Medication Approaches to the Neuropsychiatric Sequelae of TBI TW McAllister, M.D. Professor of...
101
Medication Approaches to the Neuropsychiatric Sequelae of TBI TW McAllister, M.D. Professor of Psychiatry Director of Neuropsychiatry Dartmouth Medical School
-
Upload
shanon-blair -
Category
Documents
-
view
215 -
download
1
Transcript of Medication Approaches to the Neuropsychiatric Sequelae of TBI TW McAllister, M.D. Professor of...

Medication Approaches to the Neuropsychiatric Sequelae of TBI
TW McAllister, M.D.
Professor of Psychiatry
Director of Neuropsychiatry
Dartmouth Medical School

Why learn about meds?
• Improves care
• Improves your clinical skills
• Fosters participation in treatment
• Facilitates holistic approach to care

Bottom line…
• You need to decide what you are treating…– Not “organicity”– Not “tbi”– No sloppy thinking allowed– It’s ok to be wrong, not ok to be vague– Avoid collecting psychotropics like notches
on a pharmacological belt

General Principles
• Challenges in assessment
• Vulnerability to side effects
• Clarification of goals

MIXED AND FLUCTUATINGSYMPTOM PICTURE
• PROMINENT MOOD CHANGES
• PROMINENT ANXIETY/AGITATION
• PROMINENT IMPULSIVITY
• PROMINENT FEATURES
FLUCTUATE OVER TIME

VARIABLE COGNITIVE DEFICITS
• IMPAIRED ATTENTION AND CONCENTRATION
• IMPAIRED PLANNING AND
PROBLEM SOLVING
• IMPAIRED MEMORY AND
LEARNING
• IMPAIRED LANGUAGE FUNCTION

COMMUNICATION DEFICITS
• PROPOSITIONAL AND PROSODICFUNCTION CAN BE IMPAIRED
• DIFFICULT TO MATCHAFFECT AND CONTENT
• DENIAL SYNDROMES
• LACK OF EXPERIENCE WITHPSYCHIATRIC LANGUAGE


One effect of ALS is that certain emotional breaks seem to be ineffectual.
…I was not as upset or as sad as my crying would imply, nor as uproariously amused as my uncontrollable laughter would indicate.
You have no idea how terrible it is when the crying is fully triggered and takes hold like a seizure. I can’t control any of it. I simply disintegrate and it isn’t only emotionally horrible with me, it is physically painful and debilitating.
______________________________________________Lieberman A, Benson DF: Control of emotional expression in pseudobulbar palsy: A
personal experience. Archives of Neurology 34:717-719, 1977.

Filter Effects of CNS Injury
• What does depression look like in someone who is non-verbal?
• What does manic hyperactivity look like in someone with quadriplegia?
• How do hallucinations and delusions present in someone who cannot describe them?

Vulnerability to Side Effects
• Neuropsychiatric patients show increased frequency & severity of side effects to most psychotropics
• Can manifest as worsening of neurological sx’s (tremor, cognition, slowing, etc.)

Is the Behavior Related to The CNS Pathology?
Implications For
• Conceptualization of the Behavior
• Interpretation of the Behavior
• Therapeutic Approach
• Prognosis

General Principles
• Impact on Cognition– Memory – Benzodiazepines,
antidepressants (anticholinergic effects)– Attention – Benzodiazepines, neuroleptics– Speed of Information Processing –
Benzodiazepines, neuroleptics, others
• Thus the very areas most affected by TBI can be made worse!

Clarification of Tx Goals
• As always, accurate Dx is critical first step
• Know what you are treating before Rxing
• Are you treating the underlying disorder, or the comorbid psychopathology?

