island hospitals to con-vert to the HEICS system, to elevate ourdisaster preparedness and coordinate ouroverall response efforts.
Obstacles frequently arise whenhospitals make plans to convert to theHEICS model. Managers may believeit will be too difficult to change exist-ing plans. Some hospitals have felt thatthe system is too cumbersome and con-voluted. Further concerns deal with theexpense of converting, as well as staffreactions to the new system. Most fa-cilities, however, find that implementa-tion of the system is simpler thanexpected. The HEICS Manual and thetemplates for the job action sheets areavailable on the Internet free of charge.The expense of implementation is

195Vol. 86 No. 7 July 2003
mostly due to employee training.4 Fur-thermore, most staff understand theflexibility and appreciate the simplicityof HEICS after initial training.
In summary, HEICS has proven tobe a flexible and easily implementedsystem for disaster response that can beintegrated into hospitals’ disaster plans.It has a record of reliability and cost ef-fectiveness. HEICS facilitates commu-nication and coordination betweenhospitals and the many local, state andfederal agencies typically involved indisasters. Physicians should familiarizethemselves with HEICS while imple-mentation continues across the nation,and in Rhode Island.
REFERENCES1. Schultz CH, Koenig KL, Noji EK. Cur-
rent concepts: A medical disaster re-sponse to reduce immediate mortalityafter an earthquake. NEJM 1996;334:438-44.
2. Using JCAHO standards as a startingpoint to prepare for an emergency.www.jcrinc.com/subscribers/
3. San Mateo County EMS Agency TaskForce. Hospital Emergency IncidentCommand System Version 3. http://www.emsa.ca.gov/dms2/heics3.htm
4. Hospital Emergency Incident Com-mand System http://www.ncha.org/public/docs/bioterrorism/HEICS.pdf
5. Silber SH, Oster N, Simmons B, et al.Y2K medical disaster preparedness inNew York City: Confidence of emer-gency department directors in their abil-ity to respond. Prehospital DisasterMedicine 2001;16:88-94.
6. Londorf D. Hospital application of theincident management system.Prehospital Disaster Medicine 1995;10:184-88.
7. Huser TJ. Implementing the incidentcommand system in the healthcare set-ting. J Healthc Prot Manage1997;14:48-54.
Liudvikas Jagminas, MD, FACEP,is Assistant Professor of Surgery, BrownMedical School, and Attending Physician,Department of Emergency Medicine,Rhode Island Hospital.
Gary Bubly, MD, FACEP, is Clini-cal Assistant Professor of Medicine, BrownMedical School, and Associate Director,Department of Emergency Medicine, TheMiriam Hospital.
CORRESPONDENCE:Liudvikas Jagminas, MD, FACEPRhode Island Hospital593 Eddy StreetProvidence, RI 02903Phone: (401)-444-5826Fax: (401)-444-4307e-mail: [email protected]

196Medicine and Health / Rhode Island
�Disaster Medicine: The Potential Role of High Fidelity
Medical Simulation for Mass Casualty Incident Training
Leo Kobayashi, MD, Marc J Shapiro, MD, Selim Suner, MD, Kenneth A Williams, MD
With a dramatic increase in highlyvisible and costly mass casualty
incidents over the past few decades, di-saster planning and preparedness nowrepresent a prominent part of healthcare policy and practice. Apart fromthe upsurge in natural calamities thathas accompanied population growthand dispersal as well as global climac-tic change, willful acts of mass destruc-tion and indiscriminate injury havealso cropped up at a disturbing rate.Consequently, significant effort hasbeen directed towards improving theinitial management of disastrous eventsthrough anticipatory and mitigatoryinterventions.
The study of disaster medicine,focusing on pre-event planning, emer-gent medical care and public healthmeasures, has matured rapidly in thepast few years through quantum leapsin networking, communications, andcomputer technologies. Examinationof prior events and intercession withongoing disasters has become muchmore sophisticated, timely, and perti-nent. We now have the opportunityto apply hard-won knowledge to pre-pare for the next catastrophe.
Implementation of preventive,preparatory, and training protocols hasbeen avidly recommended in the hopeof minimizing the harmful conse-quences of these large-scale events.1,2
Proactive educational exercises mayalso serve to lessen the loss of life, limb,and property.3 Such measures mayrange from simple regular fit-testing ofprotective gear, to complex multifac-torial computer simulations evaluatinghospital bed availability in the eventof a community-wide disaster.4
CURRENT DISASTER TRAINING
Who needs to be trained?For rescue workers potentially re-
sponding to mass casualty incidents,adequate training must be established,implemented, and maintained to en-
sure their safety, the optimal care oftheir patients, and the best interest ofthe public. In some form, these ef-forts should reach prehospital andhospital-based healthcare providers,law enforcement, fire department per-sonnel, and disaster relief organiza-tions (e.g. American Red Cross).Hospital, state and federal adminis-trators need to be active participantsin disaster education and become pro-ficient in incident management, re-source planning and allocation, andinteragency coordination.
Who thinks we should train?With significant cost and effort, the
US Department of Health and HumanServicesí Office of Emergency Responsehas developed a standardized Web-basedprogram for all National Disaster Medi-cal System (NDMS) field teams. TheDepartment of Defense has been in-volved with a weapons of mass destruc-tion (WMD) Domestic PreparednessProgram for health care providers, butavailability is limited.5 Several organi-zations, including the American College
of Emergency Physicians (ACEP), haverecommended the inclusion of disastereducation in prehospital, nursing, medi-cal school, residency, and post-gradu-ate curricula.2,6 Notably, the AmericanRed Cross has developed a training cen-ter geared to prepare its workers for situ-ations involving WMDs.
What needs to be taught?Educational experiences for disas-
ter responders must be accurate, thor-ough, relevant, and up-to-date. Theyneed to impart a specialized medicalknowledge-base and increase the inter-face with other agencies. Dissemina-tion of key factual knowledgeencompassing natural, bioweapon,chemical and nuclear hazards has to takeplace. Furthermore, the basic tenets ofdisaster management ñ triage, decon-tamination, communications, incidentcommand, transport ñ have to be suc-cessfully conveyed. The ability to rap-idly form multi-disciplinary work teamsthat communicate and function effec-tively has to be cultivated. Relevant ar-eas of expertise generally beyond thescope of basic training are crisis psychol-ogy, tactical training, and hazardousmaterials (HazMat).
Adding to the complexity of di-saster training is the need to teach spe-cific and unique skill sets, which areuncommonly utilized, yet will need tobe performed efficiently when the needarises. As no amount of training willbe able to fully prepare for all contin-gencies, a flexible and dynamic ap-proach to disaster response has to beencouraged. Finally, attrition ofknowledge after training is to be ex-pected, creating the need for ongoingtraining and refresher courses.
How do we currently train?Lectures and seminars are a large
component of any disaster curriculum.Emergency Medical Technician (EMT)courses at all levels incorporate presen-
�
Computer-drivenmanikins cost $30,000to $200,000 and are
capable of verbalcommunication, accuraterepresentation of physicalexam findings (airwaycompromise, lung andcardiac sounds, pulses,etc), and physiologicresponses to drug and
treatment interventions.

197Vol. 86 No. 7 July 2003
tations covering the basic elements ofdisaster response. Emergency Medi-cine residencies would be expected todo the same, but attainment of such agoal is not uniform.1 Already burdened
with full schedules, medical and nurs-ing schools rarely venture into therealm of disasters. Moreover, a recentACEP task force analysis of availabledisaster-related courses for EMTs,
nurses, and physicians found them un-satisfactory relative to expert panel-de-rived teaching objectives.6 An effortby the Office of Emergency Responseto create a uniform curriculum has led
A B C D E F G H I J
K L M N O
C D E F G H I J
Deceased
K L M N O
Treated and Released
Disposition to“AlternativeFacility”
DISASTER SCENE
Key:
Patient: Live High- Low- Triage Acuity: Black Red Yellow Green Actor Fidelity Fidelity
TRIAGE /TREATMENT
TREATMENT
SIMULATION CENTER HOSPITAL
C D H I J X
DEFINITIVE TREATMENT / INTEGRATION
INCIDENT COMMAND
INCIDENT DEBRIEFING
DECONTAMINATION /
COMMUNICATION / TRANSPORT
Contaminated
Non-Contaminated

198Medicine and Health / Rhode Island
to a novel Web-based course in disas-ter training, although access is limitedto NDMS members.
A central activity in disaster train-ing should be simulation. Disasters arechaotic, and the responses so multi-faceted and necessarily labile, that rec-
reating a calamitous event is a betterway to teach, reinforce, and test con-cepts not readily transmitted by thelecture format. By constructing stress-ful situations that adjust and updatethemselves in real-time to participantdecisions and actions, simulation can
cultivate dynamic problem-solving fordisaster management. In addition,teamwork and familiarity between per-sonnel from various responding depart-ments and agencies can be fosteredduring multi-disciplinary simulations.
The scale and nature of the simu-

199Vol. 86 No. 7 July 2003
lated disaster may vary from ìtable-topîcomputer re-enactments and field ex-ercises with local, state, and federalagency interfacing, down to moremoderately scaled disaster drills withcooperation between a few local unitsor departments.7,8 Published accountsof recent large-scale exercises, such asthe 1999 Wisconsin joint civilian-mili-tary field maneuver ìWake-Up Callî in-volving bioweapon terrorism and themulti-agency crisis administration andconsequence management exerciseìTOP OFF,î are available.9,10
How does high fidelity simulationfit in?
As with any simulation, the higherthe fidelity of the disaster exercise, thegreater the immersion in the trainingexperience. Current disaster simula-tions use actors and volunteers as wellas low-fidelity manikins in the role ofvictim. Physician participation in therole of interactive ìsmart simulatedcasualtiesî who directly observe and de-brief trainee rescue workers has beenone method of enhancing simulation.11
Low-fidelity manikins feature life-likeform and surface features, can undergolife-support interventions such as in-tubation and CPR, but do not exhibitphysiologic behaviors such as breath-ing or blinking. In contrast, invasiveor dangerous interventions cannot bepracticed on individuals portraying vic-tims, albeit they may be fully interac-tive and ìrealistic.î
High fidelity medical simulation(SIM) technology can help overcomethe obstacles and the resultant discon-nect between preparatory exercise andactual incident. Fully programmableto display physiologic responses to in-jury and absolutely free of the restric-tions inherent to live patient actors,SIM allows for ìpractice without riskîand greater verisimilitude.12 SIM sce-narios can bring the distressing, dis-tracting sights and sounds of disastersand their victims to life, ultimatelyhelping reconcile the theory with prac-tice of disaster response. Taking careof a moaning, breathing, moulagedmanikin with deteriorating vitals signsin a field setting while wearing aHazMat suit can only assist in improv-
ing the incident-readiness of rescue per-sonnel.
HIGH FIDELITY MEDICAL
SIMULATION (SIM) TECHNOL-OGY
What exactly is high fidelitysimulation?
Simulation training is well estab-lished in other complex, high-risk in-dustries such as aviation, nuclearpower, and the military, all of whichare regarded as high reliability organi-zations. Anesthesiologists pioneeredthe use of realistic high fidelity inter-active patient simulators in the mid-1980s. However, only recently hassimulation technology come into morewidespread medical use, and its fullpotential for medical education has notbeen realized.
SIM allows for clinical scenariosusing life-sized computerized patientmanikins that respond in real-time to avariety of clinical interventions and phar-macologic agents, letting medical edu-cators control situational learning.Computer-driven manikins cost $30,000to $200,000 and are capable of verbalcommunication, accurate representationof physical exam findings (airway com-promise, lung and cardiac sounds, pulses,etc), and physiologic responses to drugand treatment interventions. Realisticrepresentations of actual treatment set-tings allow simulation participants tosuspend disbelief and immerse them-selves in the exercise.
SIM is currently used in variousinstructive settings to improve clinicaldecision-making and psychomotorskills, e.g. airway management andtrauma resuscitation. Additionally, arole for SIM lies in the systematizedreduction of medical error throughteamwork and procedure training withinstructive debriefing. The appeal ofreproducible enactments embodyingcritical, stressful real-life situations,without risk of harm to patients orstaff, is clear. Drawbacks such as thecost, operation, and maintenance ofsimulator facilities are not negligible;however, improved funding and na-tional interest in disaster response af-ter recent terrorist events may proveopportune. Extension of SIM train-
ing to the field of disaster medicine islogical and to be expected.
INTEGRATION OF SIM TECHNOL-OGY INTO DISASTER TRAINING
How do we integrate SIM tech-nology to improve disaster training?
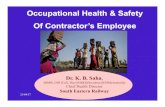
A disaster exercise outline is pre-sented (see diagrams) to demonstratehow SIM technology may be integratedinto responder disaster training, with thefocus on the design and planning aspectsof a proposed SIM implementation.Chemical agent exposure was chosen forits medical complexity, predilection to-wards interventions readily performed onmanikins, opportunity for performanceof rescue activities in personal protectiveequipment (PPE), applicability to WMDand accidental chemical releases, and thedistinct possibility of disaster actualiza-tion. A just-published account of SIM-enhanced chemical warfare responseeducation in Israel was instructive in con-ception of this proposal.13
The presence of SIM in this par-ticular exercise should accomplish thefollowing goals:
1. accurately simulate a WMD di-saster with subsequentprehospital and hospital responseto the exposure, specifically:
-incident command-communications-triage-decontamination-transport-treatment-resource management-debriefing
2. provide clinical stimuli and gen-erate a learning environmentabove and beyond what is at-tained with current disaster train-ing
3. achieve maximal training withminimal risk to rescuers and “vic-tims”
4. observe and record critical actionsin real-time, then evaluate anddebrief participants
5. allow participants to become fa-miliar with SIM technology
6. fine-tune SIM technology for thespecial needs of disaster exercises
These are in addition to the stan-

