Medications and Psychosocial Treatments for ADHD Thomas E. Brown, PhD Associate Director, Yale...
60
and and Psychosocial Psychosocial Treatments for Treatments for ADHD ADHD Thomas E. Brown, PhD Associate Director, Yale Clinic for Attention and Related Disorders Department of Psychiatry Yale Medical School
-
Upload
howard-williams -
Category
Documents
-
view
217 -
download
1
Transcript of Medications and Psychosocial Treatments for ADHD Thomas E. Brown, PhD Associate Director, Yale...

Medications and Medications and Psychosocial Psychosocial
Treatments for ADHDTreatments for ADHDThomas E. Brown, PhD
Associate Director,Yale Clinic for Attention and Related Disorders
Department of PsychiatryYale Medical School

In the Human BrainIn the Human Brain
100 billion neurons each one linked to >1000 others in complex sub-systems that have to “talk to each other” using low voltage electrical impulses that have to jump across gaps so fast that 12 can cross in 1/1000 sec.

The Jungle

Neuron
SynapseIntertwined neurons

Chemicals Jump the GapsChemicals Jump the Gaps
Inside brain >50 different chemicals are continuously made
every neuron system uses 1 of them stored in little vesicles near tip of neuron when electrical impulse comes, mini-dots
of that chemical are released, cross the gap, fire next neuron, then
reload in fractions of a second
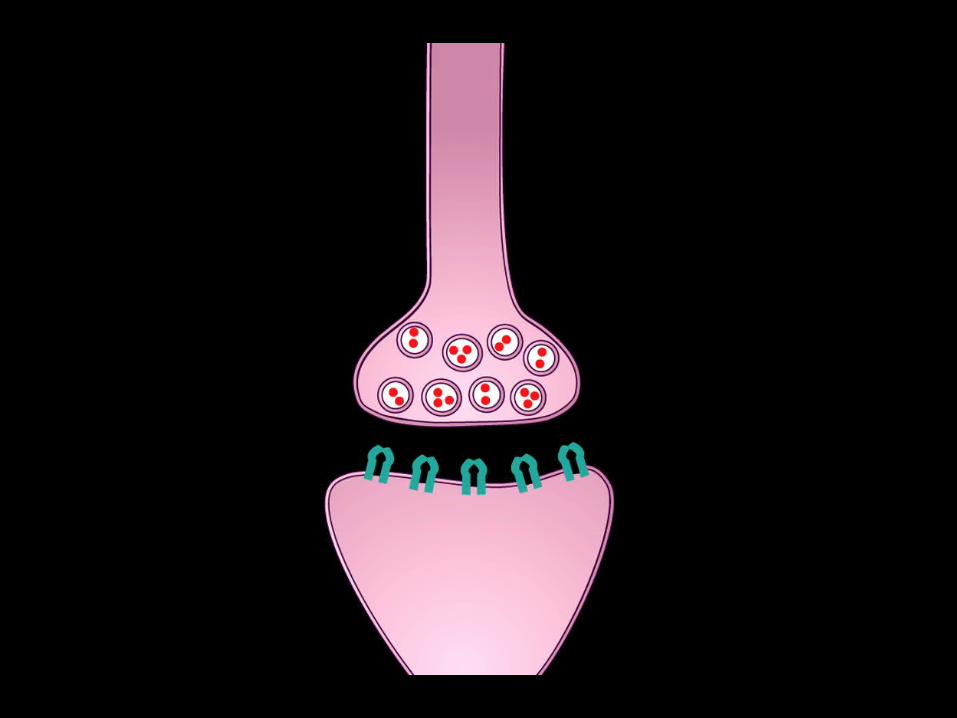

MessageZips in

Releasing transmitter

MessageZips on

Reloadingtransmitter

2 crucial chemicals: 2 crucial chemicals: (dopamine, noripinephrine)(dopamine, noripinephrine)
control most of functions impaired in ADHD Brain of person with ADHD makes these
chemicals, as does everyone else but does not release & reload effectively
control messages often not connecting For 80% of those with ADHD medications
improve this problem.