Common Behavioral Syndromes in the Brain Injured
• Depressive Syndromes
• Dyscontrol Syndromes
• Attention Deficit Syndromes
• Sleep Disorders
• Psychotic Syndromes

TBI and Psychiatric Disorders
From van Reekum et al. Can traumatic brain injury cause psychiatric disorders? J Neuropsychiatry 12:316-327, 2000
Disorder Total N
(# studies)
Max Duration of Follow-Up (yrs)
# With Disorder
% With Disorder
Relative Risk
Depression 653(8)
7.5 289 44 7.5
Bipolar Affective Disorder
354(5) 7.5 15 4.2 5.3
Gen. Anxiety Dis 398(5) 7.5 36 9.1 2.3

Despite Diagnostic Challenges…
• When behaviors change:– New behaviors– Change in frequency and intensity of
previous behaviors
• Have a high index of suspicion for the common psychiatric disorders

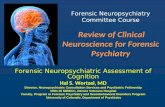
Illustration by Lydia Kibiuk

Neurotransmission at the Synapse
Illustration by Lydia Kibiuk

(From http://www.onu.edu/user/FS/tfaulkner/Dopamine.htm)
Dopamine and Norepinephrine

Principles of Signal Transmission
• OVERALL SCHEME:
• Electrical Signal (change in membrane potential)
• Change in Ion Flux (e.g., Na+, K+, Ca++)
• Release of Neurotransmitter into Synapse (first messengers)

Principles of Signal Transmission
• OVERALL SCHEME:
• Binding of Neurotransmitter to pre- and post-synaptic receptors
• Activation of specific enzymes
• Production of second messengers (e.g., cAMP, IP3, DAG) or ion flux

Principles of Signal Transmission
OVERALL SCHEME
• Phosphorylation of target proteins
• Target Effects

Principles of Signal Transmission
• Steps of Neurochemical Signaling
– Neurotransmission– Receptor Binding– Signal Transduction– Second Messenger Activation– Feed Forward/Back

Principles of Neurotransmitter Signaling
• SYNAPTIC EFFECT – to effect behavior, diseases or drugs must alter the synaptic content of a given neurotransmitter
• SYNAPTIC HOMEOSTASIS – release of any neurotransmitter tends to reduce the amount released subsequently

Ways of Altering Synaptic Content of Neurotransmitters
• Synthesis
• Storage
• Release
• Binding
• Re-uptake
• Metabolism

Adapted from BG Lehmkuhle 2000
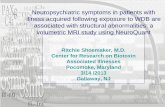
Serotonin

FC = Frontal cortex
PC = Parietal cortex
OC = Occipital cortex
H = Hippocampus
M = Medial septal nucleus (Ch. 1) and diagonal band of Broca (Ch. 2)
T = Diagonal band of Broca projecting into the olfactory tubercle (Ch. 3)
B = Nucleus basalis of Meynert (Ch. 4)
Adapted from Coyle JT et al. Science. 1983;219:1184-1190. McNeal. Alzheimer’s Disease: Unraveling the Mystery. 1995:1-48.
AcetylcholineAcetylcholine
MT

• Acetylcholine
– animal models
• susceptibility of hippocampal cholinergic systems due to
– acute cholinergic excess/acute cholinergic neurotoxicity– long-term cholinergic deficits due to acute cholinergic
neurotoxicity– strong relationship between cholinergic deficits and
memory impairment following TBI
(Saija et al. 1988; Dixon et al., 1994, 1995, 1997; Leonard (JR) et al. 1994; Schmidt and Grady, 1995; Dewar and Graham 1996; Ciallella et al., 1998; North et al.; Murdoch et al., 1998; O’Shanick 1991)
Neurotransmitter Dysfunction after TBI

• Acetylcholine
– human studies (in vivo)
• cortical cholinergic dysfunction years after TBI among those with persistent symptoms of attention and memory impairment
– P50 nonsuppression reflects hippocampal cholinergic dysfunction
– patients with impaired auditory gating, attention, and memory following TBI are P50 nonsuppressors (abnormal)
– patients with such symptoms and P50 nonsuppression following TBI have significantly reduced total brain and hippocampal volume
– cholinesterase inhibition normalizes P50 nonsuppression in 50-70% of these patients
(Arciniegas et al. 1999, 2000, 2001a, 2001b, 2002)
Neurotransmitter Dysfunction after TBI