200Medicine and Health / Rhode Island
dard objectives of an exercise not en-hanced by SIM technology, namely toassemble multi-disciplinary teams foreducational interaction and coopera-tion, to field-test and familiarize res-cuers with communications equipmentand PPE in the context of chemicalWMD hazards, and to assessprehospital and hospital medical re-sponse to disaster conditions.
WHAT IS CURRENTLY AVAILABLE
IN RHODE ISLAND FOR SIM-ENHANCED DISASTER TRAINING?
The Providence-based Rhode Is-land Hospital Medical SimulationCenter (RIHMSC) is composed of asimulation control room and simula-tor area, two trainee simulation-view-ing areas, a conference room foraudiovisual debriefings, storage andequipment rooms, and an office suite.The simulation area was designed tobe flexible to accommodate multiplesimultaneous simulations, recreateother patient care areas (e.g. operatingroom, intensive care unit, radiologysuite), and conduct disaster exercises.
All aspects of actual hospital acutecare areas, including triage and commu-nications, resuscitation rooms, standardand advanced resuscitation equipmentwith medications, medical gases, andcomputer / imaging display capabilities,have been incorporated into the design.These can be configured to emulateprehospital triage and treatment stationsas well. The audio-visual system con-sists of digital video recorders, viewingroom video monitors for displaying pa-tient data, wireless microphones for com-munication and individual participantrecording, and an audiovisual editingsetup to create educational materials forremote and off-line learning.
The RIHMSC utilizes SimMan(MPL/Laerdal) equipment and is ca-pable of supporting five separately con-trolled computerized high fidelitymanikins. The current setup includesa SimMan with fully computerizedcontrol and audiovisual interactive ca-pability, in conjunction with an intu-bation and defibrillation-ready LaerdalALS Skill trainer manikin. Scenariosinvolving multiple SimMan manikinshave already been carried out success-fully, and extension to disaster exercisesengaging more than ten victims iswithin reach. RIHMSC is currentlyworking with local disaster manage-ment agencies to realize a SIM-en-hanced disaster simulation based on thesuggested outline in this article.
REFERENCES1. Pesik N, Keim M, Sampson TR. Do
US emergency medicine residency pro-grams provide adequate training forbioterrorism? Ann Emerg Med 1999;34:173-6.
2. American College of Emergency Phy-sicians Terrorism Response Task Force.Positioning America’s emergencyhealth care system to respond to actsof terrorism. Irving: American Collegeof Emergency Physicians, 2002. http:// w w w . a c e p . o r g /download.cfm?resource=741
3. Institute of Medicine and National Re-search Council. Chemical and Bio-logical Terrorism: Research andDevelopment to Improve CivilianMedical Response. Washington, DC:National Academy Press, 1999.
4. Hirshberg A, Holcomb JB, MattoxKL. Hospital trauma care in multiple-casualty incidents: A critical view. AnnEmerg Med 2001; 37: 647-52.
5. United States Department of Defense.Report to Congress on response tothreats of terrorist use of weapons of massdestruction. Washington, DC: UnitedStates Department of Defense, 1997.
6. Waeckerle JF, Seamans S, Whiteside M,et al. Executive summary: Developingobjectives, content, and competenciesfor the training of Emergency MedicalTechnicians, Emergency Physicians,and Emergency Nurses to care for ca-sualties resulting from nuclear, biologi-cal, or chemical (NBC) incidents. AnnEmerg Med 2001; 37: 587-601.
7. Hogan DE, Burstein JL. DisasterMedicine. Philadelphia: LippincottWilliams & Wilkins, 2002.
8. Tur-Kaspa I, Lev EI, Hendler I, et al.Preparing hospitals for toxicologicalmass casualties events. Crit Care Med1999; 27:1004-8.
9. Tyre TE. Wake-Up Call: Abioterrorism exercise. Mil Med 2001;166(Suppl.12): 90-1.
10. Inglesby TV. Observations from theTop Off exercise. Public Health Rep2001; 116(Suppl.2): 64-8.
11. Gofrit ON, Leibovici D, Shemer J, etal. The efficacy of integrating smartsimulated casualties in hospital disas-ter drills. Prehospital Disaster Med1997;12:97-101.
12. Gordon JA, Wilkerson WM, Shaffer DW,et al. “Practicing” medicine without risk:Students’ and educators’ responses tohigh-fidelity patient simulation. AcadMed 2001; 76: 469-72.
13. Vardi A, Levin I, Berkenstadt H, et al.Simulation-based training of medicalteams to manage chemical warfare casu-alties. Israel Med Assoc J 2002; 4: 540-4.
Leo Kobayashi, MD, is AttendingPhysician, Department of EmergencyMedicine, Brown Medical School.
Marc J Shapiro, MD, is Director ofMedical Simulation Center, Rhode IslandHospital, and Assistant Professor, Depart-ment of Medicine, Brown Medical School.
Selim Suner, MD, is Assistant Pro-fessor, Department of Surgery, BrownMedical School.
Kenneth Williams, MD, FACEP, isClinical Associate Professor, Departmentof Emergency Medicine. Brown MedicalSchool.
CORRESPONDENCE:Leo Kobayashi, MDDepartment of Emergency Medicine1 Hoppin StreetCoro Building, Suite 106Providence, RI 02903Phone: (401) 444-6237Fax: (401) 444-5456E-mail: [email protected]

201Vol. 86 No. 7 July 2003
Biodefense: Medicine in the Time of Bioterrorism�Andrew W. Artenstein, M.D.
The idea that microbial agents ortheir toxins could be used as mod-
ern weapons of terror has been of graveconcern to a small group of military,political and scientific leaders sincedetails of the extensive Soviet and Iraqibioweapons programs became knownduring the last decade of the twentiethcentury.1,2 Since the terrorist attacksof September 11, 2001 and the anthraxattacks later that fall, however,bioterrorism has become a commontopic, covered almost daily by thenation's media. This has engenderedmajor changes in the landscape ofmedicine in the United States: numer-ous professional organizations and so-cieties have developed educationalresources, programs and websites fortheir members; medical schools have
developed new curricula inbioterrorism; major shifts in researchhave occurred at academic centers,driven by the allure of expanded fed-eral funding; industry has become in-terested in the rapid development ofnew, technology-based surveillance anddiagnostic tools for epidemic infectiousdiseases. It is hoped that the nationalfocus on bioterrorism will lead to therestoration of a robust public healthsystem, one capable of responding toboth intentional and natural threats.A recent survey from the Robert WoodJohnson Foundation reveals that anoverwhelming majority of Americansbelieve that the public health system isvitally important in all of its activitiesand support increased federal fundingto ensure its effectiveness.3
ANTHRAX: LESSONS LEARNED,FUTURE THREATS
The anthrax attacks in the US inOctober and November 2001 resulted in22 cases and 5 deaths.4 Although the over-all disease burden was low, the eventsplaced significant stresses on a publichealth infrastructure that many believe hadsuffered from years of neglect and revealedour vulnerabilities to bioterrorism. Someimportant lessons were learned from theexperiences with anthrax, lessons that canbe generalized to other potential threatagents. Chief among these is that exist-ing paradigms concerning bioterrorismmust be continually re-evaluated. Fortu-nately, there have been few events fromwhich to derive data.
Before October 2001, it had beenwidely held that major biological threat
Table 1. ABCs of Toxins

202Medicine and Health / Rhode Island
agents would be delivered via large scaleaerosolization. While this is still the mostlikely scenario in a massive bioweaponsevent, the anthrax attacks illustrated thatsmaller-scale events can still result in sig-nificant economic and psychosocial im-pact utilizing such primitive deliverydevices as letters carried by the U.S. postalsystem. A variety of other “low tech”methods to deliver agents of bioterrorismhave been discussed in the literature andmust be considered in public health re-sponse planning.
Other new findings continue toemerge from the aftermath of the anthraxattacks. Weis et al. recently reported thatindoor, secondary aerosolization of an-thrax spores in the Hart Senate OfficeBuilding occurred during such routineoffice activities as paper handling andpatting desk chair cushions after the an-thrax exposures in that location.5 Thesedata suggest a higher risk than was previ-ously predicted, largely based on the scar-city of earlier data,6 again serving as areminder that our medical systems willhave to revise and implementbioterrorism response plans based onevolving information. As was learnedduring the events of last fall this not onlyimpacts the assessment of exposure risk,prophylaxis and therapeutic delivery, butit also affects the way these messages arecommunicated to the general public.Uncertainty is a predictable accompani-ment of such events. Additional infor-mation gleaned from the events of 2001will help to inform the public health andmedical response to future threats. How-ever, we must accommodate our think-ing to the harsh reality that definitive,new data about anthrax or other agentsof bioterrorism may only emerge duringfuture events. Clearly, our medical re-sponse planning cannot await futureevents. We will need to anticipate poten-tialities when planning for a broad arrayof contingencies.
THE CLINICIAN'S FIRST ROLE:EARLY RECOGNITION
An important tenet in the responseto bioterrorism, yet an equally vexingproblem, is that of early recognition. Thisis hampered by multiple factors: 1) clini-cal illnesses due to bioterrorism will likelybe manifest in the absence of a known
release event; 2) the extent of pathogenexposure will be difficult to discern with-out specific information about the cir-cumstances surrounding the release,information that is unlikely to be readilyavailable; 3) initial symptoms of manyof the syndromes associated withbioterrorism are non-specific and diffi-cult to distinguish from more commondiseases, especially within the group ofrespiratory infections.7 Further compli-cating the latter is thatthe laboratory manipula-tion inherent inbioterrorism raises thespecter that the diseasesmay present with atypi-cal clinical features, insettings where even theclassic clinical features ofthese uncommon infec-tions are difficult to di-agnose.
Early recognition ofbioterrorism may be fa-cilitated by certain epide-miologic and clinicalclues. Case clustering ofcommon syndromes;unusual patterns of dis-ease, especially followingcommon source expo-sures; or the occurrenceof geographically-limiteddiseases outside of theirendemic zones shouldraise the possibility of abioterrorism event. Therecent focus onbioterrorism has had thedesired effect, at least inthe short term, of keep-
ing these possibilities foremost in theminds of clinicians. A plethora of re-sources are now available to aid physi-cians in the differential diagnosis ofdiseases associated with bioterrorism.8
The key issue is to consider the possibil-ity of bioterrorism when evaluating cer-tain presentations of clinical illness.
BOTULISM AND OTHER THREATS
Another important caveat regardingbioterrorism is that the list of potentialthreat agents is long and ever-expanding.While the anthrax attacks of 2001 re-sulted in a flurry of educational initia-tives concerning anthrax and otherrespiratory pathogens, the potentialthreat of smallpox has dominated discus-sion since that time. Issues surroundingsmallpox vaccination will be covered inthe September issue of Medicine &Health/Rhode Island. An area that hasreceived relatively less attention recently,but one of clear importance, is toxin-in-duced bioterrorism. Toxin-induced dis-ease may be associated with a variety of
Table 2BIOTERRORISM WEB SITES
John Hopkins Medicine: Center for CivilianBiodefense Strategieshttp://www.hopkins-biodefense.org/
Institute for Homeland Securityhttp://www.homelandsecurity.org/
St. Louis University School of Public Health: Centerfor the Study of Bioterrorismhttp://www.slu.edu/colleges/sph/csbei/bioterrorism/
UCLA School of Public Health: Department ofEpidemiologyhttp://www.ph.ucla.edu/epi/bioter/bioterrorism.html
University of Minnesota: Center for InfectiousDisease Research and Policyhttp://www.cidrap.umn.edu/cidrap/content/bt/bioprep/
Medline Plus Health Informationhttp://www.nlm.nih.gov/medlineplus/biodefenseandbioterrorism.html
E-Bioterrorism.comhttp://www.e-bioterrorism.com/
Infectious Disease Societyhttp://www.idsociety.org/BT/ToC.htm
Biodefense: Medicine in the Time of Bioterrorism
�
Clinicians mustrecognize that any singlecase of botulism could
represent a manifestationof bioterrorism or couldsignal a warning of anaturally occurring
epidemic.