How do ADHD Impairments of EF How do ADHD Impairments of EF Usually Respond to Medication?Usually Respond to Medication?
This wide range of cognitive impairments responds to medication treatment in 70-90% of cases in children, adolescents and adults
Symptom improvement varies from modest to very dramatic
Adverse effects are usually transient, not significant

Safety of ADHD MedicationsSafety of ADHD MedicationsAmerican Medical Assn. ReportAmerican Medical Assn. Report
“More than 170 studies involving >6,000 children using stimulant medications for ADHD…up to 90% will respond to at least 1 stimulant without major adverse events if drug titration is done carefully “
Adverse effects from stimulants are generally mild, short-lived, & responsive to dosing or timing adjustments”
(Goldman, et. al., 1998, pp 1103-1104)

Substance Abuse Substance Abuse Associated With ADHDAssociated With ADHD
Risk of developing SUD over lifetime is 52% for adults with ADHD vs 27%
In ADHD, substance-use disorders onset earlier, last longer, & remit more slowly
If ADHD is appropriately treated with stimulant medications in childhood and adolescence, risk of SUD reduced 84%
Wilens, Farone, Biederman, et al, Pediatrics, 2003)

ADHD: Targets of PharmacotherapyADHD: Targets of Pharmacotherapy
Core symptoms:
• Inattentive ± hyperactive, impulsive
Associated impairment:
• occupational failure, social and academic deficits
Pattern of comorbid disorders:
• oppositional, antisocial, substance use, mood and anxiety disorders

MTA Study of ADHD TxMTA Study of ADHD Tx
579 children (7-9 years)
ADHD Combined Type
14 months duration (10 yr f/u)
Six sites

MTA GroupsMTA Groups
1. Med Mgmt: tailored dose design
TID dosing, monthly monitoring
2. Behav Tx: 8 wk summer prog, pt training child tx, schl aide, tchr consults, daily rpts.
3. Combined Med Mgmt + Behav Tx
4. Com Care: evals, 67% on meds, BID

MTA ResultsMTA Results
1. Med Mgmnt, Comb Tx >Beh Tx, ComCare
2. Combined Tx = Med Mgmt for ADHD Sx
3. Comb Tx slightly better for assoc probs
4. Med Mgmt better than ComCare meds

MTA StudyMTA Study“Excellent Response” to Tx“Excellent Response” to Tx
% of Ss scoring average of <1
(“just a little”) on SNAP-IV for
Inattn, Hyper/Impulsive, Opp/Defiant
25% Community Care
34% Behavioral Treatment only
56% Medication Mgmt only
68% Combination Tx(Swanson, et. al., 2001)

Rates of Sudden Death in Rates of Sudden Death in population vs. on stimulantspopulation vs. on stimulants
SD rates in General Population (Berger et al. Ped Clin N America, 2004)• 0.6-6 / 100,000 children/ year• 1 / 1000 adults/year
Estimated SD rate on stimulants (based on Rx data)• 0. 25/ 100,000 people/ year (calculated based on
data)• 0.50/ 100,000 people/ year (assuming 50%
underreporting)
(T.Wilens, 2006)
FDA Pediatric Advisory Committee 3/24/06FDA Pediatric Advisory Committee 3/24/06
Reassessment by larger FDA Pediatric Advisory 3/24/06
• No additional CV risk in medically healthy kids
• risk with structural heart defects approximates that in child athletes (T. Wilens, 2006)
FDA Advisory Committee 2/9/06FDA Advisory Committee 2/9/06RecommendationsRecommendations
American Heart Association Guidelines (Gutgesell et al., Circulation; 1999; J Am Acad Child Adoles Psych; 1999)
No need for ECG, Echo, Cardiac biopsy in routine cases
But if:
-- Family history of SD (<30 yrs of age)• Hx of structural / congenital cardiac structural defects• Syncope• Chest pain• Palpitations• Hypertension
Monitor during treatment(T. Wilens, 2006)
Patients’ Fears of Medications Patients’ Fears of Medications for ADHDfor ADHD
Change personality “zombie”? Slow growth? Start tics? Lose appetite? Sleep? Later drug or alcohol problems? Dependence on meds for lifetime? Being labeled, attribution problems? Reactions of family, teachers, peers?