Neurobiological Changes after TBI• The principal neurobiological consequences of TBI are:
– cortical contusions (mostly in severe TBI)
• results in a loss of function served by that area
– white matter lesions• results in interruption of information processing between cortical
areas
– diffuse axonal injury• results in slowed and inefficient information processing• disproportionately affects glutamatergic and cholinergic
projections– results in problems with attention, memory, and various aspects of
frontally-mediated cognition (ie, working memory, executive function)
• may affect serotonergic systems• dysfunction in these systems may secondarily affect the
efficiency of function in dopaminergic or noradrenergic systems

Psychopharmacological Issues
• Medication approaches generally take three broad approaches: – amelioration of psychiatric complications– amelioration of specific somatic symptoms
(e.g., headache, dizziness, sleep disturbances)
– augmentation of cognition

Psychopharmacological Issues
• At present, there are no FDA approved treatments for cognitive, emotional, or behavioral impairment due to TBI
• pharmacotherapies are generally modeled after those for patients with phenomenologically similar but etiologically distinct disorders (i.e., attention-deficit hyperactivity disorder, Alzheimer’s disease, etc.).

Psychopharmacological Issues
• General Principles:– Clarify/simplify current regimen– Clarify critical target symptoms to treat– Target specific symptoms


Dosage Considerations
• Start lower
• Go slower
• Stop sooner

Approach to Cognitive Deficits
• Main target domains:– Memory
• Particularly working memory
– Attention– ?Executive Functions

Neurotransmitter Dysfunction after TBI
• Many neurotransmitters are involved in the regulation of cognition
• Several neurotransmitters are particularly relevant to the regulation of frontal and frontotemporal structures involved in cognition:– dopamine– norepinephrine– serotonin– acetylcholine– glutamate gamma-aminobutyric acid (GABA)

Neurochemical Rationale
• Most work in animals and humans suggest important role in memory and attention for both:– Catecholaminergic systems
• Dopaminergic• Alpha-2-adrenergic
– Cholinergic systems
• Thus most agents are directed towards augmentation of these systems

Dopamine Agonists
• A variety of agonists have been shown effective in animal models and are used clinically:– Methylphenidate (and other stimulants)– Amantadine– Bromocriptine– Bupropion

Alpha-2-Adrenergic Agonists
• Infusion of A2A agonists improves WM function in primates and rodents
• guanfacine can improve WM in healthy individuals and may improve working memory after TBI
• Methylphenidate also has A2A agonist properties

Cholinergic Augmentation
• Multiple studies demonstrate that cholinergic augmentation, generally using one of several cholinesterase inhibitors (e.g., physostigmine, donepezil) can improve TBI-induced attention and memory deficits even in the late post-injury period (>1 year) in some TBI survivors – Taverni 1998; Whelan 2000; Cardenas 1994;
Arciniegas 2001

Approach to Cognitive Deficits
• Baseline testing• Trial of DA, A2A, or Cholinergic agent
– Methylphenidate – start 5 mg/day– Aricept - start 5 mg/d
• Titrate up slowly as tolerated• Discontinue after 2 months if no improvement

Approach to Depression
• Trials of– SSRI– second SSRI– Low dose Desipramine or Bupropion
• Other– MAOIs– ECT

Approach to Mania
• Valproic Acid
• Lithium
• Combination approaches
• Newer anticonvulsants– Lamotrigine– Topirimate

Psychotic Syndromes
• Relatively rare compared to other behavioral changes
• However, more disturbing and disabling
• Psychosis is primary Dx in 10% of post –TBI psychiatric hospital admissions
• Impede rehabilitative process

Chronic Psychotic Syndrome Following TBI as an Adult
• Mr C is a 33 yr old man referred for paranoia– No neuropsychiatric history, and no family
hx of psychiatric illness until age 22 when suffered a severe TBI in an MVA ( LOC for several days, PTA several wks)
– Sequelae included post-traumatic epilepsy and cognitive deficits

Chronic Psychotic Syndrome Following TBI as an Adult
• VIQ of 113, PIQ of 102, FIQ 108. Some frontal executive deficits
• Within 3 yrs developed chronic severe suspiciousness and intermittent paranoid psychotic syndrome. – Convinced that people were plotting to
harm him. Notified police. – Experienced delusions of being controlled
by alien forces.