203Vol. 86 No. 7 July 2003
clinical presentations (Table1); botulismrepresents a classic example.
Botulism is an acute neurologic dis-ease resulting from intoxication withClostridium botulinum that occurs spo-radically and in focal outbreaks through-out the world due to bacterialcontamination of food and wounds.However, Iraq produced massive quan-tities of weaponized C. botulinum andloaded them into warheads during thefirst Gulf War. [There is no evidence itwas released.] Some experts believe thatthere are significant technical constraintsin its use as a strategic bioweapon on thebattlefield; however, it could be used withsignificant morbidity and mortality in ci-vilian populations.2
Botulinum toxin, considered to beamong the most toxic molecules known,acts by inhibiting acetylcholine release,thereby blocking neurotransmissionacross presynaptic vesicles.9 The diseasepresents as an acute, afebrile, symmetric,descending flaccid paralysis. Symptomstypically begin in the bulbar muscles withdiplopia, dysphagia, dysarthria, ptosis,tongue weakness and facial muscle pare-sis. Progression typically involves respi-ratory muscles leading to neuromuscularrespiratory failure. Sensation and cogni-tion typically remain intact. The differ-ential diagnosis includes myastheniagravis, brain stem cerebrovascular acci-dent, chemical intoxication and Guillain-Barre syndrome variant. The diagnosisis largely clinical; laboratory confirma-tion requires the use of a mouse bioas-say. Treatment is largely supportive andmay necessitate prolonged mechanicalventilation. While modern methods ofsupport have resulted in substantial re-ductions in the mortality associated withbotulism, a large-scale event or multi-focal, simultaneous, smaller events relatedto bioterrorism and involving botulismcould rapidly overwhelm hospital re-sources.
Clinicians must recognize that anysingle case of botulism could represent amanifestation of bioterrorism or couldsignal a warning of a naturally occurringepidemic. In practical terms the differ-ences in the public health and medicalresponse may only be slight and largelyinvolve magnitude. In either case onewould anticipate that available surveil-
lance systems would be primed andwould incorporate methods for rapid,real-time communication over a nationalnetwork. Other agents of bioterrorism,including plague and tularemia can oc-cur as natural outbreaks in this country,but in the current climate, a worst-casescenario (from a public health stand-point) may have to be assumed until afull epidemiologic investigation rules outbioterrorism.
THE DUALITY OF BIODEFENSE
The technology used for the pro-duction of bioweapons is considered“dual use,” i.e. it can serve legitimate pur-poses such as vaccine or pharmaceuticalproduction as well as sinister purposes.This property stymied United Nationsinspectors in the past2 and is expected tobe a problem in the current round of in-spections. This concept of “dual use” iscentral to both bioterrorism andbiodefense. For the latter, this featuremay prove beneficial in preparing ourpublic health system for response.
The economic realties of preparingthe public health system for bioterrorismare so enormous that they can only beborne if the revamped system functionseffectively in all modalities, i.e. meets theday-to-day public health needs of soci-ety as well as the more extreme demandsrequired in the response to public healthdisasters such as bioterrorism and epi-demic disease. Americans expect thattheir public health infrastructure will beprepared to deal with the full gamut ofissues, from childhood vaccination cam-paigns to emerging pathogens such asSARS and West Nile virus to abioterrorism event.3
Because many of the potentialbioterror threat agents can occur as natu-ral outbreaks, a robust biodefense systemwill be, by definition, dual use. Addi-tionally, we continually face public healththreats from emerging infections, notonly new ones, but also recurring prob-lems such as epidemic influenza. Thesurveillance and communication systems,clinical networks, and therapeutic initia-tives put into place during biodefenseplanning will serve all aspects of the pub-lic health mission. The threat ofbioterrorism has galvanized our medicalresponse planning and should inform the
full spectrum of biodefense. The ben-eficiary of this will be the nation's publichealth system.
REFERENCES1. Alibek K. Biohazard. New York, NY,
Random House, 1999.2. Zilinskas RA. Iraq’s biological weapons:
The past as future? JAMA 1997;278:418-24.
3. Americans speak out on bioterrorismand U.S. preparedness to address risk.The Robert Wood Johnson Foundation,December 2002. http://w w w. i m m r e g i s t r i e s . o r g / p d f /smallpox_survey02.pdf on 14 Dec 2002.
4. Jernigan J, Stephens DS, Ashford DA,et al. Bioterrorism-related inhalationalanthrax: The first 10 cases reported inthe United States. Emerg Infect Dis 2001;7:933-44.
5. Weis CP, Intrepido AJ, Miller AK, et al.:Secondary aerosolization of viable Bacil-lus anthracis spores in a contaminatedUS senate office. JAMA 2002;288:2853-8.
6. Inglesby TV, O'Toole T, Henderson DA,et al. Anthrax as a biological weapon,2002: Updated recommendations formanagement. JAMA 2002; 287:2236-52.
7. Considerations for distinguishing influ-enza-like illness from inhalational an-thrax. MMWR 2001; 50:984-6.
8. Artenstein AW, Neill MA, Opal SM.Bioterrorism and physicians. Med &Health RI 2002;85:74-6.
9. Arnon SS, Schechter R, Inglesby TV, etal. Botulinum toxin as a biologicalweapon: Medical and public health man-agement. JAMA 2001;285:1059-70.
Andrew W. Artenstein, MD, is Di-rector, Center for Biodefense and Emerg-ing Pathogens, Division of InfectiousDiseases, Memorial Hospital of RI, andAssociate Professor of Medicine, BrownMedical School.
CORRESPONDENCE:Andrew W. Artenstein, M.D.Memorial Hospital of R.I.111 Brewster St.Pawtucket, RI 02860phone 401-729-2252fax 401-729-2795e-mail: [email protected]

204Medicine and Health / Rhode Island
Hospitals have an opportunity todesign new emergency depart-
ments every 10 to 20 years. The mainconcerns of Emergency Department(ED) design are to provide efficiency andspace for routine levels of care and peakvolumes. ED designs must accommodatespecialized care; pediatric, cardiac,trauma, geriatric or stroke care depend-ing on the community needs and hospi-tal specialization. Designs allowprioritization of care into critical, emer-gent and urgent treatment. Finally EDdesign must allow access to the commu-nity for disaster and other mass casualtyneeds.1,2 Most EDs are re-designing tomeet disaster needs. For the most part,they “retrofit” a decontamination area totheir existing ED. After 9/11/01, hos-pitals have the challenge to design EDsthat can better meet needs generated bythe impact of terrorist attacks.
Reacting to concerns about hazard-ous material exposures (HAZMAT),many EDs have included a small seriesof rooms off an outside entrance to al-low for decontamination of a single ora few victims exposed to hazardous ma-terials. Some more recent designs haveincluded the capacity to hose down alarge number of victims outside the EDin inflatable tents or covered areas. Re-cent events chellenge ED planners tobuild EDs to meet the needs of vic-tims of events triggered by weapons ofmass destruction.
We have learned some ED Designlessons from recent weapons of massdestruction (WMD) events. From theTokyo Sarin gas event and subsequentvulnerability analyses we know we mustbuild more surge capacity. Better meth-ods of alerting ED staff to contamina-tion potential and protectingemergency care providers should bebuilt into EDs by design. From theNYC World Trade Center event weknow we must add a capacity to respondout to a disaster scene and continue tomeet a sustained volume over a pro-longed period. In NYC the “clean up”
�Emergency Department Design After 9/11/2001
By Robert Woolard, MD, Melisa Lai, MD, Marc J. Shapiro, Leo Kobayashi, MD, Gregory Jay, MD, PhD,Selim Suner, MD, MS, FACEP, Kenneth Williams, MD, FACEP, Francis Sullivan, MD
phase after the event was prolonged andmost care was provided close to groundzero outside the ED. From the Anthraxmailings we know we must address pub-lic reactions and screening needs. Sincethe EDs remain the most accessiblehealthcare sites in US medical systems,we should anticipate increased volumesof patients during and after any WMDor disaster-related event. The ED willalso get overflow from other providersincluding public health, psychosocialand primary care providers. While post-traumatic stress, information and healthscreening needs should be accomplishedoutside the ED, the ED will need toprovide counseling information andscreening when other services are over-whelmed. Fortunately, in most disasters,shelter needs can and most appropriatelywill be met outside the ED.
ED design after 9/11/01 has be-come a larger concern of the federalgovernment. A federally funded effortis underway, coordinated by MedStar(Washington Hospital Center) to de-velop recommendations for ED designthat meet these new needs. Their focusis to suggest designs for new EDs thataddress health needs that could arise inthe event of a WMD event. Few of therecommendations of this ED designproject for “ER1,” have been released.Updates are available at www.er1.org.3
We hope ED designers will create“all risks ready” emergency departments
using the suggestions of ER1. Their ideais to incorporate the surge capability tohandle biological and chemical threatsas well as large numbers of injured pa-tients in much larger EDs. When webuild urban emergency departmentssuch as the new ED at RIH ( to be com-pleted in 2005), it should be built withthe capacity to serve as a SoutheasternNew England (SENE) regional resourcein the event of a disaster.
New facilities should have physi-cal design and infrastructure to meetrequirements driven by WMD sce-narios, such as the space to increasetreatment capacity, accomplish antici-pated tasks and perform decontamina-tion procedures. Information systemsshould be available to provide real-timepoint of service information and anyneeded “just in time” training. ED andpre-hospital staff cannot be expected tohave immediate knowledge of all pos-sible terror related biological, chemical,nuclear and conventional weapons.However, the technology needed to re-spond to WMD, such as personal pro-tective garments and respirators, shouldbe available both in the field and at theED. The information needed to use thetechnology should also be immediatelyavailable. Large volumes of patients maybe generated and should be anticipatedfrom disasters such as a terror event.ED design solutions must be devised tohandle these large volumes withoutmajor interruptions of lifesaving criti-cal ED care.
Clearly the new EDs must prima-rily function day-to-day as emergencydepartments, chest pain centers, strokeand trauma centers. They must also havethe capability to handle consequencesof a terrorist attack or natural disaster.Trauma centers offer an example of anational and regional network thatcould expand to become a disaster net-work as well. Some capacity to handlean inpatient surge volume must be ad-dressed as well as the pre-hospital andED surge of victims.
�
The greatest post 9/11challenge is to provide
“surge capacity” to meetpotential, anticipatedWMD needs while thevital services of the ED
continue.

205Vol. 86 No. 7 July 2003
Fortunately, with careful planninglarge spaces can be reserved for contin-gency ED operations. For example, agarage under or adjacent to an ED couldprovide additional space during disas-ter operations. Thus, a new facilitycould have the capability of handlinglarge surges of patients presenting forcare by annexing garage or other adja-cent space.
The management of multitude ca-sualties under unusual conditions mustbegin at point of contact, triage areas,ambulance and public entry points.Previous disaster planning efforts haveassumed that victims will be contained,treated and triaged from a disaster scene.Real events suggest that many victimswill “appear” at EDs. Individual EDstaff (security, nurses, clerks, etc.) can-not be expected to know beforehand thenature of the WMD or disaster event.Even when forewarned they may notrecall fully and immediately the perti-nent information critical to the particu-lar disaster response. Information accessmust be built into multiple sites in anynew ED facility. Simply worded disas-ter protocols must be available by com-puter, telephone, etc.
Investigators from ER1 and theRhode Island Disaster Initiative arestudying responses to a variety of chemi-cal and biologic warfare agents. They areplanning and testing new technologiesfor detection surveillance, disaster com-munications and informatics. Betteraddressing psychological health, secu-rity, toxic materials, and mass casualtieswill require innovations in ED design.Recommendations from these expertswill further inform the design of newEDs. The aspects of ED design thatmust be “rethought” include surge ca-pacity, flexibility, decontamination, in-formation needs and security.
RETHINKING THE SURGE CAPAC-ITY OF AN ED
The number of routine treatmentspaces in an ED is planned to matchpatient volume, roughly 1/1100 EDannual visits or 1/400 ED hospital ad-missions is recommended.1 In additionto routine treatment spaces, procedureareas, critical care and resuscitation ar-eas, and other specialized areas for psy-
chiatric or sexual assault evaluation mustbe built to provide those services. Thegreatest post 9/11 challenge is to pro-vide “surge capacity” to meet potential,anticipated WMD needs while the vi-tal services of the ED continue. Hospi-tals are woefully overcrowded and EDsare routinely housing admitted pa-tients.4,5,6 Daily volume excess and de-creased spending on building hospitalbed capacity means that surge capacitymust be addressed in the ED and prehospital environments as well as thehospital.
RETHINKING STRUCTURE,FLEXIBILITY AND MODULARITY
New EDs should choose a site andstructure that allows “growth” into ad-jacent space, opening a ground level oran upper level, using a garage or expand-ing into a parking lot. Garage and park-ing lot space may be most expedient.Often garages and parking lots have ac-cess from streets separate from the EDentrance, allowing separation of disas-ter traffic and ED traffic. NeededWMD response supplies (antidotes, res-pirators, personal protective gear, etc.)can be stored in the ED or garage facil-ity for deployment when needed. Ven-tilation, heat, air conditioning,communication, security and access canbe built into a garage, and also broughtinto tenting over a parking lot. A modu-lar “second ED” with collapsible walls(which fold and stack) and flooring pan-els, could be housed in a garage andunpacked in modules or a system oftents erected to provide surge capacityand meet disaster needs as they grow.More capacity to provide minor androutine care could easily be made avail-able in these new areas. Critical carewould most likely remain in the main
ED. General access could be preservedin the ED with most disaster victimsusing the newly opened “surge” space.According to ER1, a major urbantrauma center ED built for 100,000 vis-its per year should have surge contin-gencies to handle 100 patients per hourfor up to four hours and up to 1000patients per day for up to four days. Toaddress these needs ED designers shouldplan modularity and flexibility into theuse of adjacent spaces. Depending onthe WMD scenario anticipated, as manyas 40,000 square feet could be needednear the ED.
RETHINKING DECONTAMINATION
AND ISOLATION
Decontamination areas must beadequate to meet expected surges. Anuncovered parking lot with heated andvented modular tent units, and modi-fied sprinkler systems could meet mostneeds for mass decontamination. Whilemobilizing these systems to decontami-nate victims at the scene should be partof the WMD and HAZMAT plan,many victims may come to EDs need-ing decontamination. An uncoveredparking area should be accessible to boththe ED and become part of the disasterresponse area. Underground holdingtanks near the tents and at the lowestpoints of the parking lot could trap haz-ardous waste. Filtered modular venti-lation and water supply should helpisolate biohazards.
RETHINKING INFORMATION
NEEDS
The variety of WMD scenarios ar-gues for a strong emphasis on flexibil-ity, adaptability and immediate “just intime” information access. While infor-mation is available and many ED staffhave attended courses, immediate cor-rect response is not assured. Multiplecomputer screens throughout the EDand at remote areas (e.g. parking lot at-tendants), cellular links and/or wirelessportable devices should broadcast mes-sages and be open for staff to access fur-ther information needed immediatelyand specific to the individual staff role.
An example of unanticipatedneeds is the anthrax mailings and thepublic hysteria, which taxed the
�
The design of a post 9/11ED must allow a
complete ED “lock down”for security purposes, to
protect health careproviders and patients.