Controversial Treatments for ADHDControversial Treatments for ADHD
Dietary restrictions (food dyes, sugar) Diet supplements: anti-oxidants, algae optometric vision training EEG neuro-feedback
No scientific evidence for the safety or effectiveness of these treatments for ADHD, but NIMH is doing study on neurofeedback

ADHD “miracle” duped thousandsADHD “miracle” duped thousands
Dore treatment claimed to help ppl with dyslexia and ADHD by stimulating cerebellum with exercises
40K ppl completed 12 mo program at cost of $4970.
Journal article in Dyslexia praised Dore (biased & flawed)
Clinics closed, company bankrupt, many clients got no refund
A Chemical ProblemA Chemical Problem
ADHD is fundamentally a chemical problem
Most effective treatment is to change the chemistry with medication
Unless the problematic chemistry is changed, other interventions are not likely to be very effective

Adapted from Wilens TE, et al. Annu Rev Med. 2002;53:113-131. Greenhill LL. Childhood attention deficit hyperactivity disorder: pharmacological treatments. In: Nathan PE, Gorman J, eds. Treatments That Work. Philadelphia, Pa: Saunders; 1998:42-64.
Attention Deficit Attention Deficit Hyperactivity DisorderHyperactivity Disorder
Pharmacologic Treatments
Not Approved by FDA for ADHD
AntidepressantsTricyclicsBupropionAntihypertensives
Clonidine Guanfacine
Miscellaneous
Combined pharmacotherapyModafinilVenlafaxineNeuroleptics (only in severe cases with monitoring)
Approved by FDA for ADHD
Stimulants
MethylphenidateAmphetamine compounds Dextroamphetamine Lisdexamfetamine
Nonstimulant
Atomoxetine

Stimulant MedicationsStimulant Medications Amphetamine
- dextroamphetamine (Dexedrine): 4-6 hours
• d, l amphetamine (Adderall): 4-6 hours
• Extended release (Adderall-XR) 8-10 hours
• Lisdexamfetamine (Vyvance) 10-12 hours
Methylphenidate• Ritalin: 4 hours
• Concerta: triphasic, 10-12 hours
• Metadate CD: biphasic, 8 hrs
• Focalin (d -isomer) 4 hours
• Focalin-XR 8 hours
• Ritalin-LA (biphasic) 6-8 hours

Medications for ADHD SyndromeMedications for ADHD Syndrome
Demonstrated safe and effective
Often do not follow mg/kg
Effective dose not based on age, wt or severity of sx
Require titration and monitoring to “fine tune” to:
- individual sensitivity
- time frames for schedule and tasks

Time Frames and ReboundTime Frames and ReboundIf sustained feeling/acting
excessively:
• “wired” or racy
• irritable
• serious, loss of “sparkle”
during the time dose is active, dose is probably too high
ActiveDrop-off
If these effects occur as med is wearing off, problem is more likely to be “rebound”, ie dropping too fast.
IngestionTime
Lev
el o
f m
ed i
n t
he
blo
od
stre
am
TE Brown, 2002

ADHDADHDResponse to StimulantsResponse to Stimulants
0
10
20
30
40
Best Response(Percent)
Dextroamphetamine Methylphenidate Equal response to either stimulant
Meta-analysis of within-subject comparative trials evaluating response to stimulant medications
36%
26%
38%