Chronic Psychotic Syndrome Following TBI as an Adult
• Unable to hold several jobs because became suspicious of co-workers and accused them of plotting against him.
• No clear relationship with seizures
• Responded poorly to various meds, but refused antipsychotics.

Traumatic Insanity
• Meyer’s 1904 paper often credited with popularizing the idea that brain trauma can produce “insanity”
• Referenced several previous studies, including one of Franco-Prussian War veterans, with an incidence of post-injury psychosis of 2.5%

Issues in Attributing Causality
• Consistent association between causative agent (TBI) and outcome (psychosis)
• Biologic gradient (more of the agent causes more of the outcome)
• Temporal sequence (TBI before psychosis)
• Biologic rationale

TBI & Schizophrenia(Adapted from Davison K, Bagley CR. Schizophrenia-like psychosis associated with
organic disorders of the CNS: A review of the literature. Br J Psychiatry 4(suppl):113-184, 1969
N % With Psychosis
Observation Period
Author
500 0.4 3 mosAita & Reitan, 1948
3,000 0.07 2 yrsPoppelreuter, 1917
1,821 1.2 10 yrsHillbom, 1951
1,110 1.5 15 yrsMeinertz, 1957
1,564 1.7 15 yrsFeuchtwanger and Mayer-Gross, 1938
4,807 0.7 15 yrsLiberman, 1964
1,168 9.8 15 yrsLobova, 1960
415 2.6 20 yrsHillbom, 1960

Intermittent Delusional Syndrome Following TBI
• Mr D is a 43 yr old man referred for delusions after a TBI
• No neuropsychiatric history until a severe TBI at age 22 (comatose for 3 wks.)
• Aphasic, with right hemiplegia initially, then made remarkable recovery of speech/language and motor function

Intermittent Delusional Syndrome Following TBI
• VIQ – 108, PIQ – 114, FIQ – 111. Some frontal executive deficits
• Within 3yrs of TBI had onset of strong conviction that God had saved his life for a reason, and that he was chosen to reveal God’s power on earth. Directed to take specific vitamins which would enlarge his breasts and shrink his penis.

Intermittent Delusional Syndrome Following TBI
• Delusions at times accompanied by auditory hallucinations, heightened activity, irritability, and assaultiveness suggesting irritable mania.
• Some response to lithium carbonate. Twice he discontinued the Li with a return of symptoms

Temporal GradientStudy Sample Latency
Achte et al 1969, 1991. (Psychopath 24:309-315)
WWII veterans, mainly penetrating TBI
2 days to 48 yrs, 42% occurring 10 yrs after
Fujii and Ahmed, 1996 (Neuropsychiatry, Neurospych, Beh Neurol. 9:133-138)
State hospital sample
3 mos – 19 yrs, mean of 5.9 yrs
Feinstein and Ron 1998 (J Neuropsychiatry,10:448-452
44 subjects with psychosis after neurol dis
0-54 yrs, mean of 11.7 yrs

Latency of Psychotic Symptoms
• Most studies suggest latencies from injury to psychotic symptoms of 10 –20 years

Does TBI cause psychosis, or activate “latent psychotic
disorder”?
• Hillbom and Meinertz noted only rare family history of schizophrenia in their series of psychotic TBI patients
• Many studies have found no increase in rates of pre-morbid “schizoid personality”, or schizophreniform disorders in first degree relatives

Psychiatric Disorders and TBI
• Traumatic Brain Injury and Schizophrenia in Members of Schizophrenia and Bipolar Disorder Pedigrees– Malaspina D, Goetz R, Friedman J et al.– Am J Psychiatry 2001; 158: 440-446

Malaspina et al.
• Compared rates of history of TBI in multiplex pedigrees of schizophrenia (n= 565) and bipolar disorder (n=1275).
• Subjects came from families with at least two biologically related first-degree relatives diagnosed with the core illness (Schiz. or BAD)