206Medicine and Health / Rhode Island
healthcare system. Post traumaticstress, anxiety and public concern overpossible exposure to a biological,chemical, or nuclear agent will gener-ate a surge of minor patients at emer-gency departments. A post 9/11 EDshould be configured to open modulesto allow public access for screening andcounseling. A media center within theED could provide health informationand media briefings. The media havebecome the public informers andshould be part of any disaster plan.Internet releases from this center in theED could be displayed on close circuitscreens outside and within the ED.This information could allay publicconcerns and direct the public to ap-propriate resources and access points.
RETHINKING SECURITY
The design of a post 9/11 EDmust allow a complete ED “lock down”for security purposes, to protect healthcare providers and patients. Three unitsshould be considered from a securityprospective; the ED, the disaster re-sponse area (parking garage or otheradjacent space) for surge capacity andthe decontamination area (usually aparking lot). Access points to all build-ings and parking entrances will needto be sealed by barriers with electroni-cally operated locks to allow ambulanceaccess. Access within the ED treatmentareas and from ED to operating rooms,critical care units and other hospitalbuildings will also need to be controlledwith a system of locked barriers to pre-vent contamination patients, staff andthe public. In particular, access into thegrounds around the ED should be care-fully planned. Ideally, in an isolated EDdisaster response and decontaminationarea bordered by streets and a wall withscale deterrent fixtures would limit ac-cess. Plantings within the perimetercould render such a barrier aestheticallyneutral. All access points, the ED, hos-pital interior, disaster areas and theparking lots should be monitored byclosed circuit video. Guard stationsshould be “biosafe”, multiple and stra-tegically placed. Most would be un-manned until required during a WMDevent.
CONCLUSION
Plans for EDs built after 9/11 willcontinue to be informed by the expertsat Rhode Island Disaster Initiative(RIDI)7 and ER1. As RIDI, ER1 andother expert panels make recommenda-tions and as technology progresses andbecomes more widely available, thebuilders of any new ED will have theopportunity to adjust and improve theirpreparedness. As always our hope is thatWMD events never happen, but after9/11 we muct be prepared for terror-related disaster scenarios. The rarity ofWMD events creates a need for us totest our disaster plans, skills and capaci-ties in drills. New EDs should be made“drill-ready” by design.
Why pour such resources intobuilding capacity that we hope never touse? Among the lessons learned fromrecent WMD events is the need to de-velop disaster skills and disaster responsesystems that are in daily use. Certainlythe surge capacity of a post 9/11, “di-saster ready” ED would be used fornatural disaster response and disasterdrills. The surge space could also be usedfor public health events, such as massimmunizations, health screening, andwellness events. Systems that are usedare more familiar and more likely to bedeployed during the real event. A post9/11 ED should serve as a communityresource and deploy its capacities regu-larly to support other communityprojects, thus maintaining “readiness”and being of greater value to the com-munity even in the absence of a disas-ter event.
REFERENCES1. Emergency Department Design Guide-
lines :pg 3. http://www.acem.org.au/open/documents/ed_design.htm
2. Emergency Department Design.Functional and space programming(pg 111). LM Riggs(ed): Dallas, TX,American College of Emergency Phy-sicians.
3. All Risks Ready Emergency Depart-ment. Available at: http://www.er1.org/
4. Andrulis DP, Kellermann A, Hintz EA,Hackman BB, Weslowski VB. Emer-gency departments and crowding inUS teaching hospitals. Ann Emerg Med1991; 20:980-6.
5. Meggs WJ, Czaplijski T, Benson N.Trends in emergency department uti-lization, 1988-1997. Acad Emerg Med1999; 6:1030-5.
6. Bazarian JJ, Schneider SM, NewmanVJ, Chodosh J. Do admitted patientsheld in the emergency departmentimpact the throughput of treat-and-release patients? Acad Emerg Med1996; 3: 1113-8.
7. Rhode Island Disaster Initiative. http:// w w w . r i d i p r o j e c t . o r g /page_manager.asp
Robert Woolard, MD, is Chairmanof the Section of Emergency Medicine, andAssociate Professor of Medicine, BrownMedical School.
Melisa Lai, MD, is Clinical ChiefResident in Emergency Medicine,Harvard Affiliated Emergerncy MedicineResidency, Brigham and Women’s/Massa-chusetts General Hospitals.
Marc J Shapiro, MD, is Director ofMedical Simulation Center, and AssistantProfessor, Department of Medicine, BrownMedical School.
Leo Kobayashi, MD, is AttendingPhysician, Department of EmergencyMedicine, Brown Medical School.
Gregory Jay, MD, PhD, is AssociateProfessor of Medicine In Bioengineering,Brown Medical School, and AttendingPhysician, Rhode Island Hospital.
Selim Suner, MD, MS, FACEP, isPrincipal Investigator RIDI, and AssistantProfessor of Surgery In Emergency Medi-cine, Brown Medical School.
Kenneth Williams, MD, FACEP, isPrincipal Investigator RIDI, and Clini-cal Associate Professor, Department ofEmergency Medicine, Brown MedicalSchool.
Francis Sullivan, MD, is PrincipalInvestigator RIDI, and Clinical AssociateProfessor of Medicine, Brown MedicalSchool.
CORRESPONDENCE:Robert Woolard, MDRhode Island Hospital593 Eddy StreetProvidence, RI 2903Phone: (401) 444-5826Fax: (401) 444-4307Email: [email protected]

207Vol. 86 No. 7 July 2003
�Rhode Island Disaster Initiative
Kenneth Williams, MD, Selim Suner, MD, Francis Sullivan, MD, Robert Woolard, MD
The Rhode Island Disaster Initia-tive (RIDI),1 is a federally funded
research project focused on improvingemergency medical response to disas-ters. The focus of the project is emer-gency medical services (EMS), firstresponders and emergency department(ED) staff during the first few hoursof a disaster event. Project planningbegan in 1999, and congressional fund-ing was released early in September2001. There are three RIDI projectphases. In phase 1 we determined theextent of current knowledge, assessedvulnerabilities, and planned future ac-tivities. In Phase 2 we will perform aseries of disaster drills, testing equip-ment and response. In Phase 3 we willdemonstrate best practices for disasterresponse. In this article we report onPhase 1.
The RIDI Principal Investigators,Drs. Sullivan, Suner, and Williams, ex-amined three main areas: readiness,training, and technology during Phase1. Various federal agencies have sup-ported the RIDI effort, including theDepartment of Health and Human
Services (Phase 1) and the Office forNaval Research (Phases 2 and 3). TheRIDI project investigators collaboratewith other Rhode Island state agencies,such as the Emergency ManagementAgency, Department of Health, andothers who receive federal funds fordisaster preparedness.
The Chemical-Biological Infor-mation Analysis Center (CBIAC) andBattelle Memorial Institute coordinateadministration and funding for theproject. Charles Seekell, Battelle Prin-cipal Research Scientist, is the BattelleOn-Site Project Manager in Rhode Is-land. In RIDI Phase 1, the tasks com-pleted include the vulnerabilityassessment, literature review, technol-ogy evaluation, training program de-velopment, and multiple expert paneldiscussions.
READINESS AND VULNERABILITY
ASSESSMENT
The RIDI investigators definereadiness as the ability to performspecified tasks upon request, in a timelymanner. In drills and in actual events,
many disaster responsesfail to meet readinesschallenges posed by thesituation. These failuresare noted in the medi-cal literature, popularpress, and anecdotal re-ports from actual events.Recurring failures in-clude unfamiliarity withthe disaster plan, failureto follow the plan, im-proper or inadequateequipment for respond-ers, logistic and commu-nication failures,difficulties controllingaccess to the disasterscene, delays in treat-ment, contamination ofthe hospital and EMSequipment, and a vari-ety of other issues.While some of these fail-
ures can be attributed to the challengesdisasters pose, many are embarrassinglycommon and recurring.
Disasters can overwhelm localability for rescue and recovery. World-wide and nationwide, disasters arecommon. However, because they arewidely distributed geographically, in-dividual EMS systems and EDs infre-quently experience a disaster.Consequently, many systems are notready to respond to a disaster. Thethreshold that separates manageabletragedy from disaster is variable. Thedeath of a single important individualmay lead, through psychologic impact,to disaster for a company, school, orhospital. A large number of peoplemay be killed in an event, but, becauseno survivors need medical care, the lo-cal medical system may not be over-whelmed. An incident that is easilymanaged within a busy city health caresystem may overwhelm the rural emer-gency care system a few miles away.Thus, the number of injured or killedpersons necessary to constitute a disas-ter varies widely.
Most systems have planned, tosome degree, for multiple casualtiesfrom locally anticipated natural disas-ters (hurricanes, floods, forest fires,etc.) and transportation accidents.These plans typically activate assets,provide resources, and invoke proce-dures in use daily. However, these planstraditionally do not consider epidem-ics, weapons of mass destruction(WMD), internal disasters at facilities,and other currently contemplated sce-narios. Rhode Island is more prone tohurricanes than tornados, although thelatter are possible. Some disasters aremore threatening for some types of re-sponders than others. A flu epidemicraises more concern for hospitals thanfor snowplow operators, while a bliz-zard has the opposite impact.
During RIDI Phase 1, an exter-nal analysis of Rhode Island first re-sponder readiness was conducted. Thisanalysis determined the number of
Table 1. Disaster ManagementWebsites
Health RI, Bioterrorism Preparedness Program:http://www.healthri.org/environment/biot/home.htm
Rhode Island Disaster Initiative:http://www.ridiproject.org/
CDC, Public Health Preparedness and response:http://www.bt.cdc.gov/
United States Army Medical Research Institute ofInfectious Disease:http://www.usamriid.army.mil/education/instruct.html
Center for Civilian Biodefense strategies:http://www.hopkins-biodefense.org/index.html
Disaster Help:http://www.disasterhelp.gov/
Federal Emergency Management Agency:http://www.fema.gov/

208Medicine and Health / Rhode Island
personnel, hospital beds, ambulances,police cruisers, and hazardous mate-rial (HAZMAT) response teams withinthe state. Assumptions made includedlimited aid from other states and anability to focus all available state re-sources on the disaster at hand. Fifty-one potential disaster scenarios weremodeled with variations in type of di-saster (biological, chemical, explosion,radiation, electromagnetic pulse, andnatural), location (indoors, contained,outdoors) and environmental condi-tions (wind, geography). The casualtyload was matched against availablemedical resources. Again, assumptionswere made to determine the resourcesavailable, such as the number of casu-alties transported in each ambulance,and the number of patients each emer-gency physician could treat during oneepisode. Based on these scenarios andassumptions, the analysis determinedwhether available resources could man-age the casualty load.
In almost all scenarios, medical re-sponse capability was inadequate. Pub-lic safety, sanitation, food, shelter, andother disaster resources were more avail-able than rescue, transport, and emer-gency care. Without significantassistance from outside Rhode Island, theemergency medical response system willbe overwhelmed by any event produc-ing between 500-1000 casualties accord-ing to this analysis. Events that producemore seriously ill or injured casualties,or contaminate and incapacitate re-sources could be even more challenging.
The current Rhode Island emer-gency medical system lacks surge capac-ity. Years of budget constraints andincreasing patient volumes have led toan emergency care system with almostno capacity to handle a surge in patientvolume. In fact, EMS services in RhodeIsland frequently call neighboring com-munities for aid because they are unableto handle routine increases in patientload. EDs frequently request ambulancediversion because of overwhelming pa-tient loads and full hospitals.
The Emergency ManagementPlanning Group (EMPG) conducted asecond type of vulnerability assessment.2
While the first obtained broad informa-tion such as total resource numbers, the
EMPG review included facility disasterplans and site visits at a sample of threeRhode Island hospitals and two urgentcare facilities. For example, the EMPGteam asked not just how many maskswere available, but if the staff on dutyknew where they were, and when andhow to use them. Each hospital visitedwas found to have the required disasterplans in place, but was unlikely to followthese plans in a real event. Instead, func-tional success would occur because ofstrong and talented leadership in a dedi-cated and flexible staff environment. Thehospitals were prepared to handle disas-ter victims with traumatic injury, but lessprepared for victims with contaminationor medical illness. EDs estimated that60% of their beds could be dedicated tocaring for disaster victims. Decontami-nation would be a challenge for hospi-tals and cross contamination with otherpatients was likely. Lack of facilities out-side of EDs for performing emergencydecontamination was a vulnerability.Access to hospitals was easy, making themvulnerable because of weak security pro-grams. Urgent care facilities surveyedwere prepared for typical, traumatic in-jury, but unprepared for biological orchemical disasters.
LITERATURE REVIEW
The RIDI Principal Investigatorsand Battelle consultants reviewed re-cent medical literature related to disas-ter response, management, andresearch. An annotated bibliographywas produced from these efforts and isavailable at www.RIDIproject.org .1
The literature abounds with case re-ports from disaster events.3 A subsetof the literature describes proposed so-lutions.4 Many recent articles, websites, (Table 1) and other sources focuson WMD issues. There is almost noliterature describing any controlled re-search on multiple casualty or disasterevents. A few articles describe the suc-cess of an intervention (a triage tech-nique5 or piece of equipment) at asingle drill or in a non-disaster envi-ronment. However, there is a paucityof true evidence, randomized con-trolled trials, etc. supporting protocols,techniques or equipment.
SURVEILLANCE TECHNOLOGY
EVALUATION
Three surveillance technologieswere considered as potential solutionsto a known lack of an online “earlywarning” system; remote radio moni-toring, ED activity monitoring and ED911 volume surveillance.
RADIO MONITORING
Internet control of remote fre-quency-agile radio equipment orInternet transfer of audio from suchreceivers enables monitoring of radiotraffic from command sites and otherareas distant from the disaster. Thistechnology requires placement of ra-dio receiver/internet computer units tocover a geographic area, intact electri-cal power and Internet connectionduring the disaster. Potential benefitsare the ability of remote listeners in acommand or control situation to gainreal-time information of scene opera-tions. The disadvantages are neededtechnical expertise to operate the ra-dio interface, possible informationoverload from unfiltered radio trans-missions, and technical challenges in-volved in ensuring operatingequipment within the disaster scene.
AUTOMATIC MONITORING OF
EMERGENCY DEPARTMENT
ACTIVITY
Use of motion sensors, doorswitches, or other passive monitors tomeasure facility activity was proposed asa surveillance technique. These measurespotentially correlate with overall ED ac-
�
Without significantassistance from outside
Rhode Island, theemergency medical
response system will beoverwhelmed by any
event producing between500-1000 casualties
according to this analysis.