OROS (methylphenidate HCI)-
Concerta Capsule-Shaped Tablet
Orifice/Exit Port
Drug Compartment #1
DrugCompartment #2
PushCompartment
Before Operation During Operation
Water
Water
R
Drug Overcoat
Rate Controlled Membrane
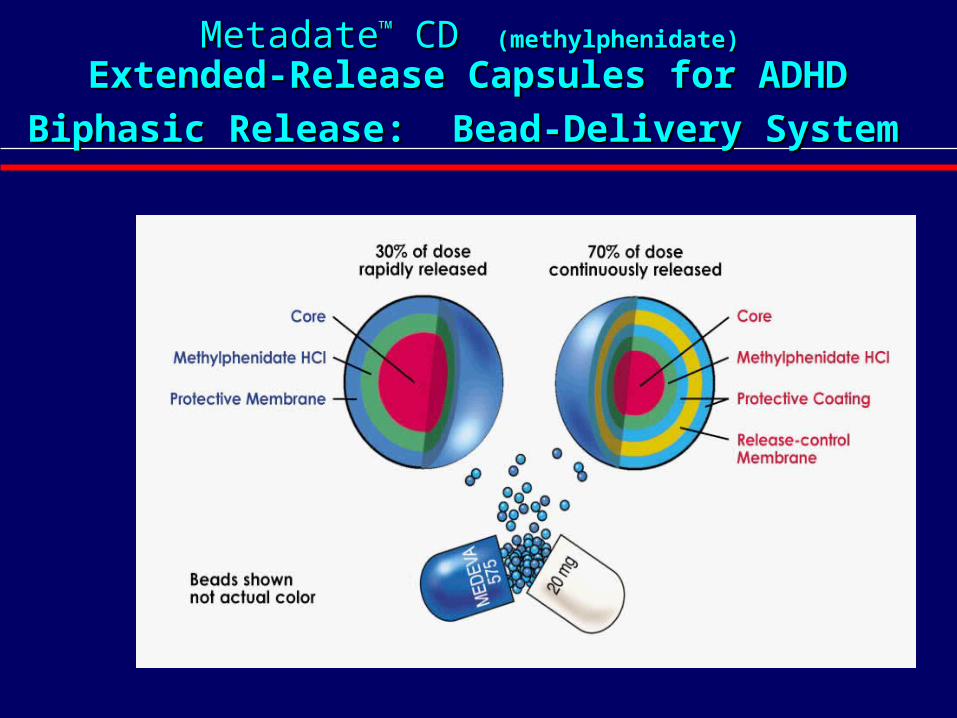
MetadateMetadate™™ CD CD (methylphenidate) (methylphenidate)
Extended-Release Capsules for ADHD Extended-Release Capsules for ADHD
Biphasic Release: Bead-Delivery SystemBiphasic Release: Bead-Delivery System

dd-MPH-XR -MPH-XR (Focalin XR(Focalin XR™™))
SODASTM release system
• 50% IR d-MPH beads and 50% ER d-MPH beads covered by polymer overcoat
• Can be sprinkled on food
Single isomer technology
• Composed of only the d-MPH stereoisomer (dexmethylphenidate)
0 4 8 12 16 20 24 28 320
5
10
15
20
Time (h)
d-MPH-XR 20 mg qd
SODASTM MPH 40 mg qd
MPH MR 20 mg qd
OROS® MPH 18 mg qd
Mea
n P
lasm
a M
eth
ylp
hen
idat
eC
on
cen
trat
ion
(n
g/m
L)
Mean plasma concentrations over time
• Two peaks
Source: Focalin XRTM [package insert], Novartis Pharmaceuticals Corporation.

Stimulant DosingStimulant Dosing Medication Starting Dose Maximum Dose* Usual Dosing
Ritalin® 5 mg QD/BID 2 mg/kg/day TID (4 h) Focalin® 2.5 mg 1 mg/kg/day BID (5-6h?)
Dexedrine® 2.5 to 5 mg QD 1.0 mg/kg/d BID/TID (4 h)Dex Spansule 5 mg 1.0 mg/kg/d BID (6 h)
Adderall® 2.5 to 5 mg QD 1.0 mg/kg/d BID (6 h)AdderallXR® 5-10 mg 1.0 mg/kg/d QD (12 h)Vyvanse 30 mg 30 to 70 qd QD (13 hr)
Wilens, et al. Annu Rev Med. 2002;53:113-131; updated 2005.
Concerta® 18 mg QD 2 mg/kg/day QD (12 h)MetadateCD® 20 mg QD 2 mg/kg/day QD (6-8 h)Ritalin LA 10 mg QD 2 mg/kg/day QD (6-8 h)Focalin XR 5 mg QD 2 mg/kg/day QD (8-10h?12)
*Maximum dosing may exceed FDA approved dose limits.
Advantages of Extended-Release Advantages of Extended-Release Formulations of StimulantsFormulations of Stimulants
Provides sustained medication levels Provides sustained medication levels throughout the daythroughout the day
Smoother: minimizes ups and downs during Smoother: minimizes ups and downs during dayday
No midday dose required, eliminating trips to No midday dose required, eliminating trips to the school nurse, doses during workdaythe school nurse, doses during workday
Reduces stigmaReduces stigma
Enhances patient complianceEnhances patient compliance
May reduce illicit diversion and abuseMay reduce illicit diversion and abuse