Malaspina et al.
• Compared to never mentally ill family members:– Threefold greater rate of reported TBI in
those with schizophrenia– Twofold increased rate of TBI in those with
BAD and MDD
• Argue for interaction between genetic vulnerability and injury (protective role for no injury)

Other Links to Psychosis
• PTA – resembles delirium in many respects– Restlessness, fluctuating level of consciousness,
agitation.– Hallucinations and delusions occur frequently
• Mood Disorders– Depression– Mania
• Seizure Disorders

Post-traumatic Epilepsy
• Psychotic syndromes most often associated with complex partial seizures with temporal and frontal lobe foci (4-12 times more commonly)
• Can be peri-ictal (episodic), or interictal (chronic)

Post-ictal Psychotic Syndrome
• Mr E is a 24 year old male referred because of hyper-religiosity.
• Neuropsychiatric history unremarkable until age 8 when he was struck by a car and sustained a severe TBI. No family history of psychiatric illness
• Developed post-traumatic epilepsy (complex-partial type) 3 yrs later

Post-ictal Psychotic Syndrome
• At age 14, developed an episodic psychotic syndrome characterized by florid hyper-religiosity, auditory hallucinations (messages from Jesus, God, or the devil).
• These episodes usually preceded within 24-48 hrs by a seizure or more typically a cluster of seizures

Post-ictal Psychotic Syndrome
• EEGs showed R temporal lobe epileptiform activity.
• When seen, Mr E reported hearing Jesus, and seeing “a brilliant light” which he said signified the location of Ross Perot. These symptoms resolved after 72 hrs.
• Improved seizure control resulted in fewer psychotic episodes

Summary
• Disorders of thought content and thought process complicate recovery from TBI
• Psychotic syndromes occur at rates greater than those in general population
• Injury severity positively correlated with risk• Even in absence of formal criteria,many with
TBI have psychotic symptoms

Summary
• Thus good evidence for:
– Consistent association
– Temporal gradient
– Severity gradient
• What about biological rationale?

Results – IBIA Evidence Based Review of NBC of TBI
• There were no Class I, or II studies found which addressed the treatment of psychotic syndromes
• Some Class III studies addressed these patient populations, many of these had such methodological flaws that they were not useable in establishing treatment guidelines.

Class III – Psychotic Disorders
• Agents Used– Typical Antipsychotics
• Chlorpromazine – Bamrah, 1991; n=1
– Atypical Antipsychotics• Clozapine – Burke, 1999; n=1, Laddomada
1999; n=1• Olanzapine – Butler, 2000; n=1, Umansky,
2000; n=1• Risperidone – Schreiber, 1998; n=1

Common Methodological Problems
• Small numbers (mainly case reports or small case series)
• Selection bias (convenience samples)• Absence of:
– Standardized diagnostic measurements– Standardized outcome measurements– Blinded assessments and placebo trial– “on/off” crossover design
• Presence of:– Other diagnoses– Other interventions

Side Effects and Toxicity
• Overall no clear indication from the literature that those with TBI suffer increased frequency or severity of side effects, nor novel side effects/toxicity
• Usual side effects do occur:– Akathisia on SSRI’s– Mania on TCA’s and SSRI’s– Sedation, weight gain, seizures on Clozapine– Cognitive impairment on Lithium
• Not clear that this is different from those who have not been injured

Conclusions
• The use of standard psychotropics for standard indications (i.e. antipsychotics for the treatment of psychosis) is an option for clinicians– Use same meds, but dose differently– Cannot match clinical profile to neurotransmitter
profile of various meds– There is clearly a need for randomized clinical
trials to assess the efficacy of antidepressants, anxiolytics, and antipsychotics in the treatment of brain-injured individuals


Thanks to:
Michael J. Ryan, M.D.David Arciniegas, M.D.Jonathan Silver, M.D.
For ideas, discussions, slides….