209Vol. 86 No. 7 July 2003
tivity. A preliminary trial demonstratedfeasibility. As a monitor of a terrorism-related event emergency department vol-ume may be as sensitive as passivesurveillance systems. Automated mea-sures of ED visit volume may be easierto implement than syndromic systems,and require no access to HIPPA-sensi-tive patient information.
EMERGENCY DEPARTMENT
COMPUTERIZED SURVEILLANCE
Emergency department census,chief complaint log and/or 911 datacould serve as a surveillance source. AnInternet link between Rhode Island EDswas designed and a web site establishedto host this link. Surveillance using pa-tient data is possible, but raises HIPPA-related privacy concerns. Volume datafrom 911 and EDs is expected to be themain source providing an early warningof disaster. During RIDI Phase 2 thisoption will be further explored.
TRAINING PROGRAM DEVELOP-MENT
Various options, including briefand extensive courses delivered in a va-riety of formats, were explored. Anoverview of EMS education and train-ing techniques, and a variety of train-ing technologies, including emergingtechniques such as hand-held comput-ers, internet distributed learning, in-teractive video, and high-fidelitysimulation were explored. Traditionalextensive lecture and psychomotor skilldevelopment was felt to be needed forsome topics. Time, funding, and staffavailability will limit the use of this typeof training for ED and EMS staff.Since the events of September 11, 2001a large number of courses related toWMD have been promoted and devel-oped. Many courses are available butmost are longer than one day. There-fore, a variety of other formats will befurther explored during Phase 2.
READINESS EXPERT PANEL
DISCUSSIONS
Outcome measures for disasterdrills or actual events are necessary toevaluate interventions and improveperformance. Surprisingly, no objec-tive measure of EMS performance dur-
ing disaster drills could be found in theliterature. Objective measures of per-formance were therefore developed. Adata collection tool and scoring systembased on time to perform critical ac-tions, patient outcomes, and quality ofperformance was developed for useduring drills. An individualized scoresheet is used, based on the critical ac-tions necessary for each drill patient’smedical problems. An acceptableelapsed time to each critical action (e.g.locate victim, stop hemorrhage, splintfracture) is developed through expertpanel discussion. The data collectiontool allows observers to score responderperformance as it relates to each vic-tim. In addition to elapsed times, thequality of each critical action is alsoscored on a scale. Combined resultsgive an overall evaluation of the drill.This system was widely distributed toa panel of experts, and accepted as aviable means of measuring readiness.
The role of EMS in disaster re-sponse as related to WMD mustchange. Traditionally, EMS profession-als are trained to rush in and renderaid in a disaster. WMD events, on theother hand, involve contaminationwith hazardous materials. EMS pro-fessionals are currently trained to stayaway from such incidents and requestassistance from HAZMAT teams.While HAZMAT response capabilitiesare improving, many EMTs will beneeded in any large-scale WMD event.They currently lack the equipment,training, and response paradigms tosafely and effectively provide this care.
TECHNOLOGY EXPERT DISCUS-SIONS
Surveillance systems based onanalysis of patient records for specificsymptoms are cumbersome, expensive,and slow. In addition, they may raiseHIPPA concerns. The quest for highlevels of specificity may miss an eventwith a cluster of unrelated symptoms.For example, many proposed systemssuggest that an electronic search ofrecords for “flu symptoms” will provideearly warning of an anthrax attack.However, there are significant chal-lenges involved in accessing and pars-ing records for “flu symptoms”. If an
attack involves ingesting anthrax (indry cereal, for example), then the pri-mary symptoms will be gastrointesti-nal, and may not fit the “flu symptoms”model programmers envisioned. Chiefcomplaints may vary, particularlysymptoms experienced by those withsuspected exposure to a WMD agent.6
Instead, a more promising, flexible andefficient model appears to be detect-ing surges of volume which prompt anexpert investigation to discern thecause.
Current Rhode Island emergencycommunications systems are not re-dundant and do not provide inter-agency interoperability. Systems basedon cellular technology are vulnerableto the system, radio communication,and circuit availability during a disas-ter. Experts suggest collaborating toimprove multiple communication av-enues, interagency radio communica-tions, an internet link, a web site andsoftware allowing status posting, real-time chat communications, and infor-mation security. In cooperation withefforts by state agencies, RIDI will ex-plore some of these options duringPhase 2.
SUMMARY
In summary, RIDI is a multi-yearresearch project to identify and developsolutions to some of the challengesposed by disaster response, with a fo-cus on WMD incidents. September 11,2001, changed the RIDI timeline withincreased pressure to produce tangibleresults and recommendations rapidly.Phase 1 was an effort to identify prob-lems and potential solutions throughvulnerability assessment, literature re-view and expert panel discussion.Many disaster response “solutions” mayfail because of a rush to use untestedequipment or processes. RIDI is work-ing cooperatively with other RhodeIsland disaster experts to avoid thesefailures. Informed by Phase 1, RIDIPhase 2 will carefully and progressivelytest potential “solutions” during re-search trial disaster drills. Only afterresearch can RIDI identify best prac-tices in disaster response. As RIDIprogresses to Phase 3, the demonstra-tion project phase, specific improve-

210Medicine and Health / Rhode Island
ments are expected in Rhode Island’sreadiness for disaster. A main featureof Phase 3 is use of a RIDI demonstra-tion vehicle to bring identified solu-tions to the scene as requested byRhode Island EMS agencies. Togetherwith others working to improve RhodeIsland readiness for disaster threats,RIDI hopes to improve the outcomefor patients and providers in RhodeIsland as they face the current disasterthreats.
REFERENCES1. Rhode Island Disaster Initiative. http://
www.ridiproject.org/page_manager.asp2. Emergency Medical Planning Group,
Worcester, MA. www.empginc.com3. Burgess JL, Kovalchick DF, Harter L,
et al. Hazardous materials events:Evaluation of transport to health carefacility and evacuation decisions. AmJ Emerg Med 2001;19:99-105.
4. Hirshberg A, Holcomb B, Mattox KL.Hospital trauma care in multiple-ca-sualty incidents: A critical view. AnnEmerg Med 2001; 37:647-52.
5. Garner A, Lee A, Harrison K, et al.Comparative analysis of multiple-ca-sualty incident triage algorithms. AnnEmerg Med 2001; 38:541-8.
6. Kawana N, Ishimatsu S, Kanada D.Psycho-physiological effects of the ter-rorist sarin attack on the Tokyo sub-way system. Milit Med 2001; 166(12Suppl):23-6.
Kenneth Williams, MD, FACEP, isPrincipal Investigator RIDI, and Clini-cal Associate Professor of Surgery, BrownMedical School.
Selim Suner, MD, MS, FACEP, isPrincipal Investigator RIDI, and Assis-tant Professor of Surgery in EmergencyMedicine, Brown Medical School.
Francis Sullivan, MD, is PrincipalInvestigator RIDI, and Clinical Associ-
ate Professor of Medicine, Brown Medi-cal School.
Robert Woolard, MD, is Co Investi-gator RIDI, and Chairman of the Sectionof Emergency Medicine, and Associate Pro-fessor of Medicine, Brown Medical School.
CORRESPONDENCE:Kenneth Williams, MD, FACEPRhode Island Hospital593 Eddy StreetProvidence, RI 02903Phone: (401) 444-4302Fax: (401) 444-4307Email: [email protected]
ACKNOWLEDGMENT:This material is based upon the work supported by the Office of Naval
Research. The Rhode Island Disaster Initiative (RIDI) is work performedunder Chemical-Biological Information Analysis Center (CBIAC) Contractnumber SP0700-00-D-3180, Task Number 128, Delivery Order # 0122sponsored by the U.S. Office of Naval Research (ONR).”
DISCLAIMER:Any opinions, findings, and conclusions or recommendations expressed
in this material are those of the authors and do not necessarily reflectthe views of the Office of Naval Research.

211Vol. 86 No. 7 July 2003
�CME Background Information
CME REGISTRATION FORM PRINT OR TYPE
Name ____________________________________________________
Address __________________________________________________
City, State, Zip ____________________________________________
Phone ( ) ___________________________________________
Fax ( ) _____________________ e-mail ___________________
___Hospital ___Private Practice ___Resident ___Intern ___Other
Keep a copy for your files. Compare them with the correct answers, which will be made available upon request, and receipt of submis-sion requirements.
EvaluationPlease evaluation the effectiveness of the CME activity on a scale of 1 to 5 (1 being poor, 5 being excellent) by circling your choice.1. Overall quality of this CME activity 1 2 3 4 52. Content 1 2 3 4 53. Format 1 2 3 4 54. Faculty 1 2 3 4 55. Achievement of educational objectives
* discuss the Hospital Emergency Incident Command system 1 2 3 4 5* describe the role of high fidelity medical simulation for mass casualty incident training 1 2 3 4 5* list threats posed for biodefense by anthrax and botulism 1 2 3 4 5* list the features of emergency department design in the post-9/11 era 1 2 3 4 5* list key features of the Rhode Island Disaster Initiative 1 2 3 4 5
Please comment on the impact that this CME activity may have on your practice of medicine.
_______________________________________________________________________________________________________
_______________________________________________________________________________________________________
Additional comments and/or suggested topics for future CME activities.
_______________________________________________________________________________________________________
This CME activity is sponsored by Brown Medical School.
TARGET AUDIENCE: This enduring material is designed for physicians licensed in Rhode Island.
CME OBJECTIVES: At the conclusion of this course, participants should be able to:* discuss the Hospital Emergency Incident Command system* describe the role of high fidelity medical simulation for mass casualty incident training* list threats posed for biodefense by anthrax and botulism* list the features of emergency department design in the post-9/11 era* list key features of the Rhode Island Disaster Initiative
NEEDS ASSESSMENT: In the wake of terrorist events, both here and abroad, physicians must understand the current disaster preparedness system, as well as effortsneeded to improve that system.
ACCREDITATION STATEMENT: Brown Medical School is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to providecontinuing medical education for physicians.
CREDIT DESIGNATION: Brown Medical School designates this activity for a maximum of 2 category 1 credits towards the AMA Physician’s Recognition Award.
FACULTY DISCLOSURE: In accordance with the disclosure policy of Brown Medical School, as well as standards set forth by the Accreditation Council onContinuing Education (ACCME), authors have been asked to disclose (1) any significant financial or any other relationship with the manufacturer(s) or anycommercial product(s) and/or provider(s) of commercial services discussed in any educational presentation and (2) with any commercial supporters of thisactivity.
The intent of this policy is not to prevent an author with a potential conflict of interest from making a presentation. It is merely intended that any potentialconflict should be identified openly so that the reader may form his/her own opinion.
Andrew W. Artenstein, MD, Consultant–GlaxoSmithKline, Dupont, Merck, Bristol Meyers Squibb; Speaker’s Bureau–GlaxoSmithKline, Dupont, Merck,Pfizer. The following authors have disclosed that they have no significant commercial relationships: Gary Bubly, MD, Selim Suner, MD, Leo Kobayashi, MD,Robert Woolard, MD, Liudvikas Jagminas, MD, Marc J. Shapiro, MD, Kenneth Williams, MD, Melisa Lai, MD, Francis Sullivan, MD, Gregory Jay, MD.
ACKNOWLEDGEMENT: The material contained in this issue is a result of the editorial work by Robert Woolard, MD, guest editor. The opinions expressed hereinare those of the authors and do not necessarily reflect the views of the sponsors, publisher or the planning committee.
TO OBTAIN CREDIT: To obtain credit, submit answer sheet and $25 fee to Office of Continuing Medical Education, Brown Medical School. Respondents mustscore 70 or higher for credit.
DEADLINE FOR SUBMISSION: For credit to be received, please mail your registration with $25 fee to Office of Continuing Medical Education, Brown MedicalSchool, Box G-A@, Providence, RI 02912. Submit your answers no later than June 30, 2004.
Keep a copy for your files. Keep a copy of the answers for your files. Compare themwith the correct answers, which will be made available upon request, and receipt ofsubmission requirements.
PAYMENT METHOD: CHOOSE A OR BA. ___ payment enclosed. Make check payable to Brown University CME.
B. ___ charge to my credit card
___ VISA ___ MasterCard ___ American Express
(please print)
Account number _______________________________________
Expiration date____________
Cardholder’s Name _____________________________________
Cardholder’s signature ___________________________________and mail with answer sheet to CME Office, Brown Medical School,Box G-A2, Providence, RI 02912 or fax to 401-863-2660