Management Strategies for:Management Strategies for:
Severe Decrease
In appetite
• Monitor weight
• Administer with or after meals
• Give high-calorie snacks
• Consider medication holidays
• Eat in reverse
Headache/Stomachache,
Irritability/Moodiness, or OCD Symptoms
• Decrease dose
• Switch to another stimulant
• Switch to 2nd line agent
Wilens & Spencer, 2000

Management Strategies for:Management Strategies for:
Delayed Sleep Latency
Sleep Hygiene/Bedtime rituals
Change to shorter acting stimulant
Consider adjunctive treatment (e.g., clonidine)
Relaxation training
Irritability Evaluate when it
occurs• Peak (too high dose)
• Wear off (? rebound)
Change dose Assess for comorbidity Consider adjunctive
therapy
Wilens & Spencer, 2000

Non-StimulantNon-Stimulant options for ADHD options for ADHD
Specific noradrenergic agent approved for ADHD -Strattera (atomoxetine)
Antidepressants (not approved for ADHD)-Wellbutrin (buproprion)-Pamelor (nortriptyline)-Norpramin (desipramine)
Alpha-2 Agonists (not for cognition) (Not Approved for ADHD)-Catapres (clonidine)-Tenex (guanfacine)

PDR Recommendations (Not a controlled substance)
• Start ≈ 0.5 mg/kg/d
• Target 1.2 mg/kg/d
• Max of 1.4 mg/kg/d or 100 mg/d
Example: 8 year old
• Start 18 mg for 4-7 days in AM after food
• 25 mg for 4-7 days then increase to 40 mg
If already on stimulant, cross-taper, introduce ATMX then reevaluate need for stimulant
Available in 10mg, 18mg, 25mg, 40mg, 60mg
Sprinkling not formally tested and may irritate GI tract
Full benefits often not seen until 4 to 6 weeks of treatment!
Dosing of Atomoxetine in ADHDDosing of Atomoxetine in ADHD
Physician Desk ReferencePhysician Desk Reference®®.. MMonvale, NJ:Thompson PDR;2005.onvale, NJ:Thompson PDR;2005.

Dosing of Atomoxetine in AdultsDosing of Atomoxetine in Adults
Initial: total daily dose of 40 mg increased after ≥ 1 week to a target of ~80 mg
Administered either as:• Single daily dose in the morning • Evenly divided doses in the morning and late
afternoon/early evening (bid dosing in adult trials)
After 2 to 4 additional weeks, dose may be increased to a maximum of 100 mg daily (patients without an optimal response)
Full benefits often not seen until 4 – 6 weeks of steady treatment!
Strattera® [package insert]. Indianapolis, Ind: Eli Lilly; 2003.

Comparative Study of ATX vs OROSComparative Study of ATX vs OROS
492 patients with ADHD (6-16 yrs) randomized to ATX (0.8-1.8 mg/kg/d)
OROS (18-54 qd) or PBO for 6 wks Response (≥40% sx improvement)
ATX: 45% OROS: 56% PBO: 24% Of 70 Non-responders to OROS 43% + Of 69 Non-responders to ATX 42% +
(Newcorn, Kratochvil, et al, 2008)

Types of non-pharmacological Types of non-pharmacological treatmentstreatments
1. Psychoeducation about ADHD and its treatment to address prejudices/fears
2. Cognitive-behavioral treatments to modify maladaptive attitudes
3. Remedial instruction/coaching to modify deficits or maladaptive behaviors

Non-Pharmacological TreatmentsNon-Pharmacological Treatmentsare important to ADHD treatmentare important to ADHD treatment
ADHD/ADD results from impairment brain chemistry and medication is most effective treatment
BUT, medication is not effective if not taken
cannot fully alleviate some symptoms

Some ADHD patientsSome ADHD patientsdo not take their ADHD medicationsdo not take their ADHD medications
Because they:
have prejudices about the disorder
fear and don’t understand ADHD meds

Primary Primary PrejudicePrejudice about ADHD about ADHD
“It’s essentially a simple problem, a matter of willpower” because….
“It’s just being too hyper and not listening”
“Everyone with ADHD can pay attention very well for certain specific activities”