Aggression and TBIAggression and TBI• Acute phase: 35% - 96% of patients exhibit
agitated behaviors– 89 patients assessed during the first six months
after TBI, aggressive behavior found in 33.7% of TBI patients, compared to 11.5% of patients with multiple trauma but without TBI (Tateno et al)
• Recovery phase: 31% - 71% of patients with severe TBI and 5% - 70% of patients with mild TBI are agitated or irritable
• Irritability increases with more TBI’s

Characteristics of Aggression After TBI
Characteristics of Aggression After TBI
• Reactive: Triggered by modest or trivial stimuli• Nonreflective: Usually does not involve
premeditation or planning• Nonpurposeful: Aggression serves no obvious
long-term aims or goals• Explosive: Buildup is NOT gradual• Periodic: Brief outbursts of rage and aggression,
punctuated by long periods of relative calm• Ego-dystonic: After outbursts, patients are
upset, concerned, and/or embarrassed, as opposed to blaming others or justifying behavior

Neuropathology of AggressionNeuropathology of Aggression
• HypothalamusOrchestrates neuroendocrine response to sympathetic arousalMonitors internal status
• Limbic systemAmygdala
Activates and/or suppresses hypothalamusInput from neocortex
Temporal cortexAssociated with aggression on both ictal and interictal status
• Frontal neocortexModulates limbic and hypothalamic activityAssociated with social and judgment aspects of aggression

Neurotransmitter Dysfunction after TBI
• Many neurotransmitters are involved in the regulation of cognition, emotion, behavior, and physical/motor function
• Principal neurotransmitters in regulation of frontal and frontotemporal functions include:– dopamine– norepinephrine– serotonin– acetylcholine– glutamate – gamma-aminobutyric acid (GABA)

Human Models of Aggression
Low 5-Low 5-HTHT
ObservationObservation StudiesStudies Behavioral Behavioral FindingsFindings
CSF StudiesCSF Studies
Pharmacologic Pharmacologic ChallengesChallenges
Genetic StudiesGenetic Studies
irrititability,irrititability, fire setting fire setting
impulsive homicideimpulsive homicide
maternal aggressionmaternal aggression
self destructive behaviorself destructive behavior
recidivism of murderersrecidivism of murderers

Human Models of Aggression
Low NELow NE
ObservatioObservationn
StudiesStudies Behavioral Behavioral FindingsFindingsCSF StudiesCSF Studies
-Adrenergics-Adrenergics
CSF StudiesCSF StudiesChallengesChallengesNeurolepticsNeuroleptics
Aggressive behavior inAggressive behavior in military personnelmilitary personnel
Dominance levelsDominance levelsAggressivityAggressivity High DAHigh DA

Factors Associated with Agitation in Brain Injury
AGITATIONAGITATIONPsychosisPsychosis
AnxietyAnxiety
InsomniaInsomnia
SundowningSundowning
DepressionDepression
Aggression as Aggression as direct effect of direct effect of
Brain InjuryBrain Injury
Medical Medical IllnessIllnessAdverseAdverse
EnvironmentEnvironment

Important Causes of Agitation
• Medication interaction
• UTI
• Accidental misuse of prescribed meds
• Recent CVA
• Respiratory infection
• Occult TBI
• Poor nutrition

Medications and Drugs Associated with Aggression
Medications and Drugs Associated with Aggression
• Alcohol: intoxication and withdrawal • Hypnotic and anxiolytics: intoxication and withdrawal• Analgesics (narcotics): intoxication and withdrawal• Steroids (prednisone, cortisone, and anabolic
steroids)• Antidepressants: especially during initial phases of
Rx• Amphetamines and cocaine• Antipsychotics: secondary to akathisia• Anticholinergic drugs: delirium • Quinolone antibiotics?