212Medicine and Health / Rhode Island
1. HEICSa. Is only used for Prehospital command and control.b. Was first developed by California’s Orange County EMS.c. The features of HEICS confers adaptability for use inmany different health care settings.d. B&C.e. All of the above.
2. HEICS can only be used:a. At major medical institutions.b. By Prehospital personnel.c. For environmental disasters.d. In response to earthquakes.e. None of the above.
3. Major features of HEICS are:a. Predictable chain of commandb. Applicability to varying types of disasters.c. Common terminology to promote communication.d. Flexibility and cost effectiveness.e. All of the above.
4. Which of the following are crucial elements of disaster re-sponse that need to be incorporated into a meaningful edu-cational program for potential rescue workers facing terrorrelated events?a. incident commandb. communicationsc. decontaminationd. medical knowledge of terror related agentse. all of the above.
5. What are educational advantages of implementing high-fi-delity simulation in disaster training compared with currentdisaster exercises?a. less realistic disaster enactments allowing for reduced costand less organizational planningb. perfect disaster reenactments and scenarios allowing forabandonment of all other disaster medicine educational pro-gramsc. an integrated learning experience with improved realismof patient clinical care, need for real-time interactive com-munications, fostering of teamwork, field-testing of re-sponder equipment, and capacity for in-depth debriefing
d. even though disaster medicine is amenable to high-fidel-ity simulation techniques, there are no educational advan-tages in implementing them in disaster traininge. disaster medicine is not amenable to high-fidelity simula-tion techniques
6. Early, clinical recognition of illness due to bioterrorism ishindered by all but one of the following:a. there may not be an overt release eventb. symptoms and signs of such illnesses may be non-specificc. these illnesses are quite common in the U.S.d. disease caused by bioterrorism may not present in classicfashione. surveillance systems are poorly developed across the US
7. Common signs and symptoms of botulism include all butone of the following:a. ptosisb. bulbar palsiesc. dysphagiad. paresthesiase. airway compromise
8. The anticipated most accessible point of medical care forterror related disaster victims is thought by RIDI and ER1experts to bea. primary care office.b. department of health.c. emergency departments.d. local fire/rescue stations.e. field hospitals erected by national guard or NDMS
9. Concerned physicians should prepare for potential terror re-lated disaster event bya. participating in local and regional disaster drillsb. identifying sources of up to date medical informationc. reading their hospital and community disaster pland. all of the abovee. none of the above
10. WMD disaster planners such as RIDI and ER1 experts aredeveloping scenarios involving what surge rate?a. at peak 100 patients/hour for 4 hours and 500 patients/day for 5 daysb. at peak 50 patients/hour for 5 hours and 1000 patients/day for 10 daysc. at peak 100 patients/hour for 4 hours and 1000 patients/day for 4 daysd. at peak 500 patients/hour for 1 hour and 5,000 patients/day for one daye. 10,000 patients over a week
11. Readiness is:a. Saying that something can be done.b. Best assessed through estimation of assets.c. The demonstrated ability to perform a specified task in atimely manner.d. Improved through occasional use of arcane policies.e. Assured through complex plans.
12. A major disaster response vulnerability in Rhode Island is:a. Lack of surge capacity in the medical system.b. Recurring challenges in disaster response such as commu-nications difficulties and uncontrolled medical response.c. Disaster plans that do not expand upon daily operationsd. All of the above.e. B and C only.
Disaster Preparedness CME Questions: Circle One Response for Each Question.

213Vol. 86 No. 7 July 2003
First Case of West Nile Infection in Rhode IslandHaris Mirza, MD, Shimae Cross, Maria Mileno MD
THE CREATIVE CLINICIAN CASE
“The practice of medicine is an art, not a trade; a calling, not a business …” – WILLIAM OSLER, Aequanimitas
A 66 year-old woman presented to a RI community hos-pital on September 24th, 2002 with a chief complaint
of fever and headache. The patient had been in her usualstate of health until 3 weeks prior to admission when shebegan to experience weakness, anorexia and myalgias. Tendays prior to admission she also developed fever, nauseaand occasional neck pain. Three days prior to admissionher condition worsened with the new onset of headacheand photophobia. Past medical history was non-contribu-tory
The patient lived in Providence county, Rhode Island.She denied any overseas travel, but had traveled withinNew England. From August 25th to September 3rd, she hadvacationed at a southern Rhode Island beach community,where she remembered getting bitten by mosquitoes. Justprior to admission she was bitten by mosquitoes during avisit to a nearby town in Massachusetts.
On the initial physical exam, the patient’s vital signswere normal apart from a temperature of 100°F. She hadprominent neck stiffness and enlarged lymph nodes in herright axilla and bilateral anterior cervical chains. Her examwas otherwise normal. Peripheral blood testing revealed6.6k/Ul white blood cells (WBC)’s (65% neutrophils, 25%lymphocytes and 9% monocytes). The cerebrospinal fluid(CSF) from the lumbar puncture was clear with 15 redblood cells (RBC)’s, 30 WBC’s (81% Lymphocytes, 13%Monocytes and 6% Neutrophils), glucose of 60mg/dl (se-rum glucose of 97) and protein of 50mg/dl. Testing of theCSF for Lyme disease by enzyme-linked immunosorbentassay (ELISA) and PCR for HSV 1 and 2 were negative.Computed tomography (CT) scan of her sinuses and amagnetic resonance imaging (MRI) of the brain showedno abnormalities.
Throughout her hospital stay, the patient continuedto have moderate to severe temporoparietal headaches andoccasional drenching night sweats. She showed gradualimprovement in her neck stiffness and photophobia. Thepatient was discharged on hospital day 5. Her ELISA ofserum and CSF were positive for West Nile directed IgM.A subsequent plaque reduction neutralization antibody testconfirmed the WN infection, with a P/N(positive/nega-tive control) value of 11.53 for serum and 12.07 forCSF.(Range P/N <2.0 un-interpretable, P/N 2-2.99 equivo-cal, P/N> 3.0 positive)
After discharge, night sweats and weakness persisted
for several weeks. These symptoms slowly improved. As ofthis writing she has recovered completely.
EPIDEMIOLOGY
WN virus is a member of the genus flavivirus of thefamily Flaviviridae. The West Nile virus belongs to a sub-group of viruses known as the Japanese encephalitis com-plex, which includes St Louis encephalitis, Murray valleyencephalitis and Kunjin viruses.1 Birds function as the natu-ral reservoir, while mosquitoes propagate the cycle by feed-ing on infected birds. It has been isolated from 29 differentmosquito species and at least 111 bird species in NorthAmerica. Culex pipiens is the most common species infectedwith the virus. Infected birds develop viremias which al-lows the transmission of the virus to feeding mosquitoes..The virus is particularly virulent in species belonging to thefamily Corvidae (eg, crows and jays).2 Although most in-fected birds develop permanent immunity, some becomeill and die. These dead birds are the basis of surveillanceprograms for tracking the virus. WN virus has also beenshown to infect horses, cats, bats, chipmunks, skunks, squir-rels, and domestic rabbits.
First identified in 1937 in Uganda, the West Nile virusis known to be indigenous to Africa, Asia, Europe and Aus-tralia.2 Since the mid-1990s, outbreaks have been docu-mented in Romania, Russia and Israel. After an outbreak inNew York City in 1999, the American public became in-creasingly aware of the disease, which has been spreadingacross the US. States as far south as Florida, as far north asVermont, and as far west as California have reported thedisease.3 The Centers for Disease Control and Prevention(CDC) reported 4156 cases of WN viral infection for theyear 2002; of these cases, 284 have been fatal.4
Grant Summers ad

214Medicine and Health / Rhode Island
TRANSMISSION
The peak incidence of outbreaks occurs in late Augustand early September.5
The predominant mode of human disease is the mos-quito bite but transmission through blood transfusions andorgan transplantation has been documented in the UnitedStates.6 There is one reported case of transplacental (mother-to-child) WNV transmission and two recent cases of WNVinfection of laboratory workers.15 There is one published caseof possible transmission to an infant through breast feedingin Michigan.7 Current recommendations, however, do notsuggest cessation of breast feeding due to maternal WNVinfection.7 There is no person-to-person transmission.
PATHOGENESIS
The WN virus is a single-stranded RNA virus 50mmin diameter. The surrounding envelope contains the Eprotein involved in cell receptor recognition, fusion, virionassembly, agglutination of red blood cells and induction ofantibodies. While the exact mechanism of West Nile virusreplication and spread are not known, initial replication isthought to occur within the skin and regional lymph nodes.Replication at these sites leads to a primary viremia withsubsequent seeding of the reticulo-endothelial system(RES). Replication within the RES could then perpetuatea secondary viremia with the potential for spread to theCNS. Information gained from studies with St Louis virusindicates that likelihood of viral CNS infection correlateswith the level and duration of the viremia.2 Other factorsthought to affect the severity of a WN viral infection in-clude the virus strain, the age of the patient, genetic sus-ceptibility and the immune status of the host.8
Pathological examination of central nervous system(CNS) tissue from fatal cases of encephalitis in the NewYork outbreak revealed mononuclear inflammation , mi-croglial nodules consisting of lymphocytes and histiocytesand perivascular inflammation in white and grey matter.Findings were most common in the brain stem but alsoinvolved the thalamus, cerebellum and cerebral cortex.
CLINICAL FEATURES
The incubation period ranges from 3 to 14 days.5 Whilethe most common consequence of West Nile viral infectionis an asymptomatic infection, the virus can causing a varietyof clinical presentations, including uncomplicated febrilesyndrome, meningitis, meningoencephalitis, encephalitis, po-liomyelitis-like syndrome,9 or paralysis resembling Guillan-Barre syndrome. Rare extra-neurological manifestationsinclude myocarditis, pancreatitis and fulminant hepatitis.
The most frequent symptoms reported among hospi-talized patients during the 1999 NYC outbreak were fever(90%), weakness (56%), nausea (53%), vomiting (51%),headache (47%), changes in mental status (46%)and diar-rhea (27%). Other reported symptoms seen with variablefrequency included rash, cough, stiff neck, lymphadenopa-thy, myalgias and arthralgias.5
Approximately 1 in 150 WN infections will progress to
severe neurological disease.10 The case fatality rates reportedfrom the 1999 NYC outbreak were 12% for hospitalized pa-tients. A significant risk factor for development of more se-vere disease is advanced age. Children and infants have notbeen found to be at greater risk than the general population.11
DIAGNOSIS
The current gold standard diagnostic test for WN viralinfection is ELISA detection of IgM and IgG antibodies tothe virus in the serum or CSF. IgM antibody can be de-tected 4 days after onset of symptoms in 40% of cases.TheIgM titre peaks around day 21 and may be detectable 2-4months post-infection. IgG antibody is detectable by the10th day of clinical symptoms and can persists for years afterinitial infection. As the IgM antibody does not cross theblood-brain barrier, a positive IgM ELISA test result fromthe CSF is highly suggestive of CNS infection.10 A falsepositive ELISA test can result from cross reactions in pa-tients recently vaccinated against Japanese encephalitis oryellow fever, or recently infected with a related flavivirus(dengue, JE, SLE). It is therefore recommended that a posi-tive ELISA test result be confirmed by the more specificplaque reduction neutralization test.1 The neutralizationtest is particularly useful when testing patients from endemicareas as they are likely to have persistent IgM antibody titresfrom a previous assymptomatic infection. In this case, anincrease in the antibody titer in acute and convalescent se-rum specimens confirms acute infection.
Other diagnostic tests including detection of nuclear an-tigens and molecular amplification tests such as RT-PCR andTaqMan have limited usefulness because of low sensitivities.2
Other laboratory findings include normal or elevatedleukocyte counts, lymphocytopenia, anemia and hyponatre-mia in the peripheral blood. CSF may show lymphocyticpleocytosis, elevated protein and normal glucose levels.10
TREATMENT AND PREVENTION
Treatment for WN viral infections is entirely support-ive. There is no specific therapy. Potential future therapiescurrently under investigation include high dose Ribavirinand IFN-alpha-2b which demonstrate some activity againstWN virus in vitro.10 No vaccine against West Nile viralinfection is available.2
Prevention focuses on both regional mosquito populationcontrol and personal protection with protective clothing, insectrepellants and avoidance of habitats infested by mosquitoes.
Current CDC recommendations are to use DEET-basedrepellents on both clothing and exposed skin. The New YorkCity Department of Health is currently recommending thatadults limit the concentration of DEET in their repellants to30%. It is important to remember that DEET-repellents willwash off with heavy perspiration or rain, and are known tohave decreased efficacy at higher outdoor temperatures.
DEET has been used and studied for several decadesand has a very reassuring safety profile in human adults.Cases of toxicity are rare and associated with long-term,heavy, frequent, or whole body applications.12 Despite this