Primary Primary fearsfears about ADHD medications about ADHD medications
“This will make problems for me”
“make me too hyper or too slow”
“take away my personality”
“get me dependent or addicted”

Patient Education is needed about Patient Education is needed about medicationsmedications
Need to be “fine-tuned” in collaboration with each patient
Set patient expectations to collaborate adjust med, dose or timing to individual
needs and body chemistry prevent stimulant “rebound” Need to report any side effects

Home Interventions Home Interventions for ADD/LD School Problemsfor ADD/LD School Problems
daily parental reading with child daily parental help with organization/study early computer training and use supplementary audio or videos remedial tutoring avoid micro-managing homework for teens protect non-academic strengths
Parent Training for Management of Parent Training for Management of ADHD Behavior ProblemsADHD Behavior Problems
positive attending rewards for appropriate behavior planned ignoring transition management target behaviors & point systems use of “time out” & “response cost”(Cunningham, 1998; Teeter, 1998)

Improving Interactions of ADHD Teens Improving Interactions of ADHD Teens and Their Parentsand Their Parents
recognize aims & limits of parental control facilitate appropriate independence seeking maintain adequate structure & supervision establish & enforce “bottom line” rules negotiate all “non-bottom line” issues use consequences wisely to influence focus on positives, practice forgiveness(A.Robin, 1998, C.Dendy, 1995)

School AccommodationsSchool Accommodationsfor ADD/LDfor ADD/LD
Daily check of assignments & organization preferential seating reduced volume of work weekly/daily progress reports alternative test delivery (oral/written) extended time for tests (as needed)(S.Rief, 2005, C.Dendy, 2000)

Cognitive Behavioral Treatments for:Cognitive Behavioral Treatments for:
Defensive attitudes about self & others: “Everyone expects too much from me.” “I may seem smart, but I’m really stupid.” “High goals just bring disappointment.” “It’s not worth trying; the world is unfair.” “I’m just destined to be a loser.”
These attitudes have cognitive & emotional aspects

Remedial instruction or Coaching for: Remedial instruction or Coaching for:
Skill deficiencies that persist Study skills and academic deficits Organization of ideas and stuff Priority setting & time management Budgeting income and spending Monitoring self in conversations
Pills don’t teach skills.

Clinical Tips for Psychosocial Treatment Clinical Tips for Psychosocial Treatment of Adult ADHD of Adult ADHD
(Ramsay & Rostain, 2005, 2007)(Ramsay & Rostain, 2005, 2007)
Assess patients’ “readiness for change” (motivation and resources)
Provide psychoeducation about ADHD
Maintain an active therapeutic stance and collaboration with patients
Pay attention to the quality of the therapeutic relationship
Maintain focus on specific functional problems faced by patients

Clinical Tips for Psychosocial Treatment Clinical Tips for Psychosocial Treatment of Adult ADHD of Adult ADHD
(Ramsay & Rostain, 2005, 2007)(Ramsay & Rostain, 2005, 2007)
Implement cognitive modification and foster resilient attitudes
Normalize trial-and-error nature of the therapy process for adult ADHD
Encourage individualized coping strategies for “living with ADHD”
Maintain ongoing case conceptualization Consider referrals for additional clinical services
(e.g., medications, coaching)

Cognitive Model of PsychotherapyCognitive Model of Psychotherapy (Ramsay & Rostain, 2005, 2007)(Ramsay & Rostain, 2005, 2007)
• Based on cognitive model of psychopathology
• Time efficient • Structured, active• Collaborative problem-solving• Regular homework

Interventions to ProvideInterventions to ProvideTherapy & SupportTherapy & Support
relevant articles, books and websites support groups: CHADD, ADDA on-site support: for patient, teachers psychotherapy- individual, conjoint parent support/training mgmnt skills crisis intervention “realistic hope” vs. “optimism”

Levels of Care for ADHDLevels of Care for ADHDtailor to pt & family needstailor to pt & family needs
Comprehensive assessment for ADHD,
comorbid disorders, and context Family Education re: ADHD and its tx PE, “fine-tuning” of meds, monitoring Parent support & behavior mgmnt training Accommodations/Interventions in school Psychotherapy: individual, family