“Past” Treatment of Agitation• Agitation often treated non-specifically with
sedatives
– Should target underlying causes
• No medication is approved by the FDA for agitation or aggression – May reflect inconsistent concepts and goals

Evidence Based Guidelines
• Workgroup for Neurobehavioral Consequences of TBI– sponsored by IBIA, CDC
• Reviewed current literature• Class I - randomized, double-blind, placebo
controlled• Class II - data collected prospectively, or
retrospective analyses based on clearly reliable data (observational, cohort, prevalence, case control)
• Class III (case reports, retrospective, etc)

Literature Review
• 75 articles reviewed for content• 46 review articles examined for references• Studies must have focused on patients with
TBI (and not other neuropsychiatric disorders)• 9 articles were potentially Class I or II• 2 articles remained after review as Class II
evidence

Emotion Dysregulation Spectrum
Aggression
ImpulsivityImpulsivityIrritability
Agitation AngerAnger

Approach to Dyscontrol Syndromes
• Consider if due to:
– Depression
– Mania
– Psychosis
– Environmental factors
– Anxiety
• If so, treat accordingly

Aggression and Depression
• Clear link in adolescents and adults without developmental disabilities
• Several studies found high rates of aggression (30-55%) associated with depression in more severely impaired
– (Myers,1998; Charlot et al 1993; Charlot, 1997; Reiss & Rojahn 1993; Meins 1995)

Dyscontrol and Mood Disorders
DyscontrolAssault
SIBPerseveration
Activation
Depression ManiaMania

Mania
• Can present with periodic increase in the frequency and intensity of assaultive or dyscontrolled behavior

Psychotic Syndromes
• Unpredictable “out of the blue”
• Consistent misinterpretation of events in the environment
• Hypervigilance

Dyscontrol
• If not due to other Axis 1 conditions:– Beta blockers– Lithium– SSRI’s– Antipsychotics– Calcium channel blockers– Anticonvulsants
• Our current choice is Risperdal

Risperidone in Neuropsychiatic Aggression
• DBPC trial of risperidone in 31 adults w/ Autism or PDD, NOS– Mean daily dose 2.9 mg (McDougle et al., Arch Gen McDougle et al., Arch Gen
Psychiatry, 1998)Psychiatry, 1998)
• Dementia – RTCs (Katz 1999; Brecher, 1997; DeDeyn, DeDeyn,
19991999)– Signif improvement, again at low dose
(<2mg)

Choosing Among Atypical Antipsychotics
• Among individuals, there is differential efficacy*
• Cannot tell in advance who will respond to what agent
• Choice determined by other factors
* Personal opinion * Personal opinion

Nonpharmacologic Approaches
• Modify environment
• Optimize stimulation
• Use consistent routines
• Assess/adapt to aggravating factors
• Behavior management principles
• Education
• Support of patient and caregivers

Neurobehavioral Metaphors
Identify most salient symptom clusterIdentify most salient symptom cluster
Is there a pattern analogous to a more Is there a pattern analogous to a more typically drug-responsive syndrome?typically drug-responsive syndrome?
Use as a rational guide to therapyUse as a rational guide to therapy
Tariot, 1996Tariot, 1996

Examples of Metaphors “Depressive” Irritable, pessimistic, sad,
weepy, socially withdrawn, vegetative
features
“Psychotic” Angry when approached, overly
suspicious, fragmented speech/thinking
“Manic” Euphoric, irritable, accelerated,
hypersexual, reduced sleep

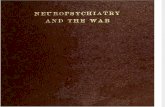
Flow Chart for Management of Aggression
Successful?
Employ nonpharmacologicprinciples
Identify ,most prominent neurobehavioral sx cluster match to relevant class
Depressive features Manic features Anxious features Psychotic features Aggression only
AntidepressantsAnticonvulsants
Lithium
AnticonvulsantsAntidepressantsAnticonvulsants
AnxiolyticsAntipsychotics
Empirical trials: blockers
•Anticonvulsants•Lithium
•Antidepressants•Atypicals
Yes
No
Continue treatment as appropriate
Effective? NoContinue as appropriate
Consider eventual empirical withdrawal Yes Adapted from Tariot et al; Ryan

Psychotropic Approach
• Careful diagnostic evaluation
• Use meds appropriate to your diagnosis
• Alter dosing strategy, accounting for heightened sensitivity to side effects