215Vol. 86 No. 7 July 2003
safety profile, however, DEET-repellants are not recom-mended for children younger than 2 years, for pregnantwomen or on the bedding or bedclothes of children. Fur-thermore, the New York City DOH and the AmericanAcademy of Pediatrics recommend that only repellents with10% or less DEET concentrations be used for children.13,14
We advise travelers to use a permethrin insecticide spraywhich binds to clothing and kills insects on contact for 2to 4 weeks. This ingredient is not to be applied to skin butis safe and effective once the application has dried on cloth-ing. Travel Medicine experts advise such treatment of cloth-ing for the prevention of exposure to Anophelinemosquitoes which are far more resistant to DEET to avoidtransfer of malaria parasites in endemic regions.
CONCLUSION
This is the first confirmed West Nile case in humansin Rhode Island. It is of great concern that one of fourmosquito pools(Culex pipiens) that tested positive werefound within 2 miles of this patient’s residence in Provi-dence county. Around the same time in September last yearanother patient living within half a mile of the former casewas thought to have a probable West Nile infection. Physi-cians need to be aware about up-to-date testing of mos-quito pools in the community and this information isavailable at the Department of Health’s website. This casereport also serves to remind physicians of theimportanceof screening for West Nile virus and to underscore the im-portance of counseling patients about measures to preventWest Nile infection. Extra care should be taken to preventthe elderly from being exposed to West Nile virus.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the assistanceof Uptala Bandy MD, MPH, State Epidemiologist, andstaff at the Health Laboratory of the Rhode Island Depart-ment of Health for the local laboratory and epidemiologicinformation in this publication.
REFERENCES1. Horga MA, Fine A. West Nile Virus. Pediatric Infect Dis J 2001; 20.2. Campbell GL, Marfin AA, Lanciotti RS, Gubler DJ. West Nile
Virus. Lancet Infectious Diseases 2002; 2: 519-29.3. CDC Statistics, Surveillance, and Control Web Site: Surveil-
lance and Control of West Nile Virus – CDC Division of Vec-tor-Borne Infectious Diseases. www.cdc.gov/ncidod/dvbid/westnile/surv&control.htm
4. CDC Media Relations – West Nile Virus Case Countwww.cdc.gov/od/oc/media/wncount.htm
5. Peterson LR, Marfin AA. West Nile Virus: A Primer for theClinician. Ann Internal Med 2002; 137: 173-9.
6. CDC, West Nile Virus Activity-United States, September 26-October 2, 2002, and Investigations of West Nile Virus Infec-tions in Recipients of Blood Transfusion and OrganTransplantation. MMWR 2002; 28.
7. CDC. Possible West Nile Virus transmission to an infantthrough breast-feeding- Michigan 2002, JAMA 2002. 288:1976-7.
8. White E, Morse DJ, Dale L. West Nile Virus, Detection, sur-veillance and control. Annals NY Acad Sciences 2001;951: 200.
9. Glass JD, Samuels O, Rich MM. Poliomyelitis due to West
Nile Virus. NEJM 2002; 347: 1280-1.10. CDC. West Nile Virus (WNV) Infection: Information for Cli-
nicians, www.cdc.gov/ncidod/dvbid/westnile/resources/fact_sheet_clinician.htm
11. New York City Department of Health & Mental Hygiene –DOH West Nile Virus – School, Day Camps and Child Care.www.ci.ny.us/html/doh/html/wnv/wnvfaq15.html
12. Fradin MS, Day JF. Comparative efficacy of insect repellentsagainst mosquito bites. NEJM 2002; 347:13-4.
13. New York City Depatment of Health:Common Insect Repel-lents and Mosquito Control Products.City Health Informa-tion. 2000;19 S.1
14. New York City Department of Health & Mental Hygiene –DOH West Nile Virus–MosquitoRepellant:DEET,www.ci.nyc.ny.us/html/doh/html/wnv/wnvfaq4.html
15. CDC. Intrauterine West Nile Virus infection — New York,2002. MMWR 2002; 51:1135-6.
Haris Mirza, MD, is a fellow in the Department of Infec-tious Diseases, Miriam Hospital/Brown Medical School.
Shimae Cross is student at Brown Medical School.Maria Mileno, MD, is Associate Professor of Infectious
Diseases, Brown Medical School, and Director of Travel Medi-cine Services, The Miriam Hospital.
CORRESPONDENCE:Haris Mirza, MDMiriam Hospital164 Summit AvenueProvidence, RI 02906Phone: (401) 793-4357e-mail: [email protected]
20 Years ExperienceReferences
508-336-5066
Healthcare ProviderAHA CPR Training
in Your Building
AED & AMBU bag training,Barrier Device for each
person included. Best CPRclass, Certification good for2 years. $35 per person,
minimum of 5.
Dr. Rajabiun ad

216Medicine and Health / Rhode Island

217Vol. 86 No. 7 July 2003
Edited by Jay S. Buechner, PhD
Health Risk Disparities Among Rhode Island Adults, 2001Jana E. Hesser, PhD
Rhode Island Department of Health
Patricia A. Nolan, MD, MPH, Director of Health
Health by Numbers
Eliminating health disparities among Americans is a na-tional and a Rhode Island goal for the Year 2010.1,2 Dis-
parities in health outcomes and health risks exist between menand women, between groups defined by race and ethnicity,and between groups defined by other criteria such as educa-tion, geography, and income. Disparities in health outcomesand health risks can be attributed to differences in access toadequate health care, exposure to environmental factors, ge-netics, and individual behaviors. This paper presents surveydata from Rhode Island’s 2001 Rhode Island Behavioral RiskFactor Surveillance System (BRFSS) for nine health risk in-dicators, and examines disparities between men and womenand between groups defined by race and ethnicity.
MethodsThe BRFSS is a national telephone survey of randomly
selected adults (ages 18 and older) who live in householdswith telephones. It asks respondents questionsabout a variety of key health risk behaviors, abouthealth insurance coverage, access to care, and par-ticipation in health screening. Fifty states and fourterritories perform the BRFSS with funding andmethodological standards provided by the Cen-ters for Disease Control and Prevention(CDC).3 Rhode Island has participated in theBRFSS since 1984; a professional survey researchfirm conducts the annual survey. Results forRhode Island are reported annually.4
In 2001, 4,120 Rhode Island adults wereinterviewed throughout the year at a rate ofapproximately 343 per month. This includedinterviews with 1,550 males, 2,570 females,with 3,404 White non-Hispanic (NH) respon-dents, 122 Black non-Hispanic (NH) respon-dents, 292 Hispanic respondents, and 302respondents in other race/ethnicity groups;3,328 respondents were between the ages of 18and 64 and 792 were 65 or older.
ResultsThere are disparities between males and
females for several health-risk behaviors, withmales more often at higher risk than females.(Figure 1) Rates for males are twice those forfemales for: no particular place to go if sick or for health
advice (15% vs. 8%), binge drinking (21% vs. 10%), andfirearms in the home (18% vs. 9%). Males are also at higherrisk than females for: overweight (66% vs. 46%), no healthcare coverage (ages 18-64) (10% vs. 7%), and smoking ciga-rettes daily or some days (26% vs. 22%). Females are atgreater risk than males for no leisure time physical activity(28% vs. 21%).
There are also disparities for groups defined by race/ethnicity for eight of the nine health-risk behaviors. (Figure2) Black NHs and Hispanics both have higher rates thanWhite NHs for three measures of access to care — no healthcare coverage, unable to see a doctor due to cost, and haveno particular place to go if sick or for health advice. Bothminority groups have higher rates than White NHs for twohealth risk behaviors — overweight, and no leisure timephysical activity. The proportion of Hispanics reportingpoor or fair general health is higher than that for either Black
Figure 1. Health Risks Among Rhode Island Adults (Ages 18 and Older) by Gender,2001.

218Medicine and Health / Rhode Island
NHs or White NHs. Black NHs (26%)and White NHs (24%) are at greaterrisk than Hispanics (18%) for currentsmoking. White NHs are at highestrisk for keeping a firearm in or aroundthe home (14% compared with 6% ofBlack NHs and 10% of Hispanics). Allthree groups have comparable rates forbinge drinking (between 13% and15%).
For some of these measures, dispari-ties between these race/ethnic groups areespecially large. The percentage of BlackNHs and Hispanics with no health insur-ance coverage (19% and 16%, respectively)is more than twice the rate for White NHs(7%). The percentages of Black NHs(12%) and Hispanics (14%) unable to seea doctor in the past 12 months due to costare also twice that for White NHs (6%).Forty-two percent of Hispanics report noleisure time physical activity, comparedwith 23% of White NHs and 29% of BlackNHs. 35% of Hispanics rate their healthstatus as fair or poor, more than twice theproportion of Black NHs (17%) and ofWhite NHs (13%).
DiscussionFor the majority of the nine BRFSS
health risk measures presented here,males are disadvantaged compared with females, and BlackNH and Hispanic populations are disadvantaged comparedwith White NH ones. Overall, greater disparities exist be-tween minority populations and the majority White NHpopulation than exist between the genders. Eliminating dis-parities is a national overarching health goal for 2010 andRhode Island shares this goal.2 To eliminate disparities willrequire substantial enhancements over the next decade inaccess to care and in health promotion programs targetingthe groups at greatest risk.
Jana E. Hesser, PhD, is Program Manager for Health Sur-veys and BRFSS Coordinator, Office of Health Statistics, RhodeIsland Department of Health, and a Clinical Teaching Associ-ate in Community Health, Brown Medical School.
REFERENCES1. US Department of Health and Human Services. Healthy People
2010: Volumes I and II. Understanding and Improving Health,Objectives for Improving Health. 2nd Edition, Washington, DC:US Government Printing Office, November 2000.
2. RI Department of Health. Healthy Rhode Islanders 2010. DraftObjectives and Targets, Providence, RI, August 2001.
3. CDC’s BRFSS website: www.cdc.gov/brfss.4. RI Department of Health BRFSS webpage: www.health.ri.gov/
chic/statistics/brfss.htm and reports at www.health.ri.gov/publications/list.htm.
Figure 2. Health Risks Among Rhode Island Adults (Ages 18 and Older), by Race/Ethnicity, 2001.

219Vol. 86 No. 7 July 2003
Progress in the Control of OropharyngealCancer in Rhode Island, 1987–2000
John P. Fulton, PhD, Dorothy M. Darcy, CTR, Leanne Chiaverini
PUBLIC HEALTH BRIEFING
Edited by John P. Fulton, PhD
Rhode Island Department of Health
Patricia A. Nolan, MD, MPH, Director of Health
PROFILE
About 770 Rhode Island residents alive today were diag-nosed with cancer of the oral cavity and pharynx at some pointin the past (467 men and 299 women in 1998); about 115 arenewly diagnosed with oropharyngeal cancer each year (an an-nual average of 77 men and 38 women in the five years 1996-2000); and about 30 succumb to the disease annually (anannual average of 16 men and 13 women in the five years1996-2000). Oropharyngeal cancers are not among the mostprevalent cancers in the state (and the nation), but they aresignificant for cancer control efforts, because most tumors ofthe oral cavity and pharynx are considered preventable.
CONTROL STRATEGY
Oropharyngeal cancer is strongly related to chronic to-bacco use and chronic “high-risk” drinking (14 or more al-coholic drinks per week for men and 7 or more alcoholicdrinks per week for women), and is therefore theoreticallypreventable by abstaining from tobacco and limiting alcoholconsumption.1 The effectiveness of screening for early oropha-ryngeal tumors is equivocal,2 although survival is clearly re-lated to stage of disease at diagnosis.3 The US PreventiveServices Task Force last issued a recommendation on screen-ing for oral cancer in 1996, when it stated: “There is insuffi-cient evidence to recommend for or against routine screeningof asymptomatic persons for oral cancer by primary care cli-nicians. All patients should be counseled to discontinue theuse of all forms of tobacco and to limit consumption of alco-hol. Clinicians should remain alert to signs and symptomsof oral cancer and premalignancy in persons who use to-bacco or regularly use alcohol.”2 In line with these recom-mendations, the Rhode Island Cancer Control Plan,4
published in September, 1998, recommends:
Tobacco Recommendations• Do not smoke.
Alcohol recommendations• Limit alcohol consumption.
Screening Recommendations: Oral Cancer• Primary care providers should remain alert to the
signs of early oral cancer, particularly leukoplakiaand erythroplakia, and should refer patients withthese lesions to a surgical specialist for further evalu-ation and treatment.
2010 TARGETS
Healthy People 2010, the most recent set of health ob-jectives for the United States,5 suggests the following targetsfor the control of oropharyngeal cancer:
Tobacco UseBy 2010, reduce cigarette smoking by adults aged 18
years and over to 12% (baseline = 24% in 1998), and re-duce tobacco use by students in grade 9 through 12 to 21%(baseline = 40% in 1998).
Alcohol UseBy 2010, reduce the proportion of adults aged 21 years
and over who exceed guidelines for low-risk drinking to 50%of people who regularly use alcohol (baseline = 73% in1992). [Low risk drinking: Men—less than 14 drinks perweek; women—less than 7 drinks per week.]
MortalityBy 2010, reduce the oropharyngeal cancer death rate
to 2.7 deaths per 100,000 population (age-adjusted to theyear 2000 standard population of the United States; baseline= 3.0 deaths per 100,000 population in 1998).
Holistic Ad

220Medicine and Health / Rhode Island
TRENDS
Tobacco UseFrom 1990 through 2001, the proportion of Rhode
Island men who had reported being a current smoker var-ied between 23 and 27%, showing no definite trend. Themedian proportion of U.S. men who had reported being acurrent smoker remained at around 25% for the entireperiod of observation.
From 1990 through 2001, the percent of Rhode Is-land women who had reported being a current smoker var-ied between 20 and 25%. Among all the states, incomparison, the median proportion of U.S. women whoreported being a current smoker hovered around 21%.
Alcohol UseFrom 1990 through 2001, the proportion of Rhode
Island men who had reported an average of 14 or morealcoholic drinks per week varied between 7 and 10%, show-ing no definite trend, but substantially exceeding the U.S.state median throughout the period.
From 1990 through 1999, the proportion of Rhode Is-land women who had reported an average of 14 or more alco-holic drinks per week varied between 1 and 2%, showing no
definite trend, but substantially exceedingthe US state median throughout the pe-riod in all years but one. In 2001, the firstyear in which the Behavioral Risk FactorSurveillance System (a national surveillancesystem organized by the CDC and run bythe separate states and territories) used therevised standard for chronic drinkingamong women (an average of 7 or morealcoholic drinks per week), the proportionof Rhode Island women who met or ex-ceeded the standard (6.6%) was almostdouble the U.S. state median (3.9%).
INCIDENCE
The average annual age-adjusted in-cidence of invasive oropharyngeal cancer(2000 standard) among Rhode Islandmen of all races declined from 17.6 per100,000 in 1987-1991 to 14.7 per100,000 in 1990-1994, then increased to16.7 per 100,000 in 1996-2000. In con-trast, the age-adjusted incidence of inva-sive oropharyngeal cancer (2000standard) among U.S. men of all racesdecreased from 20.1 per 100,000 in 1987-1991 to 17.2 per 100,000 in 1996-2000.
The age-adjusted incidence of invasiveoropharyngeal cancer (2000 standard)among Rhode Island women of all racesvaried from 7.5 per 100,000 in 1990-1994to 6.3 per 100,000 in 1996-2000, suggest-ing a decline. The age-adjusted incidenceof invasive oropharyngeal cancer (2000 stan-
dard) among U.S. women of all races declined from 7.5 cases per100,000 in 1987-1991 to 6.9 cases per 100,000 in 1996-2000.
MORTALITY
The age-adjusted mortality of invasive oropharyngealcancer (2000 standard) among Rhode Island men of all racesdeclined strongly from 7.0 per 100,000 in 1987-1991 to3.5 per 100,000 in 1996-2000, paralleled by a weaker de-cline among U.S. men of all races (from 5.5 in 1987-1991to 4.4 in 1996-2000). The disparity between the mortalityrates for Rhode Island men and U.S. men changed over theperiod of observation, with Rhode Island beginning the de-cade with higher-than-U.S. mortality and ending the de-cade with lower-than-U.S. mortality.
The age-adjusted mortality of invasive oropharyngeal can-cer (2000 standard) among Rhode Island women of all racesshowed little variation over the 1987-2000 period, averagingabout 1.8 per 100,000. The age-adjusted mortality of invasiveoropharyngeal cancer (2000 standard) among U.S. women ofall races declined from 2.0 in 1987-1991 to 1.7 in 1996-2000.The disparity between the mortality rates for Rhode Islandwomen and US women decreased over the period of observa-tion, with US women as a whole benefitting.

221Vol. 86 No. 7 July 2003
Did yourmoney manageroutperform theS&P 500 last year?
We did.
Phoenix Investment Management has consistently
and significantly outperformed the markets for over a
decade. Can you continue to tolerate disappointment
in your portfolio’s performance? If you’re investing
$1 million or more, we are confident our track record
can work for you. To learn more about our firm and its
investment results, call Marie Langlois or Jerry Fogarty,
Managing Directors of Phoenix Investment Management,
a division of The Washington Trust Company, at
401-331-6650.www.washtrust.com
ASSESSMENT
Among men and women in Rhode Island, the propor-tion of current smokers varied little from 1990 through 2001,as did the proportion of chronic drinkers. Unfortunately, dataon trends in spit tobacco use during the period were unavail-able, but the proportion of people who use spit tobacco is farless than the proportion who smoke, and the link betweenoropharyngeal cancer and tobacco is not limited to spit to-bacco. The incidence of all invasive oropharyngeal tumorsamong men declined, then increased over the 1987-2000 pe-riod, but mortality rates plummeted. Among Rhode Islandwomen, there was little change in oropharyngeal cancer inci-dence or mortality through the 1990s.
Rhode Island has already reached the 2010 goal for amortality decline from oropharyngeal cancer (when recentmortality rates for men and women are averaged), but giventhe state’s average (for US) rates of tobacco use, and itsabove-average rates of chronic drinking, will Rhode Islandbe able to sustain this decline? Is there potential for furtherdecline, or has the state reached a plateau that will notchange until we experience declines in the use of tobaccoand alcohol? In this vein, public health efforts should focuson discouraging youth from starting to smoke and from allunder-age alcohol use, increasing cessation among thosewho do smoke and discouraging more-than-low-risk alco-hol use among all adults. Primary care physicians can assistby addressing chronic tobacco and alcohol use among pa-
tients and by performing oral cancer screenings on high-risk patients, in line with the 1996 recommendations of theUS Preventive Services Task Force.
REFERENCES1. National Institutes of Health, National Cancer Institute. Can-
cer Rates and Risks. 4th edition, 1996.2. US Preventive Services Task Force. Guide to Clinical Preventive
Services, 2nd ed. Baltimore: Williams and Wilkins, 1996.3. Ries LAG, Eisner MP, Kosary CL, et al. (eds). SEER Cancer
Statistics Review, 1975-2000, National Cancer Institute.Bethesda, MD, http://seer.cancer.gov/csr/1975_2000, 2003.
4. Rhode Island Department of Health. Cancer Control RhodeIsland – Strategic Plan for 1998-2005. Providence, RI: RhodeIsland Department of Health, September, 1998.
5. U.S. Department of Health and Human Services. Healthy People2010. 2nd ed. With Understanding and Improving Health andObjectives for Improving Health. 2 vols. Washington, DC:U.S.Government Printing Office, November 2000.
John P. Fulton, PhD, is Associate Director of Health, Di-vision of Disease Prevention and Control, Rhode Island De-partment of Health, and Clinical Associate Professor ofCommunity Health, Brown Medical School.
Dorothy M. Darcy, CTR, is Director, Cancer Informa-tion System, Hospital Association of Rhode Island.
Leanne Chiaverini is Research Associate, Asthma ControlProgram, Division of Disease Prevention and Control, RhodeIsland Department of Health.

222Medicine and Health / Rhode Island
– A Physician’s Lexicon –
The Cerebral Hemispheres
(a) Cause of death statistics were derived from theunderlying cause of death reported by physicians ondeath certificates.
(b) Rates per 100,000 estimated population of1,048,319
(c) Years of Potential Life Lost (YPLL)
Note: Totals represent vital events which occurred in Rhode Is-land for the reporting periods listed above. Monthly provisionaltotals should be analyzed with caution because the numbersmay be small and subject to seasonal variation.
Rhode Island MonthlyVital Statistics Report
Provisional Occurrence Datafrom the
Division of Vital Records
Vital StatisticsEdited by Roberta A. Chevoya
Rhode Island Department of Health
Patricia A. Nolan, MD, MPH, Director of Health
Number (a) Number (a) Rates (b) YPLL (c)Diseases of the Heart 241 3,112 296.9 4,124.0**Malignant Neoplasms 221 2,454 234.1 7,598.5 *Cerebrovascular Diseases 50 545 52.0 770.0**Injuries (Accident/Suicide/Homicide) 49 417 39.8 8,000.0***COPD 40 525 50.1 512.5**
Reporting PeriodUnderlyingCause of Death 12 Months Ending with July 2002
Number Number RatesLive Births 737 13,193 12.6*Deaths 945 10,418 9.9*
Infant Deaths (11) (94) 7.1#Neonatal deaths (8) (65) 4.9#
Marriages 328 8,346 8.0*Divorces 316 3,376 3.2*Induced Terminations 593 5,598 424.3#Spontaneous Fetal Deaths 99 1008 76.4#
Under 20 weeks gestation (93) (936) 70.9#20+ weeks gestation (6) (72) 5.5#
Reporting PeriodJanuary
2003Vital Events
* Rates per 1,000 estimated population # Rates per 1,000 live births** Excludes one death of unknown age.*** Excludes two deaths of unknown age.
12 Months Ending withJanuary 2003
July2002
The brain, said Emily Dickinson,“is wider than the sky,” storing
more cherished memories, more facts,more schemes and more dreams thaneven the firmament above. Long be-fore neuro-anatomists unraveled thecomplexities of this 1.5-pound organhiding in the cranium, poets intuitivelyknew its grander purposes and mission.The names applied to the parts of thebrain by the classical anatomists there-fore represent a happy mixture of fan-ciful conjecture, a touch of mythology,far-fetched analogies and practicality.
The cerebral hemispheres, at leastin higher mammals, are seen as a com-plex series of infoldings of the corticalgray matter into numerous, convolutedgyruses and intervening sulcuses. Theword gyrus is from the Greek meaninga circule or circling, as in words suchas gyroscope or gyromancy [a bizarre
form of divination where the seer walksin circles until he develops syncope andcollapses, and the direction of his pronebody will then indicate the direction apuzzled traveler should take]. The wordsulcus is from the Latin, meaning afurrow or a groove.
The major bodies of discrete graymatter buried within the depths of thehemispheres include the globuspallidus, the caudate nucleus, the puta-men and the thalamus. The globuspallidus, the pale mass, is taken fromthe Latin root, pallio-, meaning thatwhich is cloaked or mitigated. Andthus palliative medicine refers to thecloaking or lessening of symptoms asits goal. The word putamen derivesfrom the Latin puto, meaning thatwhich falls off when pruning fruit trees,and specifically the hard nut of somesoft-fleshed fruits. The caudate nucleus
takes its namefrom the Latin cauda, meaning tail.Cauda then evolved into the Frenchword couard, meaning one who turnstail, which in turn became the Englishword coward.
The thalamus is a Latin word de-rived from the Greek, meaning an in-ner chamber and specifically abedroom or bed. The thalamus is agloboid structure resembling a roundpillow and hence the use of the Greekword for bed. The rounded eyeball jus-tifies its use in the word ophthalmic.Hypothalamus defines those gray mat-ter nuclei below the thalamus.
– STANLEY M. ARONSON,MD, MPH

223Vol. 86 No. 7 July 2003
William M. AllenTroy, Pires & AllenPawtucket • 401-728-2060
Sidney BaileyAON Risk Services of RIProvidence • 401-331-7700
Nat CalamisStarkweather & ShepleyEast Providence • 401-435-3600
John H. Lathrop Lathrop Ins. AgencyWesterly • 888-596-2530
Bill Mende Mastors & ServantEast Greenwich • 800-335-5701
Anthony Paolino, Jr.Paolino Ins. AgencyProvidence • 401-421-2588
John TicknerBabcock & HelliwellWakefield • 401-782-1800
ith important purchases, the lowest price isn’t always the best buy. Quality is more critical in the purchase of a home,
car, medical equipment and that all-important purchase: medical malpractice insurance. With the future of your practice and your reputation on-the-line you can’t afford second best.
Take a look at ProMutual Group:
• The largest provider of medical malpractice insurance in New England.
• Nearly 30 years experience.
• Insures more than 16,000 healthcare professionals.
• Financial strength that has earned us an A- (Excellent) rating from A.M. Best, the nation’s leading independent insurance rating organization.
• Over $1.3 billion in total assets with $364 million in surplus.*
• Outstanding risk management service from thelargest staff in New England.
• Experienced claim professionals close a majority of claims without payment and win in excess of 90% of those that go to verdict.
Isn’t it time you got the best protection from one of the largest providers of medical malpractice insurance in New England? Call or visit our web site today.
www.promutualgroup.com
101 Arch Street, Boston, Massachusetts 02110888-776-6888 www.promutualgroup.com
Connecticut • Maine • Massachusetts • New Hampshire • New Jersey • Rhode Island • Vermont
* As reported in our 2001 Annual Report.
Not all products are available in all states.

224Medicine and Health / Rhode Island
�
�
�
�
PROVIDENCE, R.I., JANUARY, 1917VOLUME 1NUMBER 1
PER YEAR $2.00SINGLE COPY, 25 CENTS
The Official Organ of the Rhode Island Medical SocietyIssued Monthly under the direction of the Publications Committee
THE RHODE ISLAND MEDICAL JOURNAL
� �FIFTY YEARS AGO
[JULY, 1953]� �NINETY YEARS AGO
[JULY, 1913]
TWENTY FIVE YEARS AGO
[JULY, 1978]� �Frank W. Sullivan, MD, in the President’s Address, noted
that the Medical Society library’s future was under study.Also, the Medical Society had recruited volunteer physiciansto give physicals to Ladd School residents (19 physicianscontributed 802 hours to update exams on 711 residents).
Fredy P. Roland, MD, contributed “Management ofAtypical Pneumonias in View of the New Entity‘Legionnaire’s Disease.’” He advised the importance of “se-rological testing on a large scale.”
Gail Barsel, MS, Siegried M. Pueschel, MD, HowardA. Hall, MD, Dianne N. Abuelo, MD, contributed “Expe-rience with Prenatal Diagnosis in Rhode Island.” They cau-tioned: “Physicians have the responsibility of informingat-risk couples of the availability of prenatal diagnosis.” From1974-77 the Genetic Counseling Center at Women & In-fants’ Hospital counseled 96 patients (only 7 in 1974). Themost common cause for referral was advanced maternal age.
James J. Yashar, MD, Ralph J. Burnard, MD, Albert K.Weyman, MD, John Yashar, MD, in “Axillary Distal Pro-funda Femoral Artery Bypass,” described “the new opera-tive approach for infected aortic grafts. “
An Editorial commented on administrative logistics: “Ifwe had an enemy and wished him evil, we should like
to see him appointed on the Committee of Arrangements.The members of the Society do not appreciate the workand worry which is thrust upon the unhappy three whohave charge of the …annual meeting, and thecriticism…regarding the annual dinner are uncalled for andunjust.”
Alexander B. Bruggs, MD, delivered the President’sAddress, “Some of the Changes that Have Taken Place inthe Teaching and Practice of Medicine during the past 40Years as Viewed by the General Practitioner.” Dr. Bruggscited advances in tuberculosis. When he was a student,1868-72, it was the era of Villenin’s experiments with in-oculation. The symptomatology and anatomical character-istics of typhoid have remained the same, but there havebeen “marked changes” in etiology and treatment, “althoughthe present day treatment does not yield a much greaterpercentage of cures.” Forty years ago, diphtheria was con-sidered a constitutional disease, and there were no calls forquarantine: the disease claimed “a greater percentage ofdeaths from among its victims than another other malady.”Forty years ago, malaria was thought to be a “miasma.”Today surgical operations “that would have been consid-ered criminal” are routine.
In “Umbilical Hernia, “ P. E. Truescale, MD, describeshis experience: over the past 6 years he operated on 20 pa-tients at Highland Hospital and St. Anne’s; 10 patients alsohad gall stones. He used an operation introduced by Dr.William J. Mayo.
Edwin H. Place, MD (Boston) read before the ChildWelfare Conference in Providence, January 1913, “PresentMortality of Diphtheria: Causes and Their Presentation.”The number of cases was declining, yet the death rate re-mained high. From 1901-1911. there were 2.5 times more
deaths from diphtheriathan from scarlet feverin Boston. The mor-tality of diphtheria was7.8%; of scarlet fever,4.8%.
Louis Weinstein, MD, (Associate Professor of Medicine,Boston University School of Medicine) in “What the
Practitioners Should Know About Poliomyelitis,”discusseddiagnosis, paralytic and non-paralytic cases, polioencepha-litis, and treatment. He had presented the talk at the 142nd
annual meeting of the Rhode Island Medical Society.At the same meeting, Hanson Baldwin, the Military
Editor, New York Times, presented “Where Do We Go FromHere?” In the 8 years since World War II, the author saw no“absolute security,” cited the arms race and the Cold War.
With 20 million veterans in the United States, theAmerican Medical Association advocated limiting VeteransAdministration-subsidized care to veterans with service-in-duced or service-aggravated injuries, and to veterans “withtuberculosis or psychiatric or neurological disorders of non-service connected origin who are unable to defray expensesof…hospitalization.” The Journal re-stated the AMA’s stance.